CHAPTER 26 Root Morphology and Instrumentation Implications
 Discuss significance of root morphology and positioning in the alveolar bone to root instrumentation. Describe the roots of each of the permanent teeth in terms of numbers, shapes, and characteristic landmarks.
Discuss significance of root morphology and positioning in the alveolar bone to root instrumentation. Describe the roots of each of the permanent teeth in terms of numbers, shapes, and characteristic landmarks.Various instruments (e.g., the periodontal probe, Nabers probe, dental explorer) are used for assessing root surface characteristics. Current periapical and vertical bitewing radiographs placed on the view box provide information on root number, shape, and alterations; furcation location; bone height and contour; and calculus, caries, and defective restorations that may influence instrumentation.
An anatomically correct model of the dentition with transparent gingiva is helpful for visualizing anatomy of individual roots and their positioning within the alveolar processes. Models and Table 26-1 can be used for review. See Chapters 17 and 24 for a review of periodontal assessment and assessment instruments.
TABLE 26-1 Characteristics of Roots
| Maxillary Arch | See Figure 26-17, A |
|---|---|
| Tooth No. 8 | |
| Tooth No. 7 | |
| Tooth No. 6 | |
| Tooth No. 5 | |
|
Elliptic in cross-section; broad proximal surfaces Root is approximately one and one third times the length of the crown∗
|
Tooth No. 4 |
|
Palatal root is longest and extends out beyond the lingual surface of the crown (lingual root concavity on its palatal surface)
Mesiobuccal and distobuccal roots may appear as a “pair” with their apices curved toward each other; look like pliers
|
Tooth No. 3 |
| Tooth No. 2 | |
| Mandibular Arch | See Figure 26-17, B |
| Central and Lateral Incisor | Tooth No. 25 |
| Tooth No. 26 | |
| Tooth No. 27 | |
| Tooth No. 28 | |
| Tooth No. 29 | |
| First Molar† | Tooth No. 30 |
|
Furcations on facial and lingual surface, facialconcavity before the furcation begins just apical to the CEJ
|
|
| Second Molar† | Tooth No. 31 |
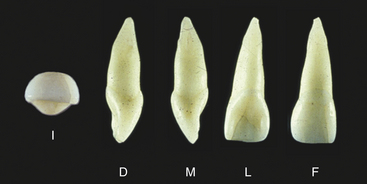

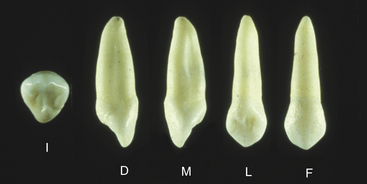
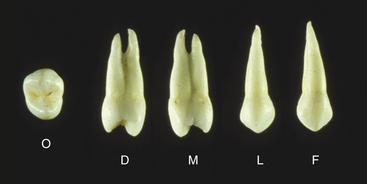
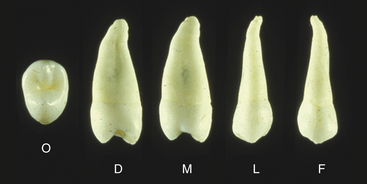
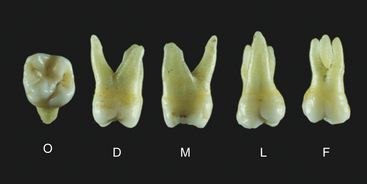


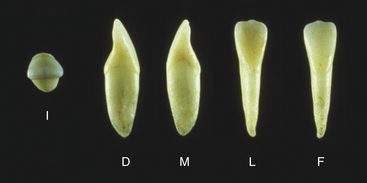

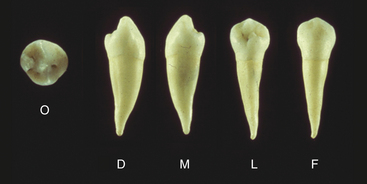
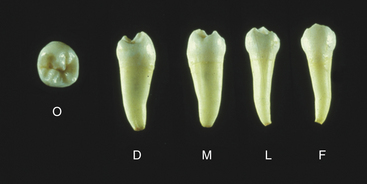

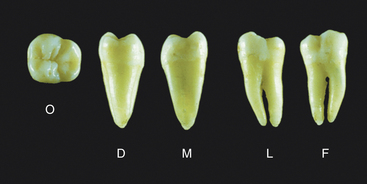
I, Incisal; D, distal; M, mesial; L, lingual; F, facial; O, occlusal.
∗ Knowing the length of the crown of a tooth is helpful in assessing the length of its root and the amount of attachment:
Maxillary central and lateral incisor crowns are the longest in the dentition, being approximately ½ inch in length. Anterior crowns are approximately 2 to 3 mm longer than posterior crowns. Roots range from approximately 12 to 17 mm in length; incisor roots are the shortest, and canines are the longest. Proportionally, when the length of roots is compared with the length of crowns, molars have the longest roots (because of their short crowns), and maxillary incisors have the shortest.† Crowns of all mandibular posterior teeth are lingually inclined and make instrument placement more difficult.
GENERAL MORPHOLOGIC CONSIDERATIONS
See Table 26-1 (Figures 26-1 through 26-14) for specific information for each tooth.
Root Terminology
The anatomic root of a tooth is that part of the dentin covered by cementum and embedded in the alveolar bone; it begins at the cementoenamel junction. The end of the root is called the root apex, and the area surrounding the apex is the periapex. At the apex is an opening, the periapical foramen, where the blood vessels and nerves enter the pulp (root) canal.
Teeth have one, two, or three roots. Teeth with two or three roots have an unbranched portion called the root trunk. The area where the root trunk branches into two roots is the furcation or furca. The opening into the furcation is the furcation entrance (Figure 26-15). The most coronal portion of the furcation is the furcation roof, which is often more coronal than the furcation entrance. The area between the roots of a two- or three-rooted tooth is the interfurcal or interradicular area.

Figure 26-15 Root terminology: root trunk and furcation entrance.
(Courtesy former Department of Dental Hygiene, Marquette University.)
When the junctional epithelium has migrated apically and there is clinical attachment loss, portions of the anatomic root are included in the definition of a clinical crown, the unattached portion of a tooth. The concept of cervical, middle, and apical thirds is one that is used when discussing root anatomy.
Cementoenamel Junction
The cementoenamel junction (CEJ) or cervical line is a structure that the dental hygienist must be able to identify subgingivally with an instrument. In health the CEJ is located within 1 mm of the free gingival margin and is slightly covered by free gingiva. The CEJ is the fixed landmark in the identification of the amount of attached gingiva. Subgingival identification of the CEJ is a competency that requires knowledge of root anatomy, development of tactile skill, and experience. Tactile, nonvisual indicators of the CEJ might include the following:
Facial and lingual contours of the CEJ on anterior and premolar teeth are convex (Figure 26-16); on molars, the CEJ is much straighter. An apical dip of the CEJ, called the cervical enamel projection (CEP), may be present toward the furcation on molars. Proximal curvature of the CEJ is more pronounced on anterior than on posterior teeth.

Root Surface Texture
Surface textures of crowns and roots differ owing to different degrees of mineralization of enamel and cementum and how it is altered by oral biofilm, as follows:
Cementum (anatomic root) is not as smooth, hard, or glassy but is more porous. Cementum can be altered by:
During root planing, varying amounts of cementum are removed and dentin may be exposed, resulting in dentinal hypersensitivity (see Chapter 38).Root Shapes
Roots of permanent teeth vary from one individual to another. For placement of instruments on root surfaces, the following are considered:
Teeth with One Root (see Table 26-1 and Figure 26-17)
All anterior teeth and maxillary second and mandibular premolars have one root. Characteristics of teeth with one root include the following:
Cone shape with facial, lingual, and proximal surfaces converging (tapering) apically with different degrees of convergence Cervical cross-sections (i.e., crown cut off the root horizontally at CEJ) are triangular, ovid, or elliptic (see Figure 26-17, A and B):
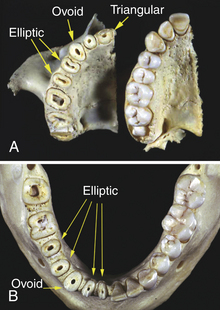
Figure 26-17 Root shapes in cervical cross-section. A, Maxillary teeth: triangular, elliptic, and ovoid. B, Mandibular teeth: elliptic and ovoid.
(Courtesy former Department of Dental Hygiene, Marquette University.)
In midroot sections, shapes of roots are generally the same as in cervical sections, though smaller.
Roots that are triangular or ovoid in cross-section have smaller lingual than facial surfaces because of proximal surface convergence (taper) toward the lingual surface. Cervical cross-section shapes may be altered by the presence of root concavities. The cervical half of a conical-shaped root has more than 50% of the root surface area because of the convergence of surfaces apically.
Teeth with Two or Three Roots (see Table 26-1)
For periodontal assessment and instrumentation, each root of a multirooted tooth must be treated individually—that is, a two-rooted tooth is like having two single-rooted teeth. In addition, the complexity of unbranched root trunks and furcas must be considered. Posterior teeth are more difficult to reach, and the clinician’s competence influences the therapeutic outcome. Characteristics of the teeth with more than one root are as follows:
Maxillary molars
Cervical cross-sections of maxillary and mandibular molar roots are larger and more difficult to describe (see Figure 26-17).

Figure 26-18 Mesial furcation on a maxillary first premolar.
(Courtesy former Department of Dental Hygiene, Marquette University.)

Furcations
Furcations generally begin as a shallow depression on the root trunk that gradually opens into a space between the roots; this opening may be too narrow for instruments. Initially, furcations can be felt by the working end of a dental explorer and then, as the space widens, by a Nabers probe. Furcations are very difficult to access with traditional scaling and root planing instruments, as their working ends are too large. Rather, precision thin and furcation inserts for ultrasonic instruments, microbladed and minibladed curets with smaller and narrower working ends, curets with extended shanks, and furcation curets are used to debride furcation areas (see Chapters 24, 25, and 28). A very narrow furcation entrance can be surgically enlarged with burs by a periodontist. Furcation characteristics are as follows:
Furcations are generally more cervical on first molars; root trunks of first molars are shorter than root trunks of second or third molars. Furcations close to the CEJ are more likely to become involved with periodontal disease, though access for instrumentation is easier and therefore such disease has a more favorable post-therapy prognosis. Furcations close to the apex are less likely to result in furcation involvement, though instrument access is more difficult and post-therapy prognosis is less favorable. Furcation involvement occurs when there is a loss of attachment apical to the furcation and is classified according to extent (see Chapter 17, Table 17-5 for classification of furcations).It is important to know the expected location of a furcation in both horizontal and vertical directions. Horizontally, most furcations are located midway on the root trunk. The mesial furcation of a maxillary first molar is generally located more toward the lingual surface in a horizontal direction, and therefore instrumentation of the mesial furcation of this tooth is easier from the lingual approach (see Figure 26-19). Vertically, furcations on a maxillary premolar are in the apical third to half (see Figure 26-18). Furcations on a maxillary molar are near the junction of the cervical and middle thirds of the root (see Figure 26-19). Furcations on maxillary second and third molars are more apical; furcations on a mandibular first molar are apical to the cervical one fourth of the root, making this the shortest root trunk in the permanent dentition and the most likely to experience furcation involvement (see Figure 26-20). Furcations on the mandibular second and third molars are more apical than on the first mandibular molar.
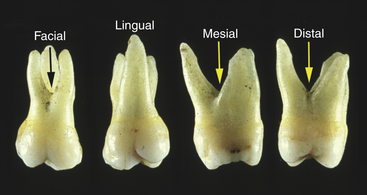
Root Concavities
Root concavities are shallow vertical depressions on the surfaces of roots. They protect the tooth from forces that could rotate it in its alveolus, and provide more root surface area and direction for periodontal fiber attachment. Root concavities complicate root instrumentation and access and make it more difficult to place the cutting edge of the instrument on the root surface. Root concavities most frequently occur on proximal root surfaces (proximal root concavities) (see Figure 26-15). Maxillary first molars have a concavity on the lingual surface of the palatal root (lingual concavity) (see Figure 26-19). Molars may have root concavities on a surface of their root toward the furcation (furcal concavities).
Tooth Alignment
Assessment of the alignment of the teeth within an arch is essential to adapting instruments subgingivally. Tooth size, prominence of its crown, contact areas, and the convergence of root surfaces determine the amount of space and interproximal bone in both health and disease. In health the mandibular anterior teeth have the narrowest amount of space and bone because they are very narrow. In disease, if loss of bone is accompanied by gingival recession, there is more access for instrumentation. When teeth have insufficient space, crowding occurs, making instrument positioning difficult. Teeth with close or altered root proximity may have minimal or no proximal space and long proximal root contact, which may significantly influence oral hygiene, periodontal health, and subgingival instrumentation.
The position of teeth within the alveoli also is a factor in root instrumentation. Axial positioning is the relationship of an imaginary vertical line representing the long axis of a tooth in relationship to a horizontal plane. This concept is diagrammed in Figure 26-21. The functions of this positioning are to bring the maxillary and mandibular teeth into an interarch relationship that facilitates incision and mastication and distributes forces throughout the bones of the skull.
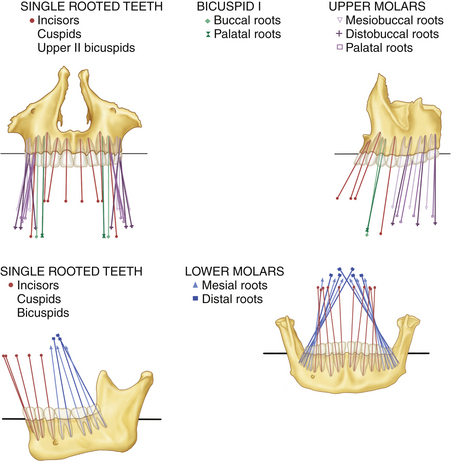
Figure 26-21 Axial positioning of the maxillary and mandibular teeth in an anterior and lateral view. The slant of the roots along their long axis is shown by vertical lines that have been extended to represent the direction of the slant in both faciolingual and mesiodistal directions.
(From Dempster WT, Adams WJ, Duddles RA: Arrangement in the jaws of the roots of the teeth, J Am Dent Assoc 67:779, 1963.)
Following the vertical lines in Figure 26-21, it is clear that in a faciolingual dimension the roots of all the teeth except the mandibular posteriors have a more lingual inclination than do the crowns. Mandibular posterior crowns are more lingually inclined than roots that are more facial in orientation, making plaque biofilm removal in this area especially difficult for clients.
Again following the vertical lines in Figure 26-21, in a mesiodistal dimension the roots of the canines, premolars, and molars have a distal inclination, which is more pronounced posteriorly. Roots of the incisors do not incline distally.
VARIATIONS IN ROOT FORM
Root alterations, anomalies, or abnormalities should be recognized and documented in the client record for instrumentation adaptations and subsequent client education.
Fused Roots, Fusion, and Concrescence
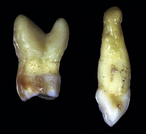
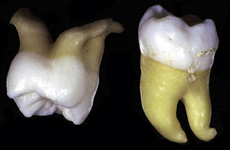
Molar roots may be fused together, especially second and third molar roots, and are a result of limited space during tooth development (Figure 26-22). Fused roots frequently can be observed on radiographs.

Figure 26-22 Fused roots on a mandibular and maxillary molar.
(Courtesy former Department of Dental Hygiene, Marquette University.)
Teeth may be joined together in an anomaly called fusion, in which two tooth buds fuse together during development and form one large tooth with a large crown and a single root that has two pulp canals. This needs to be confirmed by radiographs. Concrescence occurs when two adjacent teeth become joined by cementum after they have been formed.
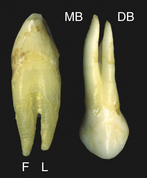
Accessory Roots
Accessory roots are extra roots. Sometimes the mandibular permanent canines are bifurcated into facial and lingual roots in the apical third (Figure 26-23). Maxillary first premolars can have three roots—two buccal and one lingual. Buccal roots are very thin, which makes treatment difficult if periodontal disease is present. Third molars sometimes have extra roots. Accessory roots may be assessed via radiographs and are instrumented only if the attachment level is apical to their occurrence.
Palatogingival Grooves (Palatoradicular Grooves)
A palatogingival groove (Figure 26-24) extends apically from the lingual concavity of the crown of a permanent maxillary incisor, usually the lateral incisor, onto the root, often resulting in an isolated, narrow pocket. This groove provides challenges in instrumentation, is highly plaque retentive, and is susceptible to periodontal disease.

Hypercementosis
Hypercementosis, the excessive formation of cementum in the apical third to half of the tooth after the tooth has erupted (Figure 26-25), may be caused by trauma, chronic inflammation of the pulp, or metabolic disturbances. It is assessed radiographically. If areas of hypercementosis are exposed with apical migration of the junctional epithelium, decisions about the extent of root instrumentation will be more difficult.
Cervical Enamel Projections
Cervical enamel projections (CEPs) are apical extensions of the CEJ toward the furcation of a molar (Figure 26-26). CEPs are classified by degree of extension, as follows:

Figure 26-26 Cervical enamel projection on a mandibular first molar.
(Courtesy former Department of Dental Hygiene, Marquette University.)
Periodontal attachment loss is more likely in CEP areas because periodontal fibers do not form the same type of attachment to enamel as to cementum. Most isolated furcation involvements in otherwise healthy dentitions are found to be related to CEPs. A CEP can be removed surgically to expose dentin and facilitate reattachment of periodontal fibers.
Enamel Pearls
Enamel pearls, most frequently seen on maxillary molars, are “droplets” of enamel in the furcation area (Figure 26-27). They are thought to be due to a genetic error in the developing root sheath as it reaches the area of furcation. As periodontal fibers will not attach to enamel, enamel pearls may encourage periodontal disease. Exploration of an enamel pearl can sometimes be puzzling if it is not visible on radiographs, because it may feel like subgingival calculus.

Dilaceration
Dilaceration is a sharp bend in the root surface caused by the displacement of the root during tooth development (Figure 26-28).
See Procedure 26-1 on root morphology and implications for root instrumentation.
Procedure 26-1 ROOT MORPHOLOGY AND IMPLICATIONS FOR ROOT INSTRUMENTATION
ASSUMPTION
The clinician has mastered instrumentation procedures from Chapter 17, Periodontal and Risk Assessment; Chapter 24, Hand-Activated Instruments; and Chapter 25, Ultrasonic and Sonic Instrumentation.
Select ultrasonic insert and universal and area-specific curets for use on cementum and root surfaces.
STEPS
General Characteristics of Roots and Their Implications for Instrumentation
Root Morphology Instrumentation
Specific Characteristics of Roots and Their Implications for Instrumentation (see Table 26-1)
Variations
ACKNOWLEDGEMENT
Technical assistance in the preparation of the photographs for this edition by the Department of Dental Informatics at the Marquette University School of Dentistry is gratefully acknowledged.
CLIENT EDUCATION TIPS
LEGAL, ETHICAL, AND SAFETY ISSUES
KEY CONCEPTS
Periodontal assessment includes the identification of root anatomy and root surface characteristics before the development of the plan for care. Approximately 60% of maxillary first premolars have two roots (one facial and one lingual), with furcations on the mesial and distal surfaces. Mandibular molars have two roots, one mesial and one distal, with furcations on the facial and lingual surfaces. Maxillary molars have three roots (mesiobuccal, distobuccal, and lingual), with mesial, facial, and distal furcations. Number and shape of the roots determine the selection and adaptation of assessment, scaling, and root planing instruments. Root surfaces converge (taper) apically; there is more root surface area in the cervical third than in the apical or middle thirds. More of the proximal surface of a single-rooted tooth with broader facial than lingual surfaces can be reached from the lingual approach because of the proximal convergence toward the lingual side. Horizontal and vertical location of the furcation determines selection and placement of instruments.CRITICAL THINKING EXERCISES
Materials: Autoclaved extracted permanent teeth with crowns sectioned off or, if available, anatomically accurate plastic specimens of permanent teeth with crowns cut off. (When natural specimens are used in this and all other exercises, personal protective equipment and infection control procedures are required.) Photographs may also be used for this exercise, but specimens are three dimensional. Refer to Table 26-1 for guidance.
Note: It is not possible to distinguish mandibular central from lateral incisor roots, or mandibular first from second premolar roots. For these, the identification of the root only as a mandibular incisor or mandibular premolar is the expectation. Sometimes it is also difficult to distinguish maxillary and mandibular canine roots.
Root Surface and Stroke Coverage Exercise
Materials: One permanent incisor and one permanent maxillary typodont or natural tooth; mechanical pencil; tray cover; and gauze square.
Root Surface Characteristic Exercise
Materials: Autoclaved extracted tooth with subgingival deposit, curets, dissecting microscope, tray cover, gauze square.
Materials: Autoclaved extracted permanent maxillary and mandibular first molars or plastic typodont molars; black nail polish; glitter; black crayon; 11/12 and 13/14 area-specific curets; tray cover; gauze square.
Preparation: Paint the cervical third to half of the root to the distal half of the root surface, sprinkle glitter on the painted area (simulates deposit, altered cementum); color the mesial half of the root with crayon (simulates subgingival plaque).
Refer to the Procedures Manual where rationales are provided for the steps outlined in the procedure presented in this chapter.
Visit the  website at http://evolve.elsevier.com/Darby/Hygiene for competency forms, suggested readings, glossary, and related websites.
website at http://evolve.elsevier.com/Darby/Hygiene for competency forms, suggested readings, glossary, and related websites.