Framework for Assistive Technologies
HUMAN PERFORMANCE AND ASSISTIVE TECHNOLOGIES
Foundation for a Human Activity Assistive Technology Model
Human Activity Assistive Technology Model
EXTRINSIC ENABLERS: THE ASSISTIVE TECHNOLOGIES
Soft Technologies as Extrinsic Enablers
Assistive Technology Devices for Specific Applications
APPLICATION OF THE HUMAN ACTIVITY ASSISTIVE TECHNOLOGY MODEL: DESIGNING ASSISTIVE TECHNOLOGY SYSTEMS FOR SUCCESSFUL OUTCOMES
Consider the Perspective of the User
On completing this chapter, you will be able to do the following:
1 Define human behavior and contrast it with human performance
2 Describe the components of an assistive technology system
3 Describe and discuss the Human Activity Assistive Technology model
4 List the major performance areas in which assistive technology systems are applied
5 Discuss the contexts in which assistive technologies are used
6 Delineate the major considerations in designing an assistive technology system
In Chapter 1 an assistive technology device was defined as “an item, piece of equipment, or product system…that is used to increase, maintain, or improve functional capabilities of individuals with disabilities” (Public Law 100-407). In this chapter this base is expanded by defining an assistive technology system as consisting of an assistive technology device, a human operator who has a disability, and an environment in which the functional activity is to be carried out. In this chapter this concept of a system is formalized and the groundwork is laid for applying it to specific applications in later chapters.
HUMAN PERFORMANCE AND ASSISTIVE TECHNOLOGIES
At the most fundamental level, assistive technology systems represent someone (person with a disability) doing something (an activity) somewhere (within a context). A major goal of the assistive technology practitioner (ATP) is to recommend an assistive device that meets an individual disabled person’s specific needs, is consistent with his or her skills, and accomplishes unique functions within the contexts of that person’s daily life. This assistive technology system selection process emphasizes use of available function (human component) to accomplish what is desired (activity) in a given context (place, environment, people). We are not concerned as much with remediation of a disability as we are with enabling functional results and helping the individual to achieve what he or she wants to accomplish. Functional results require maximizing the skills of the person with a disability, which places human performance at the center of our system. The primary outputs of the assistive technology system are communication, mobility, manipulation, and cognition. In this chapter we discuss means of achieving these outputs in a general sense. More specific applications that may facilitate performance in these areas will be discussed in subsequent chapters.
Let’s start with a case study of an individual who uses an assistive device for communication.
This case study provides a brief illustration of a situation of an individual with a disability who uses assistive technology to communicate. It hints at factors that influence whether a device will be useful in a given context and how individuals within the environment can affect the use of a device. It raises several issues involving the person using the device, the device itself, and the context in which it is used. It also points to the need for an effective evaluation that will enable selection of the most appropriate device and suggests that the interaction between the person, the device, and the contexts will influence the performance of a desired activity.
Foundation for a Human Activity Assistive Technology Model
Before a model that guides the selection and evaluation of assistive technology is described, two generic models will be presented that provide a foundation for one specific to assistive technology. These models are the International Classification of Functioning, Disability, and Health (ICF) (World Health Organization [WHO], 2001) and the Canadian Model of Occupational Performance (CMOP) (Canadian Association of Occupational Therapists [CAOT], 2002). Both these models include elements of the person, an activity, and the environment to understand a specific construct (health domains and health-related domains in the first instance and occupational performance in the second).
The ICF was described in more detail in Chapter 1. The ICF was derived from the International Classification of Disability and Handicap (WHO, 1980), with the addition of environmental factors and use of more inclusive language being two main distinctions between the two versions. It “provides a description of situations with regard to human functioning and its restrictions and serves as a framework to organize this information” (WHO, 2001, p. 7). Two components comprise factors of health and health-related states: body structures and functions and activities and participation. The framework includes two contextual factors: environmental and personal factors.
The term “body functions” refers to the functions of various systems in the body such as vision, sensation, and movement. Body structures include the anatomical structures that support the body functions (e.g., nerves, organs, and bones). Activity and participation are difficult to separate, so the ICF includes them together in its classification scheme. Activity refers to the performance of a task or action by a person, whereas participation involves performance of the activity within an individual’s life roles or situation (WHO, 2001). The environmental context includes elements related to the physical, social, attitudinal, and institutional components. Finally, the personal factors include aspects such as age, sex, and lived experiences that have the potential to affect activity and participation (WHO, 2001).
Another model that is useful for understanding the relationship between the person, the activity, and the environment is the Canadian Model of Occupational Performance (CMOP) (CAOT, 2002). It conceptualizes the relationship between these three elements and their combined influence on occupational performance, which is defined as the choice, organization, and satisfactory completion of daily activities (CAOT, 2002). Components of the person factor include physical, affective (emotional), and cognitive elements. Occupation is composed of self-care, productivity, and leisure, whereas the environment consists of physical, social, cultural, and institutional elements. The dynamic interaction of these elements influences an individual’s performance in chosen or required occupations (CAOT, 2002).
Both these models are similar in that they include elements of the person and his or her activities and environment. Assistive technology is specifically mentioned in the ICF as an aspect of the environment, specifically, products and technology for personal use in daily living, for personal indoor and outdoor mobility and transportation, communication, education, employment, and culture, recreation, and sport (WHO, 2001). It is not specifically mentioned in CMOP. These models are useful in understanding assistive technology because they identify factors that affect participation in daily activities across the life span. However, they are limited because the role and considerations of assistive technology are not specified. A model is now presented that explicitly includes assistive technology as a component of the completion of daily activities. This model is intended to be used as a framework for the selection, implementation, and evaluation of assistive technology systems.
Human Activity Assistive Technology Model
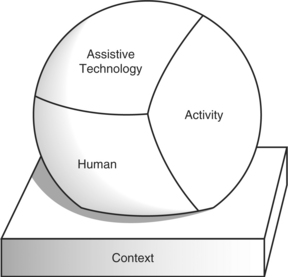
The human activity assistive technology (HAAT) model is proposed as a framework for understanding the place of assistive technology in the lives of persons with disabilities, guiding both clinical applications and research investigations. The model has four components—the human, the activity, the assistive technology, and the context in which these three integrated factors exist. The human component includes physical, cognitive, and emotional elements; activity includes self-care, productivity, and leisure; assistive technology includes intrinsic and extrinsic enablers; and the context includes physical, social, cultural, and institutional contexts. Each of the components shown in Figure 2-1 plays a unique part in the total system. Consideration of each of these elements and their interaction is necessary for design, selection, implementation, and evaluation of appropriate assistive technologies and for research into various aspects of assistive technology development and use. The characterization of the model with the elements of human, activity, and assistive technology forming a collective that is nested within a physical, social, cultural, and environmental context is intended to show the dynamic interaction between the initial three factors and the pervasive influence on them, both individually and collectively of the various contexts. The interaction among the components of the HAAT model can be illustrated through application to our case study of Marion.
This brief example illustrates how the users’ abilities are enhanced or augmented by the assistive technology to complete a desired activity. It also demonstrates that an assistive technology solution that works in one context is not as effective in another. The illustration shows that aspects of the person, the desired activity, the assistive technology, and the environment in which the technology will be used must be considered to ensure a satisfactory means to engage in daily living. What works for one person, in a particular setting for a particular activity may not be successful for another person in different circumstances. Indeed, a solution that works in one context may not transfer to another context for the same person.
THE ACTIVITY
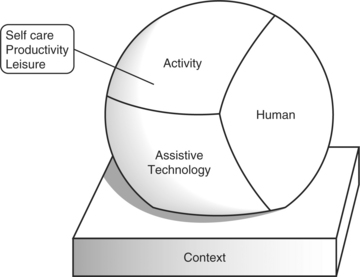
The activity is the fundamental element of the HAAT model shown in Figures 2-1 and 2-2 and defines the overall goal of the assistive technology system. The activity is the process of doing something, and it represents the functional result of human performance. Activities are carried out as part of our daily living, are necessary to human existence, can be learned, and are governed by the society and culture in which we live (CAOT, 2002).
