5 LOBAR COLLAPSE
It is very important to recognise the CXR appearances indicating lobar collapse. The inexperienced observer will not find this easy as some of the five lobes produce subtle changes on the CXR. For example, in Fig. 5.1 do you recognise which lobe is collapsed? What is your diagnosis in Fig. 5.2?
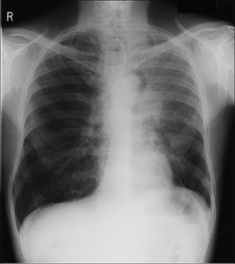

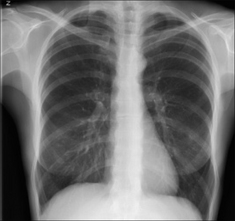
Figure 5.2 Female. Age 48. Unexplained loss of weight. Recent coughing episodes. Diagnosis on p. 68.
Basic TERMINOLOGY 1–3
Occasionally the words “consolidation” and “collapse” are used interchangeably. This is careless, incorrect, and leads to confusion.
Consolidation: An essentially homogeneous opacity in the lung characterised by little or no loss of volume…applicable only in an appropriate clinical setting when the opacity can with reasonable certainty be attributed to replacement of alveolar air by exudate, transudate, or cell debris.
Atelectasis: A synonym for collapse (i.e. volume loss). Atelectasis is the favoured term in the USA. Very small areas of collapse/atelectasis may produce a linear shadow, which is often, but not always, horizontal. This is usually referred to as “plate-like”, “linear”, or “subsegmental” atelectasis. Derivation of “Atelectasis” from the Greek: Ateles = incomplete, Extasis = expansion.
Lobar and total lung atelectasis (collapse) also occur. These larger varieties of atelectasis are usually associated with increased density in the affected part of the airless lung. To diagnose lobar atelectasis there must be specific evidence of volume loss such as displacement of a fissure, mediastinum or hilum. Elevation of a hemidiaphragm or a decrease in the spacing between the ribs can also be signs associated with atelectasis.
Collapse: Precise use of language differs between physicians in different countries. In the USA the word “collapse” generally connotes total atelectasis (i.e. total loss of volume of a lung or lobe). In everyday practice, North American physicians refer to all degrees of collapse—whether large or small—as “atelectasis”. In the UK the word “collapse” has a more general meaning and is utilised however large or small the amount of volume loss.
WHITE AREA ON THE CXR—CLARIFICATIONS
 Lung consolidation appears as a white (an extra dense) area on the CXR. The most common cause is pneumonia. A simple pneumonia will not be associated with any major loss of volume in the affected lobe. Lobar collapse: the affected lobe is also usually white…but volume loss will be evident. The whiteness is because: (a) the affected lung tissue occupies a smaller volume, (b) it has no air within it, and (c) mucus secretions back up and collect in the alveoli. Exceptions: sometimes lobar collapse is very rapid and the lobe collapses to a paper thin structure/slice. When this occurs the collapsed lobe will not necessarily be very white. Similarly, longstanding (i.e. chronic) lobar collapse can lead to scarring and contraction of the lobe. The shrivelled lobe may become a small remnant of lung tissue and may not be very white at all. When lung consolidation (i.e. a white area) is associated with lobar collapse then this often signifies very bad news. Obstructive collapse is common and it is always worrying (Table 5.1).
Lung consolidation appears as a white (an extra dense) area on the CXR. The most common cause is pneumonia. A simple pneumonia will not be associated with any major loss of volume in the affected lobe. Lobar collapse: the affected lobe is also usually white…but volume loss will be evident. The whiteness is because: (a) the affected lung tissue occupies a smaller volume, (b) it has no air within it, and (c) mucus secretions back up and collect in the alveoli. Exceptions: sometimes lobar collapse is very rapid and the lobe collapses to a paper thin structure/slice. When this occurs the collapsed lobe will not necessarily be very white. Similarly, longstanding (i.e. chronic) lobar collapse can lead to scarring and contraction of the lobe. The shrivelled lobe may become a small remnant of lung tissue and may not be very white at all. When lung consolidation (i.e. a white area) is associated with lobar collapse then this often signifies very bad news. Obstructive collapse is common and it is always worrying (Table 5.1).Table 5.1 Likely cause of a collapsed lobe by presentation.
