The general examination
The setting for a physical examination
Privacy is essential when you examine a patient. Pulling the curtains around the bed in a ward obscures vision but not sound. Talk quietly but ensure good communication, which may be difficult with deaf or elderly patients (Ch. 2). The room should be warm and well lit. Subtle abnormalities of complexion such as mild jaundice are easier to detect in natural light. The height of the examination couch or bed should be adjustable, with a step to enable patients to get on to it easily. An adjustable backrest is essential, particularly for breathless patients who cannot lie flat.
Seek permission and sensitively, but adequately, expose the areas of the body to be examined; cover the rest of the patient with a blanket or sheet to ensure that he or she does not become cold. Avoid unnecessary exposure and embarrassment. A female patient will appreciate the opportunity to replace her bra after her chest examination before you examine her abdomen. Tactfully ask relatives to leave the room before the physical examination. Sometimes it is appropriate for a relative to remain if the patient is very apprehensive, if you need a translator or if the patient requests it. Parents should always be present when you examine children (Ch. 15).
Always offer a chaperone for any intimate examination to prevent misunderstandings and to provide support and encouragement for the patient (Ch. 2). Record the chaperone’s name and presence. If patients decline the offer, respect their wishes and record this in the notes.
Collect together all the equipment you need before starting the examination (Box 3.1).
Sequence for performing a physical examination
Keep an open mind as you talk with the patient and formulate a differential diagnosis. You may miss the correct diagnosis if you are unduly swayed by early clues in the history, overvalue recent or memorable cases or lean too heavily towards diagnoses that seem to match a pattern. Examine the patient, looking for signs that will confirm or refute your diagnoses.
With experience, you will develop your own style and sequence of physical examination (Box 3.2). There is no single correct way of performing a physical examination. A regular routine reduces errors of omission.
 3.2 A personal system for performing a physical examination
3.2 A personal system for performing a physical examination
The sequence of examination is:
• Auscultation (Fig. 3.1).
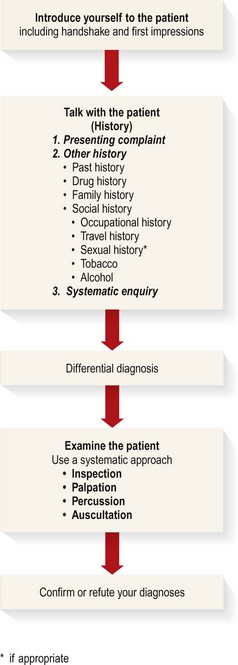
Learn to integrate these smoothly into each component of the physical examination.
First impressions
The physical examination starts as soon as you see the patient. Assess patients’ general demeanour and external appearance, and watch how they rise from their chair and walk into the room.
Gait and posture
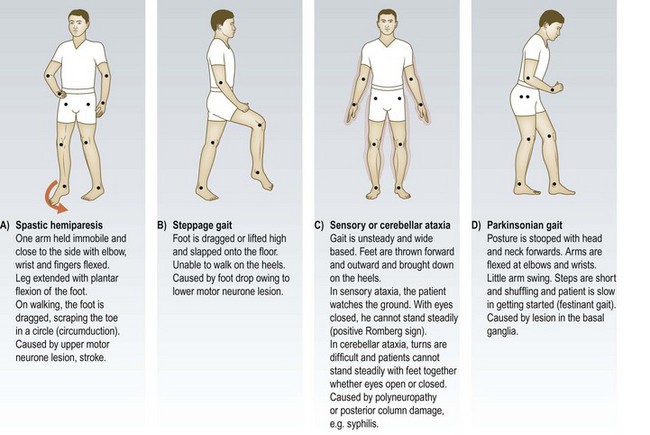
Observe the patient as he walks towards you. The gait may suggest an important neurological or musculoskeletal disorder or provide clues to the patient’s emotions and overall function. Disorders of gait occur because of pain, fixed or immobile joints, muscle weakness or abnormal limb control (Fig. 3.2). If the patient is in bed, look at his posture.
The handshake
Introduce yourself and shake hands. This may provide diagnostic clues (Box 3.3). Greet your patient in a friendly but professional manner. Note if his right hand works; in patients with a right hemiparesis you may need to shake his left hand. Avoid too firm a grip, particularly in patients with arthritis.
 3.3 Information from a handshake
3.3 Information from a handshake
| Features | Diagnosis |
| Cold, sweaty hands | Anxiety |
| Cold, dry hands | Raynaud’s phenomenon |
| Hot, sweaty hands | Hyperthyroidism |
| Large, fleshy, sweaty hands | Acromegaly |
| Dry, coarse skin | Regular water exposure |
| Manual occupation | |
| Hypothyroidism | |
| Delayed relaxation of grip | Myotonic dystrophy |
| Deformed hands/fingers | Trauma |
| Rheumatoid arthritis | |
| Dupuytren’s contracture |
Facial expression and general demeanour
Facial expression and eye-to-eye contact reflect physical and psychological well-being (Box 3.4), but in some cultures direct eye-to-eye contact is impolite. Patients who deliberately self-harm may cover their face with their hands or bedclothes and be reluctant to communicate. Actively recognise the features of anxiety, fear, anger or grief, and explore the reasons for these. Some patients conceal anxieties and depression with inappropriate cheerfulness.
3.4 Abnormal facial expressions
| Features | Diagnosis |
| Poverty of expression | Parkinsonism |
| Startled expression | Hyperthyroidism |
| Apathy, with poverty of expression and poor eye contact | Depression |
| Apathy, with pale and puffy skin | Hypothyroidism |
| Lugubrious expression with bilateral ptosis | Myotonic dystrophy |
| Agitated expression | Anxiety |
| Hyperthyroidism | |
| Hypomania |
Clothing
Clothing gives clues about personality, state of mind and social circumstances. Young people wearing dirty clothes may have problems with alcohol or drug addiction, or be making a personal statement. Unkempt elderly patients with faecal or urinary soiling may be unable to look after themselves because of physical disease, immobility, dementia or other mental illness. Anorectic patients wear baggy clothing to cover weight loss. Consider blood-borne viral infections, e.g. hepatitis B or C, in patients with tattoos. A MedicAlert bracelet (Fig. 3.3) or necklace highlights important medical conditions and treatments.

