8 Collaborative approach to nursing
assessment and care planning
• To outline the different types of assessment and consider what is required for an effective holistic assessment
• To identify the advantages and disadvantages of the different resources that may be used to conduct an assessment
• To understand goal setting and a collaborative approach to care planning
Introduction
This chapter provides an overview of assessment and care planning in mental health nursing practice and examines ways in which you can develop your skills in this area during your practice placements. It introduces the concept of holistic assessment, considering some of the areas that this might cover. The section highlights the different types of assessment that may be used, resources for the collection of, and some examples of, questions you may want to ask. The chapter also reflects on the issues faced by mental health professionals when asking questions that they may find embarrassing or difficult. Risk assessment and management are addressed separately in Chapter 9.
Assessment provides the opportunity to develop an understanding of the person and to identify their needs, problems, strengths and goals. Following on from this it is essential to work with the individual and (where they are involved) their family in order to meet their needs, help them work towards dealing with their problems and realising their goals. This involves making sense of the information gained during assessment and using this to collaboratively develop a plan which will support this to happen. The last section will outline the process of planning care. It will also locate this in the context of the Care Programme Approach which provides the overarching framework for structuring assessment and care delivery in the UK.
Assessment
Assessment is an essential process within mental health nursing care. Participating in assessment enables the healthcare professional and the person in distress to identify and prioritise problems, strengths, needs and goals. It underpins the delivery of care and facilitates the decision-making process. As such, assessment forms an integral part of the nursing process (assessment, planning, intervention, evaluation). As Barker (2004) highlights, this involves aiming to gain an understanding of that person and their circumstances. In this respect, assessment should be a holistic process. This term is often used within nursing practice, however one of the criticisms levelled towards health care is that we don't always work with people holistically. In particular, mental health services have been criticised for tending to focus on problems alone without recognising people's strengths or the context in which they are managing their experiences. A holistic assessment will therefore explore and evaluate the resources an individual has, or has access to, and their environment. Who we are, the meaning and impact of any health-related problem may in part be influenced by our culture, sexuality and spirituality. Working with the ‘whole’ person therefore entails recognising and considering this.

In the early part of your placement, identify the assessment frameworks or tools that are used in your practice area. This may involve:
 Talking to your mentor about what frameworks or tools they use.
Talking to your mentor about what frameworks or tools they use.
Looking at blank assessment forms.
Accessing individuals’ multidisciplinary records (though it is important to bear in mind this may inform your perception of that person if you haven't already met them).
Review these frameworks in light of the list below. Do these attempt to collate holistic information? If not, what information are they attempting to gain? What areas are being assessed? You might also want to think about whether these link with any of the theories covered in Section 1.
This will help you gain some familiarity with the aims of some specific types of assessment and with their structure, which will be useful when you conduct assessments in your own practice.
Areas that may be covered within nursing assessment include the following:
• Social networks and relationships.
• Description of the problems that the person is experiencing and the impact they are having (this may be symptoms of mental distress but may also include, for example, housing, relationship or employment difficulties).
• Past history such as health problems (physical and psychological), life events.
• Strengths, e.g. previous successes and areas of interest or enjoyment.
• Ways the individual uses to cope with their experiences (coping strategies).
• Medication – history, current, concordance and side effects.
• Spirituality – spiritual beliefs and expression.
• Cultural beliefs and expression.
• Sexuality (or sexual health) – may include expression and impact of health problems and medication.
• Physiology, such as physical health, blood pressure, body mass index and physical expression of distress such as hyperventilation.
• Thoughts and emotions, e.g. thoughts about suicide or problems with mood.
• The individual's perception and meaning of their distressing experiences.
• Cognition – might include memory and orientation.
• Use of alcohol and illicit substances.
This is not a complete list but, as you can see, conducting a holistic assessment is extensive. It is important to consider this broad range of areas as this contributes to an understanding of that person and their context. It is also likely to facilitate a better informed, more accurate and therefore more effective process of making decisions, planning and delivering care. It also enables the health professional and person using the service to gain a picture of what is considered as ‘normal’ for that person in their life – a standard which is likely to differ for all of us. However, there are some challenges of examining assessment as a holistic process.
Gaining an understanding of people's experiences in their context (through holistic assessment) is important at whatever stage people come into contact with mental heath services and to recognise that circumstances will change. However, this may be more the focus of assessment when people are new to services, to that particular practice area or at a point before a change, such as discharge from a service or annual review.

Have a think about going to visit your GP for the first time, the first time you met your lecturer at university or when a new neighbour moved in next door.
