ALTERATIONS OF THE INTEGUMENT IN CHILDREN


Children often develop alterations in the skin that may be minor or severe and localized or generalized. Unfortunately the skin is often underrated in regard to its vital roles as a barrier, foundation, and calorie reservoir, as well as temperature regulation, sensation, grasp, insulation, psychosocial impact, and self-image. Manifestation of skin diseases in children may differ from those in adults, although the causative mechanisms may be similar. Some diseases resolve spontaneously and require no treatment. Diagnosis is commonly made from the history, appearance, and distribution of the lesion or lesions. Common skin diseases of childhood are presented here.
ACNE VULGARIS
Acne vulgaris is the most common skin disease and affects 85% of the population between the ages of 12 and 25 years. Genetic influences may determine an individual’s susceptibility and severity of disease. Severe acne tends to run in families. The incidence of acne is the same in both genders, although severe disease affects males more often.
Distinctive pilosebaceous units, known as sebaceous follicles, are the sites for development of acne lesions. The follicles are located primarily on the face and upper parts of the chest and back. These follicles have many large sebaceous glands, a small vellus hair, and a dilated follicular canal that is visible as a “pore” on the skin surface. Acne lesions may be divided into inflammatory lesions (pustules, papules, nodules) and noninflammatory lesions (closed and open comedones).1 In noninflammatory acne the comedones are open (blackheads) and closed (whiteheads), with the accumulated material causing distention of the follicle and thinning of follicular canal walls. Inflammatory acne develops in closed comedones when the follicular wall ruptures, expelling sebum into the surrounding dermis and initiating inflammation. Pustules form when the inflammation is close to the surface; papules and cystic nodules can develop when the inflammation is deeper, causing mild to severe scarring (Figure 45-1). Both types of lesions may exist in the same individual.

Figure 45-1 Cystic acne. Multiple pustules (erythematous papules and pustules) are present, and several have become confluent. Note areas of scarring. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
The exact cause of acne is unknown and various pathophysiologic factors contribute to the development of acne. The principal factors are follicular hyperkeratinization, excessive sebum production, blockage of sebaceous glands, increased colonization of Propionibacterium acnes, and inflammation secondary to the action of extracellular inflammatory products produced by P. acnes. An excessive production and accumulation of sebum appear to be directly related to androgenic hormones and the pathogenesis of acne. Testosterone is converted to dihydrotestosterone in the skin, which increases the size and productivity of the sebaceous glands.2 Acne begins with sebum accumulation that obstructs the pilosebaceous unit. The mass of accumulated keratinous sebaceous material and bacteria within the pilosebaceous follicle (see Figure 45-1) causes inflammation when it is exposed to the dermis with rupture of a follicle.
The P. acnes anaerobic bacteria produce extracellular porphyrins and proinflammatory molecules, including chemotactic factors and lipolytic and proteolytic enzymes. The hydrolytic action of the enzymes converts triglycerides into free fatty acids that stimulate inflammation and edema that result in breakdown of the follicle wall. Chemotactic substances also may be released that involve mediation of inflammation by attraction of polymorphonuclear leukocytes.
Acne conglobata is a highly inflammatory form of severe, disfiguring acne that involves the formation of communicating cysts and abscesses beneath the skin and requires referral and aggressive treatment. Remissions tend to occur during the summer, perhaps from more exposure to sunlight. External factors, such as cosmetics, use of oral and topical medications, mechanical friction, and occupation, may be etiologic factors. Abuse of anabolic-androgenic steroids is associated with acne conglobata.3 Stress does not cause acne but can make it worse. Self-manipulation of acne must be discouraged because it leads to increased inflammation and potential scarring.
Treatment of acne should address the causative factors and be individualized. Diet has not been proven to cause acne in spite of common lay opinion that there are acne-related foods; dietary restrictions are generally not effective.4 Topical treatment, including topical antibiotics in combination with benzoyl peroxide (reduces bacterial resistance by disrupting the biofilm and increasing local oxygen tension), azelaic acid, and tretinoin should be the first line of therapy because it is the least invasive.5 Systemic therapies, including oral antibiotics, sex hormones, corticosteroids, and isotretinoin, should be pursued when first-line therapy fails. Acne surgery, including comedo extraction, intralesional steroids, and cryosurgery, may be useful. Severe scarring may be treated with dermabrasion or subincision. Special consideration must be given to treatment for those with darker skin because they have greater risk for hyperpigmentation and keloidal scarring.6
DERMATITIS
Atopic dermatitis (AD) is the most common cause of eczema with a prevalence rate of about 10% to 20% in children and 1% to 3% in adults. AD is increasing throughout the world.7 Onset is usually from 2 to 6 months of age, and 85% of cases occur within the first 5 years of life; 75% to 80% of individuals with AD have a personal or family history of asthma, allergic rhinitis (hay fever), or food allergy. The cause of this chronic relapsing form of pruritic eczema involves an interplay of genetic predisposition, altered skin barrier function associated with filaggrin gene mutations (proteins that bind keratin in the epidermis), reduced ceramide (a stratum corneum lipid) levels, altered innate immunity, and altered immune responses to allergens, irritants, and microbes.8 There is debate as to whether the pathophysiology favors an “inside-out” explanation with immunologic dysregulation leading to the skin barrier abnormality or an “outside-in” explanation with the primary barrier dysfunction causing the immunologic perturbations.9 Positive immediate skin tests to a variety of common food and inhalant allergens are seen in approximately 80% of individuals with immunoglobulin E (IgE) sensitization and children are more likely to develop asthma.10 Eosinophilia is common in both forms of AD.
In AD, memory T cells in the blood express cutaneous lymphocyte antigen (CLA), which leads to the homing of lymphocytes to the skin. In the acute phase of AD, inflammation is associated with activation of Th-1 cells with overexpression of cytokines (interleukin 4 [IL-4], IL-5, and IL13) and chemokines (CCL1 [chemotactic cytokine ligand 1] and CCL 18) with increases in IgE, eosinophils, and macrophages. In the chronic phase, there is activation of Th-1 cells with expression of interferon-gamma (IFN-γ), IL-12, and granulocyte-macrophage colony-stimulating factor (GM-CSF). There is activation of macrophages, dendritic cells (with high affinity for IgE), and mast cells with release of proinflammatory cytokines.11 Th-2 cytokine expression also contributes to reduction in antimicrobial peptides and reduced filaggrin expression; however, the mechanisms leading to this effect are unknown.12 Alterations in filaggrin protein lead to a defect of the epidermal barrier that causes transepidermal water loss and allows easy penetration of pathogens and allergens through the skin and a systemic hyperactive immune response.13,14 Filaggrin gene mutations also are associated with increased risk for asthma in AD and ichthyosis vulgaris (dry, scaly skin).15 In AD keratinocytes are deficient in their ability to express Toll-like antimicrobial peptides (see Chapter 6), including beta defensins and cathelicidins, and may predispose such individuals to skin colonization and infection with Staphylococcus aureus, viruses, and fungi.
AD has a long-term course with frequent exacerbations, severe pruritus, and characteristic eczematoid appearance with redness, edema, and scaling (Figure 45-2). The skin becomes increasingly dry, sensitive, itchy, and easily irritated because the barrier function is impaired. Microscopic epidermal cracks that let water out and irritants, allergens, and microbes in leads to further inflammation, drying, and cracking. Itching is the hallmark of atopic dermatitis, and rubbing and scratching to relieve the itch are responsible for many of the clinical changes of AD. Unlike its role in urticaria, histamine is not considered a major pruritogen in AD. Peripheral and central nerve sensitization, crosstalk among keratinocytes, immune cells and nerve fibers, and release of mediators including serine proteases, IL-31, nerve growth factor, and the epidermal opioid system may contribute to pruritus of AD.16,17

Figure 45-2 Atopic dermatitis. Characteristic lesions with crusting from irritation and scratching over knees and around ankles. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
In infants, the rash appears primarily on the face, scalp, trunk, and extensor surfaces of the arms and legs. In older children and adults, the rash tends to be found on the neck, antecubital and popliteal fossae, and hands and feet. Lichenification (thickening of the epidermis from constant scratching) is more common in adults with chronic eczema. Individuals with AD tend to develop viral, bacterial, and fungal skin infections in the areas with eczema. The irritation and itching interfere with sleep and cause irritability.
