SEXUALLY TRANSMITTED INFECTIONS


Throughout recorded history, infectious diseases have threatened humans. Even into the twentieth century, epidemics of diphtheria, typhoid, tuberculosis, cholera, and other catastrophic infections have decimated entire communities almost overnight (see Chapter 9). Despite medical advances, improved living standards, and better nutrition, epidemics still arise as major public health problems, and some pose lethal threats to individuals and communities. Some of these epidemics are caused by sexually transmitted infections (STIs). At this time, many people consider the number of individuals with acquired immunodeficiency syndrome (AIDS), human immunodeficiency virus (HIV), and human papillomavirus (HPV) infections to be at epidemic levels.
Sexually contracted infections affect more than 19 million Americans per year, and half of those are younger than 25 years,1 and account for about one third of the reproductive mortality in the United States. Complications of STIs include pelvic inflammatory disease, infertility, ectopic pregnancy, chronic pelvic pain, neonatal morbidity and mortality, and genital cancers. Long-term sequelae of untreated or undertreated STIs may be disastrous and can affect a person’s physical, emotional, and financial well-being.
In the past an infection transmitted through sexual intercourse was called a venereal disease. Because of its limited scope, the term venereal disease has been replaced with sexually transmitted infection (STI). STIs are contracted by intimate, as well as sexual, contact and include systemic infections, such as tuberculosis and hepatitis, that can be spread to a sexual partner. Etiology of an STI may be bacterial, viral, protozoal, parasitic, or fungal (Table 24-1). Although the majority of STIs can be treated, virally induced STIs are considered incurable. The current increase in severity and incidence of STIs can be attributed to earlier onset of sexual activity and a greater number of lifetime sexual partners. Many infected individuals do not seek treatment because symptoms are absent, minor, or transient or because health services are inaccessible. Increased numbers of single individuals, bisexuality, and premarital or extramarital sexual affairs contribute to rising numbers of lifetime sexual partners and exposure to STIs. Indulgence in high-risk sexual behaviors and poor health habits, such as failure to use a condom in nonmonogamous or new relationships, and drug use, increases an individual’s risk of exposure or the severity of infection if exposed. Perhaps partly because of risk-taking behavior (unprotected intercourse or selection of high-risk partners), adolescents have the greatest risk for STI exposure and infection. In addition, adolescent women may have a physiologically increased susceptibility to infection because of increased cervical immaturity and lack of immunity. Rates of gonorrhea, chlamydia, vaginitis, cervical condyloma, genital warts, and pelvic inflammatory disease (PID) are highest in adolescents and young women and decline exponentially with increasing age. Women and infants bear the greatest burden from STIs.
Table 24-1
Currently Recognized Sexually Transmitted Infections
| Causal Microorganism | Infection |
| Bacteria | |
| Campylobacter | Campylobacter enteritis |
| Calymmatobacterium granulomatis | Granuloma inguinale |
| Chlamydia trachomatis | Urogenital infections; lymphogranuloma venereum |
| Polymicrobial | |
| Gardnerella vaginalis interaction with anaerobes (Bacteroides and Mobiluncus spp.) and genital mycoplasmas | Bacterial vaginosis |
| Haemophilus ducreyi | Chancroid |
| Mycoplasma | Mycoplasmosis |
| Neisseria gonorrhoeae | Gonorrhea |
| Shigella | Shigellosis |
| Treponema pallidum | Syphilis |
| Viruses | |
| Cytomegalovirus | Cytomegalic inclusion disease |
| Hepatitis B virus (HBV) | Hepatitis |
| Hepatitis C virus (HCV) | Hepatitis |
| Herpes simplex virus (HSV) | Genital herpes |
| Human immunodeficiency virus (HIV) | Acquired immunodeficiency syndrome (AIDS) |
| Human papillomavirus (HPV) | Condylomata acuminata, cervical dysplasia, and cervical cancer |
| Molluscum contagiosum virus | Molluscum contagiosum |
| Protozoa | |
| Entamoeba histolytica | Amebiasis; amebic dysentery |
| Giardia lamblia | Giardiasis |
| Trichomonas vaginalis | Trichomoniasis |
| Ectoparasites | |
| Phthirus pubis | Pediculosis pubis |
| Sarcoptes scabiei | Scabies |
| Fungus | |
| Candida albicans | Candidiasis |
STIs are stereotyped as occurring only among urban poor and minority populations. Because the Centers for Disease Control and Prevention (CDC) do not require that all STIs be reported, private physicians may not report them. Thus reported STIs often come from public health clinics, giving the impression that a greater number of the urban poor and minority populations are infected with STIs. In fact, STIs are prevalent in all socioeconomic groups.
SEXUALLY TRANSMITTED UROGENITAL INFECTIONS
Gonorrhea
Gonorrhea is caused by gonococci (singular, gonococcus), which are microorganisms of the species Neisseria gonorrhoeae. Neisser first identified gonococci in stained smears of vaginal, urethral, and conjunctival exudate in 1879. Until 1994 gonorrhea was the most commonly reported communicable infection in the United States. After declining 74% between 1974 and 1997, the rates for gonorrhea have remained relatively stable in the United States. The number of reported cases in 2007 was 355,991,2 but the actual number of cases is estimated to be twice as high.
Infection rates are highest in the southern region of the country, but appear to be stable.3 The number of reported cases decreased in all racial and ethnic groups between 2006 and 2007, except for blacks. The gonorrhea rate is now about 19 times greater for blacks than for non-Hispanic whites, down from 23 times higher in 1999.2 Other demographic and lifestyle risk factors may include transient or urban residence, early onset of sexual activity, multiple serial or consecutive sex partners, drug use, prostitution, and previous gonorrheal or concurrent STI.2 The risk of developing gonorrhea from intercourse with an infected male partner is 50% to 80% for women, and with an infected female partner, it is 20% to 30% for men. The risk increases threefold to fourfold for men after four exposures to an infected partner.
Transmission of gonococcal infection generally requires contact of epithelial (mucosal) surfaces, such as occurs during sexual, oral, or anal intercourse. A pregnant woman also can
transmit gonorrhea to her fetus. The infection passes from mother to child across the amniotic membranes, by direct inoculation with a fetal scalp electrode during labor monitoring, or during passage through the birth canal. Fomites (contaminated objects) are rarely involved in the transmission of N. gonorrhoeae, primarily because the gonococcus requires a rich medium (e.g., body fluids) and an environment high in carbon dioxide (5% to 10%) for growth.
PATHOPHYSIOLOGY Humans are the only natural hosts for N. gonorrhoeae, which is an aerobic, non–spore-forming, oxidase-positive gram-negative coccal (round) microorganism that usually appears in pairs (diplococci), with the adjacent sides slightly flattened. Hairlike filaments, called pili, appear to help the microorganisms attach themselves to host cells: the epithelial cells of mucous membranes (Figure 24-1). Columnar, transitional, and stratified squamous epithelial cells are infected most often. First the microorganisms become attached to the plasma membranes (cell walls) of these cells, and then they invade the cells and begin to damage the mucosa. Generally a quick leukocytic (inflammatory) response and exudation at the site of infection occur.

Figure 24-1 Gonococci. Scanning electron microscopy showing gonococci attaching to the nonciliated cells of human fallopian tube mucosa. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
In women the endocervical canal (inner portion of the cervix) is the usual site of original gonococcal infection, although urethral colonization and infection of Skene or Bartholin glands also are common. Several factors can facilitate ascent of gonococci into the uterus and the fallopian tubes, where they cause pelvic inflammatory disease (PID). Among these factors are (1) disintegration of the cervical mucous plug and a rise in vaginal pH above 4.5 during menstruation, (2) uterine contraction that may cause retrograde menstruation into the fallopian tubes, and (3) various microbes that possess virulent potentiating factors for chlamydia or gonococcal PID. Bacteria (N. gonorrhoeae, Chlamydia trachomatis) also may adhere to sperm and be transported to the fallopian tubes. In the fallopian tubes, progressive mucosal and submucosal invasion and sloughing of normal, ciliated tubal epithelium are accompanied by marked inflammatory response, causing the fallopian tubes to fill with exudate (see Chapter 23 for more on PID). In men the gonococci typically infect the urethra. Untreated urethral infection causes epididymitis in 1% to 2% of men and, rarely, urethral stricture and sterility. Commonly, concurrent oropharyngeal and anorectal infection can be found in infected men and women.4–6 Virulence is determined by variations in the bacterial properties and host response.
CLINICAL MANIFESTATIONS The clinical manifestations of gonorrhea can be categorized as local or systemic and uncomplicated or complicated. Uncomplicated local infections are seen as urethral infections in men and urogenital infections in women. In men the incubation period for urethritis is 3 to 10 days with a range of 12 hours to 3 months.7 Without treatment, urethritis persists for 3 to 7 weeks, with 95% of men becoming asymptomatic after 3 months. Approximately 60% of men infected suddenly experience marked dysuria (painful or difficult urination) and spontaneous, profuse, mucopurulent discharge from the urethra. However, some individuals have little discharge or urethral itching only, and 5% to 10% never have signs or symptoms. Most cases of untreated gonococcal urethritis resolve spontaneously after several weeks, and more than 95% of individuals are asymptomatic by 6 months after infection. Some men develop urethritis even after being appropriately treated.
In women the incubation period varies, but those who typically develop symptoms do so within 10 days of exposure or within 1 to 2 days after the next menstrual period. The clinical manifestations of uncomplicated gonorrhea in women may be absent (50% of women have asymptomatic infection) or severe; they can include dysuria, increased vaginal discharge, abnormal menses (increased flow or dysmenorrhea), or dyspareunia. Physical examination may disclose cervical friability and erythema (redness) and purulent or mucopurulent discharge from the cervical os (Figure 24-2). There may be a discharge from the Skene or Bartholin glands if these sites are involved.

Figure 24-2 Gonococcal cervicitis. The cervix is involved in 85% to 90% of cases in women, but the resultant discharge is profuse enough to be recognized in only 10%. (From McMillan A, Scott GR: Sexually transmitted infections, ed 2, London, 2000, Churchill Livingstone.)
Anal and rectal gonococcal infection is found in 30% to 50% of women diagnosed with urogenital gonorrhea. In women, anorectal infection is usually asymptomatic and not necessarily related to anal intercourse. Anorectal gonorrhea most commonly occurs in homosexual men with a history of receptive anorectal intercourse. About 50% of these infected men have symptoms.7
Symptoms of anorectal gonorrhea range from mild anal pruritus (itching), mucopurulent rectal discharge, and slight rectal bleeding to severe rectal pain, tenesmus (painful and ineffectual straining at stool), and constipation. Physical examination may disclose anal erythema and discharge and evidence of mucosal damage to the anus and rectum, such as friability, edema, and purulent exudate.
Gonococcal pharyngitis occurs primarily in homosexual or bisexual men or heterosexual women after fellatio (oral sexual contact) with an infected partner. Symptomatic pharyngitis is indistinguishable from any other bacterial pharyngitis and can include fever, lymphadenopathy, and tonsillitis. Approximately 60% of these infections are asymptomatic.
Other sites of uncomplicated local infections include the eye, leading to conjunctivitis; however, this is rare in adults. Primary cutaneous infection also has been reported and is usually manifested as a localized ulcer of the genitalia, perineum, proximal lower extremities, or fingers. It is important to determine whether such infections are the result of N. gonorrhoeae or secondary colonization by a preexisting lesion.
Localized gonococcal infections can be complicated by prostatitis, epididymitis, lymphangitis, and urethral stricture in men and salpingitis, PID, and bartholinitis in women. Chronic salpingitis or perididymitis can cause scarring and tubal adhesions that lead to sterility. Anyone who is infected and remains untreated is at risk for disseminated gonococcal infection.4–6
Before the advent of antimicrobial therapy, approximately 20% of infected men developed acute epididymitis. Men with this condition report unilateral testicular pain and swelling and commonly have overt urethritis at the same time. Penile lymphangitis is a rare complication with an unclear pathogenesis.4 Before modern antibiotics, individuals with this condition were at risk for developing urethral strictures; however, this complication is now uncommon if treatment is sought and therapy instituted properly.
Acute salpingitis, or PID, is the most common local complication in women. Approximately 10%2 of women with untreated cervical gonorrhea develop this condition. Salpingitis is significant in its development because of the potential long-term sequelae associated with it, namely, infertility and ectopic pregnancy.
The onset of symptoms may be rapid and usually occurs during menses. Women may experience chills, fever, nausea, vomiting, and lower abdominal pain that worsen with coughing, sneezing, or intercourse. Abdominal palpation often discloses bilateral lower quadrant tenderness and rebound tenderness resulting from peritoneal irritation caused by tubal exudate. Marked tenderness of the internal genitalia is often noted during pelvic examination. Enlargement or masses also may be palpable in the upper genital tract. Abscess of Skene and Bartholin glands is also a local complication associated with gonococcal infection in women. Tubal infertility is found in 8% of women after one episode of PID. If a woman has three or more episodes of PID, she has a 40% risk of tubal infertility.8 Apart from PID, abscess formation of Bartholin glands is the most common complication of gonorrhea in women.
Disseminated gonococcal infection (DGI) is a rare systemic complication brought about by the spread of infection through the bloodstream. Less than 1% of individuals with untreated gonococcal infection develop this complication.9 Men are affected more than women. Symptoms include fever, rash, and joint swelling or pain.
Spread of N. gonorrhoeae to the liver causes a condition known as perihepatitis or Fitz-Hugh–Curtis syndrome. C. trachomatis also has been identified as a causative agent. Inflammation of the capsule of the liver is the primary pathologic manifestation and produces sudden and intense right upper quadrant pain.10 This complication usually develops after acute salpingitis and is very rare in men.
Newborns are at risk most commonly for gonococcal eye infection (ophthalmia neonatorum) (Figure 24-3) but also may acquire rhinitis, anorectal infection, or an abscess at the site of electrode placement for fetal monitoring. Onset of symptoms generally occurs 1 to 12 days after birth, with a mean of 4 to 6 days. Affected newborns usually are born to mothers who have had prolonged ruptured membranes. In these cases, immediate treatment with a topical antibiotic is not effective because the infection is already established. Established infection causes bilateral corneal ulceration, with a profuse yellow or gray purulent exudate and is followed by necrosis, scarring, and compromised vision. Signs of systemic disease are seldom apparent.
