Pulmonary Care Plans
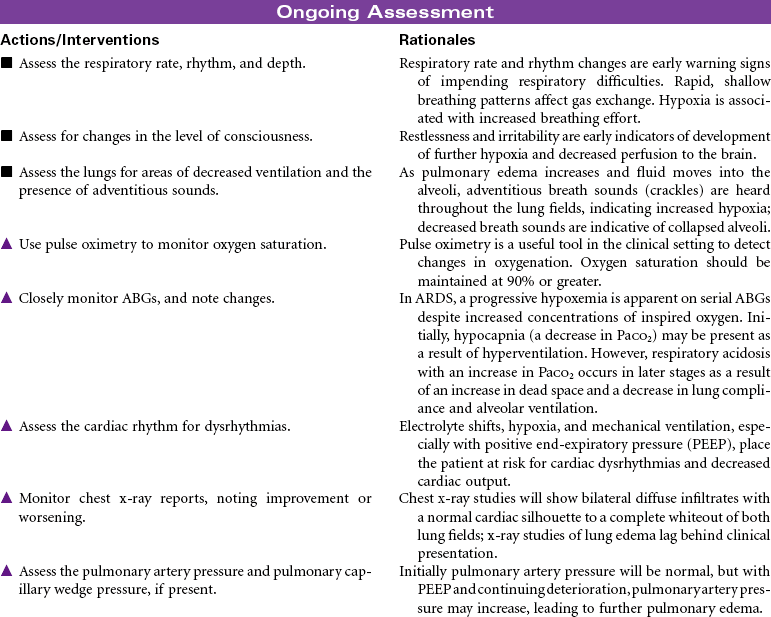
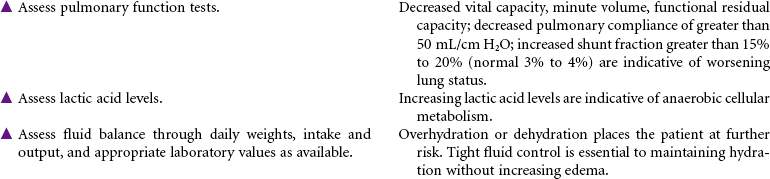
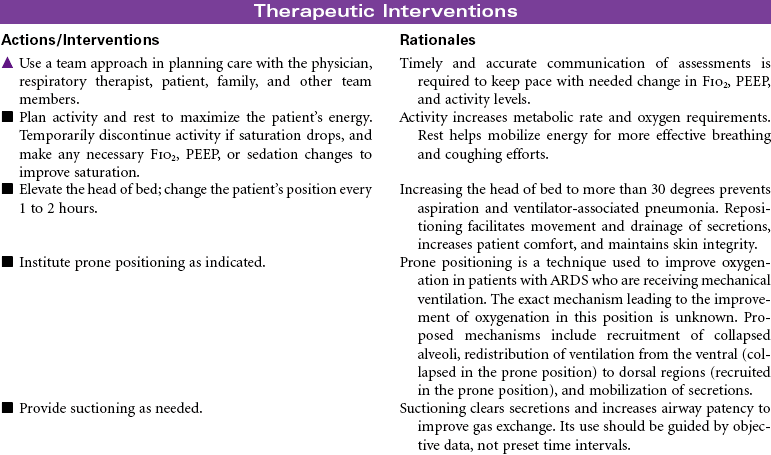
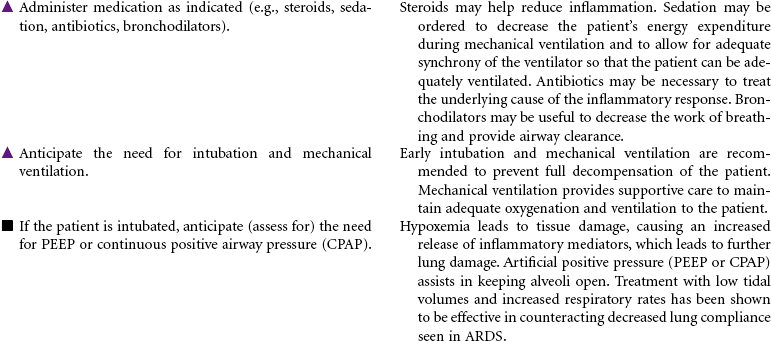
Acute Respiratory Distress Syndrome (ARDS)
 = Independent
= Independent  = Collaborative
= Collaborative For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
For additional care plans and an Online Care Plan Constructor, go to http://evolve.elsevier.com/Gulanick/.
Noncardiogenic Pulmonary Edema; Stiff Lung; Shock Lung; Wet Lung
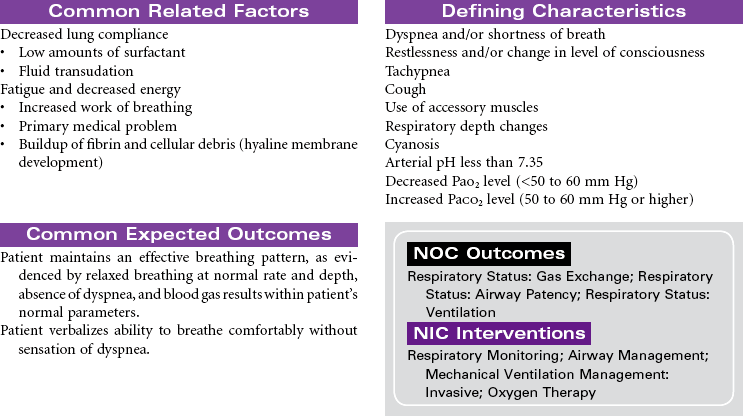
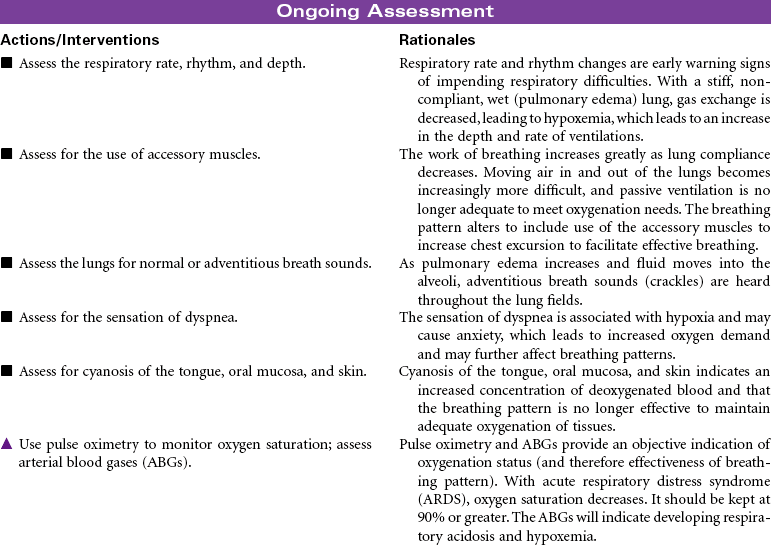
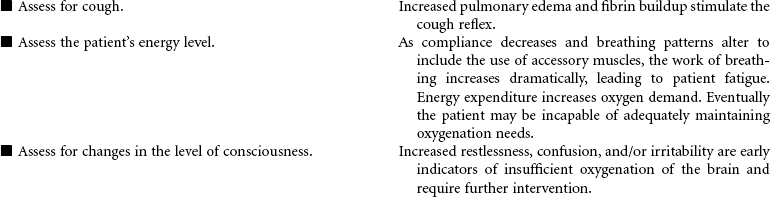
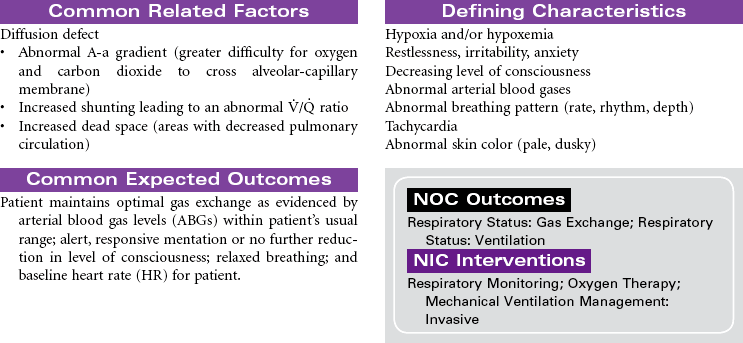
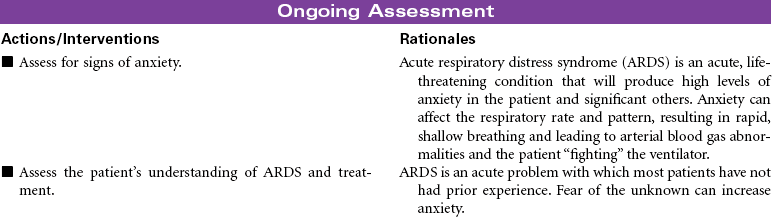
Acute respiratory distress syndrome (ARDS) is a form of respiratory failure characterized by noncardiogenic pulmonary edema and a refractory hypoxemia. The pathology results from damage to the alveolar-capillary membrane. This damage is caused by cytokines released by primed neutrophils during a massive immune response (systemic inflammatory response syndrome). These cytokines increase vascular permeability to such an extent that a massive noncardiac pulmonary edema develops. This edema not only interferes with gas exchange but also damages the pulmonary cells that secrete surfactant. Loss of surfactant allows alveoli to collapse and results in very stiff, noncompliant lungs. Fibrin and cell debris build up, forming a membrane (hyaline) and further decreasing gas exchange. The combined edema, loss of surfactant, alveoli collapse, and hyaline membrane formation lead to a progressive refractory hypoxemia and eventually death.
Anyone with a recent history of severe cell damage or sepsis is at risk for developing ARDS. Examples include individuals who have aspirated or who have suffered trauma, burns, multiple fractures, severe head injury, pulmonary contusions, near drowning (salt water aspiration seems to be slightly higher risk than fresh water aspiration), smoke inhalation, carbon monoxide exposure, drug overdose, oxygen toxicity, shock, and so on.
Even with outstanding care, the mortality rate for ARDS is 40% to 60%, and even those who survive may have permanent lung damage. With such a high mortality rate, it is clear that early detection and prevention are critical as is treatment of any causal factors. Thus careful assessment of all at-risk individuals for early warning signs of developing respiratory distress is a nursing responsibility. Unfortunately, the only early warning sign may be labored breathing and tachypnea. Once ARDS develops, nursing care focuses on maintenance of pulmonary functions. Despite evidence that ARDS is the result of an inflammatory response, anti-inflammatory therapy is not effective, and with time, respiratory failure with severe respiratory distress usually results. Research is focused on identifying new pharmacological treatments to halt the progressive downward cycle of ARDS, including human recombinant interleukin-1 receptor antagonist surfactant replacement therapy, corticosteroids, and the like.
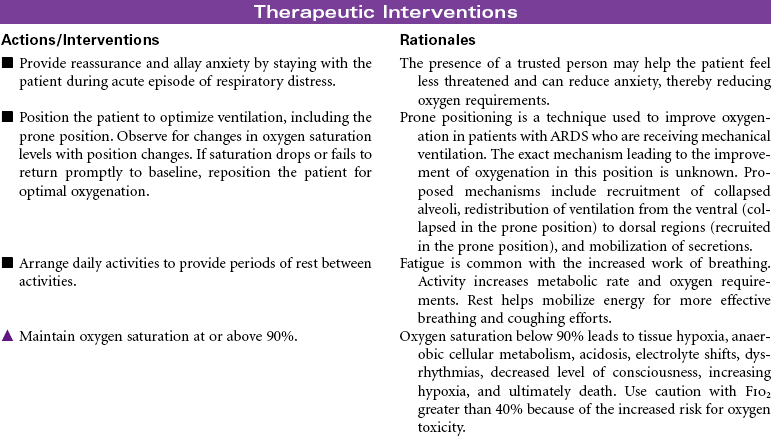
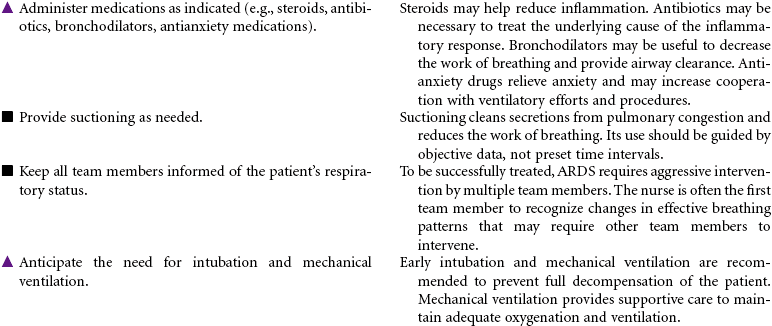
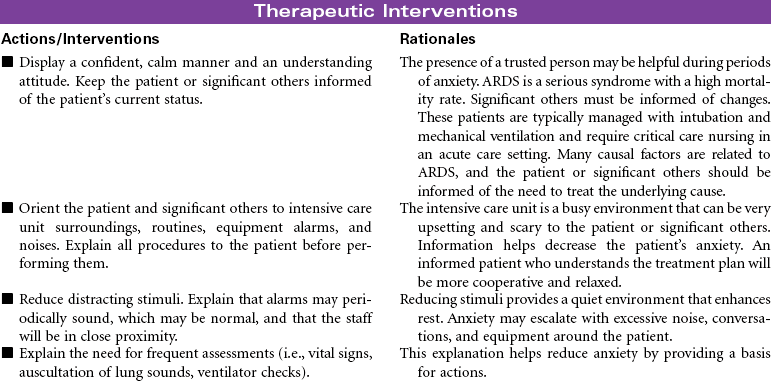
This care plan focuses on acute care in the critical care setting where the patient’s condition is typically managed with intubation and mechanical ventilation.
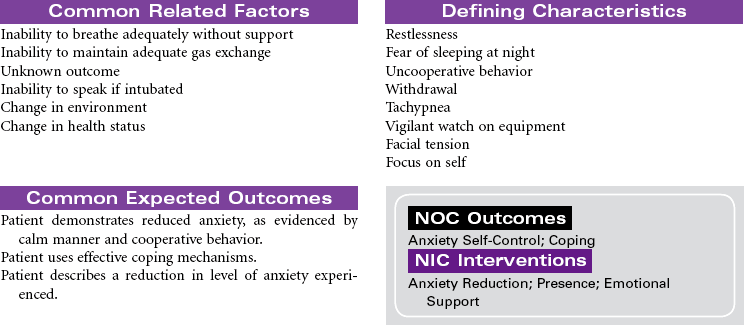
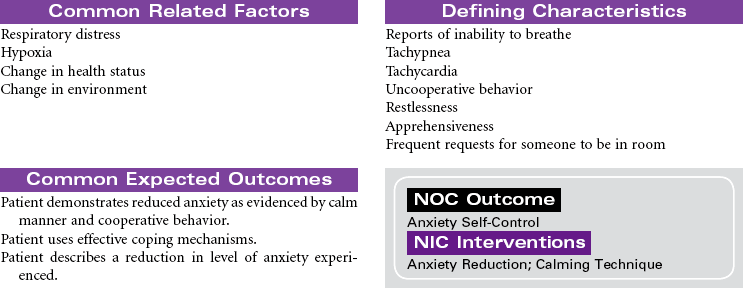
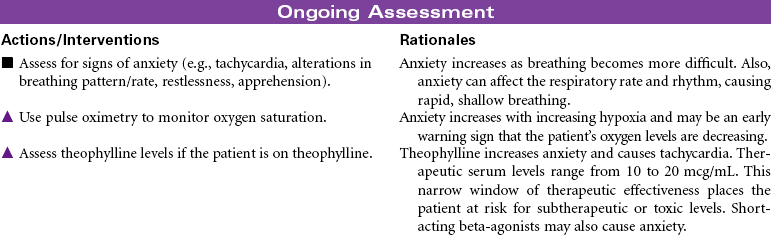
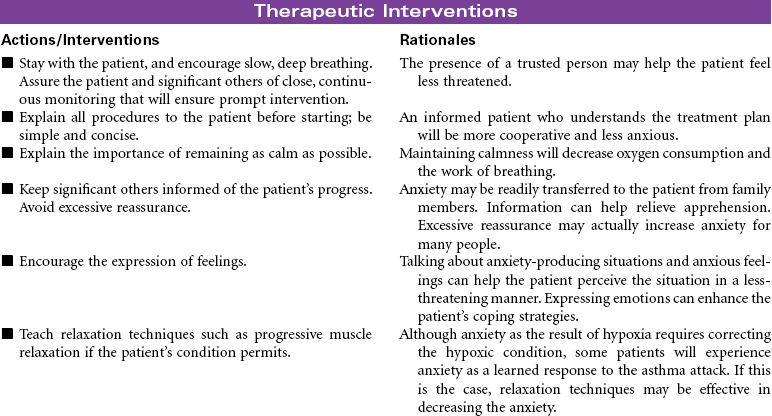
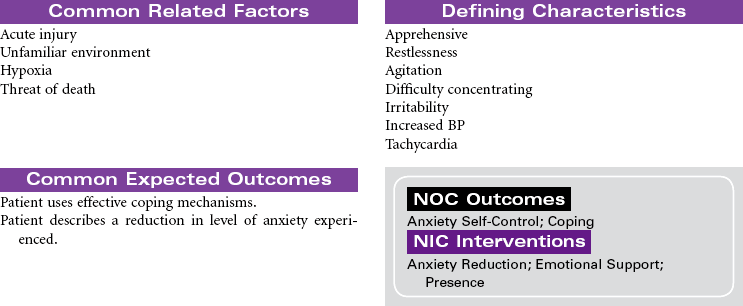
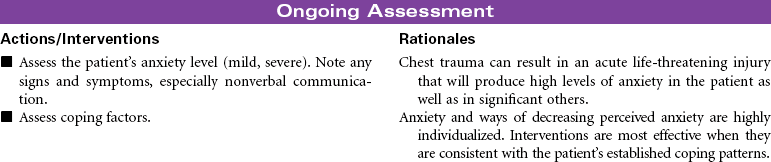
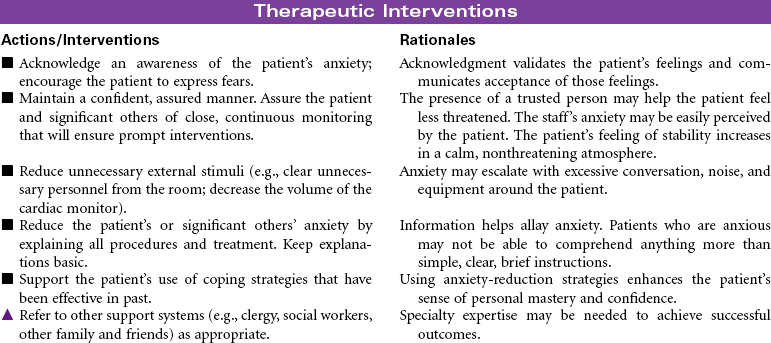
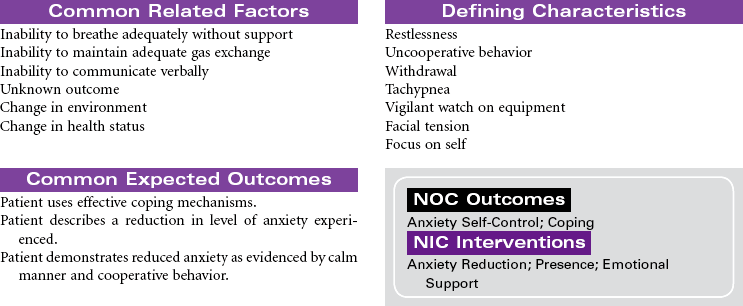
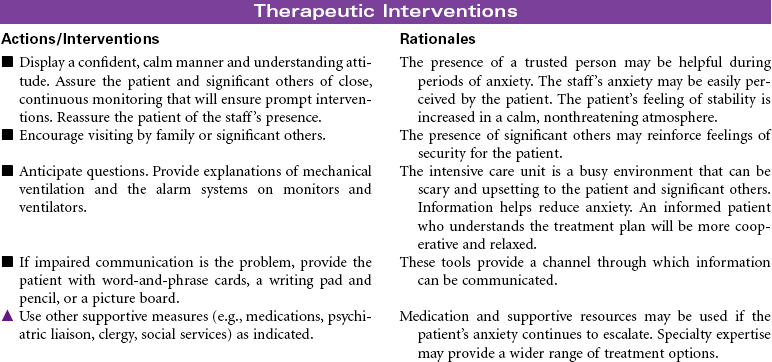
 Anxiety
Anxiety
Related Care Plans
Respiratory failure, acute, p. 490
Decreased cardiac output, p. 37
Imbalanced nutrition: Less than body requirements, p. 135
Impaired physical mobility, p. 126
