History taking
Talking with patients
Think about the last time you visited your doctor. What prompted your visit? What arrangements did you have to make? Even a straightforward visit can be a big event. You have to make an appointment, work out what you are going to say and possibly arrange time off work or for child care. People visit doctors for many reasons (Box 2.1). They may have already spoken to family, friends or other health professionals, tried various remedies, and trawled the internet for information to explain their illness or problem. Most patients have some idea of what might be wrong with them and have worries or concerns they wish to discuss.
All patients seek explanation and meaning for their symptoms. You need to work out why the patient has come to see you, what he is most concerned about, and then agree with him the best course of action.
The first and major part of any consultation is talking with your patient. Communication is integral to clinical examination and is most important both at the start of the interview, to gather information, and at the end, to find common ground and engage your patient in his management.
Patient-centred medicine
Patient-centred medicine helps you understand your patient as a whole person. Good communication supports the building of trust between you and your patient and helps you provide clear and simple information (Boxes 2.2 and 2.3). It allows you to understand each other and agree goals together. Communication means much more than ‘taking a history’; it is about involving your patients in their healthcare. Poor communication leads to misunderstanding, conflicting messages and patient dissatisfaction, and is the root cause of complaints and litigation. Over time you will develop your own consulting style; consultation frameworks are useful places to start (Box 2.4).
 2.3 Tips for effective conversations
2.3 Tips for effective conversations
• Ask open questions to start with
• Don’t interrupt your patient
• Use silence to encourage explanations
• Do not use jargon or emotive words
• Find out about your patient as a person
• Clarify and summarise what you understand – you may need to do this more than once
• Make sure the story makes sense to you – keep seeking facts until it does
Beginning
Preparation: Read your patient’s records and any transfer or admission letters before you see your patient.
Where will you see your patient?: Choose a quiet, private space. This is often difficult in hospital, where privacy may be afforded only by curtains, which means no privacy at all. Always be sensitive to privacy and dignity. If your patient is in hospital but is mobile, use a side room or interview room. If there is no alternative to speaking to patients at their bedside, let them know that you understand your conversation may be overheard and give them permission not to answer sensitive questions about which they feel uncomfortable.
How long will you have?: Consultation length varies. In UK general practice the average length is 12 minutes. This is usually adequate, as the doctor may have seen the patient on several occasions and is familiar with the family and social background. In hospital 5–10 minutes may be adequate for returning outpatients, but for new and complex problems 30 minutes or more is usually needed. If you are a student, allow at least 30 minutes.
How will you sit?: Arrange seating in a non-confrontational way. If you use a desk, arrange the seats at the corner of the desk. This is less formal and helps communication (Fig. 2.1A). If you use a computer, make sure the screen and keyboard do not get in the way. Face your patient, not the screen (Fig. 2.1B). At a bedside, pull up a chair and sit level with your patient to see him easily and gain eye contact.

Non-verbal communication: First impressions are important. Your demeanour, attitude and dress influence your patient from the outset. Be professional in dress and behaviour (p. 3) and show concern for your patient’s situation. Avoid interruptions such as the telephone (Fig. 2.1B).
Look for non-verbal cues such as distress and mood. Changes in your patient’s demeanour and body language during the consultation can be clues to difficulties that she cannot express verbally. If the patient’s body language becomes ‘closed’ – that is, she may cross her arms and legs and break off eye contact – this may indicate discomfort (Fig. 2.1B).
Starting your consultation: Introduce yourself, and anyone else who is with you. Use your patient’s and your own names to confirm identity. It may be appropriate to shake hands. If you are a student, inform the patient that you are in training; patients are usually eager to help. Write down facts that are easily forgotten, e.g. blood pressure readings or family tree, but writing notes should not interfere with the consultation.
Here are some ideas on how to get an interview going, though the words you use will change depending on the situation:
Active listening: Hearing your patient’s story about his illness experience is vital. Ask open questions to start with (see below). In the community, try ‘How can I help you today?’ or ‘What has brought you along to see me today?’
Active listening means encouraging the patient to talk by looking interested, making encouraging comments or noises, e.g. ‘Tell me a bit more’ or ‘Uhuh’, and giving the impression that you have time for the patient. Active listening helps gather information and allows patients to tell their story in their own words. Clarify anything you do not understand. Tell patients what you think they have said and ask if your interpretation is correct (reflection).
The way you ask a question is important:
• Open questions encourage the patient to talk. They start with a word like ‘where’ or ‘what’, or a phrase like ‘tell me more about …’. They are most useful initially when you are finding out what is going on and encouraging the patient to talk
• Closed questions, e.g. ‘Have you had a cough today?’ seek specific information as part of a systematic enquiry. They invite ‘yes’ or ‘no’ answers.
Both types of question have their place.
Once you have established what has happened, find out about your patient’s ICE:
Patients will have feelings and ideas about what has happened to them, and these may or may not be accurate. A patient with chest pain might think he has indigestion while you are considering angina. Ask: ‘Do you have any thoughts about what might be happening to you?’ A simple question like: ‘What were you thinking I might do today?’ can avoid unnecessary prescriptions or investigations. Modern medicine may be unable to ‘cure’ a problem, and the important issue is what you can do to help a patient to function.
Empathy: Being empathic helps your relationship with patients and improves their health outcomes (p. 2). What is empathy and how do you express it? Empathy is not sympathy, the expression of sorrow; it is much more. It is helping your patients feel that you understand what they are going through. Try to see the problem from their point of view and relate that to them.
Consider a young teacher who has recently had disfiguring facial surgery to remove a benign tumour from her upper jaw. Her wound has healed, but she has a drooping lower eyelid and significant facial swelling. She returns to work. Think how you would feel and imagine yourself in this situation. Express empathy through questions which show you can relate to your patient’s experience.
Understanding your patient’s context: The context of our lives has a major influence on how we deal with illness. Finding out about your patient’s context is crucial. It is far more than just a ‘social history’. You should understand your patients’ personal constraints and supports, including where they live, who they live with, where they work, who they work with, what they actually do, their cultural and religious beliefs, and their relationships and past experience. It is about your patient as a person. It may not be appropriate to explore these sensitive areas with everyone, or on an initial consultation, but they are important in any long-term doctor–patient relationship. Understanding the whole person modifies the information you give and the way you give it, the treatment you advise and the drugs you use.
Enquire about your patient’s job and explore in some depth what this job entails, as this may have a bearing on the illness. A single job description can cover many tasks, e.g. engineer, so find out what your patient actually does, whether there are any stresses involved, and if there are any relationships at work that affect him, for example, a bullying boss or a harassing colleague.
In the following dialogue, Patient A is under stress and Patient B may be suffering the consequences of exposure to fungal spores which can cause farmer’s lung. However, their initial answer to the first question is the same.
Find out about your patient’s home circumstances. Try asking, ‘Is there anyone at home with you?’ or ‘Is there anyone that can help?’ and be equally tactful enquiring about relationships and the home environment. If a 15-year-old newly diagnosed diabetic is about to go home, ask about the home circumstances: who is at home and are the relationships supportive? Different arrangements should be made for a patient in a stable home whose mother is a healthcare worker compared to one from a deprived background, who has a lone parent and poor relationships.
Patients’ beliefs influence healthcare. Religious and cultural beliefs affect how they cope with a disability or a dying relative, and whether they will accept certain treatments. Be sensitive to, and tolerant of, these issues.
Sometimes the consultation also gives you an opportunity to bring up issues around preventive activities, and a chance to address risk factors and lifestyle challenges. Examples include smoking cessation, dealing with obesity and drug or alcohol dependency, or illnesses that run in the family.
Sharing information and agreeing goals: Clarify and summarise what you say. Use words that the patient will understand and tailor the explanation to your patient.
Explain what you have found and what you think this means. Give important information first and check what has been understood. Provide the information in small chunks and warn the patient how many important things are coming: for example, ‘There are two important things I want to discuss with you. The first is …’.
Use simple language and ensure your patient understands the treatment options and likely prognosis. What you say should be accurate and unambiguous, and the information should be given sensitively. Imagine yourself in the patient’s position and your response. There is no place for being abrupt or for brutal honesty.
Engaging your patient: Make sure patients are involved in any decisions. Share your ideas with them, make suggestions and encourage them to contribute their thoughts. Be sensitive to your patients’ body language. If they seem unclear about something or disagree with you, reflect this back to them. Use phrases like ‘Are you comfortable with what I’m saying?’ or ‘Is there anything that I’ve said that isn’t clear to you or has maybe confused you?’ Whenever possible help decision making by giving written information to take home or by suggesting other sources of information: for example, self-help groups or the internet. Check they have understood you and discuss any investigations or treatment you think might be needed, including risks or side-effects (Box 2.3).
