Obesity
Obesity is defined as a body mass index (BMI) above 30 kg⋅m−2, compared with the ideal range of 18.5–24.9 kg⋅m−2. A BMI of 25–29.9 kg⋅m−2 is considered overweight. The prevalence of obesity is increasing in the Western world; it varies from less than 10% in the Netherlands to about 50% in some parts of Eastern Europe. In the UK it is currently about 15%, but over half the British population is now overweight.
The health consequences of obesity are considerable (Box 37.1). Obesity decreases life expectancy by 7 years at the age of 40 years. Recent data suggest that waist circumference above 102 cm in males or 88 cm in females is more closely correlated than BMI with the cluster of atherogenic risk factors known as the metabolic syndrome. Metabolic syndrome is the presence of at least two of the following characteristic features in association with large waist circumference:
 abnormally raised triglyceride,
abnormally raised triglyceride,
decreased high-density lipoprotein (HDL) cholesterol,
raised fasting blood glucose (as a result of insulin resistance),
Excess dietary calories are stored as fat in adipose tissue. Intra-abdominal (visceral) fat is most closely associated with the metabolic and atherogenic consequences of obesity. The association between central obesity and atherothrombosis is related to enlarged visceral adipocytes. These adipocytes secrete numerous inflammatory, pro-atherogenic and procoagulant cytokines such as interleukin-6, tumour necrosis factor α and plasminogen activator inhibitor-1, but secrete reduced amounts of the anti-inflammatory and anti-atherogenic hormone adiponectin. Cytokines produced by fat-laden omental adipocytes enter the portal circulation and influence many aspects of hepatic metabolism.
Pathogenesis of obesity
Food intake is controlled by numerous hormonal, societal, genetic and psychological factors. Obesity usually develops gradually, and results when energy input exceeds output for a prolonged period. A small imbalance between energy intake and exercise or muscular work is all that is required for progressive weight gain. There are polygenic influences that determine who is more susceptible to weight gain. However, the recent epidemic of obesity in the Western world suggests that major environmental factors (reduced activity and dietary changes) are responsible, rather than biological causes.
For a few individuals, obesity arises from hormonal disturbances, or from neurological conditions that lead to behavioural change. Several drugs can produce weight gain, such as antipsychotics, tricyclic antidepressants, corticosteroids, antiepileptics, antihistamines and antidiabetic drugs.
There are two types of adipose tissue: brown adipose tissue is responsible for thermogenesis and white adipose tissue for energy storage. White adipose tissue is a target for insulin and in obese people there is resistance to the action of insulin, leading to accumulation of intracellular fat.
Energy balance is regulated in the hypothalamus, which integrates neural, hormonal and circulating nutrient stimuli, and sends signals to higher centres to trigger feelings of satiety or hunger. The hypothalamus also regulates sympathetic nervous system function (which controls lipolysis for release of fatty acids as an energy source, and also thermogenesis) and pituitary hormones that help to regulate energy expenditure.
The biochemical factors that underlie the regulation of weight are increasingly well characterised (Fig. 37.1). Signals to the hypothalamus that reduce food intake (satiety signals) are provided by a number of hormones produced by the endocrine cells of the gut, adipose tissue and the pancreas. Leptin, which is released from adipocytes, and insulin both signal via specific hypothalamic receptors to indicate the degree of filling of adipocytes and induce the sensation of satiety.
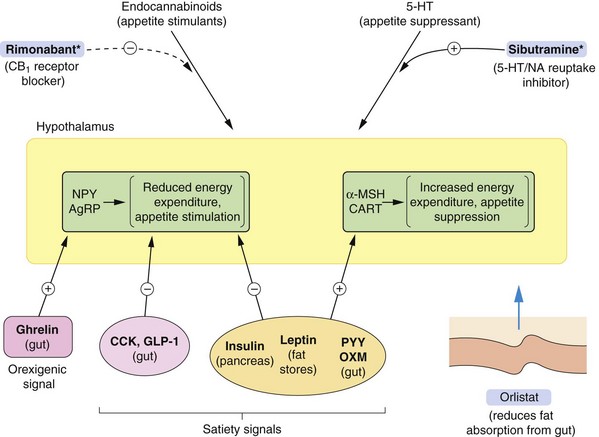
Fig. 37.1 Factors involved in the regulation of food intake.
