The ear, nose and throat
The ear
The ear is the specialised sensory organ of hearing and balance.
External ear
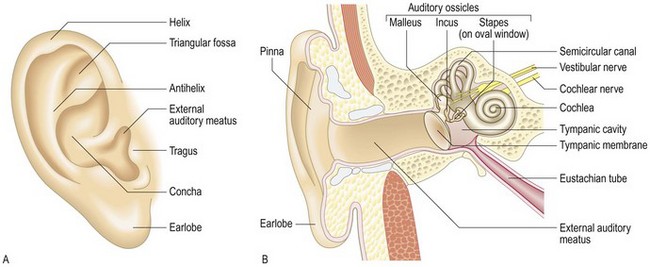
The pinna, external auditory canal (meatus) and the lateral surface of the tympanic membrane (eardrum) (Fig. 13.1) are the only blind-ending skin-lined tract in the body. It has a self-cleansing mechanism with outward migration of desquamated cells which are incorporated with cerumen to form wax.
Middle ear
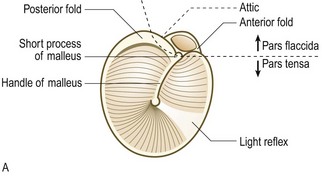
The air-filled chamber of the middle ear amplifies sound. The eardrum’s vibrations are amplified by the lever of the three articulated ossicles – malleus, incus and stapes. These vibrations are focused and further amplified on the much smaller area of the oval window. The Eustachian tube allows continual restoration of atmospheric pressure in the middle ear from the postnasal space. The handle of the malleus is attached to the drum, behind which the long process of the incus may also be visible on otoscopy (Fig. 13.2). Between the malleus and incus run the taste fibres from the anterior two-thirds of the tongue, which have ‘hitched a ride’ with the facial nerve. The upper part of the tympanic membrane is flaccid.

Inner ear
The stapes footplate vibrates in the oval window directly stimulating fluid within the cochlear (hearing) part of the inner ear. The other part of this bony labyrinth is the sensory organ of balance. Inner-ear epithelial cells convert the movement of their ‘hairs’ into electrical impulses along the vestibulocochlear (VIIIth) nerve. The vestibular part of the inner ear contains:
• the lateral, superior and posterior semicircular canals. These are arranged at right angles to each other, to detect rotational motion of their fluid (endolymph) in three planes
• the utricle and the saccule, whose cell hairs project into a gel layer containing small deposits (otoliths) which are subject to gravity, head tilt and linear endolymph movement.
Symptoms and definitions
See Box 13.1.
 13.1 Symptoms and definitions in ear disease
13.1 Symptoms and definitions in ear disease
| Symptom | Definition | Common cause |
| Otalgia | Pain | Otitis media or externa, referred from pharyngitis, trauma or, rarely, cancer |
| Pruritus | Itching | Otitis externa |
| Otorrhoea | Discharge | |
| Purulent | Eardrum perforation with infection | |
| Otitis externa | ||
| Mucoid | Eardrum perforation, severe trauma causing leak of cerebrospinal fluid | |
| Blood-stained | Granulation tissue from infection, trauma | |
| Hearing loss | Deafness | |
| Tinnitus | Noise in the absence of an objective source | Presbyacusis, noise damage |
| Vertigo | Hallucination of movement | Inner-ear disease |
| Unsteadiness | Vestibular or central disease |
Pain and itching
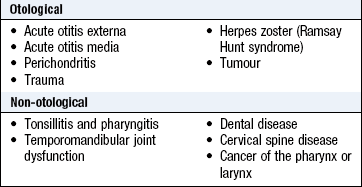
These are common. Earache may be referred from the throat (Boxes 13.2 and 13.3).
 13.3
13.3
Acute otitis media in children
No one criterion is a reliable indicator of acute otitis media in children. A 10-point scoring system, including pain, irritability, fever and otoscopic appearances, has been shown to have a sensitivity of 87%, specificity of 98%, positive predictive value of 91% and negative predictive value of 97%.
Casey JR, Block S, Puthoor P et al. A simple scoring system to improve clinical assessment of acute otitis media. Clin Pediatr 2011;50:623–629.
Otorrhoea
Otorrhoea is a discharge from the ear. A chronic offensive scanty discharge may be a sign of a cholesteatoma, an invasive keratin-filled outpouching of the drum. Bleeding is most often due to the infected granulation tissue. Painful or itchy discharge implies otitis externa.
Hearing loss
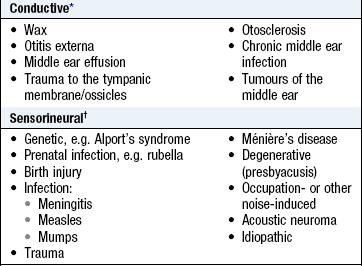
Hearing loss may be due to a failure of the VIIIth nerve or its endings – sensorineural – or of the conduction mechanisms of the middle ear by fluid, fixation or drum perforations or wax obstructing the external auditory meatus. Profound loss before speech acquisition affects speech quality, often vowel-based and lacking clear articulation (Box 13.4).
Tinnitus
Phantom ear noise, usually described as a ‘ringing’, in the absence of external stimuli, affects almost everyone at some time. Tinnitus is usually associated with hearing loss.
