Chapter 18 Diseases associated with bacteria – III
DISEASES ASSOCIATED WITH ESCHERICHIA COLI 847
ESCHERICHIA COLI INFECTIONS IN WEANED PIGS 888
DISEASES ASSOCIATED WITH SALMONELLA SPECIES 896
DISEASES ASSOCIATED WITH PASTEURELLA SPECIES 921
DISEASES ASSOCIATED WITH BRUCELLA SPECIES 963
DISEASES ASSOCIATED WITH MORAXELLA, HISTOPHILUS, AND HAEMOPHILUS SPECIES 994
Diseases associated with Escherichia coli
Colibacillosis, associated with Escherichia coli, occurs in all species of newborn farm animals and is a major cause of economic loss in this age group. Gut edema and enteric colibacillosis of recently weaned pigs are also important diseases associated with this organism.
E. coli is a major cause of diarrhea in calves, piglets, and lambs, and the term ‘colibacillosis’ is commonly used; however, diarrhea in newborn calves, for example (and in other species too), can be associated with several different enteropathogens influenced by several risk factors (Table 18.1). Colibacillosis is presented in this chapter. Information on the viral diarrheas of newborn farm animals is presented in Chapter 21. Diarrhea associated with Cryptosporidium is presented in Chapter 26. This section first outlines the general aspects of acute undifferentiated diarrhea of newborn farm animals, with emphasis on the disease in calves. Many of the principles can be applied to the other species. This is followed by the diseases associated with E. coli.
Table 18.1 Risk factors and their role in acute undifferentiated diarrhea of newborn calves
| Risk factor | Role of risk factor |
|---|---|
| Colostral immunity of calf | Low levels of serum immunoglobulins render calves highly susceptible to death from diarrhea |
| Overcrowding | Increased population density increases infection rate and high morbidity and mortality |
| Parity of dam | Calves born from heifers may not acquire sufficient level of colostral immunoglobulins |
| Meteorological | Changes in weather; wet, windy and cold weather commonly precedes outbreaks of diarrhea in beef calves. Higher mortality in dairy calves exposed to hot environmental temperatures. High environmental temperatures precipitate outbreaks |
| Quality of diet | Heat denatured skim-milk used in milk replacers is less digestible than whole milk and precipitates diarrhea |
| Calf rearer | The concern and care provided by the calf rearer will have a direct effect on morbidity and mortality associated with diarrhea |
ACUTE UNDIFFERENTIATED DIARRHEA OF NEWBORN FARM ANIMALS (PARTICULARLY CALVES AND PIGLETS)
Diarrhea in newborn farm animals, particularly calves under 30 days of age and piglets in the first week of life, is one of the most common disease complexes that the large-animal clinician encounters in practice. It is a significant cause of economic loss in cattle and pig herds and continues to assume major importance as livestock production becomes more intensified. The effective treatment and control of herd epidemics of diarrhea in calves and piglets can be frustrating and unreliable. Considerable progress has been made in the treatment of the effects of diarrhea such as dehydration and acidosis but less so in the control of these disease complexes.
The causes of calf and piglet diarrhea are complex and usually involve an interaction between enteropathogenic bacteria, viruses, and protozoa, the colostral immunity of the animal and the effects of the environment (Tables 18.1-18.3). Thus the term acute undifferentiated diarrhea of newborn calves is used to describe the acute diarrhea that occurs in newborn calves under 30 days of age, characterized clinically by acute profuse watery diarrhea, progressive dehydration and acidosis and death in a few days, or earlier after onset if treatment is not provided. Based on clinical findings alone, it is not usually possible to differentiate between the common known causes of diarrhea in newborn calves, which include enterotoxigenic E. coli (ETEC), verocytotoxic E. coli (VTEC), necrotoxigenic E. coli (NTEC), rotavirus, coronavirus, bovine torovirus (Breda virus), calicivirus, norovirus (Norwalk-like virus), Cryptosporidium spp., Giardia spp., and Salmonella spp. The common necropsy findings are dehydration, emaciation, and a fluid-filled intestinal tract, with no other obvious gross lesions. The exceptions are enteritis associated with Salmonella spp., Clostridium perfringens types B and C, Eimeria spp., and attaching and effacing E. coli, in which there are usually typical gross lesions at necropsy.
Thus the disease is considered to be a complex syndrome because one or any combination of more than one of the specific etiological agents may be the cause of the disease. Risk factors may also precipitate the disease in calves in which the disease might not normally occur, even though they are infected with a specific enteropathogen. The term acute undifferentiated diarrhea of newborn calves is useful to encompass cases of diarrhea in calves in which the etiological diagnosis is not immediately obvious and may not be determined, even after exhaustive diagnostic work.
RISK FACTORS
A risk factor is any circumstance that can contribute to the occurrence of the disease. Conversely, if that circumstance is not present the disease may not occur. Many interrelated risk factors have been associated with a high incidence of calf diarrhea and have added to the difficulty of understanding the complexity of the disease and controlling it. The identification and modification or removal of these risk factors can be very effective in the clinical management and control of epidemics of the disease.
Animal risk factors
The host risk factors include immaturity of the neonate at birth, age of the neonate, a lack of vigor of the calf or piglet at birth, the presence of intrapartum hypoxemia and acidosis from a difficult birth, and failure to acquire sufficient colostral immunity. The nutrition of the pregnant dam can affect the quantity and quality of colostrum, and consequently the vigor of the calf.
Colostral immunoglobulin status
The role of colostrum in protecting the newborn calf from the effects of enteropathogens is well known. The failure of the newborn calf to ingest an adequate quantity of good-quality colostrum containing a high level of colostral immunoglobulins within a few hours after birth is a major risk factor contributing to acute undifferentiated diarrhea. Complete or partial failure of transfer of passive immunity is highly prevalent in diarrheic veal calves infected with cryptosporidia, coronavirus, and rotavirus.1 Earlier work centered on the protective effect of colostrum against septicemic and enteric colibacillosis. More recently, the role of colostral and milk antibodies against rotavirus and coronavirus enteritis in newborn calves has been established. Specific protection against these viral diarrheas in the newborn calf depends on the level of antibody in the lumen of the intestine. While it is easy to state that calves should receive liberal quantities of colostrum, the veterinarian in the field who encounters an outbreak of acute diarrhea in beef calves, for example, cannot usually easily determine whether in fact the calves possess protective levels of immunoglobulins.
Lactose intolerance as a cause of diarrhea has been reported in a calf but its occurrence is rare.2
Cases of diarrhea due to specific nutritional deficiencies are reported rarely and not well documented. However, field observations indicate that outbreaks of diarrhea in sucking beef calves may have been associated with specific nutrient deficiencies such as copper or selenium. These are not documented but should be considered in certain situations where these deficiencies are known to be present in the herd. An epidemic of intractable diarrhea in 2-month-old beef calves was associated with deficient tissue and plasma levels of vitamin E in the affected calves, which also had lesions of skeletal and myocardial muscular dystrophy with adequate levels of selenium.3 A combination of low vitamin E status and low immunoglobulin status may be a contributing factor in neonatal diarrhea of calves,4 but this is not well documented.
Environmental and management risk factors
Veterinarians have commonly observed a relationship between adverse climatic conditions and epidemics of diarrhea in calves. During inclement weather, such as a snowstorm, a common practice in beef herds is to confine the calving cows in a small area where they can be fed and watered, and observed, more easily. The overcrowding may be followed by an outbreak of calf diarrhea. Cold, wet, windy weather during the winter months in temperate climates and hot humid weather during the summer months may be associated with an increased incidence of dairy calf mortality due to diarrhea. Changes in weather and wet, windy and cold weather are commonly associated with subsequent outbreaks of the disease in beef calves raised outdoors. Increases in population density in calf houses, and on calving grounds, resulting in highly contaminated calving grounds, are important risk factors. In beef herds in the USA and Canada, the risk factors that are associated with an increase in calf mortality from diarrhea include:
• The herd of origin. This is because of the genetic composition of the cattle, environmental conditions, degree of exposure to pathogens and management practices unique to the herd
• Increasing the percentage of heifers calving in the herd. The risk of diarrhea in calves born to heifers may be about four times greater than in calves born to cows5
• The odds of diarrhea occurring in calves born on or after the median calving date is twice that of calves born before the median calving date.5 This may be because of increased pathogen exposure as the calving season progresses
• Poor drainage and limited shelter in the nursery yards
• A decrease in the size of the effective calving yards because of poor drainage and wetness
• Wintering and calving cows and heifers on the same grounds.6
Some studies have shown that the major contributing factor to dairy calf mortality is the care provided by the calf attendant. Not infrequently, however, outbreaks can occur in herds in which the management is excellent and not uncommonly an etiological diagnosis cannot be made.
Certain herd characteristics and herd management practices are associated with an increased incidence of diarrhea in dairy herds.7 Larger herd size is associated with an increased incidence of diarrhea.7 The greater disease rate may be associated with a greater possibility of a large epidemic in a larger population, and cows in larger herds may be more densely housed. In dairy herds with 10–49 cows, the number of young stock at the end of the month, the incidence density of respiratory disease in the calves per herd per calf-month, and the cumulative incidence of vaccinations for calves given to prevent diarrhea may be associated with increased incidence of diarrhea. As the incidence of respiratory disease increases in large dairy herds, the incidence of diarrhea in the calves increases, especially in large herds of over 200 cows.7 Reduction of the incidence of respiratory disease in calves will result in a decrease in the incidence of diarrheal disease. The use of individual maternity stalls and regular removal of bedding between calvings is associated with a decrease in the incidence of neonatal calf diarrhea. As the number of calves in the herd increases, calf attendants may become too busy to perform duties of calf care thoroughly. Overcrowding may also be a risk factor.
Dairy calves fed milk replacers may develop diarrhea because of the inferior quality of some milk replacers.8
Epidemics of diarrhea in piglets are commonly associated with inadequate sanitation and hygiene in the farrowing rooms, which may be under continuous use without sufficient time for cleaning and disinfection between farrowings. Certain management procedures may be associated with differences in the prevalence of enteropathogens.
In dairy calves fed on nipple feeders there may be increased probability of the calves shedding detectable fecal levels of Salmonella, E. coli, rotavirus, or coronavirus. The use of group pens has been associated with increased odds of encountering Campylobacter jejuni, the presence of which is of uncertain significance. Calves with diarrhea on these farms tend to have increased odds of shedding rotavirus and K99+ E. coli.
Pathogen risk factors
Calves
The distribution and occurrence of enteropathogens in the feces of diarrheic and normal healthy calves varies depending on the geographical location, the farm, the age and type of calves being examined, and the extent to which the diagnostic laboratory is capable of isolating or demonstrating the pathogens.9 Rotavirus, Cryptosporidium spp., coronavirus, and enterotoxigenic E. coli, collectively, are responsible for 75–95% of infections in neonatal calves worldwide. The relative frequencies of each of the four differ between locations and between seasons and years.10 Any one of the common pathogens may predominate or be absent in a certain group of animals.11 Mixed infections are common.12 Rotavirus will be most common in some groups, especially housed calves.12 Coronavirus may predominate in beef calves in some countries and not in others, and Cryptosporidium may occur in 30–50% of diarrheic calves on a worldwide basis.13 A survey of veal calf farms revealed that Cryptosporidium infection is an important cause of transient diarrhea and that there was no association between diarrhea and infection with either Salmonella spp., enterotoxigenic E. coli, rotaviruses, or verocytogenic E. coli in the population examined.14 Cryptosporidia, rotavirus, and coronavirus are the most commonly identified enteropathogens in intensively reared veal calves.1 In dairy calves, the prevalences of giardiosis and cryptosporidiosis may be high and both parasites may be associated with diarrhea. Cryptosporidium parvum is an important pathogen in calves under 1 month of age, but Giardia duodenalis may be more important when calves are older. Calves may clear C. parvum infections within 2 weeks; however, G. duodenalis infections may become chronic in the same calves.15 The combination of Cryptosporidium sp. and rotavirus may predominate in some situations. Cryptosporidium spp. were the second most commonly detected pathogens next to rotavirus, and case-control studies indicated a highly significant association with diarrhea. Enteropathogens may not be detectable in up to 30% of diarrheic calves. Eimeria spp. can cause coccidiosis in calves any time after about 21 days after birth but the disease is more common in calves several months old.
In some countries, enterotoxigenic K99+ E. coli may occur in 30–40% of diarrheic calves, while in others the incidence may be as low as 3–6%. Attaching and effacing E. coli that cause hemorrhagic colitis and blood in the feces of diarrheic calves about 2 weeks of age are being recognized with increasing frequency. They may occur concurrently with other enteropathogens (cryptosporidia, rotavirus, coronavirus, enterotoxigenic E. coli, bovine virus diarrhea virus (BVDV), and coccidia). Some isolates of attaching and effacing E. coli produce verocytotoxin.
The age occurrence of the common enteropathogens associated with diarrhea in calves is shown in Table 18.2. Case-control studies of diarrheic and healthy calves from the same groups indicate that the enteropathogens commonly found in diarrheic calves can also be found in healthy calves but at a lower frequency, with the exception of rotavirus, which may be excreted by up to 50% of healthy calves. The prevalence of enteropathogens in healthy calves on farms where there is no recent history of diarrhea indicates an absence of Salmonella spp., enterotoxigenic E. coli, Cryptosporidium, and coronavirus, but the presence of rotavirus in some calves. It appears that healthy calves may be infected more often with enterotoxigenic E. coli, Cryptosporidium, coronavirus, and rotavirus in herds in which some calves have or recently have had enteric disease than in herds free from major enteric disease.
Table 18.2 Age occurrence of the common enteropathogens in calves
| Enteropathogen | Age (days) |
|---|---|
| Enterotoxigenic Escherichia coli | <3 |
| Attaching and effacing E. coli | 20–30 |
| Rotavirus | 5–15 |
| Coronavirus | 5–21 |
| Other viruses (Breda virus, parvovirus, bovine virus, diarrhea virus) | 14–30 (and older, up to several weeks) |
| Cryptosporidium spp. | 5–35 |
| Salmonella spp. | 5–42 |
| Clostridium perfringens types B and C | 5–15 |
| Eimeria spp. | >30 |
| Giardia spp. | 10–30 |
Campylobacter spp. and Yersinia spp. are well adapted to the bovine host and can be found in the feces of diarrheic and healthy calves at a similar prevalence.16 Their significance as pathogens in newborn calves is questionable. They are probably part of the normal enteric flora of ruminants. However, as they represent a source of gastrointestinal infections in humans, management factors limiting intestinal colonization of these bacteria should be considered in beef cow/calf herds.16
Rotavirus and coronavirus occur with almost equal frequency in the intestinal tracts of normal and diarrheic calves of some studies. Intestinal lesions compatible with the viral infections are found in about 70% of diarrheic calves. Thus, these viruses are widespread in the bovine population and only under some circumstances will the infection be severe enough to cause lesions and diarrhea. Other viruses, such as parvovirus, astrovirus, Breda virus, and calici-like virus, have been isolated from the feces of diarrheic calves but their role in the etiology is yet to be defined.
A necrotizing enteritis of suckled beef calves 7–10 weeks of age on pasture in Scotland has been reported.17 Fever, acute diarrhea and dysentery, and a case fatality rate of 25% are characteristic. No etiological agent has been identified.
Lambs and goat kids
The E. coli strains isolated from diarrheic lambs and goat kids on Spanish farms are not generally toxigenic and belong to a large number of O serogroups.18
Piglets
In outbreaks of diarrhea in neonatal piglets during the first 5 days of life, the enteropathogens that are commonly present in the feces include the transmissible gastroenteritis (TGE) virus, enterotoxigenic E. coli, Isospora spp., rotavirus, C. perfringens type C, and adenovirus. Clostridium difficile has emerged as an important pathogen causing enteritis in suckling piglets.19,20 The TGE virus causes diarrhea in piglets under 15 days of age, enterotoxigenic E. coli under 5 days of age, Isospora sp. between 5 and 15 days of age, and rotavirus in piglets over 10 days of age. During the second and third weeks of life, Isospora suis is the most common pathogen in outbreaks of diarrhea in litters of piglets. While individual piglets may be infected by a single pathogen, it is common for more than one pathogen to be present in the litter. This stresses the importance of submitting to the diagnostic laboratory some piglets that are representative of the problem. A seasonal occurrence of the common enteropathogens has also been observed. The prevalence of the TGE virus may be highest during the fall, winter, and spring months, and the coccidia and E. coli are more common during the summer, fall, and early winter, with the lowest prevalence in the spring.
Foals
Diarrhea in foals is common but most cases are mild, transient and not associated with infectious agents. Diarrhea is the most commonly reported disease in foals under 7 days of age.21 The most common occurrence is associated with ‘foal heat’ in the mare. Group A rotavirus is the most common cause of epidemics of diarrhea in foals.22 Enterotoxigenic E. coli has been isolated from a diarrheic foal. Other pathogens that have been isolated from foals with diarrhea include C. jejuni, C. perfringens, and Rhodococcus equi.
CLINICAL MANAGEMENT OF EPIDEMICS
When faced with an outbreak of acute diarrhea in newborn calves in which there is profuse watery diarrhea, progressive dehydration, and death in a few days or earlier, the following steps are recommended:
1. Visit the herd and do an epidemiological investigation to identify the risk factors that may have been responsible for the outbreak. Most outbreaks are multifactorial and an interaction between the environment, management, feeding and the pathogens.23,24 The investigation of the underlying causes of the outbreak should involve an examination of:
2. Each of the commonly recognized risk factors must be examined for its possible role in the particular outbreak:
3. Affected calves should be examined clinically, dead ones by necropsy, and a case definition should be determined to insure that diarrhea is the major problem
4. All affected calves should be identified, isolated and treated immediately with oral and parenteral fluid therapy as indicated. The use of oral fluid and electrolyte therapy for the treatment of dehydration and acidosis as soon as the calves are seen to be diarrheic must be emphasized
5. Antibacterials may be given orally and parenterally for the treatment of enteric and septicemic colibacillosis. When large numbers of calves are affected at one time it is not usually possible clinically or with the aid of a laboratory to determine which calf is septicemic, and thus all acutely affected calves should be treated. Treatment, however, should not be continued beyond 3 days
6. Fecal samples (30–50 g) should be collected from diarrheic calves at the first sign of diarrhea, and from normal calves, and submitted to a laboratory for the attempted isolation and characterization of enterotoxigenic E. coli, rotaviruses, and Salmonella spp. A rapid enzyme-linked immunosorbent assay (ELISA) test is available for the simultaneous detection of Escherichia coli K99 antigen, bovine coronavirus, and rotavirus in the feces of diarrheic calves during the acute phase of the infection. The Enterosure Kit is a monoclonal antibody ELISA for the detection of bovine coronavirus, rotavirus serogroup A, and K99+ E. coli antigen. The Cryptosure Kit is a substantial improvement over the stain method for detecting cryptosporidia in the feces. Blood samples from affected and normal calves and colostrum samples, if available, are useful for immunoglobulin and antibody studies. All moribund calves should be submitted for necropsy before they die naturally
7. Pregnant cows that are due to calve shortly should be moved to a new calving area. In a dairy herd this means a different, clean calving stall, preferably in another barn not previously occupied by cattle; in beef herds it may mean moving a large number of cows to a new, uncontaminated calving pasture
8. The control of the disease in future calf crops will depend on application of the principles of control, which are described under colibacillosis and viral diarrhea of calves. If a significant number of cows are due to calve in more than 3–6 weeks, vaccination with the calf diarrhea vaccines can be considered
9. A report should be submitted to the owner that records the observations made at the farm visit and outlines specific recommendations for clinical management of affected calves and for control of the disease in the future.
1 McDonough S, et al. Am J Vet Res. 1994;55:1516.
2 Olchowy TWJ, et al. J Vet Intern Med. 1993;7:12.
3 Radostits OM, et al. Proc Annu Conv Am Assoc Bovine Pract. 1992;24:101.
4 Wright A, et al. Can Vet J. 1995;36:36.
5 Clement JC, et al. J Am Vet Med Assoc. 1995;207:1334.
6 Driesen SJ, et al. Aust Vet J. 1993;70:259.
7 Frank NA, Kaneene JB. J Dairy Sci. 1993;76:1313.
8 Heinrichs AJ. Compend Contin Educ Pract Vet. 1994;16:1605.
9 Brenner J, et al. Israel J Vet Med. 2000;55:5.
10 Kodituwakku SN, Harbour DA. Vet Rec. 1990;126:547.
11 Adesiyun AA, Kaminjolo JS. Prev Vet Med. 1994;19:151.
12 Fagan JG, et al. Ir Vet J. 1995;48:17.
13 Fayer R. Vet Parasitol. 2004;126:37.
14 Wilson JB, et al. Can J Vet Res. 1992;56:184.
15 O’Handley RMO, et al. J Am Vet Med Assoc. 1999;214:391.
16 Busato A, et al. Vet Microbiol. 1999;69:251.
17 Caldow GL, Munro R. Vet Rec. 1995;137:307.
18 Blanco J, et al. Vet Microbiol. 1996;49:209.
19 Nagy J, Bilkei G. Vet J. 2003;166:98.
20 Yaeger M, et al. J Vet Diagn Invest. 2002;14:281.
21 Cohen ND. J Am Vet Med Assoc. 1994;204:1644.
22 Dwyer RM, et al. Proc Annu Conv Am Assoc Equine Pract. 1991;36:337.
COLIBACILLOSIS OF NEWBORN CALVES, PIGLETS, LAMBS, KIDS, AND FOALS
Etiology Pathogenic serotypes of Escherichia coli: septicemic, enterotoxigenic, enteropathogenic (EPEC), enterohemorrhagic (EHEC), also referred to as verocytotoxigenic (VTEC) or Shiga-toxin-producing (STEC), and necrotoxigenic E. coli (NTEC)
Epidemiology Newborn calves, piglets, lambs, goat kids, foals. Risk factors include colostrum deprivation, overcrowding, adverse climatic conditions, inferior milk replacers. Prevalence of enteropathogenic E. coli varies between herds. Enterohemorrhagic E. coli (O157:H7) in cattle is of major zoonotic concern
Signs Weakness and collapse (septicemia). Diarrhea. Dehydration. Complications such as meningitis
Clinical pathology Isolate organism from feces. Hematology and serum biochemistry to evaluate inflammation and acid–base and electrolyte imbalance
Lesions Septicemic lesions. Dehydration, enteritis
Diagnostic confirmation Culture of organism and serotyping
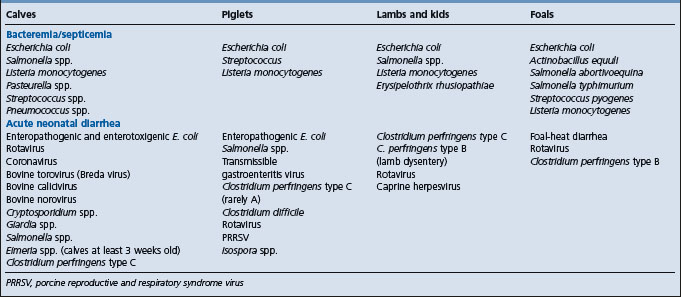
Differential diagnosis See Table 18.3. E. coli infections causing septicemia and diarrhea in newborn farm animals must be differentiated from the following:
• Septicemia in lambs and kids
• Acute neonatal diarrhea in calves
• Acute neonatal diarrhea in piglets
Treatment Antimicrobials. Fluid and electrolyte therapy
Control Reduce infection pressure on neonate. Insure adequate intake of colostrum. Vaccinate pregnant dam to induce specific colostrum antibody. Minimize stressors and their effect on neonates
ETIOLOGY
Colibacillosis is associated with pathogenic serotypes of Escherichia coli.1,2 The prevalence of the different pathogenic serotypes of E. coli in farm animals has remained relatively unchanged for many years. Certain serotypes cause diarrhea and others cause septicemia.
