Augmentative and Alternative Communication Systems
DISABILITIES AFFECTING SPEECH, LANGUAGE, AND COMMUNICATION
What Is Augmentative and Alternative Communication?
Augmentative and Alternative Communication Team
Role of Augmentative and Alternative Communication in the Lives of People With Complex Communication Needs
Partners of People With Complex Communication Needs Who Rely on Augmentative and Alternative Communication
Attitudes About and Acceptance of Augmentative and Alternative Communication
COMMUNICATION NEEDS THAT CAN BE SERVED BY AUGMENTATIVE AND ALTERNATIVE COMMUNICATION
Augmentative and Alternative Communication for Individuals With Developmental Disabilities
Augmentative and Alternative Communication for Individuals With Acquired Disabilities
Augmentative and Alternative Communication for Individuals With Degenerative Conditions
AUGMENTATIVE AND ALTERNATIVE COMMUNICATION EVALUATION AND ASSESSMENT
Assessment of Persons With Complex Communication Needs
Assessing Barriers to Participation
Relating Goals and Skills to Augmentative and Alternative Communication System Characteristics
EXAMPLES OF CURRENT AUGMENTATIVE AND ALTERNATIVE COMMUNICATION APPROACHES
No-Tech Augmentative and Alternative Communication Systems
Low-Tech Augmentative and Alternative Communication Systems
High-Tech Augmentative and Alternative Communication Systems
Examples of Vocabulary Retrieval Techniques
Examples of Vocabulary Programs for Language Development
Augmentative and Alternative Communication System Outputs
Access to Mainstream Technologies
Configurations of Commercial Speech-Generating Devices
IMPLEMENTATION OF AUGMENTATIVE COMMUNICATION SYSSSTEMS
Training System Use: Developing Communicative Competence
On completing this chapter, you will be able to do the following:
1 Describe the different communicative needs of persons with disabilities
2 Discuss the basic approaches to meeting these differing needs
3 Recognize the needs that individuals have for conversation and for graphical output such as writing, mathematics, and drawing
4 Describe the major characteristics of alternative and augmentative communication devices
5 Describe current approaches to speech output in assistive technologies
6 List and describe the major approaches to rate enhancement and vocabulary expansion
7 Describe the major assessment questions that must be asked and answered in determining the most appropriate augmentative and alternative communication device for an individual user
8 Discuss the major goals for and the significance of training in augmentative and alternative communication device use and communicative competence
9 Delineate the steps and procedures involved in implementing an augmentative and alternative communication device for an individual consumer
This chapter is devoted to augmentative and alternative communication (AAC), an area of clinical practice designed to ameliorate the communication problems of people who have severe speech and language impairments across the age span. Communication is a set of very complex behaviors and the very essence of being human. When someone is not developing speech and language skills or has lost the ability to speak or understand spoken or written language, then AAC intervention approaches are required to meet their complex communication needs (CCN). Communication is not a solitary activity, and people communicate differently with different partners and under different conditions by using a variety of tools, techniques, and strategies. Thus, AAC interventions are dynamic and include not only the individual with a disability but also his or her primary communication partners and are focused on augmenting communication in ways the person values (Figure 11-1).
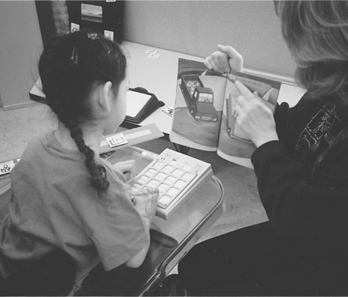
Figure 11-1 In conversations between speaking and AAC-using partners, the speaker may dominate the conversation unless careful selection, implementation, and training in use of the AAC system occurs.
There are many tools, strategies, and techniques available to help individuals meet their daily communication needs. AAC interventions acknowledge the importance of body-based modes (e.g., gestures, eye gaze, and facial expressions), nonelectronic aids (e.g., communication boards and books, paper and pencil), and electronic communication devices (e.g., speech-generating devices, talking frame, computers, etc.). Thus, the term AAC system refers to all the means and modes a person uses to communicate including the use of both AAC and mainstream approaches to communication (e.g., phones, e-mail, computers, etc.). Table 11-1 and the case studies of Joyce and Eileen illustrate this concept.

Speech-generating devices (SGDs) produce digitally recorded or synthesized speech output. They are AAC tools that can significantly improve communication for individuals with CCN. SGDs and their accessories are commercially available and currently funded by governments and third-party payer programs in many countries. SGDs have a variety of features that have changed over time to meet the needs of individuals with CCN. Today, people with CCN are using SGDs to attend schools and universities, work, carry on chats, participate in listservs, shop, order in restaurants, talk on the phone, and so on. People with severe disabilities and CCN who rely on AAC are living independently, getting married, and are active members of their communities. Individuals with CCN who do not gain access to AAC interventions are at high risk for abuse, crime, unemployment, and having limited social networks (Bryen, Cohen, and Carey, 2004; Collier, 2005). Infants, toddlers, and preschoolers with CCN require AAC interventions that support the development of language, communication, and emerging literacy skills. School-aged children with CCN need AAC interventions that enhance participation in their education, enable them to make friends, develop literacy and other academic skills, and engage with family members and people in their communities. Individuals who acquire disabilities later in life need AAC to help them sustain employment and maintain their relationships and social networks, independence, and dignity. As Daniel Webster said in 1822, “If all my possessions were taken from me with one exception, I would choose to keep the power of communication, for by it I would soon regain all the rest.”
AUGMENTATIVE AND ALTERNATIVE COMMUNICATION AFTER A STROKE
Eileen is a 62-year-old woman who has sustained a brainstem stroke and now requires maximal assistance for daily living. Eileen’s unaided communication modalities, shown in Table 11-1, include isolated words, facial expressions, yes/no responses, and inflectional vocalizations. She also has two AAC devices. The first of these is a letter board, accessed by her eye gaze, that she uses to indicate her needs and choices (Figure 11-2). All these systems have limitations. The unaided systems require significant amounts of interpretation by the partner, and the manual eye gaze device is slow because it relies on spelling and interpretation by her partner. These limitations are partially overcome by Eileen’s electronic AAC device, which she accesses by using head movement to make selections with a light pointer mounted on a headband on the side of her head (Figure 11-3). This device includes vocabulary storage, so she can use whole words and phrases, and it provides synthesized speech output. These features allow Eileen to converse with more people, and they make it easier on the communication partner. Each of these devices contributes to the quantity and quality of her communication interactions.
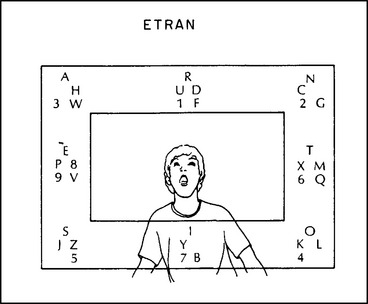
Figure 11-2 This communication system is based on the user and partner facing each other. Two eye movements are required. The first movement selects the group, and the second movement selects the letter. For example, to select the letter A, the user first looks to the upper left, then to the upper center. Eye gaze using pictures or other symbols is also common. (From Blackstone S: Augmentative communication, Rockville, MD, 1986, American Speech Language Hearing Association.)
American Speech Language Hearing Association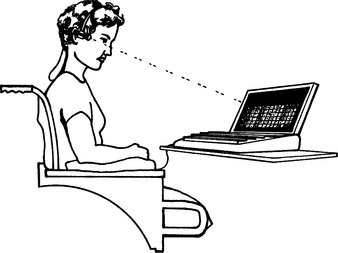
Figure 11-3 In this device a light is attached to the user’s head. When the light beam is aimed at the panel of the device, it is detected and an entry is made. (From Blackstone S: Augmentative communication, Rockville, MD, 1986, American Speech Language Hearing Association.)
American Speech Language Hearing AssociationThis chapter is devoted to a discussion of the major aspects of AAC that are important in enabling individuals with CCN to communicate across the life span, recognizing that each individual has unique needs, goals, preferences, skills, and abilities. The material presented in Chapters 3, 4, and 7 is applied to AAC here.
DISABILITIES AFFECTING SPEECH, LANGUAGE, AND COMMUNICATION
There are many disabilities that can affect an individual’s communication skills and abilities. The description of cognitive function and development in Chapter 3 serves as a backdrop for discussions in this chapter. In addition, some individuals are born with or acquire conditions that interfere with their ability to make sounds or control the muscles of the chest, diaphragm, mouth, tongue, and throat and produce intelligible speech. Dysarthria is a disorder of motor speech control resulting from central or peripheral nervous system damage that causes weakness, slowness, and a lack of coordination of the muscles necessary for speech production (Anderson and Shames, 2006). Verbal apraxia is a disorder affecting the coordination of motor movements involved in producing speech caused by a central nervous system dysfunction (Anderson and Shames, 2006). Limb apraxia may impair the ability to write. When speech or writing is severely impaired, AAC approaches are required.
There is a difference between speech disorders and language disorders. In Chapter 3 we defined language as any conventional system of arbitrary symbols organized according to a set of rules. Speech is the oral expression of language. AAC interventions for children with severe language delays or disorders are designed to support the development of receptive and expressive language and literacy skills. In adults, aphasia is a type of language disorder that often occurs as a result of a cerebral vascular accident or traumatic brain injury (TBI). Aphasia can affect both expression and reception of spoken and written language. For example, some people may lose the ability to recall vocabulary (e.g., names, places, events), and others may lose the ability to understand spoken language, organize language into meaningful utterances, and speak and write meaningful utterances. The degree to which various language functions are impaired is variable. AAC interventions for severe aphasia often focus on strategies that help individuals compensate for a severe loss of language function in ways that support functional communication.
Among the disabilities affecting communication that are ameliorated by AAC interventions are developmental conditions such as cerebral palsy (CP) and autism, acquired conditions such as TBI, stroke/cerebral vascular accident (CVA), and high-level spinal cord injury and degenerative diseases such as amyotrophic lateral sclerosis (ALS), progressive aphasia, and multiple sclerosis. Estimates indicate that approximately 2 million people in the United States and from 0.3% to 1.0% of the total world population of school-aged children have a need for AAC (Beukelman and Mirenda, 2005). Not all the people in this population are served equally. Blackstone (1990) conducted a survey to determine how well various populations were served and reported that in the early 1990s children with CP, individuals with good cognitive skills, and adults with some degenerative diseases (i.e., ALS) receive more attention from AAC practitioners than individuals with intellectual disabilities and children and adults with autism, dual sensory impairment, TBI, and the elderly (Blackstone, Williams, and Joyce, 2002).
Approaches to AAC interventions differ depending on the severity, type, and onset of an individual’s disability. There are significant differences, for example, between meeting the needs of children who have never spoken or used written language (congenital disabilities) and adults who have developed language, speech, and writing and then lost these skills because of a disease or injury. For example, young children with severe motor impairments and CCN are learning language at the same time they are learning to “talk” and “write” by using AAC approaches. Thus, conventional means of communication (i.e., speaking and using a pencil) are unavailable to them. In addition, they have few, if any, opportunities to interact with competent AAC users who might serve as models and help them learn how to communicate using AAC. On the other hand, someone in whom ALS develops at age 46 years typically has years of experience using multiple forms of communication and intact language skills; thus, AAC interventions likely focus on providing AAC technologies and strategies so they can continue to communicate effectively with preferred partners.
What Is Augmentative and Alternative Communication?
There are many ways of looking at AAC systems. Unaided communication or body-based modes describe communication behaviors that require only the person’s own body, such as pointing and other gestures, pantomime, facial expressions, eye-gaze and manual signing, or finger spelling. These modes are often used concurrently with each other and with speech. Even unaided modes of communication are typically culturally bound. Thus, when individuals have significant sensorimotor impairments, communication partners frequently misinterpret their nonverbal behaviors because eye gaze, facial expression, body movements, posture, traditional head nods, and pointing or reaching may be inaccurate, leading to communication misunderstandings (Kraat, 1986). Rush (1986) gives an example when he describes the difficulty his cerebral palsy causes him in delivering his line (a yell) in a play: “When a person with cerebral palsy wants to do something, he can’t and when he wants not to do something, he involuntarily does it. So getting my vocal cords to cooperate with the cue was as hard as memorizing a Shakespearean play [for a nondisabled person]” (p. 21).
Aided AAC components may include a pen or pencil, a letter or picture communication board, a computer, a cell phone, and an SGD. Aided AAC may be either electronic or nonelectronic. Although a paper letter board (nonelectronic) differs from a computer-based SGD (electronic), both nonelectronic and electronic devices require that the person use a symbol system and have a way to select messages. All forms of AAC require consideration of how communication partners will participate in the communication process.
Multiple Communication Modes
Everyone uses multiple communication modalities and devices when communicating to meet a full spectrum of needs. Competent communicators use speech, a range of body-based modes, and low- and high-tech aids and devices so they can interact with multiple partners across multiple contexts. However, when someone is first taught to use AAC, decisions about what modes to teach or emphasize may require consideration of multiple factors. The two case studies of Joyce and Eileen illustrate this concept. In one published study, two young children (3 years 6 months and 4 years 6 months) with cognitive disabilities illustrate why professionals should exercise caution when introducing multiple AAC approaches at the same time (Iacono, Mirenda, and Beukelman, 1993). Each child used either (1) an electronic device coupled with manual signing (dual modes) or (2) signing alone (single mode) to produce two-word semantic combinations. Results showed that one child was more effective using both modes together and that the other preferred to use only one mode.
Augmentative and Alternative Communication Team
AAC interventions require a collaborative team approach. Each member of the AAC team has important roles and responsibilities:
• The client and family have the greatest knowledge of the daily communication needs of the person with CCN. Family members are often the individuals’ primary communication partners and serve as advocates and facilitators.
• The speech-language pathologist has the greatest general understanding of communication in general and can assess language, and communication needs, abilities and skills; select AAC materials and technologies; and teach the individual, family, and staff to use AAC system components effectively.
• The teacher sets educational goals and oversees classroom implementation of each child’s AAC system and has knowledge of literacy, social interaction, and education.
• The physical therapist (PT) or occupational therapist (OT) carries out the motor evaluation, addresses seating and positioning, evaluates physical access to the AAC system, and has knowledge of how to support writing, drawing, and other activities of daily living.
• The teacher’s aide/job coach is also critical to the success of implementation. This individual supports the person in the school/work setting. Key team members are often referred to as “natural supports” because they have a continuing relationship with the individual (e.g., family, friends, coworkers, and employer). On occasion, physicians, psychologists, vision specialists, and other professionals also play an important role on AAC teams.
Role of Augmentative and Alternative Communication in the Lives of People With Complex Communication Needs
Christopher Nolan (1981), a man with cerebral palsy, wrote in the third person (as Joseph) about the importance of attentive and responsive communication partners. “Such were Joseph’s teachers and such was their imagination that the mute boy became constantly amazed at the almost telepathic degree of certainty with which they read his facial expression, eye movements, and body language. Many a good laugh was had by teacher and pupil as they deciphered his code. It was moments such as these that Joseph recognized the face of God in human form. It glimmered in their kindness to him, it glowed in their keenness, it hinted in their caring, indeed it caressed in their gaze” (p. 11).