1. How would you feel if these people were to ask you a question about each of the areas of your life identified above?
2. What would be informing how you responded to these questions?
This reflection may be useful to keep and revisit when you have observed and/or participated in an initial assessment. At this point, it may be useful to consider the following issues to help you develop a reflective practice.
According to the Oxford English Dictionary (Thompson 1996), to assess means to ‘estimate the size or quality of’. Assessment in health care is clearly an essential process to help identify what support people would most benefit from. However, it is essential to bear in mind that its very purpose is to make judgements and that conducting an assessment involves exploring areas of a person's world that may be quite private and that they may not have shared before. This process will be informed by the rapport that is developed with service users and the values and beliefs of the practitioner and their organisation. It is a clinical skill which must be developed and used with sensitivity.
Assessment is a dynamic and ongoing process. In this respect the aim and purpose of assessment may differ depending on what context and setting you are working with someone in. For example, assessment plays a vital role in the following:
• Finding out whether someone who comes to A&E having taken a paracetamol overdose is likely to repeat this and needs ongoing support or used it as an impulsive way of coping with a change in their life.
• Finding out in what situations someone's derogatory voices are triggered and the way that they deal with this.
• Identifying what impact the side effects of newly prescribed medication are having.
This highlights that it is really important to differentiate between assessment and admission or acceptance by a mental health team. During an admission or being taken onto a community nurse's case load, it will be essential to conduct an assessment. However, assessment is a continual process that happens in many different settings. Identifying the different types of assessment and how this is conducted by nurses in your practice area would highlight this and help you plan for how to contribute to mental health nursing assessments. This might be something you want to discuss with your mentor or a practitioner in a question and answer session to find out more about how assessment is conducted in your practice setting.
Types of assessment
Assessment is a process which will draw on all your senses as well as the therapeutic skills that a nurse develops. Effective and sensitive communication alongside being alert to non-verbal and environmental cues is important for all assessments. However, methods of conducting an assessment could be divided into three main groups:
Observation
This mode of conducting an assessment will entail gathering information that is observable. It can be informal such as taking into account the environment or a person's appearance (Ryrie & Norman 2009). How people act, communicate and express themselves can also be observed. In this respect, observation often informs assessments of behaviour. Physiological basic observations may also be considered under this type of assessment as they provide access to information about measurable changes in physiology such as blood pressure and blood glucose. Different levels of structured observations may be common within a range of in-patient settings such as acute care, forensic and child and adolescent. These are often used as tools or interventions to help manage risk. However, these can also operate to inform nursing assessment as during these periods staff will be observing, in particular, behaviour and communication. This can also help inform the assessment of risk.
The use of observation by looking at cues as to how individuals may present themselves, express themselves or their own environment is an assessment skill that you will be able to use in your placements throughout your training, if you are in the community, after you have been on a visit or if you are in an in-patient unit after spending one-to-one time with an individual. Consider the following:
1. What did you notice about the individual's body language and non-verbal communication (Sect. 1 and Ch. 7)?
2. What did you notice about the person's environment?
3. What might these have suggested about how they were feeling?
You may want to check these observations out with the nurse who you went on the visit with, a member of staff on the unit or the person's notes in order to get an insight into the ‘norms’ for that person and check out the accuracy of your observations. This could be something you document and communicate to other staff (all these processes could contribute to the achievement of your outcomes). It is also important to remember that our own norms and standards for environment may be different to what is a norm for another person.
Interviews
Interviews will involve gaining information from the individual and potentially others associated with their care through careful questioning and conversation. This tends to be a more formalised form of assessment where a professional will sit down with someone who uses services, skilfully ask questions and respond therapeutically to gain a picture of their current and past experiences. Clearly this is dependent on using interpersonal skills effectively and learning to really listen, so incorporates all those skills and approaches outlined in Chapters 3 and 7. Barker (2004) defines three different forms of interview and their role in assessment.
Descriptive
This includes gathering information to capture a broad overview of the person. It may also be helpful at initially establishing rapport and developing the therapeutic relationship. Open questions and statements alongside reflecting meaning back to people may be particularly helpful in this type of interview
Investigation
This relates to examining a specific area or problem in more depth. It may include considering connections between thoughts, feelings and actions. Additionally, gaining some estimate of scale can be helpful when exploring an issue in detail. This may include the impact it has on that individual's life or their perception of its severity. Questions which incorporate scaling, clarifying statements and closed questions can also be helpful communication skills to use here.