• Enterotoxigenic E. coli is the most common enteropathogen that causes diarrhea in newborn farm animals. The bacteria cause diarrhea by adhering to, colonizing and producing enterotoxins in the small intestine; they are not invasive3
• Enteropathogenic E. coli are the ‘attaching and effacing’ strains that colonize the small intestine, where they attach tightly to the epithelial cells of the villus and cause typical attaching and effacing lesions. They do not produce toxins and seldom invade the intestinal mucosa
• Enterohemorrhagic E. coli strains elaborate very potent Shiga toxins. The enterohemorrhagic E. coli are considered to be a subset of Shiga-toxin-producing or verotoxin-producing strains of E. coli. They are not an important cause of diarrhea in farm animals but some Shiga-toxin-producing E. coli have been responsible for diarrhea in calves. Cattle are an important reservoir of E. coli O157:H7, one of the important enterohemorrhagic E. coli strains, causing a broad range of clinical disease in humans including diarrhea and hemorrhagic colitis, and the highly fatal hemolytic–uremic syndrome in children.4,5 See ‘Enterohemorrhagic Escherichia coli in farm animals and zoonotic implications’, below
• Necrotoxigenic E. coli (NTEC) strains produce cytotoxic necrotizing factor (CNF)1 or 2. NTEC2 isolates are restricted to calves and lambs with diarrhea and septicemia3
• Septicemic E. coli strains of serogroup 078 are invasive and cause septicemia in calves, piglets, and lambs.1 Their powerful endotoxins cause endotoxic shock with a high case fatality rate.
EPIDEMIOLOGY
Occurrence and prevalence of infection
The prevalence of colibacillosis has increased in recent years. There are several possible reasons for this, including size of herds, shortage of qualified labor, automated livestock rearing systems, and increased population density.
Colibacillosis occurs most commonly in newborn farm animals and is a significant cause of economic loss in raising livestock. It is a complex disease in which several different risk factors interact with certain pathogens, resulting in the disease. There are at least two different types of the disease: enteric colibacillosis is characterized by varying degrees of diarrhea, dehydration, acidosis, and death in a few days if not treated; coliform septicemia is characterized by severe illness and rapid death in several hours.
Calves
The prevalence of enterotoxigenic E. coli in diarrheic calves varies widely geographically, between herds and depending on the age of the animals. The prevalence can be as high as 50–60% in diarrheic calves under 3 days of age and only 5–10% in diarrheic calves 8 days of age. In some countries the prevalence is only 5–8% in diarrheic calves under 3 days of age. Thus enterotoxigenic colibacillosis is a major cause of diarrhea in calves less than 3 days of age and is not associated with outbreaks of diarrhea in calves older than 3 days. Enterotoxigenic E. coli infection in calves older than 2–3 days will in most cases be associated with a virus infection. The prevalence of the organism is also very low or not present in clinically normal calves in herds that have not had a problem with diarrhea. In some beef herds affected with diarrhea in young calves there may be little evidence of infection with enterotoxigenic E. coli, and other factors need to be examined.
Morbidity and mortality rates
Calves
In dairy calves raised under intensive and poorly managed conditions the morbidity rate may reach 75% but is usually about 30%. Case fatality rates vary from 10–50% depending on the level of clinical management.
In beef calves the morbidity rates vary from 10–50% and the case fatality rates from 5–25% or even higher in some years. The population mortality rate in both beef and dairy calves can vary from a low of 3% in well-managed herds to a high of 60% in problem herds in certain years.
Piglets
In piglets the morbidity rate of preweaning diarrhea varies widely between herds but averages about 6% of litters, mostly in the first week of life. The morbidity rates increase with increased litter size and decrease with increasing parity of the sow. Losses due to stillbirths, traumatic injuries, starvation, and undersize at birth account for a much greater combined total preweaning loss but colibacillosis accounts for approximately 50% of the gastroenteropathies encountered during the preweaning period.
Risk factors
Several risk factors influence the occurrence of the disease, each one of which must be considered, evaluated and modified or removed if necessary when investigating the cause of an outbreak so that effective clinical management and control of the disease may be achieved.
Animal risk factors
Age and birth weight
Colibacillosis is most common in animals under 3 days of age but it may occur as early as 12–18 hours after birth and occasionally occurs in calves up to several days of age when there is a mixed infection with viral enteropathogens. Diarrhea associated with enterotoxigenic E. coli occurs in calves mainly during the first few days of life, rarely in older calves and never in adults. Epidemiological studies of both beef and dairy calves indicate that more than 80% of clinical cases associated with K99+ enterotoxigenic E. coli occur in calves younger than 4 days of age. The mechanism of this age-related resistance is not well understood but may be related to development of resistance to colonization of the small intestine as the calf becomes older. This could be associated with the replacement of villous epithelial cells that occurs in the first few days after birth.
Mortality due to colibacillosis is significantly higher in goat kids that are underweight at birth because of multiple births, which may result in the ingestion of inadequate amounts of colostrum.6
The disease is more common in piglets born from gilts than from sows, which suggests that immunity develops with developing age in the sow and is transferred to the piglets. In a survey of approximately 4400 litters of piglets over a period of 4 years in a large piggery, 64% of the litters were treated for diarrhea before weaning, and piglets born to sows under parity 2 were 1.7 times more likely to develop diarrhea before weaning than litters born to sows over parity 3. The susceptibility or resistance to E. coli diarrhea in piglets has an inherited basis.7 The cell surface receptor for the K88+ antigen is inherited in a simple mendelian way with adherence (S) dominant over nonadherence (s). Homozygous dominants (SS) and heterozygotes (Ss) possess the receptor and are susceptible, whereas in the homozygous recessive (ss) the receptor is absent and the pigs are resistant. The highest incidence of diarrhea occurs in susceptible progeny born from resistant dams and sired by susceptible sires. Most if not all pigs have intestinal receptors for K99+ pili and an inheritance pattern similar to K88+ receptors does not exist for K99+ receptors.
Immunity and colostrum
Newborn farm animals are agammaglobulinemic and must ingest colostrum and absorb colostral immunoglobulins within hours of birth to obtain protection against septicemic and enteric colibacillosis. The transfer of immunoglobulins from the dam to the neonate is termed transfer of passive immunity. Failure of transfer of passive immunity predisposes the neonate to development of infectious diseases.8
Transfer of maternal immunoglobulins to calves depends on three successive processes:
• Formation of colostrum with a high concentration of immunoglobulin by the dam
• Ingestion of an adequate volume of colostrum by the calf
• Efficient absorption of colostral immunoglobulins by the calf.
Colostral immunoglobulins are absorbed for up to 24 hours after birth in calves and up to 48 hours in piglets. However, in calves maximum efficiency of absorption occurs during the first 6–12 hours after birth and decreases rapidly from 12–24 hours after birth. Following absorption, transfer to the intestinal lumen is a major means of IgG1 clearance in calves, and this transfer results in antigen-binding antibody in the intestinal lumen. Both blood-derived antibody and lactogenic antibody are significant sources of passive antibody in the intestinal lumen of the neonatal calf. Maintenance of high concentrations of milk-derived antibodies in the small intestinal lumen may require more than twice-a-day feedings, since antibodies derived from a milk diet are predominantly cleared from the intestinal lumen by 12 hours after feeding.
Passively acquired antibody from the circulation entering the small intestinal lumen is, therefore, a reasonable hypothesis to explain the strong association between high serum passive immunoglobulin concentrations and reduced morbidity in neonatal calves.
Newborn dairy calves should ingest 80 – 100 g of colostral immunoglobulin G1, and ideally up to 150 g, within a few hours after birth in order to achieve serum immunoglobulins of 10 mg/mL.8 Calves fed colostrum containing less than 100 g immunoglobulin are at increased risk for failure of transfer of passive immunity. The highest levels of serum immunoglobulins are achieved by the ingestion of colostrum containing high concentrations of immunoglobulins within a few hours after birth. The concentrations of immunoglobulins in first-milking colostrum from dairy cows can vary from 20–150 g/L, with mean levels varying from 40–50 mg/mL.8 In one study of 919 first-milking colostrums from Holstein cows during a 4-year period on a commercial dairy farm, the colostral immunoglobulin G1 concentrations varied greatly, with a mean of 48.2 mg/mL and a standard deviation of 21.9 mg/mL. Immunoglobulin (Ig) concentration in colostrum is lower in first- and second-calf heifers than in third or subsequent lactations. It is also lower in colostrum from high-producing dairy cows. Natural sucking by the calf may enhance the efficiency of absorption of colostral immunoglobulins, but the volume of colostrum ingested by sucking calves is frequently inadequate. In dairy herds that allowed calves to suck naturally, the prevalence of failure of transfer of passive immunity was greater than 50% even among calves nursed by cows with above-average colostral immunoglobulin concentration.8 In order to ingest 100–150 g of immunoglobulins, newborn dairy calves should be artificially fed 3–4 L of fresh or refrigerated first-milking colostrum from cows that have had nonlactating intervals of normal duration.8 In beef cattle, the concentration of immunoglobulin in colostrum is generally higher than in dairy cattle but there can be deficiencies of volume production, especially in first-calf heifers.
The maximum level of serum immunoglobulins is reached in the calf at 24 hours after birth and the factors that reduce those levels below an adequate level include the effects of maternal behavior and conformation, the vigor of the calf and environmental influences. Before the newborn calf manages to suck for the first time, a chain of specific events occurs. The calf first recovers from the birth process, attempts and is successful in standing up and then begins to search for a teat. The calf must find its dam and then locate the udder and teats. There are wide variations in the length of each interval and many factors can affect the variation in the intervals, and consequently the calf’s first suck and acquisition of passive immunity. The risk of diarrhea in calves born to heifers may be about four times greater than calves born to cows, which may reflect maternal behavior and colostral immunity.9 Some first-calf heifers do not lick and stimulate their calves to get up and suck immediately after birth as does the mature cow with an ostentatious maternal instinct. Others ignore their calves completely. The conformation of the udder and the shape of the teats may be undesirable in that the calf cannot find the teat so easily on badly shaped udders or the teat may be misshapen, which makes it difficult for the calf to suck. first-calf heifers do not have as much colostrum or as wide a spectrum of specific antibodies as do mature cows.
Calves that receive their first colostrum by bucket do not acquire the same high levels of serum colostral immunoglobulins as calves which receive their first colostrum by natural sucking of the teat. In both cases the presence of the dam improves the absorption. Calves that are weak or have an edematous tongue from a prolonged, difficult parturition may not be able to suck for several hours, by which time the ability to absorb colostral immunoglobulins has decreased markedly. Postnatal respiratory acidosis in calves can adversely affect colostral immunoglobulin absorption, despite adequate colostral intake early in the absorptive period.8 Risk factors predictive of postnatal acidosis are duration of second-stage parturition greater than 1 hour, dystocia requiring traction, and weakness of the calf at birth. Beef calves born outdoors may be subjected to several influences that affect colostral intake. They may be born during a snowstorm and suffer severe cold exposure; when born they may be dropped in a snow-bank and be unable to get up, even with the assistance of the dam. In crowded calving grounds, mismothering due to mistaken identity may occur, resulting in the calf receiving no or very little colostrum.
Certain parameters measurable in dairy calves at, or shortly after birth may have important prognostic value in evaluating the risk of calf diarrhea.10 High levels of serum immunoglobulins decrease the length of an episode of diarrhea.10 The age at onset of diarrhea may be lower in lighter and in heavier newborn calves: lighter calves may be premature and unable to suck adequately, and heavier calves may have experienced dystocia.
The mortality rate from enteric disease is much higher in calves with low levels of serum immunoglobulins than in calves with adequate levels. From the evidence of surveys, up to 40% of newborn dairy calves do not acquire adequate levels of serum colostral immunoglobulins because they do not ingest a sufficient amount of high-quality colostrum soon enough after birth; this makes them very susceptible to neonatal disease, especially enteric disease. In New Zealand, about 50% of dairy calves may not receive colostrum from their dams even when they are left together for up to 24 hours after the birth of the calf.11 The failure of transfer of passive immunity was due primarily to calves not sucking soon enough after birth. Of the calves that did suck, the time between birth and first sucking ranged between 0.9 and 19.1 hours.
The prevalence of failure of transfer of passive immunity in beef calves in North America ranges from 11–31%. In beef cow/calf herds averaging 56 cows in Quebec, Canada, failure of transfer of passive immunity occurred in 19% of the calves The risk factors for failure of transfer of passive immunity (serum concentrations < 10 g/L) in the newborn included being born in a stanchion-stall (odds ratio (OR) 10.2). Calves bottle-fed colostrum were less at risk of failure of transfer of passive immunity (OR = 0.06). Calf gender, month of birth, dam parity and dam body condition were not associated with failure of transfer of passive immunity.12
Lambs with low serum colostral immunoglobulin levels are also highly susceptible to enteric colibacillosis. The factors related to the risk of neonatal mortality, birth weight and serum immunoglobulin concentrations in lambs in the UK indicate that low birth weight and low serum immunoglobulin concentration were associated with increased odds of mortality.13 Fifty-six percent of the variation in immunoglobulin concentration was at the lamb level, 36% at the ewe level and only 7% at the farm level. Factors associated with reduced serum immunoglobulin concentration included early or late birth in the lambing season, being born later than 14 days after the first lamb born on the farm, multiple-birth litters and maternal mastitis.
Newborn piglets that do not obtain a liberal quantity of colostrum within a few hours after birth are very susceptible to colibacillosis. Prolonged parturition, weak piglets, slippery floors, cold drafty farrowing crates and the condition of the sow and her colostrum supply all influence the amount of colostrum ingested by the newborn piglet. Enteric colibacillosis is the major disease in piglets that are weaned from the sow immediately after birth and reared on milk replacers. A crude preparation of porcine immunoglobulin added to the milk replacer of colostrum-deprived pigs provided good protection against enteric colibacillosis when fed for the experimental period of 21 days.
Environmental and management risk factors
Meteorological influences
While few epidemiological data are available to support the claim, many veterinarians have observed a relationship between adverse climatic conditions and colibacillosis in both calves and piglets. During inclement weather, such as a snowstorm, a common practice in beef herds is to confine the calving cows in a small area, where they can be fed and watered more easily. The overcrowding is commonly followed by an outbreak of acute diarrhea in the calves. There is evidence that cold, wet, windy weather during the winter months and hot, dry weather during the summer months has a significant effect on the incidence of dairy calf mortality.
The risk factors for mortality from diarrhea in beef calves in Alberta, Canada, have been examined.14 The odds of increased mortality were increased when the cows and heifers were wintered on the same grounds, when the herd was wintered and calved on the same grounds, and if the cows and heifers calved on the same grounds. The morbidity and mortality rates from diarrhea during the first 30 days of life increased with an increasing percentage of heifers calving in the herd. Heifers are commonly more closely confined during the calving season for more effective observation and assistance at parturition. This may lead to increased contamination of the environment and the abdominal wall and udder of the heifers. Additional factors in heifers include a higher incidence of dystocia and maternal misbehavior, and lower volume and quality of colostrum, all of which can result in weak calves that may not acquire sufficient colostral immunity.
Nutrition and feeding methods
Dairy calves fed milk substitutes may be more susceptible to acute undifferentiated diarrhea, some of which may be due to enteric colibacillosis, compared to those fed cows’ whole milk. Extreme heat treatment of the liquid skim-milk in the processing of dried skim-milk for use as milk substitutes for calves results in denaturation of the whey protein, which interferes with digestibility of the nutrients and destruction of any lactoglobulins that are present and may have a protective effect in the young calf.
Irregular feeding practices resulting in dietetic diarrhea may contribute to a higher incidence of enteric colibacillosis in calves. The person feeding and caring for the calves has been an important factor influencing calf mortality due to diarrhea. While it is generally believed that general or specific nutritional deficiencies such as a lack of energy, protein or vitamin A in the maternal diet predispose to colibacillosis, particularly in calves and piglets, there is no direct evidence that specific nutritional deficiencies are risk factors. They probably are, at least in indirect ways, for example by having an effect on the amount of colostrum available at the first milking after parturition in first-calf heifers underfed during pregnancy.
Standard of housing and hygiene
Housing and hygienic practices are probably the most important risk factors influencing the incidence of colibacillosis in calves and piglets but have received the least amount of research effort compared to other aspects, for example control of the disease through vaccination. As the size of herds has increased, and as livestock production has become more intensified, the quality of hygiene and sanitation, particularly in housed animals, assumes major importance. Where calves are run at pasture or are individually tethered, or penned, on grass the disease is much less common.
Source of the organism and its ecology and transmission
Ingestion is the most likely portal of infection in calves, piglets, and lambs, although infection via the umbilical vessels and nasopharyngeal mucosa can occur. It has been suggested that certain serotypes of E. coli may enter by the latter route and lead to the development of meningitis.
In most species, it is assumed that the primary source of the infection is the feces of infected animals, including the healthy dams and neonates, and diarrheic newborn animals, which act as multipliers of the organisms. In some cases the organism may be cultured from the vagina or uterus of sows whose litters become affected. In pig herds the total number of organisms on each sow is highest in the farrowing barn, decreases when the sow is returned to the breeding barn, and is lowest when the sow is in the gestation barn.
Calves acquire the infection from contaminated bedding and calf pails, dirty calf pens, nearby diarrheic calves, overcrowded calving grounds, and from the skin of the perineum and udder of the cow. The organism is spread within a herd through the feces of infected animals and all the inanimate objects that can be contaminated by feces, including bedding, pails, boots, tools, clothing, and feed and water supplies. The organism is one of the first encountered by newborn farm animals within minutes after birth. In cattle, the tonsil can be a reservoir for Shiga-like positive E. coli in healthy animals.15 It is possible that virulent E. coli can be present and may be transferred to calves when they are licked by their dams at birth. The high population density of animals that occurs in overcrowded calving grounds in beef herds, heavily used calving pens in dairy herds and the continuous successive use of farrowing crates without a break for clean-up contributes to a large dynamic population of E. coli. The population of bacteria in an animal barn will continue to increase with the length of time the barn is occupied by animals without depopulation, clean-out, disinfection and a period of vacancy. In some countries, where lambing must be done in buildings to avoid exposure to cold weather, the lambing sheds may become heavily contaminated within a few weeks, resulting in outbreaks of septicemic and enteric colibacillosis.
Infected animals are the main reservoir for enterotoxigenic E. coli and their feces are the major source of environmental contamination with the bacteria. Passage of the E. coli through animals causes a ‘multiplier effect’, as each infected animal excretes many more bacteria than it originally ingested. Diarrheic calves are the most extreme multipliers, because they often pass 1 L or more of liquid feces containing 1010/g enterotoxigenic E. coli within 12 hours, and recovered calves can continue to shed bacteria for several months.
Normal calves and adult cows can serve as reservoirs of infection, and the bacteria can persist in a herd by circulating through animals of all ages. Carrier animals introduced to an uninfected herd are thought to be one of the main causes of natural outbreaks. The duration and amount of shedding probably depends on the degree of confinement, resulting population density, herd immunity, environmental conditions and perhaps the serotype of the organism.
Pathogen risk factors
Virulence attributes of E. coli
The virulence attributes of enterotoxigenic E. coli include the adhesins in their pili or fimbriae that allow them to adhere to intestinal villous epithelial cells and prevent peristaltic elimination by the gut, and the production of heat-stable (ST) and heat-labile (LT) enterotoxins. The septicemic strains are invasive and commonly cause rapid death due to the effects of a septicemia involving multiple body systems. In animals that do not die of septicemia, localization of the bacteria may also occur in joints and other organs and tissues. Certain strains such as the O115:KXVX 165 can cause either diarrhea or septicemia in piglets and calves.16
The virulence attributes are relevant to vaccine efficacy. The species-specific adhesin antigens must be identified and incorporated into vaccines, which are given to pregnant females in an attempt to stimulate the production of specific antibody in the colostrum, which will provide protection against enterotoxigenic colibacillosis. An essential element of vaccine development is the detection of common fimbrial antigens occurring among most pathogenic isolates and able to induce antibodies that block bacterial adhesion. The great diversity of potential pathogenic serotypes encountered in colisepticemia and the failure of serotype-specific antibody to cross-protect against a heterologous challenge in experimental infection have made it difficult to develop vaccines against septicemic colibacillosis.
The major virulence attributes of the enterotoxigenic strains of E. coli in calves are the K99+ adhesin antigen and the heat-stable enterotoxin.1 The colonization in the small intestine of calves by K99+ enterotoxigenic E. coli appears to be site-specific, having a predilection for the ileum. Some serogroups also elaborate the F41 adhesin to the K99. Other surface-adhesive antigens such as Att 25 and F17 have been identified on bovine enteropathogenic and septicemic E. coli.1 The F17a-positive enterotoxigenic E. coli strains are no longer isolated from diarrheic calves in some countries. It is postulated that the use of a vaccine including O101, K32, and H9 antigens in addition to K99 (F5) explains the strongly reduced incidence of the O101:K32:H9, K99(F5) E. coli clone.17 A K88-related fimbrial antigen occurs on some enterotoxigenic and septicemic strains.
The heat-stable enterotoxin from bovine enterotoxigenic E. coli has been purified and characterized. There is evidence of a form of heat-stable enterotoxin that is common to bovine, porcine, and human strains of enterotoxigenic E. coli.
