21 The Abdomen of the Horse
CONFORMATION AND SURFACE ANATOMY
Like other herbivores that subsist on a diet rich in roughage, the horse has a capacious gastrointestinal tract and a correspondingly bulky abdomen. However, the extent of the abdomen is not immediately apparent because a large part is concealed within the rib cage. The olecranon and the lower end of the sixth rib are handy guides to the most cranial extent of the diaphragm (see Figure 20–3). The flank is reduced in size by the caudal inclination of the ribs, the last of which may be within a few fingerbreadths of the coxal tuber (see Figure 22–25, A/1″,3).
Abdominal conformation varies much with age, condition, and the amount and nature of the rations. The ventral contour is especially variable; it slopes gradually between the sternum and the pubic brim in animals in hard condition but dips to reach its lowest point behind the xiphoid process in those in softer condition, in pregnant mares, and in ponies generally. In the latter groups the most caudal part of the floor ascends very steeply. These differences are not always obtrusive because the most caudal part of the abdomen is covered laterally by the skin fold that passes between the flank and the thigh (Figure 22–23/6) and ventrally by the prepuce or udder.
The trunk is broadest at the last ribs. The upper part of the flank sinks in to form a paralumbar fossa, but the relative shortness of the region behind the ribs makes this feature much less obvious than in cattle. The lower part of the belly is rounded from side to side, except in foals, in which the whole abdomen is slab-sided and shallow (see Figure 23–2). The usual symmetry may be disturbed in late pregnancy or by accumulation of gas in parts of the gastrointestinal tract.
The position of the last rib is often visible, but most other skeletal boundaries of the flank and floor are less easily found. The transverse processes of the lumbar vertebrae are usually too deeply buried under muscle to be palpable. The dorsal part of the coxal tuber is very conspicuous, but the ventral part, which gives origin to the internal oblique and tensor fasciae latae, is not visible, although it is easily palpable.
Soft features that may be recognized include the internal oblique muscle, which raises a ridge along the caudoventral boundary of the paralumbar fossa (Figure 21–4/b) and the superficial thoracic (“spur”) vein, which runs over the ventral part of the abdominal wall toward the axilla, following the dorsal border of the deep pectoral muscle. The subiliac lymph nodes can usually be identified and rolled below the fingers; they are arranged in a spindle against the cranial margin of the thigh, midway between the coxal tuber and patella. They are more easily found if drawn forward. The superficial ring of the inguinal canal can be found on deep palpation of the groin, which is a procedure sometimes resented and therefore to be performed with care (Figure 21–4, A/3).
THE VENTROLATERAL ABDOMINAL WALL
STRUCTURE
The skin is thick over the flank but thins ventrally, particularly in heavy draft animals. It is especially thin in the cleft between the abdomen and thigh where it is sparsely haired and glistens with the secretion of the sebaceous glands concentrated here. In contrast, sweat glands are most abundant over the flank.
A large subcutaneous bursa, a postnatal development, is present over the coxal tuber. Elsewhere the skin is closely adherent to the cutaneous trunci, which cover most of the flank, though not the abdominal floor. The upper border of the cutaneous muscle follows a line drawn from the withers to the stifle. The muscle is thickest cranially where it extends into the fascia over both the lateral and the medial aspects of the shoulder and arm. Caudally, it continues within the flank fold to end on the lateral femoral fascia. The cutaneous muscle is employed to twitch the skin to dislodge flies and other irritants. No detached bundles are associated with the prepuce, as in many species.
The loose fascia deep to the muscle conveys the cutaneous nerves and superficial vessels and encloses the subiliac lymph nodes.
The deeper fascia consists largely of elastic tissue and, being yellowish, is also known as the tunica flava. It is well adapted to the passive support of the viscera and is thickest ventrally, where the burden is greatest. The dorsal part is easily dissected from the underlying muscle, but its ventral part exchanges fibers with the aponeurosis of the external oblique and is more tightly adherent. Bands detached from the tunic help support the prepuce or the udder. Careful suturing of this layer is necessary after abdominal surgery because its elastic nature tends to evert and draw apart the edges of a wound in the underlying muscle.
Before considering the muscles of the abdominal wall, it is necessary to pay attention to the linea alba and prepubic tendon since these and the associated structures have a particular importance in the horse. The linea alba, mainly formed from the aponeuroses of the flank muscles, is considerably strengthened by longitudinal fibers. It is unequally developed along its length, being widest where it carries the umbilical scar (see Figure 21–1/d). It finally combines with the insertion tendons of the right and left rectus abdominis muscles to form a broad plate.
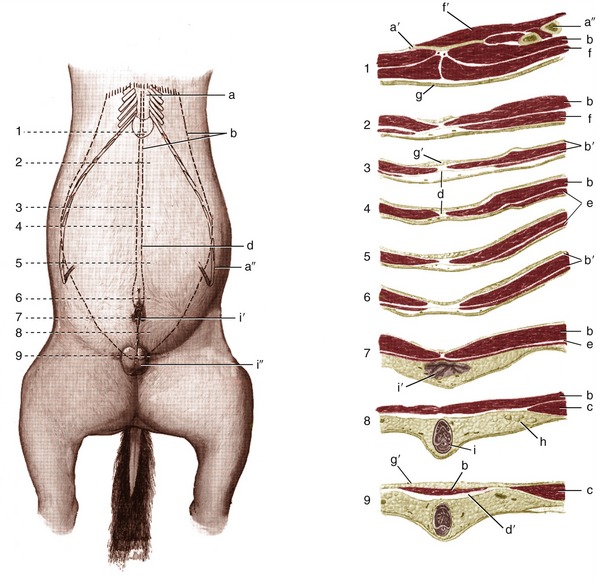
Figure 21–1 Changes in the structure of the abdominal floor shown by means of a series of transverse sections (1–9) of a gelding. a, Sternum; a′, xiphoid cartilage; a″, costal arch; b, rectus abdominis; b′, rectus sheath; c, internal oblique; d, linea alba; d′, prepubic tendon; e, cutaneous trunci; f, pectoralis ascendens; f′, diaphragm; g, skin; g′, fat; h, superficial inguinal lymph nodes; i, penis; i′, prepuce; i″, scrotum.
This may be regarded as the initial formation of the prepubic tendon* through which the abdominal muscles find attachment to the pelvic skeleton (Figure 21–2/5). Once formed, the tendon ascends almost vertically toward the pelvic brim, but before reaching this, it is augmented by a strong transverse thickening. This thickening is mainly formed by the tendons of origin of the pectineus muscles (of the thighs), which arise from both the ipsilateral and contralateral pubic bones (from and medial to the iliopubic eminences) and which thus partly decussate across the midline. Additional but lesser contributions to the prepubic tendon are made by the caudal margins of the oblique abdominal muscles and the cranial part of the gracilis. A feature of great interest, peculiar to the horse, is the detachment from the caudolateral aspects of the prepubic tendon of the stout rounded cords that furnish accessory ligaments to the hip joints (Figure 21–2/5′ and Figure 21–1). Each accessory ligament crosses the ventral surface of the pubis, heading toward the acetabulum, which it enters through the notch in the rim; it ends by inserting on the head of the femur beside the intracapsular ligament (of the head of the femur) that is found in all species. Each accessory ligament is predominantly composed of fibers from the two rectus muscles, and many fibers have decussated from the contralateral side. The ligaments appear to be the principal insertions of these muscles. Their existence partly explains the restrictions on the movements permitted at the equine hips. It is postulated that the accessory ligaments are tensed by the weight of the abdominal contents and that this tension helps secure the femoral heads in place.