| Patient | Likely cause |
|---|---|
| Middle-aged smoker | Bronchial carcinoma |
| Two days after surgery/in the intensive therapy unit | Mucus plug or incorrect position of an endotracheal tube |
| Asthmatic | Mucus plug |
| Toddler/young child | Inhaled foreign body |
TYPES OF COLLAPSE/ATELECTASIS
Three different disease processes represent the most common causes of volume loss (Table 5.2). A fourth type of collapse/atelectasis is also recognised. This is termed adhesive collapse, and occurs in neonatal surfactant deficiency, in adult respiratory distress syndrome, and as a complication of smoke inhalation.
Table 5.2 The common mechanisms causing volume loss.
| Type (also known as) | Examples |
|---|---|
Obstructive (resorptive) 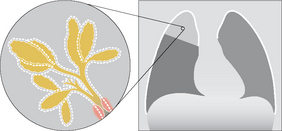 |
Intrinsic occlusion: |
Compressive (passive, relaxation) 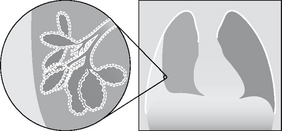 |
Compression by: |
Cicatrisation (fibrotic)  |
Fibrotic contraction due to: |
COLLAPSE ANALYSIS: BASIC ANATOMY
THE NORMAL FISSURES
We need to understand where the normal fissures are positioned.
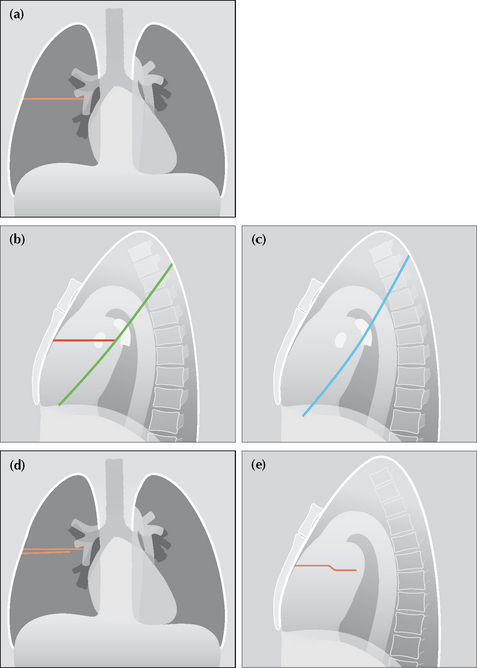
Figure 5.3 Normal fissures. (a) The horizontal fissure in normal position. The fissure is only visible in part or in whole on 67% of normal CXRs (see p. 241). (b) The horizontal and right oblique fissure. (c) The left oblique fissure. (d) Sometimes the horizontal fissure appears as two lines on the frontal CXR (see p. 241). The explanation is shown in (e); the fissure is single but not perfectly horizontal—it has taken a small step, or undulation, in the horizontal plane.
THE NORMAL HILA
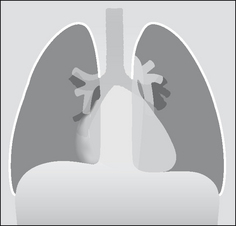
When a lobe collapses this frequently alters the position of the hilum. The one exception is collapse of the middle lobe. So we need to understand how to assess the position of each hilum. Hilar anatomy and position are described in Chapter 6 (pp. 70–73). Figs 5.4-5.6 illustrate the normal hilar appearances. These figures can be used as baseline normals as you evaluate the various examples of lobar collapse that now follow.
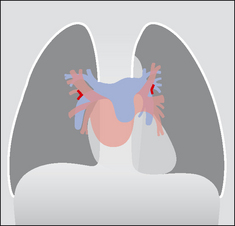
Figure 5.4 The normal hilar shadows. The left hilum is higher than the right in 95% of normal CXRs. In 5% the hila are at the same level. The right hilum is never higher than the left on a normal CXR (see p. 240). The horizontal hila vees (red arrowheads) are explained in Chapter 6, p. 73.

