The Child with a Sensory or Neurological Condition
1 Define each key term listed.
2 Discuss the prevention and treatment of ear infections.
3 Outline the nursing approach to serving the hearing-impaired child.
4 Discuss the cause and treatment of amblyopia.
5 Compare the treatment of paralytic and nonparalytic strabismus.
6 Review the prevention of eyestrain in children.
7 Discuss the functions of the 12 cranial nerves and nursing interventions for dysfunction.
8 Describe the components of a “neurological check.”
9 Outline the prevention, treatment, and nursing care for the child with Reye’s syndrome.
10 Describe the symptoms of meningitis in a child.
11 Describe three types of posturing that may indicate brain damage.
12 Discuss the various types of seizures and the relevant nursing responsibilities.
13 Prepare a plan for success in the care of a mentally retarded child.
14 Describe four types of cerebral palsy and the nursing goals involved in care.
15 State a method of determining level of consciousness in an infant.
16 Describe signs of increased intracranial pressure in a child.
17 Discuss neurological monitoring of infants and children.
18 Identify the priority goals in the care of a child who experienced near-drowning.
19 Formulate a nursing care plan for the child with a decreased level of consciousness.
 , p. 535)
, p. 535) , p. 548)
, p. 548) , p. 544)
, p. 544) , p. 539)
, p. 539) , p. 537)
, p. 537) , p. 536)
, p. 536) , p. 544)
, p. 544) , p. 532)
, p. 532) , p. 543)
, p. 543) , p. 541)
, p. 541) , p. 543)
, p. 543) , p. 544)
, p. 544) , p. 544)
, p. 544) , p. 540)
, p. 540) , p. 536)
, p. 536) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The Ears
The ear, which can be considered a part of the nervous system, contains the receptors of the eighth cranial (acoustic) nerve. The ear performs two main functions: hearing and balance. Figure 23-1 summarizes ear, eye, and neurological differences between children and adults. The three divisions of the ear are the external ear, the middle ear, and the inner ear (Figure 23-2). In the newborn the tympanic membrane is almost horizontal and is more vascular than in the adult. It has a dull and opaque appearance and an inconsistent light reflex. The eustachian tube is shorter and straighter in the infant than in the adult. Three functions of the eustachian tube are ventilation of the middle ear, protection from nasopharyngeal secretions and sound pressure, and drainage. Middle-ear infections are common during early childhood.
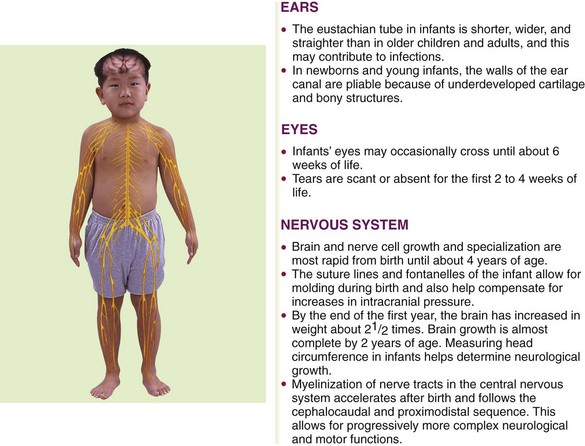
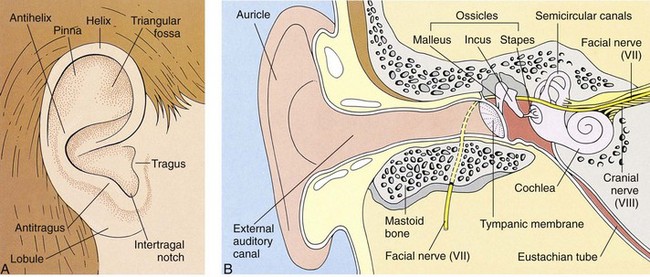
FIGURE 23-2 Anatomy of the ear. A, The normal external ear—the auricle (pinna) and tragus—is shown with common landmarks labeled. B, There are three divisions of the ear: outer ear, middle ear, and inner ear. In the newborn the mastoid process and the bony part of the external canal are not fully developed, leaving the tympanic membrane vulnerable to injury. Newborns can hear as soon as amniotic fluid is drained by the first sneeze. The eustachian tube connects the middle ear and the pharynx and serves to vent the middle ear. In infants the eustachian tube is shorter, wider, and straighter than in adults. Pooling of fluids such as milk in the throat of an infant who falls asleep with a bottle of milk can contribute to ear infections. The external auditory canal is more angulated (curved) in infants, and therefore pulling the pinna (auricle) is required to straighten the canal for an accurate tympanic temperature.
When nurses examine the ear, they observe both the exterior and the interior. Ear alignment is observed. The top of the ear should cross an imaginary line drawn from the outer canthus of the eye to the occiput (see Figure 12-6). Low-set ears may be associated with kidney disorders and mental retardation. The outer ear and the area around it are inspected for cleanliness and drainage. The inner ear is examined with an otoscope. One method of restraint used when assisting with the examination of the inner ear is to lay the child on a table with the arms held alongside the head, which is turned to the side. Another method of positioning a child for an ear examination is placing the child in the lap of the adult (see Figure 22-5).
 Nursing Tip
Nursing Tip
Before instilling ear drops in infants, gently pull the pinna of the ear down and back. In children, gently pull the auricle of the ear up and back to straighten the external auditory canal.
Disorders and Dysfunction of the Ear
An acute infection of the external ear canal is called otitis externa and is often referred to as swimmer’s ear because prolonged exposure to moisture is often the precipitating factor. Pain and tenderness on manipulating the pinna or tragus of the ear are specific signs of this type of infection. The ear canal may be erythematous, but the tympanic membrane is normal. A foreign body, cellulitis, diabetes mellitus, and herpes zoster should be ruled out. Irrigation and topical antibiotics or antivirals are the treatment of choice. The health care provider may insert a loose cotton gauze (wick) into the outer third of the ear canal. The wick is kept moist with frequent drops of the appropriate medicated solution.
Acute Otitis Media
Pathophysiology: Otitis media (ot, “ear,” itis, “inflammation of,” and media, “middle”) is an inflammation of the middle ear. The middle ear is a tiny cavity in the temporal bone. Its entrance is guarded by the sensitive tympanic membrane, or eardrum, which transmits sound waves through the “oval window” to the inner ear, which contains the organs of hearing and balance. The middle ear opens into air spaces, or sinuses, in the mastoid process of the temporal bone. It is also connected to the throat by a channel called the eustachian tube. These structures—the mastoid sinuses, the middle ear, and the eustachian tube—are lined by mucous membranes. As a result, an infection of the throat can easily spread to the middle ear and lead to mastoiditis. The eustachian tube also protects the middle ear from nasopharyngeal secretions, provides drainage of middle ear secretions into the nasopharynx, and equalizes air pressure between the middle ear and the outside atmosphere. These protective functions are diminished when the tubes are blocked. Unequalized air pressure within the ear creates a negative pressure that allows organisms to be swept up into the eustachian tube.
Otitis media (OM) occurs most often after an upper respiratory tract infection and usually affects children between 6 and 24 months of age and in early childhood. It is caused by various organisms, of which Streptococcus pneumoniae and Haemophilus influenzae are the most common. Polyvalent pneumococcal polysaccharide vaccines have reduced the incidence of pneumococcal otitis media, but these vaccines are not effective in children under 2 years of age because they are not capable of producing an antibody response.
Infants are more prone to middle ear infections than older children and adults because their eustachian tubes are shorter, wider, and straighter. When infants lie flat for long periods, microorganisms have easy access from the eustachian tube to the middle ear. Feeding methods may have a bearing on middle ear infection, for instance, the pooling of fluids such as milk in the throat of an infant who falls asleep with a bottle of milk provides a source for growth of organisms. The infant’s humoral (humor, “body fluid”) defense mechanisms are immature. Children in passive smoking environments have more respiratory infections because of the effect of secondary smoke on the protective cilia that line the nose. Day care attendance can contribute to the risk of upper respiratory infections and OM because of increased exposure to ill children. Upper respiratory infections are discussed in detail in Chapter 25.
Manifestations: The symptoms of OM are pain in the ear, which is often very severe; irritability; and diminished hearing. Fever, which may be as high as 40° C (104° F), headache, vomiting, diarrhea, and febrile seizures may also occur. Earaches in infants may be manifested by general irritability, frequent rubbing or pulling at the ear, and rolling of the head from side to side. The older child can point to the place that is tender. Visualization of the tympanic membrane via otoscope reveals a reddened and bulging membrane.
If an abscess forms, a rupture of the eardrum may result, and drainage from the ear may be evident. When this happens, the pressure is relieved and the child is more comfortable. Some amount of hearing loss may result from the rupture. OM is considered chronic if the condition persists for more than 3 months. Recurrent attacks can lead to serious complications. Chronic OM can lead to cholesteatoma (chole, “bile,” steato, “fat,” and oma, “tumor”), a cystlike sac filled with keratin debris. This may occlude the middle ear and erode adjacent ossicle bones, causing hearing loss. This condition is best treated by an otolaryngologist. Complications of repeated attacks of acute OM can include the development of chronic OM with effusion (fluid accumulation). Hearing loss can result. Treatment may be indicated because hearing loss may impair cognitive and language development that can hamper the education and communication abilities in developing children.
Treatment: When an infection is evident, treatment is directed toward finding the causative organism and relieving the symptoms. A throat culture may be taken to determine the specific organism. Broad-spectrum antibiotics may be given orally and should be continued until the prescribed amount of medication has been taken. Analgesics are given to relieve pain. Antihistamines and decongestants are not effective in treating acute OM.
Surgical Treatment: Surgical intervention may be necessary when medical treatment is unsuccessful. The physician may incise the tympanic membrane to relieve pressure and to prevent a tear by spontaneous rupture. This is called a myringotomy (myringa, “eardrum,” and otomy, “incision of”). A tympanic membrane (TM) button or tympanostomy ventilating tube (PE, pressure equalizer) may be inserted. This may fall out spontaneously within 6 to 12 months. In some children, the tubes may have to be reinserted to continue ventilation. Care is taken to avoid getting water in the ears while bathing or showering. All children should be followed up to make sure that the condition is resolved and to evaluate any hearing loss that may have occurred.
Comfort Measures: Antipyretics may be given to reduce fever, and a warm compress may be applied locally for comfort. If the eardrum has ruptured, the child is placed on the affected side. Cold may also be beneficial. An ice pack may be prescribed to reduce edema and pressure. The skin around the ears must be kept clean and protected from any drainage to prevent tissue breakdown. Parents are instructed not to insert cotton swabs into the ears.
Hearing Impairment
Pathophysiology: Approximately 1 in 1000 newborns is born with some type of hearing impairment. This number may increase to 2 in 1000 for hearing loss occurring during childhood. Hearing-impaired children present special challenges to the health care team. Hearing loss can affect speech, language, social and emotional development, and behavior, as well as academic achievement. The nurse should have a basic understanding of how to approach and work with a hearing-impaired child.
The inner ear is fully formed during the early months of prenatal life. If an expectant mother contracts German measles or other viral infection during this period, the child may be born with a hearing loss; this is termed congenital deafness. Deafness can also be acquired. Infectious diseases such as measles, mumps, chickenpox, or meningitis can result in various degrees of hearing loss. The common cold, some medications, exposure to loud noise levels, certain allergies, and ear infections may also be responsible. Hearing problems can also be temporary if they are caused by cerumen (wax) accumulation. Some rattles and squeaky toys can emit sounds as loud as 110 decibels. (Sounds above 80 decibels can cause damage.) These types of toys should not be held close to the infant’s ear.
Early diagnosis and treatment of hearing-impaired children is important to prevent adverse physical and mental complications from developing. Members of the health care team concerned with the child who is hearing impaired include the physician, otologist (ear specialist), audiologist, speech therapist, specially trained teacher, social worker, psychologist, school nurse, and members of the child’s family.