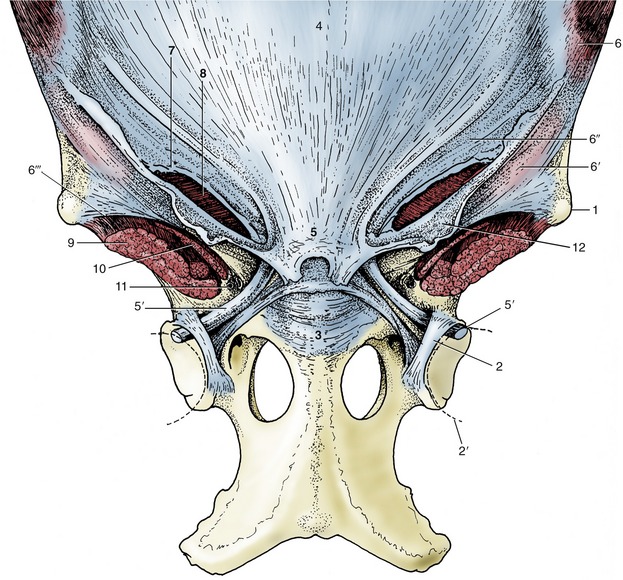
Figure 21–2 The attachment of the abdominal muscles on the pelvis and the prepubic tendon. 1, Coxal tuber; 2, transverse acetabular ligament; 2′, femoral head; 3, pubis; 4, tunica flava over linea alba; 5, prepubic tendon; 5′, accessory ligament; 6, external abdominal oblique; 6′, 6″, pelvic and abdominal tendons of external oblique aponeurosis; 6′″, attachment of pelvic tendon of external oblique aponeurosis on sartorius and iliopsoas (“inguinal ligament”); 7, superficial inguinal ring; 8, internal abdominal oblique; 9, iliopsoas; 10, sartorius; 11, vascular lacuna containing femoral vessels; 12, femoral fascia (lamina).
Since the main weight of the abdominal organs is carried by the prepubic tendon, it follows that its rupture has the most dire consequences. This mishap, fortunately rare, is for obvious reasons most common in heavily pregnant mares.
The external abdominal oblique (Figure 21–4/1) is the most extensive muscle of the flank. It arises from the thoracolumbar fascia and also from the lateral aspect of the thoracic wall (from the fifth rib caudally) by a series of digitations that engage with those of the serratus ventralis. The majority of its fascicles run caudoventrally to a broad aponeurosis that succeeds the fleshy part of the muscle along a line that sweeps from the coxal tuber toward the ventral end of the fifth rib.
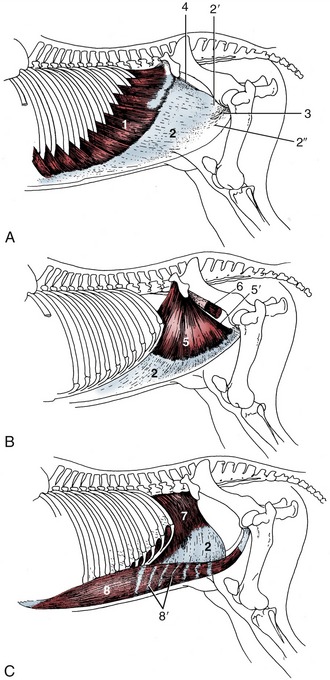
Figure 21–4 The abdominal muscles and their skeletal attachments. 1, External abdominal oblique, muscular part; 2, aponeurotic parts of 1, 5, and 7; 2′, 2″, pelvic and abdominal tendons of aponeurotic part; 3, superficial inguinal ring; 4, attachment of pelvic tendon of external oblique aponeurosis on iliopsoas and sartorius (“inguinal ligament”); 5, internal abdominal oblique, muscular part; 5′, free caudal border forming the cranial margin of the deep inguinal ring; 6, iliopsoas, partly enclosed by iliac fascia; 7, transversus abdominis, muscular part; 8, rectus abdominis; 8′, tendinous inscriptions.
Before insertion, the aponeurosis splits into (1) a large abdominal tendon that continues over the rectus to reach and insert on the linea alba and (2) a small pelvic tendon that inserts on the coxal tuber, the fascia over the iliopsoas and sartorius muscles, and the prepubic tendon (see Figure 21–2). The split between the two tendons constitutes the superficial ring of the inguinal canal (Figure 21–4/3). (The margins of the tendons are known as crura where they bound the opening, but the term is often misapplied to the tendons themselves.)
The unnecessary term inguinal ligament confuses many descriptions of these structures. It is sometimes specifically applied to the thickened caudodorsal edge of the pelvic tendon. In fact, the prominence of this edge (Figure 21–4/4) owes less to thickening than to tension through its connection with the fascia covering the iliopsoas and sartorius.
The internal oblique muscle (Figure 21–4/5) radiates from an origin concentrated on the coxal tuber but extending onto the dorsocaudal edge of the pelvic tendon of the external oblique. Most bundles run cranioventrally to insert on the last costal cartilages or, via an aponeurosis that fuses with that of the external oblique, into the linea alba. Some pass ventrally and caudoventrally, and these cover the superficial inguinal ring on its internal aspect (Figure 21–5/4). A caudal slip provides the cremaster, which passes onto the spermatic cord. The junction of the fleshy and aponeurotic parts of this muscle occurs more than halfway down the abdominal wall.
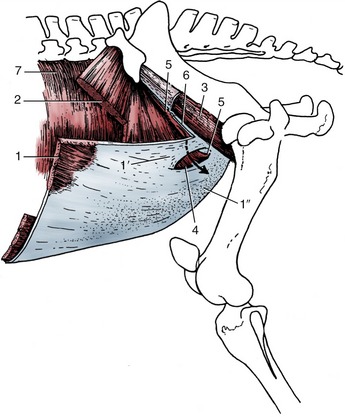
Figure 21–5 The muscles of the inguinal region. The arrow passes through the inguinal canal. 1, External abdominal oblique; 1′, 1″, pelvic and abdominal tendons of external oblique aponeurosis; 2, internal abdominal oblique; 3, iliopsoas partly enclosed by iliac fascia; 4, superficial inguinal ring; 5, cranial border of deep inguinal ring; 6, attachment of pelvic tendon of external oblique aponeurosis on iliopsoas and sartorius (“inguinal ligament”); 7, transversus abdominis.
The transversus abdominis (Figure 21–4/7) takes origin from the lumbar vertebrae and the medial aspect of the last ribs, ventral to the origin of the diaphragm. The fleshy part is continued by an aponeurosis that passes deep to the rectus abdominis to reach the linea alba. The transversus, the least extensive of the three muscles of the flank, does not extend caudal to the level of the coxal tuber; the internal lamina of the rectus sheath is thus deficient caudally.
The rectus abdominis (Figure 21–4/8) arises from the fourth to ninth costal cartilages and the adjacent part of the sternum. It inserts by way of the prepubic tendon and accessory ligaments. The muscle, relatively narrow over the thorax, widens considerably over the abdomen before again narrowing toward its insertion (see Figure 21–1/b).
Although the functions of the abdominal muscles are the same in all species, the expiratory role is relatively more important in the horse because the elasticity of the lungs is frequently reduced in older horses (resulting in heaves). Contraction of the abdominal musculature is then more necessary to return the viscera, and thus the diaphragm, from the inspiratory position. In this action the junction between the fleshy and aponeurotic parts of the external oblique muscle becomes visible as the so-called heave line.
The fascia that supports the peritoneum is often heavily but unequally infiltrated with fat. This layer, which may be 6 cm or more thick in horses in good condition, must be taken into account when making and closing a surgical incision.
THE INGUINAL CANAL
The inguinal canal follows the general pattern but merits a full description because of its relevance to castration, which is performed on the vast majority of male horses. It is the opening in the caudal part of the abdominal wall through which the testis travels in its descent into the scrotum, which is a process usually completed shortly before or shortly after birth in this species. The canal contains the spermatic cord of the colt and stallion; a stump frequently remains in the gelding. In addition, the external pudendal artery and the genitofemoral nerve travel through the canal.
