CHAPTER 23 Pediatric Endodontics
Endodontic Treatment for the Primary and Young Permanent Dentition
Despite the dental profession’s emphasis on prevention, threats to pulp survival such as caries, restorative dental treatment, and traumatic injuries have not been eliminated. As a consequence, children continue to lose teeth prematurely, and procedures aimed at preventing and treating pulp disease in the primary and immature permanent dentitions remain an integral part of contemporary dental practice.
Some may question why efforts to preserve pulpally involved primary teeth are important, since they may present a risk to developing permanent successors and will in any case be lost before long. Preservation of arch space is one of the principal objectives of pediatric dentistry. Premature loss of primary teeth may cause aberration of the arch length, resulting in mesial drift of the permanent teeth and consequent malocclusion. Whenever possible, the tooth with pulp involvement should be maintained within the dental arch in a functional and disease-free condition.
Other objectives of preserving primary teeth are to safeguard esthetics and mastication, prevent aberrant tongue habits, aid in speech, and prevent the psychological effects that may be associated with tooth loss. Premature loss of the maxillary incisors before 3 years of age has been shown to cause speech impairment that may persist in later years.242
It is equally undesirable for children to suffer the unplanned loss of permanent teeth, and it should be noted that the prognosis for lifelong retention of an immature tooth with a short root and fragile dentinal walls is far worse than for a mature permanent tooth. Special treatments for the immature permanent tooth thus focus on preserving pulp vitality, at least until dental development is complete (see also Chapter 16).
This chapter attempts to provide a review of current therapies for the prevention and treatment of pulpal disease in primary and young permanent teeth. The biologic basis of these procedures will be emphasized and supported with clinically relevant evidence to help clinicians preserve functional and disease-free teeth in children.
The Pulp-Dentin Complex in Primary and Young Permanent Teeth
Pulp therapies should be based on an understanding of dental tissues and their innate reaction patterns. Some fundamentals of tissue structure and behavior merit review (see also Chapter 12).
Fundamentals of Dentin/Pulp Histology
The pulps of primary and permanent teeth are histologically and functionally similar.248,249 Odontoblasts are the dentin-forming cells that line the periphery of the pulp chamber and extend their cytoplasmic processes into its tubular structure. They become increasingly crowded as they retreat centrally, and tubular density therefore increases in deep dentin (Fig. 23-1). A cell-free zone is located just below the odontoblastic layer and contains an extensive plexus of nerves (Raschkow’s plexus) and blood capillaries that may support and regulate odontoblast activity and provide sensory innervation to the pulp. Raschkow’s plexus does not fully mature until the late stages of root formation, and pulp sensitivity tests may therefore be inconclusive in immature permanent teeth. Beneath the cell-free zone is the cell-rich zone of Höhl, a band of tissue containing uncommitted cells capable of differentiation into odontoblast-like cells should primary odontoblasts be lost.110 The core of the dental pulp contains larger blood vessels and nerves which are surrounded by loose connective tissue.204 The volume of perfusion through the incomplete apices of immature teeth is considerable and underpins the enormous reparative capacity of young pulps in the face of injury.
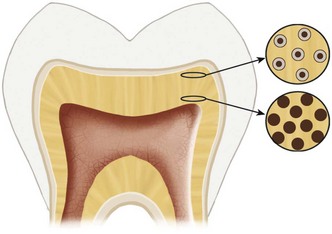
FIG. 23-1 Odontoblasts move closer as they retreat centrally on an ever-diminishing pulp circumference. Deep dentin contains wider and more closely arranged dentinal tubules, making it more porous than superficial dentin.
Chapter 12 provides a more detailed review of tissue structure and functions within the dentin-pulp complex, and Box 23-1 provides relevant key points.
BOX 23-1 The Pulp-Dentin Complex—Key Points of Clinical Relevance
Dentinogenic Response to Injury
Without dentin, the pulp would be a highly sensitive and vulnerable organ, and in the absence of a pulp, the defensive capacity of dentin would be limited. The tissues are therefore inseparable and work together as a functional complex.
Key responses of the dentin-pulp to injury include the deposition of tertiary dentin, which increases the distance between the injury and the pulp, and a reduction in dentin permeability by the formation of sclerotic dentin.309 Chapter 13 further discusses pulpal responses to injury.
The nature and quality of the tertiary dentin depend on its tubular structure and influence local dentin permeability. In the case of a mild injury, the odontoblasts responsible for primary odontogenesis can frequently survive the challenge and are stimulated to secrete tertiary, reactionary dentin (Fig. 23-2) beneath the site of injury.275 Because the original odontoblasts are responsible for this matrix secretion, tubular continuity and communication with the primary dentin matrix will be present [see Fig. 23-2, B; Fig. 23-3, A].184
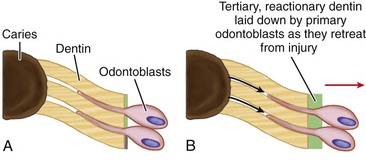
FIG. 23-2 Schematic representation of tertiary reactionary dentin. A, A mild insult to dentin, such as dental caries that does not extend deeply to threaten survival of primary odontoblasts. B, Liberation of dentin matrix components such as TGF-β leads to upregulation of odontoblast activity, with deposition of a reactionary dentin matrix whose tubular pattern is continuous with underlying tissue.
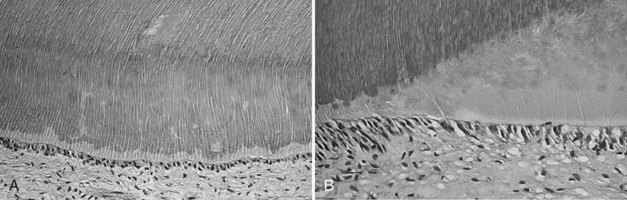
FIG. 23-3 Histologic sections of tertiary reactionary and reparative dentin. A, Reactionary dentin: histologic section showing tubular continuity. B, Reparative dentin: histologic section showing lack of continuity.
(From Pinkham JR, Casamassimo PS, McTigue DJ, et al: Pediatric dentistry: infancy through adolescence, ed 4, St Louis, 2005, Saunders; Courtesy Carlos Alberto S. Costa, DMD, PhD.)
When the injury is severe, as in pulp exposure, the affected odontoblasts may die. Since odontoblasts are postmitotic cells with no capacity for renewal, their replacement must come from elsewhere. If suitable conditions exist in the pulp, a new generation of odontoblast-like cells may differentiate, probably from the cell-rich zone, and secrete a tertiary, reparative dentin matrix (Fig. 23-4). Because this dentin is formed by a new generation of cells, discontinuity in the tubular structure will occur, with a subsequent reduction in tissue permeability (Fig. 23-3, B).31
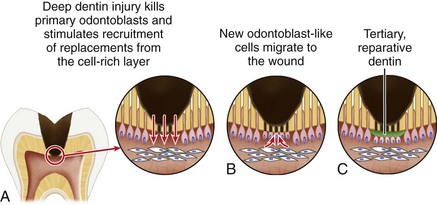
FIG. 23-4 Schematic representation of tertiary reparative dentin. A, A significant insult, such as deep caries, which kills primary odontoblasts in a localized area of pulp. B, New odontoblast-like cells differentiate from cell-rich zone. C, Secretion of a tertiary reparative dentin matrix commences. Tubular structure is irregular and has no continuity with underlying tissue.
A critical question that arises is “What are the factors responsible for triggering the stimulation of odontoblastic activity?” Although much still has to be learned about the molecular control of cell activity in general and odontoblastic activity in particular, one family of growth factors, the transforming growth factor superfamily (specifically TGF-βs)110 has been reported to have extensive effects on the mesenchymal cells of many connective tissues.180
During tooth development, the odontoblasts secrete TGF-βs, and some of them remain sequestered within the dentin matrix. These TGF-βs may be released during any process leading to tissue dissolution, such as dental caries or the use of acid etching.309 Dentin matrix should not be considered an inert dental hard tissue but rather a potential tissue store of a cocktail of bioactive molecules (particularly growth factors) waiting to be released if appropriate tissue conditions prevail.309
In contrast to reactionary responses, reparative dentinogenesis represents a more complex sequence of biologic processes. Migration and differentiation of pulpal progenitor cells must take place, creating a new generation of odontoblast-like cells before matrix secretion. A series of stereotypic wound-healing reactions will occur in the pulpal connective tissue, including vascular and cellular inflammatory reactions.
In vitro and in vivo experiments on reparative odontogenesis demonstrate that the noninflamed pulp constitutes an appropriate environment where competent pulp cells (potential preodontoblasts) can differentiate into new odontoblast-like cells, forming reparative dentin.171,203,212
Reactions to Dental Caries
When the carious process advances from enamel into dentin, sclerotic dentin is formed by the apposition of minerals into and between the dentinal tubules (intratubular and intertubular dentin), and reactionary tertiary dentin is secreted. Sclerotic dentin can be seen in radiographs as a radiopaque area as the aforementioned apposition of minerals increases the radiopacity of this dentin.
The quality and amount of tertiary dentin depend on the depth and rate of progression of the carious lesion. The faster the lesion progresses, the poorer and more irregular the reactionary dentin. In addition, if the noxious irritant is too intense, the cytoplasmic processes of the odontoblasts degenerate, and “dead tracts” are formed.
When the carious process advances more rapidly than the elaboration of reactionary dentin, blood vessels of the pulp dilate, and scattered inflammatory cells become evident, particularly subjacent to the area of the involved dentinal tubules. If the carious lesion remains untreated, a frank exposure will eventually occur. The pulp will react, resulting in an acute inflammatory infiltrate, and the previously chronic pulpitis will become acute. A small abscess may develop under the region of the exposure, and cells of the chronic inflammatory series may accumulate farther away from the central area of irritation. The remainder of the pulp may be uninflamed (chronic partial pulpitis with acute exacerbation). As the exposure progresses, the pulp may undergo partial necrosis, followed in some instances by total necrosis.
Drainage is apparently the factor determining whether partial or total necrosis occurs. If the pulp is open and drainage can occur, the apical tissue may remain uninflamed or chronically inflamed. If drainage is impeded by food packing or a restoration, the entire pulp may become necrotic.110
Reactions to Restorative Procedures
The principal factors affecting the dentin-pulp complex during restorative procedures (e.g., cavity and crown preparation) are the cutting of the dentin, the generation of heat, and the desiccation of the tissue. When uninvolved dentin is operated on, as in extension for prevention or in crown preparation, tubules unprotected by reactionary dentin are cut. The tissue reaction that occurs is similar to that occurring with caries: intratubular and intertubular mineralization takes place, resulting in sclerotic dentin, followed by the formation of tertiary dentin. Remaining dentin thickness (RDT) is apparently the most significant factor determining pulp survival and the secretion of tertiary reactionary dentin. Maximal reactionary dentin was observed in a study wherein the cavity RDT was between 0.5 and 0.25 mm. The reduced reactionary dentin beneath cavities with an RDT below 0.25 mm (described in the same study) appeared to be related to reduced odontoblastic survival.188 In these deep cavities, little more than 50% of the odontoblasts survived, whereas in shallow cavities, odontoblastic survival was about 85% or greater, and despite the cutting of the odontoblastic process, the cells responded by secreting reactionary dentin. The same authors demonstrated that the choice of restorative material influenced the secretion of reactionary dentin to a lesser extent than the RDT. The effect of cutting dentin can be observed histologically as a calciotraumatic band, which represents an interruption of the apposition between the secondary and tertiary dentin.