AAC systems can enhance interaction, but they can also become the center of attention, as Rush (1986) noted:
My new friend (Wendy) was good looking. She was just over five feet tall and had brown eyes that matched the color of her shoulder length hair. Her skin showed a summer tan and she had a dynamite smile. “Did he show ya all his electronic stuff?” one of my dorm mates asked her. “Go on, Bill, show her.” So I demonstrated the controls for my lights and clock radio. I showed off my door opener, which I could control via a radio transmitter attached to the Plexiglas tray on my wheelchair. She was impressed with the space-age technology. “Hey, show her your wheelchair and how it works. I’ll never understand how it works. It baffles me,” another dorm mate said. So, wondering if I should sell tickets, I wheeled about the room. I demonstrated how I went straight, reverse, and turned left and right. I was angry at my dormmates because I was a man, not a side show freak. My wheelchair was a tool for my mobility, not a novelty. Why couldn’t they see that? And why couldn’t they see that I was trying to get to know Wendy. Why didn’t they understand I had a right to my privacy just as they did? As I was wheeling around the room, I noticed that Wendy was typing something. I was disappointed in her. I thought she knew that I could hear and that she didn’t have to write things to me. Apparently I was wrong. When I was done showing my electric marvels to her and the guys, I rolled back to my typewriter to read, “I wish they would go, so we could talk by ourselves.” They finally left and we finally got to talk. Our friendship had started. (p. 137)
The loss of speech can also occur later in life. Doreen Joseph (1986) lost her speech after an accident. Here’s what she said, “I woke up one morning and I wasn’t me. There was somebody else in my bed. And all I had left was my head. Speech is the most important thing we have. It makes us a person and not a thing. No one should ever have to be a ‘thing’” (p. 8). Sue Simpson (1988) lost her speech after a stroke at age 36 years. She wrote: “So you can’t talk, and it’s boring and frustrating and nobody quite understands how bad it really is. If you sit around and think about all the things you used to be able to do, that you can’t do now, you’ll be a miserable wreck and no one will want to hang around you long” (Simpson, 1988, p. 11).
Dowden and Cook (2002) defined three types of AAC communicators. Emergent communicators have no reliable method of symbolic expression, and they are restricted to communicating about here-and-now concepts. Context-dependent communicators have reliable symbolic communication, but they are limited to specific contexts because they are either only intelligible to familiar partners, have insufficient vocabulary, or both. Independent communicators are able to communicate with unfamiliar and familiar partners on any topic. Each of these communicators has different needs and goals.
Partners of People With Complex Communication Needs Who Rely on Augmentative and Alternative Communication
Communication almost always involves a partner who may be in the room, on the phone, or a continent away on e-mail. Some “partners” may be merely imagined, as when someone writes a story. The Circle of Communication Partners (Figure 11-4) is helpful in defining the range of partners that a person with CCN who relies on AAC might encounter (Blackstone, 2003a). The first circle represents the person’s life-long communication partners. This is primarily immediate family members. The second circle includes close friends (i.e., people who you tell your secrets to). These are often not family members. Acquaintances such as neighbors, schoolmates, coworkers, distant relatives (such as aunts and cousins), the bus driver, and shopkeepers are included in the third circle. The fourth circle is used to represent paid workers such as a speech-language pathologist (SLP) or a PT, OT, teacher, teacher assistant, or babysitter. Finally, the fifth circle is used to represent those unfamiliar partners with whom the person has occasional interactions. This includes everyone who does not fit in the first four circles. Thus, the familiarity with partners decreases as we move from circle 1 to 5 and the modes of communication required to communicate with people in each circle will vary. For example, Blackstone and Hunt Berg (2003) found that SGDs and low-tech displays were often used primarily with people in circle 4. They also noted that SGDs are required for successful interactions with partners in the third and fifth circles. Gestures and impaired speech are often preferred modes in circles 1 and 2. An AAC intervention tool, Social Networks: A Communication Inventory for Individuals with Complex Communication Needs and Their Communication Partners, described in Box 11-1, is based on a number of theoretical frameworks including the circle of friends (Falvey et al, 1994), the field of social networks, the Participation Model (Beukelman and Mirenda, 2005), and person-centered planning.
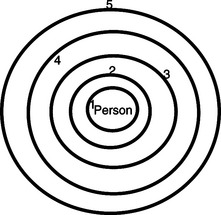
Figure 11-4 Circle of friends. 1, Lifelong communication partners; 2, close friends; 3, neighbors, acquaintances; 4, paid workers; 5, unfamiliar partners.
Although the experience of the assistive technology practitioner (ATP) with individuals who have CCN may be limited to a brief encounter, the family has a long-term relationship with the individual and are key members of AAC assessment and decision-making team (Parette, Botherson, and Huer, 2000). In fact, when one family member relies on AAC, it always has an impact on the entire family (Goldbart and Marshall, 2004). Parents, spouses, and siblings need clear, jargon-free information that is presented objectively and honestly. Information about options, funding, timelines, and training in the use of the recommended AAC device or strategy is particularly important (Parette, Botherson and Huer, 2000). There is great diversity among families, of course, and this will affect the way they respond to their family member’s communication needs and to AAC itself (Goldbart and Marshall, 2004). For example, parents report feeling additional pressure to use AAC in communicating with their child and to help others to do so (Angelo, 2000). Researchers also report that the goals of mothers and fathers may differ for their children (Angelo, Kokoska, and Jones, 1996). Mothers ranked social opportunities with both nondisabled children and other AAC users, integrating AAC into the community, and planning for future needs as their highest priorities. Fathers focused on planning for future needs, knowing how to program, repair, and maintain the SGD; integration of AAC into educational settings; and obtaining computer access with the SGD. Parents also indicated that they have to become strong advocates for their child to receive necessary services (Goldbart and Marshall, 2004).
Attitudes About and Acceptance of Augmentative and Alternative Communication
McCarthy and Light (2005) reviewed 13 research studies on the attitudes toward individuals who rely on SGDs. They identified several factors affecting attitudes: characteristics of typically developing individuals, characteristics of the person using AAC, and characteristics of the AAC system. These are elements of the social context of the human activity assistive technology (HAAT) model. Attitudes toward individuals who use AAC vary across the parameters of gender, type of disability, age, experience of the user of AAC, experience and familiarity with disability and AAC by the partner, and social context. Attitudes appear to be formed by the interaction of many of these factors.
The attitudes of children who do not have disabilities toward children who do and who use AAC is influenced by their familiarity with children who have disabilities (i.e., whether the nondisabled students had a classmate with a disability) and by age (older children are less positive than are younger children) (Beck et al, 2002). In general, girls are more positive toward disabled peers than boys are (Beck and Dennis, 1996). Although the number of conversational turns (one exchange between the speaker and partner) was almost identical in both groups, children who use AAC communicate mostly through responses and their typically developing peers initiate almost all of the requests (Clarke and Kirton, 2003). Beck et al (2002) reported that the longer the messages produced (two- vs. four-word utterances), the more positive were the peers’ attitudes toward the child using AAC. Consistent with the second-circle relationship, much of the interaction among peers involves expressions of humor and intimacy (e.g., laughing, joking, teasing, tickling, etc.). In general, the attitudes of peers toward an AAC user do not appear to be affected by the type of AAC system used (Beck and Dennis, 1996). However, in one study the use of voice output led to more positive peer attitudes than when the output was only visual (letters on a display) (Lilienfeld and Alant, 2002).
Many students who use AAC are enrolled in inclusive classroom settings. Thus, the attitudes of general education teachers (circle 4) toward AAC are important to their success (Kent-Walsh and Light, 2003). Both the students who use AAC and their typically developing classmates in general education classes can develop skills and positive interactions during classroom activities. However, unequal status with classmates and dissimilar interests lead to social exclusion for students who rely on AAC. Often peers speak to the teacher or teacher’s assistant rather than directly to the student. Teachers are also concerned about lack of academic gain. Some device features (e.g., speech synthesis) are perceived as disruptive to other students. School-related barriers to successful inclusion include large class sizes, the physical layout of the classroom, and the tendency of the schools to apply inclusion guidelines very liberally without a focus on educational needs. Teachers require time to adjust to the idea of having students with disabilities in class, full access to school resources for the AAC students, and availability of specialists for consultation and training.
Employers and coworkers are also influenced by workers who use AAC (McNaughton, Light, and Gulla, 2003). Benefits for the worker using AAC are social interaction, personal enjoyment, and financial gain. Benefits to the employer include positive impacts on other employees, high quality of work performance by the employee using AAC, loyalty of the employee, and the ability to fill “hard-to-fill positions.” Employment challenges fall into several themes: finding a good job match to individual skills, communication challenges (e.g., noisy AAC device, speaker phone use), difficulty with typical office tasks (e.g., manipulation of paper, telephone use), education or vocational skill level too low, lack of knowledge of work culture, and physical challenges necessitating assistance from other workers and financial (e.g., insurance costs to company).
COMMUNICATION NEEDS THAT CAN BE SERVED BY AUGMENTATIVE AND ALTERNATIVE COMMUNICATION
When someone is unable to speak or write so that all current and potential communication partners can understand them, then an AAC system is required. As humans, we communicate in a myriad of ways depending on the circumstances. Although we rely most heavily on speaking and writing, when these modes are unavailable, then we search for (and find) other ways of communicating. People with CCN often are unable to speak and write so others can understand them. Thus, they need AAC approaches to help them communicate face to face, on the phone, and across the Internet. Use of these mainstream technologies such as the Internet and cell phones are addressed later in this chapter. In considering writing, such activities as drawing, plotting graphs, and mathematics are included, all the things that are normally done with a pencil and paper, computer, calculator, and other similar tools. Assistive technologies for writing include not only AAC devices, discussed in this chapter, but also other approaches discussed in Chapters 15 (those primarily used for educational access) and 16 (those primarily used for vocational pursuits).
Light (1988) describes four purposes of communicative interaction: (1) expression of needs and wants, (2) information transfer, (3) social closeness, and (4) social etiquette. Expression of needs and wants allows people to make requests for objects or actions. Information transfer allows expression of ideas, discussion, and meaningful dialog. Social closeness serves to connect individuals to each other, regardless of the content of the conversation. Social etiquette is used to describe those cultural formalities that are inherent in communication. For example, students will speak differently to their peers than to their teachers.
In considering communication needs, three perspectives are addressed: (1) individuals with developmental disorders, (2) individuals with acquired conditions, and (3) individuals with degenerative conditions. Although the focus of AAC interventions may vary across these groups, there is also substantial overlap in the issues faced when communication is severely limited, no matter what the causes may be.
Augmentative and Alternative Communication for Individuals With Developmental Disabilities
Because the development of speech, language, and communication begins at birth, early intervention is important. Effective AAC intervention for children with developmental disabilities requires that AAC be integrated into the child’s daily experiences and interactions and that it take into account what we know about child development (Light and Drager, 2002). For example, many young children do not have the physical or cognitive skills to learn to use current AAC selection techniques (e.g., scanning or encoding) and thus are unable to access AAC systems. Also, the design of current AAC technologies often requires a child to stop playing to use a communication device. A more desirable approach is to design AAC technologies and strategies that incorporate the use of AAC into the child’s play activities so the child can talk about his or her play or interact with peers while engaged in the activity. In short, to be effective, the design, type, and layout of AAC system components should match the desires, preferences, abilities, and skills of children.
A major concern for parents is whether the use of AAC will impede their child’s development of speech. Research data put all such fears to rest (see Blackstone, 2006). The use of AAC does not interfere with speech development and may in fact enhance the development or return of speech. There are a number of possible explanations for this, including increased acoustic feedback (from voice output SGD), increased experience with conversational turns and other communicative functions, reduced pressure to speak that releases motor stress, and the development of an internal phonology as a result of AAC systems use (Blishcak, Lombardino, and Dyson, 2003).
Research shows that children with a broad range of developmental disabilities can benefit from AAC interventions. This includes children with CP, intellectual disability, Down syndrome, other genetic disorders, and autism spectrum disorder (ASD). The latter is used here as an example of AAC intervention for individuals with developmental disabilities. (Intellectual disabilities and more mild disorders such as learning disabilities are discussed in Chapter 10.)
ASD is characterized by significant social communication challenges throughout life that reflect impairments in social interaction, verbal and nonverbal communication, and restricted, repetitive, stereotypical patterns of behavior, interests, and activities (Blackstone, 2003b). Early intervention (starting as young as age 2 years) improves outcomes for children with ASD. These children often have difficulty with joint attention (i.e., coordinating attention between people and objects) and understanding and using symbols. Approximately one third to one half of children with ASD do not use speech functionally (Blackstone, 2003b). The learning styles of children with ASD show a strong preference for static information and, as a result, they often benefit from the use of “visual supports.” Because speech and other elements of conversations are transient, AAC devices and communication displays that use static visual symbols provide possible advantages for the child with ASD. Also, because of their dependence on rote or episodic memory, children with ASD often benefit from contextual clues and prompts, and this can lead to them becoming prompt or context dependent. Thus, AAC interventions that extend the use of language and appropriate communication behaviors across different contexts and partners are needed. Blackstone (2003b) argues that AAC can be effective for children with ASD because it addresses both their unique learning styles and their communication needs.
Children with ASD can use no-technology (e.g., manual signs) and high- and low-technology approaches to AAC (Mirenda, 2003). At this time, there is no clear evidence that one approach is superior to any other. The use of total communication (speech and manual signing) provides advantages because there is no device to worry about and because it promotes more natural forms of communication. However, not all children (or their partners) do equally well with this approach. Some children develop more functional communication using low-tech aided systems. PECS* is one widely used example. Voice output communication aids can also support interactions. For example, Schlosser and Blischak (2001) suggested that electronically generated speech might be beneficial for children with ASD who have difficulty processing natural speech. Also, computer aided instruction may help children with ASD attend to instructions and prompts when provided by electronic speech output. There are many considerations in choosing among the many available AAC approaches, including an individual’s preferences, ease of learning, effect on the development of speech and language, ability to use the approach functionally across partners and contexts, and the communication tasks the person needs to accomplish. Finally, the degree of partner support and responsiveness is considered. Currently, best practice relies on clinician judgment as much as evidence because current research on the use of AAC approaches for individuals with ASD is promising but inconclusive in each of these areas.
Augmentative and Alternative Communication for Individuals With Acquired Disabilities
Adults with acquired disabilities such as TBI, aphasia, and other static conditions may require the use of AAC interventions as part of the rehabilitation process (Beukelman and Ball, 2002). Persons with recovering conditions often have changing levels of motor, sensory, or cognitive/linguistic capability that benefit from the use of human/technology interfaces, including AAC, to help them accommodate. Although many people may be unable to speak or write directly after a severe head injury or brainstem or cortical stroke, most will recover these abilities. However, over the long term, some individuals continue to benefit from the use of AAC. In this section TBI and aphasia are discussed as examples of individuals with acquired AAC needs.
Traumatic Brain Injury.
TBI can result in the loss of speech and often causes physical, cognitive, and language impairments (Beukelman and Garrett, 1988; Light, Beesley, and Collier, 1988). Although the long-term recovery of speech is variable, immediately after the injury many individuals benefit from the use of AAC interventions to support functional communication. Associated changes in motor, perceptual, cognitive, and language abilities also may have detrimental effects on communication (Carlisle Ladtkow and Culp, 1992). Thus, it is critical that the limitations associated with a severe brain injury from a car accident, gun shot wound, explosion, and so forth be identified and considered when AAC goals and interventions are determined (Beukelman and Yorkston, 1989). In a follow-up study of nonspeaking individuals with TBI 1 year after discharge, DeRuyter and Kennedy (1991) found that only 56% of those for whom an AAC device was recommended were using the device, 24% had completely discarded the device, and 20% only used it in limited environments (DeRuyter and Kennedy, 1991). In many cases, speech had returned. However, there was no indication as to why 44% of the devices were abandoned or not being used to their full potential. Beukelman and Yorkston (1989) point out that there is a need for AAC devices to be integrated and adapted into the person’s living situation, outside the rehabilitation center. Frager, Hux, and Beukelman (2005) found that a group of communication partners and the continuing support of an AAC facilitator contribute to success. In a recent study, Frager, Hux, and Beukelman (2005) found that high-tech devices were favored over low-tech systems and that low-tech systems were apt to be used temporarily by people with TBI who regained speech.
Aphasia.
Persons who sustain CVAs often have language difficulties that we collectively call aphasia. One lasting problem these individuals have is vocabulary retrieval or word-finding difficulties. There are several AAC-related approaches with potential for aphasia rehabilitation (Jacobs et al, 2004; Kraat, 1990). For example, individuals who can recall first letters and recognize a desired word from a list may use word prediction devices/software. The individual begins typing a letter and then the device predicts several words from which to choose (see Figure 7-8). Colby et al (1981) developed a microcomputer-driven device that used a specially designed database containing words, their frequency of use, and features of each word, which was specifically designed for persons with aphasia. Features included words that “go with” the desired word. This can be a sound-alike relationship; a semantic (meaning) relationship; a categorization (e.g., a piece of furniture or a fruit); and initial, middle, and ending letters. Each was shown to be effective for persons with certain types of aphasia. A similar approach was developed by Hunnicutt (1989).