The profession of occupational therapy is based on the use of occupation, or activity, in the daily lives of individuals. Both the American Occupational Therapy Association (AOTA) and CAOT define these terms in the same way:
[A]ctivities…of everyday life, named, organized, and given value and meaning by individuals and a culture. Occupation is everything people do to occupy themselves, including looking after themselves…enjoying life…and contributing to the social, and economic fabric of their communities. (AOTA, 2002; CAOT, 2002)
Activities are categorized within three basic performance areas: activities of daily living, work and productive activities, and play and leisure activities (CAOT, 2002). Activities of daily living include dressing, hygiene, grooming, bathing, eating, personal device care, communication, health maintenance, socialization, taking medications, sexual expression, responding to an emergency, and mobility. Included in work/productive activities are home management activities, educational activities, vocational activities, and care of others. The play and leisure area includes activities related to self-expression, enjoyment, or relaxation. Although these lists suggest that certain activities form specific categories, in reality the meaning an individual gives to an occupation determines in which performance area it is placed (CAOT, 2002; Miller Polgar and Landry, 2004). For example, gardening may be a productive activity for one person and a leisure activity for another. Further, the meaning of an activity may vary depending on the role the individual assumes at the time the activity is performed. Christiansen and Baum (1997) define roles as “positions in society having expected responsibilities and privileges” (p. 54).
A person can have multiple roles simultaneously, and roles change throughout the person’s life span. Examples of roles we hold during our lifetime include student, parent, son or daughter, sibling, employee, friend, and homemaker. Performance of an activity may differ depending on the nature of the role in which it is performed. For example, a parent reading to her child reads in a different way than when the reading is completed as part of the role of worker or student. Activities can be broken down into smaller tasks. The skills and abilities intrinsic to the human allow the individual to complete a series of tasks to produce the functional outcome of the activity. These skills may require any combination of physical abilities, cognitive abilities, or emotional aids for their successful completion. When an individual lacks the capacity to complete a task, the manner in which that task is completed, including the use of assistive technologies, must be changed. Understanding the activity is part of the assistive technology selection process as it requires identifying the tasks, skills, and abilities required for successful completion, the meaning the individual gives to the activity, and the different roles in which the individual uses the activity. Returning to the case study of Marion, communication is identified as the activity in which she needs to participate. She has the cognitive skills to complete the activity but not the physical ones. Further, the contexts in which she must communicate, including with different communication partners, affect her performance of this activity. Careful analysis of the activity of communication for Marion is required to identify the communication device that is most useful to her.
THE HUMAN
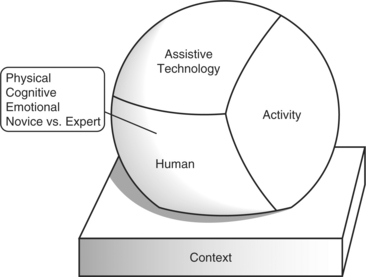
The model in Figure 2-1 represents someone doing something someplace. Who is doing it? The individual with a disability is “operating” the system. Figure 2-3 highlights the human component of the HAAT model. Two theoretical approaches are useful when considering the human operator and his or her ability to use assistive technology: the conceptualization of the person from the CMOP (CAOT, 2002) and occupational competence (Matheson and Bohr, 1997). The CMOP conceptualizes human abilities as composed of three elements: physical, cognitive, and affective (CAOT, 2002). Physical abilities include strength, coordination, range of motion, balance, and other physical properties. Cognitive components include attention, judgment, problem solving, concentration, and alertness, whereas affect includes emotional elements. It is important to understand a person’s abilities in each of these areas as they relate to the use of the desired technology. An appropriate match is needed between the person’s abilities and the requirements of the technology to ensure effective use (Scherer, 1998). Where a mismatch occurs, devices will be misused or abandoned because they do not meet the user’s needs.
In the HAAT model, the motor outputs of communication, mobility, and manipulation are required to accomplish the goals defined by activities. These three areas require that the human operator possess motor output skills and sensory function to perform these activities. These are akin to the physical domain of CMOP. For example, visual or auditory input is typically required for communication. If these skills are impaired, assistive technology systems can provide assistance by requiring different skills. For example, when a hearing aid compensates for reduced hearing thresholds or a Braille output system avoids visual reading, the assistive technology provides replacement or augmentation of a sensory system. Finally, central processing is required for the successful completion of activities. Components of central processing include perception, motor control, and cognition, similar to the CMOP cognitive domain. If the human’s capabilities are limited, then assistive technology systems can often provide assistance in this area as well. For example, procedures for device operation may be simplified for an individual who has difficulty in sequencing tasks, or recall aids may be incorporated to assist someone who has memory deficits. Psychological function (referred to as affect in CMOP) influences performance of activities through motivation, self-efficacy, and perception of the value of the activity, as examples. These human performance components of the HAAT model are examined in detail in Chapter 3.
Occupational competence gives a dynamic context to the understanding of human abilities and how a person changes and adapts his or her engagement in activity in response to environmental demands and his or her own abilities. Although CMOP is useful to conceptualize human behavior at a given point in time, occupational competence helps understand behavior across the life span. Five constructs are important to the notion of occupational competence (Matheson and Bohr, 1997). Capacity refers to the potential skill, ability, or knowledge that an individual can apply to a given activity. Capacity changes with development, aging, or with trauma or illness. Effectance is the extent to which individuals reach or use their capacity in a given task. When a person is motivated to perform well in an activity, effectance approaches capacity. Affordances are those environmental elements that can facilitate performance of a task, providing the individual perceives them as a facilitator. Self-efficacy is a well-known concept described by Bandura (1977) that refers to an individual’s belief that he or she can be successful in a particular situation. Finally, competence is the self-perception of satisfactory performance compared with some defined standard.
Collectively, these constructs contribute to occupational competence that is the ability to meet the demands that are required for successful engagement in various life roles (Matheson and Bohr, 1997). Thus, expectations by and of the individual, relative to performance of an activity, change as the person grows and acquires new skills, or conversely, as the person ages or experiences illness or trauma and loses skills. This notion of occupational competence illustrates the dynamic elements of physical and cognitive capacities and how they are influenced by the individual’s attitudinal and motivational characteristics to meet the demands of various life roles.
Skills and Abilities
It is possible to distinguish between a person’s skill and his or her ability. An ability is a basic trait of a person, what a person brings to a new task, whereas a skill is a level of proficiency, which is comparable to effectance described by Matheson and Bohr (1997). In assistive technology applications, this distinction is important. It is usually possible to obtain an assessment of a person’s abilities, but it is difficult to predict the level of skill that he or she will develop using the technology. Ability can also mean transferring a skill from a related area and applying it to a new task. For example, a person with a disability might develop skill in the use of a joystick as a computer interface and then transfer this motor skill to the use of a power wheelchair. In this type of situation, the acquired skill in the first task becomes an ability that can be used in the second task.
Although it is possible for most humans to perform more than one task at a time, it is generally necessary to concentrate on one task to learn it. For example, a beginning user of an augmentive communication system may need to concentrate initially on the development of motor skills necessary to make selections with a keyboard. Eventually, he or she will have mastered this motor task sufficiently that he or she can perform it reliably while also concentrating on the language content of his or her message.
In Chapter 1 soft technologies were defined as “the human areas of decision making, strategies, training, and concept formation.” In particular, strategies are part of the human skills required for the success of an assistive technology system. As Enders (1999) has pointed out, people who have disabilities use strategies to complete tasks. These can often either replace assistive technologies completely or compensate for deficiencies in the technology. For example, Marion uses strategies to enhance her augmentative communication system functionality. She may wave instead of typing “hi,” or she may use prestored words to increase her speed at times and spell at other times to increase the participation of her communication partner. As in other aspects of the assistive technology system, the strategies used are highly dependent on all the other aspects of the assistive technology system. The context determines which strategies are important and useful, the characteristics of the technology affect which strategies are important to success, and the activity dictates the choice of strategies. Enders has proposed that strategies make up one side of a three-pronged approach to assistive technology applications that she calls “a human accomplishment support system.” This framework is consistent with the HAAT model. The other two aspects of the framework are personal assistants and assistive technology devices.