Pulp reactions to restorative procedures can be mild or severe, depending on the technique used. When the technique is gentle, the reaction will be mild, and minor alterations in the odontoblastic layer can be observed as a result of fluid accumulation. In a severe reaction, the nuclei of the odontoblasts may be aspirated into the dentinal tubules, hemorrhage may be present, and inflammation is extensive, sometimes resulting in cell necrosis. A gentle technique implies using appropriate cooling and minimal pressure. Cutting a cavity without using water cooling might lead to irreversible changes in the pulp because of the heat generated at the tip of the bur. The application of pressure increases the damage. Prolonged air blasts are also deleterious to the pulp. To prevent the generation of heat and damage to the pulp, the following measures should be taken: (1) The cavity preparation should be as shallow as possible, respecting the principles of cavity preparation and embracing contemporary partial and serial caries excavation techniques (see later); (2) suitably sized, sharp burs should be used, balancing the need for conservatism with the risks of localized overcutting with small burs; (3) appropriate cooling should be employed and minimum pressure exerted; and (4) excessive drying of dentin by air syringe should be avoided.226
Reactions to Dental Materials
There is substantial evidence that adverse responses within the dentin-pulp complex to restorative materials are more closely linked with microbial agents than with irritant or toxic components of the materials themselves.22
The routine lining of cavities has long been advocated as a means of pulp protection. Both calcium hydroxide (Ca[OH]2) and zinc oxide eugenol (ZOE) cements have proven track records for promoting pulp health by destroying residual microorganisms in the depths of cavity preparations.14,69,147,153 The antimicrobial and remineralizing potential of glass ionomer cements has been recognized during the last 2 decades,166 and the importance of marginal seal has been supported by evidence on favorable pulp outcomes following bonded composite restorations.42-44,145,277,292
Researchers201 have begun to use the term artificial enamel to describe their aspirations of hybrid-layer formation202 and impervious, pulp-protecting barriers formed by resin-based materials. The response of the pulp to direct contact with dental materials is of special importance in the primary and young permanent teeth of children where pulp capping, pulpotomy, and apexification procedures are important modalities of treatment.
A variety of materials, medicaments, antiseptics, antiinflammatory agents, antibiotics, and enzymes have been used as pulp-capping agents, but Ca(OH)2 has been the standard by which all others were judged.9,58,110 Before 1930, when Hermann115 introduced Ca(OH)2 as a successful pulp-capping agent, pulp therapy consisted of devitalization with arsenic and other fixative agents. Hermann demonstrated the formation of “secondary dentin” (now termed tertiary dentin) over the amputation sites of vital pulps capped with Ca(OH)2.
In 1938, Teuscher and Zander296 introduced Ca(OH)2 in the United States, confirming complete dentinal bridging with healthy radicular pulp under Ca(OH)2 dressings. Further reports firmly established Ca(OH)2 as the pulp-capping agent of choice. After these early works, many studies have reported on various forms of Ca(OH)2, with success rates ranging from 30% to 98%.82 The dissimilar results have been attributed to variables in study design, including the model (human or animal), tooth selection, area of the pulp involved (coronal or cervical), type of Ca(OH)2 employed, outcome criteria, and study duration.
When Ca(OH)2 is applied directly to pulp tissue, necrosis of the adjacent pulp tissue and inflammation of the contiguous tissue occur. Dentin bridge formation occurs at the junction of the necrotic tissue and the vital inflamed tissue. Although Ca(OH)2 works effectively, the exact mechanisms are not fully understood. Compounds of similar alkalinity (pH 11) cause liquefaction necrosis when applied to pulp tissue, but Ca(OH)2 maintains a local state of alkalinity necessary for bone or dentin formation. Beneath the region of coagulation necrosis, cells of the underlying pulp tissue differentiate into odontoblast-like cells and elaborate dentin matrix.110
Occasionally, in spite of successful bridge formation, the pulp remains chronically inflamed or becomes necrotic. Internal resorption may occur after pulp exposure and capping with Ca(OH)2. In other cases, complete mineralization of the remaining pulp tissue occludes the canals and greatly complicates any future attempts at root canal treatment.
It was postulated330 that calcium diffused from a Ca(OH)2 dressing into the pulp to participate in reparative dentin formation. Experiments with radioactive ions, however, have shown that calcium ions from the circulation, not from the Ca(OH)2 pulp cap are involved in bridge formation.16,227,260 Calcium hydroxide promotes bridge formation by creating low-grade irritation in the underlying pulpal tissue, a phenomenon observed even after short-term application and removal of the material.54
Different forms of Ca(OH)2 have produced markedly different responses when applied as a pulp cap.291,305 The reactions to Dycal (DENTSPLY/Caulk, Milford, DE), Prisma VLC Dycal (DENTSPLY/Caulk), Life, and Nu-Cap (GC America, Alsip, IL) have been shown to be similar.279,280,291 The chemically altered tissue created by application of these compounds is resorbed first, and the bridge is then formed in contact with the capping material.302,305 With Ca(OH)2 powder and nonsetting products such as Pulpdent Paste (Pulpdent Corp, Watertown, MA) the bridge forms at the junction of the chemically altered tissue and the remaining subjacent vital pulp tissue. The altered tissue degenerates and disappears, leaving a void between the capping material and the dentin bridge. For this reason, a bridge can be visualized better on radiographs with products such as Pulpdent Paste than with the other commercial compounds. The quality of the dentin bridging was equally good with either material. Investigators have, however, highlighted the frequent occurrence of porosities and tunnel defects in Ca(OH)2-generated dentin bridges.48 A related study47 further demonstrated long-term evidence that Ca(OH)2 becomes softened and allows leakage, resulting in recurrent pulpal inflammation and necrosis after 1 to 2 years. Despite its widespread use, the body of good evidence on Ca(OH)2 pulp capping is surprisingly limited,214 and efforts to improve the body of evidence or develop well-documented alternatives are justified.
Direct Bonding of Pulp Exposures
Although direct bonding of pulp exposures is controversial, it has been advocated by numerous researchers.42,213 This may be explained by investigators45,46 who have demonstrated that immediate and long-term biologic seal are more important to the healing of pulp exposures than the stimulatory effects of any particular wound dressing material. This was revealed graphically in surface-sealing experiments44,45 where severe pulp inflammation followed direct pulp capping with composite, silicate cement, zinc phosphate cement, and amalgam. When similar pulp caps were surface sealed with ZOE to prevent microbial ingress, cell reorganization and dentin bridge formation occurred under the acid cements and composite. Although healing occurred beneath the surface-sealed amalgam, there was no evidence of bridge formation. The conclusion is that in the absence of microbial contamination, the pulp has an inherent healing capacity, with low-grade irritation promoting hard-tissue repair. These findings agree with experiments142,222 on gnotobiotic animals that showed pulpal healing in the absence of bacterial contamination, whereas the introduction of bacteria prevented healing.
Numerous bonding materials and composite resin systems have been tested as pulp-capping agents, with reported healing of the pulp and deposition of hard tissue at the exposure site.4,43-45,106,213,323 Unanimity exists among these researchers that healing does not depend on the material but on its capacity to provide a biologic seal.
Although direct bonding of pulp exposures has gained widespread popularity, it should be noted that no long-range histologic studies have been published. Also, unfavorable effects with direct bonding have been reported. In a comparison of acid-etched, bonded, composite pulp caps, and Dycal, Pameijer and Stanley218 found 45% versus 7% pulpal necrosis and 25% versus 82% dentin bridging, respectively. Another report112 comparing All Bond 2 (Bisco, Schaumburg, IL) with Ca(OH)2 showed persistent inflammatory reactions and hyaline alteration of extracellular matrix inhibiting complete pulpal repair or bridge formation in the bonded specimens. Conversely, the Ca(OH)2 specimens produced complete dentin bridge formation. These results led the authors to conclude that direct bonding is not recommended for human pulp, and vital pulp therapy using acidic agents and adhesive resins is contraindicated.
This remains a controversial area with no universally-adopted conclusions. However, the advent of new materials such as mineral trioxide aggregate (MTA) offer much promise in pulp capping and may make the debates over bonded pulp caps academic.
Mineral Trioxide Aggregate
Favorable pulp responses have been reported following the use of MTA.1,140,198,200,228 When compared with Ca(OH)2, MTA produced significantly more dentinal bridging in a shorter period of time with significantly less pulpal inflammation. Dentin deposition also began earlier with MTA.
MTA is a biocompatible material with an antibacterial effect similar to that of Ca(OH)2 and the property of providing a biologically active substrate for cell attachment. This feature makes it effective in preventing microleakage and improving the prognosis of treatment. MTA has been shown to promote pulp healing with dentin bridge formation and minimal inflammatory reaction in exposed pulps in monkeys228 and humans,200 and its dentinogenic effect in short-term capping experiments was demonstrated in dogs.71 The material was approved for use by the United States Food and Drug Association (FDA). Following promising preliminary studies,2 it has been shown to provide impressive results for pulp capping (Fig. 23-5) and pulpotomy treatments in young permanent teeth27,326 and for pulpotomies in the primary dentition.3,63
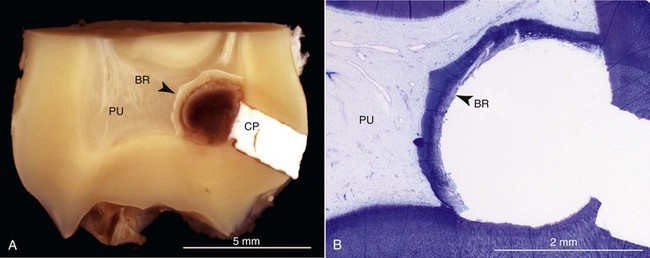
FIG. 23-5 Pulpal response to mineral trioxide aggregate (MTA) capping after 3 months observation. Distal macrophotographic view of the mesial half of a maxillary left third molar (tooth 28 [FDI]) shows remnants of restorative and capping material (CP) and a distinct hard-tissue bridge (BR) across the exposed pulp (PU). The photomicrograph (B) is part of a histologic section of the specimen in (A). Note mineralized hard-tissue barrier (BR) stretching across full length of exposed pulp (B).
(Reproduced from Nair PNR, Duncan HF, Pitt Ford TR, Luder HU: Histological, ultrastructural and quantitative investigations on the response of healthy human pulps to experimental capping with mineral trioxide aggregate: a randomised controlled trial. Int Endod J 41:128, 2008.)
Differences in Primary and Permanent Tooth Morphology
Successful pulpal therapy in the primary dentition requires a thorough understanding of primary pulp morphology, root formation, and the special features associated with physiologic resorption of primary tooth roots. These factors are considered in the following sections.
According to Finn78 and Nelson and Ash,205 there are 12 basic differences between primary and permanent teeth (Fig. 23-6):

FIG. 23-6 Cross section of primary and permanent molars. Divergence of the primary molar roots allows space for the developing permanent premolar.
Root Formation
According to Orban,215 development of the roots begins after enamel and dentin formation has reached the future cementoenamel junction (CEJ). The epithelial dental organ forms Hertwig’s epithelial root sheath, which initiates formation and molds the shape of the roots. Hertwig’s sheath takes the form of one or more epithelial tubes (depending on the number of roots of the tooth, one tube for each root). During root formation, the apical foramen of each root has a wide opening limited by the epithelial diaphragm. The dentinal walls diverge apically, and the shape of the pulp canal is like a wide-open tube. Each root contains one canal at this time, and the number of canals is the same as the number of roots (Fig. 23-7, A). When root length is established, the sheath disappears, but dentin deposition continues internally within the roots.
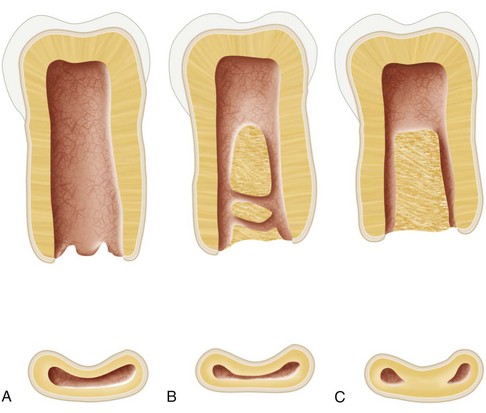
FIG. 23-7 Faciolingual cross section of the mesial root of a mandibular primary molar. A, Formation of the root at the time the root length is completed; only one canal is present. B, Differentiation of the root into separate canals by the continued deposition of dentin (shaded areas). Small fins and branches are present between the two canals. C, Canals are completely divided; root resorption has begun.