In this way, you will be able to negotiate a mutually agreed plan. For example, a patient with cancer may have the choice of surgery or radiotherapy. By involving him and discussing the pros and cons of treatments, you will enable the patient to reach a decision that you both understand and agree with. The patient will have to live with the consequences of the treatment, which will be much easier to accept if he has chosen the treatment himself.
Try to agree realistic goals. These might be areas that your patient needs to work on. For example, if the patient is trying to stop smoking, then you may set goals together that involve when he is going to stop, what help he will need, e.g. support groups, nicotine replacement therapy or both, how he will identify risky situations, e.g. socialising, and handle these to avoid being tempted to have a cigarette.
Finally, arrange for follow-up if necessary or give the patient some idea about when to return. This depends on how the patient is feeling and on any treatment you have suggested. End a complex discussion by briefly summarising what you have agreed, or ask your patient to summarise for you (Box 2.4).
Difficult situations
Your patient has communication difficulties
If your patient does not speak your language, or has hearing or speech difficulties such as dysphasia or dysarthria, follow the principles of good communication, but in addition you can do the following:
Your patient has cognitive difficulties
Be alert for early signs of dementia. You may have to rely on help from relatives or carers. If you do suspect this, use a memory or mental status test (Ch. 16).
Sensitive situations
Doctors sometimes need to ask personal or sensitive questions and examine intimate parts. If you are talking to a patient who may have a sexually transmitted disease, broach the subject sensitively. Indicate that you are going to ask questions in this area, and make sure the conversation is entirely private. Here are some examples of questions that might work.
Ask permission sensitively if you need to examine intimate areas. This is most likely for examination of the breasts, genitals or rectum, but may apply in some circumstances or cultures whenever you need to touch the patient. First warn your patient; then seek permission to carry out an examination, explaining what you need to do. Always offer a chaperone, even if you are of the same gender as the patient. Record the chaperone’s name and position. If patients decline the offer, respect their wishes and record this in the notes.
Give clear instructions about what clothes they need to remove. If necessary, reschedule an intimate examination until sufficient time, appropriate facilities or a chaperone are available.
Your patient is emotional: Ill people feel vulnerable and may become angry or distressed. Exploring their reasons for the emotion often defuses the situation. Recognise that your patient is angry or sad and ask him to explain why. Use phrases such as, ‘You seem angry about something’ or ‘Is there something that is upsetting you?’ Recognise your patient’s emotion, show empathy and understanding, encourage him to talk and offer what explanations you can.
Talkative patients or those who want to deal with a lot of things at once may respond to: ‘I only have a short time left with you, so what’s the most important thing we need to deal with now?’ If patients have a long list of complaints, suggest: ‘Of the six things you’ve raised today, I can only deal with two, so tell me which are the most important to you and we’ll deal with the rest next time.’
Set professional boundaries if your patient becomes overly familiar: ‘Well, it would be inappropriate for me to discuss my personal issues with you. I’m here to help you so let’s focus on your problem.’
Cultural sensitivity: Patients from a culture that is not your own may have different social rules (Box 2.5). Ideas around eye contact, touch and personal space may be different. In some western cultures, it is normal to maintain eye contact for long periods; in most of the world, however, this is seen as confrontational or rude. Shaking hands with the opposite sex is strictly forbidden in certain cultures. Death may be dealt with differently in terms of what the family expectations of physicians may be, who will expect to have information shared with them and what rites will be followed. Appreciate and accept differences in your patients’ cultures and beliefs. When in doubt, ask them. This lets them know that you are aware of, and sensitive to, these issues.
Third-party information: Confidentiality is your first priority (p. 2). You may need to obtain information about your patient from someone else: usually a relative and sometimes a friend or carer. Ask your patient’s permission and have the patient present to maintain confidentiality. If the patient cannot communicate, you will have to rely on family and carers to understand what has happened to the patient. Third parties may approach you without your patient’s knowledge. Find out who they are, what their relationship to the patient is, and whether your patient knows the third party is talking to you. Tell third parties that you can listen to them but cannot divulge any clinical information without the patient’s express permission. They may tell you about sensitive matters, such as mental illness, sexual abuse, or drug or alcohol addiction. This information needs to be sensitively explored with your patient to confirm the truth.
Telephone consultation: Consulting with patients using the telephone brings specific challenges as there are no visual cues to changes in body language or demeanour. The principles of good communication apply, but it is even more important to listen actively to your patient and frequently check your mutual understanding. Do not make assumptions or jump to diagnoses. Much of clinical medicine relies on direct observation and your intuition as a physician, so err on the side of caution when deciding whether to see a patient or not (Box 2.6).
2.6 Talking to patients by telephone
• Listen actively and take a detailed history
• Frequently clarify and paraphrase to ensure that the messages got across in both directions
• Listen for cues (such as pace, pauses, change in voice intonation)
• Offer opportunities to ask questions
• Safety net – make sure the patient knows what to do if things don’t improve
• As the assessment is based solely on the history, and the management plan cannot be reinforced with non-verbal cues, being systematic in covering all issues is especially important
Breaking bad news: Breaking bad news is one of the most difficult communication tasks you will face. Follow the principles of good communication. Speak to your patient in a quiet private environment. Ask patients who else they would like to be present – this may be a relative or partner – and offer a nurse or counsellor. Then find out how much they know and how much they want to know. Share the information you have. Plan in advance what you need to share, and prioritise so that the important information, which may include a diagnosis and the next steps in planning, do not get lost in a lot of detail. Respond to their feelings, as they may be upset or bewildered, and ensure that they understand and agree on the next steps (Box 2.7).
Gathering information
Diagnosis: Experienced clinicians make a diagnosis by recognising patterns of symptoms. With experience you will refine your questions according to the presenting complaint; you should then have a list of possible diagnoses (a differential diagnosis), before you examine the patient.
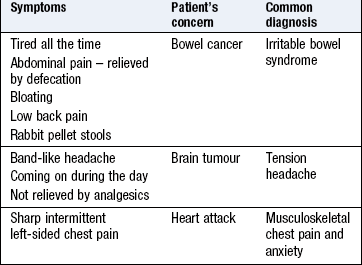
Ensure that patients tell you the problem in their own words and record this. Use your knowledge to direct your questioning. Clarify what they mean by any term they use. Some terms need to be explored (Box 2.8). Each answer increases or decreases the probability of a particular diagnosis, and excludes others.
In the following example, the patient is a 65-year-old male smoker. His age and smoking status increase the probability of certain diagnoses related to smoking. A cough for 2 months increases the likelihood of lung cancer and chronic obstructive pulmonary disease (COPD). Chest pain does not exclude COPD since he could have pulled a muscle on coughing, but the pain may be pleuritic from infection or thromboembolism. In turn, infection could be caused by obstruction of an airway by lung cancer. Haemoptysis lasting 2 months dramatically increases the chance of lung cancer. If the patient also has weight loss, the positive predictive value of all these answers is very high for lung cancer. This will focus your examination and investigation plan.
Follow up by asking key questions to clarify the cough. Follow this up by asking key questions about the pain (see Box 2.10).What sort of pathology does the patient have?: Think about which pathological process may account for the symptoms. Diseases are either congenital or acquired, and there are only certain pathological processes that cause acquired disease. The onset, progression, timescale and associated symptoms of the presenting complaint may guide you to the likely pathology (Box 2.9).
 2.9
2.9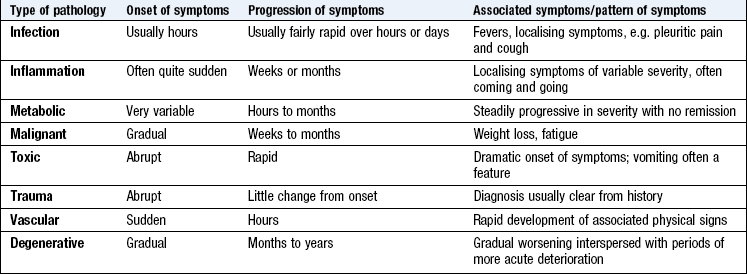
What about physical signs?: Some diseases have no physical signs, e.g. migraine or angina. Other conditions almost always produce physical signs, e.g. fractured neck of femur or stroke. The absence of physical signs may simply reflect the early stage of a disease while some diseases have few or no signs, e.g. Addison’s disease. Experience should help you to rank the reliability of signs to support your diagnosis, e.g. the patient with a history suggesting a transient ischaemic attack may have a carotid bruit but its absence would not exclude this diagnosis. However, a moderately breathless patient with suspected asthma is likely to have wheeze on chest auscultation. If there is no, or minimal, wheeze and the patient has an elevated jugular venous pressure (Ch. 6) with peripheral oedema and inspiratory crackles on inspiration, heart failure with pulmonary oedema is likely. You should have a clear differential diagnosis before examining the patient. Always reconsider your diagnosis if you do not find an expected physical sign or find an unexpected one.