Novice Versus Expert User
Another consideration related to the person, in the selection or evaluation of assistive technology, is whether that person is a novice or expert user of the specific technology. The term novice describes a user of an assistive technology system who has little or no experience with that particular system or the task for which it is used. As the user practices and gains more experience, he or she may become an expert user (i.e., demonstrating a high degree of skill in the use of the system). What differentiates an expert from a novice? The novice is more likely to use the system in prescribed ways, relying on soft technologies to use it effectively. The novice is less likely to generalize use of the system from one task to another and must use more conscious effort to control it. An expert takes more risks with the equipment in terms of stretching the way it is used and trying new activities with the system. For example, a skilled manual wheelchair user will take the chair up or down an escalator rather than use an elevator. A skilled communication aid operator will develop strategies to increase the rate of communication.
Understanding the differences between a novice and expert user has important implications for teaching people how to use a system and the development of strategies (soft technologies). An expert user exerts less conscious effort in the operation of the system—because he or she does not need to do so. Analysis of the strategies of an expert user and translation of these into teaching programs can be an effective means of assisting a novice to become an expert user of a system.
THE CONTEXTS
Over the past several decades the models used to describe disability and the disablement process have changed dramatically (Pope and Brandt, 1997). In the 1950s the focus was on the “problem” of an inability to participate in work, play, education, and daily activities of living by the disabled person; this problem was “in the person”; that is, it was strictly the result of the impairment. More recently, there has been an increasing awareness that the difficulties experienced by individuals with disabilities result as much from environmental factors as from the impairment itself. Initially the focus was on the physical or built environment, with much effort to make curb cuts, install elevators, and so on. As individuals with disabilities began to participate more fully in society, it became evident that the social and attitudinal barriers were just as great as the physical ones. A “minority group model” of disability emerged in which the attention was shifted away from the impairment to the social, political, and environmental disadvantages forced on people who have disabilities (Brooks, 1998). Bickenbach et al (1999) conceptualized disability in a different way. In their view, disability was a universal experience, if a person lives long enough. Contrary to the minority group model, which advocated for special status for individuals with disability, the universalism concept advocated for broader social justice and policies that were more inclusive of persons with disabilities; actions that will benefit a broader segment of society. With these new perspectives, problems of societal participation were no longer attributed to the impairment of the person with a disability. Rather, lack of participation in society was viewed as resulting from limitations in the social and physical environments. The emphasis on participation in the ICF is indicative of the move away from a “problem in the person” concept to a “problem in the environment” model. In the HAAT model we have captured these external influences in the context.
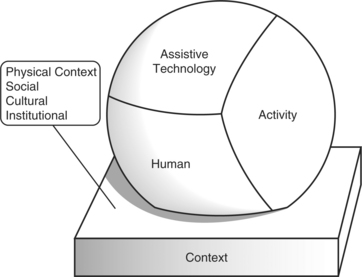
As shown in Figure 2-4, the context includes four major considerations. These are (1) physical context, including natural and built surroundings and physical parameters, (2) social context (with peers, with strangers), (3) cultural context, and (4) the institutional context, including formal legal, legislative, and sociocultural institutions such as religious institutions. The contexts in which the human carries out the activity can be determining factors in whether the person successfully uses an assistive technology system. The supports and barriers in these environments are important considerations in the selection and evaluation of these systems.
One further distinction is important in the consideration of context: the level of environment. Three levels of environments have been described in the literature: microenvironment, mesoenvironment, and macroenvironment (Fougeyrollas and Gray, 1998; Law, 1991). The microenvironment refers to the closest, most intimate environments in which a person functions such as the home, school, or work setting. Here the person and his or her abilities are known, roles are defined, and rules and expectations are understood. The mesoenvironment describes those settings in which a person functions less frequently and includes various community facilities such as community centers, shopping malls, and churches. The macroenvironment refers to the broader social and cultural contexts that impose a legislative and moral behavioral framework on the person (Law, 1991). Each of these environments influences the use of assistive technology systems. It is important to understand how each aids or hinders the use of technology.
Physical Context
Perhaps the easiest environmental component to understand is the physical context. This context involves the physical attributes of the environment that enable, hinder, or affect performance of daily activities, either with or without assistive technology. It is important to identify the physical attributes of the environments in which the individual intends to use an assistive device to determine whether the device is compatible with those environments. In some cases, a device will work in one environment but not in another. Voice recognition software is an example of a device that does not readily transfer from one environment to another. In the relative quiet of an individual’s home, voice recognition software may be an excellent alternative to direct input of computer keystrokes. However, it may not work in an office environment where noise interferes with the software and its use may interfere with the work of colleagues in close proximity to the individual.
A distinction that is important to understanding the physical environment is between the natural and the built surroundings. The natural surroundings include non-man-made elements such as parks. Conversely, built surroundings include those structures or elements that are man made such as buildings and sidewalks. It is critical to know whether the individual intends to use an assistive device in both built and natural surroundings because it will affect the technology selection and performance. A wheelchair with tires that facilitate travel over uneven and loose surfaces should be recommended for a person who intends to use a chair both indoors and outdoors on unpaved areas. One with smooth tires will not be useful for outdoor travel.
Assessment of the physical environment for selection or evaluation of assistive technology begins with the activities the person wants or needs to do and in which environments those activities will be performed. Within buildings, a person needs to enter and exit the building, access various locations, possibly move between levels, and perform a variety of daily activities. Further, a person needs to move from one environment to another (e.g., home to place of employment). Some of the physical aspects of the environment that should be considered include width of hallways or doorways, distances between locations the person must navigate, surface (e.g., carpet, transitions, floor surface), height and weight of devices and objects (e.g., door) the person must manipulate, and sensory cues (visual or auditory) required to successfully complete daily activities. Physical safety is an important consideration when the environment is assessed.
Three commonly measured parameters of the physical environment—heat (related to temperature), sound, and light—most directly affect the performance of assistive technologies. Many materials are sensitive to temperature and are affected by excessive heat or cold. For example, the properties of foams and gels used in seat cushions can change under conditions of very high or very low temperatures. Liquid crystal displays are affected by temperature and by ambient (existing) light.
Ambient light in classrooms or work environments can affect the use of assistive technologies. Some displays emit light and are better in conditions of reduced ambient light, whereas others reflect light and are better used in bright light. For example, lighting that is appropriate for normal classroom work may be too bright for the use of some displays, such as computer screens, because of glare.
Ambient sound (including noise) can have a major effect on the intelligibility of voice synthesizers or voice recognition systems. Sounds generated by such devices as printers, power wheelchairs, voice output communication aids, and auditory feedback from computer programs can be disruptive in a classroom. Church and Glennen (1992) discuss ways of controlling sound and lighting to avoid interference in the classroom while still facilitating the functional gains provided by the assistive technology.
Social Context
For assistive technology use, the social aspects of the context can be the most important. The social context refers to those individuals who interact with the individual using assistive technology, either directly or indirectly. Their acceptance or rejection of the assistive technology or their understanding of the purpose and need for the assistive technology is a critical component of whether the individual will be successful with technology use. As Fougeyrollas (1997) points out, social influence on individuals is related to what is considered normal or expected. Individuals who have disabilities may be stigmatized because of their disability. A frequent comment by persons with disabilities is that it is often the social environment, the attitude of others, that creates more of a handicap than the physical barriers in the environment. The use of assistive technologies can contribute to this stigmatization and lead to further isolation. For these reasons, it is important to understand the social aspects of the environments in which the individual will use the technology. If others in the environment do not support the use of the technology, the individual faces greater challenges to successful use of the device.
Relationships with others in the environment affect the use of technology. Those close to the individual, such as family, friends, teachers, or coworkers, have a better understanding of the person’s capacities so use of technology is often eased. With unfamiliar people, technology use may be more complex because expectations differ as well as the understanding of how the technology works. For these reasons, it is important to determine who provides assistance to individuals using assistive technology in various environments, in particular, in key environments such as home, school, and workplace. Technology use, and consequently function, is eased when assistance is received from consistent individuals, such as family or personal care attendants, because these individuals understand the user’s needs and the function of the assistive technology. When assistance is provided by several attendants, the result may be inefficient and incorrect use of the assistive technology because each successive attendant must learn the user’s preferred method of completing activities and how the assistive technology is integrated into daily activities. In such situations, the user or the caregiver should be able to provide instruction to attendants.
