Babies and children
Examination of babies
A baby is a neonate for the first 4 weeks of life and an infant for the whole of the first year. Neonates are classified by gestational age or birthweight (Box 15.1).
 15.1 Classification of newborn infants
15.1 Classification of newborn infants
| Birthweight | |
| Extremely low | <1000 grams |
| Very low | <1500 grams |
| Low | <2500 grams |
| Normal | ≥2500 grams |
| Gestational age | |
| Extremely preterm | <28 weeks |
| Preterm | <37 weeks (<259th day) |
| Term | 37–42 weeks |
| Post-term | >42 weeks (>294th day) |
Symptoms and definitions
Infants cannot report symptoms so you must recognise the signs of illness, which are non-specific in young infants. Always take seriously the concerns of parents as they describe symptoms.
Pallor
Always investigate pallor in a newborn as it implies anaemia or poor perfusion. Newborn infants have higher haemoglobin levels than older children and are therefore not normally pale. Haemoglobin levels <120g/dl in the perinatal period are low. Preterm infants look red because they lack subcutaneous fat.
Respiratory distress
Respiratory distress is tachypnoea (respiratory rate) >60 breaths/min with intercostal and subcostal indrawing, sternal recession, nasal flaring and the use of accessory muscles.
Cyanosis
The bluish discoloration of the lips and mucous membranes due to hypoxia is difficult to see unless oxygen saturation (SpO2) is <80% (normal is >95%) because of the high haematocrit of newborn infants (Box 15.2). Causes include congenital heart disease and respiratory disease and it always needs investigation (p. 149).
 15.2
15.2
Neonatal congenital heart disease screening
Measurement of oxygen saturation (SpO2) by pulse oximetry is a simple, non-invasive method to assist clinical examination of the neonate in screening for congenital heart disease.
Ewer AK, Middleton LJ, Furmston AT et al. PulseOx Study Group. Pulse oximetry screening for congenital heart defects in newborn infants (PulseOx). Lancet 2011;378:785–794.
Acrocyanosis
Acrocyanosis is a bluish-purple discoloration of the hands and feet and, when the newborn is centrally pink, is a normal finding.
Jaundice
Many newborns develop jaundice in the early days after birth. Inspect the sclerae in newborns with coloured skin or you may miss it (Box 15.3). Normal or physiological causes cannot be distinguished clinically from pathological ones.
15.3
Jaundice in the newborn
When looking for jaundice in the newborn, examine the naked baby in bright, preferably natural light. Do not rely on visual inspection alone to estimate the bilirubin level in a baby with jaundice.
NICE. Neonatal jaundice. 2010. Available online at: www.nice.org.uk/CG98.
Jitteriness
Jitteriness is high-frequency tremor of the limbs. It is common in term infants in the first few days. It is stilled by stimulating the infant and is not associated with other physiological disturbance. Exclude hypoglycaemia, polycythaemia and neonatal abstinence syndrome (due to withdrawal of drugs) if it is excessive. Infrequent jerks in light sleep are common and normal, but regular clonic jerks are abnormal.
Dysmorphism
Dysmorphism is an abnormality of body structure. Identifying dysmorphic features is subjective because of human variability. Individual features may be minor and isolated, or may signify a major problem requiring definitive investigation and management. When certain dysmorphic features occur together in a recognisable pattern, a ‘dysmorphic syndrome’ is present, e.g. Down’s syndrome (p. 47). Discuss possible dysmorphic features with parents in the immediate newborn period with great caution and sensitivity.
Hypotonia
Hypotonia (reduced tone) may be obvious when you handle the infant or the infant may lack normal flexion at rest. Term infants’ muscle tone normally produces a flexed posture at the hips, knees and elbows. Hypotonia occurs in systemic conditions such as hypoxia, hypoglycaemia or septicaemia or may be due to a specific problem of brain, nerve or muscle. Preterm infants have lower tone than term infants and are much less flexed at rest.
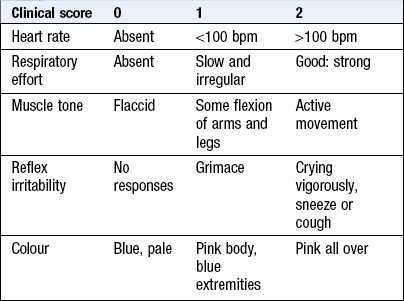
Apgar score
This first clinical assessment of a neonate is made immediately after birth. It describes the tone, colour, breathing, heart rate and response to stimulation. Each element is scored 0, 1 or 2 (Box 15.4), giving a total maximum of 10. Healthy neonates commonly score 8–10 at 1 and 5 minutes. The score provides feedback about the need for, and efficacy of, resuscitation. A low score should increase with time. A decreasing score is concerning. Persistently low scores at 10 minutes predict death or later disability. Neonates with scores of less than 8 at 5 minutes require continued evaluation until it is clear they are healthy.
The history
Ask the mother and look in the maternal notes for the medical history (Box 15.5).
15.5 The medical history
Outcome of previous pregnancies
Maternal health in the current pregnancy, including drug history
Issues identified by antenatal screening tests
Meconium staining of the amniotic fluid
Non-reassuring fetal status during labour
Condition at birth, including cord blood gas results and Apgar scores
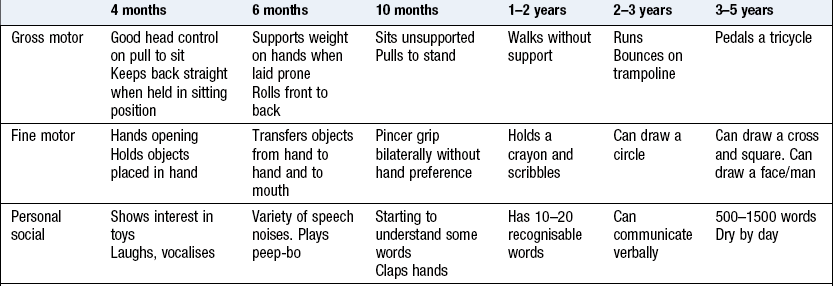
In later infancy, ask additional questions about specific signs and systems as well as obtaining information about developmental progress, depending on the presenting complaint (Box 15.6).
The physical examination
Timing and efficacy of the routine neonatal examination
Examine a newborn with the parents present. There is no ideal time. If performed on day 1 some congenital heart disease may be missed because signs are not yet present. If delayed, some babies will present before this with illness that may have been detected earlier. Nine per cent of neonates have an identifiable congenital abnormality, but most are not serious. Always clearly record which elements of the examination you perform to avoid problems if symptoms and signs develop later. Explain clearly to the parents the limitation of the examination (Box 15.7).
15.7
Structural heart lesions in the newborn
Two per cent of babies have a cardiac murmur, but only half of these have structural heart disease. More than half of the infants with important structural heart lesions have no murmur in the immediate newborn period.
Ainsworth S, Wyllie JP, Wren C. Prevalence and significance of cardiac murmurs in neonates. Arch Dis Child 1999;80:F43–F45.
General examination
Examine babies and infants in a warm place. Have a system to avoid omitting anything, but refrain from an overly rigid approach as you may be unable to perform key elements if you unsettle the baby. Examine newborn infants on a bed or examination table but older infants on their parent’s lap.
Examination sequence
Leave things that may disturb the baby until later.
