The musculoskeletal system
Musculoskeletal examination
Symptoms and definitions
Site: Determine whether the pain originates from a joint (arthralgia) (Box 14.1), muscle (myalgia) or other soft tissue. The site may be well localised and suggest the diagnosis, e.g. the first metatarsophalangeal joint in gout (Fig. 14.2), or in several joints suggesting an inflammatory arthritis.
 14.1 Common causes of arthralgia (joint pain)
14.1 Common causes of arthralgia (joint pain)
• Viral, e.g. rubella, parvovirus B19, mumps, hepatitis B, chikungunya
• Rheumatoid arthritis, systemic lupus erythematosus (SLE), ankylosing spondylitis, systemic sclerosis
• Primary, e.g. osteosarcoma, chondrosarcoma
• Metastatic, e.g. from lung, breast, prostate
• Systemic tumour effects, e.g. hypertrophic pulmonary osteoarthropathy
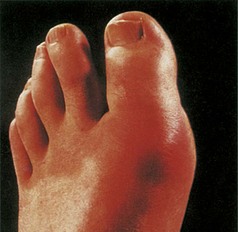
Fig. 14.2 Acute gout of the first metatarsophalangeal joint. This causes swelling, erythema, and extreme pain and tenderness (podagra).
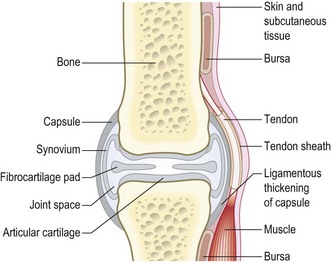
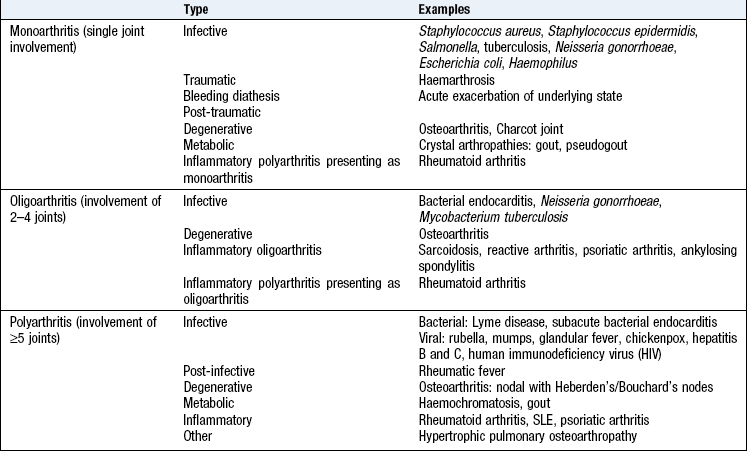
How many joints are involved? One joint is a monoarthritis; 2–4 joints, oligoarthritis; >4 is polyarthritis (Box 14.2). Are the small or large joints of the arms or legs affected? Different patterns of joint involvement help the differential diagnosis (Fig. 14.3 and Box 14.3). Surrounding structures can be painful and include ligaments, tendons, tendon sheaths, bursae, muscle and bone (Fig. 14.1).
 14.3 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis
14.3 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis
| Joint distribution (0–5) | Score |
| 1 large joint | 0 |
| 2–10 large joints | 1 |
| 1–3 small joints (large joints not counted) | 2 |
| 4–10 small joints (large joints not counted) | 3 |
| >10 joints (at least one small joint) | 5 |
| Serology (0–3) | |
| Negative RF and negative ACPA | 0 |
| Low positive RF or low positive ACPA | 2 |
| High positive RF or high positive ACPA | 3 |
| Acute-phase reactants | |
| Normal CRP and normal ESR | 0 |
| Abnormal CRP or abnormal ESR | 1 |
A score of ≥6 classifies the patient as having definite rheumatoid arthritis. This should be distinguished from a definite diagnosis as a patient may clinically have rheumatoid arthritis but not fulfil all criteria.
RF, rheumatoid factor; ACPA, anticyclic-citrullinated peptide antibodies; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate.
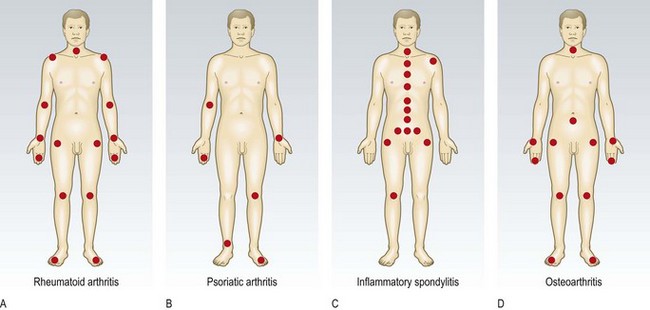
Fig. 14.3 Contrasting patterns of involvement in polyarthritis. (A) Rheumatoid arthritis (symmetrical, small and large joints, upper and lower limbs). (B) Seronegative psoriatic arthritis (asymmetrical, large > small joints, associated periarticular inflammation, giving dactylitis, inflammation of a whole digit, finger or toe). (C) Seronegative inflammatory spondylitis (axial involvement, large > small joints, asymmetrical). (D) Osteoarthritis (symmetrical, small and large joints).
It may be difficult to determine the source of referred pain (Box 14.4). Almost all adults with arthritis (inflamed and swollen joints) have arthralgia (joint pain), but only a minority of patients with arthralgia have arthritis.
 14.4 Common patterns of referred and radicular musculoskeletal pain
14.4 Common patterns of referred and radicular musculoskeletal pain
| Site of pathology | Perceived at |
| Cervical spine | |
| C1/C2 | Occiput |
| C3, 4 | Interscapular region |
| C5 | Tip of shoulder, upper outer aspect of arm |
| C6, 7 | Interscapular region or the radial fingers and thumb |
| C8 | Ulnar side of the forearm, ring and little fingers |
| Thoracic spine | Chest |
| Lumbar spine | Buttocks, knees, legs |
| Shoulder | Lateral aspect of upper arm |
| Elbow | Forearm |
| Hip | Anterior thigh, knee |
| Knee | Thigh, hip |
Onset: Pain from traumatic injury is usually immediate and is exacerbated by movement or haemarthrosis (bleeding into the affected joint). Pain from inflammatory arthritis can develop over 24 hours, or more insidiously. Crystal arthritis (gout and pseudogout) causes acute, sometimes extreme pain which develops quickly, often overnight. Joint sepsis causes pain that develops over a day or two.
Character: Bone pain is penetrating, deep or boring, and is characteristically worse at night. Localised pain suggests tumour, osteomyelitis (infection), osteonecrosis or osteoid osteoma (benign bone tumour)
Generalised bony conditions, such as osteomalacia, usually cause diffuse pain.
Muscle pain (Box 14.5) is often described as ‘stiffness’ and is poorly localised, deep and aggravated by use of the affected muscle(s). It is associated with muscle weakness in some conditions, e.g. polymyositis, but not in polymyalgia rheumatica. Partial muscle tears are painful; complete rupture may be less so.
14.5 Causes of muscle pain (myalgia)
Fracture pain is sharp and stabbing, aggravated by attempted movement or use, and relieved by rest and splintage.
‘Shooting’ pain is often caused by mechanical impingement of a peripheral nerve or nerve root: e.g. buttock pain which ‘shoots down the back of the leg’, caused by lumbar intervertebral disc protrusion.
Chronic joint pain in patients >40 years with progression over years is commonly caused by osteoarthritis.
Neurological involvement in diabetes mellitus, leprosy, syringomyelia and syphilis (tabes dorsalis) may cause loss of joint sensation, so pain is less than expected from examination. In these conditions, even grossly abnormal joints may be painfree (Charcot joint).
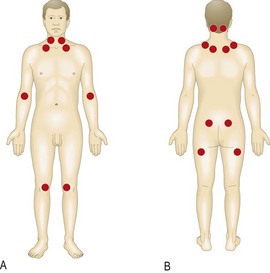
Chronic pain syndrome (fibromyalgia) causes widespread, unremitting pain with little diurnal variation that is poorly controlled by conventional analgesic/anti-inflammatory drugs. Chronic pain syndrome is defined as pain present for more than 3 months. It is due to pain pathway sensitisation and is commonly associated with sleep disorders, psychological stress and depression. Examination is normal except for the presence of typical tender points (Fig. 14.4) (p. 27).
Pain disproportionately greater than expected is seen in compartment syndrome acutely (increased pressure in a fascial compartment, which compromises perfusion and viability of the compartmental structures) and complex regional pain syndrome, chronically. This latter condition develops after injury or illness, or spontaneously, and is characterised by severe ‘burning’ pain, local tenderness, oedema, abnormal sweating and colour, temperature changes and localised osteoporosis.
Radiation: Pain from nerve compression radiates to the distribution of that nerve, e.g. lower leg pain in prolapsed intervertebral disc or hand pain in carpal tunnel syndrome. Neck pain radiates to the shoulder or over the top of the head. Hip pain is usually felt in the groin, but may radiate to the thigh or knee.
Alleviating factors/associated symptoms: Pain caused by a mechanical problem is worse on movement and eases with rest. Pain due to inflammation is worse first thing in the morning and eases with movement. Pain from a septic joint is present both at rest and with movement.
Timing (frequency, duration and periodicity of symptoms): A history of several years of pain with a normal examination suggests chronic pain syndrome. A history of several weeks of pain, early-morning stiffness and loss of function is likely to be an inflammatory arthritis. ‘Flitting’ pain starting in one joint and moving to others over a period of days is a feature of rheumatic fever and gonococcal arthritis. If intermittent with resolution between episodes it is likely to be palindromic rheumatism.
Stiffness
Establish what the patient means by stiffness. Is it:
Stiffness may relate to the soft tissues rather than the joint itself. In polymyalgia rheumatica stiffness commonly affects the shoulder and pelvic areas. There are characteristic differences between inflammatory and non-inflammatory presentations of joint stiffness:
Inflammatory arthritis presents with early-morning stiffness that takes at least 30 minutes to wear off with activity.
Non-inflammatory, mechanical arthritis has stiffness after rest which lasts only a few minutes on movement.
Swelling
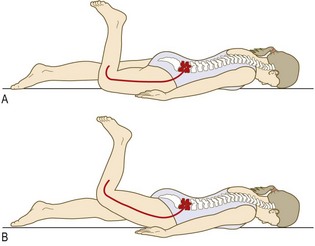
Establish the site, extent and time course of any swelling. Active inflammatory arthritis from any cause results in swelling. When vascular structures, e.g. bone and ligament, are injured, bleeding into the joint or soft tissues produces tense swelling within minutes (Fig. 14.5). This is even more rapid and severe if the patient takes anticoagulants or has an underlying bleeding disorder, e.g. haemophilia. If avascular structures, e.g. the menisci, are torn or articular cartilage is abraded, it can take hours or days to produce a significant effusion.