The term inguinal canal suggests a roomier passage, but the canal is no more than a potential space between the flesh of the internal abdominal oblique and the aponeurosis of the external abdominal oblique. The entrance (deep inguinal ring) lies along the free caudal edge of the internal abdominal oblique muscle, which determines its oblique orientation (Figure 21–5/5); the origin of the internal abdominal oblique from the external abdominal oblique and the convergence of the two muscles on the lateral edge of the prepubic tendon determine its length (generally ca. 15 cm).
The exit (superficial inguinal ring), between the two tendons into which the external oblique aponeurosis splits, is more or less horizontal (Figure 21–5/4). It is limited laterally by the exchange of fibers between the two tendons where they part company and medially by the tendons meeting and fusing with the edge of the prepubic tendon. The margins of the opening are less clearly defined than many accounts suggest. The lateral (dorsal) crus gives origin to the external spermatic fascia and femoral lamina, which appear to continue the lateral crus directly (see Figure 21–3). The medial (ventral) crus is somewhat frayed but can be identified on palpation through the skin. This is best performed by placing the palm against the belly and advancing the fingers into the cleft between the thigh and abdominal wall. The lateral crus is passed unnoticed, but the medial crus is recognized as a firm edge. The fingers pass into the outer part of the canal most readily with the thigh abducted (when the femoral fascia [lamina] draws the lateral crus outward). It follows from the orientation of the deep and superficial rings that the canal has a triangular outline; it is relatively long cranially and very short caudally where the two openings butt against the prepubic tendon (see Figure 21–5).
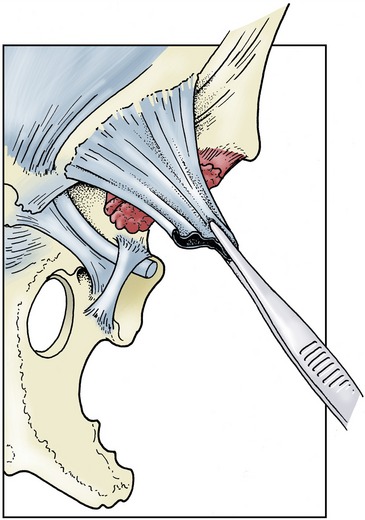
Figure 21–3 The origin of the external spermatic fascia and femoral lamina from the margin of the superficial inguinal ring. (See Figure 21–2 for orientation.)
The peritoneal sheath (vaginal tunic) of the spermatic cord contains a cavity that places the space about the testis in free communication with the peritoneal cavity of the abdomen. The communication occurs through the vaginal ring (ca. 3 cm long) situated midway in the deep inguinal ring (see Figure 22–19/10 and Figure 22–24, A-B); the vaginal ring, with the constituents of the spermatic cord converging on it, can be identified per rectum in the stallion. The vaginal cavity provides a possible route for the herniation of intestines that may even reach the scrotum. This occurrence (indirect inguinal hernia) is a comparatively common sequel to castration. Direct inguinal hernia, in which a loop of intestine forces an entry into the canal beside the vaginal tunic, is rare in horses.
Incomplete descent of one or both testes (cryptorchidism) is common in the horse (p. 579). The testis may be retained within the abdomen or may enter but fail to leave the canal. Surgical correction may be indicated. It is therefore necessary to be aware that while the spermatic cord occupies a central position within the canal, the external pudendal artery, which must be treated with respect, occupies the caudomedial corner. The artery is accompanied by the genitofemoral nerve and a small vein; the larger (accessory) external pudendal vein makes a separate passage between the pectineus and gracilis muscles.
INNERVATION AND VASCULARIZATION
The segmental innervation of the abdominal wall corresponds to the common pattern, and the minor variations are of little importance because paravertebral anesthesia is rarely practiced in the horse. The vascularization also follows the common pattern in the main. Mention may be made of a cranial branch of the deep circumflex iliac artery, which extends forward from the region of the coxal tuber between the muscles of the flank; it is susceptible to injury during surgery in this region. The artery of the right side is also at risk in trocarization, which is occasionally performed to relieve tympany of the cecal base. The abdominal floor and lower flank are served in the usual way by the cranial and caudal epigastric arteries and their superficial branches. Paradoxically, these vessels are at less risk when the classic procedures are employed than in laparoscopic surgery in which stab wounds are blindly made to create the necessary instrument portals. No warning of the exact position of the vessels is available, and should vascular damage occur, control of the resulting hemorrhage may be troublesome and time-consuming. It is said that the caudal epigastric artery is the vessel most often traumatized. The superficial thoracic or spur vein runs toward the axilla in the superficial fascia at the ventral edge of the cutaneous muscle. Connections with tributaries of the external pudendal vein make it available as an alternative drainage route from the prepuce or udder.
GENERAL ASPECTS OF ABDOMINAL TOPOGRAPHY
The influences on abdominal topography common to all species have been discussed (p. 123). The horse is prone to adhesions of the peritoneum especially after abdominal surgery.
Except in advanced pregnancy, when the uterus has an even greater influence, the topography of the equine abdomen is dominated by the large intestine. The cecum and ascending colon are the seat of the microbial fermentation that makes the cellulose constituents of the diet available, and their significance is therefore comparable to that of the forechambers of the ruminant stomach. The large intestine is so voluminous that it is almost always encountered immediately when the abdomen is opened, whether the incision is made in the flank or in the floor. Its disposition is complicated, and although it is necessary to give a systematic account of each individual part, a first impression may be obtained from such illustrations as Figures 21–6, 21–7, and 21–10).
THE SPLEEN
The spleen lies within the left dorsal part of the abdomen where it is largely, if not wholly, protected by the most caudal ribs, from which it is separated only by the diaphragm. The broad dorsal base lies under the last three ribs, although a small corner may project against the flank. The pointed ventral apex reaches forward to about the ninth or tenth rib, a handbreadth above the costal arch (Figure 21–6/4). The cranial margin is concave, the caudal margin is convex, and the organ is thus approximately sickle-shaped. The parietal surface is generally smooth, though sometimes marked by depressions that may even perforate to the visceral surface. It lies against the diaphragm but is not joined to this. The visceral surface presents three parts. A small dorsal region fits against the left crus of the diaphragm and left kidney and is bound to these by phrenicosplenic and renosplenic ligaments (Figure 21–8/6,7). The remainder of the visceral surface is divided by a ridge along which the splenic artery runs and to which the greater omentum attaches. The narrow strip cranial to the ridge, the gastric surface, is applied to the greater curvature of the stomach (see Figure 21–21); the larger area caudal to the ridge, the intestinal surface (Figure 21–21/1), is related to various parts of the intestinal mass.
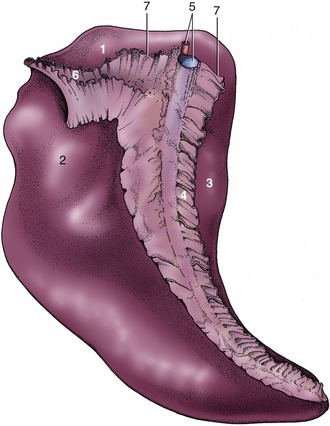
Figure 21–8 Visceral surface of the spleen. 1, Renal surface; 2, intestinal surface; 3, gastric surface; 4, greater omentum (gastrosplenic ligament); 5, splenic artery and vein; 6, renosplenic ligament; 7, phrenicosplenic ligament.
The thick capsule contains a considerable amount of smooth muscle, which allows much variation in volume because the spleen becomes engorged when the capsule is relaxed. This occurs in certain diseases and is very obvious in animals that have succumbed to anthrax. The organ is steel blue on first removal from the fresh carcass but turns reddish brown on exposure to the air. This color is derived from the red pulp that forms the bulk of the parenchyma. The white pulp that flecks the red is not normally visible to the naked eye.
The position of the spleen naturally varies with respiration. Usually only the caudal margin is within reach on rectal exploration (see Figure 22–23/10); a greater part becomes accessible when the stomach is distended.