Let’s return to Marion and examine how her use of communication devices differs with various communication partners.
Communication systems are not the only type of assistive technology affected by social context. Brooks (1990) asked 595 disabled scientists and engineers to evaluate the assistive devices they used. She found that users applied devices in a variety of social settings, but use varied depending on the specific setting. For example, intimate, essential devices, such as those for personal hygiene, are not as frequently used as are those devices that assist in employment. Brooks interpreted this result as a reflection of the complex ties between the human (especially self-esteem), the technology, the activity, and the social setting. It is not possible, nor is it desirable, for us to separate the contexts (social and physical) from the other components of the assistive technology system.
A final point to consider relative to the social context is that the degree to which different types of assistive technologies contribute to stigma differs. Stigma is defined as a mark of shame. Certain devices, such as hearing aids and power wheelchairs, seem to convey greater disability than others, such as spectacles or manual wheelchairs. Consequently, persons with disabilities may choose not to use particular assistive technology within a social environment because of the stigma it conveys. If others within an environment perceive an individual as generally incapacitated because of the presence of a specific disability, the individual may reject the use of an assistive device that brings additional attention to that disability. Consider an office worker, Ted, who has the capacity to use a manual wheelchair but who might choose to use a power chair because of the energy savings it affords. The behavior of certain colleagues in the office suggests that they perceive Ted to be less competent in performing his job tasks then he actually is. Ted’s reaction may be to minimize the appearance of his disability through use of a manual wheelchair, although this choice might result in negative consequences such as excessive energy expenditure and fatigue in the short term and shoulder injury in the long term.
Cultural Context
The effectiveness of assistive technology systems is closely related to and influenced by the cultural context. Krefting and Krefting (1991) define culture on the basis of three concepts: (1) “culture is a system of learned patterns of behavior,” (2) it is “shared by members of the group rather than being the property of an individual,” and (3) it includes effective mechanisms for interacting with others and with the environment (p. 102). The first of two of these are closely related to our definition of activity or occupation. The third concept, interaction with the external world both socially and physically, illustrates the relationship of culture to the social and physical aspects of assistive technology context. Thus these three elements of culture clearly couple it with the HAAT model and emphasize the importance of cultural considerations in the design and implementation of assistive technology systems.
Krefting and Krefting (1991) point out that we all view the world through a “cultural screen” (p. 105) that is the product of our experiences, family relationships, heritage, and many other factors. This cultural screen differs for each of us, and it biases the way we interact with others and the ways in which we perceive various activities, tasks, and life roles. For example, in some cultures leisure is recognized as a desirable and socially acceptable pursuit. However, in other cultures pursuit of leisure time is thought to indicate laziness and lack of productivity. If the ATP and the consumer have differing cultural screens, they may have difficulty establishing and achieving mutual goals. For example, if the ATP views leisure as a desirable and satisfying occupation, he or she may recommend assistive technology systems that enable leisure activities, which could include modified computer or video games or an adapted wheelchair for tennis or other sports. However, if the consumer is from a culture in which leisure is viewed as being nonproductive, he or she may reject these assistive technology systems as frivolous.
There are many cultural factors that must be considered when assistive technology systems are applied. Box 2-1 lists factors that affect how assistive technology systems are perceived and used by consumers from different cultures (Krefting and Krefting, 1991). These factors must be kept in mind by the ATP throughout the assistive technology delivery process. For example, consider three of these: importance of appearance, independence and its importance, and family roles. Wheelchair manufacturers now fabricate their products in a variety of colors, which allows choice and avoids the “institutional chrome” appearance for those who care about such things.
Another example involves Frank, a man with amyotrophic lateral sclerosis (ALS) (Murphy and Cook, 1985). Before his disability, Frank was dominant as head of his family. He was fiercely independent, and he valued his role as provider. As he lost the ability to speak because of the ALS, he used a small typewriter-like device to interact with his family. It allowed him to retain his head-of-household role, and he used his communication device to make investment decisions, plan legal affairs, and make shopping lists. His family provided the legwork to carry out his directions. As the ALS progressed, his motor control deteriorated until he could only raise his eyebrows. A new communication device, which used this limited movement, was obtained for him, but he was uninterested in using it. After repeated unsuccessful attempts to provide support for the use of this new device, those working with Frank began to realize that his role in the family had changed. Because of his dependence on aids and the difficulty in communicating with the new device, he lost all interest in his family role. His wife became the family leader, and she began to make decisions that had always been reserved for him. These changes in the family, a difficult concept for Frank because of his cultural perception of family roles, led to his withdrawal and the failure of the assistive technologies to meet his needs.
Institutional Context
The institutional context refers to larger organizations within a society that are responsible for policies, decision-making processes, and procedures. CMOP includes economic, legal, and political components, such as government-funded services, legislation, and political regulations and policies (CAOT, 2002). The ICF section that categorizes similar aspects is labeled services, systems, and policies (WHO, 2001). Services are “benefits, structured programs and operations in various sectors of society” that meet the needs of individuals (WHO, 2001, p. 192). Systems refer to the administrative and organizational layer, at all levels of government or other authorities, that plan, implement, and monitor services. Policies are rules, regulations, conventions, and standards that regulate systems, and again, exist at all levels of government or other organizations (WHO, 2001, p. 192).
The institutional context has major implications for the acquisition and use of assistive technology. Funding is probably the most influential element in this context. Funding policies and regulations establish who is eligible to receive assistance for the purchase of devices, which devices are supported in funding schemes and who (i.e., which professional group) serves as the funding gatekeepers. Government programs also provide regulation and support for environmental modifications that enable the inclusion of persons with disabilities. Funding of assistive technology devices and services is discussed in more detail in Chapter 5.
Legislation in many countries establishes laws, policies, and regulations that enable persons with disabilities to engage in activities in various contexts with both their local community and more broadly. These laws specifically comment on environmental access issues, modifications required in employment and educational and other community settings, and the responsibility of the employer or educational system in providing accommodations for eligible individuals, including the provision of assistive technology. Examples of such legislation include the Americans with Disabilities Act (1990), Ontarians with Disabilities Act (2005), and the Individuals with Disabilities Education Act (IDEA) (1997). The implications of legislation are discussed further in Chapter 1.
A final implication of the institutional environment on assistive technology is legislation and standards that govern product design, function, and safety standards. For a product to be marketed and, in particular, for it to be included as a device for which funding assistance is provided, the developers or manufacturers must ensure that testing and other measures have been undertaken to ensure that the product meets certain technical standards. Standards for individual types of assistive technologies are discussed in later chapters.
EXTRINSIC ENABLERS: THE ASSISTIVE TECHNOLOGIES
The final component shown in Figure 2-1 is the assistive technology. A detailed characterization of this component is presented in Chapter 1 (see Box 1-1). Assistive technologies are also described as extrinsic enablers because they provide the basis by which human performance is improved in the presence of disability. The components shown in Figure 2-5, B, represent the flow of information and forces among the assistive technologies and the other components of the HAAT model. Interaction with the human is through the human/technology interface component of the assistive technology. This component represents the boundary between the human and the assistive technology. This interaction is two way; that is, information and forces may be directed from the human to the technology or vice versa. For the technology to contribute to functional performance, it must provide an output, which is accomplished by the activity output component. The human-technology interface and activity output are linked by the processor, which translates information and forces received from the human into signals that are used to control the activity output. Finally, some assistive technologies (e.g., sensory aids) must also be capable of detecting external environmental data. The environmental interface accomplishes this function. Once the external data are detected, the processor interprets and formats them so they can be provided to the user through the human-technology interface. Not all assistive technologies have all the components of Figure 2-5, A. However, all of them have at least one of the components, and most have two or three.
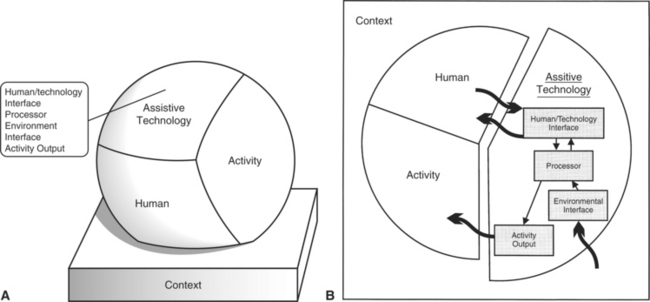
Figure 2-5 A, HAAT model with assistive technology elements identified. B, The assistive technology component of the HAAT model includes both the specific purpose and general purpose technologies.