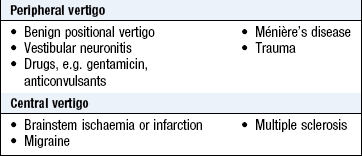
Vertigo
Vertigo is a sensation of movement relative to surroundings. Rotational movements are most common and usually originate in the semicircular canals or, less often, centrally in the brainstem or cerebellum (Box 13.5). Ask about the following to make the diagnosis (Boxes 13.6 and 13.7):
 13.7 Drugs that cause ototoxicity
13.7 Drugs that cause ototoxicity
| Type | Examples |
| Antibiotics | Aminoglycosides, e.g. gentamicin |
| Cytotoxics | Cisplatin |
| Diuretics | Furosemide given intravenously after aminoglycosides |
| Analgesics | Aspirin |
| Others | Quinine |
• positional and other precipitating factors
• associated or fluctuating hearing loss or tinnitus
• whether the ear feels ‘full’ during the episode
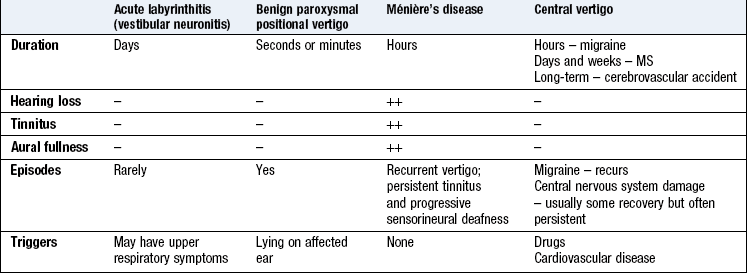
Benign paroxysmal positional vertigo (BPPV) causes attacks that are particularly marked when lying on one side. It may be due to debris in the posterior semicircular canals. Idiopathic acute vestibular dysfunction (vestibular neuritis) is possibly due to reactivation of latent herpes simplex virus type 1. There is nausea, acute rotatory vertigo and horizontal spontaneous nystagmus (with a rotational component) toward the unaffected ear. The patient tends to falls towards the side of the affected ear. The condition lasts for days or weeks before resolving completely.
Ménière’s disease is a rare condition that causes an episodic sensation of fullness in the ear with tinnitus, severe vertigo and headache. Between attacks, examination is normal, but hearing may be disturbed – most commonly, low-tone deafness. The diagnosis is confirmed by demonstrating excess endolymph on gadolinium-enhanced magnetic resonance imaging.
Unsteadiness
Feeling lightheaded is not a vestibular symptom, but unsteadiness may be. The rare, life-threatening causes of vertigo and unsteadiness are central, i.e. from brainstem or cerebellar changes.
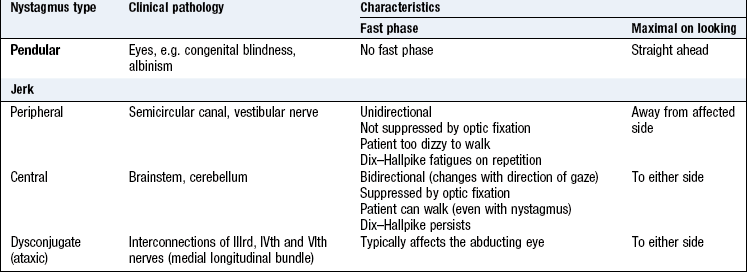
Nystagmus
Nystagmus is an involuntary rhythmical oscillation of the eyes. It may be vertical, horizontal, rotatory or multidirectional. The commonest form is horizontal, jerk nystagmus with a slow (pathological) drift of both eyes in one direction, then a fast correction in the opposite direction. The direction of the fast jerk is used to define the direction of the nystagmus. A patient with horizontal jerk nystagmus visible on examination and who is steady enough to be able to walk into a consulting room has a central lesion. Pendular nystagmus (oscillations equal in rate and amplitude about a central point) occurs with central vision defects.
The history
Ask about previous middle ear infection or trauma and systemic disorders associated with hearing loss, e.g. granulomatosis with polyangiitis (previously known as Wegener’s granulomatosis).
The physical examination
 Examination sequence
Examination sequence
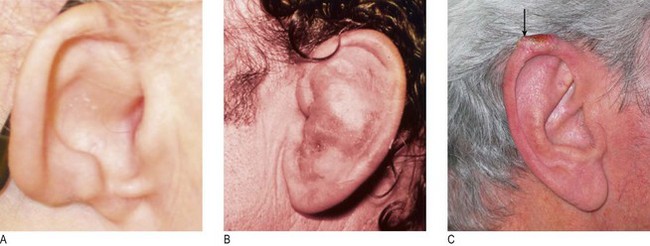
 Note the skin, shape, size and any deformity of the pinna (Fig. 13.4A).
Note the skin, shape, size and any deformity of the pinna (Fig. 13.4A).
Gently pull on the pinna to check for pain.
Use the largest otoscope speculum that will comfortably fit the meatus. Explain to the patient what you are going to do.
Hold the otoscope comfortably and rest the ulnar border of your hand against the patient’s cheek (Fig. 13.3). Then, if the patient’s head moves, your hand will cause less ear trauma.
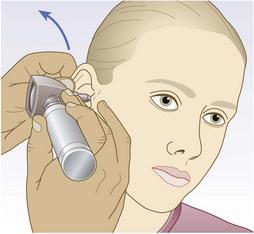
Gently pull the pinna upwards and backwards to straighten the cartilaginous external auditory meatus. Look at the canal skin through the speculum. Check for discharge, wax and foreign bodies. You should see a light reflex on a pearly grey, translucent normal tympanic membrane (Fig. 13.2B).
Abnormal findings: Congenital deformities are linked to sensorineural deafness. Low-set ears imply a first branchial arch abnormality. Trauma may produce a haematoma of the pinna (Fig. 13.4B), or mastoid bruising (if there is a skull base fracture). Basal cell and squamous cell cancers affect the fine skin of the rim of the pinna (Fig. 13.4C). Tenderness on palpation of the tragus suggests inflammation of the canal or adjacent temporomandibular joint. A very wide meatus suggests previous mastoid surgery. If the drum is not perforated, discharge is due to otitis externa (Fig. 13.5A), which may be so severe as to close off the meatus completely (furunculosis). The bony canal occasionally reveals exostoses (Fig. 13.5B).

Fig. 13.5 Auditory canal abnormalities.