Normal findings: The skin may look normal, dry, wrinkled or vernix-covered in healthy babies. There may be meconium staining of the skin and nails.
Prominent capillaries commonly cause pink areas called ‘stork’s beak marks’ at the nape of the neck, the eyelids and the glabella (Fig. 15.1). The facial ones fade without treatment over subsequent months. Marks on the neck often persist. Milia (fine white spots) and acne neonatorum (larger cream-coloured spots) are due to collected glandular secretions and disappear within 2–4 weeks.

Abnormal findings: Document any trauma, e.g. scalp cuts, bruising.
Dense capillary haemangiomas (port wine stains) will not fade. Laser treatment may help. Around the eye they may indicate Sturge–Weber syndrome (a facial port wine stain with an underlying brain lesion associated with risk of later seizures, cerebral calcification and reduced cognitive function). Melanocytic naevi require follow-up and treatment by a plastic surgeon or dermatologist. A mongolian blue spot (Fig. 15.2) is an area of bluish discoloration over the buttocks, back and thighs. Easily mistaken for bruising, it usually fades in the first year. Erythema toxicum is a common fleeting blanching idiopathic maculopapular rash of no consequence, seen on the trunk and face.

Subcutaneous fat necrosis causes palpable firm plaques, often with some erythema under the skin, over the body. If extensive, there can be associated hypercalcaemia that may require treatment. Blisters or bullae are usually pathological; causes include infection and significant skin disease (Box 15.8).
Examination sequence
 Note the baby’s head shape (Box 15.9) and any swellings.
Note the baby’s head shape (Box 15.9) and any swellings.
 15.9 Neonatal head shapes
15.9 Neonatal head shapes
| Head shape | Description |
| Microcephalic (small-headed) | Small cranial vault |
| Megalencephalic (large-headed) | Large cranial vault |
| Hydrocephalic (water-headed) | Large cranial vault due to enlarged ventricles |
| Brachycephalic (short-headed) | |
| Dolichocephalic (long-headed) | |
| Plagiocephalic (oblique-headed) | Asymmetrical skull |
Feel the anterior fontanelle (Fig. 15.3) and whether it is sunken, flat or bulging.
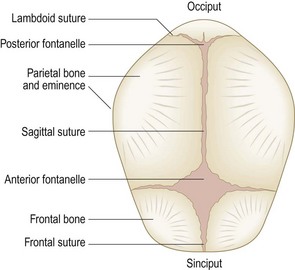
Normal findings: Head moulding is common after birth. Caput succedaneum is soft-tissue swelling over the vertex due to pressure in labour. The cranial sutures may be overriding, giving a palpable step.
Abnormal findings: Cephalhaematoma is a firm, usually parietal swelling due to a collection of blood under the periosteum of a skull bone. It may be bilateral and is not mobile. Periosteal reaction at the margins gives the feeling of a raised edge. No treatment is required. Do not confuse this with the boggy, mobile, poorly localised swelling of subgaleal (beneath the flat sheet of fibrous tissue that caps the skull) haemorrhage which can conceal a large blood loss capable of causing life-threatening shock if unrecognised.
Separated cranial sutures with an obvious gap are due to raised intracranial pressure.
In rare cases the cranial sutures are prematurely fused (synostosis), producing ridging, and the head shape is usually abnormal.
Examination sequence
Look at the eyebrows, lashes, lids and eyeballs.
Gently retract the lower eyelid and look at the sclera for jaundice or any discoloration.
Test ocular movements and vestibular function:
Turn the newborn’s head to one side; watch as the eyes move in the opposite direction. This is called doll’s-eye movements and disappears in infancy (Fig. 12.25).
Hold the infant upright at arm’s length and move him in a horizontal arc. The infant should look in the direction of movement and have optokinetic nystagmus. This response becomes damped by 3 months.
Normal findings: Harmless yellow crusting without inflammation is common after birth in infants with narrow lacrimal ducts.
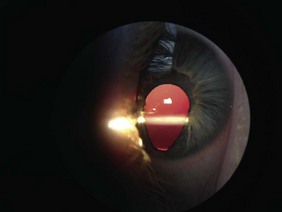
Abnormal findings: Eye infection gives a red eye and purulent secretions. An abnormal pupil shape is usually due to coloboma (a defect in the iris inferiorly that gives the pupil a keyhole appearance: Fig. 15.4). This can affect deeper structures in the eyeball, including the optic nerve, leading to visual impairment. It can be associated with various syndromes, as can microphthalmia (small eyeballs). Large eyeballs that feel hard when palpated through the lids suggest buphthalmos (congenital glaucoma).
Examination sequence
Hold the baby in your arms. Gently rotate your upper body from side to side so that the baby will open his eyes.
Keep your eye close to the ophthalmoscope and look through it at each pupil from about 20 cm. You should see the red reflex of reflected light from the retina (like ‘red eye’ in a photo).
Normal findings: Epstein’s pearls are small white mucosal cysts on the palate that disappear spontaneously.
White coating on the tongue which is easily scraped off with a swab is due to curdled milk.
Abnormal findings: Macroglossia (a large protruding tongue) occurs in Beckwith–Wiedemann syndrome. A normal-sized tongue protrudes through a small mouth in Down’s syndrome (glossoptosis). Ankyloglossia (tongue tie) is when the lingual frenulum which joins the midline of the tongue to the floor of the mouth is abnormally short. Consequently the tongue cannot move freely, interfering with feeding. A white coating on the tongue, not easily removed and which may bleed when scraped, is due to the fungus, Candida albicans (thrush).
Cleft palate may involve the soft palate or both hard and soft palates. It can be midline, unilateral or bilateral and may involve the gum (alveolus). Cleft lip can appear in isolation or in association with it. Refer affected infants early to a specialist multidisciplinary team. Micrognathia (a small jaw) is sometimes associated with cleft palate in the Pierre Robin syndrome with posterior displacement of the tongue (glossoptosis) and upper-airway obstruction.
A ranula is a mucous cyst on the floor of the mouth related to the sublingual or submandibular salivary ducts. Congenital ranulas may resolve spontaneously but sometimes require surgery.
Teeth usually begin to erupt at around 6 months but can be present at birth.
Examination sequence
Note the size, shape and position.
The helix should join the cranium above an imaginary line through the inner corners of the eyes.
Check that the external auditory meatus looks normal.
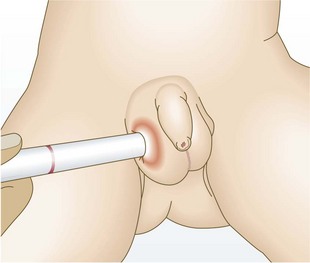
Otoscopic examination is not required for the newborn but is indicated in young infants to exclude otitis. A carer should hold the child to keep the head still (Fig. 15.22).
Choose the smallest earpiece available that fits the child’s meatus.
Gently pull the earlobe down and back to straighten the external auditory canal.
Insert the otoscope to approximately 0.5 cm. Adjust the angle gently until you see the tympanic membrane.
Abnormal findings: See Chapter 13.
Examination sequence
Inspect the neck for asymmetry, sinuses and swellings.
Palpate any masses. Use SPACESPIT to decide their likely origin (Box 3.11).
Transilluminate swellings to see if they are cystic. Cystic swellings glow, as the light is easily transmitted through clear liquid. Solid or blood-filled swellings do not.
