The Child with a Metabolic Condition
1 Define each key term listed.
2 Relate why growth parameters are of importance to patients with a family history of endocrine disease.
3 List the symptoms of hypothyroidism in infants.
4 Discuss the dietary adjustment required for a child with diabetes insipidus.
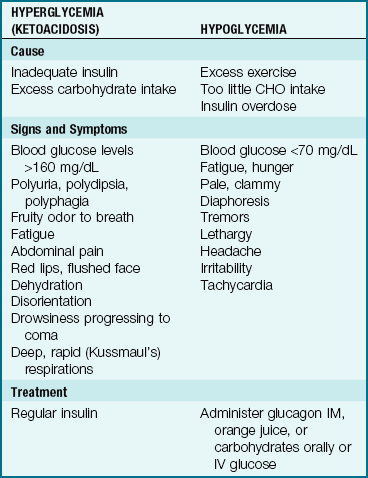
5 Compare the signs and symptoms of hyperglycemia and hypoglycemia.
6 Differentiate between type 1 and type 2 diabetes mellitus.
7 List three precipitating events that might cause diabetic ketoacidosis.
8 List a predictable stress that the disease of diabetes mellitus has on children and families during the following periods of life: infancy, toddlerhood, preschool age, elementary school age, puberty, and adolescence.
9 Outline the educational needs of the parents and the child with diabetes mellitus in the following areas: nutrition and meal planning, exercise, blood tests, glucose monitoring, administration of insulin, and skin care.
10 List three possible causes of insulin shock.
11 Explain the Somogyi phenomenon.
12 Discuss the preparation and administration of insulin to a child, highlighting any differences between pediatric and adult administration.
 , p. 714)
, p. 714)
 , p. 714)
, p. 714) , p. 714)
, p. 714) , p. 721)
, p. 721) , p. 711)
, p. 711) , p. 715)
, p. 715) , p. 720)
, p. 720) , p. 714)
, p. 714) , p. 714)
, p. 714) , p. 714)
, p. 714) , p. 711)
, p. 711) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Integration of the Nervous and Endocrine Systems
The two major control systems that monitor the functions of the body are the nervous system and the endocrine system. These systems are interdependent. The endocrine, or ductless, glands regulate the body’s metabolic processes. They are primarily responsible for growth, maturation, reproduction, and the response of the body to stress. Figure 31-1 depicts the organs of the endocrine system and outlines how this system in children differs from that in adults. Hormones are chemical substances produced by the glands. They pour their secretions directly into the blood that flows through them. An organ specifically influenced by a certain hormone is called a target organ. Too much or too little of a given hormone may result in a disease state.
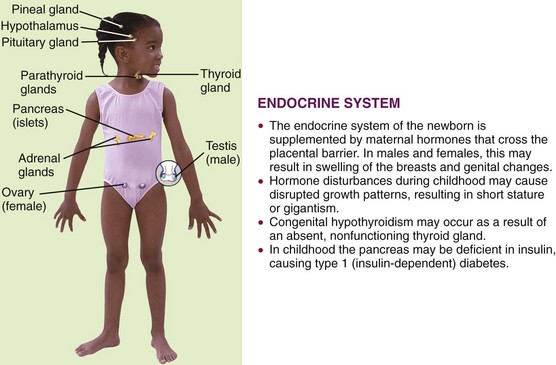
FIGURE 31-1 Summary of some endocrine system differences between the child and the adult. The endocrine system consists of the ductless glands that release hormones. It works with the nervous system to regulate metabolic activities.
Most of the glands and structures of the endocrine system develop during the first trimester of fetal development. Hormonal control is immature until at least 18 months of age, and therefore infants are more prone to problems related to the functioning of the endocrine system. Maternal endocrine dysfunction may affect the fetus; therefore an in-depth maternal history is a valuable tool in data collection.
The absence or deficiency of an enzyme that has a role in metabolism causes a defect in the metabolism process; this can result in illness. Most inborn errors of metabolism can be detected by clinical signs or screening tests that can be performed in utero. Lethargy, poor feeding, failure to thrive, vomiting, and an enlarged liver may be early signs of an inborn error of metabolism in the newborn. When clinical signs are not manifested in the neonatal period, an infection or body stress can precipitate symptoms of a latent defect in the older child. Unexplained mental retardation, developmental delay, convulsions, an odor to the body or urine, or episodes of vomiting may be subtle signs of a metabolic dysfunction. Phenylketonuria (PKU), galactosemia, and maple syrup urine disease are discussed in Chapter 14. Cystic fibrosis is discussed in Chapter 25.
Radiographic studies to determine bone age are valuable diagnostic tools. Serum electrolytes and glucose, hormonal, and calcium level tests may be required. PKU testing of newborns is an important screening device for identifying an enzyme deficiency. Chromosomal studies and tissue biopsy are other diagnostic tools. Sexual maturation and skin texture, pigment, and temperature may be indicators of specific disorders. Thyroid function tests may be required. Ultrasonography is helpful in determining the size and character of adrenal glands, ovaries, and other organs. A 24-hour urine specimen may reveal important data. Genetic counseling can help prevent some disorders. Most endocrine dysfunctions involve chronic problems and call for long-term nursing management. The nurse must assess the effect on growth and development, advocate for early detection and intervention, and promote comprehensive follow-up care that will minimize complications.
 Nursing Tip
Nursing TipDisorders and Dysfunction of the Endocrine System
The term inborn errors of metabolism was coined at the turn of the twentieth century by Archibald Garrod. There are literally hundreds of these hereditary biochemical disorders that affect body metabolism. The pattern of inheritance is generally autosomal recessive. These conditions range from mild to severe.
Tay-Sachs Disease
Pathophysiology: Tay-Sachs disease involves a deficiency of hexosaminidase, an enzyme necessary for the metabolism of fats. Lipid deposits accumulate on nerve cells, causing both physical and mental deterioration. This is a disease found primarily in the Ashkenazic Jewish population. It is an autosomal recessive trait carried by 1 in 30 of the Ashkenazic Jewish population, resulting in an occurrence of 1 in 4000 live births.
Manifestations: The infant with Tay-Sachs disease is normal until about age 5 to 6 months, when physical development begins to slow. There may be head lag or an inability to sit. The disease progresses, and when deposits occur on the optic nerve, blindness may result. Mental retardation eventually develops because the brain cells become damaged. Most children with Tay-Sachs disease die before 5 years of age from secondary infection or malnutrition.
Treatment and Nursing Care: There is no treatment for this devastating disease. The nursing care is mainly palliative. Most care is given in the home, with periodic hospitalization for complications such as pneumonia. Chapter 27 discusses the care of the dying child. Carriers can be identified by screening tests in the first trimester of pregnancy. Genetic testing and prenatal counseling have markedly decreased the occurrence of Tay-Sachs disease.