(A) Otitis externa. (B) Exostosis of external auditory meatus. (C) Cholesteatoma.
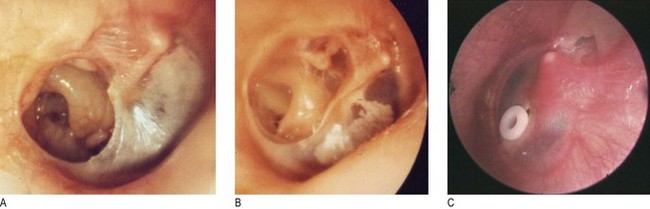
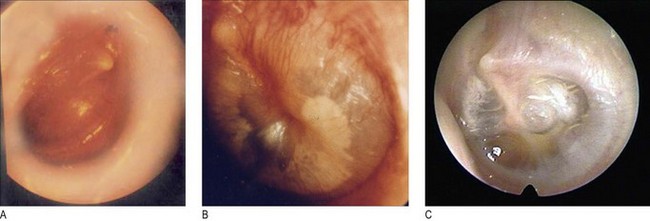
White scars on the tympanic membrane are tympanosclerosis. Note the position and percentage of the drum involved by any perforation (Fig. 13.6A). A severe retraction pocket of the pars tensa may mimic a perforation (Fig. 13.6B), as may a cholesteatoma sac of the pars flaccida (Fig. 13.5C). The drum may look normal, or dull, or golden, or bluish. Fluid or effusion behind the drum is called otitis media with effusion (Fig. 13.7B) and a fluid level may be seen (Fig. 13.7C). Surgical treatment is by insertion of a ventilation tube or grommet (Fig. 13.6C). In acute suppurative otitis media the drum becomes gradually more inflamed (Fig. 13.7A) and may eventually perforate.
Testing hearing
Examination sequence
Start with your mouth about 15 cm from the ear you are testing.
Mask hearing in the other ear by rubbing the tragus.
Ask the patient to repeat your words. Use a combination of multisyllable numbers and words. Start with a normal speaking voice to confirm that the patient understands the test. Lower your voice intensity to a clear whisper.
Repeat, but this time at arm’s length from the patient’s ear.
People with normal hearing can repeat words whispered at 60 cm.
Tuning fork tests: Use a 512 Hz or 256 Hz tuning fork to help differentiate between conductive and sensorineural hearing loss.
Examination sequence
Hit the prongs of the fork against a padded surface to make it vibrate.
Place the base of the vibrating tuning fork in the middle of the patient’s forehead.
Ask: ‘Where do you hear the sound?’
Record which side Weber’s test lateralises to if not central (Fig. 13.8).
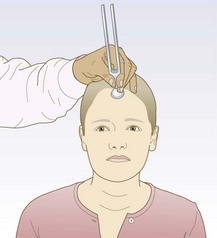
Abnormal findings: The noise is louder in an ear with conductive deafness (test on yourself by putting a finger in your outer canal to block out surrounding noise). In unilateral sensorineural deafness the sound is heard better in the better-hearing ear. In symmetrical hearing loss it is heard in the middle.
Examination sequence
Place the vibrating prongs at the patient’s external auditory meatus; ask if he can hear it.
Now place the still-vibrating base on the mastoid process. Ask: ‘Is it louder in front, or behind your ear?’ (Fig. 13.9).
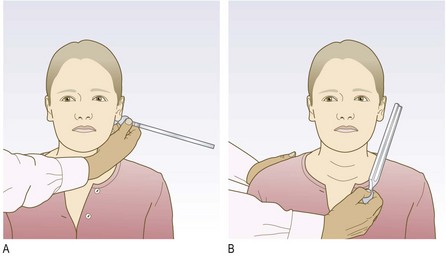
Normal findings: The sound is louder at the ear, that is, air conduction is better than bone conduction. Record this as AC > BC; this is normal (Rinne positive).
Abnormal findings: If the sound is louder on the mastoid process, bone conduction is better than air conduction. Record this as BC > AC (Rinne negative). This applies in conductive deafness.
A false-negative Rinne’s test may occur if hearing is very poor on one side. Then, the sound travelling through the air is not perceived but, when the tuning fork is placed on the mastoid process of the ‘poor’ ear, the sound is conducted through the skull and heard in the ‘good’ ear.
In a mild conductive deafness, the Weber test is abnormal (lateralised) before the Rinne.
Testing vestibular function
Examination sequence
With the patient seated, hold your finger an arm’s length away, level with the patient’s eyes.
Ask the patient to look at, and follow, the tip of your finger. Slowly move your finger up and down and then side to side. Be careful not to get the eyes too far deviated to the side as this generates a physiological nystagmus (Box 13.8).
Look at the patient’s eyes for any oscillations and note:
whether they are horizontal, vertical or rotatory
which direction of gaze causes the most marked nystagmus
in which direction the fast phase of jerk nystagmus occurs
whether jerk nystagmus changes direction when the direction of gaze changes
if nystagmus is more obvious in one eye than the other (ataxic or dysconjugate nystagmus).
Examination sequence
Ask the patient to sit upright, close to the edge of the couch. Warn the patient about what you are going to do.
Turn the patient’s head 45° to one side.
Rapidly lower him, so that the head is now 30° below the horizontal. Say: ‘Keep your eyes open even if you feel dizzy.’
Watch the eyes carefully for nystagmus. Repeat the test, turning the head to the other side (Fig. 13.10).
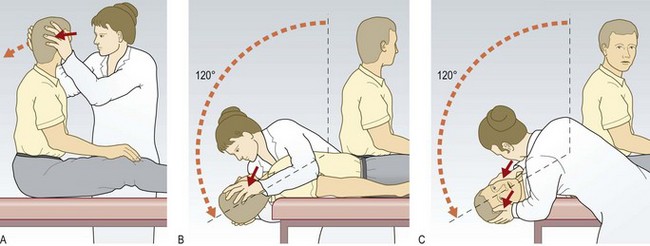
Normal patients have no nystagmus or sensation of vertigo.