Different sets of the components shown in Figure 2-5, A, are required to meet the needs of different consumers. These components function together to facilitate the completion of tasks that underlie specific activities. Because the use of assistive technologies has the effect of adapting the skills required for the task to match those of the human, these technologies enable the human operator. The specific characteristics of the assistive technology components are determined by the person’s needs and skills together with the goals determined by the activities to be performed. This process is described in Chapter 4 as part of the needs assessment procedures.
Human-Technology Interface
All the interactions between the human user of the technology and the device occur through the human-technology interface. As we have said, these interactions can occur in either direction (e.g., from human to technology or from technology to human), and they include both forces and information. Sometimes separate components are used to provide input to the device and output from the device. For example, a computer keyboard is used for typing and a video monitor provides feedback to the typist. Sometimes bidirectional interaction occurs in one component. For example, the computer keyboard provides tactile, auditory, and visual feedback to the typist.
Positioning devices, or postural support systems, are one type of human-technology interface. Any person must be stable and in a position that allows interaction with his or her environment to complete functional tasks. Some individuals with disabilities have insufficient postural control to support the efficient and effective movements needed for this interaction. Provision of some form of seating or positioning system can influence their postural control. As discussed in Chapter 6, the human exerts forces on the postural support system, and the postural support system exerts forces on the human. This two-way interaction also involves the human sensory system. For example, if paralysis causes absence of sensation, the human may not detect the forces exerted by the human-technology interface (e.g., a seat cushion). If the pressures exerted on the human user by the human-technology interface are too high or are unrelieved for too long, they can lead to tissue damage. Likewise, if the human user reduces the forces that the body exerts on the device’s human-technology interface (e.g., through performance of weight shifts), the total pressure at the human-technology interface is reduced, which decreases the possibility of tissue damage.
Another commonly used human-technology interface is called the control interface, the boundary between the user and an electronic or mechanical assistive technology device that allows the individual to operate, or control, the device. For electronic assistive technology systems, control interfaces include joysticks for power wheelchairs, keyboards for computers and communication devices, and single switches used to control household devices such as lights or radios. In addition to the motor output to the control interface exerted by the human user, sensory feedback is provided to the user during operation. This bidirectional interaction is essential to effective performance (see Chapter 7). The ways in which persons with disabilities are assessed for control interfaces, how they are selected, how they are used, and how training can be accomplished are also described in Chapters 4 and 7.
Displays that provide information to the human user are another type of human-technology interface. Displays are used in a wide range of technology, from power wheelchairs to computers to augmentative communication devices to environmental control systems to sensory aids. Examples include the lighted display of remaining battery energy on a power wheelchair and the lights used in a scanning display for augmentative communication. The major types of displays are visual, auditory (including synthesized speech), and tactile (e.g., Braille). Visual and tactile output modes are discussed further in Chapter 8. Speech output is discussed in Chapter 8.
Processor
Many assistive technology devices require control and processing of data to accomplish the desired functional task. The processor, often a computer, performs these actions. Many assistive devices (e.g., power wheelchairs, environmental control units) contain computers as integral components. These greatly increase flexibility and adaptability in performing functional tasks and also allow systems to be tailored to individual needs much more readily. Stand-alone personal computers also play an important role in increasing access to education, work, financial management, and recreation for persons with disabilities. The role of computers in assistive technology systems is discussed in Chapters 7 and 8. The processor in an assistive technology device may also be a simple mechanical component that links the control interface to the activity output. A common manipulation device is a mechanical reacher, which is used to obtain objects from shelves that are too high. The user controls the reacher through a hand grasp, which is coupled with a mechanical linkage that closes a gripper to reach and carry the object. In this case the mechanical linkage is the processor.
Activity Outputs
The activity outputs include communicating; moving from place to place; manipulating objects for self-care, work, school, or recreation; and performing cognitive activities. Each of these activities can be either replaced by a functional equivalent (e.g., a computer word processor for someone who cannot use a pencil and paper) or augmented (e.g., a holder that allows someone with limited grip to manipulate the pencil). Assistive technology systems may provide one or more activity outputs that facilitate performance. These outputs include communication, manipulation, mobility, and cognition. The activity output for communicating is transmission of information, usually provided through voice synthesis, visual display, or printed copy. Devices for manipulation are either special purpose (e.g., a modified spoon, brush, or shoe horn) or general purpose (e.g., environmental control units or robotic systems). Wheelchairs, modified driving aids for vehicles, and similar devices provide mobility outputs. Memory aids, computer sensors within the home, and computer software such as word recognition provide cognitive outputs.
Environmental Interface
The final component of the assistive technology, the environmental interface, provides the link between the device and the external world, represented by the context. This interface supports sensory performance: seeing, hearing, and feeling. For augmentation or replacement of vision, the environmental sensor is a camera capable of imaging the information to be input to the human. Two broad classes of performance are typically aided: reading and orientation and mobility for persons with visual impairments. Systems for aiding hearing often use a microphone as an environmental interface. Finally, systems designed to assist with tactile input (feeling) use transducers to detect external pressures or forces. The environmental interface is linked to the human-technology interface by a processor, often a computer.
Soft Technologies as Extrinsic Enablers
The extrinsic enablers described for general and specific purposes are hard technologies. Soft technologies can serve as extrinsic enablers, in addition to their role as strategies that were included as part of the human component of the HAAT model. For example, performance aids, written instructions, and training are all extrinsic enablers. Performance aids are often conceptual (e.g., a method of remembering vocabulary in a communication system by using pictures that can have multiple meanings). Marion, our augmentative communication system user, benefits from the use of soft technologies. With the electronic communication system, Marion must use codes to represent words or phrases. If she has many codes or difficulty remembering the codes, a list of the codes can be displayed on the device. This is referred to as a performance aid.
Training is often required to make a system useful. Not only the user but also the caregivers and family must be included in this training process. When adequate training in the use of an assistive device is provided to both the user and caregivers, that device is more likely to be used properly, with less likelihood of abandonment (Chen et al, 2000). Finally, written instructions and other documentation can make the difference between success and failure in the use of an assistive device. The quality of these materials varies widely. Performance aids, training, and development of written documentation are discussed in Chapter 4.
Assistive Technology Devices for Specific Applications
Specific application devices for mobility, communication, or manipulation have a human-technology interface, a processor, and an activity output. For example, for a manual wheelchair system, the human-technology interface includes positioning components and the push rims used for turning the wheels. The processor consists of the mechanical linkages between the push rims and wheels, and the activity output is mobility. For augmentative communication, the human-technology interface has two parts: a control interface and a user display. The processor is typically a computer with a software program that relates the control interface to stored vocabulary and controls the outputs. The output is synthetic speech, print, or visual display. An environmental aid to daily living for television, lights, telephone dialing, and other appliance control typically has a keypad or single switch and display as the human-technology interface. The processor is an electronic circuit, possibly a computer. The output is a signal or signals used to control the appliance and replace direct physical manipulation of its controls (e.g., television channel change or volume control).
Sensory aids have an environmental interface, a processor, and a human-technology interface. For example, a hearing aid uses a microphone as an environmental sensor, an amplifier as a processor, and a speaker (often called a receiver) as a human-technology interface. A reading machine for persons with severe visual impairments uses a camera as an environmental sensor, a computer as a processor, and a speech synthesizer as the human-technology interface.
APPLICATION OF THE HUMAN ACTIVITY ASSISTIVE TECHNOLOGY MODEL: DESIGNING ASSISTIVE TECHNOLOGY SYSTEMS FOR SUCCESSFUL OUTCOMES
To meet the needs of an individual, an assistive technology system must be designed, although this idea does not refer to the research and design process that results in the development of a new product. Rather it means the ultimate recommendation of assistive technology and how it will be used by a certain person within relevant contexts. An assistive technology system is designed through the process of assessing a consumer’s needs, goals, and skills; using these to determine the necessary characteristics that an assistive technology system must have; conceiving of and planning the system for that individual; delivering the device and training in its use; and following up to evaluate success. In this section the assistive technology system is defined and then a process for designing such systems is described.