The various degrees of hearing loss range from a complete bilateral loss (which affects both ears) to a loss so mild that the problem is never recognized. Hearing loss can result from defects in the transmission of sound to the middle ear, from damage to the auditory nerve or ear structures, or from a mixed hearing loss that involves both a defect in nerve pathways and interference with sound transmission. If hearing loss is complete, the child misses all the pleasures of sound and has difficulty in communication (children learn to talk by imitating what they hear). Behavior problems may arise because these children do not understand verbal directions. They may become aggressive with other children in their attempt to communicate. If they are ridiculed by playmates, personality development will be affected. Unless these children are helped early in life, they may become socially isolated.
Partial bilateral deafness may be responsible for behavior problems and poor progress in school. It is most commonly caused by chronic ear infections, such as OM, or by blockage of the eustachian tube. Children who have hearing losses in one ear are less affected if hearing in the other ear is normal.
Diagnosis and Treatment: The American Academy of Pediatrics recommends a goal of universal detection of hearing impairment in infants before 3 months of age, with interventions started no later than 6 months of age to minimize problems with growth and development (Wolff et al., 2010). The evoked otoacoustic emissions (OAE) test is a preferred method for neonatal testing. The brainstem auditory evoked response (BAER) test records brain wave responses generated by the auditory system. These tests are easily administered to the newborn infant, and many hospitals routinely screen newborns for hearing ability before discharge. Lack of response by the infant to sounds or music or lack of the startle reflex in infants under 4 months of age are the first signs that may alert the parents or nurse to the possibility of hearing impairment. Early diagnosis and prompt treatment are primary requisites, regardless of the child’s age. Complete bilateral deafness is usually discovered during infancy. Partial deafness may be unrecognized until the child begins school. Many hearing problems are detected by the school nurse administering standard hearing tests.
Tympanometry measures ear pressure but is difficult to perform adequately on an active infant or small child. A tuning fork is used to evaluate for air conduction (Rinne test) or bone conduction (Weber test). This type of test requires the child to be cooperative and able to communicate what is heard or felt. Diagnosis of hearing loss can be confirmed by visual reinforcement audiometry (VRA), which identifies sensitivity to sounds in young infants.
Many hearing defects are amenable to medical or surgical treatment. Hearing aids can amplify sound waves. Surgically placed cochlear implants are used for some children with nerve damage. Children who suffer a severe loss of hearing need more extensive help from personnel at an auditory training center. These children must begin treatment as soon as the hearing loss is discovered.
Nursing Care: Various methods are used to bring the child into the world of sound. Lip reading, sign language, writing, visual aids, and amplified sound are but a few examples. The parents are instructed in means of communication that correspond with those used by the teachers.
The nurse must be aware of the symptoms of deafness in the child. Newborns are observed for their response to auditory stimuli. The Brazelton Neonatal Behavioral Assessment Scale evaluates the infant’s orientation response to the sound of a voice. The persistence of the Moro reflex beyond 4 months of age may also be an indication of deafness. The infant who makes no verbal attempts by 18 months of age should undergo a complete physical examination. Indifference to sound, behavior problems, or poor school performance may also be signs of deafness. The nurse inquires into the facilities that are available in the community for such a child.
The hearing-impaired child in the hospital needs the same opportunities to communicate as the child who does not have this disability. The nurse smiles when approaching the child. Body language communicates a lot, especially if there is a severe communication problem. The nurse faces the child when speaking and is positioned at eye level with the child. The nurse must ensure that the child sees him or her before touching to avoid startling the child. Sign language is the use of hand signals that correspond to words and assist in communication with a deaf child. Previously developed speech patterns may regress during hospitalization. Visual aids, writing, or drawing can be used to enhance communication.
If a hearing aid is indicated, the child is equipped with one and taught how to use it. Regular checkups ensure that the hearing aid is working properly. A hearing aid is expensive and invaluable to the child. It is put in a safe place when not in use. When the child goes to surgery, it is given to the parents or placed in the hospital safe. The pockets of hospital gowns are checked before the gowns are placed in the laundry.
The National Hearing Center provides information about hearing aids. Hearing aids are designed to fit in the ear, behind the ear, on eyeglass frames, or on the body with wires to the ear. The nurse should check ear hygiene and be sure hairs are not caught on the end of the hearing aid to ensure a proper fit and to minimize noise and whistling problems. Teaching safe battery handling and storage and promoting self-care are important nursing responsibilities.
Home care of the hearing-impaired child should include speech therapy. Flashing lights should be installed in the home to alert the child to doorbells and other sound-based devices.
Telecommunication devices for the deaf (TDD) are available to enable telephone communication. Closed captioning devices for television are available to the child who can read.
The school nurse can help the family nurture socialization skills. Some hearing-impaired children attend special schools for the deaf, and some are mainstreamed into the general school population. Each hearing-impaired child and each family unit should be followed by the multidisciplinary health care team.
Barotrauma
Barotrauma occurs when there is a change in the atmospheric pressure between the internal body systems and the surrounding environment. An example of barotrauma would be the painful obstruction of auditory tubes when in a pressurized cabin of an airplane. Today many children travel with their family via airplanes and may react to a change in altitude and barometric pressure. During airplane descent, children should be encouraged to yawn or chew on gum to promote swallowing. Infants should be bottle-fed juice or water to promote swallowing, which produces autoinflation and relief of symptoms. Systemic decongestants can be taken before air travel and timed so that their peak effectiveness occurs during airplane descent.
Adolescents may participate in recreational underwater diving that can cause barometric pressure stress to the ear and result in severe earaches and other serious problems. Underwater diving should be slow during the descent phase to minimize negative pressure buildup. Sensory hearing loss and vertigo with nausea and vomiting may be early signs of decompression sickness when it occurs during the ascent phase of diving. The diver should be referred for medical care. Upper respiratory infections or tympanic membrane perforation are contraindications to diving because vertigo, nausea, vomiting, and disorientation can occur, with dangerous results.
The Eyes
The eye is the organ of vision. The anatomy of the eyeball is depicted in Figure 23-3. The eyes begin to develop as an outgrowth of the forebrain in the 4-week-old embryo. The retinal vessels vascularize (develop) at 40 weeks of gestation, and therefore infants born prematurely often have vision problems throughout their life. At birth, the eye is 65% of adult size. The newborn’s sight is not mature, but the newborn can see. Visual acuity is estimated to be in the range of 20/400. This improves rapidly and may reach 20/40 to 20/30 by 2 or 3 years of age. The shape of the newborn’s eye is less spherical than the adult’s eye. Newborns keep their eyes closed most of the day and can focus and fixate on objects 12 to 30 cm (8 to 12 inches) away for only a few seconds at a time and cannot coordinate or follow without turning their head. By 2 to 4 months infants can move their eyes to follow people or objects. By 4 to 5 months their eyes are open most of the day and the lacrimal glands begin to secrete tears for eye protection. Eye-hand coordination develops. The nurse should document this because the ability to transfer objects from one hand to another is partially dependent on the ability to see the object. The development of the ability to crawl is also partially dependent on the ability to see an object at a distance and attempt to reach it. Depth perception is not developed until 9 months of age. When the child walks or runs, visual depth perception influences the child’s ability to run without falling. The American Academy of Pediatrics (AAP) recommends that all children undergo preschool visual screening during well-child visits between 2 and 3 years of age (Kuhn, 2009).
FIGURE 23-3 The normal eye. A, External view. B, Internal view showing relationship of the optic nerve, eye muscles, and chambers of the eye.
Nursing Tip
At birth the quiet, alert infant will respond to visual stimuli by ceasing to move. Visual responsiveness to the mother during feeding is noted. The infant’s ability to focus and follow objects in the first months of life should be documented. Coordination of eye movements should be achieved by 3 to 6 months of age.
On physical examination the nurse observes the eyes to see if they are symmetrical and are an equal distance from the nose. Epicanthal folds (epi, “upon,” and canthus, “angle”) are folds of skin that extend on either side of the bridge of the nose and cover the inner eye canthus. Some folds are broad and cover a large portion of the inner eye, causing the eye to appear crossed. Large epicanthal folds occur as part of some chromosomal anomalies. Pupils are observed for size, shape, and movement. Their reaction to light is observed by shining a penlight into the eye and quickly removing it. The healthy pupil constricts (gets smaller) as the light approaches and dilates (gets larger) as it disappears (see Figure 23-14). Older children are given explanations concerning the examination. The nurse should assess and document the general appearance of the child as well as achievement of developmental milestones. This includes observing for symmetry of the eye orbit and eyelids, excessive tearing, squeezing of the eyelids, and strabismus (crossed eyes).
Nursing Tip
The achievement of developmental milestones such as transferring objects from hand to hand is partially dependent on seeing the object. Therefore, assessment of visual ability is part of assessment of growth and development.
Visual Acuity Tests
The ability of an infant to fixate and focus on an object can be demonstrated by 6 weeks of age. The object should not emit a sound so it is certain the infant is turning toward a sight stimulus rather than a sound stimulus. Visual acuity can be tested by  to 3 years of age.
to 3 years of age.
There are a variety of visual acuity charts (Figure 23-4). The Snellen alphabet chart and the Snellen E version for preschoolers who have not learned the alphabet are commonly used to assess the ability to see near and far objects. Picture cards are also useful for children who do not know letters.
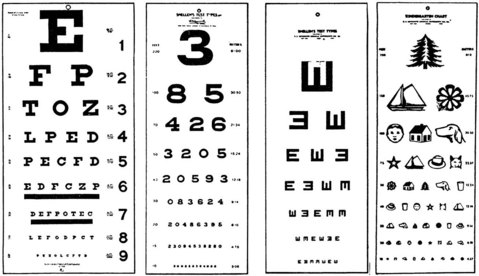
FIGURE 23-4 Various types of visual acuity charts. The “E” chart is often used for young children who can “show which way the fingers of the E are pointing.”
The Titmus machine is often used for school-age children and adolescents. Directions for testing are standardized and must be carefully adhered to for proper results. Computerized tests, such as the random-dot stereogram, are also useful in the visual screening of children. Visual acuity is important in the learning process. Retinopathy of prematurity (ROP) is discussed in Chapter 13.
Disorders and Dysfunction of the Eye
Dyslexia (dys “difficult,” and lexis, “diction”) is a reading disability that involves a defect in the cortex of the brain that processes graphic symbols. Although an eye evaluation is recommended when a child has mirror vision or word reversal, the problem does not involve any local eye defect. Correcting vision problems will aid in optimal visual function, but treatment for dyslexia involves remedial instruction.
Amblyopia
Pathophysiology: Amblyopia (lazy eye) is a reduction in or loss of vision that usually occurs in children who strongly favor one eye. If both retinas do not receive a clearly defined image, bilateral amblyopia may result. However, it is more common for one eye to be affected. When abnormal binocular interaction occurs (such as crossed eyes or strabismus), the prognosis depends on how long the eye has been affected and on the age of the child when treatment begins. The earlier the treatment is given, the better the results. One commonly accepted diagnostic sign is that vision in the normal eye is at least two Snellen lines (E charts) better than that in the affected eye. There are various types of amblyopia. Strabismus is the most common; however, dissimilar refractory errors can also result in this condition. Because amblyopia occurs as a result of sensory deprivation of the affected eye, children are at risk for developing the problem until visual stability occurs, usually by 9 years of age.
Treatment and Nursing Care: Early detection and prompt treatment are essential. The goal of treatment is to obtain normal and equal vision in each eye. Treatment consists of eyeglasses for significant refractive errors such as hyperopia (farsightedness) or myopia (nearsightedness) and patching (occlusion) of the good eye. The good eye is patched to force the use of the affected eye. Daytime patching may be tried first, since part-time occlusion is sufficient in some cases. Occlusion therapy is often difficult to maintain. The nurse can be of help by explaining the importance of the procedure and by offering support, but the child is often subjected to teasing by peers. Providing a safe place to express feelings is important to promoting a healthy self-image. In most cases an opaque contact lens or a contact lens of sufficiently high power to blur the vision in the better eye is used (Kliegman et al., 2007).