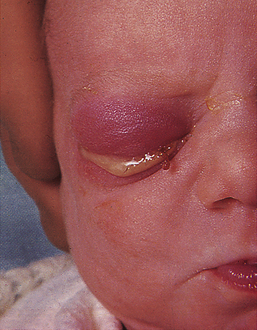
Figure 24-3 Gonococcal ophthalmia neonatorum. (Examiner would be gloved.) (From McMillan A, Scott GR: Sexually transmitted infections, ed 2, London, 2000, Churchill Livingstone.)
EVALUATION AND TREATMENT Clinical signs and symptoms are not sufficient for the differential diagnosis of gonococcal infections. Microscopic evaluation of Gram-stained slides of clinical specimens is deemed positive for N. gonorrhoeae if gram-negative diplococci with typical “kidney bean” morphology are seen inside polymorphonuclear leukocytes. Such a finding is considered adequate for the diagnosis of gonococcal urethritis in a symptomatic man. For women the Gram-stain technique is less accurate and reliable and is replaced with a single culture of endocervical secretions. Most clinic settings now use ligase chain reaction (LCR), polymerase chain reaction (PCR) testing, or deoxyribonucleic (DNA) testing because these samples do not require an anaerobic incubation, are highly sensitive, and can be easily transported to a laboratory for testing. Because of the large percentage of infected women without symptoms, routine screening for at-risk women is recommended. Tests should be obtained from any site that may be exposed.11
The many different strains of N. gonorrhoeae vary with respect to pathogenicity, virulence, and susceptibility to antibiotics. Several types of drug-resistant strains have been identified, including penicillinase-producing N. gonorrhoeae (PPNG), which is resistant to penicillin; tetracycline-resistant N. gonorrhoeae (TRNG), which is resistant to tetracycline; chromosomal control of mechanisms of resistance of N. gonorrhoeae (CMRNG), which is resistant to penicillin and tetracycline; and increasingly a fluoroquinolone-resistant N. gonorrhoeae (QRNG).12,13 Of all the isolates collected in 2006 by the Gonococcal Isolate Surveillance Project (GISP), 25.6%2 were resistant to penicillin, tetracycline, ciprofloxacin, or some combination of these antibiotics.2 In the United States the overall percentage of PPNG isolates has declined every year since 1991.12 However, QRNG has been increasing in Asia, the Pacific Islands, Hawaii, and has now become widespread in the United States. The CDC no longer recommends fluoroquinolone treatment for the treatment of gonococcal infections and associated conditions, such as pelvic inflammatory disease, and issued an important treatment update in 2007. Until 2007, fluoroquinolones were the first line treatment recommended by the CDC. The only class of drugs still recommended for treatment of gonorrhea are the cephalosporins.14
Another major concern is the coexistence of chlamydial infection with gonorrhea.15 (Chlamydial infections are discussed on p. 935.) Approximately 20% to 30% of men and a higher proportion of women have coexistent chlamydia infections. In the absence of gonorrhea, chlamydia may go undetected until complications such as PID or urethritis manifest themselves.
Treatment for gonorrhea is influenced by three factors: (1) the spread of infection caused by drug-resistant strains, (2) the high frequency of chlamydia infection accompanying gonorrhea, and (3) recognition of the serious complications of chlamydia and gonorrheal infections. CDC treatment guidelines are updated regularly, and the most recent edition should be used. Current CDC treatment guidelines for uncomplicated gonorrheal infections are listed in Box 24-1; complicated infections require intravenous antibiotic therapy and possibly hospitalization.
Sexual partners also are assessed and treated according to these protocols, and sexual contact is avoided until treatment is completed. Condoms are strongly recommended to prevent future infection.
Syphilis
Syphilis, a disease with local and systemic manifestations, has been well known throughout history. Many famous figures from the ancient world and from the royal families of Europe were thought or known to have had syphilis.16 In the early half of the 1900s, an estimated 1 in 4 to 1 in 20 Americans were infected.17 With the advent of antibiotics and intensive public health efforts during and after World War II, the prevalence of syphilis declined sharply to 3 in 100,000 Americans in 2002. Rates of syphilis declined in the 1990s and reached an all-time low in 2000 (2.2 cases per 100,000). However, between 2000 and 2007, the syphilis rate in the United States increased. Between 2006 and 2007, the national primary and secondary rate increased 15.2%, from 3.3 to 3.8 cases per 100,000 population, with the number of cases increasing from 9756 to 11,466 between 2006 and 2007.4 The rate of primary and secondary syphilis has risen 54% among men in the past 5 years. Data suggest this increase is driven by increased transmission of primary and secondary syphilis among men who have sex with men (MSM), and accounts for 65% of these cases. The rate of primary and secondary syphilis is now nearly six times greater in men than women, whereas rates were almost equivalent a decade ago. Syphilis remains a problem in certain geographic regions, particularly in the South. Syphilis facilitates the transmission of HIV infection and seems to contribute to HIV transmission in those parts of the United States where rates of both infections are high. The rates of syphilis increased for all groups except for blacks between 2000 and 2003. Since 2003 the rates have increased for all groups; in 2007 the reported rate among non-Hispanic whites was 2.0 per 100,000, among Hispanics the rate was 4.3 per 100,000, among Asian/Pacific Islanders the rate was 1.2 per 100,000, among Native American/Alaskan Natives the rate was 3.8, and among Blacks the rate was 14 per 100,000. Rates in women have also increased; 10% between 2006 and 2007.18 Subsequently, the yearly 14% percent decrease in congenital syphilis since 1996 ended in 2005 with increases of 11% and 15.4% for 2006 and 2007. The subsequent result is a reported 10.5 cases of congenital syphilis per 100,000 (it had been reported at 0.8 per 100,000 in 2003). During pregnancy, untreated early syphilis results in perinatal death in as many as 40% of cases and, if acquired in the previous 4 years, may lead to fetal infection in more than 70% of cases.19
Race, ethnicity, and gender alone do not alter STI risk but rather act as risk markers that correlate with other more fundamental determinants of health status, such as poverty, access to quality care, and health-seeking behavior. Higher infection rates have been associated with urban areas, with the exchange of sex for drugs, especially crack cocaine, and with prison populations.3,20 A growing concern is the incidence of coinfection with HIV among MSM.3,18
PATHOPHYSIOLOGY Treponema pallidum, the cause of syphilis, is an anaerobic bacterium that cannot be cultured in vitro. The treponema (individual microorganism) looks like a corkscrew, with regular, tight spirals and a rotary motion; it can infect any body organ or tissue. Because the bacterium is present in exudate from moist mucosal or cutaneous lesions, the spirochete is transmitted during the first few years of infection. Transmission generally occurs through minor abrasions during sexual intercourse but can occur extragenitally as well. Approximately 30% to 50% of partners who have sexual intercourse with an individual in early stage syphilis develop the disease.16
Syphilis becomes a systemic disease shortly after infection and can be transmitted from a pregnant woman to her fetus as early as the ninth week of gestation. The risk of transmission to the fetus gradually declines with each subsequent pregnancy; therefore, a mother who has had several children with severe congenital syphilis may go on to bear a healthy child. After about 8 years, even without treatment, the mother’s infection is not transmitted to her fetus.17
The course of untreated syphilis consists of four stages: primary, secondary, latent, and tertiary (Box 24-2).
Primary syphilis begins at the site of bacterial invasion (Figure 24-4). There T. pallidum multiplies in the epithelium, producing a granulomatous tissue reaction called a chancre. Some microorganisms drain with lymph into adjacent lymph nodes. Within the nodes and at the site of the chancre, the cell-mediated and humoral immune responses are stimulated.
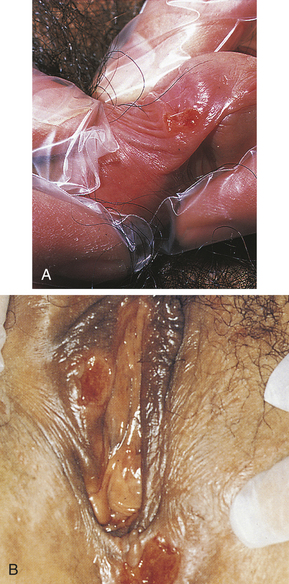
Figure 24-4 Primary syphilis. A, Penile chancre. B, Vulval chancres; the the labia and perineum show induration and edema of chancres. (A from McMillan A, Scott GR: Sexually transmitted infections, ed 2, London, 2000, Churchill Livingstone; B from Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
Secondary syphilis is systemic. During this stage, blood-borne bacteria spread to all major organ systems. The secondary stage is followed by a period during which the immune system is able to suppress the infection. Even without treatment, spontaneous resolution of the skin lesions occurs and the individual enters the latent stage of infection. Latent syphilis may be subdivided into early and late stages; however, no specific criteria delineate one from the other.20 Medical history and serologic studies show that syphilis is present, but the individual has no clinical manifestations. Transmission is possible during the late and early latent stages.
Tertiary syphilis is the most severe stage, involving significant morbidity and mortality. The pathogenesis of syphilitic manifestations at this stage remains unclear. The destructive skin, bone, and soft tissue lesions (called gummas) of tertiary syphilis probably are caused by a severe hypersensitivity reaction to the microorganism. Within the cardiovascular system, infection with T. pallidum may cause aneurysms, heart valve insufficiencies, and heart failure. Within the central nervous system (CNS), the presence of T. pallidum in cerebrospinal fluid may cause the manifestations of neurosyphilis.17
The risk of acquiring congenital syphilis (CS) is estimated at 50% in primary and secondary syphilis, 40% in early latent syphilis, and 10% in late latent syphilis.21 Intrauterine infection causes fetal or perinatal death in 40% of affected infants.19,22
Primary Stage: In adults the incubation period of syphilis ranges from 12 days to 12 weeks after exposure and averages 3 weeks. At the site of treponemal entry a sore, or hard chancre, develops. Typically the chancre is an eroded, painless, firm, and indurated (hard) ulcer that may be a few millimeters to 2 cm in diameter. Firm, enlarged, and nontender regional lymph nodes accompany chancres. Figure 24-4 shows typical chancres of the penis and vulva. Syphilitic chancres are not always typical, however, and syphilis should be considered in the presence of any open lesion. Secondary infection can cause chancres to become necrotic and painful, and lesions on the fingers may be dry, scaly, and papular or moist and vegetative. If left untreated, the chancre of primary syphilis heals in 2 to 8 weeks and then spontaneously disappears, usually without leaving a scar.
Secondary Stage: Clinical manifestations of secondary syphilis usually develop 6 weeks after the first appearance of the chancre but may overlap with those of the primary stage. Typically this stage presents with variable systemic symptoms, including low-grade fever, malaise, sore throat, hoarseness, anorexia, generalized adenopathy, headache, joint pain, and skin or mucous membrane lesions or rashes. Cutaneous (skin) rashes are generally papulosquamous (raised and scaly), but any variation or combination of macular (flat), papular (raised), and pustular (pus-filled) lesions may be seen. Often lesions are widespread and bilateral and appear on the palms and soles (Figure 24-5). Some lesions become hypertrophied, flat, moist, and wartlike or vegetative (e.g., cauliflower-like). These lesions, called condylomata lata, are highly contagious and develop on the perineum, vulva, and groin of women (Figure 24-6) and around the inner thigh and the anal area in men and women. Besides skin sores, oral mucous membrane lesions (known as mucous patches), lymphadenopathy, pruritus, and alopecia are common. Some individuals develop anemia, leukocytosis, increased sedimentation rate, hepatitis, transitory proteinuria, arthritis, electrocardiographic abnormalities, and CNS symptoms. Regardless of whether treatment is given, the cutaneous lesions generally heal in 2 to 10 weeks, but relapses may occur for several years.21


Latent and Tertiary Stages: The asymptomatic, latent stage of syphilis may be as short as 1 year or as long as a lifetime. After the latent stage, tertiary syphilis may present with gummas, cardiovascular lesions, and neurosyphilis. These manifestations of tertiary syphilis are quite rare because antibiotics can cure syphilis.
Congenital Syphilis: Congenital syphilis is characterized by vasculitis, necrosis, fibrosis, and distribution of T. pallidum throughout the tissues; it is divided into early and late stages. Signs and symptoms of early CS manifest in the first 2 years of life, and clinical manifestations of the late stage often occur near puberty. Affected newborns often are premature and show evidence of intrauterine growth restriction, hepatosplenomegaly, bone marrow depression, destructive bone and skin lesions (see Figure 24-5), retinal inflammation, glaucoma, blood dyscrasia, nephrotic syndrome, and varying degrees of CNS involvement.17 Late manifestations of classic congenital syphilis correspond to those of tertiary syphilis in the adult and are rare.
EVALUATION AND TREATMENT Because T. pallidum cannot be cultured in vitro, early definitive diagnosis of primary or secondary syphilis depends on darkfield microscopy of a specimen taken from a chancre, regional lymph node, or other lesion. If the initial result is negative, the darkfield examination is repeated on 2 successive days. When suspicion of syphilis—based on history and physical examination—persists, serologic testing is required. An algorithmic approach to the diagnosis of genital ulcers is presented in Figure 24-7.
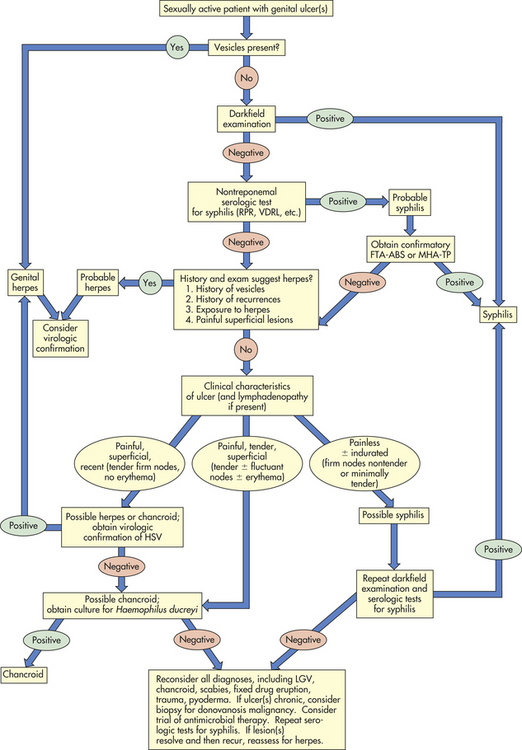
Figure 24-7 Genital ulceration. Algorithm outlining an approach to the diagnosis of an individual who presents with a genital ulceration. FTA-ABS, Fluorescent treponemal antibody absorption; HSV, herpes simplex virus; LGV, lymphogranuloma venereum; MHA-TP, microhemagglutination assay–Treponema pallidum; RPR, rapid plasma reagin; VDRL, Venereal Disease Research Laboratory. (Redrawn from Pitot P, Plummer FA. In Holmes KK et al, editors: Sexually transmitted diseases, ed 2, New York, 1990, McGraw-Hill.)
