Chapter 29 The maxillary antra
INTRODUCTION
The maxillary antra, because of their close proximity to the upper teeth, are the most important of the paranasal sinuses in dentistry. Nowadays the imaging modalities of choice to investigate possible disease within the antra are computed tomography (CT), cone beam CT and magnetic resonance (MR) (see Ch. 19). However, as the antra are often imaged on conventional dental radiographs, as well as on certain skull views, clinicians still need to know:
• The anatomy of the antra, including their shape, size, normal variations and related structures.
• How the antra are represented normally on conventional dental and skull radiographs and how these radiographs are assessed.
Similar radiographic changes can be seen in the other paranasal sinuses — frontal, ethmoidal and sphenoidal. They are of less clinical relevance in dentistry and are discussed only briefly.
NORMAL ANATOMY
The maxillary antrum or sinus is an approximately pyramidal cavity. It contains air, is lined by mucoperiosteum with a pseudostratified ciliated columnar epithelium and occupies most of the body of the maxillary bone. It is present at birth, but at that stage it is little more than a slit-like out-pouching of the nasal cavity. It grows rapidly by a process known as pneumatization during the eruption of the deciduous teeth and reaches about half its adult size by three years of age. The final size of the antra (like the other air sinuses) is very variable.
Pneumatization in adulthood causes further changes in antral shape and size. The cavity often enlarges downwards into the alveolar process or laterally into the body of the zygoma. The internal surface can be smooth or ridged with prominent bony septa. The lateral wall contains canals or grooves for the nerves and blood vessels supplying the upper posterior teeth.
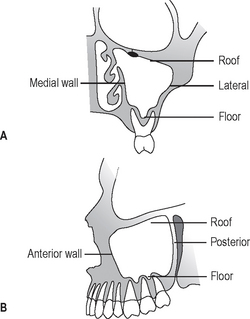
The main anatomical parts of the antra (see Fig. 29.1) can be divided into:
• A roof or upper border, bounded by the orbit
• A medial wall, bounded by the nasal cavity
• A posterior wall, related to the pterygopalatine fossa
• A lateral wall, related to the zygoma and cheek
• An anterior wall, related to the cheek
• A floor, related to the apices of the upper posterior teeth.
NORMAL APPEARANCE OF THE ANTRA ON CONVENTIONAL RADIOGRAPHS
An antrum appears radiographically as a radiolucent cavity in the maxilla, with well-defined, dense, corticated radiopaque margins or walls. In general, the larger the cavity the more radiolucent it will appear. The internal bony septa and blood vessel canals in the walls all produce their own shadows. The thin epithelial lining is not normally seen. The different parts of the antra shown on conventional dental and skull radiographs are summarized in Table 29.1. Typical normal radiographic appearances are shown in Figures 29.2-29.4. In addition a suggested systematic approach to viewing the antra on the 0° OM is shown in Figure 29.4.
Table 29.1 Summary of the different parts of the antra shown on conventional dental and skull radiographs
| Area of antrum shown | Radiographic projection |
|---|---|
| Floor | |
| Main antral cavity | |
| Lower aspect of antral cavity | |
| Posterior wall | |
| Anteromedial wall | |
| Lateral wall | 0° OM |
| Roof | 0° OM |
| Relationship with upper posterior teeth |
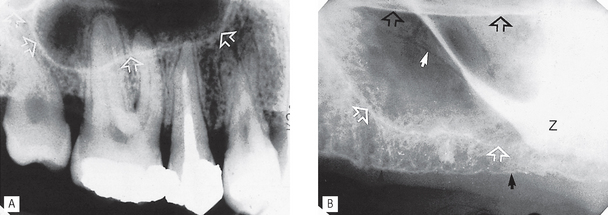
Fig. 29.2 A Periapical of  showing the usual appearance of the floor (arrowed) and base of the antral cavity in relation to the upper posterior teeth in a dentate adult. B Periapical of
showing the usual appearance of the floor (arrowed) and base of the antral cavity in relation to the upper posterior teeth in a dentate adult. B Periapical of  showing the various normal anatomical structures evident in an edentulous adult. These include: the floor of the antrum (white open arrows), the floor of the nasal cavity (black open arrows), the inferior surface of the alveolar ridge (black solid arrows), radiolucent neurovascular channels in the antral wall (solid white arrow) and the zygomatic buttress (Z).
showing the various normal anatomical structures evident in an edentulous adult. These include: the floor of the antrum (white open arrows), the floor of the nasal cavity (black open arrows), the inferior surface of the alveolar ridge (black solid arrows), radiolucent neurovascular channels in the antral wall (solid white arrow) and the zygomatic buttress (Z).