Most strains of septicemic E. coli belong to certain serogroups with virulence properties that enable them to resist the defense mechanisms that would normally eliminate other E. coli. Septicemic strains produce endotoxin, which results in shock and rapid death, usually in calves that are less than 5 days of age and are agammaglobulinemic because of failure of transfer of colostral immunity. Isolates of E. coli from the blood of critically ill bacteremic calves on a calf-rearing farm in California constituted a heterogeneous group and were aerobactin positive and often resistant to the bactericidal effects of serum.18 The P fimbriae F11 and F165 have been identified in septicemic E. coli strains isolated from calves.19
Enterohemorrhagic E. coli and verocytotoxin-producing E. coli are being recognized in humans and animals with increased frequency20 and constitute a major zoonotic concern. These organisms are members of O111, O1O3, O5, and O26 serogroups, and none produces heat-stable or heat-labile enterotoxin, nor do they possess the K99 pili.3 They produce potent verotoxins, also known as the Shiga-like toxins, SLT1 and SLT2; and some strains, the attaching and effacing E. coli (AEEC), attach to and efface the microvilli of the enterocytes, causing diarrhea and dysentery due to a hemorrhagic colitis in calves 2–5 weeks of age. The effacing (eae) gene and the gene coding for the Shiga-like toxin 1 (SLT1) are associated with most isolates of AEEC in cattle.21 They have been isolated from both diarrheic and healthy sheep and goats.22
A study of the onset and subsequent pattern of shedding of verotoxin-producing E. coli O26, O103, O111, O145, and O157 in a cohort of beef calves on a mixed cattle and sheep farm in Scotland found that O26 was shed by 94% of the calves and that 90% of the O26 isolates carried the vtx1, eae, and ehl genes.23 E. coli O103 was the second most commonly shed serogroup of the tested calves and the pattern of shedding was sporadic and random. There was an absence of shedding of E. coli O111 and the prevalence of shedding of O145 was low. While some shedding of O157 occurred, shedding in calves was sporadic and infrequent. For O26, O103, and O157, there was no association between shedding by calves and shedding by dams within 1 week of birth. For O26 and O103, there was no association between shedding and diarrhea, and no significant change in shedding following housing. In a sample of Australian dairy farms, calves as young as 48–72 hours had evidence of fecal excretion of Shiga-toxin-producing E. coli, indicating that dairy cattle are exposed to Shiga-toxin-producing E. coli from birth.24 Calves at weaning are most likely to be shedding Shiga-toxin-producing E. coli O26 or E. coli O157, similar to the prevalence surveys in the northern hemispheres.
Naturally occurring cases of attaching and effacing lesions of the intestines in calves with diarrhea and dysentery and infected with E. coli O126:H11, the predominant verotoxin-producing E. coli in humans, have been described in the UK.25 Verotoxin-producing E. coli and eae-positive non-verotoxin-producing E. coli have been isolated from diarrheic dairy calves 1–30 days of age.26
E. coli O157 has been isolated from neonatal calves and has been implicated as a cause of diarrhea in calves.27 The isolates carried various virulence genes such as Ehly, eae, stx1, and stx2. The Ehly gene may be a virulence marker for bovine enterohemorrhagic E. coli O157 strains. Similar findings have been reported in dairy cattle herds in Brazil.28 Strains of E. coli, possessing a subtype beta intimin, normally found in human enteropathogenic E. coli, have been found in diarrheic calves in Brazil.29
Non-O157 Shiga-toxin-producing E. coli have been isolated from diarrheic calves in Argentina and the serotypes carried virulence traits associated with increased pathogenicity in humans and cattle.30 Severe clinical syndromes associated with non-O157 Shiga-toxin-producing E. coli are common in children under 4 years of age and may be associated with diarrheic calves, which shed highly virulent Shiga-toxin-producing E. coli strains and could act as a reservoir and contamination source in these areas.
E. coli O116, a serogroup previously associated with cases of hemolytic– uremic syndrome in humans, has been associated with an outbreak of diarrhea and dysentery in 1–16-week-old calves in India.31 E. coli O103:H2, a Shiga toxin strain causing disease in humans, has been isolated from calves with dysentery, and from a sheep in Australia.32
Necrotoxigenic E. coli, which produce cytotoxic necrotizing factor, have been isolated from cattle in Northern Ireland33 and Spain, and from diarrheic piglets in England.34 NTEC1 strains from cattle, pigs, and humans can belong to the same sero/biogroups, carry genes coding for adhesions belonging to the same families, and possess other identical virulence-associated properties, and therefore do not exclude the possibility of cross-infection between humans and farm animals in some cases.35 Necrotoxigenic E. coli were detected by tissue culture and polymerase chain reaction (PCR) in 15.8% of diarrheic dairy calves in Spain from 1–90 days of age; the majority were necrotoxigenic E. coli producing CNF2 and the risk increased with age. There was also a strong association between CNF2 and F17 fimbriae.36 The necrotoxigenic E. coli with their associated adhesins and toxins were present in diarrheic and septicemic calves as early as 1958 and their prevalence seems to be increasing.37 Their role in causing disease needs further examination.
Most enteropathogenic E. coli from neonatal pigs belong to the so-called ‘classical serogroups’ O8:K87, O45, O138:K81, O141:K85, O147:K89, O149:K91, and O157:KXVX17.1 Strains of these serogroups usually express and produce K88+, 987P+, or K99+ pilus antigens, which adhere to ileal villi, colonize intensively and cause profuse diarrhea when given to newborn pigs. The K88, K99, and 987P pili are also designated F4, F5, and F6, respectively. However, there are also some enterotoxigenic strains that produce none of the three antigens.38 K88+ produces heat-labile enterotoxin (LT), the 987P+ and the K99+ do not produce LT, and all three types produce heat-stable enterotoxin STa in infant mice. Some isolates produce neither LT or STa but produce enterotoxin in ligated intestinal loops of pigs (STb). The K99+ piliated strains are a major cause of enteric disease in piglets under 2 weeks of age.1 Strains of enterotoxigenic E. coli that produce 987P pili colonize the small intestines and cause diarrhea in neonatal pigs under 6 days of age but not older pigs. Other ‘nonclassical’ strains colonize the small intestine to a certain extent, do not strongly adhere to the intestinal epithelium, and produce enterotoxin and diarrhea in neonatal piglets. Vaccination of a sow population for several years with vaccines containing O149 and K88 antigens may change the pattern of virulent E. coli inducing neonatal diarrhea during the first week of life so that other serogroups may dominate.
The porcine enterotoxigenic E. coli strains which induce fluid secretion in the intestine of piglets less than 2 weeks of age but not in older pigs are designated class 2, whereas those strains which induce fluid secretion in the intestines of older pigs are class 1 enterotoxigenic E. coli. The bovine strains of enterotoxigenic E. coli have several features in common with the porcine class 2 organisms which include the possession of the 0 antigens 8, 9, 20, or 101, characterization as mucoid colonies, possession of K99+ pili and production of heat-stable enterotoxin. Most strains of enterotoxigenic E. coli of pigs belong to a restricted number of serogroups.
Enterotoxigenic strains of E. coli can be isolated from the feces of approximately 35% of diarrheic lambs. Enterotoxigenic strains of E. coli have also been isolated from the blood of a small percentage of diarrheic lambs. K99 piliated E. coli are associated with outbreaks of diarrhea in lambs under a few days of age. F17 fimbriae E. coli have been isolated from diarrheic lambs and kids but none of the isolates produced any of the toxins normally associated with enteropathogenic strains. Attaching and effacing E. coli negative for verocytotoxin but positive for eae have been isolated from goat kids affected with severe diarrhea with a high case fatality rate.
An enterotoxigenic strain of E. coli with some evidence of K99 and F41 pilus antigens, K87 capsular antigens and serotype 101 somatic antigen has been isolated from newborn foals affected with diarrhea. However, they are not considered to be major pathogens in foals. The strains of E. coli isolated from the feces of diarrheic and healthy foals are very diverse and enterotoxigenic strains of the organism are not implicated in sporadic foal diarrhea. The isolates of E. coli obtained from the blood and tissues of septic foals are different from those obtained from the feces of healthy foals.39 Isolates from septic foals were resistant to equine serum. Some isolates of E. coli from septic foals contained conjugal plasmids that encoded resistance to multiple antimicrobial agents linked to equine serum resistance and to the production of aerobactin, which permits the growth of the organisms in an iron-limited environment, a trait considered a virulence determinant.
Zoonotic implications of E. coli
Cattle are a major source of E. coli O157:H7, which infects and causes food-borne disease in humans.4,5 Several strains of enterohemorrhagic E. coli associated with enteric disease in humans produce a verotoxin also known as a Shiga-like toxin. The literature on the epidemiology and virulence mechanisms of E. coli O157:H7 has been reviewed.4,5 (See ‘Enterohemorrhagic Escherichia coli in farm animals and zoonotic implications’, below.)
PATHOGENESIS
The factors important in understanding the pathogenesis of colibacillosis are the immune status of the animal and the virulence attributes of the strain of E. coli, particularly its capacity to invade tissues and produce a septicemia, or to produce an enterotoxin that causes varying degrees of severity of diarrhea. Septicemia, bacteremia, diarrhea, dehydration, and metabolic acidosis are the major pathogenetic events in the various forms of colibacillosis.
Septicemic colibacillosis (coliform septicemia)
This occurs in all species as a result of invasive strains of E. coli invading the tissues and systemic circulation via the intestinal lumen, nasopharyngeal mucosa and tonsillar crypts, or umbilical vessels. The intestinal permeability to macromolecules in the newborn piglet may predispose to the invasion of septicemia-inducing E. coli. These strains are able to invade extraintestinal tissues, to resist the bactericidal effect of complement, to survive and multiply in body fluids, to escape phagocytosis and intracellular killing by phagocytes, and to induce tissue damage by the release of cytotoxins. Calves and piglets that are deficient in colostral immunoglobulins are highly susceptible to septicemia. Colostrum provides protection against colisepticemia but may not prevent diarrhea associated with E. coli. Also, colostrum-fed calves are much more resistant to endotoxin than colostrum-deprived calves. Calves, piglets, and lambs that have normal levels of serum immunoglobulins are generally protected from septicemia. The clinical findings and lesions in septicemic colibacillosis are attributable to the effects of endotoxin, which causes shock. The general effects of endotoxin in cattle include hypothermia, decreased systemic blood pressure, tachycardia and decreased cardiac output, changes in blood counts, alterations in blood coagulation, hyperglycemia followed by hypoglycemia, and depletion of liver glycogen. Animals that recover from septicemia or bacteremia may develop lesions due to localization in other organs at varying periods of time later. Arthritis is a common sequel in calves, foals, and lambs. Meningitis is common in calves and piglets. Polyserositis due to E. coli has been recorded in pigs.
Enteric colibacillosis
Enterotoxigenic colibacillosis
Enterotoxigenic strains of E. coli colonize and proliferate in the upper small intestine and produce enterotoxins, which cause an increase in net secretion of fluid and electrolytes from the systemic circulation. The adhesion of E. coli to the intestinal epithelial cells is mediated by bacterial pili. The enterotoxigenic form of colibacillosis occurs most commonly in calves and piglets and less commonly in foals and lambs.
The factors that allow or control the colonization and proliferation of these strains and their production of enterotoxin are not well understood. The bacterial fimbriae attach to specific receptor sites on villous epithelial cells, following which the bacteria multiply and form microcolonies that cover the surface of the villi. The capsular polysaccharide of E. coli may also be involved in adhesion and colonization. The fimbriae of E. coli are strongly immunogenic, a factor that is utilized in the production of vaccines. Experimentally, the intestinal fluid from the most proximal small intestine of calves is more suppressive of K99+ pilus expression than fluid from more distal segments of the small intestine. Thus any factor that results in an increase of the pH in the lumen may allow the proliferation of the organism and, conversely, lowering the pH may reduce the severity of colibacillosis.
Diarrhea, dehydration, metabolic acidosis and electrolyte imbalance
The production of the enterotoxin results in net secretion of fluid and electrolytes from the systemic circulation into the lumen of the intestine, resulting in varying degrees of diarrhea, dehydration, electrolyte imbalances, acidosis, hyperkalemia when the acidosis is severe, circulatory failure, shock and death. The hyperkalemia in calves with neonatal diarrhea and acidosis has been associated with cardiac rate and rhythm abnormalities, including bradycardia and atrial standstill.40 The response to the enterotoxin in calves and piglets is similar to cholera enterotoxin in humans and takes place through an intact mucosa. Enterotoxin stimulates mucosal adenylcyclase activity, leading to an increase in cyclic adenosine monophosphate (AMP), which increases intestinal fluid secretion. The secretion originates primarily in the intestinal crypts but the villous epithelium also has a secretory function. The fluids secreted are alkaline and, in comparison to serum, isotonic, low in protein and high in sodium and bicarbonate ions. Distension of the right abdomen of diarrheic calves may occur, which may be associated with fluid distension of the abomasum and the intestines.41
When the disease is confined to the intestine, it responds reasonably well to treatment in the early stages. If death occurs, it is due to acidosis, electrolyte imbalance, and dehydration. The acid–base and electrolyte changes in piglets 1–3 days of age infected naturally and experimentally with enterotoxigenic E. coli reveal a severe dehydration and metabolic acidosis.
Severe metabolic changes can occur in calves with diarrhea. If the disease is progressive, the acidosis becomes more severe, lactic acidosis develops because of a reduced ability to utilize lactic acid, and severe hypoglycemia may occur because of a reduced rate of conversion of lactic acid to glucose. If extensive fluids are lost, hypovolemia and shock occur. The blood oxygen-binding capacity may be impaired in calves with diarrhea and severe dehydration.39
The most commonly accepted explanations of the metabolic acidosis in diarrheic calves are fecal bicarbonate loss and l-lactic acidosis. l-lactic acidosis is thought to occur from inadequate perfusion because of dehydration or endotoxemia, with subsequent anaerobic glycolysis and decreased clearance of l-lactate. However, neonatal diarrheic calves have high serum concentrations of d-lactate, with relatively low serum l-lactate concentrations.42-44 d-lactic acidosis is a contributory factor in calves with high anion gap acidosis. The anion gap significantly correlates with d- and total dl-lactate concentrations in serum but not with serum l-lactate concentrations.44 The elevated serum and urine concentrations of serum d-lactate are probably gastrointestinal in origin and the rumen and colon in diarrheic calves are considered as sites for the sources of d-lactate.43
The anion gap is defined as the sum of the major cations minus the sum of the major anions and is a measure of ‘unmeasured anions’:
Anion gap = [Na+] + [K+] − [Cl−] − [HCO3−].
The anion gap may be changed in numerous disturbances, including those of acid–base imbalance, and is useful in the interpretation of acid–base findings, but is of no value in assessing the intrinsic severity of acid–base disturbances.
Diarrheic calves are generally hyperkalemic with a high serum anion gap, a depressed serum bicarbonate and a low blood pH.
The severity and nature of the acidosis in diarrheic calves varies with the age of the calf. Diarrheic calves under 1 week of age often have a lactic acidosis, while those over 1 week of age have a nonlactic acidosis. Younger calves tend to dehydrate more rapidly and severely than older calves, which may be related to the greater incidence of enterotoxigenic colibacillosis in the young age group. The severity of dehydration, hypothermia, and metabolic acidosis is associated with the level of mental depression.45 The clinical signs and age of the calf can be used to predict the severity of acidosis; the more severe the acidosis, the greater the depression.
Metabolic acidosis without clinical evidence of dehydration occurs in some calves that have had a history of diarrhea in the previous several days.46 A similar syndrome has been described in goat kids. The pathogenesis is unclear but is thought to be associated with diarrhea in the preceding several days. One possibility is an inadequate amount of bicarbonate in the fluids and electrolytes used for the treatment of the dehydration.
Hyperkalemia in the diarrheic calf
Hyperkalemia is most common in dehydrated diarrheic calves that are severely acidotic. The potassium moves out of the intracellular space into the extracellular space, resulting in hyperkalemia. The predominant clinical finding is bradycardia (heart rate < 90 bpm) in a dehydrated diarrheic calf. However, hypoglycemia and hypothermia may be associated with bradycardia in a similar calf.
Hypernatremia in the diarrheic calf
Acute hypernatremia may occur in diarrheic calves.46,47 Clinical findings are nonspecific and include depression, weakness, dehydration, and diarrhea. Laboratory determination of serum electrolytes is necessary to make the diagnosis. The serum sodium concentration is above 160 mEq/L. It is presumed that mixing errors in the preparation of oral electrolyte solutions for diarrhea is the cause. The experimental oral administration of 1 L of electrolyte concentrate containing 2750 mEq sodium found that calves would willingly consume the solution mixed with milk and developed signs of hypernatremia within 6 hours of administration.
Hypernatremia (serum sodium > 153 mEq/L) in neonatal elk calves has been described.48 The most common clinical findings were diarrhea, dehydration, depression, and anorexia.
Effect of colostral immunoglobulin status
An adequate level of serum immunoglobulins protects calves from death due to the effects of diarrhea, but not necessarily from diarrhea. The best protection is provided if both the immunoglobulin levels in the serum and the levels in the colostrum and milk during the first week after birth are high. The immunoglobulin subclasses in the plasma of calves that have received sufficient colostrum are IgG, IgM (and IgM is probably the more important of the two for the prevention of septicemia) and IgA. The serum IgG concentrations of calves under 3 weeks of age dying from infectious disease were much lower than in normal calves. Of the dead calves 50% had serum IgG levels that were more than 2 standard deviations below the normal mean, and an additional 35% had concentrations greater than 1 standard deviation below the normal mean. In the intestine, no single subclass of immunoglobulin is known to be responsible for protection against the fatal effects of diarrhea. Individually, each immunoglobulin subclass can prevent death from diarrhea even though calves may be affected with varying degrees of diarrhea. In contrast to the situation in the pig, IgA appears to be least effective.
In pigs, IgA becomes the dominant immunoglobulin in sow colostrum after the first few days of lactation, and this is the immunoglobulin that is not absorbed but is retained in, and reaches a high level in, the gut and plays a major role in providing local protection against enteric colibacillosis in piglets. Porcine colostral IgA is more resistant to gastrointestinal proteolytic enzymes than IgG2 and IgM. On the other hand, IgG is at a peak concentration in colostrum in the first day after parturition, is readily absorbed by the newborn piglet and is vital in providing protection against septicemia. Lysozyme in sows’ milk may assist in the control of the bacterial population in the gut of the unweaned piglet.
Intestinal mucosa
In general, the enterotoxigenic E. coli exert their effects by the enterotoxin causing hypersecretion through an intact intestinal epithelium. However, the intraluminal exposure of the jejunum of 3-week-old pigs to sterile crude culture filtrates from strains of E. coli known to produce two types of heat-stable enterotoxin will induce microscopic alterations of the villous epithelium. Focal emigration of neutrophils, especially through the epithelium above aggregated lymphatic follicles, stunting of jejunal and ileal villi, and adherence of bacteria to jejunal and ileal mucosae are the most consistent finding. These changes are useful in making the diagnosis of enterotoxigenic colibacillosis in calves. While enterotoxigenic strains are considered to be noninvasive this does not preclude the possibility that invasion into the systemic circulation may occur, resulting in septicemia, or that septicemic strains may not also be present.
Enzyme histochemistry studies of the small intestinal mucosa in experimental infections of calves with rotavirus and enterotoxigenic E. coli indicate a marked decrease in enzyme activity in dual infections and a lesser decrease in monoinfections. Increased enzyme activity occurred in parts of the intestinal mucosa that were not affected or only slightly affected by the enteropathogens, which may be an adaptation of the mucosa to maintain absorptive function. Lactose digestion is slightly impaired in calves with mild diarrhea. Calves with acute diarrhea are in a catabolic state and respond with a larger increase of plasma glucose concentration to a given amount of absorbed glucose than do healthy calves.49 Fat and carbohydrate malabsorption frequently occurs in diarrheic calves over 5 days of age and may contribute to the death of these animals in cold weather.
Attaching and effacing colibacillosis
Attaching and effacing enteropathogenic E. coli can cause naturally occurring diarrhea and dysentery in calves at 18–21 days.1 They do not produce enterotoxin but adhere to the surface of the enterocytes of the large intestine. Affected calves pass bright red blood in the diarrheic feces. The lesions in experimentally infected calves are indistinguishable from those produced by some E. coli that are enteropathogenic for humans, rabbits, and pigs. They do not produce enterotoxin. The bovine O118:H16 enterohemorrhagic E. coli strain is able to colonize the intestine of newborn calves and to induce diarrhea 24 hours after challenge and to produce attaching and effacing lesions in the small and large intestines.50
Synergism between enteropathogens
Enterotoxigenic colibacillosis occurs naturally and can be reproduced experimentally using enterotoxigenic E. coli in calves under 2 days of age but not in calves 1 week of age. Diarrheic calves older than 3 days of age may be infected with enterotoxigenic K99+ E. coli and rotavirus. There is evidence that prior or simultaneous infection of the intestine with rotavirus will enable the E. coli to colonize in older calves.1 Thus, there may be synergism between rotavirus and enterotoxigenic E. coli in calves older than 2 days; this may explain the fatal diarrhea that can occur in calves at 1 week of age, which normally would not be fatal with a single infection. The rotavirus may enhance colonization of the E. coli. In the Kashmir valley of India, diarrheic lambs from birth to 3 months of age are commonly infected with group A rotavirus and pathogenic serogroups of E. coli O26, O113, O157, all of which are pathogenic to humans.51
The simultaneous experimental infection of neonatal gnotobiotic calves at 24 hours of age with rotavirus and enterotoxigenic E. coli results in a severe diarrheal disease. The same situation occurs in piglets. However, in both species the effect was considered to be additive rather than synergistic.
Summary of pathogenesis
Septicemic colibacillosis occurs in newborn animals that are agammaglobulinemic because they have not ingested sufficient colostrum early enough, or have absorbed insufficient colostral immunoglobulins, thus rendering them highly susceptible. Enteric colibacillosis occurs in colostrum-fed animals and is associated with the colonization and proliferation of enteropathogenic E. coli, which produce enterotoxin and cause varying degrees of diarrhea and acidosis and dehydration. While single infections occur commonly, as in piglet diarrhea, and what was previously described as enteric–toxemic colibacillosis in calves, multiple infections with enteropathogenic E. coli and viruses and other agents are more common.
CLINICAL FINDINGS
Calves
Coliform septicemia
This is most common in calves during the first 4 days of life. Most affected calves have low levels of serum colostral immunoglobulins because of inadequate transfer of colostral immunoglobulins.16 The illness is peracute, the course varying from 24–96 hours with a survival rate of less than 12%.16 There are no diagnostic clinical signs. Affected animals are depressed and weak, commonly recumbent, and dehydrated; tachycardia is present and, although the temperature may be high initially, it falls rapidly to subnormal levels when the calf becomes weak and moribund. The suck reflex is weak or absent, the oral mucous membranes are dry and cool, and the capillary refill time may be prolonged. Cold extremities, weak peripheral pulse and prolonged capillary refill time are common. Scleral injection is common. Diarrhea and dysentery may occur but are uncommon.
Multiple body system and organ involvement is characteristic of neonatal septicemia and careful clinical examination is required to detect abnormalities. If a calf survives the septicemic state, clinical evidence of postsepticemic localization may appear in about 1 week. This includes arthritis, meningitis, panophthalmitis and, less commonly, pneumonia. In a series of 32 cases of meningitis in neonatal calves, the most frequent clinical findings were lethargy, anorexia, recumbency, loss of the suck reflex, stupor, and coma.52 Opisthotonos, convulsions, tremors, and hyperesthesia were seen less frequently. The case fatality rate was 100% in spite of intensive therapy, and lesions of septicemia were present at necropsy.