Erythema (redness) and warmth
Erythema is common in infective, traumatic and crystal-induced conditions and may be mildly present in inflammatory arthritis. All joints with an inflammatory or infective component will be warm.
Erythema associated with distal interphalangeal (DIP) joint swelling helps to distinguish DIP joint psoriatic arthritis from the Heberden’s nodes of osteoarthritis.
Weakness
Weakness suggests joint, neurological or muscle disease. The problem may be focal or generalised.
Weakness due to joint disorders is either from pain inhibiting function or to disruption of the joint or its supporting structures. For neurological disorders producing weakness, see Chapter 11. Always consider nerve entrapment as a cause, e.g. carpal tunnel syndrome at the wrist and leg weakness due to spinal root compression caused by a prolapsed intervertebral disc or spinal stenosis. Muscle disorders can produce widespread weakness associated with pain and fatigue, e.g. in polymyositis and with a rash in dermatomyositis. Proximal muscle weakness can occur in endocrine disorders, e.g. hypothyroidism.
Locking and triggering
‘Locking’ is an incomplete range of movement at a joint because of an anatomical block. It may be associated with pain. Patients use ‘locking’ to describe a variety of problems, so clarify exactly what they mean. True locking is a block to the normal range of movement caused by mechanical obstruction, e.g. a loose body or torn meniscus, within the joint. This prevents the joint from reaching the extremes of normal range. The patient is characteristically able to ‘unlock’ the joint by trick manoeuvres.
Pseudo-locking is a loss of range of movement due to pain.
Triggering is a block to extension, which then ‘gives’ suddenly when extending a finger from a flexed position. In adults it usually affects the ring or middle fingers and results from nodular tendon thickening or fibrous thickening of the flexor sheath due to chronic low-grade trauma, e.g. occupational or associated with inflammatory arthritis. Triggering can be congenital, usually affecting the thumb.
Extra-articular features
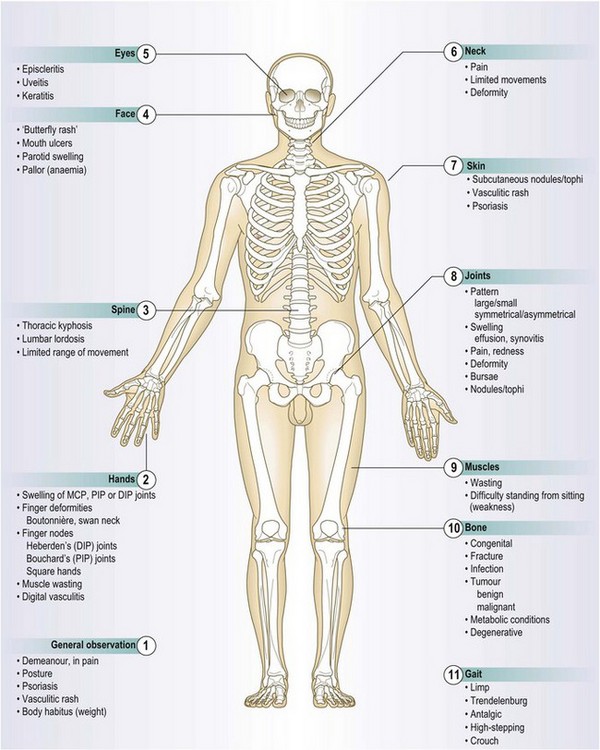
Patients may present with features of extra-articular disease which they may not connect with musculoskeletal problems (see Box 14.7 and Fig. 14.14). The pattern of the joint condition (a/symmetric, flitting) and extent (mono-, oligo- or polyarthritis) suggests the diagnosis and directs the history.
14.7 Extra-articular features
| Condition | Extra-articular features |
| Septic arthritis | Fever, malaise, source of sepsis, e.g. skin, throat, gut |
| Gout | Tophi, signs of renal failure or alcoholic liver disease |
| Reactive arthritis | Urethritis, mouth and/or genital ulcers, conjunctivitis, iritis, enthesopathy, e.g. Achilles tendinopathy/plantar fasciitis, rash (keratoderma blenorrhagica) |
| Ankylosing spondylitis | Enthesopathy, iritis, aortic regurgitation, pulmonary fibrosis |
| Psoriatic arthritis | Psoriasis, nail pitting, onycholysis |
| Rheumatoid arthritis | Subcutaneous rheumatoid nodules, episcleritis, dry eyes, pulmonary fibrosis, pleural effusion, small-vessel vasculitis, splenomegaly, Raynaud’s phenomenon |
| Sjögren’s syndrome | ‘Dry eyes’ (keratoconjunctivitis sicca), xerostomia (reduced or absent saliva production), salivary gland enlargement and Raynaud’s phenomenon |
| Systemic lupus erythematosus | Photosensitive rash, especially on face, mucocutaneous ulcers, alopecia, fever, serositis, Raynaud’s phenemenon, lymphopenia |
| Juvenile idiopathic arthritis | Rash, fever, hepatomegaly, splenomegaly |
Ask about rashes (psoriasis, vasculitis, erythema nodosum) and whether they are photosensitive (systemic lupus erythematosus: SLE).
Weight loss, low-grade fever and malaise are associated with rheumatoid arthritis and SLE. High-spiking fevers in the evening with a rash occur in adult-onset Still’s disease. Headache, jaw pain on chewing (claudication) and scalp tenderness are features of temporal arteritis. Connective tissue disease may present with Raynaud’s phenomenon, sicca symptoms (dryness of mouth and eyes), rash, mouth ulcers, dysphagia and gastrointestinal problems. Dyspnoea may be related to lung disease associated with rheumatoid arthritis or connective tissue disease. Abdominal pain, diarrhoea, bloody stool and mouth ulcers may suggest an arthritis associated with inflammatory bowel disease.
The history
Record the nature and duration of pain using SOCRATES (Box 2.10), and of stiffness, swelling, weakness and locking. Instability, deformity, sensory disturbance and loss of function may also be presenting complaints.
Obtain an exact account of the mechanism of any injury and subsequent events, e.g. development of swelling.
Establish the pattern of joint involvement (Fig. 14.3). Predominant involvement of the small joints of the hands, feet or wrists suggests an inflammatory arthritis, e.g. rheumatoid arthritis or SLE. Medium or large joint swelling is more likely to be degenerative or a seronegative arthritis, e.g. osteoarthritis, psoriatic arthritis or ankylosing spondylitis (Box 14.6). Nodal osteoarthritis has a predilection for the DIP joints and carpometacarpal joint of the thumb. Ask about extra-articular features (Box 14.7).
14.6 Nomenclature in inflammatory arthritis
Seropositive: indicates either the presence of IgM rheumatoid factor (RF) or anti cyclic-citrullinated peptide antibodies (ACPA) in significant titres in the serum of patients with a polyarthritis. ACPA are more specific for rheumatoid arthritis (RA), are particularly associated with smoking and can be present for up to 10 years prior to the onset of clinical manifestations of RA.
Seronegative: indicates the absence of RF in the serum of patients with inflammatory arthritis. If the disease is morphologically the same as rheumatoid arthritis, it is seronegative rheumatoid arthritis. Other inflammatory arthritides, such as psoriatic arthritis, reactive arthritis and ankylosing spondylitis, are also seronegative and are the seronegative arthritides. They are more likely to be associated with HLA B27, share extra-articular features and have an asymmetric pattern of joint involvement.
Past history
Note past episodes of musculoskeletal involvement. Identify co-morbid factors, e.g. diabetes mellitus, steroid therapy, osteoporosis, fractures, ischaemic heart disease, stroke and obesity.
Drug history
Many drugs have side-effects that may either worsen or precipitate musculoskeletal conditions (Box 14.8).
14.8 Drugs associated with adverse musculoskeletal effects
| Drug | Possible adverse musculoskeletal effects |
| Steroids | Osteoporosis, myopathy, osteonecrosis, infection |
| Statins | Myalgia, myositis, myopathy |
| Angiotensin-converting enzyme (ACE) inhibitors | Myalgia, arthralgia, positive antinuclear antibody |
| Antiepileptics | Osteomalacia, arthralgia |
| Immunosuppressants | Infections |
| Quinolones | Tendinopathy, tendon rupture |
Family history
Inflammatory arthritis is more common if a first-degree relative is affected. Osteoarthritis, osteoporosis and gout are heritable in a variable polygenic fashion. Seronegative spondyloarthritis is more common in patients with HLA B27 (Box 14.9). A single-gene defect (monogenic inheritance) is found in hereditary sensorimotor neuropathy (Charcot–Marie–Tooth disease), osteogenesis imperfecta, Ehlers–Danlos syndrome, Marfan’s syndrome and the muscular dystrophies (Box 14.10 and Fig. 14.6).
14.10 The muscular dystrophies
| Inheritance | Gene product | |
| Duchenne | X-linked | Dystrophin |
| Becker | X-linked | Dystrophin |
| Dystrophia myotonica | Autosomal dominant | Myotonin |
| Fascioscapulohumeral | Autosomal dominant | |
| Limb girdle | Autosomal recessive |
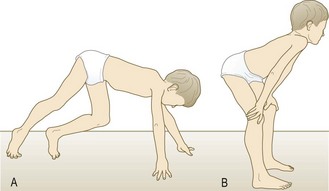
Fig. 14.6 Gower’s sign.
(A) Duchenne muscular dystrophy leads to great difficulty in getting up from a prone position. After rolling over the affected individual walks the hands and feet towards each other. (B) He then uses the hands to climb up the legs, reaching an upright position by swinging the arms and trunk sideways and upwards.
Environmental, occupational and social histories
Ask about current and previous occupations. Is the patient working full- or part-time, on sick leave or receiving benefits? Has the patient had to take time off work because of the condition? If so, is the patient’s job at risk? Litigation may be pending in personal injury cases and occupation-related complaints, e.g. repetitive strain disorder, hand vibration syndrome and fatigue fractures. Army recruits, athletes and dancers are at particular risk of fatigue fractures.
Identify functional difficulties, including ability to hold and use items such as pens, tools and cutlery. How does the condition affect activities of daily living (Box 14.11), e.g. washing, dressing and toileting? Can patients use stairs and do they need aids to walk? Ask about functional independence, especially cooking, housework and shopping.
14.11 Joints involved in activities of daily living
| Activity | Joint(s) involved | Function required |
| Pinch grip | Thumb, index finger | Opposition and flexion of thumb (note: sensation is also required for optimal function) |
| Key grip | Thumb, index finger | Adduction and opposition of thumb |
| Gripping taps, handles, bottle tops | Hand, wrist | Grasp |
| Eating, cleaning teeth and face | Hand, elbow | Grasp, elbow flexion |
| Dressing, washing, hair care | Hand, elbow, shoulder | Pinch, grasp, elbow flexion, shoulder abduction/rotation |
| Toileting, cleaning perineum | Hand, wrist, elbow, shoulder | Grasp, wrist/elbow flexion, forearm supination, internal shoulder rotation |
Some conditions are seen in certain ethnic groups, e.g. sickle cell disease may present with bone and joint pain in African patients. Osteomalacia is more common in Asian patients. Bone and joint tuberculosis is more common in African and Asian patients.
Take a sexual history (Box 2.19), since sexually transmitted disease may be relevant, e.g. reactive arthritis, gonococcal arthritis, human immunodeficiency virus (HIV) infection and hepatitis B (Box 14.12).
The physical examination
Dynamic tests are difficult to describe in pictures and text, so ask an experienced clinician to check your technique. Practise examining as many joints as possible to become familiar with normal appearances and ranges of movement.
General principles
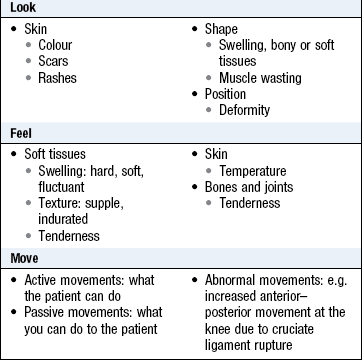
After taking the history, follow a process of observation, palpation and movement.
Examine the overall appearance for pallor, rash, skin tightening and hair changes. Look at the skin, subcutaneous tissues and bony outline of each area. Before palpating, ask the patient which area is painful or tender. Feel for warmth, swelling, stability and deformity. Assess if a deformity is reducible or fixed. Assess active before passive movement. Do not cause the patient additional pain.
• Compare one limb with the opposite side.
• Always expose the joint above and below the one in question.
• In suspected systemic disease, examine all joints and fully examine all systems.
Use standard terminology to describe joint limb positions and movement.
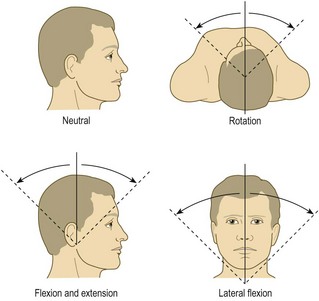
• Always describe movements from the neutral position (Fig. 14.7). Commonly used terms are:
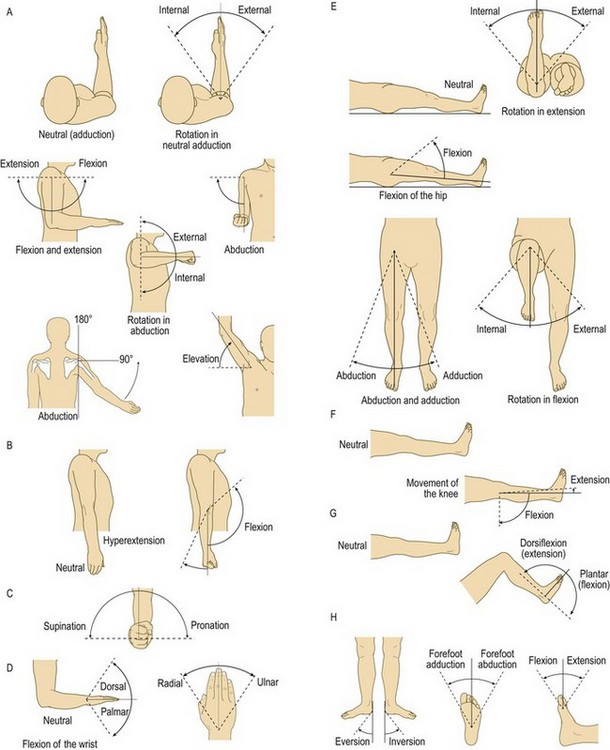
• flexion: bending at a joint from the neutral position
• extension: straightening a joint back to the neutral position
• hyperextension: movement beyond the normal neutral position because of a torn ligament or underlying ligamentous laxity, e.g. Ehlers–Danlos syndrome
• adduction: movement towards the midline of the body (finger adduction is movement towards the axis of the limb)
• Describe the position of a limb because of joint/bone deformity:
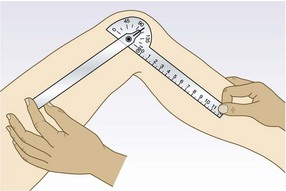
Equipment: You need a tape measure, tendon hammer, goniometer (a protractor for measuring the range of joint movement) (Fig. 14.8), stethoscope and blocks for assessing leg-length discrepancy.
General examination
Abnormal findings: The skin and related structures are the most common sites of associated lesions. The skin and nail appearances in psoriasis may be hidden, e.g. the umbilicus, natal cleft, scalp (Figs 4.4 and 4.15). The rash of SLE is induced by ultraviolet light exposure.
Small, dark red vasculitic spots due to capillary infarcts occur in many systemic inflammatory disorders, including rheumatoid arthritis, SLE (Fig. 4.15F) and polyarteritis nodosa. These indicate active disease. Common sites are the nail folds, finger and toe tips and other pressure areas.
Raynaud’s phenomenon is episodic ischaemia of the fingers precipitated by stimuli such as cold, pain and stress. There is a typical progression of colour changes: blanching (white) is followed by cyanosis (blue), and reactive hyperaemia (red). There is associated dysaesthesia (altered sensation) and pain. Raynaud’s phenomenon is common in otherwise healthy individuals but is a frequent feature in systemic sclerosis and SLE (p. 131).
In systemic sclerosis, the thickened, tight skin produces a characteristic facial appearance (Fig. 3.11C). In the hands, flexion contractures, calcium deposits in the finger pulps (Fig. 14.9) and tissue ischaemia leading to ulceration may occur. The telangiectasias of systemic sclerosis are purplish, blanch with pressure and are most common on the hands and face.

