Drug Abuse
1 Define addiction, dependence, tolerance, and withdrawal in relation to drug abuse.
2 Name several types of central nervous system depressants that are commonly abused and outline the typical pattern of abuse, treatment, adverse reactions, management of overdose and withdrawal, and dental treatment implications of each.
3 Identify several types of central nervous system stimulants that are commonly abused.
4 Describe the pattern of abuse and treatment options associated with tobacco use, and summarize the role of the dental health care worker in tobacco cessation.
5 Discuss ways in which the dental health care worker can identify patients or colleagues who may be abusing drugs.
Dental health care workers may become involved with drug abuse in a variety of ways. Drugs that can be abused include both legal and illegal drugs. Patients seen in the dental office may be abusing drugs. Another interaction with the abusing patient involves the “potential” patient. Potential patients call the dental office, complain of pain, and request a prescription. Employees working in the dental office, including the dentist, dental hygienist, dental assistant, receptionist, bookkeeper, or other employees, may abuse drugs. Friends and relatives, as well as their friends and relatives, may abuse drugs. In our society, drug abuse, especially in adolescents, is epidemic. Wherever there are people, drug abuse can occur. Therefore the dental health care worker should become familiar with the various types of drugs commonly abused and their patterns of abuse. It is important to be able to recognize the problem in others. Because drug abuse is also a community issue, the dental health care worker should have a heightened awareness of the potential for patients to present with abuse problems (a high index of suspicion but not unrealistically high). The proper awareness is only learned with experience.
Alcohol and tobacco abuse causes more medical problems than all the other drugs of abuse combined. If no one in the United States used tobacco or drank alcohol, half of the filled hospital beds would be empty.
The idea of using drugs to produce profound effects on mood, thought, and feeling is as old as civilization. Only the kinds of substances used for this purpose have changed. Abuse has assumed a much bigger role in society because the forms of drugs used today are much stronger and have a much faster onset of action. This quick reinforcement produces abuse more quickly. For example, natives in Colombia have chewed coca leaves for many years as part of their culture, with little inappropriate use. Purifying cocaine and making it into a powder form to be “snorted” increased its abuse. When cocaine was “free based,” it became easier to abuse, but the chemical reaction was dangerous. The most recent adaptation of cocaine, making it into “rocks,” has increased abuse of the drug even more by making it available to smoke in convenient, small, reasonably priced doses. As is common with drugs of abuse, the potential for abuse is greatly increased when a drug is very potent, has a quick onset of action, is inexpensive, and is easy to distribute, making it the perfect drug of abuse.
Agents used for their psychoactive properties (capable of changing behavior or inducing psychosis-like reactions or both) can be divided into those that also have therapeutic value (opioids and sedative-hypnotics) and those that have no proven therapeutic value (psychedelics). Some agents may move from one category to the other. For example, marijuana, an agent previously considered to be worthless, is now claimed to be useful in the treatment of the nausea associated with cancer chemotherapy and for glaucoma. However, more controlled studies are needed to determine whether this claim is true.
GENERAL CONSIDERATIONS
Abuse of a drug is defined as the use of a drug for nonmedical purposes, almost always for altering consciousness. Both legitimate and illegitimate drugs may be abused. Whether a drug has an abuse potential is determined by the drug’s pharmacologic effect. In contrast, the misuse of a drug means using the drug in the wrong dose or for a longer period than prescribed. The difference between these two uses is subtle.
Definitions
Terms relating to abuse that are used in this chapter are defined as follows:
• Abstinence syndrome: A state of being free of drugs that is the goal of any treatment program.
• Addiction: This vague term, although still used, should be replaced with dependence. Addiction is the pattern of abuse that includes compulsive use despite complications (medical or social) and frequent relapses after “quitting.”
• Dependence: A combination of either physical or psychological manifestations (withdrawal) occurring in a drug-dependent person when the drug is removed.
• Drug abuse: Self-administration of a drug in a socially unacceptable manner, resulting in negative consequences. A component of abuse is that harm is being produced from using the drug.
• Drug dependence: A state, which may be physical, psychological, or both, that occurs as a consequence of the interaction between a drug and a patient. It is characterized by a compulsion to take the drug to obtain its effects or to prevent the abstinence syndrome. Tolerance may occur.
• Enabling: The behavior of family or friends that associate with the addict that results in continued drug abuse. This inappropriate coping mechanism requires family therapy.
• Habituation: Physiologic tolerance to or psychological dependence on a drug, short of addiction.
• Misuse: Use of the drug for a disease state in a way considered inappropriate.
• Physical/physiologic dependence: The state in which the drug is necessary for continued functioning of certain body processes. In a dependent person, discontinuing the drug produces the abstinence syndrome, sometimes called withdrawal (physiologic reactions).
• Psychological dependence: The state in which, following withdrawal of the drug, there are manifestations of emotional abnormalities and drug-seeking behavior. Craving is present, but there is no physiologic dependence.
• Tolerance: With repeated dosing, the dose of a drug must be increased to produce the same effect. Or, the same dose of a drug, with consecutive dosing, produces less effect.
• Withdrawal: The constellation of symptoms that occurs when a physically dependent person stops taking the drug.
Psychological Dependence
Psychological dependence is a state of mind in which a person believes that he or she is unable to maintain optimal performance without having taken a drug. Psychological dependence can vary in severity from mild desire (e.g., for a morning cup of coffee) to compulsive obsession (e.g., for the next dose of cocaine). Although some highly abused drugs have only psychological dependence, the “need” to use these drugs can be as strong as or stronger than drugs with a physical dependence. Other examples include benzodiazepines, opioids, and amphetamines.
Physical Dependence
Physical dependence refers to the altered physiologic state that results from constantly increasing drug concentrations. The presence of physical dependence is established by the withdrawal or abstinence syndrome, a combination of many drug-specific symptoms that occur on abrupt discontinuation of drug administration. Withdrawal symptoms are often the opposite of the symptoms of use of the drug, for example, excessive parasympathetic action (e.g., diarrhea, lacrimation, and piloerection [“goose flesh”]) when withdrawing from the opioids.
Tolerance
Tolerance is characterized by the need to increase the dose continually to achieve the desired effect or the giving of the same dose, which produces a diminishing effect. The type of tolerance referred to in this discussion of abuse of psychoactive drugs is central (functional or behavioral) tolerance, that is, a definite decrease in the response of brain tissue to constantly increasing amounts of a drug. (One can think of the brain becoming “stronger” [less responsive] to “withstand” the large doses it must tolerate.) In terminal patients, this tolerance requires ever-increasing doses of opioids even if the pain remains constant. The doses reached over time with the terminally ill would be fatal to a patient without tolerance.