Two categories of serologic testing exist: nontreponemal antigen tests and treponemal antibody tests.23 Nontreponemal antigen tests, which demonstrate the presence of reagin (a group of antibodies present in syphilis) in serum, provide indirect evidence of infection. Examples of nontreponemal analysis are the Venereal Disease Research Laboratory (VDRL) antigen and the rapid plasma reagin (RPR) tests (Box 24-3). These tests yield a positive result (presence of reagin) in more than 50% of individuals with primary syphilis and 100% of individuals with secondary disease. When the serologic test is negative and another stage of syphilis is suspected, the test is repeated. If latent or tertiary syphilis is suspected, a treponemal serologic test is done. Treponemal tests are serologic-specific tests that are used to assess antibody response to T. pallidum and include the fluorescent treponemal antibody absorption (FTA-ABS) test and the microhemagglutination (MHA-TP) test.
Numerous dermatologic disorders can mimic the skin lesions of secondary syphilis, making differential diagnosis difficult. Again, laboratory confirmation is important; darkfield microscopy of scrapings from the condylomata lata or other skin lesions discloses the treponemata. Serologic tests are almost always strongly positive in this stage.
During the latent stage, individuals continue to have serologic evidence of untreated disease, but confirmation through darkfield microscopy is difficult. Examination of cerebrospinal fluid may confirm that the treponemata are present and the insidious onset of neurosyphilis has begun.
Preferred treatment for all stages of syphilis is parenteral injection of benzathine penicillin G. If the individual has had signs of the disease for less than 1 year, a single dose is appropriate. If signs have been present for more than 1 year, the treatment is three weekly injections. This therapy is also appropriate for pregnant women. There is no evidence to date that T. pallidum has developed resistance to penicillin. In fact, it is highly sensitive but because of the slow replication time serum levels must be maintained for 7 to 14 days. Duration of therapy depends on estimated length of infection. Treatment for 14 days is recommended if the individual has been infected less than 1 year; treatment is for 28 days if the individual has been infected for longer than 1 year. Individuals who are allergic to penicillin may receive oral doxycycline, 100 mg twice daily for 14 days. Pregnant women with a penicillin allergy should be desensitized and then treated with benzathine penicillin G as recommended by the CDC.14 Because treatment failures do occur, all individuals should have follow-up evaluation. Sexual partners also are examined and treated, and the use of condoms is recommended.
Definitive diagnosis of CS is made by microscopic identification of T. pallidum in material from skin lesions or nasal discharge. Probable diagnosis is assumed on the basis of a rising or persistently reactive FTA-ABS value and clinical manifestations. In all cases of maternal syphilis, the goal is to treat the mother to prevent CS. Maternal treatment with penicillin before delivery usually prevents CS. If the infant requires treatment, penicillin is the drug of choice because allergy does not pose a problem in the neonatal period. Such infants are then given serologic tests for syphilis every 2 to 3 months until the test becomes nonreactive or the titer has decreased fourfold. Nearly all tests become nonreactive (negative) by the time the infant is 6 months of age.19
Chancroid
Chancroid, or soft chancre, is an acute infectious disease that was first differentiated from syphilis in 1852. It is caused by Haemophilus ducreyi, a gram-negative bacillus. Chancroid occurs most often in underdeveloped or developing tropical countries. Although incidence in the United States is low, 54 cases were reported to the CDC in 20032; sporadic outbreaks can occur and tend to be associated with conditions such as poverty, urban prostitution, and illicit drug use, in which individuals continue to engage in intercourse in spite of the presence of a lesion.24
PATHOPHYSIOLOGY H. ducreyi is a gram-negative bacillus with rounded ends. Under a microscope it is commonly observed in small chains or clusters along mucous strands. Transmission can occur through sexual contact and autoinoculation. There is no evidence of maternal-fetal transfer before or after delivery. Chancroid lesions usually are found on the internal surface of the foreskin or its point of attachment to the penis (the frenulum) in men and on the labia, clitoris, or fourchette in women. Initially the papule enlarges; it then erodes into a soft, circumscribed ulcer containing a superficial exudate. Beneath the ulcer is a lesion characterized by edema, endothelial proliferation, and a base of granulation tissue that is full of lymphocytes and plasma cells. Adjacent lymph nodes are acutely inflamed and full of polymorphonuclear leukocytes and necrotic cells.25
CLINICAL MANIFESTATIONS Chancroid has an incubation period of 3 to 10 days.26 Generally women are asymptomatic, but depending on the site of infection, can present with less obvious symptoms (dysuria, dyspareunia, vaginal discharge, pain on defecation, or rectal bleeding). Constitutional symptoms are unusual. At the site of inoculation, an initial vesicopustule lesion forms and erodes into a soft ulcer with a necrotic base, surrounding erythema, and a ragged, serpiginous (spreading) border (Figure 24-8). Unilateral, painful, local lymphadenopathy presents in about half of infected individuals—primarily men. (Women tend to have multiple lesions.) Inguinal buboes (unilocular abscess of the inguinal lymph nodes) develop 7 to 10 days after the initial chancre and fill with exudate. In 25% to 60% of cases, the buboes spontaneously rupture. Multiple lesions spread through autoinoculation.
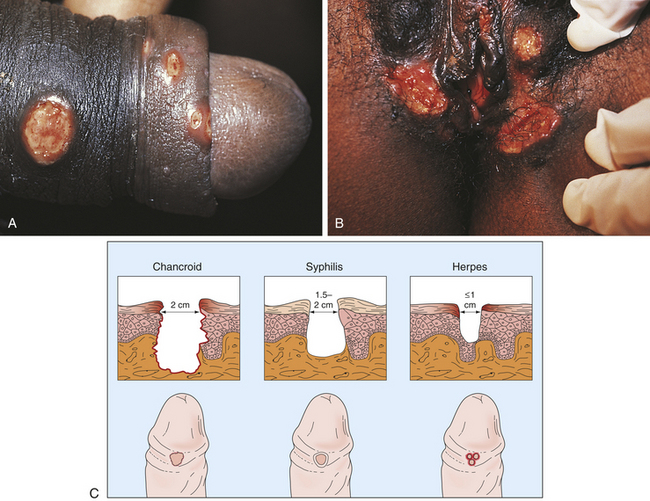
Figure 24-8 Chancroid. A, Ulcers on the penile shaft. B, Multiple vulvar lesions. C, Differences in clinical appearance among chancroid, syphilis, and genital herpes. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
Frequently, ulcers on the prepuce may lead to phimosis or paraphimosis. Other complications of chancroid include balanitis, secondary infections, necrosis, and fistula formation. Recalcitrant, serpiginous lesions may take months or years to heal.
EVALUATION AND TREATMENT Chancroid is easily confused with other types of genital ulcers, particularly those of syphilis, genital herpes, and granuloma inguinale (see Figure 24-8). Unlike the syphilitic ulcer, chancroidal ulcer is painful, tender, and nonindurated. Microscopic analysis of a gram-stained smear from the chancroid helps to identify the microorganism. Definitive diagnosis depends on recovery of H. ducreyi from cultured specimens. Fluorescent monoclonal antibody stains and PCR provide more specific diagnosis but are not routinely available. Because 10% of infected individuals are coinfected with syphilis or herpes simplex virus (HSV), testing includes serologic examination for syphilis and viral culture for HSV. In addition, HIV testing is recommended: chancroid is a cofactor for transmission of HIV.
Resistance to recommended antibiotics has emerged in isolated instances worldwide. Recent treatment recommendations include a single intramuscular injection of ceftriaxone (250 mg) or a single dose of oral azithromycin (1 g). Effective oral multiple-dose regimens include ciprofloxacin, 500 mg orally twice daily for 3 days; or erythromycin, 500 mg three times daily for 7 days. Persons infected with HIV have higher rates of treatment failure with single-dose therapy and may require a longer treatment regimen. As a palliative measure, buboes can be aspirated through adjacent, healthy skin. In approximately 5% of cases, relapses at the site of original ulcer have occurred.26,27 Simultaneous treatment of sexual partners and condom use are recommended to prevent reinfection.
Granuloma Inguinale
Granuloma inguinale (donovanosis) is a chronic, progressively destructive bacterial infection caused by Calymmatobacterium granulomatis, recently reclassified as Klebsiella granulomatis.24 Although sexually transmissible, granuloma inguinale is only mildly contagious and repeated exposure is necessary to cause disease. Often, individuals are coinfected with syphilis.28
Indigenous granuloma inguinale no longer occurs in the United States (cases that occur are imported).26 Yet in some parts of the world (India, New Guinea, Africa, central Australia, and to a lesser extent the Caribbean and Brazil), granuloma inguinale is among the most prevalent of the present STIs. Incidence of infection is found in tropical and subtropical environments with sustained high temperature and high relative humidity. Infection is usually acquired through sexual intercourse with an individual who has active disease or asymptomatic rectal infection. As with all genital ulcerative diseases, granuloma inguinale plays a role in HIV transmission.24
PATHOPHYSIOLOGY C. granulomatis is a gram-negative, nonsporing, nonmotile, encapsulated rod that is not easily isolated in the laboratory. After exposure the bacteria survive and multiply within vacuoles of large histiocytic cells or polymorphonuclear leukocytes. The bacteria reproduce within these cells until a vacuole may contain 20 to 30 microorganisms. These bacteria-filled vacuoles were identified by Donovan in 1905 and are termed Donovan bodies. The presence of Donovan bodies in tissue smears of material from the lesions is considered the gold standard for diagnosis of lymphogranuloma inguinale.28,29
The initial lesion is an indurated subcutaneous nodule that is often preceded and accompanied by itching. The primary sites for development of the lesions are the distal penis in men and the introitus in women. Single lesions often coalesce with nearby lesions or form new lesions by autoinoculation of nearby skin surfaces. Progression from the initial nodule to a large, granuloma-heaped ulcer occurs slowly. Secondary infection may occur, increasing tissue damage and residual scarring. The disease may spread to the bones, joints, and liver.
CLINICAL MANIFESTATIONS The incubation period of granuloma inguinale is 8 to 80 days. The initial lesion is an indurated, sharply defined, painless, subcutaneous nodule that is often preceded and accompanied by itching. Nodules bleed easily and contain abundant red, beefy-looking granulation tissue. Progression to a large granuloma-heaped ulcer occurs slowly; single lesions coalesce or form new lesions by autoinoculation of nearby skin surfaces. Secondary infection may occur, increasing tissue damage and residual scarring. Although systemic symptoms are rare, the disease may spread to the bones, joints, and liver. In some cases, infection spreads to the inguinale area and produces pseudobuboes. In these instances, the affected lymph nodes are not directly affected, but the surrounding area may be infected and abscessed.
EVALUATION AND TREATMENT Although the clinical manifestations of this disease are important for diagnosis, confirmation involves microscopic examination in which Donovan bodies are found in a smear or biopsy specimen. No FDA-cleared PCR tests for the detection of K. granulomatis DNA exists, but such an assay would be helpful.14
Many antibiotics have been used successfully against K. granulomatis. Because other STIs frequently coexist, individuals should be tested for chlamydia, gonorrhea, syphilis, hepatitis B, and HIV. Because of the indolent nature of the disease, duration of therapy tends to be relatively long. With effective antibiotic treatment, lesions begin to heal in 7 days, but treatment is continued for at least 3 weeks and until all lesions are completely healed. Oral therapy includes doxycycline (100 mg) twice a day, azithromycin (1 g) once a week, ciprofloxacin (750 mg) twice a day, erythromycin base (500 mg) four times a day, or trimethoprim-sulfamethoxazole (160 mg/800 mg, double-strength tablet) twice a day. Relapses can occur 6 to 18 months later despite effective initial therapy, so prolonged follow-up is necessary, as is treatment of sexual partners.
Bacterial Vaginosis
Bacterial vaginosis (BV)—previously called nonspecific vaginitis; nonspecific vaginosis; or Haemophilus, Corynebacterium, or Gardnerella vaginitis—is a sexually associated condition, but is not necessarily considered an STI. Bacterial vaginosis occurs almost exclusively in sexually active women of reproductive age and is uncommon in sexually inexperienced women. Prevalence rates vary from 17% among women in family planning clinics to 37% among some groups of pregnant women.1 Fifty percent of women with signs of BV are asymptomatic.
PATHOPHYSIOLOGY The exact etiology of BV is unknown. Gardnerella vaginalis and various anaerobes, including Mycoplasma hominis, Bacteroides, and Mobiluncus, interact and proliferate when lactobacilli (the normal predominant vaginal flora) are decreased or absent. Bacteria adhere to vaginal epithelium, and massive overgrowth occurs and causes a noninflammatory response. Catabolic enzymes degrade proteins into amines. In turn, amines elevate vaginal pH and produce the characteristic fishy odor associated with BV. BV has been implicated in PID, chorioamnionitis, preterm labor, and postpartum endometritis (Box 24-4). Sexual intercourse is believed to be the primary method of initiating BV, but definitive proof is lacking and the syndrome has been identified in virgins.28,30
CLINICAL MANIFESTATIONS BV is characterized by a thin, gray, homogeneous, and malodorous discharge that adheres to the vaginal walls but is often copious enough to drain into the vulva. Occasionally the discharge is bubbly or frothy. Usually the vaginal pH is 5 to 5.5 and there are no signs of vaginal or cervical inflammation. Individuals often complain of a strong, foul, fishy vaginal odor, particularly after intercourse and during menses. Odor is caused by contact with alkaline secretions, including semen and menstrual discharge. Male partners of infected women may harbor the microorganisms that are responsible for BV but have no signs or symptoms of active disease.
EVALUATION AND TREATMENT Diagnosis of BV can be made based on three of four of the following criteria: (1) presence of adherent gray vaginal discharge, (2) pH greater than 4.5, (3) positive amine odor, and (4) presence of clue cells on wet mount.32 Clue cells are considered pathognomonic for BV. The saline wet mount also may show absence of lactobacilli and few or no leukocytes. Clue cells are vaginal epithelial cells that are covered with bacteria and look as if pepper has been sprinkled on them. When a drop of potassium hydroxide (KOH) solution is added to the slide, a characteristic amine odor is released immediately. Cultures are neither useful nor recommended; however, individuals should be screened for gonorrhea and chlamydia.