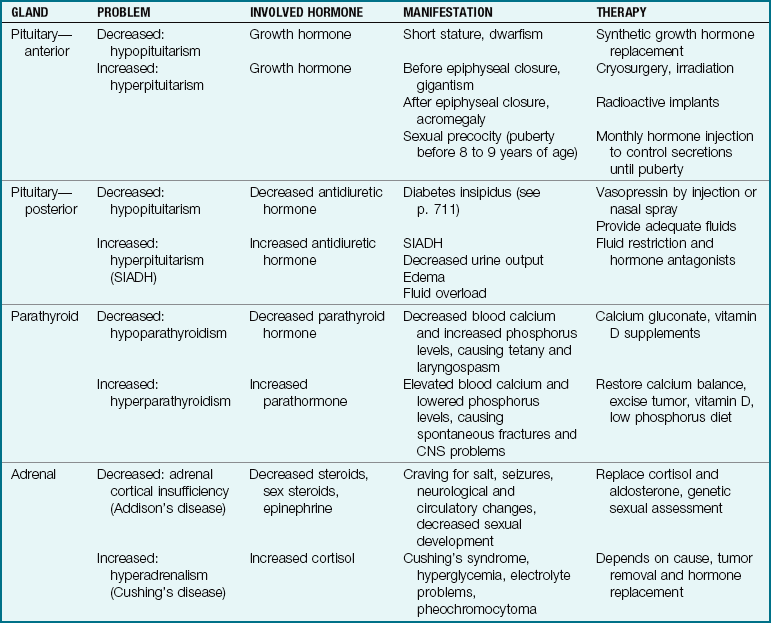
Endocrine Disorders
Pathophysiology: Hypothyroidism occurs when there is a deficiency in the secretions of the thyroid gland. It may be congenital or acquired. It is one of the more common disorders of the endocrine system in children. The thyroid gland controls the rate of metabolism in the body by producing thyroxine (T4) and triiodothyronine (T3). In congenital hypothyroidism the gland is absent or not functioning. The symptoms of hypothyroidism may not be apparent for several months.
Juvenile hypothyroidism is acquired by the older child. It may be caused by a number of conditions, the most common being lymphocytic thyroiditis. Often it appears during periods of rapid growth. Infectious disease, irradiation for cancer, certain medications containing iodine, and lack of dietary iodine (uncommon in the United States) may predispose the child. The symptoms, diagnosis, and treatment are similar to those for congenital hypothyroidism. Because brain growth is nearly complete by 2 to 3 years of age, mental retardation and neurological complications are not seen in the older child.
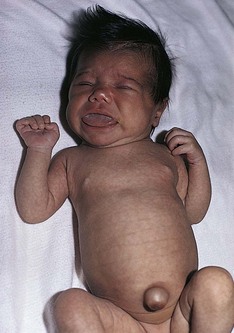
Manifestations: The infant with hypothyroidism is very sluggish and sleeps a lot. The tongue becomes enlarged, causing noisy respiration (Figure 31-2). The skin is dry, there is no perspiration, and the hands and feet are cold. The infant feels floppy when handled. This hypotonia also affects the intestinal tract, causing chronic constipation. The hair eventually becomes dry and brittle. If hypothyroidism is left untreated, irreversible mental retardation and physical disabilities result.
Treatment and Nursing Care: Early recognition and diagnosis are essential to prevent the developing sequelae. A screening test for hypothyroidism is mandatory in the United States and is performed at birth. This is generally part of an overall screen for other metabolic defects. Treatment involves the administration of the synthetic hormone sodium levothyroxine (Synthroid, Levothroid). Hormone levels are monitored regularly. Therapy reverses the symptoms and prevents further mental retardation but does not reverse existing retardation; therefore early detection of congenital hypothyroidism is very important.
The medication is taken at the same time each day, preferably in the morning. Parents are cautioned not to interchange brands. Children may experience reversible hair loss, insomnia, and aggressiveness, and their schoolwork may decline during the first few months of therapy. This is temporary. It may take 1 to 3 weeks for the medication to reach the full therapeutic effect. Medication is not to be discontinued because hormone replacement for hypothyroidism is lifelong. Parents should be taught the signs and symptoms of overdose, which include rapid pulse rate, dyspnea, irritability, weight loss, and sweating. Signs of inadequate dosage or noncompliance are fatigue, sleepiness, and constipation. Parents are instructed about these issues and are advised to consult their physician before giving other medications.
Common Metabolic Dysfunctions
Other common metabolic dysfunctions, their manifestations, and their treatment are discussed in Table 31-1.
Diabetes Insipidus
Pathophysiology: Diabetes insipidus can be hereditary (autosomal dominant) or acquired as the result of a head injury or tumor. It is the consequence of posterior pituitary hypofunction that results in a decreased secretion of vasopressin, the antidiuretic hormone. A lack of antidiuretic hormone results in uncontrolled diuresis. The kidney does not concentrate the urine during dehydration episodes.
Manifestations: Polydipsia and polyuria are the initial signs. The infant cries and prefers water to milk formula. Loss of weight, growth failure, and dehydration occur rapidly. As the child grows older, enuresis may be a problem. Excessive thirst and the search for water overshadow the desire to play, explore, eat, learn, or sleep. Perspiration is deficient, and the skin is dry.
Treatment and Nursing Care: Treatment involves hormone replacement of vasopressin in the form of desmopressin by subcutaneous injection or DDAVP (desmopressin acetate) nasal spray. Parents should be taught to monitor for signs of overdose, which include symptoms of water intoxication (edema, lethargy, nausea, central nervous system signs). Children with diabetes insipidus who are admitted to the hospital in an unconscious state and are unable to express thirst are at great risk. A medical identification bracelet should be worn. School personnel should be advised of the child’s needs. School protocol often limits children’s access to bathrooms and water fountains, even during or after physical activity. Such restrictions could be life threatening to a child with diabetes insipidus. The child’s nurse should contact the school nurse and physical education instructors and educate parents concerning the child’s needs and the lifelong administration of the medication. Home care instructions should include recognizing the signs of water intoxication and dehydration.
Diabetes Mellitus
Pathophysiology: Diabetes mellitus (DM) is a chronic metabolic syndrome (group of symptoms) in which the body is unable to use carbohydrates properly, leading to an impairment of glucose transport (sugar cannot pass into the cells). The body is also unable to store and use fats properly. There is a decrease in protein synthesis. When the blood glucose level becomes dangerously high, glucose spills into the urine, and diuresis occurs. Incomplete fat metabolism produces ketone bodies that accumulate in the blood. This is termed ketonemia and is a serious complication. DM affects the physical and psychological growth and development of children because it requires lifestyle alterations (diet, glucose monitoring, and insulin administration). There are also many long-term complications related to hyperglycemia that result in blindness, circulatory problems, kidney disease, and neuropathy that loom in the future for these children. Treatment is designed to optimize growth and development and to minimize complications.
Classification: To help eliminate confusion in terminology, the National Institutes of Health appointed an international committee, the National Diabetes Data Group, to classify the carbohydrate intolerance syndromes (Mayfield, 1998). Further refinements in classification will be necessary as more is learned about diabetes (Table 31-2). The following classifications are pertinent to this discussion of pediatric diabetes mellitus:
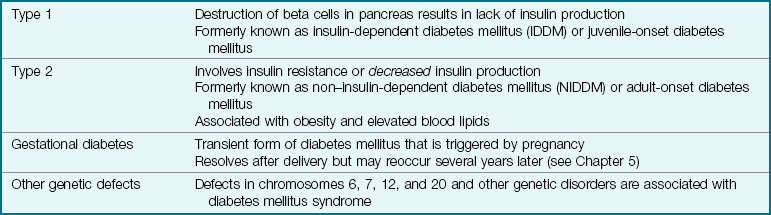
• Type 1, formerly known as insulin-dependent diabetes mellitus (IDDM) and juvenile-onset diabetes mellitus: Type 1 DM is an autoimmune condition that occurs when a child with a genetic predisposition is exposed to an environmental factor such as a viral infection that triggers the syndrome by causing destruction of beta cells in the pancreas and resulting in insufficient insulin production. In some cases, the beta cell destruction may be caused by drugs, chemicals, and ionizing radiation (Kliegman et al., 2007).