Tolerance of metabolic origin (dispositional or metabolic tolerance) is caused by an accelerated rate of metabolism of the drug and is excluded in this discussion. Metabolic tolerance is an insignificant factor in the tolerance observed in humans to most of the psychoactive drugs.
Addiction, Habituation, and Dependence
Addiction and habituation are terms that have been misused almost as much as the drugs they attempt to characterize. Any use of these terms must be preceded by an adequate definition. In both addiction and habituation, the desire to continue using the drug is present, but in addiction, dependence is also present. Habituation and addiction are really only degrees of misuse or abuse of drugs. It has been recommended that these terms be replaced by the term dependence, a state of psychological or physical desire to use a drug.
Drugs that produce tolerance and physical dependence are grouped according to their ability to be substituted for one another. For example, if a person is addicted to heroin, an opioid, then other opioids, such as morphine, can prevent withdrawal. However, a barbiturate cannot be substituted for an opioid and vice versa. Therefore the opioids and barbiturates are separate groups of dependence-producing drugs. The phenomenon of substitution to suppress withdrawal between different drugs is called cross-tolerance or cross-dependence. It is observed among members of the same drug group but not among different drug groups. Cross-tolerance may be either partial or complete and is determined more by the pharmacologic effect of the drug than by its chemical structure.
Most characteristics of drug abuse are determined by the individual drug involved, but the following generalizations can be made:
• When comparing drugs in the same group, the time required to produce physical dependence is shortest with a rapidly metabolized drug and longest with a slowly metabolized drug.
• The time course of withdrawal reactions is related to the half-life of the drug. The shorter the half-life, the quicker the withdrawal is.
Approximately 80% of incarcerated (jailed) individuals are there because of drug abuse problems.
Many drugs have been abused extensively, and whether abuse can occur is a function of a particular drug’s effects on neurotransmitters (combined with some genetic component within the user). At various times, sniffing airplane glue, inhaling propellant, smoking banana peels, smoking peyote (contains mescaline), and ingesting morning glory seeds have been attempted. The problems and treatment of drug abuse are less related to the drugs themselves, although they can cause definite problems, than to the “inner person” of the patient involved in this type of behavior and his or her genetic predisposition. To treat abuse, a multifactorial approach is needed: counseling, education, self-help groups, and an intense desire to stop.
Propellant that is included in paint cans is preferred. The procedure is called “huffing” because the contents are sprayed into a plastic bag and fumes are repeatedly inhaled. Abuse of paint can easily produce irreversible damage to the liver and brain.
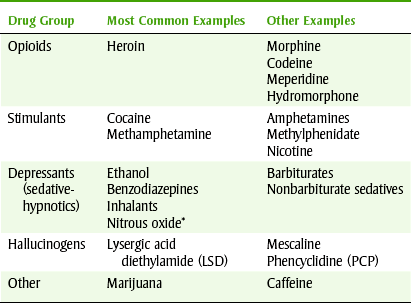
This chapter discusses the properties of the specific groups of agents abused and the differences among the groups. The abusable drugs are divided into the following groups: central nervous system (CNS) depressants (“downers”), CNS stimulants (“uppers”), and hallucinogens. Some drugs, depending on the dose, may fall in more than one group. For example, marijuana may be classified as either a CNS depressant or a hallucinogen. Table 25-1 lists the common drugs of abuse by categories.
CENTRAL NERVOUS SYSTEM DEPRESSANTS
CNS depressants include alcohol, opioids, barbiturates, benzodiazepines, volatile solvents (glue and gasoline), and nitrous oxide (abused mainly in dentistry).
Ethyl Alcohol
Ethyl alcohol, or ethanol (ETH-an-ol), is a sedative agent used socially. Because it is legal, its availability makes it the most often abused drug. Abuse of alcohol, called alcoholism, is the number one public health problem in the United States and is associated with many major medical problems. The incidence of alcoholism in the United States is about 10% (i.e., 1 in 10). Many “accidental” deaths are associated with the use of alcohol. Two-fifths of traffic fatalities involve alcohol. More than 50% of gunshot wounds in teenagers are preceded by abuse of alcohol. The best use of resources for addiction would be to deal with alcoholism as soon as it can be identified.
 PHARMACOKINETICS
PHARMACOKINETICS
Ethyl alcohol is rapidly and completely absorbed from the gastrointestinal tract. Peak levels while fasting occur in less than 40 minutes. Food delays absorption and reduces the peak levels. Alcohol is oxidized in the liver to acetaldehyde, which is then metabolized to carbon dioxide (CO2) and water (H2O) (Figure 25-1).

Its metabolism follows zero-order kinetics, so a constant amount of alcohol is metabolized per unit of time regardless of the amount ingested. Because of its zero-order kinetics, excessive intake of alcohol can produce a prolonged effect. It is also excreted from the lungs (alcohol breath) and in urine.
ACUTE INTOXICATION
With mild intoxication, impairment of judgment, emotional lability, and nystagmus occur. When intoxication is moderate, dilated pupils, slurred speech, ataxia, and a staggering gait are noted. If intoxication is severe, seizures, coma, and death can occur. Treatment includes fluids and electrolytes, thiamine (B6), sodium bicarbonate, and magnesium.
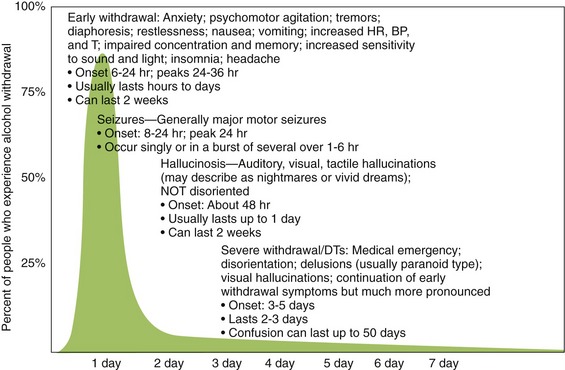
WITHDRAWAL
Withdrawal from alcohol use occurs after the use of alcohol. The more alcohol consumed and the more time spent consuming, the more violent the withdrawal syndrome is (Figure 25-2). Stage 1 usually begins 6 to 8 hours after drinking has stopped and includes withdrawal, psychomotor agitation, and autonomic nervous system hyperactivity. Stage 2 withdrawal includes hallucinations, paranoid behavior, and amnesia. Stage 3 includes disorientation, delusions, and grand mal seizures. It takes 3 to 5 days after cessation of drinking alcohol for stage 3 to occur. A cross-tolerant benzodiazepine (e.g., chlordiazepoxide; see Chapter 11) may be used to prevent withdrawal symptoms. Withdrawal from alcohol is termed delirium tremens (DTs) because the patient will often experience shaky (tremor) movements. Alcohol withdrawal can be life threatening if not properly treated.