Pain: The characteristics of pain suggest the likely cause. Explore these to make a differential diagnosis. Use the SOCRATES approach (Box 2.10), the principles of which can also be helpful for other symptoms, including dizziness or shortness of breath.
Associated symptoms: Any severe pain can produce nausea, sweating and faintness from the vagal and sympathetic response but some associated symptoms suggest a particular underlying cause; e.g. visual disturbance may precede migraine; palpitation (suggesting an arrhythmia) might occur with angina. Pain disturbing sleep suggests a physical cause.
Effects on lifestyle: Ask ‘How do you cope with the pain?’ This helps you to gain insight into the patient’s coping strategies (ICE: p. 8). Areas to consider in relation to chronic pain are shown in Figure 2.2.
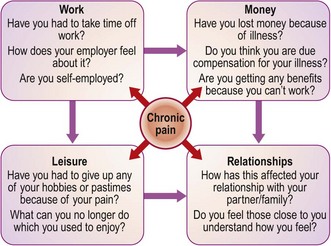
Fig. 2.2 The effects of chronic pain: questions you might ask.
Note that pain affects several areas of a patient’s life but that these are interlinked.
Attitudes to illness: Many symptoms, such as pain and fatigue, are subjective and patients with identical conditions can present with dramatically different histories.
• Pain threshold and tolerance: these vary between patients and also in the same person in different circumstances. Patients vary in their willingness to speak about their discomfort (Box 2.11).
• Past experience: personal and family experience influence the response to symptoms. A family history of sudden death from heart disease may affect how a person interprets chest pain.
• Gains: most illness brings some gains to the patient. These vary from attention from family and friends to financial allowances and avoiding work or stress. Patients may not be conscious of these but sometimes deliberately exaggerate symptoms (p. 27).
Examples of questions that can be used to ask about common symptoms are shown in Box 2.12.
 2.12 Questions to ask about common symptoms
2.12 Questions to ask about common symptoms
| System | Question |
| Cardiovascular | Do you ever have chest pain or tightness? |
| Do you ever wake up during the night feeling short of breath? | |
| Have you ever noticed your heart racing or thumping? | |
| Respiratory | Are you ever short of breath? |
| Have you had a cough? | |
| Do you ever cough anything up? | |
| Have you ever coughed up blood? | |
| Gastrointestinal | Are you troubled by indigestion or heartburn? |
| Have you noticed any change in your bowel habit recently? | |
| Have you ever seen any blood or slime in your stools? | |
| Genitourinary | Do you ever have pain or difficulty passing urine? |
| Do you have to get up at night to pass urine? If so, how often? | |
| Have you noticed any dribbling at the end of passing urine? | |
| Have your periods been quite regular? | |
| Musculoskeletal | Do you have any pain, stiffness or swelling in your joints? |
| Do you have any difficulty walking or dressing? | |
| Endocrine | Do you tend to feel the heat or cold more than you used to? |
| Have you been feeling thirstier or drinking more than usual? | |
| Neurological | Have you ever had any fits, faints or blackouts? |
| Have you noticed any numbness, weakness or clumsiness in your arms or legs? |
Past history
Past medical history may be relevant to the presenting complaint: e.g. previous migraine in a patient with headache; haematemesis and multiple minor injuries in a patient with suspected alcohol abuse.
Ask open questions initially but move to closed questions to obtain relevant, meaningful information (Box 2.13).
Drug history
Ask about prescribed drugs and other medications, including over-the-counter remedies, herbal and homeopathic remedies, laxatives, analgesics and vitamin/mineral supplements. Note the name of each drug, dose, dosage regimen and duration of treatment, along with any significant adverse effects. Clarify, if necessary, with the general practitioner (GP). For patients being prescribed drugs for addiction, e g. methadone, ask the dispensing community pharmacy to stop dispensing for the duration of the hospital admission (Box 2.14).

Compliance, concordance and adherence: Half of all patients do not take prescribed medicines as directed. Patients who take their medication as prescribed are said to be compliant. Concordance implies that the patient and doctor have negotiated and reached an agreement on management, and adherence with therapy is likely (though not guaranteed) to improve.
Ask patients to describe how and when they take their medication. Check to see if they know the names of the drugs and what they are for. Give them permission to admit that they do not take all their medicines by saying: ‘That must be difficult to remember’.
Drug allergies/reactions: Ask if your patient has ever had an allergic reaction to medication, especially before prescribing an antibiotic (particularly a penicillin or vaccine). Clarify exactly what patients mean by allergy. Drug allergies are overreported by patients: only 1 in 7 who report a rash with penicillin will have a positive penicillin skin test. Note other allergies, such as foodstuffs or pollen. Record true allergies prominently in the patient’s case records, drug chart and computer notes. If the patient has had a severe or life-threatening allergic reaction advise him to wear an alert necklace or bracelet (Fig. 3.3).
Family history
Start with open questions, such as: ‘Are there any illnesses that run in your family?’ Follow up the presenting complaint, e.g. ‘Is there any history of heart disease in your family?’ Many illnesses are associated with a positive family history but are not due to a single-gene disorder (Box 2.15).

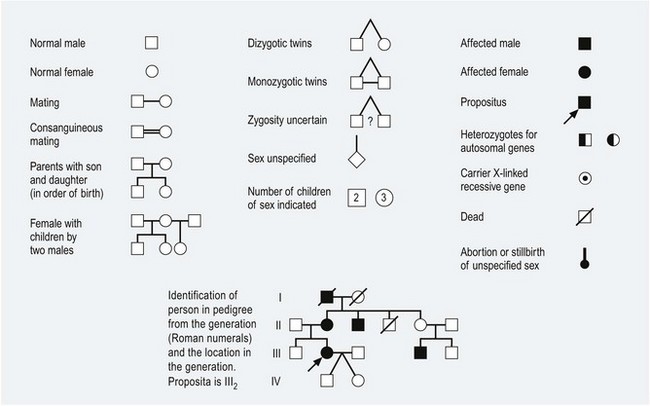
Document illness in first-degree relatives, i.e. parents, siblings and children. If you suspect an inherited disorder such as haemophilia, go back three generations for details of racial origins and consanguinity (Fig. 2.3). Note whether your patient or any close relative has been adopted. Record the health of other household members, since this may suggest environmental risks to the patient’s health.
Social history
The social history helps you to understand the context of the patient’s life and possible relevant factors (Box 2.16). Focus on the relevant issues; for example, ask an elderly woman with a hip fracture if she lives alone, whether she has any friends or relatives nearby, what support services she receives and how well suited her house is for someone with poor mobility.
2.16 The social history
• Birth injury or complications
• Early parental attachments and disruptions
• Schooling, academic achievements or difficulties
• Emotional, physical or sexual abuse*
• Current and previous (clarify exactly what a job entails)
• Exposure to hazards, e.g. chemicals, asbestos, foreign travel, accidents and compensation claims
Relationships and domestic circumstances
• Married or long-term partner
• Partner’s health, occupation and attitude to patient’s illness
• Who else is at home? Any problems, e.g. health, violence, bereavement?
• Type of home, size, owned or rented
• Details of home, including stairs, toilets, heating, cooking facilities, neighbours
Sexual history*
Substance misuse*
*only ask if relevant to the history
The patient’s illness may affect others such as a relative for whom the patient cares; but there may be no one at home to look after the patient because, although she is married, her husband works abroad. Successful discharge from hospital to the community requires these problems to be addressed.
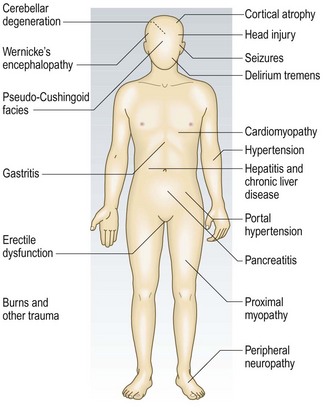
Occupational history: Work profoundly influences health, while unemployment is associated with increased morbidity and mortality. Some occupations are associated with particular illnesses (Box 2.17).
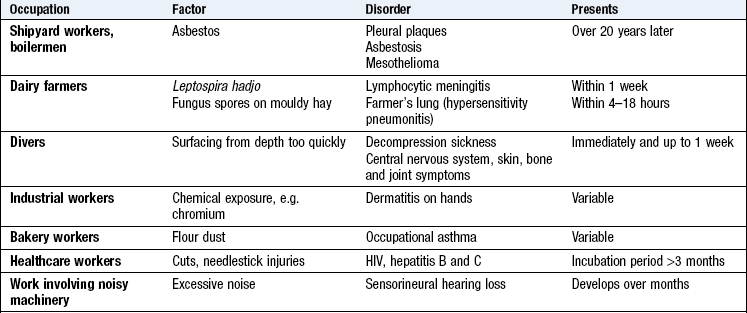
Take a full occupational history from all patients. ‘Tell me about all the jobs you have done in your working life.’ Clarify what the patient does at work, in particular, any chemical or dust exposure (p. 8). Symptoms that improve over the weekend or during holidays suggest an occupational disorder. Hobbies may also be relevant, e.g. psittacosis pneumonia or hypersensitivity pneumonitis in those who keep birds.
