The Child with a Gastrointestinal Condition
1 Define each key term listed.
2 Discuss three common gastrointestinal anomalies in infants.
3 Discuss the postoperative nursing care of an infant with pyloric stenosis.
4 Discuss the dietary management of celiac disease.
5 Understand the symptoms, treatment, and nursing care of a child with Hirschsprung’s disease.
6 Understand the treatment and nursing care of a child with intussusception.
7 Interpret the nursing management of an infant with gastroesophageal reflux.
8 Differentiate between three types of dehydration.
9 Explain why infants and young children become dehydrated more easily than adults.
10 Understand how nutritional deficiencies influence growth and development.
11 Review the prevention of the spread of thrush in infants and children.
12 Trace the route of the pinworm cycle and describe how reinfection takes place.
13 Prepare a teaching plan for the prevention of poisoning in children.
14 List two measures to reduce the effect of acetaminophen poisoning in children.
 , p. 663)
, p. 663) , p. 667)
, p. 667) , p. 657)
, p. 657) , p. 653)
, p. 653) , p. 665)
, p. 665) , p. 661)
, p. 661) , p. 662)
, p. 662) , p. 662)
, p. 662) , p. 662)
, p. 662) , p. 660)
, p. 660) , p. 669)
, p. 669) , p. 670)
, p. 670) , p. 649)
, p. 649) , p. 648)
, p. 648) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The Gastrointestinal Tract
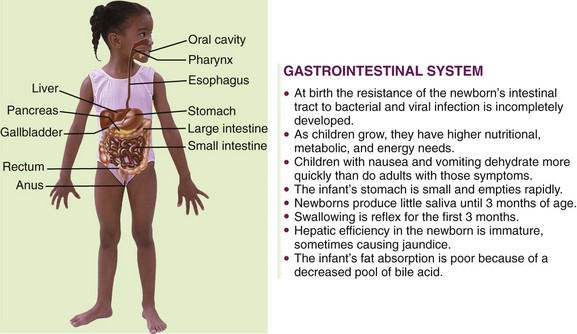
The gastrointestinal (GI) tract transports and metabolizes nutrients necessary for the life of the cell. It extends from the mouth to the anus. Nutrients are broken down into absorbable products by enzymes from various digestive organs. The anatomy of the digestive tract, with some of the differences between that of the child and that of the adult, is depicted in Figure 28-1. The primitive digestive tube is formed by the yolk sac and is divided into the foregut, the midgut, and the hindgut. The foregut evolves into the pharynx, the lower respiratory tract, the esophagus, the stomach, the duodenum, and the beginning of the common bile duct. The midgut elongates in the fifth fetal week to form the primary intestinal loop. The remainder of the large colon is derived from the primitive hindgut. The liver, pancreas, and biliary tree evolve from the foregut. The anal membrane ruptures at 8 weeks of gestation, forming the anal canal and opening.
Disorders and Dysfunction of the Gastrointestinal Tract
A number of procedures are available to determine GI disorders. Laboratory work, such as a complete blood count (CBC) with differential, will reveal anemia, infections, and chronic illness. An elevated erythrocyte sedimentation rate (ESR) is indicative of inflammation. A comprehensive chemical panel will reveal electrolyte and chemical imbalances. X-ray studies often used include GI series, barium enema, and flat plates of the abdomen. Endoscopy allows direct visualization of the GI tract through a flexible lighted tube. Upper endoscopy permits visualization and biopsy of the esophagus, the stomach, and the duodenum. It is also valuable to remove foreign objects and cauterize bleeding vessels. Visualization of the bile and pancreatic ducts is also possible through endoscopy. The lower colon is inspected by sigmoidoscopy. Colonoscopy provides visualization of the entire colon to the ileocecal valve. Stool cultures and rectal biopsy are also important diagnostic tools. Ultrasonography is a noninvasive procedure useful in visualizing intestinal organs and masses, particularly of the liver and pancreas. Some liver function blood tests include alanine aminotransferase (ALT), aspartate aminotransferase (AST), prothrombin time (PT), and partial thromboplastin time (PTT). Liver biopsy may also be indicated. Overall malabsorption tests, such as the 72-hour fecal fat test and the Schilling test (which can determine the absorption capacity of the lower ileum) are also useful. For more detailed information concerning preparation for various tests, refer to a laboratory diagnostics textbook.
Symptoms of GI disorders may be manifested by systemic signs such as failure to thrive (FTT; failure to develop according to established growth parameters such as height, weight, and head circumference) or jaundice. Pruritus (itching) in the absence of allergy may indicate liver dysfunction. Local manifestations of a GI disorder include pain, vomiting, diarrhea, constipation, rectal bleeding, and hematemesis.
Nursing intervention focuses on providing adequate nutrition and freedom from infection, which can result from malnutrition or depressed immune function. Developmental delays in children should be investigated to determine whether they are related to the GI system. Skin problems in these patients may be related to pruritus from liver disease, irritation from frequent bowel movements, or other disorders. Pain and discomfort may occur during acute episodes; however, they may also result from medication side effects, or they may be referred pain. Cleft lip and cleft palate are discussed in Chapter 14. Anorexia is discussed in Chapter 33, and necrotizing enterocolitis is discussed in Chapter 13. Oral care in health and illness is discussed in Chapter 15.
Congenital Disorders
Esophageal Atresia (Tracheoesophageal Fistula)
Pathophysiology: Atresia of the esophagus (tracheoesophageal fistula [TEF]) is caused by a failure of the tissues of the GI tract to separate properly from the respiratory tract early in prenatal life. There are four types of TEF:
1. The upper esophagus and the lower esophagus (leading from the stomach) end in a blind pouch.
2. The upper esophagus ends in a blind pouch; the lower esophagus (leading from the stomach) connects to the trachea.
3. The upper esophagus is attached to the trachea; the lower esophagus (leading from the stomach) is also attached to the trachea.
4. The upper esophagus connects to the trachea; the lower esophagus (leading from the stomach) ends in a blind pouch.
The diagnosis of this condition is based on clinical manifestations and confirmed by x-ray study (Figure 28-2).
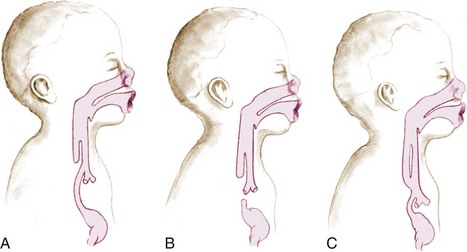
FIGURE 28-2 Esophageal atresia (failure of the esophagus to contact with the stomach), or tracheoesophageal fistula (TEF). The three most common types of TEF are (A) the upper esophagus ending in a blind pouch and the lower esophagus ending in the trachea; (B) the upper esophagus and the lower esophagus ending in a blind pouch (fetal swallowing is prevented, and the mother will develop polyhydramnios during pregnancy); and (C) both the upper and the lower esophagus end in the trachea. In TEF, the newborn will have excessive mucous secretions (drooling) and may choke or vomit if fed.
Manifestations: The earliest sign of TEF occurs prenatally when the mother develops polyhydramnios. When the upper esophagus ends in a blind pouch, the fetus cannot swallow the amniotic fluid, resulting in an accumulation of fluid in the amniotic sac (polyhydramnios). At birth the infant will vomit and choke when the first feeding is introduced. Because the upper end of the esophagus ends in a blind pouch, the newborn cannot swallow accumulated secretions and will appear to be drooling. Although drooling after age 3 months is related to teething, drooling in a newborn is pathological and is related to atresia. If the upper esophagus enters the trachea, the first feeding will enter the trachea and result in coughing, choking, cyanosis, and apnea. If the lower end of the esophagus (from the stomach) enters the trachea, air will enter the stomach each time the infant breathes, causing abdominal distention.
Treatment and Nursing Care: The nursing goals involve preventing pneumonia, choking, and apnea in the newborn. Assessment of every newborn during the first feeding is essential. The first feeding usually consists of clear water or colostrum (if breastfed) to minimize the seriousness of aspiration should it occur. If symptoms are noted, the infant is placed on NPO status (nothing by mouth), suctioned to clear the airway, and positioned to drain mucus from the nose and throat. Surgical repair is essential for survival.
Imperforate Anus
Pathophysiology: Imperforate anus occurs in about 1 of every 5000 live births. The lower GI tract and the anus arise from two different tissues. Early in fetal life the two tissues meet and join; the tissue separating them then perforates, allowing for a passageway between the lower GI tract and the anus. When this perforation does not take place, the lower end of the GI tract and the anus end in blind pouches. This is called imperforate anus. There are four types of imperforate anus, ranging from a stenosis to complete separation or failure of the anus to form.
Manifestations: A routine part of the newborn assessment is determining the patency of the anus. Often the first temperature of the newborn is taken rectally to ascertain patency. (All subsequent and routine temperature readings are usually taken via the axillary route.) Failure to pass meconium in the first 24 hours must be reported. Infants should not be discharged to the home before a meconium stool is passed.
Treatment and Nursing Care: Once a diagnosis of imperforate anus is established, the infant is given nothing by mouth and is prepared for surgery. Diagnosis is confirmed by x-ray study or magnetic resonance imaging (MRI). The initial surgical procedure may be a colostomy. Subsequent surgery can reestablish the patency of the anal canal.
Pyloric Stenosis
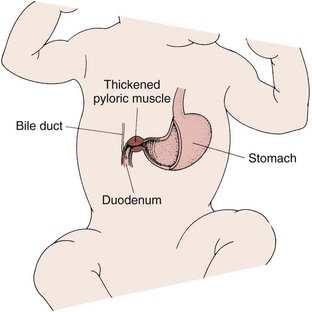
Pathophysiology: Pyloric stenosis (narrowing) is an obstruction at the lower end of the stomach (pylorus) caused by an overgrowth (hypertrophy) of the circular muscles of the pylorus or by spasms of the sphincter. This condition is commonly classified as a congenital anomaly; however, its symptoms do not appear until the infant is 2 or 3 weeks old. Pyloric stenosis is the most common surgical condition of the digestive tract in infancy (Figure 28-3). Its incidence is higher in boys than in girls, and it has a tendency to be inherited.
Manifestations: Vomiting is the outstanding symptom of this disorder. The force progresses until most of the food is ejected a considerable distance from the mouth. This is termed projectile vomiting, and it occurs immediately after feeding. The vomitus contains mucus and ingested milk. The infant is constantly hungry and will eat again immediately after vomiting. Dehydration as evidenced by sunken fontanelle, inelastic skin, and decreased urination, as well as malnutrition, can develop. An olive-shaped mass may be felt in the right upper quadrant of the abdomen. Ultrasonography or scintiscans are commonly used today for diagnostic purposes, because they are noninvasive and accurate. In severe cases the outline of the distended stomach and peristaltic waves are visible during feeding.
Treatment: The surgery performed for pyloric stenosis is called a pyloromyotomy (pylorus, myo, “muscle,” and tomy, “incision of”). The surgeon incises the pyloric muscle to enlarge the opening so food may easily pass through it again. This is done as soon as possible if the infant is not dehydrated.