Many factors must be considered when AAC is applied in aphasia rehabilitation (Kraat, 1990). Some people with severe aphasia learn to augment their speech and communication efforts by relying on gestures and an alternative symbol system (Jacobs et al, 2004). However, although persons with aphasia may be able to use graphic symbols, many find it difficult to apply them socially or to generalize their use. One commercial device designed specifically for persons with aphasia is the Lingraphica, which organizes symbols by semantic categories (e.g., places, foods, clothing) and includes synthetic speech output and animation of verbs (Steele and Weinrich, 1986). Approaches such as CHAT and TALK that model conversational flow and provide clues to word vocabulary choices based on context can also assist aphasic individuals (Kraat, 1990).
A recent development is the use of visual scene displays (VSDs) (McKelvey et al, 2007). VSDs use personalized photos of scenes and arrange these on a dynamic display device. The technology enables individuals with severe aphasia to use familiar photographs to engage partners in interactions about multiple topics. In addition, the design of the technology makes it relatively easy for partners to provide conversational supports. Because of the dynamic nature of the display, the user is continually prompted, reducing the individual’s need to rely on recall memory. The potential for people with aphasia to benefit from the use of VSD technology is still under investigation.
The use of AAC in aphasia rehabilitation often involves the use of AAC strategies and partner training. Blackstone (1991) identified issues involved in aphasia rehabilitation that included a discussion of public policy issues (e.g., funding for assessment and therapy services) and a discussion of clinical studies involving AAC strategies and technologies. King and Hux (1995) describe the use of a talking word processor to increase writing accuracy for individuals with aphasia. The speech feedback provided additional monitoring of the written work, which helps the person to identify and correct errors. Garrett and Beukelman (1992) present a classification system for aphasic individuals that is useful in planning AAC interventions. This scheme guides intervention planning by describing five types of aphasic communicators: basic choice, controlled situation, augmented, comprehensive, and specific need. For each of these categories, the authors identify residual skills, intervention goals, and AAC skills and suggest AAC activities for both partners and the individual with aphasia. Finally, Fox and Fried-Oken (1996) propose questions related to effectiveness, efficiency, and generalization in AAC aphasiology research. One area of concern for future development in AAC is how best to represent meaning on AAC technologies for persons with aphasia (Beukelman and Ball, 2002).
Augmentative and Alternative Communication for Individuals With Degenerative Conditions
A degenerative condition in which speech or language functions are gradually lost presents a different set of challenges for the person with CCN and for AAC interventions. For many conditions, multiple AAC modes are necessary as the disease worsens. Persons with degenerative conditions often have changing levels of motor, sensory, or cognitive/linguistic capability that require the adaptation of the human/technology interfaces to accommodate their changing motor and cognitive skills. In this section ALS is discussed as an example of a degenerative condition that significantly affects communication. Dementia is discussed in general in Chapter 10.
ALS, also referred to as one of the motor neuron diseases, is a rapidly progressing neuromuscular disease that affects speech in the majority of cases (see the case study of Mr. Webster). Although persons with ALS use the same AAC systems as others, there are unique factors considered during the intervention process. For example, it is not uncommon for someone to begin using a direct-selection AAC system and later on require scanning to continue communicating. If this type of transition is not planned for initially, it can be very hard for the person to maintain effective interactions. Families differ in their desire and ability to deal with the longer term (Blackstone, 1998). Some families prefer to “plan ahead” and consider future needs, whereas others prefer to take things as they come. Some SGDs can accommodate direct selection and a variety of indirect selection modes, so these are often recommended. But they are often heavy and hard to carry and thus may be less useful at the outset when the person is still ambulatory. Patients with ALS tend to use high-tech aids with strangers and for conversation (Blackstone, 1998). No-tech approaches, including 20 questions (the person can answer yes or no by head nod, eye blink, or other means) or gestures may be most effective with family and to express basic needs. Low-tech approaches such as letter boards are more often used with strangers than with family members.
Acceptance of AAC by persons who have ALS is reported by several authors. In one 4-year study, more than 96% of those given the choice of AAC accepted that choice (Ball, Beukelman, and Patee, 2004). There are several factors leading to acceptance and successful use of AAC by persons with ALS. First, it is important that clinicians provide information regarding the speech-language characteristics of ALS at the outset of intervention. There is a relationship between speaking rate and intelligibility, with 80% intelligibility occurring at about 130 words per minute (Ball, Beukelman, and Patee, 2004). Speech rate is used to determine the timing of AAC interventions. The rate continually drops as ALS progresses, and evaluation is initiated when the rate is at 90%. The second success factor is maintaining continuous contact to monitor speech rate and intelligibility along with other routinely measured motor system parameters. Finally, it is important that the family remain aware of AAC service intervention opportunities. Flexible AAC devices and strategies that will accommodate for changes over the course of the disease are important. A key reason for acceptance of AAC by persons with ALS is their desire to continue interacting with communication partners in a variety of contexts. The literature strongly supports the use of AAC as a key component of evidence-based practice in the treatment of ALS.
AUGMENTATIVE AND ALTERNATIVE COMMUNICATION EVALUATION AND ASSESSMENT
AAC assessment requires systematic consideration of many factors (Beukelman and Mirenda, 2005; Coleman, 1988; Lloyd, Fuller, and Arvidson, 1997). These factors are described by the four components of the HAAT model. The most important step is to define the goals and needs of the person with CCN and his or her current and potential communication partners through a careful analysis of the desired activity or activities. The Social Networks tool is useful at this stage (see Box 11-1). An evaluation of the various contexts in which communication will occur helps to further inform the assessment goals. The Participation Model (see below) helps to define opportunities and barriers in various contexts. Once the goals, needs (activity component of the HAAT model), and contexts (HAAT model) are clearly understood and agreed to by all team members (e.g., person with CCN, parent, spouse, teacher, employer, care provider, speech pathologist, OT, PT, and others), physical, sensory, cognitive, and language skills (the human component of the HAAT model) are assessed as they relate to augmentative communication. Finally, if a low- or high-tech AAC system component (e.g., SGD, computer) is indicated, the assistive technology characteristics can be matched to consumer skills and goals by systematically identifying the human/technology interface, the processing (e.g., SGD rate enhancement, vocabulary storage), and the activity output modes.
Assessment of Persons With Complex Communication Needs
Several types of AAC assessment may be conducted. A predictive assessment has a goal of understanding the client needs and status today, predicting future needs, and selecting a system to meet both of these. A serial assessment is a continuing evaluation to meet changing needs (e.g., as a child develops). A curriculum-based assessment is continuous in classrooms to help coordinate AAC interventions with the achievement of educational goals. In any case, the assessment process takes into consideration the individual’s skills and abilities and current and future communication needs and preferences. From these, an intervention plan is developed.
The overall goals of AAC assessment are as follows: (1) to document communication needs, (2) to determine how many needs can be met through current communication methods, including speech, and (3) to reduce the number of unmet communication needs through systematic AAC intervention. Each member of the AAC team described earlier in this chapter has a specific role in the assessment process.
There are many tools available to the AAC team. However, assessment approaches designed for other populations often require adaptations of materials and procedures so that assessment results are valid and reliable, as described by Beukelman and Mirenda (2005). One tool is the Social Networks Inventory described earlier in this chapter. It enables the perceptions of many individuals to be considered when planning an intervention (Blackstone, 2003a) and it provides a structure for gathering of information. When used in combination, the HAAT model, Social Networks, and the Participation Model (Beukelman and Mirenda, 2005) provide a comprehensive framework for ensuring that all information needed for successful AAC implementation is obtained during the assessment process.
Assessing Barriers to Participation.
In the Participation Model, opportunity and access barriers to successful AAC use are identified. Beukelman and Mirenda (2005) present detailed information regarding the implementation of the participation model, including sample assessment forms and case examples. For example, opportunity barriers are those that involve policies, practices, attitudes and knowledge, and skills of those who support the person with CCN and that interfere with successful AAC interventions. As an illustration, consider the situation where a school district purchases an SGD for a child, but the child is required to leave it at school at all times. This practice is a barrier to full societal participation and academic success. Keeping the device at school may be a policy of the district because uninformed administrators worry about the cost of the device and possible breakage or loss if it goes home. After all, schools allow students to take home band instruments, uniforms, books, and pencils. Another example of an opportunity barrier is the employer who is resistant to a worker using an AAC device. This may reflect the employer’s attitudes about disability or a lack of knowledge about AAC or a lack of skill in supporting individuals with CCN.
Another key element of the Participation Model is an “activity standards inventory” in which desired communication-related activities of the person with CCN (termed “target person”) are listed. The standard of desired performance is that a nondisabled peer carry out the same activity. The target person is then rated as to the level of participation (independent, independent with setup, verbal or physical assistance, or unable to participate), and the discrepancy between peer and target person (if any) are ascribed to “opportunity” or “access” barriers. These are evaluated in terms of potential needs: (1) to increase natural abilities, (2) to make environmental adaptations, and (3) to use AAC systems and/or devices. Finally, AAC potential is determined through an operational profile, a constraints profile, and a capability profile.
As described in Chapter 7, the human-technology interface evaluation is part of a capability profile. An important component of the capability assessment involves documenting the individual’s speech, language, motor, sensory, cognitive, and social communication skills. Dowden (1997) describes assessment approaches for individuals with CCN who have some functional speech. There are many language tests for both children and adults. Cognitive assessments help to determine how the individual understands the world and how communication can be best facilitated within this understanding (Beukelman and Mirenda, 2005). There are no formal tests that accurately predict the ability of an individual to meet the cognitive requirements of various AAC techniques and technologies, and expressive language by use of AAC is itself required to accurately assess cognitive ability. Thus, the individual’s cognitive ability is often estimated. Some cognitive skills that are important for AAC are shown in Box 11-2. Social communicative skills (e.g., degree of interaction, attention to task) are generally assessed by interviews with family, caregivers, teachers, and others and through observation during an assessment or during opportunities created specifically to encourage social interaction. One example of the information that may be required (and how it may be assessed) is delineated in the Medicare funding request for SGDs in the United States (shown in the first column of Table 11-2).
TABLE 11-2
Assessment of Feature Required for a Speech-Generating Device
*Blackstone S: Assessment protocol for SGDs, Augment Commun News 13:1-16, 2001.
Assessing Representation.
One area of assessment unique to the area of AAC is determining what types of symbols an individual can use to communicate. A variety of symbol types are shown in Figure 11-5. Clinicians may select from several assessment protocols (Beukelman and Mirenda, 2005). In one protocol (functional object use), the evaluator shows the person a symbol and says “Show me what you do with this.” The response may be a gesture (e.g., hand to mouth for “eat it”) or pointing at a picture or symbol (e.g., “drink” if prompt is a soft drink can). In another approach (visual matching) the evaluator asks the individual to find a single stimulus item from a multiple symbol array or vice versa. The most flexible AAC systems are those that depend on spelling and require literacy skills, so word recognition and reading comprehension are often used to assess reading level, and spelling evaluations also may be conducted (Beukelman and Mirenda, 2005). There are multiple levels of spelling skills that may be useful in AAC:
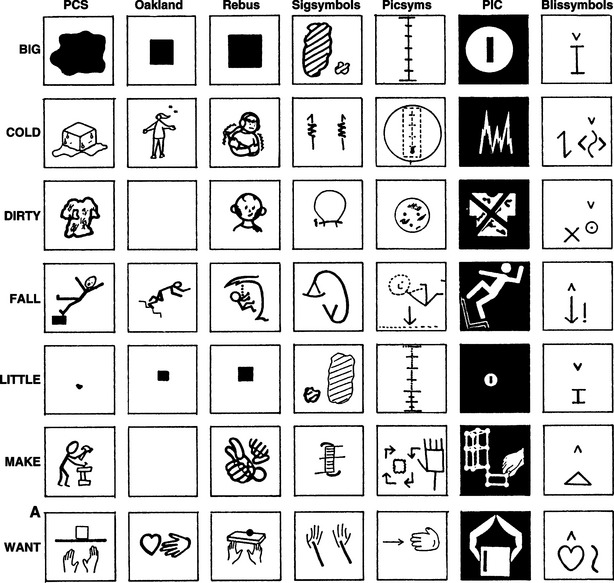
Figure 11-5 Examples of the variety of symbol systems that have been developed for AAC use. (From Blackstone S: Augmentative communication, Rockville, MD, 1986, American Speech Language Hearing Association.)
American Speech Language Hearing Association1. Recognition spelling requires the client to pick the correct entry from a list of options. This can enable someone to use an SGD that presents word lists or other stored vocabulary choices and that relies on recognition memory.
2. Word completion tests evaluate the person’s ability to correctly select the first letter of a word and recognize the completed word (see Chapter 7).
3. Spontaneous spelling requires the person to spell the requested word letter by letter.
Many types of symbol systems are used in augmentative communication (Lloyd, Fuller, and Arvidson, 1997; Vanderheiden and Lloyd, 1986). Several of these are illustrated in Figure 11-5. Perhaps the most concrete type of symbol is the use of real objects (full size or miniature). However, to a person with cognitive disabilities, a miniature object may not appear to represent the full-size version, and care must be taken to ensure that the association is made by the user (Vanderheiden and Lloyd, 1986). Real objects and photographs have the disadvantage that many communicative concepts (e.g., good, more, go, hurt) are difficult to portray. Pictographic symbols include provisions for more abstract communicative intents and allow much greater flexibility in developing vocabulary usage. A more flexible symbol type is the use of a symbol system possessing grammar and syntax (e.g., Blissymbols). The nature of this symbol system allows the inclusion of more linguistic functions, such as categorization by parts of language. Traditional orthography is the symbolic representation based on letters and words. Some individuals have reading skills that exceed their spelling skills, and they cannot rely on spelling for communication. If the person has a large word recognition vocabulary, the selection set should be based on words with possible “carrier phrases” that are filled in with limited spelling (e.g., “I would like a drink of ____”). Spelling is the most flexible symbol system because it can be used to create a large number of different utterances, but it can also be the slowest because of letter-by-letter entry rather than selection of whole words. Many computers, printers, and keyboards accommodate languages other than English.
Relating Goals and Skills to Augmentative and Alternative Communication System Characteristics
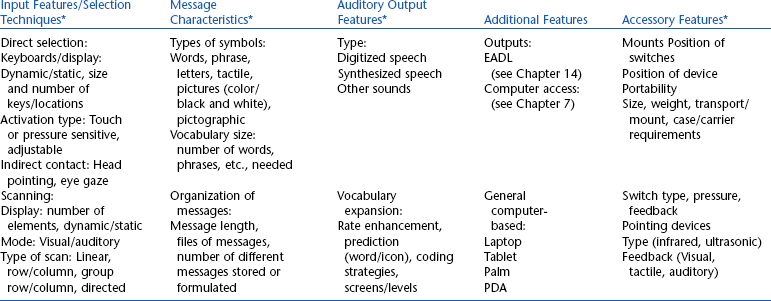
Chapter 2 describes the assessment and recommendation process in assistive technology as designing a total system for a specific person. This approach is particularly true in AAC because it is necessary to define a set of system characteristics that meets the needs of the person with CCN, is consistent with his or her skills, and will support communication across multiple partners and contexts. When an SGD is a part of the recommended AAC approach for the individual with CCN, it is important to determine a match between the needs and goals of the person and the characteristics of the SGD. Table 11-2 illustrates the relationship between assessment results and device characteristics in terms of U.S. Medicare funding guidelines for SGDs. Input features, message characteristics, output features, and accessories are all specified on the basis of the assessment results. Blackstone (2001) includes several case studies that illustrate the application of this matching process for the selection of an AAC device and the preparation of a funding justification for submission to Medicare. This type of systematic approach to recommendations allows the characteristics and skills of the individual with CCN to be matched with available SGDs.