There are no specific laboratory features of AD that can be used for diagnostic purposes, and diagnosis is based on clinical history and presentation of symptoms.18 Management of AD requires a systematic, multipronged approach. The approach includes parent education; identification and elimination of triggers or exacerbating factors, such as irritants, allergens, and emotional stressors; and incorporates skin moisturization, and pharmacologic and nonpharmacologic therapies. Hydration of the skin is the key to good therapy but is often difficult to achieve. Topical therapy can include baths, skin moisturizers, and wet wraps.9 Anti-inflammatory agents, such as topical corticosteroids, topical calcineurin inhibitors, or tar preparations, are applied during active flares of eczema. Topical calcineurin inhibitors (tacrolimus and pimecrolimus) have an important role in the management of AD. Phototherapy may be beneficial. Systemic therapy includes the use of sedating antihistamines and antibiotics for treatment of infection. Systemic corticosteroids usually are not warranted. Treatment plans should be individualized to address the individual’s skin reaction pattern and acuity of the rash.19,20
Diaper Dermatitis
Diaper dermatitis is probably the most common skin disorder of infancy and early childhood. It is a contact dermatitis (see Chapter 44) caused by chemical irritation. This form of irritant contact dermatitis is initiated by a combination of factors that include prolonged exposure to and irritation by urine and feces, maceration by wet diapers, airtight plastic diaper covers, and possibly increased association with intercurrent illnesses and early introduction of cereals. Diaper designs have decreased diaper dermatitis in infants.21 Frequently, the infant with diaper dermatitis is secondarily infected with Candida albicans.
The lesions vary from mild erythema to erythematous papular lesions. Candidal (monilial) diaper dermatitis is usually very erythematous, with sharp margination and pustulovesicular satellite lesions (Figure 45-3).
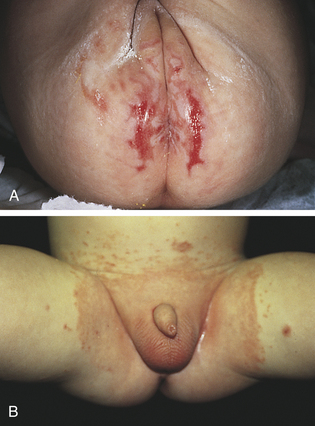
Figure 45-3 Diaper dermatitis. A, Diaper dermatitis with erosions. B, Diaper dermatitis with Candida albicans secondary infection. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
Treatment is changing the diaper frequently to keep the area clean and dry or frequently exposing the perineal area to air. Topical antifungal medication is used to treat C. albicans when present. Short-term use of low-potency topical steroids alternately with antifungals at each diaper change helps reduce inflammation. Various topical agents provide a barrier from the irritating agents and promote healing.
INFECTIONS OF THE SKIN
Infectious diseases caused by bacteria, viruses, and fungi constitute the major forms of skin disease. Breaks in the skin integrity, particularly those that inoculate pathogens into the dermis and epidermis, may cause or exacerbate infections. Most infections tend to occur superficially; however, systemic signs and symptoms do develop occasionally and rarely may be life threatening.
Bacterial Infections
Impetigo is a common bacterial skin infection in infants and children, usually caused by S. aureus or group A streptococcus. The disease is more common in midsummer to late summer, with a higher incidence in hot, humid climates. Impetigo is particularly infectious among people living in crowded conditions with poor sanitary facilities. It affects children in good health, but conditions such as anemia and malnutrition are predisposing factors. There are two common types of impetigo: bullous and vesicular.22 Both start as vesicles with a very thin vesicular roof composed of stratum corneum.
Bullous Impetigo: Bullous impetigo is a rarer variant of impetigo caused by S. aureus. The staphylococci produce a bacterial toxin called exfoliative toxin (ET) that causes a disruption in desmosomal adhesion molecules with blister formation.23 This form characteristically occurs in newborns and is highly contagious. The source of the infection is usually a staff member in a newborn nursery or a family member with a pustule or who is an asymptomatic carrier. The pathogen is often carried in the anterior nares, perineal region, or fingernails and is transmitted by contact with the individual or contaminated equipment.24
The exfoliative toxin stimulates the formation of vesicles that enlarge or coalesce to form superficial bullae. There may be a few localized lesions or many lesions scattered over the skin. As the bullae rupture, a thin, flat, honey-colored crust appears. The crust is the hallmark of impetigo. A moist, inflamed serum-weeping base is revealed when the crust is removed. The lesions are often located on the face around the nose and mouth, but the hands and other exposed areas are also involved. Regional lymphadenitis is uncommon.
Vesicular Impetigo: Vesicular impetigo is a contagious, acute, superficial, vesiculopustular form of impetigo caused by group A Streptococcus pyogenes (alone or in combination with S. aureus). The microorganisms are disseminated by direct physical contact from other infected individuals or through insect bites. The lesions begin as small vesicles with a honey-colored serum. Yellow to white-brown crusts form as the vesicles rupture and extend radially (Figure 45-4). Untreated lesions may last for weeks and extend to cover a large area. In contrast to bullous impetigo, regional lymphadenitis is common.

Figure 45-4 Impetigo and herpes simplex virus (HSV) of upper lip. Note weeping and crusting lesions. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
The risk of nephritogenic strains of streptococci varies considerably in North America.25 Aggressive treatment of infected individuals and their contacts significantly reduces the chance of acute glomerulonephritis, which is clearly the most serious complication of streptococcal impetigo.
Treatment of choice for both types of impetigo is topical mupirocin and topical fusidic acid or oral antibiotics.22 Antibiotic therapy should be determined by bacterial culture and drug sensitivity because antimicrobial resistance is increasing.26 Removal of crusts and scrubbing the lesions with antibacterial soaps have not been shown to be effective.27 Good handwashing techniques and isolation of the infected child’s washcloth, towels, drinking glass, and linen are important to control this highly contagious disease.
Staphylococcal Scalded-Skin Syndrome
Staphylococcal scalded-skin syndrome (SSSS) is the most serious staphylococcal infection that affects the skin and usually is seen in infants and children younger than 5 years.28 SSSS is caused by virulent group II staphylococci, which produce an exfoliative toxin that attacks desmoglein and adhesion molecules and causes a separation of the skin just below the granular layer of the epidermis.29 The toxins are usually produced at body sites other than the skin and arrive at the epidermis through the circulatory system. Staphylococci typically are not found in the skin lesions themselves. Adults have circulating antistaphylococcal antibodies and are better able to metabolize and excrete the toxin. Newborns are at the highest risk because of their lack of immunity (not having prior exposure to the toxin).
The clinical symptoms begin with fever, malaise, rhinorrhea, and irritability followed by generalized erythema with exquisite tenderness of the skin. There may be an associated impetigo, but the infection often begins in the throat or chest. The erythema spreads from the face and trunk to cover the entire body except the palms, soles, and mucous membranes. Within 48 hours, blisters and bullae may form, causing severe pain (Figure 45-5). Fluid loss from ruptured blisters and water evaporation from denuded areas may cause dehydration. Perioral and nasolabial crusting and fissures develop. In severe cases the skin of the entire body may slough. When secondary infection can be prevented, healing of the involved skin occurs in 10 to 14 days, usually without scarring.