Travel history: Returning travellers commonly present with illness. They risk unusual or tropical infections, and air travel itself increases certain conditions, e.g. middle-ear problems or deep vein thrombosis. The incubation period is helpful in deciding on the likelihood of an illness (Box 2.18).
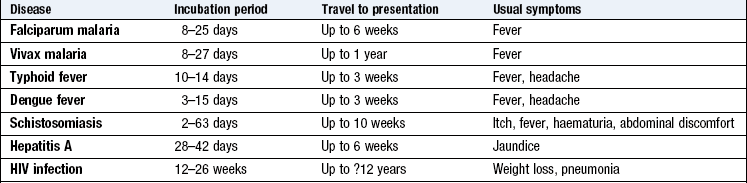
List the countries visited and the dates they were there. Enquire about the type of accommodation used and the activities undertaken, including sexual contacts. Note any travel vaccination or malarial prophylaxis taken.
Sexual history: Only take a full sexual history if this is appropriate (p. 224). Ask questions sensitively and objectively. Signal your intentions: ‘As part of your medical history, I need to ask you some questions about your relationships. Is this all right?’ (Box 2.19).
2.19 Taking a sexual history
• Are you currently in a relationship?
• How long have you been with your partner?
• Is it a sexual relationship?
• Have you had any (other) sexual partners in the last 12 months?
• How many were male? How many female?
• When did you last have sex with:
• Do you use barrier contraception – sometimes, always or never?
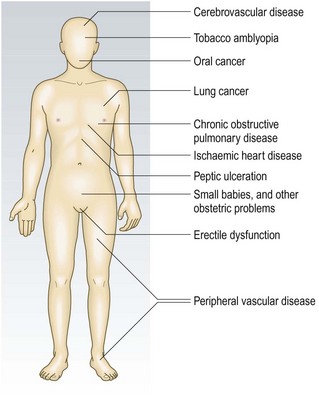
Smoking: Ask if your patient has ever smoked; if so, find out for how long, what form (cigarettes, cigars, pipe, chewed) and how much. For smokers, use ‘pack years’ (Box 2.20) to estimate the risk of tobacco-related health problems (Fig. 2.4) (p. 147). Most patients with COPD have tobacco consumption >20 pack years. If appropriate, enquire about other substances smoked, e.g. cannabis, heroin. Don’t forget to ask non-smokers about their exposure to environmental tobacco smoke (passive smoking).

Alcohol: Try asking: ‘Do you ever drink any alcohol?’ Use open questions, giving permission for patients to tell you, and do not judge them. Follow up with closed questions covering:
• how much? (Box 2.21).
Other useful questions are:
The number of units of alcohol consumed each week can be calculated in two ways (Box 2.22).
2.22 Calculating units of alcohol

1 litre of 40% proof spirits contains 400 ml ethanol or 40 units
750 ml (standard bottle) contains 30 units alcohol
1 litre of 4% beer contains 40 ml ethanol or 4 units
500 ml can contains 2 units of alcohol
Alternatively, use an online calculator, e.g. http://www.drinkaware.co.uk/how-many-units.html.
• Hazardous drinking is the regular consumption of more than:
• Binge drinking, involving a large amount of alcohol causing acute intoxication, is more likely to cause problems than if the same amount is consumed over 4 or 5 days. Everyone should have at least 2 days per week when they drink no alcohol.
• Harmful drinking results in physical or mental health damage or disruption to social circumstances.
• Alcohol dependence is when alcohol use takes a higher priority over other behaviours that previously had greater value (Box 2.23).
2.23 Features of alcohol dependence
• A strong, often overpowering, desire to take alcohol
• Inability to control starting or stopping drinking and the amount that is drunk
• Tolerance, where increased doses are needed to achieve the effects originally produced by lower doses
• Withdrawal state when drinking is stopped or reduced, including tremor, sweating, rapid heart rate, anxiety, insomnia and occasionally seizures, disorientation or hallucinations (delirium tremens). It is relieved by more alcohol
• Neglect of other pleasures and interests
• Continuing to drink in spite of being aware of the harmful consequences
Identifying alcohol problems early is important because of the health risks to patients and their families (Fig. 2.5). It can be difficult and screening tests can help. The CAGE questionnaire is easy to remember and will identify heavy drinkers but is not very sensitive (Box 2.24). The fast alcohol screening test (FAST) questionnaire is more sensitive but more complex (Box 2.25).
2.24 The CAGE questionnaire
• Cut down: Have you ever felt you should cut down on your drinking?
• Annoyed: Have people annoyed you by criticising your drinking?
• Guilty: Have you ever felt bad or guilty about your drinking?
• Ever: Do you ever have a drink first thing in the morning to steady you or help a hangover (an eye opener)?
Positive answers to two or more questions suggest problem drinking; confirm this by asking about the maximum taken.
2.25 The fast alcohol screening test (FAST) questionnaire
For the following questions please circle the answer that best applies
1 drink = 1/2 pint of beer or 1 glass of wine or 1 single measure of spirits
1. Men: How often do you have eight or more drinks on one occasion?
Women: How often do you have six or more drinks on one occasion?
2. How often during the last year have you been unable to remember what happened the night before because you had been drinking?
3. How often during the last year have you failed to do what was normally expected of you because of drinking?
4. In the last year has a relative or friend, or a doctor or other health worker been concerned about your drinking or suggested you cut down?
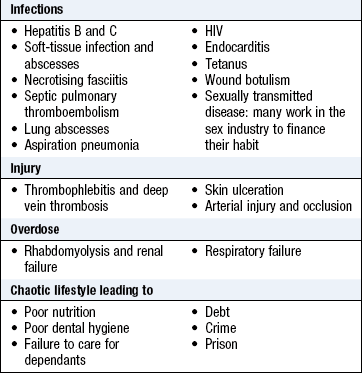
Non-prescribed drug use: Ask all patients who may be using drugs about their use of non-prescribed drugs. In Britain about 30% of the adult population has used illegal or non-prescribed drugs (mainly cannabis) at some time (Boxes 2.26 and 2.27).
2.26 Non-prescribed drug history
• How long have you been taking drugs?
• Any periods of abstinence? If so, when and why did you start using drugs again?
• What symptoms do you have if you cannot get drugs?
• Do you ever inject? If so, where do you get the needles and syringes?
• Do you ever share needles, syringes or other drug paraphernalia?
• Do you see your drug use as a problem?
• Do you want to make changes in your life or change the way you use drugs?
Systematic enquiry
Systematic enquiry uncovers symptoms that may have been forgotten. Ask: ‘Is there anything else you would like to tell me about?’ Until you are experienced, run through with every patient all of the symptoms in Box 2.28. Follow up any positive response by asking questions to increase or decrease the probability of certain diseases.
2.28 Systematic enquiry
cardinal symptoms
Some examples of targeted systematic enquiry are as follows:
• The smoker with weight loss: are there any respiratory symptoms, e.g. unresolving chest infection or haemoptysis to suggest lung cancer?
• The patient with recurrent mouth ulcers: do any alimentary symptoms suggest Crohn’s disease or coeliac disease?
• The patient with palpitation: are there any endocrine symptoms to suggest thyrotoxicosis or is there a family history of thyroid disease? Is the patient anxious or drinking too much coffee?
• If a patient smells of alcohol, ask about related symptoms, such as numbness in the feet due to alcoholic neuropathy.
The psychiatric history
Mental disorders are very common, frequently coexist with physical disorders, and cause much mortality and morbidity. Psychiatric assessment has four elements:
The history
The distinction between symptoms and signs is less clear in psychiatry than the rest of medicine. The psychiatric interview, which covers both, has three purposes:
• to obtain a history (Boxes 2.29 and 2.30) – symptoms
2.29 Content of a psychiatric history
Sensitive topics
In some settings, and for some subjects, use particular skill and tact to obtain answers and to maintain rapport. This applies particularly to:
• sexual issues, e.g. sexual dysfunction, gender identity
• major traumatic experiences, e.g. rape, childhood sexual abuse, witnessing a death
You should develop good rapport at the first interview, and consolidate it before raising a sensitive topic, though sometimes you have to cover such material without delay. In these cases, tell the patient about the nature of and reason for your sensitive enquiries (Box 2.31).