THE STOMACH
The most remarkable feature of the stomach is its small size in relation to the animal and to the volume of fodder consumed. It is probably flattered by the figure of 5 to 15 L commonly quoted as the physiological capacity. It is relatively larger in the unweaned foal.
The equine stomach lies mainly within the left half of the abdomen (Figure 21–10/2). Like other simple stomachs, it consists of two limbs that meet at a ventral angle. The left limb comprises the fundus (unusually large and often termed saccus cecus [blind sac] in this species) and the body; the right limb or pyloric part is much narrower and extends across the midline to join the duodenum (Figure 21–9, A). Although the situation naturally varies with the degree of distention, the stomach remains within the protection of the rib cage even when grossly distended; it is therefore inaccessible by the ordinary methods of clinical examination, either through the flank or per rectum. Gross overdistention may be revealed by a raising of the overlying ribs on the left side, which destroys the normal symmetry of the trunk. When moderately distended the fundus extends under the upper part of the fifteenth rib (or thereabouts), and the lowest part of the body reaches the ventral parts of the ninth and tenth ribs. The cardia provides a relatively fixed point, opposite the upper part of the eleventh rib, and enlargement after feeding is therefore mainly downward and forward (Figure 21–6/2).
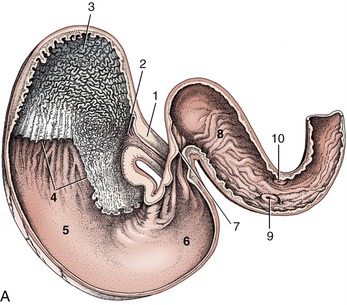

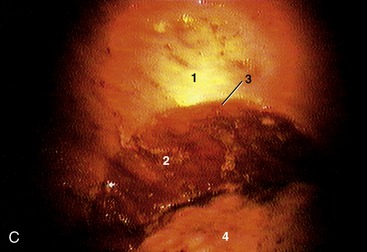
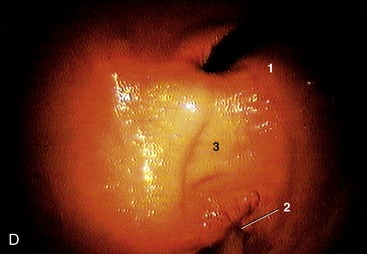
Figure 21–9 A, Interior of the stomach and cranial part of the duodenum. 1, Esophagus; 2, cardiac opening; 3, fundus (blind sac); 4, margo plicatus; 5, body; 6, pyloric part; 7, pylorus; 8, cranial part of duodenum; 9, major duodenal papilla within hepatopancreatic ampulla; 10, minor duodenal papilla. B, Notice the white mucosa of the fundus. The Gastrophilus larvae are an incidental finding in this part of the stomach. 4, Margo plicatus is clearly visible. C, Endoscopic view of stomach. 1, Nonglandular mucosa; 2, glandular mucosa; 3, margo plicatus; 4, ingesta. D, Endoscopic view of stomach. 1, Fiber optic cable of endoscope entering through cardia; 2, pylorus; 3, lesser curvature.
The cranial surface is directed against the diaphragm above and against the left lobe of the liver more ventrally; it faces cranially, dorsally, and laterally. The caudal surface faces in the opposite direction and makes contact with various viscera, including coils of small intestine and descending colon dorsally and the dorsal diaphragmatic flexure of the ascending colon ventrally. The left part of the greater curvature is followed by the hilus and adjoining gastric surface of the spleen (see Figure 21–21).
A stepped edge (margo plicatus; Figure 21–21/2″) divides the interior between a large nonglandular region, occupying the fundus and part of the body, and a glandular region. The nonglandular part resembles the mucosa of the esophagus and is dirty white and harsh to the touch (see Figure 21–9). The softer glandular region consists of cardiac, proper gastric, and pyloric glandular zones; although the borders between these zones are ill-defined, the zone occupied by the proper gastric glands is somewhat darker and redder than the yellowish cardiac and pyloric zones in the fresh specimen. Both the cardiac and pyloric regions are incidentally parasitized by botfly (Gasterophilus) larvae; when these relinquish their hold to pupate in the soil they may leave the mucosa densely pocked by small focal ulcerations. These, when semihealed, can be misinterpreted as normal features (Figure 21–9, B).
The cardiac sphincter is exceptionally well developed, and this, coupled with the oblique entrance of the esophagus, is held responsible for the horse’s reputed inability to eructate or vomit; however, eructation and vomiting, though rare, is possible. The canal or distal portion of the pyloric part is more muscular than the remainder of the organ and is bounded by proximal and distal thickenings that converge at the lesser curvature. Even when the second of these, the pyloric sphincter, is fully relaxed, the actual exit is remarkably narrow (Figure 21–21/5).
THE INTESTINES
The intestines occupy the greater part of the abdominal cavity. The small intestine is unremarkable, but the large intestine is greatly modified and enlarged. It provides the reservoir for microbial fermentation and assumes a form and disposition that make it difficult to recognize the homologies of its parts with those of the gut of other species. However, these may be deduced from the attachments and arterial supply and confirmed by reference to the development.
THE SMALL INTESTINE
The small intestine measures about 25 m in the carcass, although it is probably much less in life. The duodenum is relatively short, and because it is closely tethered, it is more or less constant in position. It commences ventral to the liver where the initial (cranial) part forms a sigmoid flexure of which the first curve is convex dorsally, the second convex ventrally. The second (descending) part then runs caudally, still below the liver, until it reaches the lateral margin of the right kidney, which it follows to the caudal pole; it then bends medially behind the root of the mesentery (Figure 21–10/6 and Figure 21–11/2,3). The descending duodenum is also related to the right lobe of the pancreas and crosses above the last part of the right dorsal colon and the base of the cecum to which it is attached (see Figure 21–14). This relationship permits the formation of a temporary duodenocecal anastomosis in the treatment of gastroduodenojejunitis, obviating the reflux of fluid and consequent overloading of the stomach that characterizes this condition. The third (ascending) part runs forward against, and adherent to, the left face of the mesentery; it bends ventrally below the left kidney to continue as the jejunum. The caliber of the duodenum is uniform except at its commencement, where the first bend of the sigmoid flexure is somewhat widened. The bile and pancreatic ducts open here. The bile and major pancreatic ducts discharge through a single papilla within an enclosure (ampulla hepatopancreatica) bounded by a circular mucosal rampart. This is situated on the convex margin of the flexure, while the accessory pancreatic duct opens on a small papilla on the facing margin (see Figure 21–21/7,8).
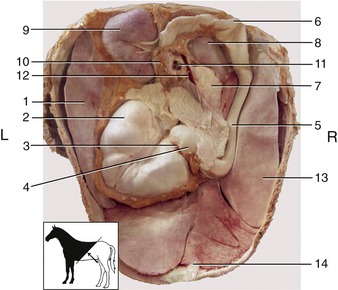
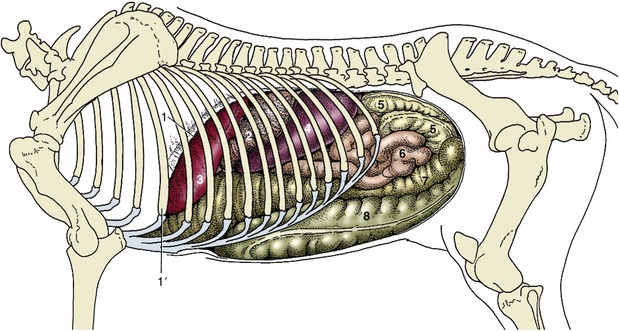
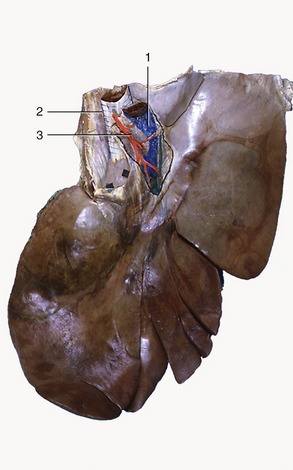
Figure 21–10 The organs in the craniodorsal part of the abdominal cavity of a young horse, caudoventral view (see inset). 1, Spleen; 2, stomach; 3, pylorus; 4, 5, cranial and descending parts of duodenum; 6, caudal flexure of duodenum; 7, pancreas; 8, right kidney; 9, left kidney; 10, left adrenal gland; 11, cranial mesenteric artery and vein; 12, portal vein; 13, liver; 14, falciform ligament.