Figure 45-5 Staphylococcal scalded-skin syndrome (SSSS). The skin lesions, showing desquamation and wrinkling of the skin margins, appeared 1 day after drainage of a staphylococcal abscess. (From Habif TP: Clinical dermatology: a color guide to diagnosis and therapy, ed 5, St Louis, 2010, Mosby.)
Before medical intervention is begun, culture, histology, or exfoliative cytology must be done to differentiate SSSS from toxic epidermal necrolysis (TEN) (see p. 1692). When the infection is confirmed, treatment with oral or intravenous antibiotics is begun.30 Topical antibiotics are ineffective. The skin should be treated the same as that with a severe burn—with meticulous aseptic technique. Special care is required in serious cases and when the lips and eyelids are involved.28
Fungal Infections
Fungal disorders are known as mycoses and, when caused by dermatophytes (fungi that thrive on keratin), the mycoses are termed tinea (dermatophytosis or ringworm).31 Tinea pedis (a chronic, superficial fungal infection of the skin of the foot) occurs in children but is rare. Scaling disorders of the toes and feet in prepubertal children are usually eczema. Tinea capitis (infection of the scalp) and tinea corporis (infection of the body) are much more common in children than adults. (The different types of tinea are described in Chapter 44.) Epidermophyton are the major cause of superficial fungal infections in children.32 These dermatophytes invade the stratum corneum and not the remainder of the epidermis or dermis. The inflammatory response is thought, in part, to be secondary to the toxins released by the dermatophyte. It is important to confirm by culture which microorganism is causing the fungal infection before commencing therapy.
Tinea Capitis
Tinea capitis, a fungal infection of the scalp, is the most common fungal infection of childhood. It rarely affects infants and is seen in children younger than age 12. Primary microorganisms responsible for the disease are Microsporum canis and Trichophyton tonsurans. M. canis is found on cats, dogs, and certain rodents. Humans appear to be a terminal host for M. canis, and children who handle such animals are possible hosts. Human-to-human transmission does not occur. T. tonsurans conversely is transmitted by human-to-human contact. Areas of crowding are the most prevalent environments for this microorganism, which frequently affects inner-city children. T. tonsurans is often the predominant dermatophyte found on inner-city children, and many of these infections are not symptomatic. The prevalence of asymptomatic carriers among household contacts of a child with active T. tonsurans disease is high.33 Treatment of household contacts with a sporicidal shampoo should be considered and co-sleeping and comb sharing must be discouraged. When symptoms are present, the clinical presentations vary, depending on the microorganism. Often the lesions are circular and manifest by broken hairs 1 to 3 mm above the scalp, leaving a partial alopecia 1 to 5 cm in diameter34 (Figure 45-6). Slight erythema and scaling with raised borders can be observed.
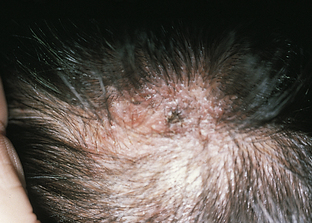
Figure 45-6 Tinea capitis. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
Diagnosis is best confirmed by performing Wood light examination, potassium hydroxide (KOH) examination, and fungal culture, in that order. T. tonsurans does not fluoresce with Wood light examination. Oral griseofulvin is the treatment of choice because topical fungicides do not penetrate to the hair bulb. Terbinafine, itraconazole, and fluconazole are effective alternatives.35 Adjunct therapy includes 2% ketoconazole and 1% selenium sulfide shampoos.36
Tinea Corporis
Tinea corporis is a common superficial dermatophyte infection in children. The microorganisms most commonly responsible for this disease are M. canis and Trichophyton mentagrophytes. As in tinea capitis, contact with kittens and puppies is a common source of the disorder. Tinea corporis preferentially affects the nonhairy parts of the face, trunk, and limbs. Lesions are often erythematous, round or oval scaling patches that spread peripherally with clearing in the center, creating the ring appearance, which is why this disease is commonly referred to as ringworm. The lesions are distributed asymmetrically, and multiple lesions (when present) overlap. KOH examination of the scale from the border of the lesions confirms the diagnosis for most lesions. Most lesions respond well to applications of appropriate topical antifungal medications.32
Thrush
C. albicans infection is a superficial fungal infection that commonly occurs in children. C. albicans is part of the normal skin flora in certain individuals and invades susceptible tissue sites if the predisposing factors are not eliminated. C. albicans penetrates the epidermal barrier more easily than other microorganisms because of its keratolytic proteases and other enzymes. C. albicans attracts neutrophils to skin sites of invasion and generates inflammation by activation of the complement system within the skin.
Thrush is the term used to describe the presence of Candida in the mucous membranes of the mouth of infants and, less commonly, adults. Thrush is characterized by the formation of white plaques or spots in the mouth that lead to shallow ulcers. The tongue may have a dense, white covering. The underlying mucous membrane is red and tender and may bleed when the plaques are removed. The disease is often accompanied by fever and gastrointestinal irritation. The infection commonly spreads to the groin, buttocks, and other parts of the body. Treatment may be difficult and may include oral antifungal washes, such as nystatin oral suspension. Gentian violet can also be effective. Simultaneous treatment of a Candida nipple infection or vaginitis in the mother is helpful in reducing the C. albicans surface colonization of the infant. Feeding bottles and nipples should be sterilized to prevent reinfection. The diaper area should be kept clean and dry.
Viral Infections
Viral infections of the skin in children are caused by poxvirus, papovavirus, and herpesvirus. The most common infections are described here.
Molluscum Contagiosum
Molluscum contagiosum is a common highly contagious poxvirus infection of the skin and occasionally conjunctiva that affects primarily children. It is transmitted by skin-to-skin contact, autoinoculation, and fomites, such as clothing, wash devices, and towels. This disease appears to be more common in individuals with atopic dermatitis and a variety of immunodeficient states, including human immunodeficiency virus (HIV).37 The poxvirus induces epidermal cell proliferation and blocks immune responses that would control the virus. The epidermis grows down into the dermis to form saccules containing clusters of virus. The characteristic molluscum body is composed of mature, immature, and incomplete viruses and cellular debris.38
The lesions of molluscum are discrete, slightly umbilicated, dome-shaped papules 1 to 5 mm in diameter that appear anywhere on the skin or conjunctiva. The skin distribution in children is mainly on the trunk, face, and extremities (Figure 45-7). The pubic, genital, and perineal areas are favored in adults (see Chapter 24). Usually no inflammation surrounds molluscum lesions unless they are traumatized or secondary infection occurs. Scarring occurs with healing.

Figure 45-7 Molluscum contagiosum. Waxy pink globules with umbilicated centers. (From Habif TP: Clinical dermatology: a color guide to diagnosis and therapy, ed 3, St Louis, 1996, Mosby.)
The best three diagnostic procedures are: (1) staining smears of the expressed molluscum body, (2) examining a biopsy, and (3) inoculating a molluscum suspension into cell cultures to demonstrate the cytotoxic reactions. Most lesions are self-limiting and clear in 6 to 9 months if not manipulated. However, because children often do manipulate these lesions, spontaneous involution may take 2 to 4 years without therapy.
Treatment options include topical, oral, and surgical approaches (cryotherapy, curettage or laser ablation), and no treatment is universally effective. Destructive therapy is poorly tolerated by children.39 Measures to prevent spread of infection must be taken and recurrences are common. Children must be taught not to manipulate or scratch these lesions.
Rubella (German or 3-Day Measles)
Rubella is a common communicable disease of children and young adults caused by a ribonucleic acid (RNA) virus that enters the bloodstream through the respiratory route. This disease is mild in most children. The incubation period ranges from 14 to 21 days. Prodromal symptoms are few but may include enlarged cervical and postauricular lymph nodes, low-grade fever, headache, sore throat, runny nose, and cough. A faint-pink to red, coalescing maculopapular rash develops on the face, with spread to the trunk and extremities 1 to 4 days after the onset of initial symptoms (Figure 45-8). The rash is thought to be the result of virus dissemination to the skin. The rash subsides after 2 to 3 days, usually without complications. Children are generally not contagious after development of the rash. There is lifelong immunity to rubella—as there is for measles, chickenpox, and roseola—after contracting the disease. Differential presentations of viral diseases producing rashes are given in Table 45-1.
