DISORDERS OF THE MALE REPRODUCTIVE SYSTEM
Urethritis and urethral strictures are common disorders of the male urethra. Urethral carcinoma occurs in men older than 60 years, but it is an extremely rare form of cancer.
Urethritis
Urethritis is an inflammatory process of the urethra without concurrent bladder infection that is usually, but not always, caused by a sexually transmitted microorganism. Biologic agents associated with infectious urethritis in males include N. gonorrhoeae and C. trachomatis, U. urealyticum, and other, less common, mycobacteria; parasites (e.g., Trichomonas vaginalis); and viruses (herpes simplex virus [HSV]).126,127 Infectious urethritis caused by N. gonorrhoeae often is called gonococcal urethritis (GU); infection caused by other microorganisms is called nongonococcal urethritis (NGU).128 (Sexually transmitted urethritis is described in Chapter 24.) Nonsexual origins of urethritis include inflammation or infection as a result of urologic procedures, insertion of foreign bodies into the urethra, anatomic abnormalities, or trauma.
Noninfectious urethritis is rare and is associated with the ingestion of wood alcohol, ethyl alcohol, or turpentine. It is seen also with Reiter syndrome, which involves a number of mucocutaneous lesions.
Symptoms of urethritis include urethral tingling, itching, or burning sensation on urination (dysuria), frequency, and urgency. The individual may note a purulent or clear mucus-like discharge from the urethra. Nucleic acid detection amplification tests allow easy detection of N. gonorrhoeae and C. trachomatis in first-void urine.128 Treatment consists of appropriate antibiotic therapy for infectious urethritis and avoidance of future chemical or mechanical irritation.
Urethral Stricture
A urethral stricture is a fibrotic narrowing of the urethra caused by scarring. The scars may be congenital but are more likely to result from trauma or untreated or severe urethral infections, most often from long-term use of indwelling urinary catheters. Large catheters and instruments cause internal trauma and ischemia, whereas external trauma, such as pelvic fracture, can partially or completely sever the urethra and cause severe and complex strictures.129 In addition, a report has concluded that stricture may occur decades after initial hypospadias surgery.130 Urethral carcinoma is a less common cause of urethral stricture. Prostatitis and infection secondary to urinary stasis are common complications. Severe and prolonged obstruction can result in hydronephrosis and renal failure. In addition, chronic, severe strictures may lead to urethral fistulas and periurethral abscesses.129
The clinical manifestations of urethral stricture are caused by bladder outlet obstruction. The primary symptom is diminished force and caliber of the urinary stream; other symptoms include urinary frequency and hesitancy, mild dysuria, double urine stream or spraying, and postvoiding dribbling. Symptoms of acute urinary retention may occur in the presence of infection or urinary obstruction. Induration at the stricture site may be palpable. Tender, enlarged masses along the urethra usually indicate periurethral abscesses.
Urethral stricture is diagnosed on the basis of history, physical examination, urinary flow rates, voiding cystourethrogram, and urethroscopy; biopsy confirms carcinoma. Treatment is usually surgical and may involve urethral dilation, urethrotomy, or a variety of open surgical techniques. The choice of surgical intervention depends on the age of the individual and the severity of the problem. Strictures may recur up to 1 year after treatment. Follow-up is necessary during this time; urinary flow measurements and urethrogram help determine extent of residual obstruction.
Disorders of the Penis
Phimosis and paraphimosis are disorders in which the foreskin (prepuce) is “too tight” to be moved easily over the glans penis. Phimosis is a condition in which the foreskin cannot be retracted back over the glans, whereas paraphimosis is the opposite: the foreskin is retracted and cannot be moved forward (reduced) to cover the glans (Figure 23-22). Both conditions can cause penile pathologic conditions.
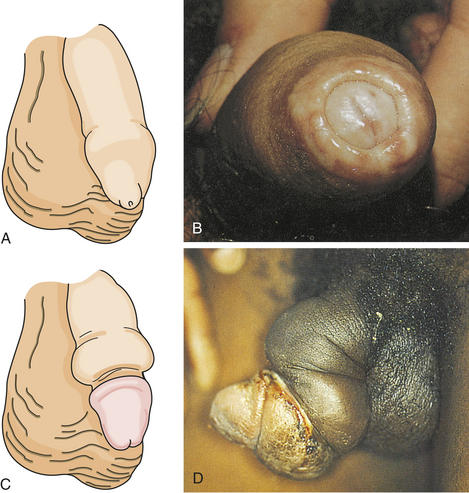
Figure 23-22 Phimosis and paraphimosis. A, Phimosis: the foreskin has a narrow opening that is not large enough to permit retraction over the glans. B, Lesions on the prepuce secondary to infection cause swelling, and retraction of foreskin may be impossible. C, Paraphimosis: the foreskin is retracted over the glans but cannot be reduced to its normal position. Here it has formed a constricting band around the penis. D, Ulcer on the retracted prepuce with edema. (A, C from Phipps WP, Sand JK, Marek JF: Medical-surgical nursing: concepts and clinical practice, ed 6, St Louis, 1999, Mosby; B from Taylor PK: Diagnostic picture tests in sexually transmitted diseases, London, 1995, Mosby-Wolfe; D from Morse SA, Moreland AA, Holmes KK: Atlas of sexually transmitted diseases and AIDS, ed 2, London, 1996, Mosby-Wolfe.)
The inability to retract the foreskin is normal in infancy and is caused by congenital adhesions. During the first 3 years of life, these adhesions separate naturally with penile erections and are not an indication for circumcision. Although most cases occur in uncircumcised males, stenosis and resultant phimosis can occur in males with excessive skin remaining after circumcision.129 Phimosis can occur at any age and is caused most commonly by poor hygiene and chronic infection. Chronic balanoposthitis (inflammation of the glans and prepuce) predisposes older diabetic men to phimosis. It rarely occurs with normal foreskin.
Edema, erythema, and tenderness of the prepuce and purulent discharge are usually the reasons for seeking treatment; inability to retract the foreskin is a less common complaint. Circumcision, if needed, is performed after infection has been eradicated. Complications of phimosis include inflammation of the glans (balanitis) or prepuce (posthitis) and paraphimosis. There is a higher incidence of penile carcinoma in uncircumcised males, but chronic infection, most likely with HPV, is usually the underlying factor in such cases.131,132
Paraphimosis, in which the foreskin is retracted, can constrict the penis, causing edema of the glans. If edema is such that the foreskin cannot be reduced manually, surgery must be performed to prevent necrosis of the glans caused by constricted blood vessels. Severe paraphimosis is a surgical emergency and phimosis may require immediate release if there is urinary obstruction.
Peyronie Disease
Peyronie disease (bent nail syndrome) is a fibrotic condition of the tunica albuginea of the penis resulting in varying degrees of curvature and sexual dysfunction133 (Figure 23-23). Peyronie disease develops slowly and is characterized by tough, fibrous thickening of the fascia in the erectile tissue of the corpora cavernosa. A dense fibrous plaque is usually palpable on the dorsum of the penile shaft. The problem usually affects middle-age men and is associated with painful erection, painful intercourse (for both partners), and poor erection distal to the involved area. In some cases, impotence or unsatisfactory penetration occurs. There is no pain when the penis is flaccid.

Figure 23-23 Peyronie disease. (From Taylor PK: Diagnostic picture tests in sexually transmitted diseases, London, 1995, Mosby-Wolfe.)
Although the exact cause is unknown, a local vasculitis-like inflammatory reaction occurs and decreased tissue oxygenation results in fibrosis and calcification. Peyronie disease is associated with Dupuytren contracture (a flexion deformity of the fingers or toes caused by shortening or fibrosis of the palmar or plantar fascia), diabetes, tendency to develop keloids, and in rare cases, use of beta-blocker medications.
There is no definitive treatment for Peyronie disease. Spontaneous remissions occur in as many as 50% of cases. Treatment with pharmacologic therapies include colchicine, aminobenzoate potassium (Potaba), L-carnitine, and liposomal superoxide dismutase.133 Placation, as well as surgical resection of the fibrous plaque followed by grafting, has been successful.129
Priapism
Priapism is an uncommon condition of prolonged penile erection. It is usually painful and is not associated with sexual arousal (Figure 23-24). Priapism is idiopathic in 60% of cases; the remaining 40% of cases are associated with spinal cord trauma, sickle cell disease, leukemia, pelvic tumors or infections, or penile trauma. Priapism also has been associated with cocaine use.134 Intracavernous injection therapy for impotence seems to be the most common cause. Prolonged sexual stimulation often is associated with initial development of the idiopathic type.129 The two corpora cavernosa within the erect penis are filled with blood and are tender to palpation; neither the corpus spongiosum nor the glans is engorged. The vascular congestion is thought to be associated with venous obstruction. If the erection remains over a period of days, edema and fibrosis develop, leading to erectile dysfunction (impotence).

Figure 23-24 Priapism. (From Lloyd-Davies RW et al: Color atlas of urology, ed 2, London, 1994, Mosby-Wolfe.)
Priapism is a urologic emergency. Treatment within hours is effective and prevents impotence. Conservative approaches include iced saline enemas, ketamine administration, and spinal anesthesia. Needle aspiration of blood from the corpus through the dorsal glans is often effective and is followed by catheterization and pressure dressings to maintain decompression. More aggressive surgical treatments include the creation of vascular shunts to maintain blood flow. Erectile dysfunction results in up to 50% of prolonged cases.
Balanitis
Balanitis is an inflammation of the glans penis (Figure 23-25) and usually occurs in conjunction with posthitis, an inflammation of the prepuce. It is associated with poor hygiene and phimosis. The accumulation under the foreskin of glandular secretions (smegma), sloughed epithelial cells, and Mycobacterium smegmatis can irritate the glans directly or lead to infection. Skin disorders (e.g., psoriasis, lichen planus, eczema) and candidiasis must be differentiated from inflammation resulting from poor hygienic practices. Balanitis is seen most commonly in men with poorly controlled diabetes mellitus and candidiasis. Antimicrobials are used to treat infection. Circumcision can prevent recurrences and can be considered after the inflammation has subsided.

Penile Cancer
In the United States, carcinoma of the penis is rare and affects about 1 in 100,000 men. Approximately 1290 cases and 290 deaths were estimated in the year 2009.1 Although rare in North America and Europe, where it accounts for about 0.2% of cancers and 0.1% of cancer deaths in men, penile cancer may account for up to 10% of cancers in African and South American men.
In the United States it is twice as common in black men than in white men131 and in men older than age 50.135 Major risk factors include infection with HPV (mainly serotypes 16, 18, 33, 35, and 45), smoking, and psoriasis treated with a combination involving the drug psoralen and ultraviolet (UV) light. Men circumcised at birth have less than half the chance of getting penile cancer than those who were not.131 Penile cancer is more common in men with phimosis and those with AIDS.131 About two thirds of men with penile cancer are diagnosed at more than 65 years of age.1
Before the development of penile cancer, signs of premalignant cancer or epidermal cancer in situ are present.136 These include thick white plaque (leukoplakia) that typically involves the meatus; red, inflamed areas of Paget disease; red, velvety, ulcerative lesions of erythroplasia of Queyrat that usually involve the glans; large, invasive, scaly growths of Buschke-Löwenstein tumor; red plaque with encrustations of Bowen disease; and in situ carcinoma that generally affects the penile shaft. Men with leukoplakia or erythroplasia of Queyrat may have concurrent invasive penile carcinoma.131,137 Pain and bleeding are late signs of penile cancer. Condylomata (genital warts) caused by HPV may be involved in the development of precancerous lesions (see Chapter 24 for a discussion of HPV). At times the penis might be the site of metastatic spread of solid tumors from the bladder, prostate, rectum, or kidney. Early squamous cell carcinoma and premalignant epidermal lesions are easily treated but are often ignored. Delays in seeking treatment are attributed to denial, embarrassment, failure to detect lesions under a phimotic foreskin, fear, guilt, and ignorance.
Penile cancer is mostly squamous cell carcinoma, which usually begins as a small, fat, ulcerative or papillary lesion on the glans or foreskin that grows to involve the entire penile shaft (Figure 23-26). Extensive lesions are associated with metastases and a poor prognosis. These lesions are not as painful as the amount of tissue involvement would seem to indicate. The regional femoral and iliac nodes are common metastatic sites. Rarely the urethra and bladder are involved. Weight loss, fatigue, and malaise accompany chronic suppurative lesions. Untreated, progressive disease causes death within 2 years.
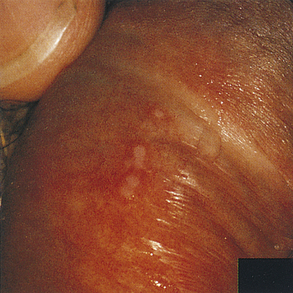
Figure 23-26 Carcinoma in situ of penis. Flat papules turn white after diagnostic treatment with acetic acid. (From Morse SA, et al: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
The specific diagnosis is made by biopsy after examination to document the location, size, and fixation of the lesion. After a positive biopsy, the extent of cancer spread is determined by imaging tests such as ultrasound, CT, or MRI. Fine-needle aspiration of lymph tissue confirms absence or presence of regional adenopathy.131 About 30% of penile cancers spread to lymph nodes before diagnosis.135 Distant metastases occur in less than 10% of cases and may involve lung, liver, bone, or brain.137 Staging of penile cancer uses a system created by the American Joint Committee on Cancer (AJCC) and the International Union Against Cancer (IUCC). The AJCC/IUCC staging system is also known as the tumor, node, metastasis (TNM) system.1 Although this system initially seems cumbersome, it is a simple and easy method of communicating degree of cancer (Box 23-12).
For invasive penile carcinoma, complete excision leaving adequate tumor-free margins is the goal. A simple circumcision may be sufficient for localized lesions of the prepuce. If the primary site is glans and distal shaft, removal of the penis may be necessary. Although conventional radical surgery continues to be an effective approach, the emasculating nature of the treatment has serious psychologic and sexual consequences. Recent studies have challenged the conventional belief that a 2-cm margin was required for adequate cancer control.138 Newer innovative surgical techniques can now preserve as much penile tissue and functional integrity as possible without compromising cancer control. Inguinal lymph nodes also are removed if metastasis to these structures is known or suspected. Palliative treatment with radiation or chemotherapy may be used when the disease is inoperable and bulky inguinal metastases have occurred. Options for individuals with carcinoma in situ include local excision, radiation, laser surgery, cryosurgery, chemosurgery, or chemotherapy with topical (5%) 5-FU. Differentiation, tumor stage, and age influence prognosis.139 The 5-year survival rate for stage I disease is greater than 80%1,135; average 5-year survival rate for all stages is 50%.1,131
Disorders of the Scrotum, Testis, and Epididymis
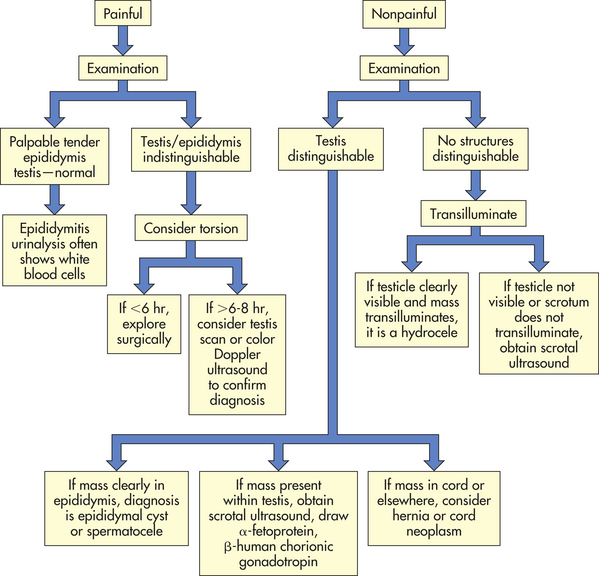
Men may seek treatment for painful or painless scrotal masses. Masses may be serious (cancer or torsion) or benign (hydrocele or cyst); they may require immediate surgical intervention or allow for careful observation. A flow diagram for diagnosing scrotal masses140 is provided in Figure 23-27.