Fig. 29.3 Panoramic radiograph showing the usual appearance of the antral floor, medial and posterior walls. These have been drawn in on the patient’s LEFT side and are arrowed on the RIGHT side.
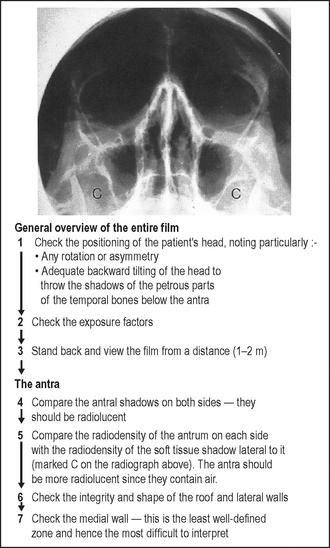
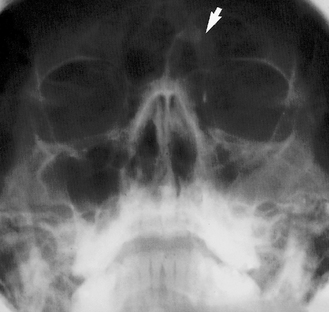
Fig. 29.4 Standard occipitomental (0° OM) showing the normal radiolucent appearance of the antral cavities together with a suggested systematic approach for examining the antra. Note: Swelling of the soft tissues of the cheek overlying an antrum may cause that antrum to appear opaque when compared to the other side, but it will still be radiolucent when compared with the adjacent cheek shadow.
ANTRAL DISEASE
The major pathological conditions that can affect the antra, directly or indirectly, include:
• Other bone abnormalities (see Ch. 32)
These various disease entities can result in the following radiological changes:
• Total or partial opacity/obliteration of the main antral cavity
• Alteration in the integrity of the antral walls, including discontinuity as a result of a fracture or destruction by an intrinsic or extrinsic tumour
• Alteration in the antral outline, including expansion or compression caused by an intrinsic or extrinsic lesion or disease process
INVESTIGATION AND APPEARANCE OF DISEASE WITHIN THE ANTRA
Various imaging modalities can be used to investigate possible disease within the antra, depending on their availability. These include:
• Computed tomography (CT) — currently recommended by the Royal College of Radiologists in the UK
• Multidirectional (spiral) tomography
• Dental panoramic radiography
Appearances of antral diseases using various imaging modalities are shown in Figures 29.5-29.23.
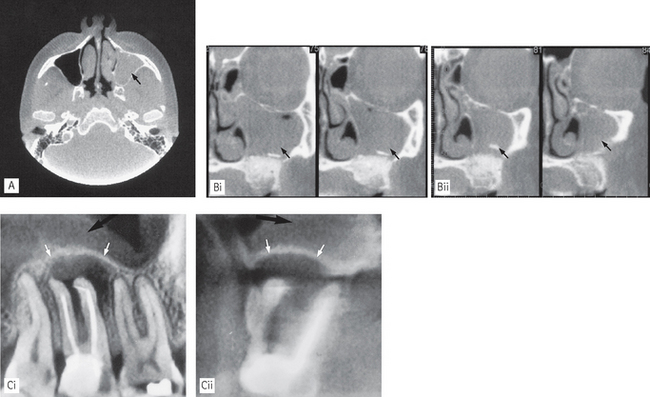
Fig. 29.5 Examples of antral infection/inflammation shown using cone beam CT. A Axial scan and B series of coronal images showing total opacity of the antrum on one side (arrowed).
(Reproduced with kind permission of Imaging Sciences International, Inc.) C (i) Sagittal and (ii) coronal images showing apical infection associated with  that has resulted in re-modelling of the antral floor creating the antral halo appearance (white arrows), with associated mucosal thickening (black arrows) (kindly provided by Prof D. Benn).
that has resulted in re-modelling of the antral floor creating the antral halo appearance (white arrows), with associated mucosal thickening (black arrows) (kindly provided by Prof D. Benn).