Nursing Care: The dehydrated infant is given intravenous (IV) fluids preoperatively to restore fluid and electrolyte balance. If this is not done, shock may occur during surgery. Thickened feedings may be given until the time of operation in hopes that some nutrients will be retained. The physician prescribes the degree of thickness of the formula, which is given by teaspoon or through a nipple with a large hole. The infant is burped before as well as during feedings to remove any gas accumulated in the stomach. The feeding is done slowly, and the infant is handled gently and as little as possible. The infant is placed on the right side after feedings to facilitate drainage into the intestine. Fowler’s position is preferred to aid gravity in passing milk through the stomach (see Fowler’s sling, p. 656). If vomiting occurs, the nurse may be instructed to refeed the infant. Charting of the feeding includes time, type, and amount offered; amount taken and retained; and type and amount of vomiting. The nurse also notes whether the infant appeared hungry after the feeding or if vomiting occurred again.
The nurse obtains and records a baseline weight and weighs the infant at about the same time each morning. Other factors to be charted include the type and number of stools and the color of urine and frequency of voiding (intake and output). Position is changed frequently, because the infant is weak and vulnerable to pneumonia. All procedures designed to protect from infection must be strictly carried out.
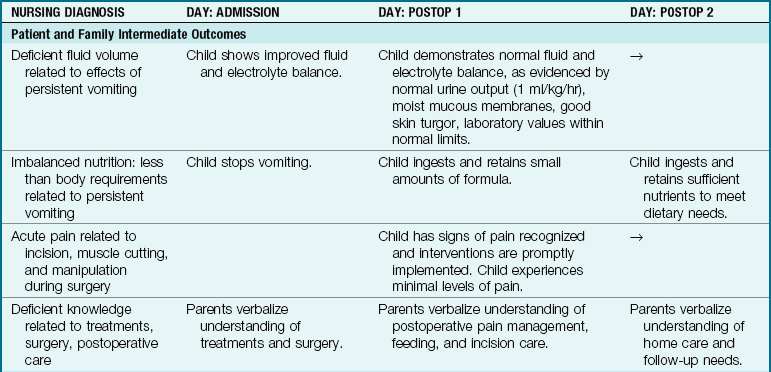
The care of the infant after surgery includes a careful observation of vital signs and the administration of IV fluids. The wound site is inspected frequently (see Chapter 22 for postoperative care). The surgery involves cutting into the hypertrophied muscle but not through the mucous membrane of the bowel; therefore the infant will not need nasogastric decompression postoperatively and will be able to resume oral feedings shortly after recovering from anesthesia. The physician prescribes oral feedings of small amounts of glucose water that gradually increase until a regular formula can be taken and retained. Overfeeding is avoided, and the nurse reviews feeding techniques with parents. The diaper is placed low over the abdomen to prevent contamination of the wound site (Clinical Pathway 28-1).
Clinical Pathway 28-1
An Interdisciplinary Plan of Care for the Infant with Pyloric Stenosis
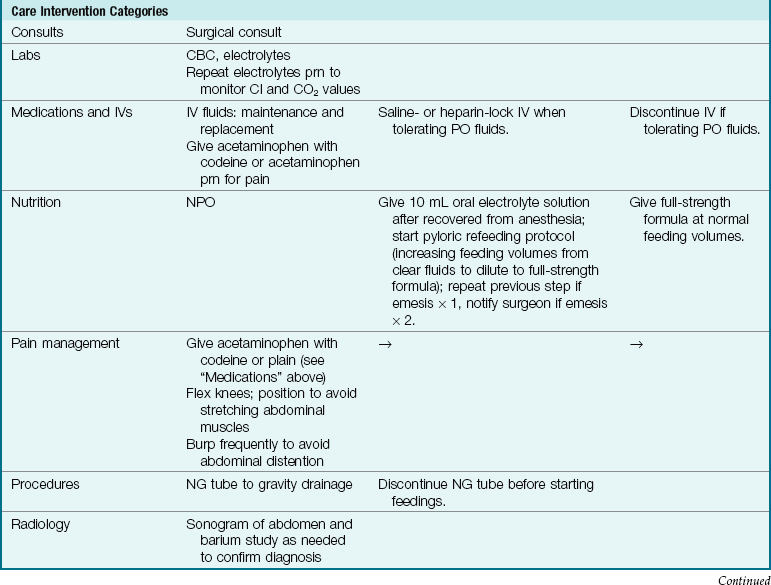
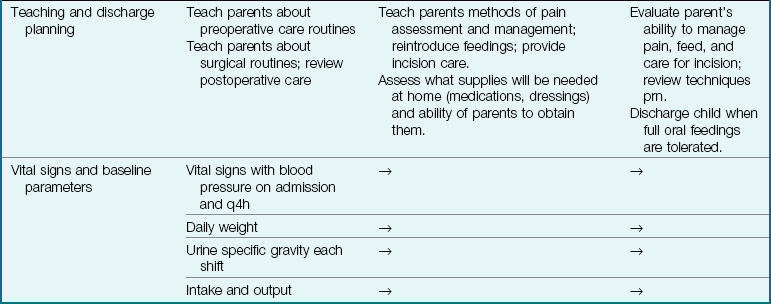
CBC, Complete blood count; Cl, chloride; CO2, carbon dioxide; IV, intravenous route; NG, nasogastric; NPO, nothing by mouth; PO, by mouth; prn, as needed.
Modified from Bowden, V., Dickey, S., & Greenberg, C. (1998). Children and their families: The continuum of care. Philadelphia: Saunders.
Celiac Disease
Pathophysiology: Celiac disease is also known as gluten enteropathy and sprue and is the leading malabsorption problem in children. The cause is thought to be an inherited disposition with environmental triggers (Figure 28-4).
Manifestations: Symptoms are not evident until 6 months to 2 years of age, when foods containing gluten are introduced to the infant. Gluten is found in wheat, barley, oats, and rye. Repeated exposure to gluten damages the villi in the mucous membranes of the intestine, resulting in malabsorption of food. The infant presents with failure to thrive. Stools are large, bulky, and frothy because of undigested contents. The infant is irritable. Diagnosis is confirmed by serum immunoglobin A (IgA) test and small bowel biopsy. The characteristic profile of a child with a malabsorption syndrome is abdominal distention with atrophy of the buttocks.
Treatment and Nursing Care: The treatment involves a lifelong diet restricted in wheat, barley, oats, and rye. It is a nursing challenge to teach the family the importance of dietary compliance. A professional nutritionist or dietitian can aid in identifying foods that are gluten free. Long-term bowel pathology can occur if dietary compliance is not lifelong.
Hirschsprung’s Disease (Aganglionic Megacolon)
Pathophysiology: Hirschsprung’s disease, or aganglionic megacolon, occurs when there is an absence of ganglionic innervation to the muscle of a segment of the bowel. This usually happens in the lower portion of the sigmoid colon. Because of the absence of nerve cells, there is a lack of normal peristalsis. This results in chronic constipation. Ribbonlike stools are seen as a result of feces passing through the narrow segment. The portion of the bowel nearest to the obstruction dilates, causing abdominal distention (Figure 28-5). It is seen more often in boys than girls and has familial tendencies. The incidence is approximately 1 in 5000 live births. There is a higher incidence in children with Down syndrome. The condition may be acute or chronic.
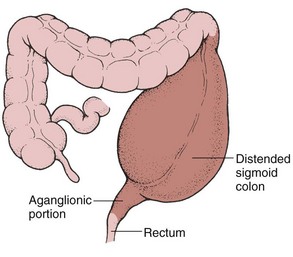
Manifestations: In the newborn, failure to pass meconium stools within 24 to 48 hours may be a symptom of Hirschsprung’s disease. In the infant, constipation, ribbonlike stools, abdominal distention, anorexia, vomiting, and failure to thrive may be evident. Often the parent brings the young child to the clinic after trying several over-the-counter laxatives to treat the constipation without success. If the child is untreated, other signs of intestinal obstruction and shock may be seen. The development of enterocolitis (inflammation of the small bowel and colon) is a serious complication. It may be signaled by fever, explosive stools, and depletion of strength. Diagnostic evaluation usually includes a barium enema and rectal biopsy, which shows a lack of innervation. Anorectal manometry tests the strength of the internal rectal sphincter. In this procedure a balloon catheter is placed into the rectum, and the pressure exerted against it is measured.
Treatment and Nursing Care: Megacolon is treated by surgery. The impaired part of the colon is removed, and an anastomosis of the intestine is performed. In newborns a temporary colostomy may be necessary, and more extensive repair may follow at about 12 to 18 months of age. Closure of the colostomy follows in a few months.
Nursing care is age dependent. In the newborn, detection is a high priority. As the child grows older, careful attention to a history of constipation and diarrhea is important. Signs of undernutrition, abdominal distention, and poor feedings are suspect.
Because the distended bowel in a child with megacolon provides a larger mucous membrane surface area that will come in contact with fluid inserted during an enema, an increased absorption of the fluid can be anticipated. For this reason, when a child is given an enema at home, normal saline solution, not tap water, is used. Tap water enemas in infants and small children can lead to water intoxication and death. Parents can obtain normal saline solution from the pharmacy without prescription, or they can make it at home by using one half of a teaspoon of noniodized salt in 1 cup of lukewarm tap water. The amount of fluid administered should be determined by the health care provider. The nurse stresses to parents the importance of using saline solution. Postoperative care of children is discussed in Chapter 22.
Intussusception
Pathophysiology: Intussusception (intus, “within,” and suscipere, “to receive”) is a slipping of one part of the intestine into another part just below it (Figure 28-6). It is often seen at the ileocecal valve, where the small intestine opens into the ascending colon. The mesentery, a double fan–shaped fold of peritoneum that covers most of the intestine and is filled with blood vessels and nerves, is also pulled along. Edema occurs. At first this telescoping of the bowel causes intestinal obstruction, but strangulation takes place as peristalsis forces the structures more tightly. This portion may burst, causing peritonitis.
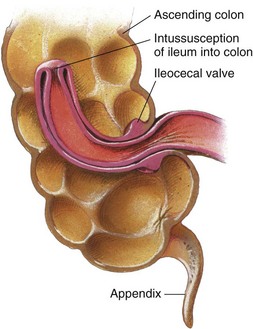
FIGURE 28-6 Intussusception. The most common type begins at or near the ileocecal valve, with this part of the intestines (bowel) pushing into the cecum and on to the colon. At first the obstruction is partial, but complete obstruction occurs as the bowel becomes inflamed and edematous.
Intussusception generally occurs in boys between 3 months and 6 years of age who are otherwise healthy. Its frequency decreases after age 36 months. Occasionally the condition corrects itself without treatment. This is termed a spontaneous reduction. However, because the patient’s life is in danger, the physician does not waste time waiting for this to occur. The prognosis is good when the patient is treated within 24 hours.
Manifestations: In typical cases the onset is sudden. The infant feels severe pain in the abdomen, as evidenced by loud cries, straining efforts, and kicking and drawing of the legs toward the abdomen. At first there is comfort between pains, but the intervals shorten and the condition becomes worse. The child vomits. The stomach contents are green or greenish yellow (this results from bile stain), and the contents are described as bilious. Bowel movements diminish, and little flatus is passed. Movements of blood and mucus that contain no feces are common about 12 hours after the onset of the obstruction; these are termed currant jelly stools. The child’s fever may run as high as 41.1° C (106° F), and signs of shock, such as sweating, weak pulse, and shallow, grunting respirations are evident. The abdomen is rigid.
