The Infant
1 Define each key term listed.
2 Describe the physical and psychosocial development of infants from age 1 to 12 months, listing age-specific events and guidance when appropriate.
3 Discuss the major aspects of cognitive development in the first year of life.
4 Relate the nursing responsibilities in health promotion and illness prevention of infants during the first year of life.
5 Discuss the nutritional needs of growing infants.
6 Compare breastfeeding, bottle feeding, and the various infant formulas available.
7 Describe how to select and prepare solid foods for the infant.
8 List four common concerns of parents about the feeding of infants.
9 Discuss the development of feeding skills in the infant.
10 Compare and contrast natural, organic, and processed foods.
11 Examine nutritional counseling for the infant.
12 Identify the approximate age for each of the following: posterior fontanelle has closed; central incisors appear; birth weight has tripled; child can sit steadily alone; child shows fear of strangers.
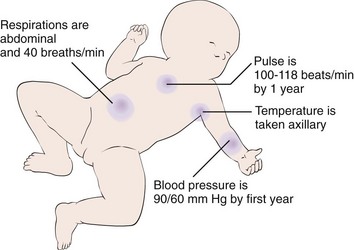
13 Describe normal vital signs for a 1-year-old infant.
14 Discuss safety issues in the care of infants.
15 Discuss the approach to and the specifics of care of an infant with colic.
16 Identify age-appropriate toys and their developmental or therapeutic value.
 , p. 397)
, p. 397) , p. 398)
, p. 398) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Physical, emotional, and cognitive growth and the development of motor abilities occur rapidly during the first year of life. Milestones of growth and development describe general patterns of achievements at various stages of infancy. These milestones, or patterns, are referred to as norms. Norms can vary greatly for the individual child, but the nurse must understand the normal range for milestone achievement to assess the progress of growth and development of the infant and initiate early referral for follow-up care.
During the neonatal phase of development, the chief tasks mastered were the establishment of effective feeding patterns and a predictable sleep-wake cycle. Infants who have unmet hunger needs can become irritable, may not perceive feeding as pleasurable, and may fail to develop trust in the caregiver. Parental bonding and social interaction begin in the neonatal phase but heighten when the infant begins to respond with a social smile, making the caregiver feel “loved.”
By the time the infant is age 4 to 6 months, the positive parental interaction with the infant should be obvious during clinic visits. If the parent does not appear to enjoy the developmental changes in the infant at this age or does not appear relaxed during interactions with the infant, further follow-up of possible family dysfunction or social or mental stresses should be initiated.
By age 9 months, control of feeding may become an issue of conflict between parent and infant. The parent needs to “let go” and introduce the infant to finger foods and initiate drinking from a cup. Offering limited choices can reduce conflict as the infant reaches toward autonomy. If the nurse notices an overly neat and orderly approach during feeding, parental guidance may be necessary. Separation anxiety (see Chapter 21) can be expected by the ninth-month clinic visit, and the nurse should expect to spend some time playing with the infant and getting to know the infant to establish the rapport necessary for a successful physical assessment. Repetition is the key to successful parent teaching and counseling by the nurse.
Children, unlike adults, are in the process of growing while they are hospitalized. To provide total patient care, the nurse must be able to recognize a patient’s needs at various stages of growth and development. The pulse rate, respiration, and blood pressure measurements that are normal for an infant are not normal for the adult patient (Figure 16-1). The nurse must try to meet individual needs effectively and to administer the specialized nursing care required for the particular patient. The most common cause for concern about a child is a sudden slowing, not typical for age, of any aspect of development.
General Characteristics
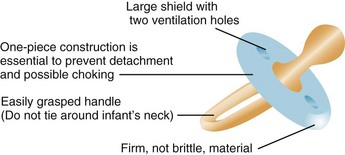
Sucking brings the infant comfort and relief from tension. This oral stage of personality development is important for the infant’s physical and psychological development. The nurse, knowing the importance of sucking to the infant, holds the infant during feedings and allows sufficient time to suck. Infants who are warm and comfortable associate food with love. The infant who is fed intravenous fluids is given added attention and a pacifier to ensure the necessary satisfaction of sucking (Figure 16-2). When the teeth appear, the infant learns to bite and enjoys objects that can be chewed. Gradually, the infant begins to put fingers into the mouth. When infants can use their hands more skillfully, they will not suck their fingers as often and will be able to derive pleasure from other sources.
Motor Development
The grasp reflex is seen when one touches the palms of the infant’s hands and flexion occurs. This reflex disappears at about 3 months. Prehension, the ability to grasp objects between the fingers and the opposing thumb, occurs slightly later (age 5 to 6 months) and follows an orderly sequence of development (Figure 16-3).
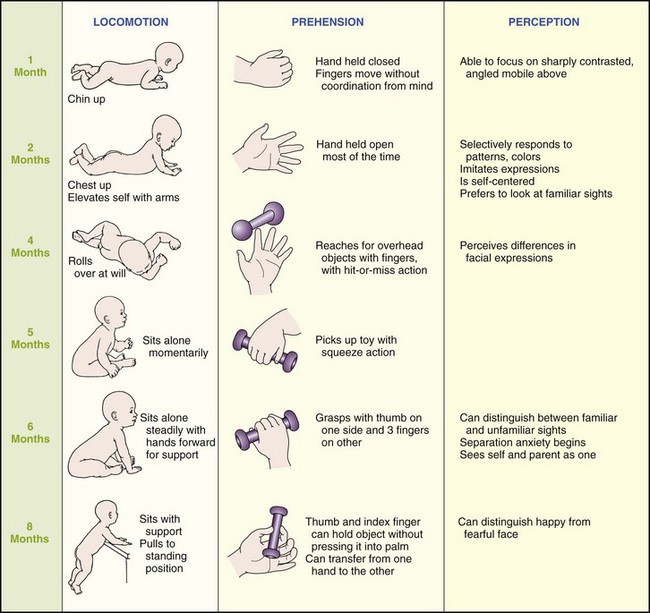
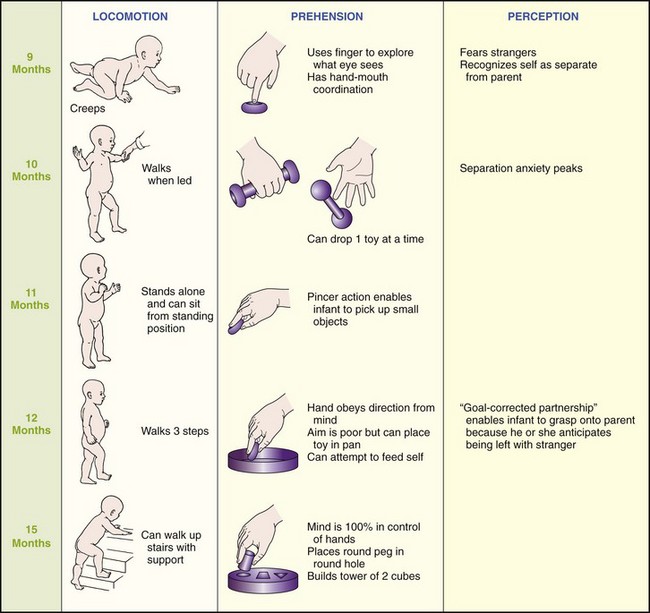
The parachute reflex appears by age 7 to 9 months. This is a protective arm extension that occurs when an infant is suddenly thrust downward when prone. By age 1 year the pincer grasp coordination of index finger and thumb is well-established.