Varicocele, hydrocele, and spermatocele are common intrascrotal disorders.141–143 A varicocele is an abnormal dilation of a vein within the spermatic cord and is classically described as a “bag of worms” (Figure 23-28). Most (95%) occur on the left side and may be painful or tender. Varicocele occurs in 10% of males and is seen most often after puberty. Sudden development of a varicocele in an older man is a late sign of renal tumor.142 Unilateral right-sided varicoceles are rare and result from compression or obstruction of the inferior vena cava by a tumor or thrombus. Color Doppler ultrasonography is used to confirm the diagnosis.140
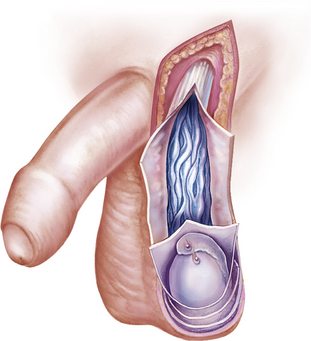
Figure 23-28 Varicocele. Dilation of veins within the spermatic cord. (From Seidel H et al: Mosby’s guide to physical examination, ed 4, St Louis, 1999, Mosby.)
The cause of varicocele is incompetent or congenitally absent valves in the spermatic veins. The valves that normally prevent backflow are absent or do not close adequately, permitting blood to pool in the veins rather than flow into the venous system. Varicocele decreases blood flow through the testis. This interferes with spermatogenesis and is a cause of infertility.141,142 If infertility is a problem, treatment consists of ligation of the spermatic vein or occlusion of the vein by percutaneous methods, such as balloon catheter and sclerosing fluids.142,144 If varicocele is mild and fertility is not an issue, a scrotal support usually is sufficient to relieve symptoms of scrotal heaviness or “dragging.”
A hydrocele is a collection of fluid within the tunica vaginalis140–142 (Figure 23-29). It is the most common cause of scrotal swelling. Hydroceles occur in 6% of male newborns and are congenital malformations (patent processus vaginalis) that often resolve spontaneously in the first year of life. Surgical ligation is recommended if hydrocele persists after age 1 year.143 Hydroceles in adults may be caused by an imbalance between the secreting and absorptive capacities of scrotal tissues. Hydroceles range in size from slightly larger than the testes to the size of a grapefruit or larger and may be flaccid or tense. Compression of testicular blood supply may lead to atrophy.
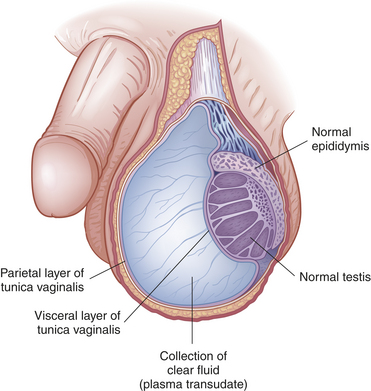
Figure 23-29 Hydrocele. Accumulation of clear fluid between the visceral and parietal layers of the tunica vaginalis.
The exact mechanism of idiopathic hydrocele is unknown. Secondary hydrocele may result from trauma or infection of the testis or epididymis or from a testicular tumor. Rapid accumulation of fluid occurs after local injury, radiotherapy, or infection (epididymitis or orchitis), or it may accompany testicular neoplasm. Chronic hydroceles are more common and occur in men older than 40 because of an imbalance between fluid secretion and reabsorption in the tunica vaginalis. A painless, extratesticular mass that easily transilluminates is found on physical examination. Ultrasonography of a large hydrocele, which may conceal a testicular tumor, is recommended. Treatment is usually not required unless a large, bulky hydrocele causes considerable physical discomfort or undesirable cosmetic appearance.141 Treatment for uncomplicated hydrocele is aspiration of the fluid and injection of a sclerosing agent into the scrotal sac.140,145 The goal of treatment is to remove the hydrocele and prevent recurrence by sclerosing or excising the tunica vaginalis.
A spermatocele is a painless diverticulum of the epididymis located between the head of the epididymis and the testis. In other words, efferent ducts of the epididymis have potential for cystic dilation to form a spermatocele140,142 (Figure 23-30). Spermatoceles are filled with milky fluid that contains sperm. Spermatocele is differentiated from a hydrocele in that aspiration of the hydrocele recovers a clear, yellow fluid, and unlike a hydrocele, a spermatocele does not cover the entire anterior surface of the testis. An epididymal cyst is similar to a spermatocele but does not communicate with the epididymis. Spermatoceles and epididymal cysts manifest as discrete, firm, freely mobile masses distinct from the testis that may be transilluminated. Epididymal cysts do not require treatment.140 A spermatic cord tumor may feel like a tense spermatocele but does not contain fluid and will not transilluminate.142 Spermatoceles that cause pain or discomfort are excised. Usually, however, spermatoceles are asymptomatic or produce mild discomfort that is relieved by scrotal support. Neither hydroceles nor spermatoceles are associated with infertility.

Figure 23-30 Spermatocele. Retention cyst of the head of the epididymis or of an aberrant tubule or tubules of the rete testis. The spermatocele lies outside the tunica vaginalis; therefore, on palpation it can be readily distinguished and separated from the testis. (From Lloyd-Davies RW, Gow JG, Davies DR: Color atlas of urology, ed 2, London, 1994, Mosby-Wolfe.)
Cryptorchidism and Ectopy
Cryptorchidism is a condition of testicular maldescent, whereas an ectopic testis has strayed from the normal pathway of descent. Ectopy may be caused by an abnormal connection at the distal end of the gubernaculum testis that leads the gonad to an abnormal position, usually at the superficial inguinal site. In cryptorchidism the descent of one or both testes is arrested, with unilateral arrest occurring more often than bilateral arrest.142 The testes may remain in the abdomen, or testicular descent may be arrested in the inguinal canal or the puboscrotal junction. About 3% to 6% of full-term infants and 20% to 30% of premature male infants have undescended testes at birth143; half of such testes descend in the first month of life and a few more at puberty. The incidence of cryptorchidism in adults is 0.7% to 0.8%.142 Cryptorchidism is commonly associated with vasal or epididymal abnormalities. These congenital anomalies affect about one third to two thirds of newborns with cryptorchidism. Other structural anomalies include posterior urethral valves (less than 5%), upper tract abnormalities (less than 5%), and hypospadias. The presence of hypospadias as well as cryptorchidism raises the suspicion of mixed gonadal dysgenesis (intersex infant). It has been hypothesized that cryptorchidism may result from an absence or abnormality of the gubernaculum, a cordlike structure that extends from the lower pole of the testis to the scrotum; a congenital gonadal or dysgenetic defect that makes the testis insensitive to gonadotropins (a likely explanation for unilateral cryptorchidism); or lack of maternal gonadotropins (a likely explanation for bilateral cryptorchidism of prematurity).142 Mechanical possibilities include a short spermatic cord, fibrous bands or adhesions in the normal path of the testes, or a narrowed inguinal canal. Chromosomal studies do not support a genetic component. Physiologic cryptorchidism, also called retractile or migratory testis, is an involuntary retraction of the testes out of the scrotum that occurs with excitement, physical activity, or exposure to cold and is caused by the small mass of prepubertal testis and the strength of the cremaster muscle. This is a common phenomenon that is self-limiting (descent occurs at puberty).
Physical examination discloses the absence of one or both testes in the scrotum and an atrophic scrotum on the affected side. If the undescended testis is in a vulnerable position, for example, over the pubic bone, an individual may complain of severe pain secondary to trauma. The adult male with bilateral cryptorchidism may be infertile. Ultrasonography, CT, or MRI can be used to locate an intra-abdominal or nonpalpable testis.
Undescended testes are susceptible to neoplastic processes: the risk of testicular cancer is 35 to 50 times greater for men with cryptorchidism or a history of cryptorchidism than for the general male population. Because definite histologic change (decreased Leydig cells, loss of germ cells, and peritubular fibrosis) occurs in the cryptorchid testis by 1 year of age, surgical correction is recommended earlier.142,146 Treatment often begins with administration of GnRH or hCG, hormones that may initiate descent, making surgery unnecessary. GnRH is given as a nasal spray in Europe and may enhance germ-cell counts even when the testis does not descend.146 If hormonal therapy is not successful, the testis is located and moved surgically (orchiopexy) in young children or removed (orchiectomy) in adults and children older than 10 years.142,146 The testis that is properly placed in the scrotum provides adequate hormonal function and gives the scrotum a normal appearance. A successful operation does not ensure fertility if the testis is congenitally defective. Approximately 20% of males with unilateral undescended testis remain infertile even though orchiopexy is performed by age 1 year; most individuals with treated or untreated bilateral testicular maldescent have poor fertility. In addition, placement of the cryptorchid testis into the scrotal sac does not decrease the potential for malignancy; it does facilitate examination and tumor detection.
Torsion of the Testis
Torsion of the testis is rotation of a testis, which twists blood vessels in the spermatic cord. It causes an acute scrotum, which is testicular pain and swelling (Figure 23-31). Differentiation between testicular torsion and two other common causes of an acute scrotum is based on physical examination and history140,143 (Table 23-10). This event is most common among neonates and pubertal adolescents, but it can occur in males at any age.140,143 Onset may be spontaneous or follow physical exertion or trauma. Torsion twists the arteries and veins in the spermatic cord, reducing or stopping circulation to the testis. Vascular engorgement and ischemia develop, causing scrotal swelling and pain. These manifestations are not relieved by scrotal elevation (Prehn sign), rest, or scrotal support. On physical examination, men have a tender, high-riding testis, a thickened spermatic cord, and an absent cremasteric reflex. Unlike epididymitis, the epididymis cannot be differentiated from the testis.143 Diagnostic testing includes urinalysis (to rule out infection) and color Doppler ultrasonography.125,142,143 Torsion of the testis is a surgical emergency. If the torsion cannot be reduced manually, surgery must be performed within 6 hours after the onset of symptoms to preserve normal testicular function. Surgery includes untwisting the spermatic cord and anchoring both testes in correct position within the scrotum to prevent recurrences. With successful manual detorsion, surgical fixation should be done within a few days.


Orchitis
Orchitis is an acute inflammation of the testes (Figure 23-32) and is uncommon except as a complication of systemic infection or as an extension of an associated epididymitis127 (see p. 859). Infectious microorganisms may reach the testes through the blood or the lymphatics or, most commonly, by ascent through the urethra, vas deferens, and epididymis. Most cases of orchitis are actually cases of epididymo-orchitis. Occasionally, in middle-age men, a nonspecific, apparently noninfectious, inflammatory process (called granulomatis orchitis) can occur. It seems to be an autoimmune disease that triggers a granulomatous response to spermatozoa.
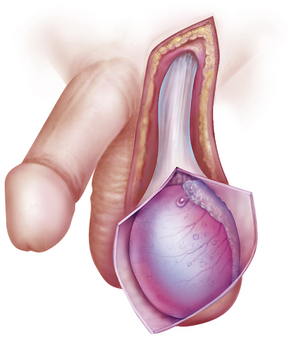
Figure 23-32 Orchitis. (From Seidel H et al: Mosby’s guide to physical examination, ed 4, St Louis, 1999, Mosby.)
Mumps is the most common infectious cause of orchitis and usually affects postpubertal males. The onset is sudden, occurring 3 to 4 days after the onset of parotitis. Signs and symptoms include high fever, reaching 40° C (104° F), marked prostration, bilateral or unilateral erythema, edema and tenderness of the scrotum, and leukocytosis. An acute hydrocele may develop. Urinary signs and symptoms, which accompany epididymitis, are absent. Atrophy with irreversible damage to spermatogenesis may result in 30% of affected testes. Bilateral orchitis does not affect androgenic function but may cause permanent sterility.
Treatment is supportive and includes bed rest, scrotal support, elevation of the scrotum, hot or cold compresses, and analgesic agents for relief of pain. If an acute hydrocele develops, it is aspirated. Testicular abscess usually requires orchiectomy (removal of the testis). Appropriate antimicrobial drugs should be used for bacterial orchitis, and corticosteroids are indicated in proved cases of nonspecific granulomatous orchitis.
Cancer of the Testis
Testicular cancer is among the most curable of cancers; for nearly all common types, cure rates are more than 95%. Overall, testicular cancers are rare, accounting for only 1% of cancers and 0.24% of cancer deaths1 in men, yet they are the most common form of cancer in young men between ages 15 and 35. Approximately 8400 cases and 380 deaths were estimated for 2009.1 In the United States, the lifetime probability of developing testicular cancer is 0.2% for white men, an incidence that is four times higher than for blacks. Testicular tumors are slightly more common on the right side than on the left, a pattern that parallels the occurrence of cryptorchidism; about 1% to 2% of primary testicular cancers are bilateral (Figure 23-33), and 50% of these tumors arise from treated or untreated cryptorchid testes.

Figure 23-33 Testicular tumor. (From 400 Self-assessment picture tests in clinical medicine, London, 1984, Wolfe Medical.)