The individual or family may wish to use the SGD for a trial period, during which valuable information can be gained. For example, the person’s interest in using the SGD may increase when he or she sees how effective it is in meeting needs or he or she may not like how it sounds or how friends react to it. A trial period can also help identify specific training goals for the person and his or her communication partners so that communicative competencies can be developed that enable the individual to interact effectively and efficiently. If there are special features that require learning new skills (such as storing and retrieving information), these may be assessed during the trial. For individuals who prefer a longer trial period, many companies will lease a device for a 1- to 3-month period. The outcomes of an SGD assessment should include recommendations for the SGD and any accessories or mounts and instructional strategies required to meet the person’s unique needs and goals.
EXAMPLES OF CURRENT AUGMENTATIVE AND ALTERNATIVE COMMUNICATION APPROACHES
The HAAT model (Chapter 2) describes activity outputs as part of the assistive technology component. AAC is the communication activity output. As Figure 11-6 illustrates, AAC systems are composed of “no-tech” (gestures, sign language) components, nonelectronic (low-tech), and electronic (high-tech) components. Not everyone uses all these approaches, but many people do.
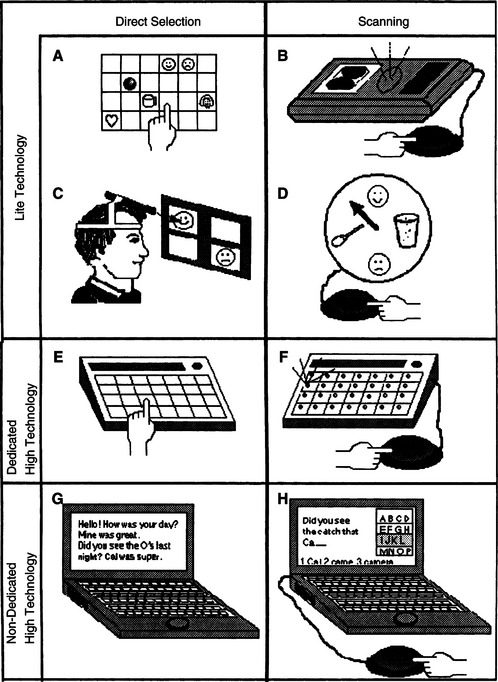
Figure 11-6 A, Manual communication display. B, Two choice voice output speech-generating device (SGD). C, Communication display accessed with a head-mounted light. D, Clock-face communication device. E, Direct selection SGD. F, Scanning SGD. G, Direction-selection laptop computer-based SGD. H, Scanning laptop computer-based SGD. (From Glennen SL, DeCoste DC: The handbook of augmentative and alternative communication, 1997, San Diego, Singular Publishing.)
Singular PublishingNo-Tech Augmentative and Alternative Communication Systems
Gestures, facial expressions, and body movements help display emotional states, regulate and maintain a conversation, and support information exchange. Formal gestural codes (American Indian, Tadoma) and formal manual sign systems (e.g., ASL, SEE) are examples of more formal approaches (Beukelman and Mirenda, 2005).
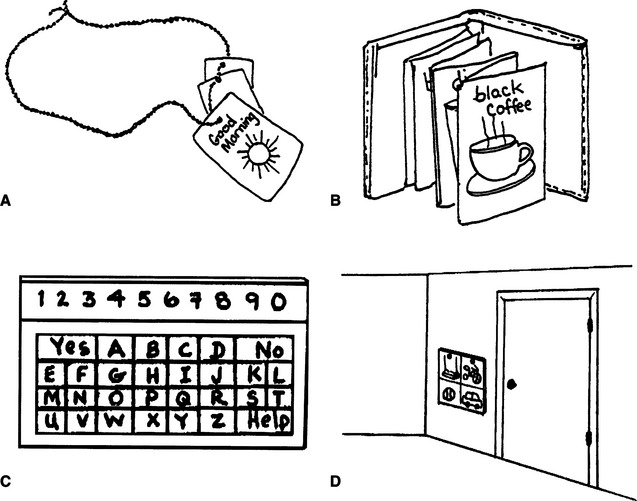
Low-Tech Augmentative and Alternative Communication Systems
Chapter 1 defined low technology as inexpensive devices that are simple to make and easy to obtain. Many types of AAC approaches fit into this category. The communication vest shown in Figure 11-7, A, is worn by a teacher in classrooms to generate eye contact and enhance interaction with students. The activity-related symbols face the child so the teacher or child can point to them as they are discussed, which can assist in the teaching of labeling, requesting, and similar skills. The communication displays shown in Figure 11-7, B and C, are based on letters/words/phrases or graphic symbols, respectively. The communication display in Figure 11-7, D, is an example of an activity-specific communication display. Other low-tech approaches may include placing symbols on items around a room to develop labeling skills, using miniature objects as labels, and formal systems such as the PECS to teach requesting, as described earlier in this chapter.
High-Tech Augmentative and Alternative Communication Systems
High-tech AAC systems typically use SGDs, some of which are based on standard computers. The salient general characteristics of these devices are described in this section.
Human Technology Interface.
The human technology or control interface for SGDs is the hardware by which the person with CCN accesses the low- or high-tech device (see Figure 2-6 and Chapter 7). The most commonly used control interfaces for augmentative communication devices are keyboards, single or dual switches, joysticks or multiple-switch arrays, and mouse or alternative pointing interfaces. SGDs; other AAC approaches use either direct selection or indirect selection (e.g., scanning, directed scanning, or coded access). These are discussed in Chapter 7. Most selection sets use visible symbols (e.g., letters, graphics, pictures) so individuals who have visual impairments and physical limitations requiring scanning may not be able to use visual arrays. For these individuals auditory scanning is used. Choices are presented in auditory form by a partner or an AAC and the user selects his or her choice from the auditory prompts. In some cases, both a prompting phrase and a selected auditory utterance are included and the user hears the prompting phrase through an earphone. In nonelectronic voice auditory scanning a list of vocabulary items is read aloud by the communication partner. The AAC user then chooses a vocabulary item by using a predetermined signal such as a vocalization to identify the desired vocabulary item. Kovach and Kenyon (1998) analyze a variety of approaches to auditory scanning, summarize current research in this area, and describe considerations to be included when developing an auditory scanning system for an AAC user.
Examples of Vocabulary Retrieval Techniques.
Many SGDs use the approaches to increase input rate that are discussed in Chapter 7 (abbreviation expansion, word prediction, word completion). In addition, there are several methods for storing and retrieving vocabulary that are designed specifically for SGDs.
Instant phrases are those used frequently for greetings, conversational repairs (e.g., “that’s not what I meant”) or similar actions; these are often included as single keystroke entries in an “activity row” or in a row of the scanning matrix, near the beginning of the scan. They can also serve as “floor holders” (e.g., “please wait while I type my question/answer.)
Coding of words, sentences, and phrases on the basis of their meanings and also known as semantic encoding or Minspeak (Baker, 1982). This approach uses pictorial representations that can have multiple meanings as codes, making recall easier. For example, when a picture of an apple is used for “food” and a sun rising for “morning.” then selection of “apple” and “sunrise” could be a code for “What’s for breakfast.” Icons can have multiple meanings. Thus the apple symbol can take on the meaning of “eat” or “red” or “fruit” rather than food. Several examples of Minspeak sequences are shown in Figure 11-8. Baker (1986) also developed an approach based on the use of syntactical labels coupled with icons. Figure 11-9 illustrates this concept. For example, the apple icon becomes “eat” when combined with the key labeled “verb” and becomes “food” when combined with the noun key. Unity is a family of Minspeak application programs included with Prentke Romich (Wooster, Ohio, www.prentrom.com) AAC devices. It includes 4, 8, 15, 32, 45, 84, and 128 location overlays that differ in the pointing resolution required by the user. Sequences of icons and their locations on the keyboard are kept as consistent as possible among the overlays to account for motor skill development while allowing growth in language usage. Versions of Unity vary from a few hundred words to more than 4000 words intended to address the core vocabulary that is responsible for the majority of conversational utterances. When large numbers of sentences, words, and phrases are stored, the icon sequences can become difficult to remember. Icon prediction initially lights an indicator associated with each symbol that forms the beginning of an icon sequence. When one of these icons is selected, only those icons that are part of a sequence light up or flash, beginning with the first selected icon. This continues until a complete icon sequence has been selected. This feature can aid recall and increase speed of selection because the device limits the number of icons that must be visually scanned for each selection.
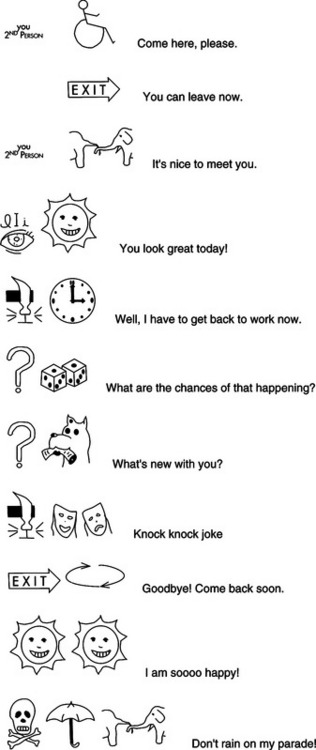
Figure 11-8 Examples of Minspeak symbol sequences. (From Romich B: Liberator manual, Wooster, OH, Prentke Romich.)
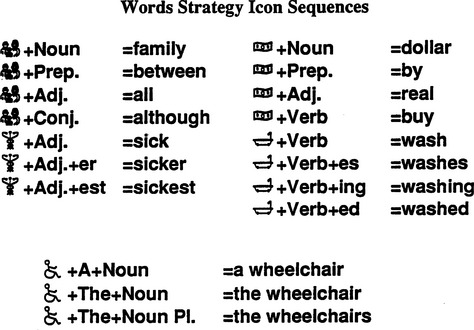
Figure 11-9 Symbols such as those used with Minspeak can be given syntactical meaning, as in this example from the Word Strategy application program. (From Liberating the power of Minspeak, Wooster, OH, 1991, Prentke Romich.)
Prentke RomichWilliams (1991), an accomplished user of numerical abbreviation expansion and word-based Minspeak, describes several advantages of this approach. In comparison to sentence-based Minspeak, he states that he (and most of the rest of us) does not think in sentences but in words or short phrases. This makes a word-based device easier to use. Second, he indicates that of the three encoding approaches in which he has achieved skill (each after hundreds of hours of practice), the word-based Minspeak “offers powerful advantages over the rest” (p. 133). His major reasons for this are the ease with which words are recalled during use and the large vocabularies that are possible with the use of icons rather than arbitrary codes. Williams also points out that it requires a large amount of practice and effort to become proficient with this type of device, which must be built into training programs. Williams also addresses the initial reluctance that many cognitively able but physically limited adults with CCN have to using pictorial representations as codes.
Examples of Vocabulary Programs for Language Development.
The Gateway (Dynavox Systems, Inc, Pittsburgh, Pa., www.dynavoxsystems.com) series is an approach to vocabulary organizations that is based on language development in typically developing children. The levels of Gateway are designated by the number of elements in the selection set, from 12 through 75. These are intended for six distinct target user groups beginning with the 12- to 24-month language development level, progressing to two formats for mild/moderate cognitive disability for children or adults, arrays for children and adolescents/adults with typical cognitive/language development and physical limitations, and a high-end array for augmented communicators who have well-developed syntactical skills. Pop-up menus with frequently used items (word, phrases, or sentences) are available on the larger arrays.
WordPower (Inman Innovations, available on several commercial AAC systems) combines a core vocabulary of 100 words that represent about 50% of spoken communication. It includes approximately 100 single hit words, hundreds of two and three hit words, a core dictionary for word prediction of 30,000 words, automatic grammatical endings (-ed, -ing, -s), and a QWERTY keyboard for spelling. For literate users, this approach is intuitive and leads to efficient communication. There are both direct and indirect (scanning) versions available. Picture WordPower uses labeled symbols as word cues. The same basic core vocabulary is available.
Conversationally based vocabulary storage and retrieval.: Vocabulary selection can be based on conversational patterns. An early approach to this technique was CHAT (Conversation Helped by Automatic Talk) based on the premise that each keystroke should produce a complete “speech act” (an utterance with a purpose) (Alm, Newell, and Arnott, 1987). The CHAT model had five sections that could be scripted in advance: (1) greetings, (2) small talk, (3) main section, (3) wrap-up remarks, and (5) farewells. CHAT also included small talk (comments and repair). CHAT also allowed the superimposition of mood on the other features: polite, informal, humorous, or angry (Alm, Arnott, and Newell 1992).
Many conversational topics are repeated. TOPIC (Text Output In Conversation), a companion to CHAT, included a database and an intelligent user interface to hold each “conversational contribution” subject descriptors (e.g., work, family, books, science), speech act descriptors (e.g., request for information, information, disclosure), and a frequency of use counter (Alm, Arnott, and Newell, 1989). For example, a conversation about work or family or a joke is often repeated in different contexts and with different communication partners.
Dye et al (1998) combined the concepts of CHAT, TOPIC, and VSDs to develop a script-based system that used a scene-based interface. Five groups of conversational categories were included: I’m listening (“uh-huh”), openers (greetings, responses, small talk), closers (wrap-ups, farewells), feedback (comments), and control (repair of breakdowns) and were automatically presented to the user to match the flow of the conversation. Scripts can be organized in a predictive fashion as well. One example presented was a physician’s office picture in which the user can click on an icon representing the receptionist to introduce himself or herself and indicate that he or she uses an SGD. The display then highlights the appointment book picture to request an appointment. The rest of the conversation is similarly scripted. These concepts have been implemented in several commercial AAC devices.
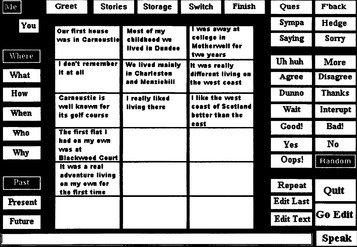
TALK (Todman, 2000) is an extension of CHAT and TOPIC based on the perspective of a typical conversation: person (me/you), queries (where, what, how, who, when, why), and tense (present, past, future). Figure 11-10 shows a typical TALK board with “where me/where/past” perspectives selected. This leads to the display of a particular set of phrases that can be chosen and spoken with one switch selection. There are also a set of comments, repair phrases along the right side, and the conversation sections similar to CHAT along the top. These may be randomly spoken, as in CHAT, or the user may choose which phrase to use. The bottom of the screen has an area for letter-by-letter text entry. Using TALK and similar systems, the AAC user can obtain conversational rates of 30 to 60 words per minute. One version of TALK is available with Speaking Dynamically Pro (Mayer Johnson, Solana Beach, Calif., www.mayer-johnson.com). When individuals who have limited experience with conversations are introduced to systems such as TALK, significant training specifically oriented toward conversational flow is required (Todman, 2000).
Frame Talker (Higginbotham et al, 2005) is an AAC approach that allows the selection of natural language utterances by using a schematic format that represents the situational structure of communication events. The situational structure of communication events is represented by a communication frame. Frames can be used to semantically and functionally organize related conversational utterances. A communication frame consists of component frames, utterance constructions and lexical fields, a topic domain, and a frame hierarchy. The communication frame can be viewed as an utterance-based augmentative communication device designed to enable a person with CCN to communicate quickly and effectively. The internal structure of a communication frame consists of component frames and utterance constructions. Component frames uniquely identify typical subtopics or distinct situational portions within the larger communication frame (e.g., “severity” versus “cause” of pains) with utterance constructions located within them. A potentially large number of different utterances can be generated by each utterance construction in combination with its associated lexical field (i.e., group of semantically related terms). Topic domains are organized as clusters of individual communication frames that share similar generic topic interests.
Augmentative and Alternative Communication System Outputs.
Dynamic communication displays create greater flexibility in selection sets by changing the selection set displayed when a choice is made, as shown in Figure 11-11. For example, a general selection set may consist of categories such as work, home, food, clothing, greetings, or similar classifications. If one of these is chosen, either by touching the display surface directly or by scanning, then a new selection set is displayed. For example, a variety of food-related items and activities (eat, drink, ice cream, pasta, etc.) would follow the choice of “foods” from the general selection set. The symbols on the display can be varied, and this changes the targets for the user. Because each new selection set is displayed, the user does not have to remember what is on each level. This approach, illustrated in Figure 11-12, also avoids having to squeeze several pictures into one square on a static display. It also relies on recognition memory rather than recall for identification of the selection set elements, which can make it easier to use. A dynamic passive display requires the user to select the next page to be displayed. The dynamic active display automatically branches to the selected new page once the item is selected.