Emotional Development
Love and security are vital needs of infants. They require the continuous affection of their parents. If trust is to develop, consistency must be established. Parents are assured that they need not be afraid of spoiling their infants by attending promptly to their needs. Infants who are consistently picked up in response to crying show fewer crying episodes when they are toddlers and less aggressive behavior at age 2 years. Loving adults affirm that the world is a good place in which to live. Each day the infant becomes impressed by parental actions and learns to imitate and trust caregivers. A sense of trust is vital to the development of a healthy personality. Many consider it to be the foundation of emotional growth. The child who does not develop a sense of trust learns to mistrust people, which could have a permanently negative effect on personality development.
Parents are taught to talk, sing, and touch their infants while providing care. They should not expect too much or too little from them. Infants will easily accomplish various activities if they are not forced before they reach readiness. When an infant shows readiness to learn a task, parents should provide encouragement.
Need for Constant Care and Guidance
The full-time caregiver needs and deserves the understanding of and kind support from relatives at home and from the nurse in the hospital. Pediatrics involves family-centered care. A short break from pressures provides renewed energy with which to enjoy the infant. A trip to the store or a stroll with the infant in the carriage affords stimulation and a change of environment for the infant and the caregiver. The infant who is constantly left in a crib or playpen and is not introduced to a variety of learning experiences may become shy and withdrawn. Sensory stimulation is essential for the development of the infant’s thought processes and perceptual abilities.
If a mother is unable to room-in with her hospitalized infant, personnel should try to imitate her care by promptly fulfilling the infant’s physical and emotional needs. In the nursery the nurse first feeds the infant who appears hungry, rather than delaying feeding to adhere to a specific routine. Wet diapers are changed as soon as possible. The crying child is soothed. The exactness of time or method of bathing or feeding the infant is less important than the care with which it is done. The infant easily recognizes warmth and affection or the lack thereof.
Development and Care
Box 16-1 is a guide to infant care from the first month to the first birthday. Some of the aspects of care (e.g., safety measures) are important throughout the entire year. The nurse explains to parents that physical patterns cannot be separated from social patterns and that abrupt changes do not take place with each new month. Human development cannot be separated into specific areas any more than the body’s structure can be separated from its function.
Box 16-1 Physical Development, Social Behavior, and Care and Guidance of Infants
Weighs approximately 3.6 kg (8 lb). Has regained weight lost after birth. Gains about 2.5 cm (1 inch) in length per month for the first 6 months. Lifts head slightly when placed on stomach. Pushes with toes. Turns head to side when prone. Head wobbles. Head lags when infant pulled from lying to sitting position. Clenches fists. Stares at surroundings.
Vaginal discharge in girls and breast enlargement in boys and girls from maternal hormones received in utero are not unusual and disappear without treatment.


Sleep: On back; if side-lying position, support back with blanket roll. Use a firm, tight-fitting mattress in a crib with bars properly spaced so that the infant’s head cannot be caught between them. Raise crib rails. Do not use a pillow.
Diet: Breast milk every 2 to 3 hours or iron-fortified formula every 4 hours as infant indicates need. Vitamin D (400 international units/day) in dark-skinned infants, breastfed infants, or infants who are not regularly exposed to sunlight. Burp infant well.
Exercise: Allow freedom from the restraints of clothing before bath. Provide fresh air and sunshine whenever possible. (Protect the infant from sun and insects with sunscreen or protective clothing.) Support head and shoulders when holding infant. Attend promptly to physical needs. Provide colorful hanging toys out of infant’s reach for sensory stimulation.
Sleep: Develops own pattern; may sleep from feeding to feeding.
Exercise: Provide a safe, flat place to kick and be active. Do not leave infant alone, particularly on any raised surface. Physical examination by the family doctor or pediatrician.
Immunization: First diphtheria, tetanus, and whooping cough (DTaP), injectable polio vaccine (IPV), Haemophilus influenzae type b (Hib), and second hepatitis B virus (HBV) vaccine. Still completely depends on adults for physical care. Needs a flexible routine throughout infancy and childhood.
Pacifier: If used, select for safety. Choose one-piece construction and loop handle to prevent aspiration (see Figure 16-2).
Hiccups: Are normal and subside without treatment. Small amounts of water may help.
Colic: Consists of paroxysmal abdominal pain, irritable crying. Usually disappears after 3 months. Place infant prone over arms (see Chapter 22, Figure 22-4, D). Use pacifier. Massage back. Relieve caregiver periodically.

Weighs about (5.9 to 6.8 kg (13 to 14 lb). Drooling indicates appearance of saliva and beginning of teething. Lifts head and shoulders when on abdomen and looks around. Turns from back to side. Sits with support. Begins to reach for objects he or she sees. Coordination between eye and body movements. Moves head, arms, and shoulders when excited. Extends legs and partly sustains weight when held upright. Rooting, Moro, extrusion, and tonic neck reflexes are no longer present.

Sleep: Stirs about in crib. Sleeps through ordinary household noises.
Diet: Mother’s milk or formula.
Exercise: Plays with hand rattles and dangling toys. Start acquainting with a playpen, where infant can roll with safety.
Immunization: Second DTaP, IPV, and Hib.
Elimination: One or two bowel movements per day. May skip a day.


Doubles birth weight. Gains about 3 to 5 or 4 to 7 oz per week during the next 6 months. Grows about 1.3 cm ( inch) per month. Sits alone momentarily. Springs up and down when sitting. Turns completely over. Hitches (moves backward when sitting). Bangs table with rattle. Pulls to a sitting position. Chewing more mature. First solid food introduced. Approximates lips to rim of cup.
inch) per month. Sits alone momentarily. Springs up and down when sitting. Turns completely over. Hitches (moves backward when sitting). Bangs table with rattle. Pulls to a sitting position. Chewing more mature. First solid food introduced. Approximates lips to rim of cup.

Immunization: Continues; see Chapter 32.

Two lower teeth appear. These are the first of the deciduous teeth—the central incisors. Begins to crawl. Moves forward, using chest, head, and arms; legs drag. Can grasp objects more easily. Transfers objects from one hand to the other. Appears interested in standing. Holds an adult’s hands and bounces actively while standing. Struggles when being dressed.


Diet: Add vegetables. Continue to add new foods slowly, observing for reactions.
Exercise: Enjoys jump chair. Rides in stroller. Stuffed toys or those that squeak or rattle are appropriate.
Safety: Remain with infant at all times during bath in tub. Protect from chewing paint from windowsills or old furniture. Paint containing lead can be poisonous. Use safety-lock doors to ovens, dishwashers, washing machines, dryers, and refrigerators.