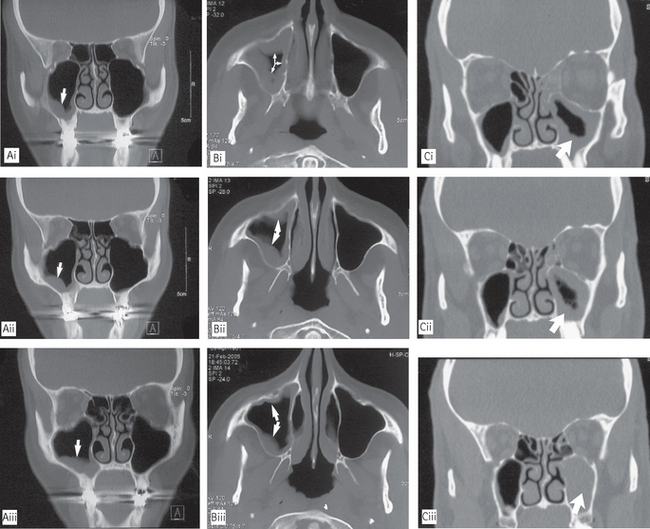
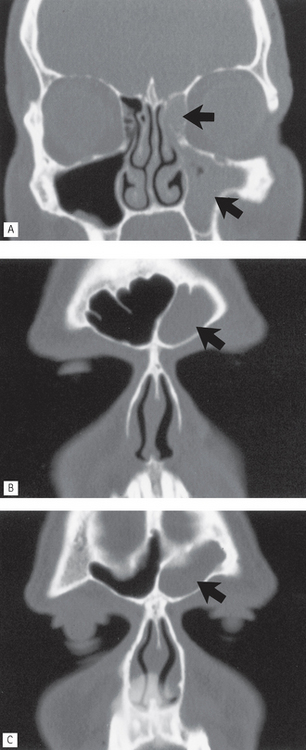
Fig. 29.6 Various appearances of the effects of chronic sinusitis shown on CT. A Contiguous coronal CT scans showing mucosal thickening in the base of the antrum (arrowed). B Contiguous axial CT scans showing mucosal thickening on the medial and lateral walls of the antrum (arrowed). C Contiguous coronal CT scans showing mucosal thickening and total opacity of the antrum (arrowed).
(kindly provided by Drs J. Kabala and J. Luker)
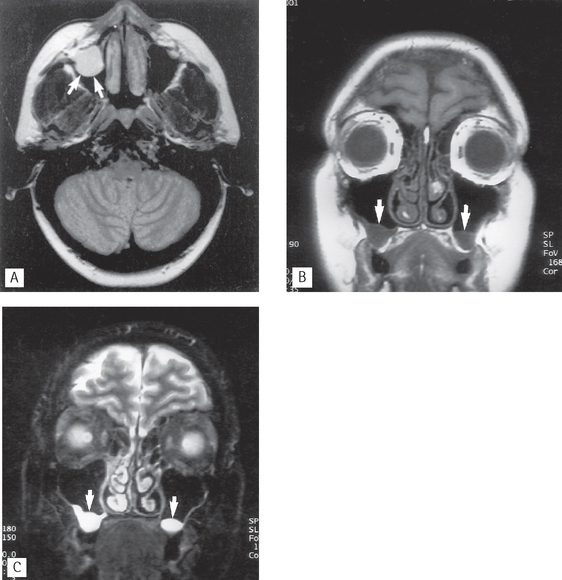
Fig. 29.7 Various appearances of the effects of chronic sinusitis shown on MR. A Axial MR scan showing a round antral mucous retention cyst (arrowed) arising from the anterolateral wall. B T1-weighted and C T2-weighted coronal MR images of the same patient with bilateral mucosal retention cysts (arrowed)
(kindly provided by Drs J. Kabala and J. Luker).

Fig. 29.8 A 2mm-thick Scanora® spiral tomographic cross-sectional image showing a totally opaque chronically infected right antrum (arrowed).