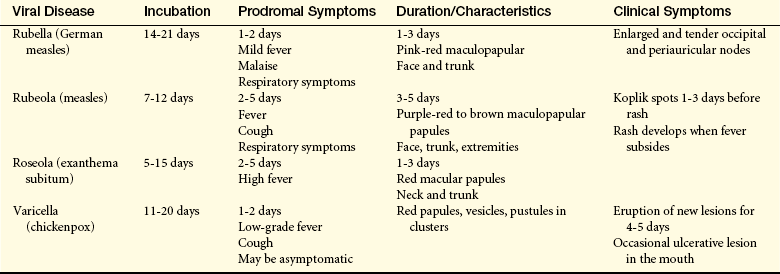
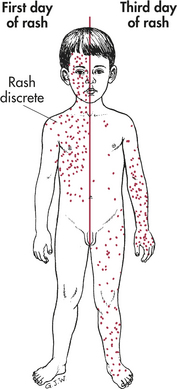
Figure 45-8 Measles. Full-blown maculopapular rash with tendency to coalesce. (From Wehrle PF, Top FH Sr: Communicable and infectious diseases, ed 9, St Louis, 1981, Mosby.)
Vaccination for rubella is usually combined with vaccines for mumps and measles (rubeola) (MMR). A quadravalent vaccine MMRV, combining the attenuated virus MMR vaccine with the addition of varicella (chickenpox), has been approved in the United States and Europe for children ages 1 to 12 years. Vaccine recommendations are presented in Chapter 9, Table 9-13. In the past, parents chose not to give the vaccine because of the misbelief that it would cause the disease. Studies have confirmed that measles or rubella-like illnesses in MMR-vaccinated children are often caused by other viruses.40 Measles is known to occur in previously immunized children.41
More recently parental concern has focused on the belief that MMR vaccination may cause autism. Although MMR vaccine may rarely be associated with adverse neurologic events, studies conclude that MMR immunization does not cause autism.42 Lack of vaccination, however, leads to significant morbidity and mortality,43,44 with pneumonia, croup, and encephalitis being causes of death worldwide.45,46
Women of childbearing age are immunized if their rubella hemagglutination-inhibition titer is low. Pregnancy should be avoided for 3 months after vaccination because the attenuated virus in the vaccine may remain for this period. Pregnant women who have rubella early in the first trimester have an 80% risk of congenital defects.47
There is no specific treatment for rubella. Recovery is spontaneous, although lymph nodes may remain enlarged for weeks. Supportive therapy includes rest, fluids, and use of a vaporizer. In rare cases a mild encephalitis or peripheral neuritis may follow rubella.
Rubeola (Red Measles)
Rubeola is a highly contagious, acute viral disease of children. It is transmitted by direct contact with droplets from infected persons and is caused by an RNA-containing paramyxovirus with an incubation period of 7 to 12 days, during which time no symptoms manifest. Prodromal symptoms include high fever (up to 40.5° C [104.9° F]), malaise, enlarged lymph nodes, runny nose, conjunctivitis, and “barking” cough. Within 3 to 4 days, an erythematous maculopapular rash develops over the head and spreads distally over the trunk, extremities, hands, and feet. Early lesions blanch with pressure, followed by a brownish hue that does not blanch as the rash fades. Characteristic pinpoint white spots surrounded by an erythematous ring develop over the buccal mucosa and are known as Koplik spots. These spots precede the rash by 1 to 2 days. The rash then subsides within 3 to 5 days.
Complications associated with measles may be caused by the primary infection or a secondary bacterial infection. Measles encephalitis occurs in about 1 of 800 cases, and most children recover completely. Only a small minority develop permanent brain damage or die. Bacterial complications include otitis media and pneumonia, usually caused by group A hemolytic streptococcus, Haemophilus influenzae, or S. aureus infection.
Measles is prevented by a single vaccination of live attenuated measles virus. There is no specific treatment for measles, and supportive therapy is the same as for rubella. Antibiotic therapy is initiated if secondary bacterial infections develop.
Roseola (Exanthema Subitum)
Roseola is a presumed viral infection of infants between 6 months and 2 years of age, but it can be seen in children as old as 4 years. The incubation period is 5 to 15 days, followed by the sudden onset of fever (38.9° to 40.5° C [102° to 104.5° F]) that lasts for 3 to 5 days. After the fever an erythematous macular rash that lasts about 24 hours develops primarily over the trunk and neck. Children usually feel well, eat normally, and have few other symptoms. Usually no treatment is required.
Chickenpox and Herpes Zoster
Chickenpox (varicella) and herpes zoster (shingles) are produced by the varicella-zoster virus (VZV). VZV is a complex herpes group deoxyribonucleic acid (DNA) virus. The incubation period is 10 to 27 days, averaging 14 days. Productive infection occurs within keratinocytes such that the vesicular lesions occur in the epidermis, and an inflammatory infiltrate is often present. Histologically, VZV lesions form intraepidermal vesicles. Infected keratinocytes degenerate, swell, detach from each other, and often contain inclusions surrounded by a clear halo and a circle of darkly staining chromatin. As the vesicle evolves, polymorphonuclear cells enter the vesicle and can lead to a pustular appearance. The vesicle eventually ruptures and is followed by crust formation. On mucous membranes the vesicles rupture and leave superficial, transient ulcers. Varicella occurs in people not previously exposed to VZV, whereas herpes zoster occurs in partially immune individuals who have had varicella.48
Chickenpox (Varicella): Chickenpox is a disease of early childhood, with 90% of children contracting the disease during the first decade of life. It is a highly contagious virus that is spread by person-to-person contact and airborne droplets. Introduction of an infected person into a household results in a 90% possibility of susceptible persons in the household developing the disease within the incubation period—usually 14 days. Children are contagious for at least 1 day before development of the rash. Transmission of the virus may occur until approximately 5 to 6 days after the onset of the first skin lesions in normal children. In immunocompromised children the virus is recoverable for a longer period, but these children must be considered contagious for at least 7 to 10 days. Chickenpox occurs most commonly in the late winter and early spring. Transmission occurs more readily in temperate climates than in tropical climates.
Healthy children who develop chickenpox have no prodromal symptoms. The first sign of illness may be itching or the appearance of vesicles, usually on the trunk, scalp, or face. The rash later spreads to the extremities. Characteristically, lesions can be seen in various stages of maturation with macules, papules, and vesicles present in a particular area at the same time (Figure 45-9). The vesicular lesions are superficial and can be easily ruptured. New lesions will erupt for 4 to 5 days, until there are approximately 100 to 300 in different stages of development. The vesicles become crusted, with only the crust remaining. Occasionally a vesicle may appear on the palm later in the disease. Although uncommon, ulcerative lesions are sometimes seen in the mouth and, less commonly, on the conjunctiva and pharynx. Fever usually lasts 2 to 3 days and ranges from 38.5° to 40° C [101.3° to 104° F]).
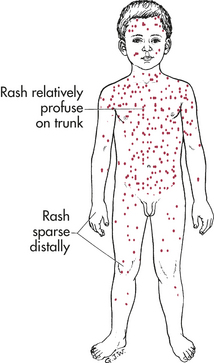
Figure 45-9 Chickenpox. Generalized, polymorphous eruption. (From Wehrle PF, Top FH Sr: Communicable and infectious diseases, ed 9, St Louis, 1981, Mosby.)
