CHAPTER 17 Corrective dental procedures
Introduction
Corrective dental procedures in the form of floating or reduction of sharp enamel points and tall tooth crowns have been performed on equine patients for hundreds of years. These procedures performed on a regular basis have traditionally been part of a horse health care program with very little scientific evidence to support this practice. Corrective floating procedures are often performed to: 1) relieve discomfort associated with oral soft tissue injuries caused by sharp enamel points; 2) reduce dental elongations, which place stress on affected teeth and jaws; 3) improve mastication and digestion of feedstuffs; 4) alleviate stresses on abnormally worn teeth; and 5) prevent discomfort and improve performance in the horse wearing a bit and bridle.1–10 Most dental corrective procedures concentrate on reduction of abnormal dental elongations. The true pathology often involves the tooth opposite or out of occlusion with the elongated dental area. Failure to evaluate and properly address the pathological process may lead to recurrence of the elongations and a temporary or unsatisfactory result for the patient. A careful and complete oral examination is critical in the diagnosis of dental pathology and the planning of dental corrective procedures. A more scientific approach to equine dentistry has changed the way that many cases are managed. The practitioner should strive to do no harm to the horse or its teeth. The utilization of a complete set of good quality hand floats or power equine dental equipment allows dental corrective procedures to be performed with precision in an efficient manner (see Ch. 16).
There are four distinct levels of equine dental care. Historically, the first level of dentistry has been labeled dental prophylaxis or ‘floating teeth.’ It involves an oral examination and routine dental maintenance procedures, such as reduction of sharp enamel points, and reduction of small crown projections (hooks, beaks, small waves, and transverse ridges). The second level of dentistry is often referred to as performance dentistry. This includes dental prophylaxis and additional procedures developed in the hope of improving the horse’s comfort in accommodating the bit or other equipment (tongue-tie, hackamore, nose band, or martingale) and allowing free rostrocaudal mobility of the mandible. Such additional procedures may include rounding off the rostral and buccal edges of the 06s (creating bit seats), the removal of loose deciduous teeth, and the extraction of wolf teeth. Corrective dentistry or dental equilibration describes the third level of equine dental care and involves procedures devised to reduce dental crown elongations (odontoplasty) and treat associated pathologies. Dental overgrowths may involve a portion of a tooth (hooks, abnormal transverse ridges), the entire tooth (step, ramp), several teeth (wave), or the entire arcade (shear mouth). Dental elongations can place abnormal stress on the affected tooth. These stress forces can cause the teeth to shift and ultimately lead to rostral or caudal displacement, linguoversion, or buccoversion. The resulting diastema caused from tooth displacement is a leading cause of periodontal disease. This high level of dental care usually requires a more thorough examination and at times ancillary diagnostics and imaging techniques to properly diagnose the problems and develop a precise plan for correction. Oral and dental surgery, periodontics, orthodontics and endodontics, the fourth level of equine dentistry, will be covered elsewhere in this text.
It is not always possible to assign an equine patient to a level of dental care prior to making clinical contact. A dental history and physical examination along with a complete oral/dental examination usually establish the level of care the horse requires. Occasionally, the veterinarian may be involved in what appears to be a routine prophylaxis when a tall, decayed, loose, or broken tooth is encountered. This may move the horse into a higher level of care. Horses requiring special diagnostic and therapeutic oral procedures may require referral to veterinarians with the equipment and expertise to properly diagnose and treat such problems. Taking a moment to educate trainers and owners about the value of a thorough dental examination, types of pathology, and indicated dental corrective procedures is time well spent. Dental forms or charts should be used to record abnormalities, corrective procedures performed, and any planned treatment. Dental forms also help in itemizing the bill and provide an estimate of professional fees before procedures are performed (see Ch. 12).
Two approaches to performing dental corrective procedures have become standard over the past few years. Both involve examination and dental corrections carried out in a standing, sedated equine patient. In rare cases, general anesthesia may be required to thoroughly examine and treat dental problems. The less involved type of standing restraint has been described as ‘performing dentistry by feel.’ This type of dentistry is performed with the horse’s head at the level of the operator’s waist or chest (Fig. 17.1). This requires minimal sedation and works well for most horses with relatively normal occlusions that need only minimal routine dental corrective procedures. The horse’s head can be periodically elevated, and the oral cavity visually evaluated during the procedure.11–14 The second method commonly employed is ‘visual dentistry.15 Working in the horse’s mouth visually requires the patient to be well restrained and more heavily sedated (Fig. 17.2). The animal’s head must be elevated and supported at a height that allows visualization of the mouth while the veterinarian maintains a comfortable ergonomic body position.16 Visual dentistry allows for a more thorough dental examination and precise correction of dental abnormalities. Both methods have their place in practice, but visual dentistry has many advantages over dentistry by feel, especially in horses with dental pathology or severe wear abnormalities. Working with dental instruments, including power equipment, requires strength, dexterity, and mastery of technique. The visual method allows better access to the mouth and lowers the learning curve on the use of equipment.

Fig. 17.1 Performing dentistry by feel. The horse is restrained with its head and mouth at chest level to the veterinarian. This method allows the practitioner to remain standing with correct posture for dental work.

Fig. 17.2 Performing visual dentistry. The horse is restrained with its head elevated, and the veterinarian is working while seated in front of the horse.
Dental corrective procedures, such as floating teeth, were once considered fairly innocuous. With the development of better quality and more efficient equipment to instrument the mouth and reduce dental crowns, dental correction can be overdone and have severe detrimental effects on the patient. Rasping teeth has been shown to amputate odontoblast processes, leave deep grooves in the surface of the dentin, and/or chip the enamel surface and peripheral cement. Modern motorized dental tools remove greater amounts of dental tissue, thereby increasing the risk of damage to pulp horns from overheating or direct exposure. It has recently been speculated that horses may suffer dental pain after corrective procedures.17 A fine-toothed burr or dental rasp used with light intermittent cutting strokes causes less damage in reduction. An efficient water cooling system and frequently cleaning the burrs may reduce the chance of thermal injury to the dentin and pulp.18,19
This chapter is divided into five sections: 1) dental prophylaxis; 2) performance dentistry; 3) special concerns in treatment of miniature horses and draft breeds; 4) correction of cheek teeth and incisor overgrowths and associated pathology; 5) complications of dental corrective procedures. The dental equipment and instruments needed to carry out corrective procedures have been covered previously in Chapter 16.
Dental prophylaxis
In veterinary medicine the concept of prophylaxis, i.e., the ability to use a practice that prevents the development of subsequent serious disease, is the foundation of any health maintenance program. Dental prophylaxis, the examination of the oral cavity, and the use of corrective procedures to arrest disease processes before clinical signs are seen, have been reaffirmed as important parts of a patient’s health care program. Historically, ‘floating’ was a term that originated in the masonry and/or carpentry professions to describe leveling or smoothing out of plaster. In equine veterinary practice, floating involves the use of files, burrs, or chisels to remove the enamel points from the buccal aspects of the upper and lingual edges of the lower cheek teeth. Reducing and smoothing these sharp elongations make these areas that contact soft tissue less irritating, thus providing more comfortable mastication and bitting for the horse.20–25 Floating may be the first dental procedure performed and can make the mouth more comfortable when using a full-mouth speculum. Or, it may be preceded by cutting, grinding, or extracting teeth to provide a dental arcade that can be properly rasped. Hand floating by feel with minimal sedation will be described in detail. However, many practitioners use power tools in routine floating. Since each type of equipment requires varied techniques, it is recommended that one works closely with practitioners who have experience with the specific tools being used. Manufacturer recommendations on the use of particular power tools should be followed very closely.
Equine dental floating should be approached in a sequential fashion. A full set of floating instruments is needed to reach the various areas of the mouth. The upper buccal aspect of the central four cheek teeth is the easiest point of the arcades to float. The most appropriate tool to reach this area is a straight head float. The practitioner can introduce the float to the horse by allowing the animal to view, sniff, and feel the float’s action on the outside of the cheek before inserting the instrument into the mouth. The initial strokes should be light and short, progressing along the length of the dental arcade. As the horse becomes more receptive to the tool, the stroke can be lengthened and more pressure applied to the head of the float. The position of the float head should be at a 45° angle to the buccal cusps. Hand position, which influences float head position, should be adjusted according to feel and sound. The high-pitched rough sound of sharp enamel points being rasped softens as floating continues. The 45° angulation of the float head should not be rigidly maintained, or two sharp angles could be left on the buccal aspect of the tooth. The float should be rotated slightly along the longitudinal plane to round the buccal tooth edges and reduce prominent singulare. This procedure should be performed on both upper dental arcades before proceeding to the next area.
The upper caudal molars (110, 111, 210, 211) should be floated next using a long-shafted straight float with an upward tilted or obtuse 10–15° head (back molar float; Fig. 17.3). The instrument is placed in the buccal space and eased to the back of the mouth. With short strokes on the pull, the float head is pressed against the buccal aspect of the last two molars. The final area to be floated on the upper arcade involves the second and third upper premolars. The instrument of choice to use on these teeth is a short-shafted upper premolar float with a 20° angled head or a 9-inch offset head float (Fig. 17.4). The float is worked back into the mouth along the buccal aspect of premolars 2 and 3. Horses with 06 hooks, or performance horses that are bitted, require special considerations, and these are addressed later in this chapter.