The most commonly used treatment for Gardnerella-associated BV is a course of oral metronidazole (Flagyl), 500 mg twice daily for 7 days, or 0.75% vaginal gel once daily for 5 days. Alternative regimens include oral clindamycin (300 mg) twice daily for 7 days or 2% vaginal cream once daily for 7 days. Clindamycin vaginal suppositories have been newly approved for use as a 3-day treatment regimen in nonpregnant women. Clindamycin cream is oil based, and for up to 72 hours after completing therapy, it may weaken latex condoms. BV treatment in women infected with HIV is the same for HIV-negative patients. It is especially important in women who are pregnant, because BV and chorioamnionitis may increase the risk of perinatal transmission of HIV.27 No evidence indicates that treatment of sexual partners reduces recurrence and is not recommended.31
Chlamydial Infections
Chlamydia is the common name for infections caused by Chlamydia trachomatis (CT). C. trachomatis is responsible for a variety of syndromes, including acute urethral syndrome, nongonococcal urethritis (NGU), mucopurulent cervicitis, and PID. Chlamydia, the most common bacterial STI in the United States, affects about 3 million individuals annually5 and is the leading cause of preventable infertility and ectopic pregnancy. In 2007, 1,108,374 cases of chlamydial infections were reported. This is more than three times the number of reported gonorrhea infections. The rate of chlamydia in 2007 was 544 cases per 100,000 population, and has increased for all race/ethnic groups except among Native Americans/Alaskan Natives. This increase probably reflects the continued expansion of screening efforts and increased use of more sensitive diagnostic tests as well as a frank increase in incidence.32 Approximately 75% of women with CT infection are asymptomatic. In addition, C. trachomatis can be recovered from the urethra in 25% to 60% of men with NGU, in 4% to 35% of men with gonorrhea, in 28% of asymptomatic men whose partners have chlamydial cervicitis, and in 0% to 7% of men without urethritis who are seen in STI clinics.
Chlamydia is most common among young (less than 20 years old) heterosexuals who have new or multiple partners, are economically disadvantaged, are entering juvenile detention centers, and have been diagnosed with gonorrhea.5 The incidence of CT infection in pregnancy has been estimated at between 2% and 30%. Age younger than 25 years (with highest rates in women younger than 20 years), a new sexual partner and first pregnancy were strongly and independently associated with infection in a study of more than 7000 pregnant women who were screened for CT at their first prenatal visit. Like gonorrhea, Chlamydia infection is transmitted from mother to infant through the infected birth canal. Estimated rate of transmission ranges from 60% to 70%.33
PATHOPHYSIOLOGY C. trachomatis is an obligate, gram-negative intracellular bacterium that lacks the ability to reproduce independently. Like viruses, Chlamydia can reproduce only within host cells. It is differentiated from other bacteria by its unique two-part growth cycle. The first part consists of an elementary body that is small, resilient, metabolically inert, and able to survive extracellularly. Once this elementary body attaches itself to a receptor host cell, it is able to enter by endocytosis. Once inside the cell, the second part of the cycle begins and the microorganism becomes a metabolically active parasite, reproducing within the cell until the cell is destroyed and ruptures, disseminating up to 1000 new elementary bodies. Rarely does this cause a secondary infection. Infection with C. trachomatis produces a mononuclear inflammatory reaction rather than a polymorphonuclear inflammatory reaction. The former reaction produces permanent scarring of tissues.34
Chlamydia microorganisms are always pathogens; they are not part of the normal flora of the urogenital tract, despite the fact that infection is often asymptomatic. Numerous serotypes, or strains, of C. trachomatis have been identified. Some cause urogenital infection; some, ocular trachoma; and others, lymphogranuloma venereum, which is discussed in the next section.
The strains of C. trachomatis that cause urogenital infection apparently require squamous-columnar and columnar-epithelial cells as hosts. C. trachomatis infects and disrupts epithelial tissues but does not seem to invade or destroy deeper tissues or organs. Urogenital chlamydial infections may have a fairly self-limited acute course followed by a chronic, low-grade, persistent infection that lasts for years.34
In newborns, several sites may be inoculated with Chlamydia during passage through the infected maternal cervix. These include the eye, nasopharynx, rectum, and vagina. The infant also may aspirate infected secretions with its first breaths, resulting in chlamydial pneumonitis and substantial newborn morbidity.
CLINICAL MANIFESTATIONS Asymptomatic chlamydial infection is common. Urogenital infections caused by Chlamydia closely parallel those caused by gonorrhea. Both microorganisms infect superficial genital tract tissues, such as mucosa of the urethra and cervix, and both can invade the epididymides, fallopian tubes, and hepatic capsule. Table 24-2 lists the pathophysiologic similarities of chlamydial and gonococcal infections.
Table 24-2
Similarity of Clinical Syndromes Caused by Chlamydia trachomatis and Neisseria gonorrhoeae
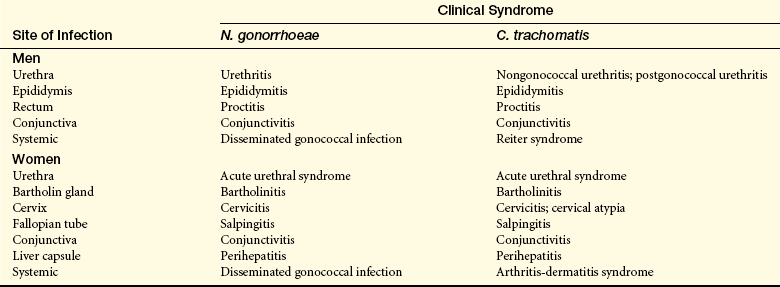
Data from Stamm WE, Holmes KK: Chlamydia trachomatis infections in the adult. In Holmes KK et al, editors: Sexually transmitted diseases, ed 2, New York, 1990, McGraw-Hill.
Chlamydial infection accounts for 50% to 60% of cases of NGU in men. Clinically, urethritis caused by gonorrhea and chlamydia cannot be differentiated: both have a 7- to 21-day incubation period and cause dysuria. Although urethral discharge in men may be similar in the two infections, chlamydial discharge tends to be more clear and gonococcal discharge more purulent. Men might note a clear, mucous discharge on rising in the morning; dry, clear discharge on their underwear; or mild burning with urination. Chlamydial urethritis is generally milder than gonorrheal urethritis and more likely to be asymptomatic. Symptoms may be intermittent or unnoticeable. Gram-stained smears of the urethral discharge show numerous polymorphonuclear leukocytes, which indicates ongoing inflammation. Screening men without symptoms is not cost effective at this time.
Chlamydial epididymitis can accompany chlamydial urethritis and is characterized by fever and a unilaterally painful, swollen scrotum. Chlamydial infection also causes proctitis (rectal inflammation) in homosexual men and occasionally in heterosexual women and is linked to the practice of receptive anal intercourse. Chlamydial proctitis is generally mild, although it may, like gonorrheal proctitis, cause rectal bleeding, mucous discharge, and diarrhea. Reiter syndrome (urethritis, conjunctivitis, arthritis, and characteristic mucocutaneous lesions) is also associated with untreated chlamydial infections of the urogenital tract.
Chlamydia infection is the leading cause of tubal infertility in women. Risk factors for infertility include numbers of chlamydial infections and duration and severity of infection. Even women with asymptomatic salpingitis have a risk of subsequent infertility. This may reflect an antigen-antibody response rather than inflammatory damage.35
In young sexually active women, C. trachomatis is a cause of acute urethral syndrome (dysuria, urinary frequency, and presence of sterile pus in the urine). C. trachomatis also causes asymptomatic urethral infection in women. Chlamydial infection of Bartholin glands can cause purulent discharge and formation of a Bartholin cyst. Women with chlamydial cervicitis may be asymptomatic or may have a yellow mucopurulent discharge from the cervical os and a hypertrophic, edematous, and friable area of cervical ectopy. The woman also may report intermenstrual or postcoital spotting. Although ectopy alone does not indicate a pathologic condition, a raised, erythematous, raw, and friable ectopy is abnormal and strongly suggestive of chlamydial cervicitis (Figure 24-9).
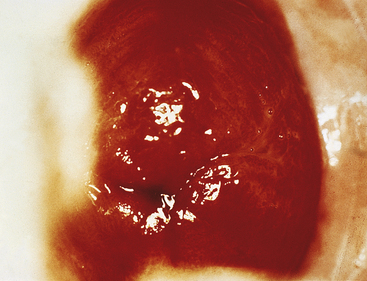
Figure 24-9 Chlamydial cervicitis. Beefy red mucosa of columnar epithelium of cervix. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
The most common clinical manifestations of chlamydial infections in the newborn are conjunctivitis and pneumonia. Like gonococcal infection, prophylactic treatment with antibiotic eye ointment at birth does not provide complete protection against neonatal conjunctivitis and does not protect against neonatal pneumonia. Chlamydial conjunctivitis begins between 5 and 14 days after delivery, when the infant’s eyes begin to water. This discharge may become purulent, and both eyes may become red and swollen (Figure 24-10). Scarring of the conjunctivae may result, but this infection does not cause blindness, as does the ophthalmia neonatorum caused by N. gonorrhoeae. The pneumonia is mild or severe and may accompany the conjunctivitis. Infants with chlamydial pneumonia are seen at 3 to 11 weeks of age with staccato coughing spells, nasal congestion, dyspnea, and minimal fever. Other signs include otitis media, tachypnea, wheezing, bronchospasm, crepitant inspiratory rales, and apneic spells.

Figure 24-10 Chlamydial ophthalmia. (From McMillan A, Scott GR: Sexually transmitted infections, ed 2, London, 2000, Churchill Livingstone.)
EVALUATION AND TREATMENT Methods for diagnosing chlamydial infections include tissue culture techniques, direct chlamydia enzyme immunoassay, fluorescein-labeled monoclonal antibody tests, and DNA probe testing. Currently, tests using chlamydia-specific nucleic acid sequences (LCR, PCR, and DNA) are the most sensitive and cost-effective tests available.33 Concurrent DNA testing for gonorrhea can be done using the same swab.
C. trachomatis is susceptible to inexpensive, readily accessible antibiotics. Treatment includes antibiotic therapy for infected individuals and all sexual contacts; abstinence or use of condoms during treatment is recommended. Azithromycin is given 1 g orally, as a single dose or a 7-day course of oral doxycycline, 100 mg twice daily. Alternative regimens include a 7-day course of oral erythromycin, 500 mg four times a day, or erythromycin E 800 mg four times daily for 7 days. Ofloxicin 300 mg, twice daily or levofloxacin 500 mg once daily for 7 days are also effective alternatives.5 Azithromycin is the drug of choice in pregnancy. Because of the asymptomatic nature of Chlamydia and the potential sequelae of untreated infection, extensive widespread screening is warranted.
Lymphogranuloma Venereum
C. trachomatis (invasive serovars of strains L1, L2, or L3) can cause a chronic STI known as lymphogranuloma venereum (LGV), which may be confused with syphilis, herpes, or chancroid. Although LGV is rare in the United States, it has been endemic in Asia and Africa. The infection is acquired during sexual intercourse or through contact with contaminated exudate from active lesions. Inapparent infections and latent disease are rare.36
PATHOPHYSIOLOGY The strain of C. trachomatis that causes LGV probably penetrates skin and mucous membranes through tiny abrasions. LGV begins as a skin lesion and spreads to genital and rectal lymphatic tissue, where it causes marked inflammation, necrosis, buboes, abscesses of inguinal lymph nodes, and infection of surrounding tissues. Healing occurs by fibrosis after several weeks or months and results in scarring, which damages the lymph nodes and disrupts nodal function. Affected nodes become chronically swollen, hardened, and enlarged. C. trachomatis also spreads systematically through the bloodstream and can enter the CNS.37
CLINICAL MANIFESTATIONS The primary lesion of LGV appears after an incubation period of 5 to 21 days. The lesion is most commonly a herpetiform (multivesicular) ulcer, but it can take various forms. The ulcer generally is asymptomatic and inconspicuous and heals rapidly, leaving no scar. In men the lesion is found most commonly on the penis or scrotum; in women it is found on the vaginal wall, cervix, or labia. Other signs of primary LGV include a large, tender lymphatic nodule or bubo, urethritis, and cervicitis.
The secondary stage of untreated LGV in men is characterized by inflammation and swelling of the lymph nodes. At first the inguinal bubo is a firm, somewhat painful mass. As the bubo gradually enlarges, it becomes very painful, thereby restricting mobility, and deep blue. This color change signals impending rupture of the bubo through the skin. Thick yellow pus may drain from the site for weeks or months. Healing is slow and results in scar formation. Systemic manifestations of secondary LGV include meningitis, pneumonitis, and other major infections. In some cases the bubo does not rupture but rather involutes and becomes firm. Bubo formation is most common in men. In women the inguinal lymph nodes are involved in less than one third of cases.
Anorectal LGV may be caused by direct inoculation during anal intercourse, or it may be a chronic or late manifestation of lymphatic spread from the inguinal area. Most individuals with anorectal LGV are women or homosexual men. Clinical symptoms include multiple ulcerations of the rectal mucosa, chronic inflammation, mucopurulent rectal discharge, and rectovaginal fistulas in women. Individuals may have fever, rectal pain, and tenesmus. Rectal strictures, perirectal abscesses, and anal fissures may develop and are the cause of most of the severe morbidity associated with LGV.
EVALUATION AND TREATMENT Clinical manifestations and laboratory tests are used to diagnose LGV. Tests include the LGV complement-fixation test, isolation of the microorganism in tissue culture, and monoclonal antibody tests. The diagnosis usually is made serologically and by excluding other causes of genital ulcers or inguinal lymphadenopathy. LGV is treated with oral doxycycline, 100 mg twice daily for 21 days. A 21-day course of erythromycin is also effective. Sex partners also should be treated.
Nongonococcal or Nonspecific Urethritis
Nongonococcal urethritis (NGU), also known as nonspecific urethritis, is a nonreportable STI. In student health centers and STI clinics, more than 50% of individuals with urethritis have NGU. The morbidity is equal to or greater than that associated with gonorrhea. Approximately 2 million men are affected each year. Most commonly it affects heterosexual men and men of higher socioeconomic status. NGU may be complicated by epididymitis in heterosexual men younger than 35 years, proctitis in homosexual men, and Reiter syndrome.