Complexion
Facial colour depends on oxyhaemoglobin, reduced haemoglobin, melanin and carotene. Unusual skin colours are due to abnormal pigments, e.g. the sallow yellow-brownish tinge in chronic kidney disease. A bluish tinge is produced by abnormal haemoglobins, e.g. sulphaemoglobin or methaemoglobin, or by drugs, e.g. dapsone. Some drug metabolites cause striking abnormal coloration of the skin, particularly in areas exposed to light, e.g. mepacrine (yellow), amiodarone (bluish-grey) and phenothiazines (slate-grey) (Fig. 3.4).
Haemoglobin
Untanned European skin is pink due to the red pigment oxyhaemoglobin in the superficial capillary–venous plexuses. A pale complexion may be misleading but can suggest anaemia (Box 3.5). The pallor of anaemia is best seen in the mucous membranes of the conjunctivae, lips and tongue and in the nail beds (Fig. 3.5). Angular stomatitis (Fig. 3.19B) and koilonychia (spoon-shaped) nails (Fig. 4.15F) can be features of iron deficiency anaemia. Ask about dyspepsia, change in bowel habit and heavy menstrual periods if you are investigating anaemia.
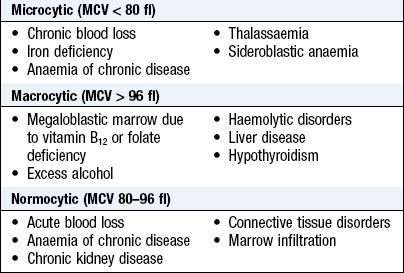

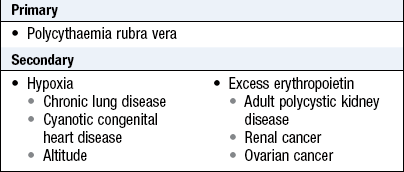
Pallor from vasoconstriction occurs during a faint or from fear. Vasodilatation may produce a pink complexion, even in anaemia. Perimenopausal women may have transient pink flushing, particularly of the face, due to vasodilatation, which may be accompanied by sweating. Facial plethora is caused by raised haemoglobin concentration with elevated haematocrit (polycythaemia) (Box 3.6). Blue sclerae are a sensitive indicator of iron deficiency anaemia.
Cyanosis
Cyanosis is a blue discoloration of the skin and mucous membranes that occurs when the absolute concentration of deoxygenated haemoglobin is increased (Box 3.7). It can be difficult to detect, particularly in black and Asian patients.
 3.7
3.7
Central cyanosis
The minimum arterial level of deoxyhaemoglobin required to detect central cyanosis is 2.38 g/dl. The mean value for detection is 3.48 ± 0.55 g/dl.
Barnett HB, Holland JG, Josenhans WT. When does central cyanosis become detectable? Clin Invest Med 1982;5:39–43. McGee S. Evidence based physical diagnosis, 2nd edn. St Louis, MO: Saunders, Elsevier, 2007, p. 86.
Central cyanosis: This is seen at the lips and tongue (Fig. 3.6). It corresponds to an arterial oxygen saturation (SpO2) of <90% and usually indicates underlying cardiac or pulmonary disease. Anaemic or hypovolaemic patients rarely have central cyanosis because severe hypoxia is required to produce the necessary concentration of deoxygenated haemoglobin. Conversely patients with polycythaemia can become cyanosed at normal arterial oxygen saturation.

Peripheral cyanosis: This occurs in the hands, feet or ears, usually when they are cold. In healthy people it occurs in cold conditions when prolonged peripheral capillary flow allows greater oxygen extraction and hence increased levels of deoxyhaemoglobin. In combination with central cyanosis, it is most often seen with poor peripheral circulation due to shock, heart failure, vascular disease and venous obstruction, e.g. deep vein thrombosis.
Melanin
Skin colour is greatly influenced by the deposition of melanin (Box 3.8).
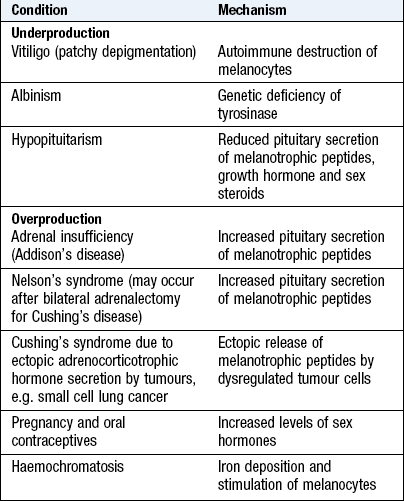
Vitiligo: This chronic condition produces bilateral symmetrical depigmentation, commonly of the face, neck and extensor aspects of the limbs, resulting in irregular pale patches of skin. It is associated with autoimmune diseases, e.g. diabetes mellitus, thyroid and adrenal disorders, and pernicious anaemia (Fig. 3.7).

Albinism: This is an inherited disorder in which patients have little or no melanin in their skin or hair. The amount of pigment in the iris varies; some individuals have reddish eyes, but most have blue.
Overproduction of melanin: This can be due to excess of the pituitary hormone, adrenocorticotrophic hormone, as in adrenal insufficiency. It produces brown pigmentation, particularly in skin creases, recent scars, sites overlying bony prominences, areas exposed to pressure, e.g. belts and bra straps, and the mucous membranes of the lips and mouth, where it results in muddy brown patches (Fig. 5.19A–C).
Carotene
Hypercarotenaemia occurs in people who eat large amounts of raw carrots and tomatoes, and in hypothyroidism. A yellowish discoloration is seen on the face, palms and soles, but not the sclerae, and this distinguishes it from jaundice (Fig. 3.8).

Bilirubin
Jaundice is detectable when serum bilirubin concentration is elevated and the sclerae, mucous membranes and skin become yellow (Fig. 8.8 and Box 3.9). In longstanding jaundice a green colour develops in the sclerae and skin due to biliverdin. Patients with pernicious anaemia have a lemon-yellow complexion due to a combination of mild jaundice and anaemia.
3.9
Jaundice
Clinical detection of jaundice depends upon the level of serum bilirubin, ambient lighting and colour perception of the examining clinician: 70–80% of observers will detect jaundice if levels are 43–51 umol/L, 83% at 171 umol/L and 96% if levels are >256 umol/L.
Hung OL, Kwan NS, Cole AE et al. Evaluation of the physician’s ability to recognise the presence or absence of anaemia, fever and jaundice. Acad. Emerg. Med. 2000: 7; 146–156 Ruiz MA, Saab S, Rickman LS. The clinical detection of scleral icterus: Observations of multiple examiners. Mil. Med. 1997: 162; 560–563
Iron
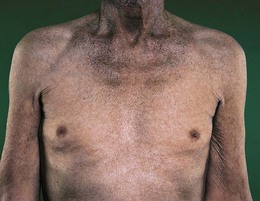
Haemochromatosis increases skin pigmentation due to iron deposition and increased melanin production (Fig. 3.9). Iron deposition in the pancreas causes diabetes mellitus and the combination with skin pigmentation is called ‘bronzed diabetes’.
Haemosiderin, a haemoglobin breakdown product, is deposited in the skin of the lower legs following extravasation of blood into subcutaneous tissues from venous insufficiency. Local deposition of haemosiderin (erythema ab igne or ‘granny’s tartan’) occurs with heat damage to the skin from sitting too close to a fire or from applying local heat, such as a hot water bottle, to the site of pain (Fig. 3.10).

