Seating Systems as Extrinsic Enablers for Assistive Technologies
OVERVIEW OF NEEDS SERVED BY SEATING
Physical Skills or Mat Assessment
Matching Device Characteristics to a Consumer’s Needs and Skills
Sitting Postures and Center of Pressure
PRINCIPLES OF SEATING FOR POSTURAL CONTROL
Guidelines for Postural Control
PRINCIPLES OF SEATING FOR TISSUE INTEGRITY
Incidence and Costs of Pressure Ulcers
Other Factors That Contribute to Pressure Ulcer Development
Microclimate at the Seat/Buttock Interface
Transfers and Handling Techniques
PRINCIPLES OF SEATING FOR COMFORT
TECHNOLOGIES FOR SEATING AND POSITIONING MANAGEMENT
Design and Construction of Seating Systems
Prefabricated Adjustable Backs
PROPERTIES OF MATERIALS USED TO CONSTRUCT SEATING SYSTEMS
Classification of Cushion Technologies
Cushions Made From Cellular Materials
SEATING FOR PRESSURE DISTRIBUTION AND POSTURAL SUPPORT
Technologies to Enhance Sitting Comfort for Wheelchair Users
On completing this chapter, you will be able to do the following:
1 Identify the potential outcomes of seating for postural control, tissue integrity, and comfort
2 Describe a comprehensive seating assessment
3 Describe key biomechanical principles related to sitting and seating technologies
4 Describe the principles of seating for postural control
5 Describe the factors that contribute to the development of pressure ulcers
6 Discuss pressure mapping systems and the issues related to their use in the clinic
7 Discuss the principles of seating for comfort
8 Discuss the design and construction of seating technologies
9 Describe the different characteristics of seating materials
10 Discuss the different classifications of materials used to construct seats
For a user of assistive technologies, a prerequisite to any interaction or activity is a physical position that is comfortable and that promotes function. The primary purpose of seating devices is to maximize a person’s ability to function in activities across all performance areas (self-care, work or school, play or leisure); for this reason, they are considered to be general-purpose extrinsic enablers.
The first part of this chapter describes the needs served by seating systems, evaluation of individuals for seating, and biomechanical principles related to seating. The remainder of the chapter provides in-depth information on each of the three categories of seating needs, including related principles and the technologies used for intervention. Seating components are typically interfaced with some type of mobility base. For purposes of this text, however, these two systems are separated. Mobility is viewed as a specific-purpose extrinsic enabler (see Chapter 12).
OVERVIEW OF NEEDS SERVED BY SEATING
Three distinct areas of seating intervention have emerged, each serving a particular consumer need. These three categories of seating intervention are (1) seating for postural control, (2) seating for tissue integrity, and (3) seating for comfort (Geyer et al, 2003).
The needs of children and adults with cerebral palsy and other neuromuscular disorders have led to the development of seating interventions for postural control and deformity management. These individuals typically have abnormal muscle tone, muscle weakness, primitive reflexes, or uncoordinated movements that impair their ability to maintain an upright posture in a wheelchair. Their impaired motor control affects their ability to participate in activities of daily living, can compromise their general health status, and can result in skeletal deformities.
The principles that guide seating design and selection for individuals with cerebral palsy are also relevant to individuals with other neurological disorders resulting in impaired motor control, such as cerebral vascular accident and traumatic brain injury. One commonality across all these groups is the dynamic nature of their seating needs over time. Individuals whose motor control impairment results from trauma usually realize improvements in motor function with recovery. In other situations, individuals lose motor control as a disease progresses. Children grow and develop motor skills. The seating system that is designed for individuals in these groups must be flexible so that it can accommodate their changing needs. The primary population served by the category of seating interventions for pressure management is individuals with spinal cord injury. These individuals can have partial or complete paralysis and reduced or absent sensation below the level of their lesions. As a result, they are susceptible to breakdown of the tissue over bony prominences on weight-bearing surfaces. Individuals with multiple sclerosis, those with muscular dystrophy, the elderly, and others who have limited mobility and therefore a reduced ability to relieve pressure from weight-bearing surfaces also benefit from technologies in this category. Postural management to achieve even pressure distribution is a further need of this group.
The third category of seating addresses the need to improve an individual’s level of physical comfort through postural accommodation. Persons in this category may or may not use a wheelchair on a regular basis and typically have normal or near-normal sensation; however, any prolonged sitting causes discomfort from which they are unable to obtain relief. Therefore they have unique needs and are not completely served by either category described above. Specialized seating can help to alleviate this chronic discomfort and maximize function. Box 6-1 shows some of the potential outcomes of seating intervention for these populations.
EVALUATION FOR SEATING
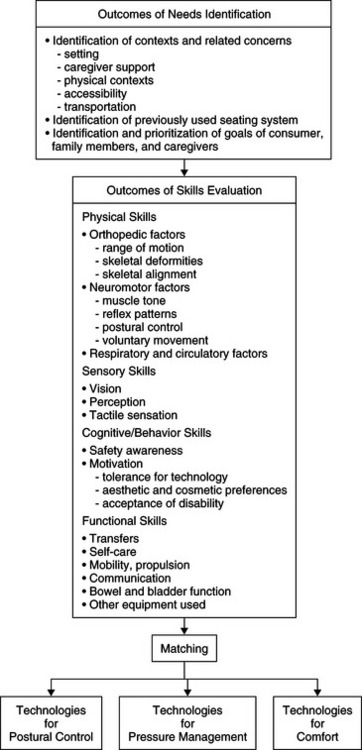
The process of assessing individuals for the purpose of recommending seating technologies requires a systematic method that includes consideration of many factors. The discussion of design of an assistive technology system in Chapter 2 gave a general framework to guide assessment. The purpose of this section is to provide a framework for evaluating consumers specifically for seating. Figure 6-1 outlines a framework to guide the assistive technology practitioner (ATP) through the decision-making process and ultimate selection of seating and positioning technologies that match the needs and skills of the user.
As with other areas of assistive technology, the process of delivering seating services is a transdisciplinary effort involving the skills of several professionals. Occupational and physical therapists typically provide expertise in neuromotor function, human development, and knowledge of disabilities. A physician documents the medical status and prognosis of the consumer and the medical justification for the seating system. The physician can also indicate whether surgery or other medical procedures are planned and what effects these procedures may have on the consumer’s seating. Assistive technology suppliers often provide knowledge of available technologies and their application to meet specific goals. Sometimes a rehabilitation engineer provides this service. In cases where the consumer’s need cannot be met by commercial products, the rehabilitation engineer or seating technician can design and build a custom system.
Needs Identification
Figure 6-1 lists the desired outcomes of the identification of needs. It is important to determine exactly what an individual’s specific needs are regarding seating. From the identified needs, goals to be addressed by the seating intervention are developed. It is the ATP’s responsibility to facilitate the identification and prioritization of these goals. Design of a seating system sometimes involves compromising the various goals. For example, desired biomechanical alignment may not be possible for a person with severe postural deformities when the resulting properly aligned position is too uncomfortable. Any assessment with the goal of identifying seating needs and recommended technology starts with discussion of the occupations the user wants and needs to complete while using the seating system. A general measure such as the Canadian Occupational Performance Measure (Law et al, 1997) provides a systematic means of discussing key occupations in the area of self-care, productivity, and leisure. There are some measures that are specific to seating and wheeled mobility, including the Functioning Everyday in a Wheelchair measure (Mills et al, 2002). The Wheelchair Outcome Measure (Miller, Mortenson, and Garden, 2006) is a new measure that considers function in self-care, productivity, and leisure specifically from the view of an individual who uses seating and mobility devices.
The level of assistance an individual requires to use the seating system is an important consideration in the assessment. Consideration must be given to whether an individual can transfer to the system and fasten any straps independently when he or she expects to use the seating system independently. The complexity of the system and the ease of access influence the demands placed on an individual providing assistance with a transfer.
Functional skills, including transfers to and from different surfaces (e.g., bed to wheelchair, car to wheelchair), self-care skills (e.g., feeding, dressing), wheelchair mobility, written and verbal communication skills, and bowel and bladder care should be evaluated. Equipment the person will use while in the seating system needs to be taken into consideration. For example, respiratory equipment and augmentative communication devices are frequently mounted on the wheelchair and need to be in a position that is functional for the user.
It is important that the individual’s ability to perform functional activities be evaluated both in the existing system and in a simulation of the proposed system. By observing the consumer performing functional activities from his or her existing system, the ATP learns two things. First, the ATP can determine the consumer’s level of independence and areas where function is impeded. The ATP can also learn what strategies the individual currently uses to complete functional activities. By using the methods described below, the ATP can then simulate different positions with the consumer. The ATP can have the individual perform functional tasks while in these simulated positions. Changing the sitting position will affect the person’s ability to perform certain activities. It is important to select a system that maximizes the person’s function and does not interfere with the use of strategies that have proven to be beneficial. For example, a teenager who uses an abnormal asymmetrical tonic neck reflex to operate a single switch should not be prohibited from doing so unless another movement can be found that accomplishes this task. It will sometimes be necessary to trade an ideal seated posture for a posture that allows the individual to be more functional.
Human Factors
Physical Skills or Mat Assessment.
The physical evaluation includes assessment of orthopedic factors, postural control, and respiratory and circulatory factors (see Figure 6-1). It is recommended that evaluation of physical skills take place with the person both in a sitting position and supine on a flat surface such as a mat.
Orthopedic Factors.: Orthopedic evaluation involves measurement of joint range of motion and assessment of skeletal deformities and skeletal alignment to determine optimal angles for sitting. Obtaining information regarding limitations in range of motion and deformities is necessary to determine whether the goal of the seating system will be to prevent deformities, correct deformities, or accommodate deformities (Trefler, Hobson, and Taylor, 1993).
Starting with the consumer supine on the mat, mobility of the lumbar spine and pelvis are assessed, followed by range of motion measurements of the hips, knees, ankles, upper extremities, and neck. Joint angle and body measurements as shown in Figure 6-2 should also be made at this time. Alignment of the individual’s head, shoulders, and trunk with the pelvis is determined next. Range of motion and skeletal alignment should also be assessed with the individual in a sitting position to determine how the body parts are affected by gravity. Bergen, Presperin, and Tallman (1990) describe in detail a process for measuring joint angles and assessing skeletal alignment.
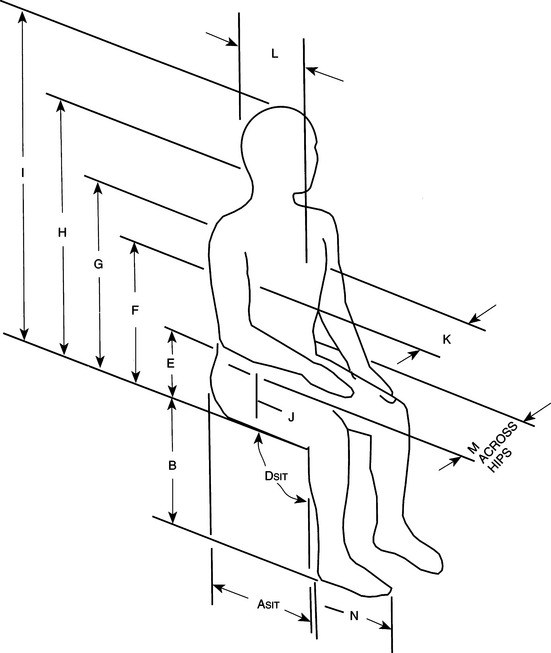
Figure 6-2 Joint angle and body measurements taken during the evaluation.ASit (R and L), behind hips/popliteal fossa; B (R and L), popliteal fossa/heel; DSIT, knee flexion angle; E, sitting surface/pelvic crest; F, sitting surface/axilla; G, sitting surface/shoulder; H, sitting surface/occiput; I, sitting surface/crown of head; J, sitting surface/hanging elbow; K, width across trunk; L, depth of trunk; M, width across hips; N, heel/toe. (From Bergen AF, Presperin J, Tallman T:Positioning for function: Wheelchairs and other assistive technologies, Valhalla, NY, 1990, Valhalla Rehabilitation Publications.)
Valhalla Rehabilitation PublicationsIt is important to determine whether any skeletal deformities present are fixed or flexible. In a fixed deformity, permanent changes have taken place in the bones, muscles, capsular ligaments, or tendons that restrict the normal range of motion of the particular joint. Fixed deformities affect the skeletal alignment of the other joints and typically require a seating system that is designed to accommodate the deformity. Often, increased tone and muscle tightness cause persons to assume certain postures, and they may appear to have a deformity. With externally applied resistance (passive stretch) in the opposite direction, however, it is possible to move the joint and reduce the deformity. The person is then considered to have a flexible deformity at that joint. Depending on the situation, the seating system may be designed to correct a flexible deformity. Specific deformities and their effects on sitting posture are described in the section on seating principles for postural control.
Some individuals have had surgery to correct one or more deformities. The ATP should be aware of any surgery the consumer may have undergone and be knowledgeable about the implications it has for seating intervention. In other cases, the team may decide during the evaluation that surgical or orthotic intervention should be considered before seating intervention takes place. If this is the situation, referral to the appropriate medical professional is necessary. Letts (1991) examines surgical interventions related to the seated position.
Postural Control.: The user’s postural control is a key element to assess, particularly for children developing motor control, individuals recovering motor function after a neurological injury such as traumatic brain injury, or someone losing motor control as a consequence of a progressive illness. Two important aspects should be considered: the individual’s ability to control the posture in a sitting position (i.e., how much support is required to maintain a comfortable sitting position with a reasonable amount of effort) and the response to various positional changes. The most effective way to assess these aspects is with the client seated on a mat.
The ability of an individual to control his or her posture during sitting is determined with the client seated on a mat with the feet supported. The client’s sitting ability is described by the amount of support required to maintain a seated position. Hands-free sitters are those who do not need to use their hands to support themselves to maintain sitting, whereas hands-dependent sitters do need to use their hands. These individuals could not perform a seated activity using the hands without some type of external support. A dependent sitter does not have sufficient motor control to support himself or herself in sitting at all. Postural control tends to be less than in those in the other two categories.
Postural control typically develops in a cephalocaudal direction, although recovery of postural control after traumatic brain injury does not necessarily proceed in this fashion. The amount of external control required to assist an individual to maintain a seated position is an important determination. Kangas (2000) recommends provision of the minimal amount of external support. Support may vary with the activity. Less support may be needed when the individual is engaged in a sedentary activity such as watching television. Alternatively, more support is needed when the individual is using his hands for an activity and the focus of attention is on the activity. The individual should not need to divert attention to the maintenance of posture when engaged in an activity.
Finally, the ATP needs to determine the individual’s response to various postural changes. Primarily, the ATP should assess the effect of changes of pelvic position on the client’s postural control. What happens when the pelvis is positioned in a neutral, anterior-tipped or posterior-tipped position? Similarly, what effect does change of spinal alignment or lower limb position have on postural control? The client’s response to these position changes will influence the configuration of the seating system and whether any dynamic elements need to be provided.