Treatment and Nursing Care: Intussusception is an emergency, and because of the severity of symptoms, most parents contact a physician promptly. The diagnosis is determined by the history and physical findings. The physician may feel a sausage-shaped mass in the right upper portion of the abdomen during bimanual rectal and abdominal palpation. Abdominal films also may indicate the mass. A barium enema is the treatment of choice, with surgery scheduled if reduction is not achieved. The recurrence rate after barium enema reduction is approximately 10%.
During the operation a small incision is made into the abdomen, and the wayward intestine is “milked” back into position. The intestine is inspected for gangrene; if all is well, the abdomen is sutured. Barring complications, recovery is straightforward. If the intestine cannot be reduced or if gangrene has set in, a bowel resection is done and the affected area is removed. The cut end of the ileum is joined to the cut end of the colon; this is called an anastomosis. Routine preoperative and postoperative care is discussed in Chapter 22.
Meckel’s Diverticulum
Pathophysiology: During fetal life the intestine is attached to the yolk sac by the vitelline duct. A small blind pouch may form if this duct fails to disappear completely. This condition is termed Meckel’s diverticulum. It usually occurs near the ileocecal valve, and it may be connected to the umbilicus by a cord. A fistula may also form. This sac is subject to inflammation, much like the appendix. This disorder is the most common congenital malformation of the GI tract. It is seen more often in boys.
Manifestations: Symptoms may occur at any age but appear most often before 2 years of age. Painless bleeding from the rectum is the most common sign. Bright red or dark red blood is more usual than tarry stools. Abdominal pain may or may not be present. In some persons it may exist without causing symptoms. Barium enema and radionuclide scintigraphy are useful in diagnosing Meckel’s diverticulum. X-ray films are not helpful because the pouch is so small that it may not appear on the screen.
Hernias
Pathophysiology: An inguinal hernia is a protrusion of part of the abdominal contents through the inguinal canal in the groin. It is more common in boys than in girls. It is also commonly seen in preterm infants. An umbilical hernia is a protrusion of a portion of intestine through the umbilical ring (an opening in the muscular area of the abdomen through which the umbilical vessels pass, Figure 28-7). This type of hernia appears as a soft swelling covered by skin, which protrudes when the infant cries or strains. Hernias may be present at birth (congenital) or may be acquired, and they can vary in size. A hernia is called reducible if it can be put back into place by gentle pressure; if this cannot be done, it is called an irreducible or an incarcerated hernia. Incarceration (constriction) occurs more often in infants under 10 months of age. Hernias may be bilateral.

Manifestations: The infant with a hernia may be relatively free of symptoms. Irritability, fretfulness, and constipation are sometimes evident. The diagnosis is made when physical examination shows a mass in the area that reappears from time to time, particularly when the child cries or strains. A strangulated hernia occurs when the intestine becomes caught in the passage and the blood supply is diminished. This happens more often during the first 6 months of life. Vomiting and severe abdominal pain are present. Emergency surgery is necessary if strangulation occurs, and in some cases a bowel resection is performed.
Treatment and Nursing Care: Hernias are successfully repaired by the surgical operation called a herniorrhaphy. This is a relatively simple procedure and is well tolerated by the child. Most children are scheduled for procedures in same-day surgery units. The benefits of this method are both economic and psychological. Parents are instructed to bring the fasting child to the hospital about 1 hour before surgery. Parents remain with the child during the entire time except during the actual procedure. They are encouraged to assist in routine postoperative care.
Often no dressing is applied to the wound. Sometimes a waterproof collodion dressing, which looks like clear nail polish, is applied. Postoperative care is directed toward keeping the wound clean. Diapers are left open for this purpose. Wet diapers are changed frequently.
Disorders of Motility
Pathophysiology: Gastroenteritis involves an inflammation of the stomach and the intestines; colitis involves an inflammation of the colon; enterocolitis involves an inflammation of the colon and the small intestine. The most common noninfectious causes of diarrhea involve food intolerance, overfeeding, improper formula preparation, or ingestion of high amounts of sorbitol (a substance found in sweetened “sugar-free” products). The priority problem in diarrhea is fluid and electrolyte imbalance and failure to thrive.
Treatment and Nursing Care: Treatment is focused on identifying and eradicating the cause. Nursing responsibilities include teaching parents and caregivers proper and age-appropriate diet and feeding techniques. The priority goal of care includes preventing fluid and electrolyte imbalance.
Oral rehydrating solutions (ORS) such as Pedialyte, Lytren, Ricelyte, and Resol are used for infants in small, frequent feedings. Although formula feeding is withheld, breastfeeding can accompany oral rehydration therapy (ORT) because of breast milk’s osmolarity, antimicrobial properties, and enzyme content.
The nursing care of gastroenteritis includes maintaining intake and output records and providing skin care and frequent diaper changes to prevent excoriation from the frequent stools. Parents should be taught good handwashing techniques, proper food handling, and principles of cleanliness and infection prevention. The infant should be weighed daily, observed for dehydration or overhydration, and kept warm. Transmission-based contact precautions should be used to prevent the spread of infection (see Appendix A). Sometimes parents need help in interpreting food labels to avoid foods to which their child may be allergic. Table 28-1 lists some terms that often need clarification for the parents of a child who is food intolerant.
Table 28-1
| INGREDIENT LISTED | MAY CONTAIN THIS: |
| Binder | Egg |
| Bulking agent | Soy |
| Casein | Cow’s milk (often in canned tuna) |
| Coagulant | Egg |
| Emulsifier | Egg |
| Protein extender | Soy |
Vomiting
Pathophysiology: Vomiting, a common symptom during infancy and childhood, results from sudden contractions of the diaphragm and the muscles of the stomach. It must be evaluated in relation to the child’s overall health status. Persistent vomiting requires investigation because it results in dehydration and electrolyte imbalance. The continuous loss of hydrochloric acid and sodium chloride from the stomach can cause alkalosis. In this condition the acid-base balance of the body becomes disturbed because of a loss of chlorides and potassium. This can result in death if left untreated.
Manifestations: The child may vomit from various causes. Some stem from improper feeding techniques that should be assessed by the nurse. Sometimes the difficulty lies with formula intolerance. The introduction of foods of a different consistency may also precipitate this symptom.
Other causes of vomiting are systemic illness such as increased intracranial pressure or infection. Aspiration pneumonia is a serious complication of vomiting. In aspiration, vomitus is drawn into the air passages on inspiration, causing immediate death in extreme cases. Health professionals and laypersons should become familiar with lifesaving procedures such as cardiopulmonary resuscitation (CPR) for use in such emergencies.
Treatment and Nursing Care: To prevent vomiting the nurse must carefully feed and burp the infant. Treatments are avoided immediately after feedings. The infant is handled as little as possible after feedings. To prevent aspiration of vomitus the nurse places the infant on the right side following feedings. When an older child begins to vomit, the head is turned to one side, and an emesis basin and tissues are provided.
Factors to be charted include time, amount, color (e.g., bloody, bile-stained), consistency, force, frequency, and whether or not vomiting was preceded by nausea or by feedings. IV fluids may be given. Oral fluids are withheld for a short time to allow the stomach to rest. Gradually, sips of water are given according to the infant’s tolerance and condition. The infant’s intake and output are carefully recorded so the physician is able to compare the urine output with the total fluid intake.
Drugs such as trimethobenzamide (Tigan) or promethazine (Phenergan) may be prescribed when vomiting is persistent. They are available in rectal suppository form. The nurse lubricates the suppository and inserts it into the rectum, where it dissolves. Slight pressure is exerted over the anus for a short time to ensure that the suppository is not expelled. Charting includes the time administered and whether or not vomiting subsided.
Gastroesophageal Reflux
Pathophysiology: Gastroesophageal reflux (GER, or chalasia) results when the lower esophageal sphincter is relaxed or not competent, which allows stomach contents to be easily regurgitated into the esophagus.
The term chalasia is derived from the Greek word chalasis, which means “relaxation.” Although many infants have this condition to a small degree, about 1 in 300 to 1 in 1000 have significant reflux and associated complications. The condition is associated with neuromuscular delay and is often seen in preterm infants and children with neuromuscular disorders, such as cerebral palsy and Down syndrome. In many infants the symptoms decrease around age 12 months, when the child stands upright and eats more solid foods.
Manifestations: Symptoms include vomiting, weight loss, and failure to thrive. The vomiting occurs within the first and second weeks of life. The infant is fussy and hungry. Respiratory problems can occur when vomiting stimulates the closure of the epiglottis and the infant presents with apnea. Aspiration of vomitus can also occur.
Treatment and Nursing Care: A careful history is taken. Of particular interest is when the vomiting started, type of formula, type of vomiting, feeding techniques, and the infant’s eating in general. Tests used to determine the presence of GER include scintigraphy, which involves the infant drinking a radioactively labeled formula and following the path of the fluid with imaging studies to determine the presence of reflux or poor swallowing coordination. Prolonged esophageal pH monitoring is one of the most definitive diagnostic tests and helps to determine the acuity of the disease and the course of treatment to prevent esophagitis.
Therapy depends on the severity of symptoms. Most parents need only reassurance and education about feeding the infant. Teaching should include careful burping, avoiding overfeeding (which distends the stomach), and proper positioning. A general guide to determine optimum intake to prevent gastric distention is to feed the infant no more than the age in months plus 3, every 3 to 4 hours. For example, a 3-month-old infant should be fed a maximum of 6 oz in one feeding (Weill, 2008).
Medication and surgical intervention may be required in infants with more complicated gastroesophageal reflux disorder (GERD). Parents are instructed to burp the infant frequently. Feedings can be thickened with cereal (1 teaspoon to 1 tablespoon of cereal per ounce of formula). Adding cereal to the formula increases the caloric density from 20 calories per ounce to 27 calories per ounce. The formula Enfamil AR is a milk-based formula with added rice starch for thickness, that provides 20 calories per ounce (see Table 16-3).
After being fed, the infant should be placed in an upright position or propped on the right side. The body is inclined about 30 to 40 degrees, and the infant is held in place by a Fowler’s sling (Figure 28-8). Sitting upright in an infant seat or swing is not recommended because it increases intraabdominal pressure. The upright prone position has been recommended for the infant with GER when awake and monitored. (The supine [back] sleep position is recommended for all healthy infants.) Medications that relax the pyloric sphincter and promote stomach emptying may be used, such as metoclopramide (Reglan). The medication must be administered before meals. Side effects such as drowsiness or restlessness can occur. Ranitidine (Zantac) may be prescribed to reduce stomach acid and prevent the development of esophagitis. Proton pump inhibitors such as omeprazole (Prilosec) and lansoprazole (Prevacid) are awaiting U.S. Food and Drug Administration (FDA) approval for use in infants.
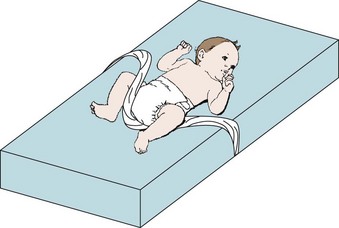
FIGURE 28-8 Fowler’s sling. Fowler’s sling is used to maintain Fowler’s position and to prevent the infant from sliding down to the foot of the bed. The bed is in Fowler’s position; the rolled blanket is tucked under the mattress on each side at armpit level; when the infant is in the side-lying position or prone, the legs straddle the sling to maintain positioning.