Figure 11-11 Dynamic display devices are often accessed with touch screen interfaces, making them accessible and providing a cognitively concrete user interface. (Photo courtesy Dynavox.)
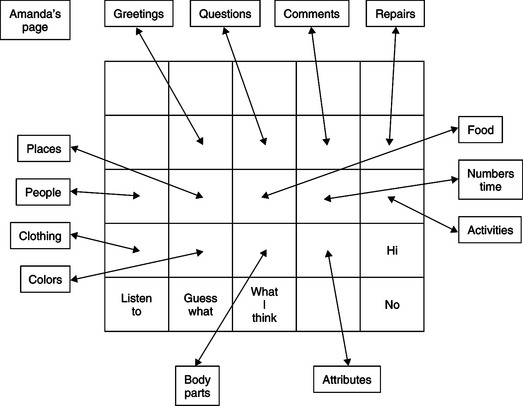
Figure 11-12 Dynamic display devices change the selection set presented to the user each time an entry is made.
Two types of dynamic displays were used in a matching task in a case study of a 16-year-old girl with a severe cognitive disability who had several years of experience in using fixed and dynamic displays (Reichle et al, 2000). There were no differences in accuracy of the matching tasks between the three types of display for a small number (15) of symbols. However, as the number of symbols increased (to 30 in dynamic and 60 in passive) the dynamic active display was significantly better than the other two. The response time was fastest for the passive display because all possible choices were displayed at once.
Blackstone (1994) describes a number of key features of dynamic displays. The nature of these devices allows the user to quickly change the screen and to configure the size, color, and arrangement of the symbols to match the topic. Dynamic displays reduce memory requirements because the user is prompted by the display after each choice. The constant vigilance to the screen requires a high level of visual attention and constant decision making. The user must also have mastered the concept of object permanence (Chapter 3). These may be challenging for some individuals who have cognitive limitations.
Visual scene displays (VSDs) take advantage of the graphical user interface (see Chapter 7) to create displays that capture events in a person’s life on the screen with “hot spots” that can be accessed to retrieve information (Blackstone, 2004). They also offer the AAC user and his or her partner a greater degree of contextual information to support interaction. The richness of the display and the information content also enables communication partners to participate more actively in a conversation. VSDs may represent either a generic or personalized context. The former includes drawings of places (e.g., house, schoolroom), whereas the latter is specific to user (e.g., a picture of his house, a family outing). Table 11-3 illustrates the difference between a traditional AAC display (referred to as a grid) and a VSD (Blackstone, 2004). The traditional grid supports communication of needs and wants and information exchange well. This type of display is usually restricted to symbols, text, or static drawings (although some animation is used with dynamic display items) and the vocabulary items are separated from any context to maximize their versatility. Figure 11-13 illustrates the differences between a typical grid display and a VSD (Blackstone, 2004). Personalization is also limited. The VSD is developed for conversational support as a shared activity. Because it uses a range of information media, including video and family pictures in addition to text, symbols and line drawings, it can be highly personalized, as shown in Figure 11-14 (Blackstone, 2004). In addition to communication of needs, wants and information exchange, VSDs also support social closeness. Because of the dynamic nature of the VSD approach, it can also serve as a learning environment. VSDs can stimulate conversation between interactants in which they play, share experiences, and tell stories. The dynamic nature of VSDs facilitates active participation of interactants during these shared activities. VSDs can also provide instruction, specific information, or prompts to help the user interact effectively. The populations expected to be served by VSDs are those with cognitive (e.g., Down syndrome) or language (e.g., aphasia, autism) limitations.
TABLE 11-3
Comparison of Visual Scene Displays and Traditional Grid Displays
| Variable | Typical AAC Grid | VSD |
| Type of representation | Symbols, TO, line drawings | Digital photos, line drawings |
| Personalization | Limited | High |
| Amount of context | Low | High |
| Layout | Grid | Full or partial screen, grid |
| Display mgmt | Menu, pages | Menu pages, navigation bars |
| Concept retrieval | Select grid space, popups | Hotspots, speech key, select grid space |
Based on Blackstone S: Visual scene displays, Augment Commun News 16:1-5, 2004.
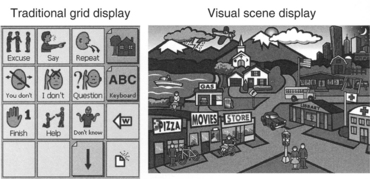
Figure 11-13 Visual scene display versus grid. (From Blackstone S: Visual scene displays, Augment Commun News 16:1-5, 2004.)
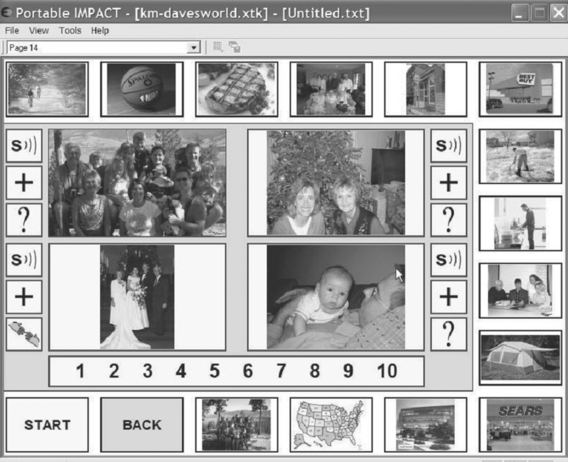
Figure 11-14 VSD layout for family outing or wedding (personalized). (From Blackstone S: Visual scene displays, Augment Commun News, 16:1-5, 2004.)
Young (2½ years old) typically developing children did significantly better at a birthday party communication task when using a schematic VSD layout (based on activities) than when using a grid layout (schematic or taxonomic) (Drager, 2003). One explanation is that the provision of a more meaningful context in the VSD reduced the language demand on the child. The VSD was organized around scenes of rooms: living room (arrival of children for party), kitchen (eating cake), family room (opening presents), and playroom (playing games); this reduces the demands on the child’s working memory because the location of the item required fewer demands on the VSD. The grid was organized around the activities, which required more language processing by the child (e.g., categorizing, remembering the symbols). For example, the topic of play could be illustrated by a digital photograph of the child’s room including the toy box in the VSD and as a symbol for play on the grid. Clicking on the hot spot associated with the toy box in the VSD or on the grid element for play resulted in branching in both formats to more detailed information.
Speech Output.: The two major types of speech output use in SGDs are digitized and synthesized. These are both described in Chapter 7. Speech output allows use with partners who cannot read (e.g., small children or cognitively impaired persons). It is also the only type of output that can be used conveniently for speaking to groups (including use in classroom discussions) or speaking over the telephone (unless both the user of the device and the partner each have special TTY equipment; see Chapter 9). Typical additional outputs that are available on AAC devices are printers, computer access, and electronic aids to daily living (EADL) (primarily appliance control). These are discussed in Chapters 7 and 14, respectively.
Access to Mainstream Technologies.
Specialized assistive technologies such as EADL (Chapter 14) and power wheelchairs (Chapter 12) are also often of use to individuals with CCN. Many SGDs either provide the functions of EADL or interface with them through wireless connections. The use of an SGD interface to control a power wheelchair is a common application as well. The real power in connecting people with CCN to the rest of the information society lies in access to mainstream technologies. This includes entertainment (e.g., DVD, CD players) and other electronic devices such as electronic games. However, two technologies with enormous potential to create greater connectivity for people with CCN are the Internet and the cell phone.
Internet access.: The Internet provides significant resources from the computer desktop. Quick, easy, and low-cost communication with individuals around the world is routine by use of e-mail. Many people who have disabilities use e-mail to communicate with friends, business associates, and organizations (see the case study of Heidi). Many individuals with CCN access the Internet with their SGDs. Any stored vocabulary or special access methods are available for use while on-line. Some commercial SGDs are actually portable computers with AAC software that can also function as Internet workstations. The Internet also provides access to information through company, organization, and individual Web sites (see Resources, page 556) By accessing this information, AAC users can learn about new technologies, conduct business independently, carry out research for academic pursuits, book airline reservations, and many other activities. Access to the Internet can provide many opportunities for reading and writing, and this can have a positive impact on literacy skills for AAC users (Blackstone 2003c). It is also used to train mentoring individuals who rely on AAC as demonstrated by 2 weeks of intensive training at Temple University (http://disabilities.temple.edu/programs/assistive/aces/index.htm) and 1 year of follow-up through the Internet. Program graduates now mentor new students in the program. The benefits of using the Internet are not available to everyone. Those without an Internet connection or the ability to use an SGD and those who are not literate, however, can still depend on friends or family to support their participation by reading Internet content (e-mails, Web sites) and typing responses on the basis of input from the AAC user (e.g., using symbols or pictures). However, this strategy has implications for the privacy of the user.
AUGMENTATIVE AND ALTERNATIVE COMMUNICATION IN POSTSECONDARY EDUCATION
Heidi (Figure 11-15) is a doctoral student studying English at a major university. She has cerebral palsy, bowhich limits her ability to speak and to use her hands for writing. She uses her computer to complete writing assignments and has written two plays (one for her master’s degree thesis) and one book for teenagers who have cerebral palsy. She uses her notebook computer with a speech synthesizer for conversation and a word processor for writing. She also uses e-mail to communicate with her PhD thesis advisor, colleagues, students, and friends. This technology allows her to keep in touch with people without the use of the telephone, which is difficult with her AAC device. Her computer system allows her several modes of communication, as well as providing the opportunity for her to work at home much of the time and avoid the hassles of special transportation arrangements. Her e-mail contacts also prevent her from being isolated in her home environment.

Figure 11-15 Access to the Internet provides Heidi with the tools necessary to pursue her PhD. She contacts her professors and students by e-mail, conducts literature searches over the Internet, and participates in Web-based courses and discussion groups. This access is all obtained with the same laptop computer that she uses as an AAC device in face-to-face conversations.
E-mail allows composition at a slower speed because the recipient reads it at a later time (Blackstone, 2003c). E-mail also allows an AAC user to communicate with another person without someone else being present. Because the person’s disability is not immediately visible, AAC users report that they enjoy establishing relationships with people who experience them first as a person and then learn of their disabilities.
Internet chat rooms where people who have common interests can exchange information in a real-time format can help AAC users establish advocacy groups, share information, and engage in leisure pursuits. Listservs, which consist of a group of individuals with common interests but are more like bulletin boards, also provide rich sources of information and friendly interaction. A popular AAC listserv is ACOLUG hosted by Temple University.
Cell Phones.: Issues facing people with CCN in accessing cell phones are very similar to those faced by individuals who have low vision or blindness (see Chapter 8). Four changes in cell phone technology described in Chapter 8 will increase access: (1) increased processing power, (2) ease of downloading into the phone, (3) wireless connection to a worldwide network, and (4) low cost and reachable by persons with disabilities because these features will be built into standard cell phones (Fruchterman, 2003). The move away from proprietary software to an open source approach, much like personal computers of today, will lead to greater diversity of software for tasks such as text-to-speech output, voice recognition, and downloadable user profiles that allow customization for a particular activity or task. For example, a specific stored vocabulary, word prediction/completion list, and key word index for text messaging could be resident on the Internet and downloaded as needed. Because the operating system will be open source, many applications for people with CCN can be downloaded from the Internet. An additional advantage is that features such as speech synthesis will be useful to individuals who are blind as well as to those with CCN, so the number of potential customers for software developers will rise and the cost of applications will fall. Features that were developed for people with disabilities (e.g., word completion/prediction, voice recognition, abbreviation expansion) are also being found to be useful for the general public. This will further increase their availability to individuals with CCN. Digital photography built into cell phones also increases utility for persons with CNN. In addition to the mainstream use (i.e., photography for recording family events, business, or school), the camera features can be used as an additional AAC option, reducing the descriptive information required to convey a message.
Configurations of Commercial Speech-Generating Devices.
To describe current SGDs, we have created seven categories of the major commercially available devices, shown in Table 11-4. The categories reflect different groupings of the characteristics discussed earlier in the section on AAC characteristics as well as the funding codes and categories for Medicare reimbursement of SGDs in the United States (Blackstone, 2001). Table 11-4 also includes accessories and mounting systems for AAC devices. We have opted for a few large categories on the basis of the most essential features, resulting in variability within each category. The format in Table 11-4 appropriately groups devices serving distinct populations. Within each category there is still significant opportunity for decision making that is based on a thorough assessment of skills and needs. The commercial devices listed in each category are examples and, although a variety of manufacturers, models, products, and varying device features are included, Table 11-4 is not inclusive.
TABLE 11-4
Feature Categories Commonly Combined in Commercial Augmentative and Alternative Communication Systems
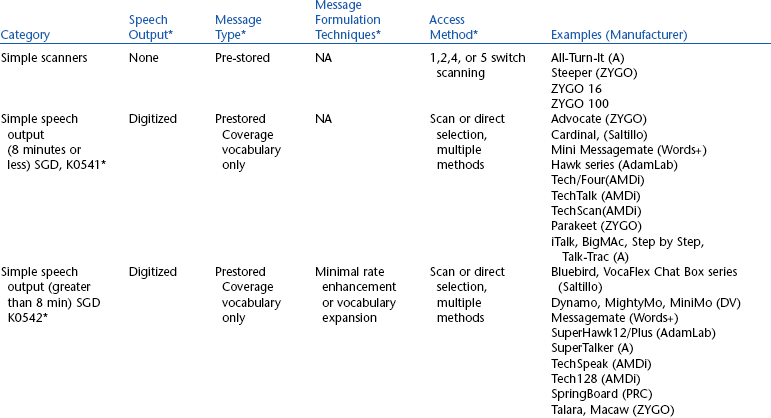
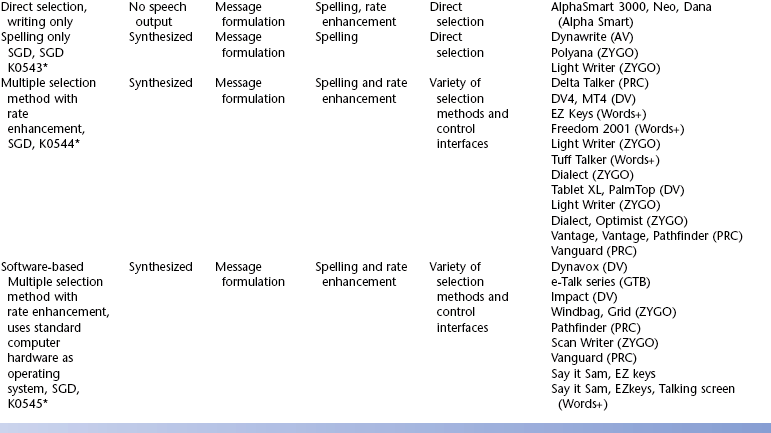

A, Ablenet; ACS, Adaptive Communication Systems; DJ, Don Johnston Developmental Systems; DV, Dynavox; IC, Innocomp; PRC, Prentke Romich Co., D, Daessy, GTB, Great Talking Box Company.
*Categories, funding codes and features included in U.S. Medicare funding for “speech-generating devices”; elements adapted from Blackstone S: Assessment protocol for SGDs, Augment Commun News 13:1-16, 2001. Note: restrictions on software options required for Medicare funding.
†Vary by manufacturer; examples shown.
Simple scanners, the first category in Table 11-4, are generally operated by a single switch, although some can have dual-switch scanning and others allow four- or five-switch directed scanning. The devices in this category are distinguished by the use of a light to indicate the output selection, very limited vocabularies (32 items or less), no rate enhancement or vocabulary, and the general absence of voice output as a standard feature.
The devices categorized as simple speech output are further delineated by length of recorded digital speech. They were all developed to provide a limited-vocabulary, easy-to-use output for very young children or individuals with limited language abilities. In general, they require direct selection, but some also allow scanning. Rate enhancement in this category varies from none, to levels, to simple codes or key sequences. Vocabulary storage varies from a low of a few seconds to several minutes.