Respiratory and Circulatory Factors.: The person’s respiratory status and circulation are other factors addressed during the evaluation. With skeletal deformities, pulmonary and cardiac function can be compromised. It is important to know whether certain positions enhance or limit respiration. Circulation, particularly in the lower limbs, needs to be considered as well. Some individuals may have a condition that predisposes them to circulatory problems; particularly for these consumers, positions that impair circulation should be avoided.
Sensory and Perceptual Skills
Vision and visual perception, as discussed in Chapter 3, contribute to a person’s balance and sitting posture, and deficits in these areas need to be considered during the evaluation. The configuration of the seat can affect the user’s line of vision. For example, an individual with poor postural control who is unable to maintain spinal extension with consequent neck flexion may not be able to maintain the head in an upright position if the seat to back angle is set at 90 degrees. The user’s line of vision will be downward in this seating configuration. A person’s awareness of body position (proprioception) in space also influences body posture.
Tactile sensation is another factor to consider. Some individuals may react defensively to the touch of certain textures or positioning components on the body. Other individuals lack tactile sensation, which can contribute to skin breakdown. The ATP should determine whether there is any known decrease in sensation, particularly in the buttock area, and whether there is a history of pressure ulcers. The condition of the person’s skin on weight-bearing surfaces (including areas on the trunk that are braced by lateral supports) should be checked for evidence of skin breakdown, circulation, color, smoothness, sensation, and moisture (Tredwell and Roxborough, 1991).
Cognitive Skills
Cognitive skills such as problem solving and motor planning are not as much of an issue in seating as in mobility. However, there are a few areas that require consideration. Individuals with poor safety judgment may not be aware of the need to keep a positioning belt fastened, and special considerations may be necessary. When the seating system is complex, understanding the client’s cognitive abilities will aid the decision to teach the client or the caregiver about the proper use of the system. Knowing the individual’s language and communication skills (see Chapter 11) will help determine how the ATP gathers information during the evaluation. For example, if a person relies on an augmentative communication device or on yes/no responses, these modes of communication should be used during the evaluation process. If it is known that the consumer is not reliable in his or her responses, then the ATP should seek assistance from a caregiver in interpreting the consumer’s responses to the seating system.
Psychosocial Factors
The meaning that technology holds for the individual is an important factor to explore with the user, although it is more significant for the mobility component of a seating and mobility system. Many clients prefer technology that does not draw attention to a disability. This preference will be a factor in the selection of a seating system. Esthetics is an important factor in acceptance and rejection of the technology (Pape, Kim, and Weiner, 2002). Behavioral problems, such as an agitated person who throws himself against the back of the chair, can also present a safety problem that needs to be addressed. Working together with the consumer and the caregiver to address these concerns is essential.
Environmental Considerations
The seating assessment should determine in which environments the seating system will be used (e.g., home, school, workplace, and vehicle and whether it is necessary for the system to be used in different environments). Knowledge of where the seating system will be used helps the ATP determine whether the system will be removed and reinstalled in the mobility device or other devices. For instance, an individual who transfers to the car seat when traveling from home to school will remove the seating system when the mobility device is stored in the vehicle and replace it on arrival at the destination. Many seating devices designed for young children are intended to pair with different bases (e.g., the system may be used in a stroller, high chair, or floor sitter).
The ATP should determine the extent to which the seating system will be used outdoors. Temperature is an important factor to consider when designing a seating system. Extreme heat or cold will affect the function of many materials, limiting their ability to meet the goals set for use of the system. A more complete discussion of the effect of temperature on materials used in seating systems follows. Exposure to light sources may affect some materials used to cover a system component, altering its properties and again, affecting the function of the system.
Social Context.
The ATP must know who is available to assist the consumer with the use of the system when it is used in multiple settings. This knowledge influences the instruction given to the users of the system and influences considerations with respect to the weight, complexity, and maintenance of the system. Many ATPs who recommend seating products have seen situations where a simple seat cushion is placed backward in a mobility device, causing great discomfort to the user. The risk of misuse is much greater with complex seating systems. Consequently, the ATP must ensure that the user and any caregivers are familiar with proper use of the seating system. Adequate instruction is key to preventing misuse of the system.
Individuals who routinely lift and carry a seating system must be able to do so without risk of injury. Materials used to construct seating systems have changed in recent years, in part to decrease the weight. However, some custom-made systems, such as foam in place, which will be discussed below, can be quite heavy. Maintenance of the system is another consideration. Air-filled cushions require careful attention to ensure that they are properly inflated and free of punctures. As mentioned above, the properties of some materials are affected by extremes of temperatures, so whoever is responsible for maintenance of the system must take care to avoid damage to it in this manner. In some situations, the system that is most ideal for the client cannot be recommended because of the ability of the caregiver to use and care for it.
Institutional Context.
Funding implications are a key institutional consideration. General considerations with respect to funding were described in Chapter 5. The ATP needs to remain current on funding requirements when recommending seating products. Another type of legislation has unique implications for seating products: the use of restraints. Certain legal jurisdictions have legislation that regulates the use of restraints with individuals residing in institutional settings. The intent of this legislation is to limit inappropriate use of restraints, such as tying an individual into a chair simply to prevent him or her from moving around, when safety is not an issue. This legislation has implications for the use of straps, pelvic belts, and sub–anterior-superior iliac spine (ASIS) bars that are used in seating systems for positioning and safety reasons. The ATP should be aware of whether these types of legislation affect the ability to incorporate positioning belts, and so forth, in a seating system.
Matching Device Characteristics to a Consumer’s Needs and Skills
The information that has been gathered regarding needs and skills provides a profile of the user. It can then be determined which of the three categories in Figure 6-1 matches the consumer’s profile, which allows identification of potential technologies and evaluation of their effectiveness in meeting the consumer’s needs.
The next step is to actually simulate with the consumer one or more of the alternatives. The ATP can observe the effects of changes in body position and materials by having the consumer try variations of the positioning system. Trial positioning is also helpful for assessing the person’s ability to use control interfaces such as the joystick of a power wheelchair. Changes in position can be made to see whether there are beneficial or adverse effects on the person’s ability to control a device or perform other functional skills. Simulation makes it easier to document the need for and effectiveness of a particular system so that funding can be obtained. If specific cushions or positioning components are being considered for a consumer, it helps to have him or her try the actual product and determine whether he or she likes it. In some instances it may be desirable for the consumer to take the system home for a trial period, which allows the person to use the system over a longer period and in his or her natural environment.
There are several critical questions that can help the ATP evaluate the effectiveness of the technologies that have been simulated and to select an appropriate seating system for the consumer. These questions, which summarize the needs evaluation, the skill assessment, and the simulation, are shown in Box 6-2. The primary concern is whether the simulated seating system meets the goals identified during the needs assessment. The ATP should consider the extent to which the system achieves desired goals with respect to positioning, support of function, and comfort. The caregiver’s ability to lift, carry, and maintain the seating system is a further factor to consider. A system that does not meet these goals to the satisfaction of the client of the caregiver will not be used.
BIOMECHANICAL PRINCIPLES
To design and implement seating systems effectively for consumers with disabilities, it is important to understand how the laws of physics govern the actions and effects of the mechanical elements of the postural control system. These principles are embodied in biomechanics, the study of body position and movement. This section presents the major concepts of biomechanics, which are fundamental to an understanding of seating and positioning systems for persons with disabilities.
Kinematics: Study of Motion
When seating systems are designed, the position of the consumer, the position of the seating system components, and their movements should be considered. The term kinematics describes movement. The term displacement is used to define the position of a body in space; a change in displacement results in a new position. For example, in a postural support system, one goal is to bring the trunk to a midline position. This action may require a displacement from the rest position to midline by application of an external lateral trunk support. The rate of change in displacement is called velocity. It is also important to know how fast the velocity is changing (increasing or decreasing); this change is called acceleration. One of the most common accelerations is that of gravity. The term gravity actually refers to the acceleration of an object toward the center of the earth. Acceleration of an object is directly related to the force generated by the object’s movement.
There are two fundamental types of displacement: linear and rotational. When all parts of a body move in the same direction, at the same time, and for the same distance, the movement is linear (Low and Reed, 1996). For example, a person generates translational movement when walking. Displacements caused by external positioning components can also be translational. If the direction, distance, and time of the movement occur simultaneously, but the movement is through an angle instead of in a straight line, the movement is called rotational. Rotational movements occur around an axis called the fulcrum. The majority of body movements are rotational, such as hip or elbow flexion and shoulder flexion or extension. Some positioning components cause rotational displacements (e.g., reclining the back of a wheelchair causes rotation at the pelvis and hip).
Kinetics: Forces
Force is a major element in biomechanics and seating for individuals with disabilities. Force is anything that acts on a body to change its rate of acceleration or alter its momentum (Low and Reed, 1996). It is described by both magnitude and direction (Sprigle, 2000). Forces always occur in equal and opposite action-reaction pairs between bodies, although it is often convenient to think of one body being in a force field. Forces can be applied to the body internally or externally. Internal forces are generated inside the body, such as muscle contractions that cause movement of the joints. Externally applied forces come from outside the body and act on it in some way, such as the forces applied by a support surface and components of a seating system such as lateral supports. The force resulting from the acceleration of gravity is another external and ever-present force that acts on the body and influences its posture and movement (Sprigle, 2000). This force on the body acts along a line called the gravitational line, and its effect is localized around a point in the body called the center of gravity. The force of the earth’s gravitational field tends to pull the body toward the center of the earth and must be accounted for in designing a seating system. The center of gravity changes as posture changes from standing to sitting and in different sitting positions.
Four properties of force, which ultimately determine its result, are magnitude, direction, line of application, and point of application.Magnitude is the amount or size of the force measured in newtons, pounds, or kilograms. Forces are applied in some direction, either pushing or pulling, and are applied along a particular line of application. The force acts at a particular point on the body, called the point of application (Low and Reed, 1996).
Types of Forces.
There are three different types of force. Each of these types produces different effects on the body, and it is important to understand these differences when designing seating and positioning systems. Tension forces act in the same line but away from each other (pulling apart), such as the force applied on the antagonist muscle during contraction of the agonist muscle. Compression occurs when forces act toward each other (pushing together), such as the force of the vertebrae on the disks in the spinal column. Shearing occurs when the forces are parallel to each other (sliding across the surfaces), such as the movement that occurs as the head of the femur moves across the acetabulum during hip movement. Each of these types of forces can also be applied externally to the body, such as the force exerted by a seating surface on the ischial tuberosities (compression), the force exerted by lateral supports to extend the trunk (tension), or the force exerted on the tissues in the buttocks when a seat back is reclined (shearing).
Stress.
Stress is the resulting molecular change inside biological (e.g., soft tissue and bone) or nonbiological (e.g., metals, plastics, or foams) materials. Stress is caused by the same three types of forces—tension, compression, or shear—and can result in damage to the biological tissue or other material if it is prolonged. For example, a shear force applied to a foam seat cushion can result in tearing of the foam. This is a change in the molecular structure of the foam caused by an externally applied force. Likewise, a piece of connective tissue that is subjected to severe or prolonged compression loading by sitting (e.g., under the ischial tuberosities) may be damaged by crushing of the tissue. This externally applied force results in compression inside the tissue, causing a change in the structure of the biological material.
Pressure.
Every force is applied over a surface area. For example, with a postural support system, the force of each component is applied to an area of the body. It is important to determine the effect of each of these forces, and the concept of pressure is important. Pressure is defined as force per unit area, which means that a force applied over a very small area generates more pressure than the same force applied over a larger area. Imagine a 10-pound cat lying on a surface such as your stomach. The force generated by the cat is applied over the entire surface of its body and the pressure is uniform. Now imagine the same cat standing on your stomach. The force of the cat is the same, but the pressure at each of the cat’s paws is much greater (and it hurts more) because the area of application (the paw) is much smaller than when the force is distributed over the whole surface area of the cat. This basic concept of distributing pressure by increasing the area of application is applied extensively in seating and positioning systems.
Newton’s Laws of Motion.
The English scientist Sir Isaac Newton formulated three laws relating to forces on bodies at rest and in motion.Newton’s first law states that a body at rest tends to remain at rest and that a body in motion in a straight line tends to remain in motion unless external forces act to change either of these states. In other words, a body likes to continue what it is doing, moving or resting. This law defines inertia, which is equal to the force required to accelerate an object.Newton’s second law relates three parameters: the mass of a body, the change in velocity (acceleration), and the forces acting on that body. The force is equal to the mass (in kilograms) multiplied by the acceleration of the body (Force = Mass × Acceleration), which means that the greater the force, the greater the acceleration, or conversely, the greater the mass for the same force, the smaller the acceleration. The force of gravity is the mass of the object multiplied by the acceleration of gravity. This force is commonly referred to as the weight of an object, and it is the reason that an object weighs less on the moon, because the gravitational acceleration there is less than that on the earth.
Newton’s third law is the one most applicable to seating and positioning systems. This law states that if one body exerts a force on another, there is an equal and opposite force, called a reaction, exerted on the first body by the second (Low and Reed, 1996). This law is applied to seating systems with the assumption that every force exerted by the human body while sitting in a wheelchair or a seating system is balanced by an opposite force exerted by the sitting surface on the person (Sprigle, 2000). The force generated by the body is equal in magnitude and opposite in direction to the force generated by the seating system, which is often referred to as equilibrium. When a body is at rest and all internal and external forces are balanced, the body is in a state of static equilibrium. When forces are balanced around a body during movement, resulting in a constant velocity, it is described as dynamic equilibrium. Both types of equilibrium are important in seating and positioning systems.
Friction.
Throughout this discussion, it has been assumed that ideal circumstances exist. For example, a shear force applied to a body causes it to move across a surface, and ideally it encounters no resistance to movement from that surface. In reality, of course, this is not truebecause frictional forces exist between two bodies in contact moving in opposite directions (Sprigle, 2000). Two types of friction are defined: static friction and dynamic friction.Static friction is that force that must be overcome to start a body in motion. Static friction is proportional in magnitude to the perpendicular (compression) force holding the two bodies together. Static friction is independent of the area of contact between the two bodies. Once motion is initiated, the resistive force is generally smaller, and it takes less force to keep the bodies moving relative to each other than to start movement. Friction during movement is called dynamic friction. Both these frictional forces are affected by surface conditions such as moisture, heat, texture, and lubricants, and both are important considerations in the recommendation and design of seating surfaces.
Sitting Posture and Center of Pressure
Stability and mobility are two related dimensions of seated postural control. Stability allows an individual to maintain an upright seated position while mobility allows movement that enables function; for example, mobility allows the individual to lean forward to reach to shake a friend’s hand. Seating interventions for postural control must achieve an optimal balance between stability and mobility.
Two constructs are important to consider when discussing postural control: center of gravity and center of pressure. The location of the center of gravity is fairly well defined in standing. Its location is described as passing through the mastoid processes of the jaw, a point just in front of the shoulder, a point just behind the center of the hip joints, a point just in front of the center of the knee joints, and approximately 5 to 6 cm in front of the ankle joints (Figure 6-3). In this posture the pelvis is in a neutral position and there is a natural lordosis of the lumbar spine (Zacharkow, 1988). The location in sitting is more difficult to determine, but it is usually considered to be lower, with the buttocks and thighs forming the base of support. The individual must maintain the center of gravity over the base of support to maintain an upright posture in either sitting or standing. Seating interventions for postural control assist the client to keep the center of posture within the limits of the base of support.