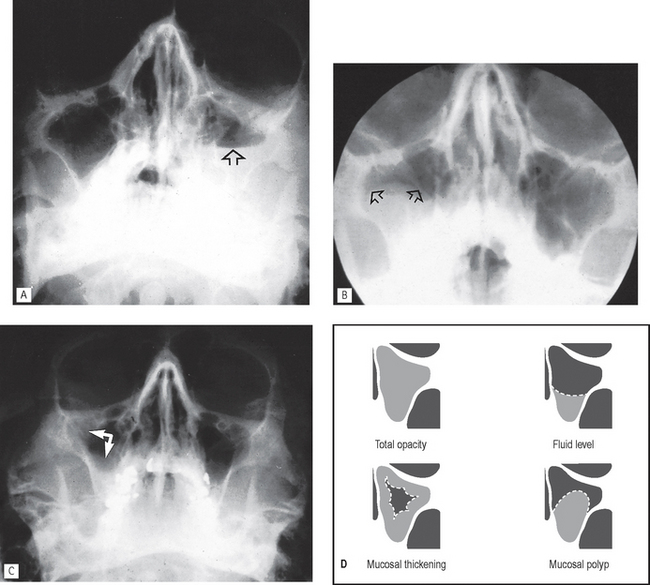
Fig. 29.9 Various appearances of chronic sinusitis evident on conventional occipitomental radiographs. A Fluid level in left antrum (arrowed) — note the shape of the meniscus. B Round, domed antral polyp in the base of the right antrum (arrowed). C Mucosal thickening on the inner aspects of the lateral walls of the right antrum (arrowed). D Simplified line diagrams of the left antrum (as depicted on a 0° OM) illustrating the various appearances.
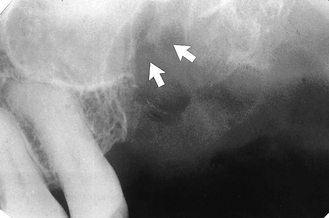
Fig. 29.10 Periapical of  showing a discontinuity of the antral floor (arrowed) following the extraction of the molar tooth that resulted in a clinical oro-antral communication. Note this break in continuity of the floor is not always evident in cases of oro-antral communication.
showing a discontinuity of the antral floor (arrowed) following the extraction of the molar tooth that resulted in a clinical oro-antral communication. Note this break in continuity of the floor is not always evident in cases of oro-antral communication.
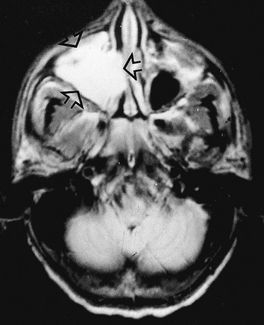
Fig. 29.11 Axial MR scan showing a white right antrum (arrowed) that was filled with blood following a middle third facial fracture.
(Kindly supplied by Mrs J. E. Brown.)
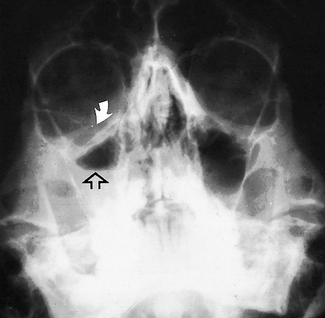
Fig. 29.12 Standard occipitomental showing fracture of the right zygomatic complex with a break in the antral roof (white arrow). The right antrum shows a definite fluid level as a result of blood in the antrum (open arrow).
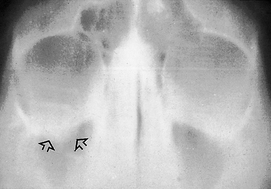
Fig. 29.13 Coronal section tomograph of a patient with an orbital blow-out fracture of the right orbital floor/antral roof showing the downward herniated contents of the orbit into the antrum (arrowed), the so-called hanging drop appearance.
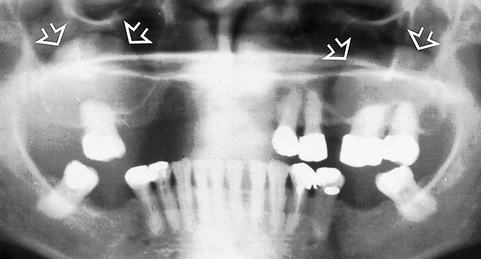
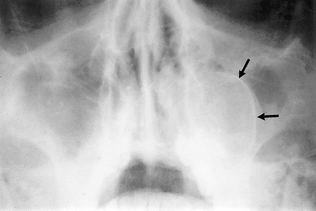
Fig. 29.15 Occipitomental showing the well-defined, round, domed opacity on the left side caused by a radicular (dental) cyst arising from  . The radiopaque (white) corticated margin to the top of the meniscus (the displaced antral floor) is arrowed.
. The radiopaque (white) corticated margin to the top of the meniscus (the displaced antral floor) is arrowed.
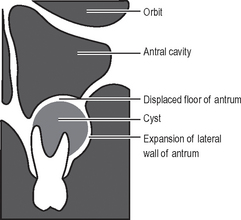
Fig. 29.16 Simplified line diagram illustrating the essential radiographic features of a small odontogenic cyst and its effects on the antrum (as depicted on an 0° OM).