Easy bruising
Approximately 20% of patients complain they bruise easily (Fig. 3.24). It is more common in the elderly because of increased skin and subcutaneous tissue fragility and a greater likelihood of increased episodes of minor trauma. A lifelong tendency suggests an inherited disorder whereas recent onset suggests an acquired disorder. Enquire if there are other family members with a similar problem (bleeding disorder), what drugs the patient is receiving, e.g. anticoagulants, corticosteroids and ask about recurrent nose bleeds (epistaxis) and heavy menstrual periods (menorrhagia).
Odours
Everybody has a natural smell, produced by bacteria acting on apocrine sweat; this may be altered by antiperspirants, deodorants and perfume. Excessive sweating and poor personal hygiene increase body odour and may be compounded by dirty or soiled clothing and stale urine. Excessive body odour occurs in:
Tobacco’s characteristic lingering smell pervades skin, hair and clothing. Marijuana (cannabis) can also be identified by smell. The smell of alcohol on a patient’s breath, particularly in the morning, may suggest an alcohol problem.
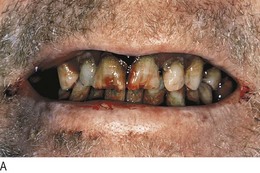
Halitosis (bad breath) is caused by decomposing food wedged between the teeth, gingivitis, stomatitis, atrophic rhinitis and tumours of the nasal passages.
Other characteristic odours include:
• fetor hepaticus: stale ‘mousy’ smell of the volatile amine, dimethylsulphide, in patients with liver failure
• ketones: a sweet smell (like nail varnish remover) due to acetone in diabetic ketoacidosis or starvation
• uraemic fetor: fishy or ammoniacal smell on the breath in uraemia
• putrid or fetid smell of chronic anaerobic suppuration due to bronchiectasis or lung abscess
• foul-smelling belching in patients with gastric outlet obstruction
Spot diagnoses
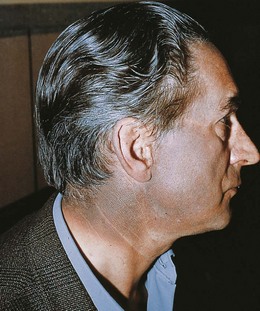
Many disorders have characteristic facial features (Fig. 3.11). Osteogenesis imperfecta is an autosomal dominant condition causing fragile and brittle bones in which the sclerae are blue due to abnormal collagen formation. In systemic sclerosis the skin is thickened and tight, causing loss of the normal wrinkles and skin folds, ‘beaking’ of the nose, and narrowing and puckering of the mouth. Hereditary haemorrhagic telangiectasia is an autosomal dominant condition associated with small dilated capillaries or terminal arteries (telangiectasia) on the lips and tongue. Dystrophia myotonica is an autosomal dominant condition with characteristic features of frontal balding, bilateral ptosis and delayed relaxation of grip after a handshake.
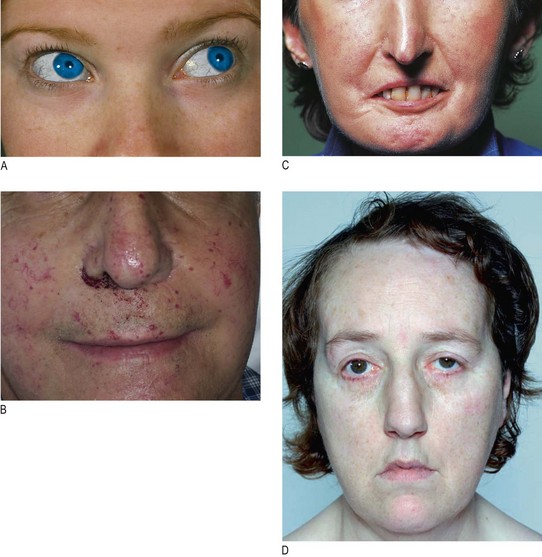
Fig. 3.11 Characteristic facial features of some disorders.
(A) Blue sclerae of osteogenesis imperfecta. (B) Telangiectasia around the mouth typical of hereditary haemorrhagic telangiectasia. (C) Systemic sclerosis with ‘beaking’ of the nose and taut skin around the mouth. (D) Dystrophia myotonica with frontal balding and bilateral ptosis.
Major chromosomal abnormalities
There are several genetic or chromosomal syndromes that you should easily recognise on first contact with the patient.
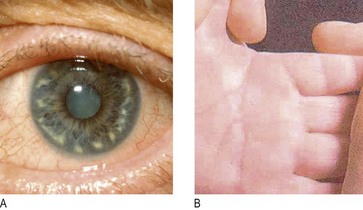
Down’s syndrome (trisomy 21 – 47XX/XY + 21): Down’s syndrome is characterised by typical physical features, including short stature, a small head with flat occiput, upslanting palpebral fissures, epicanthic folds, a small nose with a poorly developed bridge and small ears. Grey-white areas of depigmentation are seen in the iris (Brushfield’s spots; Fig. 3.12A). The hands are broad with a single palmar crease (Fig. 3.12B), the fingers are short and the little finger is curved.
Turner’s syndrome (45XO): Turner’s syndrome is due to loss of a sex chromosome. It occurs in 1 : 2500 live female births and is a cause of delayed puberty in girls. Typical features include short stature, webbing of the neck, small chin, low-set ears, low hairline, short fourth finger, increased carrying angle at the elbows and widely spaced nipples (‘shield-like chest’).
The hands
Abnormal findings
Deformity may be diagnostic: for example, the flexed hand and arm of hemiplegia or radial nerve palsy, and ulnar deviation at the metacarpophalangeal joints in longstanding rheumatoid arthritis (Fig. 14.34). Dupuytren’s contracture is a thickening of the palmar fascia causing fixed flexion deformity and usually affecting the little and ring fingers (Fig. 3.13). Arachnodactyly (long thin fingers) are typical of Marfan’s syndrome (Fig. 3.28B). Trauma is the most common cause of hand deformity.