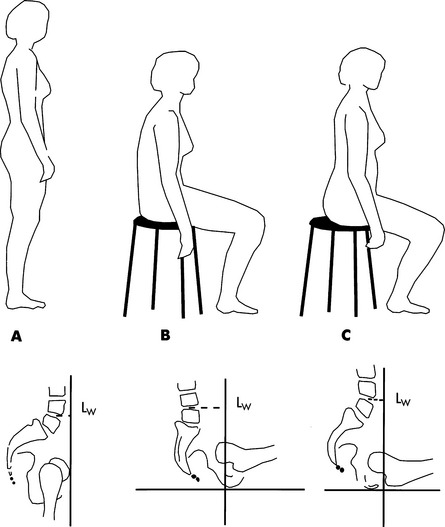
Figure 6-3 A, Line of gravity in erect upright standing. B, Relaxed unsupported sitting resulting in backward tilt of the pelvis and flattening of the lumbar lordosis. C, Erect sitting with reduction in backward pelvic tilt and increased lordosis.LW, Lever arm. (From Frankel VH, Nordin M:Basic biomechanics of the skeletal system, Philadelphia, 1980, Lea & Febiger.)
Lea & FebigerIt is not practical to measure or monitor the center of gravity in the clinic. The center of gravity is defined by three-dimensional coordinates. The center of pressure is described only in the horizontal plane, which makes it a much more clinically useful outcome. Its location in the frontal and lateral planes can be identified and monitored in the clinic by using a pressure mapping system. These systems use various technologies to monitor the pressure between the individual and a support surface (i.e., between the client’s buttocks and thighs and the seat cushion). They are most commonly used to show pressure distribution when pressure-relief cushions are evaluated, so their function will be described in greater detail in that section.
As mentioned above, the aim of postural control in seating intervention is to provide the client with a functional upright position (i.e., provide enough support to enable him or her to retain a seated position but also to enable sufficient movement to promote function in sitting). Monitoring of the center of pressure during quiet and active sitting is one way to evaluate the outcome of specific seating interventions. Discussion of the center of pressure is a relatively recent occurrence in the literature. The ideal location of the center of pressure is midway between the ischial tuberosities. Dunk and Callaghan (2005) found that the location of the center of pressure in the frontal plane varied between men and women. They studied various sitting postural parameters of university students engaged in computer activities while sitting on different office chairs. They found that the center of pressure was behind the center of mass of the chair for men and ahead of it for women. This finding has interesting implications for seating intervention, although it has not been explored.
Parkinson, Chaffin, and Reed (2006) describe the stability zone or limit, which they define as the balance limits for a person in either sitting or standing. A seat back and laterals or armrests will affect the stability limits in sitting. The authors initially hypothesized that the stability was limited laterally by the ischial tuberosities and posteriorly by the coccyx in the absence of these system features. The thighs provide support when the individual is reaching forward. Age, strength, and range of motion were identified as additional factors that affected the stability zone. They quantified the center of pressure during a lateral reaching task with a sample that included both young and older individuals and subjects with a body mass index range from underweight to obese. The greater trochanter, rather than the ischial tuberosities, was found to be more indicative of the stability zone because subjects shifted their weight laterally as they reached. Stability during reach was also affected by age, reach direction (lateral and forward reach were greater than rearward), and hip breadth (Parkinson, Chaffin, and Reed, 2006).
The center of pressure is an interesting phenomenon that has been explored recently, primarily in a nonclinical population. The studies described above suggest that differences exist in parameters related to center of pressure between men and women (Dunk and Callaghan, 2005), body mass, and age (Parkinson et al, 2006). These studies did not include individuals with disabilities, so the implications of the findings to this group are not clear. Further study is needed to explore the relationship between center of pressure and function and the effect of various seating interventions on this relationship.
Principles of Seating for Postural Control
Children and adults who have irregular tone, muscle weakness, abnormal reflex patterns, shortening of a muscle group, or skeletal deformity are likely to require external positioning devices to control their posture and prevent deformities. Within this category some individuals have mild impairment and require only minimal support, whereas other individuals have severe physical impairment and require extensive postural support. The components making up a seating system can provide support to the body to improve skeletal alignment, normalize tone, prevent deformities, and enhance movement.
Guidelines for Postural Control
The most important principle related to postural control is that proximal stabilization, near the center of the body, facilitates movement and control of the head and the extremities (e.g., function). During normal development, the infant achieves stability in the proximal joints before using the distal limbs for manipulation. For example, before a baby can successfully reach out and grab a toy while sitting, he must have mastered the ability to maintain a balanced sitting posture (Bertenthal and Von Hofsten, 1998; Hadders-Algra, Brogen, and Forssberg, 1998; Hadders-Algra et al, 1999; Savelsbergh and Van der Kamp, 1994). Otherwise the hands must be used to maintain balance, which limits their use for manipulation. Seating for postural control provides external positioning components for the individual who does not have internal mechanisms to control body posture. Tredwell and Roxborough (1991) present a classification scheme (Box 6-3) that is useful in describing the amount of control a person exhibits in sitting. Each category is matched with a brief description of the recommended degree of support provided by the seating system.
When any type of external support is provided, care needs to be taken so that the individual is not excessively positioned. We need to keep in mind that sitting is a dynamic activity. We often associate sitting with relaxation and lack of activity and movement, when in fact many activities are performed while sitting, such as writing, driving, talking on the phone, and typing. Even during quiet sitting an individual frequently shifts weight to maintain comfort. It is not uncommon to see individuals “properly” positioned to the point that they are no longer able to use the motor movements they have used in the past to complete functional tasks. The fewest restraints necessary to optimize function should be used (Kangas, 2000).
In this section we present a set of general guidelines for proceeding with the development of a postural seating system for an individual.
Pelvis and Lower Extremities.
We have described the important role of the pelvis in relation to the center of gravity and sitting. The pelvis is a key point of control, and its position affects the posture of the rest of the body. Therefore, alignment and stabilization of the pelvis is normally the first area addressed in positioning an individual. A position with the pelvis in neutral or in a slight anterior tilt is desired (Mayall and Desharnais, 1995). The pelvis should be level and in midline.
Research examining the role of pelvic stability in the facilitation of function supports the assertion of starting with the pelvis when an appropriate seating system in being determined. Two studies investigated the effect of two methods of pelvic stabilization: a regular lap belt, typically using hook and pile fastening versus a rigid pelvic stabilizer (a sub-ASIS bar in one case and the Embrace Pelvic Positioner [Body Tech NW, Mukilteo, Wash.; http://www.dresch.org/web/BodyTechNW.com/] in the second) on function of children with cerebral palsy (Miller Polgar et al, 2000; Rigby et al, 2001). Both these studies compared daily function, as perceived by the participants and their families, when using the typical lap belt versus the rigid pelvic stabilizer. Results were comparable in both, with better function found with the rigid pelvic stabilizer. Significant differences were found on the Canadian Occupational Performance Measure (Law et al, 1997) before and after implementation of the rigid pelvic stabilizer. The results of these studies are limited by the small sample size, but the convergence of their findings provides evidence for the practice of controlling the pelvis in seating for postural control.
A position with the hips flexed at approximately 90 degrees is recommended for most individuals (Bergen, Presperin, and Tallman, 1992; Trefler, Hobson, and Taylor, 1993; Tredwell and Roxborough, 1991). This angle of hip flexion helps to inhibit extensor tone and reduces posterior tilt of the pelvis, thus keeping the individual positioned back in the seat. In some instances it is necessary to increase the amount of hip flexion (thus reducing the angle to less than 90 degrees) to further inhibit extensor tone. On the other hand, in some instances 90 degrees of hip flexion is not achievable (because of deformity) or is not the most appropriate position. Some individuals are not able to maintain an upright position when placed in a position of 90 degree hip flexion. Similarly, tight hamstrings may prevent achievement of 90 degrees at the knees. The ATP needs to determine the effect of deformities and muscle tone on both function and comfort in the sitting position, during a mat assessment, to determine the most appropriate position of the pelvis, hips, and lower extremities. Asymmetrical postures that may be present in the pelvis and hips include pelvic obliquity, pelvic rotation, pelvic tilt, and windswept hips. These postural asymmetries are often interrelated. They may be flexible postures or fixed bony deformities that restrict the mobility of the pelvis and limit the attainment of the recommended pelvic position.
An individual with a pelvic obliquity has one side of the pelvis higher than the other when viewed in the frontal plane (Figure 6-4, A). The obliquity is named for the side that is lower; for example, with a left pelvic obliquity the left side is lower than the right. This deformity is often accompanied by pelvic rotation, where one side of the pelvis is forward of the other side (Figure 6-4, B). Windswept hip deformity manifests itself with one hip adducted and the other hip abducted. This deformity has usually been found to be the end stage of a sequence that proceeds as follows: hip subluxation and dislocation, pelvic obliquity, scoliosis, windswept hip deformity. Typically, all these components are present in this deformity. The hip on the high side is typically dislocated, and the opposite hip may or may not be dislocated (Letts, 1991). When fixed deformities such as these are present, the seating system should be designed to accommodate them rather than to attempt to correct them (Mayall and Desharnais, 1995).
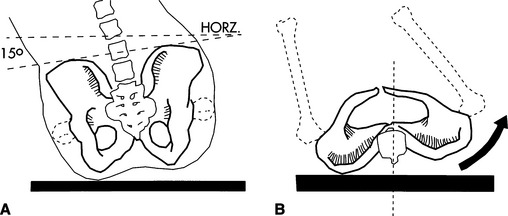
Figure 6-4 A, Pelvic obliquity viewed in the frontal plane. B, Pelvic rotation. (From Siekman A: The biomechanics of seating: a consumer’s guide,Action Dig March/April:8-9, 1992.)
Support to the pelvis can be provided under, behind, in front, or from the sides. At the very least, a firm seating surface for the individual to sit on will level and stabilize the pelvis. Individuals with moderate to severe involvement typically need more support for stabilization. This support can be provided by contours around the buttocks and up into the lumbar area. Alteration of the seat to back angle may be required when the individual has severe extensor tone. During the mat assessment, with the person in sitting, the therapist should move the client through different hip ranges to determine which hip angle achieves the most functional muscle tone. This optimal angle can then be replicated in the seating system, bearing in mind that the actual angle of the hip (femur to acetabulum) will be more acute than the seat to back angle of the seating system. A seat with a preischial block is another option used to control excessive extensor tone (Figure 6-5). With this approach, a depression is made in the cushion to accommodate the pelvis and to stop forward movement. Supports to prevent lateral shifting of the pelvis or external rotation of the hips can be provided either by contouring the seat to provide channels that position the thighs or with some form of lateral support at the pelvic level. To support the pelvis from the front, various types of pelvic positioning belts or knee blocks are used. The placement of the belt is important to effectively maintain pelvic position. Depending on the person’s pelvic mobility, comfort, and positioning needs, the pelvic positioning belt is placed at an angle ranging from 45 to 90 degrees to the seating surface, as shown in Figure 6-6. In most cases, a belt with an angle of pull at 45 degrees sufficiently maintains the pelvis in position. If there is excessive hip extension or a need for anterior pelvic mobility, positioning the belt at a 90-degree angle of pull is more effective. Pelvic positioning belts can be soft and flexible (e.g., webbing or padded vinyl) or rigid when more support is required. A rigid pelvic positioning device, also called a sub-ASIS bar (Figure 6-7), is typically a close-fitting, padded metal bar that is attached to the wheelchair frame or seat insert to position the pelvis below the individual’s ASIS. It is designed to be used in conjunction with a complete seat and back system for individuals who require greater control to maintain the neutral position of the pelvis and to prevent pelvic rotation. Similarly, handling of the client to determine the effect of pressure, or control, around the pelvis (e.g., at the ASIS or posterior-superior iliac spine) will help determine optimal placement of any pelvic stabilizing devices.
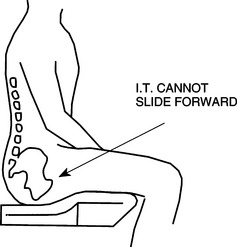
Figure 6-5 Antithrust seat. (From Bergen AF, Presperin J, Tallman T:Positioning for function: wheelchairs and other assistive technologies, Valhalla, NY, 1990, Valhalla Rehabilitation Publications.)
Valhalla Rehabilitation Publications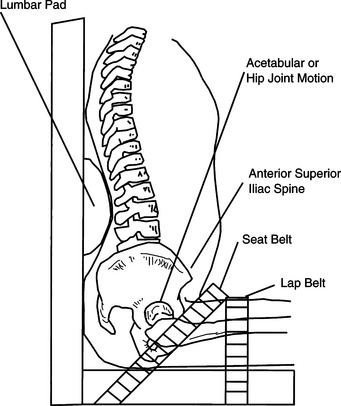
Figure 6-6 Pelvic positioning belts can be applied at 45 degrees (seat belt) or at 90 degrees (lap belt). (From Church G, Glennen S:The handbook of assistive technology, San Diego, 1992, Singular Publishing Group.)
Singular Publishing Group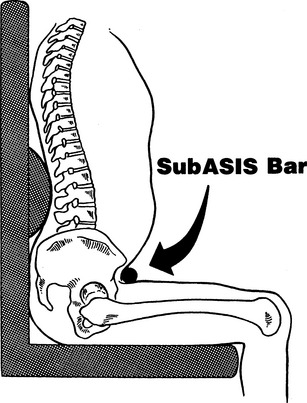
Figure 6-7 Sub-ASIS bar. (From Margolis SA, Jones RM, Brown BE: The subASIS bar: an effective approach to pelvis stabilization in seated positioning,Proceedings of the RESNA eighth Annual Conference, pp 45-47, June 1985.)
Adequately positioning the lower extremities helps to maintain the pelvic and hip positions. The positions of the legs and feet affect the position of the pelvis and therefore need to be addressed simultaneously. It is recommended that the legs be positioned so that the femurs are neutral with respect to abduction and adduction and rotation and with approximately 90 degrees of knee flexion, although there are some exceptions that will be noted below. Some form of sculpting is frequently used in the seat to keep the femurs in a neutral position and to limit adduction and internal rotation (Figure 6-8). A frequently encountered problem in the lower extremities is hamstring tightness, which may or may not result in flexion contractures of the knees. Recall that these muscles are closely related to the position of the pelvis. Attempts to position the individual to stretch these muscles and reduce the flexion contracture only result in posterior pelvic tilt and a sliding forward in the chair into a sacral sitting position. Instead, it is best to accommodate this problem by modifying the seating surface (shortening the seat depth or undercutting the front edge) so that the legs are allowed to flex under the seating surface. This maintains the correct pelvic position. If there is fixed knee extension, the lower leg must be completely supported with pads or troughs that match the range of motion in the knee.
Figure 6-8 Example of sculpted foam cushion to maintain pelvic and femur alignment. (Courtesy invacare Corp., www.invacare.ca.)