Abnormal findings: In BPPV there is a delay of up to 20 seconds before the patient experiences vertigo and rotatory jerk nystagmus towards the lower ear occurs (geotropic). The response fatigues, so there is less, or no, response if you repeat the test immediately (adaptation).
Central pathology produces immediate nystagmus, not necessarily with vertigo, and no adaptation. Lack of dizziness plus relatively coarse nystagmus is central till proved otherwise.
The nose and sinuses
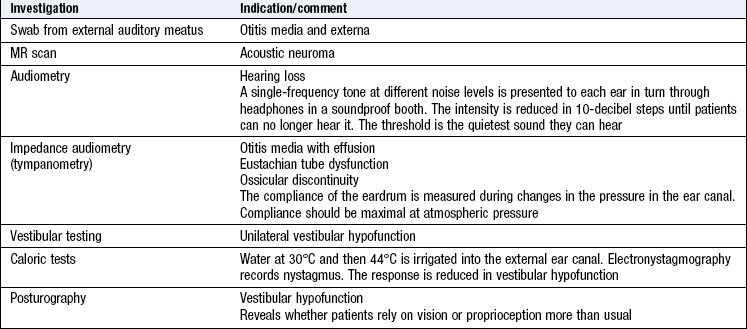
The nasal vault is formed from two nasal bones above, a middle pair of cartilages and two tip cartilages around the nostrils. The septum divides the nose into two nasal cavities. Posteriorly, the cavities open up, with three air baffles down each side. These are the turbinates which filter, warm and moisten the nasal airflow. The sensory olfactory epithelium is high up in the cavities (Fig. 13.11).
The paranasal sinuses – maxillary, frontal, ethmoid and sphenoid – are air-filled spaces in the skull bones. They connect through narrow openings (ostia) with the nasal cavity.
Symptoms and definitions
Persistent unilateral obstruction is often due to a deviated nasal septum, either congenital or secondary to trauma. Bilateral obstruction may be due to rhinitis, with or without sinusitis or polyps (Box 13.10).
13.10 Symptoms and definitions in nasal disease
| Symptom | Definition | Common cause |
| Nose blocked | Viral illness, deviated nasal septum, nasal polyp | |
| Rhinorrhoea | Discharge | Watery – allergic rhinitis, cerebrospinal fluid leak |
| Purulent – infection, foreign body | ||
| Epistaxis | Nose bleed | Trauma, infection |
| Sneezing | Allergy, infection | |
| Coughing | Postnasal drip | |
| Anosmia | Absence of smell | Head injury, viral neuropathy |
| Hyposmia | Reduced smell | Nasal polyps, nasal blockage |
| Cacosmia | Unpleasant smell | Chronic anaerobic sepsis |
| Nasal deformity | Trauma, rhinophyma | |
| Pain | Sinus infection, dental infection | |
| Septum perforation | Nose-picking, granulomatous disease, e.g. granulomatosis with polyangiitis, cocaine use, inhalation of industrial dusts, e.g. nickel, chromium |
Nasal discharge
Bilateral watery discharge suggests allergic or vasomotor rhinitis. Purulent discharge suggests bacterial infection, such as after the common cold, in localised sinus infection or when there is a foreign body in the nose. New onset, unilateral, crystal clear discharge following head injury suggests a cerebrospinal fluid leak.
Epistaxis
This is bleeding from inside the nose. There is a rich blood supply to an area of the anterior nasal septum (Little’s area) that is easily traumatised and is a common site for bleeding. Epistaxis may be life-threatening in the elderly, notably those with impaired coagulation from disease, medication or alcohol excess.
Sneezing
This protective sudden expulsive effort clears the nasal passages of irritants. It is common in viral upper respiratory infection and allergic rhinitis.
Disturbance of smell
Anosmia (complete loss of sense of smell) may follow head injury with damage to the olfactory epithelium/olfactory nerve or can occur after a viral upper respiratory tract infection. Mechanical obstruction of the nose by nasal polyps or severe mucosal oedema and swelling in allergic rhinitis usually causes hyposmia (reduced sense of smell). Cacosmia is an unpleasant smell due to chronic sepsis in the nose or sinuses. Parosmia is a distorted sense of smell. Brief olfactory hallucinations (phantosmia) may occur in temporal lobe epilepsy.
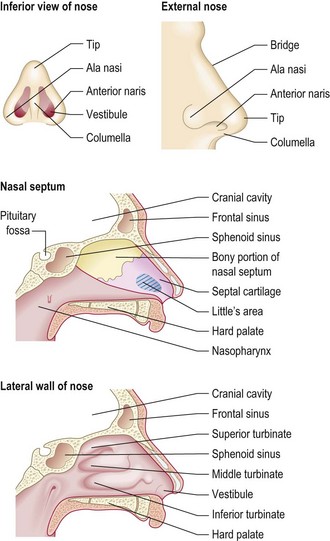
Nasal deformity
Swelling and bruising from trauma settle over 2 weeks but nasal deformity may remain if the nasal bones have been displaced. Skin affected by acne rosacea over years causes rhinophyma (Fig. 13.12). Destruction of the nasal septum produces flattening of the bridge and a ‘saddle’ deformity. Causes include granulomatosis with polyangiitis, trauma, congenital syphilis and chronic abuse of cocaine (a powerful vasoconstrictor which renders the mucosa ischaemic). Widening of the nose is a feature of acromegaly and advanced nasal polyposis.
Nasal and facial pain
Nasal pain is extremely rare, except following trauma. Facial pain is caused by temporomandibular joint dysfunction, migraine, dental disease, sinusitis or trigeminal neuralgia. Cluster headache characteristically causes unilateral nasal discharge and eye watering (Box 13.11).