Sleep: Has generally begun to sleep later in the morning.
Diet: Add meat, beans. Introduce chopped and mashed foods. Place newspaper beneath feeding table. Use unbreakable dishes. Allow infant to pick up pieces of food by hand and put them into mouth.
Safety: Know phone number of nearest poison control center. Avoid using tablecloths with overhangs infant could reach.
Exercise: Is busy most of the day exploring surroundings. Provide sufficient room and materials for safe play. Help infant to learn. Distract curious child from danger. In this way punishment is limited—avoid excessive spankings and “no’s.”


Sleep: Avoid strenuous play before bedtime. A night light is convenient for parent and makes infant’s surroundings more familiar. Use pajamas with feet, because infant becomes uncovered easily.
Diet: Takes juice and water from cup. Solid foods in general are taken well.
Exercise: Tours around room holding adult’s hands. Daytime clothing should be loose so as not to interfere with movement.
Sleep: Greets parents in morning with excited jargon.
Diet: Still spills from cup. Enjoys blowing bubbles.
Exercise: Plays with toys in tub. Enjoys gross motor activity. Kicks, pulls self up.
Safety: Cover electrical outlets. Put household cleaners and medicines out of reach if not previously done. Parent may need to sit infant down in playpen at times, because infant tends to stand to point of exhaustion.
Pulse rate 100 to 140 beats/min. Respirations 20 to 40 breaths/min. Triples birth weight. Height is about 74 cm (29 inches). Stands alone for short periods. May walk. Puts arm through sleeve as an aid to being dressed. Six teeth (four above and two below). Drinks from a cup; eats with a spoon with supervision. Pincer grasp is well-established. Handedness (the preference for the use of one hand), although not fully established, may be evidenced.

Sleep: May take one long nap daily.
Diet: Gradually add egg white and fish (baked, steamed, or boiled). Add orange juice. Add well-cooked table foods. Interest in eating dwindles.
Exercise: Enjoys putting objects in a basket and then removing them. Places objects on head. Distraction is an effective way to deal with determination to do what infant wants regardless of outcome.
No two infants are exactly alike at a certain age. Box 16-1 is just a guide. However, individual variations fall in a range about central norms that serve as guidelines in the evaluation of an infant’s or child’s progress. The addition of the various solid foods to the diet and the time of immunizations vary slightly, depending on the infant’s health and the physician’s protocol. See Table 15-5 for an outline of the parental tasks involved in guiding the infant through the stages of growth and development.
Community-Based Care: A Multidisciplinary Team
The prevention of disease during infancy is of the utmost importance and includes all measures that improve the physical health and psychosocial adjustment of the child. The concept of periodic health appraisal is not new. In the late 1800s, “milk stations” were established at various locations throughout the United States to provide safe water and milk for infants in an effort to reduce the number of deaths from infant diarrhea. Today there are many community resources for the health promotion of infants, including the following:
• The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) program assists parents to obtain formulas and foods.
• Public health and hospital clinics provide follow-up care.
• Head Start and The First Five offer varied support programs.
The social service worker and home health nurse are valuable links to community-based care resources.
Health Promotion
Parenting skills can be impaired because of socioeconomic factors, as well as by physical and mental problems. A prime responsibility of the nurse in the community-based clinic is to guide the parents and assist in the development of the skills necessary to ensure the proper growth and development of their child. The nurse can provide encouragement and explanations of strategies that will enable parents to be successful in coping with various infant behaviors.
The nurse is the important link in the initiation of referral to the multidisciplinary health care team, follow-up of progress, and maintenance of communication between the family and members of the health care team. A home-based infant stimulation program can use a teacher, nurse, occupational or speech therapist, or physical therapist (depending on the specific need of the infant) to directly stimulate the infant and teach the parents how to provide care.
Coping with the Irritable Infant: One of the goals of early parent-infant interaction is to promote a calm, alert infant who can respond to parents and the environment. Success in this area promotes a feeling of competence in the parent. Some infants cannot tolerate environmental stimulation and handling and start to cry during diaper changes, feeding, and rocking. Lights, sound, and movement cause some infants to become irritable. Techniques to cope with these problems include the following:
• Shield the infant’s eyes from bright light.
• Sit quietly with the infant without talking or singing.
• Eliminate noise from radio, television, and computer.
• Change the infant’s position slowly.
• Stop the interaction and reduce environmental stimuli if the infant turns away, squirms, grimaces, or puts the hands in front of the face.
• Swaddle the infant snugly in a lightweight blanket with extremities flexed and hands near the face.
• Provide nonnutritive sucking.
• Rock the infant slowly and gently.
• Cradle the infant firmly in the lap during feeding and remain still during sucking efforts.
Coping with Colic: Colic is characterized by periods of unexplained irritability and crying in a healthy, well-fed infant. Although the exact cause is unknown, it is thought to be a combination of infant, parental, and environmental factors. Colic can interfere with parent-infant interactions if the infant is not soothed by holding or carrying and parental fatigue and guilt develop. Providing periods of rest and “breaks” to parents of colicky infants can prevent a cycle that may lead to child abuse. See Figure 22-4 for an illustration of the “colic carry.” Holding the infant face down and close to the body while supporting the abdomen and providing a gentle rocking motion often soothes the colicky infant. See Nursing Care Plan 16-1 for care of the infant with colic.
 Nursing Care Plan
Nursing Care Plan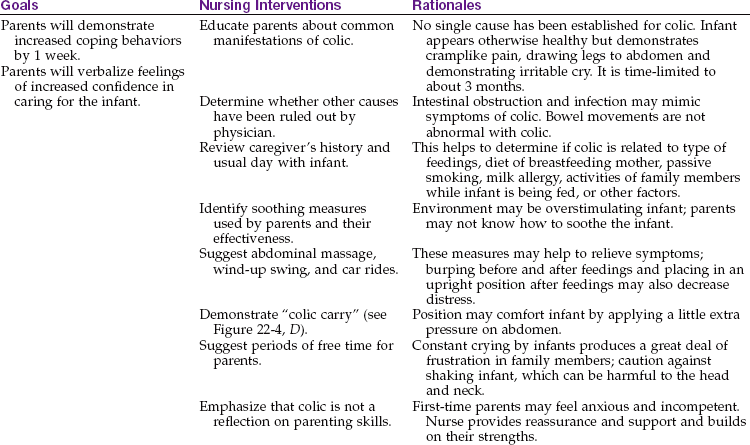
Coping with the Lethargic Infant: Stimulation, interaction, and nourishment are essential for optimal infant growth and development. Some infants respond to an excessively stimulating environment by “shutting down” and sleeping. Coping strategies for dealing with this infant include the following:
Developing Positive Sleep Patterns: Most newborns sleep at 4-hour intervals and increase their sleep intervals to 8 hours by age 4 to 6 months. Synchronizing the circadian rhythm of the infant to the family routine is a learned behavior. Parents must be alert to the infant’s individual rhythm and promote activities that foster a stable synchronized pattern. Infants should be positioned for sleep on their backs and on a firm mattress, both for their safety and to prevent sudden infant death syndrome (SIDS).