Differentiation of a root into separate canals, as in the mesial root of the mandibular molars, occurs by continued deposition of dentin. This narrows the isthmus between the walls of the canals and continues until there is formation of dentin islands within the root canal and eventual division of the root into separate canals. During the process, communications exist between the canals as an isthmus and then as fins connecting the canals (Fig. 23-7, B). (See Chapter 12 for a complete description of pulp and dentin formation.)
As growth proceeds, the root canal is narrowed by continued deposition of dentin, and the pulp tissue is compressed. Additional deposition of dentin and cementum closes the apex of the tooth and creates the apical convergence of the root canals common to the completely formed tooth (Fig. 23-7, C).
Root length is not completed until 1 to 4 years after a tooth erupts into the oral cavity. In the primary dentition, root length is completed in a shorter period of time than in the permanent tooth because of the shorter length of the primary roots.
The root-to-crown ratio of the primary teeth is greater than that of the permanent teeth. The primary roots are narrower than the permanent roots. The roots of the primary molars diverge more than those of the permanent teeth. This feature allows more room for the development of the crown of the succeeding premolar (see Fig. 23-6).204
The primary tooth is unique insofar as resorption of the roots begins soon after formation of the root length has been completed. At this time, the morphology of the root canals roughly corresponds to the form and shape of the external anatomy of the teeth. Root resorption and the deposition of additional dentin within the root canal system, however, significantly change the number, size, and shape of the root canals within the primary tooth. A more detailed description of how this affects the primary teeth is presented later in this section.
It should be noted that most variations within the root canals of primary and permanent teeth are in the faciolingual plane; dental radiographs do not visualize this plane but show the mesiodistal plane. Therefore, when reviewing clinical radiographs, many of the variations that may be present are not visible. Figs. 23-8 and 23-9 show silicone models of root canals, and Fig. 23-10 shows a reconstructed digital image to illustrate morphology not visible with plain radiographs. The increasing availability of three-dimensional imaging techniques such as cone-beam computerized tomography221 is bringing greater understanding of such anatomic features to practicing clinicians.
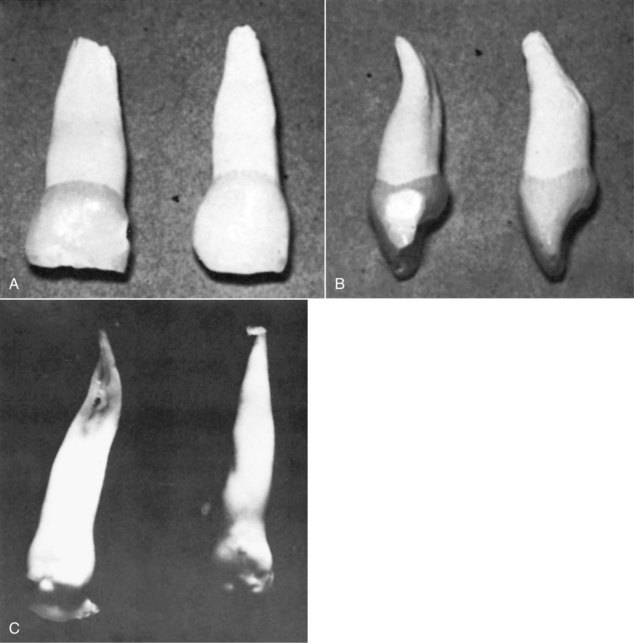
FIG. 23-8 Primary central incisors and silicone models of pulp canals. A, Facial surfaces. B, Beginning resorption of roots on apical third of lingual surfaces. C, Models. Pulp canals were injected with silicone, and the tooth structure decalcified away, leaving a model of the root canal systems. Note division of the canal in model on left.
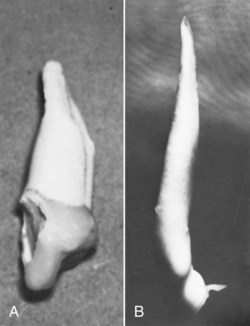
FIG. 23-9 Maxillary primary canine and silicone model of the root canal. A, Mesial surface. B, Model of the root canal.
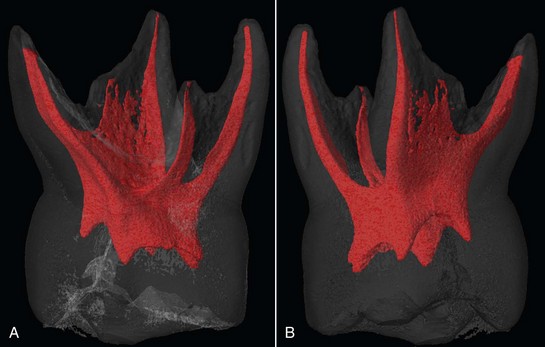
FIG. 23-10 Three-dimensional tomographic images of a maxillary second primary molar. A, Mesial view of primary molar with four root canals. Note the fins of pulp tissue between distofacial and palatal canals. B, Same tooth from the distal view. Note wide area of pulp tissue connection between distofacial and palatal canals.
(Courtesy Paul Dummer and Sue Bryant, Cardiff University, UK.)
Primary Root Canal Anatomy
To treat the pulps of primary teeth successfully, the clinician must have a thorough knowledge of the anatomy of the primary root canal systems and the variations that exist within them.205 To understand some of the variations in the primary root canal systems requires an understanding of root formation (see previous discussion and Box 23-2).
Primary Anterior Teeth
The morphology of root canals in primary anterior teeth resembles the form and shape of the roots of the teeth themselves (see Figs. 23-8 and 23-9). The permanent tooth bud lies lingual and apical to the primary anterior tooth, so physiologic root resorption of primary incisors and canines begins on the lingual aspect of the apical third of the roots (see Fig. 23-8, A).
Maxillary Incisors
The root canals of maxillary primary incisors are almost round in cross section but somewhat compressed in a faciolingual direction. Commonly these teeth have one canal without bifurcations. Apical ramifications and accessory and lateral canals are rare but may occur (see Fig. 23-8).331
Mandibular Incisors
The root canals of primary mandibular incisors are flattened on the mesial and distal surfaces and are sometimes grooved, progressing in an apical direction to an eventual division into two canals (facial and lingual). The presence of two canals is seen less than 10% of the time. Occasionally, lateral or accessory canals are observed.331
Maxillary and Mandibular Canines
The root canals of primary maxillary and mandibular canines correspond to the exterior root shape: a rounded, triangular shape with the base toward the facial surface. Sometimes the lumen of the root canal is compressed in the mesiodistal dimension. The canines have the simplest root canal systems of all the primary teeth and offer few challenges during endodontic treatment. Bifurcation of the canal does not normally occur. Lateral canals and accessory canals are rare (see Fig. 23-9).331
Primary Molars
Often, primary molars have the same number and position of roots as the corresponding permanent molars (see Fig. 23-10). Maxillary molars have three roots, two facial and one palatal; mandibular molars have two roots, mesial and distal. The roots of the primary molars are long and slender compared with crown length and width, and they diverge to allow for permanent tooth bud formation.
When full-length root formation has just been completed in the primary molars, only one root canal is present in each of the roots. The continued deposition of dentin internally may divide the root into two or more canals. During this process, communications exist between the canals and may remain in the fully developed primary tooth as isthmi or fins connecting the canals (see Fig. 23-7, B and Fig. 23-10).
In primary teeth, the deposition of secondary dentin has been reported to occur after root-length completion.24,117,134 This may result in changes to the basic root canal morphology, producing variations and alterations in the number and size of the root canals. This deposition begins at about the time root resorption begins. Variations in form are more pronounced in teeth that show evidence of root resorption.117
Greatest variation in morphology of the root canals occurs in the mesial roots of maxillary and mandibular primary molars. This variation originates in the apical region as a thinning of the narrow isthmus between the facial and lingual extremities of the apical pulp canals. Subsequent deposition of secondary dentin may produce complete separation of the root canal into two or more individual canals. Many fine connecting branches or lateral fibrils form a connecting network between the facial and lingual aspects of the root canals (see Fig. 23-10).
The variations found in the mesial roots of the primary molars are also found in the distal and lingual roots but to a lesser degree. Accessory canals, lateral canals, and apical ramifications of the pulp are common in primary molars, occurring in 10% to 20%.117,331
In the primary molars, resorption usually begins on the inner surfaces of the roots next to the interradicular septum. The effects of resorption on canal anatomy and root canal filling on the primary teeth are discussed in detail later in this chapter.
Maxillary First Primary Molar
The maxillary first primary molar has two to four canals that correspond approximately to the exterior root form, with much variation. Usually, the palatal root is round and often longer than the two facial roots. Bifurcation of the mesiofacial root into two canals is common and occurs in approximately 75% of maxillary first primary molars.204,331
Fusion of the palatal and distofacial roots occurs in approximately a third of maxillary primary first molars. In most of these teeth, two separate canals are present, with a very narrow isthmus connecting them. Islands of dentin may exist between the canals, with many connecting branches and fibrils.
Maxillary Second Primary Molar
The maxillary second primary molar has two to five canals roughly corresponding to the exterior root shape. The mesiofacial root usually bifurcates or contains two distinct canals. This occurs in approximately 85% to 95% of maxillary second primary molars.117,331
Fusion of the palatal and distofacial roots may occur. These fused roots may have a common canal, two distinct canals, or two canals with a narrow connecting isthmus of dentin islands between them and many connecting branches or fibrils.
Mandibular First Primary Molar
The mandibular first primary molar usually has three canals, again corresponding approximately to the external root anatomy, but it may have two to four canals. It is reported that approximately 75% of the mesial roots contain two canals, whereas only 25% of the distal roots contain more than one canal.117,331
Clinical Pulpal Diagnosis in Children
Restorative dental treatment should never commence without a working diagnosis and treatment plan. Chapter 1 provides a comprehensive account of diagnostic procedures, but certain points demand emphasis for the child patient. As always, the diagnostic process should follow an orderly pattern, with attention to the medical and dental history, clinical examination, and special tests, including radiographs where appropriate. Parents or caregivers may be helpful in clarifying the case history and may need to be involved if any systemic condition is likely to influence clinical management. The medicolegal dimensions of careful history taking, diagnostic procedures, and case documentation should also be recognized.
Every effort should be made to establish a working pulp diagnosis before anesthetizing the suspect tooth and isolating it with a rubber dam. These conditions are rarely conducive to accurate history taking or diagnostic reliability, especially in young children. The opportunity should also be taken before treatment to discuss contingent alternatives that may become necessary as a result of an unexpected event, such as the exposure of a pulp during deep caries excavation.
Established tests to determine the extent of pulpal inflammation are crude at the best of times and may be of little or no value in young and anxious children and on primary or immature permanent teeth. The literature on pulp diagnosis in children is mostly outcome reports based on empirical treatment and anecdotal case reports. Assumptions regarding pulpal status prior to treatment have often been based on retrospective findings rather than histologic or microbiologic data to support the prerestorative diagnosis. Histologic investigation remains the only true method of determining the nature and extent of pulp inflammation, and any correlation with clinical signs and symptoms is limited.58,176,282
Although every effort should be made to discern the condition of the pulp before treatment, exhaustive pulp provocation tests may not be helpful in children. From a clinical standpoint, the characteristics of the presenting pain are often critical to the working diagnosis, especially when summated with additional information from the clinical and radiographic examination. Further evidence can be provided by clinical observations during the procedure, such as the nature, volume and ability to control hemorrhage from an exposed pulp. It should be recognized that pulp diagnosis in children is as much an art as a science.