13.11 Chronic rhinosinusitis
Chronic rhinosinustis is characterised by the triad of pain, obstruction and persistent purulent discharge. Nasal endoscopy may confirm the diagnosis.
Tahamiler R, Canakcioglu S, Ogreden S et al. The accuracy of symptom-based definition of chronic rhinosinusitis. Allergy 2007;62:1029–1032. Bhattacharyya N, Lee LN. Evaluating the diagnosis of chronic rhinosinusitis based on clinical guidelines and endoscopy. Otolaryngology – Head Neck Surg 2010;143:147–151.
The history
A past history of atopy may indicate rhinitis. One-third of patients with nasal polyps have asthma. Recurrent upper respiratory tract infections may cause sinusitis. Nasal bleeding is prolonged by hypertension and bleeding diathesis. Trauma to the face and nose may cause nasal blockage, deformity and anosmia.
Drug history
Anticoagulants and non-steroidal anti-inflammatory drugs may aggravate epistaxis. ‘Snorting’ cocaine can cause perforation of the nasal septum (Fig. 13.14B).
Social history
Ask allergic patients about their pets. Exposure to inhaled hardwood dust in certain occupations is associated with an increase of sinus cancer. Exposure to other occupational dusts or chemicals may exacerbate rhinitis. Alcohol use is important in epistaxis and rhinophyma. Smoking impedes nasal mucociliary clearance.
The physical examination
Examination sequence
Look at the external surface and appearance of the nose. Note any skin disease or deformity.
Stand behind the patient; look down the nose from above for any external deviation.
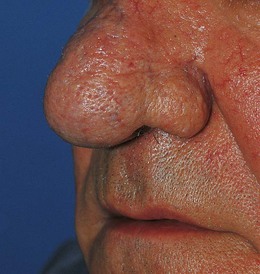
At rest, the nostrils face down towards the floor but the nasal cavity passes posteriorly along the upper surface of the hard palate. To look into the nose, ask your patient to hold her head in the normal position (discourage her from throwing her head back). Gently elevate the tip of her nose with the pad of your thumb to align the nostrils with the rest of the cavity.
Look in and assess the alignment and mucosal covering of the septum (Fig. 13.13).
Fig. 13.13 Nasal examination.
(A) Elevating the tip of the nose to give a clear view of the anterior nares. (B) Anterior rhinoscopy using an otoscope with a large speculum.
In an adult use a large-size speculum on your otoscope to see the inferior turbinates. Do not try to pass instruments into a child’s nose.
Feel the nasal bones gently to distinguish bony from cartilaginous deformity. In trauma, check the integrity of the infraorbital ridges and of the range of eye movements to exclude ‘orbital blowout’.
Place a metal spatula under the nostrils and look for the condensation marks to assess airway patency or lightly occlude each nostril and ask the patient to sniff.
Palpate for cervical lymphadenopathy (p. 53).
Tests of olfaction are usually confined to specialist clinics.
Abnormal findings: The nasal mucosa is pale, moist and hypertrophied in allergic rhinitis (Fig. 13.14A). In chronic rhinitis, it is swollen and red. A pale grey, moist swelling blocking the nostril may be a polyp (Fig. 13.14C). Facial swelling is unusual in sinusitis but occurs with a dental root abscess and cancer of the maxillary antrum.
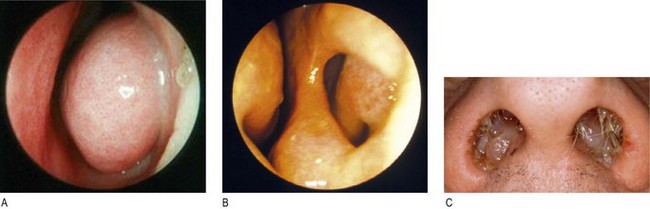
Fig. 13.14 Nasal abnormalities.
(A) Turbinate hypertrophy. (B) Nasal septum perforation postsurgery. (C) Nasal polyps.
In functional anosmia there is no response to a nasal irritant. Nasal irritation is mediated via the trigeminal and not the olfactory nerve.
Investigations
Tests of olfaction are usually only done in specialist clinics (Box 13.12).
 13.12 Investigations in nasal disease
13.12 Investigations in nasal disease
| Investigation | Indication/comment |
| Plain X-ray | Nasal bone fracture |
| Only required if you suspect associated facial fracture | |
| Lateral X-ray nasopharynx | Adenoidal hypertrophy |
| Young children | |
| Nasal endoscopy | Sinus disease |
| Computed tomography | Sinus disease, trauma and cancer |
| Radiation dose to the eyes is significant, so avoid repeat imaging |
The mouth and throat
The mouth
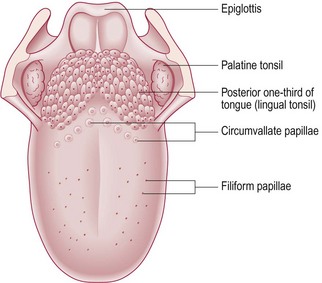
The mouth extends from the lips anteriorly to the anterior pillar of the tonsils posteriorly and has two compartments: the vestibule between the buccal (cheek) mucosa and the teeth and the oral cavity internal to the teeth. In the oral cavity are the anterior two-thirds of the tongue, the floor of the mouth, the hard palate and the inner surfaces of the gums and the teeth (Fig. 13.15). The lips form a seal for the oral cavity. The tongue’s normal colour varies from pink through to very dark brown. Its velvet texture is due to the filiform papillae containing taste buds (Fig. 13.16). Circumvallate papillae are groups of taste buds which mark the boundary of the anterior two-thirds and posterior third of the tongue.