Until age 6 months, infants rely on parents to soothe them back to sleep when they awaken during the night. If the parent resorts to midnight pacing or car rides, the infant will learn to rely on the parent to get them back to sleep after age 6 months. The mother should assist the infant to develop “self-soothing” behaviors so the infant can roll over, grasp the pacifier, and return to sleep on his or her own. Helping the infant to achieve this ability will also make parents feel more confident in their parenting skills and less fatigued and frustrated.
 Safety Alert!
Safety Alert!
The American Academy of Pediatrics recommends a supine or back-lying position for infants to avoid sudden infant death syndrome (SIDS). Care should be taken to use a sturdy mattress and avoid soft pillows that can inhibit breathing. Comforters; quilts; loose bedding; and thick, pillowlike crib bumpers can be a danger to an infant in a crib.
Infants with Special Needs
Infants with special needs may require referral to community agencies for follow-up care. Early childhood education programs at colleges and in some day care centers can offer parent guidance concerning growth and development through their infant stimulation programs. A daycare nursery school can be used, and the public school system offers special classes and tutoring for children with special needs. Counseling, behavior management techniques, and cognitive therapy can be provided by a psychologist. Neurodevelopmental therapy (NDT) can be provided by a professional therapist or by an occupational or physical therapist. Speech therapy and auditory testing are also available within the community. The social worker can assist with social and environmental problems (see Chapter 18).
Illness Prevention
Skilled health services today encompass periodic health appraisal; immunizations; assessment of parent-child interaction; counseling in the developmental processes; identification of families at risk (e.g., for child abuse); health education and anticipatory guidance; referrals to various agencies; follow-up services; appropriate record-keeping; and evaluation and audit by peers. These services are provided in a variety of health care facilities. Ideally the infant is seen in the health care setting at least five times during the first year at specific intervals (2 months, 4 months, 6 months, 9 months, and 1 year). Private group practices, hospital-based clinics, and neighborhood health centers are examples of health care settings.
These visits are as important for parents as they are for the infant. They provide caregiver support and reassurance as well as information and anticipatory guidance for the many developmental changes and health issues of the infant’s first year. A common concern is diaper rash, which can cause discomfort to the infant. The mother should be taught the importance of frequent diaper changes, how to wipe from front to back, and the importance of exposing the skin in the diaper area to the air for periods of time. Some commercial diaper wipes may contain fragrance or other ingredients that can further irritate a diaper rash. Soiled areas can be washed with water and mild soap if needed. To prevent skin breakdown, A + D or another protective ointment such as Desitin can be applied when the skin in the diaper area appears pink and irritated.
A careful health history is obtained during routine clinic visits. Growth grids during infancy include measures of weight, length, and head circumference. The reading and recording of growth charts is described in Chapter 15. There are numerous developmental screening tests. In the 1986 Amendment to the Education of All Handicapped Children Act (PL99-457), all states are required to assess for developmental disabilities before age 5 years. Most pediatricians initiate their assessment at birth to enable early intervention. General screening tools are available to identify children in need of referral and further care. Some of the tests include the following:
• Denver Developmental Screening Test (DDST): This test is widely used and tests social, fine-motor adaptive, language, and gross motor abilities from birth to age 6 years.
• Denver Home Screening Questionnaire: This tool provides information concerning the child-rearing environment.
• Early Language Milestone Scale (ELM): Because language is necessary for cognitive development, this test assesses expressive, receptive, and visual language from birth to age 3 years.
• Clinical Linguistic and Auditory Milestone Scale (CLAMS): This test assesses language milestones from birth to age 3 years.
• Ages and Stages Questionnaire (ASQ): This is administered between ages 4 and 48 months.
• Brazelton Neonatal Behavioral Assessment Scale: This scale is of particular value during the newborn period, helping to describe the infant’s emerging personality and evaluate infant reflexes, general activity, alertness, orientation to spoken voice, and response to visual stimuli (see p. 286).
The physical examination is adapted to the infant’s needs. Routine assessments of hearing and vision are an integral part of the examination. In the newborn period, loud noises should precipitate the startle, or Moro, reflex. Localization of sound during infancy can be roughly ascertained by standing behind the child seated on the mother’s lap and ringing a bell or repeating voice sounds. The infant’s response is compared with the average for that age level. Vision is mainly assessed by light perception. The examiner shines a penlight into the eyes and notes blinking, following to midline, and other responses. Laboratory tests may include urinalysis and measurement of hemoglobin or hematocrit levels to detect anemia. Screening tests for various asymptomatic diseases are assuming greater importance; examples of these are the phenylketonuria (PKU), tuberculin, and sickle cell tests.
Immunizations
Health personnel must repeatedly stress to parents the importance of immunizations. A delay can lead to undue risks of serious illness, sometimes with fatal complications.
The nurse can stress to working parents that an unprotected child may become sick, making it necessary for them to lose valuable working hours. Immunization also prevents numerous physician and hospital expenses and is required before school entry. A delay or interruption in a series does not interfere with final immunity. It is not necessary to restart any series, regardless of the length of delay. Accurate records prevent confusion. A detailed discussion of immunizations and common childhood communicable diseases is in Chapter 32.
Nutrition Counseling
The nutritional needs of infants reflect rates of growth, energy expended in activity, basal metabolic needs, and the interaction of the nutrients consumed (Mahan & Escott-Stump, 2008). The infant is born with a rooting reflex, which aids in finding the nipple. The sucking reflex is present at birth. There is a forward and backward movement of the tongue. As the infant grows, neuromaturation of the cheeks and tongue enables advancement to a more mature sucking pattern that uses negative pressure to obtain milk. At about the third to fourth month, the extrusion reflex (protrusion of the tongue), which pushes food out of the mouth to prevent intake of inappropriate food, disappears.
The digestive system continues to mature. By 6 months, it can handle more complex nutrients and is less susceptible to food allergens. The stomach capacity expands from 10 to 20 mL at birth to 200 mL by 12 months. This expansion enables the infant to consume more food at less-frequent intervals. As the pincer grasp becomes more developed, the infant can pick up food with tiny fingers and place it in the mouth. By age 2 years, the child masters spoon feeding.
Taste cells develop during the eighth week of gestation, and the fetus begins to respond to flavors when swallowing amniotic fluid. At birth the infant demonstrates a preference for certain tastes, preferring sweet and rejecting sour. Breast milk may supply flavor experiences based on the mother’s diet. Infants should be given an opportunity to develop their own personal tastes by being offered various foods when solids are introduced.
Parental Concerns: Parents have many concerns about feeding their infant during the first year of life. This is a period when readiness to receive nutrition education is usually high; therefore the nurse looks for opportunities to provide accurate information. Assessment of parental knowledge; infant development, behavior, and readiness; parent-child interaction; and cultural and ethnic practices is important. Nutritional care plans based on developmental levels assist parents in recognizing changes in feeding patterns. The components of a nutritional assessment are discussed in Chapter 15.