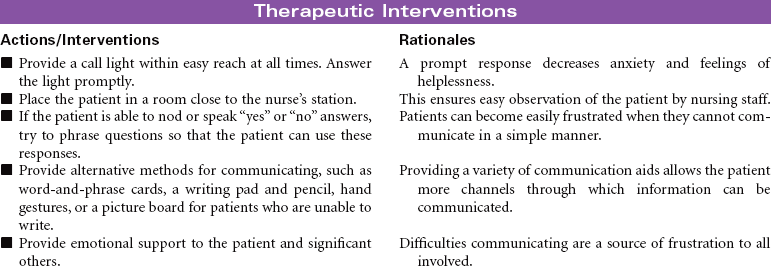
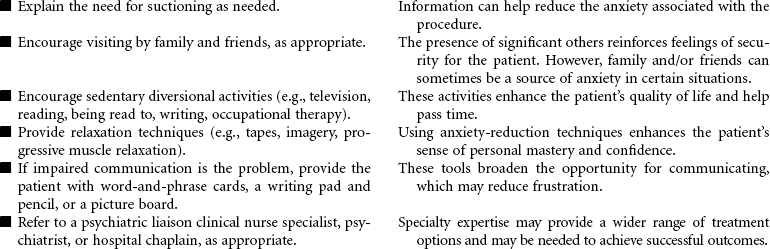
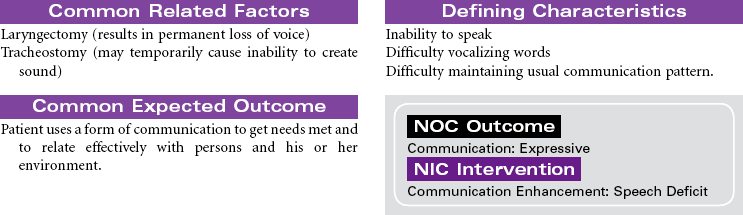
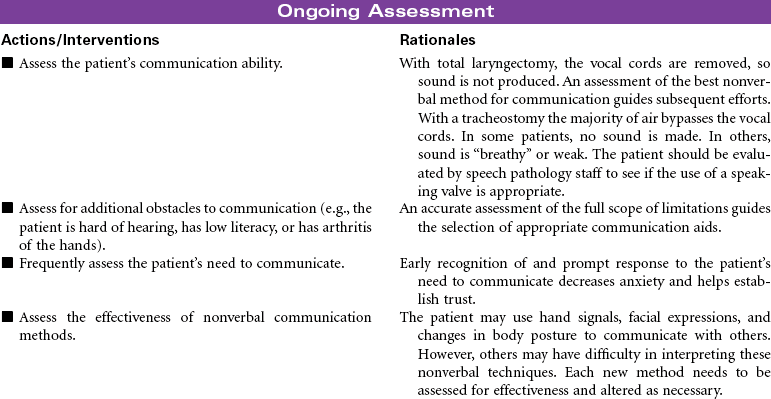
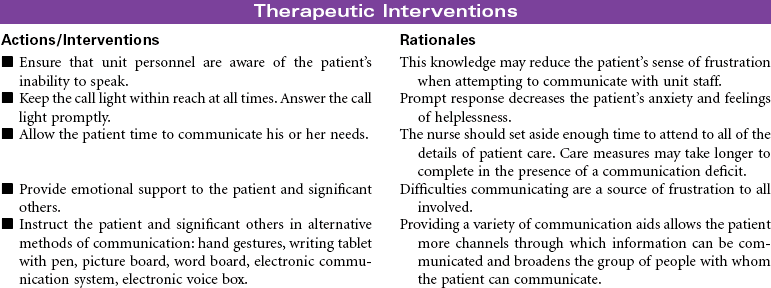
Impaired verbal communication, p. 43
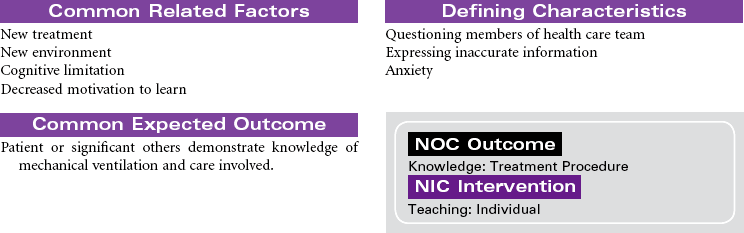
Mechanical ventilation, p. 461
Powerlessness, p. 155
Risk for impaired skin integrity, p. 178

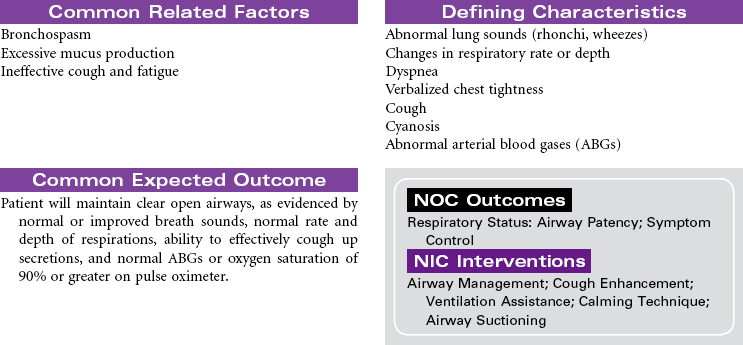
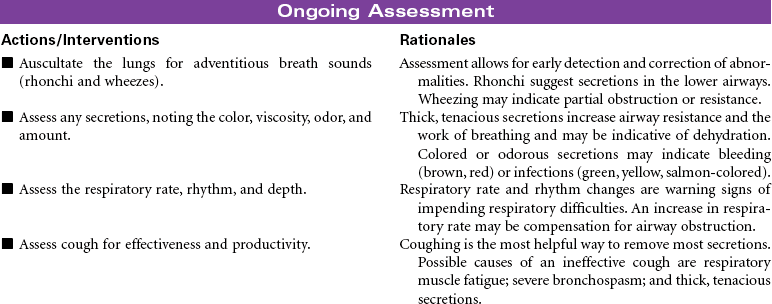
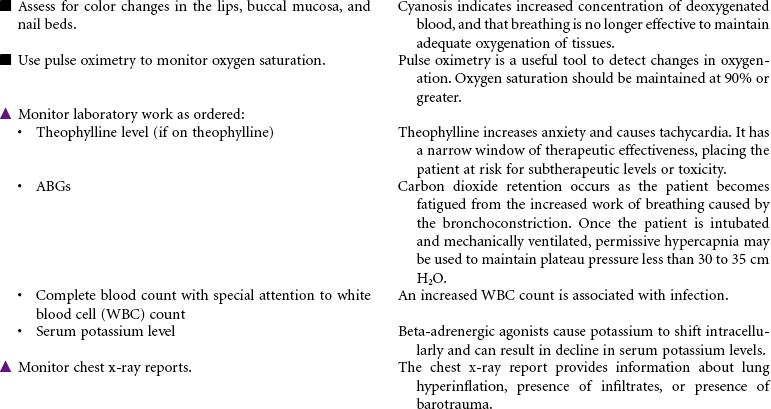
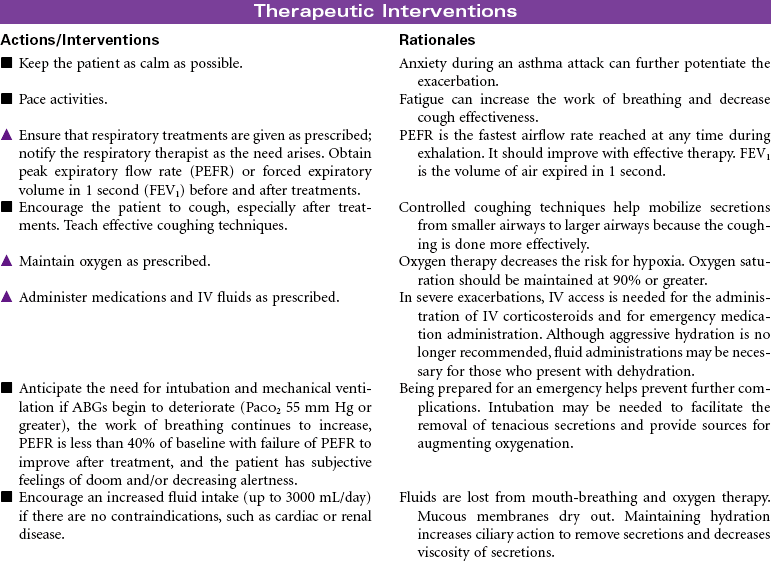
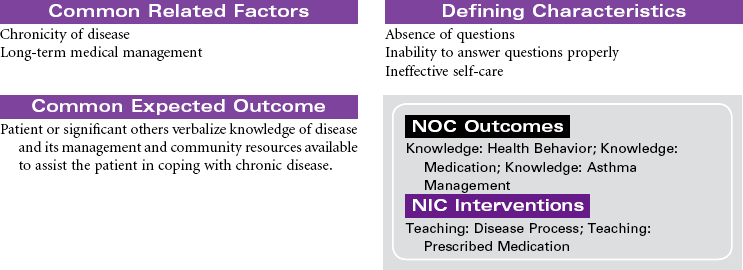
Asthma
Bronchial Asthma; Status Asthmaticus
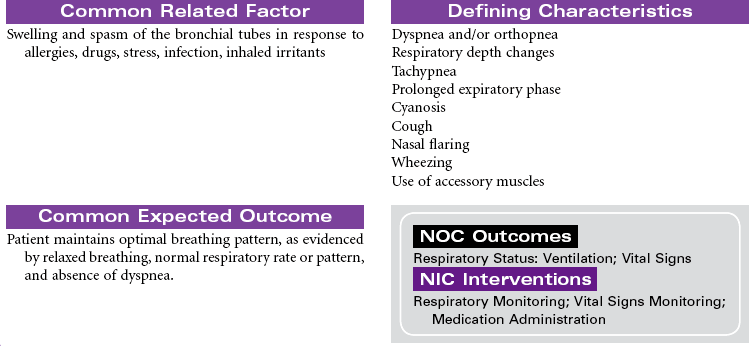
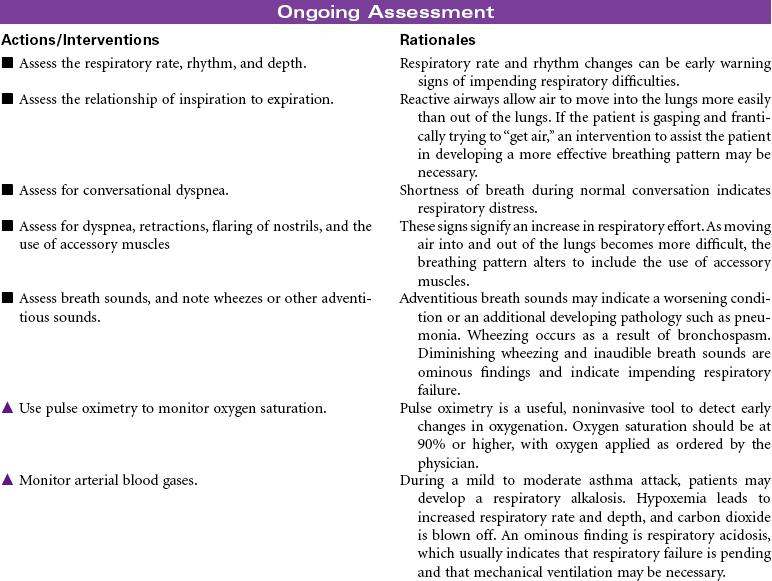
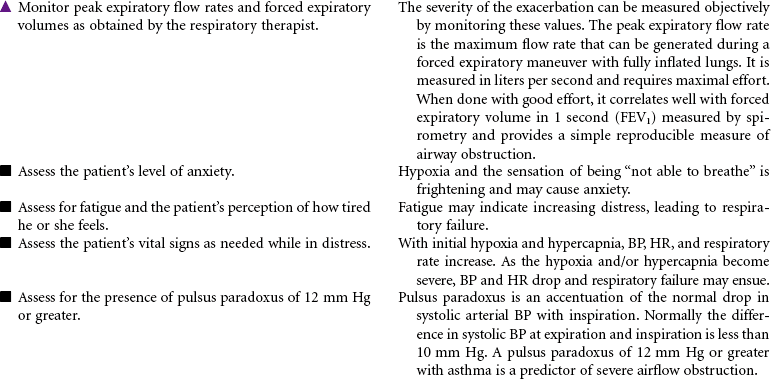
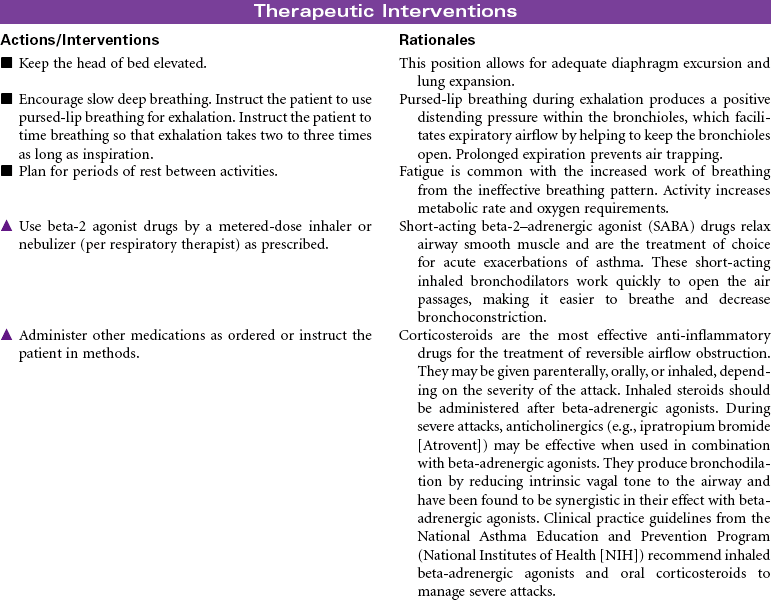
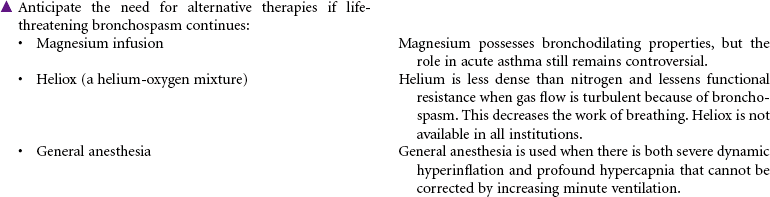
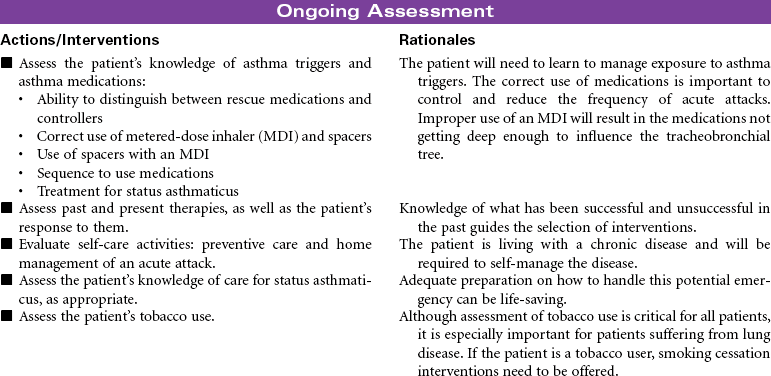
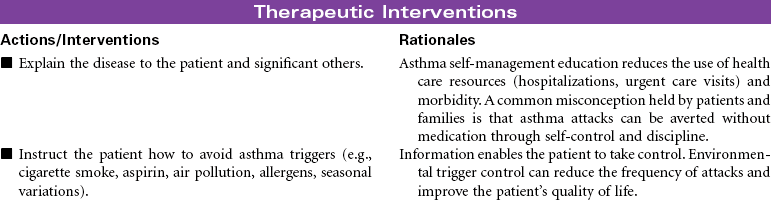
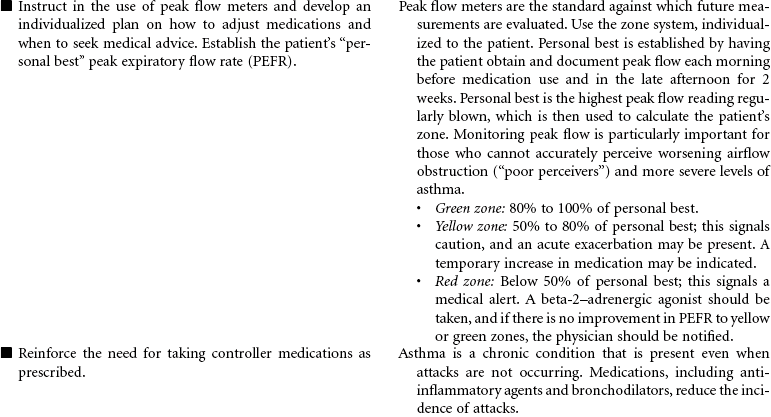
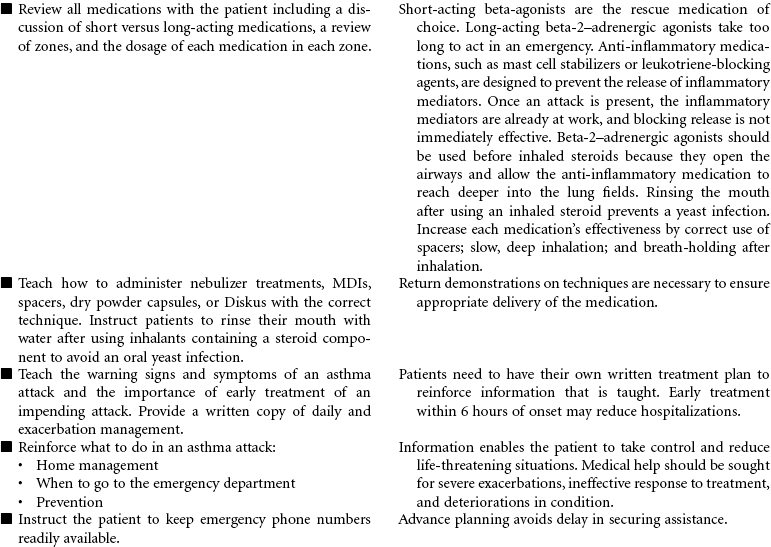
Asthma is a chronic inflammatory disorder that is characterized by airflow obstruction. This inflammatory response causes bronchoconstriction, increased mucus production, and hyperresponsiveness of the airways to a variety of stimuli. Although the stimuli for this exaggerated bronchoconstrictive response are individually defined, respiratory infection, cold weather, physical exertion, some medications, and allergens are common triggers. When a hypersensitive individual is exposed to a trigger, a rapid inflammatory response with subsequent bronchospasm occurs. Proinflammatory cells, primarily mast cells, signaled by immunoglobulin E (IgE), release inflammatory mediators that produce swelling and spasm of the bronchial tubes. This causes adventitious sounds (wheezing), coughing, increased mucus production, and feelings of “not being able to breathe” (dyspnea). Eosinophils and neutrophils rush to the area, and additional cytokines are released, some of which are long acting and result in epithelial damage, late-phase airway edema, continued mucus hypersecretion, and additional hyperresponsiveness of the bronchial smooth muscle. Reversal of the airflow obstruction usually occurs spontaneously or with treatment. Status asthmaticus occurs when the asthma attack is refractory to the usual treatment, with clinical manifestations that are more severe, prolonged, and life threatening. With repeated attacks, remodeling of the airway occurs through hypertrophy and hyperplasia of normal tissues.
Although this care plan focuses on acute care in the hospital setting, current thinking is to prevent the hypersensitivity reaction and thus keep airway remodeling at a minimum. For this reason, an asthma plan individualized for each patient and for optimal outpatient management is emphasized.
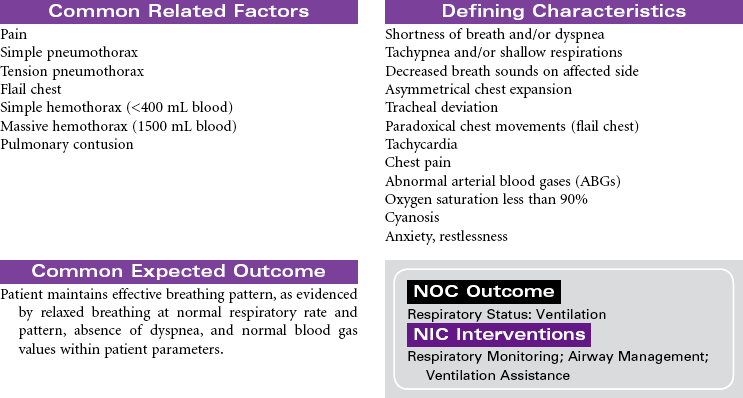
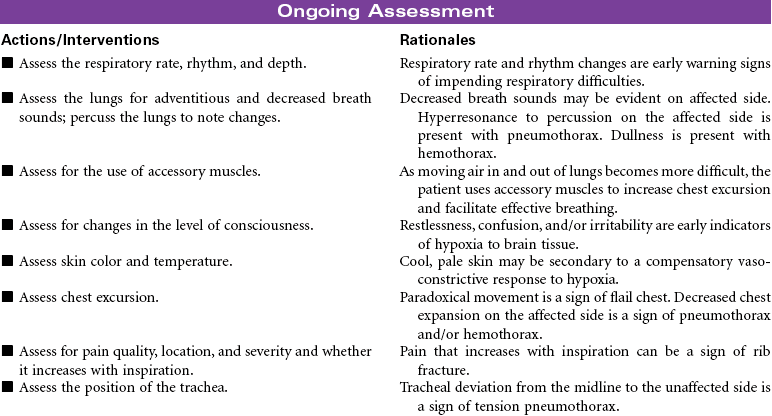
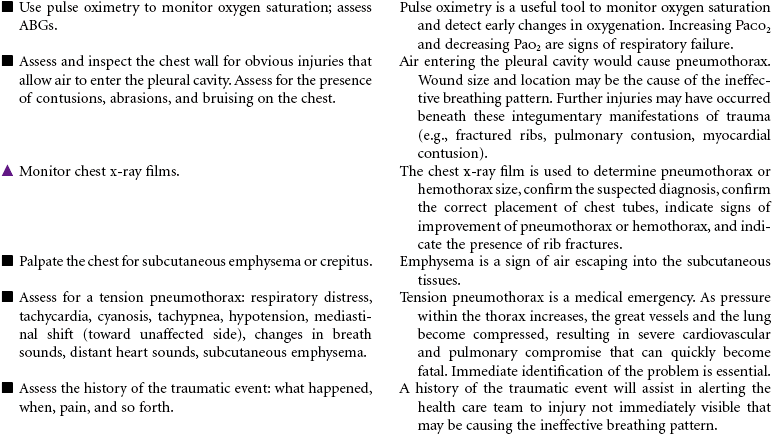
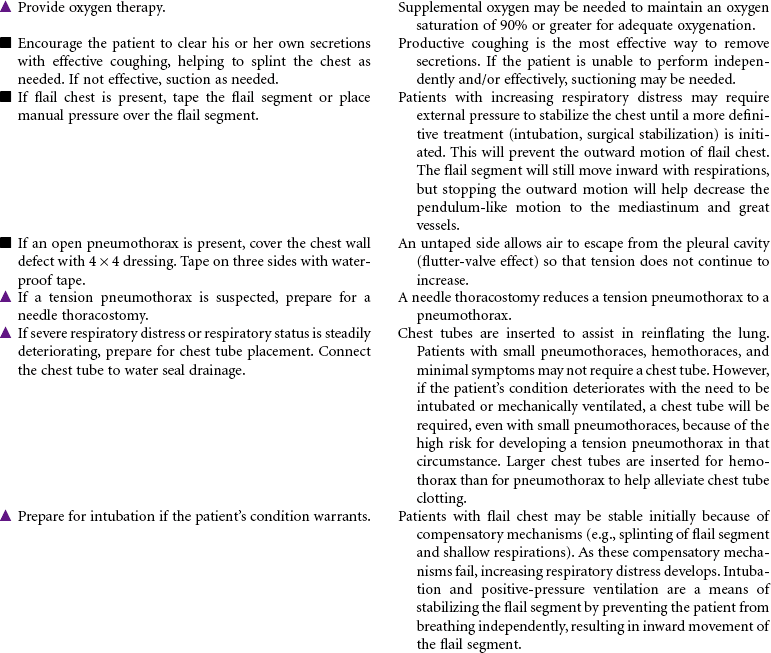
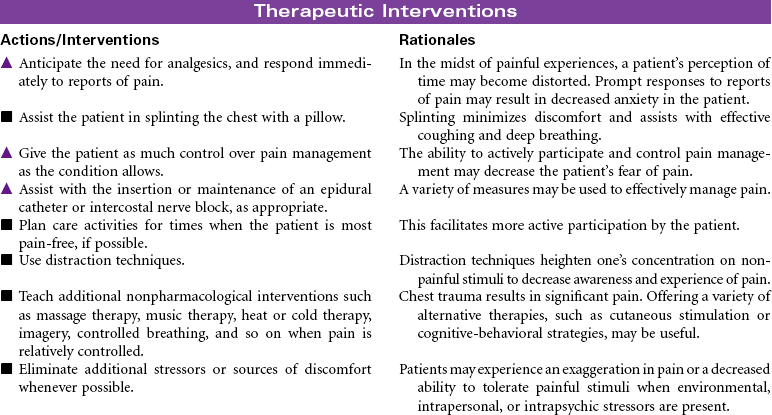
Chest Trauma
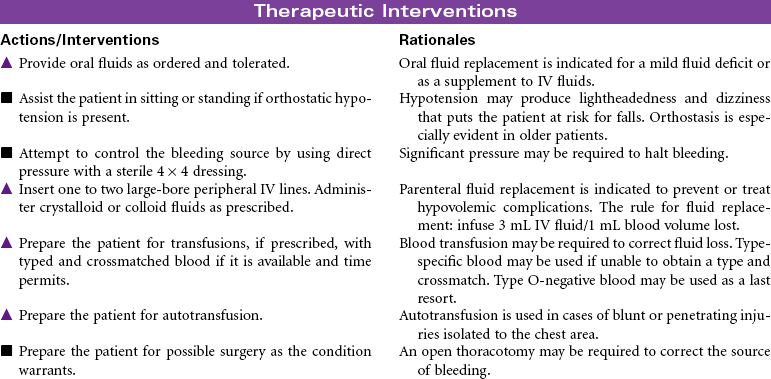
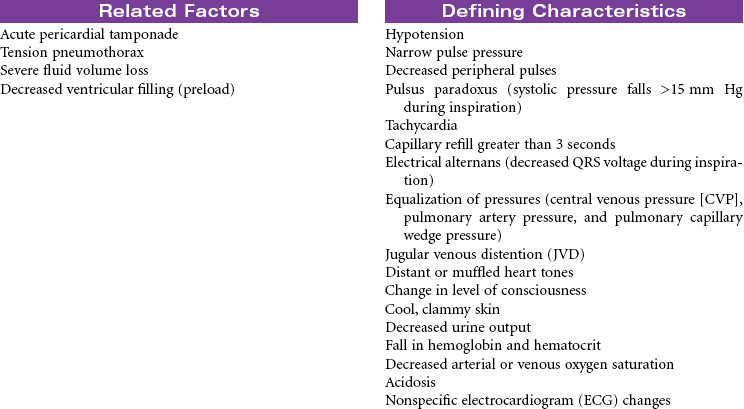
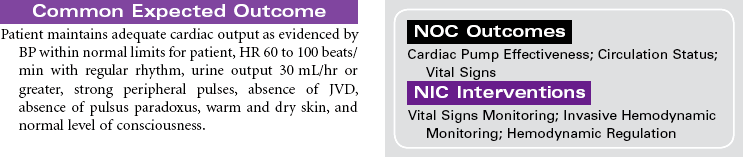
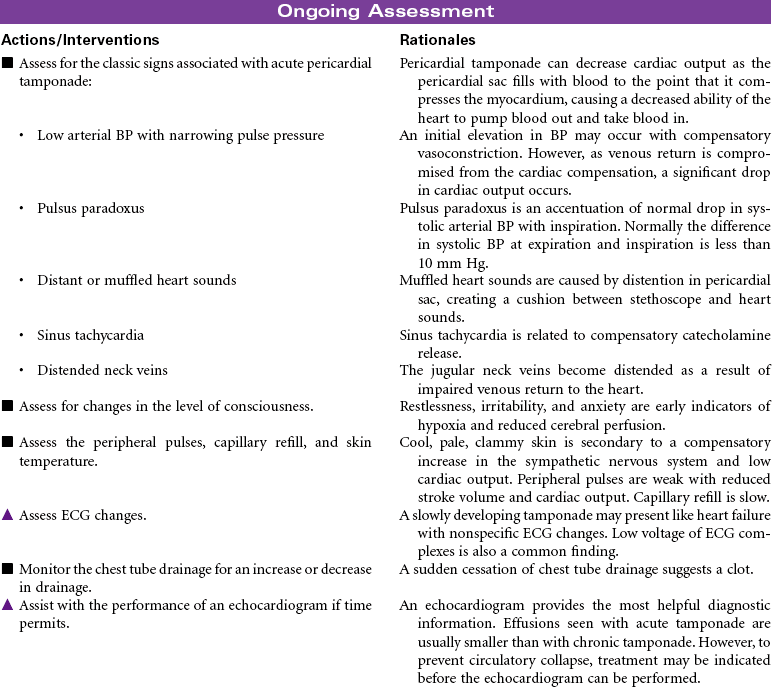
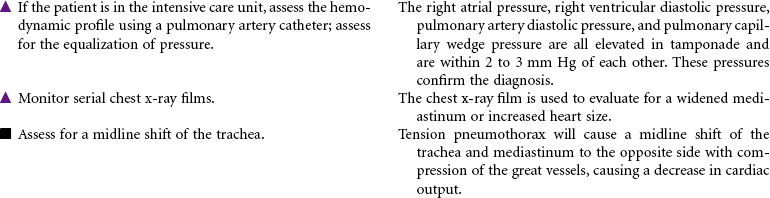
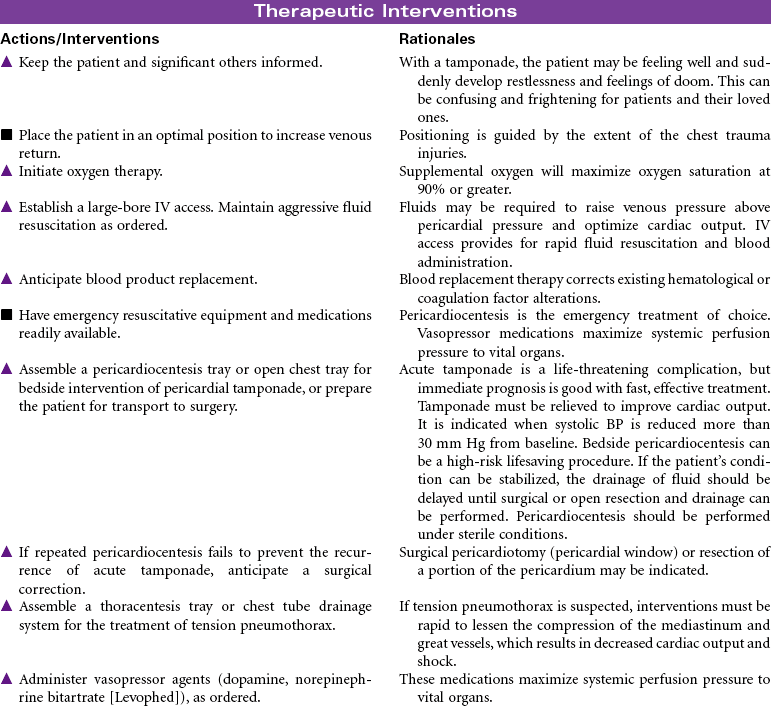
Pneumothorax; Tension Pneumothorax; Flail Chest; Fractured Ribs; Pulmonary Contusion; Hemothorax; Myocardial Contusion; Cardiac Tamponade
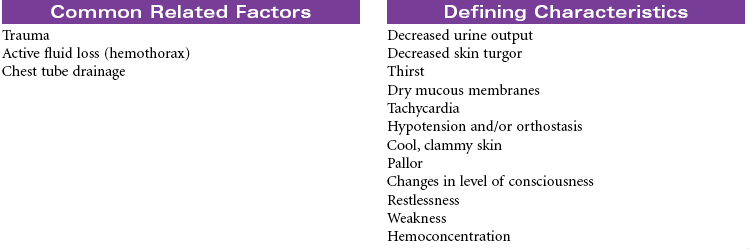
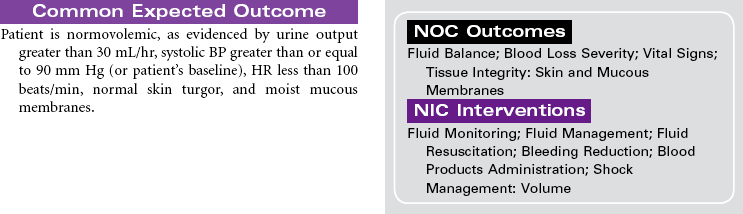
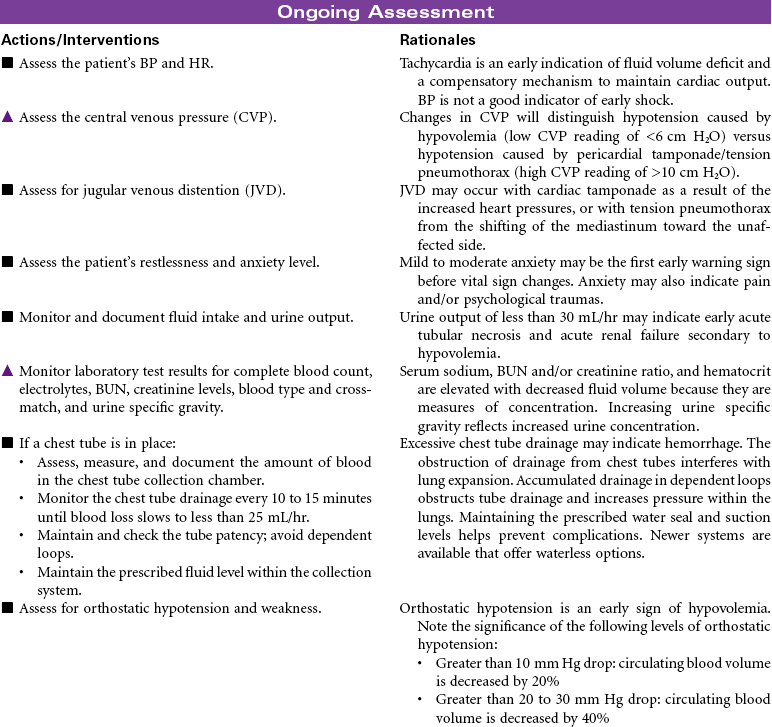
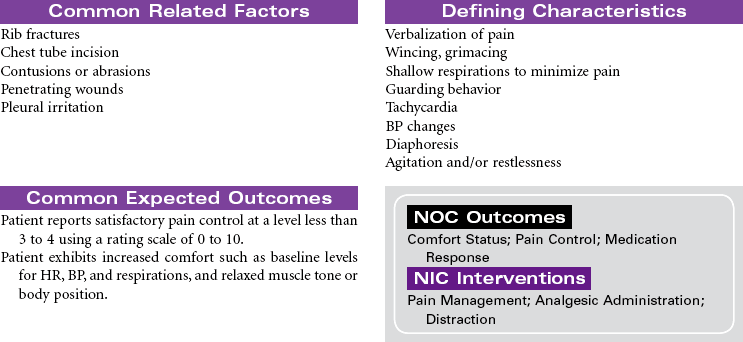
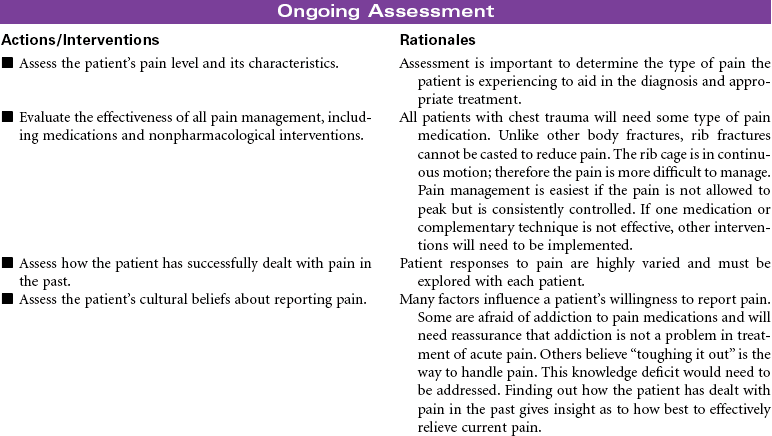
Chest trauma is a blunt or penetrating injury of the thoracic cavity that can result in a potentially life-threatening situation secondary to hemothorax, pneumothorax, tension pneumothorax, flail chest, pulmonary contusion, myocardial contusion, and/or cardiac tamponade. This care plan focuses on acute care in the hospital setting.