Feedback loops between the periphery and the brain control food intake. Peripheral signals stimulate or inhibit transmitters in the arcuate nucleus of the hypothalamus (shown in yellow) that control appetite and energy expenditure. The hypothalamus sends signals to higher centres, indicating satiety or hunger. The peripheral orexigenic (appetite-stimulating) signals include ghrelin, released pre-prandially from the gut, and satiety signals include insulin, leptin, peptide YY3-36 (PYY) and oxyntomodulin (OXM). Other hypothalamic signalling mechanisms are described in the text. Endocannabinoid pathways are involved in stimulating appetite, and serotonin acts on the hypothalamus to suppress appetite. *Centrally acting appetite-suppressant drugs have been withdrawn due to unwanted effects, but rimonabant and sibutramine are shown to illustrate mechanisms. Orlistat reduces fat absorption from the gut by inhibiting pancreatic lipase. AgRP, agouti-related protein; CART, cocaine- and amfetamine-regulated transcript; CCK, cholecystokinin; GLP-1, glucagon-like peptide-1; α-MSH, α melanocyte-stimulating hormone; NA, noradrenaline; NPY, neuropeptide Y.
Several gut-derived peptides act as short-term appetite regulators. Ghrelin is released by the stomach pre-prandially, and stimulates orexigenic (appetite-stimulating) peptides. Oxyntomodulin, glucagon-like peptide-1 (GLP-1), cholecystokinin and peptide YY3-36 (PYY) are released from the small intestine and colon in response to the presence of carbohydrates and lipids, and inhibit release of orexigenic peptides in the hypothalamus.
When energy levels are low, ghrelin release and reductions in leptin, insulin and other gut-derived peptides act on the hypothalamus to stimulate key hypothalamic neurotransmitters, including neuropeptide Y (NPY) and agouti-related protein (AgRP). This decreases activity in the melanocortin system which releases signalling by the orexigenic hormones melanin-concentrating hormone (MCH) and orexin (ORX) to stimulate appetite. Following a meal, high plasma concentrations of insulin, glucose, cholecystokinin and leptin stimulate the hypothalamic appetite-suppressing substances pro-opiomelanocortin (POMC) and cocaine- and amfetamine-regulated transcript (CART). These mediators increase α-melanocyte-stimulating hormone (α-MSH) release which inhibits MCH/ORX activity and signal satiety.
Unexpectedly, the circulating concentration of leptin is usually high in obesity. This may reflect the excess fat accumulation and hypothalamic resistance to satiety cues such as leptin.
Other neurotransmitters and hormones that influence appetite include the appetite inhibitors serotonin and dopamine, while cannabinoids, cortisol and growth hormone-releasing hormone stimulate appetite. The role of the endocannabinoid system in regulating appetite has received increased attention in recent years. Acting via CB1 receptors, the natural agonists such as anandamide and 2-arachidonylglycerol have both CNS and peripheral actions. Endocannabinoids in the CNS are released from postsynaptic neurons, and act on presynaptic receptors to inhibit neurotransmitter release. They stimulate appetite by actions at the hypothalamus and nucleus accumbens. Peripherally, endocannabinoids have effects on gastrointestinal motility that reduce satiety signals.
Improved understanding of the biochemical signals that regulate appetite has led to a search for more effective appetite-suppressant drugs. So far there has been little translation into clinical practice.
Drugs for treatment of obesity
Drugs acting on the gastrointestinal tract
Mechanisms of action
Orlistat acts by binding to pancreatic lipase in the gut and inhibiting its action. It reduces triglyceride digestion and, therefore, energy intake from dietary fat. An effect on energy intake is seen after 24–48 h, and orlistat achieves sustained weight loss when used as an adjunct to dietary restriction and exercise. However, only about 20% of people will lose more than 5% of body weight. Continuous use of orlistat for more than 2 years is not recommended.
Methylcellulose is taken before meals and swells when hydrated and produces a sense of satiety. There is little evidence to support its ability to reduce appetite, and it has little use in the treatment of obesity. It is also used in constipation as a bulk-forming laxative (Ch. 35).
Pharmacokinetics
Methylcellulose and orlistat undergo minimal absorption after oral administration, and are largely excreted unchanged in the faeces.
Unwanted effects
Orlistat produces gastrointestinal upset, including flatulence, faecal urgency and faecal soiling. These are most common with poor adherence to a low-fat diet while taking the drug, and result in discontinuation of treatment by one-third of people. There is also impaired absorption of fat-soluble vitamins, especially vitamin D.
Methylcellulose swells rapidly when hydrated and should be taken with water to avoid oesophageal obstruction. It may have a laxative effect.
Centrally acting appetite suppressants
All centrally acting appetite suppressants, such as dexfenfluramine, fenfluramine, phentermine and sibutramine, have been withdrawn because of the increased risks of valvular heart disease and pulmonary hypertension. The selective CB1 receptor antagonist rimonabant that suppresses appetite by an effect on the hypothalamus has been withdrawn due to psychological disturbances.
Centrally acting drugs that work by different mechanisms are under development, but none are available for clinical use.
Management of obesity
Weight loss reduces the morbidity associated with obesity, but it is not known whether it prolongs life. Weight loss can be difficult to achieve and to maintain. Obesity is not usually caused by psychological disturbances, but these commonly arise in obese people. The social prejudice against obesity, concern about body image and the depression and irritability that arise from dieting are all contributory factors.