PATHOPHYSIOLOGY Nongonococcal urethritis is a syndrome caused by a variety of microbes, including C. trachomatis and Ureaplasma urealyticum. Postgonococcal urethritis occurs in 15% to 35% of men diagnosed with gonorrhea. These men usually have coexistent gonorrheal and chlamydial infection and develop biphasic illness because of the longer incubation period of CT. Chlamydial infections are discussed earlier in this chapter (see p. 935).
C. trachomatis is the most common cause of NGU (15% to 55%). Trichomonas vaginalis and HSV sometimes cause NGU. However, Ureaplasma, U. urealyticum, and possibly Mycoplasma are implicated in as many as one third of the cases of NGU.2 Genital colonization with U. urealyticum occurs with an increasing number of sexual partners. That is, urethral cultures of men with a history of three to five lifetime sexual partners yield U. urealyticum whether those men have urethritis or not. The difference in symptomatology may be the result of infection by different serotypes. Some of the 14 different serotypes of U. urealyticum may be more pathogenic than others—20% to 30% of men with acute urethritis are negative for N. gonorrhoeae, C. trachomatis, and U. urealyticum. Some of these men respond to antibiotic treatment; others experience persistent and recurrent infection. No clear association has been found between NGU and infection caused by herpes simplex virus, trichomonads, cytomegalovirus, and other microorganisms.
CLINICAL MANIFESTATIONS Clinically, NGU infection caused by CT cannot be differentiated from NGU caused by another microbe. In both cases, men present after a 7- to 21-day incubation period with complaints of dysuria and mild to moderate white or clear urethral discharge. Discharge may be absent, and urethral itching may be the only symptom. Asymptomatic infection is common.
EVALUATION AND TREATMENT NGU is a diagnosis of exclusion. Urethral exudate is Gram stained, and an endourethral swab is taken for testing or culture. Urine sediment also may be examined. All individuals who have urethritis should be evaluated for the presence of gonococcal and chlamydial infection. A treatment of a single 1-g oral dose of azithromycin should be initiated as soon as possible after diagnosis. Doxycycline, 100 mg orally twice a day for 7 days, is also effective. Single-dose regimens have the advantage of improved compliance and of directly observed therapy.2
Viral Infections
Genital herpes, which causes blisters (cold sores), is the most common infectious genital ulceration in the United States. In fact, genital infection with HSV is an epidemic in the United States. Genital herpes can be caused by either of the two serotypes of HSV: HSV-1 or HSV-2. Although infections caused by the serotypes are clinically indistinguishable, serologic studies show that more than 80% of initial and 98% of recurrent genital HSV infections are caused by HSV-2.
Herpes simplex virus is not a reportable disease, and any reporting that is done is nonstandardized, so national statistics are not available. However, primary HSV infections are estimated to affect 1 million individuals each year. Recurrent infections are mostly asymptomatic (50% to 70%) and affect an estimated 50 million Americans annually.1 The seroprevalence of HSV-2 is estimated to range from 16% to 20% of the total adult population to 35% to 60% for subgroups, for example, STI clinic patients and black women. The incidence of HSV infection tends to be highest in the teen to young adult age group (12 to 29 years) and in non-white lower socioeconomic groups.2 Infection with HSV is not commonly associated with other STIs, for example, gonorrhea.19
Herpes simplex virus infection is transmitted through intimate contact with a person who is shedding the virus in a secretion or from a peripheral lesion or mucosal surface. Persons without symptoms probably transmit most infections. Transmission rates are not well identified; however, it is estimated that a woman has an 80% to 90% risk of developing genital herpes after being exposed to an infected man. In 1992 Mertz and colleagues38 studied monogamous heterosexual couples in which one partner had HSV-2 infection. The noninfected partner seroconverted in 10% of couples over a 1-year period. As many as 70% of such infections seem to be acquired during periods of asymptomatic shedding. Uninfected female partners were at greater risk than men, especially if they were seronegative for HSV-1 antibodies as well. The likelihood of nonsexual transmission of genital herpes, through aerosolized secretions of other fomites, is quite rare and unlikely.5,34
Neonatal infections can occur in utero or, more commonly, during the intrapartum or postpartum period. The risk of transmission of HSV to the neonate varies from <1% among women with recurrence of known herpes at term who acquired HSV during the pregnancy and up to 30% to 50% in women who are exposed and acquire HSV near term.14 Perinatal transmission can cause extensive morbidity and mortality.
Intrauterine transmission can occur through transplacental or ascending infection and can cause spontaneous abortion or premature delivery.19 Most infections are transmitted intrapartally. Infants are at greatest risk if the mother has a primary infection acquired near the time of delivery rather than a recurrent infection or an infection acquired during the first half of pregnancy. Ruptured membranes have a role in the development of HSV. Membranes that have been ruptured for more than 4 hours increase the risk for contracting HSV. Internal fetal monitoring devices also increase the risk of the infant contracting HSV.39
PATHOPHYSIOLOGY After initial exposure and entry of the virus at mucocutaneous sites or abraded skin, the virus undergoes replication locally in the dermis and epidermis. This leads to cell destruction, transudation, and vesicle formation. The virus spreads to contiguous cells and eventually into sensory nerves. Eventually the virus is transported intra-axonally to the dorsal root, where it remains in a latent stage until it becomes reactivated. During the latent period the genome for the virus is maintained in the host cell nucleus without causing the death of the cell. After oral infection the latent virus resides in the trigeminal ganglion; after genital infection it resides in the dorsal sacral nerve roots.
Latent infections can become reactivated and cause a recurrent infection with similar manifestations. Reactivation of the HSV-2 infection is twice as common as HSV-1 infections, and the likelihood of HSV-2 recurrent infections is 8 to 10 times. Reactivation of HSV is not well understood but may be attributable to physical, hormonal, and immunologic stimuli. Other triggering events may be menstruation, stress, and sun exposure.33 During reactivation the viral genomes are transported through the peripheral sensory nerves back to the dermal surface.
CLINICAL MANIFESTATIONS Three distinct syndromes associated with HSV infection are first-episode primary genital infection, first-episode nonprimary HSV, and recurrent infections. The manifestations of each one depend on the individual’s previous immune state. First-episode primary genital infection occurs when an individual has no antibodies to HSV-1 or HSV-2. Up to 60% of primary infections with HSV-2 and one third of primary infections with HSV-1 are asymptomatic.40 If symptoms occur, the individual may have small (1 to 2 mm), multiple, vesicular lesions that are generally located on the labia minora, fourchette, or penis (Figure 24-11). They also may appear on the cervix, buttocks, and thighs and are often painful and pruritic. These lesions usually last about 10 to 20 days. The lesions of HSV-1 and HSV-2 are indistinguishable to the naked eye. These wet lesions actively shed virus for about 10 to 14 days, after which they heal by reepithelialization. Small lesions may coalesce into larger ulcers and become secondarily infected.

Figure 24-11 Herpes lesions. A, Herpetic vesicles on the penis. B, Herpetic ulceration of the vulva. (From McMillan A, Scott GR: Sexually transmitted infections, ed 2, London, 2000, Churchill Livingstone.)
Systemic manifestations often accompany primary HSV infection, and an individual may experience fever, malaise, myalgias, lymphadenopathy, and urinary retention. Pharyngitis, aseptic meningitis, and hepatitis also may accompany primary HSV infection. Figure 24-12 illustrates the clinical course of primary genital HSV.
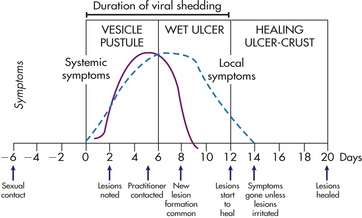
Figure 24-12 Clinical course of primary genital herpes. (From Corey L: Genital herpes. In Holmes KK et al, editors: Sexually transmitted diseases, ed 2, New York, 1990, McGraw-Hill.)
First-episode nonprimary HSV occurs in individuals who have preexisting antibodies. In some individuals the primary infection may not have had any clinical manifestations. The HSV becomes latent within the nerve root and is reactivated at a later date. Compared with primary infection, the first episode of nonprimary HSV is often milder with fewer lesions that are less painful and heal faster. Fewer systemic manifestations occur and viral shedding is of shorter duration.
Recurrent infections produce mild local symptoms. The number of lesions is greatly reduced, and the lesions are less painful. Lesions are often unilateral, with crusting within 4 to 5 days. Recovery and healing are usually complete within 10 days.41 Asymptomatic viral shedding can occur with both HSV-1 and HSV-2.
Individuals affected with HSV-2 are more likely to experience recurrent infections. Recurrent infections occur an average of five to eight times per year but may be as frequent as every month or as rare as every few to many years. Individuals may experience prodromal symptoms (e.g., pruritus, tingling, dysesthesias) a few hours to 2 days before the eruption of lesions. Women may experience a vaginal discharge and dysuria, and 44% of men have dysuria. Symptomatic HSV infection of the newborn may occur any time in the first month of life. Manifestations range from a local infection of the eyes, skin, or mucous membranes to a severe disseminated infection with CNS involvement. About 70% of affected infants present with skin lesions. CNS involvement includes seizures and is associated with a mortality of more than 50% and extensive neurologic sequelae in survivors.
EVALUATION AND TREATMENT Genital HSV infection is suggested if typical genital lesions are present. A presumptive diagnosis of HSV-associated infection is supported by the identification in a Papanicolaou (Pap) test of multinucleated giant cells with intranuclear inclusions. Definitive diagnosis is made after viral tissue culture. HSV-1 and HSV-2 are distinguished by fluorescent antibody, neutralization, or serologic tests. Serologic testing may be useful in identifying symptomatic carriers of HSV, for use in discordant couples and to screen pregnant women.
No curative treatment for HSV infection is known. A vaccine is in development but is only effective in women who have not been infected with HSV-1; however, it is not yet available.42 Oral acyclovir, valacyclovir, penciclovir, and famciclovir are used for primary and periodic outbreaks and to prevent recurrences. Neither valacyclovir nor famciclovir is approved by the U.S. Food and Drug Administration for use in children younger than 12 years.4 Intravenous acyclovir is reserved for severely immunocompromised individuals.43 Acyclovir-resistant strains of HSV have been identified periodically; no specific definitive resistant strains are known to exist. Suppressive treatment is recommended for individuals with more than six recurrences per year. Suppressive treatment also may reduce asymptomatic viral shedding. Although condoms offer some protection, individuals with HSV should refrain from all genital contact when symptomatic and understand that an undetermined risk of transmission exists even during asymptomatic periods.
Human Papillomavirus Infection
Human papillomavirus (HPV) infection is the most common symptomatic viral STI in the United States. Although more than 5.5 million cases are diagnosed yearly, prevalence is considered underestimated because HPV infection is often subclinical. More sensitive measures of HPV indicate that 57% to 60% of all sexually active young women are infected with the virus. Currently the incidence of HPV is at epidemic proportions; an estimated 75% of the reproductive-age population has been infected with HPV.1
More than 120 different types of HPV have been identified. More than 30 serotypes are unique to the stratified squamous epitheliums of the genital area. These are divided into serotypes that have a high risk of causing cervical cancer and low-risk serotypes, which are associated with benign lesions: condylomata acuminata of the vulva, vagina, penis, and perianal areas. High-risk types 16 and 18 are the most common, found in more than half of cases of cervical dysplasia.44 High-risk type 18 is associated with adenocarcinoma of the cervix.44 Serotypes associated with genital warts include types 6 and 11, among others. These lesions can coexist with the high-risk types but do not cause cancer. Although rare, these types also may cause oral lesions. It is now known that infection with persistent, high-risk serotypes of HPV are necessary for the development of cervical cancer (see also Chapters 11 and 23). Fortunately, most cases of HPV are transient and resolve by 2 years.44 Persistence of the virus, immune response, and the presence of cofactors, including smoking and hormonal contraceptive exposure, may play a role in the development of cervical dysplasia and cancer following HPV exposure.45 HPV infection is closely associated with multiple sexual partners and early onset of sexual activity and is most common in teens and young adults, 16 to 25 years of age.
Genital warts are quite contagious, with transmission rates among individuals estimated to be between 38% and 95%. Such a wide range is attributable to the subclinical nature of some infections and various influencing factors that include number of exposures, HPV type, location of lesions, and cellular immunity response. Infants and children also have been identified as being infected with HPV. Infants can be infected in utero and by passage through an infected birth canal. HPV infection in children has been traced to child sexual abuse; however, reports vary in making this connection.4,46
PATHOPHYSIOLOGY HPV is a nonenveloped, circular, double-stranded DNA virus, one of the papovaviruses, that belongs to the Papovaviridae family.47 Information about HPV was not readily available until the late 1970s, when it became possible to clone the viral genomes directly from infected tissues by recombinant DNA technology.48
Transmission of the virus is believed to occur through sexual contact; however, the exact transmissibility of the virus into the cell is unknown. The initial infection follows trauma to the epithelium that allows the virus to reach and infect the basal cells of the epithelium, which appear to be supportive of viral propagation. Such minor trauma may occur during sexual intercourse. Epithelial cells that are infected with HPV undergo transformation, proliferate, and form a warty growth. HPV manifestations appear in about 2 to 3 months.
CLINICAL MANIFESTATIONS Condylomata acuminata are soft, skin-colored, whitish pink to reddish brown discrete growths. They may occur singly or in clusters and may be broad based or pedunculated and feathery or smooth (Figure 24-13). Sometimes the warts enlarge to form cauliflower-like masses on the male frenulum, glans, foreskin, urinary meatus, shaft, scrotum, or anus and on the female labia, clitoris, perineum, vagina, or anus (Figure 24-14). Although the lesions are usually not painful, they may cause dyspareunia (painful intercourse) and may be friable and bleed easily. Some individuals complain of pruritus. Cervical lesions are generally flattened and may not be seen easily without colposcopy.16 Urethral condylomata may occur in men, are always preceded by skin lesions, and can become cancerous.49 Ninety percent of lesions are found in the distal urethra.