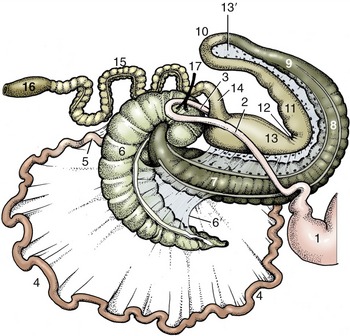
Figure 21–11 The intestinal tract seen from the right, schematic. The caudal flexure of the duodenum and the cranial mesenteric artery (17) have been displaced to the right of the animal to lie over the base of the cecum. 1, Stomach; 2, 3, descending and ascending duodenum; 4, jejunum; 5, ileum; 6, cecum; 6′, cecocolic fold; 7, right ventral colon; 8, ventral diaphragmatic flexure; 9, left ventral colon; 10, pelvic flexure; 11, left dorsal colon; 12, dorsal diaphragmatic flexure; 13, right dorsal colon; 13′, ascending mesocolon; 14, transverse colon; 15, descending (small) colon; 16, rectum; 17, cranial mesenteric artery.
The position and restricted mobility of the duodenum make its access difficult through the usual surgical exposures; fortunately, indications for duodenal surgery are largely restricted to the condition recently mentioned.
The remainder of the small intestine lies within the free margin of the great mesentery, which is sufficiently long to allow the coils considerable latitude in position. Most are piled into the left dorsal part of the abdomen where they mingle with those of the descending colon; however, some insinuate themselves between the large intestine and the flanks, while others may reach the abdominal floor between the body of the cecum and the ventral parts of the ascending colon. The ileum (according to the convention we employ [p. 129]) is very short, and in most circumstances it is distinguished from the remainder of the small intestine by its much thicker wall and firmer consistency. It approaches the left side of the cecal base from below and ends by protruding into the cecal interior, raising a papilla on which it opens.
The mobility of the small intestine may be blamed for the incarceration of a part within one of several openings such as the epiploic foramen,* vaginal ring, or even a rent in the mesentery. Intussusception is also relatively common, especially in the young horse. A form peculiar to the horse involves the passage of the terminal part of the small intestine into the interior of the cecal base. Necrosis of the intruded part follows quickly unless surgical correction is undertaken.
THE LARGE INTESTINE
In addition to its enormous capacity, the large intestine is also characterized by having a sacculated form. The sacculations or haustra result from the shortening of the teniae, bands formed by the concentration of the external longitudinal muscle and elastic fibers at certain (from one to four) positions on the circumference. Semilunar folds project internally where grooves divide adjacent haustra externally (see Figure 21–11). The haustral segmentation is not constant but is constantly modified in life by gradual “haustral flow” and by intermittent disappearance of the contractions followed by their re-formation in a different pattern.
The arrangement of the large intestine of the horse predisposes to various forms of obstruction and displacement, conditions collectively known as colic (although this term is widely used to include any painful abdominal disorder).
The Cecum
The cecum incorporates an initial portion of the ascending colon as is revealed by its extension distally beyond the entrance of the ileum. It follows that the so-called cecocolic orifice is actually a constriction of the ascending colon set some distance distal to its true origin. However, the conventional terminology pays no regard to such considerations and is based entirely on the form of the adult organ (Figure 21–12).
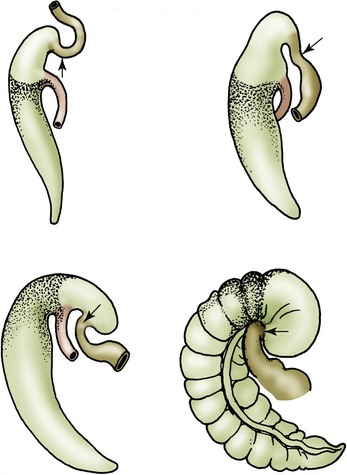
Figure 21–12 Development of the equine cecum, schematic. The stippled part of the cecum is homologous with the cecum of other species. The nonstippled part is the annexed first part of the colon. The cecocolic orifice is a constriction of the ascending colon (arrows).
The cecum consists of an expanded dorsal base, a curved tapering body, and a blind ventral apex; these parts merge smoothly, and the organ is often likened to a comma (Figure 21–13). In large horses it may have a capacity in excess of 30 L and may measure a meter or more between extremities. The base lies in the right dorsal part of the abdomen, partly against the flank and partly under cover of the ribs. It has an extensive contact with the abdominal roof and sublumbar organs from the fifteenth rib (or thereabouts) to the coxal tuber, but the direct dorsal adhesion is confined to the region of the pancreas and right kidney. This retroperitoneal attachment extends caudally to the level of the second lumbar vertebra. The base also fuses with the root of the mesentery medially and with the right dorsal colon cranially. The cranial part of the base forms an overhanging enlargement that at first sight appears to be blind (Figure 21–14); closer inspection reveals the origin of the colon from the middle of the caudal wall of this overhang. The caudal part of the base merges imperceptibly with the body of the cecum. Microbial fermentation within the cecum produces gas that is normally discharged at intervals into the right ventral colon. Occasionally, gas is produced excessively, causing the overhanging part of the base to press on the origin of the right ventral colon, interfering with the normal mechanism. The resulting tympany of the base can only be relieved by needle decompression through the paralumbar fossa.
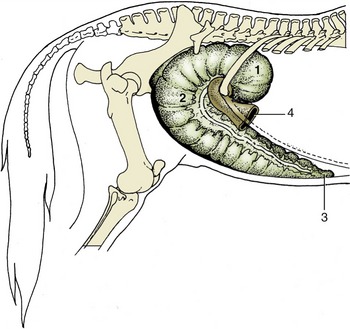
Figure 21–13 The cecum in situ. 1, Base of cecum; 2, body of cecum; 3, apex of cecum; 4, right ventral colon.
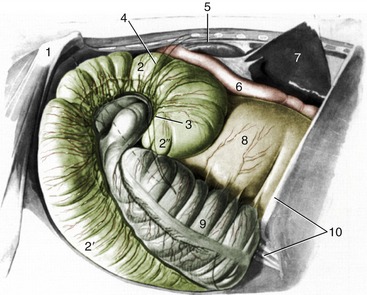
Figure 21–14 Cecum and related organs lying against the right abdominal wall and flank. The broken line indicates the position of the cranial branch of the deep circumflex iliac artery crossing the flank. 1, Coxal tuber; 2, 2′, base and body of cecum; 2″, overhanging part of cecal base; 3, position of cecocolic orifice; 4, position of last rib; 5, right kidney; 6, descending duodenum; 7, right lobe of liver, elevated; 8, right dorsal colon; 9, right ventral colon; 10, tenth rib and costal arch.
The body runs ventrally before turning cranially (Figure 21–13/2). At first it lies against the right flank, following the caudal border of the right ventral colon, but as it sinks within the abdomen, it is displaced medially; when it reaches the abdominal floor, it lies between the ventral parts of the ascending colon. It terminates in the apex, close to the xiphoid cartilage. There are four teniae over most of the organ, but the number diminishes toward the apex. Retroflexion of the apical part of the cecum is occasionally encountered in apparently healthy subjects.