2.31 Sensitive topics
what to ask
• You said a few minutes ago that sometimes you wish you had died in your sleep. I need to ask you a bit more about that thought. Have you ever considered doing something that would make that happen?
• You’ve just told me that you feel your life isn’t worth living. Do you ever think in the same way about your children’s lives?
• You indicated that something terrible happened to you when you were a child. Do you want to tell me more about that now?
The uncooperative patient
Adapt your assessment when a patient is mute, agitated, hostile or otherwise uncooperative, and place greater reliance on observation and collateral information. The safety of the patient, other patients, staff and yourself is paramount so you may only be able to make a partial assessment of agitated or hostile patients.
Mental state examination
The MSE systematically evaluates the patient’s mental condition at the time of interview (Box 2.32). The aim is to establish signs of disorder that, with the history, enable you to make, suggest or exclude a diagnosis. While making specific enquiries, you should observe, evaluate, and draw inferences in the light of the history. This is daunting, but with good teaching, practice and experience you will learn the skills.
• incorporation of relevant elements of the history
The focus is determined by the history and potential diagnoses. For example, detailed cognitive assessment in an elderly patient presenting with confusion is crucial; similarly, carefully evaluate mood and suicide risk when the presenting problem is depression.
Behaviour
• cooperation, rapport, eye contact
• social behaviour, e.g. aggression, disinhibition
• overactivity, e.g. agitation, compulsions
• underactivity, e.g. stupor, motor retardation
• abnormal activity, e.g. posturing, involuntary movements (Box 2.33).
2.33 Behaviour
definitions
| Term | Definition |
| Agitation | A combination of psychic anxiety and excessive, purposeless motor activity |
| Compulsion | An unnecessary, purposeless action that the patient is unable to resist performing repeatedly |
| Disinhibition | Loss of control over normal social behaviour |
| Motor retardation | Decreased motor activity, usually a combination of fewer and slower movements |
| Posturing | The maintenance of bizarre gait or limb positions for no valid reason |
Speech
• articulation, e.g. stammering, dysarthria
• quantity, e.g. mutism, garrulousness
• rate, e.g. pressured, slowed
• volume, e.g. whispering, shouting
• tone and quality, e.g. accent, emotionality
• fluency, e.g. staccato, monotonous
• abnormal language, e.g. neologisms, dysphasia, clanging (Box 2.34).
2.34 Speech
definitions
| Term | Definition |
| Clang associations | Thoughts connected by having a similar sound rather than by meaning |
| Mutism | Absence of speech without impaired consciousness |
| Neologism | An invented word, or a new meaning for an established word |
| Pressure of speech | Rapid, excessive, continuous speech (due to pressure of thought) |
| Word salad | Meaningless string of words, often with loss of grammatical construction |
| Echolalia | Senseless repetition of the interviewer’s words. |
Mood
This is the pervasive emotional state. Affect is the observable expression of emotions, which is more variable over time. A useful analogy is to think of a patient’s mood as a climate, with affect as the current weather.
Assess mood objectively by observation, and subjectively from the history and specific enquiries (Boxes 2.35 and 2.36). Disturbance of mood is the most important feature of depression, mania and anxiety, but mood changes commonly occur in other mental disorders such as schizophrenia and dementia.
2.35 Mood
definitions
| Term | Definition |
| Blunting | Loss of normal emotional sensitivity to experiences |
| Catastrophic reaction | An extreme emotional and behavioural overreaction to a trivial stimulus |
| Flattening | Loss of the range of normal emotional responses |
| Incongruity | A mismatch between the emotional expression and the associated thought |
| Lability | Superficial, rapidly changing and poorly controlled emotions |
Thought form
Loosening of associations is sometimes termed formal thought disorder, and is a core feature of schizophrenia. Subjectively, patients may report having difficulty thinking clearly. Hypomania is characterised by pressure of thoughts and flights of ideas. With depression these processes are slowed and impoverished; this is also characteristic of dementia (Box 2.37).
2.37 Thought form
definitions
| Term | Definition |
| Circumstantiality | Trivia and digressions impairing the flow but not direction of thought |
| Concrete thinking | Inability to think abstractly |
| Flight of ideas | Rapid shifts from one idea to another, retaining sequencing |
| Loosening of associations | Logical sequence of ideas impaired Subtypes include knight’s move thinking, derailment, thought blocking and, in its extreme form, word salad |
| Perseveration | Inability to shift from one idea to the next |
| Pressure of thought | Increased rate and quantity of thoughts |
• rate, e.g. pressure of thought, retardation (slowing)
• flow, e.g. flights of ideas, circumstantiality, perseveration
Record examples of speech from the history to show how a person thinks and expresses thoughts.
Thought content
This is assessed from the history and specific enquiries (Box 2.38). Note thought content from what the patient has discussed during history taking and then explore it by further questioning. It is divided into preoccupations, ruminations and abnormal beliefs:
2.38 Thought content
definitions
| Term | Definition |
| Hypochondriasis | Unjustified belief of suffering from a particular disease in spite of appropriate examination and reassurance |
| Morbid thinking | Depressive ideas, e.g. themes of guilt, burden, unworthiness, failure, blame, death, suicide |
| Phobia | A senseless avoidance of a situation, object or activity stemming from a belief that has caused an irrational fear |
| Preoccupation | Beliefs that are not inherently abnormal but which have come to dominate the patient’s thinking |
| Ruminations | Repetitive, intrusive, senseless thoughts or preoccupations |
| Obsessions | Ruminations which persists despite resistance. |
• Preoccupations are common in normal and abnormal mood states: an anxious person worries about physical illness, or the morbid thoughts of depression.
• Ruminations are preoccupations which are abnormal because they are so repetitive or groundless. They occur in hypochondriasis and obsessional disorders (Box 2.39).
• Abnormal beliefs fall into two categories: those that are not diagnostic of mental illness, e.g. overvalued ideas, superstitions, magical thinking, and those that invariably signify mental illness, i.e. delusions. The main difference is that delusions either lack a cultural basis for understanding the belief or have been derived from abnormal processes.
Overvalued ideas are beliefs of great personal significance that are abnormal because of their effects on a person’s behaviour or well-being. For example, patients with anorexia nervosa may still believe they are fat when they are seriously underweight. They respond to beliefs about their body image rather than their weight (Box 2.40).
2.40 Abnormal beliefs
definitions
| Term | Definition |
| Delusion | An abnormal belief, held with total conviction, which is maintained in spite of proof or logical argument to the contrary and is not shared by others from the same culture |
| Delusional perception | A delusion which arises fully formed from the false interpretation of a real perception, e.g. a traffic light turning green confirms that aliens have landed on the rooftop |
| Magical thinking | An irrational belief that certain actions and outcomes are linked, often culturally determined by folklore or custom, e.g. fingers crossed for good luck |
| Overvalued ideas | Beliefs that are held, valued, expressed and acted on beyond the norm for the culture to which the person belongs |
| Thought broadcasting | The belief that the patient’s thoughts are heard by others |
| Thought insertion | The belief that thoughts are being placed in the patient’s head from outside |
| Thought withdrawal | The belief that thoughts are being removed from the patient’s head |
Delusional beliefs matter greatly to the person, resulting in powerful emotional and important behavioural consequences: they are always of clinical significance. They are classified by their content, such as:
Bizarre delusions are easy to recognise, but not all delusions are weird ideas: a man convinced that his partner is unfaithful may or may not be deluded. Even if a partner were unfaithful, it would still amount to a delusional jealousy if the belief were held without evidence or for some unaccountable reason, such as finding a dead bird in the garden.
Delusions can sometimes be understood as the patient’s way of trying to make sense of his experience. Their content often gives a clue that may help type the underlying illness, e.g. delusions of guilt suggest severe depression whereas grandiose delusions typify mania (Box 2.41). Some delusions are characteristic of schizophrenia, most notably a delusional perception or primary delusion. These include ‘passivity phenomena’: the belief that thoughts, feelings or acts are no longer controlled by the person’s free will.
Perceptions: Assess perceptions using the history and specific enquiries backed up by observation (Box 2.42). People normally distinguish easily between their inner and outer worlds and know what is real and what reality feels like. This can occasionally be disrupted so that normal perceptions become unfamiliar while abnormal perceptions seem real. These anomalies fall into several categories:
2.42 Perceptions
definitions
| Term | Definition |
| Depersonalisation | A subjective experience of feeling unreal |
| Derealisation | A subjective experience that the surrounding environment is unreal |
| Hallucination | A false perception arising without a valid stimulus from the external world |
| Illusion | A false perception that is an understandable misinterpretation of a real stimulus in the external world |
| Pseudohallucination | A false perception which is perceived as part of one’s internal experience |
Depersonalisation and derealisation are associated with severe tiredness and intense anxiety, but also occur in most types of mental illness. With altered perceptions there is a real external object but its subjective perception has been distorted. Sensory distortions, such as unpleasant amplification of light (photophobia) or sound (hyperacusis), can occur in physical diseases, but are also common in anxiety states and drug intoxication or withdrawal. Diminution of perceptions, including pain, can occur in depression and schizophrenia.