PATHOGENESIS Ninety percent of testicular cancers are germ-cell tumors arising from the male gametes. Germ-cell tumors constitute 90% of testicular cancers and can be broadly classified into two types: seminomas and nonseminomas. Seminomas are the most common, are the least aggressive, and make up about 30% to 35% of testicular cancers. Nonseminomas include embryonal carcinomas, teratomas, and choriocarcinomas, the most aggressive but rare (less than 1%) form of testicular cancer. Testicular cancers can include a mix of types.147 In addition, testicular tumors can arise from specialized cells of the gonadal stroma. These tumors, which are named for their cellular origins, are Leydig cell, Sertoli cell, granulosa cell, and theca cell tumors and constitute less than 10% of all testicular cancers.148
The cause of testicular neoplasms is unknown. A genetic predisposition is suggested by the fact that the incidence is higher among brothers, identical twins, and other close male relatives. Genetic predisposition is supported further by statistics showing that the disease is relatively rare among black Africans, black Americans, Asians, and native New Zealanders. Risk factors include history of cryptorchidism, abnormal testicular development, HIV and AIDS, Klinefelter syndrome, and history of testicular cancer.147
CLINICAL MANIFESTATIONS Painless testicular enlargement commonly is the first sign of testicular cancer. Enlargement is usually gradual and may be accompanied by a sensation of testicular heaviness or dull ache in the lower abdomen.147,148 Occasionally, acute pain occurs because of rapid growth, resulting in hemorrhage and necrosis. Ten percent of affected men have epididymitis, 10% have hydroceles,148 and 5% have gynecomastia or hydrocele. Incidence of gynecomastia increases considerably (30% to 45%) in men with Sertoli or Leydig tumors. Approximately 10% of individuals already have symptoms related to metastases at the time of initial diagnosis, which correlates with the typical delay of 3 to 6 months from initial recognition to definitive treatment. Lumbar pain may be present and usually is caused by retroperitoneal node metastasis. Signs of metastasis to the lungs include cough, dyspnea, and bloody sputum (hemoptysis). Supraclavicular node involvement may cause difficulty swallowing (dysphagia) and neck swelling. Alterations in vision or mental status, papilledema, and seizures may be experienced with metastasis to the CNS. Approximately 10% of affected individuals are asymptomatic; the tumor may be detected by the man’s sexual partner or incidentally following trauma.
EVALUATION AND TREATMENT An incorrect diagnosis at the initial examination occurs in as many as 25% of men with testicular cancer. Epididymitis and epididymo-orchitis are the most common misdiagnoses; others include hydrocele and spermatocele. Evaluation begins with careful physical examination, including palpation of the scrotal contents with the individual in the erect and supine positions. The abdomen and lymph nodes are palpated to rule out metastases. Signs of testicular cancer include abnormal consistency, induration, nodularity, or irregularity of the testis. A firm, nontender testicular mass or diffuse enlargement is found in the majority of cases. Primary testicular cancer can be assessed rapidly and accurately by scrotal ultrasonography. Tumor markers are higher than normal in the presence of a tumor and may help detect a tumor that is too small to be palpated during physical examination or seen on imaging.147 Tumor type is identified after inguinal biopsy or orchiectomy. Scrotal incisions may cause dissemination of the tumor and increase the risk of local recurrence and therefore are avoided. Chest x-ray, lymphangiogram, IVP, abdominal ultrasound, and CT are used in clinical staging of disease. Treatment is based on type of tumor, stage of disease, general health, and age. Besides surgery, treatment involves radiation and chemotherapy singly or in combination. A number of factors influence the prognosis (Table 23-11). They include histology of the tumor, stage of the disease, and selection of appropriate treatment. Serum markers, such as AFP, β-hCG, and lactate dehydrogenase, are useful for detecting metastases and assessing responses to therapy. Most individuals treated for cancer of the testis can expect a normal life span, although some have persistent paresthesias, Raynaud phenomenon, or infertility. Almost 90% of disease-related deaths occur in the first 2 years after cessation of therapy; disease-free survival of 3 years is considered a cure. Approximately 10% of men treated for testicular cancer will experience a relapse; if the relapse is discovered early and treated, 99% can be cured. Orchiectomy does not affect sexual function, but infertility can result from chemotherapy or surgical removal of affected abdominal lymph nodes if nerves necessary for ejaculation are severed. After orchiectomy, testicular silicone implants may be used to restore “normal” scrotal appearance.
Table 23-11
Testicular Tumors of Germ-Cell Origin
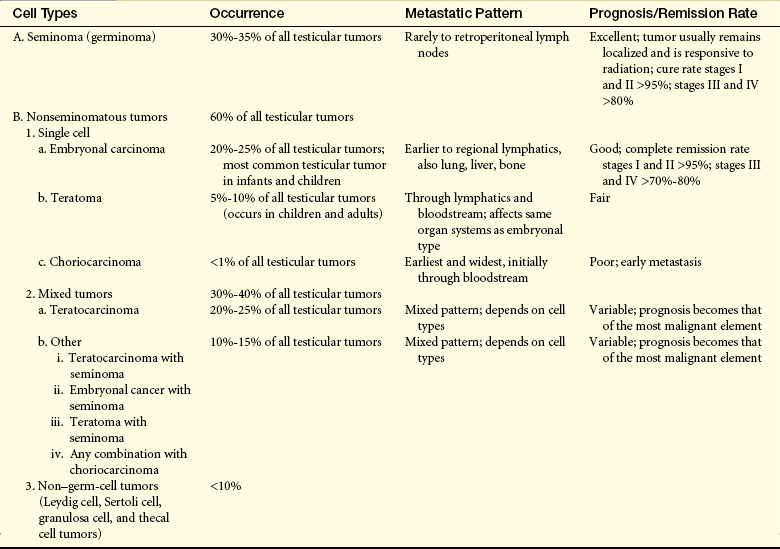
Data from American Cancer Society. In Cancer response system document #10029, New York, 1995, The Society; Cancer Net: Cancer facts: questions and answers about testicular cancer, National Cancer Institute, 2000. Available at www.cancernet.nci.nih.gov.
Epididymitis
Epididymitis, or inflammation of the epididymis, generally occurs in sexually active young males (younger than 35 years) and is rare before puberty (Figure 23-34). In young men the usual cause is a sexually transmitted microorganism, such as N. gonorrhoeae or C. trachomatis. Men who practice unprotected anal intercourse may acquire sexually transmitted epididymitis because of E. coli, H. influenzae, tuberculosis (especially in regions where incidence of pulmonary tuberculosis is high), Cryptococcus, or Brucella.149 In men older than 35 years, Enterobacter (intestinal bacteria) and Pseudomonas aeruginosa associated with urinary tract infections and prostatitis also may cause epididymitis. Besides an infectious etiology, epididymitis may result from a chemical inflammation caused by the reflux of sterile urine into the ejaculatory ducts.149,150 It is associated with urethral strictures, congenital posterior valves, and excessive physical straining in which increased abdominal pressure is transmitted to the bladder. Chemical epididymitis is usually self-limiting and does not require evaluation or intervention unless it persists.

Figure 23-34 Epididymitis secondary to gonorrhea or nongonococcal urethritis. Secondary to gonorrhea or nongonococcal urethritis, this infection spread to the testes, and rupture through the scrotal wall is threatened. (From Taylor PK: Diagnostic picture tests in sexually transmitted diseases, London, 1995, Mosby-Wolfe.)
PATHOPHYSIOLOGY The pathogenic microorganism usually reaches the epididymis by ascending the vasa deferentia from an already infected urethra or bladder. The presence of bacteria initiates the inflammatory response, causing symptoms of bacterial epididymitis. Epididymitis caused by heavy lifting or straining results from reflux of urine from the bladder into the vas deferens and epididymis. Urine is extremely irritating to the epididymis and initiates an inflammatory response called chemical epididymitis.
CLINICAL MANIFESTATIONS Pain is the main symptom of epididymitis. Scrotal or inguinal pain is caused by inflammation of the epididymis and surrounding tissues. The pain is usually acute and severe. Flank pain may occur if, as the urethra passes over the spermatic cord, edematous swelling of the cord obstructs the urethra. The individual may have pyuria and bacteriuria and a history of urinary symptoms, including urethral discharge. The scrotum on the involved side is red and edematous as a result of inflammatory changes. The tail of the epididymis near the lower pole of the testis usually swells first; then swelling ascends to the head of the epididymis. The spermatic cord also may be swollen and tender.
Complications of epididymitis include abscess formation, infarction of the testis, recurrent infection, and infertility. Infarction probably is caused by thrombosis (obstruction by blood clots) of the prostatic vessels secondary to severe inflammation. Recurrent epididymitis may result from inadequate initial treatment or failure to identify or treat predisposing factors. Chronic epididymitis can cause scarring of the epididymal endothelium. Once scarring has occurred, treatment with antibiotics is ineffective because adequate antibiotic levels cannot be achieved within the epididymis.149,150
EVALUATION AND TREATMENT A history of recent urinary tract infection or urethral discharge suggests the diagnosis of epididymitis. The relief of pain when the inflamed testis and epididymis are elevated (Prehn sign) is also diagnostic. Definitive diagnosis is based on culture or Gram stain of a urethral swab. Epididymal aspiration may be necessary to obtain a specimen, especially if the individual has been taking antibiotics and has sterile urine.
Treatment includes antibiotic therapy for the infection itself (see Chapter 24) and various measures to provide symptomatic relief. Bed rest and scrotal elevation are recommended until the scrotum is no longer tender. Scrotal elevation facilitates maximal lymphatic and venous drainage. Abscess formation is rare with antibiotic therapy. If an abscess occurs and persists, it is drained surgically and an orchiectomy may be indicated. Complete resolution of swelling and pain may take several weeks to months. The individual’s sexual partner should be treated with antibiotics if the causative microorganism is a sexually transmitted pathogen.
Disorders of the Prostate Gland
Benign prostatic hyperplasia (BPH), also called benign prostatic hypertrophy, is the enlargement of the prostate gland (Figure 23-35). (Because the major prostatic changes are caused by hyperplasia, not hypertrophy, benign prostatic hyperplasia is the preferred term.) This condition becomes problematic as prostatic tissue compresses the urethra, where it passes through the prostate. The prevalence among U.S. men 60 years and older is about 50% and among men 70 years or older 90%. 151 BPH is common and involves a complex pathophysiology with several endocrine and local factors and remodeled microenvironment. Its relationship to aging is well documented. At birth the prostate is pea sized, and growth of the gland is gradual until puberty. A period of rapid development continues until the third decade of life, when the prostate reaches adult size. Around 40 to 45 years of age, benign hyperplasia begins and continues slowly until death. Although dihydrotestosterone (DHT) is necessary for normal prostatic development, its role in BPH remains unclear. Among all androgen-metabolizing enzymes within the human prostate, 5α-reductase is the most powerful. This reductase corresponds to an age-dependent DHT level. Therefore, although 5α-reductase and DHT decrease with age in the epithelium, they remain relatively constant in the stroma of the prostate gland.
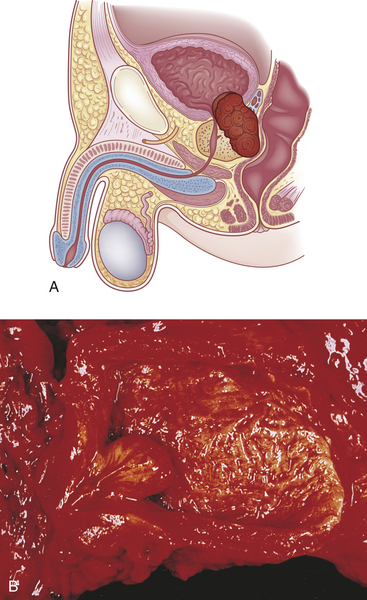
Figure 23-35 Benign prostatic hyperplasia (BPH). A, Condition becomes a problem as prostatic tissue compresses the urethra. B, Gross appearance of BPH showing transition zone resulting from bulging nodules of varying size. (B from Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 1996, Mosby.)
PATHOGENESIS Current causative theories of BPH focus on levels and ratios of endocrine factors such as androgens, estrogens, gonadotropins, and prolactin and changes in the balance between autocrine/paracrine growth-stimulatory and growth-inhibitory factors. These factors include insulin-like growth factors (IGFs), epidermal growth factor, nerve growth factor, fibroblast factors, IGF binding proteins, and transforming growth factor-beta (TGF-β).152
Aging and circulating androgens are associated with BPH and enlargement. These factors are predisposed as disrupting the balance of growth factor signaling pathways and stromal/epithelial interactions creating a growth-promoting and tissue remodeling microenvironment.153 All together these interactions lead to an increase in prostate volume. The remodeled stroma promotes local inflammation with altered cytokine, reactive oxygen/nitrogen species, and chemoattractants.153 The resultant increased oxygen demands of proliferating cells causes a local hypoxia that induces angiogenesis and changes to fibroblasts. Functional and phenotypic changes (transdifferentiation) of fibroblasts to the myofibroblasts is a hallmark of the remodeled microenviroment.153
BPH begins in the periurethral glands, which are the inner glands or layers of the prostate. The prostate enlarges as nodules form and grow (nodular hyperplasia) and glandular cells enlarge (hypertrophy). The development of BPH occurs over a prolonged period, and changes within the urinary tract are slow and insidious.
CLINICAL MANIFESTATIONS Clinical manifestations are a result of complex interactions involving prostatic urethral resistance to the mechanical and spastic effects of BPH, intravesical pressure during voiding, detrusor muscle strength, neurologic functioning, and general physical health.
During the early stages of urethral obstruction, the detrusor muscle hypertrophies to help the bladder force urine out against increasing resistance. Symptoms are considered obstructive (weak urinary stream, prolonged voiding, abdominal straining, hesitancy, intermittency, incomplete bladder emptying, postmicturitional dribble) or irritative (frequency and repeated urination, nocturia, urgency, incontinence, and bladder pain and dysuria)154 and may wax and wane.155 As obstruction progresses, often over a period of several years, the detrusor muscle decompensates and the bladder is unable to empty all of the urine. Increasing volumes of urine are retained until urine retention is chronic. The volume of urine retained may be great enough to produce uncontrolled “overflow incontinence” with any increase in intra-abdominal pressure. At this stage the force of the urinary stream is reduced significantly and much more time is required to initiate and complete voiding.
Progressive bladder distention causes sacculations or diverticular outpouchings of the bladder wall, and some neural degeneration of smooth muscle cells occurs. The ureters may be obstructed where they pass through the hypertrophied detrusor muscle. Hematuria, bladder or kidney infection, bladder calculi, acute urinary retention hydroureter, hydronephrosis, and renal insufficiency are common complications.154 Some men initially have signs of uremia and renal failure. On digital rectal examination (DRE) the hyperplastic prostate is a soft or firm enlargement with smooth mucosal surface and no discernible distinction between lobes; asymmetry is common. The palpated prostate does not always reflect the degree of BPH because a substantial portion of the enlargement is intravesicular.156 Thirty percent of men with mild to moderate symptoms improve with watchful waiting.
There is no way to reverse progressive BPH, but the hyperplasia is not always progressive. For these reasons, timing of intervention is variable and depends on severity of symptoms and the presence of complications. Annual DREs are used to screen men older than 40 years for BPH. If marked enlargement, moderate to severe symptoms, or complications are present, transrectal ultrasound (TRUS) is used to determine bladder and prostate volume and residual urine. Urinalysis, serum creatinine and blood urea nitrogen, uroflowmetry, postvoid residual (PVR) urine, pressure-flow study, cystometry, and cystourethroscopy are used to determine kidney and bladder function.154 Physical examination with DRE and prostate-specific antigen (PSA) is conducted to determine hyperplasia.157 PSA density (PSAD) is helpful in differentiating BPH from prostatic cancer. PSAD is calculated by dividing PSA serum levels by the volume of prostate tissue, which is determined by TRUS. When necessary, the hyperplastic tissue may be removed surgically to prevent the serious consequences of urethral obstruction. Glands less than 60 g are treated by transurethral resection, laser therapy, or microwave thermotherapy,158 whereas larger glands are removed surgically (prostatectomy). A permanent indwelling catheter is inserted if the individual cannot tolerate surgery. BPH has been treated successfully with drugs. α1-Adrenergic blockers (prazosin and tamsulosin) are used to relax the smooth muscle of the bladder and prostate. Antiandrogen agents, such as finasteride (Proscar), selectively block androgens at the prostate cellular level and cause the prostate gland to shrink.159 These drugs offer an alternative to surgery for as many as 75% of men with mild prostate enlargement.159 Neither α1-adrenergic blockers nor finasteride seems to affect sexual desire or potency; finasteride may cause bone loss and lower levels of PSA. PSA is used as a screen for prostate cancer.