CHRONIC EFFECTS
The chronic medical effects of alcoholism can include deficiency of proteins, minerals, and water-soluble vitamins. Impotence, gastritis, esophageal varices, arrhythmias, and hypertension have been reported. If a pregnant woman is using ethanol chronically, fetal alcohol syndrome can occur (see Figure 24-4). The infant is retarded in body growth and has a small head (microencephaly), poor coordination, underdevelopment of the midface, and joint anomalies. More severe cases include cardiac abnormalities and mental retardation. Chronic alcohol use increases the risk of cancer of the mouth, pharynx, larynx, esophagus, and liver, which may occur with tobacco use to make the risk higher than with alcohol alone. The liver can be affected with alcoholic hepatitis and amnesic syndrome (Wernicke-Korsakoff syndrome), and peripheral neuropathy can occur.
ALCOHOLISM
Alcoholism is a disease in which the alcoholic continues to drink despite the knowledge that drinking is producing a variety of problems (Box 25-1). There is a genetic link for alcoholism; children of alcoholics are at a much greater risk for becoming alcoholics. In the future, genetic testing may be able to identify at-risk children and target that population for intense educational and social intervention for prevention.
“Red flags” for alcohol abuse include drinking at an inappropriately early time, shaking when not drinking, blackouts when drinking, and being told that you drink too much. Missing work and problems in personal relationships are also strong warning signs.
TREATMENT
Alcoholics Anonymous: Alcoholics Anonymous, the most successful group for treating alcoholism, is a self-help organization made up of recovering alcoholics. The members (who are recovering alcoholics) give support to alcoholics who are attempting recovery. In most alcoholics, inpatient detoxification is usually not required. In fact, inpatient treatment does not give the alcoholic any experience in recovery in the “real world.” Outpatient psychiatric treatment can help provide some insight for alcoholics.
Drug Treatment: Alcoholics who are motivated and socially stable can be given disulfiram (dye-SUL-fi-ram) (Antabuse). Occasionally, employers will insist on the ingestion of disulfiram as a condition of employment.
Because disulfiram inhibits the metabolism of aldehyde dehydrogenase, a buildup of acetaldehyde occurs. Acetaldehyde produces significant side effects if alcohol is ingested. These include vasodilation, flushing, tachycardia, dyspnea, throbbing headache, vomiting, and thirst. The reaction may last from 30 minutes to several hours. Certain drugs that produce the disulfiram-like reaction (e.g., metronidazole) may cause a minor version of these symptoms with alcohol intake.
Naltrexone (ReVia), an oral opioid antagonist, is an old drug with a new use. Originally, it was indicated to prevent relapse in the opioid-dependent patient. Its new use is to reduce alcohol craving. Because naltrexone is partially effective in decreasing craving from alcohol, the logical conclusion is that alcohol stimulates some of the opioid receptors (among other receptors). More detailed knowledge of the receptors affected by alcohol may increase the chance of developing other agents to manage this disease. Other agents that might be useful are related to other neurotransmitters such as dopamine or serotonin.
DENTAL TREATMENT OF THE ALCOHOLIC PATIENT
The dental health care worker must have an index of suspicion for alcoholism in patients treated in the dental office. The great majority of alcoholics look exactly like our neighbors, not like those characterized in old movies (e.g., unshaven, shaky). All health care workers have been given the charge to identify and assist patients in obtaining treatment.
The dental treatment of the alcoholic patient includes some modifications, depending on the severity of the disease process. Most alcoholic patients have poor oral hygiene. Check for the sweet musty breath and painless bilateral hypertrophy of parotid glands characteristic of alcoholism. Cirrhosis of the liver can occur when alcoholics continue to abuse alcohol (Figure 25-3). The major problem in these patients is a failure of the liver to perform adequately. Because of hepatic failure, the liver is able to store less vitamin K and the conversion of vitamin K to the coagulation factors is reduced. The outcome of these effects is a deficiency in coagulation factors II, VII, IX, and X (vitamin K–dependent factors) with resulting bleeding tendencies. The patient’s international normalized ratio (INR) can be elevated to 6 or more without the presence of other concomitant medications. Thrombocytopenia secondary to portal hypertension and bone marrow depression magnifies the hemostatic deficiency, sometimes resulting in spontaneous gingival bleeding. With the presence of esophageal varices, spontaneous bleeding can occur. Later in liver failure, the abdomen becomes distended with fluid (the patient appears 9 months pregnant).
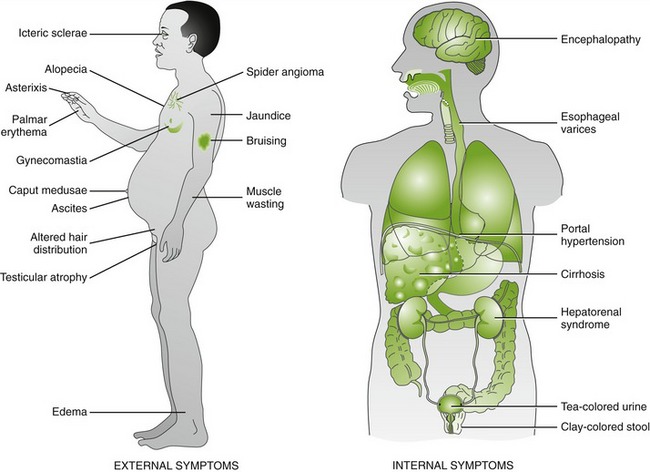
FIGURE 25-3 Clinical manifestations of cirrhosis. (From Mahan LK, Escott-Stump S: Krause’s food, nutrition, & diet therapy, ed 12, St Louis, 2008, Saunders.)
Oral complications of alcoholism include glossitis, loss of tongue papillae, angular/labial cheilosis, and Candida infection. Healing after surgery may be slow, and bleeding may be difficult to stop.