Assistive Technology System
In the previous sections each of the four components of the assistive technology human performance model was discussed. The assistive technology system is defined to be the four components shown in Figure 2-1. Needs arise from all aspects of a person’s life, and the assistive technology system goals are defined by the chosen activities (see Figure 2-2). The tasks required by the activity, together with the contexts of use (see Figure 2-4) and the human operator’s skills, determine the characteristics of the assistive technologies. The tasks must be matched to the human operator’s abilities and skills to be completed successfully. This match is facilitated through the assistive technologies that replace or augment the human operator’s function that would be precluded by his disability. The choice of the assistive technology characteristics (see Figure 2-5) and the matching of them to the skills and needs of the consumer complete the design process and the specification of the assistive technology system.
Define Key Activities
The first step in the process of designing the assistive technology system is the identification of an activity or activities that are meaningful to the consumer (Figure 2-6). These are activities that the consumer either needs or wants to do. The categories of self-care, productivity, and leisure, described earlier, are useful to help organize the evaluation and ensure that relevant activities are identified. The Canadian Occupational Performance Measure (Law et al, 1998) is a useful tool to assist with this identification. It involves the client and the ATP in a process that identifies important activities in self-care, productivity, and leisure areas and is useful to initiate a discussion of how and where these activities occur.
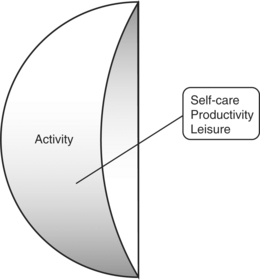
Figure 2-6 The first step in designing the assistive technology system is to define the key activities.
There are a number of questions that help define the activity. Who will perform the activity? Is it important for the client to perform the activity independently or will he or she accept assistance from others or technology? When the client will accept assistance from others, it is important to determine whether this assistance can be provided by family, friends, or a personal care attendant. If the activity is a sensitive one, such as toileting, the consumer may be very particular about the person from whom he or she will accept this assistance.
It is important to determine the meaning of the activity to the consumer and what adaptations they will accept to that activity. Klinger and Spaulding (1998) identified several different ways in which an activity could be adapted, including changing how it is completed, who does it, when and how frequently it is completed, stopping the activity, and substituting one activity for another. The consumer’s acceptance of adaptation of an activity will depend on the meaning that engagement in that activity has for them. For example, a consumer who performed an activity at a highly skilled level, such as a competitive sport, may not find satisfaction with involvement in the same activity if his or her performance no longer meets previous standards. The meaning given to the activity will be a predictor of whether the consumer will accept technology as an alternate means to its completion (Spencer, 1998).
An additional factor that helps to define the activity relates to time. How frequently does the consumer engage in that activity and will a change be accepted in that activity? One that is completed regularly and frequently is of higher priority than something that is only done infrequently. It is also useful to ask how long it takes the person to complete the task and whether the person is willing to invest that amount of time in it.
A thorough occupational or activity analysis is important for identification of the task demands. These demands are considered to be physical, cognitive, or affective skills, knowledge, or behaviors that are required for successful completion of the activity. Although they are attributes of the human, they are independent of the attributes of any specific individual. Rather, the analysis describes the skills, behaviors, and so forth required to successfully complete the activity and its subtasks. Several schemes for conducting an occupational or activity analysis are found in the literature (e.g., Blesedell Crepeau, 2003; Watson, 1997).
Consider the Perspective of the User
Once the activities have been defined, with input from the user, the focus of the system design process shifts to the human (Figure 2-7). The activity and the human are linked and it is artificial to separate the activity from the person. In this section the focus is on the attributes, perceptions, and preferences of the specific individual who will use the assistive technology. A thorough assessment should be completed of the user’s physical and cognitive abilities and his or her affective state. Elements of the physical, cognitive, and affective domains and assessment specific to each of the types of assistive technologies are discussed in subsequent chapters.
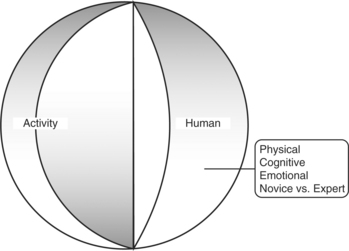
Figure 2-7 Once the activities are defined, the skills and perspective of the human user should be investigated.
Individual choice is important to determine at this stage. The consumer participates in the choice of activities in which to engage and the choice of how to adapt a specific activity. The assistive technology practitioner contributes expertise that assists the consumer in the choice of assistive technologies but must recognize the consumer’s right to exercise that choice. How much input the ATP must have depends on many things such as whether the consumer is a novice or expert assistive technology user and the capacity of the consumer and the caregivers to understand the implications of the use of the assistive technologies for the consumer.
Choice is also seen in how a consumer completes an activity. Denison (2003) theorized that assistive technology users choose between performing a task themselves, using technology, or seeking assistance from others. For any given activity, the person may choose a combination of these three components. Let’s return to the case of Marion presented at the beginning of this chapter. In some situations, she chooses to use a voice output communication aid for oral communication. When she uses this device, she performs some of the task herself (physically accessing the device), she may rely on another person to set up the device for her, and she relies on the device for oral output. In this situation, she primarily chooses to use her own abilities and the device to complete the task of communication.
What are some of the factors that influence a person’s choice to complete an activity himself or herself, receive assistance from another or use technology, or, as in the example above, some combination of the three? These factors are unique to the individual user and are outside the person’s actual physical and cognitive abilities. The individual may choose to complete an activity, or part of it, when the individual perceives himself or herself to have the ability to do so (i.e., self-efficacy [Bandura, 1977]). Conversely, when the person does not believe that he or she has the ability to perform a task, the person is more likely to avoid doing it altogether or rely on someone else even when he or she actually has the ability.
People make choices in their activities partially on the basis of the amount of energy they are willing to expend on the activity. For example, a person with a spinal cord injury resulting in quadriplegia who works outside the home may choose to have a personal care attendant assist with bathing and dressing in the morning when these activities would require a significant time and energy investment to be completed independently. So, even when a person is physically capable of completing a task on his or her own, it might not be worth the energy consumption if it leaves the person tired and unable to engage in activities that carry a higher personal importance. To some extent, people make choices on the basis of short- and long-term benefits and risks. The person with a spinal cord injury might be physically capable of propelling a manual wheelchair independently. However, evidence is confirming that long-term manual wheelchair use results in repetitive injuries to the shoulder (Curtis et al, 1994) that affects not only wheelchair propulsion but other important activities such as transfers. Thus, although physically capable of propelling a manual wheelchair, the client might choose to use a power chair to conserve the integrity of the joints and energy consumption, both for the short-term gains of engaging in meaningful activities and long-term benefits of retaining physical abilities.
Features of the device itself will determine whether or how the individual chooses to use it to complete an activity. A device that is reliable (i.e., performs the task for which it is intended in a consistent manner) and one that is simple and intuitive to use is more likely to be used than one that is not (Pape, Kim, and Weiner, 2002). If use of a device conveys a stigma, then it is less likely that the person will choose to use it. Esthetics, portability, maintenance, and affordability are other device features that have been shown to influence whether a person will choose to use a device.
Elements of the social environment also affect a person’s choice of how to complete an activity. Assistance is more likely to be received from another person when that person is knowledgeable of and effective with the assistance provided. In the example of Marion, her decision to use a communication board versus a VOCA was made, in part, on the basis of her specific communication partner. The communication board requires more assistance from another person (as the person must interpret the symbols or understand her abbreviations) so it was only used with more familiar partners. The VOCA, which requires less effort on the part of the communication partner, was used with less familiar partners.
Others in the environment can influence the choices an individual makes regarding task completion. For some the notion of “use it or lose it” results in the individual expending more of his or her own effort on a task. A common example is the use of a power versus a manual wheelchair. A person who chooses power over manual mobility may be seen as lazy by others, including family or therapists, even when the power chair enables more independence in other functional areas. Others may only focus on a single activity, in this case wheelchair propulsion, rather than seeing the larger picture, which may be for example, the energy expenditure of a university student propelling himself or herself across campus. In this case, the person may be so tired from propelling the chair that he or she has difficulty concentrating on academic tasks.