Fig. 14.9 Systemic sclerosis in the hand. (A) Calcium deposits ulcerating through the skin. (B) X-ray showing calcium deposits.
Reactive arthritis has extra-articular features (Fig. 14.10A) and is associated with skin and nail changes similar to those of psoriasis, together with conjunctivitis, circinate balanitis (painless superficial ulcers on the prepuce and glans; Fig. 14.10B), urethritis and superficial mouth ulcers (Fig. 14.10C).
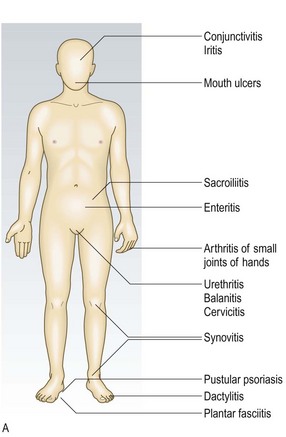


Fig. 14.10 Reactive arthritis. (A) Clinical features. (B) Lesions on the glans penis. (C) Ulcerated tongue.
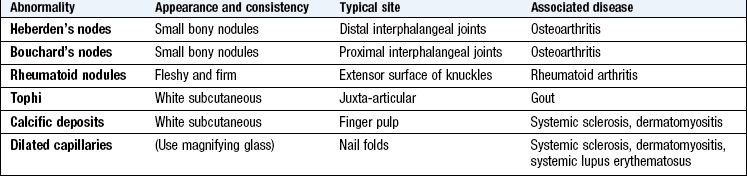
Nodules: Subcutaneous nodules in rheumatoid arthritis most commonly occur on the extensor surface of the forearm (Fig. 14.11). They are firm and non-tender, and may also be felt at sites of pressure or friction, e.g. the sacrum or Achilles tendon. Multiple small nodules can occur in the hands and are particularly associated with methotrexate therapy. Rheumatoid nodules are strongly associated with a positive rheumatoid factor and can occur at other sites, e.g. the lungs.

Bony nodules in osteoarthritis affect the hand and are smaller and harder than rheumatoid nodules. They occur on the lateral aspects of the interphalangeal (IP) joints. At the DIP joints they are called Heberden’s nodes, and at the proximal interphalangeal (PIP) joints, Bouchard’s nodes (Fig. 14.12).
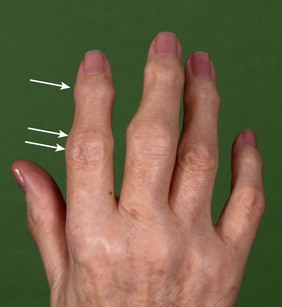
Fig. 14.12 Osteoarthritis of the hand. Heberden’s (single arrow) and Bouchard’s (double arrow) nodes.
Gouty tophi are firm, white, irregular subcutaneous crystal collections (monosodium urate monohydrate). Common sites are the olecranon bursa, helix of the ear and extensor aspects of the fingers, hands, knees and toes (Fig. 14.13). The overlying skin may ulcerate, discharge crystals and become secondarily infected.

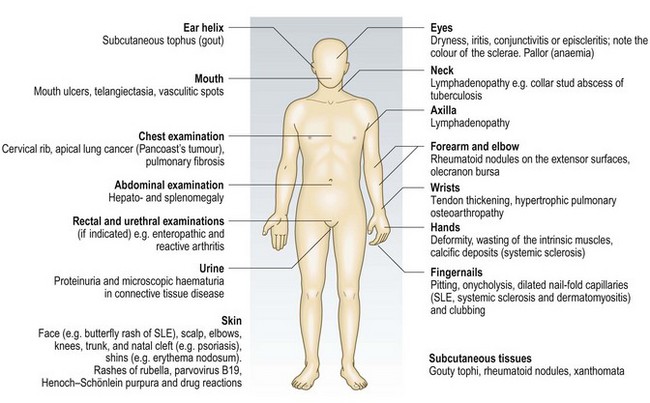
Other extra-articular features (Fig. 14.14).
Eyes: The eyes are affected in many musculoskeletal conditions.
Examination sequence
Perform Schirmer’s tear test to diagnose keratoconjunctivitis sicca.
 Hook a small strip of notched blotting paper ~40 mm long over the lower eyelid while the patient looks upwards. The notch is ~5 mm from one end of the strip and is where the strip is bent over the eyelid.
Hook a small strip of notched blotting paper ~40 mm long over the lower eyelid while the patient looks upwards. The notch is ~5 mm from one end of the strip and is where the strip is bent over the eyelid.
Ask the patient to close the eye.
Wait for exactly 5 minutes, then remove the strip.
Measure the distance that tears travel down the strip with a millimetre rule; >15 mm is normal, 5–15 mm equivocal and <5 mm abnormal.
Abnormal findings: Conjunctivitis is a feature of reactive arthritis. Reduced tear production with ‘dry eyes’ (keratoconjunctivitis sicca) contributes to conjunctivitis and blepharitis (inflammation of the eyelids). This occurs in Sjögren’s syndrome and as secondary changes in rheumatoid arthritis and other connective tissue disorders. Scleritis and episcleritis (Fig. 14.15) are found in rheumatoid arthritis and psoriatic arthritis. Anterior uveitis (iritis) occurs in ~25% of patients with ankylosing spondylitis and reactive arthritis but is asymptomatic in juvenile idiopathic arthritis (JIA), so ophthalmological assessment is essential if JIA is suspected. The sclerae are blue in certain types of osteogenesis imperfecta (Fig. 3.11A) and in the scleromalacia of long-standing rheumatoid arthritis (Fig. 14.15).

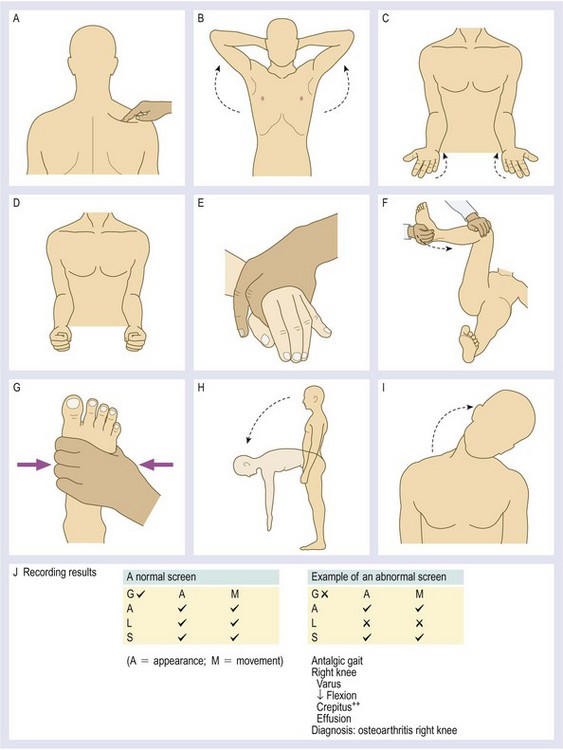
The joints – the GALS screen
The GALS (gait, arms, legs, spine) screen is a rapid screen for musculoskeletal and neurological deficits, and functional ability (Fig. 14.16).
• Do you have any pain or stiffness in your muscles, joints or back?
If all three replies are negative, the patient is unlikely to have a significant musculoskeletal problem. If the patient answers positively, carry out a more detailed assessment.
 Examination sequence
Examination sequence
Ask the patient to undress to his underwear and stand in front of you. Demonstrate actions to the patient rather than simply telling him what to do.
Ask the patient to walk ahead in a straight line for several steps, then turn and walk back towards you. Look for smoothness and symmetry of the gait.
Stand in front of the patient.
Ask him to clench his fists (Fig. 14.16D), and then open his hands flat. This tests both wrists and hands.
Inspect the dorsum of the hands and check for full finger extension at the MCP, PIP and DIP joints.
Ask him to squeeze your index and middle fingers. This tests the strength of the power grip.
Have him touch each fingertip with his thumb. This tests precision grip and problems in co-ordination or concentration.
Gently squeeze the metacarpal heads (Fig. 14.16E). Tenderness suggests inflammation, e.g. rheumatoid arthritis, involving the MCP joints.
Show him how to make a ‘prayer sign’, bending the wrist back as far as possible. Put the backs of the hands together in a similar fashion. This tests wrist flexion and extension.
Ask him to put his arms straight out in front of the body. This tests elbow extension.
Ask the patient to bend the arms up to touch the shoulders. This tests elbow flexion.
Have him place the elbows by the side of the body and bend them 90°. Turn the palms up and down (Fig. 14.16C). This tests pronation and supination at the wrist and elbow.
Ask him to put his hands behind the head, with the elbows going back (Fig. 14.16B). This tests abduction and external rotation of the glenohumeral joint.
Firmly press the midpoint of each supraspinatus to detect hyperalgesia (Fig. 14.16A).
Ask the patient to lie supine (face up) on the couch.
If there is no contraindication, perform Thomas’s test for fixed flexion deformity on both hips (p. 347, Fig. 14.47).
Palpate each knee for warmth and swelling. Check for patellar tap. These detect inflammation and effusions.
Flex each hip and knee with your hand on the patient’s knee. Feel for crepitus in the patellofemoral joint and knee (Fig. 14.16F).
Flex the patient’s knee and hip to 90°, and passively rotate each hip internally and externally, noting pain or limited movement.
Look at the feet for any abnormality. Examine the soles, looking for calluses and ulcers, indicative of abnormal load bearing.
Gently squeeze the metatarsal heads for tenderness (Fig. 14.16G).
Stand behind the patient. Assess the straightness of the spine, muscle bulk and symmetry in the legs and trunk. Look for asymmetry at the level of the iliac crests (unilateral leg shortening) and swelling or other abnormality of the gluteal, hamstring, popliteal and calf muscles. Look at the Achilles tendons and hindfoot regions for swelling or deformity.
Stand beside the patient. Ask him to bend down and try to touch his toes (Fig. 14.16H). This highlights any abnormal spinal curvature or limited hip extension. If he can put his hands flat to the floor, he may have hypermobility.
Stand behind the patient, hold the pelvis, and ask him to turn from side to side without moving his feet. This tests thoracolumbar rotation.
Ask him to slide the hand down the lateral aspect of the leg towards the knee. This tests lateral lumbar flexion.
Stand in front of the patient. Ask him to put his ear on his shoulder (Fig. 14.16I) to test lateral cervical flexion.
Ask him to look up at the ceiling and then down at the floor to test cervical flexion and extension.
Ask him to let the jaw drop open and move it from side to side. This tests both temporomandibular joints.
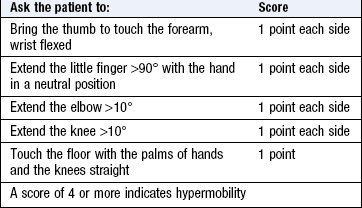
Hypermobility: Some patients have a greater than normal range of joint movement. They may present with recurrent dislocations or sensations of instability if this is severe, but frequently only complain of arthralgia. Mild hypermobility is normal but two inherited conditions affecting connective tissues – Marfan’s syndrome and Ehlers–Danlos syndrome – cause hypermobility.
Assess hypermobility (Box 14.13).
Further examination
The GALS screen provides a rapid, but limited, assessment. This section describes the detailed examination required for better evaluation.
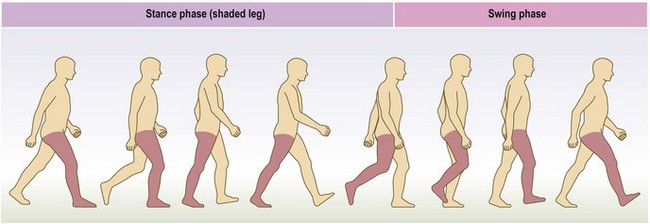
Gait: Gait is the cyclical pattern of musculoskeletal motion that carries the body forwards. Normal gait is smooth, symmetrical and ergonomically economical, with each leg 50% out of phase with the other.
For each leg, gait has two phases: stance and swing. The stance phase is from foot-strike to toe-off, when the foot is on the ground and load bearing (Fig. 14.17). The swing phase is from toe-off to foot-strike, when the foot clears the ground. When both feet are on the ground this is double stance.
A limp is an abnormal gait due to pain or structural change, e.g. lower limb length discrepancy, tone abnormality (including spasticity and co-contraction, in both of which there is inappropriate muscle contraction) or weakness.
Pain: An antalgic gait is one altered to reduce pain. Pain in a lower limb is usually aggravated by weight-bearing, so minimal time is spent in the stance phase on that side. This results in a ‘dot–dash’ mode of walking. If the source of pain is in the spine, axial rotatory movements are minimised, resulting in a slow gait with small paces. Patients with hip pain may lean towards the affected side as this decreases the compression force on the hip joint.
Structural change: Patients with limb-length discrepancy may walk on tiptoe on the shorter side, with compensatory hip and knee flexion on the longer side. Assess for limb-length discrepancy with block testing (p. 346). Other structural changes producing an abnormal gait include joint fusion, bone malunion and contracture.
Weakness: This may be due to nerve or muscle pathology or alteration in muscle tone. In a normal gait the hip abductors of the stance leg raise the contralateral hemipelvis. In Trendelenburg gait, abductor function is poor when weight bearing on the affected side, so the contralateral hemipelvis falls (Fig. 14.46).
Common causes of a Trendelenburg gait are:
• weakness of the hip abductors, e.g. in polio or paresis of the superior gluteal nerve after total hip replacement
• structural hip joint problems, e.g. congenital dislocation of the hip
Foot drop occurs in common peroneal nerve palsy. The gait is high-stepping to allow clearance of the weak foot.
Increased tone: This occurs following an upper motor neurone lesion, e.g. cerebrovascular accident (stroke) or cerebral palsy. The gait depends on the specific lesion, contractures and compensatory mechanisms. A common pattern in cerebral palsy is the crouch gait, in which the hips and knees are always flexed.
Examination sequence
Ask the patient to walk barefoot in a straight line; then repeat in shoes.
Observe the patient from behind, in front and from the side.
Evaluate what happens at each level (foot, ankle, knee, hip and pelvis, trunk and spine) during both stance and swing phases.
Assess each joint (Box 14.14).
The spine
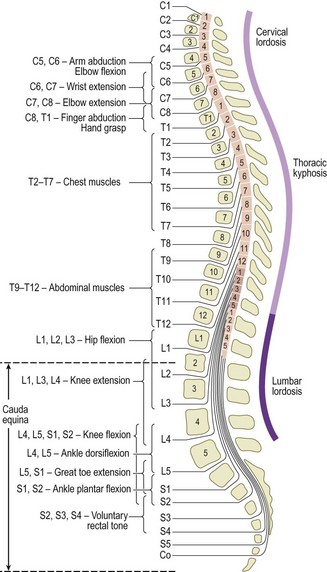
The spine is divided into the cervical, thoracic, lumbar and sacral segments. Most spinal diseases affect multiple segments, causing alteration in the posture or function of the whole spine. Spinal disease may occur without local symptoms and present with pain, neurological symptoms or signs in the trunk or limbs. Accurate diagnosis depends on knowing the underlying bony and neurological anatomy (Fig. 14.18), a careful history, and eliciting signs and symptoms to differentiate between mechanical (non-inflammatory) and inflammatory causes (Box 14.15).
14.15 Common spinal problems
Definitions: Scoliosis is lateral curvature of the spine (Fig. 14.19A).
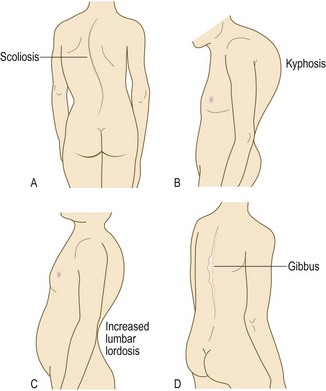
Kyphosis is curvature of the spine in the sagittal (anterior–posterior) plane, with the apex posterior (Fig. 14.19B). The thoracic spine normally has a mild kyphosis.
Lordosis is curvature of the spine in the sagittal (anterior–posterior) plane, with the apex anterior (Fig. 14.19C).
Gibbus is a spinal deformity caused by an anterior wedge deformity localised to a single vertebra, producing an increase in forward flexion (Fig. 14.19D).
Spondylosis is degenerative change in the spine.
Spondylolysis is a defect in the pars interarticularis of a vertebral arch (Fig. 14.20A).
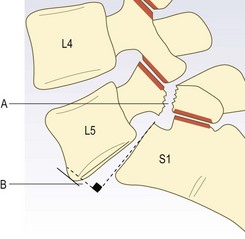
Fig. 14.20 Lumbosacral junction. (A) Defect in pars interarticularis (spondylolysis). (B) Anterior translation of L5 on S1 (spondylolisthesis).
Spondylolisthesis is one vertebra slipping anteriorly on an inferior vertebra (Fig. 14.20B).
Retrolisthesis is one vertebra slipping posteriorly on an inferior vertebra.
Anatomy: Head nodding occurs at the atlanto-occipital joints, and rotational neck movements mainly at the atlantoaxial joint. Flexion, extension and lateral flexion occur mainly at the mid-cervical level. The neural canal contains the spinal cord and the emerging nerve roots, which pass through exit foramina bounded by the facet joints posteriorly and the intervertebral discs and neurocentral joints anteriorly. The nerve roots, particularly in the lower cervical spine, may be compressed or irritated by lateral disc protrusion or by osteophytes arising from the facet or neurocentral joints. Central disc protrusions may press directly on the cord (Fig. 11.34).
The history: The most common symptoms are pain and difficulty turning the head and neck. Patients find difficulty driving, especially when attempting to reverse. Neck pain is usually felt posteriorly but may be referred to the head, shoulder, arm or interscapular region. Cervical disc lesions cause radicular pain in one or other arm, roughly following the dermatomes of the affected nerve roots (Box 14.4). If the spinal cord is compromised (cervical myelopathy), then lower limb weakness, difficulty walking, loss of sensation and sphincter disturbance may occur.
Be particularly careful when examining patients with rheumatoid arthritis, as atlantoaxial instability can lead to spinal cord damage when the neck is flexed.
In patients with neck injury, never move the neck. Splint it and check for abnormal posture. Check neurological function in the limbs and X-ray to assess bony injury.
Examination sequence
Ask the patient to remove enough clothing for you to see the neck and upper thorax, then to sit on a chair.
Face the patient. Observe the posture of the head and neck. Note any abnormality or deformity, e.g. loss of lordosis (usually due to muscle spasm) (Box 14.16).
Feel the midline spinous processes from the occiput to T1 (the T1 process is usually the most prominent).
Feel the paraspinal soft tissues.
Feel the supraclavicular fossae for cervical ribs or enlarged lymph nodes.
Feel the anterior neck structures, including the thyroid.
Note any tenderness in the spine, trapezius, interscapular and paraspinal muscles.
Assess active movements (Fig. 14.21).
Ask the patient to put his chin on to the chest to assess forward flexion. The normal range is 0 (neutral) to 80°. Record a decreased range as the chin–chest distance.
Ask him to look upwards at the ceiling as far back as possible, to assess extension. The normal range is 0 (neutral) to 50°. Thus the total flexion–extension arc is normally ~130°.
Ask him to put his ear on to the shoulder, to assess lateral flexion. The normal range is 0 (neutral) to 45°.
Ask the patient to look over his right/left shoulder. The normal range of lateral rotation is 0 (neutral) to 80°.
If active movements are reduced, gently perform passive movements. Establish if the end of the range has a sudden or a gradual resistance and whether it is pain or stiffness that restricts movement. Pain or paraesthesiae in the arm on passive neck movement suggests nerve root involvement.
Perform a neurological assessment of the upper and lower limbs (Figs 11.18 and 11.19).
Anatomy: This segment of the spine is the least mobile and maintains a physiological kyphosis throughout life. Movement is mainly rotational with a very limited amount of flexion, extension and lateral flexion.
The history: Presenting symptoms in the thoracic spine are localised spinal pain (Box 14.17), pain radiating round the chest wall or, less frequently, symptoms of paraparesis, including sensory loss, leg weakness, and loss of bladder or bowel control. Disc lesions are rare but may be accompanied by pain radiating around the chest (girdle pain), mimicking cardiac or pleural disease. Patients with osteoporotic vertebral fractures may not complain of pain, but lose height and have deformity (increased kyphosis).
Patients with vertebral collapse due to malignancy may have associated spinal cord compression. Consider infection as a cause of acute pain, especially if systemic upset or fever is present. With poorly localised thoracic pain, consider intrathoracic causes, e.g. myocardial ischaemia or infarction, oesophageal or pleural pain and aortic aneurysm.
Anatomy: The surface markings are the spinous processes of L4/5, which are level with the pelvic brim, and the ‘dimples of Venus’, which overlie the sacroiliac joints. The normal lordosis may be lost in disorders such as ankylosing spondylitis and lumbar disc protrusion.
The principal movements are flexion, extension, lateral flexion and rotation. Most patients can bring the tips of their fingers at least to the level of the knees in forward and lateral flexion. Extension should be approximately 10–20°. In flexion, the upper segments move first, followed by the lower segments, to produce a smooth lumbar curve. However, even with a rigid lumbar spine, patients may be able to touch their toes if their hips are mobile.
In the adult, the spinal cord ends at L2. Below this, the spinal nerve roots may be injured or compressed by disc protrusion. Above this level the spinal cord itself may be involved.
The history: Low back pain is extremely common. Most is ‘mechanical’, and due to degenerative disease. Radicular back pain due to nerve root compression radiates down the posterior aspect of the leg to the lower leg or ankle. Pain due to inflammation of the sacroiliac joints is commonly felt in the buttocks, but may be referred down both legs to the knees. Groin and thigh pain in the absence of hip abnormality suggests referred pain from L1–2.
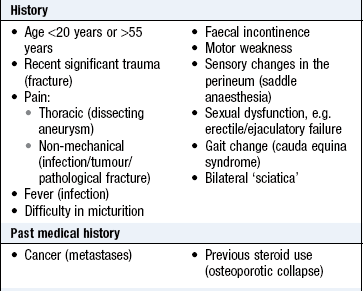
Red flag features suggest significant spinal pathology (Box 14.18). Consider abdominal and retroperitoneal pathology too, e.g. abdominal aortic aneurysm, pancreatitis, peptic ulcer and renal disorders.
14.18 ‘Red flag’ and ‘yellow flag’ features for acute low back pain
These are psychosocial factors associated with greater likelihood of long-term chronicity and disability
• A history of anxiety, depression, chronic pain, irritable bowel syndrome, chronic fatigue, social withdrawal
• A belief that the diagnosis is severe, e.g. cancer. Faulty beliefs can lead to ‘catastrophisation’ and avoidance of activity
• Lack of belief that the patient can improve leads to an expectation that only passive, rather than active, treatment will be effective
• Ongoing litigation or compensation claims, e.g. work, road traffic accident
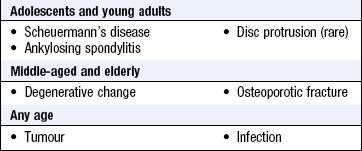
Important spinal conditions are acute disc protrusion, spinal stenosis, ankylosing spondylitis (Fig. 14.22), osteoporotic fracture, infection and tumours. Infection and tumours are associated with fever or weight loss. In many patients, however, backache reflects age-related degenerative change in discs and facet joints (spondylosis).

