Teamwork and Collaboration
The time spent with a patient in any setting is limited. Therefore collaborate with family members, colleagues, and other specialists to achieve the established goals and expected outcomes. Some patients need to improve their exercise and activity tolerance; for other patients continuing care involves participating in a community-based cardiopulmonary rehabilitation program. Finally, some patients need home physical therapy.
Collaboration with physical therapists, nutritionists, and community-based nurses is valuable for patients with heart failure or chronic lung conditions. These professionals work with patients and use resources in the community to assist them in attaining and maintaining the highest possible level of wellness. In addition, professionals identify community resources and support systems for both the patient and family in preventing and managing symptoms related to cardiopulmonary diseases. Communicating among everyone on the patient’s health care team and recognizing everyone’s contributions in achieving the health care goals for the patient are imperative.
 Nursing Care Plan
Nursing Care Plan
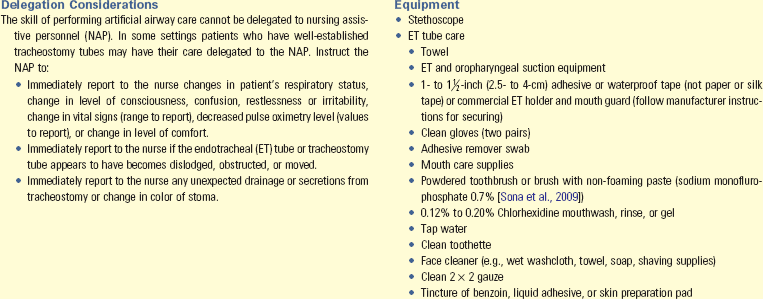
Ineffective Airway Clearance
Mr. Edwards is a 75-year-old Caucasian male who is currently lying in a semi-Fowler’s position in bed talking with his wife. Kathy Allen is a nursing student completing a respiratory assessment. Mr. Edwards has a history of chronic obstructive pulmonary disease for 2 years. He continues to smoke  pack of cigarettes a day and does not participate in any exercise. He does not “see any reason” to increase his fluid intake. His SpO2 ranges from 78% to 84%. He must do his self-care activities slowly because of fatigue. Presently he is admitted for right upper lobe pneumonia. He reports having an intermittent productive cough that occasionally produces thick, yellow sputum. He has more episodes of coughing when lying flat. His vital signs are temperature, 101.4° F (38.5° C); pulse, 102 beats/min; respirations, 30 breaths/min; blood pressure, 130/90 mm Hg; and SpO2, 84%. He has episodes of chilling and diaphoresis. His health care provider has told him that, if he gradually increases his exercise, drinks more fluids, and stops smoking, his respiratory status will improve.
pack of cigarettes a day and does not participate in any exercise. He does not “see any reason” to increase his fluid intake. His SpO2 ranges from 78% to 84%. He must do his self-care activities slowly because of fatigue. Presently he is admitted for right upper lobe pneumonia. He reports having an intermittent productive cough that occasionally produces thick, yellow sputum. He has more episodes of coughing when lying flat. His vital signs are temperature, 101.4° F (38.5° C); pulse, 102 beats/min; respirations, 30 breaths/min; blood pressure, 130/90 mm Hg; and SpO2, 84%. He has episodes of chilling and diaphoresis. His health care provider has told him that, if he gradually increases his exercise, drinks more fluids, and stops smoking, his respiratory status will improve.
| Assessment Activities | Findings/Defining Characteristics* |
| Ask Mr. Edwards how long he has had this cough. | He replies, “I have a morning cough every day, but this cough is different. It started about a week ago. It is worse when I lie flat.” |
| Ask Mr. Edwards what is different about this cough. | He replies, “My ribs are getting sore. It is difficult to cough up anything, my mouth is dry, and I have become more fatigued.” |
| Observe Mr. Edwards’ skin and mucous membranes. | Skin and mucous membranes are dry. |
| Auscultate lung fields. | Abnormal lung sounds (crackles) are heard in lower lobes bilaterally. |
| Ask Mr. Edwards to produce a sputum sample. | Sputum is thick and discolored yellow to yellow-green. |
Ineffective airway clearance related to retained thick pulmonary secretions
| Goals | Expected Outcomes (NOC)† |
| Respiratory Status: Airway Patency | |
| Mr. Edwards will be able to effectively clear secretions by discharge. | Lung sounds will be clear in 48 hours. |
| Mr. Edwards will notice increased ease in coughing within 48 hours. | |
| Sputum will be thin and white within 3 days. | |
| Respiratory rate will be within 12 to 20 breaths/min in 48 hours. | |
| Mr. Edwards will increase oral hydration within 48 hours. | Mr. Edwards will drink 2500 mL of water or preferred liquids every 24 hours starting today. Mr. Edwards will verbalize that his mouth is not dry in 48 hours. |
†Outcome classification labels from Moorhead S et al.: Nursing outcomes classification (NOC), ed 4, St Louis, 2008, Mosby.