• Type 2, formerly known as non–insulin-dependent diabetes mellitus (NIDDM) or adult-onset DM or maturity-onset DM: Type 2 DM involves a resistance to insulin. It is often aggravated by a sedentary lifestyle and obesity. It also occurs more frequently in certain ethnic groups, such as African American and Pacific Islanders, especially those who have hypertension and elevated blood lipid levels. Acanthosis nigricans (a dark pigmentation in the flexor creases of the skin) may be a cutaneous marker for patients with type 2 DM. Table 31-3 lists the clinical features of types 1 and 2 DM. Lifestyle intervention is the cornerstone of preventing or delaying the onset of type 2 diabetes mellitus in susceptible individuals. The accepted criterion for diagnosing diabetes mellitus is a fasting blood glucose level of 126 mg/dL or higher (Kliegman et al., 2007).
Table 31-3
Clinical Features of Type 1 and Type 2 Diabetes
| FEATURE | TYPE 1 | TYPE 2 |
| Onset | Abrupt; patient can often state week of onset | Insidious; often found by screening tests |
| Body size | Normal or thin | Often obese |
| Blood glucose level | Fluctuates widely with exercise and infection | Fluctuations are less marked |
| Ketoacidosis | Common | Infrequent |
| Sulfonylurea responsiveness | Rare | >50% |
| Insulin required | Almost all | <25% |
| Insulin dosage | Increases until glucose control is stable | May remain stable |
• Gestational diabetes mellitus (GDM) is the appearance of symptoms for the first time during pregnancy (see Chapter 5).
Incidence: Approximately 12 million Americans have diabetes mellitus. In the United States, the annual incidence is about 1 newly diagnosed case of type 1 DM per 500 children (Kliegman et al., 2007). The frequency is increasing. Symptoms of type 1 DM may occur at any time in childhood, but the rate of occurrence of new cases is highest among 5- and 7-year-old children and pubescent children 11 to 13 years of age. In the former group, the stress of school and the increased exposure to infectious diseases may be the precipitating event that triggers the onset.
During puberty, rapid growth, increased emotional stress, and insulin antagonism of sex hormones may be implicated as contributing to development of diabetes. DM occurs in both sexes with equal frequency. The disease is more difficult to manage in childhood because the patients are growing, expend a great deal of energy, have varying nutritional needs, and face a lifetime of diabetic management. Young children with type 1 often do not demonstrate the typical “textbook” picture of the disorder. The initial diagnosis may be determined when the child develops ketoacidosis. Therefore the nurse must be particularly astute in subjective and objective observations.
Manifestations: Children with diabetes mellitus present a classic triad of symptoms: polydipsia, polyuria, and polyphagia. The symptoms appear more rapidly in children. The patient complains of excessive thirst (polydipsia), excretes large amounts of urine frequently (polyuria), and is constantly hungry (polyphagia). An insidious onset with lethargy, weakness, and weight loss is also common. The child who is toilet trained may begin wetting the bed or have frequent “accidents” during play periods, may lose weight, and is irritable. The skin becomes dry. Vaginal yeast infections may be seen in the adolescent girl. There may be a history of recurrent infections. The symptoms may remain unrecognized until an infection becomes apparent or coma results. Laboratory findings indicate glucose in the urine (glycosuria). Hyperglycemia (hyper, “above,” gly, “sugar,” and emia, “blood”) is also apparent. Hyperglycemia occurs because glucose cannot enter the cells without the help of insulin, and therefore glucose remains in the bloodstream. The cells use protein and fat for energy; therefore protein stores in the body are depleted. The lack of glucose in the cells triggers the body to develop polyphagia and the increase in glucose intake further increases glucose levels in the blood. Hyperglycemia is the cause of the many complications associated with uncontrolled diabetes mellitus.
The honeymoon period: When type 1 is initially diagnosed and the child is stabilized by insulin dosage, the condition may appear to improve. Insulin requirements decrease and the child feels well. This phenomenon supports the parent’s phase of “denial” in accepting the long-term diagnosis of DM for their child. The “honeymoon period” lasts a short time (a few months), and parents must be encouraged to closely monitor blood glucose levels to prevent complications.
Blood glucose: A random blood glucose level may be obtained at any time and requires no preparation of the patient. The results should be within the normal limits for both nondiabetic patients and diabetic patients who have good control of their disease.
Fasting blood glucose: A fasting blood glucose level is a standard and reliable test for diabetes. The blood glucose level is measured in the fasting patient, usually immediately upon awakening in the morning. The results of the test will not be accurate if the patient is receiving a dextrose intravenous solution. If the child is known to have diabetes, food and insulin are withheld until after the test. If a person’s fasting blood glucose level is greater than 126 mg/dL on two separate occasions and the history is positive, the patient is considered to have diabetes mellitus and requires treatment.
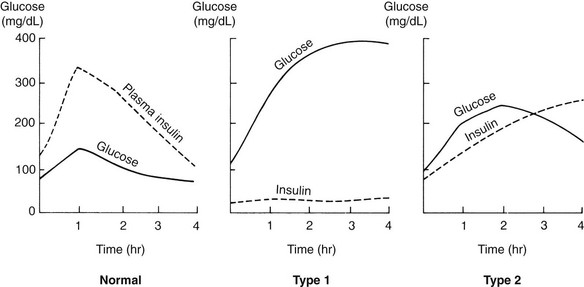
Glucose tolerance test: Another test to determine the amount of glucose in the blood is the glucose tolerance test (GTT). The results are plotted on a graph (Figure 31-3). This procedure is time-consuming, and therefore is no longer in routine use since the glycosylated hemoglobin test is fast and accurate and reveals longer-term elevation of glucose levels. A blood glucose concentration greater than 200 mg/dL is considered positive. Normal values may not return for more than 3 hours.
Glycosylated hemoglobin test: The glycosylated hemoglobin test (HgbA1c) reflects glycemic levels over a period of months. Values are found to be elevated in virtually all children with newly diagnosed diabetes. This study also helps to confirm the results of blood and urine tests done either at home or by the physician. Glucose in the bloodstream constantly enters red blood cells and links with, or glycosylates, molecules of hemoglobin. The more glucose in the blood, the more hemoglobin becomes coated with glucose. The red blood cells carry this glucose until they are replaced by cells with fresh hemoglobin. This process takes about 3 to 4 months. Values vary according to the measurement used. Values of 6% to 9% represent very good metabolic control. Values above 12% indicate poor control.
The future of testing: The Human Genome Project has identified the genes responsible for many diseases. Because DM is considered an autoimmune response, it is possible to predict the occurrence risk of DM by use of genetic, immunological, and metabolic markers. Research is ongoing concerning the screening techniques and preventive immunotherapy. C-peptide (connecting chains of insulin peptides) may also be measured to determine how much insulin the body is producing (endogenous). This is of particular value during the honeymoon period of the disease.
Diabetic Ketoacidosis: Diabetic ketoacidosis (DKA) is also referred to as diabetic coma, although a person may have DKA with or without being in a coma. It may result if a patient with diabetes contracts a secondary infection and does not follow proper self-care. It may also occur if the disease proceeds unrecognized; this happens fairly often in children with diabetes. Even minor infections, such as a cold, increase the body’s metabolic rate and thereby change the body’s demand for insulin and the severity of diabetes. Ketoacidosis is the end result of the effects of insulin deficiency.
Symptoms of ketoacidosis are compared with those of hypoglycemia in Table 31-4; signs and symptoms include a fruity odor to the breath, nausea, decreased level of consciousness and dehydration. Lab values include ketonuria, decreased serum bicarbonate concentration (decreased CO2 levels) and low pH, and hypertonic dehydration. Diabetic teaching should include this information. The symptoms range from mild to severe and occur within hours to days.