Because alcohol and tobacco use and abuse predispose a patient to oral squamous cell carcinoma, the dental health care worker should check any oral lesions carefully. Special attention should be paid to leukoplakia and ulceration (especially on the lateral border of the tongue or the floor of the mouth).
With reduced liver function, the liver has difficulty metabolizing drugs usually metabolized in the liver. The levels of drugs metabolized by the liver, such as amide local anesthetics and oxidized benzodiazepines, will not fall as rapidly as in normal patients. Dose reductions are necessary because of diminished liver function. The signs of potential advanced alcoholic liver disease are listed in Box 25-2.
The dental health care worker should have an index of suspicion so that alcoholics can be identified. The dental worker should smell the patient’s breath, palpate the parotid glands, expect poor oral hygiene, and evaluate the patient’s bleeding tendency. Those with cirrhosis and severe hepatic disease will have greatly prolonged prothrombin times and may require vitamin K a few days before a surgical procedure in which bleeding is expected. Table 25-2 lists the dental management of the alcoholic patient.
TABLE 25-2
DENTAL MANAGEMENT OF THE ALCOHOLIC PATIENT
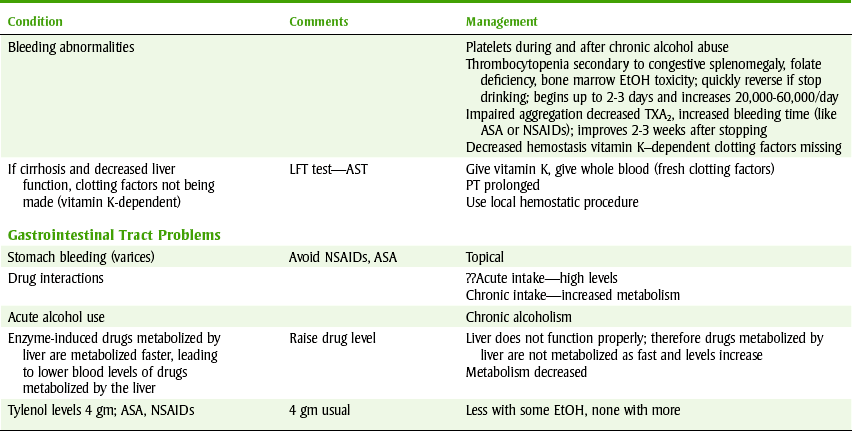
EtOH, Alcohol; TXA2, thromboxane A; ASA, aspirin; NSAIDs, nonsteroidal antiinflammatory drugs; LFT, liver function test; AST, aspartate aminotransferase; PT, prothrombin time.
Data from Glick M: Medical considerations for dental care of patients with alcohol-related liver disease, J Am Dent Assoc 128:61-72, 1997; and Mandel L, Hamele-Bena D: Alcoholic parotid sialadenosis, J Am Dent Assoc 128(10):1411-1415, 1997.
Nitrous Oxide
Nitrous oxide (N2O) is an incomplete general anesthetic readily available in many dental offices (see Chapter 10). It is abused primarily by dentists, dental hygienists, and dental assistants. Food service employees sometimes become N2O abusers because it is available in the aerosol in canned whipping cream products. Misuse often begins as “therapeutic” use only, progressing to abusive or “recreational” use at a later stage.
ABUSE PATTERN
N2O is available in the dental office in tanks and as a propellant for whipping cream (Figure 25-4). The availability of this gas to dental office personnel probably accounts for its unique abuse pattern.

FIGURE 25-4 Whippet assembly for recreational misuse of nitrous oxide (N2O). (From Clark M, Brunick A: Handbook of nitrous oxide and oxygen sedation, ed 3, St Louis, 2008, Mosby.)
Abuse of N2O can result in psychological but not physical dependence. Inhalation of 50% to 75% produces a “high” for 30 seconds followed by a sense of euphoria and detachment for 2 to 3 minutes. Tingling or warmth around the face, auditory illusions, slurred speech, and a stumbling gait can occur. The typical chemically dependent dentist (with N2O as the drug of choice) is a 40-year-old white man who has often abused illicit drugs and primarily uses alone.
ADVERSE REACTIONS
General: Adverse reactions include dizziness, headache, tachycardia, syncope, and hypotension. N2O impairs the ability to drive or operate heavy machinery. Other effects of N2O use include hallucinations and religious experiences. Equilibrium, balance, and gait are affected. With chronic use, it can produce chronic mental dysfunction and infertility.
If 100% N2O is inhaled, nausea, cyanosis, and falling may occur. Without oxygen, pure N2O can produce hypoxia that results in death. Dentists who have self-administered N2O have been found dead in their dental chairs with the mask still attached to the face.
Chronic use or abuse can lead to myelopathy (sensory and motor) resulting in a combination of symptoms pathognomonic for N2O abuse. Initial symptoms include loss of finger dexterity and numbness or paresthesia of the extremities. Position and vibration sensory neurons are lost. Other sensations, such as to pain, light touch, and temperature, may be lost. Later, Lhermitte’s sign, clumsiness, and weakness can be demonstrated. Neurologic deficiencies include extensor plantar reflex and polyneuropathy (slow conduction velocity in nerves). The neurologic deficiency is similar to that of spinal cord degeneration in pernicious anemia. The neurologic problems from vitamin B12 deficiency are improved by parenteral vitamin B12. Whether B12 improves N2O myelopathy is controversial. If the abuse of N2O is discontinued soon enough, clinical improvement can occur. However, with an increase in abuse the myelopathy is often irreversible.
Opioid Analgesics
Heroin, methadone (Dolophine), morphine, hydromorphone (Dilaudid), meperidine (Demerol), oxycodone (Percodan), and oxycodone sustained release (OxyContin) are currently the most popular abused opioids. Opioids used as analgesics are discussed in Chapter 6, which focuses on the pharmacology of the opioids themselves. It should be noted that opioids sold illegally on the street may be adulterated. They may contain other unknown agents or diluters and often contain inactive filler so the doses can be more easily divided.
In addition to being analgesics, opioids produce a state described as complete satiation of all drives in some people. The opioids elevate the user’s mood, cause euphoria, relieve fear and apprehension, and produce a feeling of peace and tranquility. They also suppress hunger, reduce sexual desire, and diminish the response to provocation. Undoubtedly, initial abuse is reinforced by this “positive” experience. Other side effects include slowed respiration, constipation, urinary retention, and peripheral vasodilation.