The devices in the direct selection, writing only category are distinguished by their small size and focus on features that support writing. Some may have a built-in printer. Several devices in this category provide direct file transfer to a desktop computer, and several also have rate enhancement (generally abbreviation expansion, instant phrases, or word completion).
The devices in the spelling only SGD category are primarily distinguished by their dependence on spelling for message formulation. They also generally are a small size and use direct selection through a keyboard or touch screen.
The last two categories in Table 11-4 represent the highest level of sophistication in currently available devices. They incorporate all the rate enhancement approaches discussed in Chapter 7. Those in the multiple selection method with rate enhancement category are based on SGD hardware that is specifically designed for AAC. The devices in the last category are software applications that are designed to run on general-purpose computers such as laptops, tablets, or PDAs. Vocabulary storage capacity varies from a few hundred utterances to thousands of utterances. Interaction with other devices (e.g., computers, Chapter 8; power wheelchairs, Chapter 12; or EADLs, Chapter 14) and peripherals such as printers is possible for most of the devices in this group using either serial or parallel ports (generally USB). Within these two categories are devices that can meet the needs of a variety of consumers, from very young children who cannot spell to quantum physicists who make full use of sophisticated rate enhancement techniques. In some cases the same device can serve a wide range of needs because the software and vocabulary stored can be customized. In other cases the devices are relatively inflexible.
Devices in the last two categories provide great flexibility in control interfaces and selection methods. Several of the direct selection types allow both standard size and expanded or contracted keyboards as control interfaces. Several devices in these two categories allow scanning with single-switch or four- or five-switch directed scanning. Some also provide both one- and two-switch Morse code, and some provide direct selection by head pointing. For direct selection by head pointing, some devices use light pointers or sensors attached to the head, whereas others use reflective systems requiring the attachment of only a reflective dot. Some light pointers can also be held in the hand.
The flexibility provided by devices in these categories is particularly useful in dealing with degenerative diseases such as ALS. Initially a person may use direct selection with the hand. As this ability is lost, direct selection by head control is feasible. However, because the device has not changed, the stored vocabulary, rate enhancement strategies, and operational characteristics of the device remain the same. If direct selection by head control becomes impossible, scanning or Morse code can be used. Once again the device is not changed, and the vocabulary, rate enhancement, and operational features remain the same. This is a great advantage over having to learn a new device at each stage of the disease.
What distinguishes the last two categories is the hardware platform. The human/technology interface may use either a static or dynamic display with a variety of ways in which each of these user interfaces is implemented on the various devices listed in Table 11-4. The devices in this category allow for a variety of physical and cognitive skills on the part of users.
In summary, the categories shown in Table 11-4 are intended to provide a rough framework with which to view SGDs. It is important for the ATP to remain current regarding technologies. One of the easiest ways to do this is to attend conferences that feature assistive technologies. If the ATP will be charged with making recommendations for AAC systems and approaches, it is also important to have his or her name placed on the mailing lists for the manufacturers of these devices. Most SGD manufacturers also maintain home pages on the Internet. There are several Web sites that provide links to SGD manufacturers.
IMPLEMENTATION OF AUGMENTATIVE COMMUNICATION SYSTEMS
As discussed in Chapter 4, in the total process of delivering assistive technologies, the recommendation of a communication device based on a formal assessment is only the beginning of the process. Once funding is obtained and the device is procured, implementation begins. Other steps that may be required include customization to integrate components from different manufacturers (e.g., a communication device from one manufacturer and a control interface from another), programming of a device to include vocabulary specific to the individual consumer, fitting of the device to the consumer’s wheelchair, and mounting a control interface in an accessible location. It is impossible in one chapter to cover all the issues related to AAC implementation. Beukelman and Mirenda (2005); Beukelman, Yorkston, and Dowden (1984); Kraat (1985, 1986); Musselwhite and St. Louis (1982); and Riechle, York, and Sigafoos (1991) are sources rich in practical information and case studies related to AAC implementation. There are also frequent case studies presented in journals such as Augmentative and Alternative Communication and newsletters such as Communication Matters and Augmentative Communication News. These case studies vary from anecdotal reports written by individual who use AAC devices or those working with them. They include formal case studies and single-subject research designs. This section discusses the most basic considerations related to training and follow-up. It is important to note that things do not always progress smoothly through the implementation phase. Fields (1991) presents a case study indicating the steps that one family went through to implement an AAC system for their son. There is also a listserv for those who rely on AAC at http://listserv.temple.edu/archives/acolug.html.
Vocabulary Selection
AAC is unique among the needs served by speech-language pathologists in that the vocabulary must be supplied by the clinician or the individual with CCN. It is not “built-in” cognitively. Once an AAC system is selected for an individual, it is necessary to create an initial vocabulary set for programming into the device or for use on a nonelectronic system. The conversational categories shown in Table 11-5 provide a useful framework for initial vocabulary selections.
TABLE 11-5
Categories to Be Included in Conversational Augmentative and Alternative Communication Systems
| Category | Sample Vocabulary |
| Initiating and interaction | Hey, I’ve got something to say. |
| Check this out. | |
| Come talk to me. | |
| May I help you? | |
| Greetings | Hello, I’m pleased to meet you. |
| Where have you been? I’ve been waiting forever. | |
| What’s happening? | |
| Response to greetings | I’m fine. |
| Great, how are you? | |
| Not so hot, and you? | |
| Requests | I’d like a __________. (object, |
| event) | |
| I’d like to go to __________. (place, event) | |
| Information exchange | What time is it? |
| I have a question. | |
| The concert begins at 8 PM. | |
| Commenting | I agree (disagree). |
| What a great idea! | |
| Uh-huh. | |
| OK. | |
| Wrap-up/farewell | Well, gotta go. See you later |
| Bye, nice talking to you. | |
| Conversational repair | Let’s start over. |
| That’s not what I meant. | |
| You misunderstood me. |
Several categories of messages are used by people who rely on AAC (Beukelman and Mirenda, 2005). Conversational messages begin with greetings and then often involve small talk as a transition between the greeting and information sharing; small talk often uses scripts for initiating and maintaining conversations. In general, SGDs do not support small talk well. Generic small talk can be used in different conversations with different people and includes topics such as “How is your family?” “What’s happening?” “Isn’t that beautiful?” “Good story!” and “She is great.” Specific small is more focused: “How is your wife?” “What are you doing?” “That is a beautiful flower,” “Good story about your vacation,” and “She is a great teacher.” A common form of conversational interaction for adults, particularly older adults, is story telling. Stories entertain, teach, and establish social closeness. An important role for the ATP or AAC facilitator is to assist those who rely on AAC to capture stories and assist with programming the device (e.g., to replay one sentence at a time to allow the pace of the story to be controlled by the individual).
Vocabulary needs vary by the context, communication mode, and individual characteristics. Beukelman and Mirenda (2005) compiled a composite list of 100 most frequently used words for a variety of categories including age and gender. Preliterate individuals require a coverage vocabulary to communicate essential messages. Because generation of novel utterances by spelling is not possible, the AAC team must ensure that as many messages as possible are stored in the device for easy retrieval. The specific vocabulary is highly dependent on the individual’s needs. Most often, the coverage vocabulary is organized by context with separate displays or pages for different activities. Preliterate individuals also need a developmental vocabulary that includes words and concepts that are not yet understood. These are selected on the basis of their educational value, not for functional purposes, and they encourage language and vocabulary growth. New words can be added around special events or activities, especially when an activity is to be experienced for the first time (e.g., going to the circus). The developmental vocabulary also encourages the use of different language structures reflecting semantic categories.
Required vocabulary resources for literate individuals include a core vocabulary that is used with a variety of situations and partners and occurs frequently. There are word lists based on successful general patterns, the needs of a specific individual, and the performance of natural speakers or writers in similar contexts (http://aac.unl.edu/). A list of 500 words covered 80% of total utterances for individuals who are operationally and socially competent with AAC systems (see training section of this chapter) (Beukelman and Mirenda, 2005). Words and messages that are unique to the individual are included in a fringe vocabulary that includes names of people, places, activities, and preferred expressions. This approach personalizes the AAC system by complementing the core vocabulary list. The fringe vocabulary content is often identified by family and friends as well as the individual. The initial items are those that are of high interest to the user and have potential for frequent use. It is important to include items that denote a range of semantic notions and pragmatic functions. To ease learning, the vocabulary should reflect the “here and now” and have potential for later multiword use. Ease of production by the individual and interpretation by the partner is also essential.
Environmental inventories are another form of identifying vocabulary. Some formal procedures for these are available (Beukelman and Mirenda, 2005). These inventories document the individual’s experiences by noting precipitating events and subsequent consequences. The documentation includes words used by peers with and without disabilities. The identified pool of vocabulary items is reduced to a list of most critical words that the individual can manage. Communication diaries and checklists are records of words and phrases needed by an individual for AAC that are kept by informants such as family members. There are some published lists that can also act as a shortcut to vocabulary selection (Beukelman and Mirenda, 2005).
Yorkston et al. (1988) studied 11 vocabulary lists compiled from various sources. They found that most lists were unique because they contained mostly content words (those related to a specific topic) rather than function or structure words (e.g., articles, pronouns, conjunctions). The authors also compiled these 11 lists into one large list that can be used as a starting point for developing individual vocabularies for AAC devices. This list was then applied to a case study to illustrate the process of selecting vocabulary for a person who cannot read and is severely physically disabled (Yorkston et al., 1989). The list developed for this person contained words that were not on even the largest of the 11 lists of the earlier study. This finding indicates how unique the needs of each individual are. Beukelman, McGinnis, and Morrow (1991) describe the factors that need to be considered in selecting vocabulary for AAC devices. These include the need to have vocabularies for different contexts (e.g., small talk, school, and home) and considerations regarding acceleration vocabularies versus coverage vocabularies. They also analyze the factors that differ in developing AAC vocabularies for individuals who can spell (and therefore have access to a large vocabulary with only the alphabet) and those who cannot spell (and who need a large coverage vocabulary).
Participants in adult programs (day care and residential) who have learning disabilities have unique needs for vocabulary (Graves, 2000). The vocabulary needs of this population differ from those of typical adults or children (with or without disabilities). With use of diaries compiled by staff working with adults who needed AAC, more than 80% of the conversational topics were functional (e.g., physical needs and daily activities) for those with the most severe disabilities. For individuals with more moderate disabilities, the percentage of functional topics was twice that of physical needs. Emotional (feelings of anger, anxiety, fear, love) amounted to only 3.4% of all topics. Possible reasons for this low response may relate to the cognitive difficulties in expressing feelings and to cultural factors that limit the degree to which staff are able to provide emotional support to residents. These results differ from standard vocabulary lists in content and emphasis, and they reinforce the need for care in applying standardized vocabulary lists to AAC vocabulary selection.
Because most AAC devices are programmable, it is possible to continually add or amend vocabulary as needs change. The choice of additional vocabulary items is generally made on the basis of needs that occur frequently; input from family, care providers, and other communication partners and new situations that arise. In the majority of cases, vocabulary development (after the initial set is implemented) is relatively slow and occurs over a long period. Some devices (e.g., word completion or prediction systems) automatically add items to the stored vocabulary on the basis of the frequency of use.
Beukelman and his colleagues and students at the University of Nebraska at Lincoln have compiled a large number of resources relating to vocabulary selection and messaging in AAC. This information can be accessed through their Web site (http://aac.unl.edu/vbstudy). Included in this resource are core vocabulary lists consisting of high-frequency words for preschool and school-age children, young adults, and older adults. They also include unabridged vocabulary lists (with use statistics) for nondisabled persons (20- to 30-year-old adults, older adults, and preschool children) and AAC users (four volumes). Vocabulary lists of small talk for children and adults, as well as context-specific messages suggested by AAC specialists, are also included. This site also provides vocabulary lists for school settings (preschool activities and classroom activities). Finally, vocabulary lists for use as initial recommendations in AAC are reported, as are references for AAC messaging and vocabulary selection. This site is a rich source of information for the ATP charged with developing vocabulary for individuals who use AAC.
Physical Skill Development
AAC devices require physical skill, whether direct selection or scanning, to operate them effectively. It takes practice to develop this skill, and it can be useful to separate the physical skills required for the use of an augmentative communication device from the communication skills required. This aspect of training is described in Chapter 7.
If the individual has insufficient motor skill to make reliable selections but is expected to develop the necessary motor control, it is important that this physical competence be developed separately from the use of the physical skill for communication. If the ATP attempts to teach motor skills by using the communication device, it is possible that errors in selection caused by lack of motor skill will be misinterpreted as lack of communicative skill; for example, the person may have intended to select the picture of the apple (signifying “eat”) but missed the mark and selected the picture of the cup (“drink”). Conversely, errors caused by communication or language inability may be interpreted as motor selection difficulties. In the previous example the person may have been capable of physically choosing apple but chose cup because he or she did not understand either the question or the communication task.
Training System Use: Developing Communicative Competence.
Figure 11-16 shows a completed installation of an SGD. When the installation is completed, the individual and those working with him (e.g., care providers, family, teachers, employers, therapists, and speech-language pathologists) can begin the process of learning to use the device. Depending on the complexity of the device and the sophistication of the features included, this process can take from a few hours to several months.

Figure 11-16 Implementation of an AAC system includes proper mounting of the AAC device and control interface to the wheelchair if necessary. Here is a completed installation ready for checkout.
The development of communicative competence is most effective when a comprehensive program is used. One such approach is the System for Augmenting Language (SAL) (Sevick, Romski, and Adamson, 2004). SAL involves a multimodal approach to training of individuals who rely on AAC, their partners, and continuing follow-up. Sevick, Romski, and Adamson (2004) illustrate the application of SAL through a case study of a preschool child who used both a VOCA and a manual display consisting of PCS symbols. For young children with cognitive and language disabilities, the development of both expressive and receptive vocabulary can be developed by using a VOCA in an exercise to teach requesting (Brady, 2000). Children were taught to request objects using PCS symbols on a VOCA. After learning these symbols, the children’s comprehension was evaluated. The use of the VOCA during the labeling instruction appeared to increase later comprehension of the symbols.
Scripts that are programmed into an AAC device can be used in a training paradigm. One formal approach is called “Script Builder” (Linda J. Burkhart, Eldersberg, Md., www.Lburkhart.com). The scripts are a way of training individuals to achieve greater social competence and more effective interactions. The scripts are coplanned and oriented toward the development of social closeness by encouraging social purposes and a sense of belonging. Typical topics of trivia, sports, gossip, hanging out, and “who’s cute” allow the individual to display aspects of his or her personality through humor, teasing, whining, and joke telling. Scripts change perceptions of individuals who use AAC because greater social competence is evident. Some scripts focus on information content, others on conversation scripts (new information plus social closeness). Example scripts are shown in Box 11-3. There are three roles in the training: the individual who is developing AAC skills, his or her partner, and a “prompter” who prompts only when necessary in an unobtrusive way. The partner’s role is communicating as naturally as possible, pausing when necessary, and not prompting at all. All social scripts start with a greeting and include a range of communicative functions such as positive and negative comments, teasing, and questioning. They provide for multiple turns and use topic maintainers like “tell me more.” They need to be designed to ensure that the individual doesn’t get “backed into a corner.” The vocabulary chosen is appropriate to the individual’s age and setting and personality.
Communicative competence depends on many factors (Light, 1989). The context in the HAAT model affects competence in several ways. The partner and his or her skill in listening, the environment of use, and cultural factors all contribute to or detract from communicative competence. The degree of competence is also variable, and complete mastery of an AAC device is not necessary to have functional communication interactions. Light (1989) describes four areas of competence required for successful use of AAC devices: (1) operational, (2) linguistic, (3) social, and (4) strategic.
Operational competence requires the physical skills described earlier and an understanding of the technical operation of the AAC device. Once again, the degree of operational competence can be quite variable, from very basic operation to advanced features. An AAC device is like a musical instrument that can be played by an accomplished AAC communicator. Operational competence includes the cognitive demands dictated by rate-enhancement techniques. Training operational competence requires a systematic introduction of technical features, coupled with ample opportunities for practice in their use, as shown in Figure 11-17. The individual’s facilitators must also be trained in certain operational features of the device (e.g., battery charging, connecting control interfaces), even though they will not develop the same level of competence as the individual.