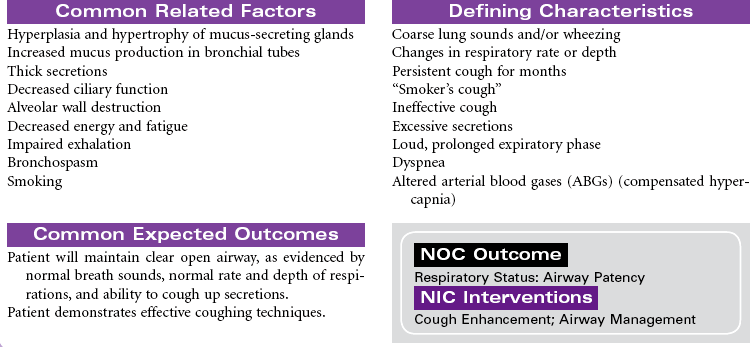
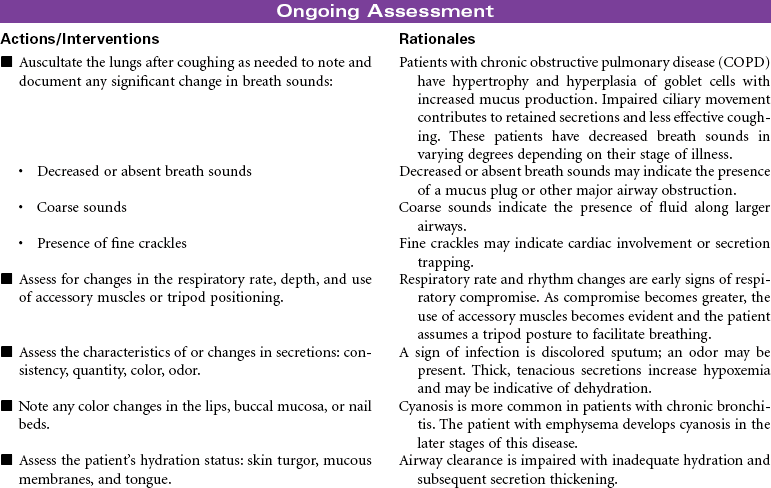
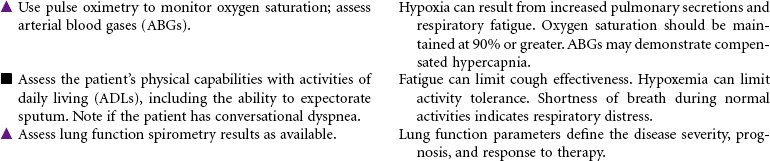
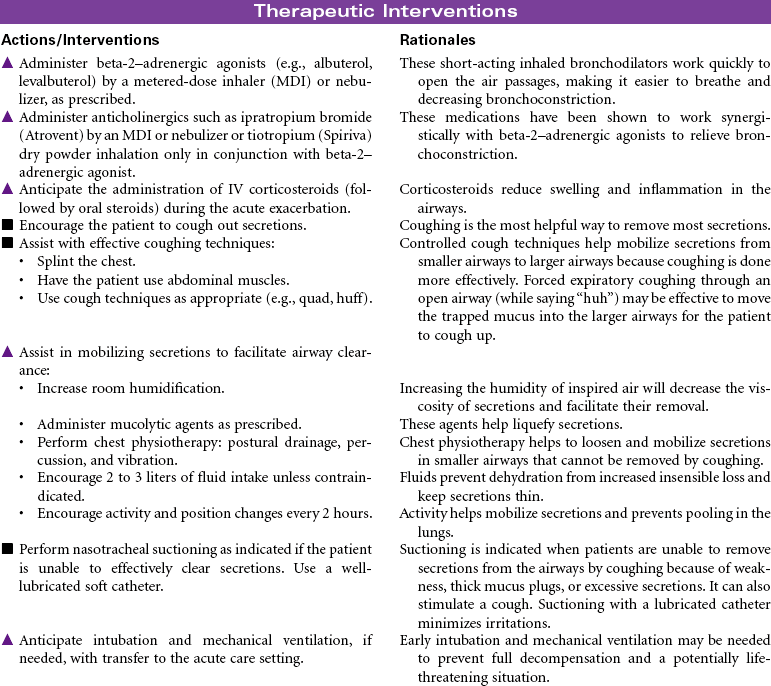
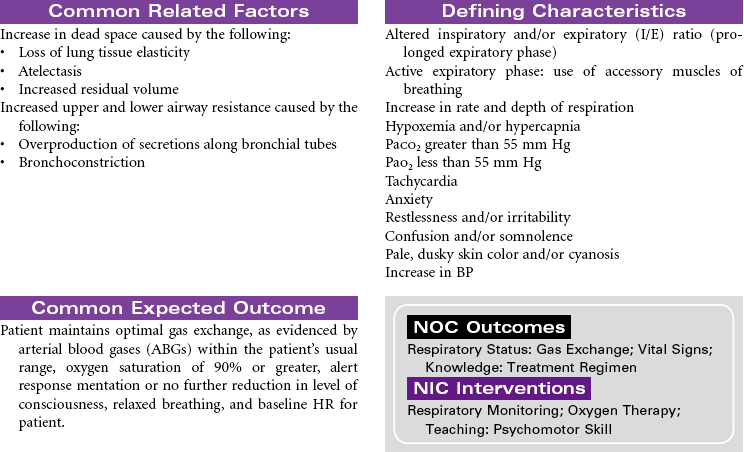
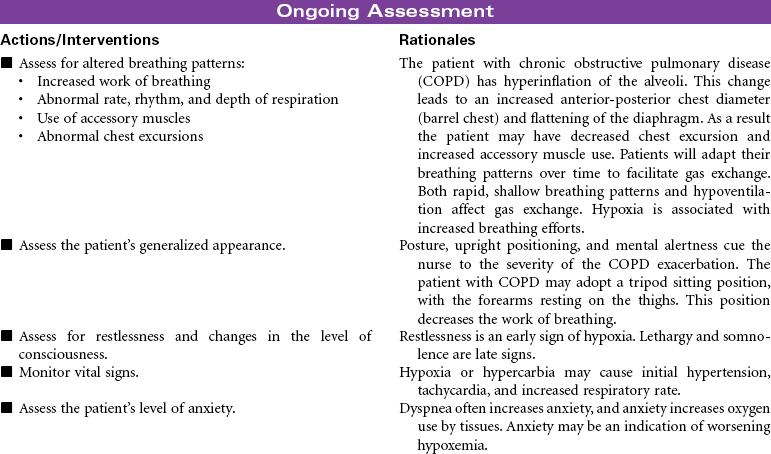
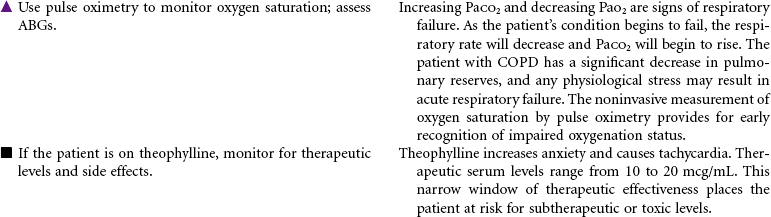
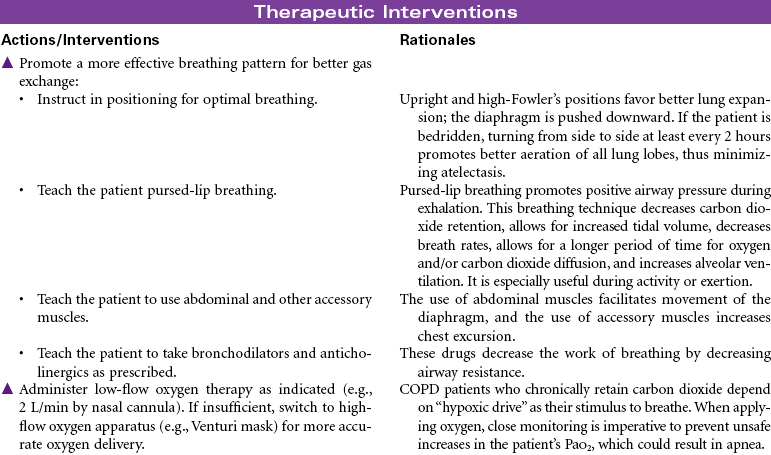
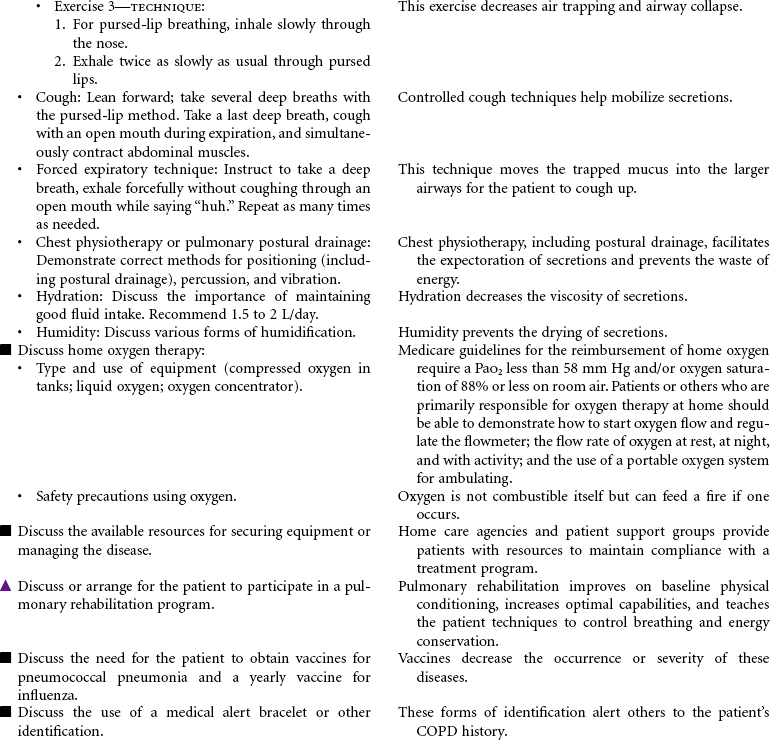
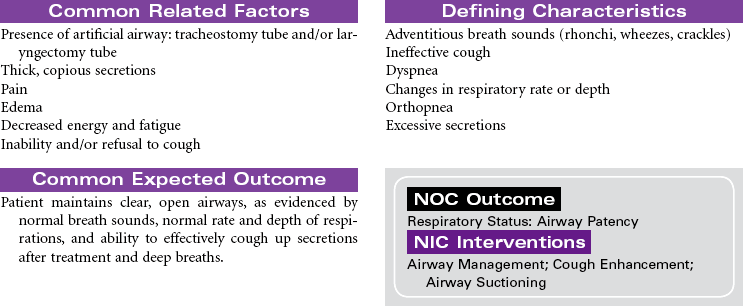
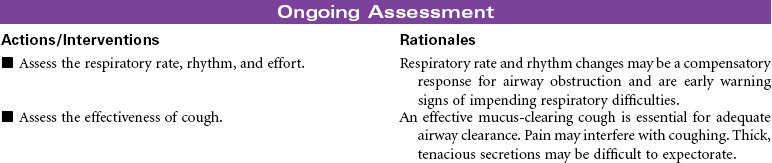
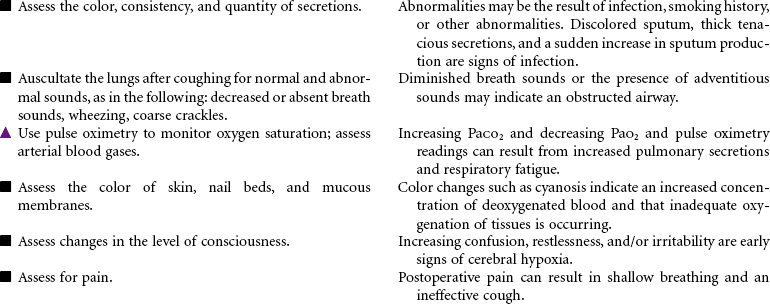
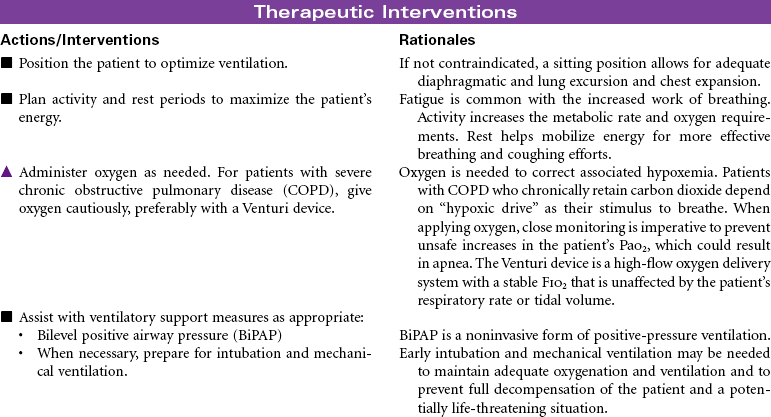
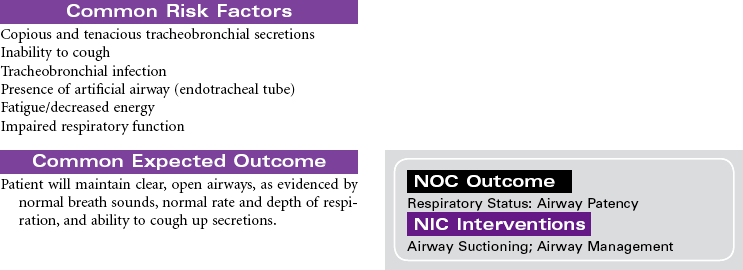
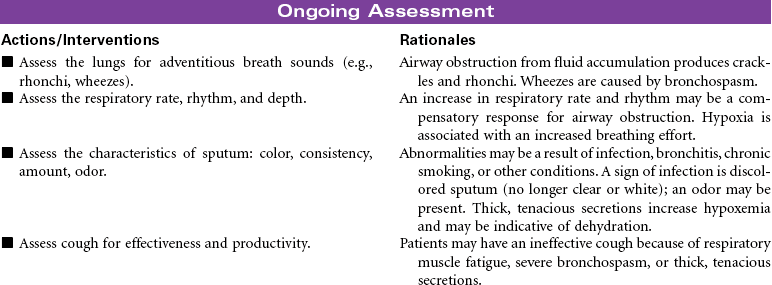
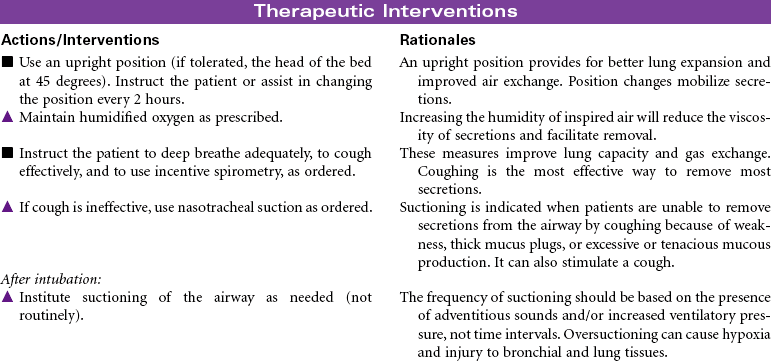
Chronic Obstructive Pulmonary Disease
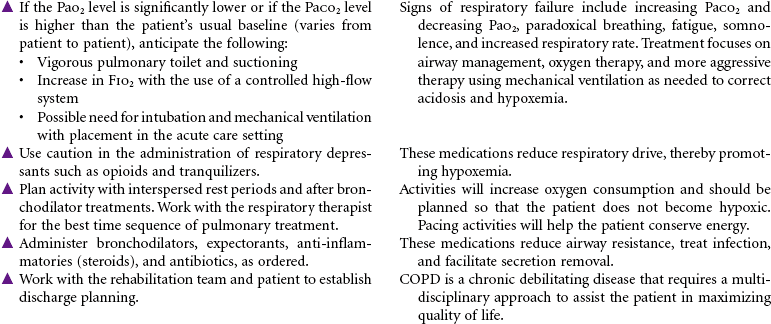
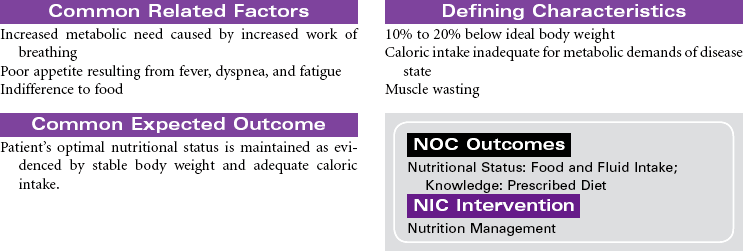
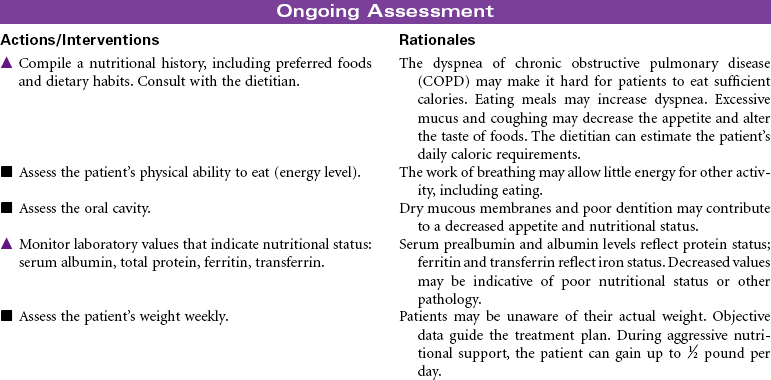
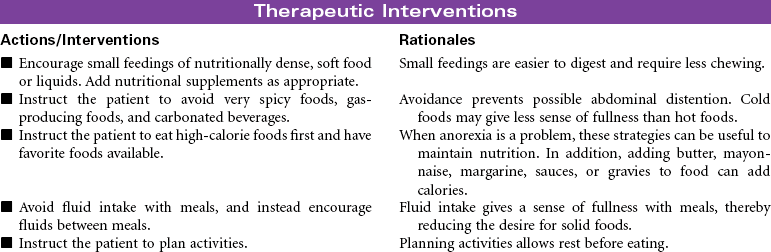
Chronic obstructive pulmonary disease (COPD) refers to a group of diseases, including chronic bronchitis and emphysema, that cause a reduction in expiratory outflow. It is usually a slow, progressive, debilitating disease, affecting those with a history of heavy tobacco abuse and prolonged exposure to respiratory system irritants such as air pollution, noxious gases, and repeated upper respiratory tract infections. It is also regarded as the most common cause of alveolar hypoventilation with associated hypoxemia, chronic hypercapnia, and compensated acidosis. This care plan focuses on exacerbation of COPD in the acute care setting and chronic care in the ambulatory setting or chronic care facility.