Strabismus
Pathophysiology: Strabismus (cross-eye), also known as squint, is a condition in which the child is not able to direct both eyes toward the same object. There is a lack of coordination between the eye muscles that direct movement of the eye. When the eyes cannot coordinate sight together, the brain will disable one eye to provide a clear image. The disabled eye can develop permanent visual impairment because of sensory deprivation (amblyopia). Normal binocular vision is the goal and must be accomplished by intervening early before the eye matures.
There are several types of strabismus. Nonparalytic strabismus (concomitant) involves a constant deviation in the gaze related to faulty insertion of the eye muscle. One eye always looks crossed. The extraocular muscles are normal. Paralytic strabismus (nonconcomitant) involves a paralysis or weakness in the extraocular muscle. Double vision is experienced. Deviation of the gaze occurs with movement, when the eye attempts to focus. To prevent double vision (diplopia) the child will tilt his or her head or squint when focusing on an object. Strabismus may be present at birth or may be acquired after a disease or injury. This type of strabismus can occur after head trauma or a neurological disease. It is important to note that epicanthal folds can give a false impression of strabismus.
Treatment: In nonparalytic strabismus the refractory error is usually corrected with eyeglasses. When paralytic strabismus is seen during early infancy, the physician may recommend that the unaffected eye be covered by a patch until the infant is old enough to wear glasses. The affected eye may improve through use and often becomes normal. Eye exercises and glasses are effective ways of treating the condition medically. If they do not help, surgery should be considered. It is generally performed when the child is 3 or 4 years of age. Early correction is necessary to prevent amblyopia. If strabismus is left untreated, blindness in the affected eye may result because the brain tends to obliterate the confusing double image by disabling the eye.
Nursing Care: The child undergoing surgery for strabismus may be hospitalized for only a brief period. The surgery involves structures outside the eyeball; therefore the child is allowed to be up and about postoperatively. Eye dressings are kept at a minimum, and elbow restraints may be sufficient to keep the child from touching the dressings.
Prevention of Eyestrain: Children who are beginning to read need books with large type in which the letters are spaced far apart. The lighting must be adequate and without glare. Chairs and desks must be of the proper height.
Symptoms that may indicate eyestrain include inflammation, aching or burning of the eyes, squinting, a short attention span, frequent headaches, difficulties with schoolwork, or an inability to see the blackboard. It is important for the nurse to observe the child for eyestrain, to teach proper eye care, to prevent complications of eyestrain or strabismus, to refer as needed for follow-up care, and to assist in rehabilitation.
Conjunctivitis
Conjunctivitis (conjungere, “to join together,” and itis, “inflammation”) is an inflammation of the conjunctiva, or the mucous membrane that lines the eyelids (Figure 23-5). It is caused by a wide range of bacterial and viral agents, allergens, irritants, toxins, and systemic diseases. Conjunctivitis that occurs with viral exanthems such as measles are usually self-limiting. It is common in childhood and may be infectious or noninfectious. The acute, infectious form is commonly referred to as pinkeye. Pinkeye is considered no longer contagious after 24 hours of appropriate antimicrobial therapy. Conjunctivitis can also result from an obstruction of the lacrimal duct. In general, the common forms of conjunctivitis respond to warm compresses and topical antibiotic eye drops or eye ointments. Ointments blur vision and are not generally used during daytime hours in the ambulatory child.
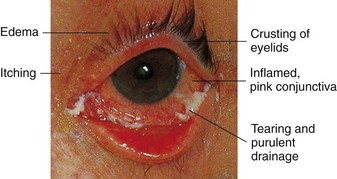
FIGURE 23-5 Acute bacterial conjunctivitis. Signs of conjunctivitis are evident in this highly contagious infection.
The nurse instructs parents to administer the eye medication for the prescribed time to prevent recurrence. Parents and older children are taught to wipe secretions from the inner canthus downward and away from the opposite eye. Because conjunctivitis spreads easily, affected children should use separate towels and be instructed to wash their hands frequently. Ophthalmia neonatorum, an acute conjunctivitis in the newborn, is discussed in Chapter 6. Allergic conjunctivitis is often associated with allergic rhinitis (rhin, “nose,” and itis, “inflammation”) in children with hay fever. Symptoms include itching, tearing of one or both eyes, and edema of the eyelids and periorbital tissues. The child may appear distracted and irritable.
Hyphema
Hyphema, the presence of blood in the anterior chamber of the eye, is one of the most common ocular injuries. It can occur from either a blunt or a perforating injury. Blows from flying objects (e.g., baseball, snowball) and forceful coughing or sneezing can cause this condition. These accidents are common among active school-age children. Hyphema appears as a bright red or dark red spot in front of the lower portion of the iris.
Treatment includes bed rest and topical medication. The head of the bed is elevated 30 to 45 degrees to decrease intraocular pressure and decrease intracranial pressure if there is an associated head injury. The condition generally resolves itself without residual problems.
Retinoblastoma
Pathophysiology: Retinoblastoma is a malignant tumor of the retina of the eye. There are hereditary and spontaneous forms. The average ages at diagnosis are 12 months for bilateral tumors and 21 months for unilateral tumors (Kliegman et al., 2007). Gene-mapping techniques have shown chromosome 13 to be affected in hereditary forms. Chromosome 13 is also known to cause other congenital defects.
Manifestations: A yellowish white reflex is seen in the pupil because of a tumor behind the lens. This is called the cat’s eye reflex or leukokoria (leuk, “white,” and kore, “pupil”). This may be accompanied by loss of vision, strabismus, hyphema and, in advanced tumors, pain. Metastasis to the unaffected eye is common in unilateral tumors. When retinoblastoma is suspected in children, an examination is performed using an anesthetic so the pediatric ophthalmologist may carefully examine the fundus of the eye.
Treatment and Nursing Care: The standard treatment for unilateral disease is enucleation (removal) of the eye if there is no possibility of saving the vision. Small tumors are treated with laser photocoagulation to destroy the blood vessels supplying the tumor. Larger tumors can be treated with chemotherapy or external beam irradiation.
On return from surgery for enucleation, the child has a large pressure dressing on the eye. Elbow restraints may be necessary to prevent removal of the dressing. The bandage is observed for bleeding, and the vital signs are assessed. In a few days the surgeon removes the dressing and applies an eye patch. Other structures of the eye, such as the lids, lashes, and tear glands, are not affected. An eye prosthesis is fitted when the socket has healed. Instructions for care of the prosthesis are provided at the time of final fitting. Providing education and emotional support of the child and family and referral to the multidisciplinary health care team are essential.
The Nervous System
The nervous system is the body’s communication center; it receives and transmits messages to all parts of the body. It also records experiences (memorization) and integrates certain stimuli (learning). The anatomy of the nervous system is depicted in Figure 23-6. Neural tube development occurs during the third to fourth week of fetal life. This eventually becomes the central nervous system (CNS). The fusing process of the neural tube is critical. Its failure to fuse may lead to congenital conditions such as spina bifida (see Chapter 14). Most neurological disabilities in childhood result from congenital malformation (birth defects), brain injury, or infection. The 12 cranial nerves and their functions are shown in Figure 23-7.
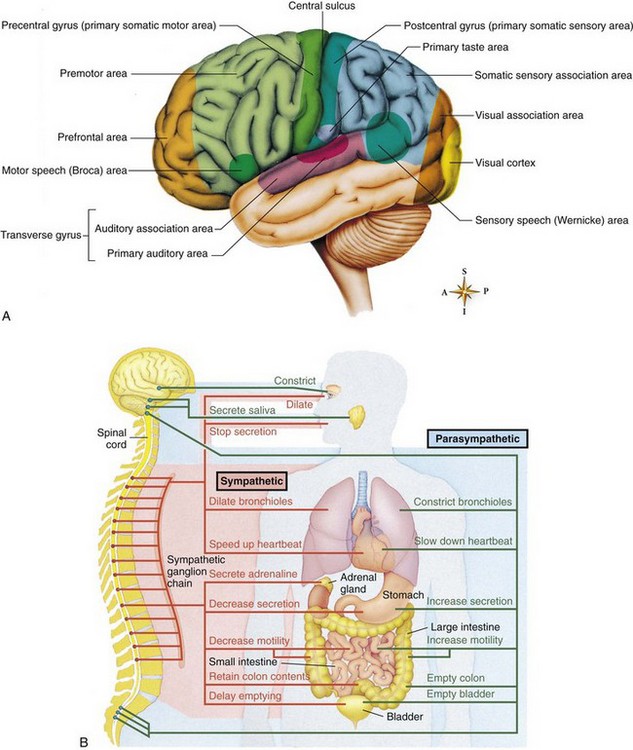
FIGURE 23-6 A, Functional areas of the brain. Each area of the brain has a specific function. Damage to the local area can cause loss of that function. B, The nervous system. The innervation of target organs by the autonomic nervous system. The sympathetic pathways are shown in orange, and the parasympathetic pathways are shown in green.
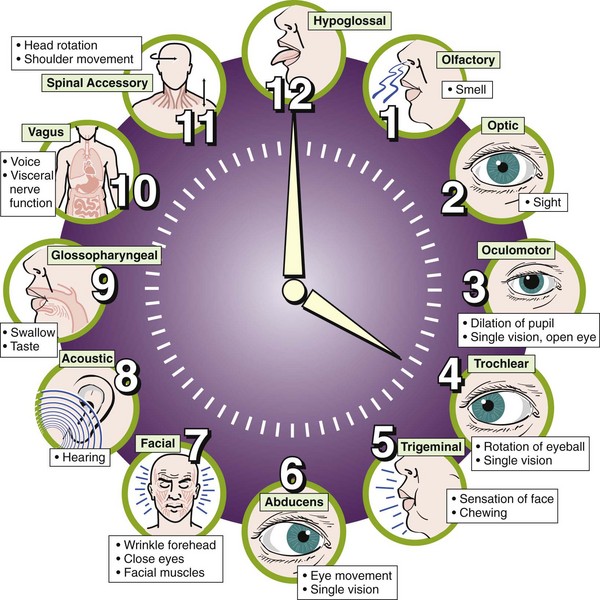
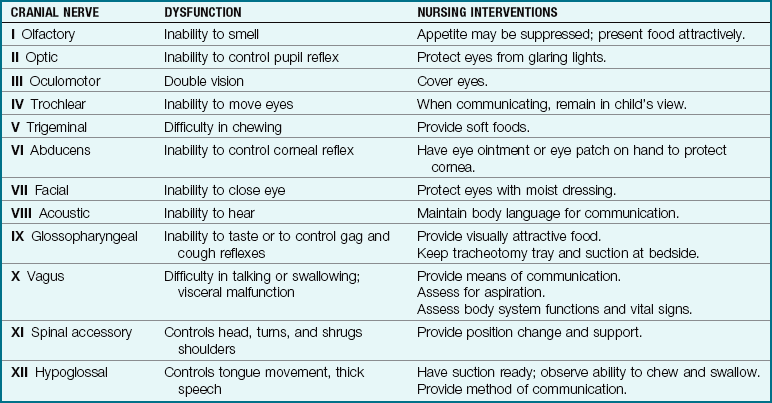
Central nervous system (CNS) dysfunction may be detected by a neurological check (see Box 23-6 and Table 23-6), skull x-ray films, electroencephalography (EEG), computed tomography (CT), magnetic resonance imaging (MRI), electromyography, and other methods. The reflexes of the newborn are good indicators of neurological health. A decreased level of consciousness in the ill child may be an indication of a neurological problem. Box 23-1 describes the causes of altered level of consciousness. In the finger-nose test (used to determine coordination), the child is asked to extend the arm and then to touch his or her nose with the index finger. This is done with the eyes opened and closed. The inability to balance on one foot in a school-age child necessitates further follow-up. The 12 cranial nerves, selected forms of dysfunction, and nursing interventions are described in Table 23-1.
Disorders and Dysfunction of the Nervous System
Pathophysiology: Reye’s syndrome is an acute noninflammatory encephalopathy (pathology of the brain) and hepatopathy (pathology of the liver) that follows a viral infection in children. There may be a relationship between the use of aspirin (acetylsalicylic acid) during a viral flu or illness such as chickenpox (varicella) and the development of Reye’s syndrome. For this reason, aspirin use is generally contraindicated for the pediatric population. Some studies show that a genetic metabolic defect triggers Reye’s syndrome.