Figure 11-17 Development of operational competence with an AAC device requires a structured training program in which the device features are carefully explained and skill in their use is developed.s
The second phase, basic operation, includes how to connect the device to the control interface, how to charge batteries, how to attach it to a wheelchair, how to add vocabulary using rate-enhancement techniques (e.g., codes), and an introduction to troubleshooting in case the device fails to operate properly.
The last features to be introduced are those related to storage of new vocabulary, input acceleration techniques, and vocabulary manipulation features such as text editing and reformatting the output. Often the first two phases are accomplished in one session. However, in some cases, they may require multiple training sessions, and the process is often a lengthy one that may be integrated with the other aspects of training in communicative competence.
Linguistic competence requires that the symbol system and rules of organization be understood by the individual using the AAC system. As Light (1989) points out, the individual often must be competent in two languages: the spoken language of the community and the language of the AAC device. It is likely that the individual also lacks models of proficient use in the language of the device. Development of competence in this area may require many hours of practice. Often this practice is built around a functional reading task, such as that shown in Figure 11-18.
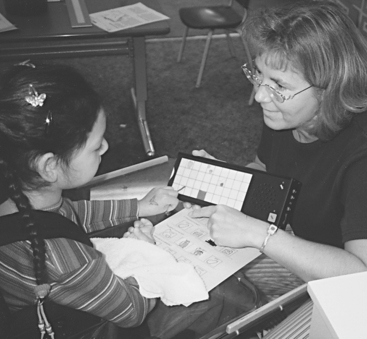
Figure 11-18 Development of linguistic competence is often taught in conjunction with other functional tasks, such as the one shown here.
In contrast to the typical “drill and practice” approach to developing vocabulary and AAC use, Mirenda and Santogrossi (1985) used a prompt-free strategy to teach a young child to use a picture-based communication board. The approach involved a four-step process, which began with a picture of a soft drink being available to the child during her regular therapy session. A drink was visible to her, as was the picture of the drink. The child was not told that touching the picture would result in her getting a drink, nor was she prompted in any way to touch the picture. If she touched the drink directly, she was told that she could have some later. If she accidentally or deliberately touched the picture, she was immediately given the drink with the explanation, “Yes, if you touch the picture, you may have the drink.” Once the deliberate response had been established over several sessions, Mirenda and Santogrossi proceeded to shape the pointing behavior by progressively moving the picture farther away, until it was out of sight and the child had to actively find it. As the child became proficient in this task, the number of pictures was increased to four and the process repeated for the other choices. Eventually the child was able to generalize to a language board of 120 pictures. The advantage of this approach is that the child learns the meaning and significance of the symbolic representation by discovery rather than by drill, which leads to greater generalization and more functional use of the AAC system.
Many people who use AAC devices have little or no experience in social discourse. Even individuals who have used natural language for communication and who have sustained a disease or injury are faced with a very different mode of interaction when an AAC device is used. Rules of conversation are altered, and the perception of the individual by his or her communication partners is different. To be socially competent, the individual must have knowledge, judgment, and skills in both sociolinguistic (e.g., turn taking, initiating a conversation, conversational repair) and sociorelational areas (Light, 1989). The latter term describes the understanding of interaction between individuals. The effective communication device user is described (Light, 1988) as having a positive self-image, interest in his or her partner, skill at drawing others into the conversation, ability to put a partner at ease, and active participation in the conversation. These are sociorelational skills, and the degree to which they are understood and used is one measure of social competence. These skills are best taught in the contexts in which they are to be used. One example of such training is shown in Figure 11-19, in which the child is being taught strategies for interacting with an adult partner. Self-determination is difficult for people who rely on AAC (Collier, 2005). They must know what they want, know how to get it, and have a sense of self-worth. To achieve these goals, they need the “language of negotiation” and negotiation skills that require transactional language to supplement requesting, information exchange and conversational control vocabulary and skill. Without these skills, individuals who rely on AAC are dependent on others for the determination of their life goals and direction. They also need these skills to avoid abuse and harassment by care givers and others or to report incidents if they do occur.

Figure 11-19 AAC users need to learn about conversational conventions and strategies. Training of these skills is often done in simulated situations. Here an aide is teaching the child how to use her AAC tools to interact with another adult partner.
Every person who uses an AAC system develops strategies to make that use more effective. Examples include letting the partner guess the next letter on a spelling board and using gestures (e.g., waving to indicate that a misunderstanding has occurred) in conjunction with an electronic device. Strategic competence describes the degree to which the person is able to develop adaptive strategies to make the most of the system. These may differ in different contexts. For example, a child’s speech may be better understood at home than at school. He or she will rely on the electronic SGD more in school but will also develop strategies to make maximal use of both systems.
Just as the individual using the AAC system must develop several types of competencies, there are many ways of carrying out the training. One approach, shown in Figure 11-19, is to simulate a situation, model the types of interaction likely to occur, and have the user “practice” the strategies and skills necessary to make it a success. This step can be followed by an actual situation in which the ATP accompanies the user as he or she encounters the situation. The ATP can then prompt the user at appropriate times, add encouragement, and help to clarify when necessary. This combination of clinic-based practice and community-based skill development is often very effective.
For training to be effective, staff must have sufficient skill and experience to assist the AAC user, which requires training for those who are supporting AAC use. Schepis and Reid (2003) identified seven basic steps in competence- and performance-based training for staff. These include specifying desired outcomes, roles for staff to support individuals in achieving these outcomes, providing both written and oral expectations and instructions to staff, demonstration of how to perform duties, and observation of staff performing the duties with corrective feedback as necessary.
Training of the individual who relies on AAC is only effective if communication partners are also trained. For children, the training of parents to recognize communication attempts and to understand the operational, linguistic, strategic, and social competencies is also important. Bruno and Dribbon (1998) evaluated a parent training program conducted as part of an AAC summer camp experience where parents attended the camp with their children. The camp featured structured therapy sessions, activities with nondisabled campers, and activities planned for families. The parent training had both device (conducted by manufacturers’ representatives) and interaction training aspects. Parents reported making positive changes in both operational and interactional skills during the camp (Bruno and Dribbon, 1998). These changes were reflected in gains made by the children in skills related to the use of pragmatic functions (e.g., giving and requesting information, requesting assistance, responding, and protesting) over the course of the camp. The camp training significantly increased the degree to which parents gave their children access to the AAC system. In some cases, skills in these areas remained constant at the 6-month follow-up, and in some there was a decrease. The areas of social exchange and giving of information continued to increase at the 6-month follow-up evaluation.
AAC training can be both complicated and lengthy (Beukelman and Mirenda, 2005). Light and Binger (1998) have developed a seven-step process for developing AAC communication competence: (1) specify the goal, do baseline observations; (2) select vocabulary; (3) teach the facilitators how to support development of the target skill; (4) teach the skill to the target individual; (5) check for generalization; (6) evaluate outcomes; and (7) complete maintenance checks. Light and Binger provide data collection and assessment forms and strategies for implementing this program. ACETS (Augmentative Communication Employment Training and Supports) (Institute on Disabilities, Temple University, Philadelphia, Pa., http://:disabilities.temple.edu) has been developed specifically to assist those who rely on AAC in seeking employment. A formal training manual is available for this program that is based on three principles: (1) immersion in the workplace culture, (2) acquiring a broad base of employment-related skills and experience, and (3) support of individualized goals.
Follow-up: Measuring Short- and Long-Term Outcomes.
The evaluation of communicative competence in the four domains (operational, linguistic, social, and strategic) will identify areas in which the AAC system is and is not adequately meeting the individual’s needs. Periodic re-evaluation of the individual’s skills and needs may also result in changes in the training or the AAC system(s). The re-evaluation may lead to new training goals in one or more of the four areas of communicative competence. In other cases the care givers, family, or other support staff may require additional training to facilitate the use of the AAC device.
The AAC device as it is configured may also be inadequate to meet the individual’s needs. It may be possible to adjust some of the features (e.g., scanning rate, stored vocabulary), or it may be necessary to consider a completely new device. The magnitude of the changes in the device dictates the amount of additional operational training required. In some cases the individual’s skills may decrease (e.g., degenerative disease) or increase (e.g., a young child who develops greater language skills). In either case a reevaluation and adjustments in the AAC system (device plus training and support) will be required.
Murphy et al (1996) identified obstacles to effective AAC system use in a study of 93 users of AAC systems and 186 partners (93 formal and 93 informal). The formal partners were speech-language pathologists (the majority), care providers in the day or living program, and teachers. Informal partners were family, friends, and others selected by the AAC users as those with whom they felt most comfortable using their AAC systems. In some cases one partner filled both the formal and informal roles. The majority of low- and high-tech AAC system use was in the day placement (90%), residential (70%), and leisure (60%) settings. Use was limited to organized therapy sessions in general.
AAC systems were only available to 48% of the users while shopping, 62% during outings such as day trips during their program, and 66% where they lived. SLPs were the most frequent (80%) formal partners, and residential or day care staff were the most common informal partners (62%). Friends and family were both reported as the primary informal partner in less than 10% of the cases. Only 57% of the low-tech and 59.4% of the high-tech AAC system users were able to independently access their systems (e.g., get a system out of a back pack on a wheelchair and set it up for use without a partner’s help). Knowledge of the system sufficient to interact with the AAC user was reported in less than half of the formal partners and one third of the informal partners. Eighty-eight percent of the users received training from their formal partners. However, for the majority of the users, the training consisted of 60 minutes or less (or 40 hours per year on the basis of sessions conducted). This number is low compared with other types of therapy and training such as that for second language instruction (estimated by Murphy et al to be more than 200 hours per year).
Murphy et al found that basic vocabulary required for daily interactions (see Table 11-5) was not included in the AAC systems. Few users had greetings, wrap ups, or conversational flow vocabulary (e.g., comments, repair vocabulary). Thus, for these areas, the users most commonly used other modes of communication (e.g., eye gaze, gestures, facial expressions) rather than their AAC devices.
The preponderance of formal partners also reinforces the need for inclusion of both useful vocabulary and multiple modes of communication. The development of strategic competence is vital to increase the likelihood that an AAC user will be able to independently carry out conversations in a variety of settings and with a variety of partners. Availability and accessibility of AAC systems can be addressed by appropriate mounting of systems on wheelchairs and training to ensure that care providers understand the need to have the system available to the user at all times. The results reported by Murphy et al also emphasize the importance of multiple modes of communication by AAC users.
Assessment of AAC outcomes can use the general measures (MPT, PIADS, Quebec User Evaluation of Satisfaction with Assistive Technology [QUEST]) described in Chapter 4. Because of the nature of communication, there are additional considerations. Because the major goal of AAC is the provision of expressive language capability, one of the most important considerations is the determination of communicative intent by the individual evaluating outcomes (typically SLP or special education teacher). Special education teachers tend to overassess intentionality (i.e., to assign intentionality more often than experienced researchers), whereas SLPs do so less often (Carter and Iacono, 2002). Individuals with different disorders are also assessed differently relative to intentionality, and observations are inconsistent across populations, sessions, and professional groups. These results are disturbing because intentionality is a key measure of communicative competence and effectiveness.
The MPT model (Chapter 4) has been adapted to AAC use as the AAC Acceptance Model (Lasker and Bedrosian, 2001). This model focuses on the prediction of acceptance of AAC by adults with acquired communication impairments. Although the technology may play a small role in acceptance or nonacceptance, other factors are more important. Among these other factors are the following: (1) the communication partners’ acceptance of the technology; (2) the rate (sudden or gradual) of onset of the communication impairment; (3) affective, behavioral, and cognitive components of a user’s attitude toward AAC technology; (4) perception of the user and other people toward the device, and (5) how other people view the person using the device. It is not clear whether this measure can be generalized to other populations (e.g., children with developmental disabilities).
There are a number of key reasons that provision of AAC systems may not achieve the goal of a “better life” for the AAC user (Beukelman and Mirenda, 2005): (1) payer resistance to or lack of acceptance of measures that reflect quality of life rather than more concrete functional outcomes, (2) increased costs of intervention necessary to achieve broader goals, (3) time limits set by payers on length of the intervention, (4) high demands on professionals to achieve and maintain skills, (5) family and user response to increases in their responsibilities in assuming a leadership role, (6) difficulty by families in envisioning the future for the AAC user, and (7) cultural differences between the user and professionals.
We can relate meaningful AAC outcomes to the three levels of the World Health Organization ICF classification system (see Chapter 2) (Beukelman and Mirenda, 2005). At the level of body structures and functions the degree to which AAC intervention compensates for lost or absent speech or language function can be determined. Evaluations related to activity focus on the quality and quantity of communication interactions and the degree to which these meet the goals and needs of the individual. Evaluations related to participation focus on the socially defined role and tasks within a sociocultural and physical environment. Some “Big Picture” AAC outcomes are shown in Box 11-4 (Beukelman and Mirenda, 2005). There are several types of measures for AAC system outcome. Operational measures evaluate the user’s ability to interact with the system itself (operational competence), whereas representational measures evaluate symbol and grammatical capability by the AAC user (Beukelman and Mirenda, 2005).
The most important result of the follow-up phase is to evaluate the outcomes of the AAC interventions to determine their effectiveness, including both the hard and soft technologies, and the appropriateness of the match between the originally specified needs and the resulting system. The principles of outcome measurement discussed in Chapter 4 apply to AAC system evaluation as well.
SUMMARY
Augmentative and alternative communication systems serve needs for both writing and conversation for individuals who have difficulties in these areas. Low-technology AAC systems provide quick and easy help for meeting communication needs, whereas high-technology devices offer great sophistication in available vocabulary, speed of communication, and flexibility of access. The latter features allow persons who have very limited physical skills to use AAC systems. AAC systems also have great flexibility in required user cognitive skills, allowing for persons with a diversity of intellectual abilities to benefit from AAC. Thoughtful assessment, careful training, and thorough follow through are essential to effective AAC intervention.
1. What are the two major communicative needs normally addressed by augmentative communication systems?
2. Distinguish between aided and unaided communication.
3. What are the major goals for augmentative communication systems designed for conversational use?
4. What AAC needs do parents have for their nonspeaking children? Do mothers and fathers have the same needs for their children?
5. Describe differences in the conversational rules that apply between two speaking persons and those between one speaking person and one augmentative communication user.
6. Describe the relationship between the Social Networks model and the Participation Model. How do each of these relate to the HAAT model described in this text?
7. How do attitudes of the communication partners differ for the five circles of the Social Networks model?
8. What factors influence the attitudes of children toward their peers who use AAC?
9. What features distinguish competent augmentative communicators from those who are not successful?
10. Select three discourse functions from those listed in Table 11-5. Now pick an augmentative communication device (e.g., electronic, direct selection, with voice output; or a language board with letters and words) and develop a vocabulary and set of strategies for the implementation of each of the discourse functions that you choose.
11. What are the three types of graphical communication? List three ways in which they differ.
12. In what ways does the formal writing of adolescent AAC users differ from that of nondisabled adolescent writers?
13. Distinguish between formal writing and note taking in terms of the characteristics AAC devices must have to meet each need. What is the most important feature in each case?
14. What two factors must be included for a math worksheet to be effective for both arithmetic and higher math (e.g., algebra)?
15. List three features that a drawing system should have to be of use in creative expression.
16. How do drawing systems differ in structure and function from systems for scientific plotting?
17. Describe auditory scanning. Give an example of both a low-tech or no-tech approach and an electronic AAC approach. What are the essential features for the AAC auditory scanning device?
18. List three encoding methods used in AAC devices, and give one advantage and one disadvantage of each.
19. What are the major types of abbreviation approaches used in AAC devices, and what are the major advantages and disadvantages of each?
20. Pick three discourse functions and develop a logical coding scheme for each using (1) numerical codes, (2) abbreviation expansion, and (3) Minspeak codes.
21. Compare word completion and prediction with abbreviation expansion and Minspeak encoding.
22. What are the major approaches used to increase conversational rate when the individual is using scanning?
23. What are dynamic displays, and what advantages do they provide?
24. What are visual scene displays and what unique features do they have?
25. What populations might benefit most from visual scene displays? Why?
26. Describe the major challenges and approaches for AAC intervention of individuals whose primary disorder is language or cognitively based? How does this compare with individuals whose primary disorder is motor or physical?