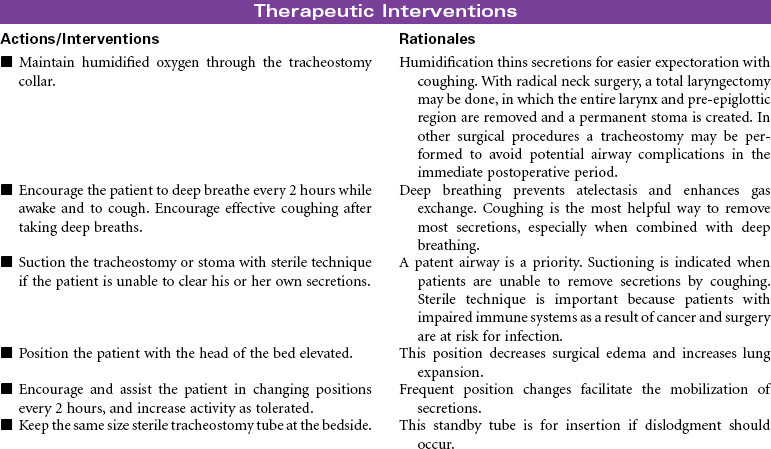
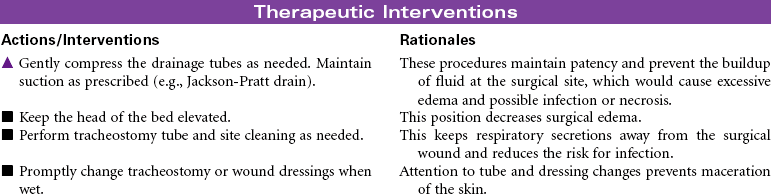
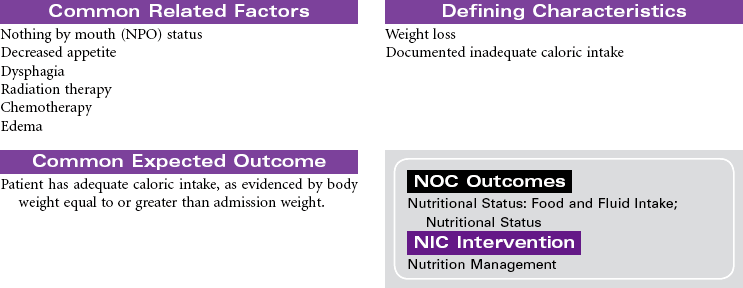
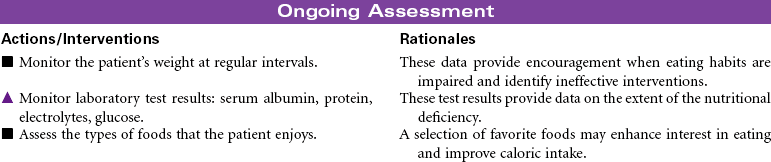
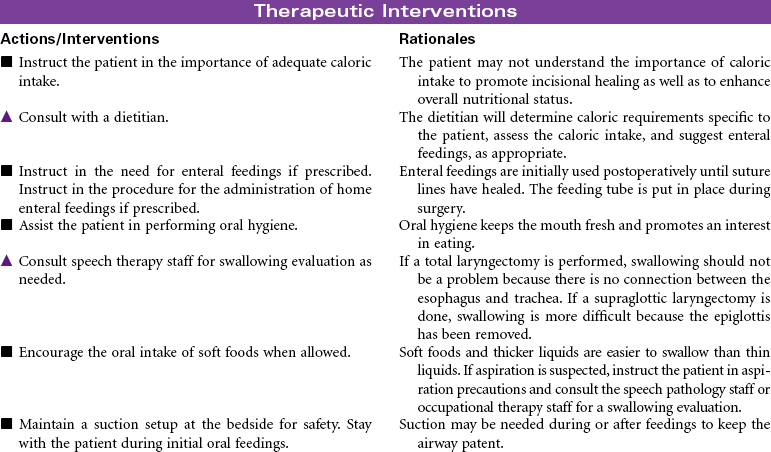
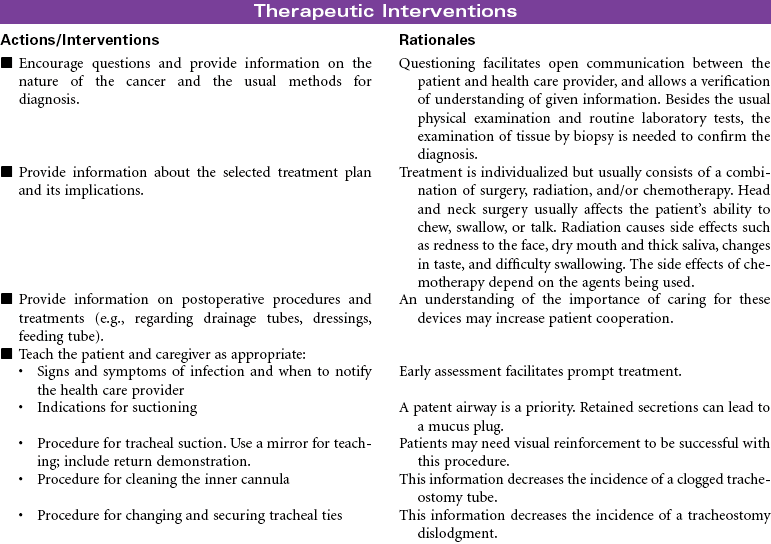
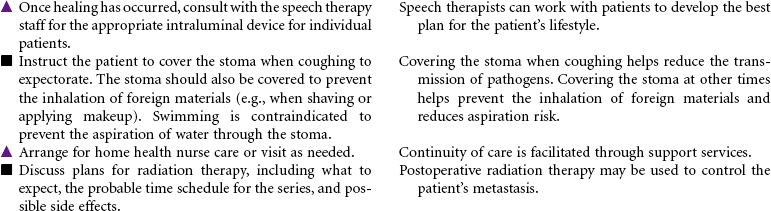
Head and Neck Cancer: Surgical Approaches
Radical Neck Surgery; Laryngectomy
Head and neck cancer accounts for approximately 3% of new cancers in the United States annually but is much more prevalent in developing nations. Ninety percent of head and neck cancers are squamous cell carcinomas, with the remaining 10% divided among lymphomas and minor salivary gland tumors. The primary risk factors for head and neck cancer are tobacco and alcohol. Although alcohol does not appear to be risk factor in and of itself, it has proven to have a synergistic effect with tobacco. New research is strongly linking human papillomavirus (HPV) infection to the development of head and neck cancer, specifically in the oral cavity and tonsil. This will be an area of continuing study over the next few years to evaluate the potential use of HPV vaccines. Head and neck cancer is often diagnosed at later stages when a patient presents with a mass in the neck, hoarseness, or respiratory distress. A computed tomography (CT) scan of the head and neck, along with a fine-needle biopsy, are the most common diagnostic tools. Treatment consists of combined modalities, such as surgery, radiation, and/or chemotherapy, in hopes of achieving the best outcome possible. The focus of this care plan is the surgical management of patients with head and neck cancer.




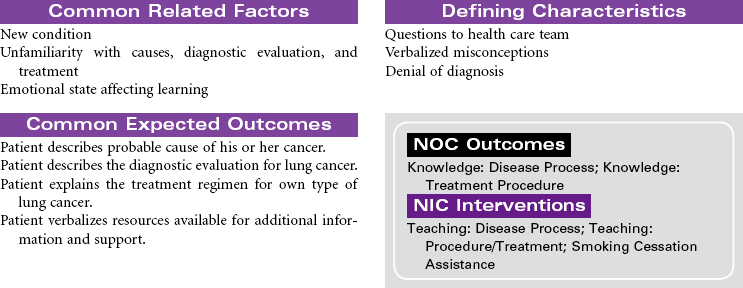
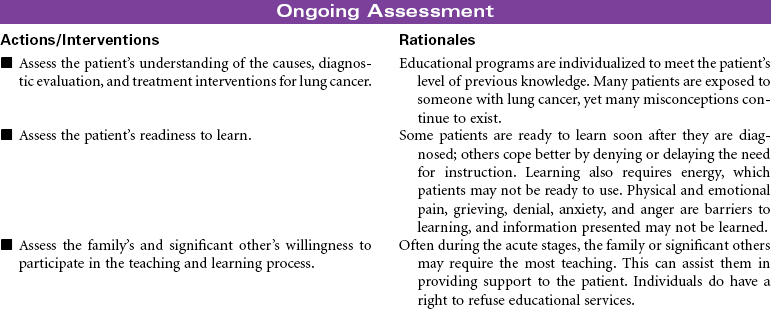
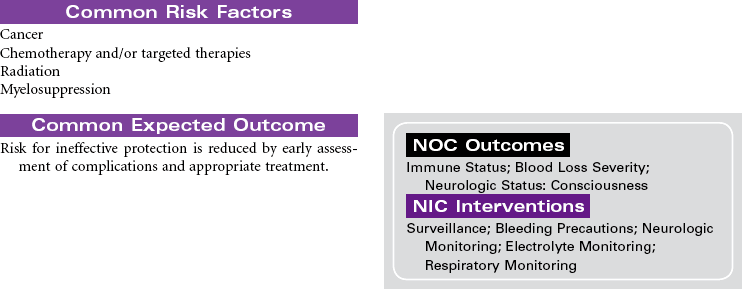
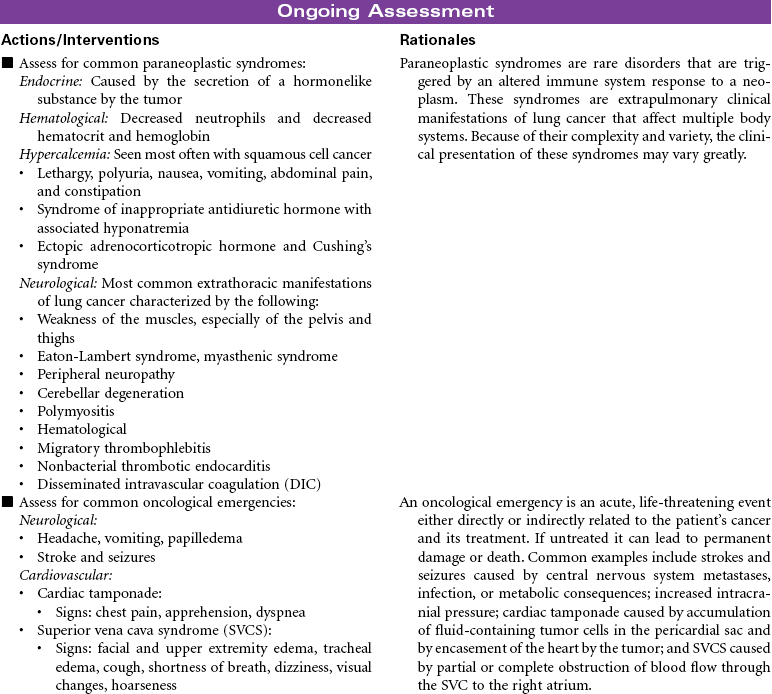
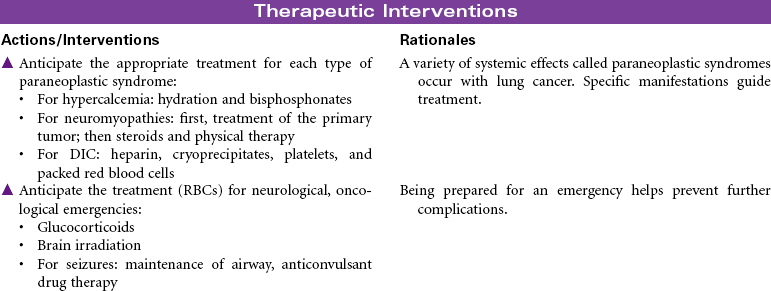
Lung Cancer
Squamous Cell; Small Cell; Non–Small Cell; Adenocarcinoma; Large Cell Tumors
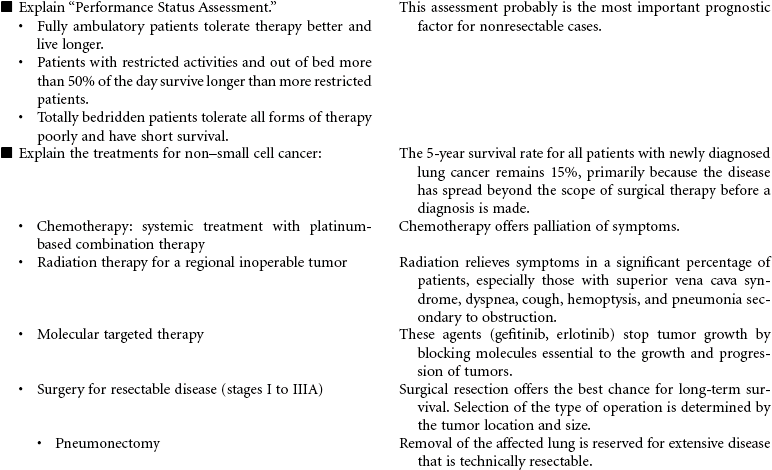
Lung cancer is the second most commonly occurring cancer among men and women, and despite all available therapies, lung cancer remains the leading cancer-related cause of death for men and women. It is one of the most preventable cancers. The American Cancer Society estimates that more than 90% of all lung cancers are related to cigarette smoking.
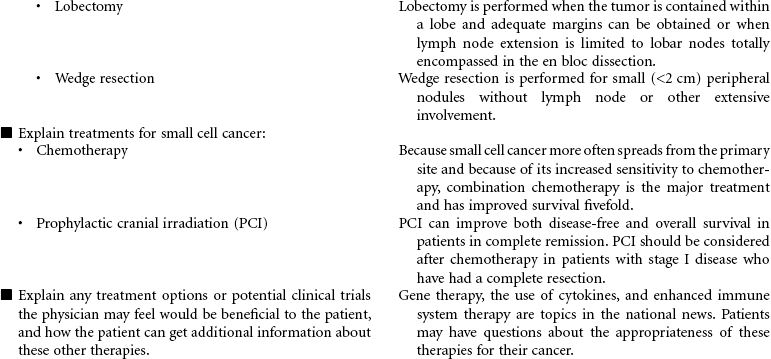
Lung cancer is divided into two major cell types: non–small cell lung cancer (NSCLC) and small cell lung cancer (SCLC). NSCLC accounts for more than 80% of cases, with adenocarcinomas being most common (approximately 40%), then squamous cell carcinoma, large cell carcinoma, and mixed cell tumors. SCLC is biologically and clinically distinct from the other histological types and accounts for approximately 15% of cases. The diagnosis and stage of lung cancer subtype are critical to the determination of appropriate treatment. NSCLC can be surgically resected in the early stages and treated with chemotherapy and/or radiation therapy based on stage. SCLC cannot be surgically resected and is always treated with chemotherapy and radiation therapy.
Prevention is essential. Providing smoke-free environments, testing for radon, and providing educational programs remain the most powerful interventions. Smoking cessation interventions are a part of all care plans for patients who smoke. Although there are currently no effective screening tests for lung cancer, it is hoped that genetic markers will soon be available to help identify people at high risk for developing cancer. Other promising research focuses on making the immune system and chemical messengers more effective in responding to early cellular changes of lung cancer. Currently work is being completed in the development of chemical messengers that control and stop abnormal cell growth (antioncogene therapy), the use of monoclonal antibodies that recognize and destroy only abnormal lung cells, and stimulation of the immune system by learning to control cytokines such as interleukin-2 and the interferons. In the future, systemic treatment (chemotherapy and targeted therapy) may be selected based on patients’ cellular mutation status.
This care plan focuses on the educational aspects of lung cancer.
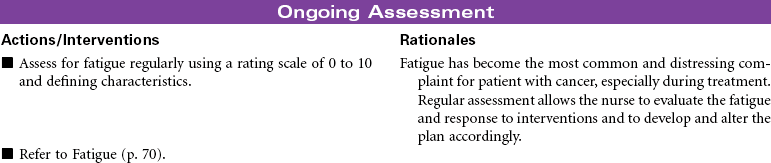
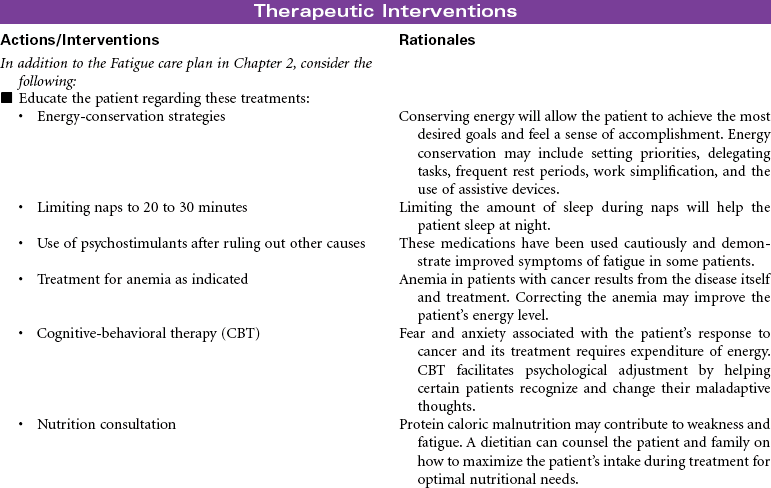
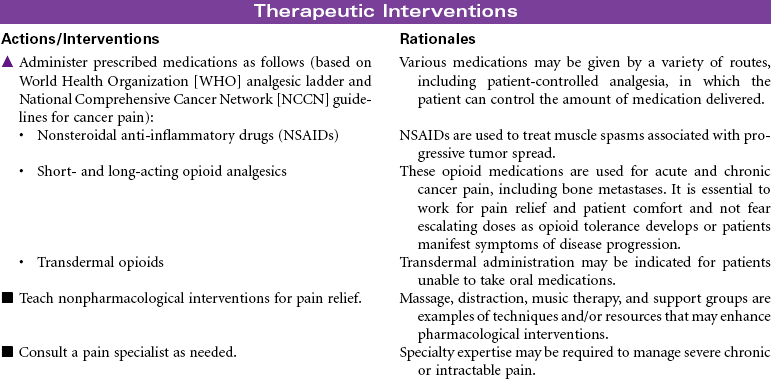
 Cancer-Related Fatigue
Cancer-Related Fatigue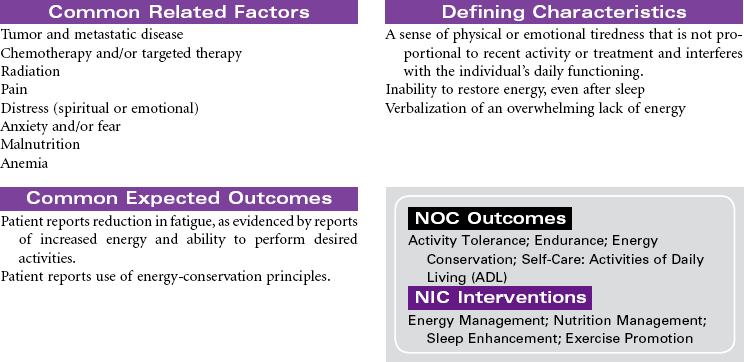
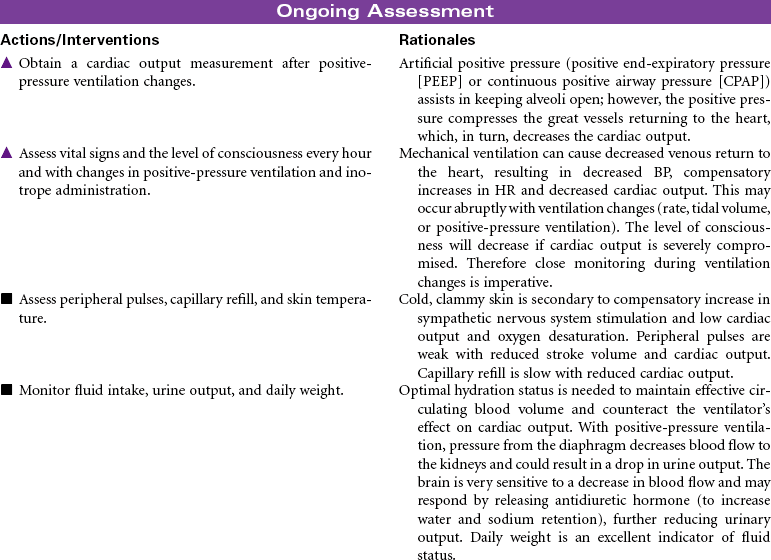
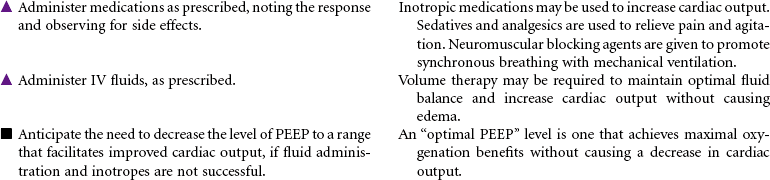
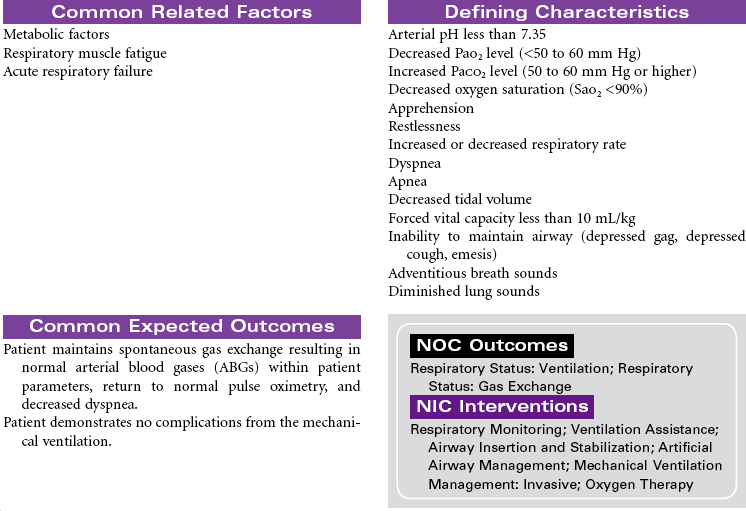
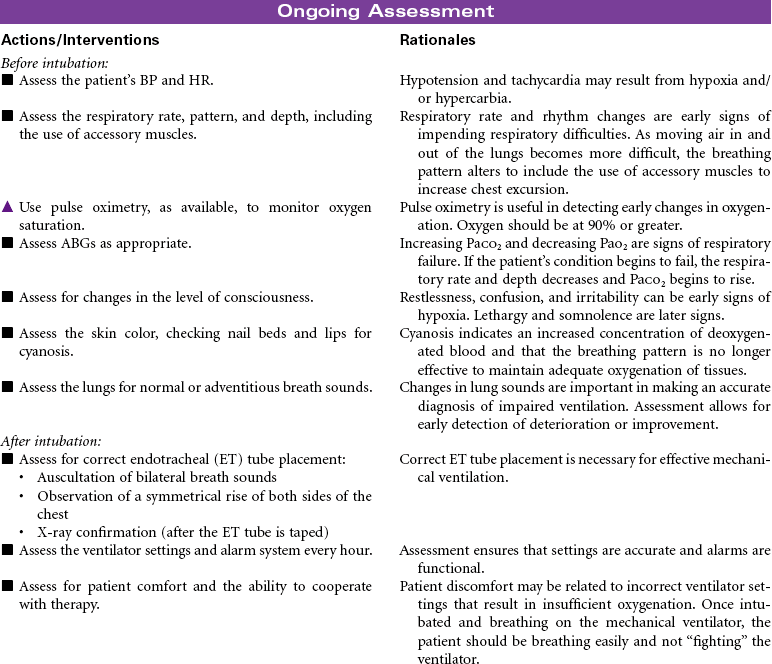
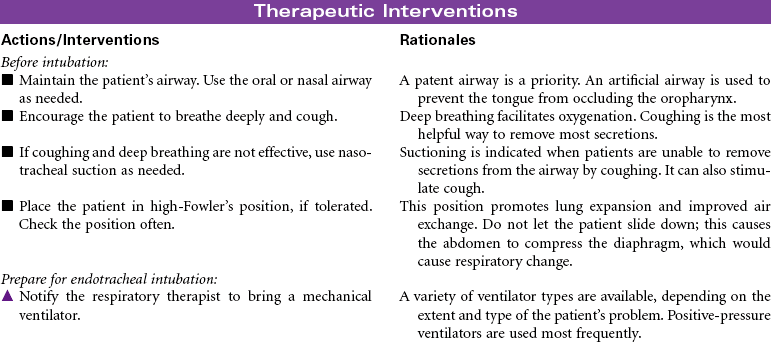
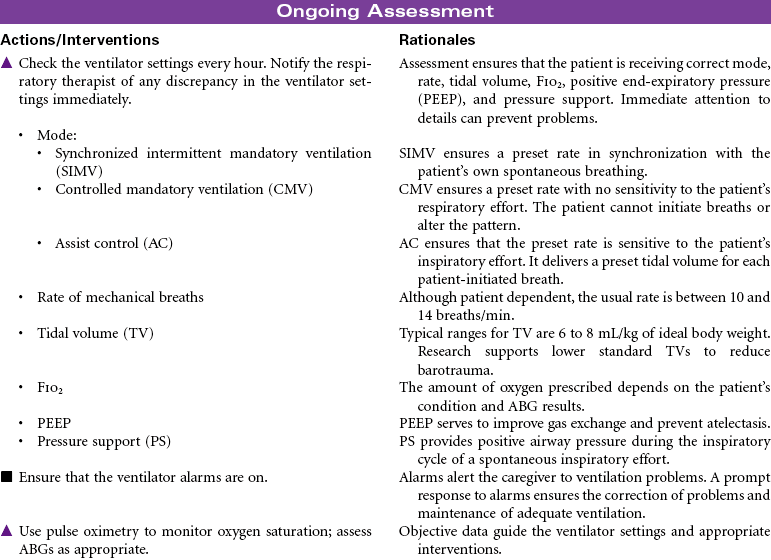
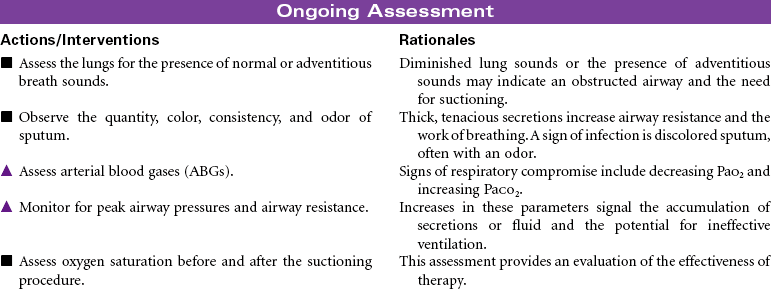
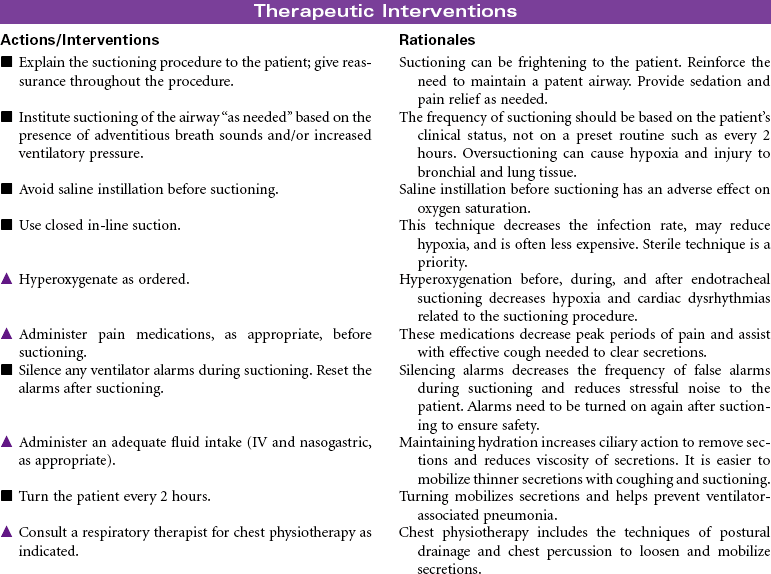
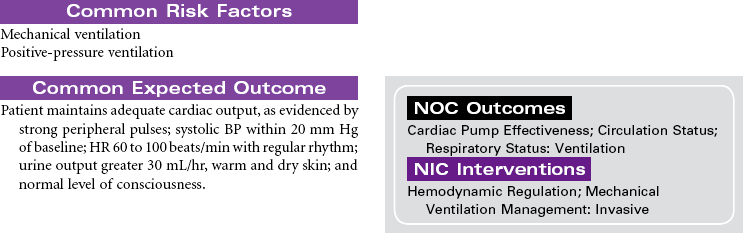
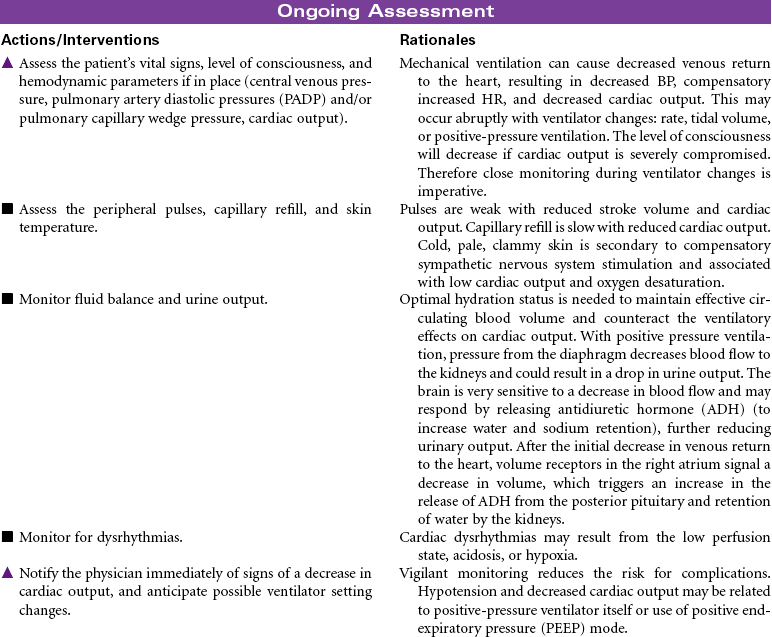
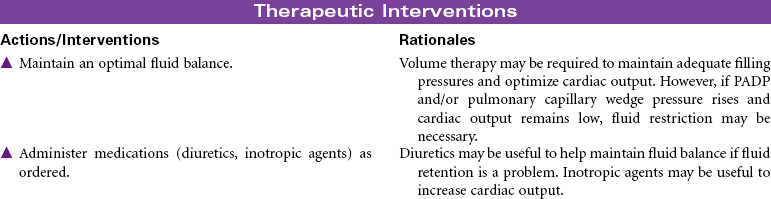
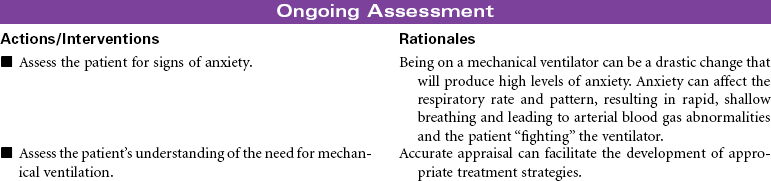
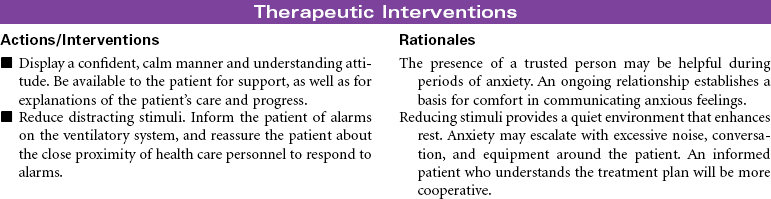
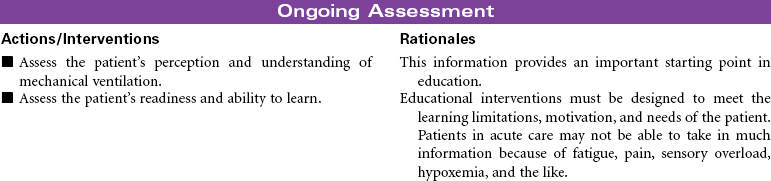
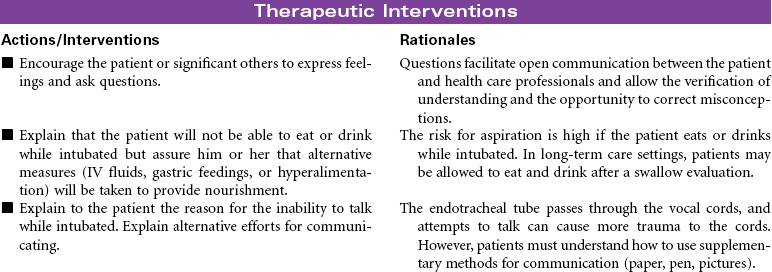
Mechanical Ventilation
Ventilator; Respirator; Endotracheal Tube; Intubation; Ventilator-Associated Pneumonia