Examination sequence
Observe the baby for pallor, cyanosis and sweating.
Look for the apex beat in the mid-clavicular line in the fourth or fifth intercostal space.
Note if the heart beat moves your hand up and down (parasternal heave) or if you feel a vibration (thrill).
Count the heart rate for 15 seconds and multiply by 4. Record the heart rate.
Feel the femoral pulses by placing your thumbs or fingertips over the mid-inguinal points while abducting the hips (Fig. 15.5).

Fig. 15.5 Palpating the femoral pulses.
The pulse can be difficult to feel at first; use a point halfway between the pubic tubercle and the anterior superior iliac spine as a guide.
Auscultate the heart. Start at the apex using the stethoscope bell (best for low-pitched sounds). Then use the diaphragm in all positions for high-pitched sounds and murmurs (Fig. 15.6).
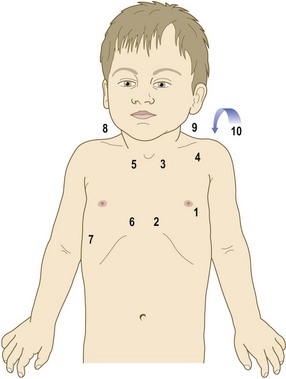
Fig. 15.6 Auscultation positions.
Recommended order of auscultation: 1, apex; 2, left lower sternal edge; 3, left upper sternal edge; 4, left infraclavicular; 5, right upper sternal edge; 6, right lower sternal edge; 7, right mid-axillary line; 8, right side of neck; 9, left side of neck; 10, posteriorly.
Describe the heart sounds S1 and S2, splitting of S2, any additional heart sounds and the presence of murmurs. The fast heart rate of a newborn makes it difficult to time additional sounds. Take time to tune into the different rate of the harsh breath sounds of a newborn as they are easily confused with a murmur.
Do not measure the blood pressure of healthy babies. In ill babies, cuff measurements overestimate the values when compared with invasive measurements. The cuff width should be at least two-thirds of the distance from the elbow to the shoulder tip.
Palpate the abdomen for hepatomegaly (p. 364).
Normal findings: In the early newborn period the femoral pulses may feel normal in an infant who later presents with coarctation because an open ductus arteriosus can maintain flow to the descending aorta. Routine measurement of postductal saturation is increasingly popular as an additional newborn screening test to avoid missing this. The liver edge is often palpable in healthy infants.
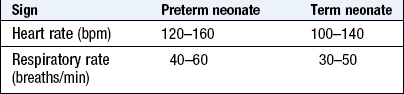
Heart rates between 80 and 160 bpm can be normal in the newborn, depending on the arousal state (Box 15.10).
Abnormal findings: Infants with heart failure typically look pale and sweaty and often present with respiratory distress (p. 358).
If the apex beat is displaced laterally there may be cardiomegaly, or mediastinal shift due to contralateral pneumothorax or pleural effusion.
Weak or absent femoral pulses suggest coarctation of the aorta. In older children and adults coarctation causes radiofemoral delay but this is not identifiable in the newborn.
Patent ductus arteriosus may cause a short systolic murmur in the early days of life because the pulmonary and systemic blood pressures are similar and this limits shunting through the duct. The murmur progressively lengthens over subsequent weeks or months to become the continuous ‘machinery’ murmur recognised later in childhood.
Murmurs are heard in up to 2% of neonates but only a minority have a structural heart problem. Many murmurs are transient. An echocardiogram is needed to make a structural diagnosis and this should be performed before discharge from hospital. If this is not possible and the infant is clinically well, with no respiratory distress and has normal femoral pulses and postductal oxygen saturation >95%, it may be reasonable to arrange outpatient review at 4–6 weeks, with advice to the parents to consult a doctor if they are concerned about breathlessness, poor feeding or cyanosis.
Examination sequence
Note chest shape and symmetry of chest movement.
Count the respiratory rate and listen for additional noises with breathing.
Look for signs of respiratory distress: tachypnoea, suprasternal, intercostal and subcostal recession, flaring of the alar nasae.
Percussion of the newborn’s chest is not helpful.
Use the diaphragm to auscultate anteriorly, laterally and posteriorly. Assess the air entry on each side and note any crackles and wheeze. Breath sounds in the healthy newborn have a bronchial quality compared with older individuals (p. 156).
Normal findings: Male and female newborn infants at term have small buds of palpable breast tissue. Small amounts of fluid are sometimes discharged from the nipple in the early days after birth.
Abnormal findings: Stridor is a large-airway sound and is predominantly inspiratory (pp. 142 and 313). Stridor and indrawing beginning on day 2–3 of life in an otherwise well baby may be due to laryngomalacia (softness of the larynx). Causes of respiratory distress include retained lung fluid, infection, immaturity, aspiration, congenital anomaly, pneumothorax, heart failure and metabolic acidosis.
Examination sequence
Inspect the abdomen, including the umbilicus and groins, noting any swellings.
From the infant’s right side, gently palpate with the flat of your warm right hand. Palpate superficially before feeling for deeper structures.
Palpate for the spleen. In the neonate it enlarges down the left flank rather than towards the right iliac fossa.
Place your right hand flat across the abdomen beneath the right costal margin.
Feel the liver edge against the side of your index finger.
If you feel more than the liver edge, measure the distance in the mid-clavicular line from the costal margin to the liver’s edge. Describe it in fingerbreadths or measure it with a tape in centimetres.
Look at the anus to confirm that it is present, patent and in a normal position.
Digital rectal examination is usually unnecessary and could cause an anal fissure. Indications include suspected rectal atresia or stenosis and delayed passage of meconium. Put on gloves and lubricate your little finger. Gently press your fingertip against the anus until you feel the muscle resistance relax and insert your finger up to your distal interphalangeal joint.
Normal findings: Distension from a feed or swallowed air is common.
You may see the contour of individual bowel loops through the thin anterior abdominal wall in the newborn, particularly with intestinal obstruction.
The umbilical cord stump usually separates after 4–5 days. A granuloma may appear later as a moist, pink lump in the base of the umbilicus. A small amount of bleeding from the umbilicus is common in the neonate.
The liver edge is often palpable in healthy infants.
In the neonate the kidneys are often palpable, especially if ballotted (Fig. 9.8).
Abnormal findings: In excessive bleeding from the umbilicus, check that the infant received vitamin K, and consider clotting factor XIII deficiency. Spreading erythema around the umbilicus suggests infective omphalitis, and requires urgent treatment.
Umbilical hernias are common, easily reduced, have very low risk of complication and close spontaneously in infancy. An omphalocoele, or exomphalos (Fig. 15.7), is a herniation through the umbilicus containing intestines and other viscera covered by a membrane that includes the umbilical cord. It may be associated with other malformations or a chromosomal abnormality. Gastroschisis is a defect in the anterior abdominal wall with intestines herniated through it. There is no covering membrane. The commonest site is above and to the right of the umbilicus.

A hydrocoele is a collection of fluid beneath the tunica vaginalis of the testis and/or the spermatic cord (p. 238). Most resolve spontaneously in infancy. Inguinal hernias are common in the newborn, especially in boys and preterm infants (Fig. 15.8).

Fig. 15.8 Bilateral inguinal hernias in a preterm infant.