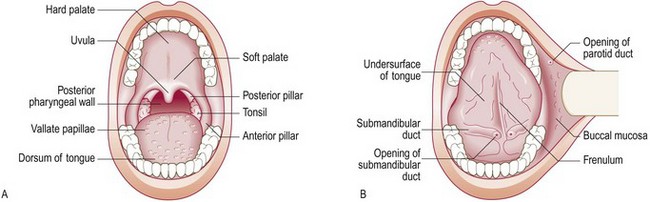
Fig. 13.15 Anatomy of the mouth and throat.
(A) Examination with the mouth open. (B) Examination with the tongue touching the roof of the mouth.
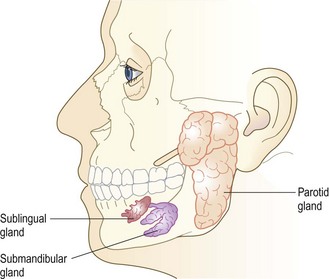
The parotid, submandibular and sublingual salivary glands secrete saliva (Fig. 13.17). The parotid gland sits in front of the ear, encasing the facial nerve. The part deep to the facial nerve is called the deep lobe (p. 254). The opening of its duct is in the buccal mucosa, opposite the second upper molar. The submandibular gland lies anterior and medial to the angle of the jaw; its duct opens into the floor of the mouth next to the frenulum of the tongue (Fig. 13.15).
The throat
The pharynx is a shared upper aerodigestive channel from the anterior faucial pillar to the laryngeal inlet. The larynx is a protective sphincter for the lower airway, known colloquially as the ‘voice box’ due to the importance of human phonation. It has two external cartilages, the thyroid cartilage (Adam’s apple) and the cricoid cartilage, the prominence at the top of the trachea. Its sensory supply is via the superior and recurrent laryngeal branches of cranial nerve X (vagus) (p. 257). Its motor supply is mainly from the recurrent laryngeal nerve, which loops up round the aortic arch on the left and the subclavian artery on the right.
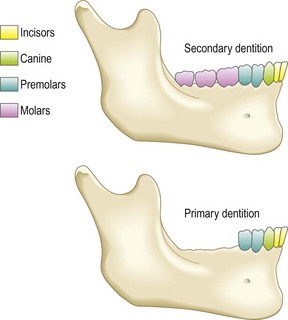
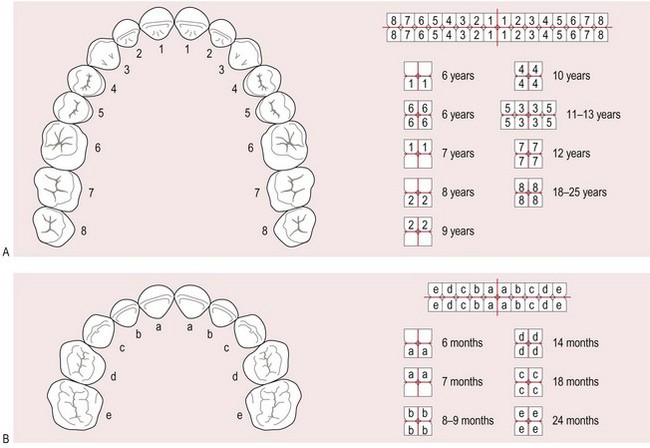
The teeth
In children the 20 deciduous teeth erupt by 3 years. There are 32 secondary teeth, erupting from ages 6 to 16 or later (Figs 13.18–13.20).

Symptoms and definitions
See Box 13.13.
13.13 Symptoms and definitions in mouth and throat disease
| Symptom | Definition | Common cause |
| Pain | Dental caries, periodontal infection | |
| Odynophagia | Pain on swallowing | Infection, cancer of oesophagus, larynx or pharynx |
| Stridor | Noise from upper airway on breathing | Upper-airways obstruction, e.g. laryngeal cancer |
| Dysphonia | Change in the quality of the voice | Cysts, polyps, cancer, laryngitis |
| Dysphagia | Difficulty swallowing | Pharyngitis Oesophageal disease |
| Lumps | Lymphadenopathy | |
| Halitosis | Bad breath | Poor dental hygiene |
| Trismus | Inability to open mouth fully | Quinsy, tetanus |
| Xerostomia | Dry mouth | Anticholinergic drugs, Sjögren’s syndrome |
Pain
Sore mouth: Gingivitis (inflammation of the gums) may cause a narrow red line at the border of the gums (Box 13.14).
13.14 The gums in systemic conditions
| Condition | Description |
| Phenytoin treatment | Firm and hypertrophied |
| Scurvy | Soft and haemorrhagic |
| Acute leukaemia | Hypertrophied and haemorrhagic |
| Cyanotic congenital heart disease | Spongy and haemorrhagic |
| Chronic lead poisoning | Punctate blue line |
Aphthous ulcers are small painful superficial ulcers on the tongue, palate or buccal mucosa. They are common, of unknown cause and heal spontaneously within a few days. The causes of oral ulcers are trauma, vitamin or mineral deficiency (anaemia), cancer or lichen planus. Unilateral painful vesicles on the palate can be caused by herpes zoster (Fig. 11.8B).
Diffuse oral infection with Candida albicans (candidiasis or ‘thrush’) may be secondary to poorly fitting dentures, the use of inhaled steroids or immunodeficiency, e.g. HIV infection or leukaemia (Box 8.4).
Sore throat: Throat pain often radiates to the ear because of the dual innervation of the pharynx and external auditory meatus via the vagus nerve.
Many viruses cause pharyngitis (acute inflammation of the pharynx). Acute tonsillitis may be viral or caused by Streptococcus pyogenes (Fig. 13.21A). There may be a pustular exudate on the tonsils and associated systemic features of fever, malaise, anorexia and cervical lymphadenopathy. You cannot distinguish viral from bacterial tonsillitis clinically.