Ongoing
Barker (2004) describes the therapeutic value in regular and ongoing meetings. In terms of assessment, these can help to clarify difficulties, consider solutions, establish goals and review progress. Using solution- and strengths-focused questions (see following sections) and clarifying meanings can be useful in this area.
While it is helpful to think about the different types of interview situation and how these may be used, it is important to note that an interview may change between these different types and there is overlap between each.
Structured questionnaires
There is a broad and extensive range of structured assessment tools. These instruments use specific structured questions or rating scales to attempt to provide quantifiable information on an individual's experiences. In this respect they often result in a numerical value or judgement according to a specific level (e.g. high, medium or low). Questionnaires may ask people to respond in a yes/no fashion or determine frequency or intensity by asking for a rating in response to a series of statements. These tools are often thoroughly researched prior to publication and being made available for use in clinical practice. This means that the tools have been tested to see whether they measure what they are supposed to (validity) and are consistent in doing this (reliability). This type of assessment may also include tools used to examine a specific area such as a voice or activity diary.
Gamble and Brennan (2006) highlight that tools should be considered for how user-friendly they are, whether they are relevant to practice and easy to follow. This is important to remember, particularly as it is advised that some assessment tools require specific training. Training helps to ensure that the tool is used in the way it was intended and therefore that the reliability and validity are maintained. Additionally, some of the structured questionnaires can be quite technical or invasive in the questions that they ask and, therefore, using them requires this to be thought through and explored. Examples of questionnaire assessment tools include the following:
• Mini-mental State Examination – measurement of cognition and memory used in people with dementia.
• Liverpool University Neuroleptic Side Effect Rating Scale (LUNSERS) – used to measure side effects of antipsychotic medication.
• Becks Depression Inventory – used to rate low mood.
• Beliefs About Voices Questionnaire – examination of voice-hearing experiences and the individuals' perceptions of their voices.
Following on from the activity at the start of this chapter, identify what types of questionnaire tools are used in your practice area.
1. What are they designed to measure?
2. What is needed for their use, such as permissions, level of training?
3. When might they be used? This might be a stage in a person's care or in response to the identification of specific problems through other types of assessment.
4. What are the recommendations, if any, of how to respond to the results?
It may be helpful to talk to the staff in your placement area to answer these questions. As highlighted above, a number of the tools have also been researched so accessing published articles will also aid this.
Deciding on a type of assessment
Each approach to assessment has its strengths and limitations. As a practitioner you will be involved in using different types of assessment on different occasions. For instance, on an initial meeting with a service user, it may be most helpful to conduct an assessment via an interview to find out more about that person's difficulties, strengths and sources of support at the current time. This might indicate that experiencing anxiety is making it difficult for them to go out. At a further meeting, using a structured assessment tool can give you more information about the triggers and severity of their anxiety. If someone is acutely distressed and it is difficult for you both to find a common ground of verbal communication, assessment using observation may be most valuable. Gamble and Brennan (2006) warn of the dangers of using only one type of assessment as it is unlikely to be able to fully address the wide-ranging needs, wishes and strengths that an individual will have.
Each type of assessment has its advantages and disadvantages. For example, an interview assessment enables the service user to set the agenda and take more control within the assessment situation, yet it is a subjective process which may be influenced by the values and beliefs of the practitioner and therefore is harder to measure change over time. Structured assessments offer more consistent measures in this respect but may be limited in what information they provide about the context of individual's experiences. Additionally, Chapman and Chessum (2009) highlight that the language that is used in structured assessments may not be meaningful to all cultures.
Preparing for assessment
Assessment is an ongoing process which is a core part of mental health practice across a diverse range of settings. Engaging in an assessment can be the first time that an individual has had contact with mental health services and a mental health professional (Chapman & Chessum 2009). In this respect the assessment process could play a significant role in forming their future perceptions of that service. This highlights the importance of a sensitive and understanding approach. In order to aid this, it is helpful to think about some key areas which should be considered prior to conducting any assessment.
Where?
• Where will the assessment be conducted?
• Is this space confidential and private?
• Have potential interruptions been planned for and minimised?
• Is the room as comfortable as possible?
• How are the chairs positioned to facilitate communication?
• Are there any safety issues that need to be addressed (such as lone worker policy or positioning within the home environment)?
Who?
• Who needs to be involved in the assessment?
• Has consideration been given to gender, culture or personal preference?
• Does the person require any support or is there anyone they would like involved such as an advocate, peer support worker?
• Is there any indication that the assessment should be conducted by a certain discipline or whether it should be a joint assessment between services?