With the development of physical dependence, however, the driving motivation to obtain the drug becomes more and more negative. Fear of the withdrawal syndrome begins to override other motivation. At this point, the addict may resort to criminal activity and violence to support the drug habit. These activities are not direct actions of the drug but are related to opioid dependence.
PATTERN OF ABUSE
Heroin is the opioid most commonly administered parenterally. The signs and symptoms of an acute overdose are fixed, pinpoint pupils, depressed respiration, hypotension and shock, slow or absent reflexes, and drowsiness or coma. Tolerance develops to most of the pharmacologic effects of the opioids, including the euphoric, analgesic, sedative, and respiratory depressant actions. However, tolerance does not develop to miosis or constipation.
The symptoms and time course of the withdrawal syndrome are determined by the specific drug abused and the dose of drug used. Withdrawal usually begins at the time of the abuser’s next scheduled dose. The first signs of withdrawal from heroin are yawning, lacrimation, rhinorrhea, and diaphoresis, followed by a restless sleep. With further abstinence, anorexia, tremors, irritability, weakness, and excessive gastrointestinal activity occur. The heart rate is rapid, the blood pressure is elevated, and chills alternate with excessive sweating. Without treatment, symptoms disappear by about the eighth day after the last dose of heroin.
MANAGEMENT OF ACUTE OVERDOSE AND WITHDRAWAL
If the triad of narcotic overdose (respiratory depression, pinpoint pupils, and coma) is present, naloxone (Narcan) should be administered immediately. If there is no response, it is unlikely that the depressed respiration is caused by opioid overdose.
In the past, immediate withdrawal reaction from an opioid sold on the street was only moderately distressing to the patient because of the poor quality and dilution of these drugs. Recently, high-quality heroin has reached the streets, and overdoses are more common and the withdrawal more intense. Some addicts go “cold turkey” because the daily cost of their habit has risen too high. After withdrawal, they begin using again, but a smaller dose (therefore less expensive) is needed to produce the desired effect.
Patients in withdrawal can be made comfortable with methadone, a long-acting opioid that can replace heroin and then be gradually withdrawn. A phenothiazine or benzodiazepine is often administered for relief of tension. Long-term rehabilitation programs use several treatment approaches such as methadone maintenance. These include substitution of a physiologically equivalent drug (e.g., methadone) in high doses, gradual weaning from methadone, or use of a long-acting opioid antagonist (e.g., naltrexone) (see Chapter 6). Other psychotropic agents may be helpful in managing the alcoholic patient because of the high incidence of comorbidity of psychiatric conditions.
DENTAL IMPLICATIONS
The following should be considered when treating a dental patient who abuses opioids (narcotics).
Pain Control: Because an opioid abuser develops tolerance to the analgesic effects of any opioid, treating pain with opioids is ineffective and can cause a recovering addict to begin using opioids again. It is best to alleviate the cause of the pain first and prescribe nonsteroidal antiinflammatory drugs (NSAIDs) for analgesia.
Opioid abusers often come to the dental office requesting an opioid for severe pain (“shopping”). Often, the drug abuser suggests the name or partial name of a specific opioid or states allergies to several less potent agents.
Increased Incidence of Disease: Certain diseases that can be transmitted by use of needles for injections have a higher incidence in opioid abusers. These include hepatitis B, human immunodeficiency virus (HIV) producing acquired immune deficiency syndrome (AIDS), and sexually transmitted diseases. Infections caused by the use of nonsterile solutions and instruments can produce osteomyelitis and abscesses in the kidneys and heart valves. Intravenous drug abusers have about a 30% chance of developing cardiac valve damage over a 3-year period.
Chronic Pain: The dental health care worker will occasionally encounter dental patients with chronic pain. There are two ways in which these patients present to the dental office: a patient with symptoms of chronic dental-related pain (temporomandibular joint disorder or trigeminal neuralgia) or a patient reporting an elongation of the period of pain related to normal dental treatment (e.g., patient gets several refills of opioids for a root canal and no pathology can be identified). Patients who have pain for a much longer time than normal deserve a workup for chronic pain. Opioids are usually not effective in the management of chronic pain. If the dentist begins providing prescriptions for opioids to some patients, it is difficult to stop writing these prescriptions for the patient. The patient may state, “I hurt real bad.” Another subtle lever that may increase the chance that the dentist would prescribe more opioids is the unsettling feeling that he or she has not performed some dental treatment correctly. Sometimes mild references to malpractice can magnify this worry. One should not be “blackmailed” into prescribing opioids if one feels uncomfortable. One should just state the office policy, for example, “The policy of this office is that no refills for an opioid (narcotic) analgesic are given without an additional office visit. It is important to identify the cause of the pain so that it can be alleviated.”
OPIOID STREET DRUGS
Opioids available on the street change with time and are different in different parts of the country. The dental health care worker should be aware that most drug abusers misuse more than one substance and that street drugs are often adulterated.
An illicitly produced meperidine derivative that produced classic opioid effects contained 1-methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine (MPTP). This powerful neurotoxic agent has a toxicity unrelated to its opioid effects. It produces classic and permanent (irreversible) Parkinson’s disease by destroying the cells in the substantia nigra (they make dopamine) within a very short period. This contaminant has become a valuable research tool because it can induce Parkinson’s disease in animals, providing an animal model for research of drugs for treatment of Parkinson’s disease.
Sedative-Hypnotics
Sedative-hypnotics include barbiturates; alcohol; meprobamate (Miltown); methaqualone (Quaalude; not made legally now, called “ludes”); chloral hydrate; benzodiazepines, such as chlordiazepoxide (Librium) and diazepam (Valium); and N2O. Although their chemical structures vary greatly, their pharmacologic actions and pattern of abuse are similar.
Initial symptoms resemble the well-known symptoms of alcohol intoxication: loss of inhibition, euphoria, emotional instability, belligerence, difficulty in thinking, poor memory and judgment, slurred speech, and ataxia. With increasing doses, drowsiness and sleep occur, respiration is depressed, cardiac output is decreased, and gastrointestinal activity and urine output are diminished. Paradoxic reactions can range from elation to excessive stimulation. The mechanism of excitement with a CNS depressant is related to an increased sensitivity to blocking of the inhibitor fibers, leaving the excitatory fibers unopposed. With additional CNS depression, the excitatory fibers are also depressed, resulting in sedation.