Colour
Look for cyanosis in the nail bed and tobacco staining of the fingers (Fig. 7.8). Examine the skin creases for pigmentation, although pigmentation is normal in many non-European races (Fig. 3.14).

Temperature
In a cool climate the temperature of the patient’s hand is a good guide to peripheral perfusion. In chronic obstructive pulmonary disease, the hands may be cyanosed due to reduced arterial oxygen saturation but warm due to vasodilatation from elevated arterial carbon dioxide levels. In heart failure the hands are often cold and cyanosed because of vasoconstriction in response to a low cardiac output. If they are warm, heart failure may be due to a high-output state, such as hyperthyroidism.
Skin
The dorsum of the hand is smooth and hairless in children and in adult hypogonadism. Manual work may produce specific callosities due to pressure at characteristic sites. Disuse results in soft, smooth skin, as seen on the soles of the feet in bed-bound patients.
Look at the flexor surfaces of the wrists and forearms. Note any venepuncture marks of intravenous drug use and linear (usually transverse), multiple wounds or scars from deliberate self-harm (Figs 3.15 and 3.16). Look carefully at the fingernails, which can provide useful diagnostic clues (Fig. 4.15).


Finger clubbing
Clubbing is painless soft-tissue swelling of the terminal phalanges. The enlargement increases convexity of the nail. It may be produced by growth factors from megakaryocytes and platelets lodged in nail bed capillaries stimulating vascular connective tissue (Fig. 3.17).


It is an important sign of major diseases, although it may be congenital (Box 3.10). It usually takes weeks or months to develop, and may disappear if the underlying condition is cured. Clubbing usually affects the fingers symmetrically, but may involve the toes. Unilateral clubbing can be caused by proximal vascular conditions, e.g. arteriovenous shunts for dialysis. Autoimmune hyperthyroidism may be associated with thyroid acropachy – clubbing which is more pronounced on the radial side of the hand (Fig. 5.3C).
Examination sequence
 Look across the nail bed from the side of each finger. Observe the distal phalanges, nail and nail bed.
Look across the nail bed from the side of each finger. Observe the distal phalanges, nail and nail bed.
Measure the anteroposterior distance at the level of the interphalangeal joint. Repeat at the level of the nail bed (Fig. 3.18).
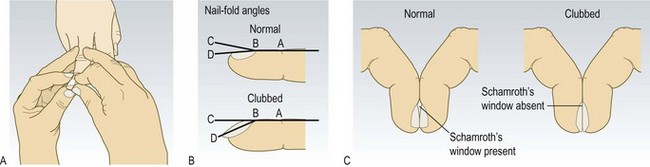
Fig. 3.18 Examining for finger clubbing.
(A) Testing for fluctuation of the nail bed. (B) Nail fold angles. (C) Schamroth’s window sign.
Measure the nail bed angle (Fig. 3.18B).
Place the nails of corresponding fingers back to back and look for a visible gap between the nail beds – Schamroth’s window sign (Fig. 3.18C).
Place your thumbs under the pulp of the distal phalanx and use your index fingers alternately to see if you can feel movement of the nail on the nail bed. This is fluctuation. (Fig. 3.18A).
Abnormal findings: Finger clubbing is present if:
• the interphalangeal depth ratio (B/A in Fig. 3.18) is >1
• Schamroth’s window sign is absent (Fig. 3.18C).
Increased nail bed fluctuation may be present, but its presence is subjective and less discriminatory than the above features.
Joints
Arthritis frequently involves the small joints of the hands. Rheumatoid arthritis typically affects metacarpophalangeal and proximal interphalangeal joints (Fig. 14.34), and osteoarthritis and psoriatic arthropathy affect the distal interphalangeal joints (Fig. 14.12).
Muscles
Small muscle wasting of the hands is common in rheumatoid arthritis, producing ‘dorsal guttering’ of the hands. In carpal tunnel syndrome, median nerve compression leads to wasting of the thenar muscles (Fig. 14.29), and cervical spondylosis with nerve root entrapment causes small muscle wasting.
The tongue
Examination sequence
Ask the patient to put out his tongue.
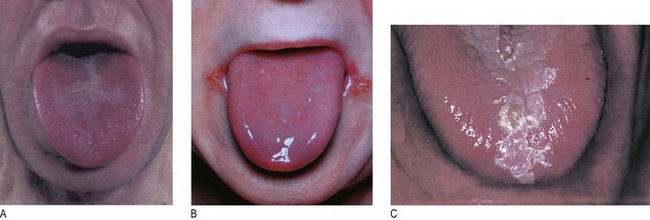
Look at the size, shape, movements, colour and surface (Fig. 3.19).
Normal findings
Tongue furring is normal and common in heavy smokers
Geographic tongue describes red rings and lines which change over days or weeks on the surface of the tongue. It is usually not significant but can be due to riboflavin (vitamin B2) deficiency
Abnormal findings
• Tremor can be due to anxiety, thyrotoxicosis, delirium tremens or parkinsonism.
• Fasciculation (irregular ripples or twitching of the tongue) occurs in lower motor neurone disorders, e.g. motor neurone disease.
• Macroglossia (enlargement of the tongue) may occur in acromegaly, amyloidosis or tumour infiltration.
• White patches that may be scraped off the tongue are due to the fungal yeast, Candida (oral thrush). Common causes include inhaled steroids, immune deficiency, e.g. HIV and terminal illness.
• Glossitis is a smooth reddened tongue due to atrophy of the papillae. It is common in alcoholics, in nutritional deficiencies of iron, folate and vitamin B12, and in 30% of patients with coeliac disease. Glossitis may cause a burning sensation over the tongue but usually a painful tongue is a symptom of anxiety or depression.
• Leukoplakia is a thickened white patch that cannot be scraped off the tongue. It may be premalignant.
Lumps or swellings
Patients often present with a lump they have just found. This does not necessarily mean that it has developed recently. Ask about any changes since they noticed it and whether there are any associated features, e.g. pain, tenderness or colour change. During examination you may find a lump the patient is unaware of.
Size
Accurately measure the size of any lump (preferably using callipers), so that with time you can detect significant change.
Position
The origin of some lumps may be obvious, e.g. in the breast, thyroid or parotid gland; in other sites, e.g. the abdomen, this is less clear. Multiple lumps may occur in neurofibromatosis (Fig. 3.20A), skin metastases, lipomatosis and lymphomas.