Illusions commonly occur among people with established impairment of vision or hearing. They are also found in predisposed patients subjected to sensory deprivation, notably after dark in a patient with clouding of consciousness.
True hallucinations arise without external stimuli; they usually indicate severe mental illness, but can occur naturally when going to sleep (hypnagogic) or waking up (hypnopompic). Hallucinations can be:
Any form of hallucination can occur in any severe mental disorder. The most common are auditory and visual hallucinations, the former are associated with schizophrenia, the latter with delirium. Some auditory hallucinations are characteristic of schizophrenia, e.g. voices discussing the patient in the third person, or giving a running commentary on the person’s activities.
Pseudohallucinations are common. The key distinction from a true hallucination is that these phenomena occur within the patient, rather than arising externally. They have an ‘as if’ quality, and lack the vividness and reality of true hallucinations. Consequently, the affected person is not usually distressed by them; and does not normally feel the need to respond, as happens with true hallucinations (Box 2.43).
Cognition: This is assessed from the history and observation; evaluate any deficit using standard tests. Use the history, observation, MSE and rating scales (see below) together to diagnose and distinguish between the ‘three Ds’ (dementia, delirium and depression) which are common in the elderly and hospital patients.
Core cognitive functions include (Box 2.44):
2.44 Cognition
definitions
| Term | Definition |
| Clouding of consciousness | A reduced level of consciousness observed as drowsiness (coma in extreme cases) |
| Confabulation | Plausible but false memories that cover memory gaps |
Mental disorders are rarely associated with a reduced level of (or clouded) consciousness, except delirium (which is both a physical and a mental disorder), where it is common.
Orientation is a key aspect of cognition, being particularly sensitive to impairment. Disorientation is the hallmark of the ‘organic mental state’ found in delirium and dementia. Abnormalities may be evident during the interview. Check the patient’s knowledge of the current time and date, recognition of where he is (place) and identification of familiar people (person).
Memory function is divided into:
• Registration: test by asking the patient to repeat the names of three unrelated objects e.g. apple, table, penny; any mistake is significant. Alternatively, slowly and clearly say several random single digits, e.g. 6, 3, 5, 9, 1, 4, 7. Then ask the patient to repeat them. A person with normal function can repeat at least five digits.
• Short-term memory: test by giving the patient some new information; once this has registered, check retention after 5 minutes (with a distracting task in between). Do the same with the names of three objects; any error is significant. Alternatively, use a six-item name and address, e.g. Mr David Green, 25 Sharp Street. More than one error indicates impairment.
• Long-term memory is assessed mainly from the personal history that the patient provides. Gaps and mistakes are often obvious, but some patients confabulate (fill in gaps in their memory with unconsciously fabricated facts) so check the account with a family member if possible. Failing long-term memory is characteristic of dementia, although this store of knowledge can be remarkably intact in the presence of severe impairment of other cognitive functions. Confabulation is a core feature of Korsakoff’s syndrome, a complication of chronic alcoholism.
Impaired attention and concentration occur in many mental disorders and are not diagnostic. Impaired attention is observed as increased distractibility, with the patient responding inappropriately to extraneous stimuli which may be real, e.g. a noise outside the room, or unreal, e.g. auditory hallucinations. Concentration is the patient’s ability to stick with a mental task. It is tested by using simple, repetitive sequences, such as asking the patient to repeat the months of the year in reverse or to do the ‘serial 7s’ test, in which 7 is subtracted from 100, then from 93, then 86, etc. Note the finishing point, the number of errors and the time taken.
Estimate intelligence clinically from a combination of the history of educational attainment and occupations, and at interview from vocabulary, general knowledge, abstract thought, foresight and understanding. If in doubt as to whether the patient has a learning disability, or if there is a discrepancy between the history and presentation, a psychologist should formally test IQ.
Insight is the degree to which a patient agrees that he is ill and in need of treatment. Insight matters, since absent or incomplete insight leads to non-compliance (Boxes 2.45 and 2.46).
Risk assessment
Risk assessment is a crucial part of every psychiatric assessment. Consider:
Usually the patient, but others at risk are likely to be family, or, less commonly, specific individuals (neighbours, celebrities) or members of specific groups (defined by age, ethnicity, occupation, etc.).
There may be direct risk to life and limb (as in suicide, self-harm or violence to others) or indirect risk to health (through refusal of treatment for physical or mental illness) or welfare (through inability to provide basic care – food, warmth, shelter, hygiene – for oneself or one’s dependants).
Evaluate risk in all psychiatric assessments (Box 2.47), but in depth when the:
Screening questions for mental illnesses
A psychiatric diagnosis is made by identifying particular clusters of symptoms and mental state changes in the patient. Cover certain areas routinely when you suspect a particular mental illness (Box 2.48). No single question clinches the diagnosis for any specific type of mental disorder, but some features are closely associated with particular mental illnesses, e.g:
• passivity phenomena and schizophrenia
• re-experiencing an ordeal and post-traumatic stress disorder
However, these features may occur in other mental disorders.
The physical examination
Physical and mental disorders are associated, so always consider the physical dimension in any patient presenting with a psychiatric complaint. The patient’s age, health and mode of presentation will determine the extent of physical assessment required. Usually, general observation, coupled with basic cardiovascular and neurological examination, is adequate.
Collateral history
This is important, especially when the patient:
• has a severe learning disability or confusional state
• has a mental disorder that prevents effective communication
Sources of third-party information include family and other carers, as well as past and present GPs and other health professionals. Previous psychiatric assessments are valuable when considering a diagnosis of personality disorder, as this depends on information about behaviour patterns over time rather than details of the current presentation (Box 2.49).
Psychiatric rating scales
Most of these were developed in research studies to assist diagnosis, or to measure change in severity of illness. Some require special training; all should be used sensibly. In general, scales are too inflexible and limited in scope to replace a well-conducted standard psychiatric interview, but they can be useful adjuncts for screening, measuring response to treatment or focusing on particular areas. In routine practice, scales are most widely used to assess cognitive function when an organic brain disorder is suspected. They include:
• Abbreviated Mental Test (AMT): takes <5 minutes (Box 2.50)
Well-known instruments assessing areas other than cognition include:
Medically unexplained symptoms (MUS)
Symptoms are not synonymous with disease but are subjective experiences that may arise from many sources (Box 2.51). There is a major distinction between disease and illness. Disease is a cluster of symptoms resulting from demonstrable pathological processes, e.g. coronary artery disease. Illness (or disorder) is a cluster of symptoms where there may be no demonstrable pathological process despite clearly impaired function, e.g. anxiety.
2.51 Examples of factors influencing symptoms
| Factors | Example |
| Pathological | Chest pain from coronary artery disease |
| Physiological | Tremor |
| Psychological | Paraesthesia from hyperventilation |
| Behavioural | Weakness from excess bed rest |
| External | Compensation and the welfare state |
When symptoms impair a patient’s normal function, do not fit characteristic patterns of disease and persist without any abnormalities on examination and investigation, they are called ‘functional’ or ‘medically unexplained’. More than 30% of patients attending their GP have MUS (with similar proportions in secondary care, where disease prevalence is much greater) (Fig. 2.6). MUS cause similar levels of disability to those resulting from disease and are often associated with significant emotional distress. If such patients are not managed effectively, fruitless investigations and harm from unnecessary drugs or procedures may result. The approach to such patients is important and may differ between specialists.
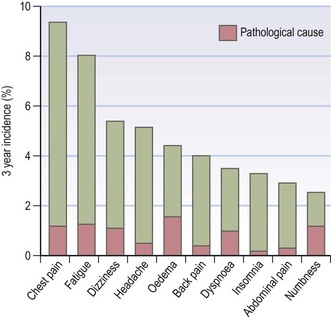
Fig. 2.6 Common symptoms presenting in primary care, showing the percentage with an underlying pathological cause.
MUS raise strong feelings in patients and doctors. Patients may feel they are not believed, or that their symptoms are being dismissed as ‘all in the mind’. Doctors may feel their competence is being questioned.
A dualistic model of mind and body as separate entities is too simplistic and clinically unhelpful. If you think of physical disorders as ‘real’ and MUS as ‘not real’ because they arise from emotional distress or psychiatric disorder your patients will soon detect this and react accordingly. Symptoms result from complex interactions between biological, social and psychological factors; each component is unique to the individual. Many people with severe diseases cope with their symptoms, function remarkably well and work in full-time jobs. Others, with apparently modest symptoms, cannot function effectively. There may be little correlation between symptom severity, disease processes, social functioning and response to treatment. Patients with a proven disease may not improve symptomatically with treatment. For example, therapy for Helicobacter pylori-associated gastritis in a patient with a peptic ulcer may cure the ulcer but not the dyspeptic symptoms. We should understand our patients as individuals and help them to cope with the distress that their symptoms provoke.