Diarrhea
Pathophysiology: Diarrhea in the infant cannot be defined in the same way as diarrhea in the adult. The number of stools per day is not often significant in the infant. Diarrhea in infancy is a sudden increase in stools from the infant’s normal pattern, with a fluid consistency and a color that is green or contains mucus or blood. Acute sudden diarrhea is most often caused by an inflammation, an infection, or a response to a medication, food, or poisoning. Chronic diarrhea lasts for more than 2 weeks and may be indicative of a malabsorption problem, long-term inflammatory disease, or allergic responses. Infectious diarrhea is caused by viral, bacterial, or parasitic infection and usually involves gastroenteritis.
Manifestations: The symptoms of diarrhea may be mild or extremely severe. The stools are watery and are expelled with force (explosive stools). They may be yellowish green. The infant becomes listless, refuses to eat, and loses weight. The temperature may be elevated, and the infant may vomit. Dehydration is evidenced by sunken eyes and fontanelle and by dry skin, tongue, and mucous membranes. Urination may become less frequent. In severe cases the excessive loss of bicarbonate from the GI tract results in acidosis.
Infectious diarrhea in infants is commonly caused by the rotavirus that often occurs in day care centers; by Escherichia coli, which is caused by lack of hygiene or poorly cooked foods; by Salmonella from contaminated food or pet (especially turtles) contact; by Shigella; and by other organisms. Clostridium difficile infection often follows prolonged antibiotic therapy. Giardia lamblia is an intestinal protozoan that causes diarrhea. It is spread by contaminated water, unsanitary conditions, and fecal contamination by animals. Prevention is important and centers around teaching the basics of hygienic practices, handwashing, and the use of disinfectants.
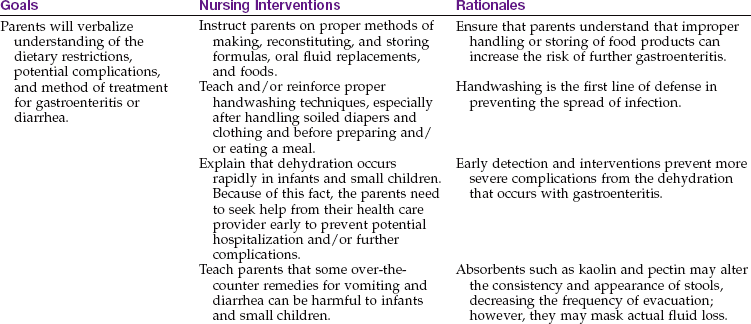
Treatment and Nursing Care: Mild diarrhea in older children may be treated at home under a physician’s direction, provided there is a suitable caregiver. Treatment is essentially the same. The intestine is rested by reducing the intake of solid foods. ORS solutions such as Pedialyte or Infalyte in liquid or frozen (ice pop) form are preferred, with the gradual introduction of a soft, bland diet. A regular intake is usually resumed within 2 to 3 days. Clear fluids, fruit juice without pulp, gelatin, and carbonated drinks have a low electrolyte content and are avoided. Caffeinated sodas act as a diuretic and can worsen the dehydration. Chicken broth is often high in sodium and not advisable. The BRAT diet (bananas, rice, applesauce, and toast) is not nutritionally sound enough to support growth and development. Nursing Care Plan 28-1 provides nursing interventions for the care of a child with diarrhea.
28-1  Nursing Care Plan
Nursing Care Plan
The Child with Gastroenteritis (Diarrhea and Vomiting)
An 11-month-old infant is admitted with a history of diarrhea for several days and vomiting related to food ingestion. A diaper rash is evident, and skin tissue turgor is poor.
Deficient fluid volume related to diarrhea and/or vomiting as evidenced by weight loss, output greater than intake, emesis, liquid stools, decreased urine output, abdominal distention/rebound tenderness, excoriation of perianal mucosa, hypotension, increased pulse rate, change in skin turgor, lethargy, irritability
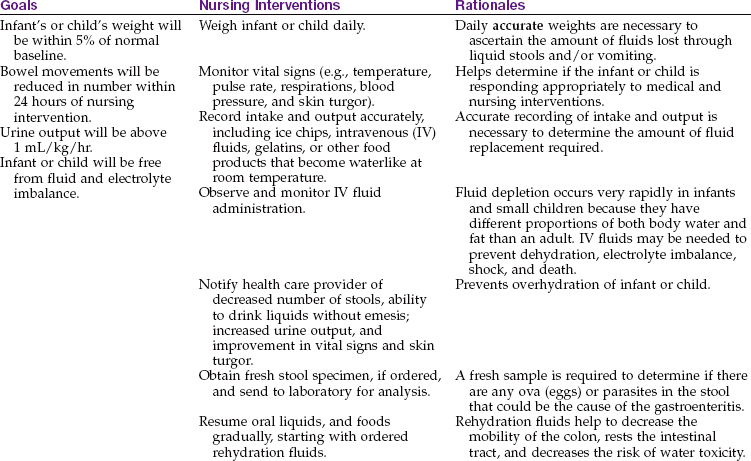
Risk for impaired skin integrity related to frequency of stools as evidenced by excoriation of skin and tissue in perianal area, erythema, pain with each stooling; complaint of burning or pain in perianal area
| Goals | Nursing Interventions | Rationales |
| Infant or child will show improvement or resolution of erythema and exhibit tissue intact and free from secondary infection. | Change diapers or underwear as soon as a stooling occurs; cleanse perianal area with warm water using a soft cloth free of any alcohol. | Liquid stools generally contain high amounts of acids. The longer the stool is in contact with the infant’s or child’s skin, the greater the risk of excoriated tissue. Alcohol can be very painful on impaired tissue. |
| Leave buttocks exposed to air whenever possible (usually after the diarrhea slows down or stops). | Air helps to keep the skin dry and free from any irritation such as from diapers or underwear rubbing on the skin. | |
| Apply soothing balm or ointment to affected area (after thorough cleansing) sparingly. | The balm or ointment is a protective barrier on the infant’s or child’s skin. If the ointment is placed on uncleansed skin, the infant or child is at increased risk of excoriation. | |
| If medicated powders are prescribed and/or used, teach the parent to put powder in the hand and then apply on the infant’s or child’s buttocks and to keep powder container away from the infant or child. | If powder is “sprayed” onto the buttocks, the infant or child is at risk to inhale the powder. |
Deficient parental knowledge related to diarrhea in infants and children as evidenced by lack of previous experience
1. An 11-month-old infant is brought to the clinic. The mother states he has watery diarrhea, and you notice that his eyes are sunken and that his skin turgor is only fair. The mother tells you she wants to give an antidiarrheal medicine that she has at home and asks how much to give. What is the best response of the nurse?
Constipation
Pathophysiology: Constipation is defecation that is difficult or infrequent, with the passage of hard, dry fecal material. There may be associated symptoms, such as abdominal discomfort or blood-streaked stools.
Manifestations: The frequency of bowel movements varies widely in children. There may be periods of diarrhea or encopresis (constipation with fecal soiling). Constipation may be a symptom of other disorders, particularly obstructive conditions. Diet, culture, and social, psychological, and familial patterns may also influence its occurrence. The daily use of laxatives and enemas should be discouraged. Most children use the bathroom every day, but they may be hurried and have an incomplete bowel movement. Some children are embarrassed or even afraid to use school or public bathrooms.
Treatment and Nursing Care: Evaluation begins with a thorough history of dietary and bowel habits. Some infants respond to formula with a high iron content by developing constipation. Changing to a low-iron formula may be helpful. The frequency, color, and consistency of the stool are noted. The nurse inquires about any medication the child may be taking. The parents are asked to define what they mean by constipation. Parent teaching concerning the prevention of constipation is essential.
Dietary modifications include adding more roughage to the diet. Foods high in fiber include whole-grain breads and cereals, raw vegetables and fruits, bran, and popcorn for older children. Increasing fluid intake is also important. A stool softener such as docusate sodium (Colace) may be prescribed. The child is encouraged to try to move the bowels at the same time each day to establish a routine. The child should not be hurried. Increased exercise may help sedentary children. Constipation can be defined as fewer than seven bowel movements in a 2-week period; within that context, the use of rectal suppositories, laxatives, and stool softeners offer relief and can prevent a chronic constipation problem from occurring (Borowitz et al., 2005).
Fluid and Electrolyte Imbalance
Principles of Fluid Balance in Children
Infants and small children have different proportions of body water and body fat than adults do (Figure 28-9), and the water needs and water losses of the infant (per unit of body weight) are greater. In children under 2 years of age, surface area is particularly important in fluid and electrolyte balance because more water is lost through the skin than through the kidneys. The surface area of the infant is from 2 to 3 times greater than that of the adult in proportion to body volume or body weight. Metabolic rate and heat production are also 2 to 3 times greater in infants per kilogram of body weight. This causes more waste products to be produced, which must be diluted to be excreted. It also stimulates respiration, which causes increased evaporation through the lungs. Compared with adults, a greater percentage of body water in children under 2 years of age is contained in the extracellular compartment.
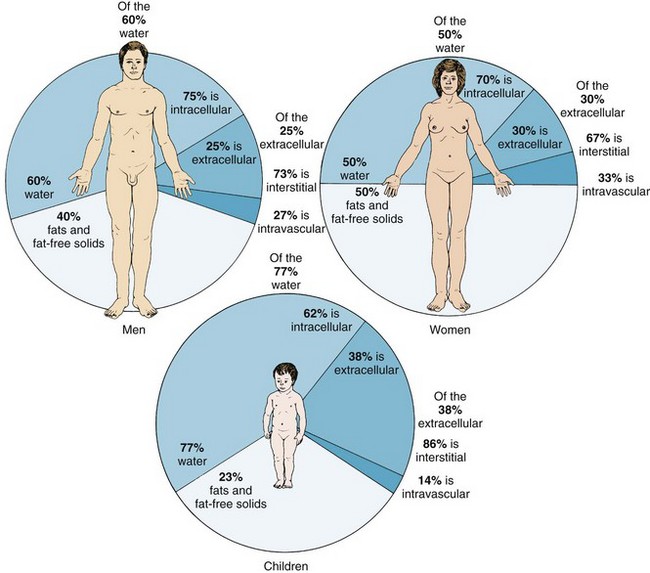
FIGURE 28-9 Relationship of body water and body solids to the body weight in the adult man and woman and in the child.
Fluid turnover is rapid, and dehydration occurs more quickly in infants than in adults (Table 28-2). The infant cannot survive as long as the adult in the presence of continued water depletion. A sick infant does not adapt as rapidly to shifts in intake and output because the kidneys lack maturity. They are less able to concentrate urine and require more water than an adult’s kidneys to excrete a given amount of solute. Disturbances of the GI tract often lead to vomiting and diarrhea. Electrolyte balance depends on fluid balance and cardiovascular, renal, adrenal, pituitary, parathyroid, and pulmonary regulatory mechanisms. Many of these mechanisms are maturing in the developing child and are unable to react at full capacity under the stress of illness, such as diarrhea and vomiting. Signs of dehydration in a child may not be evident until the fluid loss reaches 4%, and severe dehydration may not be evident until the fluid loss reaches 10% (Bender et al., 2005).