Manifestations: Liver cell pathology causes an accumulation of ammonia in the blood. Toxic levels of ammonia cause cerebral manifestations (e.g., cerebral edema, increased intracranial pressure [ICP]), which results in neurological changes such as altered behavior, altered level of consciousness, seizures, and coma.
In children, the sudden onset of effortless vomiting and altered behavior (e.g., lethargy, combativeness) or altered level of consciousness after a viral illness is characteristic of Reye’s syndrome. The results of blood tests assessing liver function will be abnormal. In infants, diarrhea, hypoglycemia, tachypnea with apneic episodes, and seizures may occur approximately 1 week after a respiratory illness.
Prevention: The education of the public concerning the dangers of using salicylate-containing medications during viral illnesses such as varicella in children may have contributed to the decline in the occurrence of Reye’s syndrome. The availability of the varicella vaccine may also have an impact on the reduced incidence of Reye’s syndrome.
Treatment: Early treatment can result in recovery with some neuropsychological deficits. However, progression to the acute stage is often rapid and unpredictable. The goals of treatment include reducing ICP and maintaining a patent airway, cerebral oxygenation, and fluid and electrolyte balance.
Frequent assessment of vital signs and a careful assessment of neurological status are essential. Observation for signs of bleeding is important because liver dysfunction causes blood-clotting abnormalities. Parental education and support are necessary. Encouraging parents to participate in their child’s care helps to reduce the parents’ and child’s level of anxiety.
Sepsis
Sepsis is the systemic response to infection with bacteria and can also result from viral and fungal infections. Sepsis causes a systemic inflammatory response syndrome (SIRS) due to the endotoxin of the bacteria that causes tissue damage. Untreated sepsis results in septic shock, multiorgan dysfunction syndrome (MODS), and death. Children who are immunocompromised, have neutropenia, or are in intensive care receiving invasive therapy are at increased risk for developing sepsis.
Manifestations: Manifestations of sepsis include fever, chills, tachypnea, tachycardia, and neurological signs such as lethargy. Septic shock is not diagnosed by a decrease in blood pressure because initially, the infant’s body compensates for the poor circulation and tissue perfusion by increasing the heart rate and vasoconstriction of peripheral blood vessels. Hypotension is an ominous sign that may indicate the body is unable to compensate adequately and cardiorespiratory arrest is about to occur. Laboratory test results may include positive blood cultures, reduced fibrinogen and thrombocyte levels, and the presence of immature white blood cells. Neutropenia (neutrophil count below 1000/mm3) is an ominous sign. The nursing responsibilities include monitoring neurological status and vital signs; observing for shock; and maintaining strict standard and expanded precautions (see Appendix A). Intravenous antibiotics are prescribed. To prevent sepsis, immunization against H. influenzae type B (Hib) and administration of pneumococcal conjugate vaccine (PCV) are recommended for all children between 2 months and 4 years of age.
Meningitis
Pathophysiology: Meningitis is an inflammation of the meninges (the covering of the brain and spinal cord). Various organisms can cause bacterial meningitis. Organisms may invade the meninges indirectly by way of the bloodstream (sepsis) from centers of infection such as the teeth, sinuses, tonsils, and lungs, or directly through the ear (otitis media), or from a fracture of the skull.
Bacterial meningitis is often referred to as purulent, that is, pus forming, because a thick exudate surrounds the meninges and adjacent structures. This can lead to certain sequelae such as subdural effusion and, less frequently, hydrocephalus. The peak incidence for bacterial meningitis is between 6 and 12 months of age. Meningococcal meningitis is readily transmitted to others. Meningitis is less common in children older than 4 years of age. H. influenzae is the most common causative agent. H. influenzae type B vaccine and PCV have decreased the incidence of bacterial meningitis. The approaches to nursing care for all types of meningitis are similar.
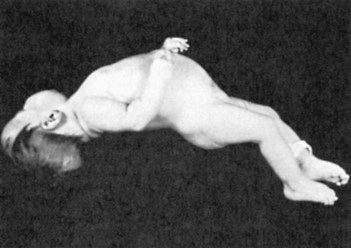
Manifestations: The symptoms of purulent meningitis result mainly from intracranial irritation. They may be preceded by an upper respiratory infection and several days of gastrointestinal symptoms such as poor feeding. Severe headache, drowsiness, delirium, irritability, restlessness, fever, vomiting, and stiffness of the neck (nuchal rigidity) are other significant symptoms. A characteristic high-pitched cry is noted in infants. Seizures are common. Coma may occur fairly early in the older child. In severe cases, involuntary arching of the back caused by muscle contractions is seen (Figure 23-8). This condition is called opisthotonos (opistho, “backward,” and tonos, “tension”). The presence of petechiae (small hemorrhages beneath the skin) suggests meningococcal infection. Diagnosis is confirmed by examination of the cerebrospinal fluid (CSF).
Treatment: At the first indication of meningitis, the physician performs a spinal tap (lumbar puncture, see Chapter 22) to obtain a specimen of CSF for laboratory testing. The spinal fluid may be clear in the early stages of the illness, but it rapidly becomes cloudy. The CSF pressure is increased, and further laboratory analysis indicates a high white cell count, an increase in protein, and a decrease in glucose.
The child is placed in isolation until 24 hours after antibiotic therapy has been initiated. An intravenous (IV) line is established for the administration of antibiotics and to restore fluid and electrolyte balance. Antibiotics are selected on the basis of culture and sensitivity laboratory results. Antibiotics are usually administered for a minimum of 10 to 14 days. A sedative may be given to make the child less restless. An anticonvulsant such as phenytoin (Dilantin) may also be required to decrease the risk of seizure activity. Dexamethasone reduces complications of bacterial meningitis but is not used in nonbacterial meningitis.
Nursing Care: The single room is prepared in accordance with hospital protocol (see Appendix A for transmission-based precautions). Nursing responsibility includes performing frequent neurological checks and maintaining an accurate recording of the child’s vital signs and intake and output. The nurse should also organize care so that the child is disturbed as little as possible.
The child with meningitis may be overly sensitive to stimuli; therefore the room should be dimly lit and the noise kept to a minimum. The nurse carefully raises and lowers the sides of the crib to avoid jarring the bed. The nurse avoids startling the child and so uses a soft voice and gentle touch. These precautions are also explained to the parents.
Frequent monitoring of the child’s vital signs is necessary. A slowed pulse rate, irregular respirations, and increased blood pressure are reported immediately, because they could indicate increased ICP. Fever may be controlled by antipyretics, sponge baths, or a hypothermia (cooling) mattress. The nurse observes the child for additional or subtle signs of increased ICP, especially a change in alertness or muscle twitchings. The joints are also observed for swelling, pain, and immobility. Oxygen is given as ordered.
The child’s intake and output are carefully observed and recorded. Careful attention is given to maintaining the IV line. Good oral hygiene is essential during this stage, when the child is receiving nothing by mouth. As the child’s condition improves, the diet progresses from clear fluids to an age-appropriate diet. A special formula may be given when nasogastric feedings are necessary. During the convalescent period, oral fluids are encouraged unless contraindicated. The nurse promptly reports a decrease in output of urine (oliguria), which could signal urinary retention. Bowel movements are recorded each day to detect constipation and prevent fecal impaction (an accumulation of feces in the rectum). The nurse continues to monitor neurological status and to record and report findings such as weakness of the limbs, speech difficulties, mental confusion, and behavior problems. The child should be assessed for developmental deficiencies. When recovery is uneventful, the child may be discharged home. The parents are taught the principles of intermittent IV therapy that can be accomplished in the home setting with visits from a home health agency nurse.
Encephalitis
Pathophysiology: Encephalitis (encephalo, “brain,” and itis, “inflammation”) is an inflammation of the brain. The condition is known as encephalomyelitis (myelo, “spinal cord”) when the spinal cord is also infected. This disorder can be caused by “togaviruses” (ribonucleic acid [RNA] viruses) and herpesvirus types 1 and 2; it can be the aftermath of disorders such as upper respiratory tract infections, German measles (rubella), or measles (rubeola) or rarely, an untoward reaction to vaccinations such as diphtheria, pertussis, and tetanus (DPT); and it may also result from lead poisoning. Other causative agents include bacteria, spirochetes, and fungi.
Manifestations: The symptoms of encephalitis result from the CNS response to irritation. Characteristically, the history is that of a headache followed by drowsiness that may proceed to coma. Because coma is sometimes prolonged, encephalitis is sometimes referred to as “sleeping sickness.” Seizures are seen, particularly in infants. Fever, cramps, abdominal pain, vomiting, stiff neck (nuchal rigidity), delirium, muscle twitching, and abnormal eye movements are other manifestations of the disease.
Treatment and Nursing Care: The treatment is supportive and aimed at providing relief from specific symptoms. Sedatives and antipyretics may be prescribed. Seizure precautions are taken. Adequate nutrition and hydration are maintained. The nurse provides a quiet environment, good oral hygiene, skin care, and frequent changes of position. Oxygen is given as ordered, and the mouth and nose are kept free of mucus by gentle aspiration. Bowel movements are recorded daily, because the child may be constipated from the lack of activity. Preventing the secondary effects of immobilization is paramount.
The nurse closely observes the child for neurological changes. Fatality rates and residual effects are higher among infants than among older children. Speech, mental processes, and motor abilities may be slowed, and permanent brain damage and mental retardation can result. Growth and development and hearing evaluations should be monitored. Parents are encouraged to help with the care of the child as soon as the condition is stable. They are instructed about the nursing procedures for home care and any required follow-up care.
Brain Tumors
Pathophysiology: Brain tumors are the second most common type of neoplasm in children (the first is leukemia). The majority of childhood tumors occur in the lower part of the brain (cerebellum or brainstem). The etiology of these tumors is unknown. They occur most commonly in school-age children.
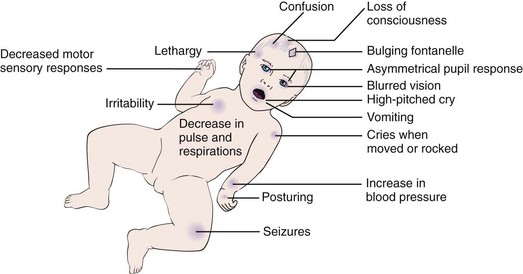
Manifestations: The signs and symptoms are directly related to the location and size of the tumor. Most tumors create increased ICP with the hallmark symptoms of headache, vomiting, drowsiness, and seizures (Figure 23-9). Nystagmus (constant jerky movements of the eyeball), strabismus, and decreased vision may be evidenced. Papilledema (edema of the optic nerve) may occur. Other symptoms include ataxia, head tilt, behavioral changes, and cerebral enlargement, particularly in infants. Deviations in vital signs are noticeable when the tumor presses on the brainstem.
Treatment and Nursing Care: Diagnosis is determined by clinical manifestations, laboratory tests, CT, MRI, and EEG. Angiography is used to assist in the surgical approach by identifying the tumor’s blood supply. Radiotherapy, chemotherapy, or surgery may be indicated.
Preoperative emphasis is placed on carefully explaining various procedures and on familiarizing the child and family with the recovery room, intensive care unit (ICU), and hospital personnel. The nurse explains that the child will have part or all of his or her head shaved. The size of the postoperative dressing is carefully explained. Applying a similar dressing to a doll may be helpful to the child. Trendelenburg position is avoided because it increases intracranial pressure (ICP).
Postoperative care is usually provided in the ICU. Adjuncts to care may include using a hypothermia (cooling) blanket or a mechanical respirator. Parents must be prepared for the appearance of the child after surgery. Empathic family support and appropriate referral are offered.
Radiation treatment may be prescribed. The radiologist outlines the areas to be treated on the child’s head. These marks are not to be washed off. Small doses of radiation are given over a period of weeks. Chemotherapy may follow irradiation.