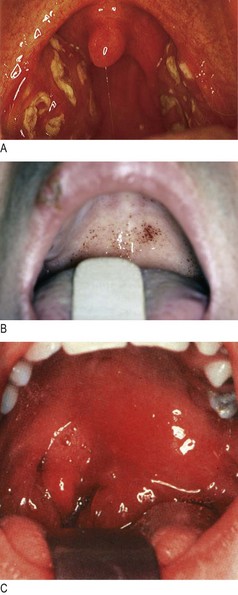
Fig. 13.21 Sore throat.
(A) Acute tonsillitis – the presence of pus strongly suggests a bacterial (Streptococcal) aetiology. (B) Glandular fever showing palatal petechiae. (C) A left peritonsillar abscess.
In infectious mononucleosis (glandular fever), palatal petechiae can be seen and the tonsil may be covered in a white pseudomembrane (Fig. 13.21B). Diphtheria causes a true, grey membrane over the tonsil but is rarely seen because of immunisation.
A peritonsillar abscess (quinsy) causes extreme pain aggravated by swallowing. The patient dribbles saliva out of his mouth, there is trismus (spasm of the jaw muscles) and the uvula is displaced to the opposite side (Fig. 13.21C).
Any persistent mass or ulcer on the tonsil associated with pain may be a squamous cancer.
Globus pharyngeus is the feeling of a lump in the throat with normal examination. It generally fluctuates from day to day. Contributory factors are believed to include anxiety, habitual throat clearing or acid reflux. Rarely, globus is progressive and occurs with ‘red flag’ symptoms as part of the presentation of underlying malignancy (Box 13.15) (Fig. 8.26).
Human papillomavirus-related oropharyngeal cancer is the commonest site of primary head and neck cancer in young, sexually active non smokers.
Stridor: Stridor is a high-pitched, often harsh noise produced by airflow turbulence through partial obstruction of the upper airway. It occurs most commonly on inspiration but also on expiration or biphasically. Inspiratory stridor indicates narrowing at the vocal cords; biphasic stridor suggests tracheal obstruction, while stridor on expiration suggests tracheobronchial obstruction. Narrowing of smaller, peripheral airways produces wheeze heard on expiration (Fig. 13.22). Always investigate stridor. Common causes include infection/inflammation, e.g. acute epiglottitis in children and young adults and tumours of the trachea and main bronchi or extrinsic compression by lymph nodes in older adults. Rarer causes include anaphylaxis and foreign body.
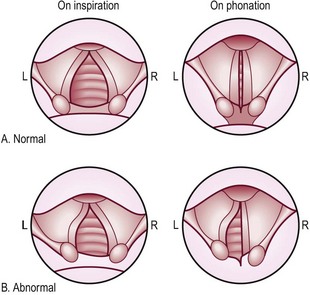
Fig. 13.22 Laryngoscopic views of the vocal cords.
(A) Normal movements. (B) Movements in the presence of recurrent laryngeal nerve paralysis, most commonly caused by lung cancer. Note that the paralysed left cord is in the cadaveric position (between inspiration and expiration).
Stertor, or muffled ‘hot potato’ speech, occurs with naso- or oropharyngeal obstruction, e.g. peritonsillar abscess (quinsy).
Dysphonia: Any disturbance of vocal cord function may cause dysphonia (Box 13.16). More than 3 weeks’ continuous dysphonia requires laryngoscopy to exclude cancer. Breathy dysphonia and a weak (bovine) cough are presenting features of lung or oesophageal cancer causing recurrent laryngeal nerve palsy (Fig. 13.22 and p. 141).
Sialadenopathy: Sudden, painful unilateral salivary gland swelling is due to a stone obstructing the duct. Other causes of enlarged salivary glands are mumps, sarcoidosis, HIV-related cysts, bacterial infection (suppurative parotitis; Fig. 13.23) and cancer.

The history
Timing of symptoms: Epiglottitis usually presents with stridor, rapidly progressive airway obstruction occurring within a few hours, sore throat, fever and drooling. It may be caused by bacterial infection, e.g. Haemophilus influenzae, Streptococcus pneumoniae and group A streptococci. With the introduction of the HIB vaccine it is now relatively more common in adults than small children. Other causes are thermal injury (burns, crack cocaine smoking), radiotherapy, and caustic or foreign-body ingestion.
Acute laryngotracheobronchitis (croup) in infants usually has a longer history (24–48 hours) and the airway obstruction is less severe.
Past history
Ask about dental problems and systemic disease, particularly affecting the gastrointestinal tract as the mouth is part of this. Neurological conditions may affect the ability to masticate and swallow, and drooling or dry mouth with superimposed infection may result. Note any facial trauma or surgery.
The physical examination
Examination sequence
Listen to the patient’s voice (Box 13.17).
 13.17 Voice changes with pathology
13.17 Voice changes with pathology
| Rough | Vocal cord pathology |
| Breathy | Recurrent laryngeal nerve palsy |
| Wet, hoarse or dysarthric | Neurological disease |
| Muffled | Oropharyngeal mass |
| Nasal escape | Soft palate dysfunction |
Have a good light source. Use a head mirror or head light to leave both your hands free to manipulate instruments.
Do not try to examine the throat in a patient with stridor, as this may induce laryngospasm and total airway obstruction.
Ask the patient to remove any dentures. Look at his lips, then ask him to half-open his mouth. Inspect the mucosa of the vestibule, buccal surfaces and buccogingival sulci for discoloration, inflammation, ulceration or nodules, then at the bite closure.
Ask him to open his mouth fully and touch behind the upper incisors with the tip of his tongue. Check the mucosa of the floor of mouth and the orifices of the submandibular glands.
Ask him to stick out his tongue. Look for deviation (XIIth nerve dysfunction), mucosal change or fasciculation.
Now ask him to deviate his tongue to one side. Retract the opposite buccal mucosa with a tongue depressor to view the lateral tongue border clearly. Repeat on the other side.
Look at the hard palate. Note any cleft, abnormal arched palate or telangiectasia.
Look at the oropharynx. Ask him to say ‘Aaah’. Use a tongue depressor if needed.