Treatment and Nursing Care: The three goals of treatment in type 1 diabetes mellitus are the following:
1. Ensure normal growth and development through metabolic control.
2. Enable the child to cope with a chronic illness, have a happy and active childhood, and be well integrated into the family.
Complications can be minimized by maintaining the blood glucose at consistently normal levels. Teaching ideally begins when the diagnosis is confirmed. A planned educational program is necessary to provide a consistent body of information, which can then be individualized. The patient’s age and financial, educational, cultural, and religious background must be considered. Many hospitals hold group clinics for diabetic patients and their relatives. These sessions are conducted by the multidisciplinary health care team and include the diabetes nurse educator, dietitian, and pharmacist. Patients who are living with the disease provide encouragement and help by sharing concerns. Health professionals become directly involved with the patient’s progress and can offer necessary feedback and support. Continuous follow-up is essential.
Because children with diabetes are growing, additional dimensions of the disorder and its treatment become evident. Growth is not steady but occurs in spurts and plateaus that affect treatment. Infants and toddlers may have hydration problems, especially during illness. Preschool children have irregular activity and eating patterns. School-age children may grieve over the diagnosis and ask, “Why me?” They may use their illness to gain attention or to avoid responsibilities. The onset of puberty may require insulin adjustments as a result of growth and the antagonistic effect of the sex hormones on insulin. Adolescents often resent this condition, which deviates from their concept of the “body ideal.” They have more difficulty in resolving their conflict between dependence and independence. This may lead to rebellion against parents and treatment regimens.
The impact of the disease on the rest of the family must also be considered. Parents may feel guilty for having passed on the disease. Siblings may feel jealous of the attention the patient receives. The sharing of responsibility by parents is ideal but not necessarily a reality. Some may have difficulty accepting the diagnosis and the more regimented lifestyle it imposes. Family members must cope with their individual reactions to the stress of the illness.
Children must assume responsibility for their own care gradually and with a minimum of pressure. Overprotection can be as detrimental as neglect. Parents who have received satisfaction from their child’s dependence on them may need help “letting go.” The diabetic camp experience is helpful in this respect. A medical identification bracelet should be worn.
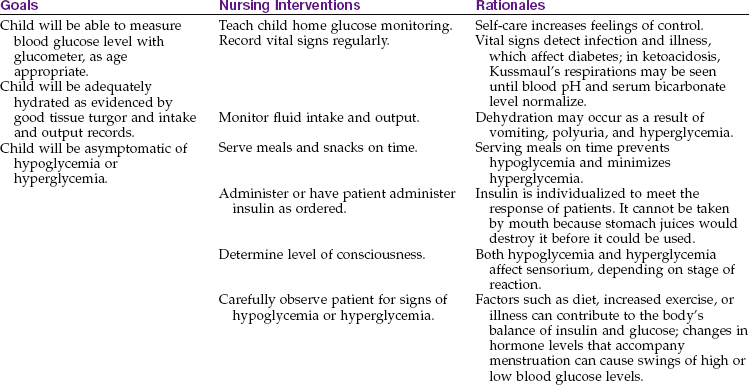
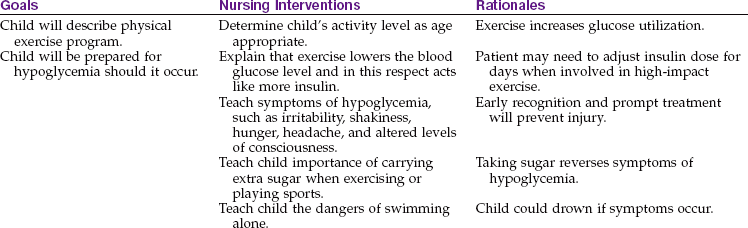
The nursing management of childhood diabetes requires knowledge of growth and development, pathophysiology, blood glucose self-monitoring, nutritional management, insulin management, insulin shock, exercise, skin and foot care, infections, effects of emotional upsets, and long-term care. Nursing Care Plan 31-1 lists interventions for the child with diabetes.
31-1  Nursing Care Plan
Nursing Care Plan
The Child with Diabetes Mellitus
A 10-year-old boy is admitted with new-onset diabetes mellitus. An insulin regimen is prescribed. The child states that he wishes to return to a normal life with his peers.
Deficient knowledge related to identification

1. A child comes to the clinic for follow-up after discharge from the hospital with a diagnosis of diabetic ketoacidosis. He states he is excited about returning to school and rejoining his cross-country team with his friends. His father states he wants his son to stay home and do more sedentary activities to prevent any more health problems. What is the best response of the nurse?
Teaching Plan for Children with Diabetes Mellitus: The patient and family are instructed about the location of the pancreas and its normal function. The nurse explains the relationship of insulin to the pancreas, differentiating between type 1 and type 2 diabetes. All information is given gradually and at the level of understanding of the child and family. Audiovisual aids and pamphlets are incorporated into the session. If the patient is newly diagnosed, hospitalization offers opportunities for instruction.
Blood Glucose Self-Monitoring: Patients can test their own blood glucose level in the home. While still being supervised by and consulting with the physician, the patient can make rational changes in insulin dosage (sliding scale dosage) based on home blood glucose tests, nutritional requirements, and daily exercise. This is of great psychological value to the child, adolescent, and parents because it reduces feelings of helplessness and complete dependence on medical personnel. Home glucose monitoring should be taught to all young patients and their caregivers. The patient not only must be skilled in the techniques but also should understand the results and how to incorporate them into daily regimens. This means involving the entire health care team in ongoing supervision, demonstrations, and support. Although instructions are included with the various products, patients need individual training.
Glucometer systems provide readouts and automatically store data by time and date. Some also keep track of diet and the amount of exercise for the day. They can be connected to a computer or computer printer for review. Records can be transmitted electronically to the physician.
Obtaining blood specimens before meals and at bedtime has been simplified by the use of capillary blood-letting devices such as the Glucolet. This device automatically controls the depth of penetration of the lancet into the skin. Other brands include Hamalet, Autoclix, Monoject, Autolet, and Accu-Chek. The sides of the fingertips are recommended testing sites because there are fewer nerve endings and more capillary beds in these areas. The best fingers to use are the middle, ring, or little fingers on either hand. The finger will bleed more easily if the child washes the hands in warm water for about 30 seconds. To perform the test, a drop of blood is put on a chemically treated reagent strip. The test strip with a drop of blood is inserted into the glucometer, and the blood glucose reading appears.
Noninvasive devices to assess blood glucose levels also have been developed. One system is worn on the wrist like a watch and uses infrared technology to provide noninvasive glucose monitoring. This system is not yet approved by the U.S. Food and Drug Administration (FDA); however the FDA has approved the “At Last” glucose monitor (Amira) that has a lancet built in and takes a sample from the forearm or the thigh. It is less painful than the fingertip devices.
The methods of glucose monitoring provide different information. The fingerstick method of glucose monitoring reveals the glucose level at a moment in time. The HgbA1c value reveals a history of several weeks’ pattern of glucose control. Continuous glucose monitoring measures levels within the interstitial tissues and reveals trends in glucose levels but does not completely replaced glucometers (Keefe, 2008).
Cost, convenience, and portability are factors to consider when selecting glucometers. Most products can be obtained at the local pharmacy. Newer and more precise instruments are being developed constantly. Frequency of use is determined by the amount of diabetes control required by the particular child.