Predictors of septicemia
The early clinical findings of septicemia in neonatal foals and calves are vague and nonspecific and are often indistinguishable from the findings of noninfectious diseases or those of focal infections such as diarrhea. Positive blood cultures are required for a definitive diagnosis of septicemia, but results are not usually available for 48–72 hours, and false negatives are common. A clinical sepsis scoring system for predicting bacteremia in neonatal dairy calves has been described but has not been adequately evaluated in the field.53,54
No single laboratory test has emerged as being completely reliable for the early diagnosis of septicemia in farm animal neonates and therefore scoring systems and predictive models using obtainable historical, clinical and clinicopathological data have been developed. The goal of these mathematical models is to identify septicemic neonates early in the course of disease when appropriate therapy would be most likely to result in a favorable outcome.55 In a study of diarrheic calves under 28 days of age submitted to a referral clinic for treatment, 31% of the calves were septicemic, based on blood culture.55 Two models to predict septicemia were used. Clinicopathological variables associated with an increased risk of septicemia were moderate (1.99– 5.55 mg/dL) and marked (> 5.66 mg/dL) increases in serum creatinine (OR 8.63), moderate to marked toxic changes in neutrophils (OR 2.88), and failure of transfer of passive immunity (IgG concentrations β 800 mg/dL, globulin β 2 g/dL (OR 2.72), and total serum protein β 5 g/dL). The clinical variables associated with an increased risk of septicemia were age under 5 days (OR 2.58), focal infection (OR 2.45), recumbency (OR 2.98), and weak suck reflex (OR 4.10).55
Enteric colibacillosis
This is the most common form of colibacillosis in newborn calves, primarily 3–5 days of age. It may occur in calves as early as 1 day of age and only rarely up to 3 weeks. The clinical severity will vary depending upon the number and kind of organisms causing the disease. The presence of a single enterotoxigenic strain of E. coli may cause a state of collapse usually designated as enteric toxemia. In this form of the disease the outstanding clinical signs include severe weakness, coma, subnormal temperature, a cold clammy skin, pale mucosae, wetness around the mouth, collapse of superficial veins, slowness and irregularity of the heart, mild convulsive movements, and periodic apnea. Diarrhea is usually not evident, although the abdomen may be slightly distended and succussion and auscultation may reveal fluid-splashing sounds suggesting a fluid-filled intestine.41 The prognosis for these calves is poor and they commonly die 2–6 hours after the onset of signs.
In the more common form of the disease in calves, there is diarrhea in which the feces are profuse and watery to pasty, usually pale yellow to white in color, and occasionally streaked with blood flecks and very foul-smelling. The dry matter content of the feces is commonly below 10%. Defecation is frequent and effortless, and the tail and perineum are soiled with feces. The temperature is usually normal in the initial stages but becomes subnormal as the disease worsens. Affected calves may or may not suck or drink depending on the degrees of acidosis, dehydration, and weakness. Calves under 8 days of age may be weak, primarily from the effects of rapid and severe dehydration; in calves older than 8 days the acidosis may be more severe and makes a greater contribution to depression and weakness. In the early stages of the disease, the abdomen may be slightly distended as a result of distension of fluid-filled intestines, which can be detected by succussion and auscultation of the abdomen. In some of these calves the diarrhea is not obvious but is delayed for several hours, when it can be quite profuse. Mildly to moderately affected calves may be diarrheic for a few days and recover spontaneously with or without treatment. However, 15–20% of calves with enteric colibacillosis become progressively worse over a period of 3–5 days, gradually become more weak, lose the desire to suck and progressively appear more obviously clinically dehydrated.
Throughout the course of the diarrhea the degree of dehydration will vary from just barely detectable clinically (4–6% body weight (BW)) to up to 10–16% of body weight. It is best assessed by ‘tenting’ the skin of the lateral portion of the cervical region and measuring the time required for the skin fold to return to normal.56 In calves with 8% of dehydration, 5–10 seconds will be required for the skin fold to return to normal; in 10–12% dehydration up to 30 seconds. Recession of the eyeball (enophthalmos) is a reliable and obvious indication of the degree of dehydration. Slight sinking of the eyeball without an obvious space between the eyeball and the orbit represents 6–8% dehydration; moderate separation of the eyeball from the orbit represents 9–12% dehydration; and marked separation of the eyeball from the orbit represents over 12% and up to 16% dehydration. A summary of the relationship between degree of dehydration (% BW), depth of enophthalmos (mm), cervical skin tent duration in seconds and the state of the mucous membranes and extremities in calves with experimentally induced diarrhea is set out in Table 18.4.56
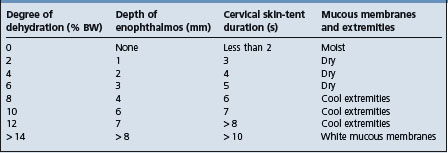
Death usually occurs in 3–5 days. Affected calves can lose 10–16% of their original body weight during the first 24–48 hours of the diarrhea. The hyperkalemia in calves with neonatal diarrhea and acidosis has been associated with cardiac rate and rhythm abnormalities including bradycardia and atrial standstill. Herd outbreaks of the disease in beef calves may last for several weeks, during which time almost every calf will be affected within several days after birth.
Veal calf hemorrhagic enteritis is a fatal syndrome of veal calves characterized by anorexia, fever, diarrhea with mucus-containing feces which become bloody in the later stages, and hemorrhagic diathesis on the conjunctivae and mucous membranes of the mouth and nose. The etiology is unknown; the E. coli strains isolated from the feces of affected calves produced enterotoxins and verocytotoxins but their significance is uncertain.
In some calves between 10 and 20 days of age with a history of diarrhea in the previous several days, from which they have recovered, there will be metabolic acidosis without clinical signs of dehydration.45 Affected calves are depressed, weak, ataxic and sometimes recumbent, and appear comatose. Affected calves respond quickly to treatment with intravenous sodium bicarbonate. A similar syndrome occurs in goat kids.
Lambs and goat kids
Although some cases manifest enteric signs, and chronic cases may occur, colibacillosis in lambs is commonly septicemic and peracute. Two age groups appear to be susceptible: lambs 1–2 days of age and lambs 3–8 weeks old. Peracute cases are found dead without premonitory signs. Acute cases show collapse and occasionally signs of acute meningitis manifested by a stiff gait in the early stages, followed by recumbency with hyperesthesia and tetanic convulsions. Chronic cases are usually manifested by arthritis. The disease in goat kids is similar to that in lambs.
Piglets
Coliform septicemia
This is uncommon but occurs in piglets within 24–48 hours of birth. Some are found dead without any premonitory signs. Usually more than one, and sometimes the entire litter, are affected. Severely affected piglets seen clinically are weak, almost comatose, appear cyanotic, and feel cold and clammy and have a subnormal temperature. Usually there is no diarrhea. The prognosis for these is poor and most will die in spite of therapy.
Enterotoxigenic colibacillosis (newborn piglet diarrhea)
This is the most common form of colibacillosis in piglets and occurs from 12 hours of age up to several days of age, with a peak incidence at 3 days of age. As with the septicemic form, usually more than one pig or the entire litter is affected. The first sign usually noticed is the fecal puddles on the floor. Affected piglets may still nurse in the early stages but gradually lose their appetite as the disease progresses. The feces vary from a pasty to watery consistency and are usually yellow to brown in color. When the diarrhea is profuse and watery there will be no obvious staining of the perineum and hindquarters with feces but the tails of the piglets will be straight and wet. The temperature is usually normal or subnormal. The disease is progressive; diarrhea and dehydration continues, the piglets become very weak and lie in lateral recumbency and make weak paddling movements. Within several hours they appear very dehydrated and shrunken, and commonly die within 24 hours after the onset of signs. In severe outbreaks the entire litter may be affected and die within a few hours of birth. The prognosis is favorable if treatment is started early before significant dehydration and acidosis occur.
CLINICAL PATHOLOGY
Culture and detection of organism
If septicemia is suspected, blood should be submitted for isolation of the organism and determination of its drug sensitivity. Blood for culture is taken aseptically from the jugular vein and inoculated directly into brain–heart infusion broth.16 At least one additional blood sample is taken a few hours later in order to enhance recovery rate and confirm septicemia.
The definitive etiological diagnosis of enteric colibacillosis depends on the isolation and characterization of the E. coli from the intestines and the feces of affected animals. The best opportunity of making a diagnosis is when untreated representative affected animals are submitted for pathological and microbiological examination. The distribution of the organism in the intestine and determination of the presence of K88+, K99+ or 987P antigens, the demonstration of enterotoxin by infant mouse test or ligated intestinal loops, and the histopathological appearance of the mucosa all contribute to the diagnosis.
The routine culture of feces and intestinal contents for E. coli without determining their virulence determinants is of limited value. The laboratory tests used to identify enterotoxigenic K99+ E. coli include a direct fluorescent antibody technique with conventional culturing methods and the ELISA, with or without monoclonal antibody, to detect the organism or the enterotoxin in the feces. DNA gene probes specific for genes encoding enterotoxin and adhesins are available and are being used to evaluate E. coli isolated from diarrheic animals. Isolates of the organism can also be examined for the presence of toxins using an enzyme immune assay test and latex agglutination test.
Detection of verocytotoxic E. coli in feces has relied on cytotoxicity testing and DNA hybridization. Several ELISAs are available, and monoclonal antibodies to the verocytotoxins VT1 and VT2 have been used to examine feces from animals.57 The isolation of E. coli O157H:7 has relied on its ability to ferment sorbitol. A sandwich ELISA using monoclonal antibodies to E. coli verocytotoxins 1 and 2 for capture and detection is available for detection of verocytotoxin-producing E. coli in animal feces.57 A PCR test is also available for detection of verocytotoxin genes in E. coli isolated from cattle, sheep, and pigs affected with diarrhea.58
The determination of drug sensitivity of the E. coli isolated from the feces of diarrheic calves and piglets is commonly done but is of limited value without determining which isolate is enteropathogenic.
Hematology and serum biochemistry
A total and differential leukocyte count and remarkable changes in the fibrinogen concentration may indicate the presence of a septicemia or severe intestinal infection.16 However, severely affected calves may not have grossly abnormal hemograms. In enteric disease, the major changes in plasma composition are dehydration, electrolyte imbalance, and acidosis. The total plasma osmolality is decreased.
The changes in the blood biochemical and hematological profile of normal neonatal calves with age have been described.59 The packed cell volume and the total solids concentration of the blood will indicate the degree of dehydration, and the blood urea nitrogen may be increased in severe cases because of inadequate renal perfusion. The blood bicarbonate values are markedly reduced, blood pH values represent acidosis, and the other serum electrolytes are variable. Calves with a venous blood pH below 7.0 are at high risk and require immediate parenteral therapy for acidosis. There is usually a decrease in serum sodium, chloride, and potassium. In severe cases of acidosis, hyperkalemia may occur; this is cardiotoxic and affected calves may die while being handled in preparation for intravenous therapy.
Harleco apparatus
The acid–base status of individual calves can be determined in the field using a simple total carbon dioxide apparatus, which provides values close to blood bicarbonate concentrations.60 Unlike the blood gas machines, the Harleco apparatus offers clinicians in practice an affordable means of diagnosing metabolic acidosis.61 The Harleco measures ‘total carbon dioxide’, the carbon dioxide liberated from a blood sample by adding strong acid. Nearly all the carbon dioxide is derived from bicarbonate rather than blood carbon dioxide. The CO2 liberated is derived from bicarbonate and from dissolved CO2, but there is so little dissolved CO2 in blood that the Tco2 may be taken for clinical purposes as a measurement of plasma bicarbonate. The level of acidosis in calves can be classified according to the Harleco readings (total carbon dioxide, mmol/L) as follows:
| Normal | 21.1–28 |
| Mild | 16.6–21 |
| Moderate | 12.1–16.5 |
| Severe | 8.1–12.0 |
| Very severe | < 8. |
The strong ion difference method of evaluating acid–base balance in cattle has been described and justified to identify the mechanism for a change in acid–base balance and thereby to focus treatment on the inciting cause, and to quantify unmeasured strong anion concentration in plasma.62 A comparison of the measurement of total carbon dioxide and strong ion difference (SID) for the evaluation of metabolic acidosis in calves did not find any advantage to the SID.61
Portable pH meter
A portal pH meter has been evaluated to measure blood pH in neonatal calves.63 Compared to a blood gas analyzer, the portable pH meter was more accurate in measuring urine pH and ruminal fluid pH in cows than blood pH in neonatal calves.
Serum immunoglobulins
The determination of the level of serum immunoglobulins of diarrheic calves may be valuable in assessing prognosis and to determine the intensity of the therapy required for survival. However, the level of serum immunoglobulins as a measure of susceptibility or prognosis is most accurate at 24 hours after birth. After this period, it is unreliable because the serum immunoglobulins may be increased in response to septicemia, increased spuriously in dehydration and decreased in enteric disease.
Several tests are available to assess transfer of passive immunity status in domestic animals.8 The radial immunodiffusion test and the ELISA are the only tests that directly measure serum IgG concentration. All other available tests, including serum total solids by refractometry, sodium sulfite turbidity tests, zinc sulfate turbidity tests, serum gamma-glutamyl transferase (GGT) and whole-blood glutaraldehyde coagulation, estimate serum IgG concentration based on concentration of total globulins or other proteins whose transfer is statistically associated with that of IgG.
Radial immunodiffusion
The radial immunodiffusion is the gold standard for measurement of serum IgG concentration. However, it is too expensive for most situations and requires considerable time before results are available.
Commercial immunoassay
An immunoassay using blood is now available for evaluating transfer of passive immunity in calves.64 The whole blood immunoassay kit consists of a 4 mm lateral flow membrane strip enclosed in a plastic test device. Test kits are incubated for 20 minutes. If the sample IgG concentration is 10 mg/mL or more, a single red line develops, indicating adequate transfer of passive immunity and a negative test result. If the sample IgG concentration is <10 mg/mL, two lines develop on the membrane slip, indicating failure of transfer of passive immunity and a positive test. The sensitivity and specificity of the blood IgG immunoassay were 0.93 and 0.88 respectively, compared with 1.00 and 0.53 for the sodium sulfite test. For refractometry, sensitivity and specificity were 0.71 and 0.83 respectively, when a serum total solids concentration of 5.2 g/dL was used as the cutoff between positive and negative results.
Serum total solid concentration by refractometer
The measurement of serum total protein by refractometer is an estimate of serum immunoglobulin concentration.65 Recommended test endpoints for serum protein concentrations have varied from 5.0–6.0 g/dL. Three refractometers, including a non-temperature-compensating instrument, provided similar results. Serum protein concentration test endpoints of 5.0 and 5.2 g/dL gave accurate results in the assessment of adequacy of transfer of passive immunity; lower or higher test endpoints misclassified large numbers of calves. The test is excellent for herd monitoring and is easily performed in the field. In clinically ill dehydrated calves, a test endpoint of 5.5 g/dL should be used when assessing adequacy of transfer of passive immunity.66 In a healthy, adequately hydrated calf a serum total protein of 5.2 g/dL or greater is associated with adequate transfer of passive immunity.8
The mortality risk associated with inadequate transfer of passive immunity in dairy calves can be partitioned using the observed population mortality and the relative risk of mortality in each serum protein concentration stratum.67 For a total of 3479 calves studied, 8.2% died before 16 weeks of age. The population baseline mortality rate was 5.0% and the mortality rate due to inadequate transfer of passive immunity was 3.2%. Thirty-nine percent of the observed mortality was attributed to inadequate transfer of passive immunity. Such partitioning of risk between sources related and unrelated to transfer of passive immunity can be useful in conducting investigations of calf mortality in dairy herds.
Sodium sulfite turbidity test
The sodium sulfite turbidity test is a three-step semiquantitative test using 1, 4, 16, and 18% sodium sulfite test solutions. The solutions cause selective precipitation of high-molecular-weight proteins, including immunoglobulins. Optimum diagnostic utility is attained using a 18% test solution. The mean serum IgG concentrations of calves at the 1+, 2+, and 3+ endpoints of test turbidity were 1250, 2116, and 2948 mg/dL, respectively.8
Serum gamma-glutamyl transferase activity
The serum levels of GGT are also reliable indicators of the level of transfer of passive immunity in newborn calves.68 Calves classified as having failure of transfer of passive immunity (< 800 mg IgG/dL) had a 9.5 times greater risk of becoming sick prior to weaning at 5 months of age compared with calves determined to have partial failure of transfer of passive immunity and clinically normal calves. In 1-day-old calves, serum GGT activity should be more than 200 IU/L; in 4-day-old calves it should be more than 100 IU/L and in 1-week-old calves more than 75 IU/L. Calves with GGT activity below 50 IU/L within the first 2 weeks of life should be considered to have failure of transfer of passive immunity. The sensitivity and specificity of cutoff value of 200 IU of GGT of serum for a diagnosis of failure of transfer of passive immunity are 80% and 97%, respectively. The sensitivity and specificity of a cutoff value of 4.2 g of protein/dL of serum for diagnosing failure of transfer of passive immunity were 80% and 100%, respectively.68
Recent studies have shown that GGT activity has no apparent advantage relative to other tests for predicting transfer of passive immunity in beef calves.8
The relationships between serum and colostrum/milk GGT activities and IgG concentration can be used to assess the transfer of passive immunity status of lambs.69 Regression models were used to calculate serum and colostrum/milk GGT activities, and it was moderately accurate in predicting serum IgG concentration. The GGT activity can be used as an alternative to single radial immunodiffusion, which is complex, expensive, and time-consuming for estimation of IgG concentration.
NECROPSY FINDINGS
In coliform septicemia there may be no gross lesions and the diagnosis may depend upon the isolation of the organism from the filtering organs. In less severe cases there may be subserosal and submucosal hemorrhages. A degree of enteritis and gastritis may be present. Occasionally, fibrinous exudates are found in the joints and serous cavities, and there may be omphalophlebitis, pneumonia, and meningitis. The histological features of such presentations of colibacillosis are those of septicemia and toxemia.
In enteric colibacillosis of piglets and calves the carcass appears dehydrated but the intestine is flaccid and fluid-filled. In calves, the abomasum is usually distended with fluid and may contain a milk clot. This clot is typically absent in calves fed milk replacers containing heat-denatured skim milk powder or noncasein milk products such as whey powder. The abomasal mucosa may contain numerous small hemorrhages. In both calves and pigs, the intestinal mucosae may appear normal or hyperemic and there may be edema of the mesenteric lymph nodes. Mild atrophy or even fusion of jejunal and ileal villi is often seen, but the key microscopic observation is the presence of bacilli adherent to the brush borders of enterocytes. Ultrastructurally, there is increased epithelial cell loss from the villus about 12 hours after experimental inoculation of calves with an enterotoxigenic E. coli.
In calves affected with attaching and effacing E. coli there is pseudomembranous ileitis as well as mucohemorrhagic colitis and proctitis. Microscopic examination of well-preserved gut segments reveals bacterial adherence, atrophy of ileal villi, and erosion of enterocytes.
In addition to traditional bacteriological culture techniques, the enterotoxigenic E. coli may be identified by several tests, including indirect fluorescent antibody tests (IFA) specific for K88+, K99+, and 987P pilus antigens. The IFA tests can be performed on impression smears or frozen sections of ileal tissue and the results are available within a few hours. Newer techniques such as DNA gene probes,12 enzyme immune assays and latex agglutination tests are now available to identify those isolates that are enterotoxin producers and have adhesin properties.
During severe disease outbreaks it is often necessary to conduct the necropsy examination on diarrheic animals that have been killed specifically for the purpose of obtaining a definitive etiological diagnosis. The combined use of bacteriological, parasitological, and virological methods, together with histological and immunofluorescent studies of fresh intestinal tissue, will provide the most useful information about the location of the lesions and the presence of enteropathogens. Postmortem autolysis of the intestinal mucosae and invasion of the tissues by intestinal microflora occurs within minutes after death, so gut samples should be collected immediately following euthanasia of the animal.
Samples for confirmation of diagnosis
Enteric colibacillosis
• Bacteriology – chilled segments of ileum and colon (including content) (CULT and/or FAT, latex agglutination, PCR)
• Histology – fixed duodenum, jejunum, ileum, colon, and mesenteric lymph node.
The definitive etiological diagnosis of septicemic colibacillosis is dependent on the laboratory isolation of the causative agent, which is usually a single species or organism. The septicemias of the newborn cannot be distinguished from each other clinically. The definitive etiological diagnosis of enteric colibacillosis in newborn calves and piglets may be difficult and often inconclusive because the significance of other organisms in the intestinal tract and feces of diarrheic animals cannot be easily determined.
Table 18.3 lists the possible causative agents of diarrhea and septicemia in newborn farm animals. Using the combined diagnostic approach of detection of enteropathogens in the feces before death, and in the intestinal mucosa after death, it is possible to identify where enterotoxigenic E. coli, rotavirus, coronavirus, Salmonella sp., and Cryptosporidium sp. appear to be the only or principal causative agents. However, as described earlier under acute undifferentiated diarrhea of newborn farm animals, mixed infections are more common than single infections.
Every effort that is economically possible should be made to obtain an etiological diagnosis. This is especially important when outbreaks of diarrhea occur in a herd or where the disease appears to be endemic. The use of an interdisciplinary approach will increase the success of diagnosis. This includes making a visit to the farm or herd and making a detailed epidemiological investigation of the problem. The diagnosis depends heavily on the epidemiological findings, the microbiological and pathological findings, and sometimes on the results of treatment.
The major difficulty is to determine whether or not the diarrhea is infectious in origin and to differentiate it from dietetic diarrhea, which is most common in hand-fed calves and in all newborn species that are sucking high-producing dams. In dietetic diarrhea the feces are voluminous and pasty to gelatinous in consistency; the animal is bright and alert and is usually still sucking, but some may be inappetent.
TREATMENT
Coliform septicemia
Intensive critical care is required for the treatment of neonatal coliform septicemia. Early identification of septicemia and early therapeutic intervention can improve treatment success. While E. coli may be cultured from the blood of septicemic calves, a significant percentage of isolates are Gram-positive, which justifies the use of antimicrobials that have a broad spectrum.16 Antimicrobials are given parenterally and may be given continuously intravenously, more than once daily and daily until recovery is apparent. Isolation of the organisms from blood and determination of drug sensitivity is the ideal protocol. Intravenous fluid and electrolyte therapy are administered continuously until recovery is apparent. Whole blood transfusions are used in calves and foals, especially when immunoglobulin deficiency is suspected from the history or is determined by measurement of serum immunoglobulins of blood (see Chapter 3 for details on measuring immunoglobulins using various tests). In one series on neonatal septicemia in calves, in which E. coli accounted for 50% of the bacterial isolates, the survival rate was only 12%.16
Enteric colibacillosis
The considerations for treatment of enteric colibacillosis include the following:
Fluid and electrolyte replacement
The dehydration, acidosis and electrolyte imbalance are corrected by the parenteral and oral use of simple or balanced electrolyte solutions. The provision of fluid therapy in diarrheic dehydrated calves under field conditions in veterinary practice has been described.68 It is important to obtain an adequate history of the case including age of the calf, duration of the diarrhea and all treatments already given by the owner. The physical examination of the calf includes a standard clinical examination with emphasis on evaluating the degree of dehydration and acidosis.