Complications are rare in children but more common in adults. They can include transient hematuria (from rupture of vesicles in the bladder), epistaxis, laryngeal edema, and varicella pneumonia. One case of chickenpox produces almost complete immunity against a second attack. Rarely, the fetus may be malformed (congenital varicella syndrome) if chickenpox develops in the mother in the first trimester of pregnancy.49,50 Infants whose mothers have chickenpox at any stage of pregnancy have a higher risk of developing herpes zoster during the first few years of life.
Uncomplicated chickenpox requires no specific therapy. Baths, wet dressings, and oral antihistamines are occasionally helpful to relieve itching and to prevent secondary infection as a result of scratching. Oral antistaphylococcal drugs should be given if secondary bacterial infection is present. Zoster immune globulin may be administered to immunodeficient individuals if given within 72 hours after exposure to chickenpox. Oral antiviral drugs may be valuable in reducing symptoms in otherwise healthy children as well as in immunosuppressed or other select groups of children.51
Chickenpox can be prevented with a safe and effective vaccine (see Chapter 9, Table 9-13).
Herpes Zoster: Although herpes zoster (shingles) occurs mainly in adults, approximately 5% of cases are in children younger than 15 years.52 A wild-type VZV (a type not included in the vaccine strains) can cause herpes zoster. The course of the disease in children with an immune defect is more complicated and requires treatment with antiviral agents.53 The chickenpox virus persists for life in sensory nerve ganglia and reactivates to cause herpes zoster. The eruption of zoster consists of groups of vesicles situated on an inflammatory base and following the course of a sensory nerve. Common dermatomal distribution in young children is cervical and sacral.54 The base of the lesions often appears hemorrhagic, and some of the lesions may become necrotic and ulcerative. In addition to the localized eruption, there are commonly a few scattered lesions resembling chickenpox. Therapy is similar to that for chickenpox unless it is ophthalmic or disseminated zoster, for which systemic antiviral treatment and (when the eye is involved) a referral to an ophthalmologist are indicated. The herpes zoster vaccine has been approved for use in persons 60 years of age and older.55 A tetravalent vaccine against measles, mumps, rubella, and varicella-zoster viruses (MMRV) is available for infants and children.56
Smallpox
Smallpox (variola) is a highly contagious and deadly but preventable disease. It is caused by poxvirus variolae. Because of worldwide mass immunization, the world is now virtually free of smallpox.57 Concerns regarding smallpox as a weapon of bioterrorism have led to vaccination programs for the military and for selected civilian populations. The U.S. government has an adequate supply of smallpox vaccine to vaccinate the population in the event of an emergency.58
INSECT BITES AND PARASITES
Insect bites and infestations are common causes of skin disorders in children and adults. Skin damage occurs by various mechanisms, including trauma of bites and stings, allergic reactions, transmission of disease, injection of substances that cause local or systemic reactions, and inflammatory reactions from retained mouthparts.
Scabies
Scabies is a contagious disease caused by the itch mite, Sarcoptes scabiei (Figure 45-10, A). It is transmitted by personal contact (see Chapter 24) and by infected clothing and bedding. Scabies is often epidemic in areas of overcrowded housing, poor sanitation, or in long-term care institutions. Scabies is often associated with immunocompromised individuals, such as those with human T-cell leukemia/lymphoma virus I (HTLV-1) and HIV.59 Infestation is initiated by a female mite that tunnels into the stratum corneum, depositing eggs and creating a burrow several millimeters to 1 cm long. Over a 3-week period, the eggs mature into adult mites, which sometimes can be recognized as tiny dots at the end of intact burrows.
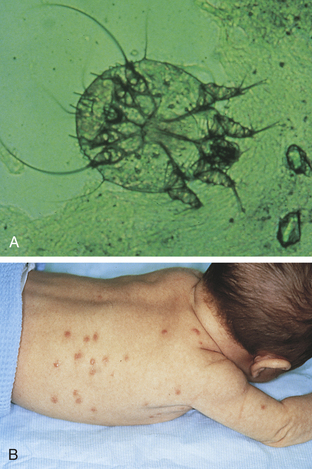
Figure 45-10 Scabies. A, Scabies mite, as seen clinically when removed from its burrow. B, Characteristic scabies bites. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
Symptoms appear 3 to 5 weeks after infestation. The primary lesions are burrows, papules, and vesicular lesions, with severe itching that worsens at night. Two or three bites (commonly referred to as “breakfast, lunch, and dinner”) usually appear in a line on exposed areas of the skin. Itching is thought to be related to sensitization to the larval stages of the parasite. In older children and adults the lesions occur in the webs of fingers, axillae, and creases of the arms and wrists; along the belt line; and around the nipples, genitalia, and lower buttocks. Infants and young children have a different pattern of distribution, with involvement of the palms, soles, head, neck, and face (see Figure 45-10, B). Secondary infections and crusting develop from scratching and eczematous changes.
Norwegian scabies (crusted scabies) is a relatively rare widespread scabetic infestation with an affinity for severely mentally retarded persons, those who are unable to effectively scratch, or in immunocompromised individuals. It is highly contagious and is characterized by heavily crusted lesions on the scalp, elbows, knees, palms, soles, and buttocks.60
Diagnosis of scabies is made by observation of the tunnels and burrows and scraping of the skin with microscopic examination of the mite or its eggs or feces. Treatment is the application of permethrin cream, a scabicide. Generalized scabies is treated with oral ivermectin.61 Even with elimination of all viable scabies microorganisms, itching may persist for 10 days or longer. All clothing and linens should be washed and dried in hot cycles or dry-cleaned.
Pediculosis (Lice Infestation)
The three known types of human lice are: (1) the head louse (Pediculus capitis), (2) the body louse (Pediculus corporis), and (3) the crab or pubic louse (Phthirus pubis). They are highly contagious parasites that survive by sucking blood. The female louse reproduces every 2 weeks, producing hundreds of nits as newly hatched lice mate with old lice. The mouthparts are shaped for piercing and sucking and attach to the skin while feeding. When piercing the skin, the louse secretes a toxic saliva; the mechanical trauma and toxin produce a pruritic dermatitis. Head and body lice are acquired by personal contact, combs, or brushes. Crab lice are spread by body contact, such as contact with an infected adult (see Chapter 24). Sharing clothing is also a common source of transmission.62
Itching is the major symptom of lice infestation. In head lice infestation the ova attach to hairs above the ears and in the occipital region. The primary lesion of the body louse is a pinpoint red macule, papule, or wheal with a hemorrhagic puncture site. The primary lesion often is not seen because it is masked by excoriations, wheals, and crusts. The crab louse is found on pubic hairs but also may involve other body hair such as eyelashes, mustache, beard, and axillae. Young children particularly may become infected with crab lice on their eyebrows or eyelashes.
The live louse, 2 to 3 mm long, is rarely observed, although the ova, or nits, can be observed as oval, yellowish pinpoint specks fastened to a hair shaft. The ova fluoresce under an ultraviolet light (Wood lamp) and can be best observed with a microscope. Infestations can be treated with a topical pediculicide (i.e., permethrin) or oral ivermectin.63 All clothes, towels, bedding, combs, and brushes should be washed and dried in hot air or boiled, or the clothes should be ironed. Individuals who have personal contact also should be treated.
Fleas
Young children are very susceptible to flea bites, and the most common are the bites of cat, dog, and human fleas.64 Bites occur in clusters along the arms and legs or where clothing fits tightly. The bite produces an urticarial wheal with a central hemorrhagic puncture (Figure 45-11). An immune response to flea bite proteins causes a chronic papular urticaria.65 Tungiasis, caused by sand fleas, causes chronic morbidity in impoverished communities in Latin America, the Caribbean, and Sub-Saharan Africa.66 Treatment includes spraying carpets, crevices, and furniture with malathion or lindane powder. Infected animals should be treated, and clothes and bedding should be washed in hot water. There is no specific treatment for tungiasis, but topical pesticides can reduce the number of lesions from embedded fleas.