Finally, the choice may be dependent on what the environment will support. If a person is not available to provide assistance in a certain environment, then alternate means of completing a task must be sought. Similarly, as has been discussed previously, different environments support the use of technology in different ways. A power wheelchair may be an excellent mobility choice when moving about the community but be less effective for mobility within the confines of a home. Voice recognition software may be a very effective means of entering information at home or in a private office where ambient noise and proximity of others are limited.
Together the personal attitudes of the user, the effectiveness of the technology in supporting the activity, and the ability of the environment to support the activity all influence the choice that the individual makes when determining how to complete an activity. The assistive technology provider’s role is to ask the questions and serve as a resource for the individual to assist with this decision-making process.
Consider the Environment
There are a number of important questions to answer regarding the environment when the assistive technology system is being designed. We discussed the effect that the environment has on the user’s choice of how to complete the activity. Some additional questions include the following: Where will the assistive technology be used? Does the consumer expect to use it in a single environment (e.g., the home or workplace) or does the consumer need to use, and thus transport it, to different locations, in which case portability and flexibility are important? If the technology is to be used across many different environments, the effect of the environment on its use must be considered. For example, extremes of temperature will affect the performance of the materials used to construct seating systems. In northern climates, extreme cold has the potential to alter the material properties, therefore influencing the ability of the device to distribute pressure. Similarly, extremes of temperature will have a detrimental influence on any device with electronic components. Available light and sounds within the environment will also influence device performance.
The effect of the environment on the performance of the activity is another consideration. What are the differences in how an activity is or can be performed across all pertinent environments? Environments that incorporate universal design principles (see Chapter 1) facilitate performance of activities by individuals with a variety of abilities. Institutional policies and procedures can be barriers or enablers to performance of an activity and may even determine whether an individual has access to necessary technology.
When a device must be used in a variety of environments, the complexity of its setup is an important consideration. A device that is very complex to set up may not be used across various environments because the setup is too time consuming and the potential for error is great. Even when device setup is simple, such as replacing a seat cushion in a wheelchair, there is a potential for misuse if the individual replacing it is not familiar with its use. Most assistive technology providers have seen wheelchair cushions placed backward in the wheelchair, obviously compromising their performance.
Funding is another reason why it is important to determine where the device will be used. Under some funding schemes, a person is only eligible to receive a device if it is used in a specific environment such as the home. In such a situation, the ATP must determine that the device and the environment in which it is to be used are compatible. Issues such as physical access and social support for use of the device are important considerations here.
At this point, definition of the activities in which the person wants to participate, an assessment of the abilities of the user along with his or her personal choice in how to complete an activity, and the influence of the environment on the use of assistive technology have been discussed. Now, selection of the assistive technology will be discussed.
Selecting the Assistive Technology
Figure 2-8 shows the interaction of the activity, the human, and the assistive technology nested within the context. Two issues will be discussed relative to selecting the assistive technology. The first is a hierarchy of assistive technology described by Trefler and Hobson (1997) (Box 2-2). The second is the notion of function allocation (Bailey, 1996) that comes from human factors engineering.
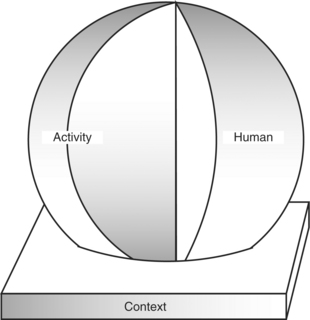
Figure 2-8 Consider the influence of the context on the human user’s performance of desired activities.
The device abandonment literature suggests that assistive technology that is simple to use is less likely to be abandoned than that which is more complex. Trefler and Hobson (1997) describe a hierarchy that moves from simple, relatively easy-to-obtain devices to those that are more complex and more difficult to obtain. Their premise is that the ATP should recommend a device that is as simple as possible yet still meets the client’s needs. As you can see from Box 2-2, these devices range from those that are commercially available for general consumption to those that are custom made for a single individual. Although it is tempting sometimes to recommend or purchase a device that promises to perform a wide variety of functions, unless the user needs or wants all the functions, a simpler device is usually the better option. Think about all the various functions that are available on current cell phones and person digital assistants. Most people do not use all these functions, even when they add to the cost. The same holds true for assistive device selection.
Allocation of Functions
In any human/device system some functions can be allocated to the human, some to the device, and some to the Personal Assistant Services (PAS). Bailey (1996) defines several approaches to function allocation that are used in general human factors design. Several of these are applicable to the design of assistive technology systems and are useful for both the user and ATP when determining how and what type of assistive technology will be beneficial to the individual. The simplest approach is comparison allocation. Here each task to be carried out is assigned completely to the human or to the device. The user’s skills define the task that can be assigned to him or her; the characteristics of the technology determine which capabilities are assigned to it. For example, a standard telephone is designed with the assumption that the user can hold the handset, press the buttons to dial, hear the other person, and speak into the telephone. These are all functions assigned to the user. However, if the user cannot perform any of these tasks, the assistive technology must provide an alternative set of tasks. For example, assume that a particular consumer is able to carry out all the functions except holding the handset and dialing. A speaker phone, which avoids the need to hold the handset, together with a mouth stick for dialing, could be used. These constitute the assistive technology component of this system. Often comparison allocation is used when characteristics of technology are matched to a consumer’s skills.
A second allocation approach is leftover allocation, in which as many functions as possible are assigned to the human and the device carries out the remainder. In assistive technology system design, this approach is often followed to give the consumer as much natural control over his activities as possible but to provide assistance when needed. For example, some manual wheelchairs are equipped with power assist wheels that amplify the user’s propulsion strokes. Thus a person who has limited strength and endurance can propel the wheelchair manually but the power assist wheels augment their abilities.
A third approach is economic allocation, in which the basic consideration is whether it is cheaper to select, train, and pay a personal assistant to do the activity or to design an assistive technology system for this purpose. Often the economic analysis initially favors the personal assistant because the purchase cost of the technology is relatively high. However, if the technology cost is amortized over its useful life, the technological approach may be significantly less expensive because the personal assistant cost (salary) rises over time.
The final approach that we use when designing an assistive technology system is flexible allocation. In this approach the consumer can vary his or her degree of participation in the activity on the basis of skills and needs. Whenever possible, we use this approach in assistive technology systems, and we couple the use of the AT system with PAS. The human and technology components are not fixed in scope; they change on the basis of specific activities and tasks to be carried out. Initially the novice operator may rely more heavily on intuitive skills to perform the desired tasks. As knowledge of the device operation increases and strategies are developed, the tasks carried out by the human operator change and system operation becomes more efficient. The role of PAS may also change over time.
As an example, consider the case of Pat.
Flexible allocation also allows for the system to change to account for decreasing human function, as in the case of degenerative disease. For example, an individual with muscular dystrophy generally regresses from walking to using a manual wheelchair and then to a powered wheelchair as the disease progresses. This loss of function often requires two new systems, a manual and a powered wheelchair. However, there are add-on powered units that can be attached to a manual wheelchair. The use of an add-on unit makes the basic manual wheelchair more flexible and allows the transfer of functions from the human (upper body strength to propel a manual wheelchair) to the device (an electric motor to power the wheelchair). Similar considerations apply to individuals whose abilities, and resulting performance, fluctuate throughout the day or from day to day because of changing neuromuscular capabilities (e.g., muscle tone, strength, attention) or fatigue. Often this fluctuation in abilities is great, and the system must compensate for these changes. If the system is able to reallocate functions flexibly, the consumer will be able to accomplish tasks with greater device assistance when he or she is tired and will be able to exert more control and independence when well rested.
Some extrinsic enablers are more flexible than others, and they allow continual alteration in the allocation between the human and technology. For example, computer-based devices can be altered by software to perform many functions with the same control interface. On the other hand, some extrinsic enablers, including some seating and postural support systems, are less flexible, and they must be redesigned or adjusted if the human component changes significantly (e.g., when a child goes through a growth phase).