Mechanical low back pain is common after standing for too long or sitting in a poor position. Symptoms worsen as the day progresses and improve after resting or on rising in the morning.
Insidious onset of backache and stiffness in an adolescent or young adult suggests inflammatory disease of the sacroiliac joints and lumbar spine, e.g. ankylosing spondylitis (Box 14.19). Symptoms are worse in the morning or after inactivity, and ease with movement. Morning stiffness is more marked than in osteoarthritis, lasting at least 30 minutes. Other clues to the diagnosis are peripheral joint involvement, extra-articular features or a positive family history.
 14.19
14.19
Ankylosing spondylitis
In a young man with gradual-onset chronic back pain, a positive family history for reactive arthritis, psoriasis or inflammatory bowel disease, and the presence of peripheral joint involvement or anterior uveitis all suggest a diagnosis of ankylosing spondylitis.
Rudwaleit M, Feldtkeller E, Sieper J. Easy assessment of axial spondyloarthritis (early ankylosing spondylitis) at the bedside. Ann Rheum Dis 2006;65:1251–1252.
Acute onset of low back pain in a young adult, often associated with bending or lifting, is typical of acute disc protrusion (slipped disc). The acute episode may be superimposed on a background of preceding episodic backache due to disc degeneration. Activities such as coughing or straining to open the bowels exacerbate the pain. There may be symptoms of lumbar or sacral nerve root compression. Cauda equina syndrome involves a central disc prolapse, or similar space-occupying lesion, impinging on the cauda equina. There are features of sensory and motor disturbances, including diminished perianal sensation and bladder function disturbance. The motor disturbance may be profound, e.g. paraplegia.
Acute back pain in the middle-aged, elderly or those with risk factors, e.g. steroid therapy, may be due to osteoporotic fracture. This is eased by lying, exacerbated by spinal flexion and not usually associated with neurological symptoms.
Acute onset of severe progressive pain, especially associated with malaise, weight loss or night sweats, may indicate pyogenic or tuberculous infection of the lumbar spine or sacroiliac joint. The patient may have a past history of diabetes mellitus or immunosuppression, e.g. steroid therapy or HIV infection, and complain of pain and great difficulty in moving. The infection may involve the intervertebral discs and adjacent vertebrae and may track into the psoas muscle sheath, presenting as a painful flexed hip or a groin swelling.
Consider malignant disease involving a vertebral body in patients with unremitting spinal pain of recent onset, disturbing sleep. Other clues are a previous history of cancer, and systemic symptoms or weight loss. Tumours rarely affect intervertebral discs.
Cauda equina syndrome and spinal cord compression are neurosurgical emergencies. If suspected, refer the patient immediately for assessment and possible surgical decompression.
Intermittent discomfort or pain in the lumbar spine occurring over a long period of time is typical of degenerative disc disease. There is stiffness in the morning or after immobility. Pain and stiffness are relieved by gentle activity but recur with, or after, excessive activity. Over years there is gradual loss of lumbar spine mobility, sometimes with spontaneous improvement in pain as the facet joints increasingly stiffen.
Diffuse pain in the buttocks or thighs brought on by standing too long or walking is the presenting symptom of lumbosacral spinal stenosis. This can be difficult to distinguish from intermittent claudication (p. 128). The pain may be accompanied by tingling and numbness and difficult for the patient to describe. Typically, it is relieved by rest or spinal flexion. Stooping or holding on to a supermarket trolley may increase exercise tolerance. Narrowing of the spinal canal or neural exit foramina is caused by degenerative changes in the intervertebral discs and facet joints, and there is a long preceding history of discomfort typical of degenerative joint disease.
Examination sequence
Ask the patient to stand with the back fully exposed.
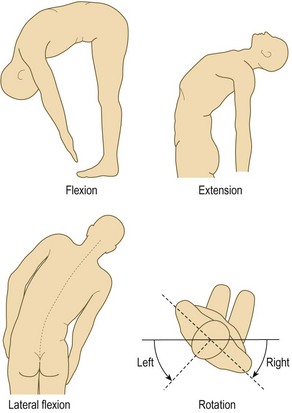
Flexion: ask the patient to try to touch his toes with his legs straight. Record how far down his legs he can reach. Some of this movement depends on hip flexion. Usually the upper segments flex before the lower ones, and this progression should be smooth.
Extension: ask the patient to straighten up and lean back as far as possible (normal 10–20° from neutral erect posture).
Lateral flexion: ask him to reach down to each side, touching the outside of the leg as far down as possible while keeping the legs straight (Fig. 14.23).
Examination sequence
Schober’s test for forward flexion
Mark the skin in the midline at the level of the posterior iliac spines (L5), which overlie the sacroiliac joints (Fig. 14.24; mark A).
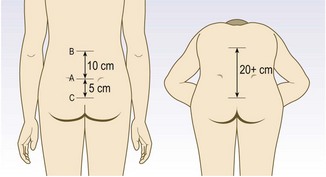
Use a tape measure to draw two more marks: one 10 cm above (mark B) and one 5 cm below this (mark C).
Place the end of the tape measure on the upper mark (B). Ask the patient to touch his toes. The distance from mark B to mark C should increase from 15 to more than 20 cm.
Root compression tests: Intervertebral disc prolapse causing nerve root pressure occurs most often in the lower lumbar region, leading to compression of the corresponding nerve roots.
The femoral nerve (L2–4) lies anterior to the pubic ramus, so straight-leg raising or other forms of hip flexion do not increase its root tension. Problems with the femoral nerve roots may cause quadriceps weakness and/or diminished knee jerk on that side.
The sciatic nerve (L4–5; S1–3) runs behind the pelvis, so manoeuvres to put tension on the lower nerve roots (L4 exiting the L4/5 foramen, L5 exiting the L5/S1 foramen) differ from those for the upper lumbar nerve roots (L2, L3).
Straight-leg raise tests L4, L5, S1 nerve root tension (L3/4, L4/5 and L5/S1 disc prolapse respectively).
Examination sequence
With the patient lying supine, lift the foot to flex the hip passively, keeping the knee straight.
Measure the angle between the couch and the flexed leg to determine any limitation (normal 80–90° hip flexion) caused by thigh or leg pain.
If a limit is reached, raise the leg to just less than this level, and dorsiflex the foot to test for nerve root tension (Fig. 14.25).
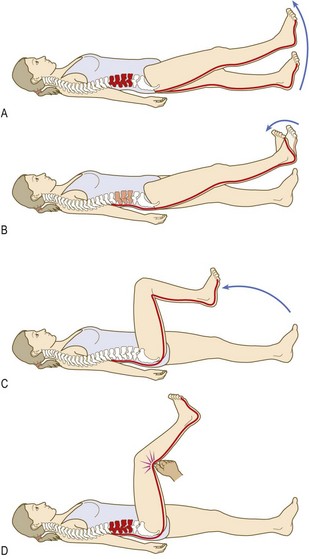
Fig. 14.25 Stretch tests: sciatic nerve. (A) Straight-leg raising limited by tension of root over prolapsed disc. (B) Tension increased by dorsiflexion of foot (Bragard’s test). (C) Root tension relieved by flexion at the knee. (D) Pressure over centre of popliteal fossa bears on posterior tibial nerve, which is ‘bowstringing’ across the fossa, causing pain locally and radiation into the back.
Tibial nerve stretch tests L4–5, S1–3:
Examination sequence
With the patient supine, flex the hip to 90°.
Extend the knee. In this position the tibial nerve ‘bowstrings’ across the popliteal fossa.
Press over either of the hamstring tendons, and then over the nerve in the middle of the fossa. The test is positive if pain occurs when the nerve is pressed, but not the hamstring tendons (Fig. 14.25D).
Femoral nerve stretch tests L2–4:
Examination sequence
With the patient lying on his front (prone), flex the knee and extend the hip (Fig. 14.26). This stretches the femoral nerve. A positive result is pain felt in the back, or the front of the thigh. This test can, if necessary, be performed with the patient lying on his side (with the test side uppermost).
Flip test for functional overlay:
Examination sequence
Ask the patient to sit on the end of the couch with the hips and knees flexed to 90° (Fig. 14.27A).
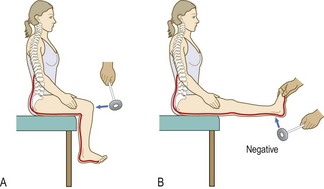
Fig. 14.27 Sciatic nerve. The ‘flip’ test. (A) Divert the patient’s attention to the tendon reflexes. (B) The patient with physical nerve root compression cannot permit full extension of the leg.
Extend the knee, as if to examine the ankle jerk. A patient with nerve root impingement will lie back (‘flip’; Fig. 14.27B).
The upper limb
The prime function of the upper limb is to position the hand appropriately in space. This requires shoulder, elbow and wrist movements. The hand may function in both precision and power modes. The intrinsic muscles of the hand allow grip and fine manipulative movements, and the forearm muscles provide power and stability.
Distinguish between systemic and local conditions. Systemic conditions, e.g. rheumatoid arthritis, usually cause pathology at several sites. Differentiate local conditions from referred or radicular pain. Establish whether the condition is inflammatory or not on the pattern of diurnal stiffness and pain.
The hand and wrist
Motor innervation of the hand is shown in Box 14.20. The wrist joint has metacarpocarpal, intercarpal, ulnocarpal and radiocarpal components. There is a wide range of possible movements, including flexion, extension, adduction (deviation towards the ulnar side), abduction (deviation towards the radial side) and the composite movement of circumduction (the hand moves in a conical fashion on the wrist). When examining and documenting the fingers, use their names to avoid confusion (Fig. 14.28). The PIP and DIP joints are hinge joints and allow only flexion and extension. The metacarpophalangeal (MCP) joints allow flexion and extension, and some abduction/adduction that is greatest when the MCP joints are extended.
14.20 Motor innervation of the hand
| Nerve | Muscles supplied |
| Median | Opponens and abductor muscles of the hand and most of the wrist and finger flexors |
| Ulnar | Adductor of thumb, most of lumbricals and interossei |
| Radial | Extensors of wrist and hand |