Bedbugs
The common bedbug, Cimex lectularius, is a blood-sucking nocturnal parasite of man. Chickens, bats, and some domestic animals are the other hosts for this bug.67 Bedbugs live in the crevices and cracks of floors, walls, and furniture and in bedding or furniture stuffing. They are 3 to 5 mm long and reddish brown. Bedbugs emerge to feed in darkness and attach to the skin to suck blood. Feeding occurs for 5 to 15 minutes, then the bedbug leaves. It will move long distances to search for food and can travel from house to house.
If the host has not been previously sensitized, the only symptom is a red macule that develops into a nodule, lasting up to 14 days. In sensitized children and adults, pruritic wheals, papules, and vesicles may form (Figure 45-12). These lesions respond to antihistamines or corticosteroids. Secondary infections require antibiotic treatment. Bedbugs are eliminated by inspecting and cleaning or disposing of bedding, mattresses, furniture and other contaminated items, and by using applications of approved insecticides, usually by a professional.68

HEMANGIOMAS AND VASCULAR MALFORMATIONs
Vascular anomalies are frequent tumors of early infancy and can be categorized as either hemangiomas or vascular malformations.69,70
Hemangiomas
Hemangiomas are benign tumors that form from the rapid growth of vascular endothelial cells, which results in formation of extra blood vessels. Hemangiomas can be superficial or deep. Superficial hemangiomas are known as strawberry hemangiomas and deep lesions are known as cavernous hemangiomas. The etiology may be related to embolization of fetal placental endothelial cells related to placental trauma or loss of placental angiogenic inhibitor of placental and maternal origin.71 There is proliferation of mast cells that are thought to promote the angiogenesis. Infiltration of fat cells, fibrosis, and the rich vascular network give the lesions a firm, rubbery feel. Females are affected more often than males. About 30% of hemangiomas are apparent at birth, with most emerging during the first few weeks of life; they grow rapidly during the first few years, then shrink or involute during childhood years. With involution the lesions become darker in color and then gradually turn to a flesh color. There may be some residual telangiectasia. Most require no treatment depending on location. Hemangiomas located over the eye, ear, nose, mouth, urethra, or anus may require treatment because they interfere with function and have a higher risk for infection or injury. Systemic or intralesional steroids are the treatment of choice. Interferons, vincristine, cyclophosphamide, and radiotherapy can suppress angiogenesis. Cryosurgery, laser surgery, sclerotherapy, and embolization are also alternative treatment options.71–73
Strawberry hemangiomas are distinct superficial hemangiomas that may be present at birth but usually emerge 3 to 5 weeks after birth. They proliferate and become bright red and elevated with minute capillary projections that give them a strawberry appearance. Only one lesion is usually present, and it is located on the head and neck area or trunk (Figure 45-13). After the initial growth, the lesion grows at the same rate as the child and then starts to involute at 12 to 16 months of age. Approximately 90% of strawberry hemangiomas involute by 5 to 6 years of age, usually without scarring.71

Figure 45-13 Strawberry hemangioma. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
Cavernous (congenital) hemangiomas are present at birth and have larger and more mature vessels within the lesion than strawberry hemangiomas. Some lesions, however, are composed of a mixture of strawberry and cavernous hemangiomas. They appear primarily on the head and neck, are bluish red, and have less distinct borders (Figure 45-14). Cavernous hemangiomas grow rapidly up to 6 months of age and mature by 1 year of age. A period of involution begins and proceeds for 6 to 12 months, with complete involution by 2 to 3 years in 30% of children and by 9 years of age in 90% of children.

Vascular Malformations
Vascular malformations are congenital anomalies of blood vessels present at birth but may not be apparent for several years. They grow proportionately with the child and never regress.70 The malformations occur equally among males and females. Occasionally they expand rapidly, particularly during the hormonal changes of puberty or pregnancy and in association with trauma. Vascular malformations are classified as low flow or high flow. Low-flow malformations involve capillaries, veins, and lymphatics. High-flow malformations involve arteries. In addition to locations within the skin they may involve the gastrointestinal tract, bone (Maffucci syndrome or Sturge-Weber syndrome), facial capillary malformation, skin, vascular malformation of the eye, and vascular malformation of the brain (leptomeningeal hemangioma).74 Overgrowth syndromes can occur with either high- or low-flow malformations, with overgrowth of the underlying structures (i.e., legs, arms, facial bones). The most common vascular malformation is nevus flammeus (port-wine stain) and salmon patches (stork bite, angel kiss).
Port-wine (nevus flammeus) stains are congenital malformations of the dermal capillaries. The lesions are flat, and their color ranges from pink to dark reddish purple. They are present at birth or within a few days after birth and do not fade with age. Involvement of the face and other body surfaces is common, and the lesions may be large (Figure 45-15). During adolescence and later adult years, the port-wine stain may become papular and cavernous. Treatments using cryosurgery or tattooing are not very satisfactory. The pulsed dye laser is the treatment of choice to successfully lighten the color and flatten the more nodular and cavernous lesions.75 Waterproof cosmetics may be used to cover the lesions.
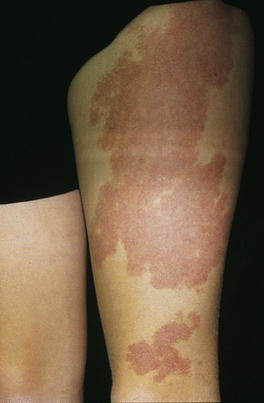
Figure 45-15 Capillary malformation in a child. (Courtesy Department of Dermatology, School of Medicine, University of Utah.)
Salmon patches are macular pink lesions present at birth and located on the nape of the neck, forehead, upper eyelids, or nasolabial fold. They are a more superficial variant of nevus flammeus and one of the most common congenital malformations in the skin. The pink color results from distended dermal capillaries, and 95% fade by 1 year of age. Those located at the nape of the neck may persist for a lifetime, but generally do not present a cosmetic problem.
OTHER SKIN DISORDERS
Miliaria is a dermatosis commonly seen in infants. It is characterized by a vesicular eruption after prolonged exposure to perspiration, with subsequent obstruction of the eccrine ducts. There are two forms of miliaria: miliaria crystallina and miliaria rubra. In miliaria crystallina, ductal rupture occurs within the stratum corneum and appears as 1- to 2-mm clear vesicles without erythema. They rupture within 24 to 48 hours and leave a white scale. In miliaria rubra the ductal rupture occurs in the lower epidermis, with inflammatory cells attracted to the site of the rupture. Miliaria rubra (prickly heat) is characterized by 2- to 4-mm discrete erythematous papules or papulovesicles (Figure 45-16). Both forms may become secondarily infected, requiring treatment with systemic antibiotics. The key to management is avoidance of excessive heat and humidity, which cause sweating. Light clothing, cool baths, and air conditioning assist in keeping the skin surface dry and cool.

Erythema Toxicum Neonatorum
Erythema toxicum neonatorum (toxic erythema of the newborn) is a benign, erythematous accumulation of macules, papules, or pustules that appear at birth or 3 to 4 days after birth. The lesions first appear as a blotchy, macular erythematous rash. The macules vary from 1 mm to 1 cm. When papules or pustules develop, they are light yellow or white and 1 to 3 mm in diameter. There may be few or several hundred lesions, and any body surface can be affected, with the exception of the palms and soles, where there are no pilosebaceous follicles. The cause of the lesion is unknown but it may be related to an innate immune response to the first commensal microflora with release of mast cell mediators.76 It is self-limiting and resolves spontaneously within a few weeks of birth. No treatment is required.