Dehydration is evaluated by two clinical observations:
• Skin elasticity. The skin of the middle of the neck is better than the eyelid. A portion of the skin is tented and twisted for 1 second, and then the time to return to the initial position is measured – less than 2 seconds in the normal calf, 6 seconds in moderate (8%) dehydration and more than 8 seconds in severe (12%) dehydration
• Position of eyeball in the orbit and extent of enophthalmos. This is determined by measuring the distance between the globe and the orbit. The eyeball is not sunken in healthy calves. Degrees of dehydration of 4%, 8, and 12% are represented by a 2 mm, 4 mm, and 7 mm enophthalmos, respectively.
Acidosis can be evaluated using the clinical findings of mental status, muscular tone, ability to stand, intensity of the sucking reflex, temperature of the inside of the oral cavity, and age of the calf that correlate with an estimate of the base deficit. The following categories for diarrheic calves are being used under field conditions:
1. Calves with good muscular tone and the ability to stand, strong suck reflex and warm oral cavity have no base deficit if younger than 8 days of age, and up to 5 mEq/L if older than 5 days
2. Calves that can stand, have a slightly cool oral cavity and weak suck reflex have a base deficit of 5 mEq/L if under 8 days of age and 10 mEq/L if older than 8 days
3. Calves in sternal recumbency with a cool oral cavity and no suck reflex have a base deficit of 10 mEq/L if under 8 days of age and 15 mEq/L if older than 8 days
4. Calves in lateral recumbency that lack a suck reflex and have a cold oral cavity have a base deficit of 10 mEq/L if under 8 days of age and 20 mEq/L if older than 8 days.
Categorizing diarrheic calves into treatment groups
Based on the history and clinical findings, affected calves can be divided into categories according to the type of therapy required and which is most economical.
1. Oral fluid therapy. Calves with a history of acute diarrhea, less than 7% dehydrated, slightly dry oral mucosa, good suck reflex, good muscle tone, alert, able to stand and warm mouth. These can be treated with oral fluids and electrolytes
2. Oral fluid therapy and hypertonic saline. Calves with 7–9% dehydration and slight acidosis, weak suck reflex, good muscular tone, warm mouth. Administer hypertonic saline (7.5% NaCl) intravenously at 3–4 mL/kg BW in 5 minutes. Administer oral fluids and electrolytes by stomach tube at 40– 60 mL/kg BW. Re-evaluate in 6–8 hours
3. Intravenous fluid therapy with alkalinizing agents. Calves are more than 9% dehydrated, dry and cool oral mucous membranes, recumbent, no suck reflex, very depressed. Provide intravenous replacement and maintenance fluid and electrolyte therapy for a period of 6–8 hours and up to 24–36 hours if necessary.
The details for parenteral and oral fluid and electrolyte therapy are described here.
Parenteral fluid and electrolyte therapy
In severe dehydration and acidosis, solutions containing the bicarbonate ion are indicated.
Parenteral fluid composition
An equal mixture of isotonic saline (0.85%), isotonic sodium bicarbonate (1.3%), and isotonic dextrose (5%) is a simple, effective solution for parenteral use. Sodium bicarbonate as an alkalinizing compound in the parenteral fluids is superior to the use of compounds such as sodium acetate or sodium lactate, which must be metabolized by the liver, myocardium, and other tissues in order to have an alkalinizing effect. The simple replacement of fluid losses using saline or fluids without alkalinizing compounds is likewise not as effective as sodium bicarbonate. Many commercial preparations are effective in correcting the dehydration and electrolyte imbalances, but only those containing bicarbonate or its precursors are effective in correcting the metabolic acidosis.45
Bicarbonate requirements to treat acidosis
The bicarbonate requirements (mmol) are calculated using the equation:
weight (kg) × base deficit (mmol/L) × 0.6 (extracellular fluid space).
The base deficit will range from –5 to –20 mmol/L with an average of about –15 mmol/L. The bicarbonate requirements for a 45 kg calf with a base deficit of 15 mmol/L, are 45 × 15 × 0.6 = 405 mmol, which requires 33.75 g of sodium bicarbonate (1 g of sodium bicarbonate yields 12 mmol of bicarbonate), which can be delivered in 2.5 L of 1.3% isotonic solution. Diarrheic calves over 8 days of age may be nearly twice as acidotic as younger calves and will require more bicarbonate to correct the acidosis. It is estimated that sternally recumbent calves under 8 days of age require 1 L of isotonic sodium bicarbonate to correct the acidosis, in addition to the necessary amounts of saline to correct the dehydration; for calves over 8 days of age, 2 L of isotonic sodium bicarbonate is necessary. For laterally recumbent diarrheic calves under and over 8 days of age, 1 and 3 L, respectively, is required. Isotonic sodium bicarbonate is a safe solution intravenously; when the degree of acidosis is uncertain, up to several liters can be used safely for the correction of acidosis and volume depletion.
For severe dehydration (10–12% BW) fluids should be replaced as follows: hydration therapy 100 mL/kg BW intravenously in the first 1–2 hours at the rate of 50–80 mL/kg BW per hour followed by maintenance therapy at 140 mL/kg BW over the next 8–10 hours at the rate of about 20 mL/kg BW per hour. For example, a 45 kg calf that is 10% dehydrated should receive 4.5 L of fluid in the first 1–2 hours as hydration therapy, followed by 6–8 L of fluid over the next 8–10 hours. Initially, both the acidosis and the dehydration can be treated by the use of isotonic sodium bicarbonate followed by the use of a combined mixture of isotonic saline and isotonic sodium bicarbonate or multiple electrolyte solutions for maintenance therapy. For moderate dehydration (6–8% of BW), fluids should be replaced as follows: hydration therapy 50 mL/kg BW intravenously in the first 1–2 hours at the rate of 50–80 mL/kg BW per hour followed by maintenance therapy as described above.
Maintenance therapy may be provided using oral fluids and electrolytes if the calf is well enough to suck from a nipple bottle or drink from a pail. The use of solutions containing potassium chloride is sometimes recommended, on the basis that total potassium stores may be depleted in severely affected calves. However, they should be used with caution because a severe hyperkalemia may be present when there is a severe acidosis. If the acidosis and hypoglycemia are corrected with glucose and bicarbonate, the administration of potassium may be beneficial in restoring total potassium stores. However, solutions containing potassium can be cardiotoxic, especially if renal function is not restored.
Hyperkalemia in the diarrheic calf
Treatment of the acidosis and expanding plasma volume and increasing the serum sodium concentration will correct hyperkalemia in dehydrated diarrheic calves.
Hypernatremia in the diarrheic calf
The treatment of hypernatremia is difficult and unreliable.46 If there is a concurrent acidosis it should be treated with a bicarbonate solution. The objective is to decrease serum sodium concentration more slowly than is possible with traditional isotonic fluids. It is recommended that a sodium-containing fluid containing sodium equal to 95–100% of the animal’s serum sodium concentration, or with a fluid containing 170 mEq/L of sodium, be used initially.47 The animal’s serum sodium concentration is monitored so as not to exceed a change of 0.3–0.5 mEq/h in serum sodium. Cerebral edema may be treated with mannitol.
Acidosis without dehydration
Some calves 10–20 days of age with a history of diarrhea in the previous several days may be affected with metabolic acidosis without obvious clinical evidence of dehydration.45 They are ataxic, weak, sometimes recumbent, and may appear comatose. The intravenous administration of 2–3 L of isotonic (1.3%) sodium bicarbonate results in recovery within an hour.
Hypertonic saline
Because the administration of large quantities of isotonic fluids may be impractical in a farm situation because it requires long-term venous catheterization, appropriate restraint and periodic monitoring, the use of hypertonic saline has been explored as a rapid, inexpensive, effective method of fluid administration in severely dehydrated calves.68,70 Hypertonic saline (7.2% NaCl) solution and 6% Dextran 70 solution have been used successfully to resuscitate animals with hypovolemic endotoxemic shock. Administration of 7.2% hypertonic saline and 6% Dextran 70 solution rapidly increases plasma volume, cardiac output and mean arterial pressure in hypovolemic and endotoxemic shock.69 The hypertonic saline and Dextran 70 are given intravenously at a rate of 4–5 mL/kg BW over a period of 4 minutes followed by allowing the calf to suck an isotonic alkalinizing oral electrolyte solution at 50 mL/kg BW.69 Calves that do not suck are given the oral fluids by stomach tube. An additional dose of oral fluids at 50 mL/kg BW is given 12 hours later. This regime provides a rapid, practical, economical and effective method for the treatment of dehydrated diarrheic calves.
Intravenous catheterization of calves
Catheterization of the jugular vein is the most widely used approach for continuous long-term intravenous fluid therapy in calves. The jugular vein may be difficult to catheterize in severely dehydrated calves when the vein is collapsed and not visible even after prolonged occlusion. In addition, the tough and dry skin makes catheterization difficult. To increase distension of the vein, calves may be raised by their pelvic limbs, thus increasing blood flow to the head and neck regions. An incision of the skin (a cut-down) makes placement of a catheter easier. A major advantage of jugular vein catheterization is the more rapid flow rate that is possible because 14-gauge catheters are commonly used.
Catheterization of the auricular veins in calves is becoming common, especially in Europe.71 Even in severely dehydrated calves, ear vein catheterization is successful. Ear catheters allow the application of sufficient amounts of fluids by continuous drip infusion and there are fewer complications compared to jugular vein catheters. In vitro flow rates for 22-gauge catheters range between 28 and 36 mL/min, providing an in vivo flow rate into the calf’s ear catheter of approximately 1.2–2.2 L/h.
Oral fluid and electrolyte therapy
Oral fluid and electrolyte therapy are indicated for calves in the early stages of diarrhea or after they have been successfully hydrated following parenteral fluid therapy. Severely dehydrated or moribund calves may not respond favorably to oral fluid therapy alone. Owners must be encouraged to provide oral fluid and electrolyte therapy to diarrheic neonatal farm animals as soon as possible after the onset of diarrhea. Almost all the information available on oral fluids has been developed following clinical studies in diarrheic calves, and the recommendations here reflect those studies.72
In neonatal calves, the ideal oral electrolyte solution should: (a) supply sufficient sodium to facilitate normalization of extracellular fluid deficits; (b) provide two or more agents (such as glucose, acetate, propionate, or glycine) that facilitate intestinal absorption of sodium and water; (c) provide an alkalinizing agent (such as acetate, propionate, citrate, or bicarbonate) to treat the metabolic acidosis often present in dehydrated diarrheic calves; (d) not interfere with milk clotting in the abomasum; (e) provide sufficient energy, as these electrolyte solutions may be administered instead of milk or milk replacer for short periods of time; and (f) facilitate repair of damaged intestinal epithelium.73
Acetate and propionate are the preferred alkalinizing agents for treating dehydrated calves with mild metabolic acidosis. Acetate and propionate have similar alkalinizing ability to bicarbonate on an equimolar basis, with the advantage that acetate and propionate produce energy. Acetate and propionate also stimulate sodium and water absorption in the calf small intestine, but in the jejunum to a greater extent than the ileum. Acetate and propionate are readily metabolized by both fed and fasted calves. Moreover, acetate and propionate are metabolized by peripheral tissues, are not produced endogenously in shock and dehydration (as is lactate) and do not have an unmetabolized isomer (d-lactate). Finally, acetate and propionate do not alkalinize the abomasum and intestine, whereas bicarbonate can permit bacteria to proliferate in an alkalinized abomasum, while also inhibiting the normal clotting of milk.
The ideal electrolyte concentration, osmolarity and energy source for an oral electrolyte solution to treat neonatal calf diarrhea remain controversial. The optimal solution should have a sodium concentration between 60 and 120 mmol/L, a potassium concentration between 10 and 20 mmol/L, a chloride concentration between 40 and 80 mmol/L, 40–80 mmol/L of metabolizable (nonbicarbonate) base, such as acetate or propionate, and glucose as an energy source. Some investigators have suggested that the optimal oral electrolyte solution required a higher sodium concentration (120–133 mmol/L) to rapidly correct extracellular electrolyte and fluid losses that typically develop in calves with diarrhea and dehydration. Combined administration of sodium and glucose is beneficial because glucose facilitates sodium absorption via the small intestinal sodium/glucose co-transport mechanism.
Oral fluid and electrolyte therapy is effective in enteric colibacillosis of neonatal farm animals because glucose continues to be absorbed by the small intestine by an active transport mechanism accompanied by glucose-coupled sodium absorption and absorption of water. In enterotoxigenic colibacillosis, while there is net hypersecretion caused by the enterotoxin, the intestinal mucosa is sufficiently intact so that water and sodium will be absorbed in the presence of glucose. Most oral electrolytes intended for the treatment of dehydration and acidosis in diarrheic calves contain sodium chloride and sodium bicarbonate with one or some of the following substances: glucose, acetates and citrates, phosphates, potassium salts, glycine and amino acids.
Several commercial oral preparations are available. The ideal solutions should be palatable and provide rapid rehydration and correction of acidosis. Diarrheic calves must receive sufficient fluid therapy to compensate for the fluid and electrolyte losses that occur and for maintenance and contemporary losses during the period of clinical diarrhea and convalescence. However, the calf must be returned to a milk diet within a few days in order to avoid the effects of malnutrition. Oral fluid and electrolyte formulas cannot provide the daily maintenance requirements of energy, protein, and fat. Some formulas contain a large quantity of glucose and are supplemented with glycine, sodium acetate, and citric acid, thus making a calorie-dense, partially nitrogen-balanced hyperosmolal solution. A glutamine-containing oral rehydration solution for the treatment of experimental E. coli calf diarrhea was more effective in correcting and sustaining plasma, extracellular fluid, and blood volume compared with standard World Health Organization solutions without the glutamine.74
There are marked variations in the alkalinizing abilities of the oral electrolyte solutions that are available commercially.72 Those that contain at least 80 mmol/L of bicarbonate are much more effective for the rapid correction of acidosis and depression in diarrheic calves than administration of rehydrating electrolyte solutions alone. The bicarbonate-rich preparations have the best alkalinizing response when given to calves affected with acidosis from experimentally induced diarrhea. Oral electrolyte solutions containing acid phosphate salts are undesirable because they cause net acidification of the blood, with a fall in blood pH. One possible theoretical disadvantage of an alkaline electrolyte solution (containing sodium bicarbonate) is that it may prolong the clotting of milk by rennin in the abomasum, which could cause maldigestion and prolong the diarrhea, especially if the oral fluids and electrolytes are diluted 1:1 with whole milk.
Several commercially available oral electrolyte solutions contain metabolizable bases such as acetate instead of bicarbonate and are formulated to correct and maintain acid–base imbalance and maintain normal milk digestion.72 Those preparations that contain either bicarbonate or acetate provide good therapeutic results and have been evaluated in experimentally induced diarrheic calves, which were also offered milk at the rate of 5% of their body weight twice daily.72 Offering milk along with the oral electrolytes is effective in maintaining body weight in experimental calves. No scientific information is available on the effects of milk and oral electrolytes in naturally occurring cases. Those preparations not containing any alkalinizing agent do not correct the acid–base imbalance and result in poor recovery rates in experimental calves.
Ideally, the oral fluids and electrolytes should not be mixed with milk but fed or offered between feedings of milk. The oral fluids should be given by nipple bottle if the animal will suck but the use of a stomach tube or esophageal feeder is satisfactory. Fluids can be administered to the dehydrated calf using an esophageal feeder, even though the reticular groove does not close. At least 2 L of fluid should be given, which results in a transfer of fluids from the rumen to the abomasum. If larger doses are required they should be divided and given at intervals of 2 hours or more to avoid abdominal discomfort from distension.
Fecal consistency is not a highly reliable criterion of success in the evaluation of oral fluid therapy for calf diarrhea. Calves with the greatest improvement in fecal consistency had no greater increase in plasma volume than calves that did not improve their fecal consistency. Thus improvement of the feces may not offer a reliable guide to the rehydration of the calf.
Response to therapy
Calves that respond and recover usually show marked improvement from intravenous and/or oral fluid therapy within 24–36 hours. Calves that respond to the hydration therapy begin to urinate within an hour after fluid administration is begun, and usually maintain hydration thereafter. Calves that do not respond will not hydrate normally; they may not begin to urinate because of irreversible renal failure, their feces remain watery, they remain depressed and not strong enough to suck or drink, and continued fluid therapy beyond 3 days is usually futile. Those calves that respond favorably to the initial fluid therapy and then become depressed 12–18 hours later may have returned to a state of metabolic acidosis. Mental depression, the loss of the suck reflex and muscular weakness are indications of acidosis, and affected calves will require retreatment with sodium bicarbonate.
Overhydration and overinfusion at too rapid an administration rate increases intravascular pressure, resulting in pulmonary edema characterized by hyperpnea, tachypnea, tachycardia, and death.
Antimicrobial therapy
Antimicrobials have been used extensively for the specific treatment of colibacillosis in calves and piglets because it was assumed that an infectious enteritis was present that had the potential of developing into a bacteremia or septicemia. Some preparations consist of a single antimicrobial, while others are mixtures with or without absorbents, astringents, and electrolytes. They have been used on an empirical basis, since few randomized controlled trials have been conducted.
It has been difficult to evaluate the efficacy of antimicrobials for the treatment of enteric colibacillosis because of the complex nature of the interactive factors that affect the outcome in naturally occurring cases. These include the presence of mixed infections, the effects of whether or not milk is withheld from the diarrheic calves, the effects of the immune status of individual calves, the variable times after the onset of diarrhea when the drugs are given, the possible presence of antimicrobial resistance, and the effects of supportive treatment such as electrolyte and fluid therapy.
The literature on the use of antimicrobials in the treatment of calf diarrhea has been critically reviewed by Constable75 and the following discussion strongly reflects his review and his evidence-based recommendations for the use of antimicrobials to treat calf diarrhea.
Change in small intestinal bacterial flora in calves with diarrhea
There has been a paradigm shift in the last 40 years towards categorizing an episode of calf diarrhea as being due to a specific etiologic agent, such as rotavirus, coronavirus, cryptosporidia, Salmonella spp., or enterotoxigenic E. coli. While the etiologic approach has correctly focused attention on preventive programs, including vaccination and optimizing transfer of colostral immunity, the approach has diverted attention from the universal finding of all studies, that calves with diarrhea have coliform bacterial overgrowth of the small intestine.75
Studies completed more than 70 years ago documented increased numbers of E. coli bacteria in the abomasum, duodenum, and jejunum of scouring calves. Moreover, calves severely affected with diarrhea had increased numbers of E. coli bacteria in the anterior portion of their intestinal tracts compared to mildly affected animals. More recent studies have consistently documented the fact that calves with naturally acquired diarrhea, regardless of age and the etiological cause for the diarrhea, have altered small intestinal bacterial flora. Specifically, E. coli bacterial numbers are increased 5–10 000-fold in the duodenum, jejunum, and ileum of calves with naturally acquired diarrhea, even when the diarrhea was not due to enterotoxigenic strains of E. coli, and where rotavirus and coronavirus were identified in the feces. The largest increase in E. coli bacterial numbers occurs in the distal jejunum and ileum, whereas the E. coli or coliform bacterial numbers in the colon and feces are similar or higher for calves with diarrhea than calves without diarrhea, with E. coli being more numerous in the feces of colostrum-deprived than colostrum-fed calves. Small intestinal overgrowth with coliform bacteria can persist after departure of the initiating enteric pathogen.
In calves with naturally acquired diarrhea, increased small-intestinal colonization with E. coli has been associated with impaired glucose, xylose, and fat absorption.
Mixed infections with enteric pathogens are commonly diagnosed in calves with naturally acquired diarrhea, and the clinical signs and pathological damage associated with rotavirus infection are more severe when E. coli is present than when it is absent. Primary viral morphologic damage to the small intestine also facilitates systemic invasion by normal intestinal flora, including E. coli.
In calves with experimentally induced enterotoxigenic E. coli diarrhea, colonization of the small intestine by E. coli has been associated with impaired glucose and lactose absorption, decreased serum glucose concentration and possibly increased susceptibility to cryptosporidial infection.
In summary, calves with diarrhea have increased coliform bacterial numbers in the small intestine, regardless of etiology, and this colonization is associated with altered small-intestinal function, morphological damage, and increased susceptibility to bacteremia. It therefore follows that administration of antimicrobials that decrease small intestinal coliform bacterial numbers in calves with diarrhea may prevent the development of bacteremia, decrease mortality, and decrease morphological damage to the small intestine, thereby facilitating digestion and absorption and increasing growth rate.
Incidence of bacteremia in calves with diarrhea
Calves with diarrhea are more likely to have failure of transfer of passive immunity or partial failure of transfer of passive immunity, and this group of calves, in turn, is more likely to be bacteremic. This is an additional reason that antimicrobials may be indicated in the treatment of calf diarrhea. Colostrum-deprived calves that subsequently developed diarrhea were frequently bacteremic, whereas bacteremia occurred much less frequently in colostrum-fed calves that developed diarrhea.
Based on field studies of diarrheic calves, it can be assumed that, on average, 30% of severely ill calves with diarrhea are bacteremic, that the risk of bacteremia is higher in calves with failure of transfer of passive immunity than in calves with adequate transfer of passive immunity, and that the risk of bacteremia is higher in calves 5 days of age or older. The frequency of bacteremia is sufficiently high that treatment of calves with diarrhea that are severely ill (as manifest by reduced suck reflex, > 6% dehydration, weakness, inability to stand or clinical depression) should include routine treatment against bacteremia, with emphasis on treating potential E. coli bacteremia. Veterinarians should also assume that 8–18% of diarrheic calves with adequate transfer of passive immunity and systemic illness are bacteremic. The prevalence of bacteremia is sufficiently high in systemically ill calves that effective antimicrobial treatment for potential bacteremia should be routinely instituted, regardless of transfer of passive immunity status and treatment cost. Withholding an effective treatment for a life-threatening condition, such as bacteremia in calves with diarrhea, cannot be condoned on animal welfare grounds.
Antimicrobial susceptibility of fecal Escherichia coli isolates
The most important determinant of antimicrobial efficacy in calf diarrhea is obtaining an effective antimicrobial concentration against bacteria at the sites of infection (small intestine and blood). The results of fecal antimicrobial susceptibility testing have traditionally been used to guide treatment decisions; however, susceptibility testing in calf diarrhea probably has clinical relevance only when applied to fecal isolates of enterotoxigenic strains of E. coli or pathogenic Salmonella spp., and blood culture isolates from calves with bacteremia. Validation of susceptibility testing as being predictive of treatment outcome for calves with diarrhea is currently lacking.