• Are there significant others involved as carers – is there a need for a carers' assessment?
• Has the person given consent for a student to be involved?
How?
Why?
• What is the purpose of the assessment?
• What information needs to be and should be examined?
• What will be done with this assessment information?
• What will it be judged against? How will this be evaluated?
This has provided an indication of some key areas that should be considered when conducting an assessment. It is proposed that asking these questions of yourself (and mentor) when involved in the assessment process will help enable the assessment to be as comfortable as possible for the person using services, but also ensure it is safe and effective.
It is important that you think about these issues when you are conducting assessments in placement settings. As this discussion has highlighted, you may be involved in using observation as an assessment skill. In conducting assessments, it is really helpful to observe different nurses conducting more formalised assessments (using questions or assessment tools) to reflect on the different approaches and skills that may be used effectively in assessment.
After this opportunity, consider what skills the professionals used? What did the person with mental health problems respond to most in the assessment?
In conjunction with your mentor, develop an action plan for how you can get involved in conducting assessments in your placement area. Depending on the stage of your learning and placements, this may include the following:
Contributing to a formal assessment by asking some questions in conjunction with a nurse.
Contributing to the interpretation and documentation of an assessment.
Leading an assessment with supervision/support from your mentor.
Producing an action plan for developing assessment skills on future placements.
Sources of information
Conducting an assessment requires consideration of the sources of information that will be used in order to gain an understanding of that person's experiences at that time. Most importantly this must begin with the person concerned. However, there are other important resources that can be helpful for the assessment. This will be both to gather data and make sense of this information. Table 8.1 outlines some examples of the other resources that a nurse might use in an assessment, and a brief overview of some of the issues that will need to be considered when using this information. You may want to add to the benefits and cautions outlined here.
Table 8.1 Sources of information for assessments
| Source | Benefits | Cautions |
|---|---|---|
| Family members, significant others and carers | They may know the person best and sometimes be able to recognise changes that the person doesn't | Their family member is their priority and accessing support can be difficult. These issues might impact on how people perceive a situation |
| Past structured assessments | These can provide some information against which current ratings may be compared | If the assessments have been conducted by different people there can be different interpretations of the ratings and, therefore, the measure is more subjective than it appears |
| Past running records/notes | This can provide detailed information about a person's situation and, through analysis, some insight into what may help people cope or cause them stress | These do not always provide an accurate picture and inaccuracies can be constantly repeated if this is the only source of information that is used |
| Other professionals that may have been working with that person | This may help to provide additional insights into specific areas of need or strengths that a person may have had. It may also help to gain a broader perspective and, in some circumstances, some facilitators for building a relationship | Interpretations may be subjective and informed by that person's beliefs and values |
Ideally, using a variety of resources assists in gaining a holistic view and will help inform any gaps in understanding that a person may not be able to share, such as when they were really unwell. There are challenges to this in terms of time, accessibility and resources. Nursing assessment has also been criticised for being too problem focused and requiring people to retell the same story (Watkins 2001), which highlights the importance of asking ourselves the questions of ‘why’ outlined above. This entails thinking about what information is needed and what might be the best source of information.
Assessment – some examples
The following part of this chapter provides some practical tools and information to help you start to get involved in the assessment process in your mental health placements.
This section examines using the interview approach to assessment. Here we highlight the different ‘types’ of question that can be used during interviews. Below are some examples of different forms of questioning style.
Rating questions
• On a scale of 1 to 10, with 1 being the worst, how has your anxiety/voices/mood been today?
• On a scale of 1 to 10, with 1 being the worst, where would you like your anxiety/voices/mood to be next month?
• How effective has that way of dealing with your distress been for you? Would you say it has been high, medium or low?
Varying the types of questions used can take time and practice to build to using as a skilful approach. However, using open, closed and clarifying questions appropriately creates space for the person to share their thoughts, feelings and emotions but ensures you have an opportunity to clarify your understanding and interpretation of this. Rating questions can be really useful when people may struggle to verbalise some of these thoughts and feelings as well as providing an opportunity to start moving towards goal planning and setting. These rating questions are informed by a solution-focused brief therapy approach (see Ch. 6 for more details). Clearly conducting an assessment also involves using the other interpersonal skills that you have learned to respond to the individual.
Biographical narrative
This is an approach most commonly used in working with older adults. It focuses on the person's story and getting to know the whole person, moving beyond their identity as a ‘patient’. This can be particularly important when working with people diagnosed with dementia and is influenced by Tom Kitwood's theories on ‘personhood’ and dementia (Kitwood 1997). He highlights the basic psychological needs of all human beings and that the individual's personality and biography will influence their experience of dementia.