Attachments
Lymphatic obstruction causes fixation of the skin with fine dimpling at the opening of hair follicles that resembles orange peel (peau d’orange) (Fig. 10.6). This is common in malignant disease when attachment to deeper structures, e.g. underlying muscle, may occur.
Consistency
The consistency of a lump can vary from soft to ‘stony’ hard. Very hard swellings are usually malignant, calcified or dense fibrous tissue. Fluctuation indicates the presence of fluid, e.g. abscess, cyst, blister or soft encapsulated tumours, e.g. lipoma.
Edge
The edge or margin may be well delineated or ill defined, regular or irregular, sharp or rounded. The margins of enlarged organs, e.g. thyroid gland, liver, spleen or kidney, can usually be defined more clearly than those of inflammatory or malignant masses. An indefinite margin suggests infiltrating malignancy, in contrast to the clearly defined edge of a benign tumour.
Surface and shape
The surface and shape of a swelling can be characteristic. In the abdomen examples include an enlarged spleen or liver, a distended bladder or the fundus of the uterus in pregnancy. The surface may be smooth or irregular, e.g. the surface of the liver is smooth in acute hepatitis but is often nodular in metastatic disease.
Pulsations, thrills and bruits
Arterial swellings (aneurysms) and highly vascular tumours are pulsatile (they move in time with the arterial pulse). Other swellings may transmit pulsation if they lie over a major blood vessel. If the blood flow through a lump is increased, a systolic murmur (bruit) may be auscultated and, if loud enough, a thrill may be palpable. Bruits are also heard over arterial aneurysms and arteriovenous malformations.
Inflammation
Redness, tenderness and warmth suggest inflammation.
• Redness (erythema): the skin over acute inflammatory lesions is usually red due to vasodilatation. In haematomas the pigment from extravasated blood may produce the range of colours in a bruise (ecchymosis).
• Tenderness: inflammatory lumps, e.g. boil or abscess, are usually tender or painful, while non-inflamed swellings are not: lipomas, skin metastases and neurofibromas are characteristically painless.
• Warmth: inflammatory lumps and some tumours, especially if rapidly growing, may feel warm due to increased blood flow.
Transillumination
In a darkened room, press the lighted end of a pen torch on to one side of the swelling. A cystic swelling, e.g. testicular hydrocoele, will light up if the fluid is translucent, providing the covering tissues are not too thick (Fig. 15.5 and Box 3.11).
Examination sequence
Inspect the lump, noting any change in colour or texture of the overlying skin.
Define the site and shape of the lump.
Measure its size and record the findings diagrammatically.
Gently palpate for tenderness or change in skin temperature.
Feel the lump for a few seconds to determine if it is pulsatile.
Assess the consistency, surface texture and margins of the lump.
Try to pick up an overlying fold of skin to assess whether the lump is fixed to the skin.
Try to move the lump in different planes relative to the surrounding tissues to see if it is fixed to deeper structures.
Compress the lump on one side; see and feel if a bulge occurs on the opposite side (fluctuation). Confirm the fluctuation in two planes. Fluctuation usually indicates that the lump contains fluid, although some soft lipomas can feel fluctuant.
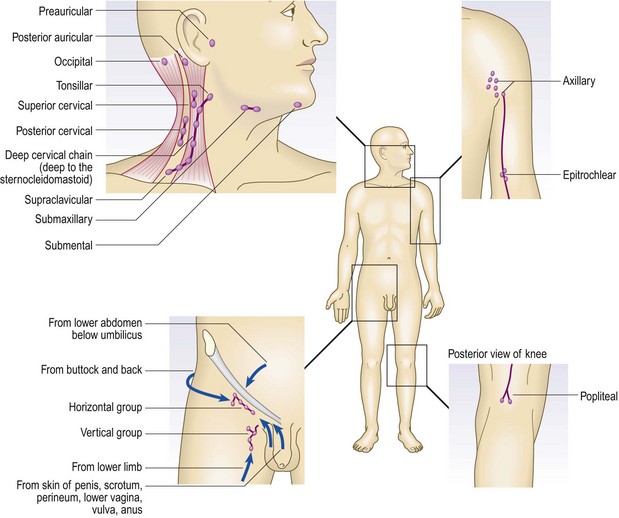
The lymph nodes
Lymph nodes may be palpable in normal people, especially in the submandibular, axilla and groin regions (Fig. 3.21). Distinguish between normal and pathological nodes. Pathological lymphadenopathy may be local or generalised, and is of diagnostic and prognostic significance in the staging of lymphoproliferative and other malignancies.
Consistency
Normal nodes feel soft. In Hodgkin’s disease they are characteristically ‘rubbery’, in tuberculosis they may be ‘matted’, and in metastatic cancer they feel hard.
Tenderness
Acute viral or bacterial infection, including infectious mononucleosis, dental sepsis and tonsillitis, causes tender, variably enlarged lymph nodes.
Examination sequence
Examine the cervical and axillary nodes with the patient sitting.
From behind, examine the submental, submandibular, preauricular, tonsillar, supraclavicular and deep cervical nodes in the anterior triangle of the neck (Fig. 3.22A).

Fig. 3.22 Palpation of the cervical glands.
(A) Examine the glands of the anterior triangle from behind, using both hands. (B) Examine for the scalene nodes from behind with your index finger in the angle between the sternocleidomastoid muscle and the clavicle. (C) Examine glands in the posterior triangle from the front.
Palpate for the scalene nodes by placing your index finger between the sternocleidomastoid muscle and clavicle. Ask the patient to tilt his head to the same side and press firmly down towards the first rib (Fig. 3.22B).
From the front of the patient, palpate the posterior triangles, up the back of the neck and the posterior auricular and occipital nodes (Fig. 3.22C).
From the patient’s front or side, palpate the right axilla with your left hand and vice versa (Fig. 3.23A).
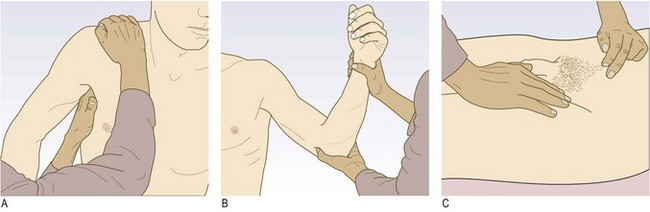
Fig. 3.23 Palpation of the axillary, epitrochlear and inguinal glands.
(A) Examination for right axillary lymphadenopathy. (B) Examination of the left epitrochlear glands. (C) Examination of the left inguinal glands.
Gently place your fingertips into the apex of the axilla and then draw them downwards, feeling the medial, anterior and posterior axillary walls in turn.
Support the patient’s right wrist with your left hand, hold his partially flexed elbow with your right hand and use your thumb to feel for the epitrochlear node. Examine the left epitrochlear node with your left thumb (Fig. 3.23B).
Examine for the inguinal and popliteal nodes with the patient lying down.
Palpate over the horizontal chain, which lies just below the inguinal ligament, and then over the vertical chain along the line of the saphenous vein (Fig. 3.23C).
Abnormal findings
If you find localised lymphadenopathy, examine the areas which drain to that site. Infection commonly causes lymphadenitis (localised tender lymphadenopathy); e.g. in acute tonsillitis the submandibular nodes are involved. If the lymphadenopathy is non-tender, look for a malignant cause, tuberculosis or features of HIV infection. Generalised lymphadenopathy occurs in a number of conditions (Box 3.12). Examine for enlargement of the liver and spleen, and for other haematological features, such as purpura (bruising under the skin), which can be large (ecchymoses) or pinpoint (petechiae; Fig. 3.24).
 3.12 Important common causes of lymphadenopathy
3.12 Important common causes of lymphadenopathy