The interior is marked by numerous folds corresponding to the external divisions of the haustra. These folds are impermanent, but a larger and more persistent fold at the level of the ileal papilla partially separates the cranial expansion from the remainder of the base (Figure 21–15). The ileal papilla is variable in form. In most postmortem specimens it is a low conical projection whose summit carries a slitlike opening bounded by lax folds of mucosa (Figure 21–15/1). In life, it is usually much more salient and more cylindrical and has a rounded orifice circumscribed by a firm and thickened rim. The erection of the papilla is caused by the tonus of the muscle and engorgement of a mucosal venous plexus.
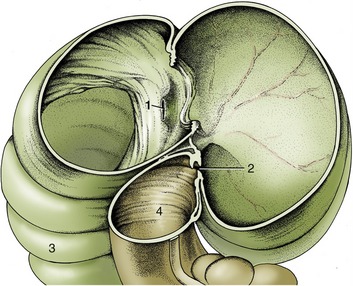
Figure 21–15 The interior of the base of the cecum, right lateral view. 1, Termination of ileum at ileal papilla; 2, cecocolic orifice; 3, body of cecum; 4, right ventral colon.
Although the exit from the cecum near the cecocolic orifice (Figure 21–15/2) lies at some distance from the ileal papilla, the curvature of the cecal base brings it more or less into the same transverse plane. In the dead specimen it is a transverse slit that scarcely admits a few fingers, but in life it generally allows the passage of a hand.
The Colon
The colon consists of the usual ascending, transverse, and descending parts (see Figure 3–45). The first two together constitute the “large colon” of common usage, and the third constitutes the “small colon” (Figure 21–11/15). The ascending colon is arranged in four parallel limbs separated by three flexures, each separately named. The sequence runs as follows: right ventral colon (Figure 21–11/7), ventral diaphragmatic flexure, left ventral colon, pelvic flexure, left dorsal colon, dorsal diaphragmatic flexure, and right dorsal colon (Figure 21–11/13). The right dorsal colon leads to the short transverse colon (Figure 21–11/14); this is followed in its turn by the descending colon, which is long and thrown into coils (Figure 21–11/15).
The cecocolic transitional region forms a sigmoid flexure: the convexity of the first bend (provided by the overhanging part of the cecal base) is directed ventrally, and that of the second bend (provided by the first part of the colon) is directed dorsally (Figure 21–14 and Figure 21–16). This conformation appears to be caused by the looser attachment of the medial and lateral teniae at this level; they run as chords across the arcs into which the bowel is drawn. The right ventral colon is narrow when it emerges from this siphon-like arrangement but soon expands to continue, first ventrally, then cranially on the abdominal floor, as a wide (ca. 20-cm) tube of uniform caliber (see Figure 21–7). It is deflected across the midline on reaching the diaphragm (ventral diaphragmatic flexure) and then becomes known as the left ventral colon (Figure 21–17). The left ventral colon runs toward the pelvis, still on the abdominal floor (see Figure 21–6) until a sharp flexure through 180° marks its junction with the following left dorsal part. The pelvic flexure is also distinguished by a reduction in caliber (see Figure 21–11) and by the disappearance of three of the four bands found on the ventral parts, of which the consequence is the loss of the haustrations. Although there is no evidence of a conventional sphincter, the pelvic flexure marks the boundary between two distinct functional units of the colon. The decrease in the fluidity of the ingesta, the sudden alteration in course, and the reduction in caliber explain why impaction is common at this level. The location of the flexure varies with the fullness of the rectum, bladder, and uterus, but because it is usually just within or in front of the pelvic cavity, it is easily found on rectal examination especially if impacted.
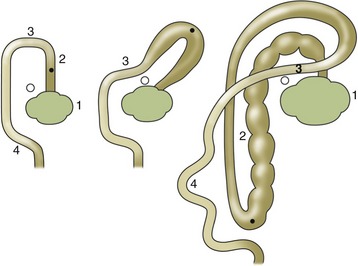
Figure 21–16 The development of the ascending colon, dorsal view. The dot indicates the position of the pelvic flexure, the circle that of the cranial mesenteric artery. 1, Cecum; 2, ascending colon; 3, transverse colon; 4, descending colon.
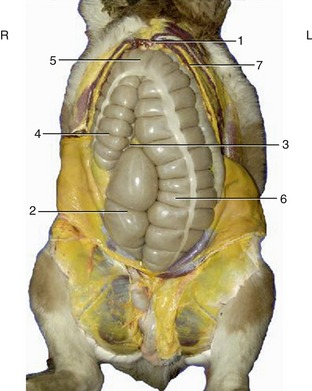
Figure 21–17 Visceral projection on the ventral abdominal wall. The position of the apex of the cecum is variable. 1, Xiphoid cartilage; 2, body of cecum; 3, apex of cecum; 4, right ventral colon; 5, ventral diaphragmatic flexure; 6, left ventral colon; 7, dorsal diaphragmatic flexure.
The left dorsal colon is narrow and smooth-walled where it emerges from the pelvic flexure, but it gradually widens; the teniae increase from one to three, and the sacculations return. It runs cranially above the left ventral colon, below the coils of small intestine and descending colon, to reach the liver, where it continues as the right dorsal colon at the dorsal diaphragmatic flexure. Toward its termination it is related to the spleen and the stomach (Figure 21–6/7). The right dorsal colon is both the shortest and, at its termination, by far the widest part (ca. 30 cm) of the ascending colon (Figure 21–18/7). It ascends below the liver to meet the cranial part of the cecal base by which it is deflected medially to become the transverse colon (Figure 21–18/8). The right dorsal colon is also the best-fixed part and is adherent to the abdominal roof, the cecal base, and the root of the mesentery. It carries three bands.
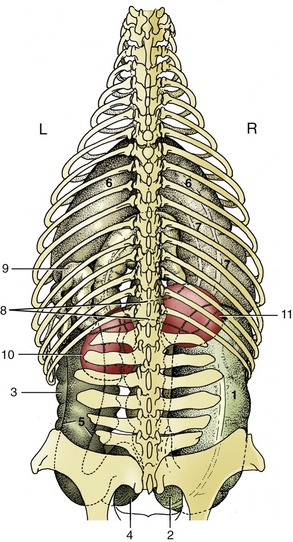
Figure 21–18 Position of the large intestine and the kidneys, dorsal view. 1, Base of cecum; 2, body of cecum; 3, left ventral colon; 4, pelvic flexure; 5, left dorsal colon; 6, dorsal diaphragmatic flexure; 7, right dorsal colon; 8, transverse colon; 9, proximal part of descending colon, cut; 10, left kidney; 11, right kidney.
The transverse colon is very short and is situated according to the common mammalian pattern, passing from right to left in front of the root of the mesentery. It carries two bands and rapidly funnels to the much smaller caliber of the descending colon (Figure 21–18/9) by which it is succeeded in the region of the left kidney. The transverse colon also has a direct retroperitoneal attachment to the abdominal roof.
Except at its origin and termination the ascending colon is free within the abdomen, although its great bulk ensures that it does not change much in position. The folding it undergoes in development transforms the original mesentery into a short peritoneal sheet (ascending mesocolon) passing between adjacent portions of the dorsal and ventral limbs (Figure 21–11/13′). Through continuity with the cecum and transverse colon it is anchored by the retroperitoneal attachments of these parts. The loose attachment between the left limbs allows the dorsal part to slip some way to the side (generally the right side) of the ventral part as a common and probably temporary variant of the usual topography. When the rotation of these parts about their common axis is pronounced, there arises the condition known as twist (torsio), which is one of the most severe abdominal catastrophes to which the horse is subject. A torsio coli initially narrows the lumen, but more important is the interruption of the blood flow in the capillaries of the bowel wall and in the vessels that follow the bowel. Another malposition of the ascending colon that has been increasingly recognized in recent years involves the lodgment of the left limbs above the spleen. Although the cause of this painful condition is not known with certainty, it is postulated that the accumulation of gas raises the left limbs against the abdominal wall until they pass over the base of the spleen to be trapped on the shelf formed by the phrenicosplenic and renosplenic ligaments (left dorsal displacement). Spontaneous restoration of normal topography is possible, but quicker restoration may be achieved by rolling and maneuvering the recumbent (anesthetized) animal. If the rolling procedure is failing, surgical intervention (decompression) is required.