History and Characteristics of Pain
The character of any presenting pain is first identified in the history. Distinction should, wherever possible, be made between provoked and spontaneous pain.
Provoked pain is usually triggered by a thermal or osmotic stimulus (e.g., cold drinks, eating candy) and usually ceases when the stimulus is removed. This history is indicative of minor, reversible pulp inflammation. Provoked pain may sometimes be confused with that caused by interproximal impaction of food (Fig. 23-11), soreness associated with tooth exfoliation, or eruption of permanent teeth.
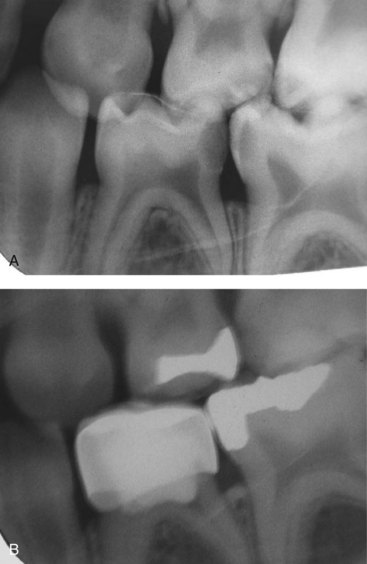
FIG. 23-11 Pain and bone loss caused by food impaction in interproximal space between primary molars. A, First and second mandibular primary molars with caries and marginal bone loss caused by food impaction. B, Healthy bone after restoration of teeth.
By contrast, spontaneous pain is not consistently associated with an external stimulus, may arise at any time of the day, or wake the child from sleep. In both primary and young permanent teeth, spontaneous pain and provoked pain which continues long after the causative factor is withdrawn are usually associated with extensive, irreversible pulpal inflammation extending into the root canals.105 Primary teeth with a history of spontaneous toothache are unreliable candidates for vital pulp therapy and should not be considered for any form of treatment short of pulpectomy or extraction. The situation is quite different for immature permanent teeth. Since the consequences of losing vital pulp functions are so serious, immature permanent teeth with a similar pain history should always be considered for pulpotomy, apexogenesis, or even regenerative techniques in an effort to safeguard tooth development (see later sections on immature permanent teeth).
Clinicians faced with an apparently graphic pain history should not, however, neglect to conduct a proper clinical examination, since other conditions such as papillitis caused by interproximal food impaction may mimic pulpitic pain.
Equally, the absence of pain should not encourage clinical complacency, since varying degrees of pulp degeneration or even complete necrosis can be encountered without any report of pain. Children may thus present without any complaint, despite extensive carious lesions and draining parules. Those who have developed early childhood caries (e.g., nursing bottle caries), may equally have no experience of their teeth feeling any other way and have no special pain history to report.226
Clinical Examination
A careful extraoral and intraoral examination is of great importance in identifying teeth with pulpal involvement. Signs such as tooth discoloration, gross caries, redness and swelling of the vestibulum, or draining parules may strongly suggest pulpal pathoses. In addition, attention should be paid to teeth with extensive fractured and missing restorations or restorations with carious marginal breakdown. All may indicate involvement of the pulp through the relatively thin and porous dentin of the cavity floor.
Palpation, Percussion, and Mobility
Fluctuation, felt by palpating a swollen mucobuccal fold, may be the expression of an acute dentoalveolar abscess before exteriorization. Bone destruction following a chronic dentoalveolar abscess can also be detected by palpation.
Though significant inflammatory bone loss can make primary teeth mobile, this is not a reliable, objective test of pulpal status. Teeth with varying degrees of pulpal inflammation may have very little mobility, whereas mobility can be significant during phases of active physiologic root resorption in primary teeth with healthy pulps.
Comparing the mobility of a suspicious tooth with its ipsilateral equivalent can be especially helpful in clarifying such quandaries. If a significant difference in mobility is noted, this along with other diagnostic information may suggest pulpal inflammation.
Sensitivity to percussion may reveal a painful tooth in which pulpal breakdown has resulted in acute periradicular periodontitis. Exceptions include recently traumatized teeth. Care should be taken in percussing the teeth of children; one author226 has recommended the gentle use of a fingertip rather than the end of a dental mirror.
Pulp Tests
Standard electrical and thermal pulp provocation tests are of limited value in the primary dentition and in young permanent teeth with incompletely developed apices.9 Although these tests may indicate the presence of some vital responsive tissue, they will not give reliable data on the extent of pulpal inflammation. Many children with perfectly normal teeth do not respond to the electrical pulp tester even at the higher settings. Equally, young patients may give unreliable responses to such provocation tests because of apprehension, fear, or general management problems.
The unreliability of electronic methods in immature permanent teeth has been reported in several studies.91,92,94,148 One author148 showed responses ranging from 11% in 6- to 11-year-olds with completely open apices to 79% in older children with complete root formation.
Thermal tests may be more reliable than electrical methods for ascertaining the presence of vital responsive tissue in immature permanent teeth, and carbon dioxide snow has been shown to be more effective than ice and ethyl chloride.91,92,94,148 Heat is unreliable as a diagnostic test in young children.92
Laser Doppler flowmetry has been reported68,272,328 to be reliable for diagnosing pulpal vitality in immature permanent teeth, but the equipment has not been perfected for clinical use68 and is cost prohibitive. It is also affected by blood pigmentation in discolored crowns.
Radiographic Examination
Clinical examination should be supplemented where appropriate with high-quality radiographs. Interradicular radiolucencies, a common finding in primary posterior teeth with pulpal pathoses, are best observed in bite-wing radiographs. If the apical area cannot be clearly observed, a periapical view should be obtained, exposed on a small film by a paralleling technique. The integrity of the lamina dura of the affected tooth should be compared with that of adjacent or contralateral teeth.226
Current radiographs are essential in examining for caries, restoration integrity, previous endodontic treatments, and resorptive and periapical changes in primary and young permanent teeth. In children, interpretation of radiographs is complicated by physiologic root resorption of primary teeth and incompletely formed roots of permanent teeth. If the clinician is not familiar with interpreting radiographs of children or does not have radiographs of good quality, these normal conditions can easily be misinterpreted as pathologic changes in need of treatment. In the case of immature permanent teeth, comparison of root formation with the antimere should always be considered.
The radiograph does not always demonstrate periapical pathosis, nor can the proximity of caries to the pulp always be accurately determined. What may appear as an intact barrier of secondary or tertiary dentin overlying the pulp may actually be a perforated mass of irregularly calcified and carious dentin overlying a pulp with extensive inflammation.58
The presence of calcified masses within the pulp is an important diagnostic sign (Fig. 23-12). Mild, chronic irritation to the pulp stimulates tertiary reactionary dentin formation. When the irritation is acute and of rapid onset, the defense mechanism may not have a chance to lay down reactionary dentin. When the disease process reaches the pulp, the pulp may form calcified masses away from the exposure site. These calcified masses can be associated with degeneration of the coronal pulp and inflammation of the radicular pulp in primary teeth.58 In the absence of other clinical evidence, it is unclear whether this warrants invasive treatment in all cases. Certainly for immature permanent teeth, the presence of calcific metamorphosis within the coronal pulp chamber would not in isolation warrant pulpectomy and root canal treatment.

FIG. 23-12 Calcified mass in the pulp chamber. There is internal and external root resorption. Calcified mass (arrow) is an attempt to block a massive carious lesion. Because of resorption, this tooth should be extracted. Note bone loss in the bifurcation area.
Pathologic changes in the periapical tissues surrounding primary molars are most often apparent in the bifurcation or trifurcation areas rather than at the apices (as generally seen in permanent teeth) (see Fig. 23-12). Pathologic bone and root resorption indicates advanced pulpal degeneration that has spread into the periapical tissues. The pulpal tissue may remain vital even with such advanced degenerative changes. Periapical radiolucencies of primary anterior teeth, like those in permanent teeth, are usually at the apices.
Internal resorption occurs frequently in the primary dentition after pulpal involvement. It is always associated with extensive inflammation,105 and it usually occurs in the molar root canals adjacent to the bifurcation or trifurcation area. Because of the thinness of primary molar roots, once the internal resorption has become advanced enough to be seen on radiographs, there is usually a perforation of the root by the resorption (Fig. 23-13). In some instances, however, the process is reversible and self-correcting, and the resorbed area becomes filled with mineralized tissue.110,219 If a perforation of the root occurs in a primary tooth because of internal resorption, all forms of pulp therapy are contraindicated. The treatment of choice is observation (if the area of the resorption is confined to the tooth) or extraction (if the process has reached the bone).110,219
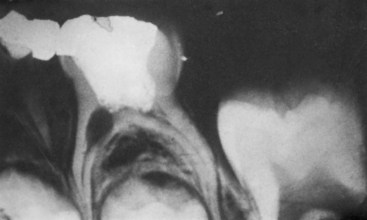
FIG. 23-13 Pulpotomy failure. Note internal resorption that has perforated the pulp chamber floor and resulted in a furcal radiolucency.
In immature permanent teeth, it is often difficult to assess the extent of apical closure. Plain-film images are frequently misleading, since under normal conditions, they show the mesiodistal plane of the tooth but give little information in the faciolingual dimension. Except for the maxillary central and lateral incisor, all other root canals of the permanent teeth are wider in the faciolingual plane than the mesiodistal. The faciolingual aspect of the root canal is two to three times as wide as the mesiodistal width and is the last to become convergent apically as the root develops. Therefore it is possible to have a dental radiograph showing an apically convergent root canal, whereas in the faciolingual plane, the root canal is divergent. Equally, canals which are apically diverging in the faciolingual view may be parallel or converging in the mesiodistal view. Again, contemporary three-dimensional imaging techniques are beginning to improve understanding, both in the research laboratory (Fig. 23-14) and in the clinic.221
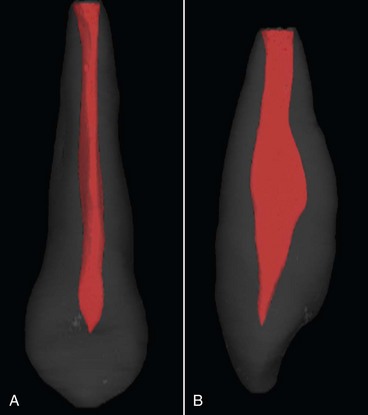
FIG. 23-14 Three-dimensional tomographic images of an immature maxillary canine. A, Faciolingual view. B, Mesiodistal view. Such imaging techniques are bringing new anatomic awareness to both the research laboratory and the clinic.
(Courtesy Paul Dummer and Sue Bryant, Cardiff University, UK.)
In summary, radiographs add to the diagnostic process by visualizing the presence or absence of:
It is important to emphasize once again that the clinician should be familiar with the normal factors that complicate interpretation of radiographs in children: larger bone marrow spaces, superimposition of developing tooth buds, normal resorption patterns of the teeth, and immature root apices.226
Restorative Diagnosis: Pulpal Exposures and Hemorrhage
It has been reported that the size of the exposure, the appearance of the pulp, and the color and amount of hemorrhage are important factors in diagnosing the extent of inflammation in a pulp exposed by caries. The presence of excessive58,226,282 or deep purple colored226 hemorrhage from an exposed or amputated pulp is evidence of extensive inflammation in both primary and young permanent teeth. A true carious exposure is always accompanied by pulpal inflammation (see Chapter 13),58,282 and even a pinpoint carious exposure can be associated with pulpal inflammation ranging from minimal to extensive or even complete necrosis. However, massive exposure in primary teeth is always associated with widespread inflammation or necrosis and makes the tooth a poor candidate for any form of vital pulp therapy. This rule does not apply for young permanent teeth with incomplete root development, where the premature loss of vital pulp functions is so catastrophic that every effort should be made to safeguard tooth development. (See later section on the management of pulpal exposure in immature permanent teeth.)