An inguinal hernia is primarily a groin swelling; only when it is large does it extend into the scrotum.
Meconium in the nappy does not guarantee that the baby has a patent anus because meconium can be passed through a rectovaginal fistula.
Examination sequence
Abduct the legs and gently separate the labia.
In preterm infants the labia minora appear prominent, giving a masculinised appearance, which resolves spontaneously over the next few weeks. Milky secretions in the vagina are normal. Later in the first week there is sometimes slight vaginal bleeding (pseudomenses) as the infant uterus ‘withdraws’ from maternal hormones. Vaginal skin tags are common and do not require investigation or treatment.
Do not attempt to retract the foreskin. It is normal for it to be adherent in babies.
Check that the urethral meatus is at the tip of the penis.
If you cannot feel the testes in the scrotum, assess for undescended, ectopic or retractile testes. Palpate the abdomen for smooth lumps, moving your fingers down from over the inguinal canal to the scrotum and perineum.
A retractile testis just below the inguinal canal may be gently milked into the scrotum. Re-examine at 6 weeks if there is any doubt about the position of the testes.
Transilluminate any large scrotal swelling by placing a torch against it to see if the light is transmitted through the skin. This suggests a hydrocoele but can be misleading, because a hernia of thin-walled bowel may transilluminate (Fig. 15.9).
An inguinal hernia usually produces a groin swelling but if large this may extend into the scrotum. Try to reduce it by gently pushing the contents upwards from the scrotum through the inguinal canal into the abdomen. If this is possible it is an indirect inguinal hernia (Fig. 15.8).
Normal findings: The testes are smooth, soft and 0.7 × 1 cm across. The right testis usually descends later than the left and sits higher in the scrotum.
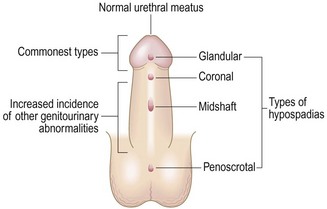
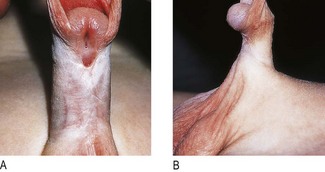
Abnormal findings: In hypospadias the meatal opening is on the ventral aspect of the glans, the ventral shaft of the penis, the scrotum or more posteriorly on the perineum (Figs 15.10 and 15.11A). In epispadias it is on the dorsum of the penis – this is rare. Chordee is curvature of the penis and is commonly associated with hypospadias and tethering of the foreskin (Fig. 15.11B).
Neurological examination: This includes tone, posture, movement and primitive reflexes.
Examination sequence
Look for asymmetry in posture and movement and for muscle wasting.
To assess tone, pick the baby up and note if he is stiff or floppy. Note any difference between each side.
Power is difficult to assess and depends on the state of arousal. Look for strong symmetrical limb and trunk movements and grasp.
Tendon reflexes are only of value in assessing infants with neurological or muscular abnormalities.
Check sensation by seeing whether the baby withdraws from gentle stimuli. Do not inflict painful stimuli or use a pin or needle.
Check eyesight by carrying the alert baby to a dark corner where she may open her eyes wide. If moved to a bright area she will then screw up her eyes.
Test hearing by noting the startle response to a sound. Ideally electronic audiological screening should be performed in the newborn period.
Normal findings: Movements should be equal on both sides.
Tone varies and may be floppy after a feed.
Reflexes are brisk in term infants, often with a few beats of clonus.
Abnormal findings: Hypotonic infants may have a ‘frog-like’ posture with abducted hips and extended elbows. Causes include Down’s syndrome, meningitis and sepsis.
Increased tone may cause back and neck arching and limb extension; the baby feels stiff when picked up. Causes include meningitis, asphyxia and intracranial haemorrhage.
Erb’s palsy affects brachial plexus roots C5 and C6, producing reduced movement of the arm at the shoulder and elbow, medial rotation of the forearm and failure to extend the wrist (Fig. 15.12).

Klumpke’s palsy may be seen after breech delivery due to damage to roots C8 and T1, with weakness of the forearm and hand.
Brachial plexus injuries can be associated with ipsilateral Horner’s syndrome and/or diaphragmatic weakness in severe cases. Most perinatal brachial plexus injuries do not involve complete disruption of the nerve roots and recover over subsequent weeks.
Facial nerve palsy causes reduced movement of the cheek muscles, and the side of the mouth does not turn down when the baby cries. Most cases are transient.
Primitive reflexes: The primitive reflexes are lower motor neurone responses present at birth but which disappear by 4–6 months as they become suppressed by higher centres. They may be absent in infants with neurological depression or asymmetrical in infants with nerve injuries. Persistence into later infancy may indicate neurodevelopmental abnormality (Ch. 11). There are many examples and there is no need to elicit them all because their individual value is limited.
Examination sequence
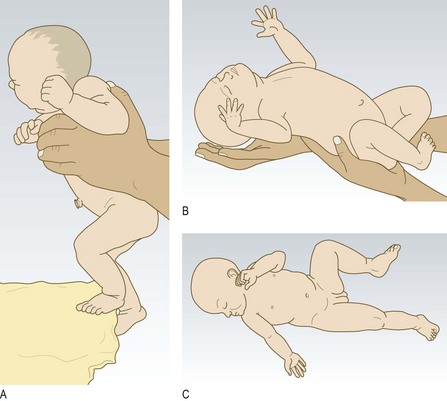
Hold the baby upright and touch the dorsum of his foot against the edge of the table. The baby will flex the knee and hip, placing the foot on the table (Fig. 15.13A).
Lower the upright baby towards the surface of the table. When the feet touch the surface, a walking movement occurs.
Support the supine baby’s trunk and head in a semi-upright position. Let his head fall backwards slightly. The baby will quickly throw out both arms and spread his fingers (Fig. 15.13B).
Turn the supine infant’s head to the side. The arm and leg on the same side will extend and the arm and leg on the opposite side will flex. This reflex is present at term and maximal at 1 month (Fig. 15.13C).
Normal findings: A small percentage of normal babies have single palmar creases but this is also associated with Down’s syndrome (Fig. 3.12B) and other chromosomal abnormalities. Tibial bowing is common in the newborn.
Abnormal findings: Oligodactyly (too few digits), polydactyly (too many) or syndactyly (joined digitis) may occur. In talipes equinovarus the foot is plantar flexed and rotated, so that the sole faces medially. In talipes calcaneovalgus the foot is dorsiflexed so that the heel is prominent and the sole faces laterally.
Hips: Check for developmental dysplasia of the hip (DDH). Many cases have associated risk factors, including a family history of DDH, breech delivery, positional talipes (especially calcaneovalgus) or oligohydramnios.
Examination sequence
Lay the baby supine on a firm surface.
Look at the thighs for symmetry of the skin creases.
Examine each hip separately. Hold the thigh with the knee and hip flexed and your thumb on the medial aspect of the thigh.
Move the proximal end of the thigh laterally and then push down towards the examining table (Barlow manoeuvre) (Fig. 15.14A); a clunk indicates that the hip is dislocatable.
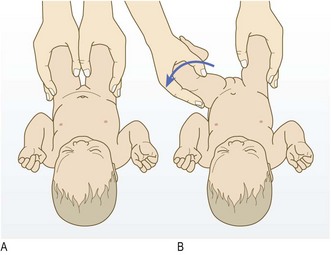
Fig. 15.14 Examination for developmental dysplasia of the hip.