The ability of fecal bacterial culture and antimicrobial susceptibility testing using the Kirby Bauer technique to guide treatment in calf diarrhea is questionable when applied to fecal E. coli isolates that have not been identified as enterotoxigenic.75 There do not appear to be any data demonstrating that fecal bacterial flora is representative of the bacterial flora of the small intestine, which is the physiologically important site of infection in calf diarrhea. Marked changes in small-intestinal bacterial populations can occur without changes in fecal bacterial populations, and the predominant strain of E. coli in the feces of a diarrheic calf can change several times during the diarrhea episode. Furthermore, and most importantly, 45% of calves with diarrhea had different strains of E. coli isolated from the upper and lower small intestine, indicating that fecal E. coli strains are not always representative of small-intestinal E. coli strains.
An additional bias present in most antimicrobial susceptibility studies conducted on fecal E. coli isolates is that data are frequently obtained from dead calves, which are likely to be treatment failures. The time since death is also likely to be an important determinant of the value of fecal culture, because such a rapid proliferation of bacteria occurs in the alimentary tract after death that the results of examinations made on dead calves received at the laboratory can have little significance. Calves that die from diarrhea are likely to have received multiple antimicrobial treatments, and preferential growth of antimicrobial-resistant E. coli strains starts within 3 hours of antimicrobial administration. A further concern with fecal susceptibility testing is that the Kirby Bauer breakpoints (minimum inhibitory concentration (MIC)) are not based on typical antimicrobial concentrations in the small intestine and blood of calves. What are urgently needed are studies documenting the antimicrobial susceptibility of E. coli isolates from the small intestine of untreated calves, based on achievable drug concentrations and dosage regimens. Until these data are available, it appears that antimicrobial efficacy is best evaluated by the clinical response to treatment, rather than the results of in vitro antimicrobial susceptibility testing performed on fecal E. coli isolates.
A comparison of antibiotic resistance for E. coli populations isolated from groups of diarrheic and control calves in the UK found a higher incidence of antibiotic-resistant E. coli in samples obtained from farms with calf diarrhea than from farms without the disease.76 Considering all samples, bacterial colonies in 84% were resistant to ampicillin, in 13% to apramycin and in 6% to nalidixic acid. Antibiotic resistance among enterotoxigenic E. coli from piglets and calves with diarrhea in a diagnostic laboratory survey of one geographic area in Canada over a 13-year period found that least resistance occurred against ceftiofur for all, followed by apramycin and gentamicin for porcine and florfenicol for bovine isolates.77
Passive surveillance for antimicrobial resistance in E. coli isolates from diarrheic food animals continues to indicate that resistance to many of the common antimicrobials is increasing. In a UK study over a 5-year period, E. coli isolates from calves with diarrhea become more resistant to furazolidone, trimethoprim-potentiated sulfonamide, clavulanic-acid-potentiated amoxicillin, and tetracycline.78 E. coli strains from outbreaks of diarrhea in lambs in Spain became increasingly resistant to nalidixic acid, enoxacin, and enrofloxacin on the basis of the National Committee on Clinical Laboratory Standards (NCCL) breakpoints for human and animal isolates.79,80 Among the fluoroquinolones used for treatment of domestic animals in Spain, enrofloxacin is approved for use for the treatment of colibacillosis and diarrhea in lambs. However, the bovine and ovine strains of E. coli that possess potential virulence factors were more sensitive to quinolones than those that do not express those factors. Some antimicrobial-resistant E. coli strains from diarrheic calves in the USA may possess a chromosomal flo gene that specifies cross-resistance to both florfenicol and chloramphenicol, and its presence among E. coli isolates of diverse genetic backgrounds indicates a distribution much wider than previously thought.81 In Spain, 5.9% of E. coli strains from cattle were resistant to nalidixic acid and 4.9% were resistant to enrofloxacin and ciprofloxacin.82 In sheep and goats only 0.5% and 1.4%, respectively, of the strains were resistant to nalidixic acid and none to fluoroquinolones. Most of the quinolone-resistant strains were nonpathogenic strains isolated from cattle.
The CTX-M-14-like enzyme has been detected in E. coli recovered from the feces of diarrheic dairy calves in Wales.74 The enzyme is an extended-spectrum beta-lactamase (ESBL), which confers resistance to a wide range of beta-lactam (penicillin and cephalosporin) compounds. Organisms possessing ESBLs are considered to be resistant to second-, third-, and fourth-generation cephalosporins, and in vitro resistance to amoxicillin/clavulanate among producers is variable, reflecting the amount of beta-lactamase produced. In addition to this enzyme, the isolates produced a TEM-35 (IRT-4) beta-lactamase that conferred resistance to the amoxicillin/clavulanate combination. These two enzymes confer resistance to all the beta-lactamase compounds approved for veterinary use in the UK. Thus their occurrence in animals may be an important development for both animal and public health. ESBLs in human infections have emerged as a significant and developing problem, occurring in patients in the community as well as in those with recent hospital contact. Spread of this form of resistance in bacteria affecting the animal population could have serious implications for animal health, rendering many therapeutic options redundant.
Antibiotic resistance to intestinal bacteria also occurs in dairy calves fed milk from cows treated with antibiotics.83 The resistance increases with higher concentrations of antibiotics in the milk.
Antimicrobial susceptibility of blood Escherichia coli isolates
The Kirby Bauer technique for antimicrobial susceptibility testing has more clinical relevance for predicting the clinical response to antimicrobial treatment when applied to blood isolates rather than fecal isolates.75 This is because the Kirby Bauer breakpoints (MICs) are based on achievable antimicrobial concentrations in human plasma and MIC90 values for human E. coli isolates, which provide a reasonable approximation to achievable MIC values in calf plasma and MIC90 values for bovine E. coli isolates. Unfortunately, susceptibility results are not available for at least 48 hours, and very few studies have documented the antimicrobial susceptibility of blood isolates in calves with diarrhea. In a 1997 study of dairy calves in California, the antimicrobial susceptibility of isolates from the blood of calves with severe diarrhea or illness produced the following results; ceftiofur, 19/25 (76%) sensitive; potentiated sulfonamides, 14/25 (56%) sensitive; gentamicin, 12/25 (48%) sensitive; ampicillin, 11/25 (44%) sensitive; tetracycline, 3/25 (12%) sensitive, although there was a clinically significant year-to-year difference in the results of susceptibility testing that may have reflected different antimicrobial administration protocols on the farm.75
Evidence-based recommendations for antimicrobial treatment of diarrheic calves
The four critical measures of success of antimicrobial therapy in calf diarrhea are (in decreasing order of importance): (1) mortality rate, (2) growth rate in survivors, (3) severity of diarrhea in survivors, and (4) duration of diarrhea in survivors.
Success of antimicrobial therapy can vary with the route of administration and whether the antimicrobial is dissolved in milk, oral electrolyte solutions, or water. Oral antimicrobials administered as a bolus or contained in a gelatin capsule are deposited into the rumen and therefore have a different serum concentration–time profile from antimicrobials dissolved in milk replacer that are suckled by the calf or administered as an oral drench at the back of the pharynx. Antimicrobials that bypass the rumen are not thought to alter rumen microflora, potentially permitting bacterial recolonization of the small intestine from the rumen. Finally, when oral antimicrobials are administered to calves with diarrhea, the antimicrobial concentration in the lumen of the small intestine is lower and the rate of antimicrobial elimination faster than in healthy calves.
Orally administered amoxicillin, chlortetracycline, neomycin, oxytetracycline, streptomycin, sulfachloropyridazine, sulfamethazine, and tetracycline are currently labeled in the USA for the treatment of calf diarrhea. No parenteral antimicrobials have a label claim in the USA for treating calf diarrhea.
In his review of the literature on the use of antibiotics for the treatment of calf diarrhea, Constable75 concluded that recommendations by some veterinarians that oral or parenteral antimicrobials should not be used were not supported by a critical evidence-based review of the literature. The arguments used to support a nonantimicrobial treatment approach have included:
• Orally administered antimicrobials alter intestinal flora and function and thereby induce diarrhea, which has been documented on more than one occasion with chloramphenicol, neomycin, and penicillin
• Antimicrobials harm the ‘good’ bacteria in the small intestine more than the ‘bad’ bacteria (an undocumented claim in the calf)
• Antimicrobials are not effective (a statement that is clearly not supported by the results of some published peer-reviewed studies)
• Antimicrobial administration promotes the selection of antimicrobial resistance in enteric bacteria.
Constable75 concluded that antimicrobial treatment of diarrheic calves should be practiced and focused against E. coli in the small intestine and blood, as these constitute the two sites of infection. Fecal bacterial culture and antimicrobial susceptibility testing is not recommended in calves with diarrhea, because fecal bacterial populations do not accurately reflect small-intestinal or blood bacterial populations and the breakpoints for susceptibility test results have not been validated. Antimicrobial efficacy is therefore best evaluated by the clinical response to treatment.
In the USA parenterally administered oxytetracycline and sulfachloropyridiazine and orally administered amoxicillin, chlortetracycline, neomycin, oxytetracycline, streptomycin, sulfachloropyridazine, sulfamethazine, and tetracycline are currently labeled for the treatment of calf diarrhea. Unfortunately, there is little published data supporting their efficacy in treating calves with diarrhea.75 Extralabel antimicrobial use (excluding prohibited antimicrobials) is therefore justified in treating calf diarrhea because of the apparent lack of published studies documenting clinical efficacy of antimicrobials with a label claim, and because the health of the animal is threatened and suffering or death may result from failure to treat systemically ill calves.
Because the two sites of infection in calf diarrhea are the small intestine and blood, administered antimicrobials should have both local (small intestinal) and systemic effects. In addition, the antimicrobial must reach therapeutic concentrations at the site of infection for a long enough period and, ideally, have only a narrow Gram-negative spectrum of activity in order to minimize collateral damage to other enteric bacteria. In general, oral and parenteral administration of broad-spectrum beta-lactam and fluoroquinolone antimicrobials have proven efficacy in treating naturally acquired and experimentally induced diarrhea, parenteral administration of trimethoprim–sulfadiazine has proven efficacy in treating experimentally induced Salmonella enterica serotype Dublin (although efficacy has only been demonstrated when antimicrobial administration starts before diarrhea is present), and oral administration of the predominantly Gram-negative-spectrum antimicrobial apramycin has proven efficacy in treating naturally acquired diarrhea. Because use of fluoroquinolone antimicrobials in an extralabel manner is illegal in the USA, and apramycin is an aminocyclitol antimicrobial that is poorly absorbed after oral administration (oral bioavailability <15%) and has relatively high MIC values against Salmonella spp. and E. coli (MIC90 > 3 μg/mL) in the calf, treatment recommendations will focus on the use of broad-spectrum beta-lactam antimicrobials such as amoxicillin, ampicillin, ceftiofur, and potentiated sulfonamides (trimethoprim– sulfadiazine).
Administration of oral antimicrobials to treat Escherichia coli overgrowth of the small intestine
Based on published evidence for the oral administration of these antimicrobial agents, only amoxicillin can be recommended for the treatment of diarrhea; dosage recommendations are amoxicillin trihydrate (10 mg/kg every 12 h) or amoxicillin trihydrate–clavulanate potassium (12.5 mg combined drug/kg every 12 h) for at least 3 days; the latter constitutes extralabel drug use. Parenteral administration of broad-spectrum beta-lactam antimicrobials (ceftiofur, 2.2 mg/kg intramuscularly or subcutaneously every 12 h; amoxicillin or ampicillin, 10 mg/kg intramuscularly every 12 h) or potentiated sulfonamides (25 mg/kg intravenously or intramuscularly every 12 h) is recommended for treating calves with diarrhea and systemic illness; both constitute extralabel drug use.
Concurrent feeding of milk and amoxicillin does not change the bioavailability of amoxicillin, although amoxicillin is absorbed faster when dissolved in an oral electrolyte solution than in milk replacer and absorption is slowed during endotoxemia, presumably because of a decrease in abomasal emptying rate. Amoxicillin trihydrate is preferred to ampicillin trihydrate for oral administration in calves because it is labeled for the treatment of calf diarrhea in the USA and is absorbed to a much greater extent. However, a field study comparing oral amoxicillin (400 mg every 12 h) and ampicillin (400 mg every 12 h) treatments for diarrhea reported similar proportions of calves with a good to excellent clinical response (79%, 49/62 for amoxicillin bolus; 80%, 59/74 for amoxicillin powder; 65%, 47/65 for ampicillin bolus; p >0.30 for all comparisons). The addition of clavulanate potassium to amoxicillin trihydrate is recommended because clavulanate potassium is a potent irreversible inhibitor of beta-lactamase, increasing the antimicrobial spectrum of activity.
Sulbactam/ampicillin was effective for the treatment of experimentally induced diarrhea in calves infected with E. coli strain B44 (O9:K30:K99H).84 The survival rate in treated calves was 100% compared to 22% in control calves treated only with saline. Ceftiofur hydrochloride – a broad-spectrum, beta-lactamase-resistant cephalosporin – at an oral dose of 10 mg/kg BW given once was effective for the treatment of experimentally induced enteric colibacillosis in piglets.
Oral administration of potentiated sulfonamides is not recommended for treating calf diarrhea because of the lack of efficacy studies. Gentamicin (50 mg/calf orally every 12 h) markedly decreased E. coli bacterial concentrations in the feces of healthy calves and treatment with gentamicin has improved stool consistency in calves with experimentally induced E. coli diarrhea.75 However, oral administration of gentamicin is not recommended, because antimicrobials administered to calves with diarrhea should have both local and systemic effects, and orally administered gentamicin is poorly absorbed.
Fluoroquinolones clearly have proven efficacy in treating calf diarrhea and a label indication exists in Europe for oral and parenteral enrofloxacin and oral marbofloxacin for the treatment of calf diarrhea. In those countries where their administration is permitted to treat calf diarrhea, oral fluoroquinolones are recommended because of their high oral bioavailability. However, it must be emphasized that extralabel use of the fluoroquinolone class of antimicrobials in food-producing animals in the US is illegal and obviously not recommended.
Also, in other countries it may be illegal to use some of the antimicrobials mentioned here because of the regulations regarding their use in food-producing animals. Some are available to farmers on a prescription-only basis, which makes examination of the animals and a diagnosis necessary before recommendations are made. The indiscriminate use of antibiotics in milk replacers for the treatment of newborn calves and piglets is widespread and must be viewed with concern when the problem of drug resistance transfer from animal to animal and to humans is considered.
In calves with diarrhea and no systemic illness (normal appetite for milk or milk replacer, no fever), it is recommended that the clinician monitors the health of the calf, and does not administer oral antimicrobials.
Administration of parenteral antimicrobials to treat Escherichia coli bacteremia
In calves with diarrhea and moderate to severe systemic illness, the positive predictive value (0.65) of clinical tests (sensitivity = 0.39, specificity = 0.91) and the positive predictive value (0.77) of laboratory tests (sensitivity = 0.40, specificity = 0.95) for detecting bacteremia are too low assuming reasonable estimates for the prevalence of bacteremia (30%).77 Accordingly, it is recommended that clinicians routinely assume 30% of ill calves with diarrhea are bacteremic, and that bacteremia constitutes a threat to the life of the calf.
The most logical parenteral treatment is ceftiofur (2.2 mg/kg intramuscularly/subcutaneously every 12 h) for at least 3 days. Ceftiofur is the most appropriate antimicrobial because it is a broad-spectrum beta-lactam antimicrobial that is resistant to the action of beta-lactamase, the MIC90 for E. coli is less than 0.25 μg/mL, the recommended dosage schedule maintains free plasma beta-lactam antimicrobial concentrations at the desired four times above the MIC90 value for the duration of treatment in 7-day-old calves, and 30% of the active metabolite of ceftiofur (desfuroylceftiofur) is excreted into the intestinal tract of cattle, providing antimicrobial activity in both blood and small intestine. Moreover, parenteral (2 mg/kg, intramuscularly once) and oral (0.5 mg/kg, once) administration of ceftiofur hydrochloride decreased mortality rate and the severity of diarrhea in pigs with experimentally induced enteric colibacillosis, although these pigs were not suspected to be bacteremic.75 The beneficial effects of parenteral ceftiofur in these pigs was attributed to decreasing intestinal luminal concentration of pathogenic E. coli. Orally administered ceftiofur sodium (<5 mg/kg daily) was also effective in treating mice with experimentally induced enteric colibacillosis.75 Administration of ceftiofur to treat bacteremia and diarrhea in calves constitutes extralabel drug use, and ceftiofur should not be administered to calves to be processed as veal.
Another recommended treatment is parenteral amoxicillin trihydrate or ampicillin trihydrate (10 mg/kg intramuscularly every 12 h) for at least 3 days. Although parenteral ampicillin has proven efficacy in treating naturally acquired diarrhea whereas ceftiofur has unproven efficacy, the broad-spectrum beta-lactam antimicrobials amoxicillin and ampicillin are theoretically inferior to ceftiofur because parenterally administered ampicillin and amoxicillin reach lower plasma concentrations and require a higher MIC than ceftiofur, and are not beta-lactamase-resistant.75 Amoxicillin or ampicillin should be injected into the neck musculature because this site provides the greatest absorption and minimizes damage to more valuable areas of the carcass. Amoxicillin and ampicillin should not be administered subcutaneously, as the rate and extent of absorption is reduced relative to intramuscular injection.
A third recommended treatment is parenteral potentiated sulfonamides (20 mg/kg sulfadiazine with 5 mg/kg trimethoprim, intravenously or intramuscularly depending upon the formulation characteristics, every 24 h for 5 d). The efficacy of potentiated sulfonamides has only been proved when treatment commenced before clinical signs of diarrhea were present.75 It is therefore unknown whether potentiated sulfonamides are efficacious when administered to calves with diarrhea and depression, although it is likely that potentiated sulfonamides are efficacious in the treatment of salmonellosis.
Oral administration of potentiated sulfonamides and apramycin is not recommended for the treatment of bacteremia, because of poor oral bioavailability. Oxytetracycline or chlortetracycline are also not recommended for the treatment of bacteremia, although tetracyclines may have some efficacy for treating E. coli bacterial overgrowth of the small intestine. Tetracycline antimicrobials are bound to calcium, and oral bioavailability when administered with milk is 46% for oxytetracycline and 24% for chlortetracycline.
Parenteral administration of gentamicin and other aminoglycosides (amikacin, kanamycin) cannot currently be recommended as part of the treatment for calf diarrhea because of the lack of published efficacy studies, prolonged slaughter withdrawal times (15–18 months), potential for nephrotoxicity in dehydrated animals, and availability of ceftiofur, amoxicillin, and ampicillin.
A label indication exists in Europe for parenteral enrofloxacin in the treatment of calf diarrhea. In those countries where administration is permitted to treat calves with diarrhea, parenteral fluoroquinolones are recommended because of their broad-spectrum bactericidal activity, particularly against Gram-negative bacteria. However, it must be emphasized that extralabel use of the fluoroquinolone class of antimicrobials in food-producing animals in the USA is illegal and obviously not recommended.
Chloramphenicol had proven efficacy in treating calf diarrhea due to Salmonella enterica serotypes Bredeney and Dublin, although its use is now illegal in the USA. The related antimicrobial florfenicol achieves high concentrations in the lumen of the small intestine and is 89% absorbed when orally administered to milk-fed calves; however, florfenicol does not provide the most appropriate antimicrobial for treating calf diarrhea, as the MIC90 for E. coli is very high at 25 μg/mL and florfenicol (11 mg/kg orally or 20 mg/kg intramuscularly) failed to reach the MIC90 value in plasma, whereas florfenicol (11–20 mg/kg intravenously) only exceeded the MIC90 value for less than 60 minutes.75
In calves with diarrhea and no systemic illness (normal appetite for milk or milk replacer, no fever), we recommend that the clinician monitors the health of the calf and does not administer parenteral antimicrobials.
Immunoglobulin therapy
One of the important factors determining whether or not calves survive enteric colibacillosis is the serum immunoglobulin status of the animal before it develops the disease. The prognosis is unfavorable if the level of immunoglobulins is low at the onset of diarrhea, regardless of intensive fluid and antimicrobial therapy. Most of the literature on therapy omits this information and is therefore difficult to assess. There is ample evidence that the mortality rate will be high in diarrheic calves that are deficient in serum immunoglobulins, particularly IgG, in spite of exhaustive antimicrobial and fluid therapy. This has stimulated interest in the possible use of purified solutions of bovine gammaglobulin in diarrheic calves that are hypogammaglobulinemic. However, they must be given by the intravenous route and in large amounts, the cost of which would be prohibitive. In addition, they are unlikely to be of value once the calf is affected with diarrhea; they are protective and probably not curative. Whole blood transfusion to severely affected calves may be used as a source of gammaglobulins but unless given in large quantities would not significantly elevate serum immunoglobulin levels in deficient calves. Limited controlled trials indicate that there is no significant difference in the survival rate of diarrheic calves treated with either a blood transfusion daily for 3 days; fluid therapy given orally, subcutaneously, or intravenously depending on the severity of the dehydration; or fluid therapy with antibiotics. Those calves that survived, regardless of the type of therapy, had high levels of immunoglobulins before they developed diarrhea. This emphasizes the importance of the calf ingesting liberal quantities of colostrum within the first few hours after birth.
Antimotility drugs and intestinal protectants
There is no good evidence that antimotility drugs are of any therapeutic value for the treatment of enteric colibacillosis. Intestinal protectants such as kaolin and pectin are in general use for diarrheic animals but likewise their value is uncertain. When they are used the feces become bulky but do not have any known effect on the pathogenesis of the disease.
Alteration of the diet
Whether or not diarrheic newborn animals should be deprived of milk during the period of diarrhea is controversial.72 Diarrheic piglets are usually treated with an antimicrobial orally and left to nurse on the sow. Diarrheic beef calves are commonly treated with oral fluids and electrolytes and left with the cow. However, it is a common practice to reduce the milk intake of diarrheic hand-fed dairy calves for up to 24 hours or until there is clinical evidence of improvement. The withholding of milk from diarrheic calves has been based on the observations that lactose digestion is impaired and that ‘resting’ the intestine for a few days minimizes additional osmotic diarrhea caused by fermentation of undigested lactose in the large intestine. Thus it has seemed logical not to feed the animal with milk, which must be digested, but rather to provide readily absorbable substances such as oral glucose–electrolyte mixtures. In contrast, the argument in favor of continuous feeding of milk is that the intestinal tract requires a constant source of nutrition, which it receives from the ingesta in the lumen of the intestine. It has also been proposed that starving diarrheic calves from milk can result in malnutrition, suboptimal growth rates and prolonged recovery.72 In one study it was shown that the offering of milk to diarrheic calves when they were willing to drink following hydration therapy in a clinic resulted in a higher but insignificant improvement in survival rate than in calves that were starved from milk for 24 hours. In another study, the continued feeding of cows’ whole milk and fluids and electrolytes to experimentally induced diarrheic calves sustained the growth rate of the animals over the trial period of 10 days even though the diarrhea persisted.72 The use of whole milk and oral rehydration solutions for calves with naturally occurring diarrhea did not prolong the diarrhea or make it worse72 but the calves were in the early stages of diarrhea and were neither severely dehydrated nor acidotic.