Seizure Disorders
Seizures are the most commonly observed neurological dysfunction in children. The etiology varies (Box 23-2). Seizures are sudden, intermittent episodes of altered consciousness that last seconds to minutes and may include involuntary tonic and clonic movements. A tonic movement is a stiffening (contraction) of muscles. A clonic movement is an alternating contraction and relaxation of muscles. It may include changes in perception, behavior, sensations, and posture.
Febrile Seizures: Febrile seizures are a transient condition common in children between 6 months and 5 years of age. There may be a genetic predisposition explaining why children in the same family have this problem. The seizure occurs in response to a rapid rise in temperature—often above a level of 38.8° C (102° F). Because the seizure lasts a short time and is no longer present when the child reaches a hospital, causes other than fever may have to be ruled out. Simple febrile seizures are treated by teaching the parent to control the fever by appropriate use of antipyretics (e.g., acetaminophen) and cooling measures (e.g., removing heavy blankets and clothing). Parents should be reassured that the condition is self-limiting. The use of phenobarbital is not effective and may decrease cognitive function. Valproic acid (Depakene) produces side effects. These drugs are not recommended for first-time treatment. Rectal or oral diazepam (Valium) for the duration of a febrile illness may be prescribed if febrile seizures recur. Side effects such as lethargy, irritability, or ataxia (lack of muscular coordination) should be reported. Febrile seizures rarely develop into epilepsy, and the affected child has an excellent prognosis without residual problems.
Pathophysiology: The term epilepsy (chronic recurrent seizures) comes from the Greek epilepsia, which means “seizure.” In the past, words such as fit, spell, and blackout commonly were used to describe this entity. These terms are nonspecific, and they tend to create confusion.
Epilepsy is a disorder manifested by a variety of symptom complexes. It is characterized by recurrent paroxysmal (sudden, periodic) attacks of unconsciousness or impaired consciousness that may be followed by contraction (tonic movements) and relaxation (clonic movements) resulting in alternating tonic and clonic movements of the muscles or abnormal behavior. It is a disorder of the CNS in which the neurons or nerve cells discharge in an abnormal way. These discharges may be focal or diffuse. The site of general discharge can sometimes be ascertained by observing the child’s symptoms during the attack. It may be caused by a head injury or meningitis. When the cause is unknown, the term idiopathic epilepsy is used.
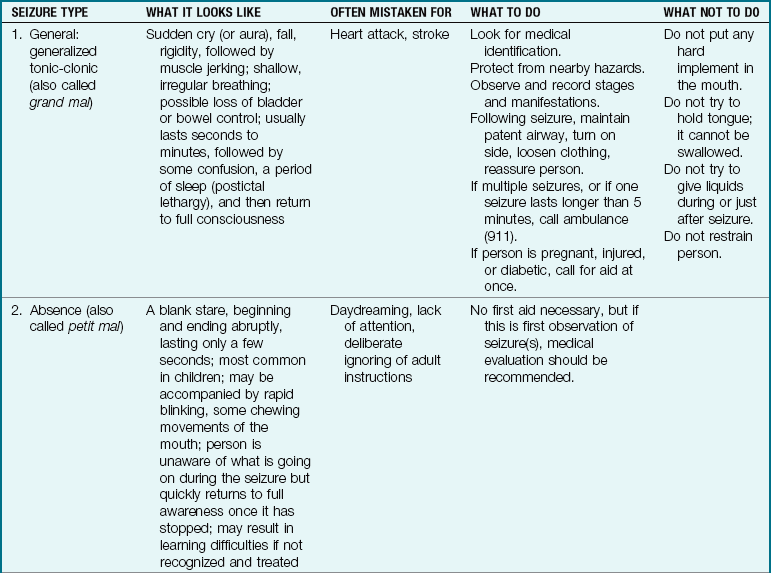
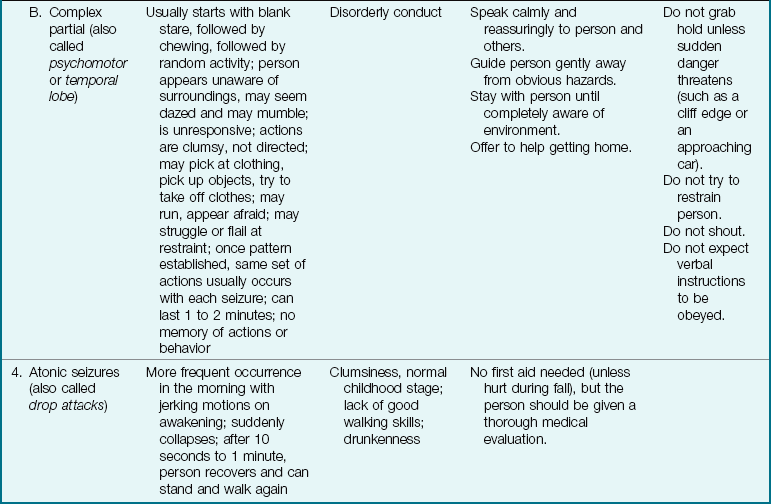
The nurse observes and records the following: the child’s activity immediately before the seizure; body movements; changes in color, respiration, or muscle tone; any incontinence; and the parts of the body involved. When possible, the seizure is timed. The child’s appearance, behavior, and level of consciousness after the seizure are also documented. Table 23-2 describes the first aid response and nursing responsibilities during a seizure.
Types of epilepsy: Childhood epilepsy is classified into partial seizures and generalized seizures.
Generalized seizures: Generalized seizures involve a loss of consciousness. The most common generalized seizure is the tonic-clonic or grand mal. A grand mal epilepsy has three distinct phases:
1. An aura (subjective sensation)
3. Postictal lethargy—a short period of sleep after a generalized seizure
Petit mal, or absence, seizures often are recognized when an intelligent child is referred for medical evaluation because of unexplained failure to achieve in school. The reason for school failure is found to be absence seizures, which cause a temporary loss of awareness that results in a lack of continuity in the learning environment.
Other types of general seizures include myoclonic spasms, where repetitive muscle contractions occur, and infantile spasms, which occur in infants under 1 year of age and are manifested by a jackknife posture for frequent but brief periods.
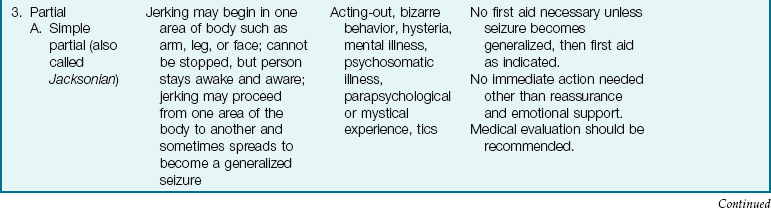
Partial seizures: Partial seizures account for 40% of childhood seizures. Consciousness may be intact or slightly impaired. Simple partial seizures (Jacksonian) are often mistaken for alterations in behavior or “tics,” which usually involve only the face or shoulders. Complex partial seizures can be manifested by motor activities, sensory signs, or psychomotor (behavioral) activity.
Treatment: Initially, treatment is aimed at determining the type, site, or cause of the disorder. Diagnostic measures include a complete history and physical and neurological examinations. Skull radiography and CT or MRI scans are used to establish the presence or absence of tumors, skull abnormalities, hematomas, and intracranial calcifications. The EEG is also a valuable tool in diagnosing seizures. It is especially helpful in differentiating between an absence seizure and a complex partial seizure. Prolonged EEG monitoring (24 hours) is another diagnostic technique.
Laboratory studies such as complete blood count (CBC), determinations of serum calcium and blood urea nitrogen (BUN), and tests to rule out lead poisoning or other metabolic disorders are done. Anticonvulsant medications are prescribed when epilepsy is the diagnosis (see Table 23-3). The drug of choice depends on the type of seizure, and the goal is the use of only one drug that will control the seizures with the fewest side effects.
Table 23-3
Properties of Selected Anticonvulsant Drugs
| DRUG | SIDE EFFECTS | COMMENTS |
| Carbamazepine (Tegretol) | Blurred vision, diplopia, drowsiness, vertigo | Few side effects, fewer sedative properties; used for general and partial seizures |
| Phenobarbital (Luminal) | Drowsiness, irritability, hyperactivity | Altered sleep patterns, often combined with other drugs |
| Phenytoin (Dilantin) | Ataxia, insomnia, nystagmus, gum overgrowth, hirsutism (hairiness), rash, nausea, vitamin D and folic acid deficiencies | Generally effective and safe; may cause cognitive impairment; regular massaging of gums decreases hyperplasia; used in combination with phenobarbital. Intravenous (IV) doses should not be mixed with glucose solutions. |
| Valproic acid (Depakene) | Gastrointestinal disturbance, liver toxicity, amenorrhea, weight gain | Take with food or use enteric-coated preparations; potentiates action of phenobarbital and other drugs |
| Primidone (Mysoline) | Aggressive behavior, personality changes, anorexia, fatigue, dermatitis | May be used alone or in combination; side effects minimized by starting with small amounts |
| Ethosuximide (Zarontin) | Anorexia, gastrointestinal upset | Often used for absence seizures |
| Clonazepam (Rivotril) | Drowsiness, excess salivation | Used in partial seizures |
| Topiramate (Topamax) | Slow cognition, fatigue | Used for complex partial seizures |
| Gabapentin (Neurontin) | Weight gain and somnolence | Used in poorly controlled seizures |
| Lamotrigine (Lamictal) | Ataxia, rash, photosensitivity, and drowsiness | Given with other seizure medications |
| Keppra (Levetiracetam) | Sleepiness, incoordination, behavior changes | Used with other medications for partial seizures |
Note: The physician determines the child’s medication by the type of seizure and other factors. The goal is to achieve the best control with the minimum dosage and the least number of side effects. An important aspect of nursing intervention includes reinforcing the need for drug supervision and compliance.
The duration of therapy is based on the individual child. Initially, the physician prescribes the lowest dose of anticonvulsant medication likely to control the seizures. The goal is to control the seizures and minimize the toxic effects of the medication. Drowsiness, a common side effect of many anticonvulsants, may interfere with the child’s activities. Careful recording of seizure activity and compliance with the drug regimen are of particular importance in determining a suitable program. The medication is given at the same time each day, generally with meals or at bedtime.
If it is necessary for the child to take medication during school hours, the parents sign a consent form so that the school nurse can monitor the administration. The responses of the nurse and teacher, particularly during and after a seizure, will have a significant effect on the attitude of classmates toward the child.
Abrupt withdrawal of anticonvulsant medications is the most common cause of status epilepticus (prolonged seizures). In the hospital the nurse clarifies with the physician whether anticonvulsants are to be withheld if the child is to be given nothing by mouth (NPO). When children are old enough, they can assume responsibility for their own medications. They should wear a medical identification bracelet. During puberty and adolescence, the dosages may have to be adjusted to meet growth needs. Anticonvulsant drugs should not be taken during pregnancy, because birth defects can occur. Premenstrual fluid retention in girls can sometimes trigger seizures. Surgery is being performed on children who are unresponsive to anticonvulsants and who have a well-defined focus of seizure activity in the brain.
 Medication Safety Alert!
Medication Safety Alert!
Children taking phenobarbital or phenytoin (Dilantin) should receive vitamin D and folic acid supplementation. Phenytoin should not be given with milk.
The ketogenic diet is sometimes prescribed for children who do not respond well to anticonvulsant therapy. The diet is high in fats and low in carbohydrates, with adequate protein. This diet produces ketoacidosis in the body, which appears to reduce convulsive episodes. A reduction of fluid intake tends to increase the ketogenic effect. The use of this diet is limited because it is boring and requires strict adherence to intake, and compliance tends to be a problem. Long-term effects of this type of diet, such as hyperlipidemia, are unknown (Levy & Cooper, 2008).
Rebellion against medical routine is not uncommon during adolescence. Some states do not allow controlled epileptics to obtain a driver’s license, which is disheartening to the child. Other states have stipulations regarding the amount of seizure-free time required before licensing. Excess intake of fluids, particularly alcoholic beverages, can trigger a seizure. Parents can obtain valuable information and support from the Epilepsy Foundation of America. Other major resources include the Department of Vocational Rehabilitation, the Department of Public Health, the Department of Social Services, and other community agencies.