Sometimes a final working diagnosis can be reached only by direct evaluation of the pulp tissue, and a decision about treatment is made accordingly. For example, if a pulpotomy is planned in a primary molar, the nature of the bleeding from the amputation site should be normal, and hemostasis should be evident after 2 to 3 minutes of light pressure with a moistened cotton pellet. Significant bleeding beyond this point indicates inflammation of the radicular pulp, and a more radical treatment such as pulpectomy or extraction should be considered. Conversely, if a pulp polyp is present and bleeding stops normally after coronal pulp amputation, a pulpotomy may be performed instead of a more radical procedure.226
In the case of an immature permanent tooth, persistent hemorrhage after several minutes of sodium hypochlorite application is an indication of serious pulp inflammation, and a tooth initially scheduled for a direct MTA pulp cap may be a better candidate for a pulpotomy, apexification, or pulp regeneration (see later section on immature permanent teeth).
Investigators105 attempted to use the first drop of hemorrhage from an exposed pulp site as a diagnostic aid for determining the extent of degeneration within the pulp. A white blood cell differential count (i.e., hemogram) was made for each of 53 teeth included in the study. A detailed history, including percussion, electrical pulp test, thermal tests, mobility, and history of pain, was obtained. The teeth were extracted and histologically examined. On correlation of the histologic findings with the hemogram and history, it was determined that percussion, electrical and thermal pulp tests, and mobility were unreliable in establishing the degree of pulpal inflammation. The hemogram did not give reliable evidence of pulpal degeneration, although teeth with advanced degeneration of the pulp involving the root canals did have an elevated neutrophil count. A consistent finding of the study, however, was advanced degeneration of pulpal tissue in teeth with a history of spontaneous toothache.
The outward clinical signs of inflammation represent a succession of cellular, vascular, and immunologic processes involving many endogenous mediators. Inflammatory mediators (vascular-mediated and cell-released) and their role in pulpal inflammation have been the subject of much research. The relationship between the concentration of a known cell-released inflammatory mediator (prostaglandin E2 [PGE2]) in pulpal blood samples and treatment outcome following vital pulpotomy in extensively carious primary molars has been reported.319 Thirty-nine primary molars with no history of spontaneous pain had blood samples harvested from the radicular pulp stumps immediately following coronal pulp amputation. Enzyme immunoassay of the samples for PGE2 detected the inflammatory mediator in all samples. A wide range of concentrations was detected, and it was shown that the concentration of PGE2 detected correlated positively with radiologic signs of failure following treatment. The authors tempered their findings by describing the dependence upon a single inflammatory mediator to predict prognosis as oversimplistic and suggested the “trauma” of pulp amputation would stimulate prostaglandin production irrespective of the underlying inflammatory status of the tissue. Similarly, a rapid and low-cost, chairside diagnostic kit to assess the extent of pulp inflammation does not yet exist. Therefore, despite research in this area, clinicians still rely upon empirical clinical findings to diagnose the inflammatory status of the pulp.
Diagnosis Following Traumatic Injuries in Children
The details of trauma management are considered in Chapter 17. Injuries to the primary dentition are common, occurring in 1 in 3 children by the age of 5 years.11,99 Diagnosis following traumatic injuries requires consideration of other factors in addition to those previously discussed. The most frequent injury in the primary dentition is tooth displacement due to less dense bone and shorter roots. Healing varies from normal without sequela to canal calcification or pulpal necrosis. Canal calcification may vary from an amorphous material resembling osteodentin to a partial or complete closure of the canal.121,247
Pulp Diagnosis and Treatment Planning After Trauma
Treatment guidelines are almost nonexistent concerning healing and complications following trauma in primary teeth. The literature is devoid of histologic or microbiologic studies in this area. Borum and Andreasen29 in a study of 545 traumatized primary maxillary incisors found that 53% developed pulpal necrosis, and 25% developed canal obliteration. The age of the patient, degree of tooth displacement, concurrent crown fracture, and amount of root resorption were factors influencing pulpal necrosis and calcification. Teeth with a coronal fracture were less likely to suffer calcific obliteration of the root canal than those which had been luxated.
When making a decision upon treatment, the proximity of the primary tooth to the permanent successor is an important consideration. Treatment least likely to damage the permanent tooth should be chosen.9,29 Studies present conflicting data on the merits of treating or extracting traumatized primary teeth. Some have suggested no relationship,11,12 others have shown more extensive developmental disturbances if the primary tooth is treated and preserved.266
Transient or permanent discoloration of the crown occurs in approximately 50% of traumatized primary incisors, varying from yellow to dark gray and usually becoming evident in 1 to 3 weeks. The yellow discolorations are frequently associated with canal calcification but are not commonly associated with pulp necrosis.29,125
Pulpal necrosis ranging from 50% to 82% is reported29,120,125,263 in traumatized primary incisors with dark gray discoloration, compared to 25% in those with no discoloration. One author49 points out that color change in the absence of other clinical findings is unreliable. Diagnosis of pulpal necrosis is usually based on dark gray color and radiographic evidence of periapical pathology or cessation of root development.
In immature permanent teeth, discoloration of the crown is also one of the best diagnostic indicators after traumatic injuries.130,136 Yellow or brown-tinted discoloration usually indicates calcification of the pulp space; a gray color is usually associated with pulpal necrosis. A return to normal after transient coronal discoloration8,38 and transient apical breakdown up to 4 months’ duration38 have been reported.
Principles of Endodontic Treatment in Children
Endodontic procedures are undertaken to preserve teeth in a comfortable, functional, and ideally disease-free condition. The following sections describe a range of clinical procedures which aim to achieve these goals in the primary and young permanent dentitions, but they should not be seen merely as technical exercises. Readers should bear in mind that clinical management goes beyond the simple restorative procedure. The general care of anything from a preschool child requiring pulp therapy on a carious primary molar to an 8-year-old who has sustained trauma to an immature maxillary incisor requires special skills. In purely dental terms, the principle adopted is that the best root filling is a healthy pulp, and emphasis is given to methods of pulp preservation in both the primary and young permanent dentitions. Pulpotomy techniques for the partial preservation of pulp tissue are also presented as legitimate therapies—in primary teeth where young and well-perfused tissues combine with the relatively transient nature of the dentition to win success, and in young permanent teeth where therapies strive to maintain the well-perfused and resilient apical pulp, at least until root formation is complete. None of this diminishes the potential for pulpectomy and root canal treatment, should this become necessary, but as new opportunities open for regenerative therapies, traditional approaches to the root canal treatment of pulpless immature teeth may be coming into question.
Pulp Therapy for the Primary Dentition
Indirect Pulp Therapy in Primary Teeth
Indirect pulp treatment (IPT) in the primary dentition is considered a contemporary, effective approach to a deep carious lesion in the absence of signs or symptoms of irreversible pulp pathosis.265 It involves the removal of caries to leave a layer of stained dentin at the cavity floor in areas where its removal would result in exposure of pulp tissue. A decision to use this treatment is derived from clinical and radiographic examination, direct evaluation of the cavity preparation, and a good knowledge of tooth anatomy and the caries process.14
The aims of IPT are250 to arrest the carious process, provide conditions conducive to the formation of reactionary dentin, and promote remineralization of the altered dentin that was left. This in turn is expected to promote pulpal healing and preserve/maintain the vitality of the pulp.
Technique
In outline, the clinical steps involved may be divided into stages involving partial caries removal, placement of an antibacterial agent, and restoration of the crown in a way that provides optimum coronal seal.
Some studies using IPT in primary teeth advocated a two-stage approach.70,305 After initial partial caries removal without local anesthetic, the cavity was restored for 1 to 3 months, using a reinforced ZOE cement or glass ionomer restoration. Following this, further caries removal and definitive restoration was undertaken using local anesthetic. It has been suggested that this approach may have a use in the very young or very anxious child, but it may be argued that a single-visit approach is more appropriate and successful.72 Thinner dentin in the primary tooth compared with the permanent tooth may result in a higher risk of pulp exposure if a primary tooth is reentered to remove residual caries.278
The following technique is based upon a recommended approach250:
Unfortunately, there is presently insufficient evidence to promote a definitive choice for the lining material placed over the residual stained dentin.250
Although additional prospective clinical evaluation of IPT is required, studies involving the primary dentition show good success rates of over 90% at 3 years.6,70,72,316 However, it has been suggested that successful outcome is highly dependent upon optimum coronal seal to eradicate the nutrient supply to residual cariogenic microorganisms. When intracoronal amalgam restorations were compared with extracoronal preformed metal (stainless steel) crowns post IPT, failure was 7.7 times more likely to occur with the use of amalgam. Similarly, adhesive restorations were also reported to provide optimum coronal seal after pulp therapy.108 Therefore, to secure the best possible outcome following IPT, or indeed any pulp therapy for the primary tooth, definitive restoration should involve a bonded restoration and/or preformed metal (stainless steel) crown.
The Hall Technique
This emerging technique of managing dental caries in primary molars is noteworthy within this section of indirect pulp therapy. The technique itself was introduced by a primary care clinician in Scotland who was overwhelmed by the number of children with dental caries. In Scotland, by the age of just 5 years, 55% of children had visible decay into dentin, and 16% had experienced tooth extraction. In response, this clinician decided to manage lesions in primary molars (that were symptom free and free from radiographic signs of periradicular pathology) by cementing a preformed metal (stainless steel) crown in place without local anesthesia, tooth preparation, or any attempt at caries removal. This is viewed in the United Kingdom as an undoubtedly novel approach to caries management and caught the attention of clinical academics in Scotland. Audit data from Dr Hall’s records indicate that her technique may have similar results to more conventional approaches in the primary care setting.132
Subsequently, a randomized, controlled clinical trial was undertaken comparing the Hall technique with conventional restorations in carious primary molars in primary care.131 Interestingly, the Hall technique was preferred to conventional restorations by the majority of children, guardians, and clinicians. After a review period of 2 years, comparing the teeth managed using Hall preformed metal (stainless steel) crowns with conventional restorations, the “Hall crowns” showed better treatment outcomes for both pulpal health and restoration longevity. In the United Kingdom, this has further stimulated an already ongoing debate related to whether restorative treatment provided by general clinicians in primary care is an effective way of managing caries in the primary dentition.74,183
Certainly this new and novel approach would appear to encompass present-day theory. Potentially cariogenic microorganisms require a very specific environment to start or progress a carious lesion. By sealing the lesion within the tooth, this removes nutrient supply and so stops or slows the lesion’s progress.173 Notwithstanding this, the importance of an effective and complete coronal seal should be of utmost importance.
Direct Pulp Capping in Primary Teeth
The lifespan of the average primary tooth from initial development to exfoliation is significantly shorter than that of a permanent tooth. Primary teeth undergo dramatic physiologic and physical changes over a relatively short period. Clinicians should keep in mind that pulp tissue is not static in nature, and outcomes for the same procedure may differ depending on the age of the patient. Further, because of the aging process within dental pulp, the likelihood of successful pulp capping diminishes with age. This may be explained by the increase in intrapulpal fibrous and calcific deposits seen with aging, together with a reduction in both pulpal volume and pulp fibroblast proliferation.110
Carious pulpal exposures in primary teeth should not be direct pulp capped. Guidelines developed by both the American Academy of Pediatric Dentistry (AAPD) and the British Society of Paediatric Dentistry (BSPD) recommend that direct pulp capping should be reserved only for small mechanical or traumatic exposures in primary teeth.7,250 Under these circumstances, it is presumed that the conditions for a favorable pulpal response are optimal.
Pulpotomy in Primary Teeth
The AAPD guidelines7 for pulp therapy for primary and young permanent teeth describe the pulpotomy procedure in primary teeth as the amputation of the affected or infected coronal portion of the dental pulp, preserving the vitality and function of all or part of the remaining radicular pulp. Evidence of successful pulp therapy includes those features listed in Box 23-3.