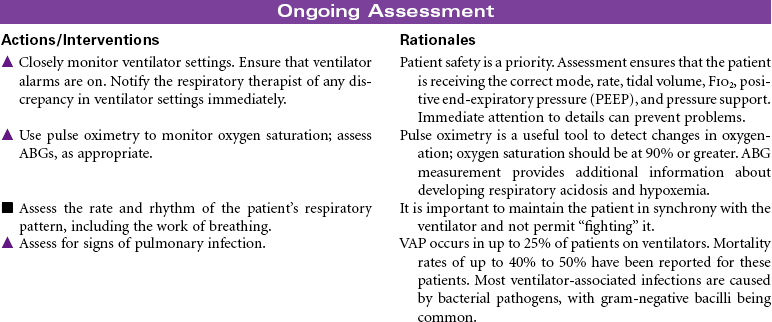
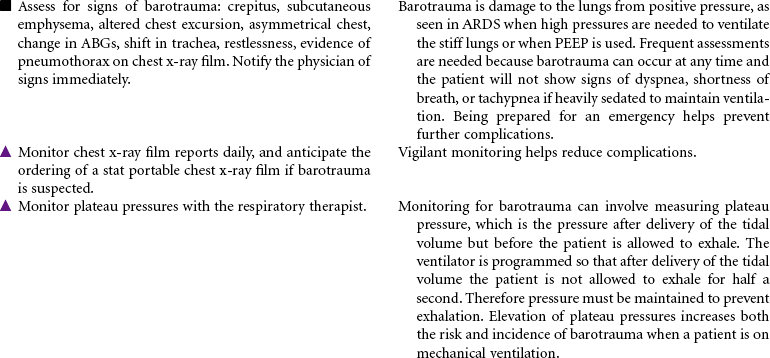
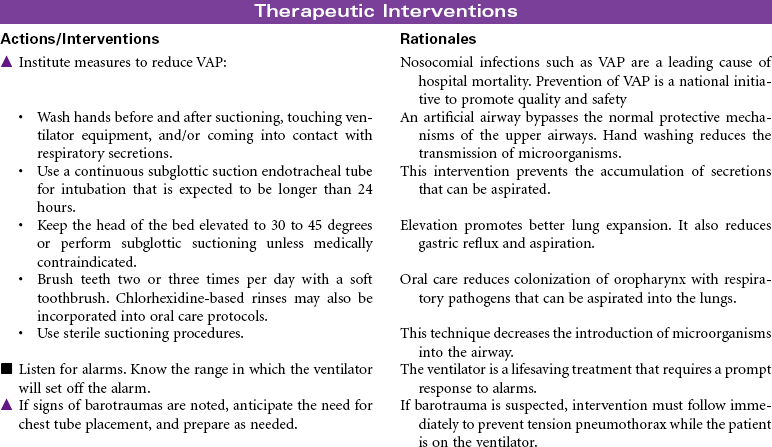
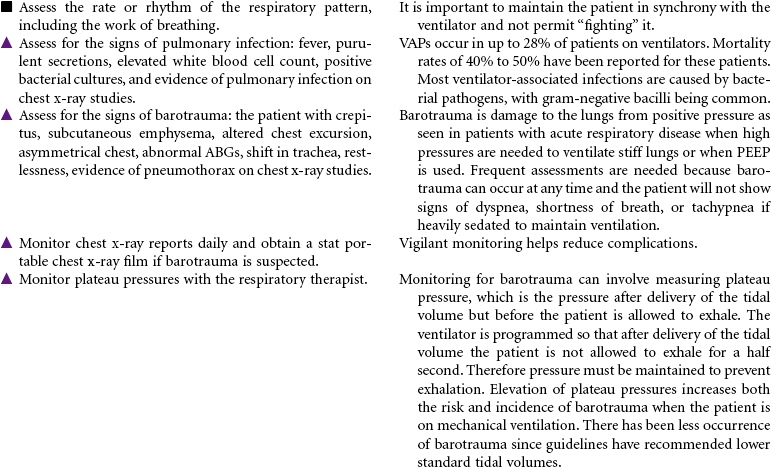
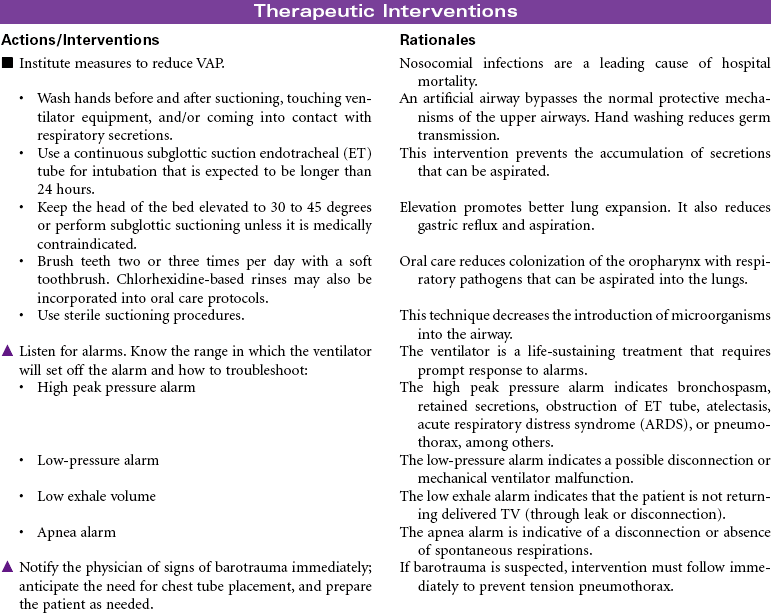
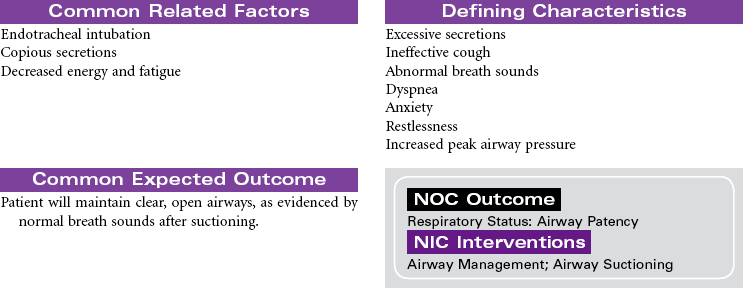
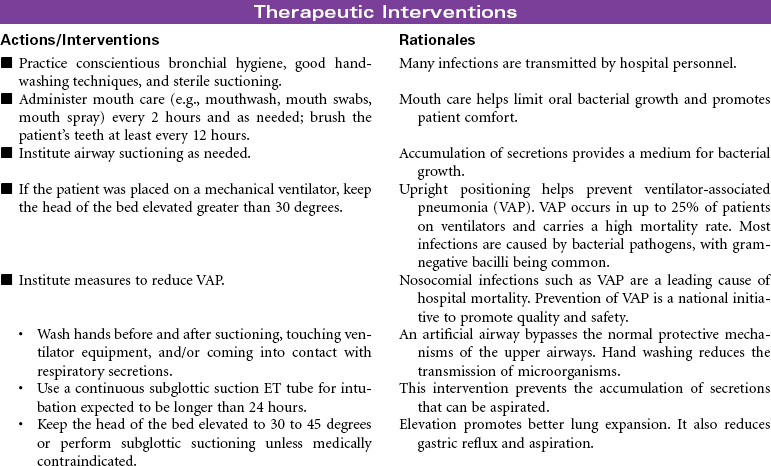
Mechanical ventilation can be a temporary or chronic lifesaving therapy. Its purpose is to maintain adequate ventilation by delivering preset concentrations of oxygen at an adequate tidal volume while reducing the work of breathing. The patient who requires mechanical ventilation must have an artificial airway (endotracheal tube) or tracheostomy. It is used most often in patients with hypoxemia and alveolar hypoventilation. Although the mechanical ventilator will facilitate movement of gases into and out of the pulmonary system (ventilation), it cannot ensure gas exchange at the pulmonary and tissues levels (respiration). It provides either partial or total ventilatory support for patients with respiratory failure. Mechanical ventilation may be used short-term in the acute care setting (e.g., after surgery; during general anesthesia) or long-term in the subacute, rehabilitation, or home care setting. Ventilator-associated pneumonia (VAP) is a significant nosocomial infection that is associated with endotracheal intubation and mechanical ventilation. Prevention of VAP is a primary focus of the 100,000 Lives Campaign to promote quality care and patient safety. This care plan focuses on patient care in a hospital setting.
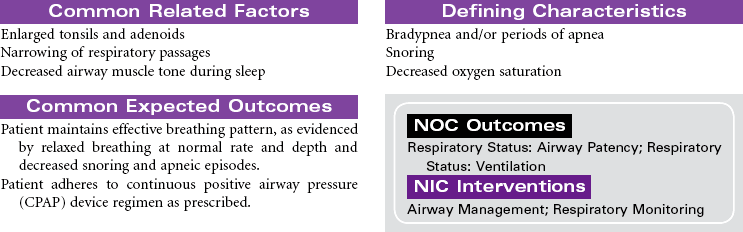
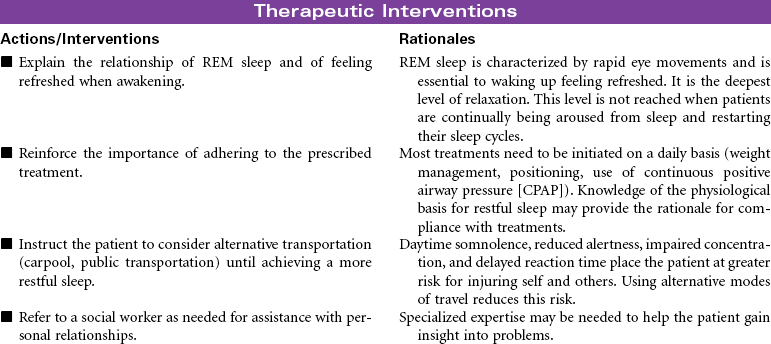
Obstructive Sleep Apnea
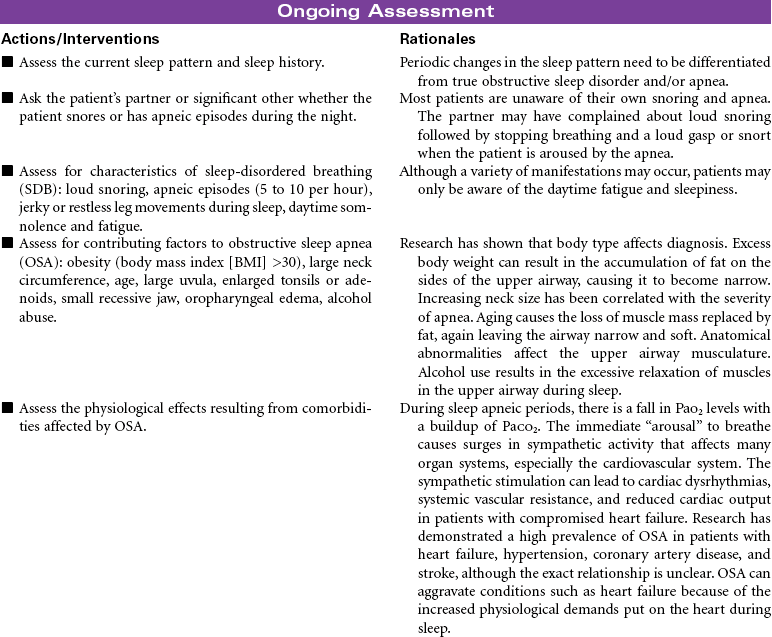
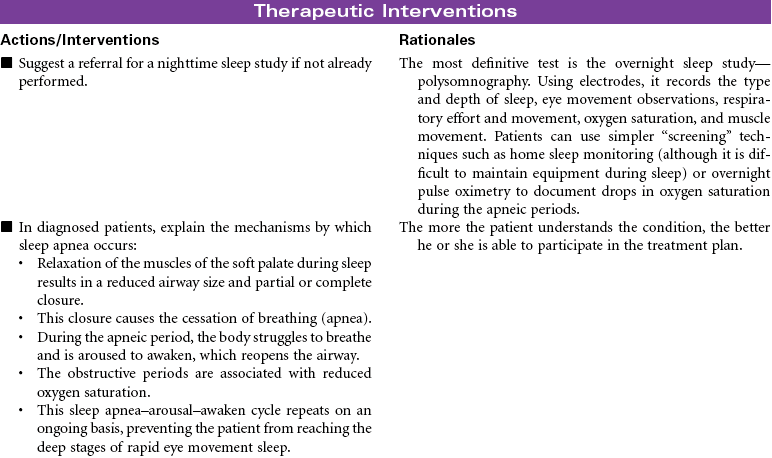
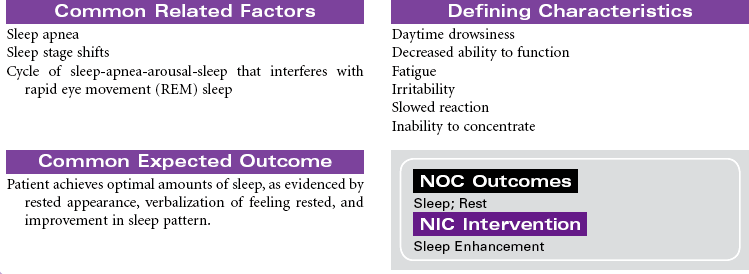
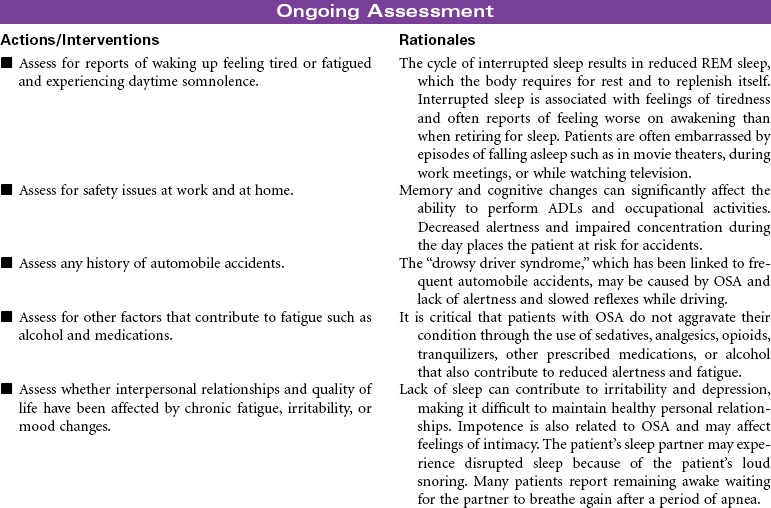
Sleep-disordered breathing (SDB) affects at least 20 million people in the United States and is defined as a cessation of breathing during sleep that is caused by repetitive partial or complete obstruction of the airway and pharyngeal structures. There are two types: the most common form, obstructive sleep apnea (OSA), and central sleep apnea. The prevalence in the general population is 2% to 4%. The manifestations of OSA include episodes of loud snoring, decreased oxygen saturation, brief periods of apnea, and arousal from sleep. These episodes may occur several times during sleep. OSA is strongly linked to cardiovascular diseases—especially hypertension and coronary artery disease, which eventually leads to heart failure—so the prevalence in patients with heart failure rises to approximately 50%. Consequences of OSA include altered alertness, daytime somnolence, cognitive impairment, and increased morbidity and mortality. Common screening methods include pulse oximetry, blood gas analysis, and/or ambulatory airflow measurements, but the diagnosis of OSA is confirmed by overnight sleep laboratory studies.
Treatment for mild OSA includes conservative measures such as weight loss, abstaining from the use of alcohol and sedatives, avoiding the supine position during sleep, and sometimes oropharyngeal appliances or surgery. However, continuous positive airway pressure (CPAP) is the most consistently effective treatment for clinically significant OSA and appears to substantially improve the condition. Unfortunately, some patients complain that the CPAP mask is uncomfortable, so compliance with the treatment is often low. As technology advances, the treatment of OSA will become more comfortable and less cumbersome. Patients must be encouraged to try different equipment to adapt to their own facial structure, because patients who use CPAP report less fatigue, better BP control, and improved quality of life.
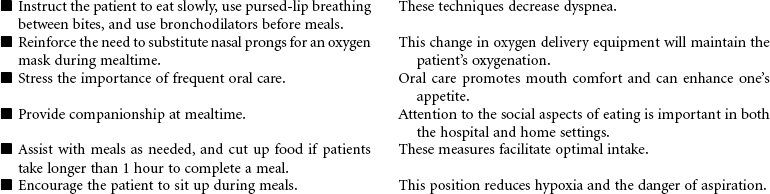
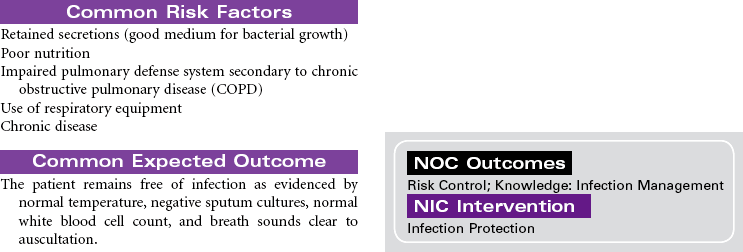
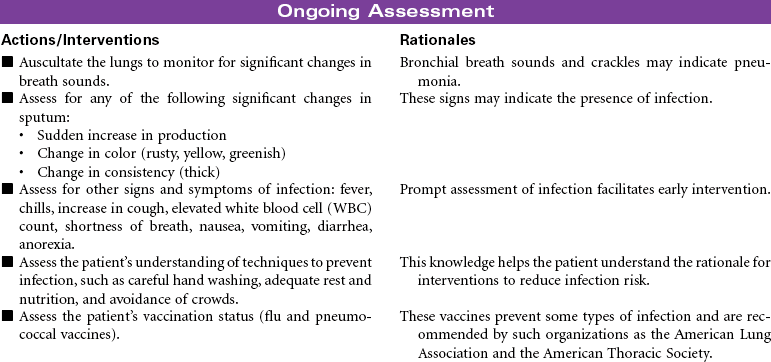
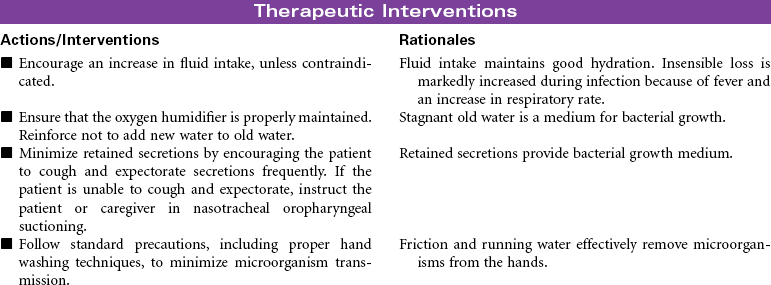
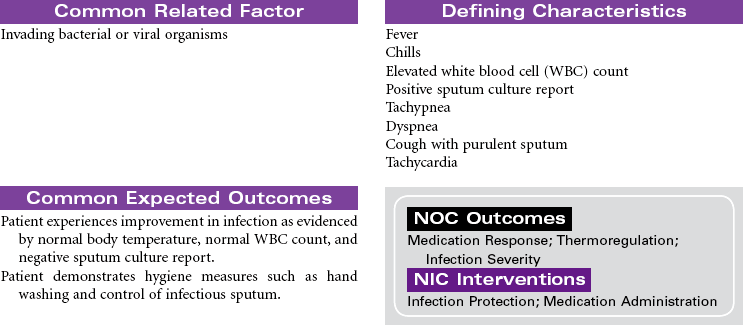
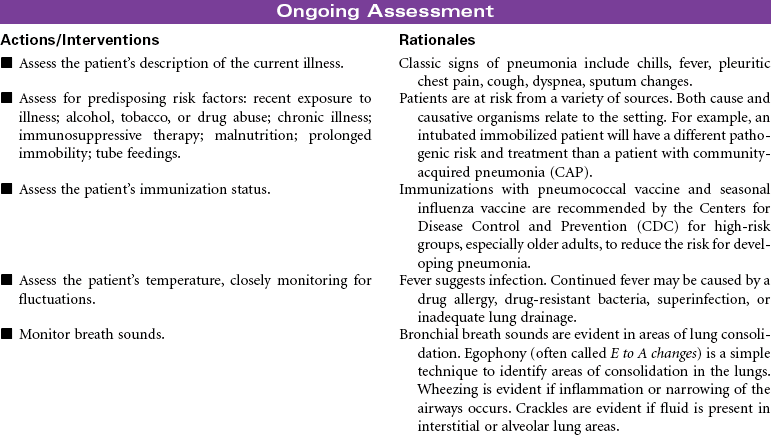
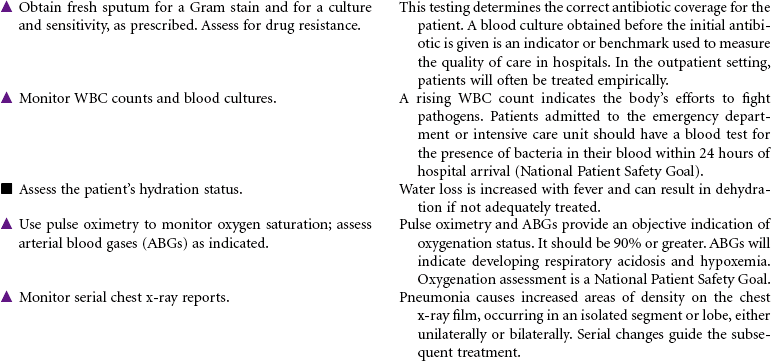
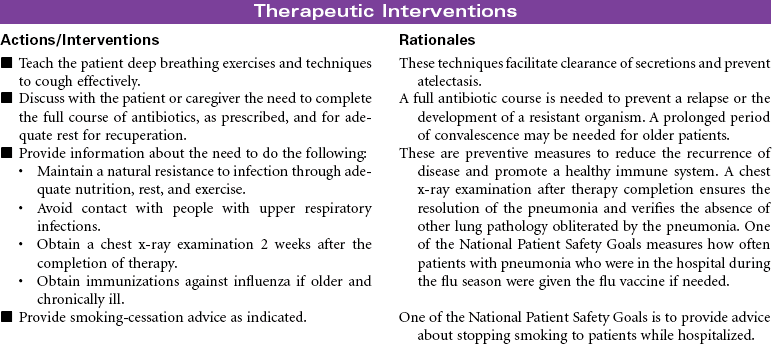
Pneumonia
Pneumonitis; Community-Acquired Pneumonia (CAP); Hospital-Acquired Pneumonia (HAP); Aspiration Pneumonia
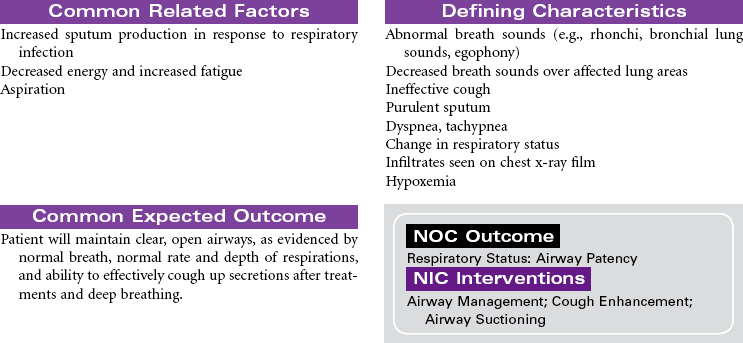
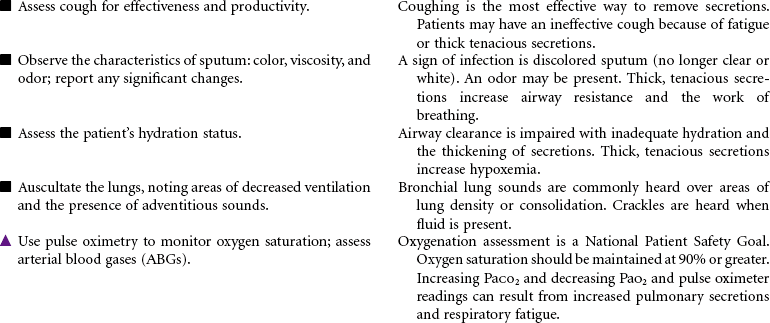
Pneumonia is caused by a bacterial or viral infection that results in an inflammatory process in the lungs. It is an infectious process that is spread by droplets or by contact and is one of the most common causes of death in older adults. Risk factors include upper respiratory tract infection, excessive alcohol ingestion, central nervous system depression, cardiac failure, any debilitating illness, chronic obstructive pulmonary disease (COPD), endotracheal (ET) intubation, and postoperative effects of general anesthesia. Pneumonia is a particular concern in persons older than 65 years or anyone who is bedridden, immunosuppressed, malnourished, or hospitalized, and patients exposed to methicillin-resistant Staphylococcus aneurysm (MRSA), as well as the very young and very old. Pneumonia may be nosocomial or community-acquired (CAP).