Toxic Epidermal Necrolysis and Stevens-Johnson Syndrome
Toxic epidermal necrolysis (TEN) and Stevens-Johnson syndrome (SJS) are rare, severe drug reactions with widespread epidermal apoptosis and detachment with mortality rates between 20% and 60%.77 They are more common in adults but their incidence is increasing in children. The hypersensitivity to drugs includes sulfonamides, nonsteroidal anti-inflammatory agents, and anticonvulsants (i.e., phenytoin). Drug-specific cytotoxic T cells are involved in the immunopathology.78 The onset of skin eruptions is preceded by malaise, anorexia, fever, and mild inflammation of the eyelids, conjunctiva, mouth, or genitalia. Erythema with tenderness is first described in the axillae and groin, extending over the body surface. Blisters and bullae form, and the entire epidermis may be shed, leaving open, weeping, painful areas of underlying skin. Complications include dehydration, protein loss, altered temperature regulation, and organ failure. About one third of children have pulmonary complications.79 A severity of illness score for toxic epidermal necrolysis (SCORTEN) syndrome guides treatment and predicts mortality.80 TEN must be confirmed by skin biopsy to differentiate from staphylococcal scalded skin syndrome (SSSS) and acute graft-versus-host disease. Skin biopsy shows full-thickness epidermal necrosis and subepidermal blister formation.81 Treatment requires intensive burn equivalent management, preferably in a burn unit. Treatment with corticosteroids and intravenous immunoglobulin need further study, which is difficult because the disease is so rare.82 Intravenous immunoglobulin may protect keratinocytes from apoptosis and oncosis from pathogenic autoantibodies.83 The offending drug must be discontinued.
Acne conglobata 1681
Acne vulgaris 1680
Atopic dermatitis (AD) 1681
Bedbugs 1689
Bullous impetigo 1683
Cavernous (congenital) hemangiomas 1690
Chickenpox 1687
Diaper dermatitis 1682
Erythema toxicum neonatorum 1692
Flea bites 1689
Impetigo 1683
Inflammatory acne 1680
Miliaria 1692
Miliaria crystallina 1692
Miliaria rubra 1692
Molluscum contagiosum 1685
Noninflammatory acne 1680
Norwegian scabies 1689
Port-wine (nevus flammeus) stains 1691
Roseola 1687
Rubella 1686
Rubeola 1686
Salmon patches 1691
Scabies 1688
Smallpox (variola) 1688
Staphylococcal scalded-skin syndrome (SSSS) 1684
Stevens-Johnson syndrome (SJS) 1692
Strawberry hemangiomas 1690
Thrush 1685
Tinea capitis 1684
Tinea corporis 1685
Tinea pedis 1684
Toxic epidermal necrolysis (TEN) 1692
Vesicular impetigo 1683
Zoster 1688
REFERENCES
1. Pochi PE et al: Report of the consensus conference on acne classification, J Am Acad Dermatol 24(3):495, 1991.
2. Zouboulis, C.C., et al. Sexual hormones in human skin. Horm Metab Res. 2007;39(2):85–95.
3. Melnik, B., Jansen, T., Grabbe, S. Abuse of anabolic-androgenic steroids and bodybuilding acne: an underestimated health problem. J Dtsch Dermatol Ges. 2007;5(2):110–117.
4. Strauss, J.S., et al. Guidelines for acne vulgaris management. J Am Acad Dermatol. 2007;56(4):651–663.
5. Krakowski, A.C., Stendardo, S., Eichenfield, L.F. Practical considerations in acne treatment and the clinical impact of topical combination therapy. Pediatr Dermatol. 2008;25(Suppl 1):1–14.
6. Callender, V.D. Acne in ethnic skin: special considerations for therapy. Dermatol Ther. 2004;17(2):184–195.
7. Horii, K.A., et al. Atopic dermatitis in children in the United States, 1997-2004: visit trends, patient and provider characteristics, and prescribing patterns. Pediatrics. 2007;120(3):e527–e534.
8. Bonness, S., Bieber, T. Molecular basis of atopic dermatitis. Curr Opin Allergy Clin Immunol. 2007;7(5):382–386.
9. Nicol, N.H., Boguniewicz, M. Successful strategies in atopic dermatitis management. Dermatol Nurs. 2008:3–18.
10. Elias, P.M. Skin barrier function. Curr Allergy Asthma Rep. 2008;8(4):299–305.
11. Boguniewicz, M., Leung, D.Y. Atopic Dermatitis. J Allergy Clin Immunol. 2006;117(Suppl 2 Mini-Primer):S475–S480.
12. Howell, M.D., et al. Th2 cytokines act on S11/A11 to downregulate keratinocyte differentiation. J Invest Dermatol. 2008;128(9):2248–2258.
13. Chan, L.S. Atopic dermatitis in 2008. Curr Dir Autoimmun. 2008;10:76–118.
14. Lipozenci, J., Wolf, R. Atopic dermatitis: an update and review of the literature. Dermatol Clin. 2007;25(4):605–612. [x].
15. McGrath, J.A. Filaggrin and the great epidermal barrier grief. Australas J Dermatol. 2008;49(2):67–73.
16. Tominaga, M., Ogawa, H., Takamori, K. Possible roles of epidermal opioid systems in pruritus of atopic dermatitis. J Invest Dermatol. 2007;127(9):2228–2235.
17. Yosipovitch, G., Papolu, A.D. What causes itch in atopic dermatitis? Curr Allergy Asthma Rep. 2008;8(4):306–311.
18. Brenninkmeijer, E.E., et al. Diagnostic criteria for atopic dermatitis: a systematic review. Br J Dermatol. 2008;158(4):754–765.
19. Boguniewicz, M., et al. A multidisciplinary approach to evaluation and treatment of atopic dermatitis. Semin Cutan Med Surg. 2008;27:115–127.
20. Ong, P.Y., Boguniewicz, M. Atopic dermatitis. Prim Care. 2008;35(1):105–117. [vii].
21. Runeman, B. Skin interaction with absorbent hygiene products. Clin Dermatol. 2008;26(1):45–51.
22. Cole, C., Gazewood, J. Diagnosis and treatment of impetigo. Am Fam Physician. 2007;75(6):859–864.
23. Nishifuji, K., Sugai, M., Amagai, M. Staphylococcal exfoliative toxins: “molecular scissors” of bacteria that attack the cutaneous defense barrier in mammals. J Dermatol Sci. 2008;49(1):21–31.
24. Rudy, S.J. Superficial fungal infections in children and adolescents. Nurse Prac Forum. 1999;19(2):56.
25. Ilyas, M., Tolaymat, A. Changing epidemiology of acute post-streptococcal glomerulonephritis in Northeast Florida: a comparative study. Pediatr Nephrol. 2008;23(7):1101–1106.
26. Bernard, P. Management of common bacterial infections of the skin. Curr Opin Infect Dis. 2008;21(2):122–128.
27. Hacker, S.M. Common infections of the skin: characteristics, causes, and cures. Postgrad Med. 1994;96(2):43.
28. Blyth, M., Estela, C., Young, A.E. Severe staphylococcal scalded skin syndrome in children. Burns. 2008;34(1):98–103.
29. Nishifuji, K., Sugai, M., Amagai, M. Staphylococcal exfoliative toxins: “molecular scissors” of bacteria that attack the cutaneous defense barrier in mammals. J Dermatol Sci. 2008;49(1):21–31.
30. Patel, G.K. Treatment of staphylococcal scalded skin syndrome. Expert Rev Anti Infect Ther. 2004;2(4):575–587.
31. Elewski, B.E. Cutaneous mycoses in children. Br J Dermatol. 1996;134(Suppl 46):7.
32. Andrews, M.D., Burns, M. Common tinea infections in children: Am Fam Physician. 2008;77(1):1415–1420.
33. White, J.M., Higgins, E.M., Fuller, L.C. Screening for asymptomatic carriage of Trichophyton tonsurans in household contacts of patients with tinea capitis: results of 209 patients from South London. J Eur Acad Dermatol Venereol. 2007;21(8):1061–1064.
34. Williams, J.V., et al. Semiquantitative study of tinea capitis and the asymptomatic carrier state in inner-city school children. Pediatrics. 1995;96(2 Pt 1):265.