 Nursing Tip
Nursing Tip
Human milk or properly prepared formula supply adequate fluid for the infant under normal conditions. The infant may require additional water during illness or hot, humid weather.
A suggested parental guide to determining the adequacy of the diet includes the following:
• The infant has gained 4 to 7 oz per week for the first 6 months.
• The infant has at least six wet diapers per day.
• The infant sleeps peacefully for several hours after feedings.
Monitoring of weight, height, head circumference, and skinfold thickness determines if the diet is adequate; therefore the value of periodic well-baby examinations is stressed. Bottle fed infants are usually fed at 3- to 4-hour intervals. Breastfed infants may require feedings at 2- to 3-hour intervals because breast milk is more easily digested. A flexible but regular schedule that provides a rest period between feedings is best for the parent and infant. The nurse reassures parents that most children eat enough to grow normally, although intake is seldom constant and varies in quantity and quality. Forced feedings are not appropriate.
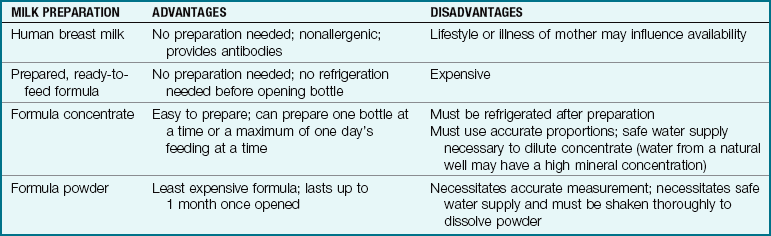
Breastfeeding and Bottle Feeding: Infants, in proportion to their weight, require more calories, protein, minerals, and vitamins than adults. Their fluid requirements are also high. It is suggested that infants remain on human milk or iron-fortified formula for the first year of life (Table 16-1).
Human milk is the best food for infants younger than 6 months. It contains the ideal balance of nutrients in a readily digestible form. Breastfeeding soon after birth helps to promote bonding and stimulates milk production. It has immunological properties that helps to protect the infant from certain microorganisms, and allergic reactions are minimal.
Nutritious commercially prepared infant formulas are available (see Table 16-3). Many pediatricians recommend iron-fortified formulas because maternal iron stores decrease by age 6 months. Whole cow’s milk is not recommended for infants younger than 1 year because the tough, hard curd is difficult to digest. This type of milk may also contribute to iron-deficiency anemia by causing gastrointestinal blood loss.
Parents are sometimes unsure of when their infant has had enough formula. It is important to explain satiety (hunger satisfaction) behavior at the various ages (Table 16-2). Coaxing infants to finish the last drop in a bottle is unnecessary. Infants who are breastfed longer than 6 months gain less weight by age 1 year than bottle-fed infants and are less apt to be obese in later life and are less apt to be obese later in life.
Table 16-2
Development of Mealtime Behavior and Implications for Caregivers
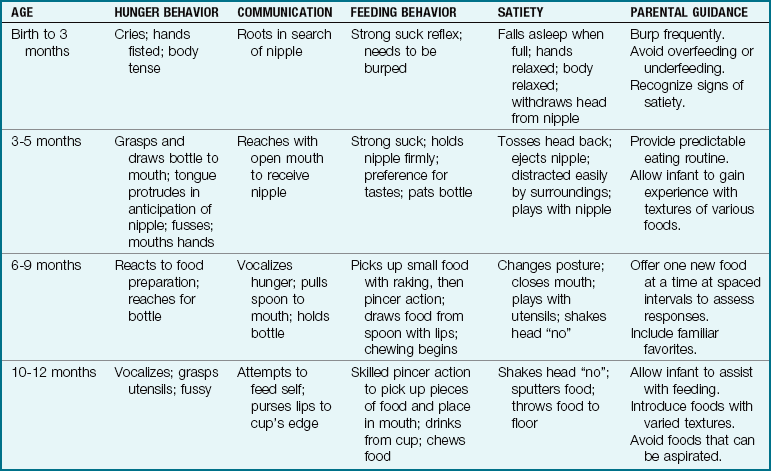
Note: Parents who are alert to infant’s communication of hunger and satiety help the infant develop self-regulation and communication skills.
Types of infant formula: The only recognized contraindications to breastfeeding are galactosemia or certain inborn errors of metabolism in the newborn (such as PKU), or mother with the following: positive human immunodeficiency virus (HIV) status; chemotherapy drug treatment; radioactive isotope therapy; illicit drug use; or active, untreated pulmonary tuberculosis.
When the mother cannot breastfeed, the American Academy of Pediatrics (AAP) recommends iron-fortified cow’s milk–based formula (Kliegman et al., 2007). The two major milk proteins are whey and casein. Human milk has a 60 : 40 ratio of whey to casein, whereas cow’s milk has a 20 : 80 ratio. These ratios differ amongst various commercially prepared formulas. Whey is comprised of amino acids that are very easily digested by stomach contents, but when unchanged whey reaches the small intestine, it may provoke symptoms of protein intolerance. Casein is more slowly digested, provides a slowly absorbed amino acid, and inhibits catabolic processes. Some formulas are 100% whey, such as Good Start Supreme cow’s milk–based formula, whereas other commercially prepared formulas provide varied ratios of whey to casein (Table 16-3).
Table 16-3
Commercially Prepared Infant Formulas
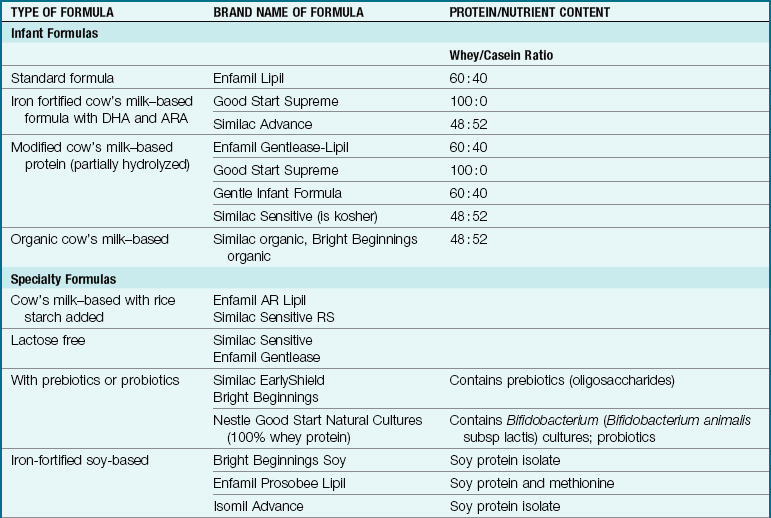
Note: Other formulas are available for specific conditions such as maple syrup urine disease, homocystinuria, phenylketonuria (PKU), etc.
ARA, Arachidonic acid; DHA, docosahexaenoic acid.