Conducting a biographical narrative with a person within the context of a therapeutic relationship involves enabling them to tell their story. Therefore, during one-to-one sessions with the individual you would use open and unstructured prompts to help them tell their narrative and share what they perceive as important. For example, ‘Tell me about your life, the things that stand out and are important to you’.
This might be something that you record in a written form with the person but may use more creative methods such as scrapbooks or photographs (this also shares some similarities with life story work). Photographs and memorabilia may be used as prompts for storytelling. Narrative in this respect can act as a therapeutic approach or intervention alongside providing a resource for assessment.
For example, Ray is on an assessment ward for older people. He wakes in the middle of the night at the same time every night and tries to get in to make a drink. He gets frustrated and verbally aggressive when the nurse guides him away from the kitchen. Through doing a biographical narrative with Ray, his key worker discovers that he was a night worker and that the time he wakes up reflects the break time during his shift.
This example highlights the potential impact of conducting a biographical narrative. Underpinned by the interpersonal skills examined in this book and with the support of your mentor, biographical narrative is an approach you might want to be involved in when in settings with older persons.
Asking the embarrassing questions
The chapter started by highlighting the importance of conducting a holistic assessment. Previously, services have been criticised for overlooking core parts of people's identity and experience within the assessment process, therefore failing to consider the impact of these on their lives. The areas that are often overlooked relate to people's spirituality, culture and sexuality (these are examples; there may be others). Some of the reasons that it may be difficult to explore these issues are that they are areas which may be more hidden, that we may not be used to sharing or talking about except with those whom we are very close to. It is also difficult to define what is meant by some of these terms.
Some of the ideas that people have when thinking about being ‘a nurse’ might involve thinking about the physical closeness and invasive techniques that this involves. However, as a mental health nurse, sometimes there are more implications for this in terms of the emotional and psychological closeness and invasiveness that this entails. We may be privy to the thoughts and feelings people have that they may not have shared with anyone, or only those very close to them. In this respect it is essential that these complex areas are handled with sensitivity in a way that respects the person's dignity. However, this also involves a recognition of the significance of these aspects of people's identity and the impact that mental health problems and using mental health services can have on these areas.
Outlined below are some suggestions for consideration in approaching topics or questions that may be perceived as sensitive by you or the person using the service.
Language
It is important to try and mirror the language that a person uses to describe a particular issue or experience. This not only demonstrates you are actively listening but also that you are respecting their values and beliefs in relation to the particular issue. There may be limits to this if derogatory language is being used.
Timing
This can be a difficult thing to judge and is often something that may be easier over time (though even experienced professionals may misjudge from time to time!). Clearly it also depends on the context in which you are engaged in the assessment as to how much flexibility there is on the time for asking more sensitive questions. It is important to respond to the verbal and non-verbal cues from the person but it may be that some people feel they can be more open about these issues when they have had the opportunity to get to know you and build a rapport. This can mean it can be important to revisit these areas in later assessments. However, it also involves recognising that people make choices not to discuss these areas.
Your own views
Using some of the skills of self-awareness explored in Chapters 5 and 7, it is important to reflect on how you feel both about asking questions which may relate to sensitive topics and about those topics themselves. What are your beliefs in relation to these areas and what if any prejudices or stereotypes may you have? Reflecting on how you feel about asking questions about such issues is important and it's not uncommon to feel embarrassed, especially to begin with, to ask sensitive questions. In managing this feeling, it is important to use the sources of support and forums of reflection that you have available to you, such as supervision. There will also be times when it is appropriate to share this feeling, reflecting congruence within your personal interaction. Here is an example of how this may be phrased sensitively:
This question is sometimes awkward for people to answer and I find it a bit awkward to ask but it's an important part of getting to know you. I also want to make sure that you have the space and opportunity to share with me anything that you feel is important for me to know in relation to/for our continued work together.
It also important to recognise that how we feel about a particular issue may inform some assumptions that can be made about how other people might feel, for instance being embarrassed to ask a question doesn't always mean that someone will find it embarrassing to answer and vice versa.
There may also be other questions or topic areas that you find difficult to ask about, particularly when first getting involved in the assessment process. These often relate to areas of ‘risk’ such as asking people about whether they have ever had thoughts about harming themselves or have ever made an attempt on their life. It is an important part of the risk assessment process to explore these areas and people can appreciate sharing these thoughts with someone who understands and doesn't judge them. Some of the suggestions offered above may also help you think through how to approach an assessment of these areas.