Prostatitis
Prostatitis is an inflammation of the prostate. Some degree of prostatic inflammation is present in 4% to 36% of the male population. This percentage increases to 50% in older men. Inflammation is usually limited to a few of the gland’s excretory ducts (Figure 23-36).
Prostatitis is characterized as (1) acute bacterial prostatitis, (2) chronic bacterial prostatitis, or (3) nonbacterial prostatitis. Prostatodynia (pain in the prostate) is sometimes considered a form of nonbacterial prostatitis. Men with prostatodynia have the same clinical manifestations as those with nonbacterial prostatitis, but physical and laboratory examinations do not show prostatic pathology. Prostatodynia may not be caused by a pathologic condition of the prostate but rather by spasms in the genitourinary tract or tension in the muscles of the pelvic floor.
A number of defense mechanisms normally protect the lower urogenital tract from infection. Mechanical defenses include urethral length, micturition (urination), and ejaculation. Structural malformations and instrumentation of the genitourinary tract may weaken these defense mechanisms. Chemical defenses include antimicrobial substances in the prostatic fluid. The most important of these is a zinc-containing polypeptide known as prostatic antibacterial factor. Coliform bacteria, particularly Enterobacter, E. coli, Enterococcus, Klebsiella, and Pseudomonas, are common pathogens of bacterial prostatitis. Ureaplasma and C. trachomatis also may be causative agents of infectious prostatitis.150
Bacterial Prostatitis: Acute bacterial prostatitis is an ascending infection of the urinary tract that tends to occur in men between ages 30 and 50 years but is also associated with BPH in older men. Infection stimulates an inflammatory response in which the prostate becomes enlarged, tender, and firm or boggy. The onset of prostatitis may be acute and unrelated to previous illnesses, or it may follow catheterization or cystoscopy.
Clinical manifestations of acute bacterial prostatitis are those of acute cystitis or pyelonephritis. Sudden onset of malaise, low back and perineal pain, high fever (up to 40° C [104° F]), and chills is common, as are dysuria, inability to empty the bladder, nocturia, and urinary retention. Myalgia and arthralgia also may occur. The individual also may have symptoms of lower urinary tract obstruction, such as a slow, small, narrowed urinary stream, which may be a medical emergency. Men are acutely ill and may look toxic. Prostatic pain may occur, especially when the individual is in an upright position, because the pelvic floor muscles tighten with standing and compression of the prostate gland occurs. Some individuals experience low back pain, painful ejaculation, and rectal or perineal pain. Palpation discloses an extremely tender, swollen prostate with normal to “boggy” consistency that may be warm to the touch.
Because acute bacterial prostatitis usually is associated with a bladder infection caused by the same microorganism, urine cultures disclose its identity. Prostatic massage may express enough secretions from the urethra for direct bacterial examination, but massage may be painful and increases the risk that the infection will ascend to adjacent structures or enter the bloodstream and cause septicemia. For these reasons, prostatic massage generally is contraindicated; transurethral instrumentation also is contraindicated.
Long-term, broad-spectrum antibiotic therapy with fluoroquinolone agents or trimethoprim-sulfamethoxazole for at least 30 to 42 days is recommended to resolve the infection and control its spread. In severe cases the individual is hospitalized and treated with combination intravenous antibiotics, usually an aminoglycoside (gentamicin sulfate, kanamycin sulfate, or tobramycin) and ampicillin for 1 week followed by 4 to 6 weeks of oral antibiotics. Pain relievers, antipyretics, bed rest, and adequate hydration also are therapeutic. Complications include urinary retention that resolves with antibiotic therapy; prostatic abscess that may rupture into the urethra, rectum, or perineum; epididymitis; bacteremia; and septic shock. Urinary retention requiring drainage is best managed with a suprapubic catheter; Foley catheterization is contraindicated during acute infection.
Chronic bacterial prostatitis is characterized by recurrent urinary symptoms and persistence of pathogenic bacteria (usually gram negative) in urine or prostatic fluid.150 This form of prostatitis is the most common recurrent urinary tract infection in men. Symptoms are variable and may be similar to those of an acute bladder infection: frequency, urgency, dysuria, perineal discomfort, low back pain, and sexual dysfunction. The prostate may be only slightly enlarged or boggy, but fibrosis caused by repeated infections can cause it to be firm and irregular in shape.
When the initial urine sample is bacteria free, prostatic massage is used to express secretions. Subsequently, the first 10 ml of voided urine is collected and examined microscopically. Prostatic secretions showing more than 10 white blood cells per high-power field and macrophages containing fat indicate bacterial infection; diagnosis is confirmed by culture. Prostatic calculi may be seen on pelvic x-ray or TRUS.
Treatment of chronic bacterial prostatitis is difficult because it is often caused by prostatic calculi. Calculi are silent and are found in up to 50% of men with prostatitis, and infected calculi can serve as a source of bacterial persistence and relapsing urinary tract infections.150 Calculi harbor pathogens within the stone, and consequently pathogens cannot be eradicated from the urinary tract. Permanent cure is achieved by surgical removal of the stones through transurethral prostatectomy, which may not be a viable option for young men. More common symptoms are tempered with chronic suppressive therapy. Quinolones, because of their bioavailability and penetration into prostatic tissue, are the treatment of choice; drug therapy lasts for a minimum of 3 to 4 weeks. If symptoms do not subside, other infectious microorganisms are considered and treated accordingly.150 Comfort measures include nonsteroidal anti-inflammatory drug therapy and liberal use of sitz baths.
Nonbacterial Prostatitis: Nonbacterial prostatitis is the most common prostatitis syndrome and consists of prostatic inflammation without evidence of bacterial infection. Symptoms tend to be milder but are persistent and annoying. Presumably, noninfectious prostatitis or prostatodynia is caused by reflux of sterile urine into the ejaculatory ducts as a result of high-pressure voiding.150 Reflux may be triggered by spasms of the external or internal sphincters. Some men may actually have interstitial cystitis and should be treated accordingly.
Men with nonbacterial prostatitis may complain of pain or a dull ache that is continuous or spasmodic in the suprapubic, intrapubic, scrotal, penile, or inguinal area. Other symptoms are pain on ejaculation and urinary symptoms, such as frequency of urination. The prostate gland generally feels normal on palpation.
Digital examination of the prostate, bacterial cultures of the urogenital tract, microscopic examination of expressed prostatic fluid, urethroscopy, and urodynamic studies are used to verify the diagnosis of nonbacterial prostatitis. Nonbacterial prostatitis is a diagnosis by exclusion.
Therapy is individualized and aimed at decreasing symptoms. α1-Adrenergic blockers (e.g., terazosin, doxazosin, and tamsulosin) may be helpful in decreasing spasms of the prostate muscle. Other treatments include skeletal muscle relaxants, pelvic floor relaxation using biofeedback, and prostatic thermotherapy.150 Additional treatments may include hot sitz baths, bed rest, anticholinergics, and anti-inflammatory drugs.
Cancer of the Prostate
Prostate cancer is among the most common male cancers but the incidence varies greatly worldwide (Figure 23-37). It is the most common cancer in American males but the third most common cancer worldwide. In the United States it accounts for more than 14% of all cancer deaths; only lung cancer accounts for more deaths. Among countries with reliable cancer statistics, prostate cancer rates are highest in westernized countries, such as the United States and Western Europe and lowest in Asian countries. It also is rare in Africa, Central America, and South America. Screening with PSA can amplify the incidence of prostate cancer by allowing detection of prostate lesions that although meeting the pathologic criteria for malignancy, many believe to have low potential for growth and metastasis; however, this is controversial. Thus screening can amplify the incidence of prostate cancer by including the detection of these localized lesions. Therefore, the incidence rates in some countries, such as the United States, reflect clinical as well as latent (preclinical) disease compared with other countries that report only clinical disease. Comparing data in the pre-PSA era does reflect less extreme incidence rates, but the United States still has the highest rates. Data from the Surveillance, Epidemiology, and End Results (SEER) program show that incidence rates in the United States for white men increased 80% from 1983 to 1987 and 1988 to 1992 (possibly because of increased screening in asymptomatic men).160
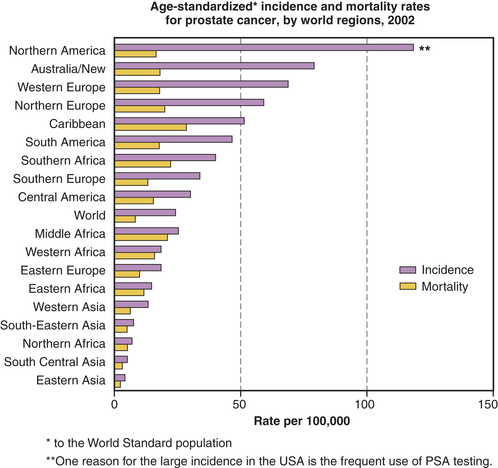
Figure 23-37 Age-standardized∗ incidence and mortality rates for prostate cancer by world regions, 2002. (Data from Cancer Research, UK Cancer Incidence Statistics updated November 2008, News & Resources.)
A small decline in the death rate has been noted during the past few years in the United States and other developing countries. The overall mortality rates are mostly in men older than 65; within younger groups, mortality has been stable across decades. Incidence increases with advancing age; more than 75% of all prostate cancer is diagnosed in men older than 65.1 By age 85, about one in six American men will develop prostate cancer in their lifetime and about 3% will die from it. With aging, most of the androgen-metabolizing enzymes undergo significant alteration. The incidence is low in black African men worldwide; however, black African-American men have the highest rate of prostate cancer in the world and in the United States.
Dietary Factors: The worldwide distribution of prostate cancer suggests that diet may play a role in the development of prostate cancer, especially if the diet affects hormone levels. Consistency across studies indicates that a high intake of fat (total and especially saturated fat) is a risk factor for prostate cancer, but the strength of the associations is modest and may be greater for blacks than for European-Americans.151,154–161 Several hypotheses concern the enhancing effect of fat on prostate carcinogenesis, including hormonal mediation and the generation of free radicals. Fat intake from dairy products increases calcium, itself a proposed risk factor. Calcium can suppress circulating levels of dihydroxyvitamin D, a possible protective factor for prostate cancer.162 In addition, a low intake of dietary fiber and complex carbohydrates and a high intake of protein are associated with an increased risk of prostate cancer.161 Some data suggest a slight increase in risk of advanced prostate cancer or death among individuals with a high body mass index.163,164 High-energy intake (consumption of excess calories) indicates that this may indeed increase insulin levels and IGF-1, a powerful carcinogenic agent165 (see Pathogenesis p. 865).
Individual nutrients or foods and their associations with prostate cancer risk are not strong, yet migration of individuals from low-risk geographic areas of the world, such as Japan, to high-risk countries, such as the United States, increases risk considerably.166 These changes in risk probably reflect differences in lifestyle and dietary habits. Geographically,
individuals who reside in regions with less sunlight have a higher risk of prostate cancer. The highest rates of mortality from prostate cancer in the world are in Scandinavian countries, where exposure to UV light is low; the possible link is less vitamin D induced by less sun exposure. The Cure of Cancer of the Prostate (CaP CURE) Report167 states that of all the risk factors for prostate cancer, only nutrition seems to explain the differences in its global distribution.
Animal studies suggest a protective effect of retinoids (vitamin A) and prostate carcinogenesis; however, consistency is lacking among epidemiologic studies. Vegetarian men have a lower incidence of prostate cancer than omnivorous males.168 Observational studies suggest that supplementation with vitamins E, C, or selenium is associated with a lower risk for developing prostate cancer. Two recent clinical trials, however, showed no benefit in lowering prostate cancer.169,170 Much debate has ensued including whether PSA screening could have lowered the baseline level of more advanced disease and whether synthetic vitamins are possibly not the same as vitamins found in a healthy diet. Mortality from prostate cancer varies according to sun exposure; vitamin D has been proposed as the important link. Vitamin D (1,25-[OH]2D3) inhibited the growth of certain human prostate cancer cell lines by an androgen-dependent mechanism.171 Higher selenium levels of vitamin D were significantly related to a better prognosis in individuals with prostate cancer.172 Lycopene, a carotenoid found in large amounts in tomatoes that gives them their color, has been associated with a lower risk of prostate cancer.173,174
Hormones: Prostate cancer develops in an androgen-dependent epithelium and is usually androgen sensitive. In addition, a few case reports exist of prostate cancer in men who used androgenic steroids as anabolic agents or for medical purposes, suggestive of a causal relationship.166,175–177 Population studies have not, however, provided clear and convincing patterns about associations between circulating hormone concentrations and prostate cancer risk.166 Only a few associations with prostate cancer risk have been observed consistently (in at least three studies), and their associations are weak: (1) slightly higher circulating testosterone and estrogen levels and lower DHEA (sulfate) levels in high-risk black men as compared with lower-risk European-American men; and (2) a cytosine-adenine-guanine (CAG) repeat-length polymorphism in the androgen-receptor gene associated with increased risk and increased receptor activity (androgen receptor). Evidence for involvement of activity of the enzyme 5α-reductase, which is critical in androgen activity in the prostate, is contradictory and inconsistent.166 In men younger than 50 years, circulating levels of androgens and estrogens appear to be higher in men of African descent than in European-American men.
Androgens promote prostatic epithelial growth during fetal and prepubertal periods. In adults androgens act through reciprocal homeostatic stromal (microenvironment; see Chapter 11) epithelial interactions to maintain normal differentiation and halt growth178 (see Pathogenesis).
Investigations directed at understanding the hormonal basis of prostate (as well as breast) carcinogenesis have numerous problems. The complexities of interacting hormones and separating out the effects of a single hormone are profound. In addition, only single blood samples are generally available, tissue hormone samples important for paracrine signaling are not consistently measured, and within-subject variations over time and differences in circadian rhythms cannot be adequately measured. The results of several animal studies do support elevation of bioavailable and bioactive androgens in the circulation and in target tissue as an important risk factor. Animal studies also indicate that increased biologic activity of the androgen receptor may be associated with prostate cancer. See the Pathogenesis section for a more thorough discussion of the role of hormones in the pathogenesis of prostate cancer.