LOBAR COLLAPSE—GENERAL FEATURES
We will concentrate on the most common type of lobar collapse—obstructive.
Will show evidence of volume loss (e.g. displacement of a fissure, hilum, trachea, or mediastinum). Sometimes there will also be elevation of a dome of the diaphragm and/or decreased spacing between the ribs. May show evidence of over-inflation of the adjacent unaffected lobe(s). This compensatory over-inflation can cause hypertransradiancy (i.e. increased blackness) of the ipsilateral hemithorax. Also, the vessels in the over-expanded lobe(s) may be more widely separated compared with the opposite normal lung (Fig. 5.7).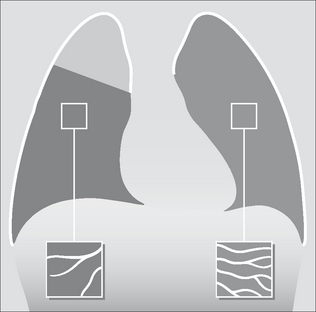
Figure 5.7 Lobar collapse will affect the other lobe(s). The right upper lobe shows partial collapse. The middle and lower lobes over-inflate and as a result often appear slightly blacker than the normal opposite lung. Also, the normal vessels in the over-inflated middle and lower lobes frequently appear more spread out than in a matching area in the opposite normal lung…as shown in the two boxes.
LOBAR COLLAPSE—SPECIFIC FEATURES
COLLAPSE OF THE RIGHT LOWER LOBE
Oblique fissure moves posteriorly and medially. The medial displacement of this fissure causes it to be seen in profile and it forms the lateral edge of a triangular density projected over the heart.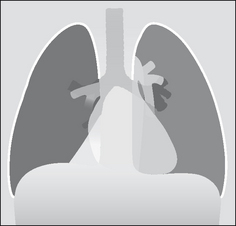
Figure 5.8 Collapsed right lower lobe. The triangular density of the collapsed lower lobe is easy to detect. When the collapse is more severe then it can be much more difficult to recognise because the lobe is tucked in behind the heart against the spine. However, hilar and lower lobe pulmonary artery changes (Fig. 5.12b) will be evident.
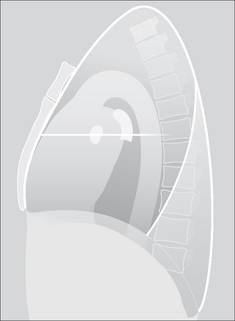
Figure 5.9 Collapsed right lower lobe. The oblique fissure has moved posteriorly and forms the anterior border of the collapsed lobe.
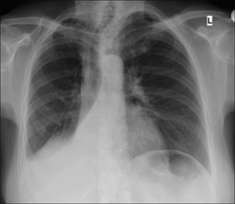
Figure 5.10 Collapsed right lower lobe. Classic triangular shadow. Note the effacement of part of the dome of the diaphragm, and effacement of the adjacent vertebral margin.

Figure 5.11 Major collapse of the right lower lobe. Contrast this CXR with Fig. 5.10. The abnormal features are more subtle. Note that the right lower lobe main pulmonary artery has disappeared (it lies within the collapsed lobe). The remainder of the right lung is hypertransradiant (i.e. blacker than the normal left lung).
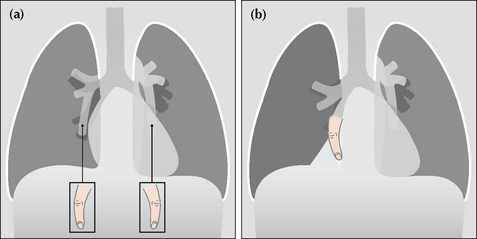
Figure 5.12 The lower lobe pulmonary arteries on each side can be likened to a “little finger”. This is explained on p. 71. When a lower lobe collapses the “little finger” disappears. (a) Normal CXR with “little finger” lower lobe pulmonary arteries visible.(b) Right lower lobe collapse. The right lower lobe pulmonary artery (the “little finger”) is not visible—it is hidden behind the heart within the collapsed lobe.