The descending colon (Figure 21–11/15), much narrower than the other parts, is several meters long and alone hangs within a conventional mesentery. These features account for its alternative names, small colon and floating colon. It lies mainly within the dorsal, caudal, and left part of the abdomen, largely dorsal to the small intestine, and ends in the rectum (Figure 21–6/5). The distinction between the descending colon and rectum is based entirely on the pelvic location of the latter, and no immediate change in structure or appearance occurs. The descending colon is drawn by two prominent bands into a linear series of sacculations occupied by the familiar dry fecal balls. The rectum is considered with the pelvic organs.
VASCULARIZATION, LYMPH DRAINAGE, AND INNERVATION OF THE GASTROINTESTINAL TRACT
The vascularization of the equine abdominal viscera was especially in the past of clinical importance because of the occurrence of vascular pathology caused by migrant nematode larvae. The fact that these lesions are not often fatal is due to the extensive system of anastomoses between the arteries supplying successive parts of the gastrointestinal tract. The pathology is often most serious in the cranial mesenteric artery and its major branches; these may be so greatly enlarged by aneurysm formation and by connective tissue reaction that the normal structure and topography are grossly disturbed. Paradoxically, obstruction of one of the large branches may have much less serious consequences than closure of a smaller one: the anastomoses of the major arteries are large and constant, but those of the minor arteries are small and often dangerously deficient. The caudal mesenteric artery, specifically concerned with the descending colon, may also be affected.
The branching and distribution of the two mesenteric arteries are shown in Figure 21–19. The celiac artery has essentially the same distribution to stomach, liver, and spleen as in other species. The venous drainage parallels the arterial supply, in that the portal vein is ultimately formed by the union of the caudal mesenteric, cranial mesenteric, and splenic tributaries.
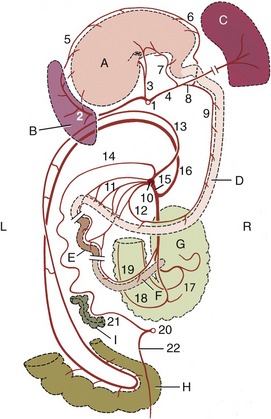
Figure 21–19 The major arteries of the gastrointestinal tract, schematic dorsal view. The structures have been stretched craniocaudally for clarity. A, Stomach; B, spleen; C, liver; D, duodenum; E, jejunum; F, ileum; G, cecum; H, pelvic flexure; I, descending colon. 1, Celiac a.; 2, splenic a.; 3, left gastric a.; 4, hepatic a.; 5, left gastroepiploic a.; 6, right gastroepiploic a.; 7, right gastric a.; 8, gastroduodenal a.; 9, cranial pancreaticoduodenal a.; 10, cranial mesenteric a.; 11, jejunal aa.; 12, caudal pancreaticoduodenal a.; 13, right colic a.; 14, middle colic a; 15, ileocolic a.; 16, colic branch of ileocolic a.; 17, lateral cecal a.; 18, medial cecal a.; 19, mesenteric ileal a.; 20, caudal mesenteric a.; 21, left colic a.; 22, cranial rectal a.
Lymph from the regional nodes of the stomach, spleen, liver, pancreas, and diaphragm drains to a lymph center about the celiac artery and thence to the cisterna chyli via a celiac trunk.
The very numerous nodes that receive lymph from the intestines (with the exception of the caudal part of the descending colon) are scattered at the root of the mesentery and along the arteries of the cecum and colon. Lymph is collected and conveyed to the cisterna chyli by an intestinal trunk. The nodes scattered along the remainder of the descending colon send lymph to a center at the root of the colic mesentery and then to the lumbar trunk; this route is also followed by most of the lymph draining the rectum and anus.
The abdominal viscera are supplied by nerves that pass through plexuses associated with the mesenteric ganglia (see Figure 21–24/18,20). The nervous structures about the celiac and cranial mesenteric arteries may be involved in the reaction provoked by the nematode larvae and are difficult to display satisfactorily except in juvenile animals. It is often asserted, although it remains unproven, that the “colic” pain and functional disturbance associated with helminth infestations are caused by secondary involvement of the nerves rather than by the primary vascular lesions.
THE LIVER
The liver is quite variable in form and size but on average weighs about 5 kg in a saddle horse, thus accounting for about 1.5% of the body weight, a much smaller proportion than in carnivores.
It is situated in the most cranial part of the abdomen directly against the diaphragm. It is markedly asymmetrical in the healthy young subject, in which about two thirds lie to the right of the median plane (see Figure 21–7/2). The most caudal part, which is also the most dorsal, lies ventral to the vertebral extremities of the sixteenth and seventeenth ribs of the right side; the most cranial and most ventral part lies against the left part of the vertex of the diaphragm (Figure 21–6/3). The long axis thus runs obliquely. In the newborn foal the liver is relatively much larger and extends onto the abdominal floor behind the costal arch; it is also more symmetrical. In older subjects atrophy is common; this is most obvious in the right lobe and probably results from chronic pressure from the right dorsal colon and cecal base. Less often, the left lobe atrophies, perhaps under pressure from the stomach.
The parietal surface is joined to the diaphragm by a complicated system of ligaments. The visceral surface lies against and is impressed by the stomach, duodenum, dorsal diaphragmatic flexure of the colon, and cecal base (see Figure 21–10). The porta is central, within an area made rough by the direct attachment of the pancreas. The dorsal fixed margin of the liver extends between the right and left triangular ligaments and is very irregular (Figure 21–20). Its right part is thick and excavated to receive the cranial pole of the right kidney; a sulcus medial to this transmits the caudal vena cava. Its left part is much thinner and does not extend nearly so far dorsally; it carries the impression of the esophagus close to the midline. The long free margin is much sharper and is interrupted by a series of fissures, of which the largest divide named lobes. The current nomenclature recognizes left, quadrate, right, and caudate lobes. The first two are separated by the fissure carrying the round ligament of the liver (vestige of the umbilical vein), but the boundaries of the others are more arbitrary and are of doubtful morphological significance.
The duct system is remarkable for the absence of a gallbladder, but its wide caliber compensates for this. The bile duct opens into the cranial duodenum on the papilla shared with the major pancreatic duct (Figure 21–21/7). The oblique passage of the duct through the duodenal wall serves as a sphincter and prevents the influx of ingesta.
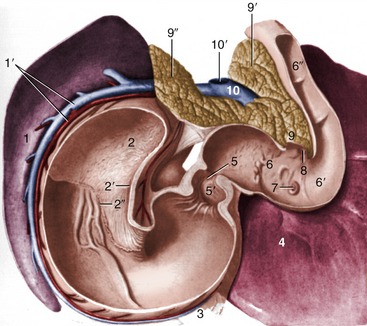
Figure 21–21 Topography of spleen, stomach, pancreas, and liver, caudoventral view. 1, Intestinal surface of spleen; 1′, splenic a. and v.; 2, fundus (blind sac) of stomach; 2′, cardia; 2″, margo plicatus; 3, greater omentum; 4, liver; 5, pyloric orifice; 5′, pyloric antrum; 6, S-shaped cranial part of duodenum; 6′, cranial flexure of duodenum; 6″, descending duodenum; 7, major duodenal papilla; 8, minor duodenal papilla; 9, body of pancreas; 9′ (right)—9″ (left), left and right lobes of pancreas; 10, portal v; 10′, stump of cranial mesenteric v.