Table 28-2
Signs of Isotonic, Hypertonic, and Hypotonic Dehydration
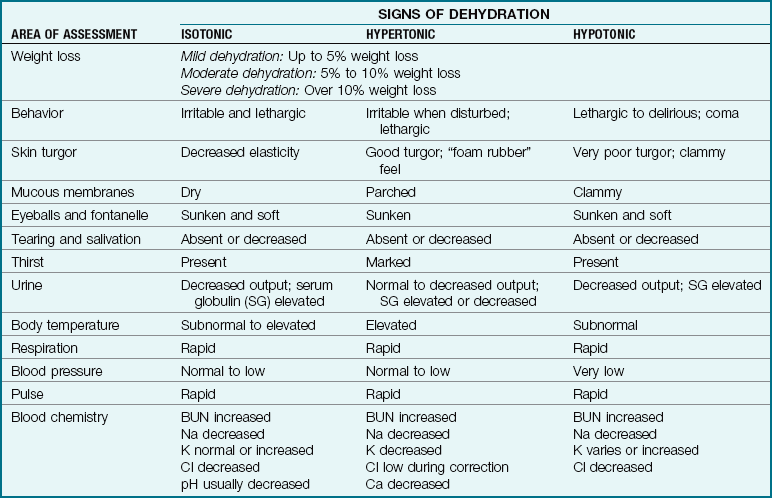
BUN, Blood urea nitrogen; Ca, calcium; Cl, chloride; K, potassium; Na, sodium.
Data from Bender, B., Skoe, C., & Ozuah, P. (2005). Oral rehydration therapy. Contemporary Pediatrics 22(4): 72-76; and Kliegman, R., Behrman, R., Jenson, H., & Stanton, B. (2007). Nelson textbook of Pediatrics, 18th ed. Philadelphia: Saunders. Data also from Barken, R., & Rosen, P. (2003). Emergency pediatrics (6th ed.). St. Louis: Mosby.
 Safety Alert!
Safety Alert!
An accurate intake and output record must be kept for all children with vomiting or diarrhea.
Oral Fluids: Oral rehydrating solution (ORS) alternatives such as Pedialyte or Infalyte are preferred to IV therapy (Bender et al., 2005). Nurses must use their ingenuity to coax sick children to take enough fluids, because they may refuse food and water and do not understand their importance for recovery. Toddlers and infants are not capable of drinking by themselves. The busy nurse must find time to offer fluids and must be patient and gently persistent. Liquids are offered frequently and in small amounts. Brightly colored containers and drinking straws may help. ORS options are available in varied flavors and in frozen ice pop forms that are more acceptable to the young child. The nurse keeps an accurate record of the patient’s intake and output. General hygiene and principles of preventing diarrhea are discussed with the parents. In 2002, the World Health Organization (WHO) advised that the contents of an optimum oral rehydration solution should contain 75 mEq/L of sodium; 75 mEq/L of glucose; and a total osmolarity of 245 mOsm/L. In the United States, most commercial “lyte” solutions, such as Pedialyte, Oralyte, Infalyte, and others, meet these criteria with a more desirable lower sodium content. Fluids with a high glucose or sodium content, such as colas and juices, should not be used. Oral rehydration fluids are usually given as 1 milliliter of ORS for every gram of output. Replacement fluid needs are usually estimated as 10 mL/kg for each stool and 2 mL/kg for each emesis. In addition, a simple protein and starch feeding, such as rice, potato, yogurt, fruits, vegetables, cereal, or bread can lessen fluid loss (Bender et al. 2005).
Parenteral Fluids: Parenteral fluids (para, “beside or apart from,” and enteron, “intestine”) are those given by some route other than the digestive tract. They are necessary when sickness is accompanied by vomiting or loss of consciousness or when the GI system requires rest. Parenteral fluids are needed in severe cases of vomiting and diarrhea in which the loss of water and electrolytes will lead to death if untreated. It also provides a means for the safe and effective administration of prescribed parenteral medications. Solutions given parenterally must be sterile to prevent a general or local infection. The nurse must be aware of the importance of parenteral therapy and the assessments required.
The infant or child receiving parenteral fluids needs the nurse’s warmth and affection. A pacifier should be used whenever infants are on NPO status. Parents should be encouraged to pick up and hold or rock their children who are receiving IV therapy. Arm boards prevent the child from pulling out the IV line and protect the tubing. Parenteral therapy is discussed in Chapter 22.
Dehydration
Pathophysiology: When a person is in good health, the intake and output of fluids are balanced and homeostasis (a uniform state) exists. This is accomplished by appropriate shifts of fluids and electrolytes across cellular membranes and by elimination of products of metabolism that are no longer needed or are in excess. The volume of blood plasma and interstitial and intracellular fluids remains relatively constant. Dehydration occurs whenever fluid output exceeds fluid intake, regardless of the cause.
Manifestations: Disorders of fluids and electrolytes—sodium (Na+), potassium (K+), calcium (Ca++), and magnesium (Mg++)—are more complex in growing children. A newborn’s total weight is comprised of approximately 77% water, compared with 60% in adults. This varies with the amount of fat. In addition, the daily turnover of water in infants is equal to almost 24% of total body water, compared with about 6% in adults. An infant’s body surface in comparison with weight is 3 times that of the older child; therefore the infant is subject to greater evaporation of water from the skin. The younger the patient, the higher the metabolic rate and the more unstable the heat-regulating mechanisms. (Elevations in temperature also increase the rate of water loss.) Rapid respirations speed up this process; when diarrhea is present, additional fluid is lost in the stools. Immaturity of the kidneys impairs the infant’s ability to conserve water. The average urine output in infants and children is seen in Table 28-3. Preterm and newborn infants are also more susceptible to dehydration from variations in room temperature and humidity. When this is coupled with higher fluid losses, life-threatening deficits can ensue within a few hours (Table 28-4).
Table 28-3
Average Daily Excretion of Urine
| AGE | FLUID OUNCES | MILLILITERS (mL) |
| Days 1 and 2 | 1-2 | 30-60 |
| Days 3-10 | 3-10 | 100-300 |
| Day 10–2 months | 9-15 | 250-450 |
| 2 months–1 year | 14-17 | 400-500 |
| 1-3 years | 17-20 | 500-600 |
| 3-5 years | 20-24 | 600-700 |
| 5-8 years | 22-34 | 650-1000 |
| 8-14 years | 27-47 | 800-1400 |
Table 28-4
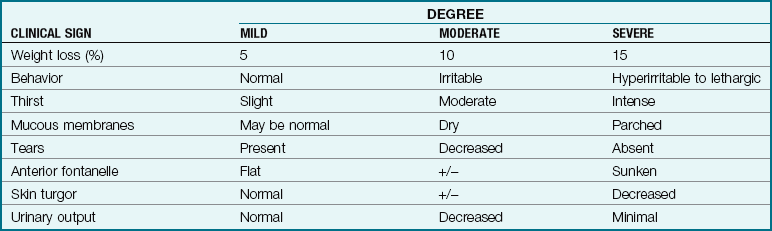
From Kliegman, R., Behrman, R., Jenson, H. & Stanton, B. (2007). Nelson textbook of pediatrics (18th ed.). Philadelphia: Saunders.
Problems of fluid and electrolyte disturbance require evaluation of the type and severity of dehydration, clinical observation of the patient, and chemical analysis of the blood. The types of dehydration are classified according to the level of serum sodium, which depends on the relative losses of water and electrolytes. These types are usually termed isotonic (the patient has lost equal amounts of fluids and electrolytes), hypotonic (the child has lost more electrolytes than fluid), and hypertonic (more fluids are lost than electrolytes) (see Table 28-2). These classifications are important because each form of dehydration is associated with different relative losses from intracellular fluid (ICF) and extracellular fluid (ECF) compartments, and each requires certain modifications in treatment.
Treatment and Nursing Care: Maintenance fluid therapy replaces normal water and electrolyte losses, and deficit therapy restores preexisting body fluid and electrolyte deficiencies. The composition of IV fluids and the amount and rate of flow are important in preventing complications.
Shock (hypovolemia) is the greatest threat to life in isotonic dehydration. The electrolyte content of oral fluids is particularly significant in the care of infants and small children suffering from disorders of fluid balance and receiving infusions. Commercially prepared electrolyte solutions, or ORS, are available. Children with hypotonic dehydration (excess water with sodium electrolyte depletion) are at risk for water intoxication. This can also occur if tap water enemas are given to small children. Potassium is lost in almost all degrees of dehydration. Replacement potassium is administered only after normal urinary excretion is confirmed. Documentation must include accurate assessment of intake and output, vital signs, daily weight, skin and fontanelles, mucous membranes, and level of consciousness.
Overhydration
Pathophysiology: Overhydration results when the body receives more fluid than it can excrete. This can occur in patients with normal kidneys who receive IV fluids too rapidly. It also can occur in a patient receiving acceptable rates of fluid, especially when the patient’s illness is related to disorders of fluid mechanism.
Manifestations: Edema is the presence of excess fluid in the interstitial (interstitium, “a thing standing between”) spaces. Interstitial fluid is similar to plasma, but it contains little protein. In healthy persons, it responds well to shifts in fluid balance. Any factor causing sodium retention can cause edema. The flow of blood out of the interstitial compartments also depends on adequate circulation of blood and lymph. Low protein levels can also disturb osmotic cellular pressure, causing edema. This is seen in patients with nephrosis, in which large amounts of albumin are lost.
Trauma to or infections of the head can cause cerebral edema, which can be life threatening. Constrictive dressings may obstruct venous return, causing swelling, particularly in dependent areas. Anasarca (ana, “throughout,” and sarx, “flesh”) is a severe generalized edema.
Treatment and Nursing Care: Edema in infants may first be seen about the eyes and in the presacral, occipital, or genital areas. In pitting edema, the nurse notices an impression in the skin that lasts for several seconds after exerting gentle pressure with the finger.
Early detection and management of edema are essential. Taking accurate daily weights is indispensable, as is close attention to body weight changes. Vital signs, physical appearance, and changes in urine character or output are noted.
Infants receiving IV therapy have their IV and oral intakes recorded. If the oral intake falls below prescribed rates, the IV rate is increased. If the oral intake exceeds prescribed levels, the IV rate is decreased or the IV is heparin- or saline-locked to maintain patency and prevent overhydration.
Electrolyte imbalance: The nurse must be able to assess the electrolyte needs of the child (Table 28-5). When fluid snacks or nourishment are ordered, the selection of fluid can influence the treatment given for dehydration. For example, if the child has a hypertonic type of dehydration (which means there is excess sodium) and the nurse offers the child tomato juice, the high sodium content of tomato juice will negatively affect the child’s prescribed treatment. If the child has hypotonic dehydration (which means the child has deficient electrolytes) and the nurse offers plain water, this will also have a negative impact on the child’s care. Therefore it is a nursing responsibility to correlate laboratory findings of the individual child with fluids and foods offered to the child.