Continuous Glucose Monitoring: The continuous glucose monitor is not intended for day-to-day, long-term monitoring of glucose levels. It consists of a sensor placed subcutaneously in the abdomen that transmits blood glucose levels every 10 to 60 seconds to a monitor worn on the clothing of the patient. This technique helps identify fluctuation and trends that cannot be picked up by the standard HgbA1c test or intermittent fingerstick measurements. The continuous glucose monitoring system is used to devise an individualized treatment plan for the patient. In 2008, the FDA approved the Freestyle Navigator Continuous Glucose Monitoring System produced by Abbott Diabetes Care.
Diet Therapy for Children with Diabetes Mellitus:
Nutrition management: The triad of diabetes management consists of a well-balanced diet, precise insulin administration, and regular exercise. The importance of glycemic control in decreasing the incidence of symptoms and complications of the disease has been established. The advent of blood glucose self-monitoring is affecting food intake in that diets can be fine-tuned and more flexible while the cornerstone of consistency (in amount of food and time of feeding) is maintained. Contrary to popular belief, there is no scientific evidence that persons with diabetes require special foods. In fact, if it is good for the diabetic patient, it is good for the entire family. The nutritional needs of diabetic children are essentially no different from those of nondiabetic children. The timing of food consumption has to be correlated with the time and action of the type of insulin prescribed so that blood glucose levels will not be abnormally high or abnormally low.
The goals of nutritional management in children are to ensure normal growth and development, to distribute food intake so that it aids metabolic control, and to individualize the diet in accordance with the child’s ethnic background, age, sex, weight, activity, family economics, and food preferences. Total estimated caloric intake is based upon body size or surface area and can be obtained in standard tables. The recommended intake is 55% carbohydrates (mostly complex carbohydrates), 30% fat, and 15% protein (Kliegman et al., 2007). Most of the carbohydrate intake should consist of complex carbohydrates that absorb slowly and do not cause sudden and wide elevation of blood glucose level. The various types of insulin allow flexibility in diet intake and improve the quality of life. There are many “sugar free” products on the market, but sorbitol and xylitol should not be used as artificial sweeteners because they may contribute to diabetic complications (Kliegman et al., 2007). Dietary fat from animal sources should be limited and replaced with polyunsaturated fats found in vegetables. Occasional excesses for birthdays or special occasions can be accommodated to prevent rebellion and to promote compliance. Special supplements may be required to accommodate the exercise patterns and growth needs of children. Once a diet prescription is received from the physician, the dietitian assists the family in designing an individualized diet plan. The dietitian also explains the use of exchange lists.
Education of the patient is ongoing. Too much information given at one time may overwhelm the parents and discourage the child. Well-informed nurses can offer much reinforcement and support. They can clarify terms such as dietetic, sugar free, juice-packed, water-packed, and unsweetened. Meal trays in the hospital provide an excellent opportunity for teaching. Children should bring their lunch to school. Respecting cultural patterns and personal preferences is important. The content of foods commonly found in fast-food chain restaurants is available through the American Diabetes Association.
The importance of fiber in diets is well documented. In the diabetic patient, soluble fiber has been shown to reduce blood glucose levels, lower serum cholesterol values, and sometimes reduce insulin requirements. Fiber appears to slow the rate of absorption of sugar by the digestive tract. Raw fruits and vegetables, bran cereals, wheat germ, beans, peas, and lentils are good sources of soluble fiber.
 Safety Alert!
Safety Alert!
Instruct the patient and family to read food labels carefully. The word dietetic does not mean diabetic. Dietetic merely means something has been changed or replaced; for example, the food may contain less salt or less sugar.
Glycemic index of foods and cholesterol intake: The glycemic index for selected foods has an impact on the manipulation of dietary needs (Table 31-5). Because persons with diabetes have an increased risk for atherosclerosis, the reduction of serum cholesterol level is another concern. Most of the general public need to reduce their intake of animal fats. This is accomplished by consuming less beef and pork and more chicken, turkey, fish, low-fat milk (depending on the age of the patient), and vegetable proteins. The form of food is also significant. An apple, apple juice, and applesauce may precipitate different blood glucose responses. The size of portions, the type of processing or cooking, and the combinations of foods have also been shown to have a bearing on these responses.
Table 31-5
Glycemic Index of Selected Foods
| FOOD | GLYCEMIC INDEX* |
| All-Bran cereal | 60 |
| Apple | 52 |
| Baked potato | 121 |
| Banana | 76 |
| Carrots | 101 |
| Cheerios | 106 |
| Cherries | 32 |
| Corn flakes | 119 |
| Fettuccini | 46 |
| French baguette bread | 136 |
| Grapes | 62 |
| Green peas | 68 |
| Instant noodles | 67 |
| Jelly beans | 114 |
| Lifesavers candy | 100 |
| Low-fat yogurt (artificially sweetened) | 20 |
| Oatmeal | 87 |
| Orange | 62 |
| Peach | 40 |
| Peanuts | 21 |
| Pretzels | 116 |
| Rice | 78 |
| Rice cakes | 117 |
| Skim milk | 76 |
| Spaghetti | 59 |
| Tomato soup | 54 |
| Watermelon | 103 |
| White bread | 100 |
*Foods with a low glycemic index take longer a longer time to increase the glucose levels in the blood.
Data from Mahan, L., & Escott-Stump, S. (2008). Krause’s food, nutrition and diet therapy (12th ed.). Philadelphia: Saunders.
Insulin management: Insulin is used principally as a specific drug for the control of DM. When injected into the diabetic patient, it enables the body to burn and store sugar. Current data emphasize the importance of blood glucose control in the prevention of microvascular disease.
The dose of insulin is measured in units, and special syringes are used in its administration. U-100 (100-unit) insulin is the standard form. All vials of U-100 insulin have color-coded caps, and all labels bear black printing on a white background.
It is important to teach the parents and child about the administration of insulin. Insulin cannot be taken orally because it is a protein and would be broken down by the gastric juices. The usual method of administration is subcutaneous injection (Figure 31-4). When injected at a 90-degree angle, the short needle enters the subcutaneous space. This technique may be easier for the child to learn because it takes less coordination to administer than a 45-degree-angle technique. The insulin pump offers continuous subcutaneous insulin infusion without the need for frequent injections. A small, pager-size, battery-powered, programmable pump holds a syringe of insulin (Figure 31-5). A catheter attaches to a needle that is inserted into the subcutaneous tissue and secured with transparent tape. In general, a child can be taught to perform self-injection after 7 years of age (Figure 31-6). The physician prescribes the type and amount of insulin and specifies the time of administration.
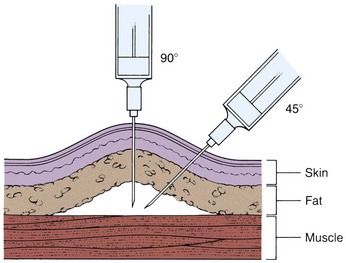
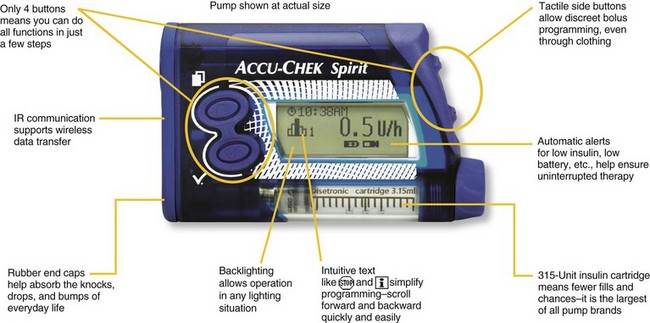
FIGURE 31-5 The Accu-Chek insulin pump. This is a type of subcutaneous insulin infusion system that eliminates the need for frequent injections. A small, battery-powered pump holds a 315-unit cartridge of insulin that requires fewer refills. A catheter attaches to a needle that is inserted into the subcutaneous tissue and secured with transparent tape. This unit allows discreet bolus programming, even through clothing, with sensitive buttons on the side. It has automatic alerts for low insulin or low battery and is available with wireless data transfer.
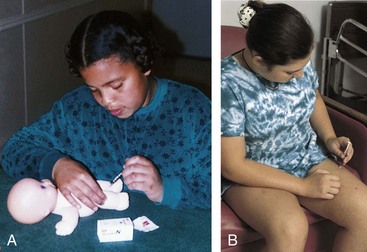
FIGURE 31-6 A, By giving injections to dolls or puppets, children can be prepared for this procedure and may be less frightened by it. B, A child 7 years of age or older can take the responsibility for self-injection with proper supervision. (A courtesy Pat Spier, RN-C.)
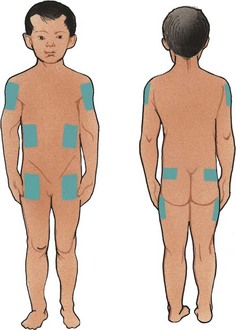
The site of the injection is rotated to prevent poor absorption and injury to tissues (Figure 31-7). Injection model forms made from construction paper and site rotation patterns are useful. One suggested site rotation pattern is to use one area for 1 week. A different site within that area is used for each injection. Injections should be about 1 inch apart. The young child can use a doll to practice self-injection.
Insulin should not be injected into an area that has a temporarily increased circulation. In such areas, a more rapid than expected absorption and effect can trigger hypoglycemia. For example, a more rapid circulation to the legs can be expected in a child who is riding a tricycle; therefore the thigh should not be selected as a site for injection. If a teen returns from playing tennis, the upper arm is avoided as an injection site.
Lipoatrophy (lipo, “fat,” and atrophy, “loss of”) and lipohypertrophy (lipo, “fat,” and hypertrophy, “increase of”) refer to changes that can occur in the subcutaneous tissue at the injection site. Proper rotation of sites and the availability of the newer purified insulins have helped to eliminate this condition. The child is taught to “feel for lumps” every week and to avoid using any sites that are suspicious.
The various types of insulin and their action are listed in Table 31-6. The main differences between insulins are the amount of time required for the insulin to take effect and the duration of the protection provided. The values listed in the table are only guidelines. The response of each diabetic child to any given insulin dose is highly individual and depends on many factors, such as site of injection, local destruction of insulin by tissue enzymes, and insulin antibodies.
Table 31-6
Types of Insulin*
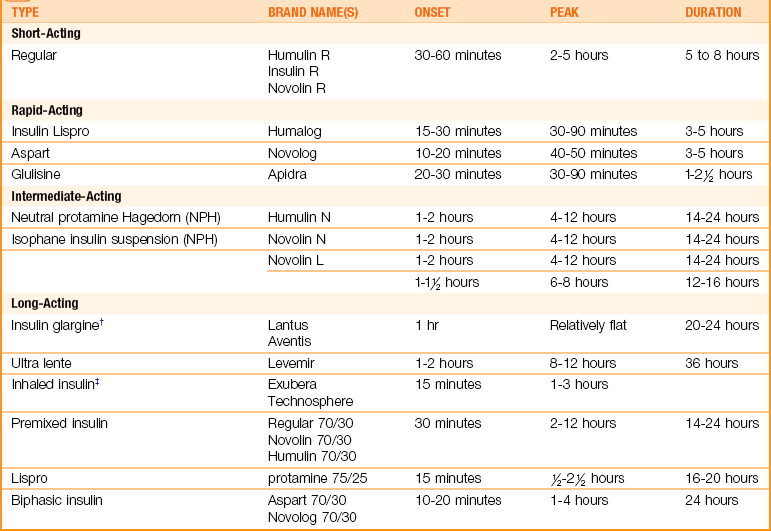
*There are many combined mixtures of insulin available commercially. Data from Schooff, M., & Ehlers, K. (2005). Cochrane for Physicians: Short acting analogs versus human insulin for diabetes. American Family Physician, 72(5), 805-906; Physician’s Desk Reference (64th ed.). (2010). Montvale, NJ: Thomson; Lewis, S., Heitkemper, M., Dirksen, S., O’Brien, G., & Bucher, L. (2007). Medical-surgical nursing (7th ed.). St. Louis: Elsevier; Fluero-Milfort. (2008). Insulin replacement treatment. Advance for Nurse Practitioners 11(16), 36-39; www.fda.gov/cdrh/devadvice/default.htm.
†Do not mix with other insulins.
‡Approved by U.S. Food and Drug Administration (FDA); awaiting continued research.
Human insulin manufactured by biosynthesis is the treatment of choice. It is available in rapid-acting, short-acting, intermediate-acting, and long-acting preparations. Extreme temperatures (below [2.2° C, or 36° F] or above [29.4° C, or 85° F]) can destroy insulin. Insulin potency can be decreased if the bottle has been opened longer than 1 month.
The physician often orders a combination of short-acting and intermediate-acting insulin; for example, “Give 10 units of NPH insulin and 5 units of regular insulin at 7:30 am.” This offers the patient immediate and longer-lasting protection. NPH insulin may be given in the same syringe as regular or crystalline insulin (Figure 31-8). Long-acting types of insulin are seldom given to children because of the danger of hypoglycemia during sleep. Stable, premixed insulins are available. Insulin “pens” and injectors for insulin are available alternatives for the traditional syringe technique of administering insulin.
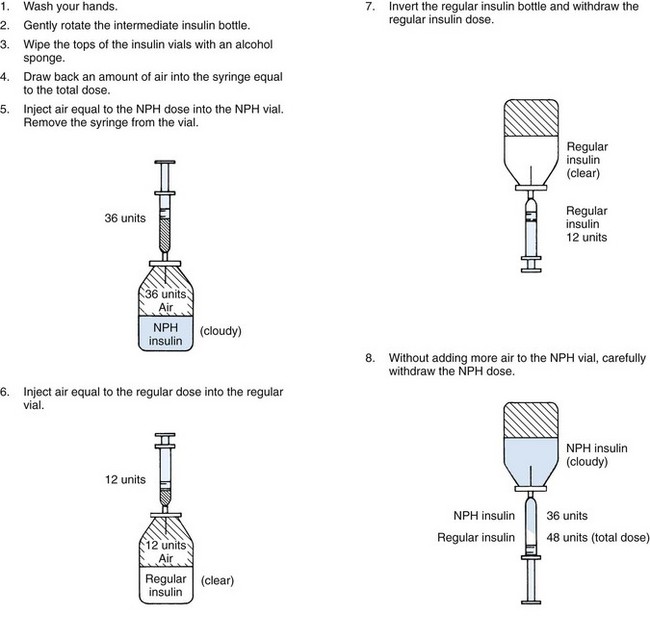
FIGURE 31-8 Mixing insulin. This step-order process avoids the problem of contaminating the regular insulin with the intermediate-acting insulin. If contamination of the regular insulin does occur, the rapid-acting effect of this drug is diminished, and it is unreliable as a quick-acting insulin in an acute situation such as diabetic ketoacidosis.
Medication Safety Alert!
When mixing insulin, always withdraw the regular insulin first and then add the long-acting insulin into the syringe.
Insulin pump: The insulin pump provides continuous subcutaneous infusion of insulin via battery-powered pump, which is worn on a belt or shoulder strap. The pump provides more even insulin release, controlled by a computerized monitor. The subcutaneous site is usually the abdomen, and the tubing is changed by the parents every 48 hours using aseptic technique. The pump should not be removed for more than 1 to 2 hours at a time, and water-safe models can be used if swimming or bathing. The pumps are equipped with alarms in case of malfunction.
Inhaled or oral insulin: Inhaled insulin has been under study and appears effective. Continued FDA study is needed to determine long-term effects on the lung tissue before it is released for general use. Oral insulin (Oralin) is currently under study but not yet available for general use (Kliegman et al., 2007). An insulin patch is under development but not yet fully approved by the FDA.
Insulin shock: Insulin shock, also known as hypoglycemia (hypo, “below,” glyco, “sugar,” and emia, “blood”), occurs when the blood glucose level becomes abnormally low. This condition is caused by too much insulin. Factors that may account for this imbalance include poorly planned exercise, reduced diet, and errors made because of improper knowledge of insulin and the insulin syringe.
Children are more prone to insulin reactions than adults because of the following:
Poorly planned exercise is often the cause of insulin shock during childhood. Hospitalized patients who are being regulated must be observed frequently during naptime and at night. The nurse becomes suspicious of problems if unable to arouse the patient or if the child is perspiring heavily.
The symptoms of an insulin reaction, which range from mild to severe, are generally noticed and treated in the early stages. They appear suddenly in the otherwise well person. Examination of the blood would reveal a lowered blood glucose level. The child becomes irritable, may behave poorly, is pale, and may complain of feeling hungry and weak. Sweating occurs. Symptoms related to disorders of the nervous system arise because glucose is vital to the proper functioning of nerves. The child may become mentally confused and giddy, and muscular coordination is affected. If insulin shock is left untreated, coma and convulsions can occur.
The immediate treatment consists of administering sugar in some form, such as orange juice, hard candy, or a commercial product. The patient begins to feel better within a few minutes and at that time may eat a small amount of protein or starch (sandwich, milk, cheese) to prevent another reaction. Glucagon is recommended for the treatment of severe hypoglycemia. It quickly restores the child to consciousness in an emergency; the child can then consume some form of sugar or a planned meal.
The Somogyi phenomenon (rebound hyperglycemia) occurs when blood glucose levels are lowered to a point at which the body’s counterregulatory hormones (epinephrine, cortisol, glucagon) are released. Glucose is released from muscle and liver cells, which precipitates a rapid rise in blood glucose levels. It is generally the result of chronic insulin use, especially in patients who require fairly large doses of insulin to regulate their blood glucose levels. Hypoglycemia during the night and high glucose levels in the morning are suggestive of the phenomenon. The child may awaken at night or have frequent nightmares and experience early morning sweating and headaches. The child actually needs less insulin, not more, to rectify the problem.
The Somogyi phenomenon differs from the dawn phenomenon, in which early morning elevations of blood glucose occur without preceding hypoglycemia and may be a response to growth hormone secretion that occurs in the early morning hours. Together the Somogyi and dawn phenomena are the most common causes of instability in diabetic children. Testing blood glucose levels around 3 am helps to differentiate the two conditions and aids in regulating insulin dosage.
Home Management of Children with Diabetes Mellitus:
Exercise: Exercise is important for the patient with diabetes because it causes the body to use sugar and promotes good circulation. It lowers the blood glucose level, and in this respect it acts like more insulin. The diabetic patient who has planned vigorous exercise should carry extra sugar to avoid insulin reactions. The patient should also carry money for candy or a drink and, if possible, a cell phone. The blood glucose level is high immediately after meals, and the child can participate in active sports at such times. Games enjoyed directly before meals should be less active. The diabetic child is able to participate in almost all active sports. Poorly planned exercise, however, can lead to difficulties.
Skin care: The patient is instructed to bathe daily and dry well, especially between the toes. Cleansing of the inguinal area, axillae, perineum, and infra-mammary areas is especially important because yeast and fungal infections tend to occur at these sites. The skin is inspected for cuts, rashes, abrasions, bruises, cysts, or boils. These lesions are managed promptly. If skin is very dry, an oil such as Alpha Keri may be used in the bath water. Adolescents are taught to use electric razors. Exposing the skin to extremes in temperatures is avoided. Injection sites are inspected for lumps.
Foot care: Although circulatory problems of the feet are less common in children, proper habits of foot hygiene must be established. Patients are instructed to wash and dry their feet well each day. The feet are inspected for interdigital cracking, and the condition of the toenails is checked. Nails are trimmed straight across. Socks are changed daily, and tight socks or large ones that bunch up are avoided. Shoes are replaced often as the child grows. The child should not go barefoot.
Infections: Immunizations against communicable diseases are essential (see Chapter 32).
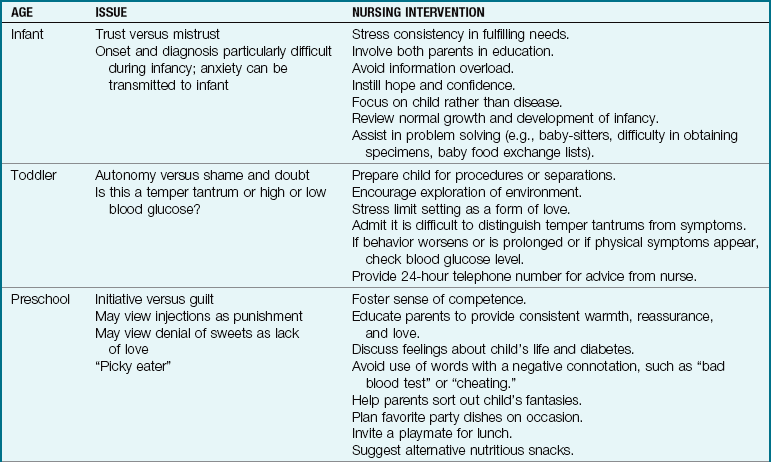
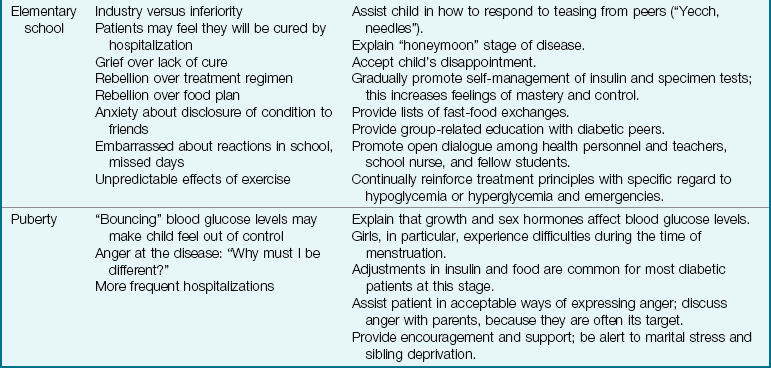
Emotional upsets: Emotional upsets can be as disturbing to the patient as an infection and may necessitate food adjustments, insulin adjustments, or both. Table 31-7 lists nursing interventions for stress on the child and family related to type 1 diabetes.
Urine checks: Routine urine checks for sugar are being replaced by the more accurate glucose blood monitoring. However, this procedure does not test for acetone, which the patient may need to determine, particularly during illness and when the blood glucose level is high. When urine checks are advocated for patients, saying urine “check” rather than “test” is less confusing to young children.