For all pulpotomy procedures for the cariously exposed vital pulp of primary teeth, the procedure common to all is the complete amputation of coronal pulp tissue. Following this, and once hemostasis has been achieved, a decision is made on the wound dressing or technique to apply to the pulp stumps.
Some of the options available are listed below, and the success of all depends upon ensuring that the residual pulp tissue is correctly diagnosed as healthy or reversibly inflamed.
Many pharmacotherapeutic agents have been used for pulp therapy in the past. Formocresol has been the most popular agent, mainly because of its ease of use and good clinical success. Yet despite these, formocresol and in particular one of its constituents, formaldehyde (FAD), has come under close scrutiny because of reported concerns related to the systemic distribution of FAD and its potential for toxicity, allergenicity, carcinogenicity, and mutagenicity. Other medicaments (e.g., glutaraldehyde, Ca[OH]2, collagen, ferric sulfate, MTA) have been suggested as possible replacements. However, varying success rates and questions over the safety of these materials make it clear that additional research on the use of these and other pharmacotherapeutic agents is required.
Nonpharmacologic hemostatic techniques have been recommended, including electrosurgery169,253,269,270 and laser therapy.64 Research involving human clinical trials on both these techniques is sparse; nevertheless, electrosurgical pulpotomy is currently being taught in several dental schools. Comprehensive reviews of the techniques and agents used in vital pulp therapy and discussion of possible new modalities are available in the literature.236,278,318
Indications and Contraindications for Pulpotomy
The pulpotomy is indicated for pulp exposure on primary teeth in which the inflammation or infection is judged to be confined to the coronal pulp.146,295 If inflammation has spread into the tissues within the root canals, the tooth should be considered a candidate for pulpectomy and root canal filling or extraction. The contraindications for pulpotomy on a primary tooth are outlined in Box 23-4.
Technique
Pulpotomy is used for primary teeth with radicular pulp tissue judged to be free from inflammation and infection. Compromise on this principle leads to a diminished success rate. If inflamed vital (coronal) pulp tissue is amputated to leave residual healthy pulp tissue (radicular), the tissue remaining has the capacity to remain healthy if managed correctly. The overall success of vital pulp therapy in the primary dentition depends upon:
An accurate diagnosis of pulp status is very important in aiding appropriate pulpal management. However, this can be challenging, particularly in young children. The points that follow highlight the diagnostic aids available:
Technique of Coronal Pulp Amputation
Removal of the coronal pulp tissue is a process common to whichever pulpotomy procedure is chosen for the cariously exposed vital primary tooth. Following successful coronal amputation and hemostasis (Fig. 23-15, A-B), the subsequent management of the radicular pulp stumps is defined by which pulpotomy technique the clinician chooses. For example, once hemostasis has been achieved, a wound dressing may be applied to the pulp wounds, or alternatively the exposed tissue might be subjected to electrosurgery or laser application. Fig. 23-15, C-H provides a schematic overview of the options and expected outcomes.
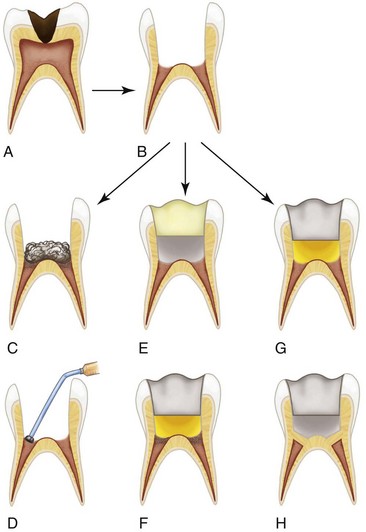
FIG. 23-15 Illustration to show three different approaches to the radicular pulp following coronal pulp amputation during pulpotomy in an extensively carious primary molar. A, Primary molar with caries extending to the pulp. Note inflammatory response in coronal pulp. B, Tooth has undergone removal of the coronal pulp. Radicular pulp tissue is healthy and has stopped bleeding. C, A 1:5 dilute solution of formocresol may be applied to pulp stumps for 5 minutes. This produces partial tissue fixation which is greatest near the point of application. D, Intracoronal restoration: zinc oxide eugenol (ZOE) is placed directly over the pulp stumps and an intracoronal restoration placed. Vital radicular pulp may remain apically. E, A 15.5% ferric sulfate solution is applied to the pulp stumps for 15 seconds. This produces mechanical blockage of open capillaries by a protein-iron complex. F, Intracoronal restoration has been provided as in D. Healthy, vital pulp tissue remains within the root canals. G, Mineral trioxide aggregate (MTA) is placed directly over the radicular pulp stumps, and the tooth is provided with an intracoronal restoration as before. H, The radicular pulp tissue remains vital beneath the MTA; a calcific bridge may form over time beneath the MTA.
Stages in the Technique of Coronal Pulp Amputation
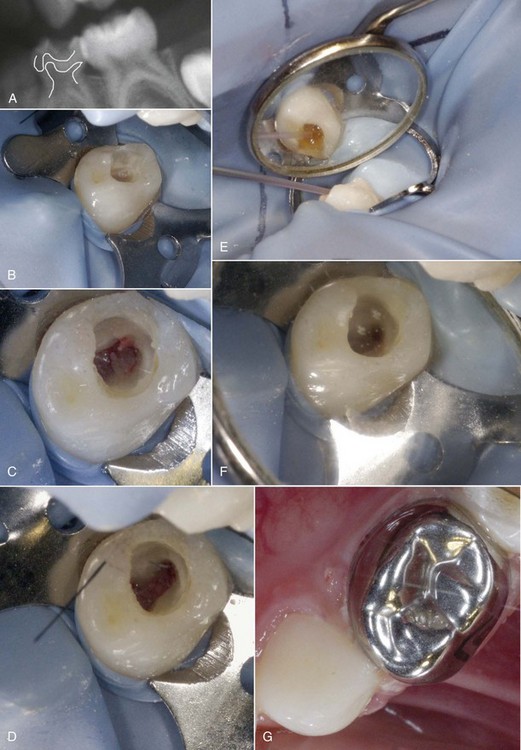
FIG. 23-16 Clinical stages of a vital pulpotomy using ferric sulfate solution. A, Extensive dental caries affecting a mandibular first primary molar. Note proximity of radiographic lesion to the mesial pulp horn. B, Caries removal showing a carious pulpal exposure; bleeding is evident. C, Partial unroofing of the pulp chamber; note bleeding coronal pulp prior to amputation. D, Roof of pulp chamber removed completely. E, A 15.5% solution of ferric sulfate is applied to radicular pulp stumps using a dento-infuser tip supplied by the manufacturer. F, Hemostasis is evident at radicular pulp stumps. G, Definitive restoration involves placement of zinc oxide eugenol, overlaid with glass ionomer intracoronally, followed by a preformed metal (stainless steel) crown.
(Courtesy of Vidya Srinivasan, Edinburgh Dental Institute, UK.)
Once bleeding has stopped at the radicular pulp stumps, the wounds are managed according to one of the following pulpotomy techniques (see Fig. 23-15):
Formocresol Pulpotomy
Technique (see Fig. 23-15, C-D)
The use of formocresol in dentistry remains controversial. Formaldehyde (FAD), a volatile organic compound, is toxic and corrosive, especially at the point of contact. Formocresol’s other active constituent, cresol, is also an irritant and corrosive in nature.225
Local and Systemic Accumulation of Formaldehyde
Localized accumulation of formocresol or FAD has been demonstrated in pulp, dentin, periodontal ligament, and bone surrounding the apices of pulpotomized teeth.93,193
Although animal studies have identified radioisotope-labeled formocresol or FAD in major organs following systemic injection or multiple pulpotomies, researchers concluded that the doses of formocresol were far in excess of those used in normal clinical practice. It has therefore been suggested that the findings should not be extrapolated to clinical use in humans.192,196,197 More recently, a review of the safety of formocresol, including FAD metabolism, suggested that FAD is rapidly metabolized, so the findings of previous studies may have been identifying FAD metabolites systemically and not FAD itself.182 Notwithstanding this, the amount of formocresol absorbed systemically by way of the pulpotomy route is small and may not contraindicate the use of the drug.220
Formocresol as an Allergen
The results of studies investigating the allergenic risks of formocresol are equivocal. Studies have shown no evidence of an allergic response in non-presensitized animals,273 and presensitized animals showed only a weak allergic potential.314 The demonstration of an immune response to formocresol-fixed, autologous tissue implanted in connective tissues or injected into root canals has, however, been reported.26,298
Is Formocresol Carcinogenic?
In respect of mutagenicity and carcinogenicity of FAD, it is generally accepted that FAD is genotoxic in vitro, inducing mutations and DNA damage in cells from a variety of organisms, including humans.101,208,217,288,324 The possible link between FAD and carcinogenesis has been investigated within the field of occupational health medicine. In a review of several large longitudinal studies, the International Agency for Research on Cancer (IARC) reported that “sufficient evidence” exists that FAD had caused nasopharyngeal cancer in humans.133 This was suggested to be linked to a localized combination of irritation and genotoxicity of FAD, which repeat-dose inhalation studies using rodents has corroborated.317 In the dental context, the amount of FAD within a diluted solution of formocresol is small, but there are no data relating to the amounts of FAD vapor inhaled by patients or dental personnel during pulpotomy procedures and whether this may constitute a potential risk. Moreover, the often disregarded cresol ingredient itself may pose a genotoxic risk to mammalian cells.109
Despite these concerns, the formocresol pulpotomy continues to be one treatment choice available for primary teeth with vital, carious exposures of the pulp in which inflammation or degeneration is judged to be confined to the coronal pulp. The last reported worldwide survey of dental schools (in 1989)17 showed a majority of pediatric dentistry departments and pediatric dentists advocated the formocresol pulpotomy technique, and it may still be widely used in clinical practice. In the United Kingdom since 2004, there has been a general trend away from using formocresol, driven by several factors: difficulty obtaining the medicament, concerns related to its safety, and promising clinical results of newer, nonaldehyde techniques.318 However, the recent U.K. Clinical Guideline, Pulp Therapy for Primary Molars, still includes the formocresol pulpotomy as an option,250 as does the AAPD guidance.7 Although formocresol pulpotomy is still widely taught in predoctoral pediatric dentistry programs in the United States,231 there is a lack of consensus over its use for vital pulp therapy in primary teeth.
The current formocresol pulpotomy technique is a modification of that reported by Sweet in 1930.287 The effect of formocresol on pulp tissue (i.e., the amount of tissue fixation) is controlled by the quantity that diffuses into the tissue and depends on length of time of application, concentration used, the method of application, or a combination of all these factors.66,96,172,177
A one-fifth dilution of formocresol solution has been widely advocated based upon the outcomes of both in vitro and in vivo studies comparing dilute formocresol (see Box 23-5) with the undiluted solution (Box 23-6). Histochemical investigations comparing dilute and undiluted formocresol noted little difference between initial effects on pulp tissue fixation but earlier recovery of enzyme activity and improvement in the rate of recovery from the localized cytotoxic effects of formocresol with diluted formocresol.164,165,286 Clinical studies have shown diluted formocresol to be as successful as full-strength formocresol.85,86,185,186
BOX 23-6 Formulation of Full-Strength Buckley’s Formocresol
| Formaldehyde | 19% |
| Tricresol | 35% |
| Glycerin | 15% |
| Water | 31% |
There is enough evidence today to conclude that if formocresol is to be used at all, the one-fifth concentration should be preferred for pulpotomy procedures because it is as effective as and less damaging than the traditional preparation.
Formocresol and the Permanent Successor
The fear of damage to the succedaneous tooth has been offered as an argument against formocresol pulpotomy on primary teeth. Results from studies are inconsistent, ranging from the same incidence of enamel defects in treated and untreated contralateral teeth187,251 to an increase in defects and positional alterations of the underlying permanent tooth.181 It should be pointed out that studies of this nature are follow-up studies long after treatment, without knowledge of the existing status of the pulp before pulpotomy.