Symptoms and definitions
Many terms are used to describe MUS and most specialities have a name for the common ones they see (Box 2.52). These include symptom labels (low back pain), symptom syndromes (chronic fatigue syndrome, irritable bowel syndrome), non-diagnoses (MUS, functional), psychological causes (psychosomatic), psychological processes (somatisation), psychiatric diagnoses (conversion disorder) and malingering (fictitious symptoms simulated for material gain).
2.52 Examples of medically unexplained symptoms and ‘functional’ syndromes in the medical specialities
| Neurology | Functional weakness, tension headache, non-epileptic attacks, hemisensory symptoms |
| Gastroenterology | Irritable bowel syndrome, non-ulcer dyspepsia, chronic abdominal pain |
| Gynaecology | Chronic pelvic pain, urethral syndrome |
| Ear, nose and throat | Functional dysphonia, globus |
| Cardiology | Atypical chest pain, unexplained palpitation, non-cardiac chest pain |
| Rheumatology | Fibromyalgia |
| Infectious disease | (Postviral) chronic fatigue syndrome |
| Immunology/allergy | Multiple chemical sensitivity syndrome |
Patients with multiple symptoms are more likely to have MUS. In general, the more symptoms a patient has, the greater the likelihood of psychiatric illness or distress, e.g. anxiety and depression. Certain symptoms are more likely to be MUS and are not accompanied by any of the usual features that suggest serious physical disease. Some symptoms are particularly unlikely to be associated with significant disease (Box 2.53).
Causes
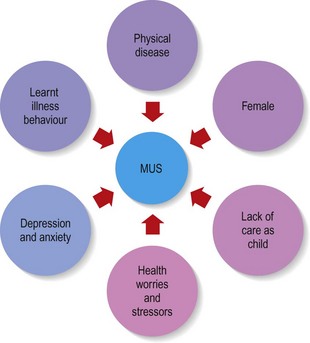
Certain factors increase the risk of MUS (Fig. 2.7 and Box 2.54).
 2.54
2.54
Risk factor for medically unexplained symptoms (MUS)
Women who have experienced parental illness or lack of care during childhood are predisposed to MUS.
Craig TKJ, Cox AD, Klein K. Intergenerational transmission of somatization behaviour: a study of chronic somatisers and their children. Psychol Med 2002;32:805–816.
History
MUS are so common that primary care physicians become adept at spotting this from the history. Making a positive diagnosis from the history and confirming this by negative findings on physical examination allow reassurance and an explanation tailored to the patient.
Presenting complaint
Keep an open mind when talking with all patients; remember that patients with MUS may also have or develop disease. Always take a full history and perform a full clinical examination. Patients will feel that you are taking them seriously and you are less likely to miss any serious physical disease (Box 2.55).
2.55
Misdiagnosis and conversion disorder
24% of people diagnosed with conversion disorder develop an illness that could have explained their presenting symptoms.
Stone J, Smyth R, Carson A et al. Systematic review of misdiagnosis of conversion symptoms and ‘hysteria’. BMJ 2005;331:989.
Accept all symptoms at face value and find out about all of them. Explore exacerbating and relieving factors. Find out when it all started; try asking ‘when did you last feel well?’
Patients’ beliefs in their illness matter; what do they think is wrong? Why have they come now and what do they hope you can do for them? How disabling are their symptoms? What do the symptoms now prevent them from doing? Find out what a typical day is like.
What has happened to them with previous doctors? Patients may complain about previous doctors or certain treatments they have been offered. Allowing a patient to express dissatisfaction shows that you are interested, and helps you avoid suggesting management options the patient is likely to reject. However, recognise that you are only being shown one side of a complicated situation. Maintain a professional approach, ensuring that you do not get drawn into criticising other healthcare providers or their actions.
Often, there are inconsistencies in the history which you should explore and highlight for the patient, e.g. a patient with severe disabling chest pain without angiographic evidence of coronary artery disease may still firmly believe he has angina. His records show that this is not the case and that he has clearly been told this previously. This needs to be explored with him to help demonstrate that his belief is not based on evidence.
Past history
Whenever possible, get all the previous notes, or at least summaries of them. Review these carefully, including childhood illnesses. This can be time-consuming but worth the effort.
Social history
Note any welfare benefits where money is being received for disability, or legal cases where financial compensation may be pending.
Psychiatric history
Leave this until last. To gain the patient’s trust you should be empathic and non-judgemental. Patients will then gain confidence that you are not going to use their emotional symptoms ‘against them’. Patients are acutely sensitive to questions that suggest they are making things up so frame your questions carefully in terms of their symptoms. Ask ‘Do your symptoms ever make you feel down or frustrated?’ rather than ‘Do you ever feel depressed?’
Do not ask about a history of abuse at a first consultation unless the patient volunteers the information. If the abuse was in the past, do not feel that you have to do anything other than bear witness to the patient’s past suffering and acknowledge it. Patients need to feel in control as their past experience has been about being in someone else’s power. Follow local guidelines for any current abuse that may be revealed.
Physical examination
The physical assessment begins as soon as you see the patient in the waiting room and ends when the patient leaves the consulting room. Watch carefully for inconsistent signs, though this does not tell you if symptoms are consciously or unconsciously produced. The symptoms dictate the clinical features that you should look for. Usually there are no physical signs of disease but some non-pathological signs are associated with MUS. These do not exclude disease so interpret them with caution. The history has often suggested the diagnosis and so you are seeking to exclude any unexpected physical findings that warrant further investigation as well as to demonstrate to patients that you are taking them seriously, e.g. in irritable bowel syndrome you may find evidence of bloating and some tenderness but otherwise the gastrointestinal examination will be normal (Ch. 8).
Any signs you find may vary between examinations but overall the examination is commonly normal.
Investigation
The main objective of investigation is to reassure the physician and the patient. Routine, standard investigations and management to exclude all physical illness are costly, unhelpful, risk side-effects and do not achieve the longer-term reassurance of patients. Before proceeding with any investigation, discuss the likelihood and significance of a normal test result with the patient. The effect of diagnostic testing will depend on what the patient thinks a normal result means. Patients are more likely to be satisfied when your explanation makes sense to them, removes blame and helps generate ideas about how they can manage their symptoms.
Putting it all together
Positively identify patients with MUS early by recognising the possibility as you listen to their complaints. Some symptoms are more likely to be medically unexplained than others (Box 2.56). Work with your patient’s ideas and together plan a way forward that avoids unnecessary investigations and treatment (Box 2.57). In 75% of primary care patients with no abnormality on physical examination, symptoms are self-limiting. Reviewing the patient may be more appropriate than performing costly and potentially confusing investigations.
2.56 Common functional syndromes
In all cases, physical examination and investigation fail to reveal an underlying physical cause and symptoms should have lasted more than 3 months in those marked with an asterisk.
| Chronic fatigue syndrome | Persistent fatigue |
| Irritable bowel syndrome | Abdominal pain, altered bowel habit (diarrhoea or constipation), and abdominal bloating |
| Chronic pain syndrome | *Persistent pain in one or more parts of the body sometimes following injury but which outlasts the original trauma |
| Fibromyalgia | *Pain in the axial skeleton with trigger points (tender areas in the muscles) |
| Chronic back pain | *Pain, muscle tension, or stiffness localised below the costal margin and above the inferior gluteal folds, with or without leg pain |
| Urethral syndrome | Recurrent dysuria and urinary frequency but absence of significant bacteriuria |
Documenting the findings: the case notes
The case notes, or records, are the written record of a patient’s medical condition. They include your initial findings, proposed investigations and plan of management, together with information about the patient’s progress. Information is recorded for each episode of illness over time and shared by all the healthcare staff caring for a patient. Notes should therefore be accurate, legible, dated and signed. Primary care records contain the whole story of a patient’s health rather than discrete episodes of hospital care, and follow the patient if he changes practices (Box 2.58).