PATTERN OF ABUSE
The CNS depressant drugs are generally taken orally, often in a combination with some of the other drugs of abuse. With an acute overdose, respiratory and cardiovascular depression occur, leading to coma and hypotension. The pupils may be unchanged or small, and lateral nystagmus is seen. Confusion, slurred speech, and ataxia are always present. Compared with opioids, the CNS depressants have a slower onset of tolerance and physical dependence. Tolerance to the sedative effect is not accompanied by a comparable tolerance to the lethal dose. With prolonged misuse, emotional instability, hostile and paranoid ideations, and suicidal tendencies are common.
Although the withdrawal syndrome for all CNS depressants is similar, its time course depends on the half-life of the drug abused. The first signs of withdrawal are insomnia, weakness, tremulousness, restlessness, and perspiration. Often nausea and vomiting, together with hyperthermia and agitation, occur. Delirium and convulsions may culminate in cardiovascular collapse and loss of the temperature-regulating mechanism.
Another troubling abuse of the sedative-hypnotics involves administering them to other people to control them. Old movies have demonstrated the “slipping of a Mickey Finn” (chloral hydrate) to knock a person out (“knock-out drops”). A recent similar practice involves using a short-acting benzodiazepine, flunitrazepam or Rohypnol (nickname is “Ruffies”) to make an unsuspecting young woman excessively sedated. After the woman becomes semiconscious, her partner would take sexual advantage of her and commit rape. This is often referred to as “date rape.” Because of the excessive sedation and the amnesia produced by the flunitrazepam, recounting or even remembering what happened is difficult. Therefore prosecution would be unlikely because it would be difficult to prove whether the action was consensual.
MANAGEMENT OF ACUTE OVERDOSE AND WITHDRAWAL
The most important consideration with an acute overdose of a CNS depressant is support of the cardiovascular and respiratory systems. An airway must always be established and maintained. Early gastric lavage after intubation and dialysis can assist in removal of some drugs. CNS stimulants are harmful and should not be given.
In contrast to withdrawal from opioids, withdrawal from CNS depressants can be life threatening and the patient should be hospitalized. The treatment of withdrawal from any CNS depressant includes (1) replacement of the abused drug with an equivalent drug and (2) gradual withdrawal of the equivalent drug.
The drug usually substituted for the abused drug is a long-acting benzodiazepine such as chlordiazepoxide or diazepam. The substitute drug is then gradually withdrawn over a period of weeks; during this time, the patient receives psychotherapy.
CENTRAL NERVOUS SYSTEM STIMULANTS
The CNS stimulants include cocaine, the amphetamines, caffeine, and nicotine.
Cocaine
Cocaine is a CNS stimulant with local anesthetic properties when applied topically. It is used primarily for its stimulant action by “sniffing,” “snorting,” or intravenous injection. The most recent variant is a free-base form that is smoked and goes by the street name of “crack” or “rock.” It is more pure and potent, and the resulting intoxication is far more intense than that of snorted cocaine. It acts much quicker and is much more euphoric and addicting. Cocaine induces intense euphoria, a sense of total self-confidence, and anorexia. Because of its short duration of action, the effects of cocaine last only a few minutes. Paranoia and extreme excitability cause some cocaine users to perform violent acts while under its influence. The paranoia produced by cocaine causes people to be unpredictable. The senseless violent acts sometimes committed by cocaine users cause society to fear cocaine abusers. Unpredictable actions are feared the most. Psychological dependence becomes intense, but neither tolerance nor withdrawal has been shown. Cocaine’s medical use is on mucous membranes (the inside of the nose) in which it produces local anesthesia and vasoconstriction to reduce hemorrhage. There is no appropriate dental use of cocaine. Although cocaine abuse is greatly publicized, the proportion of the population using cocaine is relatively small (compared with alcohol and tobacco).
Amphetamines
Drugs in the amphetamine class include methamphetamine (Desoxyn), dextroamphetamine (Dexedrine), diethylpropion (Tenuate), and methylphenidate (Ritalin). Another member of this group is phentermine (Fastin), which is the phen in Phen-Fen (a diet drug combination removed from the market). Because methamphetamine produces a much longer duration of effect than cocaine, “meth” use is spreading across the nation. Many meth laboratories (labs) have been raided, but more pop up immediately. The manufacture of methamphetamine can be carried out with common chemistry lab equipment and a precursor drug (ephedrine) that can be bought over the counter. Because of this, ephedrine is no longer available for purchase and products containing pseudoephedrine are now stocked in the actual pharmacy. Persons, over the age of 18, can only purchase a limited quantity of pseudoephedrine each year and most sign a log verifying the purchase. Unfortunately, these meth labs are explosive, smell bad (distinctive odor), and have been found in many residential neighborhoods.
The sympathomimetic CNS stimulants are abused for their ability to produce a euphoric mood, a sense of increased energy and alertness, and a feeling of omnipotence and self-confidence. Other effects include mydriasis, increased blood pressure and heart rate, anorexia, and increased sweating.
CNS stimulants are taken orally, parenterally (intravenously or “skin popping”), intranasally, or by inhalation (smoking). With prolonged use, tolerance develops to the euphorigenic effect and toxic symptoms appear, including anxiety, aggressiveness, stereotyped behavior, hallucinations, and paranoid fears.
Signs and symptoms of an acute overdose include dilated pupils (sympathetic autonomic nervous system stimulation), elevated blood pressure, rapid pulse, and cardiac arrhythmias. The patient may exhibit diaphoresis, hyperthermia, fine tremors, and hyperactive behavior. Oral adverse reactions include xerostomia and bruxism.
Although tolerance develops to the central sympathomimetic effect, no tolerance develops to the tendency to induce toxic psychoses at higher doses. Modest levels of abuse over a long period do not produce withdrawal reactions except fatigue and prolonged sleep, but large doses can precipitate a withdrawal syndrome consisting of aching muscles, ravenous appetite with abdominal pain, and long periods of sleep. This is followed by profound psychological depression and sometimes even suicide. During this period, abnormal electroencephalographic (EEG) results have been recorded.
MANAGEMENT OF ACUTE OVERDOSE AND WITHDRAWAL
Treatment of an overdose of a CNS stimulant is symptomatic. It may include a phenothiazine for psychotic symptoms, a short-acting sympathomimetic-blocking agent if hypertension is severe, and a tricyclic antidepressant if severe depression occurs.
The most serious sociologic problem with stimulant abuse is the induction of mental abnormalities, especially in young abusers. Experimental evidence suggests that amphetamine psychoses can be induced in previously unaffected volunteer subjects. The psychoses are dose related, and repeated dosing can reproduce the psychoses.