(A) The hip is dislocated posteriorly out of the acetabulum (Barlow manoeuvre). (B) The dislocated hip is relocated back into the acetabulum (Ortolani manoeuvre).
Now abduct the thigh; if you feel a clunk, this is the head of the femur returning into the acetabulum (Ortolani manoeuvre) (Fig. 15.14B). If the femoral head feels lax and you feel a clunk with an Ortolani manoeuvre without first performing the Barlow manoeuvre, then the hip is already dislocated.
Never use the term ‘clicky hips’. It is common to hear or feel minor ligamentous clicks during hip examination. These are of no consequence and feel quite different to the dislocation and relocation of DDH. If in any doubt, obtain an expert opinion. Some centres have an ultrasound screening programme.
Check the hips whenever you examine an infant until he is walking normally. After the first few months the Ortolani and Barlow manoeuvres cannot be performed and the most important signs are limitation of abduction in the hip and thigh skin crease asymmetry.
Weighing and measuring
Examination sequence
Weigh the infant fully undressed using electronic scales that are accurate to 5 grams.
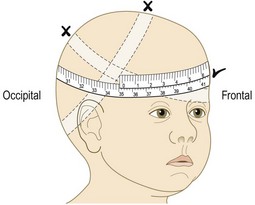
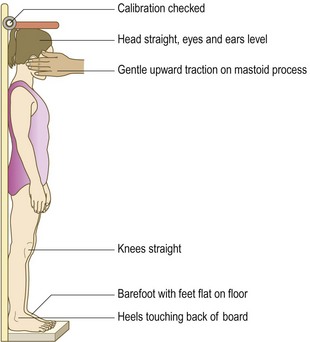
Use a paper tape to measure the occipitofrontal circumference round the forehead and occiput at the largest part (Fig. 15.15). Take the measurement three times. Note the largest measurement to the nearest millimetre.
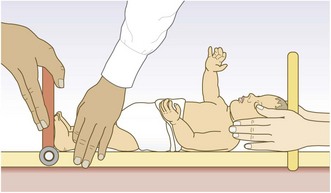
Measure the crown–heel length using a neonatal stadiometer (Fig. 15.16). Ask a parent or assistant to hold the baby’s head still and stretch out the legs so that the baby is fully extended (the least reproducible of the three measurements).
Record the results on a centile chart appropriate to the infant’s population.
Examination of Children
Children are individuals between 12 months and 16 years and are known by non-specific terms, including toddlers, preschoolers, school children, students, adolescents, teenagers or youths.
Symptoms and definitions
Growth: Growth after infancy is extremely variable. Use gender- and ethnic-specific growth charts (Fig. 15.17). These compare the individual to the general population and with his own previous measurements. Failure to thrive is failure to attain the expected growth trajectory. An individual child should grow along a centile line for height and weight throughout childhood. A child on the 0.4th centile for height may be thriving if this has always been his growth trajectory, while a child on the 50th centile for height can have failure to thrive if previously he was on the 99.6th centile.
A child’s height is related to the average of his parent’s height centile ± 2 standard deviations above and below this average. Parents whose average height centile is the 50th will have children whose height will normally lie between the 2nd and 98th centile (approximately 10 cm above and below the 50th centile).
Neurological development: Normal development is heterogeneous within the population. The major determinant is the child’s environment. The second is the child’s genetic potential. This variability makes identifying abnormalities difficult. Developmental assessment requires patience, familiarity with children and an understanding of the range of normality for a given age.
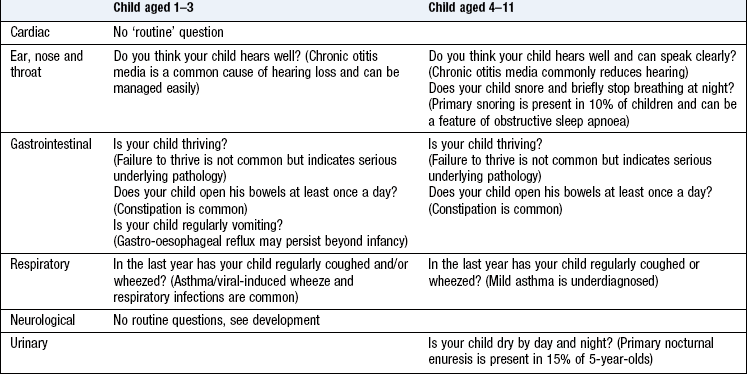
The preschool child (1–5 years)
At the younger end of this age range, questions relating to gross motor skills are most sensitive; as the child becomes older, questions relating to fine motor and personal social skills are more meaningful. Delayed speech with normal attainment of motor milestones is not uncommon, particularly in boys, but needs hearing assessment (Box 15.6).
The school-age child (5+ years)
By this age, any developmental problems are usually known to parents and relevant agencies may already be engaged, e.g. education. However, more subtle developmental problems such as dyslexia (a learning disability affecting the individual’s fluency and comprehension in reading) may be unrecognised and can be a major handicap. Ask general questions, such as: ‘How is your child getting on at school?’ and follow up by enquiring specifically about academic and social activity.
Growth and developmental assessment of the child born prematurely
Infants born prematurely are small and transiently demonstrate developmental delay in early life, partly due to their immaturity and partly to them being in a hospital environment for long periods after delivery (Box 15.11).
15.11
Development of the premature infant
Infants born prematurely without neurological complications tend to catch up in growth and developmental milestones after going home. At 1 year, they may demonstrate some subtle growth and developmental delay but by their second birthday their growth and development should be the same as that of a term infant.
Wilson SL, Cradock MM. Review: Accounting for prematurity in developmental assessment and the use of age-adjusted scores. J Pediatr Psychol 2004;29:641–649.
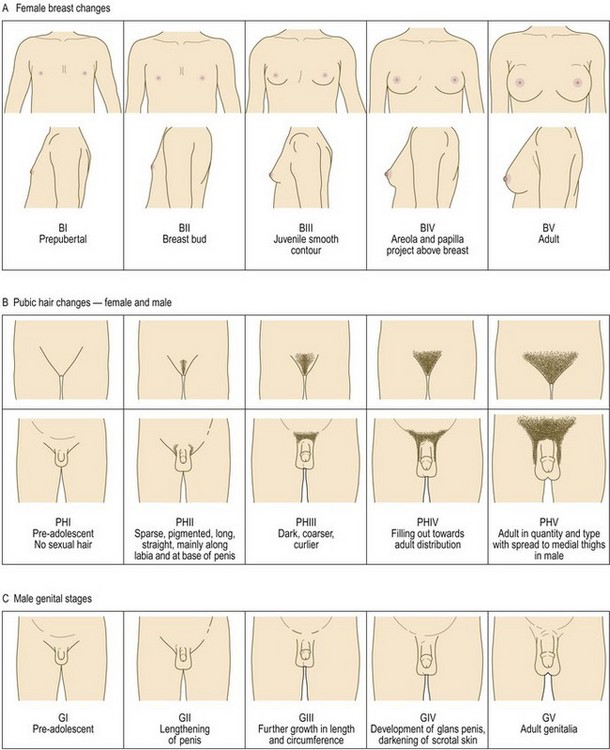
Puberty
This stage of adolescence, when an individual becomes physiologically capable of sexual reproduction, is a time of rapid physical and emotional development. The age at onset and end of puberty varies hugely but is generally 10–14 years for girls and 12–16 years in boys (Fig. 15.18). The average child grows 30 cm during puberty and gains 40–50% in weight.