Vasectomy: Vasectomy has been identified as a possible risk factor for prostate cancer in case-controlled and cohort studies.170,179,180 Three mechanisms by which vasectomy could increase risk are (1) elevation of circulating androgens; (2) immunologic mechanisms involving antisperm antibodies; and (3) reduction of seminal fluid levels of 5α-dihydrotestosterone, the active metabolite of testosterone in the prostate, in vasectomized men. Other investigators reported a decrease in SHBG and an increase in the ratio of testosterone to SHBG.181 These results suggest an elevation of circulating free testosterone following vasectomy.166 However, with these combined mechanisms it is unlikely that vasectomy plays a causal role.162
Genetic and Epigenetic Factors: Other possible causes are genetic predisposition (familial and hereditary forms). Genetic studies suggest that strong familial predisposition may be responsible for 5% to 10% of prostate cancers.1 Compared with men with no family history, those with one first-degree relative with prostate cancer have twice the risk and those with two first-degree relatives have five times the risk.182 Men with BRCA2 (suppressor tumor) germline mutations have a 20-fold increase in risk. A common type of somatic mutation that gives rise to chromosomal rearrangements is the ETS gene. The most common epigenetic alteration in prostate cancer is hypermethylation of the glutathione S-transferase (GST P1) gene. This gene is located on chromosome 11 and is part of the pathway that helps protect against carcinogen damage.183 A number of other epigenetic modifications found on tumor suppressor genes include PTEN, RB, p16/INK4a, MLH1, MSH21, and APC.182 The hereditary form constitutes about 9% of all prostate cancers and approximately 43% of cancers in men less than 55 years of age.156 There is no clear evidence of a causal link between BPH and prostate cancer even though they may often occur together. Variations in several other genes related to inflammatory pathways might affect the probability of developing prostate cancer.184
PATHOGENESIS More than 95% of prostatic neoplasms are adenocarcinomas,185 and most occur in the periphery of the prostate. Most hyperplasias, however, arise in the transitional zone (Figure 23-38). Several histologic grading systems have been developed on the basis of the glandular pattern, the degree of differentiation (anaplasia) of the cancer cells, or both. The biologic aggressiveness of the neoplasm appears to be related to the degree of differentiation rather than the size of the tumor (see Box 23-13 on p. 869).
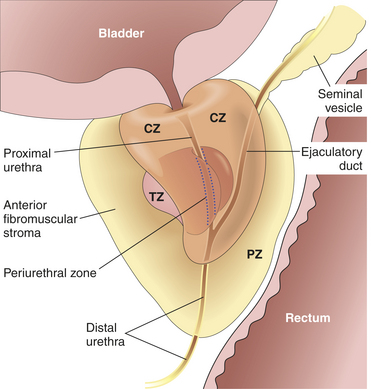
Figure 23-38 Adult prostate. The normal prostate contains several distinct regions, including a central zone (CZ), a peripheral zone (PZ), a transitional zone (TZ), and a periurethral zone. Most carcinomas arise from the peripheral glands of the organ and may be palpable during digital examination of the rectum. Nodular hyperplasia, in contrast, arises from more centrally situated glands and is more likely to produce urinary obstruction early than is carcinoma. (From Epstein JI: The lower urinary tract and male genital system. In Kumar V, Abbas AK, Fausto N, editors: Robbins and Cotran pathologic basis of disease, ed 8, Philadelphia, 2009, Saunders.)
Hormonal: Just as the testicles are the male equivalent of the female ovaries, the prostate is the male equivalent of the female uterus; in both situations they originate from the same embryonic cells. This may be important in understanding the role of the associated hormones testosterone, dihydrotestosterone, and estradiol in prostate carcinogenesis. Testosterone and DHT are the most important androgens in the adult male. Testosterone is the major circulating androgen, whereas DHT predominates in prostate tissue and binds to the androgen receptor (AR) with greater affinity than does testosterone.186
Testosterone is the major androgen from the interstitial cells of the testis (Leydig cells). Its production in men is almost 5 mg/day. The adrenal cortex contributes the far less potent androstenedione as its major androgen, at about 3 mg/day. In the target tissues and, to a lesser extent, in the testes themselves, testosterone is converted to DHT by the enzyme type 2 5α-reductase (Figure 23-39). Type 2 5α-reductase is located mostly in stromal cells. Thus DHT is the most potent intraprostatic androgen. About half of circulating testosterone is bound to SHBG, about half binds to albumin, and about 1% to 2% exists in a free state. Free testosterone, including testosterone disassociated from albumin and possibly SHBG, enters the prostate cell, where it is converted to DHT.186 DHT is a paracrine hormone because it affects the local environment or stroma. Several intraprostatic enzymes encoded by genes, HSD3A and HDS3B, are activated by DHT and are important components of intraprostatic androgen regulation. The conjugated byproduct, 3α-androstenediol glucuronide (AAG), a terminal metabolite of DHT, can be measured in the circulation and used as an indicator of DHT levels. The drug finasteride, an inhibitor of intraprostatic 5α-reductase type II enzyme, decreases AAG levels. Thus AAG is a marker of intraprostatic 5α-reductase activity and androgen levels.
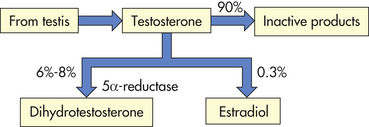
Normally a small amount of estrogen is produced per day—65 mcg of estrone and 45 mcg of estradiol—by the aromatization of androstenedione and testosterone, respectively. This reaction is catalyzed by the enzyme system aromatase. A very small quantity of estradiol is released by the testes (see Figure 23-39); the rest of the estrogens in males are produced by adipose tissue, liver, skin, brain, and other nonendocrine tissue. Thus testosterone is a precursor of the two hormones, DHT and estradiol.
Most of the androgen-metabolizing enzymes undergo a significant age-dependent alteration. In epithelium, both the 5α-reductase activity and the DHT level decrease with age; whereas in stroma not only is 5α-reductase activity rather constant over the whole age range but also the DHT level is constant. In contrast to the relatively unaltered DHT level, the estrogen content follows an age-dependent increase. Thus the age-dependent decrease of the DHT accumulation in epithelium and the concomitant increase of the estrogen accumulation in stroma lead to a tremendous increase with age of the estrogen/androgen ratio in the human prostate. In animal studies, chronic exposure to testosterone plus estradiol is strongly carcinogenic, whereas testosterone alone is weakly carcinogenic.166 The mechanism is not clearly understood but appears to involve estrogen-generated oxidative stress and DNA toxicity, and it requires androgen and estrogen receptor–mediated processes, such as changes in sex steroid metabolism and receptor status.166 In addition, there are changes in the balance between autocrine/paracrine growth-stimulatory and growth-inhibitory factors, such as IGFs, epidermal growth factor (EGF), nerve growth factor (NGF), IGF-binding proteins, and TGF-β.
Stromal Environment: A precursor lesion, prostatic intraepithelial neoplasia (PIN) has been described. PIN may be more concentrated in prostates containing cancer and are noted in proximity to cancer.182 The final fate of PIN is, however, unknown including the possibilities of latency invasion and even regression (Figure 23-40). The microenvironment (stroma) surrounding the prostatic tumor actively fuels the progression of prostate cancer from localized growth, to invasion, to development of distant metastases.187 Several types of stromal cells in the surrounding microenvironment are recruited to tumors, enhancing cancer growth and metastases.187 Important are the microenvironment balances of proliferation and apoptosis to suppress malignancy, but perturbations in the stroma, for example by chronic inflammation, override the protective mechanisms and shift the tissue microenvironment to a growth-promoting malignant state.187
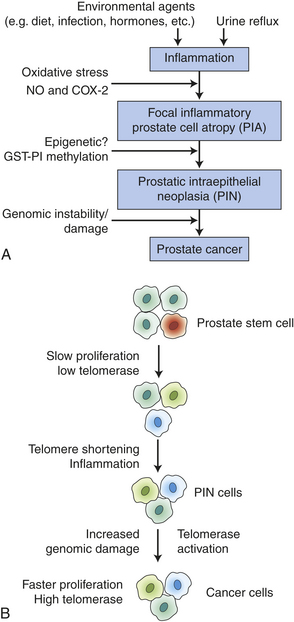
Figure 23-40 Hypothetical models of prostate carcinogenesis: inflammation and telomerase. A, Inflammation may happen early from repeated injuries or infection, or both, or from refluxed urine into the prostate. Manifestations of inflammation include oxidative stress damage with the generation of ROS. Thus, the microenvironment is inflammatory and products like nitric oxide (NO) and cyclooxygenase (COX-2) can cause genetic and epigenetic alterations. Inflammatory infiltrates can produce “focal” atrophy. In this model, proliferative inflammatory atrophy (PIA) may be considered the precursor lesion to prostatic intraepithelial neoplasia (PIN). If the oxidant damage is not detoxified by the glutathione enzyme (GST P1) the cells continue to produce PIN. Interesting is that estrogen, through ER-B, influences the protective mechanism of glutathione transferase and can cause epigenetic alterations that increase inflammation. Elevation of estrogens in the presence of testosterone results in prostate-specific inflammation. With the loss of GST P1 continued inflammation causes the transition of PIN to increased prostate cancer. B, Telomerase is an enzyme in the normal stem cell population thought to regulate telomere length and homeostasis during cell renewal (see Chapter 11). Although unknown, prostate stem cells are thought to have low levels of telomerase activity. Studies reveal that telomere length of high grade PIN were shorter than normal cells and that a subset of PIN cells activate telomerase causing cells to become immortal and progress to prostate cancer. (Data from Marian CO, Shay JW: Biochimica Biophysics Acta 2009 Mar 2 [Epub ahead of print]; Sciarra A et al: Eur Urol 52[4]:964-972, 2007.)
Androgens drive prostatic epithelial growth during fetal and prepubertal periods and in adulthood androgens participate through reciprocal homeostatic stromal-epithelial interactions to maintain differentiation but arrest growth.178 Intercellular communication between prostate tumor cells and organ-specific stroma involve diffusible molecules from stromal cell types (e.g., endothelial cells, pericytes, fibroblasts) and bone marrow-derived cells (BMDCs, macrophages, neutrophils, mast cells). All together these released mediators result in malignant progression (also see Chapter 11, p. 377). In addition, the periepithelial stroma undergoes progressive loss in smooth muscle with the appearance of carcinoma-associated fibroblasts (CAFs). Thus the stromal microenvironment is a necessary determinant of benign versus malignant growth.178,187
From all of these observations, the following multifactorial general hypothesis of prostate carcinogenesis emerges: (1) androgens act as tumor promoters through androgen receptor–mediated mechanisms to (2) enhance the carcinogenic activity of strong endogenous DNA toxic carcinogens, including reactive estrogen metabolites and estrogen—and prostatic-generated reactive oxygen species—(3) alterations in autocrine/paracrine growth-stimulating and growth-inhibiting factors between the prostate tumor cells and microenvironment, and (4) possibly unknown environmental-lifestyle carcinogens. All of these factors are modulated by diet and genetic determinants, such as hereditary susceptibility genes and polymorphic genes (especially steroid 5α-reductase type II [SRD5A2]), that encode receptors and enzymes involved in the metabolism and action of steroid hormones.166,186
The most common sites of distant metastasis are the lymph nodes, bones, lungs, liver, and adrenals. The pelvis, lumbar spine, femur, thoracic spine, and ribs are the most common sites of bone metastasis. Local extension is usually posterior, although late in the disease the tumor may invade the rectum or encroach on the prostatic urethra and cause bladder outlet obstruction (Figure 23-41; see Clinical Manifestations). The spread through blood vessels is illustrated in Figure 23-42.
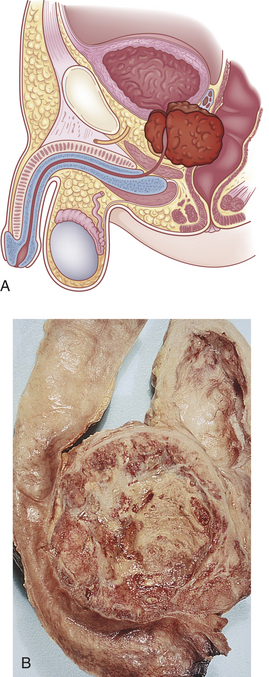
Figure 23-41 Carcinoma of prostate. A, Schematic of prostate tumor. B, Carcinoma of the prostate extending into the rectum and urinary bladder. (B from Damjanov I, Linder J, editors: Pathology: a color atlas, St Louis, 2000, Mosby.)
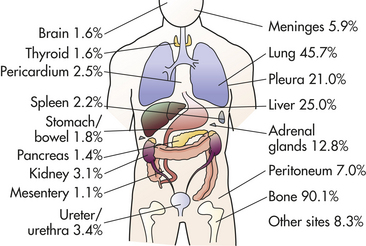
Figure 23-42 Distribution of hematogenous metastases in prostate cancer. Common sites of distant metastasis are the lymph nodes (not shown), bones, lungs, liver, and adrenals. Study of 556 patients with metastatic prostate cancer. (Adapted from Budendorf L et al: Hum Pathol 31:578, 2000.)
CLINICAL MANIFESTATIONS Prostatic cancer often causes no symptoms until it is far advanced. The first manifestations of disease are those of bladder outlet obstruction: slow urinary stream, hesitancy, incomplete emptying, frequency, nocturia, and dysuria. Unlike the symptoms of obstruction caused by BPH, the symptoms of obstruction caused by prostatic cancer are progressive and do not remit. Local extension of prostatic cancer can obstruct the upper urinary tract ureters as well. If rectal obstruction occurs, a man may experience a large bowel obstruction or difficulty in defecation. Symptoms of late disease include bone pain at sites of bone metastasis, edema of the lower extremities, enlargement of lymph nodes, liver enlargement, pathologic bone fractures, and mental confusion associated with brain metastases.
EVALUATION AND TREATMENT The most significant test used in the diagnosis and management of prostate cancer is prostate-specific antigen (PSA). DRE may detect early prostatic carcinomas but is has low sensitivity and specificity.182 A transrectal biopsy is required to confirm the diagnosis. The cut-off point between normal and abnormal PSA is a serum level of 4 ng/mL. Yet this simplified approach to serum PSA tests has led to the delay in diagnosis of prostate cancer and has caused considerable controversy (see What’s New? Continuing PSA Screening Controversy). In addition, because PSA is organ specific and not cancer specific, it can increase and overlap with BPH, prostatitis, infarct, manipulation from instrumentation, and ejaculation.182 Several progressions of PSA values have been proposed. These include (1) PSA density or the ratio between the serum PSA value and volume of prostate gland, (2) PSA velocity or the rate of change in PSA value with time, (3) age-specific PSA reference ranges, and (4) total PSA or the ratio of free and bound PSA in the serum. Serial measures of PSA have great utility in determining the response to treatment.
Screening earlier than 50 years of age with the PSA test is recommended for men at high risk for prostate cancer, such as blacks or relatives of men who have had prostate
cancer.156,188 It is important to note that PSA levels tend to be higher in blacks at baseline and all stages of cancer.189 When TRUS is added to the annual DRE and PSA testing, the ability to predict cancer rises significantly, from 41% to greater than 78%. Lymph node biopsy, bone scans, MRI, and CT may be used to determine metastasis to lymph, bone, or other adjacent tissue.