THE PANCREAS
The pancreas lies largely to the right and is pressed against the abdominal roof and sublumbar organs (Figure 21–10/7). It is triangular in outline, and its apex is fitted into the second concavity of the duodenal sigmoid flexure. The right border follows the descending duodenum; the left border passes obliquely toward the left kidney. The portal vein (Figure 21–21/10) perforates the pancreas close to the caudal border. The ventral surface is directly bound to the right dorsal colon and cecal base, the dorsal surface to the right kidney and liver. The openings of its two ducts (Figure 21–21/7,8) are described with the duodenum.
THE KIDNEYS AND ADRENALS
The kidneys lie against the diaphragm and psoas muscles dorsally, each enclosed within a capsule of fat. The right kidney lies ventral to the last two or three ribs and first lumbar transverse process; the left one lies ventral to the last rib and first two or three processes and is thus about half a kidney length caudal to the level of its fellow (Figure 21–18/10,11). Each kidney weighs about 700 g. The right one is shaped like the heart on a playing card, but the left one has a more conventional form. Both are dorsoventrally flattened.
The cranial pole of the right kidney fits into the renal impression of the liver; caudal to this it is ventrally attached to the pancreas and the base of the cecum (Figure 21–14/5,2). The duodenum winds around the lateral margin and adjoining part of the ventral surface, which is the only region sometimes covered with peritoneum. The short medial border is indented by the hilus and is related to the caudal vena cava and the right adrenal gland (Figure 21–22).
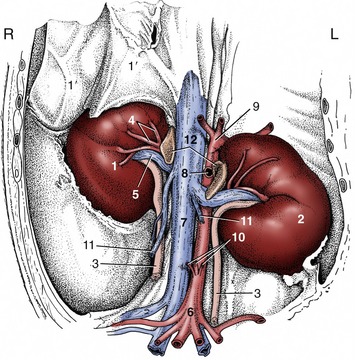
Figure 21–22 Kidneys and adrenal glands in situ, ventral view. 1, Right kidney; 1′, liver; 2, left kidney; 3, ureter; 4, renal artery; 5, renal vein; 6, aorta; 7, caudal vena cava; 8, cranial mesenteric artery; 9, celiac artery; 10, caudal mesenteric and testicular arteries; 11, testicular veins; 12, adrenal glands.
The ventral surface of the left kidney has a more complete covering of peritoneum and is related to coils of small colon and small intestine, generally including the duodenojejunal junction. Cranioventrally it lies against the spleen; it may make contact with a distended stomach (see Figure 21–10). The medial border is related to the aorta and the left adrenal gland (see Figure 21–22).
The kidneys are of a modified unipyramidal type; the numerous constituent pyramids are completely fused, and their former boundaries are revealed only by the arrangement of the interlobar arteries. A clearer indication of the lobation, with some external fissuration, is common in the foal. The structure is best revealed in section (Figure 21–23). The strong external fibrous capsule can normally be easily stripped away, except within the renal sinus, where it merges with the adventitia of the structures entering and leaving. The division of the parenchyma between cortex and medulla is indicated by a color change and by the sectioned arcuate arteries. The cortex is brownish red and granular. The peripheral part of the medulla is dark red, the inner part pale; both show radial striations. The apices of the fused medullary pyramids form a common renal crest that projects into the pelvis. This has a curious form consisting of a central expansion (Figure 21–23/4) at the origin of the ureter and two terminal recesses toward the poles (Figure 21–23/5); most papillary ducts open into the recesses. The pelvic mucosa produces a mucous secretion, and as a result the unfiltered urine normally contains some protein (physiological albuminuria).

Figure 21–23 Dorsal section through a kidney, semischematic. 1, Renal cortex; 2, renal medulla; 3, ureter; 4, pelvis; 5, terminal recess; 6, papillary ducts; 7, renal artery; 8, interlobar arteries.
The renal vessels are short and wide. The artery often splits before reaching the hilus, and a number of branches may enter the ventral surface independently (Figure 21–23/8).
The ureters are wide at their origins but soon reduce to narrow, more uniform calibers. They bend caudally on emerging from the renal sinus and thereafter pursue a tortuous course over the roof of the abdomen to reach the pelvis. Here they follow the lateral parts of the broad ligaments (genital fold in the male) before inclining medially to pierce the bladder wall close to its neck.
The elongated and irregular adrenal glands lie against the cranial parts of the medial borders of the corresponding kidneys (Figure 21–22/12). Each consists of an outer bright yellow cortex and an inner brownish red medulla. The glands are relatively large in juvenile animals.
THE ROOF OF THE ABDOMEN
The bodies of the lumbar vertebrae, the sublumbar muscles, and the diaphragm furnish the roof of the abdomen. The aorta and caudal vena cava lie within the cleft between the two psoas minor muscles: the artery is to the left, and the vein is to the right (Figure 21–22/6,7). The branches of the aorta and the tributaries of the vein are, in principle, the same as in other species.
The autonomic nerves and ganglia show some specifically equine features, although these are matters of detail rather than of substance. The general pattern is shown in Figure 21–24. The fused celiac and cranial mesenteric ganglia lie ventral to the aorta, to each side of the celiac and cranial mesenteric arteries. The right and left ganglia are joined by bridges cranial and caudal to the latter artery. They are sizable structures, 5 cm or so long, and are generally unequal: the left complex is larger and more regular than the right one (Figure 21–24/18). Each is joined by a major splanchnic nerve and, in varying fashion, by parasympathetic fibers from the dorsal vagal trunk. The nerves that leave the ganglia follow the arteries, branching where these branch and forming a dense plexus in which the sympathetic and parasympathetic contributions mingle. The whole plexiform arrangement that radiates from the major ganglia is known as the celiacomesenteric (solar) plexus. Additional small renal ganglia occur on the nerves about the renal arteries.
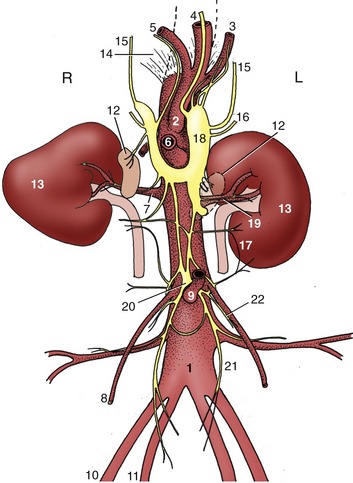
Figure 21–24 Schema of the abdominal autonomic nerves and branches of the abdominal aorta, ventral view. 1, Aorta; 2, celiac a.; 3, splenic a.; 4, left gastric a.; 5, hepatic a.; 6, cranial mesenteric a.; 7, renal a.; 8, testicular (ovarian) a.; 9, caudal mesenteric a.; 10, external iliac a.; 11, internal iliac a.; 12, adrenal glands; 13, kidneys; 14, crus of diaphragm; 15, major splanchnic nn.; 16, minor splanchnic nn.; 17, lumbar splanchnic nn.; 18, combined celiac and cranial mesenteric ganglia; 19, renal plexus; 20, caudal mesenteric ganglion; 21, hypogastric n.; 22, testicular (ovarian) plexus.
The celiacomesenteric complex is joined to the caudal mesenteric plexus by a plexus on the aorta and an additional trunk that runs at a more ventral level within the colic mesentery.
The caudal mesenteric ganglion lies cranial to the origin of the like-named artery (Figure 21–24/9,20). It gives rise to nerve plexuses that follow this vessel and the gonadal vessels to the small colon and reproductive organs, respectively, and to the hypogastric nerves (Figure 21–24/21) that pursue a retroperitoneal course on the roof of the pelvis. Lumbar splanchnic nerves join the major ganglia and the aortic plexus in an erratic fashion.
The usual direct detachment of preganglionic fibers from the splanchnic nerves to the medullary parts of the adrenal glands exists.