Support for the feet is important for maintaining hip and knee position, for preventing deformities in the ankles, and for distributing pressure. If the feet are left to hang or are positioned too low, pressure increases under the anterior thigh area, which can cut off blood flow. Positioning the feet too high places excess pressure on the ischial tuberosities and the sacrum, which can cause formation of a pressure ulcer. It is recommended that the feet be positioned flat and with 90 degrees of ankle flexion (Mayall and Desharnais, 1995). Support surfaces for the feet can be one or two platforms and in different sizes, depending on the person’s needs. Increasing the thickness of the foot support under the shorter leg serves to accommodate unequal lower leg length. Foot platforms can be angled to accommodate fixed plantar flexion contractures of the ankle. Various strapping systems can be used to maintain the desired ankle position, including straps over the top of the foot, behind the heel, and enclosing the ankle (Figure 6-9).

Figure 6-9 Example of an ankle positioning system that attaches to the footplate of a wheelchair. (Courtesy Bodypoint designs, Inc., www.bodypoint.com.)
Trunk.
Once the desired position in the pelvis and lower extremities has been obtained, the trunk is considered. An upright position with the trunk aligned in midline is desirable. This position may not be attainable if the individual has fixed deformities. Possible spinal deformities are (1) scoliosis, (2) lordosis, (3) kyphosis, or (4) a combination of these. Scoliosis of the spine occurs when there is lateral curvature or rotation of the vertebral column. Scoliotic curves are further defined according to the anatomical site in the vertebral column that is involved, that is, cervical, thoracic, or lumbar. Compensatory (or secondary) curves develop as a result of the head’s attempting to maintain its upright position (Figure 6-10, A) (Cailliet, 1975). Figure 6-10, B, shows an uncompensated curve with the spine unbalanced and the head lateral to the center of gravity. Rotation of the vertebrae is also frequently found in scoliosis and can cause greater respiratory difficulty than lateral curving (Cailliet, 1975).
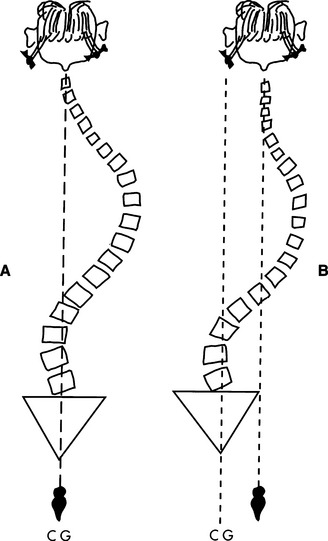
Figure 6-10 A, Development of compensatory curve in scoliosis.B, Uncompensated scoliotic curve. CG, Center of gravity. (From Cailliet R:Scoliosis: diagnosis and management, Philadelphia, 1975, FA Davis Co.)
FA Davis Co.The amount of trunk support required depends on how much control over the trunk that the individual has. As in the pelvis, trunk support can be provided from behind, at the side, or in front. The amount of support provided from behind is related to back height and contouring. The height of the back can be varied, depending on the amount of upper body support needed. Someone who requires minimal support can use a lower backrest height, whereas a higher backrest is necessary for the individual with a need for greater support. Contouring allows us to accommodate the individual’s body shape and provide optimal support. If the person has a kyphosis, the back needs to be recessed so that he or she is not pushed forward in the seat. For a lordosis, lumbar support can be added to bring the seat back in contact with the person. In cases where the shoulders are retracted, wedged blocks can be added to the back to position the shoulders forward.
When a person has difficulty maintaining a midline position (side to side) of the trunk, lateral support is provided (Figure 6-11). The positioning of the lateral supports depends on how much control the person has. Lateral supports placed high on the trunk and close to the body provide greater control than those placed lower on the trunk (Mayall and Desharnais, 1995). Because the forces placed on the body by the lateral supports can be great, care should be taken in placement of these components and selection of materials (well padded) to prevent tissue damage. If there is scoliosis, the application of force at three positions on the body is one means to attempt to limit the progress of the scoliosis, although there is limited evidence to support or refute this use. This three-point system uses the principles of equilibrium of forces to stabilize and align the trunk. As shown in Figure 6-11, one pad is applied under the apex of the curve on the convex side (F3), with two other pads opposing it to provide resistance ((F1 and (F2). One of these pads is placed up high under the armpit and the other point is on the pelvis (Trefler, Hobson, and Taylor, 1993).
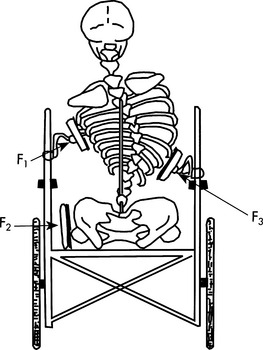
Figure 6-11 Three-point system of control for reducing the effects of scoliosis. (From Nwaobi OM: Biomechanics of seating. In Trefler E, editor:Seating for children with cerebral palsy: a resource manual, Memphis, 1984, University of Tennessee.)
University of TennesseeTilting the seating system back slightly can eliminate some of the effects of gravity for individuals with spinal deformities, low tone, decreased strength in the trunk, or poor head control and can also help the individual maintain a more symmetrical posture. The force of gravity is reduced in the tilt position, making it easier to maintain the trunk in midline and increasing the comfort of the laterals. The positive effects of tilt on trunk position must be evaluated by the limitations this position can place on function. Vision, the ability to eat, use of equipment on a tray, and social engagement are just some activities that can be compromised when the wheelchair seat is tilted.
When control is required to prevent forward trunk flexion, anterior supports can be used. This type of support is necessary for individuals who need to be in an upright position for a functional or therapeutic activity but who do not have the ability to maintain this position independently. The most common approaches used are straps, chest panels, and rigid shoulder supports. One simple approach is to use straps that are attached to the seat back below shoulder level, come up over the shoulders, and attach to the seating system near the hips (Figure 6-12, A). The chest restraint must be well maintained because it poses a safety concern if the lower attachment becomes loose, allowing the strap to constrict around the neck (Trefler, Hobson, and Taylor, 1993). Another approach is a solid chest panel in a butterfly, X, or I shape with straps that attach to the seating system as above (Figure 6-12, B). The final approach is to use rigid shoulder components (Figure 6-12, C) that come over the clavicle and hold the shoulder girdle back against the seating system. These components should be adjustable and well padded to ensure stabilization without excessive pressure.
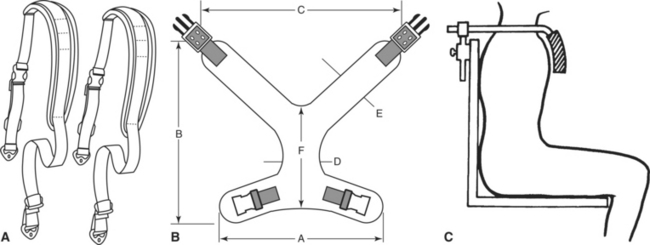
Figure 6-12 A, An example of a chest strap that attaches to the seat back below shoulder level, comes up over the shoulders, and attaches to the seating system near the hips. (Courtesy Bodypoint Designs, Inc., www.bodypoint.com.) B, Solid chest panel in an X design. (Courtesy Daher Manufacturing, Inc., www.daherproducts.com.) C, Rigid shoulder supports. (From Bergen AF, Presperin J, Tallman T:Positioning for function: wheelchairs and other assistive technologies, Valhalla, NY, 1990, Valhalla Rehabilitation Publications.)
Valhalla Rehabilitation PublicationsHead and Neck.
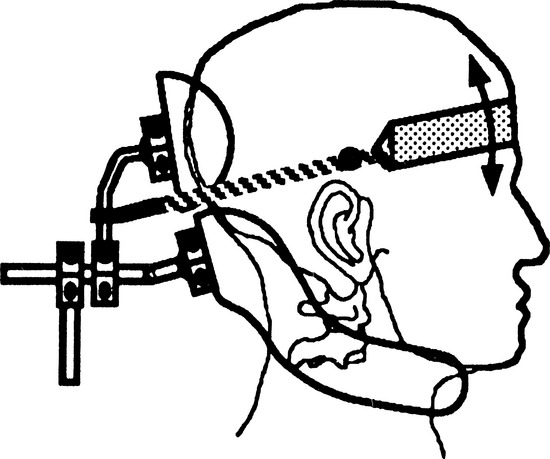
With the pelvis, lower extremities, and trunk positioned, head and neck positions are considered next. The position of the head is important in inhibiting abnormal reflexes and maximizing the visual skills of the individual. In some cases a headrest is necessary only part of the time, for example, when the individual becomes fatigued or during transportation. The most common problems leading to the need for positioning of the head include hyperextension of the neck, weak neck musculature, lateral neck flexion, and neck rotation. In addition, support may be required to right the head when the person has been reclined. As in the positioning of other body segments, posterior, anterior, or lateral components are used for support. Figure 6-13 shows examples of components for each of these types of support. Posterior support can range from a high backrest (for those requiring minimal support) to headrests of different types. With any posterior head support, it is important to avoid triggering extension or pushing the head forward into flexion. Anterior support is typically provided by headbands, which are used in conjunction with posterior head supports. Elastic materials or pulleys provide a dynamic type of support. These allow movement of the head within a limited range. Lateral supports can be incorporated into a headrest or provided as separate components. They can be applied at the temporal area, at the neck, or at the side of the face just in front of the ear.
Upper Extremities.
Support of the upper extremities is an essential component of the seating system. A lack of support for the arms can adversely affect head and neck position. Additionally, arms that are left to hang can sustain injury if caught on something or can acquire subluxation of the glenohumeral joint of the shoulder. Using an upper extremity support surface, such as a lap tray, helps with positioning of the head and neck, reduces the likelihood of damage to the arms and shoulder joints, and places the hands in a midline position that facilitates bilateral manual activities. The height of the lap tray depends on the needs of the consumer. Commonly the tray is mounted so that it allows the forearms to rest on it with the elbows bent at a 90-degree angle. For individuals with spasticity, a tray mounted higher will help to reduce upper extremity tone (Trefler, Hobson, and Taylor, 1993). Some individuals do not want a lap tray but still require positioning of the upper extremities. For these situations, individual arm troughs (Figure 6-14) mounted to the armrests of the wheelchair are available, which provide channeling and support for the arms.

Figure 6-14 Arm trough. (Courtesy Otto Bock, www.ottobockus.com/products/r_wheel.htm.)
PRINCIPLES OF SEATING FOR TISSUE INTEGRITY
A second major goal of seating interventions is pressure management. The emphasis in this area is to manage sitting pressure and maintain the skin in a healthy condition so that pressure ulcers are prevented. A pressure ulcer is a lesion that develops as a result of unrelieved pressure to the area and that results in damage to underlying tissue (Bouten et al, 2003). Pressure ulcers usually occur over bony prominences, with the sacrum, coccyx, ischial tuberosities, trochanters, external malleoli, and heels being the areas most commonly affected. These lesions have also been referred to as decubitus ulcers, bed sores, pressure sores, and dermal ulcers. Because pressure is the major factor influencing the development of these lesions, it is recommended that the term pressure ulcer be used to describe them (National Pressure Ulcer Advisory Panel, 1992).
Much research has been conducted attempting to determine the various factors that contribute to the development of pressure ulcers and to identify tools and strategies for preventing their occurrence. However, it is difficult to isolate all the variables that affect individuals as they go through their daily lives and to make substantive conclusions for a population as a whole on the basis of this research. Each person must be considered individually, and a comprehensive program of risk assessment and prevention must be developed to address his or her needs. The ATP needs to be aware of the role of seating, as well as all the other variables, to prevent pressure ulcers.
Incidence and Costs of Pressure Ulcers
Individuals who remain in bed for prolonged periods of time or who use a wheelchair and have limited ability to reposition themselves are at risk for development of pressure ulcers. In particular, individuals with spinal cord injury are at a high risk because they lack sensation and have limited movement below the level of the lesion. It is estimated that approximately one third of individuals with spinal cord injury will encounter some type of tissue breakdown during their lifetimes (Krause et al, 2001) and that approximately 25% of the health care costs associated with the consequences of a spinal cord injury are related to a pressure ulcer (Krause et al, 2001). Other populations with a high incidence of pressure ulcers include individuals with hemiplegia caused by stroke, multiple sclerosis, cancer, the elderly, and individuals who have had a femoral fracture.
Chen, DeVivo, and Jackson (2005) examined pressure ulcer prevalence in persons with spinal cord injury who were followed up through the National Spinal Cord Injury Database over the past two decades. Their sample included 3361 community-dwelling individuals with spinal cord injury who were followed up by nine centers participating in the Model Spinal Cord Injury Systems project. These nine centers were chosen because they collected continuous data throughout the duration of the study. The authors explored the relationship of risk factors and prevalence of pressure ulcer over time following the injury. Thirty-three percent of the sample had a pressure ulcer on entry to the study. It was found that the risk of pressure ulcer was relatively stable in the first 10 years following the injury. There was also a significant prevalence of recent pressure ulcers, which was not fully explained by other factors. Older subjects (50 years and older) were more likely to have a pressure ulcer. Other significant risk factors included male sex, African-American race, single marital status, education less than high school, and presence of other comorbid medical conditions (Chen, DeVivo, and Jackson, 2005).
In addition to the costs for medical care, there are social costs, which have a greater effect (Krouskop et al, 1983). Krouskop et al (1983) identify these costs as including (1) time lost from work, which affects the person and his or her family, (2) time lost from school, (3) time away from family, which can affect the person’s social development, and (4) loss of personal independence and productivity, which results in decreased self-esteem and self-worth.
Origins of Pressure Ulcers
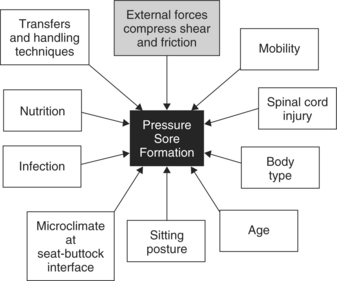
Many factors contribute to the development of pressure ulcers; these are shown in Figure 6-15. External forces applied to a localized area are considered to be the primary cause. With application of external pressure, the normal flow of blood and oxygen to tissue in that area is reduced. If this situation is sustained, changes occur in the tissue cells, and these changes eventually lead to death of the cells. Individuals who have limited movement and lie in bed or sit in a wheelchair for prolonged periods generate compression forces that reduce the blood supply to the tissues and make them prone to pressure ulcers. Pressure ulcers are most common over weight-bearing, bony prominences because the force at these sites is greater than at other locations covered by subcutaneous tissue.
The amount of external pressure sufficient to restrict the blood flow enough to cause tissue damage has been a point of discussion over the years. The average blood pressure in capillaries ranges from 12 mm Hg in the venous limb to 32 mm Hg in the arteriolar limb (Landis, 1930). External pressure on the weight-bearing surface that exceeds these pressures produces obstruction of the capillaries. When sitting pressures of subjects on various types of surfaces were measured, it was found that the pressure generated by each surface under the ischial tuberosities greatly exceeded capillary blood pressure (Kosiak et al, 1958). A contoured, alternating pressure chair was the only surface that provided intermittent reduction (in the down position) of pressure to levels in the range of capillary blood pressure. Because most of the seating surfaces in this study generated pressures that exceeded capillary pressure, investigators were led to question whether that is the primary cause of pressure ulcer formation or whether other factors are involved.