Data from Abbot Laboratories http://abbotnutrition.com/products; Bright Beginnings www.brightbeginnings.com/professionals; Mead Johnson www.meadjohnson.com; Nestle www.nestle-infantnutrition.com; Ovewehand, A. (2007). Antibacterial effects of probiotics. Journal of Nutrition 137(1), 7945-75; Gottesmen, M. (2008). Choosing the right infant formula. Adv for Nurse Practitioners 16(5): 47-51; and Kleinman, R, Ed. (2004). Pediatric nutrition handbook (5th ed.). American Academy of Pediatrics: Elk Grove Village, IL.
Docosahexaenoic acid (DHA), an omega-3 fatty acid, and arachidonic acid (ARA), an omega-6 fatty acid, are important for nervous system functioning and are added to most commercial infant formulas as a long chain polyunsaturated fatty acid (LC-PUFA), which will be noted on the label of the formula.
Probiotics have been defined by the World Health Organization (WHO) as live microorganisms (Bifidobacterium and lactobacilli) that, when administered in adequate amounts, offer a health benefit. Prebiotics are nondigestible food ingredients (oligosaccharide) that indirectly stimulate growth or activity of Bifidobacterium when it is present in the colon, ensuring a balance of bacteria is maintained. Probiotics are protective to the gastrointestinal (GI) tract and have been used to treat diarrhea with some success (Saavedra, 2007). Evidence of the value of routine use of probiotics in infant formulas is still being researched, but it is becoming a popular formula option.
Formulas that contain rice starch thicken in the stomach and do not increase caloric value or clog nipples like infant cereal added to the formula bottle does. It is used for reflux or gastroesophageal reflux disease (GERD) problems in infants and often decreases loose stools. Lactose-free formulas replace lactose with corn syrup as the carbohydrate source. Soy milk is used appropriately for infants with galactosemia, but infants allergic to cow’s milk protein often do not do better with soy milk. Soy milk is often used temporarily during a bout of diarrhea, after which the infant returns to breastfeeding or milk-based formula. Extensively hydrolyzed formula and amino acid–based elemental formulas are used for infants with severe protein sensitivity. The nurse must know the difference between various commercial formulas. Feeding an infant the wrong infant formula is considered a medication error and must be reported according to hospital policy.
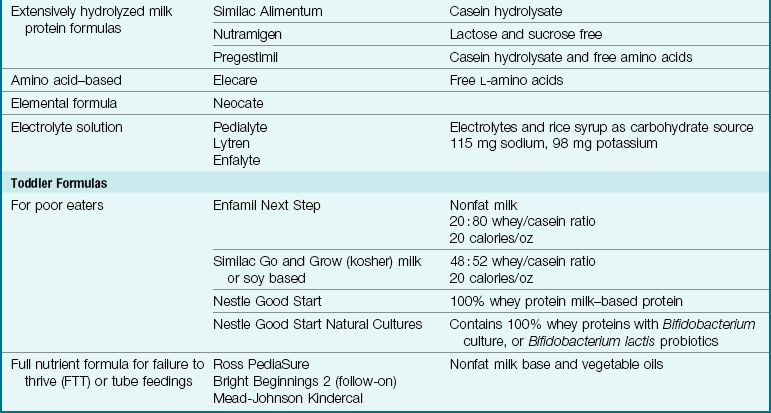
Infants who screen positive for inborn errors of metabolism will require special nutritional formulas. Infants with some genetic problems such as phenylketonuria (PKU) require formula such as Mead-Johnson’s Lofenalac or Ross Labs Phenix and cannot breastfeed exclusively. Current research has shown there is some evidence that type 1 diabetes mellitus may be associated with feeding patterns (Leise et al., 2009). Exposure to whole cow’s milk in early life may trigger its onset. Children of diabetic parents under 3 months of age who are fed gluten-containing foods may be at increased risk of developing type 1 diabetes mellitus, and the risk may decrease if gluten is withheld until 6 months of age (Zeigler et al., 2003).
The practice of feeding breast milk and then immediately supplementing with commercially prepared formula may be counterproductive because substances in the formula may compete for binding or absorption sites in the intestine, thus preventing absorption of some nutrients from the breast milk. Supplemental commercially prepared formula given at a separate time of day (separated by several hours) may not have this interaction with breast milk, but research is ongoing. Formula preparation and breast milk storage are discussed in Chapter 9. Table 16-1 reviews the advantages of the various forms of milk available. Table 16-3 discusses the various commercially prepared infant formulas that are available.
Safe bottle feeding: The nurse should teach parents the basic principles of safe bottle feeding to prevent problems that can result in illness or injury:
• Always check the expiration date on the formula container; do not buy formula that has expired.
• Wash hands thoroughly before preparing formula.
• Wash top of can with detergent and hot water before opening it.
• Use a clean can opener to open can, and wash it between uses. Check the can opener for food or rust spots before using it again.
• Have a clean container (dishpan) reserved for washing all things used for feeding newborn. Squeeze soapy water through nipple holes, then rinse several times.
• Follow the product directions precisely when mixing formula.
• Heat bottle of formula if necessary by running warm water over it. (Most newborns are just as content with their formula unheated. Be consistent in your choice.)
• Test temperature by shaking a few drops on your inner wrist, not just feeling the bottle.
• Do not heat bottle in a microwave oven; the liquid often warms unevenly unless stirred. The container may remain cool when the formula inside is hot enough to burn the newborn.
• Keep prepared bottles of formula refrigerated until ready to use.
• Opened containers of liquid formula should be tightly covered and stored in the refrigerator for no longer than is designated on the label.
• Once a formula can is opened or formula is mixed, use it right away, or refrigerate, because bacteria multiply rapidly at warm temperatures.
• Carry filled bottles away from home in an insulated bag or cooler with ice packs inside.
• Milk should not be saved for the next feeding if the newborn does not empty the bottle. Microorganisms will grow, and the newborn can develop diarrhea (infection).
• Note that hard, clear plastic bottles made of polycarbonate may contain bisphenol-A (BPA), phthalates and PVC and may be toxic. Plastic bottles with the numbers 3, 6, or 7 stamped inside of a triangle on the bottom of the bottle are not safe to reuse (Morin, 2008).
• New bottles made of tritan copolyester has no BPA. Polyethylene or polypropylene are considered safe. All bottles, sippy cups, and pacifiers should be labeled BPA free; those that are not should not be used. Microwaving food or fluids in plastic containers may allow chemicals to leach into the food or fluid and is considered unsafe.
Adding Solid Foods: Parents often wonder when to begin adding solid foods. The addition of solid food at about 6 months is recommended because this is when the tongue extrusion reflex has completely disappeared and the gastrointestinal tract is mature enough to digest the foods. There are a number of commercially prepared brands of baby foods. Parents should be instructed to read the labels on the jars to obtain nutrition information. Home-prepared foods may also be used.
 Health Promotion
Health Promotion
Directions for Home Preparation of Infant Foods
• Select fresh, high-quality fruits, vegetables, and meats.
• Be sure all utensils, including cutting boards, grinder, and knives, are thoroughly clean.