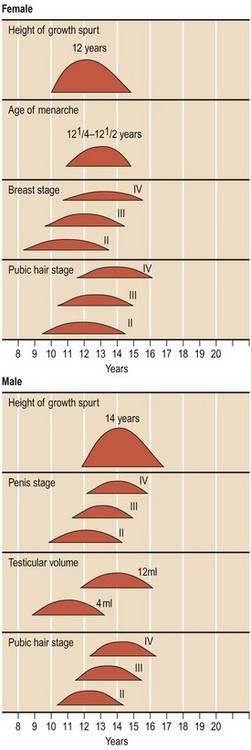
If required, a chart to stage puberty (Fig. 15.19). Pubertal staging has a wide normal range, with abnormalities only apparent on follow-up. Delayed or precocious puberty is not uncommon.
Pain
Pain and the need for analgesia can be difficult to assess in young children. Use an objective scoring system (Box 15.12).
15.12 Pain assessment tool
FLACC* scale
| 0 | 1 | 2 |
| No particular expression or smile | Occasional grimace or frown, withdrawn, uninterested | Frequently or constantly quivering chin, clenched jaw |
| Normal position or relaxed | Uneasy, restless, tense | Kicking or legs drawn up |
| Lying quietly, normal position, moves easily | Squirming, shifting back and forth, tense | Arched, rigid or jerking |
| No cry (awake or asleep) | Moans or whimpers, occasional complaint | Crying steadily, screams or sobs, frequent complaints |
| Content, relaxed | Reassured by occasional touching, hugging or being talked to, distractible | Difficult to console or comfort |
Each category is scored on a 0–2 scale to give a total score of 0–10: 0 = no pain; 1–3 = mild pain; 4–7 = moderate pain; 8–10 = severe pain.
*FLACC, face, legs, activity, cry, consolability.
The history
Introduce yourself to the child and accompanying adult. Establish who the adult is, e.g. parent, grandparent, and decide whether the child will be prepared to give a useful history. You should already be observing the child.
Similarities in history taking between children and adults
There are many similarities in taking a history from a child and an adult. Start with open-ended questions, encouraging the parent or child to respond. During this you should be considering the differential diagnosis while informally inspecting the patient. The differential diagnosis determines which closed questions you ask and also focuses your examination. The closed questions are similar to those used in adults, although the conditions may be different. Good communication skills are equally relevant in paediatrics and adult practice, e.g. listening carefully, prompts such as ‘yes’ to encourage the historian to continue, and internal summarisation, e.g. ‘so what you are saying is that…’.
Differences in history taking from adults
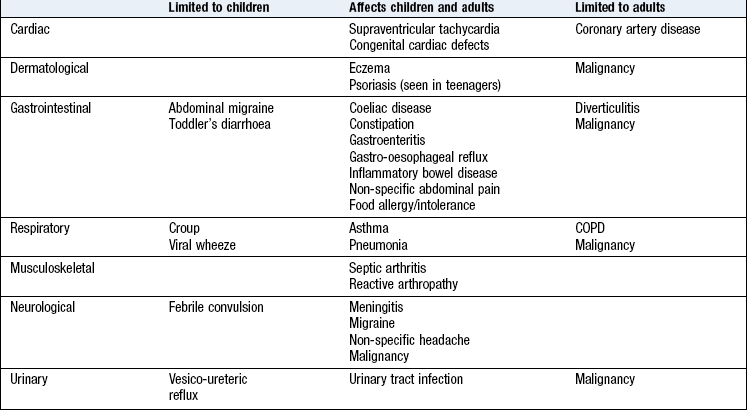
The considerable differences in physical, emotional and social attributes of children mean there is no single approach to history taking and examination. Be flexible and adapt your approach for every clinical encounter with children. The history may not be provided by the patient (Box 15.13). Children <6 years cannot give a history and children 6–11 years often have difficulty in expressing themselves clearly and are reluctant historians. If appropriate, ask the child about the problem, although in many cases the parent will volunteer the history. Direct your questions to children >11 years. Always acknowledge the younger child (say hello) even if the parent is providing the history. A paediatric history includes components not in the adult history (obstetric, developmental, immunisation histories) and the systematic enquiry is different from that for adults (Box 15.14). Some conditions affect only children, some only adults and some affect both.
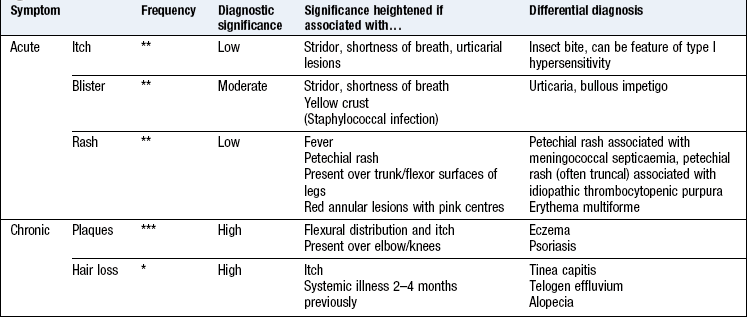
Symptoms and signs
First make a differential diagnosis by identifying the part or system of the body involved; then use closed questions to identify the most likely diagnosis. Diagnosis is built upon patterns of symptoms. Rarely will any one symptom or sign lead to a ‘spot diagnosis’. Pattern recognition is an art which requires regular practice.
Boxes 15.15–15.18 describe symptoms in the context of:
15.15 Respiratory system
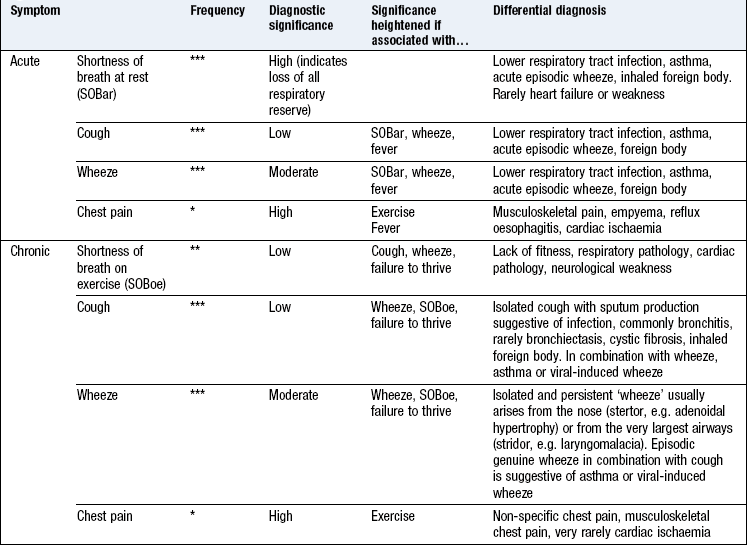
Respiratory sounds: clarify what noise the parent or child is describing. The historian can sometimes identify where the sound is coming from, e.g. nose (stertor), throat (stridor) or chest (rattle or wheeze). A constant respiratory sound is more likely to be stertor, stridor or rattle. A sound associated with vibration of the chest is a rattle. A very loud sound, e.g. heard in the next room, is not genuine wheeze.