Weight and height
Weight is an important indicator of general health and nutrition. Serial weight measurements are useful in monitoring acutely ill patients and those with chronic disease. Serial height is helpful in monitoring growth in children and osteoporotic vertebral collapse in the elderly.
Record the body mass index (BMI), rather than weight alone, as it is independent of the patient’s height. BMI is calculated from the formula: weight/height2 (using metric units, kg/m2). Obesity is defined by BMI and race (Box 3.13).
3.13 The relationship between body mass index (BMI), nutritional status and ethnic group
| BMI non-Asian | BMI Asian | |
| Severe malnutrition | <16 | <16 |
| Underweight | <18.5 | <18.5 |
| Normal | 18.5–24.9 | 18.5–22.9 |
| Overweight | 25–29.9 | 23–24.9 |
| Obese | 30–39.9 | 25–29.9 |
| Morbidly obese | ≥40 | ≥30 |
BMI, however, does not describe body fat distribution and excess intra-abdominal fat is an independent predictor of hypertension, insulin resistance, type 2 diabetes mellitus and coronary artery disease. Waist circumference correlates better with visceral fat and indirectly measures central adiposity. Health risk is increased when waist circumference exceeds 94 cm (37 inches) for men and 80 cm (32 inches) for women. Waist : hip ratio is strongly related to risk of coronary artery disease. ‘Pear shape’ and a waist : hip ratio of ≤0.8 in females or <0.9 in males have a good prognosis, whereas ‘apple-shaped’ subjects with a greater waist : hip ratio have an increased risk of coronary artery disease and the ‘metabolic syndrome’ (Fig. 3.25).
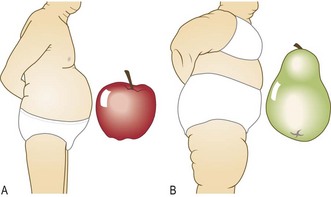
Fig. 3.25 Abdominal obesity and generalised obesity.
(A) Abdominal obesity (apple shape). (B) Generalised obesity, where fat deposition is mainly on the hips and thighs (pear shape).
Examination sequence
Note any abnormalities in stature or body proportions,
Measure height using a vertical scale with a rigid, adjustable arm piece. In the serial assessment of growth in children and teenagers, measure height to the nearest millimetre using a calibrated stadiometer (Fig. 15.20).
The patient should stand erect and be weighed in his indoor clothing without shoes. Calculate and record BMI.
Look for abnormal fat distribution.
Measure the waist with the patient standing at the level equidistant between the costal margin and iliac crest. The measurement should record the maximum diameter, so measure over any abdominal fat and not under it.
Look for any evidence of malnutrition or specific vitamin deficiencies.
Nutritional status
Illness may produce profound changes in an individual’s nutritional requirements, appetite and ability to eat. Malnutrition delays recovery from illness and surgery, and delays wound healing. Record BMI initially and repeat this at least weekly in an acute setting, and monthly in outpatients or in the community, to monitor nutritional status.
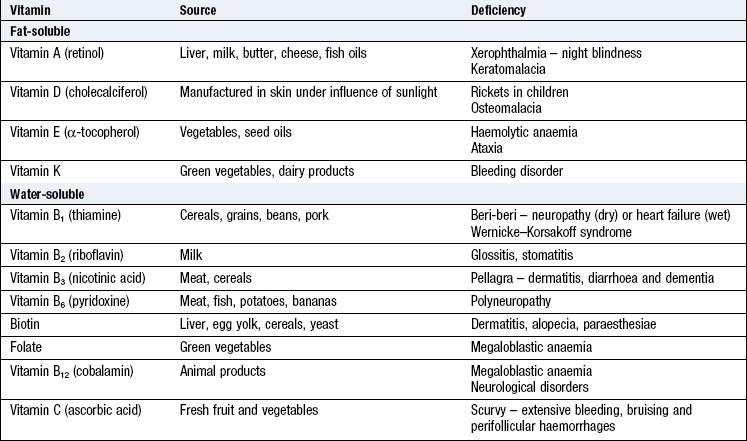
Vitamin deficiencies
Vitamins are organic substances that have key roles in certain metabolic pathways. They are fat-soluble (vitamins A, D, E and K) or water-soluble (vitamins of the B-complex group and vitamin C).
Vitamin deficiencies occur in older people and alcoholic patients, and are common in developing countries. Folate deficiency is usually due to poor intake and causes macrocytic anaemia and glossitis. Vitamin B12 deficiency is usually caused by the autoimmune disorder pernicious anaemia but can occur in vegans, small-bowel overgrowth, or ileal disease or resection. Vitamin C deficiency (scurvy) is less common and produces extensive bruising, particularly in the elderly living alone without access to fresh fruit and vegetables (Fig. 3.26). Those with alcohol dependency may eat poorly and also become deficient in vitamin B1 (thiamine). Small-bowel malabsorption and liver and biliary tract disease can lead to deficiency of fat-soluble vitamins (Box 3.14).