Figure 24-13 Condylomata acuminata—penile. Asymptomatic, flesh-colored papules are present on the shaft of the penis. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)

Figure 24-14 Condylomata acuminata—vulva and perineum. The clinical diagnosis was giant condylomata of Buschke and Löwenstein. Such large and confluent lesions should be carefully examined and multiple biopsies obtained to rule out underlying malignancy. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
Laryngeal papillomas can occur in infants whose mothers had genital warts at the time of delivery. Clinical manifestations of laryngeal warts include stridor, hoarseness, abnormal cry, cough, and respiratory distress.50 Many women with HPV may develop cytologic changes detected by Pap testing. These cell changes may be transient or may progress to dysplasia and, ultimately, cancer.
EVALUATION AND TREATMENT Generally, diagnosis of condylomata acuminata is made on the basis of clinical manifestations. Verrucose, fleshy pink lesions caused by HPV must be differentiated from condylomata lata (the whitish gray, flat lesions) of secondary syphilis. Because HPV infection often accompanies other STIs, gonorrhea culture, chlamydia culture, serologic test for syphilis, and wet mount for other vaginal microorganisms also should be performed.
HPV infection is associated with the development of squamous cell carcinoma; therefore, all atypical or persistent lesions should have a biopsy examination. HPV testing can be useful in the triage of abnormal Pap tests or can be used in conjunction with Pap testing to identify women at risk for the development of cervical dysplasia.
Treatments for external genital warts are considered cosmetic—not curative—and include patient-applied therapies (podofilox and imiquimod) and provider-administered therapies (cryotherapy, podophyllin resin, trichloroacetic acid [TCA], bichloroacetic acid [BCA], interferon, and surgery). Cervical and extensive vaginal lesions may be treated with 5-fluorouracil cream or surgical excision with CO2 laser surgery, cryosurgery, or electrosurgery. Interferons that have general antiviral, antiproliferative, and immunomodulating effects have been used successfully in treating stubborn genital warts. Success of treatment depends on response of the immune system. Approximately one third of individuals experience a cure, and another one third experience a decrease in wart size.19 Surgical excision is the treatment for laryngeal warts in infants. A vaccine against HPV serotypes 16 and 18 is available and has shown to be effective in prevention of primary cervical infection with those strains, which are associated with cervical cancer51 (Table 24-3 and see What’s New? HPV Vaccine; also see Chapter 23 What’s New? Pap Test for Cervical Screening Obsolete?).
Table 24-3
Recent Recommendations for Cervical Cancer Screening
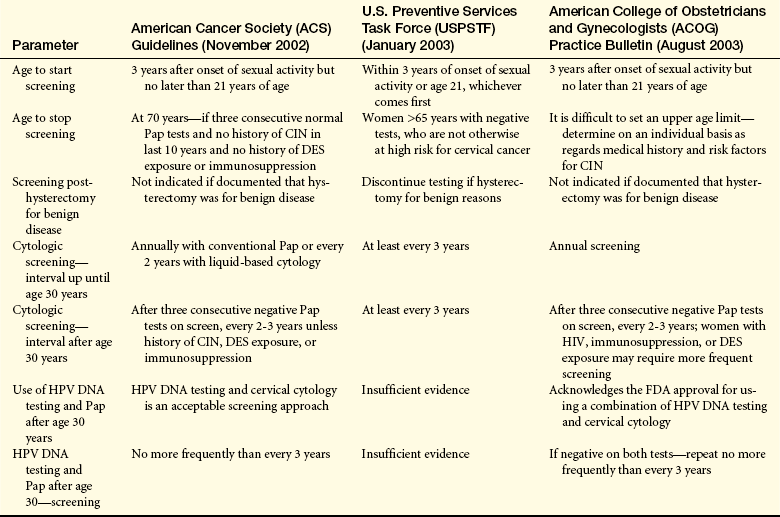
CIN, Cervical intraepithelial neoplasia; DES, diethylstilbestrol; DNA, deoxyribonucleic acid; FDA, Food and Drug Administration; HPV, human papillomavirus; Pap, Papanicolaou.
Data from American College of Obstetricians and Gynecologists (ACOG): Int J Gynaecol Obstet 83(2):237-247, 2003; Saslow D et al: CA Cancer J Clin 52:342-362, 2002 (available at: http://caonline.amcancersoc.org/cgi/content/full/52/6/342); US Preventive Services Task Force (USPSTF): Screening for cervical cancer, January 2003 (available at: htp//www/ahcpr.gov/clinic/uspstf/uspscerv.htm; also see http://www.acog.org/from_home/publications/press_releases/nr07-31-03.cfm
Molluscum Contagiosum
Molluscum contagiosum is a benign viral infection of the skin in children and adults. Primarily the face, hands, lower abdomen, and genitalia are affected; papules found on other parts of the skin or widely distributed are not uncommon. Individuals with AIDS may develop extensive lesions over the face, neck, and genital region.
Molluscum contagiosum occurs throughout the world and has been a common childhood disease in Papua New Guinea and Fiji. It is much less common in the United States, where incidence is highest among young adults. The childhood disease is transmitted by skin-to-skin contact and fomites (swimming pools, towels, gymnasium equipment) and affects the face, trunk, and limbs. Adult disease is more commonly sexually transmitted and affects the lower abdomen, genitalia, and perianal area.52 Molluscum contagiosum is most common in men 20 to 29 years of age and in those with multiple sexual partners. The molluscum contagiosum virus is taken into epithelial cells by phagocytosis and replicates within the cytoplasm, where it produces cytoplasmic inclusions (molluscous bodies) and cellular hyperplasia. The underlying skin usually is not affected.53
After an incubation period of 2 to 7 weeks, white or flesh-colored, round or oval dome-shaped papules appear. The lesions are relatively small (3 to 5 mm) but occasionally may coalesce to form larger lesions up to 15 mm. The surface has a characteristic central umbilication, from which a thick, creamy core material can be expressed (Figure 24-15). Generally the lesions are not painful or pruritic unless secondarily infected. The papules may last several months or several years and spread by autoinoculation.

Figure 24-15 Molluscum contagiosum. Flesh-colored papules of molluscum may be distinguished by their umbilicated centers. The papules contain a white cheesy substance that may be stained for the presence of viral inclusion bodies. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
The appearance of the lesions is generally all that is needed to make the diagnosis, although direct microscopic examination of stained material from the core of the papule discloses molluscous bodies within the swollen and rounded epithelial cells. The lesions often heal spontaneously after several months. Other effective means of removing the lesions include curettage and application of liquid nitrogen (cryotherapy) or silver nitrate. Topical acids have been used also but cause scarring. Individuals tend to have lifetime immunity once lesions are healed completely.
Parasitic Infections
Originally discovered in 1836, T. vaginalis was at first thought to be a harmless commensal microorganism. T. vaginalis is now known to be a common cause of sexually transmitted lower genital tract infection and urethritis.
Because trichomoniasis (infection by T. vaginalis) is not a reportable disease, its prevalence can only be estimated. The latest estimates suggest that as many as 5 million cases of trichomoniasis occur each year in the United States,1 and that T. vaginalis accounts for one of four cases of infectious vaginitis. Trichomoniasis is usually found in both sexual partners and often coexists with gonorrhea. Although sexual transmission is clearly the most common means of disease spread, transmission through fomites is theoretically possible. To cause infection, the fomite would have to introduce an inoculum of about 10,000 microorganisms directly into the vagina.54
PATHOPHYSIOLOGY T. vaginalis is an anaerobic, unicellular, flagellated, parasitic protozoan that adheres to and damages squamous epithelial cells. Because this protozoan selectively affects squamous epithelia, vaginal and urethral tissue is often infected, as are Skene and Bartholin glands. The endocervical canal is not affected because it is lined with columnar epithelium. In men the urethra is the most common site of infection, although the protozoa, called trichomonads, also can infect the epididymis and (rarely) the prostate. Zinc, which has potent antibacterial properties, is found in high concentrations in the prostate. Hence many trichomonads are cleared from the male urethra during ejaculation. This action makes urethral trichomoniasis a fairly self-limiting infection in men. Most infections of the male urethra clear up within 2 weeks.
Trichomoniasis is most common in men and women of reproductive age, and it is primarily an infection of the vagina. T. vaginalis can induce a marked inflammatory response in the vagina, causing a copious discharge that contains large numbers of polymorphonuclear neutrophils. Trichomonads adhere to but do not invade the squamous epithelial cells.
CLINICAL MANIFESTATIONS Manifestations of vaginal trichomoniasis range from none to severe, with some women reporting an increase in distressing symptoms immediately after menses. Vaginal discharge and internal pruritus are the most common complaints. Dyspareunia and dysuria are also fairly common. Secretions are usually copious, frothy, malodorous, and yellow-green to a gray-green. The vaginal walls may appear erythematous and sore. Rarely, small, punctate red marks, sometimes called strawberry spots, are visible. Vaginal pH is usually more than 4.2.
Most men with trichomoniasis remain asymptomatic. Possible clinical manifestations include scant intermittent discharge, slight pruritus, and mild dysuria.
EVALUATION AND TREATMENT History and symptoms are inadequate for diagnosis of trichomoniasis. Fresh secretions have a pH higher than 4.7 and a positive amine odor when mixed with 10% KOH (positive “whiff test”).
Microscopic confirmation of the presence of the trichomonads in vaginal secretions or urine provides a definitive diagnosis. In a fresh wet mount preparation that has been warmed slightly, the epithelial cells have relatively clean and sharp edges, the ratio of polymorphonuclear leukocytes to epithelial cells exceeds 1:1, and the trichomonads are visible. The ovoid microorganism is slightly larger than a polymorphonuclear leukocyte and has one rounded, flagellated end and one slightly pointed, flagellated end. The flagella give the trichomonads their characteristic twisting motility. In an acidic environment, such as urine, the trichomonads assume a “balled-up” or spherical shape and become less motile.
The treatment of choice for trichomoniasis is a single dose of metronidazole (Flagyl). The single-dose therapy is effective, has few side effects, and obviates the need for individual compliance with longer regimens. Sexual partners, even if asymptomatic, also are treated and examined for coexisting STIs. The 2-g single dose of metronidazole can be used to treat pregnant women. However, lactating women should suspend breast-feeding for 24 hours after single-dose therapy.55
Scabies
Scabies is a rather benign, common parasitic infection that can be spread by skin-to-skin and sexual contact. Discovered by Bonomo in 1687, it is considered to be the first human disease with a known cause.56
Scabies has a worldwide distribution, but actual prevalence is unknown.24 Traditionally the disease was attributed to conditions of poverty, overcrowding, uncleanliness, and sexual promiscuity. Today it is recognized that scabies occurs in individuals with good personal hygiene and is not limited to any social class. Outbreaks of scabies occur every 30 years or so and last about 15 years. The most recent outbreak in the United States began in 1971 and subsided in the 1980s.
Transmission of scabies requires prolonged close skin-to-skin contact, which typically occurs within families or between sexual partners. Nonsexual transmission from patient to nurse has been reported in hospitals during sponge baths and lotion application, and mites have been transferred through infested bedding, clothes, and other fomites.5
PATHOPHYSIOLOGY The adult female itch mite, Sarcoptes scabiei, is 0.3 to 0.4 mm long and has a life span of about 30 days. Once deposited on human skin, it burrows through the horny layer of the stratum granulosum. Within hours of burrowing, the female begins laying two or three large eggs per day, each of which progresses through larval and nymphal stages to become an adult itch mite in about 10 days. The most common places for scabies to burrow are on the hands (between the fingers) and on the flexor surfaces of the wrists and the extensor surfaces of the elbows. Characteristic lesions may occur on the nipples of women and as pruritic papules on the penile shaft and glans and on the scrotum.52,57 Pruritic papules may be seen on the buttocks also.57 Figure 24-16 shows the typical sites of scabies burrows.
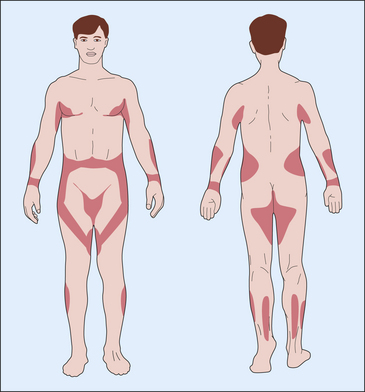
Figure 24-16 Distribution of skin lesions of Sarcoptes scabiei infestation. Unshaded areas are rarely affected in healthy adults. (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
CLINICAL MANIFESTATIONS The classic symptom of scabies is intense pruritus, which may be pronounced at night. The typical burrow of the S. scabiei is a short, linear, curved, or S-shaped line (Figure 24-17). There may be small, erythematous, excoriated larval papules near the burrows. Secondary infections are common and are caused by scratching. In some individuals a hypersensitivity reaction occurs a month or more after the infestation and causes multiple, reddish brown, pruritic nodules to develop on the covered portions of the body—most commonly, the upper thighs, buttocks, male genitalia, and axillary regions. These nodules may persist for more than 1 year despite treatment with a scabicide.

Figure 24-17 Scabies burrow. An S-shaped burrow with a tiny vesicle at one end. (From Habif TP et al: Skin disease: diagnosis and treatment, St Louis, 2001, Mosby.)
EVALUATION AND TREATMENT Although the diagnosis is often made on clinical grounds, microscopic identification of the mite or its eggs, larvae, or feces is recommended because the symptoms of scabies can imitate those of many other dermatologic conditions. Superficial scrapings from a recently developed unexcoriated papule or burrow can be observed easily under the microscope; the addition of KOH allows easier visualization of the mite.
Preferred treatment is topical application of 5% permethrin massaged and left for 8 to 14 hours. Also effective is Lindane (1%) lotion or cream applied thinly to all areas of the body below the neck and washed thoroughly at 8 hours and 10% crotamiton applied to the body below the neck nightly for 2 nights and washed thoroughly 24 hours after the second application.55,57 Close household and sexual contacts should be treated also. Permethrin has been used safely in infants as young as 2 months and is the treatment of choice for children. Pregnant women should be treated with permethrin only if infestation with scabies can be documented.55,57 To prevent reinfestation, clothing and bed linens should be machine washed and dried at high temperatures, or dry-cleaned.
Pediculosis Pubis
Phthirus pubis, the crab louse, is one of three species of lice that infest humans. P. pubis is commonly transmitted sexually and causes pediculosis pubis, or “crabs.” Adolescents and young children are most commonly infected.
P. pubis is transmitted primarily by intimate sexual contact or contact with infected bed linens or clothing. It is highly contagious; there is a 95% chance of contracting the disease during a single sexual encounter. The transfer of lice from pubic hair is probably mechanical, assisted by animated scratching; fingernails; towels; and other similar means rather than by self-propulsion. Pubic lice usually infect the perineal and axillary hair and occasionally the hair of the trunk, beard, scalp, and eyelashes.
PATHOPHYSIOLOGY The crab louse has a 25- to 30-day life cycle from egg to egg that consists of five stages: an egg (or nit) stage, three nymphal stages, and an adult stage, all of which occur in the host. The nits of crab lice are found “glued” to hairs; they are oval, 0.8 by 0.3 mm, and whitish, and they hatch in 5 to 10 days (Figure 24-18). In the adult stage, pubic lice are grayish, are approximately 1 mm in length, and have a segmented body and claws particularly designed for clinging to pubic hairs. Because lice depend on blood for nutrition, they bite into the skin to obtain food.
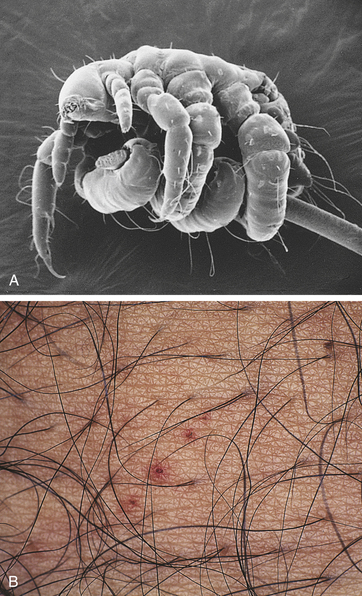
Figure 24-18 Pubic louse and crab louse. A, Pubic louse (Phthirus pubis) encircling a pubic hair; the clawlike legs produce a firm grip. B, Crab louse bites (P. pubis). (From Morse SA et al, editors: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
CLINICAL MANIFESTATIONS Symptoms range from mild pruritus to severe, intolerable itching, depending on the individual’s sensitivity to louse bites. Allergic sensitization occurs in about 5 days, when itching, erythema, and inflammation may worsen. Excessive scratching may lead to secondary infection.
EVALUATION AND TREATMENT The individual’s history usually discloses a recent exposure and the typical symptoms of infestation. Because the lice and nits are visible to the naked eye, a thorough clinical examination permits definitive diagnosis. Pediculosis pubis is treated with 1% permethrin cream rinse or 1% lindane lotion, cream, or shampoo or with over-the-counter pyrethrin or piperonyl butoxide. The pediculicide is applied to infested and adjacent hairy areas and removed after a specified length of time by thorough washing. Remaining nits can be removed with a fine-toothed comb. Permethrin is recommended for young children and pregnant women and has less potential toxicity with inappropriate use. On the other hand, lindane is the least expensive and nontoxic if used correctly. Lindane should not be used after a bath, or by persons with extensive dermatitis, by pregnant or lactating women, or by children less than 2 years of age.55 Sexual contacts and any other intimate household contacts also should be examined and treated, and clothing and bed linens should be dry-cleaned or machine washed and dried at high temperatures. Treatment can be repeated in 7 days to eradicate any newly hatched lice.
SEXUALLY TRANSMITTED INFECTIONS OF OTHER BODY SYSTEMS
Shigellosis and Campylobacter Enteritis
A variety of enteric bacterial pathogens are now recognized as being sexually transmitted, particularly among homosexual men. The bacteria most commonly involved include species of Shigella and Campylobacter. Shigella infection, termed shigellosis, is transmitted by contact with infected feces. Few microorganisms are needed to cause infection. Anal-oral spread occurs easily through household contact and anal-oral sexual practices. Campylobacter jejuni, which causes Campylobacter enteritis, is primarily an animal pathogen but also may be transmitted among humans through anal-oral sexual practices. Again, few microorganisms are necessary for inoculation and infection.
PATHOPHYSIOLOGY Shigella microorganisms are nonmotile gram-negative rods that are related to Escherichia coli. They invade and kill intestinal epithelial cells, thereby inducing a marked inflammatory response and diarrhea. Campylobacter microorganisms are highly motile, curved gram-negative rods that also invade and kill intestinal cells and cause bloody, inflammatory exudate and diarrhea.
CLINICAL MANIFESTATIONS Either microorganism may cause a mild self-limited gastroenteritis or severe dysentery. After a 24- to 48-hour incubation period, shigellosis begins with fever, abdominal distress, and diarrhea. It may resolve completely or progress to dysentery with severe cramping, abdominal pain, tenesmus, and bloody mucoid discharge from the rectum. Campylobacter enteritis typically begins, after a 1- to 7-day incubation period, with sudden fever and abdominal pain followed by diarrhea. Malaise, anorexia, headache, arthralgia, and myalgia are common.
EVALUATION AND TREATMENT Clinical manifestations and cultures of fresh stool samples are used to diagnose shigellosis. Culturing Campylobacter is expensive; therefore, microscopic analysis of a Gram-stained smear of rectal exudate may be used as a diagnostic aid.
Treatment for mild illness includes correction of fluid and electrolyte imbalance. Antidiarrheals are avoided because they may delay clearance of the microorganism. Because Shigella and Campylobacter are highly contagious, antibiotic treatment may be advisable even for mild cases. The preferred treatment for shigellosis is oral ciprofloxacin, 500 mg, twice daily for 3 days. However, susceptibility testing of a stool culture should be performed because of an increasing number of antibiotic-resistant strains of Shigella. Oral ciprofloxacin, 500 mg twice daily for 3 to 5 days, or erythromycin, 500 mg four times daily for 5 days, is effective against Campylobacter enteritis.55 Sexual partners are examined and treated, and individuals are instructed to avoid anal-oral contact until the infection is cured.
Giardiasis and Amebiasis
Two enteric protozoa that are sexually transmitted, primarily among homosexual men, are Giardia lamblia, the cause of giardiasis, and Entamoeba histolytica, the cause of amebiasis. The incidence of these infections in the male homosexual population has decreased over the past years, presumably because of safer sex practices.58 Although the principal route of transmission is contaminated drinking water, giardiasis and amebiasis are transmitted also by anal-oral or genital-anal contact.
PATHOPHYSIOLOGY G. lamblia and E. histolytica are parasites having two forms, cysts and trophozoites (uncysted protozoa). The cysts are the infective form because they can survive in moist environments outside the host. Giardiasis commonly begins with ingestion of a small number of G. lamblia cysts. Once in the upper small bowel, each cyst becomes a trophozoite, which multiplies and attaches to the bowel mucosa. Enzyme deficiencies, inflammation, and immunologic damage then apparently occur, resulting in intestinal malabsorption. Amebiasis begins similarly: the ingested cysts pass to the small or large bowel, where each returns to the trophozoite state, multiplies quickly, and begins to invade the mucosa through cytotoxic activity. Mucosal invasion results in the development of ulcers and an inflammatory response. Individuals infected with E. histolytica may excrete up to 45 million cysts per day.
CLINICAL MANIFESTATIONS Giardiasis begins with sudden, explosive diarrhea, distention, and flatulence. Upper gastrointestinal symptoms are also prominent and may include epigastric pain; vomiting; foul, sulfuric burping; and nausea. After the acute illness, which usually lasts several days, milder symptoms may persist for months, with evidence of malabsorption and weight loss. Amebiasis is often asymptomatic. Symptoms that do occur range from mild diarrhea to severe dysentery. Amebiasis may spread from the intestine to other organs, such as the liver.
EVALUATION AND TREATMENT Diagnosis of both entities usually is made by history and microscopic examination of fresh stool specimens for either trophozoites or cysts. Small bowel biopsy may aid in the diagnosis of giardiasis; rectal biopsy may aid in the diagnosis of amebiasis. Serologic testing is useful in the differential diagnosis of symptomatic individuals with amebiasis. Metronidazole is the treatment of choice in the United States, usually 250 mg three times daily for 5 to 7 days.59 Other nitroimidazoles as well as other agents including quinacrine are also effective. The dosage of metronidazole for amebiasis depends on the severity of the infection.55
Hepatitis B
Hepatitis is a liver infection that can be caused by six types of viruses: hepatitis A, hepatitis B, hepatitis C, hepatitis D, hepatitis E, and hepatitis G. Each virus causes a syndrome of acute, icteric (jaundice-producing) liver inflammation. Of the three types, the hepatitis B virus (HBV) is known to be sexually transmitted. (Hepatitis A, like most other predominantly enteric infections, may be considered an STI because of anal-oral transmission.) Although hepatitis C (HCV) is not recognized as an STI, the CDC has listed sexual exposure as an HCV risk factor (Figure 24-19). Data indicate sexual transmission of HCV appears to occur, but the virus is inefficiently spread through this manner.14 Additional information about hepatitis is found in Chapter 39.
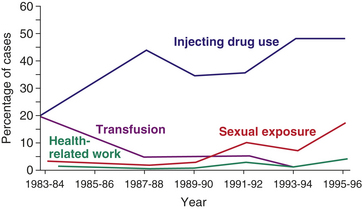
Figure 24-19 Risk for hepatitis C exposure. Comparison of injecting drug use (blue), transfusions (purple), health-related work (green), and sexual exposure (red). Note the rise in sexually transmitted incidences. (From Centers for Disease Control and Prevention: Hepatitis C: what clinicians and other health professionals need to know, 2000. Available at www.cdc.gov/ncidod/diseases/hepatitis/c_training/edu/intro.)
The prevalence of HBV infection varies dramatically worldwide. In Southeast Asia and Africa, 60% to 80% of the population may harbor serologic evidence of past or current infection. In the United States, approximately 5% to 20% of the general population has evidence of HBV infection. Seropositivity generally increases with age. Serologic tests of STI clinic patients show evidence of past infection in 28% of individuals ages 25 years and older and 7% in those younger than 25 years.55 At risk for HBV infection are those with low socioeconomic status, blacks, Indochinese refugees, healthcare workers, and male homosexuals. In groups of male homosexuals, the seropositivity rates may be as high as 80%. Other groups at risk are intravenous drug users, institutionalized mentally retarded persons, hemodialysis patients, and heterosexual partners of HBV carriers.60
Transmission of HBV can occur through needle puncture, blood transfusion, cuts or abrasions in the skin, and absorption by mucosal surfaces. Direct contact with infected body fluids, such as tears, cerebrospinal fluid, synovial fluid, gastric juices, pleural fluid, semen, and urine, may pass the infection. Fomites also can transmit hepatitis: HBV can survive on inanimate objects for up to 1 week.61
Perinatal transmission of HBV is relatively common. Neonates whose mothers are infectious have a 90% chance of becoming infected with HBV during labor or delivery; almost all become chronic carriers.62,63 HBV can be found in maternal vaginal secretions, blood, amniotic fluid, saliva, and breast milk.61
Hepatitis delta agent is a defective virus that is similar to HBV antigen but cannot cause hepatitis B by itself, requiring the presence of HBV to cause hepatitis. Hepatitis delta infection is rare in the United States, but cases have been documented in intravenous drug users and their sexual contacts and in recipients of contaminated blood. It commonly is found in homosexuals, persons requiring kidney dialysis, and healthcare workers.
PATHOPHYSIOLOGY After exposure, HBV passes through the bloodstream to the liver, where it infects liver cells and multiplies. The infection is usually self-limiting, with most patients mounting an effective immune response. Approximately 6% to 10% of infected individuals cannot eradicate the virus and become chronic carriers of HBV.
CLINICAL MANIFESTATIONS Most HBV infections are clinically unapparent and result in solid and permanent immunity. Symptoms of hepatitis usually develop only after a certain HBV antigen has been circulating in the blood for 3 to 6 weeks. Approximately 15% to 20% of individuals develop a prodromal syndrome that is similar to serum sickness. This syndrome is characterized by an erythematous rash, urticaria, polyarthralgias, and arthritis. Symptoms of infection also may include lassitude, anorexia, nausea, vomiting, headache, fever, dark urine, jaundice, and moderate liver enlargement with tenderness. Long-term sequelae include chronic persistent and chronic active hepatitis, cirrhosis, hepatocellular carcinoma, hepatic failure, and death. In neonates who contract HBV, the disease may be manifested in many ways, from mild illness to a severe, fulminant infection with a mortality of 75%.
EVALUATION AND TREATMENT HBV infection is clinically indistinguishable from other types of hepatitis. Diagnosis can be made only through serologic testing.
No specific therapy exists for HBV infection in adults. Treatment consists of supportive care and relief of symptoms. Vaccinations of only high-risk groups has proven to be ineffective. Thus a comprehensive strategy to eliminate HBV and its sequelae has been implemented by the CDC. This involves testing of all pregnant women and vaccinations of susceptible infants, children, and high-risk adults.64
The infant who is born to a mother with infectious HBV is given HBV immunoglobulin and HBV vaccine within 12 hours of birth. The HBV vaccine is administered again at 1 and 6 months if serologic tests show that a chronic carrier state has not developed.
Systemic Diseases
Recent investigations have indicated that the Epstein-Barr virus (EBV), which is transmitted orally, is also capable of being harbored within the male and female genital tracts and transmitted sexually. Further research is needed to specifically identify the role that EBV plays in STIs; however, the significance of EBV infection of the genital tract relates to its ability to transform cells and potentially contribute to the development of cancers in the genital tract.65
Acquired Immunodeficiency Syndrome
Epidemiology, modes of transmission, pathophysiology, clinical manifestations, and evaluation and treatment of AIDS are discussed in detail in Chapter 9.
Cytomegalovirus Infection
Cytomegalovirus (CMV) is a sexually transmissible herpesvirus. It is associated with a number of clinical syndromes in newborns, otherwise healthy adults, and immunosuppressed individuals.
CMV infection causes no specific genital disease, but its incidence is high in individuals being treated for other STIs. CMV infection is prevalent worldwide, especially in developing countries and lower socioeconomic groups. The virus is found in semen, cervical secretions, urine, blood, saliva, breast milk, and stool, and transmission is associated with close (although not always genital) interpersonal contact or direct transfer of cells or body fluids. It is more common in homosexual men and in young women with multiple sexual partners. Intrauterine CMV infection is the most common congenital infection and occurs in 0.5% to 3% of all live births. Like HSV, primary maternal infection carries the greatest risk of transmission and severe consequences. Infected infants can be asymptomatic or may experience varying degrees of sensorineural hearing loss or severe cognitive and psychomotor developmental deficits.2,67 Perinatal transmission of CMV may occur across the placenta, by contamination with infected secretions during passage through the birth canal, or during breast-feeding.