It is important that you talk these issues through with a mentor exploring what their perspective is on whether it would be appropriate for you to get involved in this in relation to the people you are working with on your placement.
Summary
In summary, therefore, for this part of the chapter we can consider the following:
• Conducting an assessment with a service user is a complex and important area. Its aim is to gain an understanding of that person in the context of their life and circumstances; to get to know the person and inform the nursing process of planning and delivering care.
• There are different types of assessment and a range of resources that may be used. The process has potential to be uncomfortable and invasive for the service user and must be approached sensitively in order to establish rapport and ensure the person's dignity is respected.
• It is also important to highlight that the line between assessments and delivering care is blurred. Through the assessment process, the mental health nurse invests in establishing rapport and building the therapeutic relationship.
• Additionally, some approaches that may be used during an assessment can have therapeutic benefit themselves, such as the narrative approach or rating questions. However, it is essential that a focus is maintained on what happens to the information once an assessment is conducted and how to make sense of the information to plan and deliver care. This is the focus of the next section.
Planning for collaborative care
Care programme approach
In the advent of community care (see Ch. 1), the Care Programme Approach (CPA) was introduced by the Department of Health (DH; 1990) to promote a more integrated system to ensure that the different community services involved in a person's mental health care are coordinated and work together. The CPA framework outlines the requirements of health and social services to provide the following (Care Program Approach Association 2010):
• Assessment: to conduct systematic assessment of health and social care needs for people in secondary or specialist mental health services.
• Care plan: to develop a care plan which addresses these identified needs.
• Care coordinator: to identify a person responsible for keeping in touch with the individual, coordinate and monitor care.
• Review: to provide regular review and evaluation of care, changing the care plan as agreed.
Assessment, care planning, care coordination and review are therefore viewed as the ‘cornerstones’ of the CPA (Care Programme Approach Association 2010). Over the past 20 years there have been a number of amendments at a policy level that have led to adaptations in the structure and language of the CPA process.
The CPA was modernised further by the Department of Health in 1999. This included increased emphasis on risk assessment and a requirement that the CPA include crisis and contingency plans. It also integrated the process of case management in the community with the CPA approach (DH 1999).
A partnership approach to the CPA is integral. The CPA has brought together systems within health and social care. As the CPA is one of the main frameworks for care delivery in adult mental health, a key part of the partnership approach is those that are built with service users and carers (DH 2006). However, the CPA has been criticised for failing to realise its aims in this area. It has been seen to be too problem focused and research has suggested many service users remain unaware of the existence of their CPA care plan (Rose 2003). These concerns prompted a review of the CPA and the introduction of new CPA policy in 2008 (DH 2008). Refocusing the Care Programme Approach (DH 2008) promotes a more service user-centred philosophy and suggests the CPA has to be underpinned by recovery and social inclusion. This involves working towards strengths and goals alongside addressing needs and difficulties. It also highlights the need to help people maintain control over their own support.
Role of the care coordinator
A range of different mental health professionals can be care coordinators. Psychiatrists might be care coordinators to a large number of individuals but often manage this through seeing them as out-patients. If people have complex needs or need input in a number of different areas of their life, they may be referred to secondary mental health services and be allocated a care coordinator who is most commonly a mental health nurse or a social worker but who may also be an occupational therapist.
This key role involves developing and sustaining a therapeutic relationship with service users, liaising with other professionals and services, conducting assessments, delivering care and support but also coordinating the support delivered by others. Working in this way often involves adopting a case management approach (as highlighted by the amendments to the CPA policy in 1999). This is discussed in more detail in Chapter 15.