Caffeine
Caffeine, the most widely used social drug in the world, is contained in coffee, tea, cola drinks, and other drinks named to reflect the effect of their contents. Its action on the CNS is stimulation, which is why many people use these beverages. Caffeine toxicity can occur with as little as 300 mg of caffeine (contained in two to three cups of coffee). With five cups or more of caffeine daily, physical dependence can occur. Although many people do not consider it a drug, a withdrawal syndrome can be identified that begins around 24 hours after the last cup of coffee. It consists of headache, lethargy, irritability, and anxiety. Tolerance develops to the effects of caffeine, and some persons continue to use caffeine even when it produces harm. Table 25-3 lists the caffeine content of several beverages.
TABLE 25-3
CAFFEINE CONTENT OF SELECTED CAFFEINE-CONTAINING BEVERAGES (MG)
| Beverage | Caffeine (mg) |
| Cup of coffee—brewed | 100-150/5 oz |
| Decaffeinated coffee | 2-4/5 oz |
| Cup of tea—brewed | 60-75/5 oz |
| Cola drink | 60-105/12 oz |
| Mountain Dew | 55/12 oz (0)* |
| Jolt | 71/12 oz |
| Chocolate, milk | 3-6/oz |
| Chocolate, bittersweet | 25/oz |
| No-Doz | 100 mg/tablet |
Tobacco
Awareness of the toxicity from chronic smoking and chewing tobacco has increased dramatically over the past 2 decades. The CNS-active component of tobacco is nicotine, but a large number of components of the gaseous phase of tobacco smoke contribute to its undesirable effects: carbon monoxide, nitrogen oxides, volatile nitrosamines, hydrogen cyanide, volatile hydrocarbons, and many others.
PATTERN OF ABUSE
Approximately 25% of the adult American population smokes. Children commonly begin smoking between 11 and 14 years of age. In some geographic areas, more teenage girls than teenage boys smoke. The newest “craze” is cigar smoking; it is portrayed as glamorous, and famous movie stars are observed smoking cigars. Smokers claim that the most desirable effects of smoking are increased alertness, muscle relaxation, facilitation of concentration and memory, and decreases in appetite and irritability. These are consistent with the effect of nicotine on the CNS. In addition, nicotine produces an increase in blood pressure and pulse rate and induces nausea, vomiting, and dizziness as a result of stimulation of the chemoreceptor trigger zone. Smokers are tolerant to these latter effects, but such tolerance does not last long. The first cigarette of the day may induce a certain degree of dizziness and nausea. Chronic use of tobacco is causally related to many serious diseases, including coronary artery disease and oral and lung cancers.
SMOKELESS TOBACCO
In some communities, more than one-fourth of high school males use chewing tobacco. Oral mucosal changes include chronic gingivitis, leukoplakia, and precancerous lesions. In these patients, an extremely thorough oral examination should be done at each prophylaxis. Education concerning the oral health hazards that smokeless tobacco poses should also be included.
MANAGEMENT AND WITHDRAWAL
The withdrawal syndrome that occurs after cessation of chronic tobacco smoking varies greatly from person to person. The most consistent symptoms are anxiety, irritability, difficulty in concentrating, and cravings for cigarettes. Drowsiness, headaches, increased appetite, and sleep disturbances are also common. The syndrome is rapid in onset (within 24 hours after the last cigarette) and can persist for months.
The syndrome of withdrawal from tobacco can be suppressed to some extent by administration of nicotine chewing gum (Nicorette, Nicorette DS) or nicotine patches (NicoDerm, Nicotrol, and Habitrol; Table 25-4). These products do reduce the irritability and difficulty in concentrating but appear to be less effective in controlling insomnia, hunger, and the craving for tobacco. The most important dental side effect of the use of nicotine gum is dislodging dental fillings. Another form of nicotine replacement is the nasal spray Nicotrol NS. A potential problem with the nasal spray is that the rapid rise in blood level more closely mimics the effect of using tobacco.
BUPROPION
Another approach to treating tobacco cessation involves the use of bupropion (Wellbutrin, Zyban), which is an antidepressant, to reduce craving. Dentists can prescribe bupropion but should encourage concomitant treatment modalities (e.g., behavior modification). The recommended dosage schedule is 150 mg daily (qd) for 3 days, followed by 150 mg twice a day (bid) for an additional 2 to 3 months if the patient is experiencing success. Refills should not be indicated on the original prescription because the dental health care worker should talk with the patient by phone before authorizing a refill (see Chapter 17).
VARENICLINE
The newest approach to treating tobacco cessation involves the use of varenicline (CHANTIX), Varenicline is a nicotine-receptor blocker that binds to the nicotine receptor and prevents the nicotine from tobacco from reaching its receptor site. By binding to this receptor, varenicline limits the amount of dopamine that is released in the brain. It is thought that stimulation of nicotinic receptors releases dopamine, which accounts for the feeling of pleasure that is often associated with tobacco use. Varenicline is dosed daily for the first three days of therapy and is then dosed twice daily for the remaining course of therapy. Varenicline is taken after meals with a full glass of water. A normal course of therapy is 12 weeks. The most common side effects include nausea, sleep problems, constipation, gas, vomiting, and changes in mood and behavior. It cannot be used in conjunction with other smoking cessation drug products.
THE DENTAL HEALTH CARE WORKER’S ROLE IN TOBACCO CESSATION
Dental health care workers are in a special situation to be helpful in promoting tobacco cessation because of their role in encouraging patients to change habits (e.g., floss, brush teeth, and use fluoride). Smoking cessation is another habit change (behavior modification). The dental health care worker is in a position to point out some of the oral manifestations of nicotine and tobacco abuse firsthand in the patient’s own mouth. The National Cancer Institute currently has a program for dental personnel that includes a variety of patient education devices.* Every dental office should offer its patients help in smoking cessation.
PSYCHEDELICS (HALLUCINOGENS)
The psychedelic agents are capable of inducing states of altered perception and generally do not have any medically acceptable therapeutic use. The drugs in this section include lysergic acid diethylamide (LSD) and phencyclidine (PCP), but many other agents, including psilocybin, dimethyltryptamine (DMT), 2,5-dimethoxy-4-methylamphetamine (STP), methylenedioxyamphetamine (MDMA), and mescaline (peyote), also fall into this class. Clearly, the agents discussed in this section represent only a fraction of those released on the illicit drug market. These hallucinogens are often mislabeled or adulterated with substances such as strychnine.