The history: The patient will often localise complaints of pain, stiffness, loss of function, contractures, disfigurement and trauma. If symptoms are vague or diffuse, consider referred pain or a compressive neuropathy, e.g. median nerve compression as it traverses the carpal tunnel in the wrist, which leads to symptoms and signs of carpal tunnel syndrome (Fig. 14.29). If PIP or MCP joint swelling is prominent consider inflammatory arthritis.
Examination sequence
Seat the patient, facing you, with arms and shoulders exposed. Start examining the hand and fingers first, and move proximally.
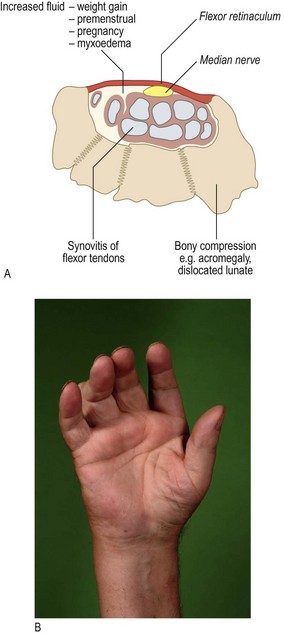
Fig. 14.29 Carpal tunnel syndrome. (A) Causes of median nerve compression. (B) Thenar muscle wasting.
Colour changes including palmar erythema.
Swelling of MCP joints produces loss of interknuckle indentation on the dorsum of the hand, especially when the MCP and IP joints are fully flexed (loss of normal ‘hill–valley–hill–valley’ aspect; Fig. 14.30A). Swelling at the PIP joints produces ‘spindling’ (Fig. 14.30B).

Fig. 14.30 Hand and wrist swelling. (A) Ask the patient to make a fist. Look at it straight on to detect any loss of ‘hill and valley’. (B) Squaring of the wrist due to osteophytes at the carpometacarpal joint of the thumb.
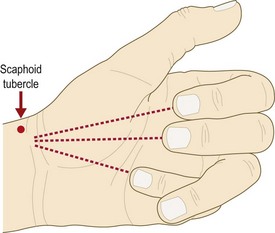
Deformity of phalangeal fractures may produce rotation. Ask the patient to flex the fingers together (Fig. 14.31) and then in turn. Normally, with the MCP and IP joints flexed, the fingers should not cross, and should point to the scaphoid tubercle in the wrist.
Small muscle wasting, especially of the interossei in inflammatory arthritis (T1 nerve root lesion or ulnar nerve palsy).
Vasculitis of the fingers, most commonly detected in the nail folds (Fig. 4.15E).
Nail changes, e.g. pitting (psoriasis) and onycholysis (loosening of the nail from its bed) in psoriatic arthritis (Fig. 4.15B).
Hard swellings are bony; soft swelling suggests synovitis.
Palpate above and below the IP joints with your thumb and index finger to detect sponginess.
Test the MCP joints by examining for sponginess and squeeze gently across them for pain.
Palpate the flexor tendon sheaths in the hand and fingers to detect local swellings or tenderness. If you detect any swelling (usually just proximal to the MCP joints), ask the patient to flex and then extend the finger and see if there is triggering or ‘locking’.
Feel for crepitus. Place your index finger across the fully extended fingers and ask the patient to open and close the fingers.
Move each finger through flexion and extension and notice any triggering.
Ask the patient to put the palms of his hands together and extend the wrists fully – the ‘prayer sign’ (normal is 90° of extension) (Fig. 14.32A).
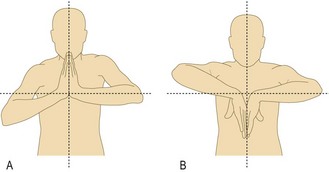
Fig. 14.32 Assessing the wrist. (A) Extension. (B) Flexion. Reduced range of movement at right wrist.
Ask the patient to put the backs of his hands together and flex the wrists fully – the ‘reverse prayer sign’ (normal 90° of flexion) (Fig. 14.32B).
Look: Erythema suggests acute inflammation caused by soft-tissue infection, septic arthritis, tendon sheath infection or crystalopathy (gout and pseudogout). Swelling at the MCP and/or IP joints suggests synovitis. Spindling is typically seen in rheumatoid arthritis and collateral ligament injuries (Box 14.21).
The fingers are long in Marfan’s syndrome (arachnodactyly; Fig. 3.28B).
At the DIP joints (Fig. 14.33), a ‘mallet’ finger is a flexion deformity which is passively correctable. This is usually caused by minor trauma disrupting the terminal extensor expansion at the base of the distal phalanx, with or without bony avulsion.
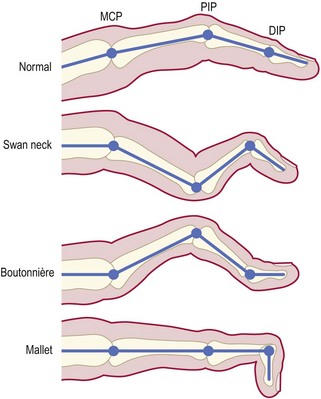
Fig. 14.33 Deformities of the finger in rheumatoid arthritis. MCP, metacarpophalangeal; PIP, proximal interphalangeal; DIP, distal interphalangeal.
Boutonnière (or buttonhook) deformity is a flexion deformity at the PIP joint with hyperextension at the DIP joint and fixed flexion at the PIP joint (Fig. 14.33). ‘Swan neck’ deformity is hyperextension at the PIP joint with flexion at the DIP joint.
There may be subluxation and ulnar deviation of the MCP joints in rheumatoid arthritis (Fig. 14.34). Dupuytren’s contracture affects the palmar fascia, resulting in the MCP and PIP joints of the little and ring fingers becoming fixed in flexion (Fig. 3.13). Anterior (or volar) displacement (partial dislocation) of the wrist may be seen in rheumatoid arthritis.