The duration of pressure is a significant variable in the development of pressure ulcers. Kosiak (1959) determined that there is an inverse relationship between the amount of pressure sustained and the time over which it is applied. In a study involving dogs, Kosiak found that a pressure of 600 mm Hg produced ulceration in approximately 1 hour and a pressure of 150 mm Hg produced ulceration in 12 hours. The results of this study are shown in Figure 6-16, A. Microscopic tissue changes were found after application of as little as 60 mm Hg of pressure over 1 hour. This finding is consistent with the theory that exceeding the capillary pressure deprives the cells of enough important nutrients to cause damage at some level.
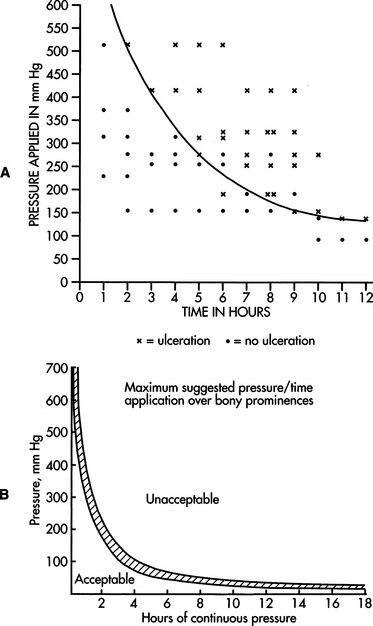
Figure 6-16 A, Relationship between applied pressure and time. Most points above the curve result in ulceration. (From Kosiak M: Etiology of decubitus ulcers,Arch Phys Med Rehab 42:19-29, 1961.) B, Allowable pressures versus time of application for tissue under bony prominences. (From Reswick JB, Rogers JE: Experience at Rancho Los Amigos Hospital with devices and techniques to prevent pressure sores. In Kenedi RM, Cowden JM, Scales JT, editors:Bedsore biomechanics, Baltimore, 1976, University Park Press.)
University Park PressTime as a variable in pressure ulcer development is taken into consideration with the broad guidelines developed by Reswick and Rogers (1976). These guidelines, based on years of clinical experience with individuals who have spinal cord injury, establish allowable amounts of pressure that tissue surrounding bony prominences can endure over certain periods. They recommend that pressures on the ischial tuberosities remain in the range of 30 to 60 mm Hg, as shown in Figure 6-16, B. Tissues that are not susceptible to the internal pressure exerted by bony prominences can tolerate higher skin surface pressures or lower pressures for longer periods.
Up to this point the effects of sustained perpendicular (compression) pressure forces on tissue have been discussed. Parallel (or shear) forces play a significant role in the formation of pressure ulcers as well. Shear forces are generated when two surfaces move across each other in opposite directions, for example, when an individual slides his hips forward in a wheelchair and assumes a sacral sitting posture. In this position the skin remains in contact with the seat surface and the superficial fascia is interlocked with the skin. The deeper portion of the superficial fascia, however, is mobile and slides forward. The blood vessels in this area are stretched and angulated, which causes occlusion. Resulting tissue damage is at a deeper level and typified by a large area of undermining around the base of the ulcer (Reichel, 1958). Bennett et al (1979) believe that it is the combination of pressure and shear that is so effective in occluding blood flow. They found that, when sufficient shear was present, only half as much pressure was needed to cause occlusion. Unfortunately, because of the difficulty in measuring shear, there is still uncertainty regarding the extent to which shear contributes to the development of pressure ulcers.
Friction, the force between two surfaces at rest or in motion, is another component of shear and the development of pressure ulcers. Friction leads to injury and ulceration of the surface of the skin. A typical friction injury to the skin occurs when it moves across a rough surface such as bedding. Dinsdale (1974) found that the skin’s susceptibility to pressure ulcer development is increased with friction. When pressure alone was applied, 290 mm Hg was required to produce ulceration. With the application of pressure and friction, ulcerations were produced with pressure levels as low as 45 mm Hg. Moisture, heat, or properties of materials such as clothing can increase frictional forces.
Other Factors That Contribute to Pressure Ulcer Development
Some individuals can be exposed to the mechanical forces of pressure and shear without pressure ulcers developing, whereas others have very little tolerance to these mechanisms. Although compression and shear forces are typically considered to be the chief causes of pressure ulcers, there are several other factors that contribute to skin breakdown and cause some individuals to be more susceptible than others.
Mobility.
Moving to relieve pressure over an area is how the body typically responds to prevent tissue damage. Nondisabled subjects make side-to-side weight oscillations several times per minute while sitting (Tredwell and Roxborough, 1991). Normally, when there is a lack of oxygen and chemical irritation, pain signals from the nerve endings trigger postural changes and there is little tissue damage. Individuals who lack normal sensation, such as those who have sustained a spinal cord injury, are unable to recognize and respond to these pain signals and are particularly susceptible to development of pressure ulcers (Chen et al, 2005).
Individuals whose ability to reposition themselves or whose activity is limited to bed or chair should be assessed for the risk of pressure ulcer development. There are scales available that determine the magnitude of risk by measuring the degree to which mobility and activity levels are limited. Two commonly used scales that assess these factors are the Norton Scale (Norton, McLaren, and Exton-Smith, 1975) and the Braden Scale (Bergstrom et al, 1987). In addition to mobility, these scales also assess other factors that place a person at risk for development of pressure ulcers, such as incontinence, impaired nutritional status, and altered level of consciousness. Individuals should be assessed with a validated systematic risk assessment tool on admission to acute care and rehabilitation hospitals, nursing homes, home care programs, and other health care facilities and at other periodic intervals. Identified risk factors can be reduced through intervention, and the development of pressure ulcers might be prevented.
Spinal Cord Injury.
As discussed above, loss of sensation and limitations in mobility put individuals with spinal cord injury at great risk for development of pressure ulcers. In addition, some researchers speculate that other changes in the body that result from the denervation caused by the spinal cord injury increase a person’s susceptibility to pressure ulcers. In a study of normal and paraplegic rats, no differences were found in their susceptibility to pressure (Kosiak, 1961). Constantian (1980) concludes that there is not adequate objective evidence that individuals with denervated tissue are predisposed to the development of pressure ulcers nor that denervated tissue heals more slowly or differently than skin with normal enervation. On the other hand, there is evidence that after spinal cord injury there may be tissue alterations (e.g., loss of collagen, abnormal vascularity, tone changes) and changes in hormonal response to stress that place a person more at risk for development of pressure ulcers and that impair the normal healing process (Patterson et al, 1992; Pfeffer, 1991; Whimster, 1976).
Differences in circulatory tissue perfusion between persons who have a spinal cord injury and those who do not have been documented (Patterson et al, 1992). With externally applied pressures of 32 mm Hg, it was found that the partial pressure of oxygen (an indicator of the perfusion of the tissue) was significantly lower in spinal cord–injured subjects than in subjects without a disability. To evaluate the response of the peripheral circulation to externally applied pressure, Patterson et al (1992) cycled the pressure loads on and off. Although oxygen perfusion was lower during both on and off periods for the persons with spinal cord injuries, it was only during the on period that these differences were statistically significant. At higher external pressures (75 mm Hg), the differences in oxygen perfusion for the two groups were not statistically significant. The difference between the two groups at the lower pressure was attributed to a lack of vascular autoregulation in the subjects with spinal cord injuries (Patterson et al, 1992). Autoregulation requires a minimal difference between internal pressure and external pressures. At 75 mm Hg autoregulation cannot occur because the external pressure is near the arterial pressure. Measurements of blood volume showed significant differences between the two groups at both external pressures. This study indicates that there are tissue perfusion changes in spinal cord injury that significantly impair the response to external pressure loads.
Measurement of these factors that may affect the development of pressure ulcers is improving but remains difficult, which makes it difficult to specify their particular effects on pressure ulcer development. However, it is likely that there are intrinsic changes in the body as a result of spinal cord injury that cannot be ignored. These changes may result in tissue with different properties and a reduced tolerance to external pressure.
Body Type.
The body type of the individual has some effect on pressure distribution. A thin person has less subcutaneous fat to act as padding, and therefore forces per unit area of the skin are increased. An overweight individual has more padding over which to distribute pressure. However, it may be more difficult for the overweight individual to perform pressure relief exercises. Caregivers may also have more difficulty moving an overweight individual, which may make shearing and friction forces a greater possibility.
Nutrition.
Inadequate nutrition is often associated with weight loss and muscular atrophy, both of which reduce the amount of tissue between the seat surface and the bony prominences. Inadequate dietary intake, which results in anemia, decreased protein levels, and vitamin C deficiency are also known to interfere with the normal integrity of the tissue (Berecek, 1981; Breslow, 1991) and have been linked not only to pressure ulcer development but also to delayed healing. An increased intake of protein and calories has been shown to improve the healing rate of pressure ulcers (Breslow, 1991).
Infection.
Torrance (1983) identifies three reasons why infection may contribute to pressure ulcer development. First, fever caused by infection increases the metabolic rate, which increases the demand for oxygen, which in turn endangers areas that are ischemic. Second, severe infection can also affect the nutritional balance of the body. Finally, localized bacteria increase the demand on metabolism in a localized area.
Age.
As people age, the skin loses some of its elasticity and muscles atrophy, which increases vulnerability to friction or shearing. Vascular and neurological diseases associated with aging (e.g., diabetes, renal disease) affect the circulation and may also increase an individual’s susceptibility to skin breakdown.
Sitting Posture.
Posture and deformity can affect the pressure distribution of the seat/buttock interface and can potentially contribute to skin breakdown. Two specific postures that pose a risk for pressure ulcer formation are pelvic obliquity and sacral sitting. Pelvic obliquity, which was discussed in detail in a previous section, results in increased pressure and shear under the affected lower ischial tuberosity and the posterior aspect of the lower greater trochanter (Hobson, 1989; Zacharkow, 1984, 1988). The loss of lumbar lordosis when sitting is another risk factor. This position occurs as a result of limited hip mobility for flexion or decreased spinal mobility for extension (Zacharkow, 1984). Consequently, a sacral sitting posture is typically assumed, which results in significant amounts of pressure being placed on the sacrococcygeal region.
Microclimate at the Seat/Buttock Interface.
The microclimate between the body and the seating surface is a critical factor that is often overlooked. The temperature of the skin and the presence of moisture both affect the formation of pressure ulcers. An increase in skin temperature of 1°C is accompanied by a 10% increase in the metabolic demands of tissue (Fisher et al, 1978; Stewart, Palmieri, and Cochran, 1980). In tissue that already has limited oxygenation as a result of pressure, the potential for breakdown is exacerbated. Moisture, from perspiration or incontinence, also increases the risk of skin breakdown for a number of reasons. Wet skin is weaker than dry skin and therefore more likely to incur damage as a result of compression and friction (Stewart, Palmieri, and Cochran, 1980). Additionally, moisture increases the potential for bacterial growth and infection. Keeping the skin clean and dry is important for these reasons.
The material of the seat cushion and its cover can alter the temperature and the amount of moisture at the seat/buttock interface. Foam cushions have been found to cause an increase in skin temperature, whereas water-filled cushions reduced skin temperature (Fisher et al, 1978; Stewart, Palmieri, and Cochran, 1980). Excessive moisture can also be a problem that varies with the cushion, its cover, and the user. Gel and water cushions have been found to increase the amount of humidity at the seat/buttock interface by 23% and 20%, respectively (Stewart, Palmieri, and Cochran, 1980). Selecting cushion materials and coverings that reduce temperature and moisture accumulation is discussed later in this chapter.
Transfers and Handling Techniques.
Abrasions or ulcerations can be caused by hitting objects or sliding across a surface during transfers. Whether the individual transfers independently or has someone providing assistance, care should be taken to prevent abrasions. The same holds true for mobility in bed. Pulling an individual across the bed sheets can cause abrasions or ulcerations from the friction. Caregivers should be reminded to lift an individual to move him or her in bed instead of sliding the individual across the bedding.
The development of pressure ulcers is a complex process, and there is still much to be learned about the exact mechanisms involved. Identifying factors that predispose an individual to pressure ulcers will help in developing a comprehensive pressure ulcer prevention program. A program for preventing pressure ulcers should include (1) a wheelchair and seating prescription for pressure distribution, postural alignment, and stability, (2) a pressure relief program, (3) dietary instruction and adequate nutrition, (4) instruction in proper transferring and lifting techniques, and (5) maintenance of good personal hygiene and skin care (McDonald, 2001). The development and implementation of the prevention program should be considered a continuing team effort involving the consumer, his or her therapists, and medical personnel.
Pressure Measurement
Pressure ulcers result from sustained compression of soft tissues, particularly under bony prominences. The predominant hypotheses concerning the pathogenesis of pressure ulcers include localized tissue ischemia, sustained deformation of the cells, impaired nutritional flow to the cells, reperfusion injury, and inadequate drainage of cellular waste products (Lander Ganz and Gefen, 2004; Stekelenburg et al., 2006). Lander Ganz and Gefen demonstrated that the pressure measured at the deep tissue level was significantly greater than that measured at the surface interface, although they could not predict a specific relationship. The prevalence of pressure ulcers and the resulting costs underscore the need to measure the forces applied to the muscle in an attempt to prevent prolonged exposure to high loads. Many sophisticated pressure measurement systems have been developed, including near infrared tissue spectrophotoscopy, Raman spectrography, and in-dwelling sensors. However, these systems are not feasible in the clinical situation.
In the clinic, pressure mapping systems are the primary means of quantifying pressure. These systems quantify pressure at the buttock/seat interface, allowing a comparison among various cushions. In measuring sitting pressure, it can also be determined whether the individual has any evidence of asymmetry in sitting and what influence changing the configuration of the seating system has on correcting the asymmetry. Many commercial pressure measurement systems are available for commercial and research use. These technologies are constantly improving, but issues remain with consistency of the measurement and lack of agreement around best practices for pressure measurement protocol. The three most common pressure mapping systems are the Force Sensing Array (Vista Medical;www.pressuremapping.com), F-Scan (Tekscan) (www.tekscan.com), and Xsensor (Xsensor Technology Corporation, www.xsensor.com). Each of these systems uses a flexible matrix of pressure sensors that provide a map of the distribution of pressure at the interface between the seat cushion or back and the client’s body. These sensors are arranged in a grid pattern on the pressure mat. The number of sensors and their sensitivity varies across the different systems and should be taken into consideration when considering the purchase of a system. They vary in the technology used to measure pressure. These technologies include capacitance sensors that measure the ability to store an electrical charge, piezo-resistive sensors that measure the change in resistance when force is applied, and electrically conductive sensors that measure the change in current flow. Two properties influence the reliability of the pressure measurements: creep and hysteresis. Creep refers to the stability of the pressure reading over time. Hysteresis refers to the change in pressure reading as the device is loaded and unloaded (e.g., as the client sits on the cushion). Each of these systems corrects for these two variables in their software, but these properties still influence the reliability of the measurement systems to varying degrees, which needs to be taken into consideration when these systems are used clinically.