The 5-year survival rate of men with localized cancer is 100% with or without treatment. However, before screening most men with prostate cancer had advanced disease and died within a few years of diagnosis. Therefore, it is unclear which men will benefit from early screening and which will not. The most important observation for pathologists to make to facilitate cure of any individual of prostate cancer is that of accurately measuring the size of the index (longest) tumor and Gleason score (degree of differentiation) (Box 23-13).190 Molecular diagnostic tests include glutathione-5-transferase P1 (GST P1) gene promoter hypermethylation, TPRSS2:EFG fusion transcripts, and prostate cancer-specific gene 3, formerly called DDS. The annual rate by which PSA rises (i.e., PSA velocity) is one way to improve the prognostic accuracy of PSA screening.191
Treatment of prostatic cancer depends on the stage of the neoplasm (see Box 23-13); the anticipated effects of treatment; and the age, general health, and life expectancy of the individual. The TNM method of staging has been used to determine extent of disease (see Chapter 11, p. 386. Options include no treatment; surgical treatments such as total prostatectomy, transurethral resection of the prostate (TURP), or cryotherapy; nonsurgical treatments such as radiation therapy, hormone therapy, or chemotherapy; watchful waiting; and any combination of these. In addition, new approaches are using immunotherapy.192 Palliative treatment is aimed at relieving urinary, bladder outlet, or colon obstruction; spinal cord compression; and pain. Treatments at an early stage can cure the disease in most, if not all, men, and treatment for advanced stage cancer can extend life and reduce tumor size, thus preventing or relieving pain. Prognosis and survival rates have improved steadily over the past 50 years. Currently, 85% of all prostate cancers are discovered in the local and regional stages; in these stages the 5-year survival rate is 100%; survival rates decline at 10 years (84%) and 15 years (56%).1
Treatment for prostate cancer may lead to loss of urinary control, which may return to normal after several weeks or months. Stress incontinence can occur after surgery and mild urge incontinence can occur after radiation therapy. Prostate cancer and its treatment can affect sexual functioning. Sensation of orgasm is not usually affected, but smaller amounts of ejaculate will be produced or men may experience a “dry” ejaculate because of retrograde ejaculation.
Sexual Dysfunction
In men the normal sexual response involves three processes: erection, emission, and ejaculation. Sexual dysfunction is the impairment of any or all of these processes. Impairment can be caused by a number of physiologic and psychologic factors.
Until the late 1970s, most cases of male sexual dysfunction were thought to be psychogenic. Studies of this problem indicate that in men older than 40 years, organic factors are involved in more than 50% of cases. The causes of organic sexual dysfunction include (1) vascular, endocrine, and neurologic disorders; (2) chronic disease, including renal failure and diabetes mellitus; (3) penile diseases and penile trauma; and (4) iatrogenic factors, such as surgery and pharmacologic therapies. Most of these disorders cause erectile dysfunction.
PATHOPHYSIOLOGY Vascular disorders can prevent erection. Some arterial diseases diminish or interrupt circulation to the penis. This prevents engorgement of erectile tissues in the corpora cavernosa and corpus spongiosum. Rarely, excessive venous drainage of the corpora cavernosa prevents erection.
Endocrine disorders that reduce testosterone production affect sexual function and libido. The reduction may be caused by inadequate secretion of the gonadotropins caused by pituitary dysfunction or hyperprolactinemia. Feminizing tumors and estrogen therapy reduce relative levels of testosterone. Testicular atrophy from any cause also decreases testosterone levels and contributes to sexual dysfunction.
Neurologic disorders can interfere with the important sympathetic, parasympathetic, and CNS mechanisms required for erection, emission, and ejaculation. They include spinal cord injury or tumor, multiple sclerosis, and disorders that cause peripheral neuropathies, such as diabetes mellitus and chronic renal failure. Spinal cord injuries or tumors can alter one or more components of the sexual response, depending on the location of the lesion. For example, in most men with upper motor neuron lesions, reflexogenic erection is possible but emission and ejaculation (i.e., orgasm) are not possible. Lesions affecting the lower motor neurons usually prevent erection. In approximately 40% of such cases, emission and ejaculation are prevented.
Many chronic diseases are associated with sexual dysfunction. In some conditions the sexual dysfunction has a specific physiologic cause. Diabetes mellitus, for example, causes peripheral vascular and neurologic pathology that can lead to erectile dysfunction. Impotence occurs in about 50% of men undergoing dialysis due to decreased testosterone levels, autonomic neuropathy, accelerated vascular disease, multiple medications, worsening of primary disease, and psychologic stress. Potency may be restored by successful renal transplantation, except in bilateral transplantation if arterial flow is diminished or interrupted. Cirrhosis of the liver, scleroderma, chronic debilitation, and cachexia also are known to cause impotence. Emotional and psychologic response to chronic illness, such as anxiety, depression, and loss of self-esteem, can affect sexual functioning. In other chronic conditions, sexual dysfunction is associated with low energy levels and loss of libido. The pathophysiologic mechanisms responsible for such changes are not known.
Priapism causes fibrosis of trabeculae (erectile tissues) within the corpora cavernosa, making erection difficult. The penile curvature caused by Peyronie disease does not make erection impossible but may make it extremely painful and intercourse impossible. Penile trauma can damage the erectile tissue, disrupt the posterior urethra, and disrupt the pudendal arteries or nerves.
Iatrogenic factors, including drugs and surgery, have a significant effect on erectile function. The following surgical procedures carry the risk of erectile dysfunction: radical pelvic surgery; radical prostatectomy; transurethral, suprapubic, or simple retropubic prostatectomy; and aortoiliac surgery. Erectile dysfunction is caused by the severing of small nerve branches that are essential for erection. Aortoiliac surgery, retroperitoneal lymphadenectomy, and sympathectomy cause the loss of ejaculation capacity in some individuals.
A few pharmacologic agents enhance the sexual response, but most have the opposite effect. Men who are taking antihypertensives, antidepressants, antihistamines, antispasmodics, sedatives or tranquilizers, barbiturates, diuretics, sex hormone preparations, narcotics, or psychoactive drugs may experience some degree of sexual dysfunction. Drug-induced sexual dysfunction consists of decreased desire, decreased erectile ability, or decreased ejaculatory ability. Ethyl alcohol may induce alcoholic neuropathy or increased estrogens because of hepatic dysfunction; marijuana depresses testosterone levels; and cigarette smoking contributes to vasoconstriction and venous leakage. A number of pharmacologic agents also diminish the quality or quantity of sperm. A few may cause priapism. Drugs can assist in maintaining an erection.
EVALUATION AND TREATMENT Evaluation of sexual dysfunction includes a physical examination, with particular attention to the genitalia, prostate, and nervous system, and basic laboratory tests to identify the presence of endocrinopathies or other underlying disorders that can cause the dysfunction. If no physiologic cause is found and the condition does not improve with psychotherapy, the man is referred for further investigation of organic causes. Psychologic evaluation is indicated for younger men with a sudden onset of sexual dysfunction or men of any age who are able to achieve but not maintain an erection.
Sophisticated diagnostic techniques can be used to assess penile blood flow, erectile tissue anatomy, nervous system function, and occurrence of erection or emission during sleep (nocturnal emission). Penile blood flow is measured by Doppler techniques and penile arteriography. Corpus cavernosography, in which contrast material is injected into the corpora cavernosa, provides anatomic information about the erectile tissue of the penis. Neuropathic causes of sexual dysfunction are evaluated by measuring the speed of the bulbocavernous reflex. Nocturnal penile tumescence monitoring measures the frequency of nocturnal erections. Depending on the equipment used, this information may be correlated to rapid eye movement (REM) or non-REM sleep.
Treatments for organic sexual dysfunction include medical and surgical interventions. Nonsurgical interventions include correction of underlying disorders, particularly drug-induced dysfunction and endocrinopathy-related (e.g., reduced testosterone associated with chronic renal failure) dysfunction. Vasodilators and cessation of smoking can benefit individuals with vasculogenic erectile dysfunction. Surgical interventions include penile implants, penile revascularization, and correction of other anatomic defects contributing to sexual dysfunction.
Impairment of Sperm Production and Quality
Spermatogenesis requires adequate secretion of FSH and LH by the pituitary; sufficient secretion of testosterone by the Leydig cells; sufficient function of the Sertoli cells, including secretion of androgen-binding protein, growth factors, inhibin B, and a number of other important (but poorly understood) peptides; and adequate spermatogonia.193,194 The Leydig cells are located in the testicular interstitium between the tubules, and the Sertoli cells and spermatogonia are located within the seminiferous tubules. The Sertoli cells extend from the basement membrane to the lumen, display tight junctions between adjacent cells, and form the blood-testis barrier. Inadequate secretion of gonadotropins may be caused by hypothyroidism, hyperadrenocortisolism, hyperprolactinemia, or hypogonadotropic hypogonadism. In these situations, gonadotropin levels are low because of feedback inhibition or idiopathic hyposecretion. In the absence of adequate gonadotropin levels, the Leydig cells are not stimulated to secrete testosterone and sperm maturation is not promoted in the Sertoli cells. Spermatogenesis depends not only on appropriate stimulation by the gonadotropins but also on an appropriate response by the testes. Defects in testicular response to the gonadotropins result in decreased secretion of testosterone and inhibin B and, as a result of normal feedback mechanisms, high levels of circulating gonadotropins. In the absence of adequate testosterone levels, spermatogenesis is impaired. Newer research demonstrates the significance of inhibin B as an important marker of the competence of Sertoli cells and spermatogenesis. Inhibin B is strongly correlated with severity of spermatogenic effects. A positive correlation exists between serum inhibin B levels and sperm concentration and testicular volume, and lower levels have been associated with azoospermia, testicular disorders, and infertility.194
Impaired spermatogenesis also can be caused by genetic disorders (such as Klinefelter syndrome), myotonic dystrophy, or testicular trauma. Other conditions associated with impaired spermatogenesis include systemic illness, such as renal failure, hepatic disease, or sickle cell disease; exposure to gonadotoxins, such as chemotherapy or radiation; varicocele; and cryptorchidism.
Fertility is adversely affected if spermatogenesis is normal but the sperm are chromosomally or morphologically abnormal or are produced in insufficient quantities. Chromosomal abnormalities are caused by genetic factors and by external variables, such as exposure to radiation or toxic substances. Ongoing research using small ribonucleic acids (RNAs) is elucidating the molecular mechanisms regulating spermatogenesis.195 A sperm count of 20 million sperm per milliliter of semen has been suggested as the minimum concentration required for fertility. Average fertile men have 50 to 100 million sperm per milliliter.144,193
Sperm motility is another important variable affecting fertility. Motility appears to be affected by the sperm’s chemical environment, that is, the characteristics of semen. Prostatic dysfunction, excessive semen viscosity, presence of drugs or toxins in the semen, and presence of antisperm antibodies are associated with impaired sperm motility. Approximately 3% to 7% of infertile males have antisperm antibodies in their semen. Antisperm antibodies may develop as a result of epididymitis or other inflammation of the genitourinary tract, testicular injury or torsion, a previous vasectomy or biopsy, and cryptorchidism. Antisperm antibodies may be (1) cytotoxic antibodies, which attack sperm and reduce their number in the semen; or (2) sperm-immobilizing antibodies, which impair sperm motility and reduce their ability to traverse the endocervical canal. Intrinsic, biologic factors leading to the production of antisperm antibodies seem to play a greater role than extrinsic factors. The exact mechanism remains unclear.193
A male factor contributes to the cause of up to 50% of cases of infertility. As understanding of the male factor in infertility increases, evaluation becomes more complex and essential to appropriate treatment (Box 23-14). Treatment for impaired spermatogenesis involves correction of any underlying disorders and avoidance of radiation or toxins. Androgens, human gonadotropins, and antiestrogens (e.g., clomiphene citrate, tamoxifen citrate) may enhance spermatogenesis. Semen can be modified to improve sperm motility. If conception is desired, the semen is obtained by masturbation (or mechanical device),193 after which it can be diluted, concentrated, or washed to remove antisperm antibodies. These alterations are followed by artificial insemination.
DISORDERS OF THE BREAST
Disorders of the Female Breast
Galactorrhea
Galactorrhea (inappropriate lactation) is the persistent and sometimes excessive secretion of a milky fluid from the breasts of a woman who is not pregnant or nursing an infant. It can occur in men, may involve one or both breasts and is not associated with breast cancer.
Incidence is difficult to estimate because of differences among definitions of the condition, examination techniques, and populations of women who have been studied. Prevalence has been documented as 0.1% to 32% of all women.
PATHOPHYSIOLOGY Galactorrhea is a manifestation of pathophysiologic processes in the body, rather than a breast disorder. These processes are chiefly hormone imbalances caused by hypothalamic-pituitary disturbances, pituitary tumors, or neurologic damage. Exogenous causes include drugs, estrogen, and manipulation of the nipples. When caused by hyperprolactinemia it is manifested by the spontaneous appearance of a milky secretion from multiple duct openings, usually from both breasts. Galactorrhea caused by oral contraceptives (OCs) is more likely to occur with high-dose use; is characterized by clear, serous, or milky discharge from multiple ducts; and is noticeable during the drug-free interval between OC packets. In premenopausal women, unilateral or bilateral spontaneous multiple duct discharge that increases before menstruation often is caused by fibrocystic change. Unilateral, spontaneous, serous, or serosanguineous discharge from a single duct usually is caused by an intraductal papilloma; bloody discharge suggests cancer; bilateral, sticky, multicolored discharge from multiple ducts is often caused by duct ectasia; and purulent discharge indicates a subareolar abscess.196
The most common cause of galactorrhea is nonpuerperal hyperprolactinemia, or excessive amounts of prolactin (the pituitary hormone that stimulates milk production) in the blood not related to pregnancy or childbirth. Nonpuerperal hyperprolactinemia can be caused by any factor that (1) stimulates or overstimulates the prolactin-secreting units of the pituitary gland; (2) interferes with production of prolactin-inhibiting factor (PIF), a neurotransmitter (probably dopamine) that inhibits prolactin secretion; or (3) interferes with pituitary receptors for PIF. A variety of exogenous agents (such as drugs) and disorders can trigger one of these three mechanisms, thereby causing hyperprolactinemia (Box 23-15).
Hypothyroidism causes increased secretion of hypothalamic TRH that stimulates prolactin release from the pituitary. Hypothyroidism also is associated with reduced metabolic clearance of prolactin, which prolongs its effects.
Many types of pituitary tumors cause hyperprolactinemia. Prolactinomas cause hyperprolactinemia by secreting prolactin, decreasing production of PIF, or putting pressure on the pituitary stalk such that delivery of PIF to the anterior pituitary is prevented. Growth hormone–secreting pituitary tumors may cause galactorrhea through the intrinsic lactogenic effect that growth hormone appears to have on mammary tissue. Prolactin-secreting lung and kidney tumors also cause hyperprolactinemia.