• Wash hands before preparing the food.
• Clean, wash, and trim the food in as little water as possible.
• Cook the foods until tender in as little water as possible. Prevent overcooking, which may destroy heat-sensitive nutrients.
• Do not add salt. Add sugar sparingly. Do not add honey to food for infants less than age 1 year. (Botulism spores have been reported in honey, and young infants do not have the immune capacity to resist this infection.)
• Add enough water so the food can be easily pureed.
• Strain or puree the food with an electric blender, food mill, baby food grinder, or kitchen strainer.
• Pour the pureed food into an ice cube tray and freeze.
• When food is frozen hard, remove the cubes and store in freezer bags.
• Unfreeze and heat (in water bath or microwave oven) in serving container the amount of food that will be consumed at a single feeding.
From Mahan, L.K., & Escott-Stump, S. (2008). Krause’s food, nutrition and diet therapy (12th ed.). Philadelphia: Saunders.
Between 4 and 6 months of age, sucking becomes more mature, and munching (up-and-down chopping motions) commences. Rice cereal is often recommended as the first solid food because it is less allergenic. Figure 16-4 illustrates how feeding skills develop in infants and toddlers.
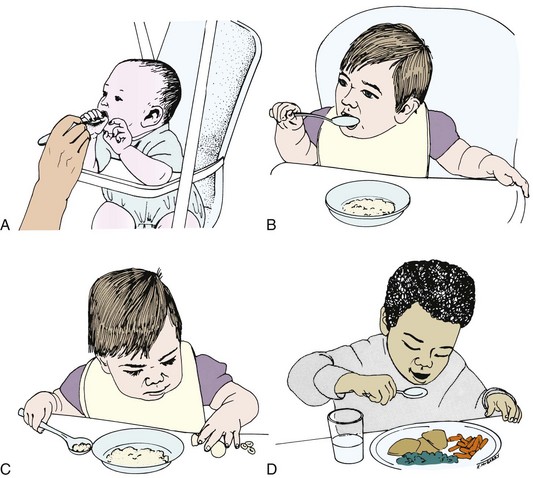
FIGURE 16-4 Development of feeding skills in infants and toddlers. A, At 7 months, this child begins to reach for the spoon. B, At 9 months, this little girl begins to use her spoon independently, although she is not yet able to keep food on it. C, The 9-month-old shows a refined pincer grasp to pick up food. D, The 2-year-old is much more skillful at self-feeding and has the ability both to rotate the wrist and to elevate the elbow to keep food on the spoon.
Only small amounts are offered at first (1 teaspoonful). A small amount of food is placed on the back of the tongue. Cereal may be diluted with formula or water. The consistency is thickened, and amounts of solid foods are gradually increased as the infant becomes more familiar with them. A small bowl and a spoon with a long, straight handle are suggested. Single-ingredient foods are introduced (green beans rather than mixed vegetables), because it is easier to determine food allergies this way. Only one new food is offered in a 4-day to 1-week period to determine tolerance.
If the infant refuses a certain food, it is temporarily omitted. Mealtime is kept pleasant. The infant is allowed to try new foods, even ones that the parents dislike. New foods should not be introduced when the infant is ill because adverse responses may not be effectively assessed. The amount of food consumed varies with the child. Fruit juices are generally offered at about 5 to 6 months of age, when the infant begins to drink from a cup. An exception is the addition of orange juice, which is withheld until the infant is 1 year old, especially when family members have known allergies. Other highly allergenic foods that may be delayed include fish, nuts, strawberries, chocolate, and egg whites.
Nursing Tip
New solid foods should be introduced before the milk feedings to encourage the infant to try the new experience. As solid food intake increases, the amount of formula or milk should decrease to avoid overfeeding.
A children’s plastic “sipper” or “sippy” cup is helpful at first. The juice is initially diluted. The National Research Council (NRC) recommends a daily liquid intake of 140 to 160 mL/kg/day for a 3-month-old, 130 to 155 mL/kg/day for a 6-month-old, 120 to 135 mL/kg/day for a 1-year-old, and 90 to 100 mL/kg/day for a 6-year-old (Kliegman et al., 2007). Baby food can be prepared in a food grinder, electric blender, or food mill or by mashing the food to the desired texture.
Recommended Fat Intake During Infancy: Fat contains more calories than carbohydrates and proteins. Because infants have a limited stomach capacity and a high caloric need, fats in easily digestible forms are needed for meeting their caloric needs for growth and development and for brain development. Infants have a high basal metabolic rate (BMR) and require almost three times more calories per kilogram of weight than adults do to maintain their rapid growth and development in the first year of life. In the young infant, breast milk and infant formulas provide the necessary fats that the infant is able to digest. Feeding a low-fat diet to infants younger than 2 years will compromise their growth and development.
The fat and cholesterol content may not be designated on the label of many baby foods. By age 6 months, amylase and lipase are present in the digestive tract to aid in digesting the fat present in solid foods. A well-balanced diet provides appropriate fat and cholesterol intake. Whole cow’s milk can be introduced after age 1 year, and low-fat milk can be introduced after age 2 years. Evaluating the height and weight of infants on a growth chart during clinic visits is an essential part of the assessment of growth and development.
Buying, Storing, and Serving Foods: Baby foods stored in jars are vacuum-packed. Parents are taught to check safety seals before purchase. Directions are generally indicated on the jar (e.g., to reject product if safety button is up). The expiration date of the product should be checked. Dates are usually found on the caps of jars and on the sides of cereal and bakery items. Unopened jars of baby food and juices are stored in a dry, cool place. Jars are rotated, and those on hand the longest are used first.
When a jar is opened, a definite “pop” is heard as the vacuum seal is broken. Food is transferred to a serving dish. The infant should not be fed out of the jar, and leftovers should not be returned to the jar, because saliva may turn certain foods to liquid by digesting them in the jar. Unused portions may be stored in the refrigerator in the original jar. Special precautions are taken when food is heated in the microwave, because food sometimes heats unevenly.
Weaning: Weaning is defined as substituting a cup for a bottle or breastfeeding. Because sucking is a major source of pleasure in the first year of life, weaning is a major step in growth and development. Signs of readiness to wean can be seen in the infant who eagerly looks forward to new tastes and textures found on the spoon. The infant may not want to be held close during feedings and may start to “bite” the nipple as teeth erupt. The approaching stage of autonomy provides the child with motivation to manipulate the cup. Imitation of older siblings or parents also contributes to readiness. Weaning should be very gradual and start with daytime feedings. Weaning is usually completed by age 2 years but may continue longer in some cultures.
Organic and Natural Foods: Natural foods are defined as those foods that do not contain any additives and that have been altered as little as possible during production. Organic foods are considered to be natural foods whose production is governed by strict regulations. In the case of plants, regulations concern soil, fertilizers, herbicides, and pesticides used for plant growth. In the case of meats, the animal must not have been treated with drugs or hormones before processing (AAP, 2004). Although appearance and taste of organic foods may vary due to production techniques, their nutritive value has not been shown by evidence-based research to be superior to that of nonorganic foods. Parents should be encouraged to read the product labels because organic foods may not contain recommended dietary allowances for some nutrients and may contain more salt, sugar, or fat than nonorganic foods. Seasonal fruits and vegetables provide the best nutritive value at the lowest cost, and meeting the nutritional needs of the infant should be the primary focus of food selection.