Nutritional Deficiencies
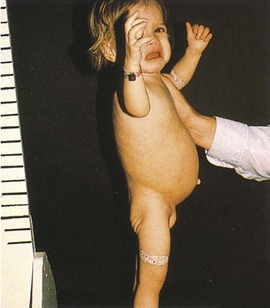
Because infancy is a period of rapid growth, poor nutrition is particularly dangerous at this time. Severe vitamin deficiencies are rare in prosperous countries; those that do occur are generally caused by poverty, ignorance, or neglect. Figure 28-10, A, shows a child, from the United States, with general, moderate malnutrition. Severe malnutrition is still rampant in many underdeveloped countries. Every person must be concerned with the plight of the starving child. Sometimes the infant’s body is unable to use food even though the diet is adequate. An example of this is celiac disease, in which the intestines are unable to handle fats and starches. Severe malnutrition may also be seen in failure to thrive.
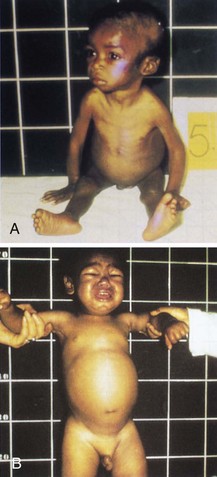
FIGURE 28-10 A, Failure to thrive is a general nutritional-calorie deficiency. Note the profound wasting found in malnutrition or starvation. B, Kwashiorkor, caused by a protein deficiency. The infant has generalized edema with a white streak in the hair.
Failure to Thrive
Pathophysiology: Failure to thrive (FTT) describes infants and children who, without an obvious cause, fail to gain and often lose weight. This condition can be caused by physical (organic) pathological dysfunction (OFTT), such as congenital heart disease or malabsorption syndromes. It may be caused by a lack of parent-infant interaction that can result from environmental factors, neglect, or lack of information concerning the nutritional needs of infants; this is nonorganic failure to thrive (NFTT). FTT can be caused by environmental stresses.
Infants who fail to thrive are often admitted to the hospital for evaluation with presenting symptoms of weight loss or failure to gain, irritability, and disturbances of food intake such as anorexia or pica (abnormal consumption of nonfood materials). Vomiting, diarrhea, and general neuromuscular spasticity sometimes accompany the condition. Children fall below the third percentile (some authorities suggest the fifth) in weight and height on standard growth charts. Their development is delayed. Children who fail to thrive seem apathetic. Some have a “rag doll limpness” (hypotonia), and they often appear wary of their caregivers. Others appear stiff and unresponsive to cuddling. The personality of the infant may not foster maternal attachment. FTT with malabsorption has been reported with frequency among autistic children and among institutionalized mentally retarded children. The child has a complete workup to identify organic reasons for FTT, and the cause is treated.
Manifestations: With NFTT, there may be a disturbance in the mother-child or caregiver-child relationship. The situation is complex and is often associated with marital discord, economic pressures, parental immaturity, low stress tolerance, and single parenthood. Alcohol and drug abuse can be present. Many mothers feel deprived and unloved and have conflicting needs. Infants suffer from the inability to establish a sense of trust in their caregivers. Their coping abilities are affected by a lack of nurturing. Obvious neglect and physical abuse are not uncommon.
Prevention of environmental FTT consists chiefly of social measures such as parenting classes, family planning, and early recognition and support of families at risk. All children should receive routine health assessments. The pregnancy history may reveal circumstances that may contribute to a lack of bonding, such as an unplanned pregnancy or desertion by the child’s father. Planning interventions that will enhance parent-infant interaction is an important nursing responsibility.
Treatment and Nursing Care: Treatment involves a multidisciplinary approach in accordance with the circumstances; that is, the physician, the nurse, the social worker, the family agency, and the counselor may all participate. If no progress can be made, temporary or permanent placement of the child or children in a foster home may be required. During hospitalization, one nurse per shift is selected to increase nurturing and interaction with the infant and parent.
Treatment of the child who fails to thrive requires maturity on the part of the nurse. It is vital to support rather than reject the mother. Maternal attachment can be facilitated by listening and helping the mother to understand her feelings and frustrations and to explore her choices. The nurse encourages her to assist with the daily care of her child. The child’s uniqueness and responses to the mother are stressed. The nurse points out developmental patterns and provides anticipatory guidance in this area. Often the mother’s lack of interest stems from her own insecurities. Parents Anonymous and parent aides are other resources.
The prognosis of this condition is uncertain. Emotional starvation, particularly in the early years, can be psychologically traumatic. Inadequacies in intelligence, language, and social behavior have been documented in children who fail to thrive.
Kwashiorkor
Pathophysiology: Kwashiorkor is a protein deficiency. In many parts of the world, children still starve to death. There are no well-planned maternal and child health programs to elevate health standards in these localities. In some areas, superstition and ignorance prevent children from using nutritious foods found in their environment. In kwashiorkor, there is a severe deficiency of protein in the diet despite the fact that the number of calories consumed may be nearly adequate. It belongs to a class of disorders termed protein-energy malnutrition (see Figure 28-10, B).
Manifestations: Kwashiorkor occurs in children 1 to 4 years of age who have been weaned from the breast. Kwashiorkor means, in native dialect, “the disease of the deposed baby when the next one is born,” indicating that the child no longer breastfeeds because a sibling is born and takes over the breast of the mother. Oral intake then is deficient in protein. The child fails to grow normally. The muscles become weak and wasted. There is edema of the abdomen that may become generalized. Diarrhea, skin infections, irritability, anorexia, and vomiting may be present. The hair becomes thin and dry. Because protein is the basis of melanin, a substance that provides color to hair, melanin becomes deficient. This is the reason the earliest sign of this protein malnutrition is a white streak in the hair of the child (depigmentation). The child looks apathetic and weak.
Treatment and Nursing Care: Treatment for kwashiorkor is mainly preventive. Although hunger may never be completely eradicated in the world, many private, public, and world health agencies sponsor programs to alleviate such suffering. Simple protein powder sprinkled on the culturally prepared meal will alleviate the problem. Early dietary treatment in established cases may prevent more serious growth retardation.
Rickets
Pathophysiology: Rickets is a disease of infancy and childhood caused by deficient amounts of vitamin D. Vitamin D and exposure to sunshine are necessary for the proper absorption and metabolism of calcium and phosphorus, which are needed for the normal growth of bones.
Scurvy
Scurvy is a disease caused by insufficient fruits and vegetables that contain vitamin C in the diet. The symptoms of scurvy include joint pains, bleeding gums, loose teeth, and lack of energy. Good sources of vitamin C are citrus fruits and raw, leafy vegetables. Vitamin C is easily destroyed by heat and exposure to air. Small amounts of water should be used for cooking vegetables to prevent vitamin C from being destroyed, because it is also water soluble. It may be given to infants in the form of orange juice, which should not be boiled. Vitamin supplements prescribed for infants and children contain vitamin C. The vitamin is not stored in the body, and daily intake from food sources is required.
Infections
The most common reason for emergency abdominal surgery in childhood is appendicitis, with over 80,000 cases each year in the United States. The average age of occurrence is 10 years of age. The challenge in diagnosing appendicitis is that rupture or perforation of the appendix can occur with serious complications within 36 hours after the onset of abdominal pain. A delay in diagnosis often occurs because the child is unable to localize or express the symptoms experienced.
Pathophysiology and Manifestations: The appendix is a small appendage arising from the cecum; it is located on the right side of the abdomen. The lumen may become obstructed with fecal matter or with lymphoid tissue after a viral illness or with parasites. There is stasis, increased swelling, edema, and growth of organisms. The initial pain perceived is usually periumbilical and increases within a 4-hour period. When the inflammation spreads to the peritoneum, the pain localizes in the right lower quadrant (RLQ) of the abdomen. The appendix may become gangrenous or rupture, causing peritonitis and septicemia. Vomiting may occur after periumbilical pain starts. (In children with gastroenteritis, vomiting precedes abdominal pain.) Infrequent mucus diarrhea may occur because of intestinal irritation due to developing peritonitis. (Frequent watery stools are associated with gastroenteritis.) Fever is not a reliable sign of appendicitis in children. On examination, characteristic tenderness in the right lower quadrant known as McBurney’s point will occur. Other diagnostic signs include the following:
• Guarding: There is a tightening of the abdominal muscles or rigidity of the abdomen on palpation.
• Rebound tenderness: Pressing the RLQ with rapid release of pressure causes severe pain.
• Pain on lifting the thigh while in the supine position is caused by muscle irritation.
• Pain in the RLQ when palpated and pain on rectal examination often occurs.
Laboratory tests may be done to confirm the diagnosis and rule out other possible diagnoses. A urinalysis will rule out a urinary tract infection. C-reactive protein levels will be increased after 12 hours if any infection is present. An abdominal x-ray study (kidney, ureter, and bladder [KUB]) will show a right-sided curvature of the spine, a dilated cecum with an air or fluid level, and a decrease in bowel gas in the RLQ (if ruptured). An ultrasound will show a thickened appendix and a soft tissue mass in the RLQ, and it is used to rule out an ovarian cyst in females who may exhibit similar clinical signs. A computed tomography (CT) scan with rectal contrast (CTRC) is administered via the rectum to confirm the enlarged appendix. A culture of the stool may be done to rule out gastroenteritis. A laboratory evaluation of the white blood cell (WBC) count will show an increased WBC with neutrophils increased 75% but may not be helpful in diagnosing an unperforated appendix. Signs of ruptured appendix and peritonitis includes sudden relief of acute pain, rigid guarding of the abdomen, abdominal distention, tachycardia, chills, and irritability.
Treatment and Nursing Care: Observing the behavior of the child in relation to the developmental level and using pain perception scales can help assess the pain level. A warmed stethoscope should be used when auscultating the abdomen of a child; it is less frightening than the approaching fingers of the hand. The child and family are prepared for the diagnostic tests and possibility of surgery. An explanation of the reason for NPO status until the need for surgery is determined will help with compliance. The nurse should explain what to expect, discuss coping mechanisms, and provide referrals as necessary. Postoperative care is similar to that for any abdominal surgery. IV therapy is gradually replaced with fluids and food. A drain may be present at the wound site if perforation has occurred, and a frequent change of dressings may be necessary. Pain management, prevention of infection, and early ambulation are the primary goals.
Thrush (Oral Candidiasis)
Pathophysiology: Thrush is an infection of the mucous membranes of the mouth caused by the fungus Candida. This organism is normally present in the mother’s vagina and is nonpathogenic. However, the altered conditions in the vagina produced by pregnancy may lead to the development of monilial vaginitis. The mucous membranes of the infant’s mouth may become infected by direct contact with this infection during delivery or by contact with the mother’s or nurse’s contaminated hands. Cross-infection of other newborns may result.
Manifestations: White patches that resemble milk curds appear on the tongue, inner lips, gums, and oral mucosa. They are painless but cannot be wiped away. Anorexia may be present. The systemic symptoms are mild if the infection remains in the mouth; however, it can pass along the mucous membranes into the GI tract, causing inflammation of the esophagus and the stomach. Pneumonitis may also develop. Epstein’s pearls, which are small, white, epithelial cysts that appear along both sides of the midline of the hard palate, are sometimes mistaken for thrush. These are harmless and gradually disappear.