The greatest untapped resource for persons with epilepsy is often within themselves. A fundamental principle of comprehensive epilepsy management is that the child must become an active member of the health care team. In a comprehensive multidisciplinary treatment approach, team members help the child to mobilize his or her inner resources to deal with the lifelong treatment and to lead a fully productive, normal life. With a few safety guidelines, this is possible.
Restriction of physical activity is not necessary, but adult supervision during swimming or bathing is advisable. A family assessment is helpful in establishing rapport and setting realistic short- and long-term goals. Too much attention to seizures by well-meaning adults can make control difficult. The child may learn to use the threat of a seizure to manipulate caregivers. Teaching should include first aid treatment for seizures (see Table 23-2), the importance of compliance with long-term medication regimens, and general reassurance that the child can lead a normal life. Medications used in the treatment of epilepsy are outlined in Table 23-3. The gum hypertrophy (Figure 23-10) that occurs as a side effect of phenytoin (Dilantin) will require meticulous oral hygiene and special care, especially if orthodontic treatment is necessary. Death or serious injury rarely occurs from a seizure, and it does not cause mental deterioration. The Individuals with Disabilities Education Act (IDEA) guarantees children with disabilities the right to publicly financed educational programs in the least restrictive environment possible.

Status epilepticus: A prolonged seizure that does not respond to treatment for 30 minutes or more is called status epilepticus; it can result in brain hypoxia. A common cause is sudden stopping of epilepsy medication or generalized infection. Treatment includes managing airway, providing oxygen, observing and documenting details of the seizure, and providing IV therapy. Diazepam, lorazepam, phenytoin, or a pentobarbital drug may be given intravenously. Rectal diazepam or intranasal midazolam are safe and effective approaches in treating status epilepticus. The child may need to be supported on a mechanical ventilator until seizures are controlled.
Other Conditions Causing Decreased Level of Consciousness
Several conditions are mistaken for epilepsy because they involve paroxysmal altered levels of consciousness. These conditions do not respond to antiepileptic drugs.
Benign Paroxysmal Vertigo: This condition occurs in children under 3 years of age, who often develop ataxia and fall. Nausea, vomiting, and complaints of motion sickness and migraine headache follow. The condition responds to dimenhydrinate (Dramamine) medication.
Night Terrors: Night terrors occur in children between 5 and 7 years of age. The child may sleepwalk, thrash, scream, and be unaware of his or her surroundings. A period of sleep follows. Brief treatment with diazepam (Valium) or imipramine (Tofranil) may be helpful, but family dysfunction should be investigated.
Breath-Holding Spells: Breath holding can result in cyanosis or extreme pallor. Episodes of breath holding are most common between 2 and 5 years of age. The child loses consciousness, and the parents are frightened. Counseling parents to avoid reinforcing the behavior by refusing to play with or hold the child after the episode is helpful.
Cough Syncope: Cough syncopes are paroxysmal coughing spells, usually at night, that result in a diminished cardiac output, cerebral hypoxia, and loss of consciousness. The condition usually occurs in asthmatic children. Prevention involves avoidance of bronchoconstriction.
Prolonged QT Syndrome: One type of sudden loss of consciousness is associated with vigorous exercise. It can be caused by a heart problem and reflected as a prolonged QT segment on the ECG, and it can result in loss of consciousness and death. It usually occurs during adolescence and arises from a defect in chromosome 11. Beta-blockers may be lifesaving. Knowledge of cardiopulmonary resuscitation (CPR) and exercise restriction are essential.
Rage Attacks, or Episodic Dyscontrol Syndrome: Rage attacks are sudden recurrent attacks of violent physical behavior. These attacks appear out of control and are followed by fatigue, remorse, and amnesia. The EEG is usually normal. This condition is often mistaken for complex partial seizure epilepsy.
Cerebral Palsy
Pathophysiology: Cerebral palsy (CP) is a term used to describe a group of motor disorders caused by dysfunction of various motor centers in the brain. A definition proposed in 2006 suggests that CP “is a group of permanent disorders of the development of movement and posture, causing activity limitations that are attributed to non-progressive disturbances occurring in the developing fetal or infant brain” (Rosenbaum, et al., 2007, p. E569). It also involves problems with sensation and communication secondary to the musculoskeletal problems. It is now believed that CP results most often from existing prenatal brain abnormalities, exposure to maternal chorioamnionitis in utero, prematurity, and severe hypoglycemia. CP can be acquired as a result of shaken baby syndrome, meningitis, or encephalitis. Some 15% to 60% of children with CP also develop epilepsy. CP is not fatal in itself, but currently there is no cure. It is one of the most common disabling conditions seen in children and occurs in as many as 2 per 1000 live births (Kliegman et al., 2007).
Manifestations: The symptoms of CP vary with each child and may range from mild to severe. Many children with CP have normal intelligence. The disease is suspected during infancy if there are feeding problems, seizures not associated with high fever, and developmental delays. Developmental milestones are not achieved at the expected age level. Persistence of primitive reflexes such as the Moro and tonic neck reflexes may be seen. Diagnostic tests may include metabolic and genetic testing and MRI. Early recognition is important for appropriate referrals.
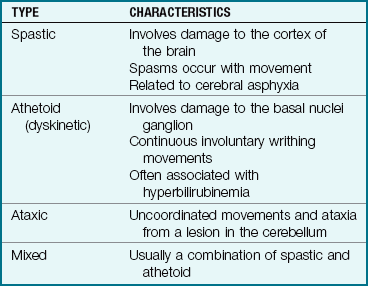
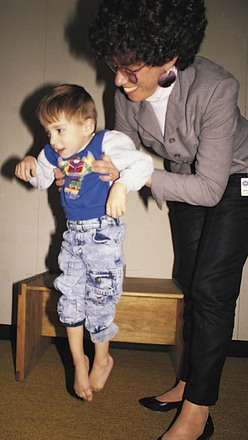
There are four types of CP (Table 23-4). Two of the more common are those marked by spasticity and athetosis (Figure 23-11). These conditions occur in about 75% of the cases. Spasticity is characterized by tension in certain muscle groups. The stretch reflex is present in the involved muscles. When the child tries to move the voluntary muscles, jerky motions result. Eating, walking, and other coordinated movements are difficult to accomplish. The lower extremities are usually involved. The legs cross and the toes point inward. The arms and trunk may also be affected. In athetosis the child has involuntary, purposeless movements that interfere with normal motion. Speech, sight, and hearing defects or seizures may be complications. The success in preventing kernicterus in the newborn by effective treatment of hyperbilirubinemia has reduced the incidence of the athetoid type of CP.
Treatment and Nursing Care: The goal of treatment of children with CP is to assist them in making the most of their assets and to guide them in becoming well-adjusted adults, performing at their maximum ability. Both short- and long-term goals must be realistic. Parents need help in accepting the child and should not be deceived into expecting miraculous cures from treatment. Early diagnosis can result in fewer physical and emotional problems. Botulinum toxin has been used successfully to manage spasticity problems, and levodopa has helped control some athetoid symptoms. An implanted pump that delivers baclofen directly into the intrathecal space around the spinal cord can reduce spasticity. This type of medication delivery produces less acute side effects than oral baclofen. Antiepileptic drugs such as carbamazepine (Tegretol) and valproic acid (Depakote) may be prescribed if seizures are present. Pain management and medication for gastroesophageal reflux may be prescribed. Dental hygiene is important because phenytoin, often prescribed for seizures, causes gum hyperplasia. Computerized toys customized to the child aid in developing hand-eye coordination. Voice-activated computer technology can also aid the child to communicate needs and manage wheelchairs. Physical therapy is essential to prevent contractures and deformities. Approximately 30% to 50% children with CP are mentally handicapped, but many children with severe, spastic quadriplegia have normal intelligence. Gastrostomy tube feedings may be required to augment nutritional intake (see Skill 22-10).
Parents must be informed of community resources available to them. The family’s religious affiliation should not be overlooked, because it can be a source of support and help during times of stress. The long course of this disability can place a financial burden on the family. Caregivers need respite care from time to time to enhance their coping skills.
The specific treatment is highly individualized and depends on the severity of the disability. It is not uncommon for the parents of children with CP to become the experts in caring for their child. Therefore the parent should be an integral part of the health care team.
Good skin care is essential for the child with CP. The nurse observes the skin for redness and other evidence of pressure sores. All precautions are taken to prevent the formation of contractures (degeneration or shortening of the muscles because of lack of use), which could result in permanent loss of function of the part involved (e.g., leg, arm, or finger). The nurse encourages these children to do as much as they can for themselves. When they bathe, they are encouraged to put their muscles and joints through the normal range of motion. The nurse must use judgment in assessing their capabilities and assist only in those areas where they are lacking.
Other measures necessary to prevent contractures include frequent changes of position, the use of splints, and the carrying out of passive, range-of-motion, and stretching exercises. The nurse must also ensure that the child maintains good posture while in bed. This is done through the use of footboards and the proper positioning of pillows and other comfort devices.
Braces are often used to treat contractures. A brace is a mechanical aid that supports weakened muscles or limbs. All braces are routinely checked for correct alignment, loose or missing parts, and the condition of straps and buckles. The child needs assistance to adjust to this unfamiliar device. Wheelchairs and crutches are designed to fit the child.
Orthopedic surgery may be indicated and may be followed by an extensive period of rehabilitation. The nurse must remember that the child is in a continuous state of psychological and physical growth during this period. Interest, or a lack of it, may have a decided effect on the personality of the child in later years.
Feeding problems can lead to nutritional deficiencies. Vitamin, mineral, or protein supplements may be indicated for some children. Swallowing and sucking may be difficult. Vomiting is common because the gag reflex is overactive. The entire body may become tense. The nurse must be especially careful to feed the child slowly to prevent aspiration. It is difficult for these infants to adjust to solid foods, and it takes a great deal of patience on the part of parents and nurses to help the child to adapt to this new experience (Skill 23-1 and Figure 23-12). As the children grow, they can be taught to manage special feeding equipment so they are able to eat independently. They are also taught such activities as dressing and combing their hair. Dental care is discussed in Chapter 15.
Skill 23-1 General Modifications and Precautions in Pediatric Feeding Techniques for Children with Cerebral Palsy








1. Ensure proper positioning and support of the head and back before feeding solid foods.
2. Place small amounts of food on a spoon to prevent choking.
3. Avoid tilting the head back during feeding of solid foods, because this will place the swallowing mechanisms out of alignment.
4. Do not touch the tip of the child’s tongue with the spoon, because this can activate the tongue extrusion reflex.
5. Use rubber-coated spoons for children with hyperactive bite reflex to protect the teeth from injury.
6. Gently stroke the angle of the jaw below the ears to relax the bite of a child who has clamped down on a spoon.
7. Gently stroke the area under the chin in a circular motion to stimulate chewing when food is held in the mouth.
8. Gently press upward under the chin to stimulate swallowing when fluid is held in the mouth.
9. To help a disabled child drink from a cup, cut the top portion of the paper or plastic cup away to provide space for the nose. This will enable the cup to be tilted without the child’s head being tilted back.
10. Avoid excessive pressure on the back of the head when positioning a disabled child for feeding to prevent reflex responses in the body or torso position.
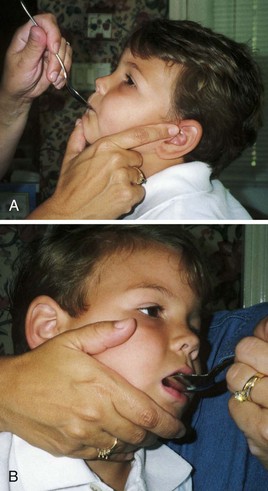
FIGURE 23-12 Feeding the disabled child. A, Manual jaw control is supplied anteriorly. B, Manual jaw control is provided from the side.