2.58 Information in the case record
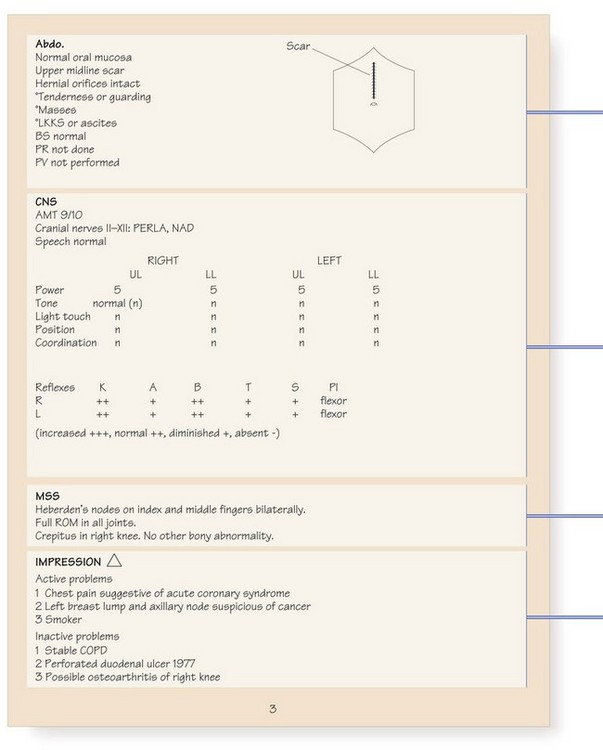
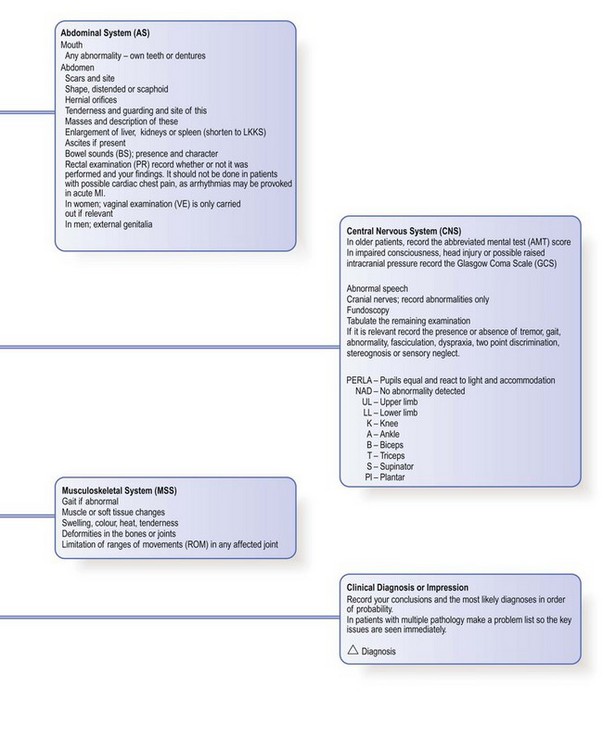
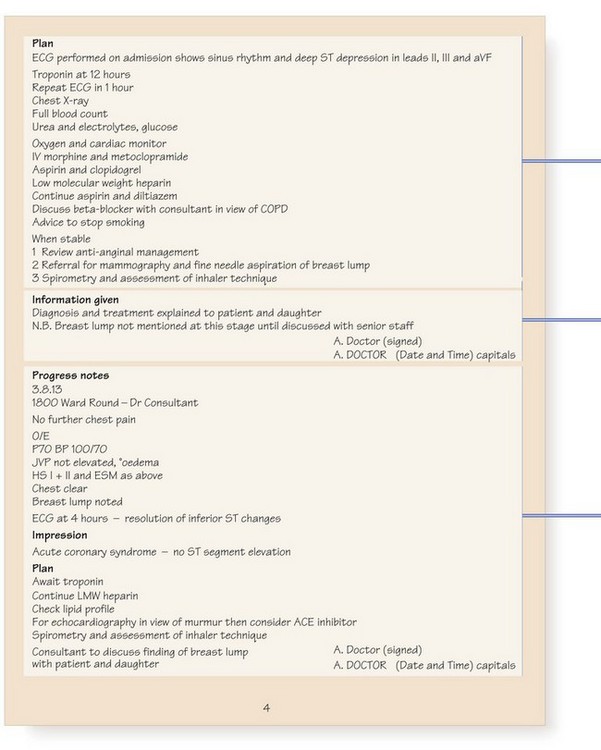
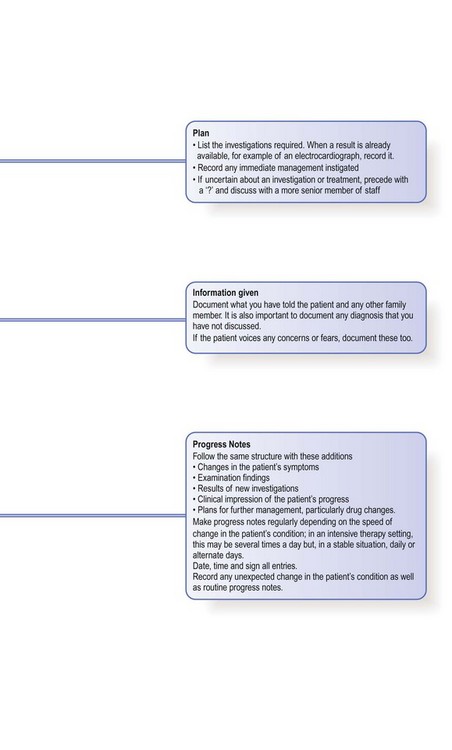
You may write notes while talking with a patient, but do not let this interrupt the discussion and maintain as much eye contact as possible. Active listening is difficult if you are writing, so make brief notes to remind yourself of the important points, and only write up the full history and physical findings when the examination is completed. Only record objective findings. Never make any judgemental or flippant remarks.
Although structured proformas for recording history and examination findings are used in many hospitals, it is not necessary to record every detail in every patient. Only record negative findings if they are relevant. For example, in a patient with breathlessness, the negative details of the respiratory enquiry are important but negative responses to the gastrointestinal enquiry can be condensed to a single entry of ‘none’. You may use abbreviations but they should not be obscure or ambiguous (Fig. 2.8). The prefix ‘°’ is often used to signify ‘no’: for example, ‘° tenderness’. Use diagrams to show the site and size of superficial injuries or wounds, and for the abdomen to illustrate the position of tenderness, masses or scars (Fig. 8.12). Record injuries accurately; you may be asked to give legal evidence from the notes many months later (Box 2.59).
2.59 Describing wounds
• Abrasion: loss of the outer skin due to impact with a rough surface
• Scratch: linear abrasion due to drawing of a sharp point over the skin
• Bruise: bleeding within the tissues beneath the skin
• Laceration: tearing of the skin due to blunt trauma; ragged edges
• Incised wound: cut or gash; sharp edges
• Penetrating wound: breaches full skin thickness; depth is greater than length

Unitary or ‘multidisciplinary’ notes allow the whole team to record their findings in one document rather than each keeping separate case records. Unitary records can be cumbersome but encourage shared care, avoid duplication and make it easy to access information.
Computer records
Records may be held on paper or online. Computers allow easy access to medical and prescribing information during the consultation. All electronic data should be stored securely, accessible only to relevant staff and password-protected. Paperless general practices hold all patient information on computer and this can be downloaded on to laptops for domiciliary use. Some patients carry Smart cards holding their entire medical record.
Confidentiality
The case record is confidential and constitutes a legal document that may be used in a court of law. You cannot share details with anyone who is not involved in a patient’s care, unless the patient gives fully informed written consent. This includes insurance companies, lawyers, the police and research workers. You may only break confidence if a patient poses a risk to himself or other members of the public.
In the UK, patients have the right to receive a copy of their paper case record and to see any personal information held on computer, including their medical records. Remember this when you make your notes or record information about third parties, particularly in cases of sexual abuse. Some patients already hold their own records, usually when antenatal or diabetic care is shared between hospital and community. You can stop patients seeing a part of their record if you think it would seriously harm their physical or mental health or that of any other individual.
Writing letters
Letters must be written when referring a patient to a specialist, and to the GP following an outpatient consultation or hospital admission. The hospital discharge letter (or summary) is structured in a standard format, which can be adapted for referral and outpatient letters. The text should be brief; concentrate on the main issues but include any unexpected findings or complications and relevant investigation results. Include the reason for referral as well as the diagnosis, along with full details of the patient’s past history and current medication. Ensure copies of letters are sent to the patient’s GP and any other specialist involved in the patient’s care.
Most letters are dictated and typed, although structured computerised letters may also be used. When dictating, remember the following:
• State your name and the date of dictation.
• State the patient’s name and date of birth.
• State other important dates, e.g. the patient’s attendance at an outpatient appointment, or hospital admission.
• Speak slowly and clearly. Spell out unusual medical terms.
• Say ‘full stop’ at the end of a sentence and ‘new paragraph’ as required, and include any details of punctuation required. Use paragraph headings as in Box 2.60.
2.60 Discharge letter headings
In many hospitals, voice-activated recognition is now in use and instructions for this may vary from the above. Letters are always easier to dictate when you have just seen the patient rather than several days later.