It has been common practice to use oral fluids and electrolytes as milk replacement during the period of diarrhea. Such mixtures are inexpensive, easy to use, readily available and, if used by the farmer when diarrhea is first noticed, will usually successfully treat existing dehydration and prevent further dehydration and acidosis.
Following recovery, calves should be offered reduced quantities of whole milk three times daily (no more than total daily intake equivalent to 8% BW) on the first day and increased to the normal daily allowance in the next few days. Milk should not be diluted with water as this may interfere with the clotting mechanism in the abomasum.
Clinical management of outbreaks
The following principles should be considered when outbreaks of colibacillosis in neonatal farm animals are encountered:
• The veterinarian should visit the farm and conduct an epidemiological investigation to identify risk factors
• Examine each risk factor and how it can be minimized
• Identify and isolate all affected animals if possible
• Treat all affected animals as necessary
• Take laboratory samples from affected and normal animals
• Make recommendations for the control of diarrhea in animals to be born in the near future
• Prepare and submit a report to the owner describing the clinical and laboratory results and how the disease can be prevented in the future.
Health and welfare of calves
A survey of calf health and welfare on dairy farms in England examined the degree of compliance with the Welfare of Farmed Animals Regulations.85 The level of veterinary involvement in calf rearing and management on dairy farms was also assessed by questionnaire sent to large-animal practitioners. Compliance with the regulations was variable. The requirements for isolation of sick calves, provision of bovine colostrum within 6 hours after birth, provision of fresh, clean water and restrictions concerning tethering were not well complied with. However, the requirements for twice-daily feeding and inspection, visual and tactile contact between calves, access to forage and the provision of clean, dry bedding were well complied with. The results also suggested that there was some lack of veterinary input into the health and welfare of calves on dairy farms visited by the practices routinely and nonroutinely. These results suggest that there are considerable opportunities to improve calf health and management practices by veterinarians who visit dairy farms. This can be done through animal health management advice provided during routine visits to the farm and encouraging compliance with current welfare regulations and through the use of herd health plans. The major challenge for the veterinarian is to be able to communicate with owners and animal attendants about the care being provided to clinically ill neonates to insure that they are being treated according to their needs and made comfortable during their convalescence.
CONTROL
Because of the complex nature of the disease, it is unrealistic to expect total prevention, and control at an economical level should be the major goal. Effective control of colibacillosis can be accomplished by the application of three principles:
• Reduction of the degree of exposure of the newborn to the infectious agents
• Provision of maximum nonspecific resistance with adequate colostrum and optimum animal management
• Increasing the specific resistance of the newborn by vaccination of the dam or the newborn.
Reduction of the degree of exposure of the newborn to the infectious agents
The emphasis is on insuring that the newborn are born into a clean environment. Barns, confinement pens, and paddocks used as parturition areas must be clean and should preferably have been left vacant for several days before the pregnant dams are placed in them.
Dairy calves
These comments are directed particularly at calves born indoors, where contamination is higher than outdoors.
• Calves should be born in well-bedded box stalls that were previously cleaned out
• The perineum and udder of the dairy cow should be washed shortly before calving
• Immediately after birth the umbilicus of the calf should be swabbed with 2% iodine. Tying the umbilicus at the level of the abdominal wall with cotton thread is also practiced
• Calves affected with diarrhea should be removed from the main calf barn if possible and treated in isolation.
Beef calves
These are usually born on pasture or on confined calving grounds.
• Calving grounds should have been free of animals previous to the calving period; the grounds should be well drained, dry and scraped free of snow if possible. Each cow–calf pair should be provided with at least 2000 square feet of space. Calving on pasture with adequate protection from wind is ideal. Covering the calving grounds with straw or wood shavings provides a comfortable calving environment
• In large beef herds, in a few days following birth when the calf is nursing successfully, the cow–calf pair should be moved to a nursery pasture to avoid overcrowding in the calving grounds.
In beef herds, breeding plans should insure that heifers calve at least 2 weeks before the mature cows. Limiting the breeding and therefore the calving season to 45 days or less for heifers also offers several advantages. A short calving season allows the producer to more effectively and economically concentrate personnel resources to the calving management compared to a longer calving season. Calving heifers earlier allows them additional time required before the next breeding season to be on an increasing plane of nutrition necessary to maintain a high conception rate. The earlier calving of heifers also provides less exposure of their calves to infection pressure from the mature animals in the herd.
The incidence and severity of neonatal disease will typically increase, and the age at disease onset will decrease as the calving season progresses. This phenomenon is common in beef herds because of the effect of the calf as a biological amplifier. The more the calving season is shortened, the more the biological amplification effect is negated.
For beef herds, it is necessary to have a plan for cattle movement throughout the calving season. This requires a minimum of four or five separate pastures. These include a gestation pasture, a calving pasture and a series of nursery pastures. To ensure that beef calves are born in a sanitary environment, the herd should be moved from the gestation pasture to the calving pasture 1–2 weeks before calving. One day after birth, the cow or heifer and her calf should be moved to a nursery pasture. Cow–calf pairs should be added to a single nursery pasture until the appropriate number of pairs has been reached. Thereafter, cow–calf pairs can be added to a second nursery pasture. The difference in age between the oldest and youngest calf in a nursery pasture should never exceed 30 days, and smaller differences are preferable. This negates the biological amplification effect. The longer the calving season, the greater the need for a large number of nursery pastures. Calves that develop diarrhea should be removed immediately to an area away from healthy calves, treated and not returned until all calves in the group are at low risk for developing diarrhea (> 30 days of age).
The nutrition of the pregnant cows, and particularly the first-calf heifers, must be monitored through gestation to insure an adequate body condition and sufficient resources to provide an adequate supply of good-quality colostrum.
Veal calves
These calves are usually obtained from several different sources and 25–30% or higher may be deficient in serum immunoglobulin.
• On arrival, calves should be placed in their individual calf pens, which were previously cleaned, disinfected and left vacant to dry
• Feeding utensils are a frequent source of pathogenic E. coli and should be cleaned and air-dried daily
• Calves affected with diarrhea should be removed and isolated immediately.
Lambs and kids
The principles described above for calves apply to lambs and kids. Lambing sheds can be a source of heavy contamination and must be managed accordingly to reduce infection pressure on newborn lambs.
Piglets
Piglets born in a total-confinement system may be exposed to a high infection rate.
• The all-in/all-out system of batch farrowing, in which groups of sows farrow within a week, is recommended. This system will allow the herdsman to wean the piglets from a group of sows in a day or two and clean, disinfect and leave vacant a battery of farrowing crates for the next group of sows. This system will reduce the total occupation time and the infection rate. The continuous farrowing system without regular breaks is not recommended
• Before being placed in the farrowing crate, sows should be washed with a suitable disinfectant to reduce the bacterial population of the skin.
Provision of maximum nonspecific resistance with adequate colostrum and optimum animal management
This begins with the provision of optimal nutrition to the pregnant dam, which will result in a vigorous newborn animal and adequate quantities of colostrum. At the time of parturition, surveillance of the dams and the provision of any obstetric assistance required will insure that the newborn are born with as much vigor as possible. Parturition injuries and intrapartum hypoxemia must be minimized as much as possible.
Colostrum management
The next most important control measure is to insure that liberal quantities of good-quality colostrum are available and ingested within minutes and no later than a few hours after birth. While the optimum amount of colostrum that should be ingested by a certain time after birth is well known, the major difficulty with all species under practical conditions is to know how much colostrum a particular neonate has ingested. Because modern livestock production has become so intensive, it is imperative that the animal attendants make every effort to insure that sufficient colostrum is ingested by that particular species. In one study, in large dairy herds, 42% of calves left with their dams for 1 day following birth had failed either to suck sufficient colostrum or to absorb sufficient colostral immunoglobulins.
Failure of transfer of passive immunity, as determined by calf serum immunoglobulin IgG1 concentration below 10 mg/mL at 48 hours of age, occurred in 61.4% of calves from a dairy in which calves were nursed by their dams, 19.3% of calves from a dairy using nipple-bottle feeding and 10.8% of calves from a dairy using tube feeding.8 A higher prevalence of failure of transfer of passive immunity in dairy calves can occur because an insufficient volume of colostrum is ingested by the calf. When artificial feeding is used, inadequate immunoglobulin concentration in the colostrum fed is the most important factor resulting in failure of transfer of passive immunity.8 The prevalence of failure of transfer of passive immunity in dairy herds can be minimized by artificially feeding all newborn calves large volumes (3–4 L) of fresh or refrigerated first-milking colostrum from cows that had nonlactating intervals of normal duration. This volume is considerably greater than the intake that Holstein calves usually achieve by sucking, and also exceeds the voluntary intake of most calves fed colostrum by nipple bottle.
Calves need to ingest at least 100 g IgG1 in the first colostrum feeding to insure adequate transfer of passive immunity. Thus the routine force-feeding of a sufficient amount of pooled colostrum immediately after birth results in high serum levels of colostrum immunoglobulins in dairy calves and is becoming a common practice in dairy herds.
Encouraging and assisting the calf to suck within 1 hour after birth is also effective. The provision of early assisted sucking of colostrum to satiation within 1 hour after birth will result in high concentrations of absorbed immunoglobulins in the majority of calves. The ingestion of 100 g or more of colostral immunoglobulins within a few hours after birth is more effective in achieving high levels of colostral immunoglobulins in calves than either leaving the calf with the cow for the next 12–24 hours or encouraging the calf to suck again at 12 hours, which will not result in a significant increase in absorbed immunoglobulins.
Despite early assisted sucking, a small proportion of calves will remain hypogammaglobulinemic because of low concentrations of immunoglobulins in their dams’ colostrum, usually associated with leakage of colostrum from the udder before calving.
In large herds where economics permit, a laboratory surveillance system may be used on batches of calves to determine the serum levels of immunoglobulin acquired. An accurate analysis may be done by electrophoresis or an estimation using the zinc sulfate turbidity test. Blood should be collected from calves at 24 hours of age. Samples taken a few days later may not be a true reflection of the original serum immunoglobulin levels. The information obtained from determination of serum immunoglobulins in calves at 24 hours of age can be used to improve management practices, particularly the early ingestion of colostrum.
Quality of colostrum
Specific gravity
Differentiating high-immunoglobulin-concentration colostrum from low-immunoglobulin-concentration is problematic.8 Measurement of the specific gravity of the colostrum of dairy cows with a commercially available hydrometer (Colostrometer) has been explored.86 Originally it was claimed that measurement of specific gravity provided an inexpensive and practical method for estimating colostral Ig concentration. However, the specific gravity of colostrum is more correlated with its protein concentration than Ig concentration and varies with colostral temperature, thus limiting the predictive accuracy of the test. In addition, different relationships between specific gravity and Ig concentration of colostrum have been observed for different populations of Holstein and Jersey cows and between herds. Specific gravity may also vary considerably according to season of the year. Specific gravity was measured in 1085 first-milking colostrum samples from 608 dairy cows of four breeds on a single farm during a 5-year period.86 The specific gravity more closely reflected protein concentration than IgG1 concentration and was markedly affected by month of calving. Colostral specific gravity values were highest for Holstein and Jersey cows, cows in third or later lactation and cows calving in autumn. They were lowest in Brown Swiss and Ayrshire cows, cows in first or second lactation, and cows calving in summer. Thus using the specific gravity of colostrum as an indicator of IgG1 concentration has potential limitations.
Frozen and thawed colostrum
Colostrum can be banked as frozen colostrum for future use.87 Excess colostrum can be stored frozen and thawed as necessary to provide an IgG source when administration of dam colostrum is impractical or insufficient. Experience has shown that the composition of frozen colostrum remains constant throughout storage. No significant changes in pH, percentage acidity, milk fat, total solids, total nitrogen, or nonprotein resulted from colostrum being stored. Feeding 4 L of frozen thawed colostrum (which had been frozen at −20°C for 24 h) to calves by oroesophageal tube at 3 hours after birth did not result in a significant difference in IgG absorption when compared to calves receiving fresh colostrum.87
Pasteurization of colostrum
Several infectious diseases of cattle can be transmitted from the dam to the calf through colostrum contaminated by direct shedding from the mammary gland or postharvest contamination. These diseases include Johne’s disease, bovine leukosis, Mycoplasma spp., Salmonella spp., and E. coli. Strategies to control transmission of infectious agents to calves include pasteurizing colostrum. Pasteurization is effective in destroying Mycoplasma bovis, Mycoplasma californicum, and Mycoplasma canadense if an adequate temperature and time are used.
The method of pasteurization of colostrum affects its quality for calves. The potential disadvantage of heat-treating colostrum is that the immunoglobulins may become denatured. Pasteurization at 76°C for 15 minutes results in a marked decrease in calf serum IgG concentrations, a severe failure of transfer of passive immunity, indicating that the colostral immunoglobulins were either destroyed or altered so that absorption was impaired. Pasteurization at 76°C for 15 minutes destroys or alters colostral proteins and affects the serum concentration of lactoferrin and neutrophil oxidative metabolism.88 Pasteurization of colostrum at 63°C for 15 minutes causes only negligible decreases in colostral IgG concentrations when fed to calves.89 However, these lower temperatures are less effective in the destruction of Mycobacterium avium subsp. paratuberculosis and other infectious agents transmitted through colostrum.
The effect of commercial on-farm batch pasteurization on colostrum IgG concentrations, fluid characteristics and serum IgG concentrations in calves fed fresh versus pasteurized colostrum have been compared.90 Pasteurization of moderately sized batches (57 L) using a commercial batch pasteurizer consistently produces a product of normal or slightly thickened consistency that can be fed to calves. Batch pasteurization of 57 L at 63°C for 30 minutes results in a significant reduction of IgG in colostrum (26%) but much less than when 95 L is pasteurized. The percentage loss of IgG is significantly reduced when starting with high-quality fresh colostrum (> 60 mg/L). Feeding pasteurized colostrum results in significantly lower serum IgG concentrations in calves. However, acceptable serum IgG levels can be achieved if the pasteurized colostrum is fed immediately after birth, if at least 4 L is fed and if the interval between the first and second feedings of colostrum is shortened.
Colostrum supplements and replacers
Some colostrum-derived oral supplements containing immunoglobulin are available for newborn calves in which colostrum intake is suspected or known to be inadequate. Colostrum supplement products have been developed to provide exogenous IgG to calves when the dam’s fresh colostrum is of low IgG concentration. Many producers also use these products to replace colostrum when it is unavailable as a result of maternal agalactia, acute mastitis or other causes of inadequate colostrum supply. However, they contain low immunoglobulin concentrations compared to those found in high-quality first-milking colostrum. Most colostral supplements provide only 25–45 g IgG/dose of 454 g, which is reconstituted in 2 L of water. Feeding one or even two doses of such supplements is insufficient to provide a mass of 100 g of IgG within the first 12 hours after birth. Colostrum replacers are intended to provide the sole source of IgG and thus must provide at least 100 g IgG. Newborn colostrum-deprived dairy calves fed spray-dried colostrum containing 126 g of immunoglobulin in 3 L of water as their sole source of Ig achieved normal mean serum immunoglobulin concentrations.91 Whey protein concentrate as a colostrum substitute, administered to calves as a single feeding, was ineffective in preventing neonatal morbidity and mortality compared with a single feeding of pooled colostrum.92
The IgG derived from bovine serum or Ig concentrates from bovine plasma are well absorbed by neonatal calves when given in adequate amounts.93,94 The serum concentration of IgG in calves at 2 days of age force-fed a colostrum supplement containing spray-dried serum (total of 90 g immunoglobulin protein) within 3 hours after birth was much lower than in calves fed 4 L of fresh colostrum.95 The mass of IgG and the method of processing are critical. Products providing less than 100 g of IgG/dose should not be used to replace colostrum.
To be successful, colostral supplements and replacers must provide enough IgG mass, which results in 24-hour calf serum IgG concentrations of more than 10 g/L.
Purified bovine immunoglobulin
The administration of purified bovine gammaglobulin to calves that are deficient appears to be a logical approach but the results have been unsuccessful. Large doses (30–50 g) of gammaglobulin given intravenously would be required to increase the level of serum gammaglobulin from 0.5 g/dL to 1.5 g/dL of serum, which is considered an adequate level. The cost would be prohibitive. The administration of gammaglobulins by any parenteral route other than the intravenous route does not result in a significant increase in serum levels of the immunoglobulin.
To be effective, infusion of immunoglobulin derived from blood must increase serum IgG concentrations and reduce morbidity and mortality prior to weaning without affecting later production. Parenteral infusions of immunoglobulins will increase the concentrations of serum IgG in calves but may not necessarily have an effect on morbidity or mortality.96 High levels of specific circulating Ig can serve as a reservoir of antibody to move into the intestine and prevent enteric infection.97 Thus immunoglobulin sources other than colostrum may not provide Ig that are specific for antigens present in the environment or might be insufficient when calves are exposed to a heavy infection pressure.
The other factors that influence the ingestion of colostrum and the absorption of immunoglobulin are presented in the section on the epidemiology of colibacillosis, above, and in Chapter 3.
Guidelines to insure transfer of colostral immunoglobulins
Some guidelines for insuring that newborn farm animals ingest sufficient quantities of colostrum and absorb adequate amounts of colostral immunoglobulins are summarized here. Additional details are presented in Chapter 3.
Dairy calves
The following should be implemented:
• Immediately after birth, unless the calf is a vigorous sucker, colostrum should be removed from the cow and fed by nipple bottle or by stomach tube at the rate of at least 50 mL/kg BW in the first 2 hours. Encouragement and assistance to suck to satiation within the first hour after birth is also highly effective in achieving high levels of colostral immunoglobulins in the serum of the calf.98 If pooled colostrum is used, calves should be fed 3–4 L of first-milking colostrum
• The calf can be left with the cow for at least 2 days. This contact will improve the absorption of immunoglobulin. However, there is now a trend, at least in large dairy herds, to remove the calf immediately after birth, place it in a stall and force-feed it colostrum. This practice may also prevent spread of infectious disease from mature cattle to calves
• Following the colostral feeding period, dairy calves are usually placed in individual stalls until weaning. The daily feeding of stored fermented colostrum to newborn calves for up to 3 weeks after birth provides a source of lactoglobulins in the intestinal tract and reduces the incidence of neonatal diarrhea of calves due to a wide variety of pathogens, but this practice may be impractical
• Calves should be fed regularly, and preferably by the same person. One of the most important factors affecting dairy calf mortality is the concern and care provided by the calf rearer. The calf mortality rate is likely to be lower when members of the family care for the calves compared to hired help
• Colostrum stored at room temperature should be handled adequately to minimize bacterial contamination. Up to 36% of colostrum samples from calf nursing bottles in dairy herds may be contaminated with Staphylococcus spp., Gram-negative rods, coliforms, and Streptococcus uberis.99 The relative risk of contamination with more than 100 000 bacteria/mL was greater in warm months than in cooler months, and in colostrum fed to male calves. The greater risk to male calves may reflect less attention to hygiene and management procedures compared to female calves
• The housing and ventilation must be adequate to avoid stress.
Beef calves
The management strategies to decrease calf death losses in beef herds has been described.100 The role of management intervention in the prevention of neonatal deaths includes measures to improve host defenses and environmental hygiene to minimize outbreaks of neonatal disease. Specific attention is centered on preventing dystocia, improving transfer of colostral immunoglobulins, and limiting environmental contamination.100
The following should be implemented:
• Management of the beef herd must emphasize prevention of dystocia, which involves limiting calf size and ensuring adequate pelvic area of the dams100
• Beef calves should be assisted at birth, if necessary, to avoid exhaustion and weakness from a prolonged parturition100
• Normally beef calves will make attempts to get up and suck within 20 minutes after birth but this may be delayed for up to 8 hours or longer. Beef calves that do not suck within 2 hours should be fed colostrum by nipple bottle or stomach tube. Whenever possible they should be encouraged and assisted to suck to satiation within 1 hour after birth. The dam can be restrained and the calf assisted to suck. If the calf is unable or unwilling to suck, the dam should be restrained and milked out by hand, and the calf fed the colostrum with a nipple bottle or stomach tube. The mean volume of colostrum and colostral immunoglobulins produced in beef cows and the absorption of colostral immunoglobulins by their calves can vary widely. Beef calves deserted by indifferent dams need special attention. Failure of transfer of passive immunity is common and estimated at 10–40% of beef calves100
• Constant surveillance of the calving grounds is necessary to avoid overcrowding, to detect diarrheic calves that should be removed, to avoid mismothering, and to insure that every calf is seen to nurse its dam. Although up to 25% of beef calves may not have sufficient serum levels of immunoglobulins, the provision of excellent management will minimize the incidence of colibacillosis. The recently developed practice of corticosteroid-induced parturition in cattle may result in a major mismothering problem if too many calves are born too quickly in a confined space. Every management effort must be used to establish the cow/calf herd as soon as possible after birth. This will require high-quality management to reduce even further the infection rate and minimize any stressors in the environment.
Lambs
Lambs require 180–210 mL of colostrum/kg BW during the first 18 hours after birth to provide sufficient energy for heat production.101 Such an intake will usually also provide enough colostral immunoglobulins. Early encouragement and assistance of the lambs to suck the ewe is important. Well-fed ewes usually have sufficient colostrum for singletons or twins. Underfed ewes may not have sufficient colostrum for one or more lambs and supplementation from stored colostrum obtained by milking other high-producing ewes is a useful practice.
Piglets
The following should be implemented:
• Every possible economical effort must be made to insure that each newborn piglet obtains a liberal supply of colostrum within minutes of birth. The farrowing floor must be well drained and it must be slip-proof to allow the piglets to move easily to the sow’s udder. Some herdsmen provide assistance at farrowing, drying off every piglet as it is born and placing it immediately onto a teat
• The washing of the sow’s udder immediately before farrowing with warm water and soap will reduce the bacterial population and may provide relief in cases of congested and edematous udders
• The piglet creep area must be dry, appropriately heated for the first week and free from drafts. During farrowing, colostrum is released in discrete ejections, possibly by discrete release of oxytocin associated with parturition. Therefore, as the piglets are born they must be as close to the udder as possible in order to take advantage of these discrete ejections.