Chronic stress may cause hyperprolactinemia by inhibiting PIF release. Cervical spinal injuries, head trauma, encephalitis, meningitis, herpes zoster, or thoracotomy scars may stimulate the afferent portion of the suckling reflex arc, which is carried in the second to sixth thoracic nerves. The suckling reflex increases prolactin secretion.
Persistent and repeated sucking or squeezing of the nipples can induce galactorrhea, and has been documented in women who manipulate their breasts and nipples daily.197 Monthly examination of the breasts for nipple discharge usually is not associated with the development of galactorrhea.
CLINICAL MANIFESTATIONS A small amount of breast milk expressed from the nipple of parous women usually is not a concern, and normal breast milk color can be other than white. Inappropriate lactation is manifested by the appearance of a milky breast secretion in nonpregnant, nonlactating women from one or both breasts. Most women with galactorrhea experience menstrual abnormality. If a pituitary process is involved, the woman usually experiences hirsutism and infertility; if a hypothalamic lesion is present, she may report such CNS symptoms as intractable headache, visual field disturbances, sleep disturbances, and abnormal temperature, thirst, or appetite.198
EVALUATION AND TREATMENT Galactorrhea requires evaluation when it (1) occurs in nulliparous women or in parous women who have not been pregnant or have not breast-fed for 12 months or (2) is associated with amenorrhea, headache, visual field abnormalities, or other symptoms implying systemic illness. Evaluation includes a variety of diagnostic tests. When amenorrhea accompanies galactorrhea, the assessment is the same as for amenorrhea. Breast secretions are examined for fat globules and neoplastic cells to verify their source. Serum prolactin levels are measured. Because such variables as eating, sleeping, stress, and breast examinations increase prolactin levels, at least two positive results are needed for a diagnosis of hyperprolactinemia. Prolactin levels greater than 25 to 30 ng/ml (by radioimmunoassay) are elevated. Those in the range of 75 to 100 ng/ml are considered to be caused by a pituitary tumor until proved otherwise. Serum thyroxine and TSH levels are measured to rule out hypothyroidism, and LH and FSH levels are obtained if the individual is amenorrheic. CT, MRI, and carotid angiography may assist in the localization of adenomas.
Treatment is specific to the underlying cause and occurs after identification of the cause. Medical and surgical therapies may be involved. A pituitary microadenoma may be surgically removed, or treated medically with bromocriptine (Parlodel), which controls the tumor but does not cure it. A pituitary macroadenoma usually is treated medically because surgical and radiologic therapies seldom succeed.
Benign Breast Disease and Conditions
Benign breast disease (BBD) is a condition of noncancerous changes in the breast. Numerous benign alterations in ducts and lobules occur in the breast, including irregular lumps, cysts, sensitive nipples, and itching. The most common symptoms reported by women are pain, palpable mass, or nipple discharge; the majority of these prove to have a benign cause. However, histologic features, age at biopsy, and degree of family history have been found as major determinants of the risk of breast cancer after a diagnosis of BBD.199 This risk varies according to the histologic category of BBD (moderate in women with proliferative lesions without atypia and substantial in women with atypical (atypia) hyperphasia [AH])200 (see p. 875). Among premenopausal women, the risk appears to be greater for those with atypical lobular hyperplasia (ALH) than with atypical ductal hyperplasia (ADH) (see p. 875). For postmenopausal women the risk of breast cancer was similar between those with ALH or ADH.200 Family history is reported as an independent risk factor for breast cancer. Women with atypia and a family history had a breast cancer risk four times the expected risk.199 Risk was lower among those with atypia and no family history.
The College of American Pathologists has classified biopsy tissue according to breast cancer risk. These classifications are listed in Box 23-16. Benign epithelial lesions can be broadly classified according to their future risk of developing breast cancer as (1) nonproliferative breast lesions, (2) proliferative breast disease, and (3) atypical (atypia) hyperplasia.
Nonproliferative Breast Lesions: The term nonproliferative has been used to discriminate from the proliferative changes commonly associated with increased risk for development of breast cancer. This group includes fibrocystic changes (FCCs)—the most widely accepted term—for physiologic nodularity and breast tenderness that wax and wane with the menstrual cycle. On palpation, breasts are lumpy or bumpy and, in radiologic studies, breast tissue appears dense with cysts. These lesions cause women to seek medical attention because the lesions mimic carcinoma and produce palpable lumps or nipple discharge. Cysts (fluid-filled sacs) are a specific type of lump that commonly occurs in women in their 30s, 40s, and early 50s. Cysts feel “squishy” when they occur close to the surface of the breast but when deeply embedded they can feel hard (Figure 23-43). It has become increasingly clear that FCC is a heterogeneous group of lesions that should be diagnosed separately. An estimated 50% to 80% of women normally experience some of these changes. The prevalence of fibrocystic lesions is probably related to hormonal changes, which in turn are affected by genetic background, age, parity, history of lactation, caffeine consumption, and use of exogenous hormones.201 Based on experimental animal studies, it is assumed that breast cysts are the result of ovarian alterations, but the exact mechanism is unknown. Calcifications, found in cysts and adenosis or an increase in the number of acini per lobule, can form mammographically suspicious alterations.202 Cysts also can be associated with unilateral nipple discharge. A variety of substances are secreted into cyst fluid, including polypeptide hormones and male and female sex steroid hormones. Cysts often rupture with release of secretory material into the adjacent tissue. The resulting chronic inflammation and scarring fibrosis contribute to the palpable firmness of the breast.202 Fibrous tissue increases progressively until menopause and regresses thereafter.
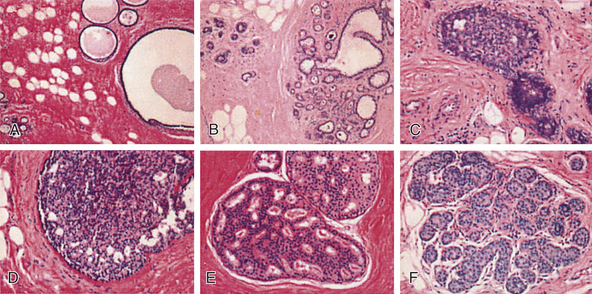
Figure 23-43 Benign breast disease. A, Nonproliferative fibrocystic changes. The architecture of the terminal-duct lobular unit is distorted by the formation of microcysts, associated with interlobular fibrosis. B, Proliferative hyperplasia without atypia. This is adenosis, a distinctive form of hyperplasia characterized by the proliferation of lobular acini, forming crowded glandlike structures. For comparison, a normal lobule is on the left side. C, Proliferative hyperplasia without atypia. There is moderate ductal hyperplasia, which is characterized by a duct that is partially distended by hyperplastic epithelium within the lumen. D, Proliferative hyperplasia without atypia, which is florid ductal hyperplasia. The involved duct is greatly expanded by a crowded, jumbled-appearing epithelial proliferation. E, Atypical ductal hyperplasia. These proliferations are complex and partially formed secondary lumens and mild nuclear hyperchromasia in the epithelial-cell population. The peripheral spaces are irregular and slitlike. F, Atypical lobular hyperplasia. Monomorphic, small, rounded, loosely cohesive cells fill the lumens of partially distended acini in this terminal-duct lobular unit.(Hematoxylin and eosin.) (From Elmore JG, Gigerenzer G: N Engl J Med 353[3]:231, 2005.)
In addition to FCC, many women experience benign breast tumors (Table 23-12 and Figure 23-44). In general, the frequency of chromosome abnormalities is lower in benign lesions than in breast cancer. Genetic aberrations are more common in proliferative than in nonproliferative lesions.202 The multiplicity of benign breast lesions, sometimes called heterogeneous benign breast disease (HBBD) in a biopsy appears to be a risk factor for progression to breast cancer.203
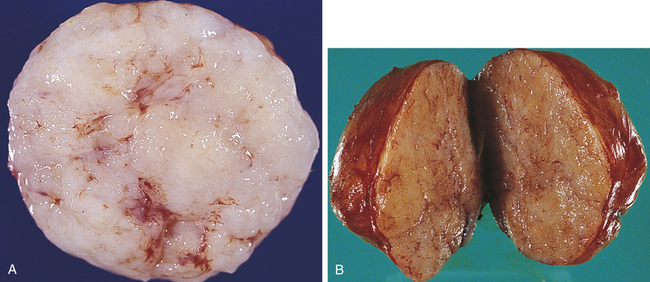
Proliferative Breast Lesions without Atypia: These disorders are characterized by proliferation of ductal epithelium and/or stroma without cellular signs of malignancy and in addition to fibroadenoma with complex features including the following structurally diverse lesions202:
1. Epithelial hyperplasia is defined by the presence of more than two cell layers above the basement membrane. In the normal breast, only myoepithelial cells and a single layer of luminal cells are present above the basement membrane.202 Moderate to florid hyperplasia is more than four cell layers above the basement membrane. The proliferating epithelium fills and distends the ducts and lobules by both luminal and myoepithelial cells.
2. Sclerosing adenosis is present when the number of acini per terminal duct is greater than twice the number found in uninvolved lobules. Calcification is commonly present within the lumens; however, the normal lobular arrangement is maintained. The acini are structurally altered and myoepithelial cells are prominent. Occasionally, stromal fibrosis may mimic the appearance of invasive carcinoma.202
3. Complex sclerosing lesion ([radial scar] radial sclerosing lesions, sclerosing papillary proliferation) refers to an irregular, radial proliferation of ductlike small tubules entrapped in a dense central fibrosis. The term scar refers to the structural appearance only because these lesions are not associated with prior injury or surgery. Radial scars (RSs) have been implicated as an independent risk factor for invasive breast cancer. However, a retrospective study of 9556 women found that although RSs mildly elevate the risk of invasive breast cancer, the risk was largely attributed to the coexistent presence of proliferative disease.204 Invasive breast cancer risk was further increased in women with AH.204,205 The appearance in mammograms of RSs, as well as the gross and microscopic appearance, can cause it to be confused with infiltrating ductal carcinoma.206
4. Papillomas consist of multiple finger-like projections or branching axes lined by myoepithelial cells and luminal cells. They constitute an important subset of mammary fibrocystic changes with about 5% of those with proliferative changes. Hyperplasia and metaplasia are often present within the ducts. Atypical hyperplasia may be present within or adjacent to papilloma, making the distinction from ductal carcinoma in situ (DCIS) difficult (see p. 898). The presence of atypia (ductal or lobular) coexisting with a single papilloma (atypical papilloma) does not appreciably modify the breast cancer risk attributable to just atypia.207 A single papilloma without atypia conveys a risk similar to proliferative fibrocystic lesions, whereas multiple papillomas, even without identified atypia, increase breast cancer risk significantly.207 Small-duct papillomas increase the risk of subsequent carcinoma; it is unknown whether large duct papillomas do as well.
Proliferative Breast Lesions with Atypia: Proliferative breast lesions with some abnormal structure or atypia include ADH and ALH.202 Atypical hyperplasia (AH) is an increase in the number of cells with some variation in cellular structure. Studies continue to indicate that women with AH have an increased risk (about fourfold) of breast cancer compared with women who have nonproliferative lesions.200 From the Nurses’ Health Study, time of benign breast biopsy appeared to influence the degree of later breast cancer risk among women with AH.200 Among premenopausal women at the time of their benign biopsy, the risk of breast cancer was substantially increased among women with AH (OR, 7.3) than among women with ADH (OR, 2.72). The risks for women who were postmenopausal at the time of benign biopsy were similar for women with ALH and those with ADH.200
Ductal hyperplasia is an increased number of cells mostly within the lumen of the terminal ducts (Figure 23-45, A). It includes a continuum of changes—cell structure and placement—ranging from an increase in cellularity to features of ductal carcinoma in situ (DCIS; see p. 898). In ADH, the cells fail to completely fill ductal spaces as compared with DCIS. Although still controversial, isoflavone exposure has been associated with a decreased risk of proliferative benign fibrocystic changes, nonproliferative changes, and breast cancer.208
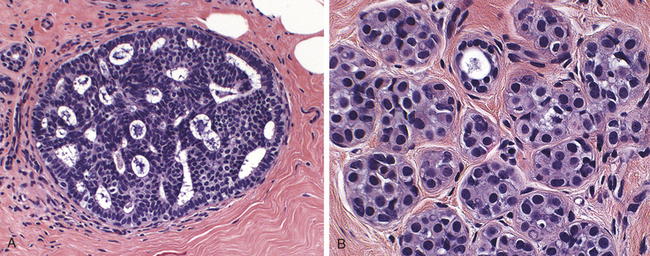
Figure 23-45 Atypical ductal and lobular hyperplasias. A, Atypical ductal hyperplasia. A duct is filled with a mixed population of cells. Although some of the spaces are round and regular, the peripheral spaces are irregular and slitlike. These features are highly atypical but fall short of a diagnosis of ductal carcinoma in situ (DCIS). B, Atypical lobular hyperplasia. A population of monomorphic small, rounded, loosely cohesive cells partially fill a lobule. (From Kumar V: Robbins and Cotran pathologic basis of disease, ed 8, Philadelphia, 2008, Saunders.)
Lobular hyperplasia refers to proliferation of small, uniform cells in the lumen of lobular units. The abnormal cells of atypical lobular hyperplasia (ALH) and lobular carcinoma in situ (LCIS) are identical, but the cells in ALH do not distend more than 50% of the acini within a lobule202 (see Figure 23-45, B). ALH can extend into ducts, and this is associated with an increased risk of invasive carcinomas.202 Other benign conditions are summarized in Table 23-13.
Table 23-13
Other Benign Breast Conditions
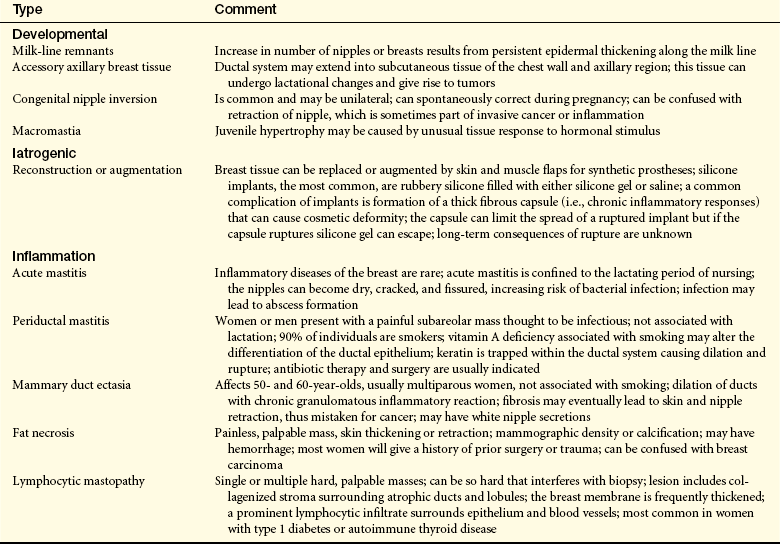
Data from Lester SC: The breast. In Kumar V, Abbas AK, Fausto N, editors: Robbins and Cotran pathologic basis of disease, ed 7, Philadelphia, 2005, Saunders.