COLLAPSE OF THE LEFT LOWER LOBE
Oblique fissure moves posteriorly and medially. The medial displacement and rotation of the fissure causes it to be seen in profile and it forms the lateral edge of a triangular density superimposed over the heart.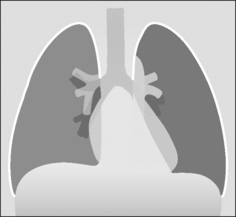
Figure 5.13 Major collapse of the left lower lobe. A triangular density is superimposed over the heart. Note the hypertransradiancy of the overexpanded remaining lung (i.e. the left upper lobe) when compared with the normal right lung.
Figure 5.14 Collapsed left lower lobe. The oblique fissure has moved posteriorly and forms the anterior border of the increased density overlying the vertebral column. Note that the posterior aspect of the left dome of the diaphragm has disappeared (see silhouette sign, p. 45).
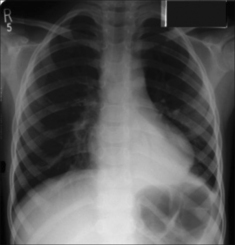
Figure 5.15 Collapse of the left lower lobe. Triangular shadow superimposed over the heart. Left hilum abnormally low compared with the right hilum. The lower lobe pulmonary artery is not identified. Adjacent vertebral margin is indistinct.

Figure 5.16 Collapsed left lower lobe. Left hilum is abnormally low. Increased density overlies the left side of the heart. The lower lobe pulmonary artery is not identified. Part of the outline of the left dome of the diaphragm is effaced.
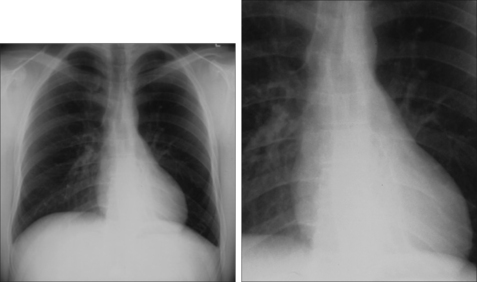
Figure 5.17 Major collapse of the left lower lobe. Detection is more difficult than for Fig. 5.15 because the collapse is nearly total. The crucial signs to note: the left hilum is low and the left lower lobe pulmonary artery is not visible; increased density overlying the heart is evident but subtle.
COLLAPSE OF THE MIDDLE LOBE
Horizontal fissure moves inferiorly.
 NB: this fissure is not always visible. In patients over 50 the fissure was visible in only 67% of normal CXRs (see data in Chapter 16, p. 241). Blurring of the right heart border (Figs 5.18, 5.20 and 5.21). Incidentally the position of the hilum does not alter.
NB: this fissure is not always visible. In patients over 50 the fissure was visible in only 67% of normal CXRs (see data in Chapter 16, p. 241). Blurring of the right heart border (Figs 5.18, 5.20 and 5.21). Incidentally the position of the hilum does not alter.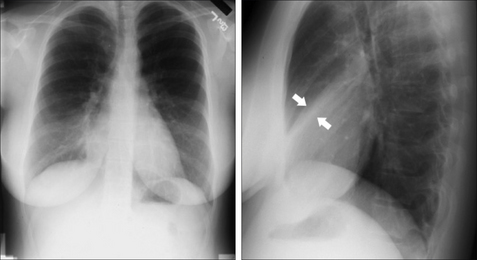
Figure 5.20 Middle lobe collapse is evident when the two views are assessed as a pair. The subtle density (between the arrows) is the collapsed lobe.
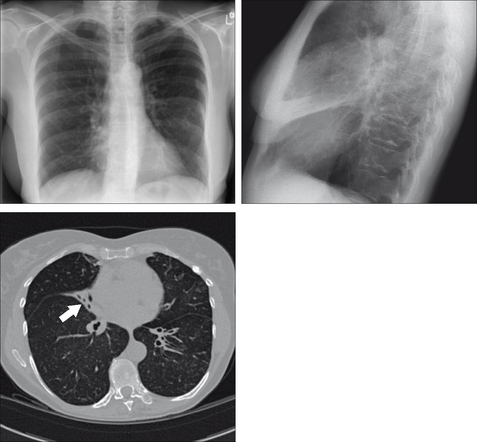
Figure 5.21 Middle lobe collapse. Subtle change on the frontal CXR—a blurred heart border. The lateral CXR shows the white wedge (or slice of cake) of the collapsed middle lobe. The CT section also shows the collapsed lobe (arrow).