Abnormal findings
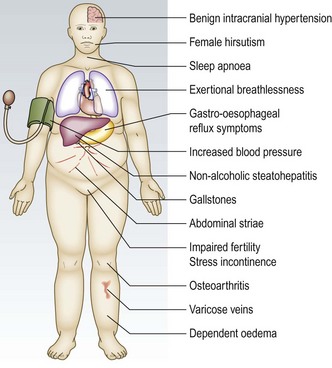
Obesity is a major worldwide health problem, largely as a result of changes in lifestyle. It is caused by excess calorie intake associated with inadequate exercise. Rarely, it is secondary to hypothyroidism, Cushing’s syndrome, Prader–Willi syndrome or drugs (Box 3.15). It is associated with hypertension, hyperlipidaemia, type 2 diabetes mellitus, gallbladder disease and sleep apnoea (Fig. 3.27). Increased BMI is associated with several malignancies, particularly oesophageal and renal cancer in both sexes, thyroid and colon cancer in men and endometrial and gallbladder cancer in women. Obesity reduces life expectancy by about 7 years, about the same as a lifetime of heavy smoking.
3.15 Drugs associated with weight gain
| Class | Examples |
| Anticonvulsants | Sodium valproate, phenytoin, gabapentin |
| Antidepressants | Citalopram, mirtazapine |
| Antipsychotics | Chlorpromazine, risperidone, olanzapine, lithium |
| Beta-blockers | Atenolol |
| Oral corticosteroids | Prednisolone, dexamethasone |
| Migraine prophylaxis | Pizotifen |
| Sulphonylureas/hypoglycaemic agents | Gliclazide, pioglitazone |
| Insulin | All formulations |
| Protease inhibitors for HIV infection | Indinavir, ritonavir, lopinavir |
Weight loss
Weight loss is important and may be due to:
• reduced food intake from a poor appetite (anorexia)
• malabsorption or loss of nutrients, e.g. in prolonged diarrhoea
• metastatic cancer, e.g. of the lung, breast or gastrointestinal tract
• serious and prolonged infection, e.g. tuberculosis
In most of these systemic disorders, weight loss is associated with anorexia. Occasionally, weight loss is associated with a normal or increased appetite (thyrotoxicosis, coeliac disease or type 1 diabetes mellitus). The patient’s complaint of weight loss does not always correlate with true weight loss. Temporary weight loss is most commonly associated with anxiety, depression or a deliberate attempt to lose weight.
Malnutrition and starvation are major problems worldwide, even in the developed world. Malnutrition is found in up to 40% of UK hospital admissions, particularly the elderly, usually due to poverty or illness. Weight loss due to malnutrition also occurs in anorexia nervosa, alcohol abuse and drug addiction.
Short stature
Short stature is usually familial, so ask about the height of the patient’s parents and siblings (p. 368). Any significant childhood illness will reduce the rate of growth and may limit final height. Identify causes of short stature from associated features. Other disorders, such as renal tubular acidosis, intestinal malabsorption and hypothyroidism, may be less obvious in young people and delay the diagnosis. Loss of height is part of normal ageing but is accentuated by compression fractures of the spine due to osteoporosis, particularly in women. In postmenopausal women loss of >5 cm height is an indication to investigate for osteoporosis.
Tall stature
Tall stature is less common than short stature and is usually familial. Most individuals with heights above the 95th centile are not abnormal so ask about the height of close relatives. Abnormal causes of increased height include:
In Marfan’s syndrome, the limbs are long in relation to the length of the trunk, and the arm span exceeds height (Fig. 3.28A). Additional features include long slender fingers (arachnodactyly) (Fig. 3.28B), narrow feet, a high-arched palate (Fig. 3.28C), upward dislocation of the lenses of the eyes (Fig. 3.28D), cardiovascular abnormalities such as mitral valve prolapse, and dilatation of the aortic root with aortic regurgitation.
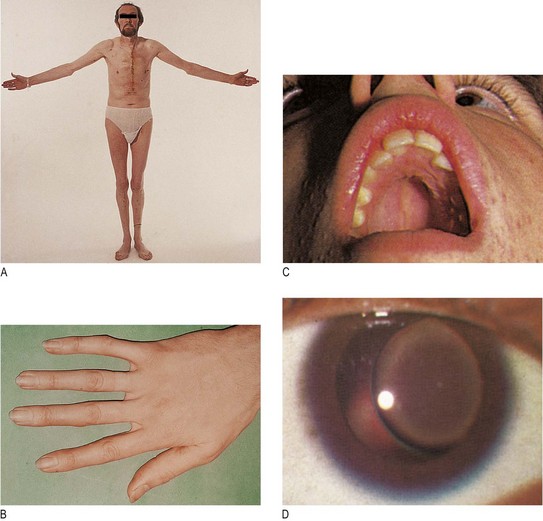
Fig. 3.28 Marfan’s syndrome, an autosomal dominant condition.
(A) Tall stature and reduced upper segment to lower segment ratio (note surgery for aortic dissection). (B) Long fingers. (C) High-arched palate. (D) Dislocation of the lens in the eye.
During puberty, the epiphyses close in response to stimulation from the sex hormones, so in some patients with hypogonadism the limbs continue to grow for longer than usual.
Pituitary gigantism is a very rare cause of tall stature due to excessive growth hormone secretion before epiphyseal fusion has occurred.
Hydration
In adults 60–65% of body mass is water. A male weighing 70 kg has 42 litres of water, of which two-thirds is intracellular (28 litres), 12% interstitial fluid (9.4 litres) and the remainder circulating blood plasma (4.6 litres). Women have a smaller percentage of total body water than men, although they may have cyclical fluctuations in weight due to perimenstrual fluid retention.
Dehydration
It is easy to underestimate the severity of dehydration. Assess hydration in all patients, especially those with excess fluid loss, e.g. vomiting, diarrhoea, sweating, burns and polyuria, and when ambient temperature is raised. If you know the patient’s usual weight, useful information is obtained by weighing him.
Tachycardia is a common feature. Loss of skin turgor occurs in severe dehydration but adults can lose 4–6 litres before the skin becomes dry and loose. Blood pressure may be low and postural hypotension may indicate intravascular volume depletion. A dry tongue is an unreliable indicator of dehydration since it often occurs in mouth breathing.
Oedema
Oedema is tissue swelling due to an increase in interstitial fluid. The capillary wall separates the interstitial fluid and plasma compartments. The distribution of water between the vascular and interstitial spaces is determined by the balance between hydrostatic pressure forcing water out of the capillary, and colloid osmotic (oncotic) pressure, drawing fluid into the vascular space (Starling’s forces). Oncotic pressure depends largely on circulating protein concentration, particularly serum albumin.
Oedema can be generalised, localised or postural.
The cardinal sign of subcutaneous oedema is pitting of superficial tissues. Pitting on pressure may not be demonstrable until body weight has increased by 10–15%. Day-to-day alterations in body weight are usually the most reliable index of changes in body water.
Hypothyroidism is characterised by mucinous infiltration of tissues (myxoedema). In contrast to oedema, myxoedema and chronic lymphoedema do not pit on pressure.
Generalised oedema
There are two principal causes of generalised oedema (Box 3.16):
3.16 Causes of oedema
Distinguish them by assessing the jugular venous pressure (p. 114). The jugular venous pressure is usually elevated in fluid overload but not in hypoproteinaemia (Box 3.17).
3.17 Features suggesting different causes of oedema