Look at the soft palate for any cleft or structural abnormality. Note any telangiectasia.
Look at the tonsils. Note their symmetry, size, colour, any discharge or membrane.
Use the tongue depressor to scrape off any white plaques gently.
Touch the posterior pharyngeal wall gently with the tongue depressor to stimulate the gag reflex. Check for symmetrical movement of the soft palate.
If there is any lesion in the mouth or salivary glands, put on a pair of gloves and palpate it with one hand outside on the patient’s cheek or jaw and the gloved finger of your other hand inside his mouth.
Feel the lesion and identify its characteristics (SPACESPIT: Box 3.11; p. 53).
If the parotid gland is abnormal or enlarged, examine the facial nerve and check if the deep lobe (tonsil area) is displaced medially.
Palpate the length of the duct, and include the submandibular gland.
Palpate the cervical lymph nodes systematically (Fig. 3.22).
Abnormal findings: Cold exposure causes desquamation and cracking of the lips (‘chapped lips’); riboflavin deficiency causes red cracking of the lips. Inflamed painful cracking of the skin at the corners of the mouth may be due to excess saliva, chronic atrophic candidiasis or iron deficiency (Fig. 13.24). Squamous and basal cell cancers occur on the lips and are associated with smoking and sun exposure.

Neurological disease, painful mouth and a tight frenulum may all limit tongue protrusion. Normal tongue appearance includes areas of smooth mucosa (geographic tongue) or, conversely, of excessive furring. A smooth red tongue with diffuse papillary atrophy occurs in iron or vitamin B12 deficiency.
Macroglossia (enlarged tongue) occurs in Down’s syndrome, acromegaly (Fig. 3.19A), hypothyroidism and amyloidosis. Wasting and fasciculation of the tongue are features of motor neurone disease.
Abnormal buccal pigmentation is found in Addison’s disease (Fig. 5.19B), haemochromatosis or the Peutz–Jeghers syndrome (with polyposis of the small intestine) or chewing betel nut (a mild stimulant chewed in Asia which is a carcinogen).
White plaques of candidiasis on the tongue or mucosa (Fig. 13.25A) come away easily when scraped but leukoplakia (a keratotic precancerous condition) does not and requires excision biopsy (Fig. 13.25B). Cancers (usually squamous) may occur at any site in the mouth; assume any painless persistent mass is oral cancer and refer urgently for biopsy. Tonsil lesions may be lymphoma.
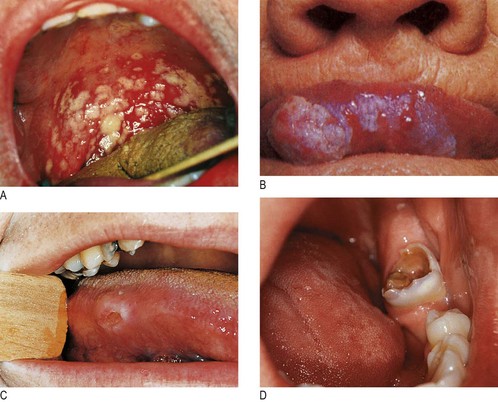
Fig. 13.25 Disorders of the tongue and teeth.
(A) Oral thrush. (B) Leukoplakia. (C) Aphthous stomatitis causing a deep ulcer in a patient with inflammatory bowel disease. (D) Dental caries.
Oral mucous retention cysts are bluish domes a few millimetres in diameter.
Aphthous ulcers (Fig. 13.25C) are small and painful, occur in crops and usually heal within a few days. Ulcers may be the presentation of Crohn’s or other inflammatory bowel diseases. Any mouth ulcers persisting for >3 weeks require biopsy to exclude oral cancer.
A stone may be felt in the submandibular (or, rarely, the parotid) duct.
Rotten teeth (dental caries) are common in patients with poor oral hygiene (Fig. 13.25D).
The neck
Examine the neck in all patients with mouth or throat symptoms. A neck mass or rash may be the main presenting complaint (Fig. 13.26 and Box 13.18).
Examination sequence
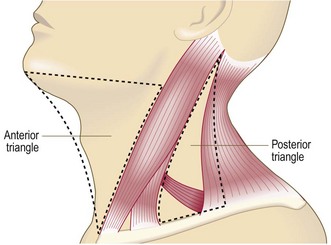
13.18 Causes of neck lumps
In the anterior triangle (bounded by the midline, the anterior border of sternocleidomastoid muscle and body of mandible):
• Submandibular gland swelling
• Malignant: lymphoma, metastatic cancer
• Infection: any bacterial infection of head/neck (including teeth), viral infection, e.g. infectious mononucleosis, HIV, tuberculosis
• Parotid gland swelling, e.g. mumps, parotitis, stones, autoimmune disease, benign and malignant tumours
In the posterior triangle (bounded by the posterior border of sternocleidomastoid muscle, the trapezius and the clavicle):
With the patient sitting down, look at his neck from in front to identify any scar or visible mass or pulsation.
From behind, palpate the neck. Work systematically around the neck, checking each of the three boundaries of the anterior and posterior triangles. Feel for midline, submental, submandibular and preauricular swellings.
Assess the consistency, mobility and size of any swellings. Is it fluctuant (cystic) or pulsatile? Listen for bruits (p. 53).
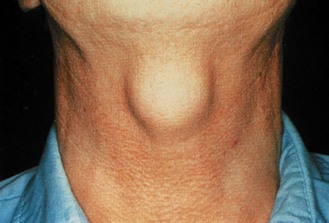
With a midline swelling, ask the patient to swallow (offer a glass of water if needed) and note if the swelling moves. A thyroid swelling will move superiorly on swallowing. If so, percuss for retrosternal dullness and check for dysthyroid features (p. 80).
Ask the patient to put out his tongue and note any movement. A thyroglossal cyst will move superiorly (Fig. 13.27).