The cornerstone of management of obesity is to reduce energy intake by 500–600 kcal below daily requirements. Fat is ‘energy dense’ and should be particularly restricted. However, dietary restriction alone is usually inadequate to achieve weight loss, and increased exercise combined with diet is more effective than either alone. Exercise need not be vigorous, provided it is maintained long-term; walking or cycling is usually enough if performed daily. Behaviour modification is essential for long-term adherence to treatment.
Drug treatment should be restricted to individuals with a BMI of more than 30 kg⋅m−2, or a BMI of more than 28 kg⋅m−2 in the presence of diabetes, hypertension or hypercholesterolaemia. Currently orlistat is the only licensed available agent. A major disadvantage is that weight gain often follows cessation of drug therapy. The use of thyroxine to encourage weight loss by increasing metabolic rate is not recommended due to long-term risks such as osteoporosis. Bulking agents such as methylcellulose are usually ineffective for reducing food intake. Specialist clinics will consider the use of metformin (Ch. 40), selective serotonin reuptake inhibitors (Ch. 22), GLP-1 inhibitors such as liraglutide (Ch. 40) or topiramate (Ch. 23). Treatments under investigation that interfere with the many neurotransmitter systems that regulate weight promise to offer more effective pharmacotherapy than the current limited range of options.
Bariatric surgery to restrict the size of the stomach (gastroplasty: gastric banding or vertical sleeve gastrectomy) or gastric bypass (such as Roux-en-Y) are used in the morbidly obese (BMI >40 kg⋅m−2), or those with a BMI over 35 kg⋅m−2 and an obesity-related medical condition.
Current drug and lifestyle treatments for obesity can be expected to produce weight loss of about 10–15%, which is often enough to ameliorate obesity-related metabolic disorders and their accompanying clinical manifestations. Bariatric surgery produces an average weight loss of 25–30%. The management of obesity should be carried out by a multidisciplinary team who can advise on lifestyle and other treatment options.
True/false questions
1. The posterior pituitary is the main central nervous system site of appetite control.
2. Ghrelin is an orexigenic hormone.
3. Satiety signals include insulin and leptin.
4. Orlistat acts centrally to inhibit release of orexigenic neurotransmitters.
5. Vitamin D deficiency can occur with orlistat treatment.
6. Methylcellulose should be taken with water.
7. Drug treatment for obesity should be restricted to individuals with a body mass index (BMI) of more than 30 kg⋅m−2.
8. Weight loss is usually sustained after 12 months of orlistat treatment.
1. False. The hypothalamus and higher brain centres are most important in regulating food intake.
2. True. Ghrelin is produced by the gut pre-prandially and has an orexigenic (appetite-stimulating) action on the hypothalamus.
3. True. Satiety signals to the hypothalamus include insulin (from the pancreas), leptin (from fat stores) and gut peptides such as cholecystokinin, oxyntomodulin and peptide YY3-36.
4. False. Orlistat reduces fat absorption in the gut by inhibiting pancreatic lipase.
5. True. People taking orlistat may unduly restrict their fat intake to avoid steatorrhoea, leading to reduced absorption of fat-soluble vitamin D.
6. True. Methylcellulose produces satiety by swelling rapidly when hydrated and should be taken with water.
7. True. Drug treatment should be restricted to obese people with BMI over 30 kg⋅m−2 (or >28 kg⋅m−2 in those with Type 2 diabetes, hypertension or hypercholesterolaemia).
8. False. Weight loss with orlistat often reverses gradually after stopping the drug; lifestyle measures including diet and exercise are important in long-term weight control.
Compendium: drugs used in obesity
| Drug | Kinetics (half-life) | Comments |
| Methylcellulose | Not absorbed | Bulk-forming agent taken before meals to produce satiety; taken with water to avoid oesophageal obstruction; little evidence of efficacy in obesity; also used as laxative (Ch. 35) |
| Orlistat | Negligible absorption (about 1%) and low systemic exposure in clinical use | Pancreatic lipase inhibitor; acts within intestine; taken orally before, during or immediately after a meal |
Eckel, RH. Non-surgical management of obesity. N Engl J Med. 2008;358:1941–1950.
Haslam, DW, James, WPT. Obesity. Lancet. 2005;366:1197–1209.
Mingfang, L, Cheung, BMY. Pharmacotherapy for obesity. Br J Clin Pharmacol. 2009;68:804–810.
Padwal, RS, Majumdar, SR. Drug treatments for obesity: orlistat, sibutramine, and rimonabant. Lancet. 2007;369:71–77.
Sargent, BJ, Moore, NA. New central targets for the treatmengt of obesity. Br J Clin Pharmacol. 2009;68:852–860.