The effect of a formocresol pulpotomy upon the exfoliation time of primary molars is also equivocal, with some studies finding no consistent effect187,312 and some reporting early exfoliation.119,185
Unlike the tissue response to Ca(OH)2, no dentin bridge should be anticipated after applying formocresol to exposed pulp tissue (see Fig. 23-15, C-D). However, narrowing of the root canal through the continued deposition of dentin by the preserved radicular pulp may be observed in some cases (Fig. 23-17).
Criteria for Success
Failure of a formocresol pulpotomy is usually detected on radiographs (see Fig. 23-13). The first signs of failure are often internal resorption of the root adjacent to the area where the formocresol was applied. This may be accompanied by external resorption, especially as the failure progresses. Sometimes, however, the internal resorption is self-corrected with the deposition of calcified tissue. In the primary molars, radiolucency develops in the bifurcation or trifurcation area. In the anterior teeth, a radiolucency may develop at the apices or lateral to the roots. With more destruction, the tooth becomes excessively mobile; a sinus tract usually develops. It is rare for pain to occur with the failure of a formocresol pulpotomy. Consequently, unless patients receive follow-up checks after a formocresol pulpotomy, failure may be undetected. When the tooth loosens and is eventually exfoliated, the parents and child may consider the circumstances normal.
The development of cystic lesions after pulp therapy in primary molars has been reported.32,259 An amorphous, eosinophilic material shown to contain phenolic groupings similar to those present in medicaments was found in the lesions. Other researchers194 have observed furcal lesions in untreated, pulpally involved primary molars containing granulomatous tissue with stratified squamous epithelium, suggesting the potential for cyst formation. In a subsequent study involving failed, pulpotomized primary molars, most specimens were diagnosed as furcation cysts.195 These findings emphasize the importance of periodic follow-up to endodontic treatment on primary teeth. Fig. 23-18 shows a favorable long-term outcome following a formocresol pulpotomy in a mandibular primary molar.
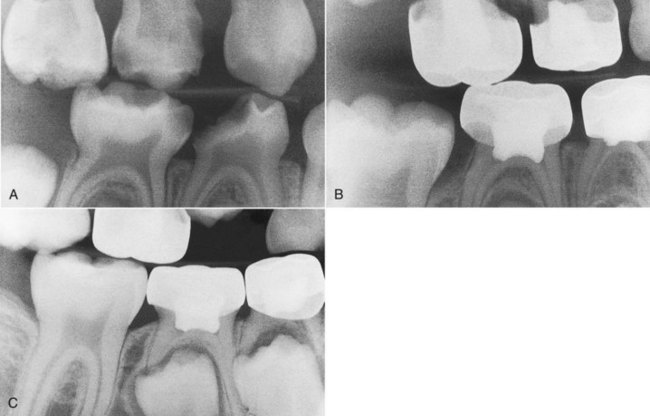
FIG. 23-18 Five-year follow-up of a primary tooth with a formocresol pulpotomy. A, Pretreatment radiograph showing deep caries on lower right first and second primary molars. B, One-year posttreatment radiograph. C, Five-year follow-up radiograph. Note eruption of lower right first permanent molar and first bicuspid.
Alternatives to Formocresol Pulpotomy
A 2006 comprehensive review is suggested for readers requiring a detailed look at the numerous alternative techniques available.278
Glutaraldehyde Pulpotomy
Glutaraldehyde has been a suggested alternative to formocresol as a tissue fixative for vital pulpotomy. Histologic studies showed that it produced rapid surface fixation of pulp tissue but with limited depth of penetration, so a larger amount of radicular pulp tissue remained vital.290,322 Fixed pulp tissue may be replaced with dense collagenous tissue over time.150 Studies have also demonstrated less systemic distribution than was thought to occur with formocresol.57,159,196,220,321
Glutaraldehyde has been shown to be rapidly metabolized with little toxic effect.118,137,143,196,240 It has also been demonstrated that although glutaraldehyde has antigenic action similar to formocresol, it is of a lower potential.237,239 However, there are perceived problems with the use of glutaraldehyde as a pulpotomy agent:
Despite the perceived enhanced safety of glutaraldehyde with respect to formocresol, it did not gain favor over formocresol for pulpotomy in the primary dentition.17,76
Ferric Sulfate Pulpotomy
Technique
Ferric sulfate has been used as a hemostatic agent for crown and bridge impressions.79 Its hemostatic action occurs by the reaction of blood with ferric and sulfate ions within the acidic pH of the solution. The agglutinated proteins form plugs that occlude the capillary orifices and prevent blood clot formation.160 Initially the use of ferric sulfate was recommended as a hemostatic agent during the Ca(OH)2 pulpotomy on the grounds that it may prevent problems arising from clot formation after coronal pulp amputation and minimize the chances for inflammation and internal resorption262—considered by some to be important factors contributing to the failure of pulpotomies using Ca(OH)2. Its first documented use in this way was in primate teeth.152
The use of ferric sulphate itself as a hemostatic pulpotomy agent was investigated by researchers using animal models (rat40 and baboon).88 From the relatively few clinical studies that have been published using ferric sulfate as a pulpotomy medicament, four are prospective comparative,75,88,129,219 and two are retrospective.30,276
In all the comparative studies, formocresol was used as the gold standard. The materials and methods used in all these studies are similar, which allows more meaningful comparison of their findings. Pulpotomies were performed in primary molars of healthy children who were selected on the basis of symptomless exposure of vital pulp by caries, absence of clinical or radiographic evidence of pulp degeneration, and possibility of proper restoration.
In all of the aforementioned ferric sulfate studies, the teeth were treated using the pulpotomy technique already outlined, and the teeth were restored with preformed metal (stainless steel) crowns. In one study,219 half of the teeth were restored with composite resin and the remaining half with preformed metal (stainless steel) crowns.
Prospective Studies
In another study,75 27 teeth were included in the formocresol group and 29 in the ferric sulfate group. Although the sample size was small, the recall rate was excellent, and in the 3- and 6-month intervals, no statistically significant difference was found between the two groups. However, at the end of this 1-year study, there was a statistically significant difference in the success rate in favor of ferric sulfate (97% for ferric sulfate, 78% for formocresol). The most frequent evidence of failure in this short-term study in both groups was furcation radiolucency. In the study by Fuks et al.,88 the sample consisted of 37 teeth in the formocresol group and 55 in the ferric sulfate group. The follow-up period ranged from 6 to 34 months, with a mean of 20.5 months. In this study, the sample size was bigger and the evaluation period much longer than the previous one. The total success rate between the two groups over the total period of 34 months did not present any statistically significant difference and was 92.7% for ferric sulfate and 83.8% for formocresol. Calcific metamorphosis and internal resorption were the most common radiographic findings. In this study, internal resorption that was stable and unchanged throughout the study was not recorded as failure.
In a later study,129 34 teeth were used in each group, and identical results were obtained 24 months post treatment for both ferric sulfate and formocresol: a 97% total success rate was recorded. In each group, only one tooth presented internal resorption and was therefore considered a failure.
In 2002, results of a larger comparative study were published219 with a sample comprising 133 pulpotomy-treated molars of 90 children from 3 to 10 years old with a mean age of 6.2 years. Sixty teeth (45%) were treated with formocresol and 73 (55%) with ferric sulfate. The number of teeth restored with either a stainless steel crown or a composite resin material was almost equal within each group. After 36 months, the clinical success rate was 97.3% for formocresol and 90.3% for ferric sulfate, but the difference in success rate between the two groups was reported to be statistically insignificant. The radiographic success rate was 78.3% for formocresol and 74% for ferric sulfate, again with no statistically significant difference between them. This success rate seems to be the lowest recorded compared with the previously mentioned comparative studies. The author feels that this finding could be due to three reasons: the larger sample size and the very good recall rate, which increased the possibility to observe and locate more failures, and the very strict radiographic assessment. Internal resorption was the most common radiographic finding for both treatments, with no statistically significant difference between ferric sulfate and formocresol. However, most cases classified initially as failures because of internal resorption remained stable throughout the 36-month observation period, and in two cases the respective areas were self-filled with reparative hard tissue. Based on this observation, the data were reevaluated, with only those cases of internal resorption that were either extensive in size or progressing with time considered as failures. After the reevaluation, the overall success rate became 78.7% for ferric sulfate and 85% for formocresol, with no statistically significant difference between them. The survival rate of the treated teeth after 6 months was 98% for both treatments and then 97% for ferric sulfate and 94% for formocresol after 1 year. These figures decreased with time for both groups, and the survival rate dropped to 81% for ferric sulfate and 78% for formocresol from 25 to 36 months.
Retrospective Studies
In a retrospective study published in 2000,276 ferric sulfate pulpotomies performed over a period of 5 years by a private pediatric dentist were evaluated. The clinical success rate was very high: 99% up to 36 months and no further failures after 36 months. The radiographic success varied from 80% for the 4- to 12-month period, 74% for the 13- to 24-month period, 81% for the 25- to 36-month period, and 74% for the over 36-month period. The estimated tooth survival time was very high, starting with 99% up to 10 months and dropping to 80% after 43 months. The two most common radiographic findings in this study were calcific metamorphosis and internal resorption. The records in this study showed that 13 teeth that presented with internal resorption did not develop osseous lesions for the period of 43 months.
A second retrospective study, published 2 years later in 2002, reported results comparing different pulpotomy treatments; 83 formocresol pulpotomies, 45 ferric sulfate pulpotomies, and 74 pulpotomies treated with a combination of ferric sulfate and formocresol were selected from the records of children treated in a public clinic at different times and by different clinicians.30 The initial results showed that the total success rate was similar in the three groups, but after a 36-month follow-up, the success rate was better for formocresol than for ferric sulfate, and the combination of the two agents was the worst. The last finding is not surprising because the teeth were treated initially with ferric sulfate for hemostasis and then with formocresol, and they had a poor prognosis (i.e., hyperemic and/or symptomatic). As pointed out by the authors, this study had several shortcomings, the most serious being that the pulpotomies were performed by many clinicians of different levels of experience and expertise; that the criteria for selection of cases were not strictly defined; and that the radiographs were not always satisfactory, compromising accurate evaluation of the periradicular and furcal areas of the treated teeth.
The studies described demonstrate a higher success rate for both ferric sulfate and formocresol in those with shorter observation times and smaller sample sizes. As the sample size increases and the observation period becomes longer, the success rate drops; this holds true for both ferric sulfate and formocresol pulpotomies. The most important finding is that no statistically significant differences in the success rates between ferric sulfate and formocresol existed, with the exception of one short-term study75 in which a statistically significant difference was observed in favor of ferric sulfate at the 1-year period. In all the reviewed studies (prospective and retrospective), both ferric sulfate and formocresol treatments gave very good results with high tooth survival rates. Moreover, the type of restoration (stainless steel crown or composite resin) was not reported to influence the success rate for either pulpotomy agent.219
Clinical Outcome
In one study, the cases of internal resorption that remained unchanged throughout the 36-month observation period were not considered as failures in the final examination of the results.219 Others proposed that internal resorption should not be considered as pulpotomy failure and based this proposal on the fact that none of the teeth with internal resorption in their sample developed an osseous lesion.276 This proposal may be accepted only in cases of minimal or unchanged internal resorption but not for severe or progressive resorption. Internal resorption may indicate pulp inflammation that is expected at the amputation site after pulpotomy. However, if the inflammation can be restricted and confined to a very small part of the pulp while the rest is healthy, the resorption process will cease or even self-heal by the apposition of hard tissue and therefore will not be a failure. In all the other cases, internal resorption indicates irreversible or extensive inflammation and should be considered a failure.