The output from each of these systems is generally similar, although care must be taken when the results of research or measurements obtained by use of the different systems are compared. As will be seen below, these systems differ in their performance. All the systems provide a visual output (Figure 6-17) that allows a quick inspection of the pressure distribution. The visual output may show pressure distribution with a color display or as peaks and depressions. The actual pressure value for each cell can be displayed as well. Data are captured continuously at varying sampling rates. The system will provide data on peak and mean pressure, number of sensors activated, minimum and maximum pressure, and the location of the center of pressure. Some systems have the capacity for a split screen that displays the pressure map on one side and a video recording on the other. Another useful feature is the ability to define a particular area of the pressure map for which the system will generate pressure statistics. The breadth of information that these systems provide is both useful and a distraction. Although data showing peak and mean pressure seem easy to interpret, there is little consensus on what is desired pressure at the seat/buttock interface. Different ways of interpreting these data will be discussed below in the discussion of a pressure mapping protocol.
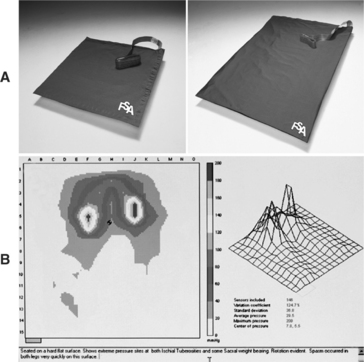
Figure 6-17 Pressure measurement system. A, Map with an array of sensors. B, Sample display of an individual’s pressure distribution profile (Courtesy Vista Medical, www.pressuremapping.com.)
Ferguson-Pell and Cardi (1993) completed an evaluation of three computer-based pressure mapping systems. Although this work evaluated technology that is dated, it continues to influence thinking about pressure measurement systems as it applies a systematic protocol, involves both consumers and users, and identifies key parameters that must be considered in both the selection of a pressure mapping system and interpretation of the resulting data. The three systems that were evaluated included: the Force Sensing Array (Vista Medical), with a 15 × 15–cell array of force-sensing resistors, the Talley Pressure Monitor (TPM, Progressive Medical), consisting of an array of bladder-type sensors, and the Tekscan Seat (Tekscan Inc.), with an array of 2056 force sensors. With these systems, Ferguson-Pell and Cardi (1993) carried out “bench tests” to determine the properties of the sensors under controlled loads. The measurement variables of interest were accuracy, linearity and reproducibility, hysteresis, and stability (Ferguson-Pell and Cardi, 1993). In other words, they measured the relationship between the pressure measured by each system and a known applied pressure, creep, and hysteresis. These were examined with planar and contour loads under laboratory conditions and across four different pressure relieving cushions, with five wheelchair users as subjects. The four cushions used to evaluate the performance of each of the pressure mapping systems included (1) foam, (2) gel, (3) hybrid (Jay), and (4) air filled (ROHO). The actual results of this work are less critical today because of the changes that have occurred in both measurement systems and cushion technology. However, this study remains an important one because of its use of a systematic research protocol and identification of critical factors that influence the reliability of pressure mapping systems.
A recent study involved a similar comparison of more current pressure mapping technologies (Hadcock et al., 2002). Incremental loading, low threshold, and stability (creep) of the F-scan FSA and Xsensor systems were evaluated under static and dynamic conditions by using planar and curved surfaces. The curved surface was cylindrical; quite different from a contoured seating surface, so the results of this aspect of the study must be interpreted with caution for the purposes of seating intervention. This study involved bench testing and did not include measurement with any wheelchair users. The results on a flat surface indicated that the FSA system was the most accurate, followed by the Xsensor and the F-scan. Creep was similar for the Xsensor and F-scan (17.62% and 17.23%, respectively) systems, and both were better than the FSA system (19.54%) (Hadcock et al., 2003). The Xsensor was better at detecting pressures under light loading conditions.
The studies by Ferguson-Pell and Cardi (1993) and Hadcock et al. (2003) provide some evidence for the difference in performance across pressure mapping systems. In addition to the performance characteristics evaluated in these studies, the selection of a system will depend on familiarity with the technology, the specific purpose (e.g., clinical evaluation versus research), and the functionality of the systems as they meet the needs of the user.
A second major issue with respect to pressure mapping is the identification of an accepted protocol for clinical use. There is no compelling evidence in the literature to suggest a particular number above which a pressure ulcer will certainly develop. Consequently, pressure mapping in the clinical situation is used to make comparisons among various cushions so that the clinician can rank the cushions for their ability to distribute pressure as measured by the pressure mapping systems. Swaine (2003) has developed a protocol for both obtaining and interpreting pressure measurements that is becoming more prevalent internationally. Swaine describes a consistent setup of the equipment and cushions to be evaluated, an initial check of the equipment, length of recording time, palpation of bony prominences, and documentation. She also suggests that interpretation of the results is based on peak pressure, the area of the client’s buttocks that are in contact with the pressure mat, and any asymmetries of pressure distribution.
Swaine’s work provides a useful basis for clinicians using pressure mapping to determine the optimal cushion for their clients’ needs. Caution is still advised because questions remain about a protocol and the interpretation of the data. For example, Swaine (2003) suggests that peak pressure is determined by taking the average of the four highest sensor cells around a bony prominence, whereas Dunk and Callaghan (2005) take the average of all sensors within 10% of the cell, measuring the highest peak pressure. Swaine recommends that clients sit on a cushion for 8 to 10 minutes, whereas Stinson, Porter, and Eakin (2002) suggest that 6 minutes is sufficient. Pressure gradient rather than absolute pressure has been suggested as a better indicator of risk for development of a pressure ulcer, but there is no consensus on what constitutes an acceptable gradient. These concerns suggest that, although pressure mapping remains a very useful tool its augment clinical judgment, it does not replace it.
Behavioral strategies to reduce the risk of development of pressure ulcers were identified earlier. Two main technologies exist to manage pressure for persons who use wheelchairs: pressure relief cushions and tilt and recline components on wheelchairs. The latter will be discussed in Chapter 12. Numerous studies have measured characteristics and properties of a variety of pressure relief cushions. The majority of investigations have used tissue interface pressure as the basis for comparing these products. Some studies have also compared changes in transcutaneous oxygen tension and capillary blood flow. Although it has been shown that seating technologies play a significant role in pressure ulcer prevention by reducing the mechanical load on the tissue, there is no evidence that one type of pressure-reducing device works better than all others under all circumstances (Brienza et al, 2001; Conine et al, 1994; DeLateur et al, 1976; Ferguson-Pell et al, 1986; Garber, Krouskop, and Carter, 1978).
PRINCIPLES OF SEATING FOR COMFORT
This section considers seating and technologies that address that comfort. There are three distinct populations who can benefit from seating technologies for comfort: (1) wheelchair users who have sitting discomfort and pain (e.g., individuals with postpolio syndrome, amyotrophic lateral sclerosis, and multiple sclerosis), (2) the elderly, and (3) individuals with low back pain, which can keep them from effectively performing their jobs. For individuals in any one of these populations, discomfort in seating can lead to a decreased ability to participate in activities of daily living. In cases of severe discomfort, the individual may be restricted to bed rest for some or all of the day, which further reduces the individual’s ability to function and can lead to medical problems as well. There are unique technologies for each of these populations, but the commonality is that they enhance comfort in the seated position.
In comparison to the other two categories of need, the technologies available to meet the comfort seating needs of individuals fall far short. There are a number of reasons for this. One is that equipment that is deemed necessary for comfort typically is not paid for by third-party funding sources because it is not considered a medical necessity. Another reason is that there is very little agreement among researchers on how to define and assess comfort and discomfort (Hobson and Crane, 2001). Although much research has been done to assess comfort, it is a difficult variable to objectively measure because it can be highly subjective and involve multiple factors. A cushion that is described as comfortable by one individual may feel uncomfortable to another. Researchers have also been unsuccessful in tying discomfort to quantitative measures such as posture, muscle fatigue as indicated by electromyographical measurements, or seat interface pressure (Hobson and Crane, 2001). The lack of outcomes relating to the effectiveness of seating products said to promote comfort makes it necessary for clinicians to use a trial-and-error approach to recommending equipment for the consumer. This can be costly and is often not funded by third-party sources. In turn, without funding at the clinical level for such products, there is no financial incentive for manufacturers to address this unmet need. It is necessary that those involved in this industry determine the best way to assess the many factors of discomfort and comfort. Only then can the efficacy of the current technologies for this population be carefully evaluated and new technologies be developed.
TECHNOLOGIES FOR SEATING AND POSITIONING MANAGEMENT
There is considerable overlap between the technologies used to address goals related to postural control, tissue integrity, and comfort. Further, many clients require seating that addresses two or more of these goals. Seating technologies in general will be discussed, with identification of their specific application to these goals where appropriate. This section is divided into two components: the design and the construction of the seating system and the properties of the materials used to construct it. The evaluation process described at the beginning of this chapter guides the selection of the most appropriate system. The client should be allowed a trial period of use of the system because comfort and functional issues will become evident with use of the system over time.
Design and Construction of Seating Systems
The design of the seating system refers to the degree of contouring present in the seat and back and the degree of adjustability that is present in the components. These technologies range from systems that are relatively flat, without any contouring to match the shape of the body segments they support, to custom-contoured systems that are constructed to match as closely as possible the body contours of the user. Prefabricated technologies are available so that the ATP no longer needs to construct the components in the seating system.
Planar.
Planar technologies are flat surfaces that support the body only where it easily comes in contact with the body, such as at bony prominences. In general, they are appropriate for individuals who require minimal support. Other positioning components can be added to this basic structure if additional support is required. Planar foam cushions, as shown in Figure 6-18, are designed from flat blocks of foam, which can be highly adaptable. These blocks can be fabricated with one layer of a selected thickness (up to 4 inches) and selected density of foam, or they can be fabricated from multiple densities and varying thicknesses of foam (Hobson, 1990). In the latter case, for example, a piece of a stiff foam that is 1 to 2 inches thick might be used on the bottom to provide a stable base and a ¾- to 1-inch-thick piece of soft foam could be placed on top for pressure relief. Planar foams can also be adapted by cutting out (e.g., under the ischial tuberosities) or building up areas as necessary for pressure distribution or postural management.
Prefabricated.
Prefabricated planar components are made in standard sizes to fit a wide range of individuals. The back and seat surfaces are generally plywood or molded plastic pieces to which foam has been attached. Lateral supports and an abductor for pelvic and hip support can be attached with hardware to the basic seat, and lateral supports for trunk stability can be attached to the back section (Figure 6-19) (Adaptive Engineering Lab, Inc., www.aelseating.com). The seat and back are attached to the wheelchair frame with interfacing hardware once the upholstery has been removed. Much of the hardware that interfaces the various components can be adjusted for angle, width, and depth. The advantage of having adjustable components is that they allow the system to be modified for growth or postural changes.

Figure 6-19 Planar seating system with positioning components. (Courtesy Adaptive Engineering Lab, Inc., www.aelseating.com.)
Custom Fabricated.
Custom-fabricated planar systems are made of similar materials and design as prefabricated systems, but the dimensions of the seating surface and components are customized to fit the individual. These systems can be fabricated on site directly with the consumer, or specifications of the consumer’s measurements can be sent to a manufacturer for fabrication. The density of the foam pieces can also be selected to accommodate the needs of the individual. Lateral supports, headrests, and other components are added to the basic foam and plywood (or plastic) structure. This approach can be highly labor intensive and is being replaced at many facilities as a result of the advent of a large array of off-the-shelf technologies.
Standard Contoured Modules
Contoured technologies are useful for individuals with moderate seating and positioning needs for postural management or who are at low risk for pressure ulcer development. These technologies use curved surfaces that more closely match the shape of the human body. The amount of contact that the body has with the seating surface is increased by contouring the seating surface to the person’s body, providing increased support and control. Further, a generic contoured cushion will distribute pressure across the seating surface and will fit people within a certain size range. This approach is also generally less costly than a custom-contoured cushion. The Matrix is one example of a standard contoured cushion (Figure 6-20) (Invacare, www.invacare.ca).
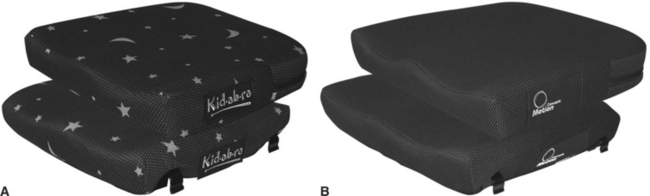
Figure 6-20 Matrix cushion. A, Child’s version. B, Adult version. (Courtesy Invacare Corp., www.invacare.ca.)
Custom Contoured
The cushion that provides the greatest amount of body contact and therefore the most support is one that has been shaped, or custom contoured, to the individual’s body. A number of technologies are available to achieve a custom-contoured system. One example is shown in Figure 6-21. These types of systems differ primarily in terms of the fabrication techniques used and whether the fabrication is completed on site or in a central location. The disadvantages of custom-contoured support surfaces include the following: transfers to and from the system are more difficult; the system is static and has no dynamic properties, thus limiting the individual to one fixed position; and there is limited ability within the system to allow for growth of the individual.

Figure 6-21 Custom-contoured seating system. (Courtesy Invacare Corp., www.invacare.com.)
Foam in place systems allows the ATP to fabricate a custom-contoured cushion on site. The client is placed in a frame that has a flexible covering over one side. This covering is matched to the shape of the person, and he or she is positioned in the most desirable seated posture. The foam materials are then added to the frame and allowed to expand to contour to the person’s shape. The person is removed from the frame, and the foam is allowed to harden for several hours. Once the foam hardens, the flexible covering is removed. Further shaping of the foam can be completed by hand at this time. The foam is encased in a fabric cover. The foam can then be attached to a solid backing (usually plywood or plastic) and mounted to the wheeled base. This approach can be used on site, and a cushion can be completed in about 12 hours.
A vacuum consolidation process seats the client on a latex bag filled with beads (Lemaire et al, 1996). This bag is placed on top of a wheelchair or fitting chair. The ATP assists the client to achieve an optimal position to support goals of function, pressure relief, or comfort. The latex bag is then manipulated to conform to this position and the vacuum is used to draw the air out of the bag, consolidating the enclosed beads. At this stage, the cushion can be fabricated either on site by a foaming procedure or sent to a central manufacturer for remote fabrication.
Seating simulators use technology that allows the ATP to map the client’s body contours, which are then digitized. Computer-aided manufacturing technology is then used to fabricate the cushion or back. The process of determining the optimal cushion or back shape is similar to that described for vacuum consolidation. A simulator chair is used that allows multiple adjustments to manipulate seat depth, seat to back angle, and other common wheelchair configurations. An initial baseline reading is taken without the client seated in the simulator. Once the client is comfortably positioned in the chair, mechanical plungers are positioned to simulate the optimal seated position of the client. This information, along with the baseline reading, is transferred to a pressure-sensitive data recording sheet. This sheet is then sent to a central fabrication facility, along with other recommendations related to foam density, special construction related to pressure relief (e.g., use of different foams), and required accessories such as laterals and strapping systems. The Shape Sensor system by Invacare (www.invacare.com) is an example of this technology.