Glucose-insulin imbalances: The patient is taught to recognize the signs of insulin shock and ketoacidosis (see Table 31-4). Early attention to changes and daily record keeping are stressed. Many excellent teaching films and brochures are available. The child should wear a bracelet identifying him or her as having diabetes. Wallet cards are also available. Teachers, athletic coaches, and guidance personnel are informed about the disease and should have the telephone numbers of the patient’s parents and health care provider.
Travel: With planning, children can enjoy travel with their families, and older adolescents can travel alone. Before leaving on a trip, the child should be seen by the physician for a checkup and prescriptions for supplies. A written statement and a card identifying the child as having diabetes should be carried. Time changes may affect meals. Additional supplies of insulin, sugar, and food are kept with the child. These are never checked with luggage, especially on an airplane, because they may be lost. If foreign travel is planned, parents must become familiar with the food in the area so that dietary requirements can be met. Local chapters of the American Diabetes Association or the Juvenile Diabetes Foundation can help vacationing families in an emergency.
Follow-up care: The child must see the physician regularly. The child should also be taught to visit the dentist regularly for cleaning of teeth and gums. Brushing and flossing daily are essential. Eyes should be examined regularly; blurry vision must not be ignored. There are many brochures, books, and journals that offer excellent suggestions and guidance at an age-appropriate level.
Illness or surgery: When illness occurs, close glucose monitoring and control is essential. Hyperglycemia causes diuresis and dehydration, and ketosis can involve vomiting. Counteracting regulatory hormones that are secreted during periods of stress interfere with the effectiveness of insulin, resulting in increased glucose levels. Modification of insulin doses may be necessary. The patient with diabetes usually tolerates surgery well. Insulin may be given before, during, or after the operation. If the patient is restricted to nothing by mouth, calories may be supplied by intravenous glucose. Details vary according to the procedure and the patient’s treatment for diabetes. Careful review of the patient’s history helps in formulating nursing care plans and provides a basis for teaching.
Prospects for the Future: Diabetic research is being conducted on many fronts. Geneticists have determined how diabetes is inherited, and soon they will be able to alter genes or prevent the condition for those at risk. Pancreas transplantation has been performed, and in vitro and in vivo regeneration therapy is under study. The laser beam has aided the treatment for complicated eye conditions. Such advances hold promise for resolving or eradicating the dilemma of diabetes.
 Nutrition Considerations
Nutrition Considerations
Diet Therapy in Pediatric Metabolic Disorders
| Disorder | Major Signs and Symptoms | Dietary Regimen |
| Phenylketonuria (PKU) | Mental retardation | Low phenylalanine diet, Lofenalac formula for infants |
| Celiac disease | Chronic diarrhea, irritability, distention, failure to thrive | Eliminate gluten; use corn flour and vitamin B supplements |
| Cystic fibrosis | Thick mucus causes obstruction of pancreatic enzymes and poor absorption of nutrients, flatulence, and foul-smelling stools | Pancreatic enzyme replacement with normal meals |
| Lactose intolerance | Abdominal distention, cramps, diarrhea, failure to thrive | Lactose-free diet; use ProSobee, soy formulas; avoid milk and milk products |
| Galactose intolerance | Jaundice, vomiting, convulsions, lethargy, blindness | No galactose or lactose in diet; use milk substitutes |
| Fructose intolerance | Vomiting, diarrhea, failure to thrive | Fructose-free diet; avoid honey, fruit, sorbitol, and sucrose; offer vitamin C and vegetables |
| Maple syrup urine disease | Acidosis, convulsions | Low-leucine and low-valine diet |
| Urea cycle defect | Lethargy | Low-protein diet |
| Acidemia | Seizures, elevated ammonia levels | May need to restrict meat proteins |
| Diabetes insipidus | Inability to concentrate urine, diuresis | Unrestricted water intake |
| Diabetes mellitus | Inability to produce insulin to metabolize sugar, protein, and fat | Controlled sugar intake regulated with insulin administration; high-fiber, balanced diet |
Type 2 Diabetes Mellitus: Type 2 diabetes is thought to be caused by insulin resistance and decreased insulin secretion. It is precipitated by obesity, low physical activity, and a lipid-rich diet resulting in insulin resistance. Type 2 diabetes mellitus is becoming more prevalent in children and young adults. Risk factors include the following:
• Family history of type 2 diabetes mellitus
• Acanthosis nigricans (a dark pigmentation of the flexure creases of the skin and back of neck)
• Increased lipids (hyperlipidemia)
• Racial or ethnic history: Native American, African American, Latino, Asian American, or Pacific Islander
• Obesity (body mass index [BMI] over the 85th percentile for age and sex or weight and height or over the 120th percentile for the ideal weight for height)
In children with type 2 diabetes mellitus, diet is the main emphasis of management concomitant with exercise and other weight control measures. Insulin or insulin combined with oral Metformin contributes to a stable control of blood glucose level. The monitoring and general nursing care are similar to those for type 1 diabetes mellitus.
Get Ready for the NCLEX® Examination!
Key Points
• The two major systems that control and monitor the functions of the body are the nervous system and the endocrine system.
• The term inborn error of metabolism refers to a group of inherited biochemical disorders that affect body metabolism.
• Screening programs for early detection of inborn errors are important because some conditions can cause irreversible neurological damage.
• Diabetes mellitus type 1 is the most common endocrine disorder of children. The body is unable to use carbohydrates properly because of a deficiency of insulin, an internal secretion of the pancreas.
• The symptoms of diabetes mellitus appear more rapidly in children. Three symptoms are polydipsia, polyuria, and polyphagia.
• Type 2 diabetes mellitus is caused by insulin resistance. It is precipitated by obesity, a lipid-rich diet and inactivity and is becoming more prevalent in children.
• The mainstays of the management of diabetes mellitus are insulin replacement, diet, and exercise.
• Diabetic ketoacidosis is a serious complication that may become life threatening.
• Self-management to maintain glucose control and to prevent complications is a major goal of education of the child with diabetes mellitus.
• A continuous glucose monitoring system can be programmed to meet individual needs.
• An insulin pump provides subcutaneous doses of insulin controlled by a computerized monitor.
• The glycosylated hemoglobin test (HgbA1c) reflects glucose control over time.
• Sugar substitutes such as sorbitol and xylitol should not be given to children.
• A child with diabetes insipidus requires unlimited access to water.
• Growth hormone is administered at bedtime to simulate the natural time of hormone release.
• A deficiency in the secretions of the thyroid gland is termed hypothyroidism. It may be congenital or acquired and necessitates lifelong treatment by oral administration of a synthetic thyroid hormone.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
 Online Resources
Online Resources• Acanthosis nigricans: www.cdc.gov/diabetes/news/docs/an.htm
• American Diabetes Association: www.diabetes.org
• Diabetes Public Health Resource: www.cdc.gov/diabetes/index.htm
• International Society of Pediatric and Adolescent Diabetes: www.ispad.org/index_html
Review Questions for the NCLEX® Examination
1. What is an important aspect of a teaching plan for the parent of a child with hypopituitarism?
1. The child should be enrolled in a special education program at school.
2. The routine administration of growth hormone should be carried out at bedtime.
3. All family members should have an endocrine workup.
4. The routine medication should be administered before the school day starts.
2. A child who has diabetes mellitus asks why he cannot take insulin orally instead of by subcutaneous injection. The best response of the nurse would be that:
3. What may indicate a need for insulin in a diabetic child?
4. The nurse teaches the diabetic child to rotate sites of insulin injection in order to:
1. prevent subcutaneous deposit of the drug.
2. prevent lipoatrophy of subcutaneous fat.
5. Kussmaul’s respirations are seen in diabetic children with: