The skin, hair and nails
Examination of the skin, hair and nails
Anatomy
The skin is the largest organ in the body, making up 16% of body weight. It protects the body from external factors and keeps the internal organs intact (Fig. 4.1 and Box 4.1).
 4.1
4.1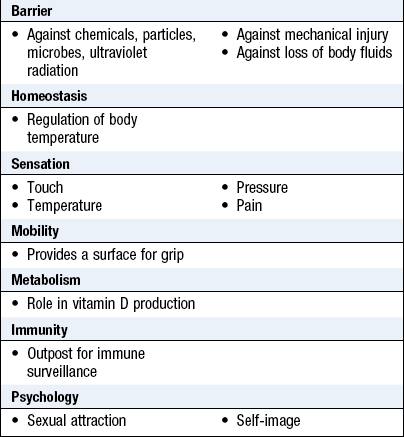
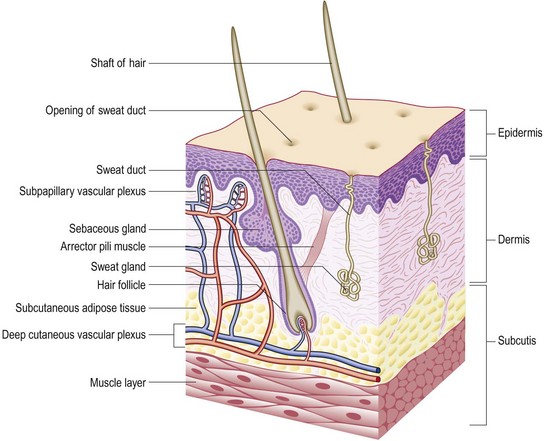
The epidermis is stratified squamous epithelium with four layers (basal, prickle, granular and horny), representing the stages of keratin maturation. The main cell, the keratinocyte, produces keratin. Keratinocytes lose their nuclei in the granular layer and, as flat plates, form the horny layer. Melanocytes (5–10% of the cell population) originate from the neural crest. They synthesise melanin and are most numerous on the face and other exposed sites. Langerhans cells are dendritic, immunologically active antigen-presenting cells that form a network throughout the epidermis.
The dermis is a supportive connective tissue matrix containing specialised structures. It is thin (0.6 mm) on the eyelids and thicker (3 mm or more) on the back, palms and soles. It contains fibroblasts, dendritic cells, mast cells, macrophages and lymphocytes. Collagen fibres make up 70% of the dermis and give strength and toughness. Elastin fibres provide the skin with elasticity. Glycosaminoglycans form a semisolid matrix that allows some movement of dermal structures, such as hair follicles, sweat glands, blood and lymphatic vessels, and nerves.
The subcutis is a loose layer of connective tissue and fat of variable thickness (up to 3 cm thick on the abdomen).
The hair and nails are specialised epidermal structures.
Hair has a protective and sexual function and hairs cover the surface of the skin, except for the glabrous skin of the palms and soles, the glans penis and the vulval introitus. The follicle density is greatest on the face. The hair shaft has an outer cuticle enclosing a cortex of packed keratinocytes.
There are three types of hair:
• lanugo: fine and long; found in the fetus
• vellus hairs: short, fine and light in colour; cover most body surfaces
• terminal hairs: long, thick and dark; found on the scalp, eyebrows, eyelashes, pubic, axillary and beard areas.
Amount and type of hair vary and are influenced by racial and genetic factors. Typically, Europeans have straight hair, black Africans have curly hair and East Asians have sparse facial and body hair. People from the Mediterranean area have more body hair than northern Europeans.
Hair cycle
Regular cycles of growth (anagen), resting (telogen) and shedding (catagen) occur. The cycle lasts up to 5 years for scalp hair, but less for eyebrow, axillary and pubic hair. Adjacent hairs are not in the same phase but illness or childbirth can synchronise the hair cycle and cause an alarming loss of large amounts of hair (telogen effluvium).
Puberty: Body hair develops with sexual maturity, with wide normal variation in its pattern (Fig. 15.19). At puberty, androgens induce vellus hairs of the pubic region to develop into terminal hairs. Gonadotrophins are not involved in this process, so patients with gonadotrophin deficiency have pubic hair but no other pubertal development. Axillary hair appears 2 years after pubic hair and coincides with the onset of facial hair in boys (p. 369).
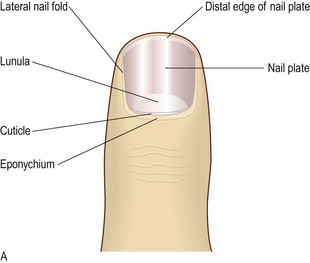
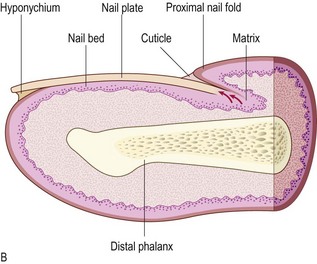
Nails
The nail is a plate of hardened, densely packed keratin protecting the finger tip. It facilitates grasp and tactile sensitivity in the finger pulp (Fig. 4.2). The nail matrix contains dividing cells that mature, keratinise and move forward to form the nail plate, which in the finger is 0.3–0.5 mm thick and grows at 0.1 mm/24 hours (Fig. 4.2). Toenails grow more slowly. Adjacent dermal capillaries produce the pink colour of the nail; the white lunula is the visible distal part of the matrix.
Symptoms and definitions: Symptoms include:
• itch (pruritus) and sleep disturbance (Box 4.2)
 4.2 Causes of severe pruritus
4.2 Causes of severe pruritus
| Condition | Look for: |
| Scabies | Burrows on hands or feet |
| Dermatitis herpetiformis | Small blisters on extensor sites |
| Urticaria | Intermittent wheals on limbs or trunk |
| Eczema | Scaly, crusted, excoriated or lichenified patches |
| Insect bites | Linear or grouped patterns of recent onset |
| Lichen planus | Typical purplish papules on wrists |
| Generalised itch | If no rash, check blood tests for renal, haematological or hepatic diseases |
• discharge, crusting and smell
• scales falling from the skin or scalp
• disfigurement and psychological distress
• inability to work or pursue leisure activities, e.g. swimming.
Rashes: The distribution on the body, morphology (shape) of individual lesions and their grouping (configuration) can be diagnostic. The history of a lesion and systemic features can also be helpful.
• Symmetrical or universal eruptions suggest systemic or constitutional causes.
• Asymmetrical rashes that spread from one focus are more likely to be due to fungal, bacterial or viral infection (Box 4.3).
 4.3 Some examples of skin lesions and systemic disease
4.3 Some examples of skin lesions and systemic disease
| Skin lesions | Associations | Ask about |
| Erythema nodosum | Sarcoidosis, tuberculosis, poststreptococcal infection, connective tissue diseases, drugs | Cough and sputum, breathlessness, sore throat, drugs |
| Pyoderma gangrenosum | Ulcerative colitis, rheumatoid arthritis, leukaemia | Rectal bleeding, joint symptoms |
| Dermatitis herpetiformis | Gluten enteropathy | Family history, change in bowel habit |
| Generalised purpura | Idiopathic thrombocytopenic purpura and other haematological disorders | Family history, haematuria, fever and weight loss |
| Dermatitis artefacta | Personality disorders | Stresses or anxieties |
The time and evolution of the spread and change in morphology help diagnosis.
• An itchy rash typically involving the flexures of the popliteal fossa, antecubital fossa, neck and face occurs in atopic eczema (Fig. 4.3).

• Extensor plaques on elbows and knees, the scalp and the sacrum suggest psoriasis (Fig. 4.4).

• Seborrhoeic dermatitis, an inflammatory reaction to a yeast, Malassezia, that forms part of normal skin flora, affects the forehead, nasolabial folds and scalp.
• Acne vulgaris produces comedones (blackheads), pustules and cysts and also affects the chest and back. Rosacea causes telangiectasia together with the above features.
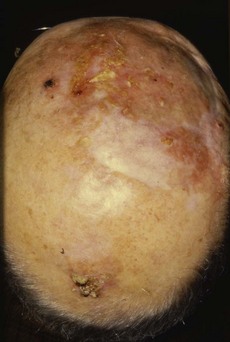
• Sun damage and malignant tumours, such as basal cell cancer, are relatively common (Fig. 4.5).

Fig. 4.5 Anatomical distribution of lesions.
Facial: (A) Seborrhoeic dermatitis. (B) Basal cell cancer showing pearly papules and telangiectasia. Facial and truncal: (C) Acne vulgaris. Truncal: (D) Pityriasis rosea. (E) Urticaria. Peripheral: (F) Necrobiosis lipoidica. (G) Vasculitis. (H) Fungal infection.
• Guttate psoriasis, following a streptococcal throat infection
• Pityriasis rosea, which usually starts with one lesion, the ‘herald patch’
• Tinea versicolor, caused by Pityrosporum yeast
• Urticaria, producing itchy wheals that clear within 24 hours (Fig. 4.5E).
• Wrist lesions suggest lichen planus (Fig. 4.6). Look at the buccal mucosa for the white lacy lesions of Wickham’s striae to confirm this.



Fig. 4.6 Diagnostic sequence, lichen planus.
(A) Discrete flat-topped papules on the wrist. (B) Wickham’s striae visible on close inspection. (C) White lacy network of striae on buccal mucosa.
• Lower leg lesions include necrobiosis lipoidica (associated with diabetes mellitus and occasionally rheumatoid arthritis: Fig. 4.5F), erythema nodosum (due to sarcoidosis or poststreptococcal infection) and vasculitis caused by circulating immune complexes damaging dermal blood vessels (Fig. 4.5G).
• Hands or feet can be affected by fungal infection, typically ‘athlete’s foot’ (caused by Trichophyton) (Fig. 4.5H).
• Sun-exposed, on the face (sparing areas beneath the eyes and lower lip), the V of the neck or the posterior neck and exposed areas of the arms and legs. Causes include connective tissue diseases, e.g. systemic lupus erythematosus (SLE), photosensitising drugs, e.g. thiazide diuretics or non-steroidal anti-inflammatory drugs, cutaneous porphyrias or a primary sun sensitivity condition, e.g. polymorphic light eruption or a photosensitive eczema.
• Dermatomal, e.g. herpes zoster (shingles) (Fig. 4.7).

Morphology is the shape and pattern of the skin lesions (Box 4.4 and Figs 4.8–4.11). Lesions may be:


Fig. 4.9 Macule.
Macules can be pigmented (a freckle), erythematous (haemangioma) or hypopigmented, as shown here in vitiligo.



Configuration is the pattern in which lesions are arranged and include linear, grouped, annular (in a ring), or the Koebner phenomenon (an eruption in an area of local trauma) (Fig. 4.12). Secondary changes of crusting, erosion and excoriation complicate primary lesions.

Duration: Actinic keratoses (Fig. 4.13) are typically present for several years and slowly increase in number. Basal cell cancers commonly develop over 1–2 years and may show ulceration. Squamous cell cancers form more rapidly over weeks or months.
Associated features: In a patient with a hand eruption, look for skin lesions elsewhere, e.g. atopic eczema affecting the antecubital or popliteal fossae or psoriasis on the elbows, knees or scalp, and for burrows of scabies between the fingers or genitalia. The vulva and penis can be affected by psoriasis but only rarely by eczema. Asymmetrical arthritis of large joints and of distal interphalangeal joints is found in up to 30% of patients with psoriasis (Fig. 14.3B).
Common patterns of hair disease
Hair loss (alopecia) can be total or partial (Fig. 4.14):



Fig. 4.14 Hair disorders.
(A) Male-pattern baldness with hair loss from the temples and vertex of the scalp. (B) Alopecia areata with ‘exclamation mark’ hairs, which taper as they approach the skin. (C) Scalp ringworm with secondary bacterial infection and localised hair loss.
• Diffuse alopecia. In common male-pattern hair loss terminal scalp hairs undergo miniaturisation to vellus hairs. This ageing phenomenon is strongly inherited and depends on androgens. Age-related hair loss in women is more diffuse. Non-scarring diffuse hair loss occurs in hypothyroidism, hypopituitarism and iron deficiency, connective tissue diseases, e.g. SLE, postpartum or postmenopausal or may be drug-induced, e.g. cytotoxic agents.
• Localised non-scarring alopecia. In alopecia areata there is circumscribed loss of scalp, beard or eyebrow hair. Alopecia areata may involve the whole scalp (alopecia totalis) or all body hair. (alopecia universalis). Localised hair loss can be caused by fungal infection, hair pulling, traction from braiding and secondary syphilis.
• Scarring alopecia. Burns, severe infections, e.g. herpes zoster, lichen planus and SLE, may permanently scar the scalp with permanent hair loss.
• Loss of secondary sexual hair. In old age, cirrhosis and hypopituitarism, axillary and pubic hair is lost.
Excess hair growth takes two forms:
• Hirsutism: in females with male-pattern growth of terminal hair, including facial and pubic hair extending towards the umbilicus (male escutcheon). It is a racial trait but may be idiopathic, and is rarely caused by an androgen-secreting tumour (Box 4.5). In these cases there are other features of virilisation, e.g. male-pattern hair loss, clitoromegaly or a deep voice.
4.5 Causes of hirsutism
| Type | Example |
| Pituitary | Acromegaly |
| Adrenal | Cushing’s syndrome, virilising tumours, congenital adrenal hyperplasia |
| Ovarian | Polycystic ovary syndrome, virilising tumours |
| Drugs | Androgens, progestogens |
| Idiopathic | End-organ hypersensitivity to androgens |
• Hypertrichosis: in males or females with excess terminal hair growth in a non-androgenic distribution. It is uncommon and usually due to a systemic disorder, e.g. porphyria cutanea tarda, malignancy, anorexia nervosa, malnutrition or drugs, e.g. ciclosporin, minoxidil and phenytoin.
Nail abnormalities
Nail changes are useful in diagnosing internal conditions and skin diseases (Box 4.6). In chronic iron deficiency the nails become brittle, flat and eventually spoon-shaped (koilonychia) (Box 4.7). White nails (leukonychia) are a sign of hypoalbuminaemia. Beau’s lines, due to arrest of nail growth, are transverse white grooves that appear on all nails shortly after a severe illness and which move out to the free margins as the nail grows. Although one or two splinter haemorrhages are commonly seen under the nails of manual workers, multiple lesions raise the possibility of bacterial endocarditis. Distal nail separation (onycholysis) is common in psoriasis. Dilated capillaries in the proximal nail fold occur in vasculitic conditions, such as SLE (Fig. 4.15 and Box 4.6).
4.6 Nail changes in systemic disease and skin disorders
| Change | Description of nail | Differential diagnosis |
| Beau’s lines | Transverse grooves | Any severe systemic illness which affects growth of the nail matrix |
| Brittle nails | Nails break easily, usually at distal margin | Effect of water and detergent, iron deficiency, hypothyroidism, digital ischaemia |
| Clubbing | Loss of angle between nail fold and nail plate. Finger tip bulbous. Nail matrix feels spongy | Familial or may signify serious cardiac or respiratory disease |
| Colour changes | Blue | Cyanosis, antimalarials, haematoma |
| Blue-green | Pseudomonas infection | |
| Brown | Fungal infection, staining from cigarettes, chlorpromazine, gold, Addison’s disease | |
| Brown longitudinal streak | Melanocytic naevus, malignant melanoma, Addison’s disease, racial variant | |
| Red streaks (splinter haemorrhages) | Infective endocarditis, trauma | |
| White spots | Trauma to nail matrix (not calcium deficiency) | |
| White/brown ‘half and half’ nails | Chronic kidney disease | |
| White (leukonychia) | Hypoalbuminaemia, e.g. associated with cirrhosis | |
| Yellow | Psoriasis, fungal infection, jaundice, tetracycline | |
| Yellow nail syndrome | Defective lymphatic drainage – pleural effusions may occur | |
| Combination changes | Longitudinal ridges and triangular nicks at the distal nail | Darier’s disease |
| Koilonychia | Spoon-shaped depression of nail plate | Iron deficiency anaemia, lichen planus, repeated exposure to detergents |
| Nail fold erythema and telangiectasia | Dilated capillaries and erythema at nail fold | Connective tissue disorders, including systemic sclerosis, SLE, dermatomyositis |
| Onycholysis | Nail separates from nail bed | Psoriasis, fungal infection, trauma, thyrotoxicosis, tetracyclines (photo-onycholysis) |
| Onychomycosis | Thickening of the nail plate with colour change, usually whitening or brown discoloration | Fungal infection |
| Pitting | Fine or coarse pits in the nail | Psoriasis, eczema, alopecia areata, lichen planus |
| Thimble pitting | A particular type of fine regular pitting, as seen on a thimble | Alopecia areata |
| Coarse pitting | Larger irregular pits in the nail plate | Eczema |
| Ridging | Transverse (across nail) | Beau’s lines (see above), eczema, psoriasis, tic dystrophy, chronic paronychia |
| Longitudinal (up/down) | Lichen planus, Darier’s disease | |
| Splinter haemorrhages | Small red streaks that lie longitudinally in the nail plate | Trauma, but can signify infective endocarditis |

Mucous membranes and other sites
Changes in the mucous membranes of the mouth and genitalia accompany, and may be characteristic of, certain skin conditions, e.g. oral Wickham’s striae in lichen planus, oral lesions in Kaposi’s sarcoma (Fig. 4.16), vulval involvement with lichen sclerosus. Fully examine patients with skin lymphoma for lymphadenopathy and hepatosplenomegaly. In patients with leg ulcers, feel the leg and foot pulses to assess the arterial supply (Fig. 6.40).

The history
Ask when, where and how the eruption or lesions began, about the initial appearance and what changes have occurred with time. Note associated features, such as itch and systemic upset, together with aggravating and relieving factors. Use SOCRATES to remember what to ask (Box 2.10).
Past and drug histories
Ask about previous skin disease, atopic symptoms (hayfever, asthma, childhood eczema), medical disorders that may involve the skin, e.g. Stevens–Johnson syndrome caused by drugs (Fig. 4.17) or have cutaneous features, and prescribed or self-medicated drugs, including creams and cosmetics.

Social, family and genetic histories
Foreign travel gives exposure to tropical infections or sunlight that could cause a photosensitive eruption. Does the patient have a fair skin type, i.e. does he burn easily and tan poorly or not at all? Skin cancers are commoner with a pale skin. Is there a family history of malignant melanoma or other skin cancer? A family history is found in 10% of patients with malignant melanoma. Psoriasis and atopic eczema also have strongly inherited traits.
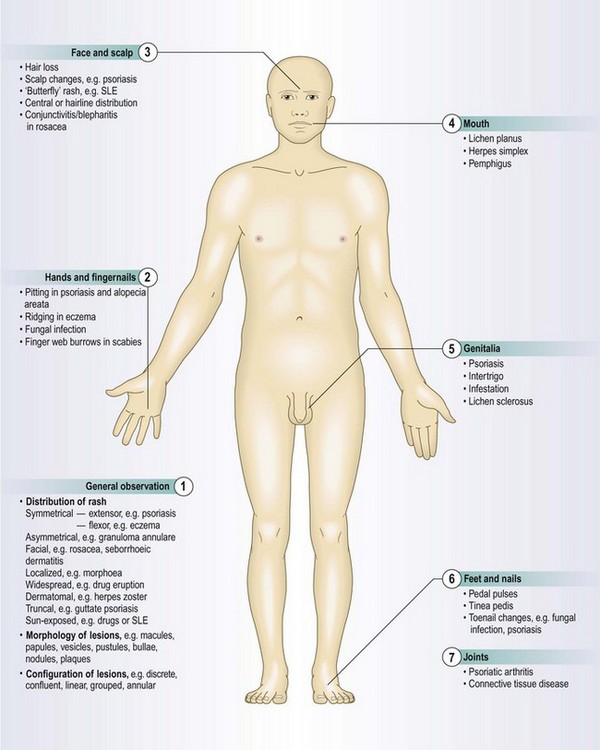
The physical examination
Examining the skin is part of the general examination. When you examine the hands or face, note any abnormalities of the skin.
Ensure a warm, well-lit, private place is available. Offer a chaperone; record the chaperone’s name or if the patient declines the offer. For widespread lesions ask the patient to undress to his underclothes. Use a hand lens to examine individual lesions. A dermoscope, using a ×10 magnification illuminated lens system, is helpful for pigmented lesions (Fig. 4.18).

The skin, hair and nails
Examination sequence
Stand back and look at the skin in its entirety: is it abnormal?
Note the distribution of lesions.
Pick a typical individual lesion and check:
 size (with a tape measure if need be)
size (with a tape measure if need be)
spatial interrelationships: are lesions confluent or separate?
Palpate with your finger tips to establish its consistency, putting on gloves if the skin is broken.
If any pigmented lesion (mole) has recently changed, note the distribution of pigment within it and whether it is inflamed or ulcerated. Malignant melanoma commonly shows variation in pigmentation and has an irregular or diffuse edge. Remember ‘ABCDE’ – Asymmetry, Border irregular, Colour irregular and Diameter >6 mm, Enlargement (Fig. 4.19 and Box 4.8). Examine the entire skin as abnormal moles are more common in patients with a malignant melanoma.
 4.8
4.8
An enlarging mole
In a patient with an enlarging mole, use the ABCDE checklist. Any single positive finding justifies a biopsy or referral for specialist advice.
Whited JD, Grichnik JM. Does this patient have a mole or a melanoma? JAMA 1998;279:696-701.

Fig. 4.19 Malignant melanoma.
A darkly pigmented nodule, with irregular margins and variability of pigmentation.
different areas of the scalp (ask the patient to point to the problem to localise, then part the patient’s hair to see)
Examine local lymph nodes in any patient with a potential squamous cell cancer, malignant melanoma or cutaneous T-cell lymphoma (Fig. 3.21).
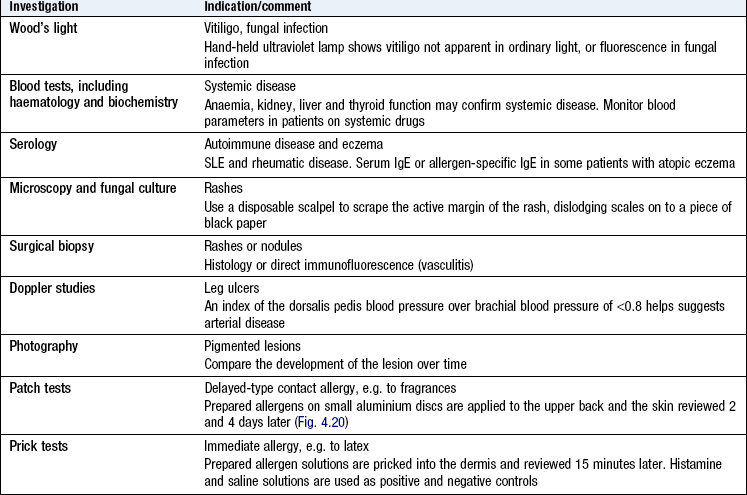
Take a skin scraping for microscopy and culture if you suspect fungal infection.
Putting it all together
In order to diagnose skin disease familiarise yourself with the patterns of skin conditions and then mentally test multiple hypotheses for the best fit against the facts of the history and examination. Not all historic or physical findings match the classic descriptions. Investigations, such as a skin biopsy, are sometimes required to establish a diagnosis.
 4.9
4.9