Prefabricated adjustable Backs
Prefabricated adjustable backs have become available in recent years. These products provide a large degree of adjustability that can be accomplished in the clinical setting. The Infinity Back is an example of an adjustable back. The ATP can make adjustments on the basis of an optimal seated position determined by a mat assessment. These backs allow the clinician to adjust height, depth, width, back angle, and placement of the laterals. Some of these systems allow the ATP to create a biplanar back in which the upper and lower segments of the back are set at different angles. This configuration is often used to provide specific postural control. Although the pivot point can be placed at any spinal level, when placed at the level of the posterior superior iliac spine, it can assist with control of the pelvis. Studies have investigated the effect of pelvic stability on function (Miller Polgar et al, 2000; Rigby et al, 2001;), but there have been no clinical studies that have evaluated the effect of this particular back configuration on postural control and subsequently function.
PROPERTIES OF MATERIALS USED TO CONSTRUCT SEATING SYSTEMS
An understanding of the properties of the materials used in seating technologies will assist in the selection of appropriate cushions. Sprigle (1992) identifies and describes five properties of cushion materials: (1) density, (2) stiffness, (3) resilience, (4) dampening, and (5) envelopment.
Density of a material is the ratio of its weight to its volume. A greater density generally means a more durable material, but not always. Low-density materials will fatigue faster than high-density ones under the same loading conditions. Stiffness of a material describes how much it gives under load. In a cushion, this is the distance that the person sinks into the cushion. Soft materials may bottom out, but failure to compress can also lead to an increase in seating pressures and tissue breakdown. The International Standards Organization standards also describe lateral and forward stiffness that describes the response of the cushion to a lateral force. It is easier to slide on a cushion with low stiffness, but the shearing forces are higher, resulting in a cushion with less stability. Sliding resistance is a cushion property related to friction. A cushion with high resistance limits how much the user slides, helping to support upright posture, but consequently makes transfers more difficult.
Resilience is the ability of a material to recover its shape after a load is removed or to adjust to a load as it is applied. Short-term resilience is the immediate recovery when a load is altered, such as when someone shifts weight on a seat cushion. Long-term resilience is the overnight recovery of a cushion that has been loaded and then unloaded. Dampening is the ability of the cushion to soften on impact; it is best observed by dropping a relatively heavy object on the material. If the object sinks into the material, then dampening is occurring. If it bounces off, or if the material does not react to the object, then the material is poorly dampened. This is the “shock absorber” feature of cushion materials and is important in minimizing the transmission of forces from the ground to the individual as they travel over rough surfaces or obstacles. Envelopment is the degree to which the person sinks into the cushion and the degree to which the cushion surrounds the buttocks. Good envelopment promotes stability and helps reduce peak pressures. Recovery refers to the degree to which a cushion returns to its preloaded state when a load is removed.
Classification of Cushion Technologies
Sprigle, Press, and Davis (2001) describe uniform terminology for classification of the material used to construct wheelchair cushions. They described the following categories of cushions: (1) made from cellular materials, (2) containing fluid, and (3) other constructions.
Cushions Made From Cellular Materials.
This category includes cushions made from “foam,” “flexible matrix,” “viscoelastic foam or matrix,” and “nondeforming foam or matrix” (Sprigle, Press, and Davis, 2001, pp. 451-2). Over the years, foams have been the material most commonly used in the fabrication of cushions. Polyurethane or latex foams come in a variety of thicknesses and densities and are often characterized by their cell structures. There are two commonly used cell structures for foams: open cell and closed cell. Open-cell foams have interconnected, perforated membranes that permit airflow between the cells and result in better ventilation (Tang, 1991). This type of foam is often less dense because of the air captured in the open cells. Open-cell foams absorb fluids, which makes them difficult to clean. Closed-cell foams are composed of individual structures encased in a membrane. These foams are generally less compliant than open-cell foams, and airflow is restricted. Examples of these foams include polyurethane and latex (open cell) and ethafoam (closed cell).
Foam cushions are typically lightweight and inexpensive. Foams compress with the application of weight, which results in good envelopment. The amount of compression depends on the stiffness of the foam. Although soft foam will compress and allow the person to sink in more, a foam that is too soft might bottom out. Because foams have a tendency to trap heat near the body, their thermal features are considered to be poor. In general, the short- and long-term resilience of foam is good, but again this varies depending on the structure and density of the foam. The two main disadvantages of using foam are that it (1) is prone to deterioration from light and moisture and (2) has a tendency to loose its resilience over time. Replacement of the foam depends on the type of foam and how much time the user spends sitting on the cushion.
Viscoelastic Foam or Matrix.
Viscoelastic foams were originally developed by the National Aeronautics and Space Administration for space travel. These foams, because of their high viscosities, tend to resist deformation if pressed quickly, but they will accommodate slowly to a constant load. They also have memory, which delays their return to the original shape. This time-dependent property is the most distinguishing feature of this type of foam (Sprigle, Press, and Davis, 2001). Viscoelastic foam also has good thermal properties and good envelopment. The resilience and dampening properties are variable depending on the density and other properties (Sprigle, 1992). Sunmate (www.sunmatecushions.com), T-foam, and Tempur-Med (www.tempurcanada.com) are examples of this type of foam (Figure 6-22).
Figure 6-22 Examples of Viscoelastic foam. Sunmate foam. (Courtesy Sunmate, www.sunmatecushions.com.)
Flexible Matrix.
Honeycomb cushion material is made from an array of thermoplastic elastomers. The material consists of layers of interconnected open cells that flex when pressure is applied. The flexibility of the cells results in a cushion that conforms to the user’s body shape, providing pressure relief. These cushions have good resiliency. The open cells allow air to flow through, which keeps the cushion cooler and prevents moisture. Cushions that use flexible matrix technology have both planar and contoured versions. Stimulite by Supracor (www.supracor.com) (Figure 6-23) is an example of a cushion with a flexible matrix technology.
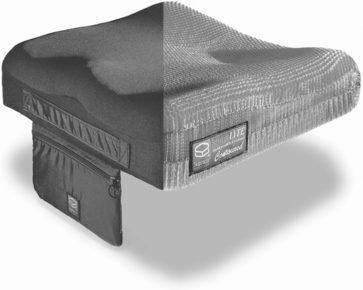
Figure 6-23 Flexible matrix technology, Stimulite cushion. (Courtesy Supracor Inc., www.supracor.com.)
Cushions Containing Fluid
Air Filled.: Air-filled cushions consist of a sealed receptacle that holds air. The cushion may be configured to allow the air to circulate within the whole receptacle, or it may be divided into compartments to better control the air flow. Air-filled cushions distribute pressure from high-pressure areas, such as the ischial tuberosities, to areas where there is less pressure. These cushions have good long-term and short-term resilience. The pressure-relieving properties of this type of cushion are typically good; however, the ability of this cushion to envelop the user and thus its effectiveness are dependent on the amount of inflation. An air-filled cushion that is overinflated will not envelop the buttocks and will result in increased pressure at bony prominences and reduced sitting stability. Underinflation of the cushion can result in the air being pushed away from the high-pressure areas, allowing them to “bottom out” against the hard sitting surface of the seat. Persons who lack sensation may not be able to feel whether the cushion is underinflated.
Commonly used air-filled cushions are the ROHO and Bye Bye Decubiti. The ROHO cushion (Crown Therapeutics, www.crownthera.com) consists of a number of rubber-balloon cells that are interconnected at the base to allow for airflow among cells (Figure 6-24). It is available in a number of configurations, including a high and low profile (4- and 2-inch cells, respectively) and various inflation configurations. The multiple compartments allow the air to be regulated in each compartment separate of the other compartments. Air-filled cushions are generally lightweight, and the materials they are made of do not deteriorate over time. A main disadvantage to these cushions is that they must be properly inflated, with consistent monitoring of the inflation to provide maximal benefits. Puncture and tears also occur, which influence their function. However, there is some evidence to support the superior pressure-relieving properties of an air-filled cushion over other pressure relief (Koo, Mak, and Lee, 1996; Shechtman et al, 2001).
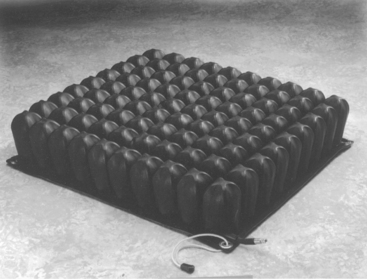
Viscoelastic Fluid.: A viscoelastic fluid is relatively stiff, yielding to small forces (Sprigle, Press, and Davis, 2001). The elastic component refers to the fluid’s ability to store energy (Sprigle, Press, and Davis, 2001). The viscous property refers to the degree to which fluid molecules move across each other. A highly viscous fluid will not flow easily because the molecules do not easily slide across each other. A low-viscosity fluid or nonviscous fluid (such as water) will flow easily (Figure 6-25). High viscosity means that envelopment is poor and short- and long-term resilience is poor. These cushions have good dampening and thermal properties (they conduct heat away from the body) and provide a more stable base than does an air cushion. However, they are affected by temperature and will freeze in cold weather. In addition, some gels that are encased in a large bladder can shift, allowing the user to sit on the hard support surface. Cushions with this construction must be kneaded to ensure that the distribution of the gel is uniform to prevent contact with the support surface.

Alternating Pressure Cushions.
Research (Kosiak, 1959; Reswick and Rogers, 1976) has documented a relationship between the amount of pressure applied and its duration and the development of pressure ulcers. In a study described earlier, it was found that the alternating pressure cushion was the only seating surface to intermittently bring pressures within the range of capillary blood pressure (Kosiak et al, 1958). All the cushions described thus far are static cushions, which have been designed on the premise that (1) they redistribute pressure over the sitting surface and (2) the individuals using them also need to follow through with pressure relief activities. Alternating pressure devices are designed on the basis that weight-bearing surfaces can tolerate high pressures for a time if alternated with increments of no pressure.
The principle of intermittent pressure relief is implemented in commercially available cushions by use of an oscillating pump to alternately inflate bellows arranged in rows (Hobson, 1990). Each individual elastomeric bellow (typical cushions have arrays of 48 arranged in eight rows of six) can be inflated individually or in groups. Generally, rows are inflated together. One approach couples every third row of the array of bellows. During operation, two of the coupled rows are inflated and one is deflated, which relieves pressure over one third of the seating surface; then the next third of the array is deflated, and so on. An alternative approach automatically cycles only the back four rows (out of eight total) under the ischial tuberosities. Each row is sequentially inflated and deflated to provide intermittent pressure relief to local tissue. These cushion systems use a recycling air pump powered by a battery to inflate the bellows. If the pressure pump should fail to operate in these systems (e.g., the battery becomes discharged), the cushion can still be used as an air-filled cushion. Because of the added weight, the need for recharging of the battery, and the cost, these seating devices have not been as widely distributed as other cushion types.
Hybrid Cushions.
Hybrid cushions consist of a combination of the materials described above. The most typical combination is a closed-cell foam base with a membrane that contains gel, viscous fluid, or air that is placed on top or inserted in a cutout. This method provides a combination of good envelopment, good thermal properties, pressure relief (because of the flotation materials), and good support and dynamic properties, which are provided by the foam base (Sprigle, 1992). The series of Jay cushions are commonly used hybrid cushions that consist of a combination of a standard-contoured, high-density foam base with a gel-filled pad that sits atop the foam base. The pad can be purchased in different configurations, such as an overfilled pad or pads with the gel sectioned off into quadrants, which prevents the pooling of gel into certain areas. The Cloud cushion from Ottobock (www.ottobock.com) (Figure 6-26) is an example of a hybrid cushion that has a foam and air-holding membrane that sits on top of a standard-contoured foam base. The overall properties of these types of cushions depend on the type of container and on the properties of the foam base.
Figure 6-26 Example of a hybrid cushion. (Courtesy Otto Bock, www.ottobock.com.)
Cushion Covers
Selection of a cover for a seat or back cushion can be as important as the determination of the material used to make the cushion because an improper cover can negate some of the benefits of that material. The cover selected should conform integrally to the cushion’s contours, particularly in nonplanar systems. It should not interfere with the envelopment properties of the cushion nor add to shearing and friction. A cover that is too tight will prevent the client from sinking into the contours of the cushion. One that is too large will wrinkle, creating additional pressure points.
The ATP should know how the fabric handles moisture, either as a result of incontinence or perspiration. Most cushions will be used in hot, humid conditions for at least part of the year, so perspiration is an issue even when incontinence is not a concern. Many technical fabrics, blending Lycra and polyester, wick moisture away from the body, which is an important consideration when prevention of pressure ulcers is a goal. The cushion cover should be easy to remove and clean.
SEATING FOR PRESSURE DISTRIBUTION AND POSTURAL SUPPORT
Individuals who are at risk for development of pressure ulcers can benefit from proper positioning in the wheelchair as well. In fact, it is recommended that positioning be addressed first because postural alignment often results in changes in pressure distribution (Minkel, 1990). Through postural alignment, pressure can be distributed more evenly; postural deformities, such as pelvic obliquity, scoliosis, and kyphosis, can be prevented; back pain can be alleviated; and stability can be increased. These changes will influence the individual’s mobility, energy expenditure, and function.
Many of the principles described regarding sitting posture and postural control apply to individuals at risk for pressure ulcer development as well. Some of the technologies for postural control are beneficial for persons with spinal cord injuries, and new technologies that specifically address the needs of this population have been developed. Some basic strategies for positioning for postural management for this population are described.
A cushion, without a firm base, placed in the seat will not totally eliminate the hammocking effect, and eventually the sling seat stretches further and the cushion conforms more to the sling. Simply installing a solid seat can minimize the hammocking effect of the sling upholstery. Solid seats can be made from a  -inch sheet of plywood, or plastic seats can be purchased from many cushion manufacturers. Any of the cushions described earlier can then be placed on the solid seat. The upholstery back of the wheelchair does not provide lumbar support and promotes a sacral sitting position with kyphosis of the spine. The upholstery back can be replaced with a solid, contoured back that is commercially available (e.g., Varilite Evolution Back or J2 Back) (Figure 6-27 shows an example of a commercially available back) or custom made of foam. The seat back should be assessed for appropriate height and seat-to-back angle. It is recommended that the back be reclined approximately 15 degrees to help stabilize the trunk and prevent forward loss of balance. The back height is determined by the amount of support needed by the individual. Many persons with paraplegia have adequate trunk strength and wish to preserve mobility (particularly for sports), so they prefer lower backs on their wheelchairs and prefer not to use trunk-positioning components. Persons with C4, C5 quadriplegia, with less trunk control, can benefit from a higher seat back that supports all or part of the scapulae, and those with C1 to C3 spared will require headrests.
-inch sheet of plywood, or plastic seats can be purchased from many cushion manufacturers. Any of the cushions described earlier can then be placed on the solid seat. The upholstery back of the wheelchair does not provide lumbar support and promotes a sacral sitting position with kyphosis of the spine. The upholstery back can be replaced with a solid, contoured back that is commercially available (e.g., Varilite Evolution Back or J2 Back) (Figure 6-27 shows an example of a commercially available back) or custom made of foam. The seat back should be assessed for appropriate height and seat-to-back angle. It is recommended that the back be reclined approximately 15 degrees to help stabilize the trunk and prevent forward loss of balance. The back height is determined by the amount of support needed by the individual. Many persons with paraplegia have adequate trunk strength and wish to preserve mobility (particularly for sports), so they prefer lower backs on their wheelchairs and prefer not to use trunk-positioning components. Persons with C4, C5 quadriplegia, with less trunk control, can benefit from a higher seat back that supports all or part of the scapulae, and those with C1 to C3 spared will require headrests.