Treatment and Nursing Care: A thrush infection responds well to the local application of an antifungal suspension such as nystatin (Mycostatin). The mouth is swabbed 3 or 4 times a day between feedings with a sterile applicator moistened with the prescribed solution. With proper care, the condition disappears within a few days after its onset.
Newborns suspected of having thrush are cared for using isolation (standard) precautions. Individual feeding equipment is necessary, and the equipment should be sterile. Disposable bottles or prefilled formula bottles are used. Disposable nipples, pacifiers, and bottles are preferred.
Candida infection of the diaper area presents as a bright red, sharply demarcated diaper rash. Nystatin cream is often prescribed.
 Nursing Tip
Nursing Tip
In the home, parents are taught to drop nystatin or other medication slowly into the side of the infant’s mouth. Medication must remain in contact with “patches” as long as possible. Instruct parents to watch for dehydration (e.g., decrease in number of wet diapers) because of the infant’s refusal to take fluids because of mouth discomfort.
Worms
The main nursing responsibility is the education of the patient and family concerning the prevention of worm infestation through general hygiene, food handling, and environmental controls.
Pathophysiology: Of the several varieties of worms that affect humans, the most common is the pinworm, Enterobius vermicularis (enteron, “intestine,” bios, “life,” and vermis, “wormlike”). It is seen more often in toddlers but can develop in older children and adults. The pinworm looks like a white thread about  inch long. It lives in the lower intestine but comes out of the anus to lay its eggs, generally during the night. These eggs become infective a few hours after they have been deposited. This type of parasite spreads from one person to another, particularly where large groups of children are in close contact with one another. The route of entry is the mouth; the child becomes infected by ingesting the eggs. Reinfection takes place by way of contact from the rectum to the fingers to the mouth or by way of the rectum to the clothing to the fingers to the mouth.
inch long. It lives in the lower intestine but comes out of the anus to lay its eggs, generally during the night. These eggs become infective a few hours after they have been deposited. This type of parasite spreads from one person to another, particularly where large groups of children are in close contact with one another. The route of entry is the mouth; the child becomes infected by ingesting the eggs. Reinfection takes place by way of contact from the rectum to the fingers to the mouth or by way of the rectum to the clothing to the fingers to the mouth.
Manifestations: The nurse or parent may notice that the child scratches the anal area and may complain of itching. There may be associated irritability and restlessness. Weight loss, poor appetite, and fretfulness during the night can develop. The rectal area may become irritated from scratching. A special pinworm diagnostic tape or paddle or a tongue blade covered with cellophane tape, sticky side out, may be placed against the anal region to obtain pinworm eggs (the “Scotch tape test”). This is done early in the morning, before the child has a bowel movement, bathes, or scratches the anal area with the fingers. The tape is put on a glass slide and examined under a microscope. The eggs are typical of pinworms.
Treatment and nursing care: Several effective anthelmintics (anti, “against,” and helminth, “worms”) are available. Mebendazole (Vermox) is a single-dose, chewable tablet and is the drug of choice for children over 2 years of age. Pyrantel pamoate (Antiminth) also controls the infestation. Pyrvinium pamoate (Povan) suspension, a one-dose treatment, is an alternative drug; nurses advise parents that Povan stains and turns the stools red.
The child must be taught to wash the hands well after bowel movements. The child’s fingernails are kept short. A soothing ointment is applied to the rectal area. The patient should wear clean underwear that fits snugly to prevent scratching the anus with the fingers.
All symptomatic members of the family should be treated for this condition to prevent reinfection. Pregnant women should not take Vermox and should consult a physician before taking any alternative drug. The toilet seats in the home are scrubbed daily. Cloth diapers and bed linens are washed in hot water.
Ascariasis (Roundworms): Ascaris lumbricoides is a roundworm, and infestation can be asymptomatic or cause abdominal pain. The infestation is estimated to affect 1 billion persons worldwide. Roundworms thrive in warm climates and among the impoverished. In the United States, it is seen more often in the Southern states and among immigrants and migratory workers living below poverty levels. It is caused by the unsanitary disposal of human feces and poor hygiene practices. An egg from an infected person can survive for weeks in the soil. The child ingests eggs from contaminated soil. The eggs develop into larvae in the intestine, penetrate the intestinal wall, and enter the liver, from which they circulate to the lungs and heart. The patient is generally without symptoms until the larvae reach the glottis, are coughed up, swallowed, and enter the small intestine. There they develop into adult male and female species. They survive on undigested food in the canal and produce eggs that are expelled in the child’s feces. A chronic cough without fever is characteristic of this condition. Diagnosis is made by confirmation of the eggs in the patient’s stool. The treatment of ascariasis is the same as that for enterobiasis (pinworms).
Poisoning
Goals in the treatment of poisoning are the following:
General Concepts
Volume of a Swallow: The volume of a swallow has been estimated to be 0.21 mL/kg of body weight. Thus a child age 2 to 3 years who takes one swallow may have ingested about 3 mL of poison.
Principles of Care: Education of parents and children is the best way to prevent poisoning. The school and the clinic are the best resources to be used in an active accident prevention program.
Poison Control Centers: The telephone number of the poison control center is listed in the telephone directory and should be posted near the phone. Dialing 800-222-1222 anywhere in the United States will route the call to the nearest poison control center that can identify the antidote or treatment needed for specific poisons.
Ipecac Syrup: Traditionally, syrup of ipecac was the treatment of choice to remove some types of poisons from a child’s system and parents were advised to keep a supply on hand in the home. However, the American Academy of Pediatrics (AAP) revised this policy in 2003 (Barclay & Nghiem, 2009). Parents are now advised to call the poison control center and bring the container of the substance ingested to the hospital emergency department as quickly as possible because stomach lavage is rarely effective 1 hour or more after ingestion. Ipecac syrup should not be kept in the home. Uncontrolled vomiting can cause serious complications. Table 28-6 indicates how to assess the type of toxic substance ingested according to the smell of the vomitus.
Table 28-6
Detecting the Poison by Specific Odor of Vomitus
| ODOR OF VOMITUS | PROBABLE CONTENT |
| Sweet | Chloroform, acetone |
| Bitter almond | Cyanide |
| Pear | Chloral hydrate |
| Garlic | Phosphorus, arsenic |
| Shoe polish | Nitrobenzene |
| Violet | Turpentine |
note: The nurse should report and document the specific odor of vomitus, which can be helpful in determining the specific poison contained in the substance ingested.
Activated Charcoal: Activated charcoal will absorb poisons such as strychnine, atropine, malathion, arsenic compounds, phenobarbital, quinine, theophylline, salicylates, valproic acid and phenytoin. When activated charcoal is given together with ipecac, however, they neutralize each other and render both ineffective in the treatment of poisoning. Activated charcoal may be given orally or by nasogastric tube. When administering oral activated charcoal it is first mixed with water to form a slurry and then administered mixed with cola or chocolate milk or flavored with sorbitol via a straw to make it more palatable. The recommended dose of activated charcoal is 1 to 2 g/kg of body weight. Charcoal or any gastric lavage may not be effective if administered more than 1 hour after ingestion and is therefore not routinely recommended.
Poisonous Plants
Many common plants used to landscape homes can be poisonous to the young child exploring in the backyard.
 Health Promotion
Health Promotion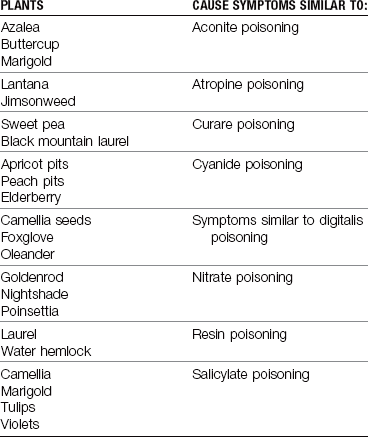
Drugs
Drugs prescribed for family members and left within the reach of children are often the cause of accidental poisoning. Many over-the-counter medications are considered harmless by parents but can be deadly to toddlers, even in small doses (Table 28-7). Even a small amount of an oral hypoglycemic drug can lower blood sugar in a small child and result in a coma. Herbal remedies can also be poisonous to small children (Hawke, 2005).
Table 28-7
Selected Over-the-Counter Drugs That Are Deadly to Toddlers
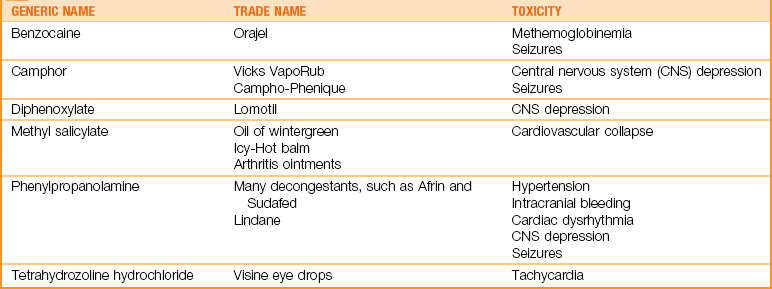
Data from Osterhardt, K. (2000). The toxic toddler: Drugs that can kill in small doses. Contemporary Pediatrics, 17(3):73; Wong, D., Perry, S., Hockenberry, M., Lowdermilk, D., & Wilson, D. (2006). Maternal-child nursing care (3rd ed.). St. Louis: Mosby; and Thomson Physician’s Desk Reference (2010). Montvale, NJ: Medical Economics.
Acetaminophen Poisoning
Acetaminophen overdose is listed along with other poisons commonly encountered in pediatrics in Box 28-1.
Pathophysiology: Acetaminophen (Tylenol) has now replaced aspirin as the most commonly ingested drug that causes toxicity. This is because it is so widely used and because aspirin, which has been associated with Reye’s syndrome, is no longer recommended for fever in children with flulike symptoms. Because parents are often informed that acetaminophen is “safer” than aspirin, they may be more careless in storing it. Acetaminophen poisoning occurs most often from acute overdose rather than from the cumulative effects seen with aspirin. Because acetaminophen is metabolized in the liver, overdose results in hepatic destruction. With early treatment, most children recover without complications. Tylenol drops and Tylenol Elixir each have a different potency. When “1 teaspoon of Tylenol” is advised, the nurse must be sure the parent understands which preparation to purchase, or a massive overdose can occur.
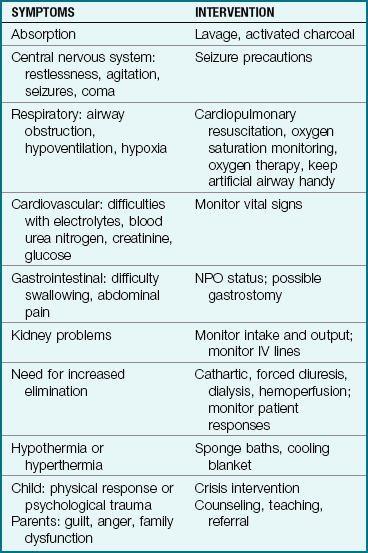
Manifestations: Manifestations and treatment modalities that the nurse might anticipate in patients with acute poisoning are shown in Table 28-8.