35. Gonzalez, U., et al. Systemic antifungal therapy for tinea capitis in children. Cochrane Database Syst Rev. (4):2007. [CD004685].
36. Chan, Y.C., Friedlander, S.F. New treatments for tinea capitis. Curr Opin Infect Dis. 2004;17(2):97–103.
37. Pereira, B., et al. Exuberant molluscum contagiosum as a manifestation of the immune reconstitution inflammatory syndrome. Dermatol Online J. 2007;13(2):6.
38. Prasad, S.M. Molluscum contagiosum. Pediatr Rev. 1996;17(4):118.
39. Scheinfeld, N. Treatment of molluscum contagiosum: a brief review and discussion of a case successfully treated with adapelene. Dermatol Online. 2007;13(3):15.
40. Davidkin, I., et al. Etiology of measles- and rubella-like illnesses in measles, mumps, and rubella-vaccinated children. J Infect Dis. 1998;178(6):1567.
41. Egami, T., Egami, K., Tanoue, A. Study of antibody titres after measles vaccination: fever within 7 days of vaccination and efficacy of booster doses. Arch Dis Child. 2008;93(4):319–320.
42. DeStefano, F. Vaccines and autism: evidence does not support a causal association. Clin Pharmacol Ther. 2007;82(6):756–759.
43. DeStefano, F., Thompson, W.W. MMR vaccine and autism: an update of the scientific evidence. Expert Rev Vaccines. 2004;3(1):19–22.
44. Kennedy, R.C., Byers, V.S., Marchalonis, J.J. Measles virus infection and vaccination: potential role in chronic illness and associated adverse events. Crit Rev Immunol. 2004;24(2):129–156.
45. Centers for Disease Control and Prevention (CDC). Progress in global measles control and mortality reduction. MMWR Morb Mortal Wkly Rep. 2007;56(47):1237–1241.
46. Update: global measles control and mortality reduction—worldwide, 1991-2001. MMWR. 2003;52(20):471–475.
47. Best, J.M. Rubella. Semin Fetal Neonatal Med. 2007;12(3):182–192.
48. Johnson, R., et al. Prevention of herpes zoster and its painful and debilitating complications. Int J Infect Dis. 2007;11(Suppl 2):S43–S48.
49. Daley, A.J., Thrope, S., Garland, S.M. Varicella and the pregnant woman: prevention and management. Aust N Z J Obstet Gynaecol. 2008;48(1):26–33.
50. Pastuszak, A.L., et al. Outcome after maternal varicella infection in the first 20 weeks of pregnancy. N Engl J Med. 1994;330(13):901.
51. Breuer, J., Whitley, R. Varicella zoster virus: natural history and current therapies of varicella and herpes zoster. Herpes. 2007;14(Suppl 2):25–29.
52. Feder, H.M., Jr., Hoss, D.M. Herpes zoster in otherwise healthy children. Pediatr Infect Dis J. 2004;23(5):451–457.
53. Ahmed, A.M., et al. Managing herpes zoster in immunocompromised patients. Herpes. 2007;14(2):32–36.
54. Leung, A.K., Robson, W.L., Leong, A.G. Herpes zoster in childhood. J Pediatr Health Care. 2006;20(5):300–303.
55. Woolery, W.A. Herpes zoster vaccine. Geriatrics. 2008;63(10):6–9.
56. Dhillon, S., Curran, M.P. Live attenuated measles, mumps, rubella, and varicella zoster virus vaccine. Paediatr Drugs. 2008;10(5):337–347.
57. Kman, N.E., Nelson, R.N. Infectious agents of bioterrorism: a review for emergency physicians. Emerg Med Clin North Am. 2008;26(2):517–547.
58. Metzger, W., Mordmueller, B.G. Vaccines for preventing smallpox. Cochrane Database Syst Rev. (3):2007. [CD004913].
59. Chosidow, O. Scabies and pediculosis. Lancet. 2000;355(9206):819.
60. Walton, S.F., et al. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune resonse in crusted scabies. Br J Dermatol. 2008;158(6):1247–1255.
61. Mounsey, K.E., et al. Scabies: molecular perspectives and therapeutic implications in the face of emerging drug resistance. Future Microbiol. 2008;3(1):57–66.
62. Burkhart, C.N., Burkhart, C.G. Fomite transmission in head lice. J Am Acad Dermatol. 2007;56(6):144–147.
63. Strong, M., Johnstone, P.W. Interventions for treating scabies. Cochrane Database Syst Rev. (3):2007. [CD000320].
64. Howard, R., Frieden, I.J. Papular urticaria in children. Pediatr Dermatol. 1996;13(3):246.
65. Cuéllar, A., et al. Functional dysregulation of dendritic cells in patients with popular urticaria caused by fleabite. Arch Dermatol. 2007;143(11):1415–1419.
66. Kehr, J.D., et al. Morbidity assessment in sand fleas disease (tungiasis). Parasitol Res. 2007;100(2):413–421.
67. Cestari, T.F., Martignago, B.F. Scabies, pediculosis, bedbugs, and stinkbugs: uncommon presentations. Clin Dermatol. 2005;23(6):545–554.
68. Ter Poorten, M.C. Prose NS The return of the common bedbug. Pediatr Dermatol. 2005;22(3):183–187.
69. Buckmiller, L.M. Update on hemangiomas and vascular malformations. Curr Opin Otolaryngol Head Neck Surg. 2004;12(6):476–487.
70. Willenberg, T., Baumgartener, T. Vascular birthmarks. Vasa. 2008;37(1):5–17.
71. Atherton, D.J. Infantile haemangiomas. Early Hum Dev. 2006;82(12):789–795.
72. Musumeci, M.L., et al. Management of cutaneous hemangiomas in pediatric patients. Cutix. 2008;81(4):315–322.
73. Song, J.K., Niimi, Y., Berenstein, A. Endovascular treatment of hemangioma. Neuroimaging Clin N Am. 2007;17(2):165–173.
74. Comi, A.M. Update on Sturge-Weber syndrome: diagnosis, treatment, quantitative measures, and controversies. Lymphat Res Biol. 2007;5(4):257–264.
75. Bernstein, E.F. Treatment of a resistant port-wine stain with a new variable pulse-duration pulsed-dye laser. J Cosmet Dermatol. 2008;7(2):139–142.
76. Nelson, A., et al. Urticaria neonatorum: accumulation of tryptase-expressing mast cells in the skin lesions of newborns with erythema toxicum. Pediatr Allergy Immunol. 2007;18(8):652–658.
77. Dorafshar, A.H., et al. Antishear therapy for toxic epidermal necrolysis: an alternative treatment approach. Plast Reconstr Surg. 2008;122(1):154–160.
78. Borchers, A.T., et al. Stevens-Johnson syndrome and toxic epidermal necrolysis. Autoimmun Rev. 2008;7(8):598–605.
79. Kim, M.J., Lee, K.Y. Bronchiolitis obliterans in children with Stevens-Johnson syndrome: follow-up with high resolution CT. Pediatr Radiol. 1996;26(1):22.
80. Basuji-Garin, S., et al. SCORTEN: a Severity-of-Illness Score for Toxic Epidermal Necrolysis. Inves Dermatol. 2000;115(5):149–153.
81. Rzany, B., et al. Histopathological and epidemiological characteristics of patients with erythema exudativum multiforme major, Stevens-Johnson syndrome and toxic epidermal necrolysis. Br J Dermatol. 1996;135(1):6.
82. Abood, G.J., Nickoloff, B.J., Gamelli, R.L. Treatment strategies in toxic epidermal necrolysis syndrome: where are we at? J Burn Care Res. 2008;29(1):269–276.
83. Michael, D., Grando, S.A. Novel mechanism for therapeutic action of IVIg in autoimmune blistering dermatoses. Curr Dir Autoimmun. 2008;10:333–343.