Infant Safety
Infant seats should be used for all infants traveling in automobiles. A rear-facing infant seat should be used for infants less than 1 year old and weighing less than 22 lb, and it should be located in the center of the rear seat of the automobile. Cars with passenger-side safety air bags pose a danger to infants in infant seats who are placed in the front seat. The infant seat should be firmly anchored to the vehicle by the car seat belt (see Chapter 17).
Fall Prevention
An infant should never be left unattended on a flat surface, such as a changing table. Newborn infants have crawling reflexes that can cause them to fall off a changing table. Infants younger than 4 months have rounded backs and can accidentally roll off a flat surface. Infants older than 4 months can voluntarily roll over. Crib rails should be raised and securely locked. Infants should be secured in high chairs or swings. An infant seat should not be placed on a table or high surface. Crawling infants should be protected from stairways, and neither heavy nor unsturdy furniture should be available for them to use to pull themselves to a standing position.
A safe environment for a crawling infant includes storage of poisonous items out of the infant’s sight and reach. Cabinet locks are available for purchase. Plants, batteries, pool areas, plugs, loose hanging wires, and pets can be hazardous to an infant. Close supervision at all times is essential to the safety of any environment. Resource consultants are available in most communities for information concerning “childproofing” the home.
Toy Safety
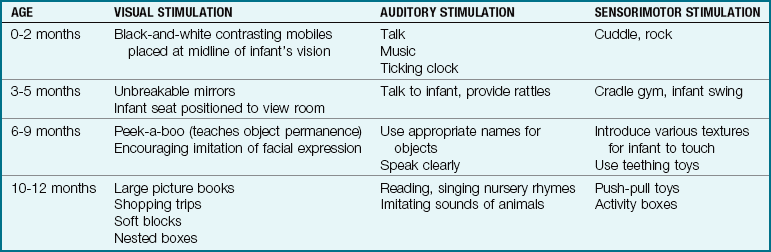
Toys should be appropriate for developmental level and diagnosis of the child, but safety is the most important feature involved in toy selection. Infants put everything into their mouths, and therefore choking is a major problem if a toy has small or removable parts. When the pincer skill is developed, infants will be able to pick up small objects such as pins and put them in their mouths. Toys appropriate for older siblings can be dangerous to infants. For example, the glue from a model airplane set an older sibling is playing with can be deadly if an infant drinks it. Constant supervision is essential. Toys should nurture growth and development (Table 16-4). A child’s response to a toy can indicate readiness to learn new skills. An infant who is able to reach for and pick up a toy shows readiness for communication.
Summary of Major Developmental Changes in the First Year
• Weight doubles by age 6 months and triples by age 1 year.
• Height increases by 1 inch per month for first 6 months to reach 74 cm (29 inches) by age 1 year (increase is mainly in the trunk of the body).
• Head circumference increases 1.5 cm (0.6 inch) each month for the first 6 months and is 46 cm (18 inches) by age 12 months.
• Head circumference and chest circumference are equal by age 1 year.
• Closure of the posterior fontanelle occurs by age 2 months.
• Closure of the anterior fontanelle occurs by age 18 months.
• Primitive reflexes are replaced by voluntary movements.
• Maternal iron stores decrease by age 6 months.
• Digestive processes increase functioning by age 3 months. Amylase and lipase are deficient until age 4 to 6 months, which decreases the ability to digest the fats found in solid foods.
• Tooth eruption begins at age 6 months, when “biting” activities start.
• Binocular vision is established by age 4 months.
• Depth perception begins to develop at age 9 months.
• Infants older than 4 months can voluntarily roll over.
• By age 1 year, infants can take some independent steps.
• Separation (of self from others), object permanence (objects exist even if they are out of visual field), and symbols (saying “bye-bye” means someone is leaving) are major aspects of cognitive development in the first year of life.
Get Ready for the NCLEX® Examination!
Key Points
• A development of a sense of trust begins in infancy and is vital to a healthy personality.
• Sensory stimulation is essential for the development of the infant’s thought processes and perceptual abilities.
• Health maintenance visits are essential during the first year to detect variations from normal growth patterns, to provide immunizations, and to educate and support parents.
• Infants should be positioned for sleep on their backs on a firm mattress, for safety and to prevent sudden infant death syndrome (SIDS). The infant can be placed on his or her abdomen during playtime.
• The nurse must stress to parents the value of immunizations for infants and children.
• Breast milk or formula is the most desirable food for the first 6 months of the infant’s life, and is followed by gradual introduction of a variety of solid foods.
• Human milk and properly prepared formula supply an adequate fluid intake for the infant under normal conditions. The infant may require additional water during illness or in very hot, humid weather.
• Various commercially prepared infant formulas are available for infants with special dietary needs.
• Seasonal fruits and vegetables provide the best nutritive value at the lowest cost.
• Parents should be encouraged to read food labels because some foods may not contain recommended dietary allowances for some nutrients.
• Feeding an infant a low-fat diet before age 2 years will compromise growth and development.
• The most common cause of concern is an atypical-for-age slowing of any aspect of development.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• American Association of Poison Control Centers: www.aapcc.org
• Forum on Child and Family Statistics: www.childstats.gov
• Immunization Action Coalition: www.immunize.org
• Recommendations of the Advisory Committee for Immunization Practices (ACIP): www.cdc.gov/vaccines/pubs/ACIP-list.htm
• Vaccines and Immunizations: www.cdc.gov/vaccines
Review Questions for the NCLEX® Examination
1. The startle reflex is also known as the:
2. A car seat for an infant under age 1 year:
1. is not needed if the infant is held securely in the lap of an adult.
2. should be placed close to the driver in the front passenger seat.
3. should face the rear and be placed in the center of the back seat.
4. should face forward and be placed on the driver’s side of the back seat.
3. To detect allergies when feeding new foods:
4. The nurse is discussing home safety with the mother of a 4-month-old infant. Which of the following is a priority topic?
1. Placing locks on cabinet doors that contain cleaning supplies
2. Covering electrical outlets
5. A mother expresses concern that her 1-year-old infant is overweight. She states that her family has a tendency to be overweight and wishes to discontinue formula feedings and start the infant on low-fat milk. The nurse assesses that the present weight of the infant is 24 lb. The infant’s birth weight was 8 lb, 2 oz. The best response of the nurse would be:
1. to place the infant on low-fat milk because the infant is slightly overweight at this time.
2. to place the infant on regular whole milk because the infant’s weight is appropriate for his age.
3. to indicate that the infant is underweight for his age and needs to have supplemental formula added to the diet.
4. to note that infancy is a period of rapid growth and weight loss will occur as the infant becomes more active.