Increasing specific resistance of the newborn by vaccinating the pregnant dam or the newborn
The immunization of neonate farm animals against colibacillosis by vaccination of the pregnant dam or by vaccination of the fetus or the neonate has received considerable research attention in recent years and the results appear promising.102
Such vaccines are practical and effective because:
• Most fatal enterotoxigenic E. coli infections in farm animals occur in the early neonatal period when antibody titers in colostrum and milk are highest
• More than 90% of the enterotoxigenic E. coli in farm animals belong to a small family of fimbrial antigens
• Fimbriae consist of good protein antigens on the bacterial surface where they are readily accessible to antibody
• Fimbriae are required for a critical step (adhesion–colonization) early in the pathogenesis of the disease
• Novel or previously low-prevalence fimbrial antigens have not emerged to render the vaccines ineffective.
The pregnant dam is vaccinated 2–4 weeks before parturition to induce specific antibodies to particular strains of enteropathogenic E. coli, and the antibodies are then passed on to the newborn through the colostrum. The mechanism of protection is the production of antibodies against the pilus antigens, which are responsible for colonization of the E. coli in the intestine.102
Vaccination is an aid to good management and not a replacement for inadequate management.
Vaccines to prevent enterotoxigenic E. coli diarrhea in calves and piglets are based on the prevailing fimbrial antigens for colonization by enterotoxigenic E. coli in calves (F5) and newborn pigs (F4, F5, and F6). Reliable data on the efficacy of the commercial vaccines based on randomized clinical field trials are not available but most animal health professionals perceive that the vaccines are effective and that disease occurs primarily in unvaccinated herds. There are unpublished anecdotal reports that use of the vaccine in cattle has shifted the peak occurrence of diarrhea in calves from the first week to the third and fourth week after birth. The extensive use of fimbria-based vaccines can select against the prevailing fimbrial antigen types as reflected in the vaccines, and emergence of new or previously low-prevalence fimbrial antigens may occur. fimbriae antigenically distinct from F1, F4, F6, F41 occur among enterotoxigenic E. coli. However, these antigen types are less prevalent than those currently used in commercial vaccines. There is no evidence that enterotoxigenic E. coli with novel colonization mechanisms or new fimbrial antigens have emerged under the selection pressure of vaccination. Nor is there evidence that previously ‘low-prevalence’ fimbrial antigen type enterotoxigenic E. coli, not represented in the vaccines, have emerged as ‘common pathogens’ filling an ecological niche left by the fimbrial antigen types targeted by the vaccines.
Calves
Vaccination of pregnant cattle with either purified E. coli K99+ pili or a whole-cell preparation containing sufficient K99+ antigen can significantly reduce the incidence of enterotoxigenic colibacillosis in calves. Good protection is also possible when the dams are vaccinated with a four-strain E. coli whole-cell bacterin containing sufficient K99+ pilus antigen and the polysaccharide capsular K antigen. Colostral antibodies specific for K99+ pilus antigen and the polysaccharide capsular K antigen on the surface of the challenge exposure strain of enterotoxigenic E. coli are protective. There is a highly significant correlation between the lacteal immunity to the K99+ antigen and the prevention of severe diarrhea or death in calves challenged with enterotoxigenic E. coli. The colostral levels of K99+ antibody are highest during the first 2 days after parturition, which is the most susceptible period for enterotoxigenic colibacillosis to occur in the newborn calf. The continuous presence of the K99+ antibody in the lumen of the intestine prevents adherence of the bacteria to the intestinal epithelium. The K99+ antibody is also absorbed during the period of immunoglobulin absorption and may be excreted into the intestine during diarrhea. This may be one of the reasons that mortality is inversely proportional to serum immunoglobulin levels. The pregnant dams are vaccinated twice in the first year, 6 and 2 weeks prior to parturition. Each year thereafter they are given a single booster vaccination. An oil emulsion E. coli K99+ bacterin given once or twice to pregnant beef cows 6 weeks before calving elicited high levels of serum antibody that provided protection against experimental infection of newborn calves for up to 87 weeks after vaccination.
Vaccines containing both the K99+ antigen of enterotoxigenic E. coli and rotavirus, and in some cases coronavirus, have been evaluated with variable results. The colostral antibodies to the K99+ antigen are higher in vaccinated than unvaccinated dams but the colostral antibodies to rotavirus and coronavirus may not be significantly different between vaccinated and unvaccinated dams. In these field trials vaccination had no effect on the prevalence of diarrhea, calf mortality or the presence of the three enteropathogens. In other field trials the combined vaccine did provide some protection against outbreaks of calf diarrhea. The use of an inactivated oil-adjuvanted rotavirus E. coli vaccine given to beef cows in the last trimester of pregnancy decreases the mortality from diarrhea and has a positive influence on the average weight gains of the calves at weaning. To be effective the rotavirus and coronavirus antibodies must be present in the postcolostral milk for several days after parturition during the period when calves are most susceptible to the viral infection. Vaccination of pregnant cows twice during the dry period at intervals of 4 weeks can increase the colostral antibody levels to E. coli K99+ by 26 times on day 1 compared to controls. Much lower increases occur at the levels of coronavirus and rotavirus.
A commercially inactivated vaccine containing bovine rotavirus (serotype G6 P5), bovine coronavirus (originally isolated from a calf with diarrhea) and purified cell-free E. coli FS (K99) (adsorbed on to aluminum hydroxide gel), formulated as an emulsion in a light mineral oil has been evaluated in a herd of Ayrshire/Friesian cows vaccinated once 31 days before the first expected calving date.103 Compared to control cows, a significant increase in the mean specific antibody titer against all three antigens occurred in the serum of vaccinated animals (even in the presence of pre-existing antibody), which was accompanied by increased levels of protective antibody to rotavirus, coronavirus, and E. coli F5 (K99) in their colostrum and milk for at least 28 days.
Because naturally acquired antibodies to the J5 antigen may have an important role in the control of neonatal disease caused by bacterial infections with associated pathogens that share antigens with E. coli (J5 strain), vaccination of calves with an E. coli O111:B4(J5) vaccine at 1–3 days of age and 2 weeks later has been evaluated to control morbidity and mortality in dairy calves up to 60 days of age.29 The use of either a killed E. coli O111:B4(J5) bacterin or a modified live, genetically altered (aro-) Salmonella dublin vaccine, or both in neonatal calves was effective in reducing mortality due to colibacillosis and salmonellosis.104 Such a vaccine may be beneficial in controlling mortality in well-managed herds but is contraindicated in poorly managed herds.
Passive immunotherapy of calves under 2 days of age with J5 E. coli hyperimmune plasma given subcutaneously at a dose of 5 mL/kg BW has been examined.105 The plasma was safe and potent. It was not superior to control plasma or to no treatment for calf morbidity and mortality.
The oral administration of a K99+-specific monoclonal antibody to calves during the first 12 hours after birth may be an effective method of reducing the incidence of fatal enterotoxigenic colibacillosis, particularly when outbreaks of the disease occur in unvaccinated herds. Clinical trials indicate that the severity of dehydration, depression, weight loss and duration of diarrhea were significantly reduced in calves that had received the K99+-specific monoclonal antibody. In experimentally challenged calves the mortality was 29% in the treated calves and 82% in the control calves.
The decision to vaccinate in any particular year will depend on the recognition of risk factors. Such risk factors include:
• A definitive diagnosis of enteropathogenic K99+ E. coli in the previous year
• A population density in the calving grounds that is conducive to the disease
• Calving during the year when the environmental conditions are wet and uncomfortable for the calves
• A large percentage of primiparous dams that do not have protective levels of K99+ antibody in their colostrum.
Piglets
Piglets born from gilts are more susceptible than those from mature sows, which suggests that immunity improves with parity. On a practical basis this suggests that gilts should be mixed with older sows that have been resident on the premises for some time. The length of time required for such natural immunization to occur is uncertain, but 1 month during late gestation seems logical.
Naturally occurring enteric colibacillosis in newborn piglets can be effectively controlled by vaccination of the pregnant dam. Field trials in large-scale farm conditions indicate that the vaccines are efficacious.106 Partial budget analysis of vaccinating pregnant sows with E. coli vaccines revealed an economic return on investment of 124% because of the decrease in morbidity and mortality due to diarrhea in piglets 1–2 weeks of age.107 Three antigen types of pili, designated K88+, K99+, and 987P, are now implicated in colonization of the small intestine of newborn piglets by enterotoxigenic E. coli. The vaccination of pregnant sows with oral or parenteral vaccines containing these antigens will provide protection against enterotoxigenic colibacillosis associated with E. coli bearing pili homologous to those in the vaccines. The parenteral vaccines are cell-free preparations of pili, and the oral vaccines contain live enteropathogenic E. coli. The oral vaccine is given 2 weeks before farrowing and is administered in the feed daily for 3 days as 200 mL per day of a broth culture containing 1011 E. coli. A simple and effective method of immunization of pregnant sows is to feed live cultures of enterotoxigenic E. coli isolated from piglets affected with neonatal colibacillosis on the same farm. The oral vaccine can be given in the feed, beginning about 8 weeks after breeding and continued to parturition. The oral vaccine results in the stimulation of IgA antibody in the intestinal tract, which is then transferred to the mammary gland and into the colostrum. A combination of oral and parenteral vaccination is superior to either route alone. The parenteral vaccine is given about 2 weeks after breeding and repeated 2–4 weeks before parturition. The parenteral vaccination results in the production of high levels of IgM antibody for protection against both experimental and naturally occurring enterotoxigenic colibacillosis. This vaccination also reduces the number of E. coli excreted in the feces of vaccinated sows, which are major sources of the organism. Immunization of pregnant sows with an E. coli bacterin enriched with the K88+ antigen results in the secretion of milk capable of preventing adhesion of K88+ E. coli to the gut for at least 5 weeks after birth, at which time the piglet becomes naturally resistant to adhesion by the organism.
The possibility of selecting and breeding from pigs that may be resistant genetically to the disease is being explored. The highest incidence of diarrhea occurs in progeny of resistant dams and sired by susceptible sires. The homozygous dominants (SS) and the heterozygotes (Ss) possess the receptor and are susceptible whereas in the homozygous recessives (ss) it is absent and the pigs are resistant. Sows that are genetically resistant may not be able to mount an immune response to the K88+ antigen because of the inability of the organism to colonize the intestinal tract.
Competitive exclusion culture
An alternative method of control is the use of competitive exclusion cultures.108 The theory of competitive exclusion technology is to colonize the neonatal gastrointestinal tract with beneficial/commensal bacteria considered to be the normal flora of the healthy animals of a particular species. The mechanism of action is not known but hypotheses include: exclusion of enteropathogens by competitive attachment sites and/or for nutrients; stimulation of the local immune mechanisms, which preclude colonization/invasion by enteric pathogens; and the production of various antimicrobial substances that either have direct action on pathogenic bacteria or produce conditions within the intestine that are unfavorable for the growth and colonization by pathogens. Experimentally, the oral administration of a porcine competitive exclusion culture to piglets within 12 hours after birth resulted in significant reductions in mortality, incidence of fecal shedding, and intestinal colonization by E. coli when compared to control values. Mortality decreased from 23% in the control group to 2.7% in the treated group.
Lambs and kids
Vaccination of pregnant ewes with K99+ antigen will confer colostral immunity to lambs challenged with homologous enteropathogenic E. coli. The pregnant ewes are vaccinated twice in the first year, at 8–10 weeks and 2–4 weeks before lambing, and in the second year one vaccination 2–4 weeks before lambing is adequate.
Immunization of pregnant goats has been used to stimulate the development of lacteal immunity against naturally occurring colibacillosis in kids.109 Vaccination of pregnant does 1 month before parturition with a subunit vaccine containing K88, K9, and 987P fimbrial antigens of E. coli, and C. perfringens types B, C, and D toxins in an aluminum hydroxide adjuvant, along with improved management conditions, was highly successful in reducing neonatal morbidity and mortality due to diarrhea.40 Compared to two control groups, one in which no improvement in management was made and the second in which improvements were made without vaccination, in the vaccinated group with improved management conditions, neonatal morbidity and mortality were both reduced by a factor of 3 in Group 1 and by factors of 9.5 and 12.5 in Group 3. Also, the duration of diarrhea was 3.7 and 12 times shorter in the kids of Groups 2 and 3, respectively.
Acres SD. Enterotoxigenic Escherichia coli infections in newborn calves: a review. J Dairy Sci. 1985;68:229-256.
Gyles CL, editor. Escherichia coli in domestic animals and humans. Wallingford, UK: CAB International, 1994.
Angelos SM, VanMetre DC. Treatment of sodium balance disorders. Vet Clin North Am Food Anim Pract. 1999;15:587-607.
Berchtold J. Intravenous fluid therapy of calves. Vet Clin North Am Food Anim Pract. 1999;15:505-530.
Constable PD. Hypertonic saline. Vet Clin North Am Food Anim Pract. 1999;15:559-585.
Garcia JP. A practitioners’ view on fluid therapy in calves. Vet Clin North Am Food Anim Pract. 1999;15:533-543.
Kasari TR. Metabolic acidosis in calves. Vet Clin North Am Food Anim Pract. 1999;15:473-486.
Naylor JM. Oral electrolyte therapy. Vet Clin North Am Food Anim Pract. 1999;15:487-504.
Weaver DM, Tyler JW, VanMetre DC, et al. Passive transfer of colostral immunoglobulins in calves. J Vet Intern Med. 2000;14:569-577.
Barrington GM, Parish SM. Bovine neonatal immunology. Vet Clin North Am. 2001;17:463-476.
DebRoy C, Maddox CW. Identification of virulence attributes of gastrointestinal Escherichia coli isolates of veterinary significance. Anim Health Res Rev. 2001;1:129-140.
George JW. The usefulness and limitations of hand-held refractometers in veterinary laboratory medicine: an historical and technical review. Vet Clin Pathol. 2001;30:201-210.
Barrington GM, Gay JM, Evermann JF. Biosecurity for neonatal gastrointestinal diseases. Vet Clin North Am Food Anim Pract. 2002;18:7-34.
Renter DG, Sargeant JM. Enterohemorrhagic Escherichia coli O157H:7: epidemiology and ecology in bovine production environments. Anim Health Res Rev. 2002;3:83-94.
Constable P. Fluid and electrolyte therapy in ruminants. Vet Clin North Am Food Anim Pract. 2003;19:557-597.
Constable PD. Antimicrobial use in the treatment of calf diarrhea. J Vet Intern Med. 2004;18:8-17.
Gyles CL, Prescott JF, Songer JG, Thoen CO. Pathogenesis of bacterial infections in animals, 3rd ed. Ames, IA: Blackwell, 2004.
Larson RL, Tyler JW, Schultz LG, et al. Management strategies to decrease calf death losses in beef herds. J Am Vet Med Assoc. 2004;224:42-48.
Moxley RA. Escherichia coli O157H:7: an update on intestinal colonization and virulence mechanisms. Anim Health Res Rev. 2004;5:15-33.
1 Gyles CL, editor. Escherichia coli in domestic animals and humans. Wallingford, UK: CAB International, 1994.
2 Gyles CL, et al. Pathogenesis of bacterial infections in animals, 3rd ed. Ames, IA: Blackwell, 2004.
3 DebRoy C, Maddox CW. Anim Health Res Rev. 2001;1:129.
4 Moxley RA. Anim Health Res Rev. 2004;5:15.
5 Renter DG, Sargeant JM. Anim Health Res Rev. 2002;3:83.
6 Vihan VS, et al. Prev Vet Med. 1992;13:179.
7 Chandler DS, et al. Vet Microbiol. 1994;38:203.
8 Weaver DM, et al. J Vet Intern Med. 2000;14:569.
9 Clement JC, et al. J Am Vet Med Assoc. 1995;207:1134.
10 Pare J, et al. Can J Vet Res. 1993;57:241.
11 Wesselink R, et al. N Z Vet J. 1999;47:31.
12 Filteau V, et al. Can Vet J. 2003;44:907.
13 Christley RM, et al. Prev Vet Med. 2003;57:209.
14 Schumann FJ. Can J Vet Res. 1990;54:366.
15 Frank GH, et al. J Clin Microbiol. 1994;32:256.
16 Aldridge BM, et al. J Am Vet Med Assoc. 1993;203:1324.
17 Contrepois M, et al. Vet Microbiol. 1998;64:75.
18 Fecteau G, et al. Vet Microbiol. 2001;78:241.
19 Bell CJ, et al. Vet Microbiol. 2002;85:251.
20 Fischer J, et al. Am J Vet Res. 1994;55:991.
21 Mainil JG, et al. Vet Microbiol. 1993;54:1064.
22 De la Feunte R, et al. Am J Vet Res. 2002;63:262.
23 Pearce MC, et al. Appl Environ Microbiol. 2004;70:1708.
24 Cobbold R, Desmarchelier P. Vet Microbiol. 2000;71:125.
25 Gunning RF, et al. Vet Rec. 2001;148:780.
26 Orden JA, et al. Vet Microbiol. 1998;63:239.
27 Kang SJ, et al. Vet Microbiol. 2004;98:323.
28 Irino K, et al. Vet Microbiol. 2005;105:29.
29 Aidar L, et al. Can J Vet Res. 2000;64:15.
30 Mercado EC, et al. J Vet Med B. 2004;51:82.
31 Wani SA, et al. Vet Rec. 2004;154:506.
32 Bettelheim KA, et al. Aust Vet J. 2001;79:289.
33 Burns AL, et al. Vet Microbiol. 1996;49:235.
34 Wray C, et al. Res Vet Sci. 1993;54:290.
35 Mainil JG, et al. Vet Microbiol. 1999;70:123.
36 Orden JA, et al. Vet Microbiol. 1999;66:265.
37 Van Bost S, et al. Vet Microbiol. 2001;82:311.
38 Casey TA, et al. Am J Vet Res. 1992;53:1488.
39 Cambier C, et al. Am J Vet Res. 2001;62:799.
40 Kristas SK, et al. Small Rumin Res. 2003;50:51.
41 Grove-White DH, White DG. Vet Rec. 1999;144:639.
42 Omole O, et al. J Nutr. 2001;131:2128.
43 Ewaschuk JB, et al. J Vet Intern Med. 2004;18:744.
44 Ewaschuk JB, et al. J Vet Intern Med. 2003;17:940.
45 Kasari TR. Vet Clin North Am Food Anim Pract. 1999;15:473.
46 Angelos SM, et al. J Am Vet Med Assoc. 1999;214:1364.
47 Angelos SM, VanMetre DC. Vet Clin North Am Food Anim Pract. 1999;15:587.
48 Carmalt JL, et al. J Am Vet Med Assoc. 2000;216:68.
49 Gutzwiller A, Blum JW. Am J Vet Res. 1996;57:560.
50 Stordeur P, et al. Microbes Infect. 2000;2:17.
51 Wani SA, et al. Small Rumin Res. 2004;52:145.
52 Green SL, Smith LL. J Am Vet Med Assoc. 1992;201:125.
53 Fecteau G, et al. Can Vet J. 1997;38:101.
54 Fecteau G, et al. Can Vet J. 1997;38:95.
55 Lofstedt J, et al. J Vet Intern Med. 1999;13:81.
56 Constable PB, et al. J Am Vet Med Assoc. 1998;212:991.
57 Randall LP, et al. Vet Rec. 1997;140:112.
58 Woodward MJ, et al. Vet Microbiol. 1992;31:251.
59 Knowles TG, et al. Vet Rec. 2000;147:593.
60 Grove-White DH, White DG. Vet Rec. 1993;133:499.
61 Grove-White DH, Michell AR. Vet Rec. 2001;148:365.
62 Constable PD. Am J Vet Res. 2002;63:482.
63 Nappert G, Naylor JM. Aust Vet J. 2001;42:364.
64 Dawes ME, et al. J Am Vet Med Assoc. 2002;220:791.
65 Calloway CD, et al. J Am Vet Med Assoc. 2002;221:1606.
66 Tyler JW, et al. J Vet Intern Med. 1999;13:40.
67 Tyler JW, et al. J Vet Intern Med. 1999;13:335.
68 Perino LJ, et al. Am J Vet Res. 1993;54:56.
69 Maden M, et al. J Vet Med B. 2003;50:128.
68 Garcia JP. Vet Clin North Am Food Anim Pract. 1999;15:533.
69 Senturk S. J Vet Med A. 2003;50:57.
70 Constable PD. Vet Clin North Am Food Anim Pract. 1999;15:559.
71 Berchtold J. Vet Clin North Am Food Anim Pract. 1999;15:505.
72 Naylor JM. Vet Clin North Am Food Anim Pract. 1999;15:487.
73 Constable P. Vet Clin North Am Food Anim Pract. 2003;19:557.
74 Teale CJ, et al. Vet Rec. 2005;156:186.
75 Constable PD. J Vet Intern Med. 2004;18:8.
76 Gunn GJ, et al. Vet J. 2003;165:172.
77 Hariharan H, et al. Can Vet J. 2004;45:605.
78 Gunn GJ, Low JC. Vet Rec. 2003;152:537.
79 Orden JA, et al. Vet Rec. 2000;147:576.
80 Orden JA, et al. J Vet Med B. 2000;47:329.
81 White DG, et al. J Clin Microbiol. 2000;38:4593.
82 Orden JA, et al. J Antimicrob Chemother. 2001;48:421.
83 Langford FM, et al. J Dairy Sci. 2003;86:3963.
84 Lofstedt J, et al. Can J Vet Res. 1996;60:210.
85 Howard P. Vet Rec. 2004;153:262.
86 Morin DE, et al. J Dairy Sci. 2001;84:937.
87 Holloway NM, et al. J Am Vet Med Assoc. 2001;219:357.
88 Lakritz J, et al. Am J Vet Res. 2000;61:1021.
89 Tyler JW, et al. J Dairy Res. 2000;67:619.
90 Godden SM, et al. J Dairy Sci. 2003;86:1503.
91 Chelak BJ, et al. Can Vet J. 1993;34:407.
92 Mee JF, et al. J Dairy Sci. 1996;79:886.
93 Arthrington JD, et al. J Dairy Sci. 2000;83:1463. 2834
94 Quigley JD, et al. J Dairy Sci. 2001;84:2059.
95 Holloway NM, et al. J Vet Intern Med. 2002;16:187.
96 Quigley JD, Welborn MG. J Dairy Sci. 1996;79:2032.
97 Besser TE, et al. J Virol. 1988;62:2234.
98 Quigley JD, et al. J Dairy Sci. 1995;78:893.
99 Fecteau G, et al. Can Vet J. 2002;43:523.
100 Larson RL, et al. J Am Vet Med Assoc. 2004;224:42.
101 Mellor DJ, Murray L. Vet Rec. 1986;118:351.
102 Moon HW, Bunn TO. Vaccine. 1993;31:213.
103 Crouch CF, et al. Vet Rec. 2001;149:105.
104 Selim SA, et al. Vaccine. 1995;13:381.
105 Selim SA, et al. Vaccine. 1995;13:1149. 1454
106 Osek J, et al. Compend Immunol Microbiol Infect Dis. 1995;18:1.
107 Wittum TE, Dewey CE. J Swine Health Prod. 1996;4:9.