It can be seen from these studies and the results of a recent meta-analysis163 that for human carious primary molars with reversible coronal pulpitis, both ferric sulfate and formocresol pulpotomies similarly give good clinical and radiographic results, with high tooth survival rates and no statistically significant differences in success rates. These findings agreed with an earlier Cochrane Review of pulp treatment for extensive decay in primary teeth.199
Based on these studies, ferric sulfate can be used instead of formocresol for treatment periods up to 36 months.
Mineral Trioxide Aggregate Pulpotomy
Technique
MTA used as a pulp capping agent in monkey teeth showed the pulp tissue responses to MTA to be superior to those produced using Ca(OH)2.228 Similar results were found when human intact third molars were used to compare the effect of pulp capping with MTA and Ca(OH)2.2 MTA was found to maintain pulp integrity after pulp capping and pulpotomy in animal studies59,255 and to have a dentinogenic effect on the pulp expressed by the induction of dentin bridge formation (see Fig. 23-15, H) where it touches the pulp tissue.255,257,310
Clinical Studies
One of the first preliminary studies published comparing MTA with formocresol in humans63 involved 45 pulpotomy-treated primary molars in 26 children with a mean age of 6 years, 5 months. Clinical and radiographic follow-up ranged between 6 and 30 months, involving 18 children with 32 teeth. Internal resorption was seen in one molar treated with formocresol (17 months post treatment). None of the teeth from the MTA group presented any clinical or radiographic pathosis. Pulp canal obliteration was observed in 9 of 32 (28%) molars evaluated.
Preliminary results of a 3-year prospective follow-up study comparing MTA with formocresol were reported at a scientific congress.245 Pulpotomies were undertaken on 60 primary molars in 22 children aged 2 to 8 years, each needing at least two pulpotomies. Each child received at least one MTA and one formocresol pulpotomy followed by preformed metal (stainless steel) crown. Six months after treatment, seven teeth of the formocresol group and two of the MTA group presented abnormal radiographic findings, but these differences were not statistically significant.
More promising results were observed122 in a more extensive study that included part of the material presented by Eidelman et al.63 and a longer follow-up time. These authors assessed the long-term success rate of pulpotomy in primary molars with carious pulp exposure using MTA or formocresol as pulp dressing agents. Sixty-four primary molars of 35 children were treated by a conventional pulpotomy technique. Following removal of the coronal pulp and hemostasis, the pulp stumps were covered with MTA in the experimental group. In the control group, formocresol was placed with a cotton pellet over the pulp stumps for 5 minutes and then removed; the pulp stumps were then covered by ZOE paste. Eight teeth from each group were restored with an amalgam restoration, and all others were covered with a preformed metal (stainless steel) crown. Thirty-three children with 62 teeth (29 treated with formocresol and 33 with MTA) were available for long-term clinical and radiographic evaluation. Follow-up ranged between 4 and 74 months, with a mean follow-up time of 38 months and with no difference between the groups. Twenty-nine teeth were followed until natural exfoliation (mean 33 months). Failures were detected after a mean period of 16 months (range 4 to 30 months). The success rate of pulpotomy was 97% for MTA (one failure) and 83% for formocresol (five failures). Eight teeth presented internal resorption. In four (two from each group), progress of the resorption process stopped, and the pulp tissue was replaced by a radiopaque calcified tissue. Pulp canal obliteration was observed in 55% (34 of 62) of the evaluated molars. This finding, which was not considered a failure, was detected in 58% (19 of 33) of the MTA and in 52% (15 of 29) of the formocresol group. The authors concluded that MTA showed a higher long-term clinical and radiographic success rate than formocresol as a dressing material following pulpotomy in primary molars and recommended it as a suitable replacement for formocresol.
The clinical, radiographic, and histologic effects of gray MTA, white MTA, and formocresol as pulp dressings in pulpotomy-treated primary teeth have been reported.107 This involved 24 children with a mean age of 6 years (range 4 to 8 years), each with at least three primary molars requiring pulpotomy, for the clinical and radiographic part of the study. An additional 15 carious primary teeth planned for serial extractions were selected for the histologic part of the study. All the teeth were evaluated periodically for 12 months except those selected for histologic evaluation; these were extracted 6 months post treatment. Sixty pulpotomy-treated teeth in 20 children were reviewed; of these, one tooth (gray MTA) exfoliated normally, and six teeth (four white MTA and two formocresol) failed because of abscesses. All the remaining 53 teeth showed success clinically and on radiographs. Pulp canal obliteration was found in 11 teeth treated with gray MTA and one treated with white MTA. The histologic evaluation demonstrated that both types of MTA induced thick dentin bridges, whereas in the formocresol group these were thin and poorly calcified. The pulpal architecture observed with the gray MTA was closer to normal than the white MTA, which presented a dense fibrotic pattern with isolated pulp calcification. These authors concluded that gray MTA was better than both white MTA and formocresol as a pulp dressing for pulpotomy-treated primary teeth.
MTA is commercially available in the United States as ProRoot MTA (DENTSPLY Tulsa Dental, Tulsa, OK), and Angelus MTA (Angelus, Londrina, Brazil) is also available in Latin America and Europe. ProRoot MTA is considered expensive, particularly because it is retailed in cartons containing a number of sealed 1-gram packets. The composition of MTA is similar to cement used in the building industry, and such material should be kept dry during storage, because contact of the powder with moist air will lead to “air-setting,” affecting its physical properties. The same could be applied to the “clinical-grade” cement, and the manufacturer of ProRoot MTA recommends the 1-gram sachet as a single-use, which would be expensive. The unused MTA remaining in a sachet may actually be stored for up to a further 4 weeks in a water-tight, air-tight container such as an Eppendorf tube (Eppendorf UK Ltd, Cambridge, UK), reducing its cost.283 Alternatively, it has been suggested that the MTA powder can be stored indefinitely if the corner of the packet is folded firmly and the packet is stored in a sealable plastic bag. Angelus MTA is presented in a sealable glass vial, with the recommendation that 1 gram may provide up to seven treatments. Care must be taken not to contaminate the MTA powder when it is dispensed.
Electrosurgical Pulpotomy
Technique
The steps in the electrosurgical pulpotomy technique are basically the same as those for the formocresol technique through the removal of the coronal pulp tissue.
Although electrocoagulation on the pulps of teeth was reported in 1957,157 it was a decade later that Mack168 became the first U.S. clinician to routinely perform electrosurgical pulpotomies. Oringer216 also strongly advocated this technique in his 1975 text on electrosurgery.
Electrosurgery is a nonpharmacologic, hemostatic pulpotomy technique used directly on the radicular pulp stumps following coronal pulp amputation. Depending on the currents used and thus the heat generated, incision, coagulation, or electrofulguration can occur. Electrosurgical pulpotomy carbonizes and denatures pulp tissue, producing a layer of coagulative necrosis. This acts as a barrier between the lining material and healthy pulp tissue below.278
Several clinical studies253,270 have produced results comparable to those found with the use of formocresol. Conflicting results have been reported from histologic studies, ranging from comparable results to formocresol pulpotomy269 to pathologic root resorption with periapical and furcal involvement.271 A retrospective human study169 in 1993 showed a success rate of 99% for primary molars undergoing electrosurgical pulpotomies. Compared with a formocresol pulpotomy study of similar design, the success rate of the electrosurgery technique was shown to be significantly higher.
Laser Pulpotomy
Several reports have appeared in the literature on the use of the carbon dioxide laser for performing vital pulpotomies on primary teeth.64,161 Investigators64 compared the use of the laser with formocresol in caries-free, primary cuspid teeth that were scheduled for extraction in children between 6 and 10 years of age. Thirty teeth were included in the study. No significant differences were found between the formocresol and laser-treated groups. Areas of isolated internal resorption were identified in one of the formocresol-treated teeth and two of the laser-treated teeth. They concluded that on the basis of symptomatic, clinical, and histologic findings, the carbon dioxide laser appeared to compare favorably with formocresol treatment. It was suggested that additional studies should be conducted to establish the ideal applied laser energy to maximize optimum residual pulpal response, and to explore the effects of laser pulpotomy upon pulps previously exposed by carious lesions.
Other researchers161 reported the use of the laser on primary teeth with vital carious pulpal exposures. Thirty-three teeth, 21 primary molars and 12 primary canines, were treated and observed for 12 to 27 months. All were clinically successful, and only one showed evidence of internal resorption at the 6-month follow-up visit. The authors observed complete calcification on radiographs after 9 months in approximately half of the treated teeth.
On the basis of these initial studies, the use of the carbon dioxide laser could be considered a viable alternative to formocresol. More randomized controlled human clinical trials are recommended.
In summary, the search for alternatives to the formocresol pulpotomy in cariously exposed vital primary teeth has yet to reveal an agent, instrument, or technique that has unequivocal long-term clinical success rates better than those of formocresol. Until such an agent, instrument, or technique is found, ferric sulfate, MTA, or formocresol (one-fifth dilution) can be used with equal confidence in primary tooth pulpotomies.84,250,278
Nonvital Pulp Therapy on Primary Teeth
Pulpectomy in Primary Teeth
The anatomic and normal physiologic features of primary teeth can present challenges to the clinician wishing to undertake pulpectomy procedures. However, with knowledge of these features and how they may impact upon clinical technique, pulpectomy and root canal obturation of primary teeth with irreversibly inflamed or necrotic pulp can be a clinically successful option.
Effect of Resorption on Canal Anatomy and Apical Foramina
In the newly completed roots of the primary teeth, the apical foramina are located near the anatomic apices of the roots. After the deposition of additional dentin and cementum, there are multiple apical ramifications of the pulp as it exits the root, just as in the mature permanent tooth.
The physiologic resorption of the roots of the primary incisors and canines starts on the lingual surfaces in the apical third because of the position of the permanent tooth bud. In primary molars, resorption usually begins on the inner surfaces of the roots near the interradicular septum (Box 23-7).
As resorption progresses, the apical foramen may not correspond to the anatomic apex of the root but be coronal to it. Subsequently, radiographic establishment of the root canal length may be challenging (Fig. 23-19). Resorption may extend through the roots and into the root canals, creating additional communications with the periapical tissues other than through the apical foramina or lateral and accessory canals. This has been shown to occur at all levels of the root.244 Because of these factors, use of an apex locator is not reliable to establish canal length.
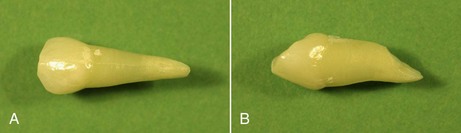
FIG. 23-19 Primary maxillary canine. A, Facial view, where apical foramen appears to be at the apex of the root. B, Physiologic root resorption has occurred at the palatal aspect of the root; apical foramen is positioned more coronally and will not be coincident with the perceived radiographic apex of the tooth.
Permanent Tooth Bud
The effects of primary endodontic therapy on the developing permanent tooth bud should be of paramount concern to the clinician. Manipulation through the root apex of a primary tooth and overextension of root canal instruments and filling materials are to be avoided because the permanent tooth bud lies in close proximity. If radiographic signs of resorption are visible, canal length is usually established by measurement of the diagnostic radiograph, ensuring the working length of endodontic instruments are 2 or 3 mm short of the radiographic apex. The use of the long-cone radiographic paralleling technique for maximal accuracy is recommended. Hemorrhage after pulp removal may indicate overextension into the periapical tissues.
Anesthesia is usually necessary for pulp extirpation and cleaning of the canals but may be unnecessary when primary teeth are filled at a subsequent appointment. The response of the patient can sometimes be used as a guide to the proximity of the apex and as a check of the length of the canal. However, this can only be done in cooperative patients, because the discomfort caused by placing the rubber dam clamp or by the approach of the instrument to the apex might create disruptive behavior in some children.
The material used to obturate root canals in primary teeth must be resorbable, so that as the tooth resorbs it offers no resistance or deflection to the eruption of the permanent tooth. Permanent obturating materials, such as gutta-percha, are contraindicated in root canal therapy for primary teeth that have permanent successors.