Coexistent failure to thrive or weight loss always increases the significance of any symptom.
15.16 Gastrointestinal system
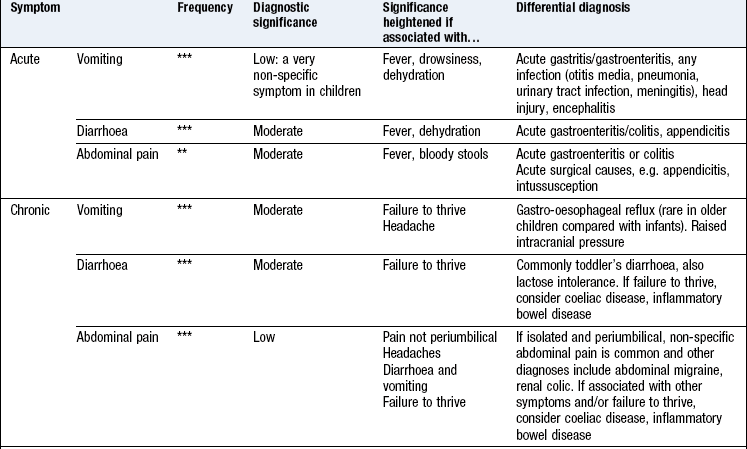
Symptoms of dehydration include dry mouth, foul-smelling breath, anuria and lethargy.
Coexisting failure to thrive or weight loss always increases the significance of any symptom.
Abdominal pain can be difficult to identify in young children who are not able to express themselves.
15.17 Nervous system
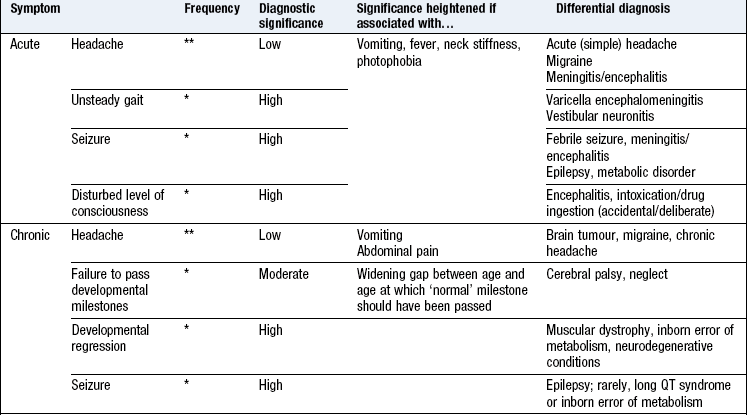
Chronic headache can also arise from the mouth, e.g. dental abscess, or face.
An acute seizure can be confused with a rigor in a febrile child. A seizure involves slow (1 beat/second) coarse, jerking which cannot be stopped, loss of consciousness and postictal drowsiness. A rigor is characterised by rapid (5 beats/second) fine jerking which can be stopped by a cuddle and no loss of consciousness.
Presenting complaint
What is the primary symptom? What is its duration? Knowing the child’s age, symptom and its duration provides an initial differential diagnosis.
For chronic conditions, establish how symptoms affect the quality of life and activities of daily living of the child and family.
Past medical history
Does the child have other health problems and medication? Has he been in hospital before and if so, why?
Vaccination history
Vaccination schedules vary over time and between countries. Are the child’s immunisations up to date and if the child is not immunised, why not?
Family history
Do any of the child’s first- or second-degree relatives have similar symptoms? This information may not be available for adopted children and when a parent is not known. Consider parental consanguinity, which is not uncommon among some ethnic groups.
Social history
Children’s families may include step siblings and several adults who share responsibility for raising them. Establish who is responsible for the child and find out how the child perceives his family. Children at risk for neglect often have complex domestic arrangements, e.g. several caregivers.
Ask about exposure to tobacco smoke and offer parents who smoke cessation advice. Asking about the presence of cats and dogs is usually unhelpful as no interventions are proven to benefit (unless there is a very clear relation between symptoms and exposure, in which case hopefully parents will have removed the pet from the household).
Some chronic symptoms are associated with anxiety or potential gain for the child, e.g. chronic cough, abdominal pain and headache in a well-looking 8–12-year-old with normal examination. A psychological history helps determine the degree of associated anxiety and potential gain for the child. Look carefully for the child’s facial expression, eye contact and body language. Ask specifically about school (avoidance and bullying), social interactions (does the child have many friends?) and out-of-school activities.
Open-ended questions showing empathy, such as ‘That sounds difficult. How did it make you feel?’ are useful. Symptoms in a child who misses a lot of school but is never unwell during summer holidays are likely to be less severe than those which stop a keen footballer from playing.
Dietary history
This is not routinely needed except in situations such as poor weight gain, obesity or food-related symptoms, e.g. anaphylaxis.
Drug history
Prescribing errors often arise from a poorly documented drug history. Transcribe the medication, dose and frequency direct from the medication package or referral letter if possible. Find out about any difficulties in taking medication to establish concordance. Clarify any adverse reactions to medications, especially antibiotics.
Psychiatric history
Psychiatric disorders are uncommon, and often atypical, in primary school children. Take a full adult psychiatric history from adolescents with a potential psychiatric diagnosis (p. 20).
Systematic enquiry
This screens for illnesses or symptoms not recognised as important by the child or parents. Use the adult questions, excluding irrelevant ones for the age group (Box 15.19).
The physical examination
Children usually present with a symptom. Children with acute symptoms often have physical signs such as wheeze (Box 15.20) but examination is normal in the majority of children with chronic symptoms. Routine screening examination after infancy is unhelpful as most paediatric diseases only produce signs late in the illness.
15.20
Wheeze
Parents and children often call wheeze, stridor, stertor or rattle, ‘wheeze’.
Saglani S, McKenzie SA, Bush A et al. A video questionnaire identifies upper airway abnormalities in preschool children with reported wheeze. Arch Dis Child 2005;90:961–964.
Similarities in examination between children and adults
The techniques used when examining children are the same as those in adults, with some exceptions. Examining a child is a skill which takes time to learn. Usually the history suggests the diagnosis; the examination confirms it and its severity.
Differences in examination between children and adults
Consider children in three age ranges: 1–3, 3–5 and >5 years.
1–3 years: Carefully inspect the child while taking the history since formal examination may not be feasible. All children pass through a stage when they can be reluctant to be examined, commonly known as the ‘terrible twos’. This developmental stage begins in mid-infancy and carries on to ~3 years. During this time children are anxious in the presence of strangers and become upset when parents leave them (separation anxiety). Carefully observe the child’s general condition, colour, respiratory rate and effort, and state of hydration while taking the history and the child is oblivious to your close attention. For the formal examination, ask the parent to sit the child on her knees. Examine the cardiorespiratory system and the abdomen with the young child sitting upright on the parent’s knee. With patience, abdominal examination can be done with the child lying supine on the bed next to a parent or on the parent’s lap. Removing your stethoscope from around your neck can trigger the child to become upset. If the child starts crying, chest auscultation and abdominal palpation become almost impossible; persevering will provoke more crying.