Psychedelics affect perceptions in such a way that all sensory input is perceived with heightened awareness; sounds are brighter and clearer, colors are more brilliant, and taste, smell, and touch are more acute. Psychedelic-induced dependence is psychologic, and tolerance develops within a short time. These two characteristics combined with the unpredictable nature of the response favor periodic rather than continuous abuse of psychedelic drugs. Prolonged use can cause long-lasting mental disturbances varying from panic reactions to depression to schizophrenic reactions.
Lysergic Acid Diethylamide
LSD is the most potent hallucinogen; only micrograms are required for an effect. In addition to its psychogenic actions, LSD has sympathomimetic effects, including tachycardia, rise in blood pressure, hyperreflexia, nausea, and increased body temperature.
An overdose of LSD produces symptoms that include widely dilated pupils, flushed face, elevated blood pressure, visual and temporal distortions, hallucinations, derealization, panic reaction, and paranoia. Because the user does not lose consciousness and is highly suggestible, treatment is to provide reassurance (“talking the user down”). Rarely, chlorpromazine has been used to treat the situation in an emergency. Flashbacks, commonly precipitated by marijuana use, can occur years after ingesting LSD. LSD is currently making another comeback.
Phencyclidine
PCP (or angel dust), originally developed as an animal tranquilizer, was popular in the 1970s. It inhibits the reuptake of dopamine, serotonin, and norepinephrine. Although it has anticholinergic properties, hypersalivation is produced. It is a powerful CNS stimulant with dissociative properties. Users may exhibit sweating and a blank stare. Changes in body image and disorganized thought have led to bizarre behavior and psychosis. Elevation of blood pressure and pulse and muscle movement and rigidity occur. It is abused alone or as an adulterant to other street drugs.
Marijuana
Marijuana (marihuana, cannabis) is derived from the hemp plant, and its active ingredient is tetrahydrocannabinol (tet-ra-hi-dro-can-NAB-i-nol) (THC). Marijuana can be administered orally or by inhalation (smoking), and its effects include an increase in pulse rate, reddening of the conjunctivae (bloodshot eyes), and behavioral changes. Slight changes in blood pressure and pupil size and hand tremors have been noted. With normal doses, euphoria and enhanced sensory perception occur. This is followed by sedation and altered consciousness (a dreamlike state).
Studies of the influence of marijuana on driving have concluded that the drug impairs motor and mental abilities required for safe driving. For example, the perception of time and distance is distorted and reflexes are decreased. A more common adverse reaction is apprehensive, nervous, and panic-stricken feelings that the user is losing his or her mind. This reaction responds to friendly reassurance. Psychological dependence on marijuana is determined by the frequency of use. Physical dependence, tolerance, and withdrawal symptoms are rare.
Of particular interest to the dental health care worker is the fact that a high level of marijuana abuse may cause xerostomia. It has been noted anecdotally that some marijuana users develop gingivitis. Heavy marijuana smoking can lead to chronic bronchitis and precancerous changes in the bronchioles. THC is known to reduce intraocular pressure and has been used in the treatment of resistant glaucoma. It is also effective as an antiemetic to treat the nausea associated with cancer therapy.
IDENTIFYING THE DRUG ABUSER
“Shoppers” interact with many health care workers in an attempt to obtain controlled substances for illegitimate uses. Some references suggest that shoppers can be identified by the presence of poor hygiene, long-sleeved shirts, scars along veins, sunglasses, abrupt changes in behavior, moodiness, and behaving as though they were under the influence of an intoxicant, although usually this is not the case.
Most shoppers are excellent storytellers and actors with convincing histories and the presence of a pathologic dental condition. They look and behave like a typical patient. They may suggest specific drugs or give a history of allergy to analgesics they do not want. One should note the patient’s response to the mention of drugs that the dental provider is going to prescribe. This can be a tip-off that the patient is hoping for a more potent drug.
Intravenous drug abusers are more likely to contract sexually transmitted diseases (STDs) and are more likely to have hepatitis (hepatitis B virus [HBV] and hepatitis C virus [HCV]) or be a carrier, be HIV positive, or have AIDS and to be infected with multidrug-resistant tuberculosis and to have altered heart valves.
The dental office should not stock many controlled substances because it can become the target of robberies and burglaries. Addicts searching for drugs can be violent. The location of the supply of controlled substances must be under lock and key and in an inconspicuous place.
THE IMPAIRED DENTAL HEALTH CARE WORKER
When dental health care workers abuse drugs, they can present a danger to the patients being treated.
A professional who is abusing drugs, like most abusers, is in denial, and confrontation by staff, relatives, and friends is often ineffective. The dentist’s dental practice deteriorates and mood swings, including depression, occur. Often, suicide is thought to be the only recourse.
Any dental health care worker who observes or suspects that another worker is abusing drugs should report the person to the appropriate “impaired professional committee” for their profession. Most state boards currently have committees to work with any impaired dental professional (those that have abused alcohol or drugs). The committee’s goal is to assist the dental health care worker in becoming a functioning practitioner again. The objective of these committees is not to punish the worker to make the person lose his or her license. These committees can also investigate a suspicion of abuse. The difficulty in self-regulation is the silent practitioners who do not want to get involved.
CLINICAL SKILLS ASSESSMENT
1. Define the following terms:
2. What physical effects occur at low and high doses of caffeine consumption?
3. Can one build tolerance or become “addicted” to caffeine?
4. What are the symptoms associated with caffeine withdrawal?
5. What is caffeine toxicity and what are its signs and symptoms?
6. What factors influence the metabolism of alcohol?
7. What are the physiologic effects of alcohol?
8. What are the chronic, long-term effects of alcohol consumption?
9. Is caffeine effective in treating acute alcohol intoxication? What should be done?
10. Describe the long-term problems associated with cigarette smoking. Mention several organs that are affected.
11. Discuss the use of smokeless tobacco in adolescents and their idols (think baseball).
12. State oral changes that can occur with smokeless tobacco.
13. Describe the increased use of cigars and hypothesize about probable causes.
14. Describe the dental health care worker’s role, if any, in a dental office tobacco cessation program. Could a community role for the dental health care worker be planned?
15. What are some of the products available to people to help them stop smoking or using other smokeless tobacco products?
 Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
Please visit http://evolve.elsevier.com/Haveles/pharmacology for review questions and additional practice and reference materials.
*National Cancer Institute: 800-4-CANCER.