Fig. 17.3 Proper positioning of the back molar float with a slim 15° upper obtuse head. The carbide blade should always be set to cut on the pull stroke when using this float in the back of the mouth.

Fig. 17.4 A short-shafted float with a 20° downward obtuse head. This area of the dental arcade can be more easily floated without the speculum in place.
A 15–17-inch long straight float with a 3-inch head or a carbide chip table rasp can be used to float the lower arcade (Fig. 17.5). This instrument is introduced along the lingual aspect of the lower molar table with a mouth speculum in place. Horses have a tendency to raise their heads when the lower arcades are floated. A dental halter used as a martingale is helpful in holding the head in proper position (Fig. 17.6). Tongue retraction should never be used as a method of restraint when floating. The hyoid apparatus can be fractured, with serious complications ensuing. A back molar float can then be used to round the caudal edges of the last lower molar. Horses with 06 hooks or performance horses that are bitted require special considerations, and these are addressed later in this chapter.

Fig. 17.5 A straight long-shafted float positioned for removing sharp enamel points from the lower arcades.
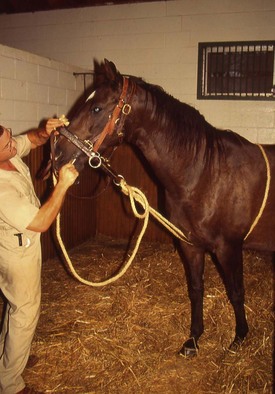
Fig. 17.6 Horse restrained with a metal frame dental halter similar to a martingale, to float the lower arcades by feel.
With a full mouth speculum in place, the entire upper and lower molar arcades should be digitally and visually inspected. Finally, any areas of asymmetry or overlooked sharp points can be addressed. The speculum is removed, and lateral jaw excursion to molar contact (EMC) re-evaluated for balance, symmetry, and incisor contact. Depending on the horse’s age and use, other corrective procedures may need to be considered (see DVD).
Performance horse dentistry
In additional to regular dental prophylaxis, several areas of the dental arcade are of particular interest to veterinarians working with performance horses. Since the horse was first domesticated, reins and bits have been used to send cues from the rider to his mount. Today’s performance horses are involved in a wide variety of disciplines. In most endeavors, the equine athlete wears a bridle and bit for control. Oral and dental problems often lead to bad habits and vices, such as resisting the bridle, poll sensitivity, and head shaking. Over 100 years ago, Merillat, in his thesis on horse dentition, summarized the importance of dental care in the performance horse:
In drivers, runners, and saddle horses enamel points are the greatest sources of annoyance. The expert reinsmen will properly recognize their presence by the horse’s behavior in harness. Lugging, side reining, ptyalism, and tenderness about the seat of the bit are manifestations of pain from the bridle and are symptoms of these points. The aim in dressing the teeth of a horse should be to simply blunt the enamel points along the course of the arcades and to round up the first superior and inferior molars as smooth as an ivory ball.26
A recent Swedish study has shown an increased incidence of oral ulcerations in horses ridden with bit and bridle than in horses not ridden.2 Floating the teeth to remove sharp points has been shown in a clinical study to have a positive effect on the trainer’s perception of the horse’s response to the bit.27 The effect is enhanced by rounding the premolars in what has been referred to as ‘bit seating.’ A randomized, controlled, blinded trial demonstrated that dental floating increased the rostrocaudal mobility of the mandible when flexing and extending the head, which may be beneficial to horses working with a more vertical head carriage.9 Studies on the position of the bit in the horse’s mouth and surgical correction of bit-induced bar injuries have shed new light on bitting problems.28,29 Performance horse dentistry entails: 1) normal dental prophylaxis; 2) slightly rounding the 06s (creating bit seats); 3) care or removal of wolf teeth; 4) deciduous teeth management; and 5) evaluating canine teeth. Types of bits and contact points on the horse are reviewed in Chapter 3.
When evaluating performance horses, the veterinarian must keep in mind that subtle points and hooks or a difficult-to-detect loose or painful tooth may cause great personality and performance changes in the elite equine athlete.30 An important consideration when working on the performance horse’s mouth is to remove any sharp or protruding edges from teeth that could make contact with the tender soft tissues of the mouth. A good test for detection of sharp points is to position the fingers just in front of the masseter muscles on both sides of the cheeks at the level of the upper molar arcade. Place firm pressure on the cheeks, pressing them into the teeth and moving the fingers forward. Press the commissures of the lips back against the rostral edges of premolar 2. If the horse flinches or tosses its head, the animal is feeling pain from sharp enamel points.31
A regular dental floating usually resolves most problems. The rostral edges of the upper and lower second premolars (106, 206, 306, 406) should be carefully rounded to provide a smooth surface against which the cheeks can rest when bit pressure is placed on them. This procedure, termed ‘creating bit seats’ is performed in an attempt to make the performance horse as comfortable as possible for a reasonable period of time as the bit pulls or pushes soft tissue against the premolar teeth. These teeth should be shaped like the end of an index finger. There are differences of opinion about the need for creating bit seats, the degree to which the teeth should be beveled, and the smoothness required.21,25,32,33
To shape the upper teeth (106, 206), several cuts are made. The first is the outside (buccal) cut. The instrument of choice for this cut is a 9-inch float with an offset head. When floating begins, the handle is held on the ipsilateral side of the tooth and is subsequently worked across to the opposite or contralateral side of the face between the open incisors (Fig. 17.7). This rolls the head of the float from the buccal aspect of the second premolar to its rostral buccal aspect and then rostral aspect. This cut is followed by an inside cut to the same tooth with the same float. The float is positioned at a 30–45° angle to the lingual surface. Strokes should be made on the lingual edge of the tooth in order to round the rostral aspect. The objectives of the inside and outside cuts are to produce a narrow edge shaped much like a boat hull which can be blunted with a crosscut. The float is introduced from the contralateral side, placed at a 45° angle, to the point, and short vibrating strokes are made. Two fingers may be placed on the outside of the cheeks to serve as guides (similar to how a person holds a pool cue). To observe float placement, the commissure of the lips should be retracted. The last cut made is the fan cut. The float head is placed at a 30–45° angle to the rostral point of premolar 2, and using a fanning action, short sequential strokes are made. Strokes are initially made on the buccal aspect of premolar 2. A half-circle is rolled or cut starting buccally and is continued around the rostral and lingual surfaces of the tooth. This blends the three prior cuts. The last cut is easier to perform using a full mouth speculum. The float is inserted into the mouth over the speculum incisor plate.

Fig. 17.7 A short-shaft float with offset head is used to create the ‘bit seat’. This float can be easily used over the incisor plates of a McPherson-type full mouth speculum.
The final step in performance horse floating requires floating the lower first cheek teeth and shaping the lower bit seats. These lower teeth, like the upper second premolars, need to be slightly rounded and shaped symmetrically, relative to one another. The bit seats are formed with the same cuts used on the upper arcade. Ideally, the bit should lie on the tongue and not against these teeth. The bit seats and the rest of the arcade should be evaluated for symmetry and balance. Sharp buccal points on premolars 3 and 4 should be reduced as they can cause nose band pain. Severe tooth damage can occur from over-reduction of the crown and lead to pulp horn damage. Finally, lateral jaw excursion should be evaluated. If indicated, the incisor teeth should be addressed appropriately, as is discussed later in this chapter.
‘Wolf tooth’ is the common term used to describe the first premolar.34 The number, position, size, and shape of these teeth are quite variable. The appearance of the exposed crown is not necessarily a reflection of the size or shape of the root (Fig. 17.8). Forty to ninety per cent of domestic horses erupt at least one upper wolf tooth. Lower first premolars are uncommon.35 Wolf teeth usually erupt at 6–18 months of age but this too may be quite variable. In some 2–3-year-old horses, wolf teeth are shed concurrently with the second deciduous premolar caps. The larger erupting permanent second premolar tooth often causes root resorption of a wolf tooth that is positioned close to the deciduous second premolar. This probably accounts for the high percentage (80–90%) of horses under 2 years old with wolf teeth and the lower percentage (15–25%) found in adults, even in groups of horses having had no previous dental work. Wolf teeth are usually positioned just rostral to the upper PM2s, but they can be positioned on the buccal side of the first cheek teeth or up to 1 cm rostrally to these teeth (Fig. 17.9). Double wolf teeth have been seen, as well as teeth displaced into the interdental space. Unerupted wolf teeth, referred to as ‘blind wolf teeth,’ can be detected as firm nodules under the buccal mucosa rostral to the first cheek tooth. These are often painful and at times are covered with ulcerated mucosa.