Types of pneumonia include the following:
• Gram-positive pneumonias: pneumococcal pneumonia, staphylococcal pneumonia, streptococcal pneumonia (these account for most community-acquired pneumonias)
• Gram-negative pneumonias: Klebsiella pneumonia, Pseudomonas pneumonia, influenzal pneumonia, Legionnaire disease (these account for most hospital-acquired pneumonias)
• Anaerobic bacterial pneumonias (usually caused by aspiration)
• Mycoplasma pneumonia (atypical bacterial pneumonia common in young adults—“walking pneumonia”)
• Viral pneumonias (most common in infants and children; influenza A is the primary causative viral agent in adults)
The Joint Commission (TJC) has identified National Quality Improvement Goals as standardized performance measures that hospitals can use to measure the overall quality of care provided to pneumonia patients. In healthy people with responsive immune systems, treatment can be administered in the outpatient setting. This care plan focuses on acute care treatment of pneumonia.



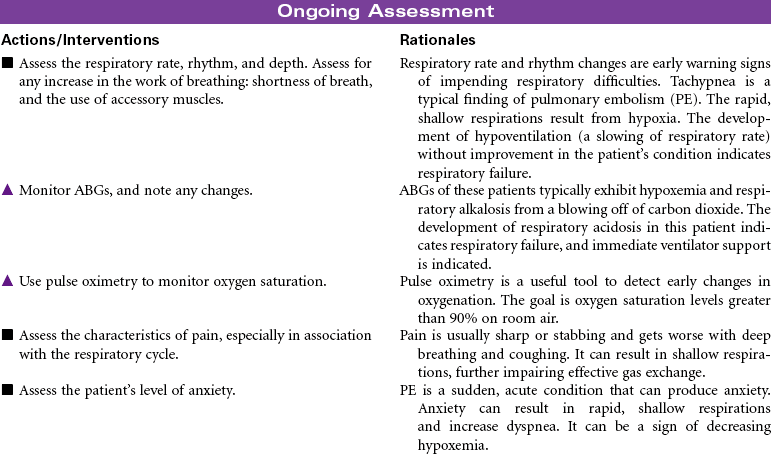
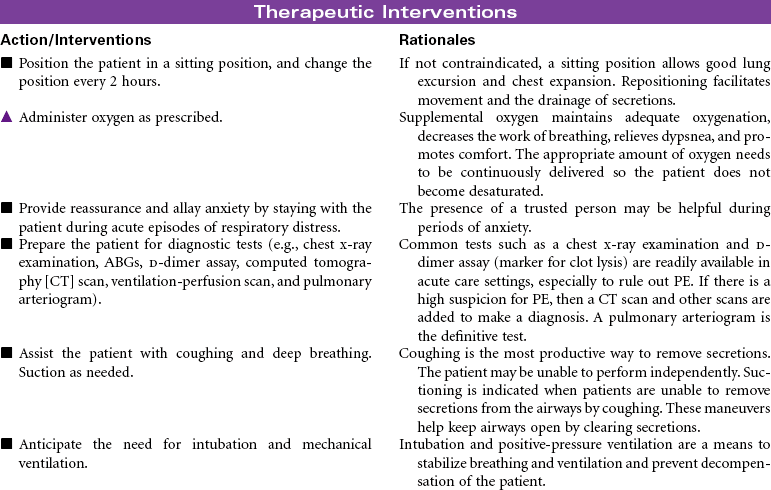
Pulmonary Embolism
Thromboembolism; Deep Vein Thrombosis
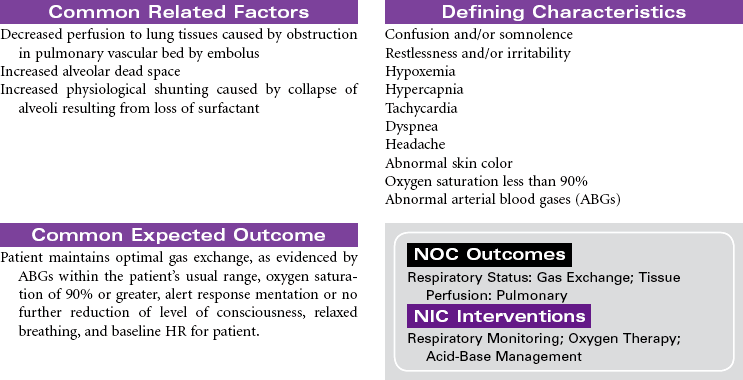
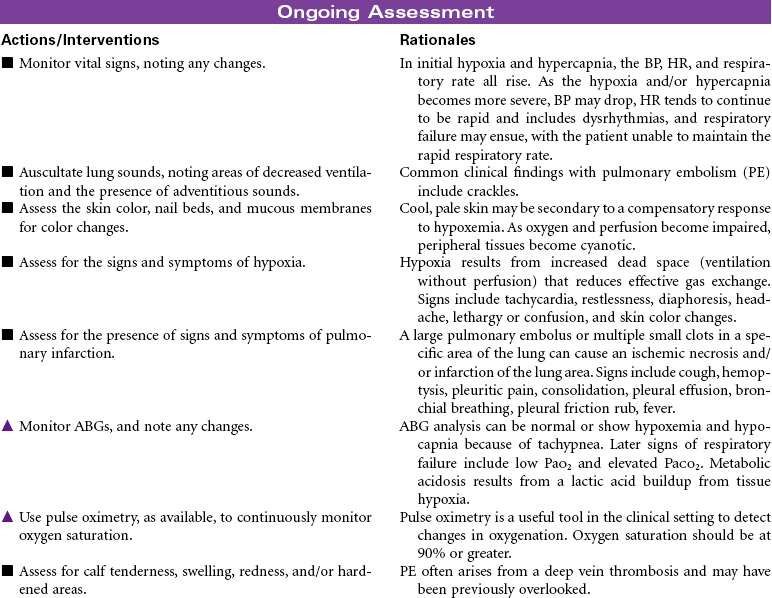
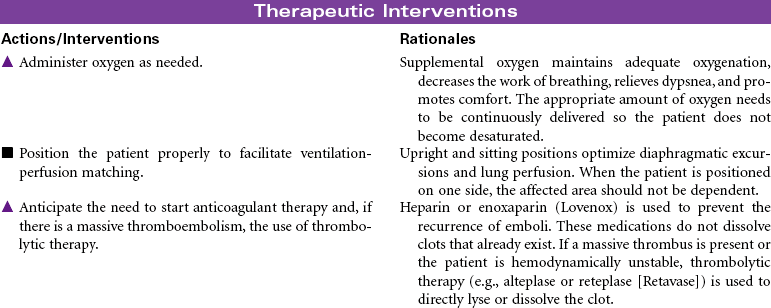
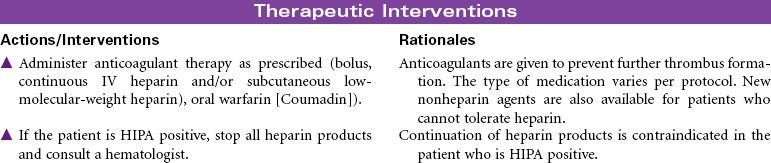
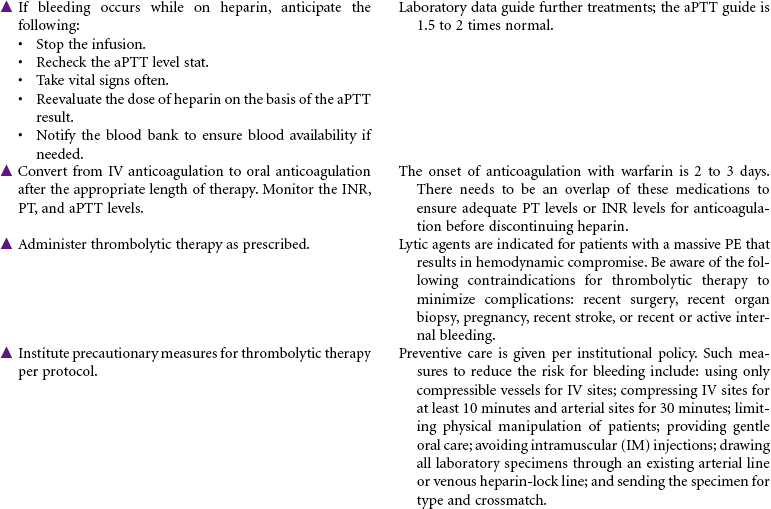
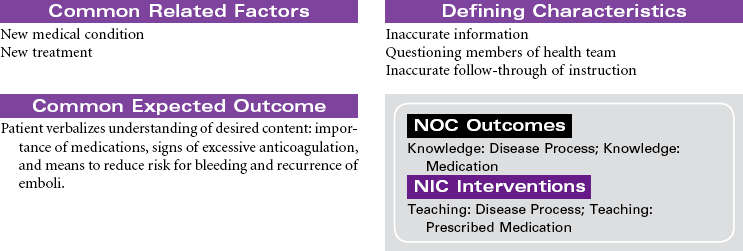
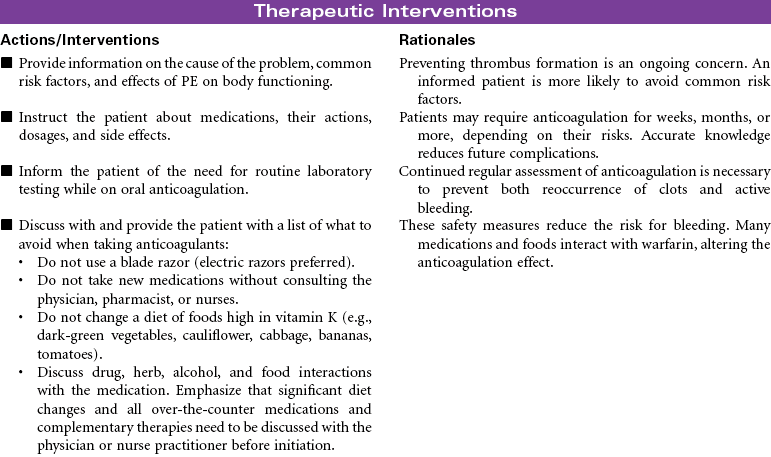
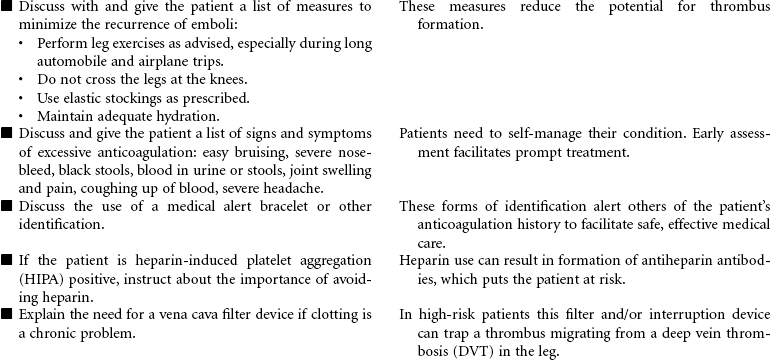
Pulmonary embolism (PE) occurs when a thrombus (blood clot) originating in the venous system or the right side of the heart obstructs blood flow in the pulmonary artery or one of its branches. The clinical picture varies according to the size and location of the embolus, making diagnosis challenging. Careful analysis of risk factors aids in diagnosis; these include prolonged immobility, deep vein thrombosis, recent surgery, postpartum state, trauma to vessel walls, hypercoagulable states, and certain disease states such as heart failure and trauma. Treatment approaches vary depending on the degree of cardiopulmonary compromise associated with the PE. They can range from thrombolytic therapy in acute situations to anticoagulant therapy and general care measures to optimize respiratory and vascular status (e.g., oxygen, compression stockings). PE is a frequent hospital-acquired condition, and one of the most common causes of death in hospitalized patients. Prevention of thrombus formation is a critical nursing role. This care plan focuses on acute care treatment for PE.


Respiratory Failure, Acute
Ventilatory Failure; Oxygenation Failure
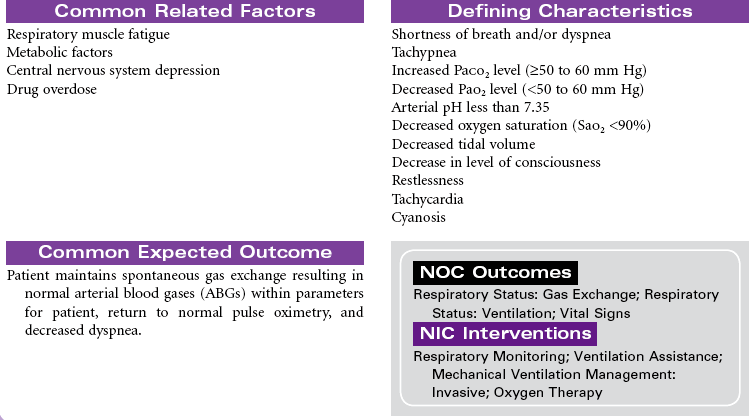
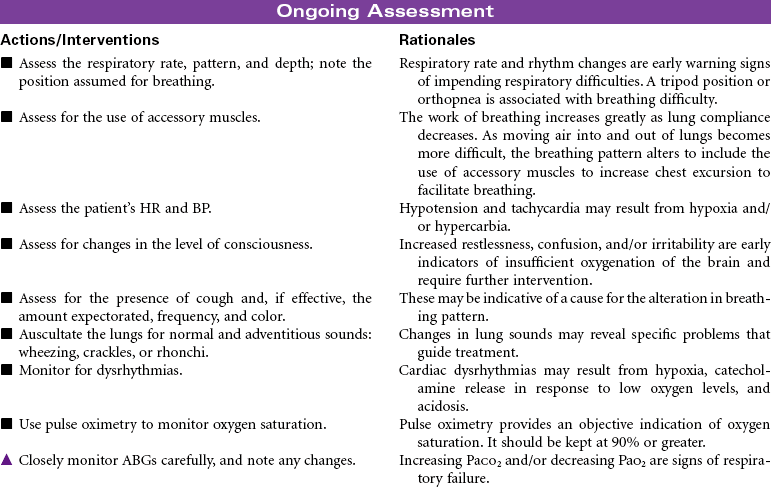
Acute respiratory failure is a life-threatening inability to maintain adequate pulmonary gas exchange. Persons with acute respiratory failure cannot carry out the two major functions of gas exchange: delivery of adequate amounts of oxygen into the arterial blood (oxygenation failure) or removal of a corresponding amount of carbon dioxide from the mixed venous blood (ventilatory failure). Respiratory failure can result from obstructive disease (e.g., emphysema, chronic bronchitis, asthma), restrictive disease (e.g., atelectasis, acute respiratory distress syndrome [ARDS], pneumonia, multiple rib fractures, postoperative abdominal or thoracic surgery, central nervous system depression), or ventilation-perfusion abnormalities (e.g., pulmonary embolism). This care plan focuses on acute care management of respiratory failure.


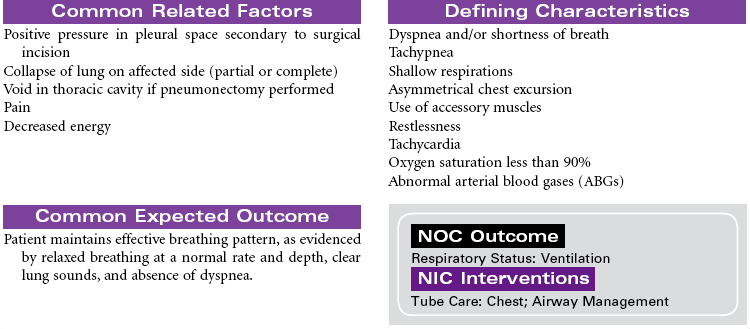
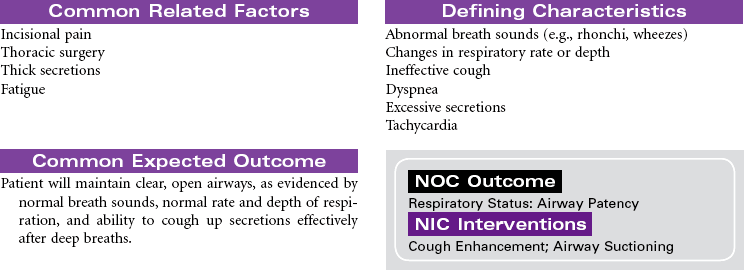
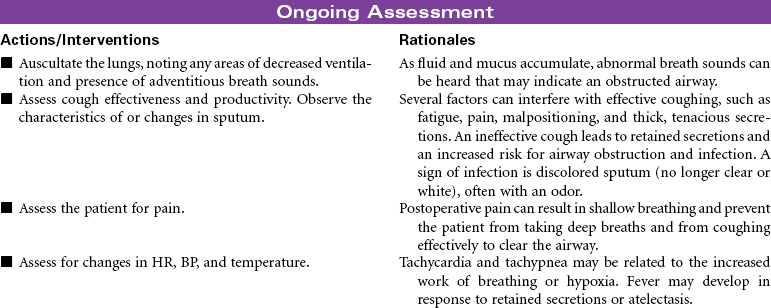
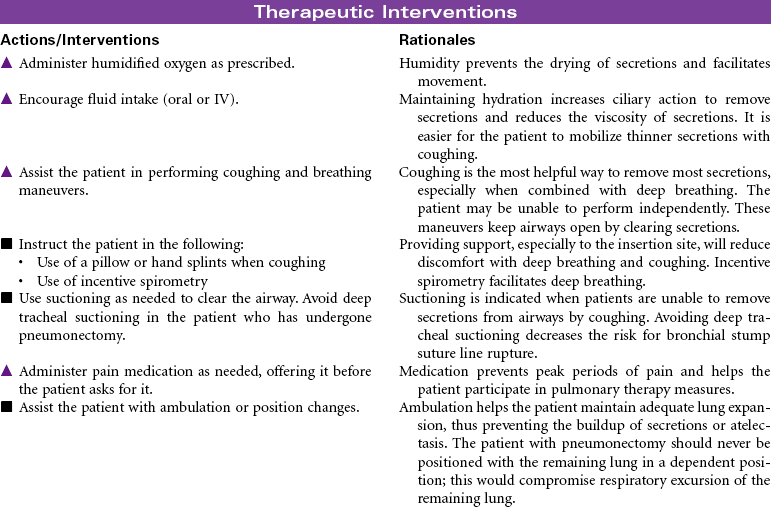
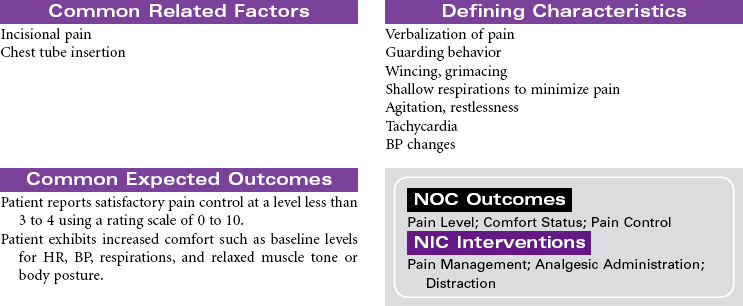
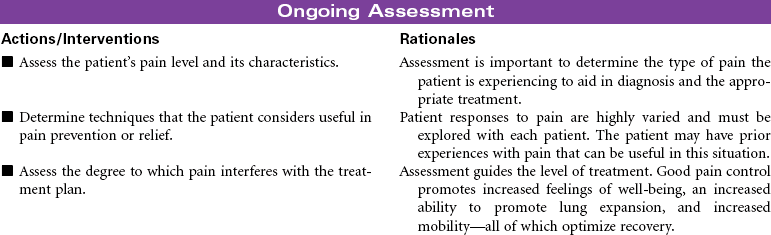
Thoracotomy
Chest Surgery; Thoracic Surgery; Lobectomy; Segmental Resection; Wedge Resection; Thoracostomy; Pneumonectomy
Thoracotomy is a surgical opening into the thorax for biopsy, excision, drainage, and/or correction of defects. The surgical procedures done by thoracotomy correction may include the following:
• Lobectomy: Removal of one lobe of the lung; lobectomy is indicated for lung cancer, bronchiectasis, tuberculosis (TB), emphysematous bullae, benign lung tumors, or fungal infections.
• Segmental resection: Removal of one or more lung segments; segmental resection is indicated for bronchiectasis or TB.
• Wedge resection: Removal of a small, localized lesion that occupies only part of a segment; wedge resection is indicated for excision of nodules or lung biopsy.
• Thoracostomy: Insertion of an endoscope through a small incision in the chest wall, useful for open lung biopsy to determine diagnosis, for lymph node biopsy, to introduce medications directly into the lungs, or to treat accumulated fluid, empyema, or blood in the space around the lungs.
• Pneumonectomy: Removal of entire lung; indicated for lung cancer, extensive TB, bronchiectasis, or lung abscess.
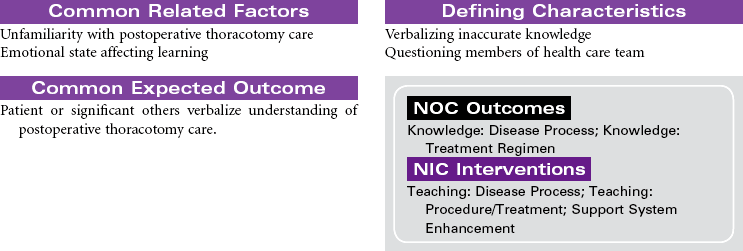
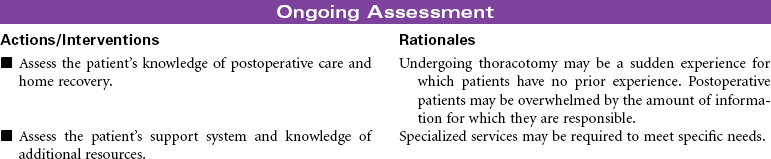
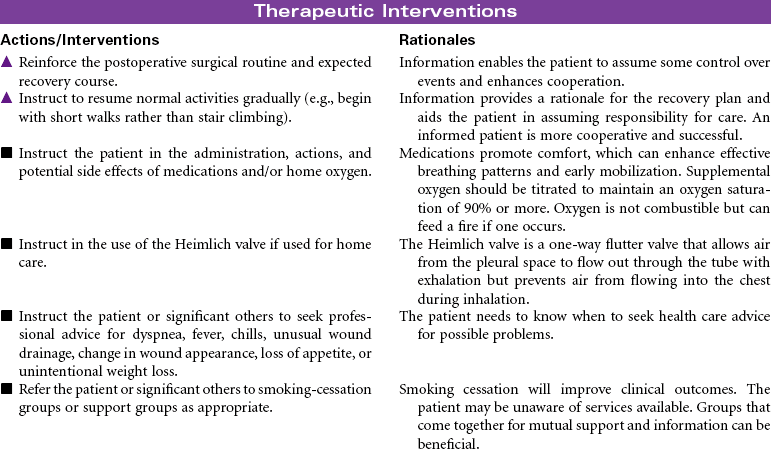
This care plan focuses on postoperative care of the patient having a thoracotomy.