SUMMARY
In the previous sections each of the four components of the assistive technology human performance model has been discussed. The assistive technology system was defined to be the four components shown in Figure 2-1. Needs arise from all aspects of a person’s life, and the assistive technology system goals are defined by the chosen activities (see Figure 2-2). The tasks required by the activity, together with the contexts of use (see Figure 2-4) and the human operator’s skills, determine the characteristics of the assistive technologies. Tasks must be matched to the human operator’s abilities and skills to successfully complete desired activities. Facilitation of this match is accomplished through the assistive technologies, which enable the consumer to complete tasks that would be precluded by his disability. The choice of the assistive technology characteristics and the matching of them to the skills and needs of the consumer, and the influence of the context complete the design process and the specification of the assistive technology system. Figure 2-1 illustrates this integrated assistive technology system.
The following chapters will expand on aspects of human performance, evaluation of the assistive technology system and then describe specific types of assistive technology in greater detail.
1. Describe the three elements common to the ICF, CMOP, and HAAT models. How does the HAAT model differ from the other two? What is the purpose of the HAAT model?
2. What are the three basic performance areas defined in the HAAT model? Give an example of each.
3. Describe the relationship between tasks and activities. How is this knowledge applied to assistive technology selection?
4. Describe the five components of occupational competence and discuss how they affect the use of assistive technology.
5. What is meant by the terms novice and expert, and how do they affect assistive technology application?
6. Distinguish between ability and skill.
7. Describe the role that strategies play in the use of assistive technology systems. How can strategies compensate for the absence or inadequacy of an assistive technology?
8. Describe the four major parts of the context and how each can affect overall assistive technology system performance.
9. What are the three physical parameters of the physical context of the HAAT model? How do they affect the performance of assistive technology?
10. How do cultural considerations affect the application of assistive technology systems?
11. Explain the shift in thinking regarding societal participation by persons who have disabilities; that is, where is the “problem” with this participation thought to lie? What implications does this have for assistive technology applications?
12. What is meant by the term institutional environment in relation to considerations of the context of assistive technology application?
13. What are the four components of the assistive technology portion of the HAAT model?
14. Why do we refer to assistive technologies as extrinsic enablers?
15. Describe three factors that affect users’ decision of whether to use assistive technology to assist with daily activities.
16. Describe the process of designing an assistive technology system.
17. Define the term stigma. How does it affect assistive technology selection and use?
18. What is the influence of the environment on assistive technology selection and use?
19. What is meant by the term function allocation, and how is it applied to assistive technology systems?
20. What are the major approaches to function allocation? What are the strengths and weaknesses of each approach when used in assistive technology system design?
References
American Occupational Therapy Association. Occupational therapy practice framework: domain and process. Am J Occup Ther. 2002;56:609–639.
Americans with Disabilities Act of 1990, 42 U.S.C. §§ 12101 et seq.
Bailey, RW. Human performance engineering, ed 3. Upper Saddle River, NJ: Prentice Hall, 1996.
Bandura, A. Social learning theory. Englewood Cliffs, NJ: Prentice-Hall, 1977.
Bickenbach, J, et al. Models of disablement, universalism and the international classification of impairments, disabilities and handicaps. Soc Sci Med. 1999;48:1173–1187.
Blesedell Crepeau, E. Analyzing occupation and activity: a way of thinking about occupational performance. In: Blesedell Crepeau E, Cohn ES, Boyt Schell BA, eds. Willard and Spackman’s occupational therapy. ed 10. Philadelphia: Lippincott, Williams & Wilkins; 2003:189–198.
Brooks, NA. Models for understanding rehabilitation and assistive technology. In: Gray DB, Quatrano LA, Lieberman ML, eds. Designing and using assistive technology: the human perspective. Baltimore: Paul H Brookes Publishing; 1998:3–11.
Brooks, NA. User’s perceptions of assistive devices. In: Smith RV, Leslie JH, eds. Rehabilitation engineering. Boca Raton, FL: CRC Press, 1990.
Canadian Association of Occupational Therapists. Enabling occupation: an occupational therapy perspective, ed 2. Ottawa: CAOT Publications/ACE, 2002.
Chen, T, et al. Caregiver involvement in the use of assistive devices by frail older persons. Occup Ther J Res. 2000;20:179–200.
Christiansen, C, Baum, C. Person-environment occupational performance: A conceptual model for practice. In Christiansen C, Baum C, eds.: Occupational therapy: enabling function and well being, ed 2, Thorofare, NJ: Slack, 1997.
Church, G, Glennen, S. The handbook of assistive technology. San Diego, CA: Singular Publishing Group, 1992.
Curtis, KA, et al. Shoulder pain in wheelchair users with tetraplegia and paraplegia. Arch Phys Med Rehabil. 1999;80:453–457.
Denison I: Technology: How much is enough? Proceedings of the Canadian Seating and Mobility Conference, Toronto, 2003.
Enders A: Technology for the next millennium: building a framework for collaboration. Presented at the 1999 conference of the Association for the Advancement of Assistive Technology in Europe (AAATE), Dusseldorf, Germany, November 1999.
Fougeyrollas, P. The influence of the social environment on the social participation of people with disabilities. In: Christiansen C, Baum C, eds. Occupational therapy: enabling function and well being. ed 2. Thorofare, NJ: Slack; 1997:378–391.
Fougeyrollas, P, Gray, DB. Classification systems, environmental factors and social change. In: Gray DB, Quatrano LA, Lieberman ML, eds. Designing and using assistive technology: The human perspective. Baltimore: Paul H Brookes Publishing; 1998:13–28.
Individuals with Disabilities Education Act Amendments of 1997, U.S.C.A. § 600, et seq.
Klinger, L, Spaulding, S. Chronic pain in the elderly: silence is golden. Phys Occ Ther in Geriat. 1998;15:1–17.
Krefting, LH, Krefting, DV. Cultural influences on performance. In: Christiansen C, Baum C, eds. Occupational therapy. Thorofare, NJ: Slack, 1991.
Law, M. 1991 Muriel Driver Memorial Lecture. The environment: a focus for occupational therapy. Can J Occup Ther. 1992;58:171–180.
Law, M, et al. Canadian Occupational Performance Measure, ed. 3. Toronto: CAOT/ACE Publications, 1998.
Matheson, LN, Bohr, PC. Occupational competence across the life span. In: Christiansen C, Baum C, eds. Occupational therapy: enabling function and well-being. ed 2. Thorofare, NJ: Slack; 1997:428–457.
Miller Polgar, J, Landry, J. Occupations as a means for individual and group participation in life. In: Christiansen C, Townsend E, eds. Introduction to occupation. Upper Saddle River, NJ: Prentice Hall; 2004:197–220.
Murphy, JW, Cook, AM. Limitations of augmentative communication systems in progressive neurological diseases. In: Proceedings of the 8th Annual Conference on Rehabilitation Technology. Washington, DC: RESNA; June 1985:120–122.
Ontarians with Disabilities Act, Bill 118, Chapter 11 of Statutes of Ontario, Legislative Assembly of Ontario, 2005.
Pape, TL, Kim, J, Weiner, B. the shaping of individual meanings assigned to assistive technology: a review of personal factors. Disabil Rehabil. 2002;24:5–20.
Pope A, Brandt E, eds. Enabling America: Assessing the role of rehabilitation science and engineering. Washington, DC: National Academy Press, 1997.
Scherer, M. The impact of assistive technology on the lives of persons with disabilities. In: Gray DB, Quatrano LA, Lieberman ML, eds. Designing and using assistive technology: the human perspective. Baltimore: Paul H Brookes Publishing; 1998:99–115.
Spencer, J. Tools or baggage? Alternative meanings of assistive technology. In: Gray DB, Quatrano LA, Lieberman ML, eds. Designing and using assistive technology: the human perspective. Baltimore: Paul H Brookes Publishing; 1998:89–98.
Trefler, E, Hobson, D. Assistive technology. In: Christiansen C, Baum C, eds. Occupational therapy: enabling function and well-being. Thorofare, NJ: Slack; 1997:482–506.
Watson, DE. Task analysis: An occupational performance approach. Bethesda, MD: American Occupational Therapy Association, 1997.
World Health Organization. International classification of impairments, disabilities, and handicaps: a manual for classification relating to the consequences of diseases. Albany, NY: World Health Organization Publication Center, 1980.
World Health Organization. International classification of functioning, disability and health (ICF). Geneva: World Health Organization, 2001.