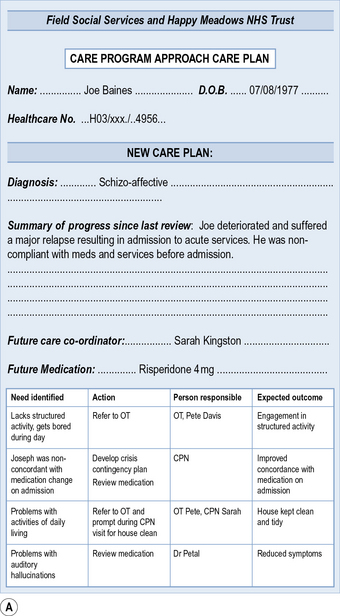
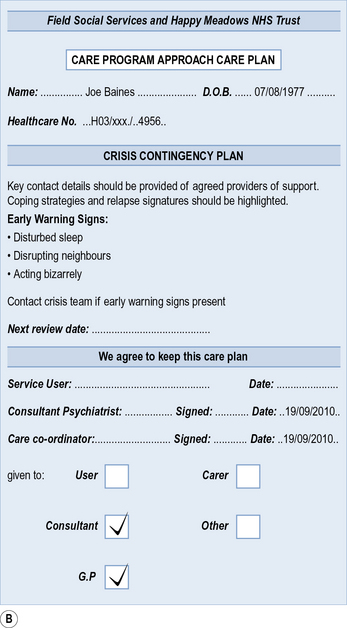
Figure 8.1 is an example of a completed CPA care plan. Have a look at this care plan and think about what you notice. Are there any problems with it?
Have a look at the CPA care plan in Figure 8.2, completed about the same person in exactly the same set of circumstances. What differences do you notice from the first one? In particular, think about:
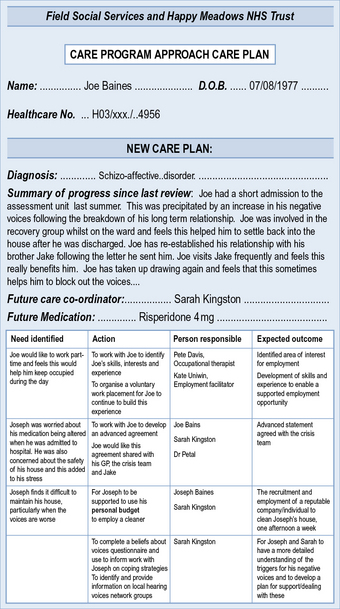
How does this compare to the CPA care plans you have seen on placement?
Planning care
A care plan provides an account of the work that the service users and the professionals supporting them will undertake to meet the individuals’ needs and achieve their goals. It is described as the next stage in the caring process following assessment and diagnosis of problems and needs (Leach 2007). In this respect it should be based on an interpretation of the information gained during assessment. Well written care plans can aid continuity of care, facilitate interdisciplinary working and consistency between care providers. CPA provides one of the core frameworks for care planning and, in some services, this may be the only care plan that underpins care. However, in some areas where guidance is required on the short-term aims and direction of care (such as in-patient services), additional care plans will be developed.
The process of developing a care plan helps to (Callaghan 2006, Gega 2009):
– identify and clarify actions or interventions needed to reach a goal or address a problem
– develop and articulate a shared understanding between the nurse and the person on what needs/goals can be met and the priority of these
– set measures for how progress towards achieving these can be measured, therefore agreeing outcomes.
Care plans should be developed in collaboration with the service user and reflect their priorities and wishes (DH 1999, Rogers 2000). In this respect, care plans should be individualised. It makes sense that any plan of action is more likely to be successful if it reflects something that the individual would like to achieve. This level of ownership can help foster individual autonomy and taking on greater responsibility. However, there are times when this level of collaboration is challenging, in particular if an individual is severely distressed or the plan relates to an issue defined as a problem by professionals or society rather than the individuals themselves, such as the management of certain risks. Rogers (2000) highlights that it is essential that these management plans do not replace collaboratively agreed care plans. Additionally, it is important that service users are given ongoing opportunities to be involved in planning their care if they are too distressed at certain times. There is also opportunity to be creative about how we access people's thoughts about their care and goals, such as for people who may find it difficult to verbalise their wishes at some points, providing them with the opportunity to write this down or express it in other ways. It may also involve changing language and amending the way in which problems are expressed (Gega 2009).
Before the care plan can be developed, the nurse and the service user need to agree the priority of needs and goals in order to plan. Having too many care plans can create confusion for the person and services, making ineffective use of resources and reducing the impact of the plan on patient care.
Care plans start with a statement which may be expressed as a problem, need or goal (Bauer & Hill 2000), such as:
Joan states that she benefits from medication and is happy to take it. However, she is regularly forgetting to take her medication as prescribed, inhibiting its therapeutic effect. Joan needs to take her citalopram 20 mg every morning.
Problem: Leon feels isolated and identifies this contributes to his low mood.
Goal: For Leon to reduce his feelings of isolation by joining the lost ramblers group.
These statements may represent a plan to move towards a more long-term goal, for instance Leon's long-term goal might be to meet a partner or have a wider network of friends. It is important to highlight these plans as part of a long-term goal.