*On examination is not possible to distinguish a deep venous thrombosis (DVT) from a ruptured Baker’s cyst.
Fluid overload: Fluid overload may be due to heart failure or renal disease, or be iatrogenic (result from medical intervention).
• Heart failure causes oedema in the following ways:
• Renal underperfusion activates the renin–angiotensin–aldosterone system (secondary hyperaldosteronism) and releases vasopressin, leading to salt and water retention.
• Renal blood flow is reduced, causing increased salt and water reabsorption.
• When the patient lies flat, blood redistributes from the legs into the torso, increasing venous return to the heart. In the failing heart this results in increased end-diastolic pressure within the left ventricle, leading to pulmonary oedema. The patient therefore experiences orthopnoea (breathlessness on lying flat).
• Renal disease, e.g. acute glomerulonephritis, may reduce urine volume, with increased circulating and extracellular fluid volume and increased tubular reabsorption of sodium.
• Iatrogenic causes include excess fluid replacement, especially intravenously, producing fluid overload.
Hypoproteinaemia: Hypoproteinaemia, particularly hypoalbuminaemia, reduces oncotic pressure and encourages fluid to move to the interstitial space, causing oedema. Nephrotic syndrome causes heavy proteinuria and most patients with a hepatic cause will have features of chronic liver disease (Fig. 8.11).
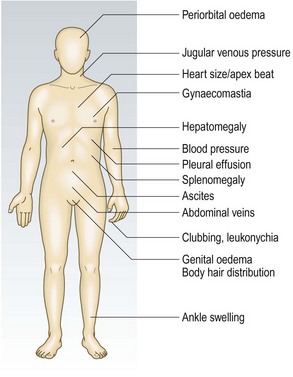
The distribution of generalised oedema (Fig. 3.29) is determined by gravity. In semirecumbent patients it is usually found in the ankles, backs of the thighs and the lumbosacral area. If the patient lies flat, it may involve the face and hands, as in nephrotic syndrome.
Localised oedema
This may be caused by venous, lymphatic, inflammatory or allergic disorders.
Venous causes: Increased venous pressure increases hydrostatic pressure within capillaries, producing oedema in the area drained by that vein. Venous causes include deep vein thrombosis, external pressure from a tumour or pregnancy, or venous valvular incompetence from previous thrombosis or surgery. Conditions which impair the normal muscle pumping action, e.g. hemiparesis and forced immobility, increase venous pressure by impairing venous return. As a result oedema may occur in immobile, bed-ridden patients, in a paralysed limb, or in a healthy person sitting for long periods, e.g. during travel (Fig. 3.30).

Lymphatic causes: Normally, interstitial fluid returns to the central circulation via the lymphatic system. Any cause of impaired lymphatic flow, e.g. intraluminal or extraluminal obstruction, may produce localised oedema (lymphoedema) (Fig. 3.31). If the condition persists, fibrous tissues proliferate in the interstitial space and the affected area becomes hard and no longer pits on pressure. In the UK, the commonest cause of leg lymphoedema is congenital hypoplasia of leg lymphatics (Milroy’s disease), and in the arm after radical mastectomy and/or irradiation for breast cancer. Lymphoedema is common in some tropical countries because of lymphatic obstruction by filarial worms (elephantiasis).

Inflammatory causes: Any cause of tissue inflammation, including infection or injury, liberates mediators, e.g. histamine, bradykinin and cytokines, which cause vasodilatation and increase capillary permeability. Inflammatory oedema is accompanied by the other features of inflammation (redness, tenderness and warmth) and is therefore painful.
Allergic causes: Increased capillary permeability occurs in acute allergic conditions. The affected area is usually red and pruritic (itchy) because of local release of histamine and other inflammatory mediators but, in contrast to inflammation, is not painful.
Angio-oedema is a specific form of allergic oedema affecting the face, lips and mouth (Fig. 3.32). Swelling may develop rapidly and may be life-threatening if the upper airway is involved.

Postural oedema
This is due to failure of muscle movement and is common in the lower limbs of inactive patients.
Examination sequence
Apply firm pressure with your fingers or thumb for at least 15 seconds (Fig. 3.33). Pitting may persist for several minutes until it is obliterated by the slow return of the displaced fluid.


Assess the state of hydration by looking for sunken orbits and dry mucous membranes. Gently pinch a fold of skin on the neck or anterior chest wall, hold it for a few seconds and then release. Well-hydrated skin springs back into position immediately, in severe dehydration skin subsides abnormally slowly.
Record weight and urine output.
Record the pulse rate and supine/erect blood pressures. Look for tachycardia >100 bpm and postural hypotension (a fall >15 mmHg in systolic pressure on standing).
Check for oedema in the ankles and legs. In bed-bound patients, check for sacral oedema.
Examine the jugular venous pressure (p. 114).
Temperature
The ‘normal’ oral or ear temperature is 37°C but may range between 35.8°C and 37.2°C (98–99°F) (Box 17.2). There is a circadian variation, with the lowest readings occurring in the early morning. Rectal temperature is about 0.5°C higher than oral. The axilla is an unreliable site for measuring temperature. Use a digital thermometer under the tongue, or in the rectum or the external auditory meatus. Mercury thermometers have been replaced by electronic devices, which are safer and more accurate (Fig. 3.34).

Fever
Fever is an increase in body temperature usually caused by a cellular response to infection, immunological disturbance or malignancy (Ch. 17).
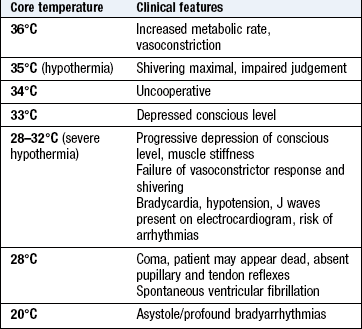
Hypothermia
Hypothermia is a core temperature <35°C and is easily missed unless rectal temperature is measured. As body temperature falls, conscious level is progressively impaired. Altered consciousness is common with core temperatures <28°C (Box 3.18), and may mimic death (Box 20.2). If you suspect hypothermia, measure temperature at more than one site, e.g. external auditory meatus and rectum.