Technologies to Enhance Sitting Comfort for Wheelchair Users
In a study that assessed the satisfaction of wheelchair users, comfort was rated as the most important variable for a wheelchair seating aid (Weiss-Lambrou et al, 1999). At the same time, comfort was rated as the least satisfying variable among these wheelchair users. The reasons stated for dissatisfaction related to comfort included seat cushions that caused pain and discomfort, fatigue, uncomfortable headrests and thoracic supports, sliding in wheelchair seat caused by discomfort, and poor posture as a result of unsuitable installation. Comfort is also related to the contact surface between the seating system and the person. For example, materials that provide good air exchange, maintain an even temperature, and control moisture are more likely to provide a comfortable sitting climate.
Wheelchair users who have discomfort and chronic pain need seating systems that allow them to relieve the discomfort and participate fully in activities of daily living. These needs are best addressed after a thorough mat assessment that identifies the user’s most comfortable seated position and the combination of technologies identified above that best addresses comfort needs. (Mobility technologies that provide users with the ability to adjust their positions in the wheelchair will be discussed in Chapter 12).
Technologies That Increase Ease of Sitting for the Elderly
People are living longer, which means that the number of well elderly and those in need of supervised care is growing considerably. As an individual ages, mobility may be reduced as a result of acute illnesses or trauma, such as stroke, hip fracture, or progressive conditions such as arthritis. Consequently, it is likely that the amount of time the individual spends sitting increases. The goal of seating in this category depends on the individual’s needs and skills, as it does for the other categories. Just as there is a range of needs for the elderly population, there is also a range of seating technologies. Seating technologies for the aging population can be matched to the level of functional mobility the individual has: (1) ambulatory (2) mobile, nonambulatory, and (3) dependent mobile (Fernie and Letts, 1991). Chairs are needed that promote comfort, safety, ease of ingress and egress, and propulsion if necessary.
SUMMARY
This chapter has shown the potential outcomes that can be achieved through seating in three primary areas of need: postural control, tissue integrity, and comfort. Procedures for evaluation and matching of device characteristics to the individual’s needs were presented. Basic principles of biomechanics frequently used in seating and positioning were discussed. Different types of seating technologies and cushion classifications were described, along with their application to the three primary goals of seating.
1. Describe the three primary goals of seating intervention. What are the key elements of a mat assessment? Describe each of these.
2. Describe three additional factors that the ATP should consider when designing a seating system.
3. Describe the influence of the physical, sociocultural, and institutional contexts on design of a seating system.
4. What are the three types of force? Why are they relevant to seating and positioning?
5. What is meant by the center of pressure, and how does it relate to seating and positioning systems?
6. Describe the basic premises underlying seating intervention for postural control.
7. Why is the pelvis the starting point when seating for postural control? Describe the major approaches used to obtain alignment and control of the pelvis.
8. Describe the three spinal deformities that may occur.
9. List three methods used to support the trunk in postural control seating systems, and describe when each method is indicated.
10. Describe how the head can be positioned posteriorly, anteriorly, and laterally. What factors lead to the use of each of these?
11. What is the major cause of pressure ulcer development? What are other factors that contribute to the development of pressure ulcers?
12. Define hysteresis and creep. Describe how each of these affects the reliability of pressure map measurements.
13. Describe Swaine’s pressure mapping protocol. Describe the output of pressure mapping systems. Discuss two controversial aspects of pressure measurement.
14. What is a honeycomb cushion? What advantages does it have over other approaches?
15. How do viscoelastic fluid-filled and foam cushions differ? List an advantage and disadvantage of each.
16. What are the primary populations for whom comfort is the major goal in developing a seating system?
17. Identify the reasons why there are limited technologies available for populations for whom comfort is the major goal.
References
Bennett, L, et al. Shear vs pressure as causative factors in skin blood flow occlusion. Arch Phys Med Rehabil. 1979;60:309–314.
Berecek, KH. Etiology of decubitus ulcers. In: Horsley JA, ed. Preventing decubitus ulcers. New York: Grune & Stratton, 1981.
Bergen, AF, Presperin, J, Tallman, T. Positioning for function: wheelchairs and other assistive technologies. Valhalla, NY: Valhalla Rehabilitation Publications, 1990.
Bergen, AF, Presperin, J, Tallman, T. Planning intervention. Team Rehabil Rep. 1992;3:38–41.
Bergstrom, N, et al. The Braden Scale for Predicting Pressure Sore Risk. Nurs Res. 1987;36:205–210.
Bertenthal, B, Von Hofsten, C. Eye, head and trunk control: the foundation of manual development. Neurosci Biobehav Rev. 1998;22:515–520.
Bouten, CV, et al. The etiology of pressure ulcers: skin deep or muscle bound? Arch Phys Med Rehabil. 2003;84:616–619.
Breslow, R. Nutritional status and dietary intake of patients with pressure ulcers: review of the research literature 1943 to 1989. Decubitus. 1991;4:16–21.
Brienza, D, et al. A randomized control trial to evaluate pressure-reducing seat cushions for elderly wheelchair users. Adv Skin and Wound Care. 2001;14:120–129.
Cailliet, R. Scoliosis: Diagnosis and management. Philadelphia: FA Davis, 1975.
Chen, Y, DeVivo, MJ, Jackson, AB. Pressure ulcer prevalence in people with spinal cord injury: Age-period-duration effects. Arch Phys Med Rehabil. 2005;86:1208–1213.
Conine, T, et al. Pressure ulcer prophylaxis in elderly patients using polyurethane foam or Jay wheelchair cushions. Int J Rehabil Res. 1994;17:123–137.
Constantian, MB. Etiology: Gross effects of pressure. In: Constantian MB, ed. Pressure ulcers: principles and techniques of management. Boston: Little, Brown, 1980.
DeLateur, BJ, et al. Wheelchair cushions designed to prevent pressure sores: an evaluation. Arch Phys Med Rehabil. 1976;57:129–135.
Dinsdale, SM. Decubitus ulcers: role of pressure and friction in causation. Arch Phys Med Rehabil. 1974;55:147–152.
Dunk, N, Callaghan, J. Gender-based differences in postural responses to seated exposures. Clin Biomech. 2005;20:1101–1110.
Ferguson-Pell, M, Cardi, M. Prototype development and comparative evaluation of wheelchair pressure mapping system. Assist Tech. 1993;5:78–91.
Ferguson-Pell, MW, et al. A knowledge-based program for pressure sore prevention. Ann N Y Acad Sci. 1986;463:284–286.
Fernie, G, Letts, RM. Seating the elderly. In: Letts RM, ed. Principles of seating the disabled. Boca Raton, FL: CRC Press, 1991.
Fisher, SV, et al. Wheelchair cushion effect on skin temperature. Arch Phys Med Rehabil. 1978;59:68–72.
Garber, SL, Krouskop, TA, Carter, RE. A system for clinically evaluating wheelchair pressure-relief cushions. Am J Occup Ther. 1978;32:565–570.
Geyer, MJ, et al. Wheelchair seating: a state of the science report. Assist Tech. 2003;15:120–128.
Hadcock L et al: Pressure measurement applications for humans, Proceedings of Association of Canadian Ergonomists Conference, August 2003, London, Ontario.
Hadders-Algra, M, Brogren, E, Forssberg, H. Development of postural control—differences between ventral and dorsal muscles? Neurosci Biobehav Rev. 1998;22:501–506.
Hadders-Algra, M, et al. Development of postural adjustments during reaching in infants with CP. Dev Med Child Neurol. 1999;41:766–776.
Hobson DA: Contributions of posture and deformity to the body-seat interface variables of a person with spinal cord injury, Proceedings of the Fifth International Seating Symposium, pp. 153-171, February 1989, Memphis, Tenn.
Hobson, DA. Seating and mobility for the severely disabled. In: Smith RV, Leslie JH, eds. Rehabilitation engineering. Boca Raton, FL: CRC Press, 1990.
Hobson, DA, Crane, B. State of the science white paper on wheelchair seating comfort, February 2001. www.rerc.pitt.edu/RERC_PDF/Comfort.pdf. [Accessed March 16, 2005.].
Kangas, KM, Creating mobility within mobility systems. Rehab Manag 2000;13:58–60. 62, http://www.rehabpub.com/trehab/672000/3.asp. [Accessed October 11, 2006.].
Koo, TKK, Mak, AFT, Lee, YL. Posture effect on seating interface biomechanics: comparison between two seating cushions. Arch Phys Med Rehabil. 1996;77:40–47.
Kosiak, M. Etiology and pathology of ischemic ulcers. Arch Phys Med Rehabil. 1959;40:6262–6269.
Kosiak, M. Etiology of decubitus ulcers. Arch Phys Med Rehabil. 1961;42:19–29.
Kosiak, M, et al. Evaluation of pressure as a factor in the production of ischial ulcers. Arch Phys Med Rehabil. 1958;39:623–629.
Krause, JS, et al. An exploratory study of pressure ulcers after SCI: Relationship to protective behaviours and risk factors. Arch Phys Med Rehabil. 2001;82:107–113.
Krouskop, TA, et al. The effectiveness of preventive management in reducing the occurrence of pressure sores. J Rehabil Res Dev. 1983;20:74–83.
Lander-Ganz, E, Gefen, A. Mechanical compression-induced pressure sores in rat hindlimb: muscle stiffness, histology and compression models. J Appl Physiol. 2004;96:2034–2049.
Landis, EM. Micro-injection studies of capillary blood pressure in human skin. Heart. 1930;15:209–228.
Law, M, et al. Canadian Occupational Performance Measure, ed 3. Toronto: CAOT Publications ACE, 1997.
Lemaire, et al. Clinical analysis of a CAD/CAM system for custom seating: A comparison of hand-sculpting methods. J Rehabil Res Dev. 1996;33:311–320.
Letts RM, ed. Principles of seating the disabled. Boca Raton, Fla: CRC Press, 1991.
Low, J, Reed, D. Basic biomechanics explained. Oxford: Butterworth Heinemann, 1996.
Mayall, JK, Desharnais, G. Positioning in a wheelchair: a guide for professional caregivers of the disabled adult. Thorofare, NJ: SLACK, 1995.
McDonald, H. Preventing pressure ulcers. Rehab Manag. 2001;14:42–46. [40,].
Miller WC, Mortenson B, Garden J: The WhOM: a client specific outcome measure of wheelchair intervention, Proceedings of the Twenty-Second International Seating Symposium, p. 65-68, March 2006, Vancouver, British Columbia.
Miller Polgar J et al: Comparison of occupational performance between two methods of pelvic stabilization, Proceedings of the Tri-Joint Congress, June 2000, Toronto, Ontario.
Mills, T, et al. Development and consumer validation of the functional evaluation in a wheelchair (FEW) instrument. Dis Rehabil. 2002;24:38–46.
Minkel, JL. Seating SCI clients. In Proceedings of the Sixth Northeast RESNA Regional Conference. Washington, DC: RESNA; 1990.
National Pressure Ulcer Advisory Panel: Statement on pressure ulcer prevention, 1992: www.npuap.org/positn1.htm. Accessed October 10, 2006.
Norton, D, McLaren, R, Exton-Smith, AN. An investigation of geriatric nursing problems in hospital. London: Churchill Livingstone, 1975. [(Original work published in 1962.)].
Pape, TL-B, Kim, J, Weiner, B. The shaping of individual meanings assigned to AT: A review of personal factors. Disabil Rehabil. 2002;24:5–20.
Parkinson, MB, Chaffin, DB, Reed, MP. Center of pressure excursion capability in performance of seated lateral-reaching tasks. Clin Biomechan. 2006;21:26–32.
Patterson R et al: The physiological response to repeated surface pressure loads in the able bodied and spinal cord injured, Proceedings of the RESNA International 92 Conference, pp. 205-206, June 1992, Toronto, Ontario.
Pfeffer, J. The cause of pressure sores. In: Webster JG, ed. Prevention of pressure sores. Bristol, United Kingdom: IOP Publishing, 1991.
Reichel SM: Shearing force as a factor in decubitus ulcers in paraplegics, JAMA 762-763, February 15, 1958.
Reswick, JB, Rogers, JE. Experience at Rancho Los Amigos Hospital with devices and techniques to prevent pressure sores. In: Kenedi RM, Cowden JM, Scales JT, eds. Bedsore biomechanics. Baltimore: University Park Press, 1976.
Rigby, P, et al. Effects of a wheelchair-mounted rigid pelvic stabilizer on caregiver assistance for children. Assist Technol. 2001;13:2–11.
Savelsbergh, GJP, Van der Kamp, J. The effect of body orientation to gravity on early infant reaching. J Exp Child Psychol. 1994;8:510–528.
Shechtman, O, et al. Comparing wheelchair cushions for effectiveness of pressure relief: a pilot study. Occup Ther J Res. 2001;21:29–48.
Sprigle, S. The match game. Team Rehabil Rep. 1992;3:20–21.
Sprigle, S. Effects of forces and the selection of support surfaces. Top Geriatr Rehabil. 2000;16:47–62.
Sprigle, S, Press, L, Davis, K. Development of uniform terminology and procedures to describe wheelchair cushion characteristics. J Rehabil Res Dev. 2001;38:449–461.
Stekelenburg, CWJ, et al. Compression-induced deep tissue injury examined with magnetic resonance imaging and histology. J Appl Physiol. 2006;100:1946–1954.
Stewart, SFC, Palmieri, BS, Cochran, GVB. Wheelchair cushion effect on skin temperature, heat flux, and relative humidity. Arch Phys Med Rehabil. 1980;61:229–233.
Stinson, M, Porter, A, Eakin, P. Measuring interface pressure: a laboratory-based investigation into the effects of repositioning on sitting time. Am J Occup Ther. 2002;56:185–190.
Swaine, J. Seeing the difference, Rehab Manag:. www.rehabpub/features/112003/4.asp. [Accessed October 31, 2006.].
Tang, S. Seat cushions. In: Webster JG, ed. Prevention of pressure sores. Bristol, United Kingdom: IOP Publishing, 1991.
Torrance, C. Pressure sores: aetiology, treatment and prevention. London: Croom Helm, 1983.
Tredwell, S, Roxborough, L. Cerebral palsy seating. In: Letts RM, ed. Principles of seating the disabled. Boca Raton, FL: CRC Press, 1991.
Trefler, E, Hobson, DA, Taylor, SJ. Seating and mobility for persons with physical disabilities. Tucson: Therapy Skill Builders, 1993.
Weiss-Lambrou, R, et al. Wheelchair seating aids: how satisfied are consumers? Assist Technol. 1999;11:43–52.
Whimster, IW. The trophic effects of nerves on skin. In: Kenedi RM, Cowden JM, Scales JT, eds. Bedsore biomechanics. Baltimore: University Park Press, 1976.
Zacharkow, D. Wheelchair posture and pressure sores. Springfield, IL: Charles C Thomas, 1984.
Zacharkow, D. Posture, sitting, standing, chair design and exercise. Springfield, IL: Charles C Thomas, 1988.