Feel: Hard swellings may be due to osteophytes (characteristic of osteoarthritis), mucous cysts or, rarely, tumours. Heberden’s and Bouchard’s nodes occur at the DIP and PIP joints respectively.
Sponginess suggests synovitis. Swelling, tenderness and crepitus are found over the tendon sheaths of abductor pollicis longus and extensor pollicis brevis in De Quervain’s tenosynovitis. Symptoms are aggravated by movements at the wrist and thumb. Crepitus at this site is often felt as a creaking sensation and may even be audible. Crepitus may also occur with movement of the radiocarpal joints in osteoarthritis, most commonly secondary to old scaphoid or distal radial fractures.
Examining the wrist and hand with a wound: Test the tendons, nerves and circulation in a patient with a wrist or hand wound. The wound site and the hand position at the time of injury can suggest the structures that are possibly damaged. However, normal movement may still be possible, even with 90% division of a tendon, so surgical exploration is needed for correct diagnosis and treatment. Sensory aspects of nerve injury are covered on page 271.
Examination sequence
Flexor digitorum profundus: ask the patient to flex the DIP joint while you hold the PIP joint in extension (Fig. 14.35A).
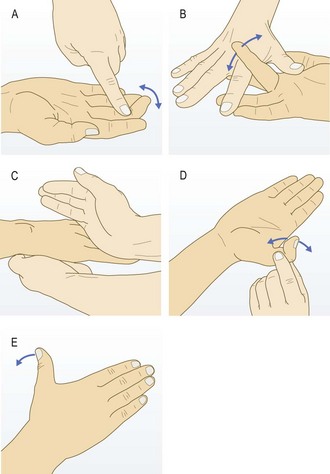
Fig. 14.35 Testing the flexors and extensors of the fingers and thumb. (A) Flexor digitorum profundus. (B) Flexor digitorum superficialis. (C) Extensor digitorum. (D) Flexor pollicis longus. (E) Extensor pollicis longus.
Flexor digitorum superficialis: hold the other fingers fully extended (to eliminate the action of flexor digitorum profundus, as it can also flex the PIP joint) and ask the patient to flex the PIP joint in question (Fig. 14.35B).
Extensor digitorum: ask the patient to extend the fingers with the wrist in the neutral position (Fig. 14.35C).
Flexor and extensor pollicis longus: hold the proximal phalanx of the patient’s thumb firmly and ask him to flex and extend the IP joint (Fig. 14.35D).
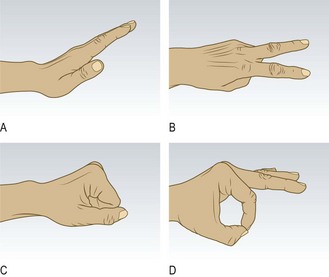
Extensor pollicis longus: ask the patient to place his palm on a flat surface and to extend his thumb like a hitch-hiker (Fig. 14.35E). If the tendon is intact, the patient will be able to do this. Pain occurs in De Quervain’s disease.
Nerves (radial, ulnar and median motor function only)
Use ‘Paper – scissors – stone – OK’ as an aide-mémoire.
Fully extend the wrist and fingers (‘paper sign’) (Fig. 14.36A).
The radial nerve supplies the wrist and finger extensors.
Make the ‘scissors sign’ (Fig. 14.36B).
The ulnar nerve supplies the hypothenar muscles, interossei, two medial lumbricals, adductor pollicis, flexor carpi ulnaris and the ulnar half of flexor digitorum profundus.
Clench the fist fully (‘stone sign’) (Fig. 14.36C).
The median nerve supplies the thenar muscles that abduct and oppose the thumb, the lateral two lumbricals, the medial half of flexor digitorum profundus, flexor digitorum superficialis, flexor carpi radialis, palmaris longus and pronator teres. Because of inconstant cross-over in the nerve supply to the thenar eminence muscles other than abductor pollicis brevis, the best test of median nerve motor function is the ability to abduct the thumb away from the palm (Fig. 14.37). However, clenching a fist fully (‘rock’ sign) also depends on median function because of its flexor supply.
Make the ‘OK’ sign (Fig. 14.36D).
The anterior interosseous nerve (commonly injured in supracondylar fractures) is a purely motor terminal branch of the median nerve. It supplies flexor pollicis longus, the index finger flexor digitorum profundus and pronator quadratus. Making the OK sign depends on both flexor pollicis longus and index finger flexor digitorum profundus functioning.
The elbow
Anatomy: The elbow joint has humero-ulnar, radio-capitellar and superior radio-ulnar articulations. The medial and lateral epicondyles are the flexor and extensor origins respectively for the forearm muscles. These two prominences and the tip of the olecranon are easily palpated. They normally form an equilateral triangle when the elbow is flexed to 90°, and lie in a straight line when the elbow is fully extended. A subcutaneous bursa overlies the olecranon and may become inflamed or infected (bursitis). Elbow pain may be localised or referred from the neck. Rheumatoid arthritis and epicondylitis commonly cause elbow pain.
Examination sequence
The bony contours of the lateral and medial epicondyles and olecranon tip, defining an equilateral triangle with the elbow flexed at 90°.
For sponginess on either side of the olecranon and ask about tenderness. Synovitis feels spongy or boggy when the elbow is fully extended.
Focal tenderness, over the lateral or medial epicondyle. When isolated to one site, this may indicate ‘tennis’ (lateral) or ‘golfer’s’ (medial) elbow.
For bursae, fluid-filled sacs which are usually soft, but if acutely inflamed or infected may be firm.
For rheumatoid nodules on the proximal extensor surface of the forearm.
Assess the extension–flexion arc: ask the patient to touch his shoulder on the same side and then straighten the elbow as far as possible. The normal range of movement is 0–145°; a range less than 30–110° will cause functional problems.
Assess supination and pronation: ask the patient to put his elbows by the side of the body and flex them to 90°. Now ask him to turn the hands upwards to face the ceiling (supination: normal range 0–90°) and then downwards to face the floor (pronation: normal range 0–85°).
The shoulder
Anatomy: The shoulder joint consists of the glenohumeral joint and the acromioclavicular joint, but movement also occurs between the scapula and the posterior chest wall (see Fig. 14.42). Movements of the shoulder girdle, especially abduction and rotation, also produce movement at the sternoclavicular joint. The rotator cuff muscles are supraspinatus, subscapularis, teres minor and infraspinatus. They and their tendinous insertions help stability and movement (especially abduction; Fig. 14.7) at the glenohumeral joint.
Symptoms and definitions: Pain is common (Boxes 14.22 and 14.23) and frequently referred to the upper arm. Glenohumeral pain may occur over the anterolateral aspect of the upper arm. Pain felt at the shoulder may be referred from the cervical spine, radicular pain caused by central nerve root compression, or diaphragm and subdiaphragmatic peritoneum via the phrenic nerve. The most common cause of referred pain is cervical spondylosis, where disc space narrowing and osteophytes cause nerve root impingement and inflammation.
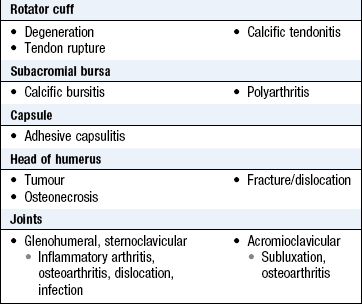
Stiffness and limitation of movement around the shoulder, caused by adhesive capsulitis of the glenohumeral joint, are common after immobilisation or disuse following injury or stroke. This is a ‘frozen shoulder’. However, movement can still occur between the scapula and chest wall.
Some rotator cuff disorders, especially impingement syndromes and tears, present with a painful arc where abduction of the arm between 60 and 120° causes discomfort (Fig. 14.38).
Examination sequence
Ask the patient to sit or stand and expose the shoulder completely.
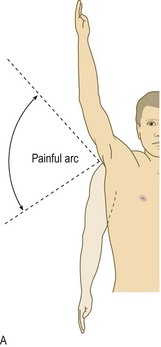
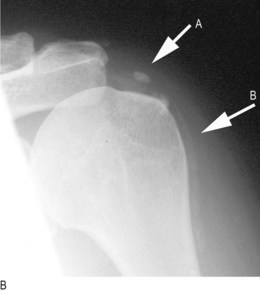
Fig. 14.38 (A) Painful arc. (B) Calcific deposits in supraspinatus (arrow A) and biceps tendons (arrow B).
Examine from the front and the back and in the axilla for:
deformity: the deformities of anterior glenohumeral and complete acromioclavicular joint dislocation are obvious (Figs 14.39 and 14.40), but the shoulder contour in posterior glenohumeral dislocation may only appear abnormal when you stand above the seated patient and look down on the shoulder


muscle wasting: especially of the deltoid, supraspinatus and infraspinatus. Wasting of supraspinatus or infraspinatus indicates a chronic tear of their tendons
the size and position of the scapula, i.e. elevated, depressed or ‘winged’ (Fig. 14.41).