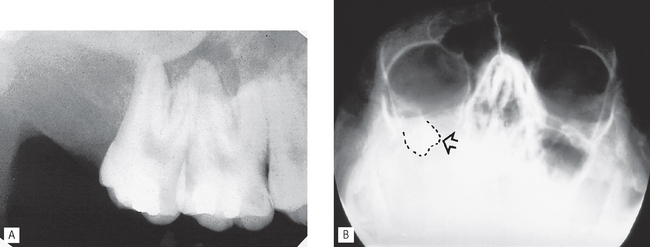
Fig. 29.17 Large dentigerous cyst associated with  . A Periapical of the upper right posterior teeth. Note the lack of antral floor outline and absence of
. A Periapical of the upper right posterior teeth. Note the lack of antral floor outline and absence of  . B Occipitomental of the same patient showing total opacity of the right antral region with no evidence of the lateral antral margin. The displaced upper wisdom tooth is evident underneath the orbit (outlined and arrowed).
. B Occipitomental of the same patient showing total opacity of the right antral region with no evidence of the lateral antral margin. The displaced upper wisdom tooth is evident underneath the orbit (outlined and arrowed).
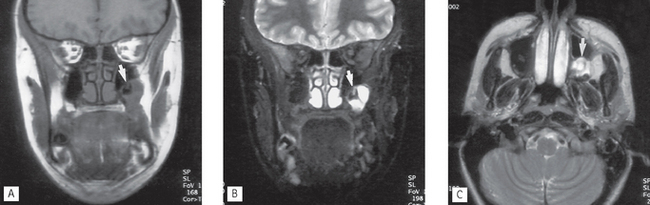
Fig. 29.18 MR images of a dentigerous associated with an unerupted displaced third molar expanding into the antrum. A T1-weighted coronal image showing the cyst and unerupted tooth (arrowed). B T2-weighted coronal image — the cyst fluid appears white (arrowed). C T2-weighted axial showing the cyst (arrowed)
(kindly provided by Drs J. Kabala and J. Luker).

Fig. 29.19 Occipitomental showing a totally opaque right antrum caused by a large squamous cell carcinoma, with destruction of the lateral antral wall (large arrow) and zygoma (small arrow).
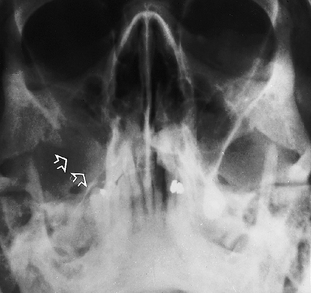
Fig. 29.20 Occipitomental showing destruction of the lateral wall of the right antrum (arrowed) by a squamous cell carcinoma. In this case, there is little evidence of increased opacity within the antrum.

Fig. 29.21 An axial CT scan showing a destructive squamous cell carcinoma (arrowed) in the pterygopalatine fossa invading the posterior antral wall.

Fig. 29.22 An axial CT scan at the level of the antral floor showing a very extensive destructive lesion (arrowed) that proved histologically to be an osteosarcoma.
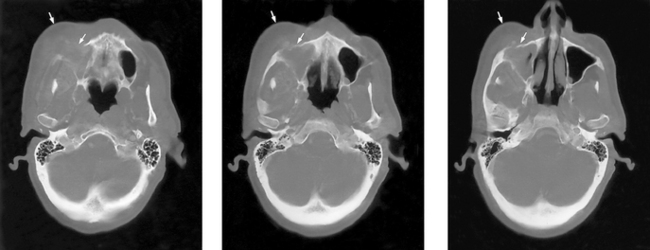
Fig. 29.23 A series of axial CT slices showing a very large mass (arrowed) of a squamous cell carcinoma probably arising in the cheek showing extensive local destruction including the lateral wall of the antrum and extension into the antrum
(kindly provided by Drs J. Kabala and J. Luker).
Infection / inflammation
Acute sinusitis
Acute sinusitis is most commonly caused by an upper respiratory tract infection, particularly the common cold. The effects on the antrum include:
Acute sinusitis can be diagnosed and treated clinically. As a result, the Royal College of Radiologists in the UK in their booklet Making Best Use of a Department of Clinical Radiology 5th ed (2003) recommend that radiological imaging is not necessary.