27. List and discuss three advantages that the Internet provides for communication by AAC users.
28. What are the major advantages of conversationally based communication devices such as CHAT and TOPIC?
29. What are the four types of competencies acquired in AAC training? Pick an AAC system for an individual and design the training. You must make assumptions regarding the person’s skills, her needs, and other people available to help facilitate the training.
30. For each of the categories of devices described in the section on current technologies, define a user profile (skills and needs) that would lead you to focus on that category in selecting a device for that person.
References
Alm N, Arnott JL, Newell AF: Database design for storing and accessing personal conversational material. In Proceedings of the 12th Annual Conference on Rehabilitation Engineering, pp 147-148, 1989, Washington, DC.
Alm, N, Arnott, JL, Newell, AF. Prediction of conversational momentum in an augmentative communication system. Commun ACM. 1992;35:46–57.
Alm N, Newell AF, Arnott JL: A communication aid which models conversational patterns. In Proceedings of the 10th Annual Conference on Rehabilitation Engineering, pp 127-129, 1987, Washington, DC.
Anderson, NB, Shames, GH. Human communication disorders: An introduction. Boston: Allyn and Bacon, 2006.
Angelo, DH. Impact of augmentative and alternative communication devices on families. Augment Altern Commun. 2000;16:37–47.
Angelo, DH, Kokoska, SM, Jones, SD. Family perspective on augmentative and alternative communication: families of adolescents and young adults. Augment Altern Commun. 1996;12:13–20.
Baker, B. Minspeak. Byte. 1982;7:186–202.
Baker, B. Using images to generate speech. Byte. 1986;11:160–168.
Ball, LJ, Beukelman, DR, Patee, GL. Acceptance of augmentative and alternative communication technology by persons with amyotrophic lateral sclerosis. Augment Altern Commun. 2004;20:113–122.
Beck, AR, Dennis, M. Attitudes of children toward a similar-aged child who uses augmentative communication. Augment Altern Commun. 1996;12:78–87.
Beck, AR, et al. Influence of communicative competence and augmentative and alternative communication technique on children’s attitudes toward a peer who uses AAC. Augment Altern Commun. 2002;18:217–227.
Beukelman, DR, Ball, LJ. Improving AAC use for persons with acquired neurogenic disorders: understanding human and engineering factors. Assist Technol. 2002;14:33–44.
Beukelman, D, Garrett, K. Augmentative and alternative communication for adults with acquired severe communication disorders. Augment Altern Commun. 1988;4:104–121.
Beukelman, DR, McGinnis, J, Morrow, D. Vocabulary selection in augmentative and alternative communication. Augment Altern Commun. 1991;7:171–185.
Beukelman, DR, Mirenda, P. Augmentative and alternative communication: management of severe communication disorders in children and adults, ed 3. Baltimore: Paul H Brookes, 2005.
Beukelman, D, Yorkston, K. Augmentative and alternative communication application for persons with severe acquired communication disorders: an introduction. Augment Altern Commun. 1989;5:42–48.
Beukelman, D, Yorkston, K, Dowden, P. Communication augmentation: A casebook of clinical management. San Diego: College Hill Press, 1984.
Blackstone, S. Populations and practices in AAC. Augment Commun News. 1990;3:1–3.
Blackstone, S. Persons with aphasia: What does AAC have to offer. Augment Commun News. 1991;4:1–6.
Blackstone, S. Dynamic displays. Augment Commun News. 1994;7:1–6.
Blackstone, S. Amyotrophic lateral sclerosis. Augment Commun News. 1998;11:1–15.
Blackstone, S. Assessment protocol for SGDs. Augment Commun News. 2001;13:1–16.
Blackstone, S. Social networks. Augment Commun News. 2003;15:1–16.
Blackstone, S. Autism spectrum disorder. Augment Commun News. 2003;15:1–6.
Blackstone, S. The Internet and its offspring. Augment Commun News. 2003;15:1–3.
Blackstone, S. Visual scene displays. Augment Commun News. 2004;16:1–5.
Blackstone, S. False beliefs, widely held. Augment Commun News. 2006;8:1–6.
Blackstone SW, Hunt Berg M: Social networks: a communication inventory for individuals with complex communication needs and their communication partners—inventory booklet, Monterey, CA, 2003, Augmentative Communication.
Blackstone, SW, Williams, MB, Joyce, M. Future AAC technology needs: consumer perspectives. Assist Technol. 2002;14:3–16.
Blishcak, DM, Lombardino, LJ, Dyson, AT. Use of speech-generating device: in support of natural speech. Augment Altern Commun. 2003;19:29–35.
Bondy, A, Frost, L. The picture exchange communication system. Behav Modif. 2001;25:725–744.
Brady, NC. Improved comprehension of object names following voice output communication aid use: Two case studies. Augment Altern Commun. 2000;16:197–204.
Bruno, J, Dribbon, M. Outcomes in AAC: evaluating the effectiveness of a parent training program. Augment Altern Commun. 1998;14:59–70.
Bryen, DN, Cohen, K, Carey, A. Augmentative communication employment training and supports: Some employment outcomes. J Rehabil. 2004;70:10–18.
Carlisle Ladtkow, M, Culp, D. Augmentative communication with traumatic brain injury. In: Yorkston K, ed. Augmentative communication in the medical setting. Tucson, AZ: Communication Skill Builders; 1992:139–244.
Carter, M, Iacono, T. Professional judgments of the intentionality of communicative acts. Augment Altern Commun. 2002;18:177–191.
Clarke, M, Kirton, A. Patterns of interaction between children with physical disabilities using augmentative and alternative communication systems and their peers. Child Lang Teach Ther. 2003;19:135–151.
Colby, KM, et al. A word-finding computer program with a semantic lexical memory for patients with anomia using an intelligent speech prosthesis. Brain Lang. 1981;14:272–281.
Coleman, CL. Augmentative communication training modules. Sacramento: Assistive Device Center, California State University, 1988.
Collier B: When I grow up … supporting youth who use augmentative communication for adulthood. In Proceedings of the 2005 Alberta Rehabilitation and Assistive Technology Consortium Conference, Edmonton, Canada (2005): www.acrat.ca. Accessed August 2007.
DeRuyter, F, Kennedy, M. Augmentative communication following traumatic brain injury. In: Beukelman D, Yorkston K, eds. Communication disorders following traumatic brain injury: management of cognitive, language, and motor impairments. Austin, TX: PRO-ED; 1991:317–365.
Dowden, P, Cook, AM. Choosing effective selection techniques for beginning communicators. In: Reichle J, Beukelman DR, Light JC, eds. Exemplary practices for beginning communicators. Baltimore: Paul H. Brookes; 2002:395–432.
Dowden, PA. Augmentative and alternative communication decision making for children with severely unintelligible speech. Augment Altern Commun. 1997;13:48–58.
Drager, KDR. Light technologies with different system layouts and language organizations. J Speech Hear Res. 2003;46:289–312.
Dye, R, et al. A script-based AAC system for transactional interaction. Natl Lang Eng. 1998;4:57–71.
Falvey, M, et al. All my life’s a circle: Using the tools of cirles, MAPS and PATHS. Toronto: Inclusion Press, 1994.
Fields, C. Finding a voice for Daniel. Team Rehabil Rep. 1991;2:16–19.
Fox, LE, Fried-Oken, M. AAC aphasiology: partnership for future research. Augment Altern Commun. 1996;12:257–271.
Frager S, Hux K, Beukelman D: AAC acceptance and use by 25 adults with TBI. CSUN Conference on Technology and People with Disabilities (2005): http:/aac.unl.edu. Accessed August 2007.
Fruchterman, JR. In the palm of your hand: a vision of the future of technology for people with visual impairments. J Vis Impair Blindness. 2003;97:585–591.
Garrett, K, Beukelman, D. Augmentative communication approaches for persons with severe aphasia. In: Yorkston K, ed. Augmentative communication in the medical setting. Tucson: Communication Skill Builders, 1992.
Goldbart, J, Marshall, J. “Pushes and pulls” on the parents of children who use AAC. Augment Altern Commun. 2004;20:194–208.
Graves, J. Vocabulary needs in augmentative and alternative communication: a sample of conversational topics between staff providing services to adults with learning difficulties and their service users. Br J Learning Disabil. 2000;28:113–119.
Helsinger S: Teaching the Picture Exchange Communication System to adults with pervasive developmental disorder/autism. Presented at the Picture Exchange Communication System Exposition, Philadelphia, 2001.
Higginbotham DJ et al: The Frametalker project: building an utterance-based communication device, Proceedings of the 2005 CSUN Conference on Technology For Persons With Disabilities, 2005, Los Angeles.
Hunnicutt S: ACCESS: A lexical access program. In Proceedings of the RESNA 12th Annual Conference, pp 284-285, 1989, Washington, DC.
Iacono, T, Mirenda, P, Beukelman, D. Comparison of unimodal and multiple modal AAC techniques for children with intellectual disabilities. Augment Altern Commun. 1993;9:83–94.
Jacobs, B, et al. Augmentative and alternative communication for adults with severe aphasia: where we stand and how we can go further. Disabil Rehabil. 2004;26:1231–1240.
Joseph, D. The morning. Commun Outlook. 1986;8:8.
Kent-Walsh, JE, Light, JC. General education teachers’ experiences with inclusion of students who use augmentative and alternative communication. Augment Altern Commun. 2003;19:102–124.
King, JM, Hux, K. Intervention using talking word processor software: an aphasia case study. Augment Altern Commun. 1995;11:187–192.
Kovach, T, Kenyon, P. Auditory scanning: development and implementation of AAC systems for individuals with physical and visual impairments. ISAAC Bull. 1998;53:1–7.
Kraat, AW. Communication interaction between aided and natural speakers: a state of the art report. Toronto: International Project on Communication Aids for the Severely Speech Impaired, 1985.
Kraat, AW. Developing intervention goals. In: Blackstone S, Bruskin D, eds. Augmentative communication: an introduction. Rockville, MD: American Speech-Language and Hearing Association, 1986.
Kraat, AW. Augmentative and alternative communication: does it have a future in aphasia rehabilitation? Aphasiology. 1990;4:321–338.
Lasker, J, Bedrosian, J. Promoting acceptance of augmentative and alternative communication by adults with acquired communication disorders. Augment Altern Commun. 2001;17:141–153.
Light, J. Interaction involving individuals using augmentative and alternative communication systems: state of the art and future directions. Augment Altern Commun. 1988;4:66–82.
Light, J. Toward a definition of communicative competence for individuals using augmentative and alternative communication systems. Augment Altern Commun. 1989;5:137–144.
Light, J, Beesley, M, Collier, B. Transition through multiple augmentative and alternative communication systems: a three year case study of a head injured adolescent. Augment Altern Commun. 1988;4:2–14.
Light, JC, Binger, C. Building communicative competence with individuals who use augmentative and alternative communication. Baltimore: Paul H Brookes, 1998.
Light, JC, Drager, KDR. Improving the design of augmentative and alternative technologies for young children. Assist Technol. 2002;14:17–32.
Lilienfeld, M, Alant, E. Attitudes toward an unfamiliar peer using an AAC device with and without voice output. Augment Altern Commun. 2002;18:91–101.
Lloyd, LL, Fuller, DR, Arvidson, HH. Augmentative and alternative communications: a handbook of principles and practices. Boston: Allyn and Bacon, 1997.
Magiati, I, Howlin, P. A pilot evaluation study of the Picture Exchange Communication System (PECS) for children with autistic spectrum disorders. Autism. 2003;7:297–320.
McCartthy, J, Light, J. Attitudes toward individuals who use augmentative and alternative communication: research review. Augment Altern Commun. 2005;21:41–55.
McKelvey M. et al: Performance of a person with chronic aphasia using a visual scene display prototype, J Med Speech Lang Pathol In press.
McNaughton, D, Light, J, Gulla, S. Opening up a “whole new world”: employer and co-worker perspectives on working with individuals who use augmentative and alternative communication. Augment Altern Commun. 2003;19:235–253.
Mirenda, P. Toward functional augmentative and alternative communication for students with autism: manual signs, graphic symbols and voice output communication aids. Lang Speech Hearing Serv Schools. 2003;34:203–216.
Mirenda, P, Santogrossi, J. A prompt-free strategy to teach pictorial communication system use. Augment Altern Commun. 1985;1:143–150.
Murphy, J, et al. AAC system use: obstacles to effective use. Eur J Dis Commun. 1996;31:31–44.
Musselwhite, CR, St. Louis, KW. Communication programming for the severely handicapped: vocal and non-vocal strategies. Houston: College Hill Press, 1982.
Nolan, C. Dam-burst of dreams. New York: St. Martin’s Press, 1981.
Parette, HP, Botherson, MJ, Huer, MB. Giving families a voice in augmentative and alternative communication decision-making. Educ Train Ment Retard Dev Disabil. 2000;35:177–190.
Reichle, J, et al. Comparison of correct responses and response latency for fixed and dynamic displays: performance of a learner with severe developmental disabilities. Augment Altern Commun. 2000;16:154–163.
Riechle, J, York, J, Sigafoos, J. Implementing augmentative and alternative communication. Baltimore: Paul H Brookes, 1991.
Rush, WL. Journey out of silence. Lincoln, NE: Media Productions and Marketing, 1986.
Schepis, M, Reid, D. Issues affecting staff enhancement of speech-generating device use among people with severe cognitive disabilities. Augment Altern Commun. 2003;19:59–65.
Schlosser, RW, Blischak, DM. Is there a role for speech output in interventions for persons with autism? Focus Autism Other Dev Disabil. 2001;16:170178.
Schwartz IS: Beyond basic training: PECS use with peers and at home. Presented at the Picture Exchange Exposition, Philadelphia, 2001.
Sevick, RA, Romski, MA, Adamson, LB. Research directions in augmentative and alternative communication for preschool children. Disabil Child. 2004;26:1323–1329.
Simpson, S. If only I could tell them. Commun Outlook. 1988;9:9–11.
Steele RD, Weinrich M: Training of severely impaired aphasics on a computerized visual communication system. In Proceedings of the RESNA 8th Annual Conference, pp 320-322, 1986, Washington, DC.
Todman, J. Rate and quality of conversations using a text-storage AAC system: Single-case training study. Augment Altern Commun. 2000;16:164–179.
Vanderheiden, GC, Lloyd, LL. Communication systems and their components. In: Blackstone S, Bruskin D, eds. Augmentative communication: an introduction. Rockville, MD: American Speech-Language and Hearing Association, 1986.
Williams, MB. Message encoding: a comment on Light et al. Augment Altern Commun. 1991;7:133–134.
Yorkston, KM, et al. A comparison of standard vocabulary lists. Augment Altern Commun. 1988;5:189–210.
Yorkston, KM, et al. Vocabulary selection: a case study. Augment Altern Commun. 1989;5:101–114.
*Pyramid Educational Products, Newark, Del. The Picture Exchange Communication System (PECS) is a commercially available program developed for people with ASD that uses graphic symbols (often the Mayer-Johnson Picture Communication Symbols(c)) and a specific instructional method. The objective of PECS is that children or adults who are not yet initiating requests, comments, and so forth, learn to spontaneously initiate communicative exchanges. The person is initially encouraged to give something (picture/symbol) to a communication partner to complete a communication exchange. Thus, by using PECS, learners gain the attention of the communication partner to make a request. By advancing through the six phases of PECS, the student progresses from a simple exchange through increasing levels of spontaneity to sequencing words and creating sentences. No prompting is used throughout the learning process. In a study conducted by Bondy and Frost (2001) in 85 children (aged 5 years or younger), more than 95% of the children were able to exchange at least two pictures, whereas 76% began using speech with or without PECS. In other studies with smaller number of participants, positive outcomes in speech improvement, rapid mastery of the system, and decrease in destructive behavior or tantrums were reported anecdotally (Helsinger, 2001; Schwartz, 2001). Recent empirical studies on PECS have reported positive effects regarding rate of mastery of the system and improvement in general communication skills (Magiati and Howlin, 2003).