COLLAPSE OF THE RIGHT UPPER LOBE
In an adult, look for Golden’s S sign (Fig. 5.22). This will sometimes be present when a tumour at the right hilum is the cause of the lobar collapse. See Chapter 10, pp. 147.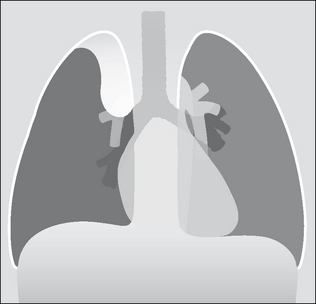
Figure 5.22 Major collapse of the right upper lobe. The collapsed lobe is easy to identify. In this example there is a bulge overlying the elevated right hilum. This bulge is the tumour that has caused the collapse, and this overall appearance is often referred to as Golden’s S sign or the reverse S sign of Golden. In clinical practice the tumour mass is not always evident and the appearance of right upper lobe collapse in Fig. 5.23 is more typical.

COLLAPSE OF THE LEFT UPPER LOBE
The pattern of collapse is very different to that seen with right upper lobe collapse. This is because there is no horizontal fissure on the left side. A most peculiar, but characteristic, appearance results.
A veil-like density covers much of the left hemithorax. This is due to the lack of aeration within the collapsed upper lobe. The Luftsichel sign may be present…i.e. a crescentic lucency around the left side of the aortic knuckle (Fig. 5.26). It is caused by the overexpanded apical segment of the left lower lobe positioning itself between the collapsed upper lobe and the aortic arch.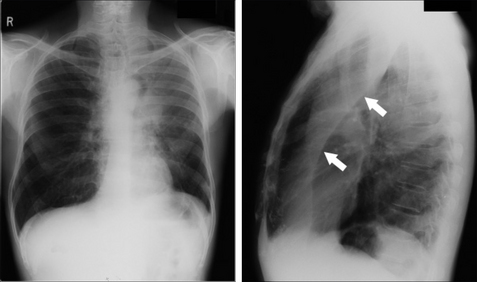
Figure 5.26 Collapse of the left upper lobe. The lateral CXR confirms the diagnosis. The oblique fissure (arrows) is displaced anteriorly. Note: this is the same frontal CXR as Fig. 5.1. The underlying lesion was a bronchial carcinoma. On the frontal CXR the Luftsichel sign is present. On the lateral CXR a lucent (black) area is present. Although it appears to outline the anterior margin of the collapsed lobe, this is a common misconception. This well-defined margin is actually the anterior wall of the ascending aorta outlined by part of the right upper lobe which has herniated across the midline4.
Figure 5.24 Collapse of the left upper lobe. Note the classic features: veil-like opacity overlies the left lung and the left heart border is ill-defined.

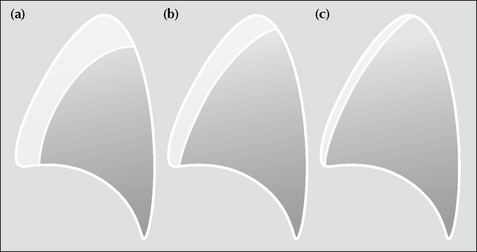
Figure 5.27 Collapse of the left upper lobe can cause slightly different appearances on the lateral CXR. In effect there is a race between the degree of collapse and the build up of secretions in the collapsed lobe. If the collapse occurs slowly then the lobe becomes full of secretions or pus and the collapse is not total—patients (a) and (b). If the bronchial obstruction is nearly complete and occurs quickly, e.g. a mucus plug and some bronchial carcinomas, then the lobe collapses very swiftly and the collapse is total—patient (c).