EVALUATION AND TREATMENT Breast problems should be diagnosed from a multimodal approach that combines physical examination, mammogram when applicable, sonogram, possibly MRI, aspiration of lumps, and surgical or needle biopsy if warranted. Breast biopsy is used to make a definitive diagnosis and assess an individual’s risk for the development of breast cancer. The principal mammographic signs of breast carcinoma are densities and calcifications. However, the dense breast tissue often seen in young women can make interpretation extremely difficult (see also What’s New? Screening Mammograms: Far from Perfect in Chapter 11, p. 386). Ultrasonography (ultrasound) is used to differentiate a solid mass from a cystic (fluid-filled) mass, which is generally benign.
Treatment consists largely of relieving symptoms. Breast pain may be minimized by wearing a brassiere that provides good support. Reduction of caffeinated beverages, cola, root beer, and chocolate, which can cause overstimulation of breast tissue for some women, may reduce pain and nodularity. Given time the cysts may disappear without treatment.
Iodine deficiency may increase fibrocystic breast change, thus may be useful for relieving pain (see Nutrition & Disease: Diet and Breast Cancer Risk Updates, p. 892).209 Although unknown, increasing omega-3 fatty acids may decrease associated pain caused by inflammation as well as the application of castor oil packs to the breasts. The use of aspirin for decreasing breast alterations is being investigated (see below and What’s New? Inflammation, Breast Carcinogenesis, Aspirin, and NSAIDs). Drugs used to treat severe breast pain are listed in Table 23-14.
WHAT’S NEW?
Inflammation, Breast Carcinogenesis, Aspirin, and NSAIDs
The role of inflammation in breast disorders and cancer is a hot topic (see Figures A & B below). Specifically the role of the inflammatory enzymes cyclooxygenase (COX)-1 and COX-2 and drugs that inhibit COX-2 (see Chapters 6 and 11). COX-2 has been found to be associated with some cancers, including breast cancer. Inactivating COX-2 may interrupt carcinogenesis by several pathways: inhibition of angiogenesis, promotion of apoptosis, alteration of insulin, signaling pathways that result in insulin resistance, and suppression of estrogen synthesis through decreased aromatase activity (see Figure B on p. 878). Interleukin-6 (IL-6) is a cytokine reported to be involved in inflammation, insulin, and estrogen pathways, and IL-6 may be associated with breast cancer through several pathways (see Figure A). Several epidemiologic studies have examined the association between nonsteroidal anti-inflammatory drugs (NSAIDs) and breast cancer with inconclusive and inconsistent results. Most case-control studies, but not all, have found relative risk reductions from 20% to 40%.227, 228 Eight prospective studies found no association, six studies found a reduced risk, and one study found a U-shaped curved association.229 Alternate-day use of low-dose aspirin for a mean of 10 years in a randomized Women’s Health Study did not reduce the incidence of breast cancer.230 The American Association of Retired Persons (AARP) Diet and Health Study found breast cancer risk was not significantly associated with NSAID use, but daily aspirin (unknown dose) was correlated with a modest reduction in ER+ breast cancer.229 In 2004, investigators reported that aspirin use in women is associated with a significant reduction in the risk of breast cancer, especially for hormone receptor–positive tumors.231 This was the first report to examine whether the protective effects of aspirin varied with estrogen receptor (ER) or progesterone receptor (PR) status. Aspirin has been associated with a reduction in mortality from cardiovascular disease and colorectal cancer.232, 233 In mice, Chang and colleagues234 defined the molecular mechanisms by which COX-2 derived prostaglandin E2 (PGE2; proinflammatory) induced tumor-associated angiogenesis and initiation or progression of mammary cancer. These investigations reported that PGE2 induced angiogenesis at the earliest stage of tumor development, even before PGE2-induced mammary gland hyperplasia! From the Mayo Clinic Benign Breast Cohort (n = 9343), 40 of the 247 women with atypia have developed breast cancer. Of those atypia samples, investigators found significantly higher COX-2 staining intensity.235 Terry and colleagues231 found the inverse association between aspirin use and breast cancer was evident for every patient subgroup except those with negative hormone receptor status (ER−, PR−). The association was strongest among frequent aspirin users, unfortunately the dose was not identified. Acetaminophen was not associated with protection in any group. Aspirin showed more effects than ibuprofen (NSAID). These findings suggest possible mechanistic connections between aspirin and estrogen. In 1996, investigators suggested genetic activation of COX-2 in transformed mammary epithelial cells.236 The COX-2
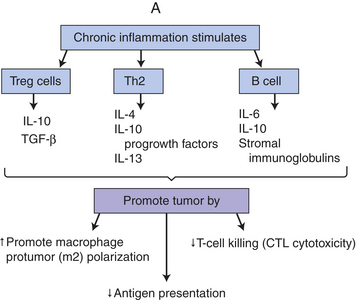
A, Chronic activated lymphocytes increase inflammation. Chronic activation of immune response when tissue injury/damage is not resolved results in accumulation of regulatory T cells (Treg), T-helper (Th2) cells, and activated B lymphocytes. These cells in turn cause the secretion of progrowth factors (i.e., interleukin 4 [IL-4], IL-6, IL-10, IL-13), transforming growth factor-beta (TGF-β), and immunoglobulins. Stromal infiltrating immunoglobulins may activate innate or inflammatory responses promoting disease progression. Retrospective studies reveal that the presence or maturation of immunoglobulin G (IgG) correlates with increases in disease stage (stage 1 versus stage 11) and in total tumor burden. Immunoglobulins found in the stroma are predominant lymphocyte populations (e.g., more than early ductal carcinoma in situ [DCIS]). These observations have been found in other types of solid tumors. Although immunoglobulins play a role in carcinogenesis, the specific mechanisms are unclear. A 2002 meta-analysis found tissue macrophage density was associated with a poor prognosis. Polarized macrophages (M1 and M2) are like Th1 and Th2 designations; that is, different macrophage phenotypes and functions. M2 cells participate in polarized Th2 reactions; promote killing of parasites; are present in tumors; and promote progression, tissue repair (thus paradoxical function), and remodeling. M2 increases production of inflammatory cytokines. Macrophages enhance angiogenesis by promoting angiogenic factors, including vascular endothelial growth factor (VEGF) and remodel the extracellular matrix, especially collagen fibrils (fibrillogenesis). Thus tumor invasion is enhanced because mobile and invasive tumor cells track along collagen fibers that are anchored to blood vessels—all potentiated by macrophages (M2). Activation of Th2 cells increases IL-4, IL-5, IL-6, IL-10, and IL-13, which induce immune unresponsiveness or T-cell anergy and loss of T-cell–mediated cytotoxicity (CTL). (Data from Bingle L, Brown NJ, Lewis CE: J Pathol 196:254-265, 2002; DeNardo NG, Coussens LM: Breast Cancer Res 9:212, 2007; Pollard JW: J Leuk Biol 84(3):623-630, 2008).
gene is normally inactive (quiescent) but becomes active in response to infection, inflammation (e.g., from arthritis), and growth factors. COX-2 has been found in precancerous breast disease (hyperplasia, hyperplasia with atypia) and noninvasive and invasive breast cancer. In the same year, Zhao and colleagues237 demonstrated that PGE2 can induce the enzyme aromatase leading to increased estrogen production in mammary adipose stromal cells. In 1999, investigators found that COX-2 is up-regulated in the normal adjacent epithelium to ductal carcinoma in situ and that COX-2 overexpression correlates with local areas of p16(INKA) hypermethylation (see Chapter 11) in vivo that might represent early neoplastic changes leading to breast cancer.238,239 All together and significant, these studies provide a notable rationale for a role of COX and prostaglandins in breast cancer, particularly among postmenopausal women. In vitro and animal studies have shown that NSAIDs inhibit COX-1 and COX-2, which oxygenate arachidonic acid and, ultimately, produce prostaglandins. Inhibiting COX-1 reduces platelet aggregation and gastrointestinal mucosa protection. Blocking or inactivating COX-2 may interrupt breast carcinogenesis and other tumors through multiple pathways (e.g., angiogenesis, apoptosis, aromatase, and estrogen synthesis).229 Emerging is inconsistent evidence of aspirin use in ER+ and PR+ breast cancers. Questions about the dosage; timing and duration of treatments; and management of side effects, such as gastric irritation and bleeding, and aspirin allergies and how to manage this risk need to be evaluated. Studies are ongoing to determine whether COX-2 selective inhibitors, either alone or in combination with other drugs, help prevent breast cancer.
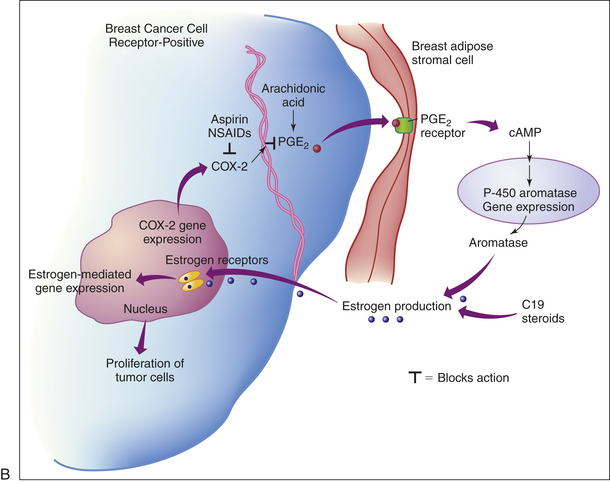
B, Proinflammatory PGE2 produced by breast cancer cells stimulates aromatase in breast stromal cells. Increased COX-2 can occur in precancerous breast disease (hyperplasia, hyperplasia with atypia) and noninvasive and invasive breast cancer. Here COX-2 in breast cancer cells leads to changes in tumor biology from increased PGE2 levels (i.e., can affect apoptosis, cell invasion, immune function, and angiogenesis). PGE2 can induce expression of local tissue levels of aromatase through increased cyclic adenosine monophosphate (cAMP) production in breast stromal cells. Thus estrogen synthesis is enhanced, which can increase proliferation of tumor cells. This paracrine loop (which is not associated with blood levels of estrogen) could explain why inhibition of COX-2 activity could decrease estrogen and decrease proliferation of hormone receptor-positive breast cancers. (Adapted from DuBois RN: JAMA 291:2488-2489, 2004.)
NUTRITION & DISEASE
Revisiting Iodine and Breast Alterations
The last national nutritional survey revealed that 15% of the U.S. adult female population are iodine deficient by the World Health Organization (WHO) standard, that is, less than 0.05 mg/L urine.210 Recommendations by the WHO, United Nations International Children’s Emergency Fund, and the International Council for the Control of Iodine Deficiency Disorders set 10 mcg/dl as the minimum urinary iodine concentration for iodine sufficiency.211 This amount corresponds to a daily intake of 150 mcg iodine. Large segments of Europe continue to have iodine deficiency. Significant deficiency is present in 45 countries in Africa, 15 in the Americas, 24 in Europe and Central Asia, 11 in Southeast Asia, 10 in the Middle East, and 9 in the Far East. Iodine deficiency is a common endocrine problem, presumably easy to correct, and the most preventable cause of mental retardation in many underdeveloped countries. Iodine is found in abundance in marine plants and animals in deposits of organic origin, in certain natural mineral waters, in phosphate rock, and in association with mineral deposits. A small fraction is from drinking water. Important factors in the depletion of iodine have been glaciation, which removes old soil and scrapes virgin rocks, the substitution of bromine for iodine in bread manufacturing, and decreases in iodinated salt intake.
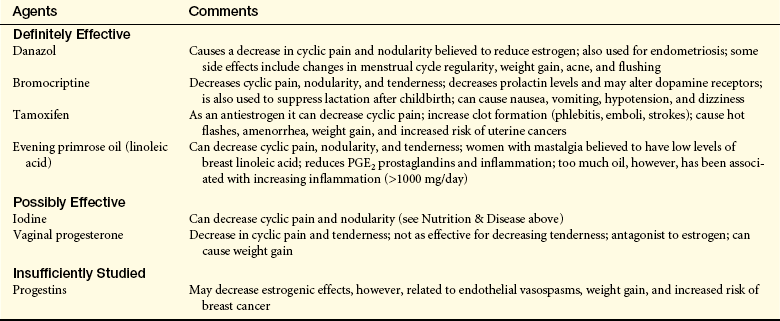
Although several extrathyroidal organs and tissues can concentrate and organify iodine, compelling evidence for iodine is its effects on the mammary gland. Intriguing is the concept that iodine deficiency causes fibrocystic changes in rodents and that iodine, and to a lesser extent iodide, induced relief of breast pain in two large uncontrolled trials and in one placebo-controlled trial.212, 213 In estradiol-treated rats, iodine deficiency has been shown to lead to pathologic changes similar to those noted in benign breast disease—cystic changes, periductal fibrosis, and lobular hyperplasia.214
Most studies on iodine function in humans and animals have focused on thyroid function. Little attention has been devoted to extrathyroidal tissues in which an important function of iodine is as an antioxidant in humans, including the eye, thyroid, and breast. The antioxidant properties of dietary iodide depend on redox reactions from iodination of tyrosine to the formation of thyroid hormones.215
Although thyroid-stimulating hormone has no role in promoting iodide intake into mammary cells, these cells have been shown to possess the sodium iodide symporter (transporter).216, 217 Uptake of iodide into mammary cells can be promoted by prolactin and other hormones (oxytocin, estrogens). Iodoproteins have been detected in breast tissue but it is not known how their facilitation occurs. Free radicals have been associated with carcinogenesis, including breast cancer. Although no direct evidence exists that iodide acts as an antioxidant in the breast, increased rates of breast cancer have been reported in iodine-deficient populations.218 Iodine deficiency also has been linked to increased fibrosis and adenosis of the mammary gland and administration of iodine has been used in the treatment of breast pain.212,219 It has been suggested that a combination of deficiency of iodine and selenium may facilitate the development of breast cancer.215,220 Funahashi and colleagues221,222 found that administration of Lugol’s iodine or iodine-rich wakame seaweed to rats treated with dimethylbenz(a)-anthracene (DMBA, a carcinogen) suppressed the development of mammary tumors. In addition, the same researchers documented that seaweed-induced apoptosis in human breast cancer cells had a stronger effect than fluorouracil (a strong chemotherapeutic agent) used to treat breast cancer. This finding led these authors and others to hypothesize that “seaweed may be applicable for prevention of breast cancer.”223 This hypothesis is intriguing because of the relatively low incidence of breast cancer in Japan in men and women who consume a diet rich in seaweed and with increasing breast cancer rates in Japanese women who emigrate to the West or consume a Western diet.224-226 The antioxidant potential of iodide may require its oxidation to iodine. Eskin and colleagues214 have postulated that normal physiologic function of mammary tissue requires iodine. Careful consideration of iodine deficiency is warranted because iodine replacement can promote problems with thyroid and extrathyroidal tissue function.