The statement of a problem or goal is followed by an outline of the objectives, which break this problem or goal down into more specific details. Objectives should be SMART: specific, measurable, achievable, realistic and time orientated. This is often best achieved by keeping things simple, having a plan that addresses one problem or goal:
Plan: For the next 7 days Joan will set her mobile phone alarm reminder every evening to alert her to take her citalopram the following morning.
Plan: Joan's keyworker will provide Joan with a tick chart in order to record when she has taken her tablet (by next visit).
This may be a useful prompt when writing, reviewing and evaluating care plans during your placements. It may be possible to contribute to the care plan process by, for instance, reviewing and evaluating a plan with a service user you are working with.
In this example the person responsible and the expected time has been included in the statement of objective, making it clear who is responsible and when the objective is expected to be achieved. It can take practise to develop objectives that are specific and measurable, particularly given that the nature of problems or the support required to reach goals may be complex.
Care plans therefore need to outline the action required to reach goals or address problems, resources that will be required, who is responsible for this, how and when progress towards this area will be monitored. This last point also highlights the importance of evaluating care plans. All plans should include the measurement of achievement within that plan and the date at which that measurement will be evaluated. This evaluation has to be documented within multidisciplinary team records and on the plan itself. It is also important that the essential requirements of record keeping are attended to when documenting a care plan, including the person's name and healthcare number, the signature and discipline of the person writing the care plan and the signature of the person whose care plan it is.
The overview of the care planning process given here has provided an insight into how care plans may be structured and developed. It has outlined the importance of ensuring this is a collaborative process and that care plans are driven by the individuals’ goals and the process of assessment. Transferring the care plan into action is the next part of the process and, for this to be successful, effective communication, negotiation, team-working and leadership skills may be required. Leading and managing care are explored in Chapter 14.
Barker P. Assessment in psychiatric and mental health nursing. In search of the whole person, 2nd ed. Cheltenham: Stanley Thornes; 2004.
Bauer B., Hill S. Mental health nursing: an introductory text. Philadelphia: WB Saunders; 2000.
Callaghan P. Essential mental health nursing skills. In: Callaghan P., Waldrock H. Oxford handbook of mental health nursing. Oxford: Oxford University Press, 2006.
Care Programme Approach Association. About the Care Programme Approach. Online. Available at: http://www.cpaa.org.uk/thecareprogrammeapproach, 2010. (accessed June 2011)
Chapman J., Chessum C. Fundamental skills of mental health nursing. In: Clarke V., Walsh A. Fundamentals of mental health nursing. Oxford: Oxford University Press, 2009.
Department of Health. Caring for people. The Care Programme Approach for people with a mental illness referred to specialist mental health services [Joint Health/Social Services Circular. C(90)23/LASSL(90)11] Department of Health, London, 1990.
Department of Health. Effective care coordination in mental health services: modernising the Care Programme Approach. London: HMSO; 1999.
Department of Health. Reviewing the Care Programme Approach 2006: a consultation document. London: HMSO; 2006.
Department of Health. Refocusing the Care Programme Approach; policy positive practice guidance. London: HMSO; 2008.
Gamble C., Brennan G. Working with serious mental illness: a manual for clinical practice, 2nd ed. Edinburgh: Elsevier; 2006.
Gega L. Problems, goals and care planning. Norman I., Ryrie I. The The art and science of mental health nursing. A textbook of principles and practice, 2nd ed., London: Open University Press, 2009.
Kitwood T. Dementia reconsidered: the person comes first. Maidenhead: Open University Press; 1997.
Leach M. Planning: a necessary step in clinical care. Journal of Clinical Nursing. 2007;17:1728–1734.
Rogers P. Forensic nursing. In: Newell R., Gournay K. Mental health nursing: an evidence-based approach. Edinburgh: Churchill Livingstone, 2000.
Rose D. Partnership, coordination of care and the place of user involvement. Journal of Mental Health. 2003;12(1):59–70.
Ryrie I., Norman I. Assessment. Norman I., Ryrie I. The art and science of mental health nursing. A textbook of principles and practice, 2nd ed., London: Open University Press, 2009.
Thompson D., ed. Oxford compact English dictionary. Oxford: Oxford University Press, 1996.
Watkins P. Mental health nursing. The art of compassionate care. Edinburgh: Butterworth Heinemenn; 2001.
The Care Programme Approach Association: http://cpaa.co.uk/thecareprogrammeapproach (accessed June 2011).
Department of Health: Effective care coordination in mental health services: modernising the Care Programme Approach – a policy booklet. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4009221 (accessed June 2011).