3–5 years: Some children in this age range have the confidence and maturity to comply with some components of the adult examination. Others remain apprehensive with strangers. Children’s social skills regress when they are unwell.
5+ years: The child may comply with a full adult style of examination. Although children <11 years are often not able to express themselves well, children >5 years are able to understand and comply with requests, e.g. finger-to-nose pointing, heel-to-toe walking, ‘sit forward’ and ‘take a deep breath in and hold it’.
Remember that a normal examination does not exclude pathology.
The acutely unwell child
There are many non-specific signs that are not diagnostic and common to a range of conditions from a simple cold to meningitis (Box 15.21). However, some signs are serious, requiring immediate investigation and management (Box 15.22).
15.22 Serious signs requiring immediate attention
• Poor perfusion (indicating shock)
• Reduced capillary refill (indicating shock)
• Cool peripheries (indicating shock)
• Petechial rash over the trunk (suggesting meningococcal septicaemia)
• Headache, photophobia or neck stiffness (suggesting meningitis)
• Dyspnoea at rest (indicating loss of respiratory reserve due to pneumonia, asthma)
Children become ill quickly. A child unwell for <24 hours where the initial examination reveals only non-specific signs should ideally be reassessed in 1–2 hours.
Leave throat and ears examination until the end and be opportunistic and flexible in the order of examination.
Ears, nose and throat
Children are often reluctant to be examined.
Examination sequence
sit the child on her knees, both facing you
place one arm over the child’s upper arms and chest (to stop the child pushing you away) (Fig. 15.21)
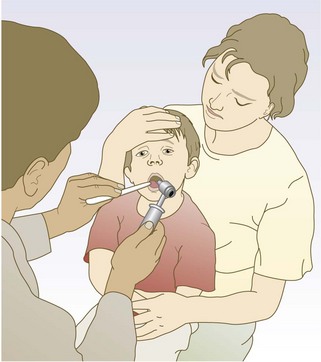
hold the child’s forehead with the other hand (to stop the child pulling his chin down to his chest).
Hold the torch in your non-dominant hand to illuminate his throat.
Slide a tongue depressor inside the child’s cheek with your dominant hand. He should open his clenched teeth (perhaps with a shout), showing his tonsils and pharynx.
Abnormal findings: Healthy tonsils and pharynx look pink; when inflamed they are crimson red.
Inspecting the throat reveals the presence, but not the cause, of the infection; pus on the tonsils and pharynx does not differentiate a bacterial from viral infection (p. 312).
Examination sequence
sit the child across her knees with the child’s ear facing you
place one arm around the child’s shoulder and upper arm facing you (to stop him pushing you away) (Fig. 15.22)

place the other hand over the parietal area above his ear facing you (to keep the child’s head still).
Use an otoscope with the largest speculum that will comfortable fit the child’s external auditory meatus.
To straighten the ear canal and visualise the canal and tympanic membrane, hold the pinna gently and pull it out and down in a baby or toddler with no mastoid development and up and back in a child whose mastoid process has formed. Mastoid development causes the canal to elongate forwards and medially, changing the direction of pull required to straighten it (p. 303).
Normal findings: Palpable neck and groin nodes are extremely common in children <5 years old. They are typically bilateral, <1 cm in diameter, hard, mobile and with no overlying redness and can persist for many weeks. In the absence of systemic symptoms, e.g. weight loss, fevers, night sweats, these are invariably a normal, healthy immune response to infection. Only very rarely are they due to malignancy (Box 15.24).
 15.24
15.24Respiratory system
Abnormal findings: The child <3 years has a soft chest wall and relatively small stiff lungs. In respiratory distress the diaphragm contracts vigorously to reduce intrathoracic pressure and draw air into the airways. This produces chest wall recession (ribs ‘sucking in’) and extrusion of the abdomen (wrongly called ‘abdominal breathing’).
Children’s thinner chests transmit noises easily and their smaller airways are more prone to turbulence and added sounds. Auscultation may reveal a variety of sounds, including a fine expiratory polyphonic wheeze, fine end-expiratory crackles (similar to the noise made by rubbing hairs between your fingers by your ear), coarse louder crackles transmitted from the larger airways and other sounds described as pops and squeaks (typically in the chest of recovering asthmatics). Loud added sounds without dyspnoea or recession are unlikely to be clinically relevant. Dyspnoea with or without recession is a more important sign than added sounds. What you see is more important than what you hear.
Cardiovascular system
Feel the brachial pulse in the antecubital fossa in children <2–3 years. Do not palpate the carotid or radial pulses in young children. Measure blood pressure using a cuff sized two-thirds the distance from elbow to shoulder tip. Repeat with a larger cuff if the reading is elevated. If in doubt, use a larger cuff as smaller cuffs yield falsely high values.
Gastrointestinal system
In children 6 months to 3 years, examine the abdomen with the child sitting upright on his parent’s knee. In the young child, splenic enlargement causes the spleen to move down into the left iliac fossa. In older children the enlarged spleen moves towards the right iliac fossa. Rectal examination is rarely indicated in children.
Nervous system
You are stronger than the child so test power by watching the child demonstrate his strength against gravity. Ask him to lift his arms above his head; raise his leg from the bed whilst lying; stand from a squatting position.
Neck stiffness is usually apparent in a child when you are talking to him or the parents. If in doubt, ask the child to move his head from side to side or test as for adults (Fig. 11.2). With a young child, move a toy to catch his attention and see if he moves his head.
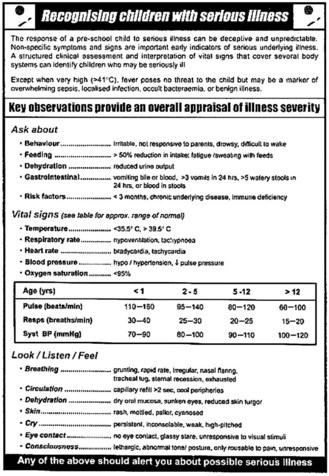
Spotting the sick child
It can be difficult to identify a child with severe illness. With experience you will learn to identify whether a child is just miserable or really ill (Fig. 15.23). Early-warning scores can help (Box 15.25).
15.25
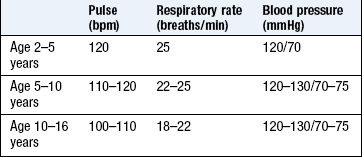
Early-warning scores in children
Early-warning scores, involving the measurement of temperature, pulse, respiratory rate and blood pressure, can help identify children at risk for severe illness.
Akre M, Finkelstein M, Erickson M et al. Sensitivity of the pediatric early warning score to identify patient deterioration. Pediatrics 2010;125:e763–e769.
Certain features correlate with severe illness (Box 15.26).
Child protection
Children who experience neglect or physical and/or emotional abuse are at increased risk of health problems. At-risk children are often already known to other agencies but this information may not be known to you in the acute setting. Injuries from physical abuse can be detected visually. Consider non-accidental injury if the history is not consistent with the injury or the injury is present in unusual places, e.g. over the back. It is difficult to detect neglect during a brief encounter but think of it if the child appears dirty and wearing dirty or torn clothes which are too small or too large. The parent–child relationship gives insight into neglect; the child is apparently scared of the parent (‘frozen watchfulness’) or the parent is apparently oblivious of the child’s attention (Box 15.27).
15.27 Signs that may suggest child neglect or abuse