Feel from the sternoclavicular joint along the clavicle to the acromioclavicular joint.
Palpate the acromion and coracoid (2 cm inferior and medial to the clavicle tip) processes, the scapula spine and the biceps tendon in the bicipital groove.
Extend the shoulder to bring supraspinatus anterior to the acromion process. Palpate the supraspinatus tendon.
To screen for shoulder dysfunction:
Ask the patient to put both hands behind the head.
Then put the arms down and reach behind his back to touch the shoulder blades.
If there is pain, swelling or limitation of movement, proceed to examine the shoulder fully.
First assess active movement, then passive.
Ask the patient to flex and extend the shoulder as far as possible.
Abduction: ask the patient to lift his arm away from his side.
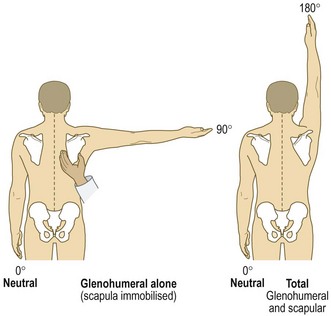
Palpate the inferior pole of the scapula between your thumb and index finger to detect scapular rotation and determine how much movement occurs at the glenohumeral joint. In all, 50–70% of abduction occurs at the glenohumeral joint (the rest with movement of the scapula on the chest wall). This increases if the arm is externally rotated. Note the degree and smoothness of scapular movement. If the glenohumeral joint is excessively stiff, movement of the scapula over the chest wall will predominate. If there is any limitation or pain (painful arc) associated with abduction, test the rotator cuff (Fig. 14.42).
Internal rotation: with the patient’s arm by his side and the elbow flexed at 90°, ask him to put his hand behind his back and feel as high up the spine as possible. Document the highest spinous process that he can reach with the thumb.
External rotation: in the same position with the elbow tucked against his side, ask him to rotate the hand out.
Deltoid: ask the patient to abduct the arm out from his side, parallel to the floor, and resist while you push down on the humerus. Compare each side.
Passively abduct the patient’s arm fully
Ask him to lower (adduct) it slowly (Fig. 14.38).
Pain occurring between 60 and 120° of abduction occurs in painful arc.
If the patient cannot initiate abduction, place your hand over the scapula to confirm there is no scapular movement.
Pain on active movement, especially against resistance, suggests impingement.
Ligamentous tears and injuries
Discrepancy between active and passive ranges suggests a tendinous tear – in particular subscapularis, where there may be an excessive range of passive internal rotation. To test the component muscles of the rotator cuff, it is necessary to neutralise the effect of other muscles crossing the shoulder.
Subscapularis and pectoralis major (internal rotation of the shoulder):
To isolate subscapularis, test internal rotation with the patient’s hand behind his back. Loss of power suggests a tear. Pain on forced internal rotation suggests tendonitis.
Supraspinatus. With the arm by his side, test abduction. Loss of power suggests a tear. Pain on forced abduction at 60° suggests tendonitis.
Infraspinatus and teres minor. Test external rotation with the arm in the neutral position, and 30° flexion to reduce the contribution of deltoid. Loss of power suggests a tear. Pain on forced external rotation suggests tendonitis.
The lower limb
Anatomy: The hip is a ball-and-socket joint and allows flexion, extension, abduction, adduction, internal/external rotation and the combined movement of circumduction. With age, the most common restrictions in movement are extension and internal rotation, followed by abduction.
Symptoms and definitions: Pain is usually felt in the groin, but can be referred to the anterior thigh, the knee or buttock. Hip pain is usually aggravated by activity, but osteonecrosis and tumours may be painful at rest and at night. Lateral hip or thigh pain, aggravated when lying on that side, suggests trochanteric bursitis.
Distinguish pain arising from the hip from:
• lumbar nerve root irritation (pp. 336-7)
• spinal or arterial claudication (p. 128)
• abdominal causes, e.g. hernias (p. 188).
Find out how the pain restricts activities. Ask about walking in terms of the time and distance the patient manages outside the house and up and down stairs, whether he does his own shopping and which walking aids he uses.
Fracture of the neck of femur is common following relatively minor trauma in postmenopausal women and those over 70 years. The fracture may be minimally displaced or impacted and need not have the classical appearance of a shortened, externally rotated leg (Fig. 14.43A). The patient may even be able to weight-bear.
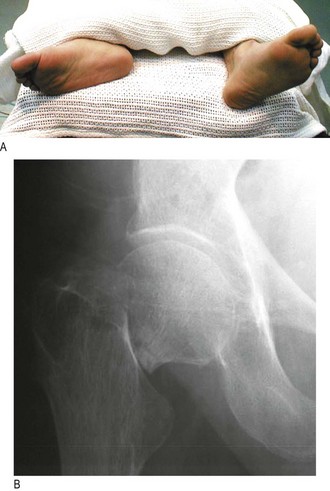
Fig. 14.43 Fracture of neck of right femur. (A) Shortening and external rotation of the leg. (B) X-ray showing translation and angulation.
Examination sequence
Patients should undress to their underwear and remove socks and shoes. You should be able to see the iliac crests.
Assess gait (p. 331).
General inspection: ask the patient to stand.
From the front, observe whether the:
shoulders are parallel to the ground and symmetrically over the pelvis (which may mask a hip deformity or true shortening of one leg)
hip, knee, ankle or foot are deformed
muscles are wasted (from polio or disuse secondary to arthritis).
From the side, assess for a stoop or increased lumbar lordosis (both may result from a flexion contracture).
the spine is straight or curved laterally (scoliosis)
there is scoliosis: note the relative positions of the shoulders and pelvis, and measure leg lengths
Look for scars, sinuses, dressings or skin changes around the hip.
With the patient face-up on the couch, check the pelvic brim is perpendicular to the spine.
Flexion: place your left hand under the back (to detect any masking of hip movement by movement of the pelvis and lumbar spine, use Thomas’s test) and check the range of flexion of each hip in turn (normal 0–120°).
Abduction and adduction: stabilise the pelvis by placing your left hand on the opposite iliac crest. With your right hand abduct the leg until you feel the pelvis start to tilt (normal 45°). Test adduction by crossing one of the patient’s legs over the other and continuing to move it medially (normal 25°) (Fig. 14.44A).
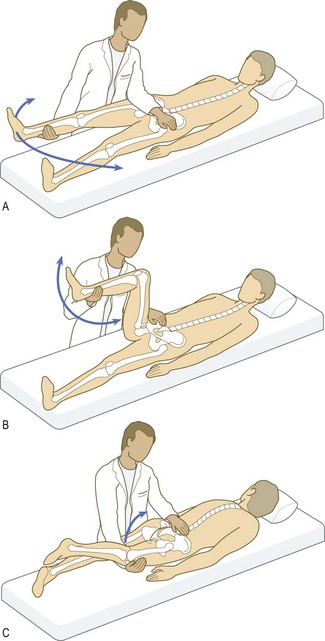
Internal and external rotation: with the leg in full extension, roll it on the couch and watch the foot to indicate the range of rotation. Test with the knee (and hip) flexed at 90°. Move the foot medially to test external rotation and laterally to test internal rotation (normal 45° for each movement) (Fig. 14.44B).
Extension: ask the patient to lie face-down on the couch. Place your left hand on the pelvis to detect any movement. Lift each leg in turn to assess the range of extension (normal range 0–20°) (Fig. 14.44C).
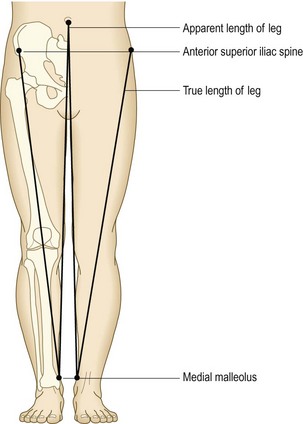
Shortening: Shortening occurs in hip and other lower limb conditions (Box 14.24). Apparent shortening is present if the affected limb appears shortened, usually because of an adduction or flexion deformity at the hip.
14.24 Causes of true lower limb shortening
Examination sequence
Ask the patient to lie supine and stretch both legs out as far as possible equally to eliminate any soft-tissue contracture/abnormal posture.
from umbilicus to medial malleolus: the apparent length
from anterior superior iliac spine to medial malleolus: the ‘true length’ (Fig. 14.45).
Examination sequence
Stand in front of the patient.
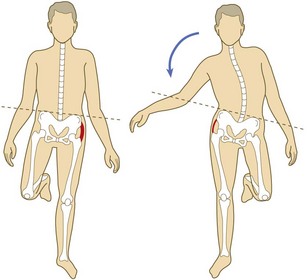
Palpate both iliac crests and ask him to stand on one leg for 30 seconds.
Watch and feel the iliac crests to see which moves up or down.
Normally, the iliac crest on the side with the foot off the ground should rise. The test is abnormal if the hemipelvis falls below the horizontal (Fig. 14.46). It may be caused by gluteal weakness or inhibition from hip pain, e.g. osteoarthritis, or structural abnormality of the hip joint, e.g. coxa vara or developmental hip dysplasia.
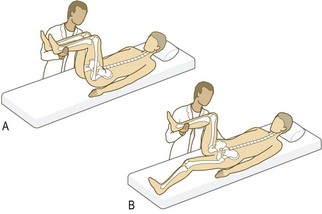
Thomas’s test: This measures fixed flexion deformity (incomplete extension), which may be masked by compensatory movement at the lumbar spine or pelvis and increasing lumbar lordosis.
Do not perform the test if the patient has a hip replacement on the non-test side, as forced flexion may cause dislocation.
Examination sequence
Ask the patient to lie supine on the couch.
Place your left hand palm upwards under the lumbar spine.
Passively flex both legs (hips and knees) as far as possible.
Keep the non-test hip maximally flexed and by feeling with your left hand confirm that the lordotic curve of the lumbar spine remains eliminated.
Ask the patient to extend the test hip. Incomplete extension in this position indicates a fixed flexion deformity at the hip (Fig. 14.47).
If the contralateral hip is not flexed enough, lumbar lordosis will not be eliminated and fixed flexion deformity of the ipsilateral knee confuses the issue. In this case, perform the test with the patient lying on his side.
The knee
Anatomy: The knee is a complex hinge joint with tibio-femoral and patello-femoral components. It has a synovial capsule that extends under the quadriceps (the suprapatellar pouch), reaching 5 cm above the superior edge of the patella. The joint is largely subcutaneous, allowing easy palpation of the patella, tibial tuberosity, patellar tendon, tibial plateau margin and femoral condyles. The knee depends on its muscular and ligamentous structures for stability (Fig. 14.48).
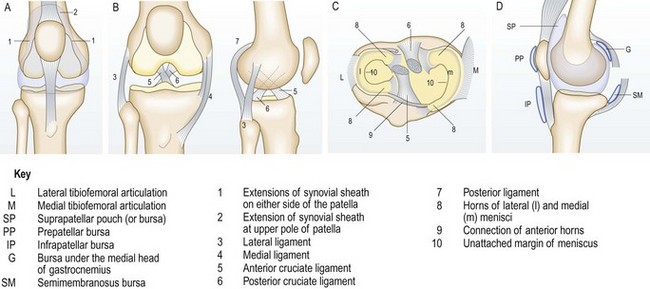
Fig. 14.48 Structure of the right knee. (A) Anterior view, showing the common synovial sheath. (B) Anterior and lateral views, showing the ligaments. (C) Plan view of the menisci. (D) Bursae. G, bursa under the medial head of gastrocnemius; IP, infrapatellar bursa; L, lateral tibio-femoral articulation; M, medial tibio-femoral articulation; P, patello-femoral articulation; PP, prepatellar bursa; SM, semimembranosus bursa; SP, suprapatellar pouch (or bursa).
The hamstring muscles flex the knee. Extension requires the quadriceps muscles, quadriceps tendon, patella, patellar tendon and tibial tuberosity. Any disruption of this ‘extensor apparatus’ prevents straight-leg raising or produces an extensor lag (a difference between active and passive ranges of extension).
The medial and lateral collateral ligaments resist valgus and varus stress respectively. The anterior cruciate ligament prevents anterior subluxation of the tibia on the femur, and the posterior cruciate ligament resists posterior translation. The medial and lateral menisci are crescentic fibrocartilaginous structures that lie between the tibial plateaus and the femoral condyles. There are several important bursae around the knee:
• anteriorly: the suprapatellar, prepatellar (between the patella and the overlying skin) and infrapatellar bursae (between the skin and the tibial tuberosity/patellar ligament)
• posteriorly: several bursae lie in the popliteal fossa (Fig. 14.48D).
Pain: In trauma, take a detailed history of the injury mechanism. The direction of impact, load and deformation predict what structures are injured. Remember that pain in the knee may be referred from the hip. Anterior knee pain, particularly after prolonged sitting or going downstairs, suggests patellofemoral joint pathology.
Swelling: The normal volume of synovial fluid is 1–2 ml and is clinically undetectable. An effusion (collection of fluid within the joint space) indicates intra-articular pathology. It may be due to synovial fluid, blood, pus or a mixture of these fluids.
Haemarthrosis (bleeding into the knee) is caused by injury to a vascular structure within the joint, e.g. torn cruciate ligament or intra-articular fracture. Patients with a coagulation disorder, e.g. haemophilia or on anticoagulant therapy, are particularly prone to haemarthroses. The menisci are predominantly avascular, and unless torn at their periphery or in conjunction with some other internal derangement, do not cause a haemarthrosis.
In acute injury the speed of onset of swelling is a clue to the diagnosis.
• Rapid (<30 minutes), severe swelling suggests a haemarthrosis.
• Swelling of a lesser degree over 24 hours is more suggestive of traumatic effusion, e.g. meniscal tear.
• Septic arthritis develops over a few hours with pain, marked swelling, tenderness, redness and extreme reluctance to move the joint actively or passively. Concurrent oral steroid or non-steroidal anti-inflammatory drug therapy modifies these features.
• Crystal-induced arthritis (gout or pseudogout) can mimic septic arthritis. Confirm the diagnosis by looking at aspirated fluid under polarised light microscopy.
Locking: This is a block to full extension. It may be longstanding or intermittent. The two common causes are a loose body, e.g. from osteochondritis dissecans, osteoarthritis or synovial chondromatosis, and a meniscal tear. Bucket handle and anterior beak meniscal tears are especially associated with locking. Posterior horn tears commonly cause pain on extreme flexion and prevent the last few degrees of flexion. Meniscal tears also cause local joint line tenderness. Congenital discoid meniscus may present with locking and clunking.
Instability (‘giving way’): Any of the four main ligaments may rupture from trauma or become incompetent with degenerative disease. Because the normal knee has a valgus angle the patella is prone to dislocate laterally.
Examination sequence
Observe the patient walking and standing, as for gait.
Note scars, sinuses, erythema or rashes.
Posture and common deformities, genu valgum (knock knee) or genu varum (bow legs).
Muscle wasting: quadriceps wasting is almost invariable with inflammation or chronic pain and develops within days. Measure the thigh girth in both legs 20 cm above the tibial tuberosity.
Leg length discrepancy (Fig. 14.45).
Flexion deformity: if the patient lies with one knee flexed, this may be caused by a hip, knee or combined problem.
Swelling: an enlarged prepatellar bursa (housemaid’s knee) and any knee joint effusion. Large effusions form a horseshoe-shaped swelling above the knee. Swelling extending beyond the joint margins suggests infection, major injury or, rarely, tumour.
Warmth: feel the skin, comparing both sides.
With the patient’s knee extended, empty the suprapatellar pouch by sliding your left hand down the thigh until you reach the upper edge of the patella.
Keep your hand there and, with the fingertips of your right hand, press down briskly and firmly over the patella (Fig. 14.49).
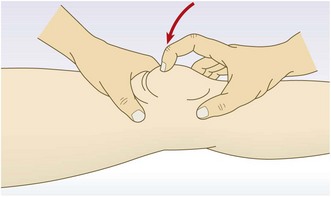
In a moderate-sized effusion you will feel a tapping sensation as the patella strikes the femur. You may feel a fluid impulse in your left hand.
The ‘bulge or ripple test’ (Fig. 14.50):
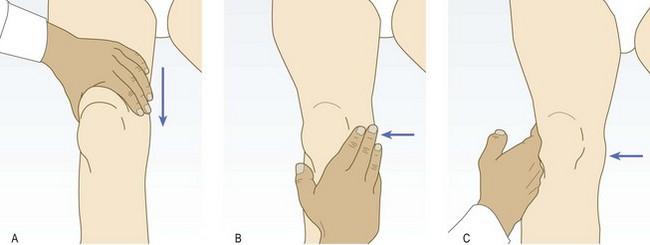
Fig. 14.50 The bulge or ripple test. (A) Empty the suprapatellar pouch, as for the patellar tap test. (B) Stroke the medial side of the joint to displace excess fluid to the lateral side of the joint. (C) Stroke the lateral side while watching the medial side closely for a bulge or ripple as fluid reaccumulates. This test may be negative if the effusion is tense.
With the patient’s knee extended and the quadriceps muscles relaxed, empty the medial side of the joint by milking the fluid to the suprapatellar pouch.
Now empty the suprapatellar pouch as for the patellar tap. Stroke the lateral side of the joint. Watch the medial side for a bulge or ripple as fluid reaccumulates on that side.
Synovitis: with the knee extended and the quadriceps relaxed, feel for sponginess on both sides of the quadriceps tendon.
Joint lines: feel the tibial and femoral joint lines. If there is tenderness, localise this as accurately as possible. In adolescents, localised tibial tuberosity tenderness suggests Osgood–Schlatter disease, a traction osteochondritis.
With the patient supine, ask him to flex his knee up to the chest and then extend the leg back down to lie on the couch (normal range 0–140°).
Feel for crepitus between the patella and femoral condyles, suggesting chondromalacia patellae (more common in younger female patients) or osteoarthritis.
Record the range of movement: if there is a fixed flexion deformity of 15° and flexion is possible to 110°, record this as a range of movement of 15–110°.
Ask the patient to lift the leg, keeping it straight. If the knee cannot be kept fully extended an extensor lag is present, indicating quadriceps weakness or other abnormality of the extensor apparatus.
Passive flexion and extension:
Normally the knee can extend so that the femur and tibia are in longitudinal alignment. Record full extension as 0°. A restriction to full extension occurs with meniscal tears, osteoarthritis and inflammatory arthritis. To assess hyperextension, lift both legs by the feet. Hyperextension (genu recurvatum) is present if the knee extends beyond the neutral position. Up to 10° is normal (Box 14.25).
Collateral ligament: With the knee fully extended, abduction or adduction should not be possible. If either ligament is lax or ruptured, movement can occur. If the ligament is strained (partially torn) but intact, pain will be produced but the joint will not open.
Examination sequence
With the patient’s knee fully extended, hold the ankle between your elbow and side. Use both hands to apply a valgus and then varus force to the knee.
Use your thumbs to feel the joint line and assess the degree to which the joint space opens. Major opening of the joint indicates collateral and cruciate injury (Fig. 14.51A).
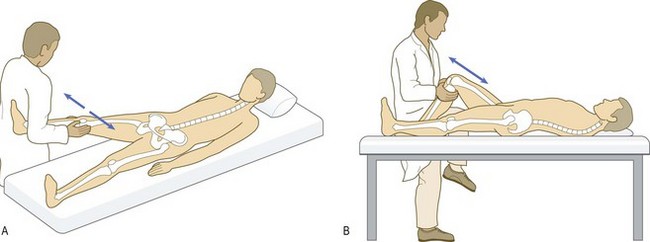
If the knee is stable, repeat the process with the knee flexed to 30° to assess minor collateral laxity. In this position the cruciate ligaments are not taut.
Flex the patient’s knee to 90° and maintain this position by sitting with your thigh trapping the patient’s foot.
Check that the hamstring muscles are relaxed and look for posterior sag (posterior subluxation of the tibia on the femur). This causes a false-positive anterior drawer sign which should not be interpreted as anterior collateral ligament laxity.
With your hands behind the upper tibia and both thumbs over the tibial tuberosity, pull the tibia anteriorly (Fig. 14.51B). Significant movement (compare with the opposite knee) indicates that the anterior cruciate ligament is lax. Movement of >1.5 cm suggests anterior cruciate ligament rupture. There is often an associated medial ligament injury.
Tests for meniscal tears: Meniscal tears in younger sporty patients usually result from twisting injury to the flexed weight-bearing leg. In middle-aged patients, degenerative horizontal cleavage of the menisci is common, with no history of trauma. Meniscal injuries commonly cause small effusions, especially on weight bearing or after exercise. Associated localised joint line tenderness is common.
Examination sequence
Ask the patient to lie face-up on the couch. Test the medial and lateral menisci in turn.
Passively flex the knee to its full extent.
Externally rotate the foot and abduct the upper leg at the hip, keeping the foot towards the midline (i.e. creating a varus stress at the knee).
Extend the knee smoothly. In medial meniscus tears a click or clunk may be felt or heard, accompanied by discomfort.
Ask the patient to squat, keeping his feet and heels flat on the ground. If he cannot do this, there is incomplete knee flexion on the affected side. This may be caused by a tear of the posterior horn of the menisci.
Test the extreme range of knee flexion with the patient face-down on the couch, which makes comparison with the contralateral side easy.
The ankle and foot
Anatomy: The ankle is a hinge joint. The talus articulates with a three-sided mortise made up of the tibial plafond and the medial and lateral malleoli. This allows dorsiflexion and plantar flexion, although some axial rotation can occur at the plantar-flexed ankle. During dorsiflexion the trochlea of the talus rocks posteriorly in the mortise and the malleoli are forced apart because the superior articular surface of the talus is wider anteriorly than posteriorly. The bony mortise is the major factor contributing to stability but the lateral, medial (deltoid) and inferior tibiofibular ligaments are also important (Fig. 14.52).
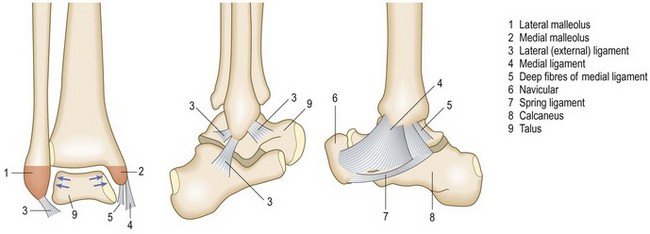
Foot movements are inversion and eversion, and principally occur at the mid-tarsal (talo-navicular/calcaneo-cuboid) and subtalar (talo-calcaneal) joints. Toe movements are dorsiflexion and plantar flexion.
Trauma: A ‘twisted’ ankle is very common, and is usually related to a sporting injury or stepping off a kerb or stair awkwardly. Establish the exact mechanism of injury and the precise site of pain. Frequently there has been a forced inversion injury stressing the lateral ligament. A sprain occurs when some fibres are torn but the ligament remains structurally intact. A complete ligament tear allows excessive talar movement in the ankle mortise with instability.
Achilles tendon rupture (see Fig. 14.55) is associated with attempted sudden plantar flexion at the ankle. It is common in middle-aged patients doing unaccustomed activity, e.g. badminton, squash or the fathers’ race at sports day, and is associated with some drug therapy, e.g. oral steroids, fluoroquinolone antibiotics. Sudden pain occurs above the heel and there is often a sensation or noise of a crack. Patients may feel as if they have been kicked or even shot.