The physically challenged child needs opportunities to play alone and with other children. Games suited to ability, such as finger painting, are fun and allow freedom of expression. Activities that require fine muscular movements of the hand cause frustration in the child whose arms and hands are affected by the disease. The nurse can learn a great deal from the parents about the types of play the child enjoys. Children with CP tire easily but find it difficult to relax. They use a great deal of energy to accomplish the simplest of tasks, and they do not respond well to being hurried or overly stimulated.
Educational opportunities geared to the child’s abilities are essential. Public Law 94-142 mandates that public schools provide education for disabled children. The child’s mental capacity is determined not just in the light of the intelligence quotient (IQ) itself but also by the demonstrated potential of the individual.
Preschools and summer camps for exceptional children are available. These programs vary in quality and extent of services. Parents are also referred to the United Cerebral Palsy Association, a national organization that provides education and support services. The expanding role of nurses in the home and schools may further assist in mainstreaming these children into educational and social situations (Box 23-3).
Successful experiences help to improve a child’s self-concept; repeated failures are demoralizing and may lower self-esteem. The health care team works to bring satisfaction to these children by making it possible for them to succeed. The amount of confidence and self-respect that a disabled child has depends a great deal on a supportive environment.
Mental Health Needs of the Physically Challenged Child: The requirements for good mental health in the physically challenged child do not differ from those of other children. They need to have their basic human needs satisfied and people who are genuinely interested in them. The disabled child must participate to the fullest extent in family, school, and community activities. Friendships with other disabled and nondisabled peers are encouraged. Extended family and the community are important resources. Educational programs are integrating the disabled more fully into the community. Barrier-free buildings and modifications that improve accessibility contribute positively to these efforts.
Cognitive Impairment
Cognitive impairment is a term that encompasses any type of mental deficiency or mental retardation.
Mental Retardation: Mental retardation is one type of developmental disability characterized by mental and physical impairment. It had been defined as below-average mental functioning (IQ below 75) and a deficit in adaptive behavior manifested during the developmental period (before 18 years of age) (Box 23-4). Beginning in 1992 the American Association of Intellectual and Developmental Disabilities (AAID) refocused the definition of mental retardation; the emphasis was shifted away from IQ alone and onto a relationship-oriented concept of the cognitively impaired person functioning within an environment (American Association on Mental Retardation [AAMR], 2010). The classification involves four levels of support systems needed for activities of daily living (ADLs): the need for intermittent support, limited support, extensive support, or pervasive (total) support. Mental retardation has many descriptive labels. The specific terminology most often used in the medical field is mental retardation, or cognitive impairment. The education system most often uses mentally handicapped, mentally deficient, mentally disabled, mentally impaired, or mentally challenged. The education system uses various criteria for classroom placement and eligibility for available resources. For educational purposes, cognitively impaired children may be classified as educable, educable-mentally retarded (mildly impaired), or trainable mentally-retarded (moderately impaired). U.S. federal law provides for services from birth to 21 years of age. Public law requires providing the least restrictive environment possible for learning, and mainstreaming with nonimpaired students whenever possible.
When a child is diagnosed as mentally retarded, it is important to correlate growth and development with mental functioning. For example, abstract thinking does not begin to appear before 12 years of age. A child classified as mentally retarded is not necessarily retarded in all areas of mental functioning (Box 23-5). There are numerous tests to measure intelligence. One test that is often given to children and adolescents is the Stanford-Binet.
Intelligence in children is difficult to evaluate and is best tested on an individual basis. Personality tests such as picture story tests, ink blot tests, drawing tests, and sentence completion tests may also be administered. All such tests have their limitations, and of course their accuracy is subject to the abilities of the person interpreting them. Nonetheless, the tests are of value when used in conjunction with a thorough study of the child’s physical, mental, emotional, and social development.
There are many causes of mental retardation. Some conditions that can be detected during the neonatal period are phenylketonuria, hypothyroidism, fetal alcohol syndrome, Down syndrome, malformations of the brain (e.g., microcephaly, hydrocephalus, craniosynostosis), and maternal infections such as cytomegalovirus (CMV). Birth injuries or anoxia during or shortly after delivery may also cause mental retardation. Conditions such as meningitis, lead poisoning, neoplasms, and encephalitis can cause mental retardation in a child or adult of any age. Heredity is a factor in mental retardation. It is also possible that living in a physically and emotionally deprived environment causes the child to be mentally retarded.
A diagnosis of mental retardation is determined after a thorough study is made. The American Psychiatric Association (2000) provides diagnostic criteria for mental retardation in the DSM-IV-TR. Conditions such as epilepsy, CP, severe malnutrition, emotional disturbances, blindness, deafness, and speech disorders must be ruled out. In certain cases, early recognition and intervention can lessen or prevent mental retardation. The child may be classified as having a developmental delay before a diagnosis of cognitive impairment is made.
Other symptoms of mental retardation are associated with milestones of the growth process. Children who do not achieve milestones at the expected age may be cognitively impaired. Unusual clumsiness and failure to respond to stimuli are also early indications. Sometimes this disorder is not discovered until the child enters school. There are many tests for assessing adaptive behaviors including the Vineland Social Maturity Scale and the Adaptive Behavior Scale. Each case must be frequently reevaluated according to the child’s individual progress. The goal of care is to normalize the child and family as much as possible.
Nursing Tip
Cognitively impaired children have the same psychosocial needs as all other children but cannot express themselves or respond as other children do.
The importance of success in the approach to the mentally retarded child: We cannot all run at the same speed, sing with the same ability, dance as gracefully, or draw as skillfully as some of our peers. Yet most of us get by. However, problems can develop if one is not good in something such as reading, writing, and communicating (which, in our culture, is very important). The problems usually relate to the consequences of chronic failure. Computers can assist with spelling deficiencies, and calculators can assist with math deficiencies.
The pediatric nurse must assist the parents to understand that providing experiences that the child can be successful in, and concentrating on his or her strengths rather than weaknesses, are the keys to dealing with a child who is developmentally different. A child who experiences consistent failure becomes angry. The anger causes behavior difficulties that can cloud the problem and the therapy.
Management and nursing goals: An individualized plan of care with goals and objectives is vital to managing mentally retarded children and helping their families. The initial step is to present the findings to the family and to provide the emotional support necessary to cope with a disabled child. The child’s competence and adaptive behaviors should be discussed along with the deficiencies. Introduction to the multidisciplinary team for long-term management is important. Play therapy should be prescribed to nurture growth and development. The Special Olympics introduce healthy competition to the cognitively and physically impaired child. Receptive and expressive communication skills are developed with professional help.
Nurses must be familiar with the resources of the community so that they can direct the family to them. The local chapter of the AAMR may provide information and support. Summer camps, such as those run by the Easter Seals Society, provide stimulation and opportunities for socialization to children with mental and physical disabilities. The child guidance clinic or the psychological services of a nearby college or hospital may be used. Arrangements for proper dental care must be made because some children may be unable to cooperate with the necessary procedures.
The nurse caring for the mentally retarded child in the hospital must know the child’s stage of maturation and ability. A detailed history, including a habit and care sheet, is completed. Self-help activities are documented. Home routines are to be followed as closely as possible to avoid the reversal of gains already made. Good communication between the parents and the nurse can help to make the transition from home to hospital as smooth as possible for the child. A positive approach is recommended when obtaining information about the child from the parents. A request such as “Tell me about Carla’s eating habits” is preferable to “Does she feed herself?” and is likely to yield more helpful information.
Nursing Tip
Nursing responsibilities for disabled children include the following:
Prevention: The outlook is good for continued success in the prevention of mental retardation. Nurses can contribute to this by promoting genetic counseling, immunizations, newborn screening, and good prenatal care (Table 23-5). Comprehensive programs for early assessment and treatment of mentally retarded persons must also be promoted. The nurse can serve as an advocate for the child and/or adolescent to help ensure that his or her rights are upheld.
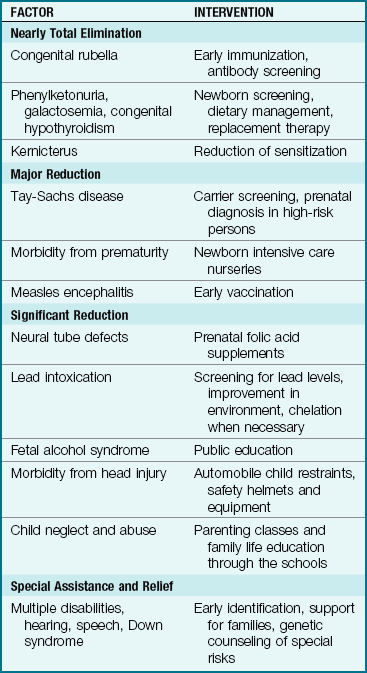
Head Injuries
Head injuries are the major cause of death in children older than 1 year of age. More physical force is needed to produce brain trauma when the head is in a fixed position than when it is freely moving—a fact that supports the use of infant car seats. The incidence of head injury among children is high. A concussion is a temporary disturbance of the brain that is usually followed by a period of unconsciousness. It jars the brainstem and is often accompanied by a loss of memory for events that occurred immediately before (retrograde amnesia), during, and after the accident. A skull fracture indicates that the skull bone is broken or depressed. Bleeding may occur, resulting in pressure being exerted on the brain.
The response of the child to a head injury may differ from that of the adult. The location and type of skull fracture may not correlate with clinical findings. Careful clinical assessment is essential to determine the extent of brain injury. The surface area of a child’s scalp is large and very vascular. Significant blood loss can result from scalp lacerations.
Safety Alert!
A concussion with resulting amnesia and confusion can be more serious than the presence of a fractured skull with no clinical symptoms.
Pathophysiology: A skull fracture, brain concussion, contusion, or intracranial hemorrhage may occur at the time of injury. Brain injury may occur at the point of impact, or on the opposite side of the brain (coup-contre-coup). Therefore, a blow to the occiput can result in an injury to the temporal area as the brain hits the bony skull. Hypoxia, increased ICP, cerebral edema, and infection can occur within a few days. Hypoxia causes the brain to need increased energy, which results in increased cerebral blood flow. This increased blood flow (hyperemia) increases cerebral edema. If the ICP rises too high, cerebral perfusion diminishes, and brain damage or death results. If the fontanelles are open, the tolerance for increased ICP is higher in infants. Older children and adults do not have this advantage.
A child who sustains a mild bump to the head, retains consciousness, and does not vomit may have a covered ice pack applied to the site. During the first night after a bump on the head, parents are advised to be sure that they can arouse the child at least once, because intracranial bleeding occasionally occurs from a minor injury. They should be advised to contact a physician if the child appears confused, has trouble seeing or speaking, or walks unsteadily. Confusion and amnesia after any head injury may indicate a concussion even if consciousness is not lost.
Roughly shaking an infant can cause the brain to strike the inside of the skull (shaken baby syndrome). This can cause tearing of the nerve fibers within the brain, which can result in retinal, subarachnoid, and subdural hemorrhages as well as high-level cervical spine injuries and permanent disability or death. Teaching coping techniques to parents of a child who cries inconsolably can prevent this type of injury. Infants suspected of shaken baby syndrome must be reported to local authorities. This type of pathologic condition can also result from an infant being held by a person who is repeatedly jumping high on a trampoline.
A child who has suffered a blow to the head is often brought to the hospital for overnight observation to rule out or confirm the extent of injury. The child may experience all or some of the following symptoms:
In severe cases, the child may be completely unconscious. Decerebrate posturing (extensor posturing) or decorticate posturing (flexor posturing) may be evident (Figure 23-13). In decerebrate (extensor) rigidity, all four limbs are extended and the hands are pronated. This may indicate brainstem injury. In decorticate (flexor) rigidity, the arms, wrists, and fingers are flexed. Plantar flexion occurs in the feet. This may indicate damage to the cortex of the brain. These pathological postures (posturing) are seen with severe brain injury.
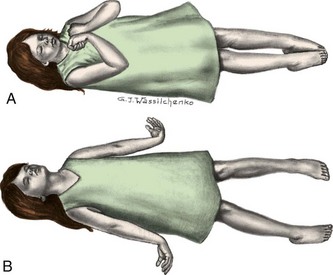
FIGURE 23-13 Posturing. Pathological posturing that may occur in the children with severe brain damage. A, Decorticate (flexor) posturing. B, Decerebrate (extensor) posturing.