PATHOPHYSIOLOGY After CMV infects a human cell, it may replicate and destroy the infected cell or become incorporated into the host cell’s DNA. Local CMV infections can persist despite the presence of large quantities of systemic antibody to CMV. Cell-mediated immunity seems to have a particular role in protecting against CMV infections. Depression of CMV-specific cell-mediated immunity has been noted in otherwise normal hosts with CMV infection. This may be caused by injury of T cells or macrophages by the cytomegalovirus.67
CLINICAL MANIFESTATIONS In healthy individuals, CMV infection can cause a number of mild subclinical or nonspecific illnesses, including mononucleosis, pneumonitis, hemolytic anemia, and thrombocytopenia purpura. In contrast, a CMV infection in an immunocompromised individual, such as a transplant recipient or an individual with AIDS, can cause a devastating, life-threatening illness.
Congenital CMV infection is the most common serious viral infection among infants. Approximately 1% of all infants (40,000) are born with congenital CMV. Of these, 10% (4000) demonstrate typical manifestations of the infection, such as hepatosplenomegaly, intracranial calcifications, microcephaly, smallness for gestational age, and hearing impairments. An additional 10% to 15% of these are asymptomatic at birth; however, they begin to develop manifestations of the infection within the first few months of life. Recent evidence suggests that symptomatic infection of infants is caused by a primary infection of the mother during her pregnancy and not necessarily by reinfection or reactivation of a prior infection.
EVALUATION AND TREATMENT The most definitive diagnostic test for CMV is isolation of the virus, usually through growth in human fibroblast cell culture. Several methods for measuring antibodies to CMV are available, including complement-fixation (CF) tests and indirect immunofluorescent antibody (IFA) tests. These methods commonly are used in clinical situations.
With the increased incidence of CMV infection among immunocompromised individuals (persons with AIDS or transplants), various treatment modalities have been investigated. Ganciclovir is similar to acyclovir and inhibits viral DNA polymerase (see Chapter 4). Relapses of CMV infection are frequent after therapy ceases; thus lifelong therapy is particularly indicated in individuals with AIDS.48 Acyclovir has been used, but optimum therapeutic benefits have not been established. Future therapies still under investigation include ganciclovir plus CMV immunoglobulin and vaccine.
Experimental antiviral drugs may prove helpful in the treatment of severe CMV infection, and preliminary studies to develop a vaccine appear promising. No treatment is indicated, however, in most cases of CMV infection.
Acute urethra 936
Amebiasis 946
Bacterial vaginosis (BV) 934
Buboes 932
Campylobacter enteritis 946
Chancre 928
Chancroid 932
Chlamydia 935
Condylomata acuminata 940
Condylomata lata 929
Congenital syphilis (CS) 929
Cytomegalovirus (CMV) 948
Disseminated gonococcal infection (DGI) 926
Donovan body 934
Epstein-Barr virus (EBV) 947
Fomite 925
Genital herpes 938
Giardiasis 946
Gonococcus 924
Gonorrhea 924
Granuloma inguinale (donovanosis) 933
Gummas 929
Hepatitis B virus (HBV) 947
Hepatitis delta agent 947
Human papillomavirus (HPV) 940
Latent syphilis 929
Lymphogranuloma venereum (LGV) 937
Molluscous body 942
Molluscum contagiosum 941
Neurosyphilis 929
Nongonococcal urethritis (NGU) 937
Ophthalmia neonatorum 927
Pediculosis pubis 945
Perihepatitis 926
Primary syphilis 928
Pseudobuboes 934
Scabies 944
Secondary syphilis 928
Shigellosis 946
Syphilis 927
Tertiary syphilis 929
Trichomonad 943
Trichomoniasis 943
Trophozoite 946
REFERENCES
1. National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Annual Report 2008. U.S. Department Health and Human Services CDC and Prevention Available. www.cdc.gov/std/stats
2. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance, 2007. Atlanta, GA: U.S. Department of Health and Human Services; December 2008. www.cdc.gov/std/stats
3. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007 Supplement, Gonococcal Isolate Surveillance Project (GISP) Annual Report 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, March 2009. www.cdc.gov/std/stats.
4. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007 Supplement, Syphilis Surveillance Report. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, March 2009. www.cdc.gov/std/stats.
5. Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2007 Supplement, Chlamydia Prevalence Monitoring Project Annual Report 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention; January 2009. www.cdc.gov/std/stats.
6. Centers for Disease Control and Prevention: Trends in reportable sexually transmitted diseases in the United States, 2007: National data on chlamydia, gonorrhea and syphilis. In STD surveillance 2007. Available at www.cdc.gov/std/stats/trends2007.htm. http://www.cdc.gov/std/stats07/main.htm
7. Hook, E.W., III., Handsfield, H.H. Gonococcal infections in the adult. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
8. Pelouze, P.S. Gonorrhea in the male and female. Philadelphia: Saunders; 1941.
9. Whittington, W., et al. Gonorrhea. In Morse S.A., Moreland A.A., Holmes K.K., eds.: Atlas of sexually transmitted diseases and AIDS, ed 3, London: Mosby-Wolfe, 2003.
10. Krieger, J.N. Sexually transmitted diseases in men. In Tanagho E.A., McAninch J.W., eds.: Smith’s general urology, ed 17, New York: McGraw-Hill, 2007.
11. Westrom, L., et al. Pelvic inflammatory disease and fertility: a cohort study of 1,844 women with laparoscopically verified disease and 657 control women with normal laparoscopic results. Sex Trans Dis. 1992;19(4):184–1982.
12. Zenilman, J.M. Gonorrhea: clinical and public health issues. Hosp Pract. 1993;28(2a):29.
13. Sperling, R.S. Infection protocols: perihepatitis. Contemp OB/GYN. 1992;37(6):51.
14. Emmert, D.H., Kirchner, J.T. Sexually transmitted diseases in women: gonorrhea and syphilis. Postgrad Med. 2000;107(2):181–184. [189-190, 193-197].
15. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2006 supplement, gonococcal isolate surveillance project (GISP) annual report. Atlanta: U.S. Department of Health and Human Services; 2008.
16. Centers for Disease Control and Prevention. Sexually transmitted disease surveillance 2006 supplement, syphilis surveillance project. Atlanta: U.S. Department of Health and Human Services; 2007.
17. Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines 2002. MMWR. 2006;51(RR-11):1–94.
18. Leu, R.H. Complications of coexisting chlamydial and gonococcal infections. Postgrad Med. 1991;89(7):56–60.
19. Brandt, A.M. No magic bullet: a social history of venereal disease in the United States since 1880, expanded edition. New York: Oxford University Press; 1987.
20. Sparling, P.F. Clinical manifestations of syphilis. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
21. Schultz, K.F., et al. Congenital syphilis. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
22. Hook, E.W., Marra, C.M. Medical progress: acquired syphilis in adults. N Engl J Med. 1992;326(16):1060.
23. Thin, R.N. Early syphilis in the adult. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
24. Wooldridge, W.E. Syphilis: a new visit from an old enemy. Postgrad Med. 1991;89(1):193–196. [199-202].
25. Tillman, J. Syphilis an old disease, a contemporary problem. J Obstet Gynecol Neonat Nurs. 1992;21(3):209.
26. Jacobs, R.A. Infectious diseases: spirochetal. In McTierney L.M., McPhee S.J., Papadakis M.S., eds.: Current medical diagnosis & treatment, ed 47, Norwalk, CT: Appleton & Lange, 2008.
27. O’Farrell, N. Tropical medicine series: donovanosis. Sex Transm Infect. 2002;78(6):452–457.
28. Para, M.F., Baird, I.M. Genital ulcer syndromes. In: Spagna V.A., Prior R.B., eds. Sexually transmitted diseases: a clinical syndrome approach. New York: Marcel Dekker, 1985.
29. Committee on Infectious Disease. Red Book 2000. Elk Grove Village, IL: American Academy of Pediatrics; 2000.
30. Ronald, A.R., Albritton, W. Chancroid and Haemophilus ducreyi. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 2, New York: McGraw-Hill, 1990.
31. Richens, J. The diagnosis of treatment of donovanosis (granuloma inguinale). Genitourin Med. 1991;67(6):441–452.
32. Hart, G. Donovanosis. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
33. Hillier, S.L., et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. N Engl J Med. 1995;333(26):1737–1742.
34. Amsel, R., et al. Nonspecific vaginitis. Diagnostic criteria ad microbial and epidemiologic associations. Am J Med. 1983;74(1):14–22.
35. Kellogg, N.D., et al. Comparison of nucleic acid amplification tests and culture techniques in the detection of Neisseria gonorrhoeae and Chlamydia trachomatis in victims of suspected child sexual abuse. J Pediatr Adolesc Gynecol. 2004;17(5):331–339.
36. Sargent, S.J. The “other” sexually transmitted diseases: chlamydial, herpes simplex virus, and human papillomavirus infections. Postgrad Med. 1992;91(4):359–362. [371-374, 377].
37. Schachter, J., Barnes, R. Infections caused by Chlamydia trachomatis. In Morse S.A., Moreland A.A., Holmes K.K., eds.: Atlas of sexually transmitted diseases and AIDS, ed 2, London: Mosby-Wolfe, 1996.
38. Westrom, L.V. Chlamydia and its effect on reproduction. J Br Fer Soc. 1996;1(1):23–30.
39. Chambers, H.F. Infectious diseases: bacterial and chlamydial. In McTierney L.M., McPhee S.J., Papadakis M.A., eds.: Current medical diagnosis and treatment, ed 35, Norwalk, CT: Appleton & Lange, 1996.
40. Perine, P.I., Osoba, A.O. Lymphogranuloma venereum. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 2, New York: McGraw-Hill, 1990.
41. Mertz, G.J., et al. Risk factors for the sexual transmission of genital herpes. Ann Intern Med. 1992;116(3):197.
42. Stagno, S., Whitley, R.J. Herpesvirus infection in the neonate and children. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 2, New York: McGraw-Hill, 1990.
43. Landenberg, A.G., et al. A prospective study of new infections with herpes simplex virus type 1 and type 2. Chiron HSV Vaccine Study Group. N Engl J Med. 1999;341(19):1432–1438.
44. Koelle, D.M., Wald, A. Herpes simplex virus: the importance of asymptomatic shedding. J Antimicrob Chemother. 2000;45(Suppl T3):1–8.
45. Stephenson, J. Genital herpes vaccine shows limited promise. JAMA. 284(15), 1913-1914.
46. Rose, F.B., Camp, C.J. Genital herpes: how to relieve patients’ physical and psychological symptoms. Postgrad Med. 1988;84(3):81–86.
47. Wright, T.C., et al. Interim guidance for the use of human papillomavirus DNA testing as an adjunct to cervical cytology for screening. Obstet Gynecol. 2004;103(2):304–309.
48. Woodman, C.B., et al. Natural history of cervical human papillomavirus infection in young women: a longitudinal cohort study. Lancet. 2001;357(9271):1831–1836.
49. Derksen, D.J. Children with condylomata acuminata. J Fam Pract. 1992;34(4):419–423.
50. Alary, M., et al. Strategy for screening pregnant women for chlamydial infection in a low-prevalence area. Obstet Gynecol. 1993;82(3):399.
51. Shah, K.V. Biology of genital tract human papillomaviruses. Urol Clin North Am. 1992;19(1):63–69.
52. McAninch, J.W. Disorders of the penis and male urethra. In: Tanagho E.A., McAninch J.W., eds. Smith’s general urology. Norwalk, CT: Appleton & Lange, 1995.
53. Camisa, C. Condyloma acuminatum and other human papillomavirus-induced diseases. In: Spagna V.A., Prior R.B., eds. Sexually transmitted disease: a clinical syndrome approach. New York: Marcel Dekker, 1985.
54. Harper, D.M., et al. Efficacy of a bivalent L1 virus-like particle vaccine in prevention of infection with human papillomavirus types 16 and 18 in young women: a randomised controlled trial. Lancet. 2004;364(9447):1757–1765.
55. Berger, T.G. Skin diseases of the external genitalia. In: Tanagho E.A., McAninch J.W., eds. Smith’s general urology. Norwalk, CT: Appleton & Lange, 1995.
56. Lambert, D.R., Yoder, F.W. Ectoparasites and molluscum contagiosum. In: Spagna V.A., Prior R.B., eds. Sexually transmitted diseases: a clinical syndrome approach. New York: Marcel Dekker, 1985.
57. Rein, M.R., Holmes, K.K. Nonspecific vaginitis, vulvovaginal candidiasis, and trichomoniasis: clinical features, diagnosis, and management. In: Remington J., Schwartz M.N., eds. Current clinical topics in infectious diseases. New York: McGraw-Hill, 1983.
58. Bartlett, J.G. Pocket book of infectious disease therapy. Baltimore: Williams & Wilkins; 1995.
59. Orkin, M., Maibach, H.I. Scabies. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 2, New York: McGraw-Hill, 1990.
60. Hammerschlag, M.R., Laraque, D. Inappropriate use of nonculture tests for the detection of chlamydia trachomatis in suspected victims of child sexual abuse: a continuing problem. Pediatrics. 1999;104(5):1137.
61. Quinn, T.C., Stamm, W.E. Proctocolitis, enteritis, and esophagitis in homosexual men. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 2, New York: McGraw-Hill, 1990.
62. Gardner, T.B., Hill, D.R., Treatment of giardiasis. Clin Microbiol Rev. 2001;14(1):114–128. Available at. http://cmr.asm.org/cgi/content/full/14/1/114?view=long&pmid=11148005.
63. Lemon, S.M., Newbold, J.E. Viral hepatitis. In Holmes K.K., et al, eds.: Sexually transmitted diseases, ed 4, New York: McGraw-Hill, 2008.
64. Klein, M.B. Hepatitis B virus: perinatal management. J Perinat Neonat Nurs. 1988;1(4):12.
65. Beasley, R.P., et al. The e antigen and vertical transmission of hepatitis B surface antigen. Am J Epidemiol. 1977;105(2):94–98.
66. Stevens, C.E., et al. HBeAg and anti-HBe detection by radioimmunoassay: correlation with vertical transmission of hepatitis B virus in Taiwan. J Med Virol. 1979;3(3):237–241.
67. Immunization Practices Advisory Committee. Hepatitis B virus: a comprehensive strategy for eliminating transmission in the United States through universal childhood vaccination: recommendations of the Immunization Practice Advisory Committee (ACIP). MMWR. 1991;40(RR-13):1–19.