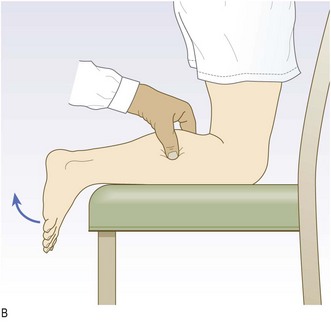
Fig. 14.55 Ruptured Achilles tendon. (A) The arrow indicates the site of a palpable defect in the Achilles tendon. (B) Thomson’s test. Failure of the foot to plantar flex when the calf is squeezed is pathognomonic of an acute rupture of the Achilles tendon.
Forefoot pain, often localised to the second metatarsal, after excessive activity such as trekking, marching or dancing, suggests a stress fracture (Fig. 14.53). Symptoms are relieved by rest and aggravated by weight bearing. X-rays in the first week may be normal.

Non-traumatic conditions: Anterior metatarsalgia with forefoot pain is common, especially in middle-aged women. Acute joint pain with swelling suggests an inflammatory arthropathy such as rheumatoid arthritis or gout. The forefoot is commonly affected in rheumatoid arthritis. In severe cases the metatarsal heads become prominent and walking feels like ‘walking on pebbles or broken glass’.
Plantar surface heel pain that is worse in the foot-strike phase of walking may be due to plantar fasciitis and tends to affect middle-aged patients and those with seronegative arthritides.
Posterior heel pain may be caused by Achilles tendonitis.
Spontaneous lancinating pain in the forefoot radiating to contiguous sides of adjacent toes occurs with Morton’s neuroma. A common site is the interdigital cleft between the third and fourth toes. This occurs predominantly in women aged 25–45 years and is aggravated by wearing tight shoes.
Examination sequence
Ask patients to remove their socks and shoes.
Examine the soles of the shoes for abnormal patterns of wear.
Gait: observe (p. 331). Look for:
increased height of step, indicating ‘foot drop’
ankle movement (dorsi/plantar flexion)
position of the foot as it strikes the ground (supinated/pronated)
With the patient standing, observe:
The position of the midfoot, looking particularly at the longitudinal medial arch. This may be flattened (pes planus – flat foot) or exaggerated (pes cavus).
If the arch is flattened, ask the patient to stand on tiptoe. This restores the arch in a mobile deformity, but not in a structural one.
A ‘splay foot’ has widening at the level of the metatarsal heads, often associated with MTP joint synovitis.
Examine the ankle and foot for scars, sinuses, swelling, bruising, callosities (an area of thickened skin at a site of repeated pressure), nail changes, oedema, deformity and position, e.g. fixed plantar flexion or foot drop.
Assess the range of plantar flexion and dorsiflexion at the ankle and inversion/eversion of the foot by asking the patient to perform these movements.
Passive ankle dorsiflexion/plantar flexion:
Grip the heel with the cup of your left hand from below, with the thumb and index finger on the malleoli.
Put the foot through its arc of movement (normal range 15° dorsiflexion to 45° plantar flexion).
If dorsiflexion is restricted, assess the contribution of gastrocnemius (which functions across both knee and ankle joints) by measuring ankle dorsiflexion with the knee extended and flexed. If more dorsiflexion is possible with the knee flexed, this suggests a gastrocnemius contracture.
Passive foot inversion/eversion:
Examine the subtalar joint in isolation by placing the foot into dorsiflexion to stabilise the talus in the ankle mortise.
Move the heel into inversion (normal 20°) and eversion (normal 10°).
Examine the combined mid-tarsal joints by fixing the heel with your left hand and moving the forefoot with your right hand into dorsiflexion, plantar flexion, adduction, abduction, supination and pronation.
Abnormal findings: Hallux valgus is common, familial and may be aggravated by footwear and activities such as ballet dancing (Fig. 14.54). A bunion (a soft-tissue bursal swelling) may develop over the protuberant first metatarsal head and become inflamed or infected. As the condition progresses, the hallux may adduct over the second toe.

Gout of the first MTP joint causes marked redness and soft-tissue swelling. This is followed by peeling of the superficial skin and pain on movement or touch.
Swelling of the entire digit, ‘sausage toe’ (dactylitis), is characteristic of psoriatic arthropathy.
Claw toes result from dorsiflexion (hyperextension) at MTP joints and plantar flexion at PIP and DIP joints. Hammer toes are due to dorsiflexion at MTP and DIP joints and plantar flexion at PIP joints.
Mallet toes describe plantar flexion at DIP joints.
Tenderness on metatarsal compression suggests Morton’s neuroma or, if associated with sponginess, synovitis due to rheumatoid arthritis. If there is toe deformity, assess whether there is impingement on the other toes, e.g. overriding hallux valgus. Pain and stiffness at the first MTP joint suggest hallux rigidus.
Examination sequence
Ask the patient to kneel with both knees on a chair.
Palpate the gastrocnemius and Achilles tendon for focal tenderness and soft-tissue swelling. Achilles tendon rupture is often palpable as a discrete gap in the tendon about 5 cm above the calcaneal insertion (Fig. 14.55A).
Thomson’s (Simmond’s) test: Squeeze the calf just distal to the level of maximum circumference. If the Achilles tendon is intact, plantar flexion of the foot will occur (Fig. 14.55B).
Fractures, dislocations and trauma
A fracture is a breach in the structural integrity of a bone. This may arise in:
• normal bone from excessive force
• normal bone from repetitive load-bearing activity (stress fracture)
• bone of abnormal structure (pathological fracture) (Box 14.26) with minimal or no trauma.

The epidemiology of fractures varies geographically. There is an epidemic of osteoporotic fractures because of increasing elderly populations. Fractures resulting from road traffic accidents and falls are decreasing because of legislative and preventive measures, e.g. seat belts, air bags and improved road engineering.
Osteoporosis is systemic skeletal loss of bone mineral density with associated microarchitectural deterioration. It is the most common cause of abnormal bone structure. The incidence increases with age, particularly in postmenopausal women (Box 14.27). In the absence of complications, osteoporosis is asymptomatic. Although any osteoporotic bone can fracture, common sites are the distal radius (Fig. 14.56), neck of femur (Fig. 14.43), proximal humerus and the spinal vertebrae. Caucasians in Europe have a lifetime risk of osteoporotic fracture of 50% in women and 20% in men.

Fig. 14.56 Colles’ fracture. (A) Clinical appearance of dinner fork deformity. (B) X-ray appearance.
A fracture may occur in the context of severe trauma (Ch. 19). Complications of fractures are shown in Box 14.28.
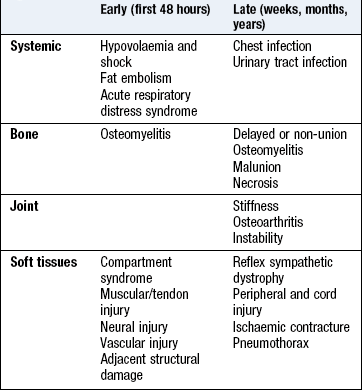
History: Establish the mechanism of injury. For instance, a patient who has fallen from a height on to his heels may have obvious fractures of the calcaneal bones in his ankles but is also at risk of fractures of the proximal femur, pelvis and vertebral column.
Physical examination: Use the Look – Feel – Move approach. Observe patients closely to see if they move the affected part and are able to weight bear.
Examination sequence
See if the skin is intact. If there is a breach in the skin and the wound communicates with the fracture, the fracture is open or compound; otherwise it is closed.
Look for associated bruising, deformity, swelling or wound infection (Fig. 14.57).
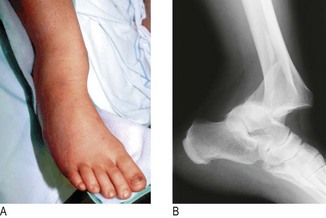
Establish whether the patient can move joints distal and proximal to the fracture.
Do not move a fracture site to see if crepitus is present; this causes additional pain and bleeding (Figs 14.58 and 14.59).

Fig. 14.58 Describing a fracture. The site of the fracture: anatomical divisions. D, diaphysis or shaft; E, epiphysis; EP, epiphyseal plate; M, metaphysis.
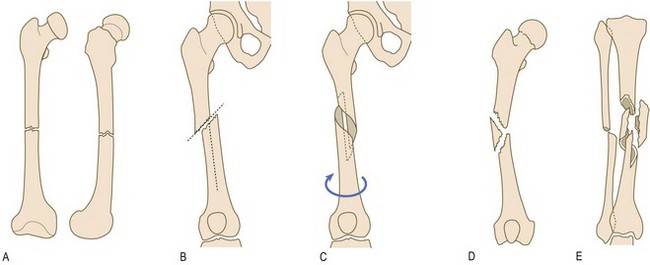
Fig. 14.59 The nature of the fracture. (A) If there is no deformity (no movement of the bone ends relative to one another), the fracture is in anatomical position. (B) Oblique fracture: the fracture runs at an oblique angle of 30° or more. (C) Spiral fracture: simple spiral fractures result from twisting forces. (D) Multifragmentary (comminuted) fracture: there are more than two fragments. (E) Multifragmentary complex fracture: there is no contact between the main fragments after reduction.
Putting it all together
Decide whether joints are affected and establish the mode of onset. If the problem was caused by a major injury follow the system in Chapter 19. Which joints, and are they affected symmetrically? How do the symptoms behave during the day? Ascertain any extra-articular symptoms. The problem may be focal, e.g. lateral epicondylitis of the elbow – ‘tennis elbow’ – medial meniscal tear of the knee, osteoarthritis at the hip, or systemic.
The history and examination direct your investigations and produce a confident diagnosis (Box 14.29).
 14.30
14.30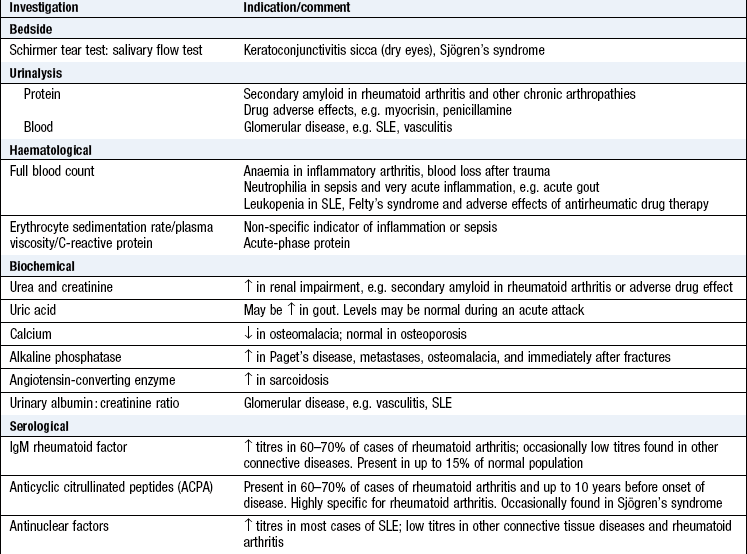
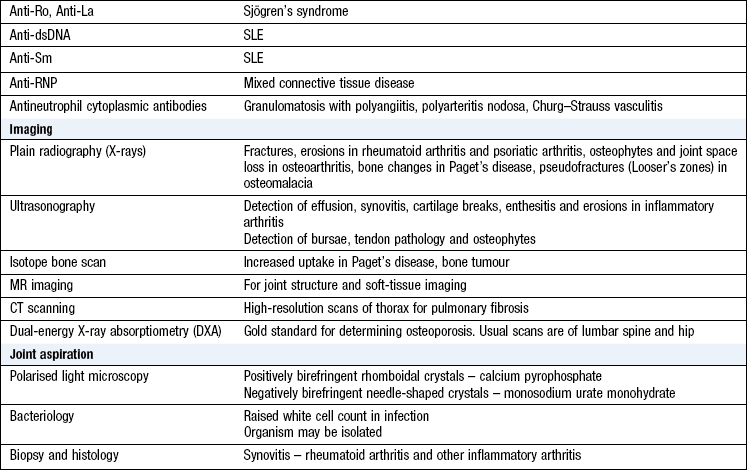
If the joints are not involved, the problem may arise from the surrounding tissues or be referred from another site, e.g. in nerve root impingement. The process may be inflammatory (infective or non-infective) or non-inflammatory. Features of systemic illness, e.g. weight loss, rash, e.g. rheumatoid arthritis, psoriasis or SLE, suggest a systemic cause.
Investigations
See Box 14.30.
14.29 Describing a fracture
• What bone(s) is/are involved?
• Is the fracture open (compound) or closed?
• Is the fracture complete or incomplete?
• Where is the bone fractured (intra-articular/epiphysis/physis/metaphysis/diaphysis)?
• What is the fracture’s configuration (transverse/oblique/spiral/comminuted/butterfly fragment)?
• What components of deformity are present?
• Translation is the shift of the distal fragment in relation to the proximal bone. The direction is defined by the movement of the distal fragment, e.g. dorsal or volar, and is measured as a percentage
• Angulation is defined by the movement of the distal fragment, measured in degrees
• Rotation is measured in degrees along the longitudinal axis of the bone, e.g. for spiral fracture of the tibia or phalanges
• Shortening: proximal migration of the distal fragment can cause shortening in an oblique fracture. Shortening may also occur if there has been impaction at the fracture site, e.g. Colles’ fracture of the distal radius
• Is there distal nerve or vascular deficit?
• What is the state of the tissues associated with the fracture – soft tissues and joints, e.g. fracture blisters, dislocation?