Fig. 17.9 Thirty-month-old horse with wolf teeth positioned close to the 106 cap and 1 cm rostral to the 206 cap.
The role of wolf teeth in causing oral discomfort has been widely debated.36–38 Tradition and client/trainer pressure are the greatest indications for extraction of these vestigial teeth.38 Certainly, most wolf teeth cause no problem to the horse but cause concern to the trainer for several reasons. It is difficult, if not impossible, to properly round the rostral edge of PM2 to accommodate bitting with a wolf tooth in place. Displaced or sharp crowned wolf teeth can cause buccal pain and ulceration when bitting pressure is placed on the cheeks. Some wolf teeth do become loose or diseased and have been suspected to be a cause of head shaking or bitting problems.
Some veterinarians advocate floating or grinding the wolf tooth crown, incorporating it into the bit seat. This has the potential to loosen the tooth or expose the pulp chamber. Both conditions could be detrimental in the long term and predispose the tooth to pulpitis and lead to eventual extraction. It is, however, customary practice to extract wolf teeth in young performance horses. In most cases, with proper restraint and equipment, these single-rooted teeth can easily be extracted from the socket in total. Horses should be sedated and given analgesia or a local anesthetic before these teeth are removed (Fig. 17.10).37 Blind or unerupted wolf teeth can be evaluated radiographically if one is uncertain about their presence or position.

Fig. 17.10 Local anesthetic (1–2 ml) administered around the wolf tooth with a small gauge needle on a short extension set attached to a lure lock syringe.
Rarely, a wolf tooth is encountered that is quite large and looks as if it has become molarized like the other cheek teeth.39 These should be evaluated radiographically and, if unopposed, they need to be shortened or extracted. These may prove to be supernumerary teeth, in some cases.
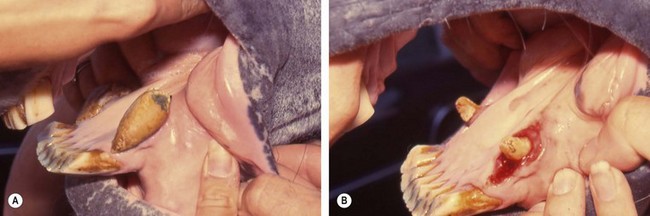
Lower first premolars (305–405) are occasionally detected in the mandibles rostral to the first cheek teeth. These are usually quite small and may only be a small tooth sliver detected soon after the deciduous teeth have been shed. However, they can be large with sharp crowns (Fig. 17.11). Lower first premolars have caused problems in bitted horses. Their presence should always be noted during an oral examination on a performance horse. They can be difficult to see on the oral examination because they may be partially covered by a loose fold of buccal mucosa at the lip commissures. Digital palpation just rostral to the first lower cheek tooth is the most accurate way to detect these short-crowned teeth. Unerupted lower wolf teeth are rare and may only be detected radiographically. These teeth can be elevated using the same techniques as for the uppers. Extraction techniques for removal of wolf teeth are covered in Chapter 20.

Fig. 17.11 (A) Lower wolf tooth (405) lingual to the crown on 406. (B) Extracted 405 with a long, slender root.
In the 2.5- to 5-year-old horse, the 24 deciduous incisors and premolars are replaced by permanent teeth. Horses have vertically successional teeth. Therefore, each deciduous tooth and its underlying permanent tooth reside in the same alveolar crypt. The development and eruption of the permanent tooth lead to resorption of the roots of the deciduous tooth. This, combined with attrition of the clinical crown, results in shedding or exfoliation of the deciduous tooth (also known as a ‘cap’). Conditions such as permanent tooth displacement, diastemata formation, and dental impactions are often attributed to disorders of tooth eruption. The equine teeth in each arcade are in tight apposition and act as a single grinding unit. It is easy to see how maleruption or displacement of a tooth can result in loss of integrity of an arcade. This would predispose to both abnormal crown wear and periodontal desease.40 Some practitioners have expressed concern about the role of early or delayed eruption of permanent teeth playing a role in the formation of certain abnormal dental wear patterns noted later in life (i.e., dominant maxillary 10s, lower 08–09 wave, incisor smile, or frown, etc.).
Incisor caps normally shed from the most mesial teeth (01s) at about 2.5 years (between 30 and 34 months), from the 02s at about 3.5 years (40–44 months), and from the corners (03s) at about 4.5 years (54–60 months of age). Miniature horses and ponies may not erupt permanent incisors for 6–18 months later than Thoroughbred horses. The permanent incisors often erupt slightly palatal to the deciduous tooth. Therefore, the incisor cap often retains the more labial portion of the root and is often displaced slightly rostral in the socket as it is shed.
Retained deciduous incisor teeth may be a source of discomfort in the 2–5-year-old horse. Head tossing while eating or rubbing the incisors on the stable wall and/or feed box can result from retained incisor caps or root slivers. Incisor caps are easily removed with small extraction forceps. Retained root slivers may need to be removed with a root elevator while the horse is sedated. Retained and displaced deciduous incisors can appear as a double tooth or a double arcade of teeth, which should be differentiated from supernumerary permanent teeth. Uneven eruption of permanent incisors has been reported as a predisposing factor in incisor malalignment and uneven wear. Premature extraction, trauma, or avulsion of a deciduous incisor tooth has resulted in maleruption, malformation, or failure of eruption.41
The sequence of eruption of permanent equine cheek teeth has been widely reported in the literature with emergence times of 2.5 years (813 days) for PM2, 3 years (1095 days) for PM3, and 4 years (1460 days) for PM4.34 Recent work has shed new light on premolar eruption times at least in the Thoroughbred horse. In this study, male animals had a younger age of emergence of 06s by 34 days compared to females. Teeth in the lower jaw had a younger age of emergence by 14 days compared to the same teeth in the upper jaw. The study showed the 06s emerging about 1055 days of age, 07s at about 1130 days of age and the 08s at about 1350 days of age.42
Worn crowns of the deciduous premolar teeth (caps) become loose and subsequently either displaced or shed into the mouth. These wafer-thin portions of deciduous tooth crown can have a variable number of root slivers (Fig. 17.12). The caps can appear much like a table with four legs lying over the top of the permanent tooth. Gingivitis and periodontal disease can result if these root slivers are broken off and remain in the subgingival space after the cap is shed.
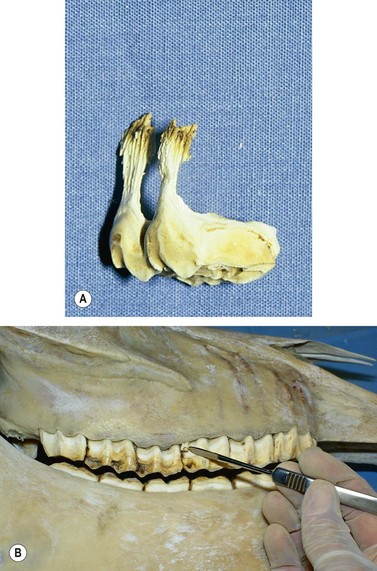
Fig. 17.12 (A) Root slivers of this premolar cap (508) can become lodged in the gum if they break off when the tooth is shed. (B) Broken (508) root sliver embedded buccal to the permanent tooth.
The eruption pattern of permanent molarized dentition follows a sequence that predisposes to entrapment (impaction) of deciduous PM3 and PM4. Delayed shedding of deciduous premolars can predispose to gingivitis and periodontal disease. Retained, split, or displaced deciduous premolars can be distracting to the training process of a young horse. Additionally, retained deciduous premolars may cause dismastication, anorexia, and predispose to malocclusion and abnormal crown wear of the permanent teeth.40,43 In some cases they have been recognized as a factor in dorsal displacement of the soft palate.44 If one cap has shed, the cap in the opposite side of the jaw should be evaluated and, if loose or close to exfoliation, removed. Impacted caps, manifested as bony enlargements or eruption bumps on the ventral mandibular ramus or maxilla rostral to the facial crest, can result from lingual displacement or delay eruption of permanent teeth. These facial bony enlargements are only cosmetic problems in most cases. However, they can become pathological if eruption is severely inhibited or blood-borne bacteria inhabit the inflamed or ischemic dental pulp. This can lead to anachoretic pulpitis and facial swelling with a draining tract on the mandible or maxilla.45 Caps should be evaluated by palpation and visual inspection, using a dental mirror or endoscope (Fig. 17.13). In some instances, open mouth radiographs may be required to evaluate the retained cap and the status of the underlying permanent tooth. Occasionally, caps may extend above the occlusal surface of the adjacent teeth but cannot be extracted without using excessive force. These caps should be floated level with adjacent occlusal surfaces and evaluated 6–8 weeks later.

Fig. 17.13 An intraoral mirror is used to evaluate a 506 cap. The corresponding permanent tooth (106) is seen just erupting through the gum beneath the cap.
Various forceps, elevators, and dental picks are available to aid in the diagnosis and treatment of retained deciduous teeth. These include Reynolds cap extractor forceps (upper and lower), molar forceps (11 inch), No. 34 gouge dental elevator, and No. 69 dental extraction forceps. To remove the cap of deciduous PM2 and PM3, small extraction forceps work well. On the PM4 cap, open head molar extraction forceps possess a better angle with which to clamp the cap. The forceps are clamped firmly on the base of the cap and pulled lingually across the arcade and the tooth extracted. Care should be taken not to place the forceps below the level of the gums as the palatine vessels along the upper arcade could be disrupted upon clamping, resulting in severe hemorrhage. Rolling the cap toward the lingual surface reduces breakage of the buccal roots, which can leave slivers of the cap behind. With this method, only the lingual cap roots may break. The residual lingual slivers can be easily removed with a root elevator. If slivers do exist on either the lingual or buccal sides of the premolars, they can be worked out of the gum with a dental pick or plucked out with a set of closed head rongeurs. When caps are removed, the underlying permanent tooth will erupt and should be in wear in 3–4 months. Sharp enamel edges will be present on these teeth in 3–6 months, and the horse should be rechecked and floated at this time.
Canine teeth (104, 204, 304, 404) are usually present in most male horses over 5 years of age. These teeth normally cause few if any problems. In a study of 400 horses, five presented with bitting or head carriage problems related to canine teeth. In four cases with displaced, supernumerary, or fractured canines, the teeth were extracted with resolution of clinical signs.46 It is suggested that displaced canines that are causing soft tissue irritation or bit interference may be successfully treated by simply rounding to the top of the clinical crown. Care must be taken not to damage the pulp which can lead to pulpitis and eventual death of the tooth. Some mares have small rudimentary canines that generally do not cause problems unless they become loose or accumulate tartar. Long or sharp canines in a stallion or gelding have been blamed with bit interference, the mechanism of which has not been determined.
In the past, tall or sharp canine teeth have been cut and blunted before performing corrective dental procedures, to reduce the likelihood of injuring one’s hands and/or wrist. This practice is not in the best interest of the horse and should be discouraged.
Erupting canine teeth in 4–6-year-old horses can cause subgingival pain and bit irritation that has been manifested by head shaking or other bad habits. This problem was reported by Percivall over 100 years ago:
I was requested to give my opinion concerning a horse, then in his fifth year, who had fed so sparingly for the last fortnight, and so rapidly declined in condition in consequence, that his owner, a veterinary surgeon, was under no light apprehensions about his life. He had himself examined his mouth without having discovered any defect or disease, though another veterinary surgeon was of the opinion that the difficulty or inability manifested in mastication, and the consequent cudding, arose from the preternatural bluntness of the surfaces of the molar teeth, which were, in consequence, filed but without beneficial result. It was after this that I saw the horse, and I confess that I was, at my first examination, quite as much at a loss to offer any satisfactory interpretation as others had been. While meditating, however, after my inspection, on the apparently extraordinary nature of the case, it struck me that I had not seen the tusks. I went back into the stable and discovered two little tumors, red and hard, in the situation of the inferior tusks, which, when pressed, gave the animal insufferable pain. I instantly took out my pocket knife and made crucial incisions through them both, down to the coming teeth, from which moment the horse recovered his appetite and, by degree, his wonted condition.47
In the mature horse, calculus can build up on canine teeth that have lost the crown enamel. These teeth should be scaled and brushed to prevent or reduce the degree of gingivitis and periodontal disease (Fig. 17.14).
Special concerns in the treatment of miniature horses, ponies, and draft breeds
Several types of horses deserve special consideration when performing dental procedures. In recent years, small ponies and miniature horses have become popular companion animals and warrant particular attention. Intensive inbreeding to reduce body size and refine the head from a large draft type to a light horse type has led to an increased incidence of dental problems. In genetic studies of other animal species, it has been shown that teeth diminish in size more slowly than the jaws.39 The teeth of a 250 lb miniature horse are about two-thirds the size of a 1000 lb Quarterhorse.48 Disproportionately large tooth size in relationship to head size seen in miniature horses can encourage tooth overcrowding and lead to dental maleruptions and malocclusions. This predisposes the small horse to a higher incidence of dental disease and abnormalities of wear.40,43 For this reason, early and frequent oral examinations and interceptive dental corrective procedures are more important in smaller horses.
The miniature’s small stature and reduced head size makes the oral cavity more difficult to evaluate. Many of these pet horses are poorly trained and require sedation to be restrained. Careful calculations of body weight and sedative medication dosing at a lower mg/kg level are important. Restraint at a level that allows the examiner/operator to be comfortable requires either elevating the horse or lowering the veterinarian. These horses can be sedated and restrained at ground level, but this requires the practitioner to work on his knees. Knee pads offer protection, and a solid bar or skirt in front of the horse provides a barrier between the operator and the horse. Elevated stocks or loading dock can bring the animal’s head to a more comfortable working height.
Special dental instruments may be required to work in the small oral cavity of miniatures/ponies. Interceptive orthodontics is more often employed in miniature horses because they experience a higher incidence of dental overcrowding. It has been found that early removal of deciduous teeth can result in destruction of permanent tooth buds. This information can be used to the horse’s advantage if there is severe overcrowding and no room for a full set of permanent teeth in the dental arcade.48 Malformed permanent teeth and severe early dental decay are other sequelae to premature deciduous tooth removal, most commonly seen affecting the upper premolars.
Draft and large warmblood breeds present special dental considerations due to their weight and size. Large horses weighing over 750 kg usually require less medication for sedation on a mg/kg basis, than medium-sized animals. A head support stand or a metal-framed dental halter suspended from a sturdy beam is necessary to support the additional weight of the heavy horse’s head. A sedated draft horse can become unsteady or stumble, which can be extremely dangerous for the veterinarian or his assistant(s). Sturdy stocks are recommended as a safe area for restraint. The operator may need a platform on which to stand in order to maintain an ergonomic working posture. Large horses may overpower a regular McPherson type speculum, and the larger MacAllen or Conrad speculums give the operator more security and safety when placing hands and arms into the caudal recesses of the mouth. The Series 2000 speculum is heavy and can be purchased with a draft horse poll strap. If hand floating, long shaft instruments are required to reach the caudal aspect of the cheek teeth. Special 24-inch-long shafts with bonded or interchangeable blades are available from at least one instrument manufacturer. Power equipment is especially convenient for working in large, deep mouths. The disk burr floats with long shafts have been found to be extremely versatile and efficient for working on draft horses (Fig. 17.15).
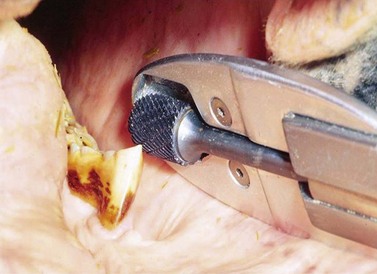
Fig. 17.15 Motorized dental burrs with long shafts. This instrument works well for reaching the caudal recesses of the mouth in large breeds.
In large breeds, deciduous tooth shedding may be delayed up to several months compared to the light breeds. This further postpones cap removal. The incidence of certain congenital craniofacial deformities (wry nose and parrot mouth) has been over-represented in draft breed horses.49 There appears to be a disproportionately large number of draft horses with molar arcade malocclusions leading to hook formation on the upper 06s and lower 11s. Clydesdale horses have a distinct ‘mustache’ appearance of the upper lip and many have large, even molarized, wolf teeth (105, 205). These large wolf teeth often require removal for correction of bitting problems. Preoperative radiographs and infiltration of local anesthetic agents are helpful in planning and successfully carrying out extractions.
Correction of cheek teeth and incisor overgrowths
The process of reducing dental protuberances to adjust the dental arcades has been practiced for centuries. Percussion type instruments described as molar cutters or chisels have been used for at least 200 years. Abnormal wear patterns develop secondary to poor dental occlusion or altered masticatory patterns. It is beneficial to explore the cause of the wear abnormality before corrective action is instituted. It should be determined whether the wear abnormality rendering the table surface uneven is a result of an overgrowth of a tooth crown or excessive attrition or lack of tooth crown. The classic types of cheek teeth abnormalities of wear are described as step mouth (tall teeth), hooks, wave mouth, exaggerated transverse ridges, and shear mouth. Common abnormalities of incisor wear include elongated teeth secondary to overjet, diagonal bite, smile or frown bite, and isolated tall teeth.13,21
Balancing a horse’s mouth is more than simply reducing the crown on tall teeth. Dental arcade balancing or equilibration allows the jaw to move symmetrically through the full range of mastication.41 The molar arcades, oral soft tissues, muscles of mastication, and temporomandibular articulation should function as a unit. Factors such as head conformation, facial asymmetry, previous trauma, dental attrition, and craniofacial deformity (congenital or developmental) determine how close to ideal dental balancing can be achieved. Keep in mind, changing the crown shape of a tooth changes the way the tooth functions in the arcade. With even a small alteration of the dental table, all associated structures of mastication (i.e., teeth, bone, muscles, tongue, and palate) must adjust. Indiscriminate use of instruments in the mouth by individuals untrained in the principles of dental anatomy, physiology, and pathophysiology can cause harm to the dental apparatus. Corrective procedures dealing with the occlusal surfaces of teeth should be conservative until one has a thorough working knowledge of not only anatomy and mastication but tools specifically developed for correction. The principles in treating all dental elongations are the same for any tooth. Reduce the tall tooth to take the damaged or worn surface of the opposite arcade out of occlusion and allow for less restricted rostrocaudal and lateral jaw motion.9 Each tooth in the dental arcade taken out of occlusion by reducing the exposed crown height places excessive masticatory forces on the teeth that remain in occlusion.
Hypsodont teeth out of occlusion with teeth in the opposite dental arcade become tall or protuberant from lack of crown wear or attrition. Congenital or developmental conditions resulting in unopposed teeth include supernumerary teeth or the absence of a tooth or several teeth in a molar or incisor arcade. Acquired conditions with this same result include teeth that have been surgically removed from one arcade or severe crown damage or fracture that has occurred; the unopposed tooth/teeth become elongated due to lack of attrition.50,51
A single unopposed tooth becomes longer over time and can cause pronounced negative effects on mastication. This condition is often referred to as ‘step mouth.’ Long crowns can reach the soft tissues of the opposite jaw and lead to mucosal ulceration, osteomyelitis, or sinus empyema. It is important to detect unopposed teeth early and keep the table surfaces even. This is easy to do during regular dental check-ups. If the teeth are not attended to on a regular basis, great difficulty may be encountered in attempting to reduce extremely tall teeth. Many power dental instruments available today are quite efficient in reducing tall teeth crowns (Fig. 17.16). These instruments should be used with caution so as not to overheat the tooth or abrade the soft tissues of the mouth. Some tall teeth, especially those in the caudal recesses of the oral cavity, may be difficult to reach with some power tools. Molar cutters and obstetrical wire may be useful in correcting some caudal elongations, but extreme care must be exercised not to fracture the crown or expose a pulp horn.

Fig. 17.16 Guarded carbide dental burr used to reduce a dental elongation on the rostral aspect of 306.
Equipment selection and placement are critical when using molar cutters to reduce tall teeth. Cutters should be sized to fit the tooth to be reduced, with blades set parallel to each other when pressure is placed on the buccal and lingual edges of the crown. The cutter blades should be placed parallel to the normal occlusal surface of the dental arcade. The tooth should be reduced with quick pressure taking care not to twist the cutter. The objective is to cleanly remove the tall tooth crown without damaging the remaining tooth. Problems seen after molars have been cut include fissure fractures down the crown and associated periodontal pockets, tooth extractions, and pulp exposure. Molar cutters have either simple or compound action. A simple cutter with B- or C-head works well for most mandibular cheek teeth. A compound D-head cutter is more effective in fracturing maxillary cheek teeth. The upper molars are wide, and the upper incisor teeth and speculum plates limit access to a long, straight-handled cutter. An open head cutter with an offset 20° angle works well to reach some maxillary cheek teeth. After cutting, the affected tooth should be palpated and probed to ensure the intact section has not been loosened or fractured. The table surface should be smoothed and leveled with a rasp. If pulp horns have been exposed, a vital pulpotomy and crown sealing are required.
Dental hooks, if present, are located on the rostral or caudal aspects of the molar arcade. They are typically the result of a malocclusion of the upper and lower jaws and can be associated with congenital or developmental disorders. Rostral or caudal displacement of the maxillary arcade or a disparity in length of cheek tooth rows results in a hook. Hooks grow and develop at a variable rate but do so in proportion to the eruption rate of the involved tooth. Most teeth that develop hooks are in partial occlusion, and supereruption is seldom a factor in the rate of hook formation. The length and table surface of premolar and molar hooks increase over time. Hooks alter mastication and place abnormal forces on the teeth and jaws.
Close and regular attention to malocclusions and abnormal wear patterns, with timely correction, keeps elongations from forming. Not all horses have routine dental care, and some develop large hooks over time. The position, size, and extent of the hook should be assessed, as should its mechanical effect on periodontal structures of the affected tooth and opposing teeth. Additionally, the pattern of mastication should be taken into account. Some hooks are bilateral and symmetric to all four molar quadrants. Large hooks can have a detrimental effect on the alignment of the incisor tables from abnormal forces placed on the jaws. Small hooks that consist mostly of enamel can be easily reduced with a carbide float. Large hooks that consume a greater portion of the table surface contain a high percentage of dentin and are much more difficult to rasp. Hooks can be narrow but quite long, as is the case in horses with slight malocclusions. Some hooks comprise almost the entire tooth. This type of hook is more common in horses with missing or extra teeth in a dental row. The hook should not be reduced below the level of the normal molar table surface.
Percussion instruments, both cutters and chippers, have been used successfully to reduce hooks. These instruments should be used with great caution and precision as teeth have been broken, loosened, and/or repelled as a result. The most efficient and safest way to remove hooks is with the use of motorized dental grinders. These instruments use high-speed rotary burrs made of tungsten carbide or diamond grit to grind down the tall crown surface of the tooth.32,33,52
Front hooks in the upper or lower arcade are usually reduced without difficulty. The cheeks and lips should be protected from the burr and visualization is aided by a good head light. Air or water should be used to reduce the amount of heat and dental dust generated when burring. Rear hooks are usually associated with a ramp or wave in the back of the mouth. It is helpful to reduce other elongations rostral to the hook before correction is attempted. The majority of rear hooks can be reduced with a solid carbide blade mounted on a long-handled, straight float. The blade should be set to cut on the pull stroke. The float is pushed to the back of the mouth until it rests on the top of the hook. A pull stroke is used to rasp the crown of the tooth. Small thin caudal hooks can be removed with an Equi-Chip. Several motorized instruments with 18–24 inch long guarded heads have been successfully used to remove back hooks. Once the hooks are reduced, forces placed on the jaws and the pattern of mastication change.
Incisor occlusion and lateral jaw excursion (EMC) should be evaluated before and after corrective procedures. A gradual upward sloping at the end of the arcades is referred to as a ramp. Many horses have the caudal lower molars erupt in the curve of the jaw. This is a normal anatomic feature in some horses and these ramps should be carefully evaluated before any crown reduction is undertaken. Special precautions should be taken if molar cutters are used to reduce rear hooks. The caudal pulp horns are easily opened when caudal hooks are reduced. This author has seen several cases of lower M3 apical abscesses that were attributed to crown reductions that damage the pulp horns.
‘Wave mouth’ is the term used to describe an undulating pattern usually involving the central portion of the dental tables. This condition is seen in horses of any age. Waves usually involve elongated lower 08s and 09s with correspondingly worn, cupped-out, or decayed upper 08s, 09s, or 10s. Waves can also form as a result of missing, misplaced, deviate, or rotated teeth in the opposing dental arcade.50 It is important to assess the cause of a wave in order to develop a plan for management. Long teeth are seldom an isolated event in the mouth but they affect the pattern of mastication and wear of all other teeth. It is important to note how many teeth are involved in the protuberant area. Rarely is only a single tooth overgrown. The usual rate of dental eruption can be increased if the involved tooth is completely out of occlusion with the opposing teeth. Completely unopposed teeth have been seen to erupt at a rate of 0.5–2 cm a year, two to four times the normal rate of eruption. Unopposed teeth do not have the normal occlusal surface stimulation to form secondary dentin, so the sensitive pulp is often closer to the occlusal surface. The most common wave seen is the slowly progressing condition of aged horses. Infundibular enamel loss or central crown attrition reduces the upper cheek teeth, and the wave may become quite tall as the upper cheek teeth wear down to the root and eventually become smooth (see Ch. 18).
Slight wave formations of the dental table can be corrected with a float or rasp. The horse’s mouth must be held open with either a speculum or wedge to gain access to the table surface of the arcade. The use of tungsten carbide blades makes small wave reduction easy, while power floats and/or grinders are often necessary to reduce extremely tall waves. When reducing a wave it is important not to take down the entire molar table but only the portion involved in the elongation. Keep in mind that by reducing the crown height of the involved teeth, this portion of the dental arcade is being taken out of occlusion. Thus, the masticatory forces are increased on the adjacent teeth. Dental waves are easy to manage if the patient is seen on a regular basis and the crown height is maintained at a normal level.
Abnormal transverse ridges are actually tall wedges of enamel and surrounding hard tissues running buccolingually across the occlusal surface of the tooth. These ridges are usually opposite a small diastema or narrow areas of excessive crown wear or fracture and should be reduced to aid in therapy of the defect that occurs in the opposing arcade. A table float or most any power tool can be used to reduce the elevated portion of the ridge. These should not be confused with regular transverse ridges seen in young horses (3–8 years of age).53 Regular transverse ridges serve a purpose by increasing the surface area of the teeth and are a normal feature in young horses. Normal ridges are not a continuation of the sharp enamel points that form on the buccal cingula of the upper cheek teeth. These ridges can be slightly contoured but no attempt should be made to reduce or flatten the table surface as this can damage the tooth and reduce its longevity. Excessive reduction of the table surface has been known to bring the molar arcades completely out of occlusion. Overzealous reduction of transverse ridges contributes to the unfortunate practice of excessive and repeated incisor reductions.
’Shear mouth’ occurs when the occlusal table surfaces of the molar arcades are worn at an extremely steep angle (greater than 45°). When dental occlusion is symmetric through a full range of jaw motion, the molar tables should wear at an even 10–30° slope. When masticatory excursion is limited on one or both sides, the teeth wear at an abnormally steep angle. Horses with loose or painful teeth, jaw malalignment, severe periodontal disease, neurological paralysis of the masticatory muscles, or temporomandibular joint problems that limit jaw motion in one direction, develop shear mouth. Quite often, horses with shear mouth will also exhibit masseter and temporalis muscle atrophy on one or both sides.
Before correcting a shear mouth, the equine practitioner should attempt to identify and correct the underlying cause. Any attempt at correction of the molar table angle abnormality should be addressed only after certain factors are considered:
1. The condition has been present for an extended period of time and the muscles, ligaments, and joints have remodeled to accommodate changed chewing patterns.
2. Steep table angles may be accompanied by a long outer buccal edge of the upper arcade (up to 4 cm) and a very short palatal edge that may progress up into the gum line. A corresponding long, sharp edge usually forms on the lower arcade.
3. The tall, scissor-like conformation of the dental arcades may prevent opening the mouth wide enough to allow visualization or instrumentation in the caudal portion of the mouth.
Correction of shear mouth should be attempted in stages, working on the horse’s mouth every 1–3 months for three–six visits. The scissor blade wear pattern on the cheek teeth prevents the operator from establishing a normal table angle even if the tall portion of the crown is reduced to a more normal height. Working from the front of the mouth caudally, the molar tables can be contoured. Over time, the muscles and joints adjust with mastication and many affected horses enjoy more normal occlusion and comfortable masticatory function. This condition is irreversible in some horses, and associated dental pathology may be severe. Many of these horses must be managed through dietary adjustments.
Abnormalities of incisors have been blamed for causing difficult mastication and decreased performance. The incisors are easy to observe and can be evaluated with less difficulty than the cheek teeth. The oral examination, prior to any corrective procedures, should include evaluation of lateral jaw excursion to molar contact (EMC). Incisor abnormalities have been separated into five classes:54–56
1. Excessively long incisor arcades from lack of occlusal contact and/or wear
2. Smile bite, or dorsal curvature of the incisor arcade
3. Frown bite, or ventral curvature of the incisor arcade
Most abnormalities can be corrected or at least greatly improved with relatively simple procedures and basic equipment. When realigning the occlusal surfaces of the incisor arcade, it is important to keep in mind the relationship between the incisor and molar arcades and the temporomandibular joints. Before the incisor tables can be properly balanced, the molar tables should be floated and wear abnormalities corrected. Horses are usually more sensitive in the incisor tooth area. Since incisor tooth corrective procedures are often the last to be performed, the horse may require sedation or resedation to complete the task of incisor reduction. For minor incisor work, a twitch may be used to restrain the horse for a short period of time.
Horses with long incisor teeth have a malocclusion of the upper and lower jaws. The congenital defects termed parrot mouth, monkey mouth, and wry nose are the most common reason for these teeth rows to be out of occlusion. Some horses may develop a slight incisor overjet or underjet over time due to abnormal forces placed on the jaws from enlarging rostral 06 and caudal 11 hooks. These elongations, if large, can force the lower jaw in a rostral or caudal direction, which leads to lack of wear on the portion of the incisor tables that is out of occlusion (Fig. 17.17). The technique to correct overlying long incisors involves reducing the exposed crown height of the long teeth. It has been shown that no more than 3 mm should be removed at one time to prevent pulp exposure and avoid drastic changes in the EMC. A simple, logical method for determining how much incisor should be removed has been proposed. Based on this work using trigonometry and measuring lateral jaw excursion and incisor elevation, a fairly accurate estimate of incisor reduction can be determined.56,57 Another method often used is estimating the distance in the interocclusal space. This has been defined as the distance between the occlusal surfaces of the upper and lower cheek teeth arcades. To estimate the interocclusal space, the sedated horse’s head is elevated and the cheek retracted. Using a penlight or other transillumination device, the distance between the cheek teeth arcades can be estimated.21
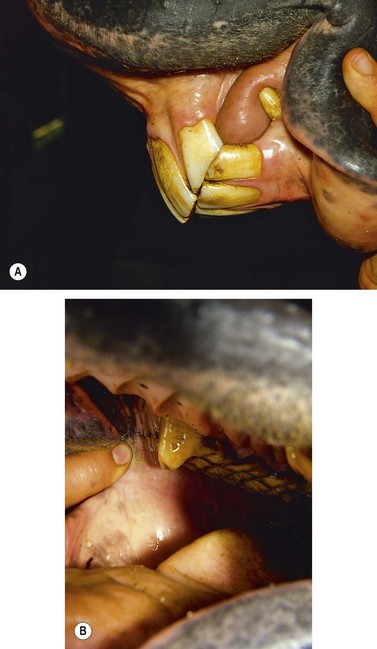
Fig. 17.17 (A) A horse with a slight incisor overjet. Only the upper 01s and 02s are out of occlusion with the lower teeth. The upper 01s and 02s have become elongated from lack of wear. (B) Rostral 106 crown elongation (hook). This tooth has been blunted during floating but the body of the hook is still mechanically forcing the lower jaw in a caudal direction. When these elongations and the corresponding lower 11 hooks were reduced, the incisor arcade came into normal occlusion. The horse could not masticate feed due to a gap between the upper and lower molar arcades. To correct this problem, the upper incisor arcades were shortened 4 mm.
It has been shown that each 1 mm shortening of incisor length decreases the lateral jaw excursion to molar contact distance (EMC) by about 4 mm. EMC rarely increases following removal of sharp enamel points, but may increase after correction of a severe wave mouth or other major cheek tooth elongations. Measuring EMC pre- and post-treatment enables one to return EMC to the original value after cheek teeth corrections. Long incisor reductions have been performed using flexible shaft, cable grinding tools with solid tungsten, carbide grit, or diamond grit burrs (Fig. 17.18). Diamond cut-off wheels, nippers, and forceps have been used to remove large amounts of incisor crown, but these tools can prove dangerous to the horse and operator. Rotary grinders with carbide burrs or fine carbide or diamond files are the preferred tools for reducing and smoothing incisors. The occlusal surface should be ground down in thin (1–2 mm) layers and then checked for molar table contact and EMC.56

Smile bite has been identified as a normal incisor conformation in donkeys.58 If it has been found to interfere with mastication, smile bite can be corrected by reducing the corner teeth in the lower arcade (303, 403). Leveling the upper incisors should only be performed if it is determined that reducing them will not create a gap between the upper central (101, 201) and lower central (301, 401) incisors. Frowning incisors are treated in the opposite manner by reducing the corners of the upper arcade (103, 203). Diagonal (or slightly tilted) arcades can be improved or corrected by shortening the upper or lower long or tall incisors. It may be impossible to completely level the more severely tilted incisors without creating a gap between the upper and lower arcades. Incremental shortening of the tall teeth should be performed every 4–6 months until the incisor occlusal surfaces are closer to level from side to side. Recent studies have shown that it is impossible to predict the long-term benefit of correcting the incisor angles in many of these cases.59 Stepped (irregular bite) incisors may be locked, with the horse unable to move the mandible laterally without opening his mouth, thus reducing cheek tooth occlusion and limiting mastication. The incisors can be leveled from side to side by reducing the tall areas as much as 3 mm at a treatment.
The treatment of horses suffering from infundibular decay of the upper cheek teeth is controversial. Through the years, the belief that cemental hypoplasia and infundibular caries could be diagnosed from an oral evaluation of the tooth has led some to advocate filling these defects.60–62 To date, the only reasonable management tool is to reduce the tall teeth or wave in the opposite arcade in order to decrease stress on the decayed tooth.
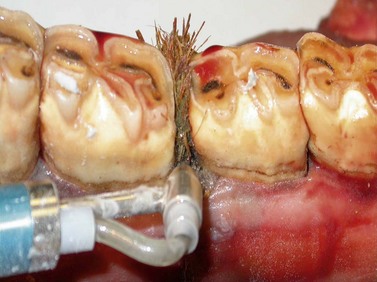
Dental overgrowth has been associated with 62.5 % of horses with diastema and is attributed to abnormal occlusal movements caused by painful periodontal disease.63 Becker described treating diastemata by enlarging the space between the teeth to reduce food trapping.64 The type of diastema he dealt with has been recently defined as a ‘valve’ (or closed) diastema.65 In this pathological situation, food material is able to enter the triangular defect, bounded rostrally and caudally by tooth, distally by gingiva or the periodontal defect, and proximally by the occlusal surface of the dental arcade. Egress of feed material from this space is impeded by the valve effect and the enlarging abnormal wedge or transverse ridge that often forms on the opposing cheek tooth. Quality regular dental care, appropriate crown reductions, and necessary extractions should be the first phase of therapy. Many horses respond positively to repeated removal of dental associated overgrowths.63 Removal of foreign material (plant awns, impacted or decayed feed, and calculi) in the interproximal spaces and gingival sulci speeds healing in many cases (Fig. 17.19). Flushing dental pockets with a syringe and infusion catheter or elongated water pick has been described.20,66 Special long-handled air abrasion units deliver water and medical grade baking soda under pressure, to flush periodontal pockets (Fig. 17.20). In cases where reimpaction of feed is likely, placement of a perioceutic within the sulcus and/or dental impression material in the larger interproximal spaces has shown good results.67,68 Special right-angle burrs have been developed to treat valve diastema (Fig. 17.21). They have been used successfully to grind the dental crown on each side of the valve, opening an occlusal space allowing it to self-clean.69

Fig. 17.19 A high pressure water irrigation unit with a right angle nozzle is used to flush material from a periodontal pocket between 307 and 308.

Complications of dental corrective procedures
Dental corrective procedures should not be attempted by persons unfamiliar with the possible damage improper equipment and/or technique might cause. Simple tooth floating is not an innocuous procedure but can lead to iatrogenic damage to the horse and its dentition. Coarse float blades chip and break the coronal structures of the tooth and open dentin tubules.17 Horses chewing on floats or dental spools have been known to fracture or loosen teeth. Floats and other sharp instruments in the mouth can cause soft-tissue damage that can lead to cellulitis and septicemia. Sharp root elevators and dose syringe tips can lacerate the roof of the mouth and cause severe hemorrhage.70 Power tools must be grounded and have GFI plugs to prevent possible electric shock to the horse and/or operator. Disinfecting agents used on equipment and for flushing the mouth, must be prepared in the proper dilution to avoid caustic irritation. Careless or improper use of molar cutters and chippers or incisor nippers can lead to tooth fracture or extraction (Fig. 17.22). Overzealous grinding of teeth to reduce elongations or even in forming bits seats and blunting canine crowns can cause complications, such as open pulp chambers, tooth decay, or tooth loss (Fig. 17.23). Reducing canine teeth to gum level can lead to tongue lolling in some performance horses. Only a licensed veterinarian should administer an intravenous sedative or analgesic to a horse. Interarterial injections have resulted in severe convulsive reactions or death in some cases. Perivascular medication can cause jugular vein phlebitis or thrombosis, which can end the career of an elite equine athlete. Improperly restrained horses (whether sedated or unsedated) have been known to injure themselves, the operators, and other persons in the work area. Iatrogenic jaw fracture has been seen following the use of a full-mouth speculum.
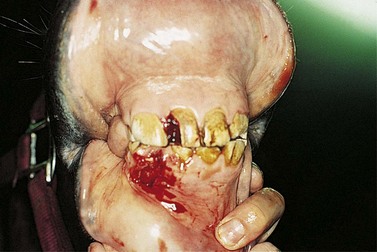

Fig. 17.23 Iatrogenic pulp horn exposure of 106. This tooth had been reduced with a carbide burr in an attempt to create a ‘bit seat’.
Post-dental-procedure pain is experienced by some horses, especially if aggressive crown reductions are performed with power equipment. Affected horses do not eat well for a few days to a few weeks after dentistry. Some veterinarians advocate giving prophylactic non-steroidal anti-inflammatory medication to all dental patients to help prevent this problem.71 This painful condition has been blamed on temporomandibular joint pain, readjustment of the masticatory muscles after speculum use, loose teeth post procedure, leaving the mouth out of balance, thus overloading isolated teeth in occlusion, or exposed dental tubule pain.17,72 These problems are enumerated to emphasize the importance that only veterinarians and veterinary technicians (under the direct supervision of a veterinarian) should perform equine dental procedures. The potential for iatrogenic damage must be kept foremost when performing equine dentistry. The equine practitioner’s job as steward of the horse must be ‘to do no harm.’
Timetable for routine dental examinations
The following timetable is a good reference for scheduling routine dental examinations and general maintenance.73
Birth. Examine for: 1) congenital defects of the lips or palate; 2) tongue motion and strength; 3) dental malocclusions; and 4) body system abnormalities. Recommended procedures are to provide genetic and orthodontic consultation and perform corrective surgery if necessary. Look for other problem signs, such as underdeveloped carpal or tarsal bones, ruptured extensor tendons, and hernias.
6–8 months. Examine for: 1) incisor and premolar occlusion (all incisors should have erupted); 2) missing teeth; 3) sharp enamel points or hooks; and 4) ulcers on the tongue and buccal mucosa. Recommended procedures are to provide orthodontic consultation and float teeth, if necessary.
16–24 months. Examine for: 1) upper and lower wolf teeth eruption; 2) points and hooks on premolars; and 3) bit lesions. Recommended procedures are to float teeth and round off the rostral corners of the second premolars. Extract wolf teeth.
2–3 years. Examine: 1) upper and lower wolf teeth or blind wolf teeth; 2) deciduous tooth eruption – central incisors and premolars; 3) bit injuries at the corners of the mouth and interdental spaces; and 4) points or hooks on molars and premolars. Recommended procedures are to float outside of upper and inside of lower cheek teeth, remove caps, if present and ready for removal, and extract wolf teeth. Rostral corners of upper and lower second premolars should be rounded if the horse wears a bit.
3–4 years. Examine 1) corners of the mouth and interdental space for bit injuries; 2) incisors for retained deciduous teeth or supernumerary teeth; 3) molars and premolars for points and retained third premolars (second cheek teeth); 4) size and shape of the lower jaw; and 5) for presence of blind wolf teeth. Recommended procedures are to remove caps if present, float teeth, and remove wolf teeth.
4–5 years. Examine: 1) incisors for eruption; 2) canine teeth for sharp edges or eruption delays; 3) molar arcade for proper eruption and alignment of fourth premolars; 4) for presence of upper rostral and lower caudal cheek teeth hooks from malocclusion; and 5) for presence of points or sharp edges on cheek teeth. Recommended procedures are to remove deciduous teeth, if ready, grind or rasp hooks, if present, float teeth, and remove mucosa over canines if gingival eruption cysts are present.
5 years and older. Examine: 1) mouth visually and digitally, especially noting hooks and uneven wear; 2) canines for sharp edges and tartar; 3) oral cavity for decay or gingivitis; 4) incisors for even wear; and 5) evaluate lateral jaw excursion. Recommended procedures are to float teeth, remove hooks, correct abnormal wear patterns, and level or shorten the incisors if indicated.
Educate owners and trainers of the need for routine dental examinations. Indicated corrective procedures should be performed before starting any horse in training.
Summary
A thorough visual and manual examination of the equine patient must be performed to identify any abnormalities. Sedating the horse and using a full-mouth speculum facilitate both the examination and corrective procedures. The use of proper dental instruments makes it much easier for both the patient and veterinarian. Dental elongations should be reduced in stages, taking care not to remove more than 3–4 mm of occlusal surface at one time. A dental form should be used to maintain a record of what procedures were performed, what needs to be done in the future, and to itemize the charges.
1 Knottenbelt DC. The systemic effects of dental disease. In: Baker GJ, Easley J. Equine dentistry. 2nd edn. Philadelphia: WB Saunders; 1999:127–138.
2 Tell A, Engenvall A, Lundstrom T, et al. The prevalence of oral ulceration in Swedish horses when ridden with bit and bridle and when unridden. Vet Journal. 2008;178(3):405–410.
3 Ralston SL, Foster DL, Devers T, et al. Effect of dental correction on feed digestibility in horses. Equine Vet J. 2001;33:390–393.
4 Gatta D, Krusic L, Casini L, et al. Influence of correcting teeth on digestibility of two types of diets in pregnant mares. In: Proceedings, 14th Symposium Equine Nutrition and Physiology Society, 1995, pp 326–331
5 Krusic L, Easley J, Pagan JD. Influence of correcting teeth on daily food consumption and glucose availability in horses. In: Proceedings, Symposium Horse Diseases, 1995, pp 53–68
6 Carmalt JL, Townsend HGG, Jazen E, et al. Effect of dental floating on weight gain, body condition score, feed digestibility. J Am Vet Med Assoc. 2004;225:1889–1893.
7 Carmalt JL, Allen A. Relationship between equine cheek tooth occlusal morphology, apparent digestibility, and ingesta particle size. Am Assoc Equine Prac Proceedings. 2008;54:386–389.
8 Tamzali Y. Chronic weight loss syndrome in the horse: a 60 case retrospective study. Equine Vet Education. 2006;18:289–296.
9 Carmalt JL, Townsend HGG, Allen AL. Effect of dental floating on the rostrocaudal mobility of the mandible of horses. J Am Vet Med Assoc. 2003;5:666–669.
10 Bonen SJ. Three-dimensional kinematics of equine temporomandibular joint. Master’s Thesis, Dept of Mechanical Engineering, Michigan State University, East Lansing, 2001
11 Allen T, Jeffery D, Moriarity LA. Routine procedures. In: Allen T, ed. Manual of equine dentistry. St Louis: Mosby; 2003:109–156.
12 Johnson LE. Equine dentistry. In: Bone JF, Catcott EJ, Gabel AA, Johnson LE, Riley WF. Equine medicine and surgery. Santa Barbara: American Veterinary Publications; 1963:739–760.
13 Easley J. Dental corrective procedures. Vet Clin North Am: Equine Practice. 1998;14(2):411–432.
14 Rucker BA. My approach to motorized equine dentistry using the Powerfloat. In: Operator’s manual, Powerfloat. Calgary: D & B Equine Enterprises; 2003.
15 Rach D. Operator’s manual. Calgary: D & B Equine Enterprises; 2003.
16 DeForge DH. Physical ergonomics in veterinary dentistry. J Vet Dent. 2002;19:196–200.
17 Kempson SA, Davidson MEB, Dacre IT. The effect of three types of rasps on the occlusal surface of equine cheek teeth: a scanning electron microscopic study. J Vet Dent. 2003;20(1):19–27.
18 Baker GJ, Allen ML. The use of power equipment in equine dentistry. Am Assoc Eq Pract Proceedings. 2002;48:438–441.
19 Dacre KJP, Dacre IT, Dixon PM. Motorized equine dental equipment. Equine Veterinary Education. 2002;14:263–266.
20 Judd RC. Equine dental prophylaxis using a pneumatic system. Comp Cont Edu. 2002;24(1):62–70.
21 Scrutchfield WL. Dental prophylaxis. In: Baker GJ, Easley J. Equine dentistry. London: WB Saunders; 1999:185–205.
22 Stubbs RC. Dentistry of equine cheek teeth. Am Assoc Eq Pract Proceedings. 2004;50:1–6.
23 Allen T. Incidence and severity of abrasions on the buccal mucosa adjacent to the cheek teeth in 199 horses. Am Assoc Eq Pract Proceedings. 2004;50:31–36.
24 Easley KJ. Equine canine and first premolar (wolf teeth). Am Assoc Eq Pract Proceedings. 2004;50:13–18.
25 Scoggins DR. Bits, bitting and dentistry. In:. Am Assoc Eq Pract Proceedings. 2001;47:138–141.
26 Merillat LA. Animal dentistry and diseases of the mouth. In: Veterinary Surgery. Chicago: Alexander Eger; 1905:189.
27 Wileweki KA, Ruben L. Bit seats: a dental procedure for enhancing performance in show horses. Eq Pract. 1999;21:16.
28 Engelke E, Gasse H. An anatomical study of the rostral part of the equine oral cavity in respect to position and size of a snaffle bit. Eq Vet Edu. 2003;5(3):200–205.
29 Johnson TJ. Surgical removal of mandibular periostitis (bone spurs) caused by bit damage. Am Assoc Eq Pract. 2002;48:463–466.
30 Easley J. Oral and dental disease. In: Hinchcliff KW, Kaneps AJ, Geor RJ. Equine sports medicine. Edinburgh: Saunders; 2004:1027–1036.
31 Fisher D, Easley KJ. Floating: making equine dentistry a practice profit center. Large Anim Vet. 1994;49:16–22.
32 Dixon PM. Removal of equine dental overgrowths. Eq Vet Edu. 2000;12(2):68–81.
33 Pence P, Wileuska K. Mature horse dentistry. In: Pence P, ed. Equine dentistry a practical guide. Lippincott: Williams and Wilkins; 2002:141.
34 Sesson S. Digestive system of the horse. In The anatomy of domestic animals, 2nd edn, Philadelphia: WB Saunders; 1921:395.
35 Nickel R, Schummer A, Seiferle E. The viscera of domestic animals, 2nd edn. Berlin: Verlag Paul Parey; 1979.
36 Lane JG. A review of dental disorders of the horse, their treatment and possible fresh approaches to management. Eq Vet Edu. 1994;6:13–21.
37 Grove T. Extractions and simple oral surgeries in equines. In: Proceedings of Eastern States Veterinary Conference, Vol. 5, (1991), 337
38 Gaughn EM. Dental surgery in horses. Vet Clin North Am: Equine Practice. 1998;14(2):387–388.
39 Colyer JF. Variations and diseases of the teeth of animals, rev edn. Cambridge: Cambridge University Press; 1990.
40 Caldwell LA. A review of diagnosis, treatment and sequelae of incisor luxation fractures in horses (from a dentist’s viewpoint). Am Assoc Eq Pract Proceedings. 2006;52:559–564.
41 Ramzan PHL, Palmer L, Barquero N, et al. Chronology and sequence of emergence of permanent premolar teeth in the horse: Study of deciduous premolar ‘cap’ removal in Thoroughbred racehorses. Equine Vet J. 2009;41:107–111.
42 Earley ET. How to manage maleruptions of upper fourth premolars in the miniature horse. Am Assoc Eq Pract Proceeding. 2007;50:7–12.
43 Faragella F. Rotated maxillary fourth premolar in a horse. J Vet Dent. 2004;21:226–227.
44 Marr T, Love S, Schumacher J, Walson E. Equine medicine, surgery and reproduction. Philadelphia: WB Saunders; 1998. p. 106
45 Easley J. Recognition and management of the diseased equine tooth. Am Assoc of Eq Proceedings. 1991;37:129–139.
46 Dixon PM, Tremaine WH, Pickles K, et al. Equine dental disease part 1: A long term study of 400 cases: disorders of incisor, canine and first premolar teeth. Eq Vet J. 1999;31(5):369–377.
47 Percivall W. Hippopathology. In: Mechener CB, ed. Special report on diseases of the horse. Washington: US Dept of Agriculture; 1911:42–43. (1852)
48 Mitz C, Allen T. Dentistry in miniature horses. In: Allen T, ed. Manual of equine dentistry. St. Louis: Mosby; 2003:175–192.
49 Vandersplassche M, Simeons P, Bouters R, et al. Etiology and pathogenesis of congenital torticollis and head scoliosis in the equine fetus. Equine Vet J. 1984;16:419.
50 Dixon PM, Tremaine WH, Pickles K, et al. Equine dental disease part 3: a long term study of 400 cases: disorders of wear, traumatic damage and idiopathic fractures, tumors and miscellaneous disorders of the cheek teeth. Equine Vet J. 2000;32(1):9–18.
51 Dixon PM, Tremaine WH, Pickles E, et al. Equine dental disease part 4: a long term study of 400 cases: apical infections of cheek teeth. Equine Vet J. 2000;32(3):182–194.
52 Johnson TJ. Correction of common dental malocclusions with power instruments. In: Robinson NE, ed. Current therapy in equine medicine. 5th edn. Philadelphia: WB Saunders; 2003:81–87.
53 Dixon PM. Dental anatomy. In: Baker GJ, Easley J. Equine dentistry. 2nd edn. Edinburgh: Elsevier; 2005:40–43.
54 Scrutchfield WL. Incisors and canines. American Association Equine Practitioner Proceedings. 1991;37:117–121.
55 Rucker BA. Modified procedure for incisor reduction. American Association Equine Practitioner Proceedings. 1995;41:42–44.
56 Rucker BA. Incisor and molar occlusion: normal ranges and indications for incisor reduction. American Association Equine Practitioner Proceedings. 2004;50:7–12.
57 Rucker BA. Utilizing cheek teeth angle of occlusion to determine length of incisor shortening. American Association Equine Practitioner Proceedings. 2002;48:448–452.
58 duToit N, Burden FA, Dixon PM. Clinical dental examinations of 357 donkeys in the UK: part 1 prevalence of dental disorders. Equine Vet J. 2008:138.
59 DeLorey MS. A retrospective study of 204 diagonal incisor malocclusion corrections in the horse. J Vet Dent. 2007;24:145–149.
60 Swanstrom OG, Wallford HA. Prosthetic filling of a cement defect in premolar tooth necrosis in a horse. Veterinary Medicine/Small Animal Clinician. 1977:1475–1477.
61 Klugh DO. Updating infundibular decay in equine cheek teeth. In: Conference Proceedings 16th Veterinary Dental Forum, Savannah, GA, 2002, pp 238–239
62 Greene S. Equine dental advances. Vet Clinics North Am: Equine Practice. 2001;17(2):319–334.
63 Dixon PM. Equine dental disease part 2: a long term study of 400 cases: disorders of development and eruption and variations in position of the check teeth. Equine Vet J. 1999;31(6):519–528.
64 Becker E. Cited in Becker E. Zähne. 1962. Handbook of specialized pathological anatomy of the horse, Verlag Paul Parey, Berlin, 1945:146.
65 Carmalt JL. Understanding the equine diastema. Eq Vet Edu. 2003;3(1):43.
66 Mueller POE, Lowder MQ. Dental sepsis. Vet Clinics North Am: Equine Practice. 1998;14(2):349–363.
67 Pence P, Basile T. Dental infections. In: Pence P, ed. Equine dentistry: a practical guide. Philadelphia: Lippincott, Williams and Wilkins; 2002:215–219.
68 Greene S, Basile T. Recognition and treatment of equine periodontal disease. American Association Equine Practitioner Proceedings. 2002;48:463–466.
69 Dixon PM, Barakzai S, Collins N, et al. Treatment of cheek teeth by mechanical widening of diastemata in 60 horses (2000–2006). Equine Vet J. 2008;40:22–28.
70 Dixon PM, Hawkes C, Townsend N. Complications of equine oral surgery. Vet Clin Equine. 2009;24:499–515.
71 Greene S. Equine dentistry, notes for Advanced Dentistry Laboratory, American Association of Equine Practitioners Annual Meeting, New Orleans, 2003
72 Johnson TJ, Iatrogenic damage caused by modern dentistry procedures. Robinson and Sprayberry. Current Therapy in Equine Medicine, 6th edn. Saunders/Elsevier, St Louis, 2009:324–327.
73 Easley KJ. Equine dental development and anatomy. Am Assoc Eq Pract Proceedings. 1996;42:1–10.