| Interventions (NIC)‡ | Rationale |
| Airway Management | |
| Position Mr. Edwards with head elevated 30-45 degrees. | An upright angle allows for thoracic expansion; lying flat allows abdominal organs to push up against the diaphragm, compromising inspiration. This allows for a more normal respiratory rate (Lawrence et al., 2006). |
| Ambulate in room or hall as tolerated at least 2 times a day. If unable to ambulate, reposition from side to side every 2 hours or more. | Body movement helps mobilize secretions (Perme and Chandrashekar, 2009). |
| Have Mr. Edwards deep breathe and cough every 2 hours. Teach him to take a deep breath, hold it for several seconds, open his mouth, tighten his abdominal muscles, and cough 2 to 3 times with his mouth open. | Retained secretions predispose patient to atelectasis and pneumonia. Controlled coughing that uses the diaphragmatic muscles make the cough more effective in removing mucus (AARC, 1993). |
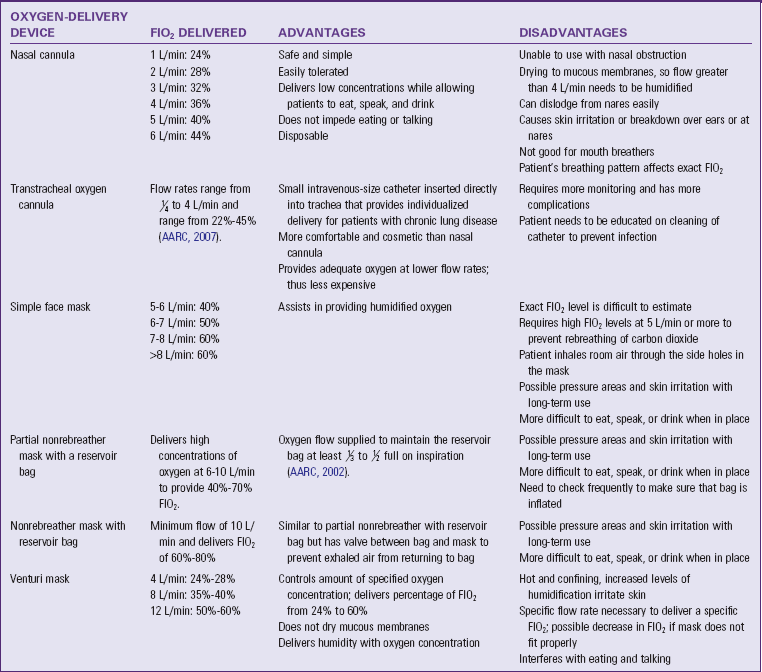
| Administer 2 L/min of oxygen as ordered per nasal cannula if SpO2 less than 90%. | This dependent nursing intervention will relieve hypoxia. |
| Increase fluids to 2500 mL in 24 hours if not contraindicated by cardiac or renal status. Offer fluids Mr. Edwards prefers. |
Fluids help to liquefy secretions and promote ease of removal. Fluids relieve oral mucosa and skin dryness. |
‡Intervention classification labels from Bulechek GM, Butcher HK, and Dochterman JM: Nursing interventions classification (NIC), ed 5, St Louis, 2008, Mosby.
| Nursing Actions | Patient Response/Finding | Achievement of Outcome |
| Auscultate the chest. | Mr. Edwards reports that he has not heard any rattling in his chest. | Lung sounds are normal. |
| Ask Mr. Edwards if he can deep breathe and cough and measure SpO2. | Mr. Edwards reports that it is easier to cough up his secretions. SpO2 is 95%. | Airway clears with coughing. SpO2 is within normal levels. |
| Observe sputum. | Mr. Edwards states, “My sputum is thinner and white now.” | Sputum is thin and white. |
| Monitor respiratory rate. | Mr. Edwards says that it is easier to breathe. | Rate is between 12 and 20 breaths/min. |
| Assess Mr. Edwards’ level of hydration (skin turgor, condition of mucosa). | Mucous membranes are moist. Fluid intake in previous 24 hours was 2600 mL. | Oral membranes are pink and moist. Minimum fluid intake of 2500 mL was achieved. |










 Answers to Clinical Application Questions can be found on the Evolve website.
Answers to Clinical Application Questions can be found on the Evolve website.