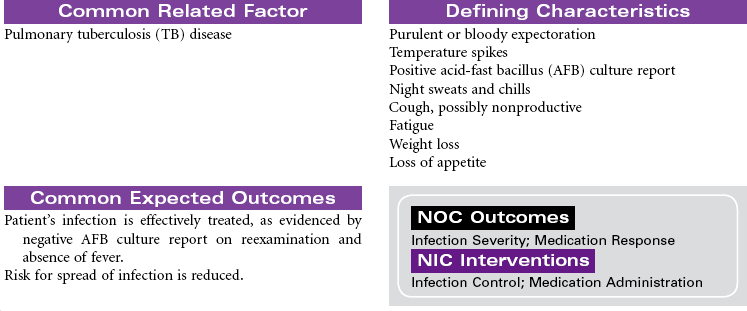
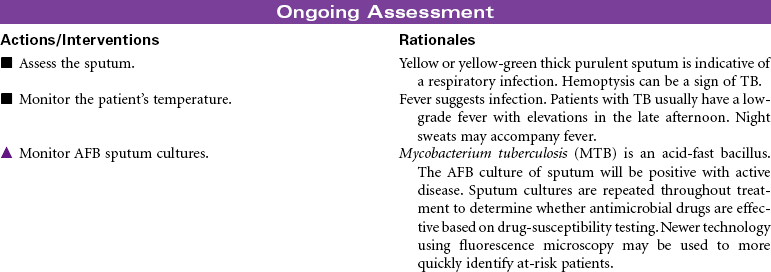
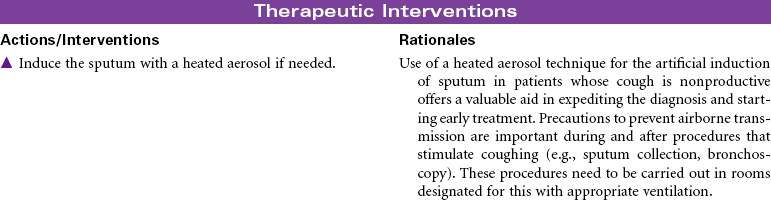
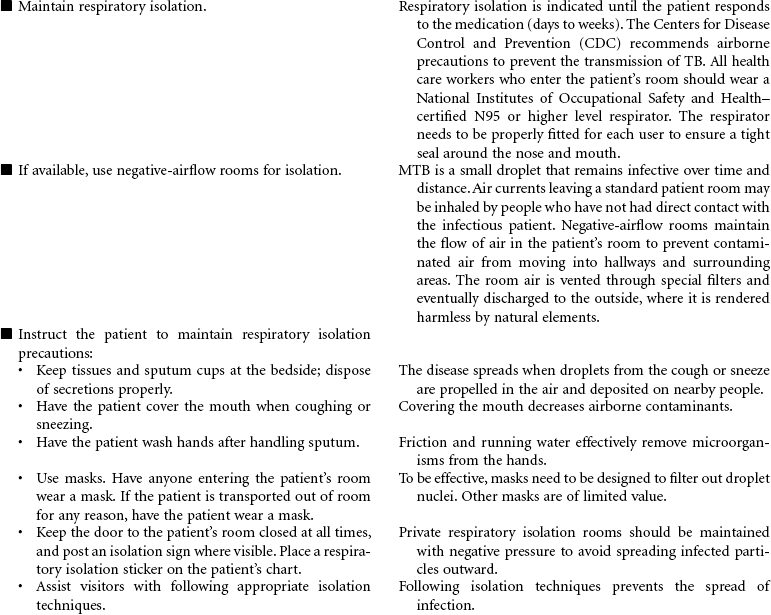
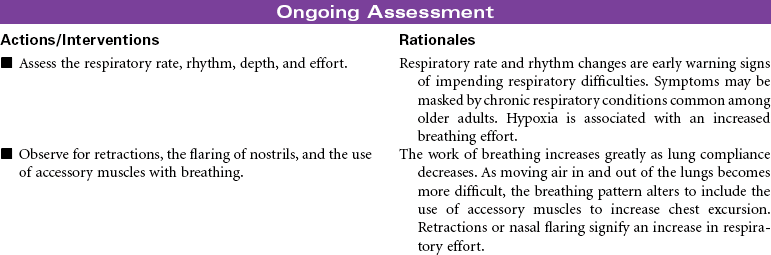
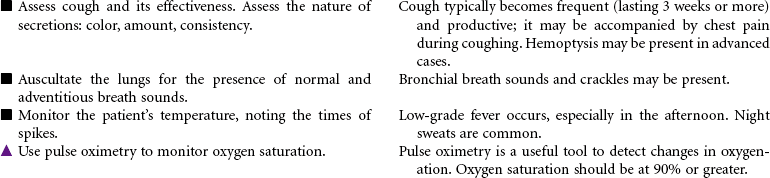
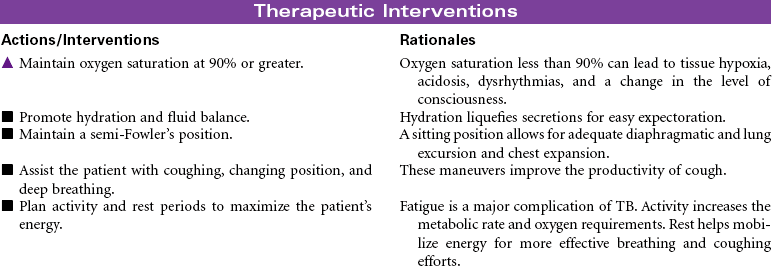
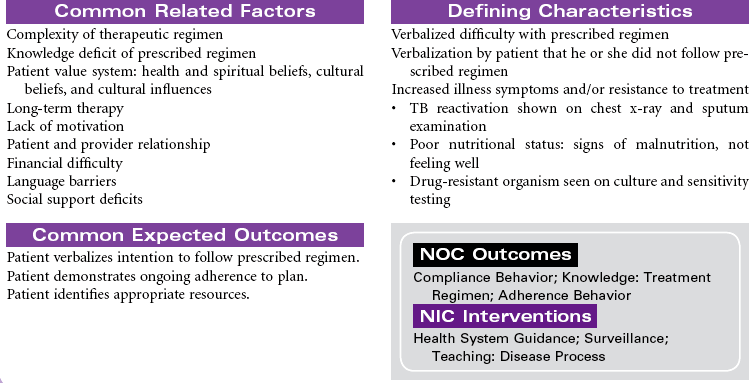
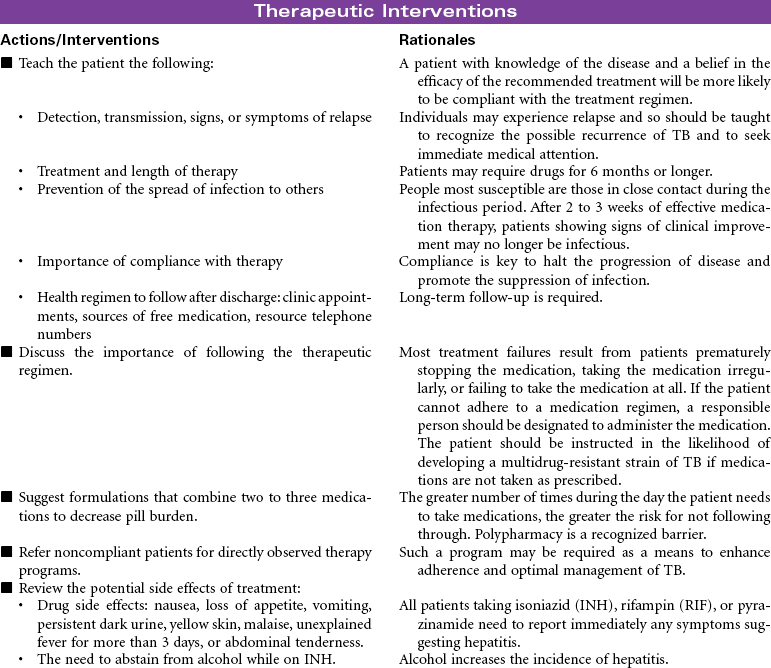
Tuberculosis
TB; Mycobacterium Tuberculosis
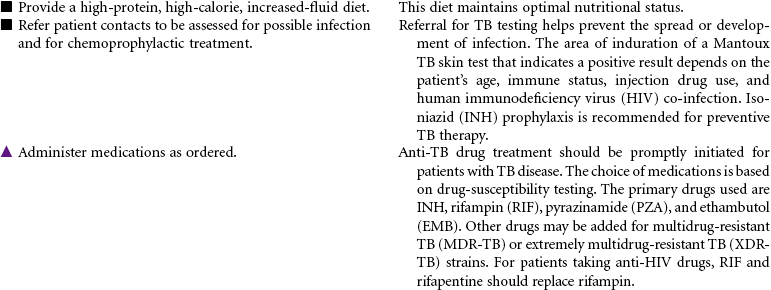
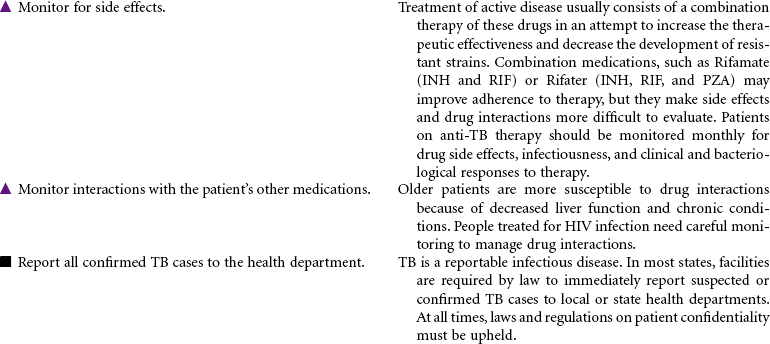
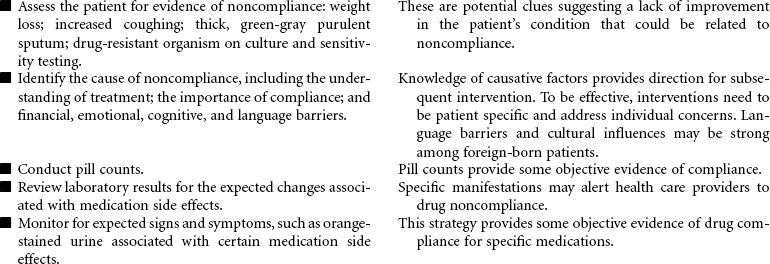
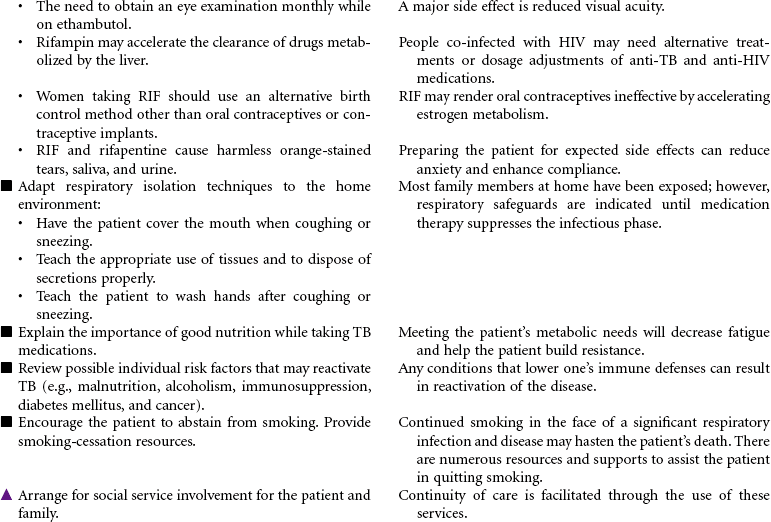
Patients infected with Mycobacterium tuberculosis (MTB) develop either latent tuberculosis (TB) infections or TB disease. Among adults, TB disease is usually confined to the respiratory tract. Everyone with TB disease needs antimicrobial therapy, as do people with latent TB infections who are at high risk for progressing to TB disease. Pulmonary TB disease is contagious, spread by airborne droplet nuclei that are produced when an infected person coughs or sneezes. Those at higher risk for development of clinical disease include the immunosuppressed (patients receiving cancer chemotherapy, patients infected with human immunodeficiency virus [HIV], patients with diabetes mellitus, adolescents, and patients younger than 2 years of age). Patients with latent TB infections may progress to TB disease. A reactivation can occur later in patients with decreased resistance, concomitant diseases, and immunosuppression. People are more likely to become infected with TB if they have consistent close contact with a person who has active disease. Crowded living arrangements contribute to disease transmission. Immigrants from countries where TB is common may have undiagnosed TB when they enter the United States. Other variables that increase the risk for infection with TB include older age, poverty, homelessness, and drug and alcohol abuse. There has been a recent resurgence of TB with the emergence of multidrug-resistant TB (MDR-TB) and extremely drug-resistant (XDR-TB) strains of the bacillus. These drug-resistant strains of the disease are more common among people with HIV disease or inadequately treated TB or people who live in areas where these strains are endemic.
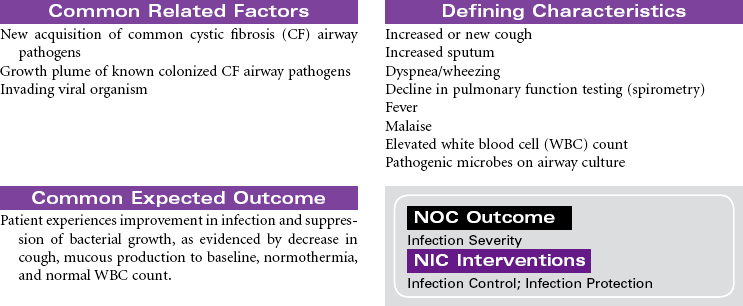
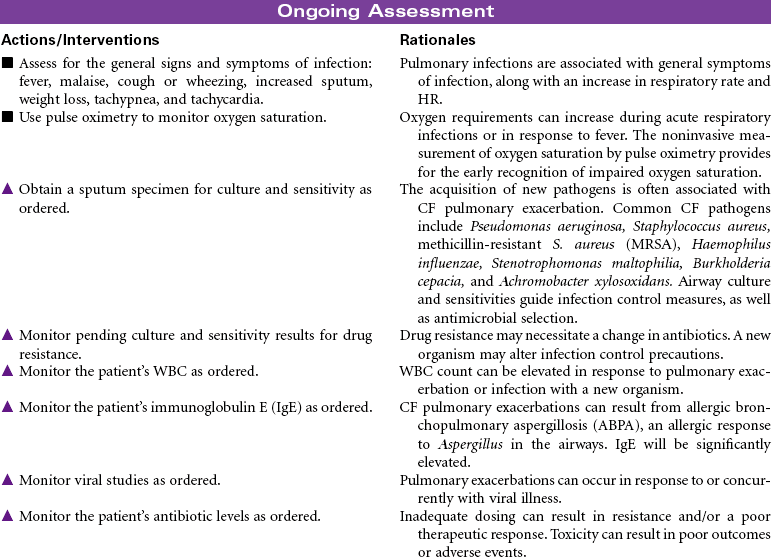
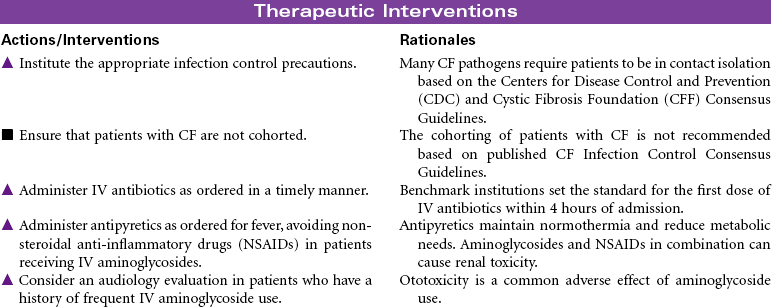
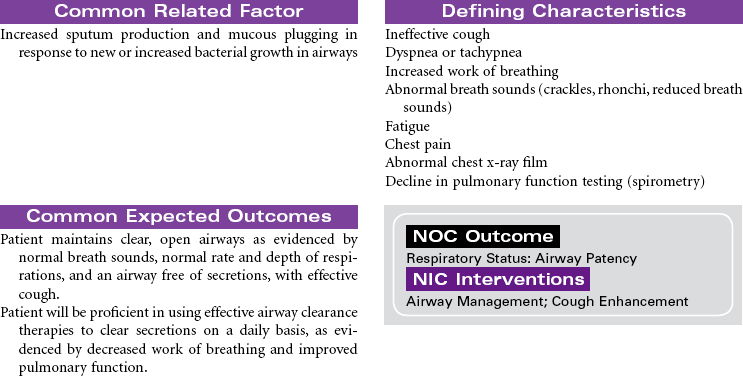
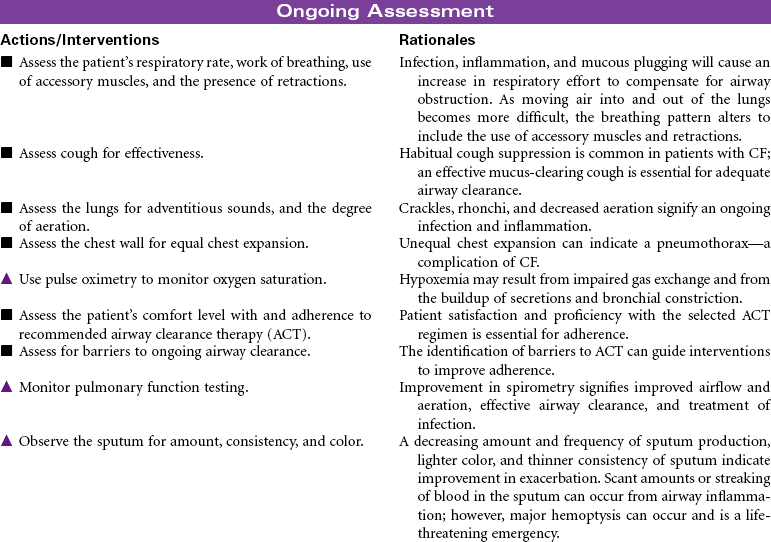
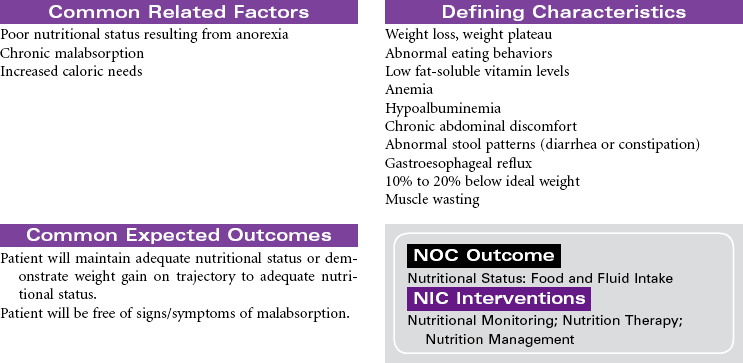
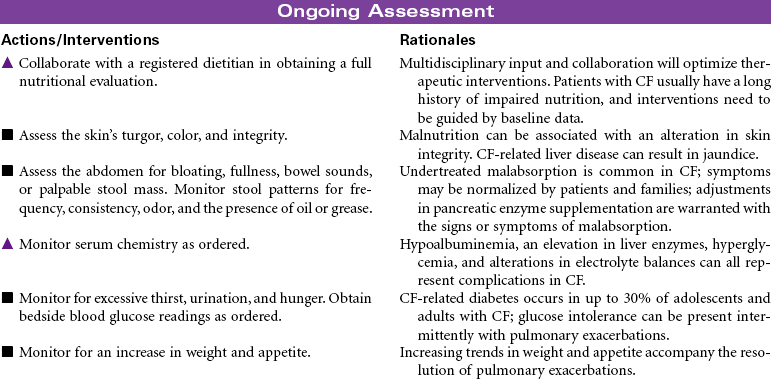
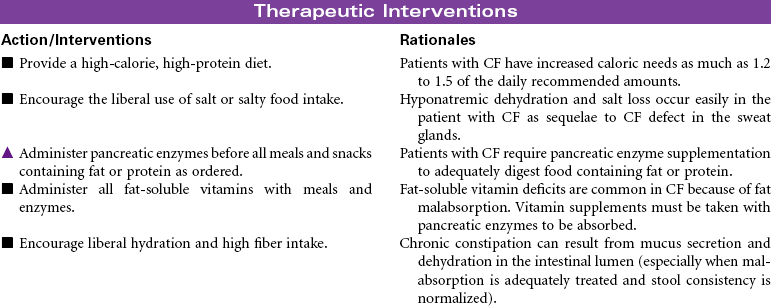
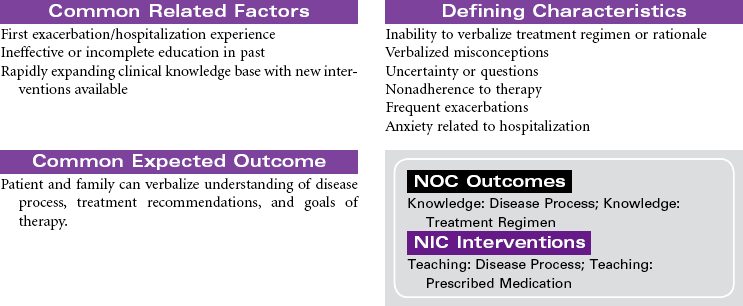
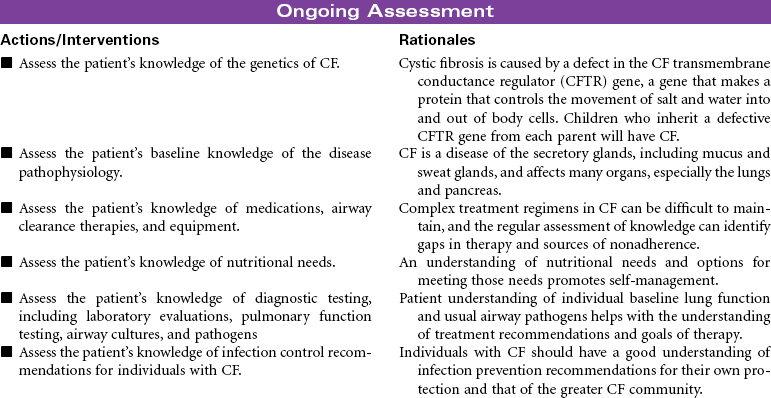
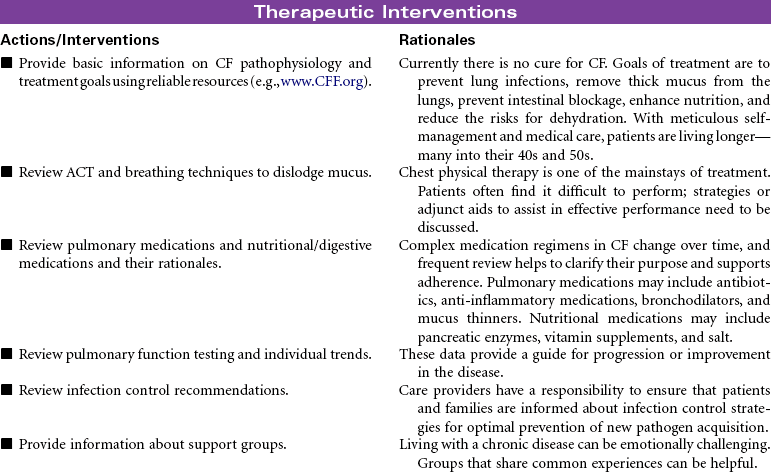
Cystic Fibrosis
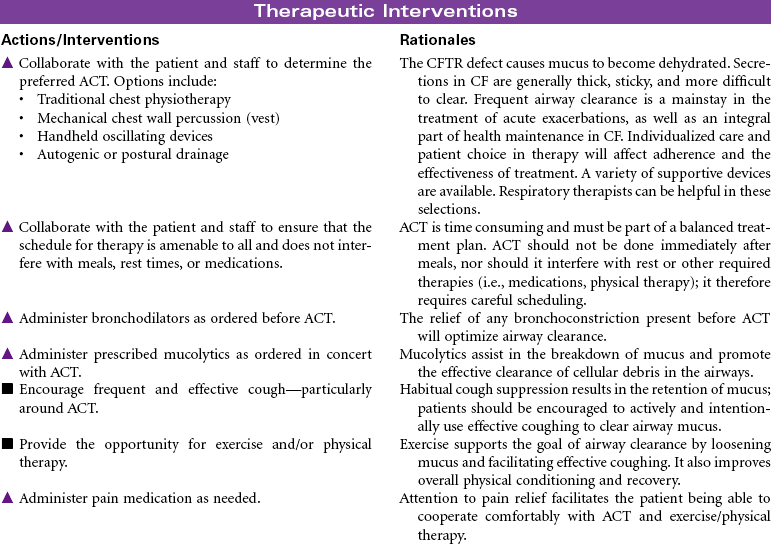
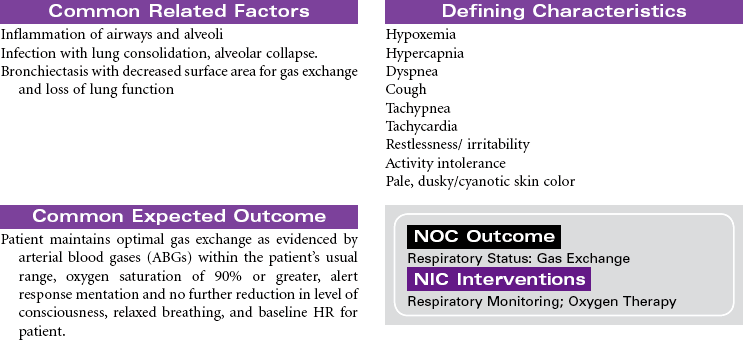
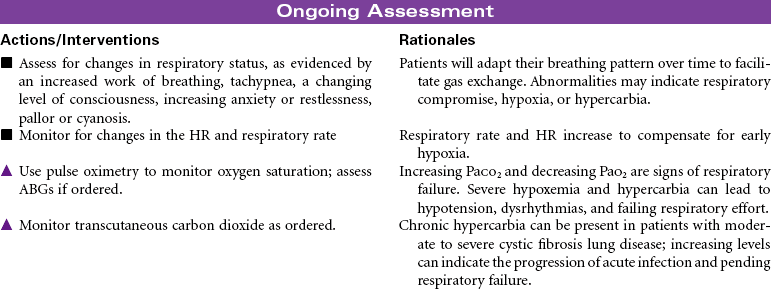
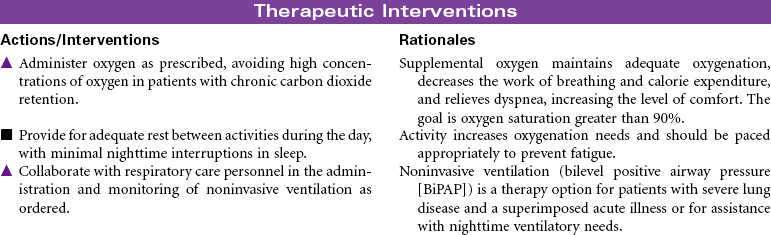
Cystic fibrosis (CF) is an autosomal recessive, profoundly life-shortening genetic disease. It occurs most commonly in whites of northern European descent but has been identified in most ethnicities. Genetic abnormalities in the seventh chromosome result in impaired function of CF transmembrane conductance regulator (CFTR) protein present in the mucus-secreting cells of the body, primarily affecting the respiratory and gastrointestinal tracts. The hallmark characteristics of CF are chronic, progressive lung disease, resulting from secretion of dehydrated mucus with airway obstruction, and malnutrition from pancreatic insufficiency. However, there is a wide range of disease severity. Respiratory symptoms can range from nearly asymptomatic disease with undetectable changes in lung function to severe obstructive disease early in childhood, whereas gastrointestinal symptoms may range from mild constipation, normal liver function, and intermittent pancreatitis to severe loss of pancreatic function, malabsorption with subsequent malnutrition, CF-related diabetes and end-stage liver disease. Nonetheless, with improved understanding and treatment, the majority of affected individuals now live well into adulthood. The sweat glands and reproductive glands are also affected; almost all males with CF are sterile because of absence or impairment of the vas deferens, whereas females have reduced fertility. The impact on the sweat gland gives rise to abnormally high chloride secretion; a simple analysis of sweat chloride content continues to be the gold standard for CF diagnosis.
Lung disease accounts for most disease morbidity and remains the primary cause of death in CF. The cycle of lung disease in CF is caused by inflammation, infection, and impaired airway clearance. Daily lifelong airway clearance, attention to infection prevention, and early, aggressive treatment of pulmonary exacerbations are the mainstays of therapy aimed at slowing decline and preserving lung function. In addition, supporting normal growth and nutrition over the life span is associated with improved respiratory health, longevity, and quality of life in the adult patient. Lung transplant may be a treatment option for some patients. This care plan focuses on acute care treatment of pulmonary exacerbation.
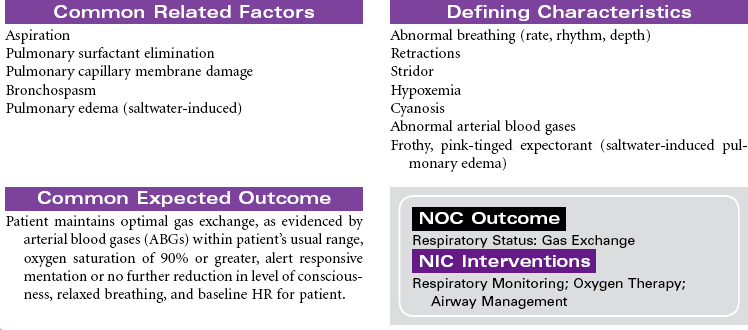
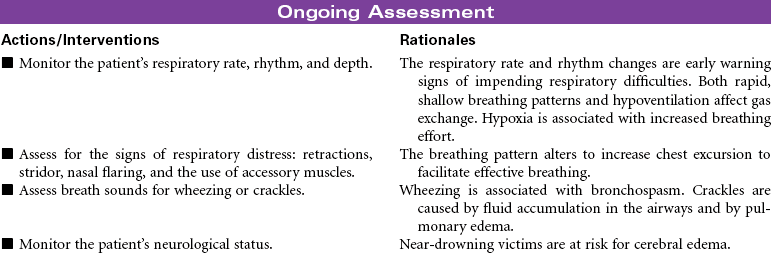
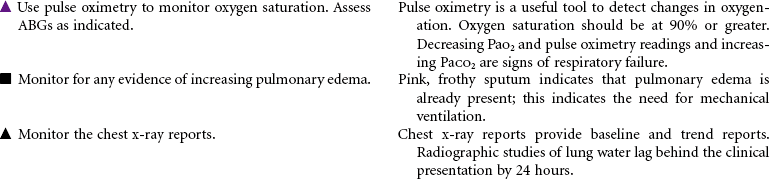
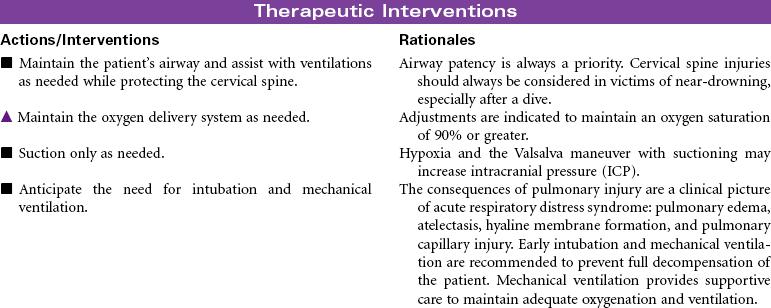
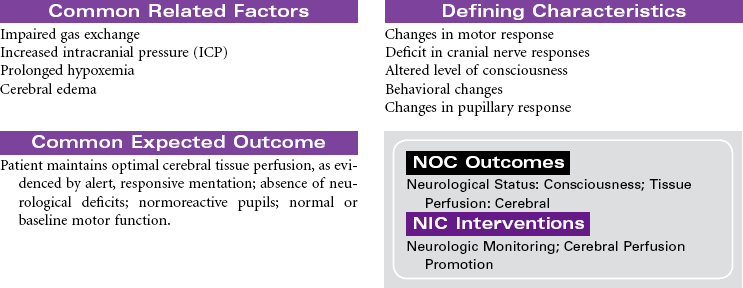
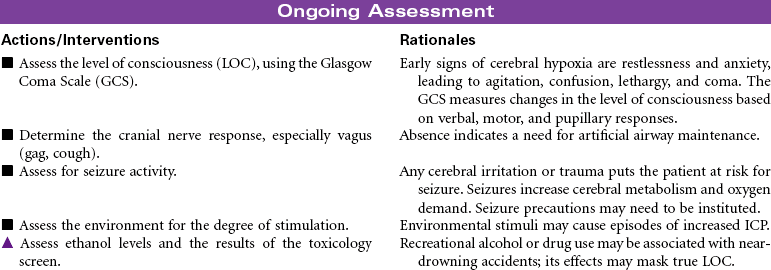
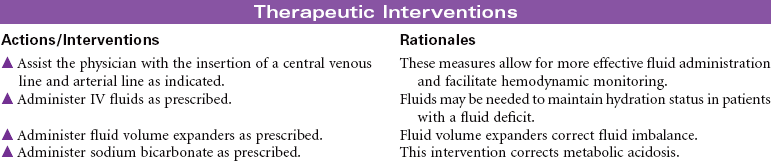
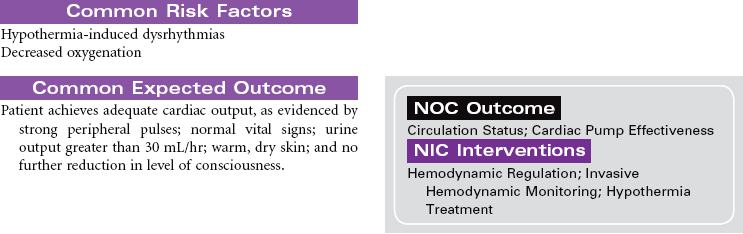
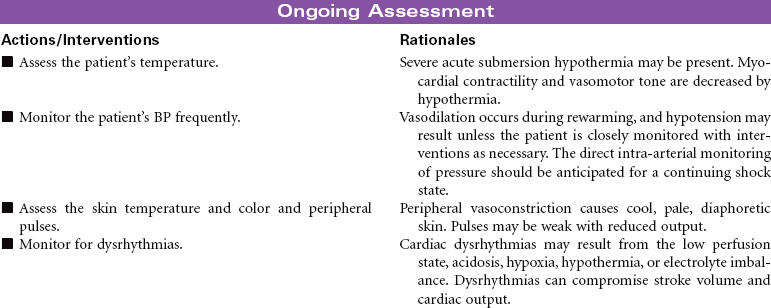
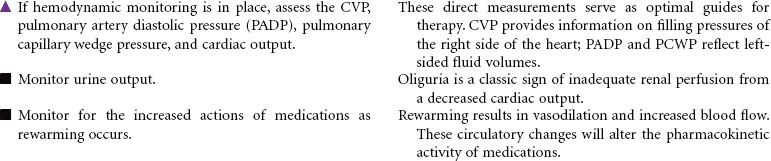
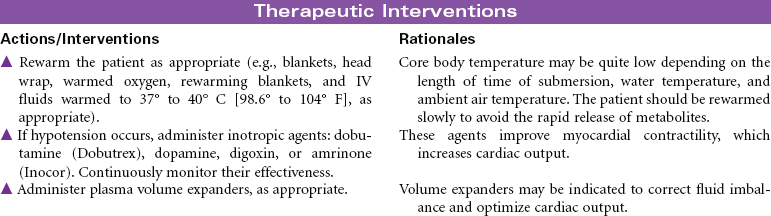
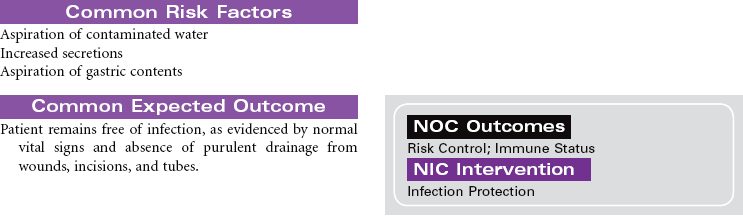
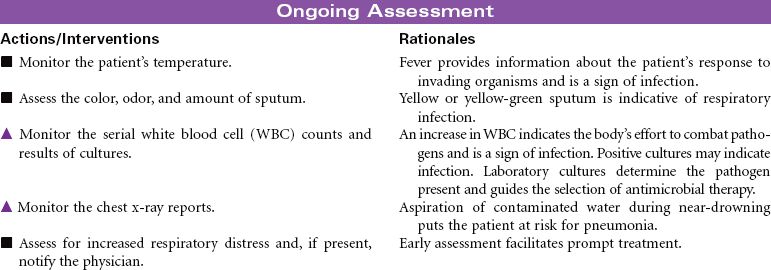
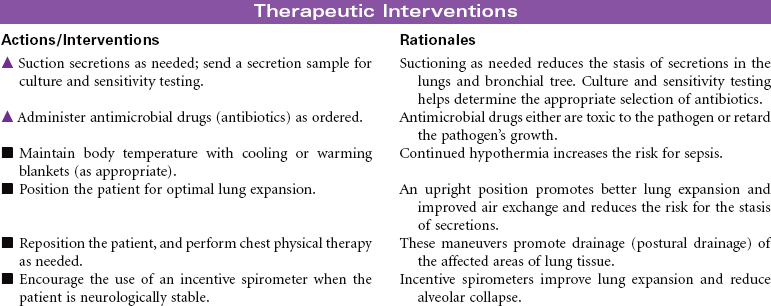
Near-Drowning
Near-drowning refers to survival at least 24 hours after submersion in a fluid medium. Aspiration of liquid causes plasma to be drawn into the lungs, resulting in hypoxemia, acidosis, and hypovolemia. Hypoxemia results from the decrease in pulmonary surfactant caused by the absorbed water that leads to damage of the pulmonary capillary membrane. Severe hypoxia can also result from asphyxia related to submersion without aspiration of fluid. Freshwater drownings are far more common than saltwater drownings. Although most drownings are accidental, patients may have an underlying seizure disorder or cardiac dysrhythmia. It is difficult to predict the neurological outcome of near-drowning within the first few days. Some patients require long-term rehabilitation or custodial care. This care plan addresses the physical needs of a patient in an acute care setting.
Pneumothorax With Chest Tube
Collapsed Lung; Tension Pneumothorax
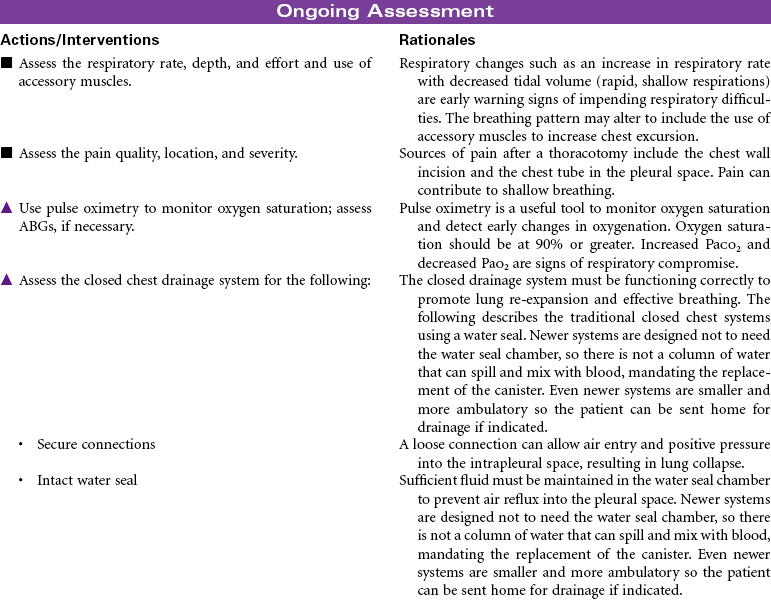
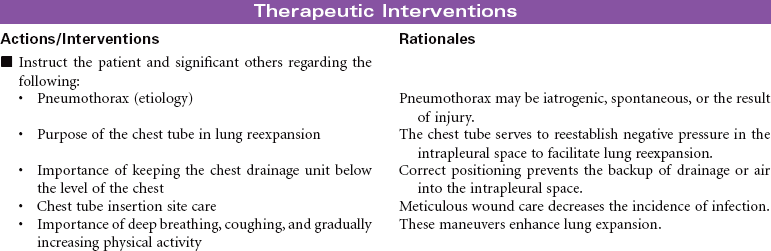
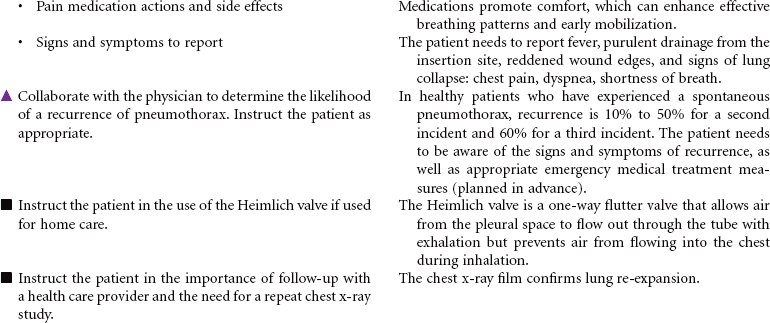
Presence of air in the intrapleural space can cause partial or complete collapse of the lung. The air causes disruption of the normal negative pressure that exists in the pleural space. Pneumothorax can be iatrogenic, spontaneous, or the result of injury. Several methods are available for treating pneumothorax, ranging from observation for collapses of less than 20% or needle or chest tube insertion for larger collapses. This care plan describes a traditional chest tube drainage system used to reestablish negative pressure in the intrapleural space to facilitate lung reexpansion. Newer systems are designed as an all-in-one plastic device that is waterless and disposable. Even newer systems are smaller and more ambulatory, so the patient can be sent home for drainage if indicated.

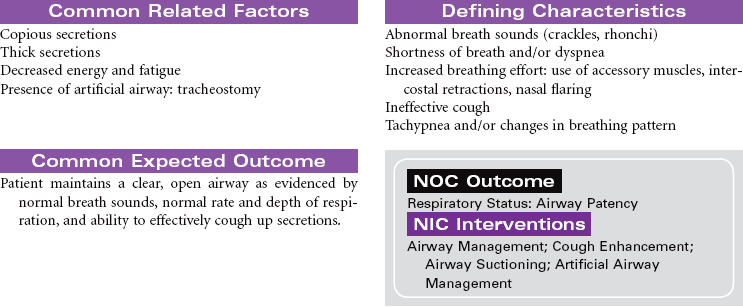
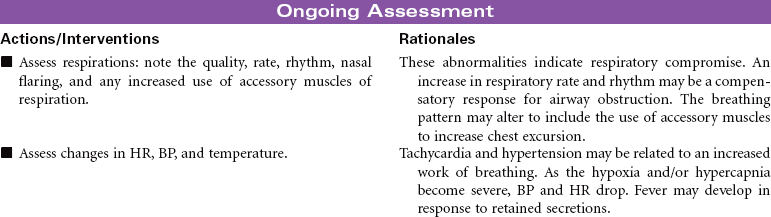
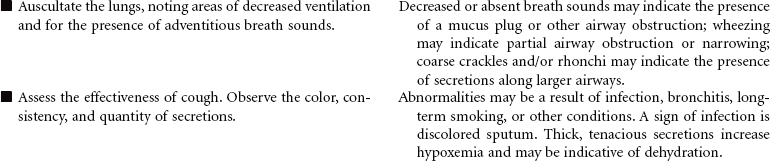
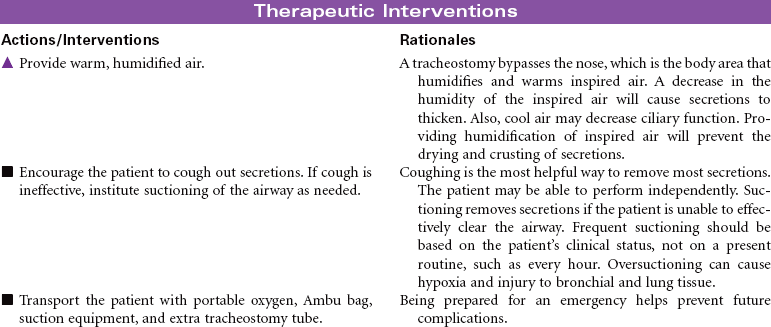
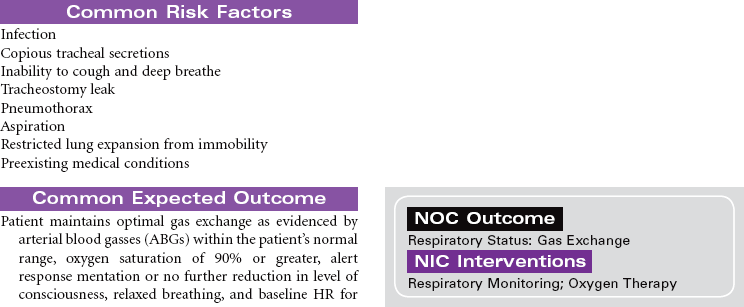
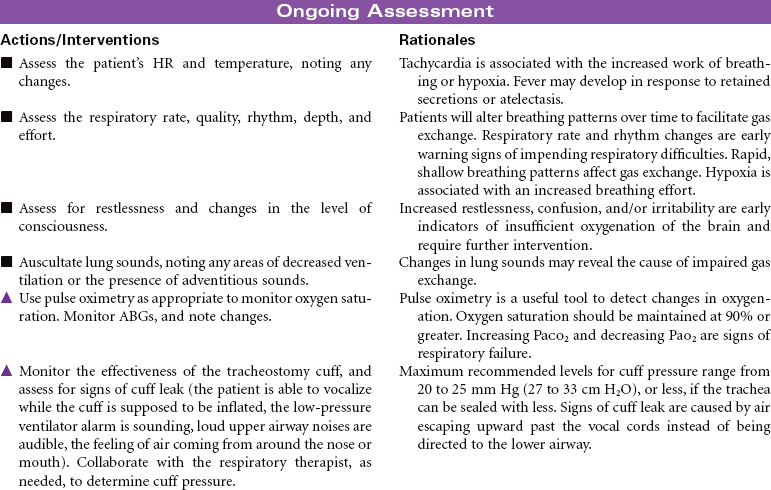
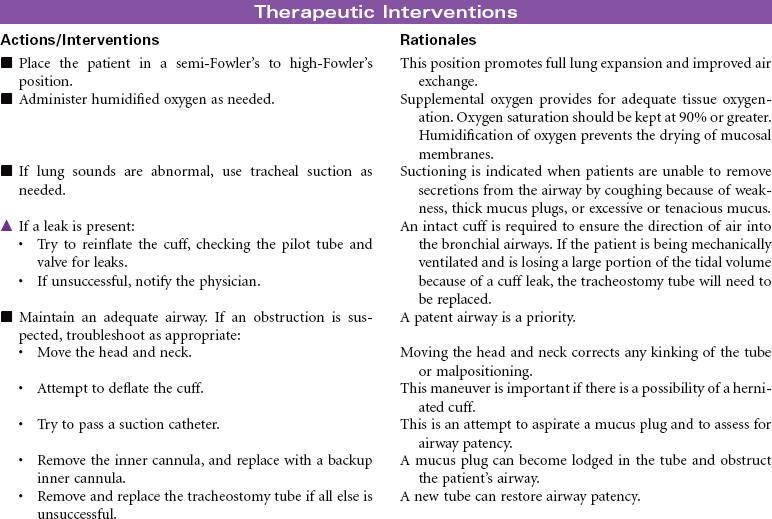
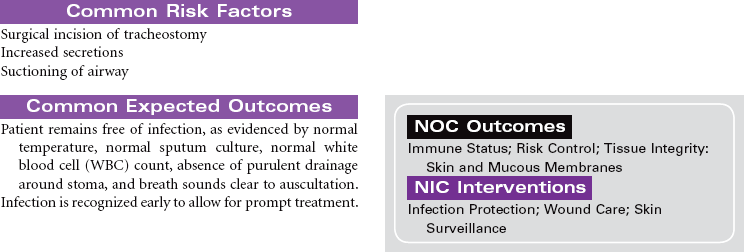
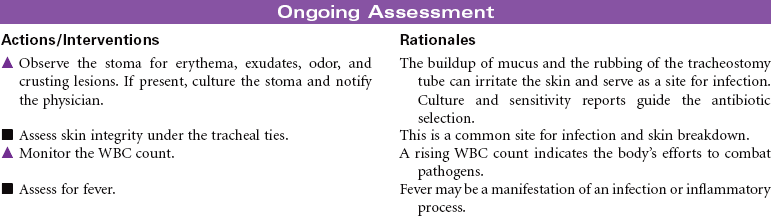
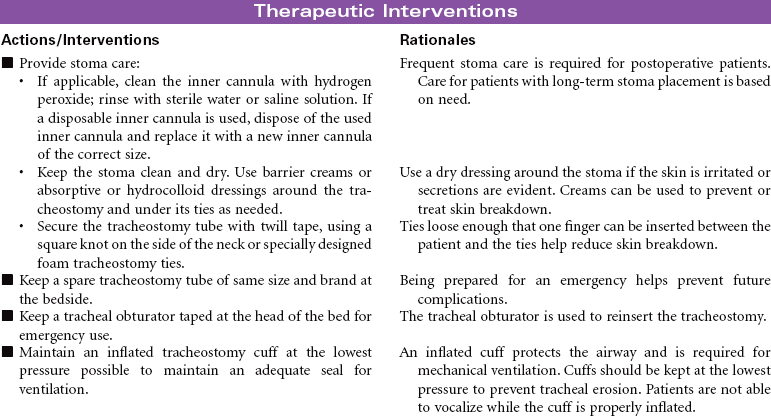
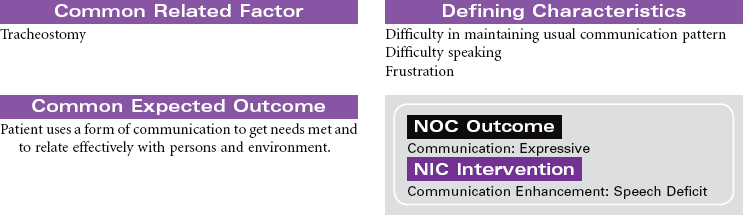
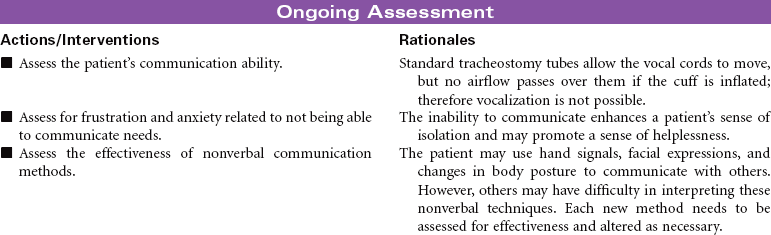
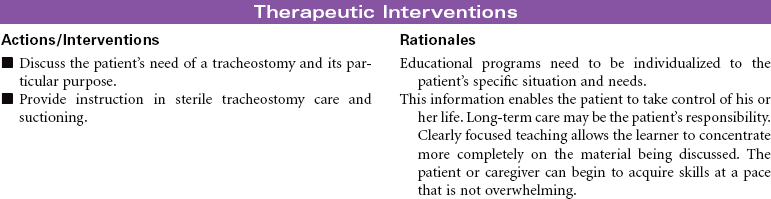
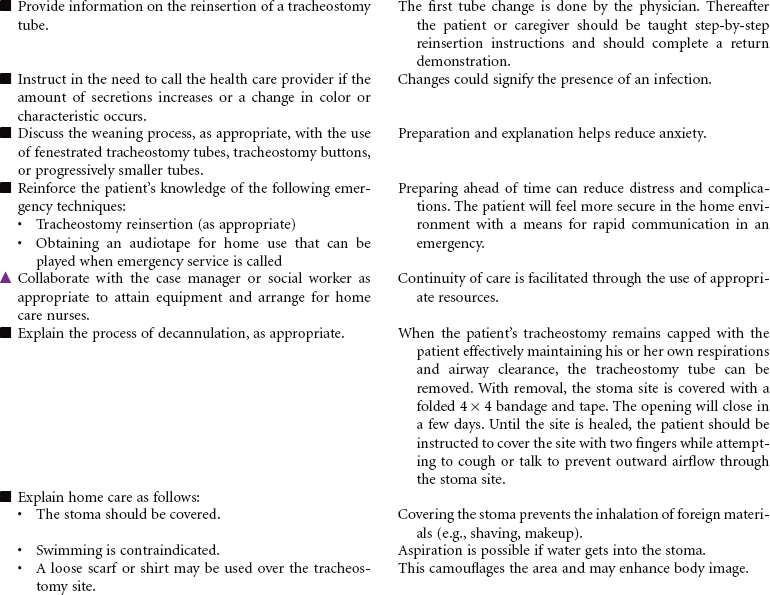
Tracheostomy
Artificial Airway; Tracheotomy; Stoma
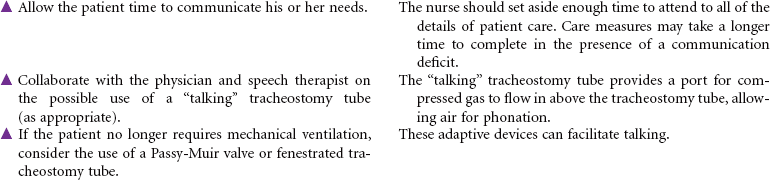
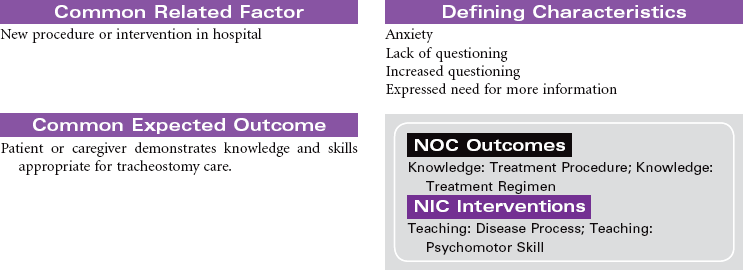
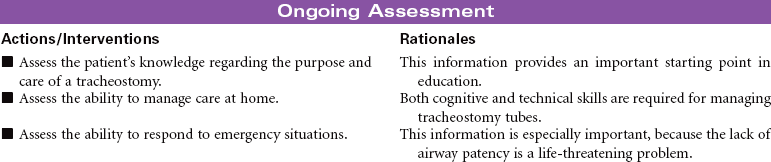
Tracheostomy is a surgical opening into the trachea that is used to prevent or relieve airway obstruction and/or to serve as an access for suctioning and for mechanical ventilation and other modes of oxygen delivery (tracheostomy collar, T-piece). A tracheostomy can facilitate weaning from mechanical ventilation by reducing dead space and lowering airway resistance. It also improves patient comfort by removing the endotracheal (ET) tube from the mouth or nose. The tracheostomy is preferred over an ET when an artificial airway is needed for more than a few days. Methods can be instituted for the patient to eat and speak, as well. This care plan focuses on tracheostomy in the acute care setting, as well as the patient in a chronic care facility or with home care.