Chronic sinusitis (Figs 29.5-29.9)
Main radiological features
• Total/partial opacity within the antral cavity.
• Fluid level — usually in the base of antral cavity with a characteristic meniscus shape.
• Round, domed opacity produced by a mucosal polyp.
• Occasionally an increase in the bony antral walls.
• Typical inflammatory changes if infected teeth are involved — this may lead to resorption and remodelling to produce the appearance described as antral halo (see also Ch. 22).
Trauma
Oro-antral communication
Main radiographic features
• Break in the continuity of the floor may be evident (see Fig. 29.10) — however, the diagnosis of an oro-antral communication is made clinically, not radiographically, since the defect in the floor of the antrum may not be evident on the two-dimensional radiograph.
• Characteristic features of acute or chronic sinusitis (see earlier) owing to the ingress of bacteria.
• Evidence of the displaced root or tooth — a second view of the antrum with the head in a different position may be required to ascertain the exact location of the displaced object.
Fractures of the maxillo-facial skeleton
Fractures are discussed in detail in Chapter 30 and only a brief summary is shown below.
Main radiographic features
• Break in the continuity of one or more of the antral walls depending on the type of fracture.
• Total opacity or fluid level within the antral cavity caused by haemorrhage (see Figs 29.11 and 29.12).
• Features of sinusitis if subsequent infection develops (this is in fact surprisingly rare).
• The orbital blow-out fracture classically produces a tear-drop-shaped opacity in the upper part of the antrum, the hanging drop appearance, caused by herniation of the orbital contents downwards into the antrum following collapse of the antral roof (see Fig. 29.13). The infraorbital margin remains intact. See also Figure 30.30.
Cysts
The more important cysts that can affect the antra include:

Mucosal retention cyst
Cause
The cause is unknown, but is presumably due to blockage of a mucus-secreting cell in the antral lining.
Main radiographic features (see Figs 29.7 and 29.9B)
• Well-defined, round, dome-shaped opacity within the antrum varying in size from a tiny lesion to one completely filling the antrum.
• Usually no evidence of thickening of the remainder of the epithelial lining.
• Usually no alteration of the antral outline
• Occasionally bilateral (see Fig. 29.14).
Odontogenic cysts
These cysts are extrinsic to the antra developing in the alveolar bone beneath the antral floor.
Main radiographic features of a small cyst
• Round, dome-shaped opacity in the base of the antrum with a well-defined, radiopaque corticated margin to the edge of the meniscus, i.e. the odontogenic cyst has a bony margin and so can be differentiated from the soft tissue mucosal retention cyst or antral polyp (see Figs 29.15 and 29.16).
Main radiographic features of a large cyst
• Total opacity of the antral region owing to complete compression of the antral cavity.
• Sometimes displacement of the associated tooth (see Figs 29.17 and 29.18).
Note: Subsequent marsupialization or decompression of the cyst will usually result in the reformation of the antral cavity.
Tumours
Malignant intrinsic tumours
Squamous cell carcinoma and adenocarcinoma — these uncommon but important tumours produce a rapidly growing, aggressive soft tissue mass within the antrum causing destruction of one or more of the antral walls.
Main radiographic features of a large well-established lesion
• Total opacity of the antral cavity (see Fig. 29.19) — in the absence of symptoms suggesting infection, or a history of trauma, a totally opaque antrum is a cause for serious concern and further investigation is necessary.
• Destruction of one or more of the antral walls (see Fig. 29.20) and invasion of surrounding hard and soft tissues—hence the need for CT.
Extrinsic tumours
Any tumour that can affect the maxilla — whether benign or malignant — can have an effect on the antra with the typical associated bony changes. All are uncommon but three of the more important tumours are:
The main radiographic features of concern are those indicating malignancy and include:
• Total/partial opacity of the antral cavity
• Destruction of one or more of the walls of the antrum
• Occasional displacement or resorption and loosening of the adjacent teeth (Figs 29.21-29.23).
OTHER PARANASAL AIR SINUSES
As mentioned earlier, the frontal, ethmoidal and sphenoidal air sinuses are of limited importance in routine dentistry. Many of the conditions described in relation to the maxillary antra can affect these paranasal sinuses and produce similar effects. Occasionally routine skull radiography reveals unusual abnormalities, such as the ivory osteoma in the frontal sinus (see Fig. 29.24). But generally the investigation of choice for the paranasal air sinuses is computed tomography (CT), as shown in Figure 29.25.