A careful history is obtained to determine any preexisting conditions and to ascertain the exact circumstances of the accident. Of particular importance is the child’s state of consciousness immediately after the accident.
The nurse observes the child for signs of increasing ICP. There are four components of a cranial or neurological check:
2. Pupil and eye movement (Figure 23-14)
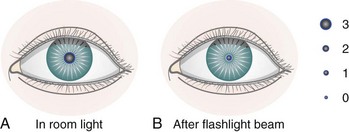
FIGURE 23-14 The response of the pupil of the eye to a flashlight beam. A, The pupil of the eye is a 3 in room light. B, The pupil of the eye is a 1 after a flashlight beam is directed at the eye. The letters B, S, and N may be used to denote brisk movement, slow movement, or nonmovement of the pupil response. This illustration would be recorded “3/1 B.” The other eye should respond symmetrically. Sluggish movement, nonmovement, or asymmetrical response should be reported immediately.
4. Motor activity (Box 23-6)
Children are handled gently and are inspected for injuries to other areas. They are placed in a crib or bed in accordance with their age. Side rails are raised, because seizures are not uncommon. The head of the bed is slightly elevated to decrease cerebral edema.
Level of Consciousness: Changes in level of consciousness are particularly meaningful and necessitate immediate medical attention. Consciousness implies awareness or the ability to respond to stimuli. It also includes cognitive power, which is the ability to produce verbal and motor responses. The child’s alertness on admission is recorded for use as baseline data. The response should be correlated with the child’s developmental age. Parents can be helpful in providing information about the child’s usual capabilities. In general, children should be oriented to person, time, and place (according to developmental capabilities). The nurse asks, “What is your name?” and “Where are you?” Older children may know the day of the week. The child should recognize parents. The nurse points to the mother and asks, “Who is this?” The child should be able to follow simple commands, such as “Turn over.”
When the child does not respond to verbal stimuli, the upper arm is gently pinched and the response is observed. The presence or absence of crying or speech is noted. It is not unusual for children to fall asleep, but they should be easily aroused. The nurse records changes in sleeping posture, movements of extremities, and any signs of tremors or restlessness. The bladder is observed for distention, which can contribute to irritability. Incontinence in the child who is toilet-trained is significant. The child’s behavior is described in the nurse’s notes. The Glasgow Coma Scale is valuable in standardizing the description and interpretation of various levels of consciousness. It includes eye opening and motor and verbal responses. The lower the score, the deeper the level of unconsciousness or coma. A score of 8 or less usually necessitates immediate medical intervention. Table 23-6 shows a scale modified for infants.
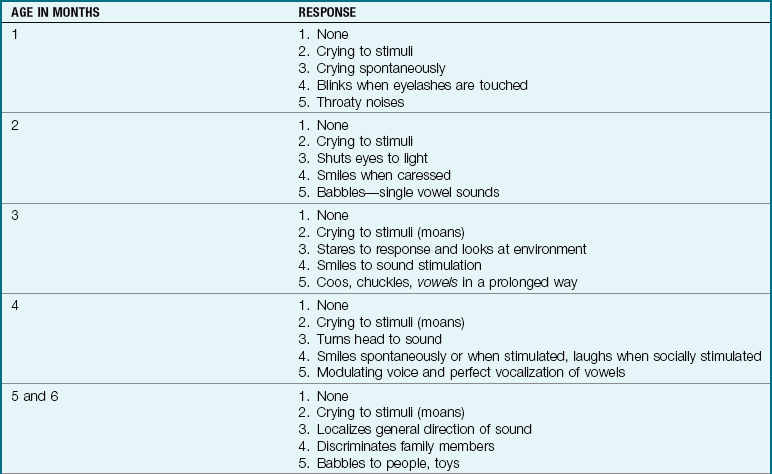
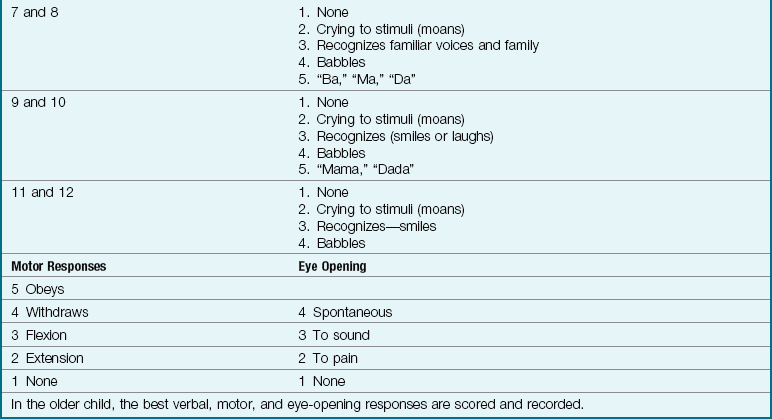
Vital Signs: An increase in blood pressure and a decrease in pulse and respiration are evidence of increased ICP. Temperature elevations may result from inflammation, systemic infection, or damage to the hypothalamus, which regulates body temperature. Mild elevations caused by trauma are not uncommon during the first 2 days after a head injury.
Motor Activity: Because nerves energize the muscle tissue, any damage to the nervous system affects body movement. The quality and strength of muscle tone are observed in all four extremities. The child should be able to move the legs and push against the nurse’s hands with both feet. The face should be symmetrical. The child can smile and frown. Drooping of the eyes (ptosis), inability to close the eyes tightly, and drooping of the corner of the mouth are considered pathological. The child should be able to raise the arms and extend the palms upward and downward. Abnormal posturing is described and recorded.
Nursing Care: Nursing care includes examination of wound swelling if a laceration of the head is present. The type and amount of drainage from the ears and nose are recorded. The nurse checks for nuchal (neck) rigidity, which might indicate infection such as meningitis. Occipital-frontal circumference of the head is monitored in infants, as are tension of the fontanelles and the presence of a high-pitched cry. Fluids are carefully monitored to control cerebral edema. Feeding difficulties should be noted as the child’s diet is increased. The child is observed for signs of shock, which can also occur. Children whose condition has remained stable are discharged. Parents are instructed about any additional observations and follow-up care.
Near-Drowning
Accidental drowning or near-drowning is the fourth leading cause of death for U.S. children under 19 years of age. Near-drowning is defined as survival beyond 24 hours after submersion. Proper supervision and environmental safety precautions are the best measures to prevent drowning. In adolescents the use of illicit drugs and alcohol during recreational swimming contributes to drowning incidents. The priorities include the immediate treatment of hypoxia, aspiration, and hypothermia.
Cardiorespiratory survival has increased with advances in emergency medical treatment by paramedics on site and the technology available in intensive care units in the hospital. However, CNS injury remains the major cause of death or long-term disability.
Submersion of more than 10 minutes with failure to regain consciousness at the scene or within 24 hours is an ominous sign and is predictive of severe neurological deficits if the child survives. Respiratory and cardiovascular support, controlled rewarming, and maintenance of adequate cerebral oxygenation are priorities of care (Nursing Care Plan 23-1). The parents need to be offered support, explanations of the therapy, and referral to social services, religious, or community agencies for follow-up. Most drownings can be prevented by adult supervision and water safety and survival training, and nurses can advocate for these in schools and communities
23-1  Nursing Care Plan
Nursing Care Plan
The Child with Altered Level of Consciousness
A 4-year-old child fell into a pool while playing, hitting his head on the pool deck. Cardiopulmonary resuscitation reestablished a heartbeat and spontaneous respirations. The child is admitted with signs of increased intracranial pressure, including a decreased level of consciousness and an absence of the gag reflex.
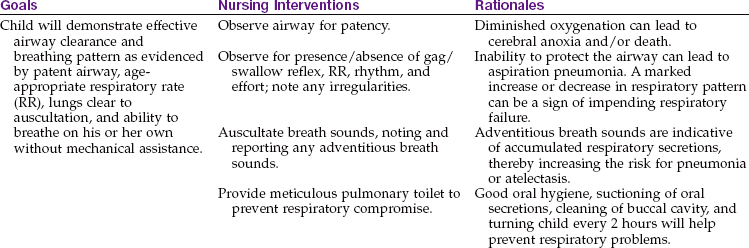
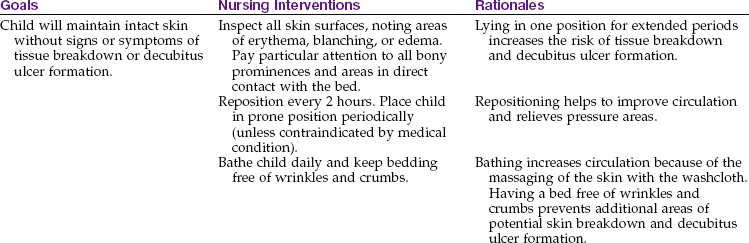
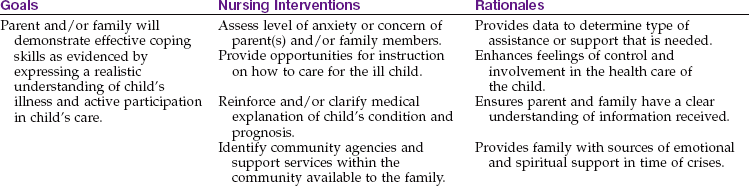
Get Ready for the NCLEX® Examination!
Key Points
• Infants are more prone to ear infections than older children because their eustachian tubes are shorter, wider, and straighter.
• When instilling ear drops in infants, gently pull the pinna down and back. In children, the pinna is gently pulled up and back.
• In paralytic strabismus the unaffected eye is patched.
• Level of consciousness is the most important indicator of neurological health.
• Nursing care of the unconscious child includes assessing the child for increased intracranial pressure (ICP), maintaining an open airway, providing adequate nutrition and fluids, positioning, maintaining flexibility of joints, and preventing injury.
• A high-pitched cry may be indicative of increased ICP.
• Do not give aspirin or other salicylates to children with symptoms of influenza or chickenpox, because the drug is linked to Reye’s syndrome, a serious and life-threatening illness.
• Meningitis is an inflammation of the meninges that cover the brain and spinal cord.
• A seizure is a symptom of an underlying pathological condition.
• Grand mal seizures involve an aura, tonic and clonic phases, and postictal lethargy.
• Decerebrate, decorticate, or opisthotonos posturing indicates brain damage.
• The response of the pupils to light and ascertaining level of consciousness are essential assessments to determine brain injury.
• The Glasgow Coma Scale is used to determine level of consciousness in infants and children.
• “Shaken baby syndrome” can result in subdural hematoma and death.
• Confusion and amnesia after a head injury may indicate concussion even if consciousness is not lost.
• The four types of cerebral palsy are spastic, athetoid, ataxic, and mixed.
• Many children with spastic quadriplegia have normal intelligence.
• Computer technology can help the physically impaired child communicate and achieve mobility.
• Mental retardation involves three components: intelligence, adaptive behavior, and onset before 18 years of age.
• The priority of care for a child who has experienced near-drowning is to prevent hypoxia, aspiration, and hypothermia.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
 Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Epilepsy Foundation: www.epilepsyfoundation.org/
• Hydrocephalus Foundation: www.hydroassoc.org
• National Hearing Center: http://nationalhearingcenter.com/
• Pediatric head injuries: www.brainline.org
• Sight and Hearing Association: www.sightandhearing.org
Review Questions for the NCLEX® Examination
1. Symptoms of an earache in an infant include:
1. external drainage, pain, and decrease in temperature.
2. tugging at the ear and rolling head from side to side.
2. A parent asks the nurse to tell her what cerebral palsy is. The best response of the nurse would be that it is a:
1. motor disability caused by a nonprogressive disturbance in brain development.
2. disorder of the brain that results in mental retardation.
3. complication of the birth process that causes brain damage.
3. Reye’s syndrome affects the:
4. A practice that has been helpful in preventing mental retardation is:
5. Which term describes a seizure in which the child cries out, falls to the floor, becomes rigid, and then has a convulsion?