PITFALLS: BEWARE OF IMPOSTERS
There are various benign appearances that can superficially mimic some of the changes of lobar collapse on the frontal CXR (Table 5.3). Whenever you are in any doubt, always obtain a lateral CXR. The lateral radiograph will confirm whether or not pathology is present.
Table 5.3 Benign appearances which can occasionally be mistaken for lobar collapse.
| Collapse | Imposters |
|---|---|
| Right upper lobe | |
| Middle lobe | |
| Right lower lobe | |
| Left lower lobe | |
| Left upper lobe | …is unique — no impersonators! |
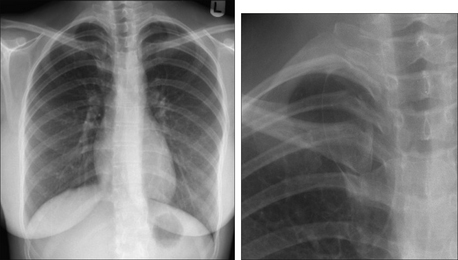
Figure 5.28 An azygos fissure is a common normal variant. It should not be confused with an elevated horizontal fissure. This fissure is formed when the azygos vein crosses the apex of the lung as it passes anteriorly to enter the superior vena cava. As a result of this minor congenital anomaly four layers of pleura are pulled down into the lung by the vein, which creates an azygos fissure.
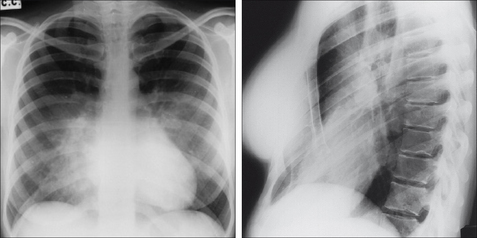
Figure 5.29 The right heart border is effaced, and there is subtle added density suggesting middle lobe consolidation. The lateral CXR shows the depressed sternum which is causing the appearance on the frontal CXR.
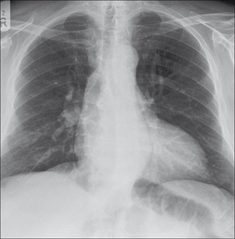
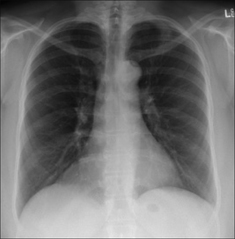
Figure 5.31 A large epicardial fat collection could be misinterpreted as consolidation—or collapse—within the right lower lobe.
Answers to Figs 5.1 and 5.2 on p. 52:
Fig. 5.1: Collapse of the left upper lobe.
Fig. 5.2: Shadowing in the middle lobe…a lateral CXR showed collapse (i.e. fissure displacement) of the lobe.
An interesting condition—Round (or Rounded) Atelectasis5,6
Occurs in patients who have long-standing pleural thickening. It represents an infolding of the visceral pleura around an area of collapsed lung tissue.
Usually an incidental CXR finding. Some, but not all, patients have been exposed to asbestos in the past5. The appearance may be mistaken for a lung tumour.
A mass in contact with a pleural surface, 2.0–5.0 cm in diameter. It may be almost round, or oval, or lobulated, or irregular or even wedge-shaped. May become visible when a pleural effusion starts to absorb. Easily confused with a peripheral bronchial carcinoma.1. Glossary of terms for thoracic radiology: recommendations of the Nomenclature Committee of the Fleischner Society. AJR. 1984;143:509-517.
2. Proto AV, Tocino I. Radiographic manifestations of lobar collapse. Semin Roentgenol. 1980;15:117-173.
3. Woodring JH, Reed JC. Types and mechanisms of pulmonary atelectasis. J Thorac Imaging. 1995;11:92-108.
4. Hansell DM, Armstrong P, Lynch DA, McAdams HP. Imaging of Diseases of the Chest, 4th ed. St Louis, MO: Mosby, 2005.
5. Schneider HJ, Felson B, Gonzalez LL. Rounded atelectasis. AJR. 1980;134:225-232.
6. Carvalho PM, Carr DH. Computer tomography of folded lung. Clin Radiol. 1990;41:86-91.