Treatment and Nursing Care: The stomach is emptied by lavage or induced emesis from syrup of ipecac. Depending on the serum acetaminophen level, this may be followed by the N-acetylcysteine (Mucomyst) antidote. In small children, it may be administered directly into the nasogastric tube after lavage. Otherwise it is generally given orally every 4 hours for 72 hours. This medicine has a bad smell and taste, and the patient needs coaxing and support to assist with compliance. The medicine may be mixed with a soft drink or juice. Levels of liver enzymes (ALT and AST) are monitored. Prevention of overdose is of utmost importance. Even in uncomplicated cases the child is subjected to unpleasant, stressful procedures.
Salicylate Poisoning
Pathophysiology: Aspirin (acetylsalicylic acid) poisoning is seen less often than in the past because of safety packaging and the increased use of acetaminophen. Nevertheless, aspirin is often used in many homes and may be stored carelessly on bedside stands or in a mother’s purse. Oil of wintergreen (methyl salicylate) is also extremely hazardous when mistakenly administered as cough medicine or swallowed by the curious child. It is sometimes used as a home remedy for arthritic pain. Even a dose as small as 1 teaspoon can cause a child’s death.
Manifestations: Salicylate acts rapidly but is excreted slowly. Ingestion of 150 mg/kg of body weight causes symptoms. Although most cases of aspirin poisoning are emergencies, a child may unknowingly be poisoned by the cumulative effect of aspirin. The use of several aspirin-containing products at once, such as over-the-counter cold remedies and aspirin, can be hazardous. Time-release aspirin is especially dangerous because the symptoms of poisoning are delayed and aspiration of the stomach is of little value. Therefore it is wise to read labels carefully and to administer aspirin sparingly. It is even better to use it only under a physician’s direction.
Treatment and Nursing Care: Vitamin K is administered to control bleeding. Peritoneal dialysis (peritoneum and dialysis, “passing of a solute through a membrane”) is a therapeutic measure used in acute renal failure. The therapy uses the principles of osmosis and diffusion through the semipermeable peritoneal membrane, with the purpose of removing toxic substances from the blood. Hemodialysis is another method used for essentially the same purpose.
The nurse must realize the danger of drug poisoning and must constantly practice and teach safety measures to prevent tragedies. Treatment and utility rooms and drug baskets are scrutinized to ensure that nothing harmful is within the reach of ambulatory children.
Lead Poisoning (Plumbism)
Pathophysiology: Lead poisoning (plumbism) results when a child repeatedly ingests or absorbs substances containing lead. The primary source is paint from old, deteriorating buildings. The lead contents of food, water, and air have decreased substantially since 1990. Lead poisoning is most common in children between 18 months and 3 years of age. Although the incidence is highest among the poor, lead poisoning is also found among suburban and middle-class children.
Children who chew on windowsills and stair rails may ingest flakes of paint, putty, or crumbled plaster. Eating nonfood items is called pica. Food, particularly fruit juices consumed from improperly glazed earthenware, is another source. Lead poisoning among Mexican Americans may result from azarcon, a bright orange powder containing approximately 93.5% lead. Azarcon is used as a folk remedy to treat “empacho” and other digestive problems in infants. Lead poisoning among Hmong Laotian refugees may be caused by paylooah, a bright orange-red powder that may be used for fever or rash. Unwashed fresh fruit sprayed with insecticides and dust from enclosed shooting galleries are also culprits. Some alternative therapies such as ayurveda medicines contain lead (Cleveland et al., 2008). Another source is dust in homes near lead-processing plants. “Spitballs” made from the colored section of newspaper comics are also a source of lead poisoning. Older synthetic venetian or vertical blinds used as window coverings, brightly colored metal vases, and lead crystal are other common sources for lead poisoning in the home when a toddler handles the item and then places the hands in the mouth. Many toys and jewelry made in China have been recalled because of high lead content.
Lead can have a lasting effect on the nervous system, especially the brain. Increased lead levels, even below 10 mcg/dL, can cause developmental delays and aberrant behaviors. Mental retardation may occur in severe cases. In much of the United States, lead poisoning is a reportable disease. The Agency for Toxic Substances and Diseases Registry (ATSDR) provides information on this condition.
Manifestations: The symptoms occur gradually and range from mild to severe. Because the infant’s or young child’s central nervous system is extremely vulnerable, acute symptoms of encephalitis may follow a relatively short period of exposure. The lead settles in the soft tissues and bones and is excreted in the urine. In the beginning, signs may be seen such as weakness, weight loss, anorexia, pallor, irritability, vomiting, abdominal pain, and constipation. In later stages, signs of anemia and nervous system involvement, such as muscular incoordination, neuritis, convulsions, and encephalitis, are seen. Being exposed to lead during pregnancy can lead to problems in the newborn.
Treatment and Nursing Care: Blood and urine tests are performed to determine the amount of lead in the system. Lead is especially toxic to the synthesis of heme in the blood; heme is necessary for hemoglobin formation and for the functioning of renal tubules. Blood lead levels are the primary screening test. X-ray films of the bones show further deposits of lead. The child’s history may reveal pica, a condition in which the child has a distorted appetite and eats a variety of things that most persons consider unpalatable, such as sand, grass, wool, glass, plaster, coal, animal droppings, and paint from furniture.
Treatment is aimed at reducing the concentration of lead in the tissues and blood. Chelating agents that render the lead nontoxic and increase its excretion in the urine are given in more severe cases. Calcium disodium edetate (Calcium Disodium Versenate, CaEDTA) and dimercaprol are commonly used. CaEDTA may be given intravenously or as a deep intramuscular injection. Mild symptomatic lead poisoning may be treated with meso-2,3,-dimercaptosuccinic acid (DMSA). It can be given orally, has not been associated with serious side effects and, unlike CaEDTA, does not cause zinc depletion. British antilewisite (BAL) is also used together with CaEDTA but may not be given to children who have a peanut butter allergy or are taking supplemental iron. Complete deleading takes several months, and retreatment may be necessary when the child has an acute infection or other metabolic disturbance.
Safety Alert!
CaNa2EDTA is a chelating agent. Na2EDTA is not interchangeable and should not be used.
The prognosis depends on the extent of poisoning. All children with elevated lead blood levels must be followed to evaluate developmental and intellectual milestone achievement. Providing an increased fluid intake and monitoring intake and output during therapy is an important nursing responsibility.
Prevention of this condition is of foremost importance. Lead paint should not be used on children’s toys or furniture. Instead, one should use paint marked for indoor use. Inexpensive lead detection kits are available at most home improvement stores. The kit contains a “crayon” that can be rubbed on the vertical blind or other items in the home; it turns a different color if significant lead is present. Lead level screening of children in high-risk areas is recommended.
Foreign Body Ingestion
Approximately 80% of all foreign body ingestion occurs in children between 6 months and 3 years of age. About 80% of the foreign bodies ingested pass through the GI tract, but others require surgical removal (Uyemura, 2005). The high level of curiosity of the young child and the tendency to place objects in the mouth increase the susceptibility to accidental ingestion of a nonfood object. Unless the object is sharp or large, passage through the GI tract may be possible and can take up to 4 to 6 days. The child is cared for at home, and the nurse should emphasize the importance of cutting and examining each stool until the object is passed successfully.
The nurse should caution parents not to use laxatives and to maintain a normal diet to prevent the intestinal spasms that may precipitate an obstruction. Parents should be instructed to notify the physician if abdominal pain or vomiting occurs. Follow-up care and teaching concerning safety in the environment and the prevention of ingesting or inhaling foreign bodies are priority nursing responsibilities.
Get Ready for the NCLEX® Examination!
Key Points
• The newborn should be closely observed for signs of tracheoesophageal fistula (TEF), which include coughing, choking, cyanosis, and apnea during feedings.
• Drooling in the newborn may be a sign of an obstructed esophagus or TEF.
• The first stool of the newborn should be documented to record the patency of the anus.
• Pyloric stenosis is caused by hypertrophy of the pyloric muscles and is manifested by projectile vomiting.
• Nursing care for the child with pyloric stenosis involves frequent assessment, careful feeding, positioning on the right side after feedings, and education and support of the parents.
• Large, bulky, frothy stools are characteristic of malabsorption syndromes.
• Celiac disease is caused by an intolerance to gluten in the diet.
• To prevent the development of water intoxication, tap water should not be used for enemas in children with megacolon.
• Intussusception is characterized by currant jelly stools.
• Hirschsprung’s disease occurs when there is an absence of ganglionic innervation of the muscle of a bowel segment.
• The treatment of gastroesophageal reflux includes thickened feedings, burping, and maintaining Fowler’s position.
• A diarrheal stool in an infant is manifested by a watery consistency and a greenish color with the possible presence of mucus or blood. Frequency of bowel movements, by itself, is not an indication of diarrhea in infants.
• Hand hygiene with soap and water rather than an alcohol-based hand sanitizer is recommended when caring for patients with Clostridium difficile diarrhea. The environment should be cleaned with a bleach disinfectant by housekeeping staff.
• Teaching parents basic hygienic practices, handwashing, and proper animal handling can prevent outbreaks of diarrhea.
• The functions of the gastrointestinal tract have a great influence on the fluid and electrolyte balance in infants and children.
• The higher daily exchange of water that occurs in infants leaves them less volume reserve when they are dehydrated.
• Oral rehydrating solutions are commercially prepared electrolyte solutions.
• Isotonic dehydration is the loss of equal amounts of water and electrolytes. Hypertonic dehydration is the loss of more water than electrolytes. Hypotonic dehydration is the loss of more electrolytes than water.
• Infants who are fed by the IV route should be picked up and held and allowed to suck on a pacifier.
• An intake and output record includes accurate documentation of information concerning oral and parenteral intake and suction, wound drainage, sweating, vomiting, urine, and stool output.
• Kwashiorkor is a protein deficiency characterized by a depigmented (white) streak of hair.
• Disposable nipples, pacifiers, and bottles should be used for infants with thrush.
• Pinworm is diagnosed by a “Scotch tape test.” Preventing the child from scratching the anal area is an essential part of breaking the cycle of worm reinfestation.
• A chronic productive cough without fever is part of the roundworm life cycle in children.
• The nurse should teach parents not to store poisonous substances in food containers.
• Prevention of accidental poisoning should be part of every parent–teaching plan.
• Pica, the eating of nonfood items, is characteristic of children with lead poisoning.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Gastrointestinal conditions: http://digestive.niddk.nih.gov/ddiseases/a-z.asp
• Poisoning: www.healthychild.net/articles/sf391ipecac.html
• Pyloric stenosis: http://kidshealth.org/parent/medical/digestive/pyloric_stenosis.html
Review Questions for the NCLEX® Examination
1. The pathologic disturbance of pyloric stenosis results from:
1. edema of the pyloric muscle.
2. ischemia of the pyloric muscle.
2. Which menu selections are best for a child diagnosed with celiac disease?
3. After surgery for pyloric stenosis, the nurse could anticipate that the infant will:
1. have nasogastric suction for 24 hours.
2. be fed clear liquids within 6 hours.
4. How are pinworms diagnosed?
1. Seeing the worm in the stool
3. A “Scotch tape test” in the early morning
4. A stool laboratory examination obtained at the hour of sleep
5. Priority teaching for a parent of a child who ingested a foreign body includes: