CHAPTER 12 Dental and oral examination
Introduction
Oral and dental diseases are common occurrences in horses, as evidenced by the results of studies carried out on abattoir specimens.1–5 Signs of dental disease are often not apparent to the owner until the disease is well advanced.6 Casual dental examination as part of a complete physical examination is not sufficient to detect most equine oral or dental problems, as demonstrated by the reported high incidence and the comparatively low clinical diagnosis of dental disease.7 Clinical signs of dental disease are often not specific and may be reflected as systemic disorders, such as weight loss, diarrhea, colic, endocarditis, and septicemia, both in the horse and other species.8–14 In order to diagnose diseases afflicting the buccal cavity, the same degree of systematic rigor must be applied as would be the case during a lameness investigation.
A complete dental examination includes detailed observation and palpation of both hard (teeth and supporting bones) and soft oral tissues (lips, cheeks, tongue, palate, gingiva, oral mucosa, salivary glands, and ducts and muscles of mastication) for evidence of pathological changes.
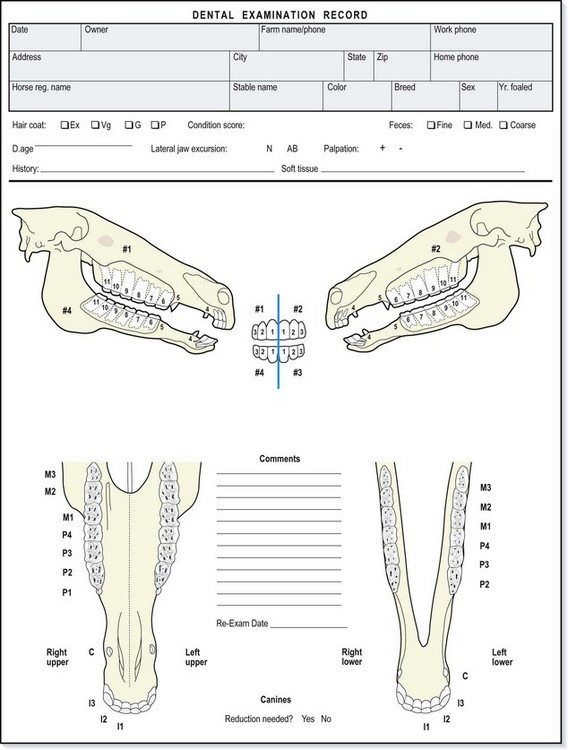
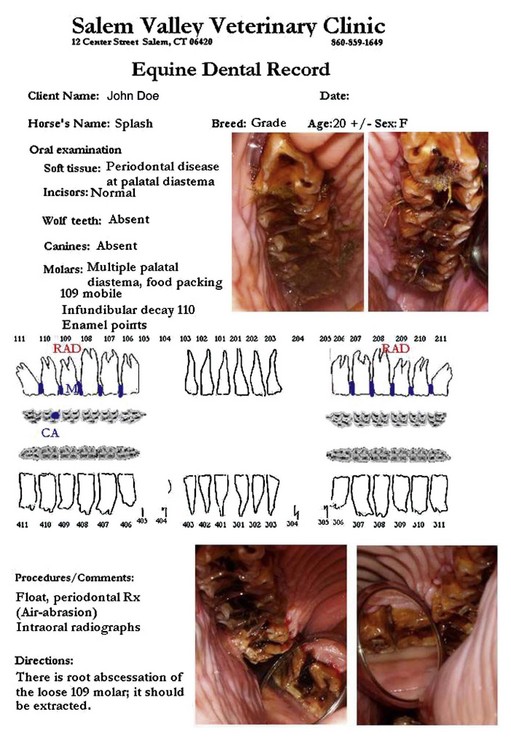
The basis of modern clinical therapy is achieving an accurate diagnosis with information obtained by a clinical examination and ancillary tests. Although performing a comprehensive history and physical examination on every patient having routine dental work would be a valuable service to clients, this is not practical in most cases. However, one must identify any possible medical problems that may impact the safe delivery of dental care. The minimal dental examination must be thorough enough to detect abnormalities in their early stages of development. Treatment can then be initiated before irreversible damage occurs. The extent of the examination should be based on the information obtained in the history and the findings from the initial examination. Variations and/or abnormalities detected at the time of the examination must consistently be documented. A standard dental record form can be an invaluable aid in helping develop good examination habits (Fig. 12.1). Computerized dental records allow information to be more available for retrieval (Fig. 12.2).15
Equipment
The technique for restraint and size of equipment needed varies for different ages and sizes of equine patients. Very large (1000 kg or more) draft breeds need restraint with more heavily constructed equipment than the typical (500 kg) riding horse. On the other extreme, the pony (100 kg) and miniature breeds require smaller equipment. Oral examination and dentistry on small horses may also be aided by walking the horse up on an elevated platform to have the oral cavity at a more comfortable height for the operator’s visualization and work plane. Equipment should include a large noseband halter, a metal-framed dental halter or head stand, mouth speculum, light source, oral irrigator, dental probes and picks, lingual and buccal retractors, and an intra-oral mirror or endoscope.16,17 Further details of this equipment are given in Chapter 16.
Dental signalment
Data on the horse’s owner and trainer/manager/agent/groom should include their names, addresses, and means of contact. This is especially important for the person granting permission to work on the horse and the person responsible for payment of services rendered. The horse’s insurance status and type of policy (mortality, loss of use, major medical, and surgical) should be recorded. Informed consent should be recorded before embarking upon any corrective procedures. Recording the stable name and address and the horse’s location on the premises (barn number, paddock, stall number, etc.) can be helpful if re-examinations are needed. The horse should be identified on the record by name and described by breed, color, sex, age, type of work, and any special identifying markings, scars, brands, or tattoos.
Dental history
The dental history should focus on oral-, dental- and gastrointestinal-related areas. Special consideration must be given to other body systems related to masticatory function or issues that may affect the safety of the horse or veterinarian. A history of cardiac abnormalities, respiratory disease, renal problems, hepatic disease, or neurological signs could affect the way the animal is restrained for examination and treatment. The animal’s breeding history and pregnancy status could have an effect on dental care scheduling, although it has been shown that it is safe to sedate mares at any time during gestation.18,19 Additionally, the horse’s show or race schedule may have an impact on when work is performed and whether drugs used to sedate or treat the horse could be considered prohibited substances. The owner should be questioned about the horse’s fitness and type of exercise, temperament, stable vices, eating and drinking habits, fecal consistency, and physical abnormalities. Specific questions asked could begin with these examples: has the horse gained or lost weight over the past year? Have the horse’s temperament or stable habits changed? Does the horse train well, and what type of bridle and bit does he wear? Have any changes been noticed in the horse’s head carriage or demeanor when bitted? Does the horse make any noises or wear a tongue-tie when exercised? Details of the horse’s eating habits and vices should be taken, and changes in eating or drinking patterns described.
Clinical detection of dental disease may at times be difficult because of the subtlety of signs. These may include reluctance to start eating, slow or intermittent eating, dribbling of food from the mouth (quidding), and head shaking or head tilting when eating. Sometimes, these signs are only detectable by careful direct observation of the mastication process while the horse eats several different types of food. This can be time consuming, but it is often unwise to accept the owner’s report of ‘normal eating.’8 Horses with sharp enamel points may pack forage in the buccal space, pushing the cheeks away from the upper teeth before eating grain. Information about water sources and drinking habits should be ascertained, and one should question if excessive salivation, oral malodor, or nasal or lacrimal discharge has been noticed.
The diagnosis of dental-related head shaking or bit resentment may be relatively easy in cases with obvious dental disease, but is often very difficult where there is no overt evidence. Head shaking is often attributed by lay persons to the presence of wolf teeth, their position, and/or size. Likewise, horses with facial pain around the mental or infraorbital nerves may present with signs of head shaking.8
The horse’s vaccination and deworming status should be determined. This is a good time to discuss these important preventative health topics, as further discussed in Chapter 4. Tetanus toxoid should be given to unvaccinated horses if corrective dental procedures, such as wolf tooth extraction, are performed or if oral abrasions occur during dental procedures. The owner should be questioned about the animal’s history of infectious disease, as well as the presence of infectious or contagious disease on the farm. This information may affect the degree of sanitation used between patients on the premises and the degree of disinfection or sterilization of equipment and personal items required before visiting the next stables. Epidemiological studies have shown 10 % of the horse population in some regions carry methicillin-resistant Staphylococcus aureus (MRSA). So, it is advised for operators working in the equine oral cavity to wear gloves (Fig.12.3).20

Fig. 12.3 Human hand infected with Staphylococcus aureus. Dental practitioners should wear gloves to protect against skin abrasions from sharp tooth points.
If the equine patient is being examined for a particular dental complaint, a complete history of the problem should be ascertained and documented. It has been shown that horses presented with a dental complaint are 5.8 times as likely to have one or more selected dental abnormalities.7 However, a complaint of a specific dental problem should not deter the veterinarian from obtaining a complete dental history and performing a thorough dental and physical examination.
Patient observation
Observation of the animal in its normal surroundings can provide information about stable management, eating habits, and vices. The area where the dental examination is performed must allow for safe restraint and should be free of obstacles that could injure the horse, an attendant, or the veterinarian. An area with a high ceiling shaded from bright sunlight with solid walls and a soft, non-slip floor is ideal. Access to warm water and electricity are beneficial.
The horse should be observed, and his temperament assessed. Hair coat and body condition should be evaluated by observation and palpation. Body condition scores range from 1–9, with 1 describing an extremely emaciated animal and 9 describing obesity (Table 12.1). The optimal condition score is between 5 and 6.21 Objective data, such as photographs and weight measured with a scale or tape can be recorded. These data can be a valuable tool in management of dental health and patient nutrition. The animal’s posture and stance should be observed, and abnormalities such as swellings, injuries, and hoof problems should be brought to the attention of the owner/groom and noted in the record.
Table 12.1 Description of the numerical body condition score system21
The stable floor should be surveyed for grain dropped from the horse’s mouth or partially chewed boluses of quidded hay (Fig. 12.4). Feces should be examined for volume and consistency, as this can reflect how well the horse is masticating its feed (Fig. 12.5).22 Manure should be semi-moist, and fecal balls should be formed. Feces with long forage stems or whole grain indicate poor mastication. Long stems in poorly masticated feed can predispose the horse to esophageal choke, intestinal impaction colic, or diarrhea.


The horse’s body and head type should be assessed and recorded. Head conformation can be reflected in the conformation of the dental arcades. Horses with short dished faces, typical of the Arabian breed, may have a more curved arcade with marked dorsal angulation of the lower 10s and 11s (exaggerated Curvature of Spee). Breeds that typically have long straight heads (Thoroughbred and some Warmblood breeds) are predisposed to malocclusion of the cheek teeth, leading to rostral and caudal cheek tooth overgrowth (‘hook’) formation. Miniature horses and ponies are more prone to dental overcrowding and subsequent misplaced or malerupted dentition.
Extraoral physical examination
During the basic physical examination (temperature, pulse, respiratory rate, auscultation of heart, lungs, and abdomen) the clinician can assess the horse’s temperament. The examination should be performed using techniques of good horsemanship that gain the confidence of the horse and owner.
The head should be evaluated for symmetry, balance, and gross abnormalities that may give clues to dental problems. Standing at the horse’s side, head shape and conformation should be assessed, and bumps or protuberances noted. Young horses between the ages of 2.5 and 4 years will have symmetrical, non-painful bony enlargements beneath the mandible and/or over the maxillary region as a result of normal eruption cyst development beneath the developing permanent teeth. If these enlargements are hot, swollen, asymmetrical, or associated with a draining tract, apical infection should be suspected (Fig. 12.6).

Fig. 12.6 Firm enlargement rostral and dorsal to facial crest. This horse suffered from an apical infection of 207 confirmed on radiographs.
The eyes should be clear and free from lacrimal discharge. Standing directly in front of the horse, the ears, eyes, facial crests, and nasal bones should be symmetrical. The temporalis and masseter muscles and temporomandibular joints should be observed and palpated. The mouth should be opened slightly, and the frontal and maxillary sinuses percussed. The parotid salivary glands and intermandibular lymph nodes should be palpated, as should the ventral aspect of both sides of the mandible, for the presence of enlargements. The blood vessels and parotid salivary duct at the rostral edge of the masseter muscle should be palpated. It has become popular to evaluate acupuncture points in the temporal region to aid in the diagnosis of dental or myofacial problems.23 The hands should be placed under the nose band of a loose halter and pressure exerted on the cheeks at the level of the upper cheek teeth. Palpation from the level of the medial canthus of the eye, progressing rostrally over the masseter muscle to the level of the nasal notch, allows detection of abnormal wear patterns on the lateral aspect of the upper cheek teeth. If the horse resists this maneuver by tossing its head, it is most likely the result of pain from sharp enamel points pressing against the buccal mucosa. If such sharp points are present, they should be floated prior to using a full-mouth speculum. Otherwise, as the mouth is opened with the speculum in place, the cheeks are pushed tightly against the sharp enamel points, and the horse will object to opening its mouth and resist examination.
The nasal passages are observed and the false nostrils palpated, with any asymmetry of air flow, odor, or discharge from the nostrils noted. Sepsis of the cheek teeth commonly results in either nasal or paranasal sinus sepsis or respiratory obstruction.
The lips should be observed and palpated for bit injuries, noticing especially any scars or ulcers in the commissures, and any focal lesions that may indicate previous suppurative tracts from incisor apices. The lips of grey horses are a common site for melanomas. The upper lip should be rolled up and the underside examined for a tattoo (Table 12.2). The labial mucosa should be salmon-pink and glisten with saliva. Ulcers or erosions should be documented, and their cause determined, keeping in mind the possibility of viral lesions, such as vesicular stomatitis, which is a reportable zoonotic disease in some countries. If dental abnormalities are suspected from the history or examination, consider observing the horse eating before the mouth is washed for the oral examination and before sedation is administered.
Table 12.2 A note on lip tattoos
| Most horses that race in the USA are permanently identified with a freeze brand on the neck or a tattoo on the upper lip. Each breed registry has a different alphanumeric system for identifying horses by their upper lip tattoo. |
| The Jockey Club of North America uses an alphanumeric system that consists of a letter of the alphabet followed by numbers. The letter corresponds to the year the horse was foaled, with 1997 starting a new 26-letter series. Therefore, 1996 would be Z and 1998 would be B. Horses imported into the USA are identified with an asterisk (*) at the beginning instead of a letter. |
| The American Quarter Horse Associationer (AQHA) uses a more random alphanumeric system of five numbers in older horses and since 1983, four numbers followed by a letter. However, in 2009 the last books with the numbers followed by Z were sent out to lip tattooers. The new books will have a series of 5 numbers. In the past, AQHA has advised owners that a series of 5 numbers indicates a paint tattoo number. That will no longer be accurate in 2009 or later. |
| The American Paint Horse Association uses a numbering system that consists of five digits. The first digit corresponds to the last digit of the horse’s year of birth. These first digits would be repeated every 10 years. |
| Since 1982, the United States Trotting Horse Association has used a system starting with A followed by three or four numbers (A in 1982 to Z in 2002). Horses born prior to 1982 were tattooed with three digits followed by a letter. Starting in 1996, 98% of trotters are freeze branded only. |
| Arabian and Appaloosa horses that race in the USA require lip tattoos for identification. Their six-digit registration number is tattooed on their upper lip. |
When evaluating the horse’s eating patterns, a distinction must be made between the horse having trouble with prehension and mastication and the horse that is dysphagic (unable to swallow). Prehension requires neuromuscular coordination and an intact jaw and incisor arcade. Mastication is usually altered by dental disease or abnormalities in the jaws, muscles, or temporomandibular joints. Tongue lesions or basal ganglion problems can also adversely affect prehension and mastication. Swallowing is a more complex process, and neurological, muscular, or mechanical abnormalities in the pharynx or esophagus should be considered in addition to dental disease. Rabies is a fatal zoonotic disease that, in its early stages in the horse, mimics other types of prehension and swallowing disorders. Equine practitioners and any assistants working in horses’ mouths should be vaccinated for rabies and have antibody titers checked periodically in areas where rabies is endemic.24
While standing in front of the horse, the lips are parted and the incisor teeth evaluated for number, shape, and symmetry. When viewed from the front, the occlusal line of the upper and lower incisors should be horizontal or parallel to the ground and the presence of diagonal incisor malocclusion is recorded (Fig. 12.7 A,B).25 When viewed from the side, the incisor occlusal surfaces should be parallel to the angle of the facial crest, which is usually about 10–15° relative to the lower molar table surface. The incisors should be checked for anatomical characteristics used in assessing the horse’s dental age, and the estimated age is then compared with the horse’s real age, with a discrepancy between these two values possibly indicating abnormal incisor development or wear. It is important to acknowledge the variation between horses in their incisor appearance and real age26–29 (see Ch. 7). The incisors should be observed while the jaw is moved. Rostrocaudal movement of the mandible can be evaluated by observing the relationship between the upper and lower incisor when the chin is raised and lowered. A normal foal has 3–4 mm (adult horse 6–8 mm) of rostral-caudal jaw excursion when the head is raised and extended as much as possible and then flexed back into a vertical position.30,31 Horses with severe wear abnormalities, such as tall cheek teeth, focal overgrowths, or a step-mouth may have limited rostral-caudal range of mandibular motion.


Fig. 12.7 (A) 14-year-old American Quarterhorse with a facial curvature. This horse was injured as a yearling, and 208 did not erupt, leaving only 5 cheek teeth in the left upper arcade. (B) Incisors of the same horse, with diagonal incisor malocclusion (200/400 DIM).
Lateral jaw excursion is best evaluated by standing to one side of the horse and holding the head stationary with one hand on the bridge of the horse’s nose. The other hand is used to grasp the mandible and, while pressing the mouth shut, move it from side to side. As the jaw is moved from one side to the other, the range of lateral movement present before contact is made by the cheek teeth (and thus separating the incisors) is recorded. The more rostral cheek teeth contact first, and the more caudal cheek teeth later contact as the jaw moves more laterally. Horses that have had their rostral cheek teeth reduced in height have to move the lower jaw further before their incisors separate. Excursion to molar contact (EMC) is the distance the mandible travels laterally to cheek teeth contact. The average light breed horse has an EMC of 12.3 mm (SD = 3.1 mm), while miniature horses and ponies have an EMC of 5–6 mm, and draft breeds an EMC of 15–16 mm.32,33
The second measurement noted in this procedure is the total lateral distance the mandible travels. By observing the incisors and listening to and feeling the molar arcades grind on one another, one can gain information about the occlusal slope of the cheek teeth and the symmetry of the occlusal contact between the upper and lower cheek teeth.34–36 The average light horse can move the center of the mandibular incisors laterally 45 mm ± 5 mm while chewing.37 Normal lateral excursion produces a relatively even, subtle to moderate vibration and sound. Deviations from this can be an indication of abnormal dental contact due to cheek teeth overgrowths. It must be kept in mind that this maneuver does not replicate the chewing motion of the horse as outlined in Chapter 6. If the horse resists this part of the dental examination, sedation may be indicated to help the horse relax and allow a more thorough physical examination. With sedation, a complete dental examination can be carried out more safely and thoroughly, although the benefits of this may require explaining to some owners who may have an innate apprehension of the perceived side-effects of sedation (see Chapter 15).
Oral examination
The mouth is the window into the body. For too long, many equine veterinarians have assumed erroneously that the gastrointestinal tract starts with the esophagus. The oral mucous membrane is a thin sheet of tissue that permits the veterinarian to view changes in vessels and connective tissue beneath the oral mucosa. There are relatively few sensory nerve endings in the gingiva, which makes it a safe area to depress for observing vascularity and capillary refill time (CRT).
Male horses between 4 and 6 years old may have canine teeth in various stages of eruption. The upper canines usually erupt 2–8 months after the lowers. Eruption cysts or tenting of the mucosa with ulceration over these teeth can cause oral pain and bitting problems. Long sharp canine teeth can be a danger to the examiner, and care should be exercised to avoid injury when manually examining the mouth. About 25 % of mares have one – four rudimentary canine teeth.38 Dental calculus around the canines leading to gingivitis is common in older horses.
The upper and lower interdental spaces should be observed and palpated. By firmly running a thumb over the mucosa, one can feel for protuberances above or below the gingiva and observe the horse’s response to pressure. The lower bars should be checked for bony irregularities, mucosal ulcers, or thickenings or the presence of wolf teeth.39 Remodeling of the mandibular cortex rostral to the 2nd premolar can be palpated through the gingival mucosa and can indicate previous bit trauma, and may be associated with bit-sensitivity. The upper diastema is then palpated for bony abnormalities and the presence of wolf teeth. Unerupted wolf teeth, referred to as ‘blind wolf teeth,’ can cause oral discomfort and training problems in bitted horses. The distance from the commissures of the lips to the rostral edge of the first cheek teeth should be noted as this varies among horses. This distance affects the ease with which one works on the rostral teeth and may affect the most comfortable position of the bit in a working horse.
The tongue should be checked for function, and any anatomical abnormalities noted. Tongues are frequently injured from harsh bits or neglected tongue ties and from sharp teeth. The so-called ‘lampas’, or thickening of the palatal mucosa just behind the upper incisors, is common, and a normal feature in young horses that are erupting permanent dentition. The hand can be introduced into the interdental space and a thumb pressed on the hard palate to make the horse open its mouth. Great care should be exercised whenever a finger is placed in the mouth, to avoid serious injury.
The easiest and safest way to thoroughly evaluate the oral cavity is by using a full-mouth speculum and a bright light source. Prior to placement of the speculum, it is advisable to rinse excess food from the mouth with a syringe, hose, or other device. To place the McPherson-type speculum in the mouth single-handed, the examiner stands to the left side of the horse. With the left hand holding the mouthpiece and the right hand holding the poll strap, the mouthpiece is introduced between the incisors in the same manner as a bit. The left thumb and forefinger are used to open the mouth and guide the mouthpiece into place between the incisors while the right hand applies steady tension to the halter strap from behind the horse’s poll. When the speculum is properly positioned, the left hand tightens the halter’s buckle to adjust the strap length until the speculum strap is snug. The bite plates are adjusted to square them with the incisors. A final check is made to ensure that the teeth and incisor plates are free of tongue, lips, and examiner’s digits when opening the speculum. It is important to loosen the noseband and chin strap to allow a stable yet comfortable fit on the horse. The jaws of the speculum are opened one notch at a time alternating each side until the jaws are adequately opened. If the mouth cannot be opened with the speculum in place, the temporomandibular joints and bony structures of the jaw should be carefully evaluated before excessive force is placed on the jaw. At this point, the oral cavity is ready for visualization and palpation. Use of a head support stand or metal frame dental halter is recommended to elevate the head of a sedated horse to a comfortable height for good visualization and palpation (Fig. 12.8).

Fig. 12.8 Horse sedated with head resting on a dental stand. The mouth is open with the speculum in place. The operator is seated in a comfortable position, allowing complete digital and visual examination of the oral cavity.
To examine the oral cavity, good illumination is critical. A battery-operated light that attaches to the upper incisor plate of the speculum or a powerful headlight provides good illumination while allowing both hands to be free for intra-oral procedures. A blade retractor fitted with an illuminator aids in the evaluation of the buccal recesses. A basket retractor keeps the tongue and buccal mucosa pulled away from the teeth for good visual access to the last few cheek teeth (Fig. 12.9). The oral soft tissues should be observed with special attention paid to the palate, tongue, and buccal mucosa (Fig. 12.10). The teeth should be evaluated for conformation, position, number, and abnormalities. Enamel points on the buccal and lingual enamel folds or cingula usually do not protrude beyond the level of occlusal surface of the cheek teeth. The acute angle between the vertical edge of the tooth and the occlusal surface can cause sharp enamel points to look and feel quite prominent. A dental pick with a long shaft can be used to probe the four corners of the cheek teeth to detect and clean out periodontal pockets (Fig. 12.11A, B). A calibrated pick can be used to measure gingival pocket depth, which will range from 0.5–12 mm for normal teeth. It has been shown that gingival pocket depth measurements at the corners of the teeth significantly increases with periodontal disease.40,41 Defects have been found over the pulp horns on the occlusal surfaces of a large number of periapically infected teeth and can be detected by carefully probing the secondary dentin of the occlusal surfaces of suspect teeth (Fig. 12.12).3,42,43

Fig. 12.9 View of the oral cavity with a mouth speculum, basket-type retractor, and attached light in place.

Fig. 12.10 Sharp enamel points on the 210 causing a deep buccal ulceration. This photo was taken using a rigid endoscope with a 45° optic.

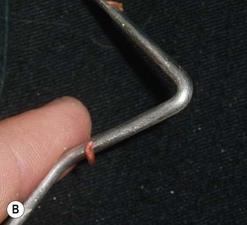
Fig. 12.11 (A) An equine oral mirror used to visualize an ulcerated area in the palatal tissue above a small diastema between 108 and 109. (B) A periodontal probe used to clean the pocket between 109 and 109. Gastrophilus (bot fly) larvae were removed from the shallow ulcerated area.

Fig. 12.12 A fine dental pick is used to explore the #1 pulp horn of 106. This pulp horn contained plant fibers in the area that should be covered with firm secondary dentin. This is a common finding in teeth with apical infections and pulpitis.
The oral cavity should be palpated, feeling the buccal, occlusal and lingual surfaces of all four arcades. The gingival margins of the cheek teeth should be uniform with no feed packed between them. The crown height should be the same on the rostral and caudal aspect of each tooth, but should be taller on the buccal aspect of the upper and the lingual aspect of the lower cheek teeth. Any deviation or asymmetry in the cheek teeth occlusal surface height or angle should be noted (Fig. 12.13). Each cheek tooth crown should be grasped between the thumb and forefinger and checked for stability, noting any movement or pain reaction. The occlusal surfaces of the cheek teeth should be palpated, noting any defects or asymmetry in the occlusal crown surface, bearing in mind that a defect in one cheek teeth row is usually reflected in a wear abnormality or defect in the opposite row.

Fig. 12.13 The caudal aspect of the left lower dental arcade is ramped. The crown height above the gum helps determine whether this is a true caudal dental elongation (hook) or simply the last molar erupting in the curve of the jaw (Curvature of Spee).
An oral examination is not complete without evaluating the mouth with the aid of an equine dental mirror or ridged endoscope. A dental mirror designed for use in the horse’s mouth needs to have a diameter of at least 5 cm set at 30–45° and should be set on a rigid shaft long enough to reach the back of the horse’s mouth. Warming the mirror in hot water or applying an anti-fogging spray helps keep it clear. The rigid shaft allows the mirror to retract the tongue and buccal tissue as it is moved into the more caudal parts of the mouth. Oral endoscopy has been found to be superior to all other examination methods in identifying all types of dental disease, except for occlusal wear abnormalities (Fig. 12.14).44–47

Fig. 12.14 Proper positioning for performing an oral endoscopic examination. The monitor should be positioned at the level of the horse’s shoulder to allow good orientation.
Oral endoscopy
Dental endoscopy facilitates the exploration, visualization, magnification, and recording of lesions of the oral cavity and has a great role to play in education as well as the demonstration and documentation of lesions within the oral cavity. Dental endoscopy enhances the diagnostic value of the oral examination and has become a routine part of dental and oral disease investigations.
Dental endoscopy can be performed with either a flexible fiberoptic or videoendoscope but is much easier using a rigid telescope, such as an instrument designed for human laparoscopy, which is less vulnerable to traumatic damage by the teeth.
A 40–50-cm telescope with a 30–90° viewing angle is ideal. The durability is improved if the telescope is protected in a stainless steel sheath. An additional outer plastic sheath is a useful addition to dampen any vibrations when the telescope contacts the rostral teeth during examinations. The telescope is coupled to a chip camera and monitor to enable viewing and, if necessary, recording of the images. More recently, a specifically designed oral endoscope, angled at 90° to the shaft with chip camera and image capture, has become commercially available.
Horses should be sedated for dental endoscopic examinations. The ideal depth of sedation results in the horse resting its chin on a stand or suspended halter with a low probability of upward jerking of the head. Tongue movement can impair a thorough endoscopic examination. Additional muscle relaxation can be achieved using 5–10 mg of diazepam, IV.
The endoscopic examination is always preceded by a thorough visual and digital examination of the oral cavity. Start with examining the occlusal surfaces and buccal and lingual aspects of all teeth beginning with cheek tooth 106 and then advancing the endoscope caudally, inspecting each occlusal surface in turn, and noting any defects in the occlusal surface that may be of pathological significance (Fig. 12.15). Any potential defects in the surface, particularly of the secondary dentin corresponding to the pulp horns or areas of infundibular cemental hypoplasia, are re-examined while inserting a fine occlusal probe or pick into the defect (Fig. 12.16). The endoscope is then rotated and repositioned to examine the palatal mucosa and interdental spaces, noting any fibrous food entrapment and diastema.

Fig. 12.15 Double crown fracture of 210. Buccal and lingual slab fracture fragments have been lost, and the surrounding gingiva healed. This photo was taken using a rigid endoscope with a 90° optic.

Fig. 12.16 Endoscopic occlusal view of an apically infected 409. A flexible probe has penetrated the degenerate secondary dentin overlying the #1 pulp horn. This photo was taken using a rigid endoscope with a 90° optic.
The endoscope is finally rotated to the buccal aspect of 106, and advanced caudally to identify diastema, displaced teeth and in particular, mucosal ulcers. The gag may need to be loosened slightly to enable sufficient cheek tooth retraction to thoroughly explore the buccal mucosa. Deep periodontal pockets are thoroughly cleaned using a pick and water jet and then re-examined for the presence of inflamed or granulating tissue (Fig. 12.17). The findings for each arcade are annotated into the dental chart, and the second arcade commencing with 206 is examined. The mandibular arcades are examined in a similar fashion. When examining the mandibular arcades, the lingual aspect of the arcade may be visualized more successfully if the tongue is retracted.

Fig. 12.17 Endoscopic view of a 310–311 diastema 3 months after periodontal treatment. Feed is no longer packing in the periodontal pocket, and the mucosa is healed. This photo was taken using a rigid endoscope with a 90° optic.
Oral endoscopy has been invaluable in the identification of open pulp horns, infundibular caries, periodontal disease, and oral soft tissue lesions, which are almost impossible to identify on the most thorough visual examination. The presence of small fissures in the secondary dentine may indicate a communicating tract between the oral and pulp cavities, or previous pulpal insult that has resulted in failure of secondary dentin production in the coronal pulp horn. A fine pick can be inserted into the fissure in an attempt to determine its depth. Infundibular cemental hypoplasia is commonly observed by dental endoscopy. The size and shape of the infundibula depends on the age of the horse. In young horses, the presence of wider infundibula that resemble incisor cups, is normal. In older horses, infundibular cemental hypoplasia most commonly affects the 109 and 209, and increases the likelihood of food impaction and decay (Fig. 12.17). After removal of the entrapped food, the extent of inflammation associated with periodontitis and the depth of periodontal pockets, can be assessed. The angled view and magnification provided by endoscopy often reveal small buccal or lingual ulcerations.
Ancillary diagnostic tests
If the initial dental examination findings reveal signs of dental disease, other diagnostic techniques can be employed to make a more definitive diagnosis. Where plant awns or bot fly larva are detected, soft tissue lesions inside the oral cavity should be assessed grossly, and surface scrapings taken for microscopic evaluation. Larger oral masses can be biopsied for histopathology. Molecular methods of tissue testing permit definitive identification when standard culture and phenotypical criteria are inconclusive (see Ch. 11). Skull radiographs, both plain and contrast film studies, and intra-oral radiographs give added information about dental, osseous, and sinus structures48 (see Ch. 13). Other imaging modalities, such as ultrasonography, computerized tomography, nuclear scintigraphy, or fluoroscopy may reveal a more accurate picture of some dental abnormalities.
Disease of the upper last four cheek teeth may be associated with sinus disease, commonly presenting with unilateral nasal discharge. Endoscopy of the nasal passages can confirm whether or not the discharge is coming from the nasomaxillary opening. Malerupted teeth have been seen to obstruct the nasal passages, which can make passing an endoscope difficult if not impossible on the affected side. Sinoscopy has been valuable in diagnosing and treating some sinus disorders without the need for exploratory flap sinusotomy, as described in Chapter 14.49,50,51
Dental records and treatment planning
The horse’s signalment, use, and management should be recorded. Pertinent history should be noted, with special emphasis on digestive system or performance problems. The horse’s general body condition should be recorded, and a numbered body score assigned. The results of the masticatory system examination should be recorded, and problems listed in order of significance. A plan for treatment of each problem should be outlined based upon the results of history, clinical findings, and oral examination before proceeding with any dental work. This problem-orientated approach is important because the owner and/or trainer should be informed of any abnormalities, given a plan for treatment, and an estimate of the cost before any corrective procedure is performed. An owner consent statement is often included in record forms and can minimize problems should a legal claim be filed against the veterinarian or a bill come in dispute for collection. Recording images, videos, and radiographs digitally allows these images to be incorporated in the computerized dental record.15,52
Oral and dental charting
Charting is the process of recording the state of health or disease of the teeth and the oral cavity.53 To properly chart the mouth, the dental formula and anatomical locations in the mouth must be standardized to make documentation consistent. Use of standard abbreviations for dental terms to describe anatomical boundaries, abnormalities, diagnostics and therapeutic procedures make communication possible between equine practitioners and other colleagues in both the veterinary and human dental professions.16,54
The American Veterinary Dental College Nomenclature and Classification Committee has endorsed the use of the Triadan tooth numbering system55,56 (see Ch. 5).
To fully understand equine tooth development and anatomy and to properly document abnormalities for dental record keeping, certain oral topographical terms have been defined. For a unique identification of each surface of a tooth, the following descriptions are used:
• Apical: toward the apex (or root once developed)
• Occlusal: masticatory surface
• Vestibular: toward the vestibule of the cheeks or lips
• L lingual: toward the tongue in the upper or lower arcade
• P palatal: toward the palate in the upper arcade
• IPM or D: proximal or interproximal: between teeth, mesial or distal
• Mesial: anterior or rostral (interproximal surface nearest to mandibular symphysis)
• Distal: posterior or caudal (interproximal surface farthest from mandibular symphysis).
Computerized dental charting and record keeping are used in human and veterinary dentistry. Standardized abbreviations and record forms are essential to make this transition into equine practice. Some common dental abnormalities and a standardized grading system are presented to help chart dental findings in a uniform manner. The system presented here has been proposed by the American Academy of Veterinary Dentistry and the American College of Veterinary Dentistry but other systems and abbreviations are in use.
• TO: tooth overgrowth: for incisors determined after cheek teeth reduction to achieve arcade balance.
• MAL2: Class II malocclusion, overbite, brachygnathism, parrot mouth.
• MAL3: Class III malocclusion, underbite, prognathism, monkey mouth.
• CV: ventral curvature of the incisor arcade, ‘smile’.
• CD: dorsal curvature of the incisor arcade, ‘frown’.
• DGL or DIM: diagonal incisor arcade. Given a number with respect to which lower incisor arcade is the longest. (i.e., DGL/4, 400 arcade longer or the two longer arcades 200/400DIM). (See Fig. 12.7.)
• PTS: sharp enamel points (these can affect individual teeth, entire rows of teeth, or all four arcades uniformly). These enamel elongations have been classified as mild (1–3 mm tall), moderate (3–5 mm tall), severe (>5 mm).47
• HK: crown hook, elongation longer than wide.
• BK: beak, small enamel point on the ends of the arcade.
• RMP: ramp, elongation wider than long.
• ETR: excessive transverse ridge.
• CUPD – cup in central portion of crown.
• BI (L, A, or U): buccal injury (laceration, abrasion, ulcer).
• LI (L, A, or U): lingual injury (laceration, abrasion, ulcer).
• PD: periodontal disease, stage 1–4.
• PP: periodontal pocket, a depth in mm can be assigned.
• INF/CA-infundibular caries, grade 1–5.
• 506X, 606X, etc. (cap extraction or retained deciduous tooth removal).
• 105X (wolf tooth extraction).
• OD: odontoplasty (reduction of excessive crown from occlusal surface).
• FTL: float (reduction of lingual and buccal enamel points).
• BS: bit seat (rounding the rostral margins of 2nd premolars).
• I/OD: incisor odontoplasty: incisor crown reduction.
• TI: ‘tooth impacted’, ‘blind’ (not completely erupted and completely or partially covered by bone or soft tissue).
Other shorthand systems have been used to grade or stage dental lesions.
Periodontal Disease Index adapted for equine anatomy57
1. Local gingivitis with hyperemia and edema: no attachment loss (probing depth, less than 5 mm)
2. Early periodontal disease (less than 25% attachment loss)
3. Moderate periodontal disease (less than 50% attachment loss or bone loss)
4. Advanced periodontal disease (more than 50% attachment loss or bone loss)
Tooth Mobility Index57
Grading of infundibular caries3
Grade 1 – Caries of the infundibular cementum
Grade 2 – Caries of infundibular cementum and surrounding enamel
Grade 3 – Caries of infundibular cementum, enamel, and dentin
This system is used on the sample dental charts provided. A dental chart can be used to record the examination, assessment, and pathology. A second diagram can be used to denote the specific treatment and post-treatment result or a single diagram can be used as a combined report form.
Summary
The basis for a complete equine dental examination is the development of a routine treatment plan that is used on each patient. By utilizing proper restraint techniques and equipment, a thorough examination can be performed with minimal stress to the horse and risk of injury to the veterinarian. Finally, a complete written record of the dental examination, findings, treatment plan, and follow-up recommendations is essential for the long-term management of equine oral health. For a visual demonstration of the oral examinations, view the accompanying DVD.
Acknowledgments
Author wishes to thank veterinarians Oliver Liyou, Ed Early, Robert Baratt, and Shelby Life editor, James Mulcahy, for their photo contributions to this chapter.
1 Kirkland K, Marretta SM, Inoue OJ, Baker GJ. Survey of equine dental disease and associated oral pathology. Proc Am Assoc Eq Pract. 1994;40:119–120.
2 Baker GJ. Some aspects of equine dental disease. Equine Vet J. 1997;2:105.
3 Baker GJ. A study of equine dental disease. PhD Thesis, University of Glasgow, 1979, pp 78–82
4 Wafa NS. A study of dental disease in the horse. MVM Thesis. National University of Ireland, University College, Dublin, 1988, pp 1–188
5 du Toit N, Gallager J, Burden FA, Dixon PM. Post mortem survey of dental disorders in 349 donkeys from an aged population (2005–2006). Part 1: Prevalence of specific dental disorders. Equine Vet J. 2008;40:204–209.
6 Greene S, Basile T. Recognition and treatment of equine periodontal disease. Proceedings of the 48th Annual Convention of the American Association of Equine Practitioners 2002: 463–466
7 Uhlinger C. Survey of selected dental abnormalities in 233 horses. Proceedings of the 33rd Annual Convention of the American Association of Equine Practitioners 1987, pp 577–583
8 Knottenbelt DC. The systemic effects of dental disease. In: Baker GJ, Easley J. Equine dentistry. 1st edn. London: WB Saunders; 1999:127–138.
9 Baker GJ. Dental physical examination. Veterinary Clinics of North America, Equine Practice, 1998; August, 247–257
10 DeBowes J, Mosier D, Logan E, et al. Association of periodontal disease and histologic lesions in multiple organs in 45 dogs. J Vet Dent. 1990;13:57–60.
11 Verdegaal E JMM, DeHeer N, Meertens NM, et al. A right-sided bacterial endocarditis of dental origin in a horse. Equine Vet Educ. 2008:245–250.
12 Tamzil Y. Chronic weight loss syndrome in the horse: a 60 case retrospective study. Equine Vet Edu. 2006:372–378.
13 Pavlica Z, Petelin M, Juntes P, et al. Periodontal disease burden and pathological changes in organs of dogs. J Vet Dent. 2008;25:97–105.
14 duToit N, Burden FA, Dixon PM. Clinical dental examinations of 357 donkeys in the UK: part 2, Epidemological studies on the potential relationships between different dental disorders, and between dental diseases and systemic disorders. Equine Vet J. 2009;41(4):395–400.
15 Earley ET. Creating a dental form for interactive use in the field. Proc Am Assoc Eq Pract. 2002;48:453–457.
16 Geiche JM. How to assess equine oral health. Am Assoc Eq Pract Proceedings. 2007;53:498–503.
17 duToit N, Burden FA, Dixon PM. Clinical dental examination of 357 donkeys in the UK: part 1, Prevalence of dental disorders. Equine Vet J. 2009;41(4):390–394.
18 Ohnesorge VB, Deegon E, Jochle W. Berl munch tierarztl wochensche. 1991;104:340–346.
19 Luukanen L, Katila T, Koskinen E. Some effects of multiple administration of detomadine during the last trimester of equine pregnancy. Equine Vet J. 1997;5:400–402.
20 Anderson MEC, Weese JS. Review of methacillin-resistant Staphylococcus aureus in horses and veterinary personnel who work with horses. Am Assoc of Eq Pract Proceedings. 2008;54:301–304.
21 Henneke DR. A condition score system for horses. Eq Pract. 1985;7:13–15.
22 Carmalt JL, Allen A. The relationship between cheek tooth occlusal morphology, apparent digestibility and ingesta particle size. Am Assoc Eq Pract Proceedings. 2008;54:386–389.
23 May KJ, Relationship between acupuncture, chiropractic, and dentistry. Large Animal, Equine N Am Vet Conf, Orlando, 2008, 141–144
24 Centers for Disease Control and Prevention: Humane rabies prevention-United States (1999) Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morbidity, Mortality Weekly, 1999, 48 (No RR-1)
25 DeLorey MS. A retrospective evaluation of 204 diagonal incisor malocclusion corrections in the horse. J Vet Dent. 2007;24:145–149.
26 Walmsley JP. Dental aging in horses between five and seven years of age. Equine Vet Edu. 1993:5.
27 Richardson JD, Lane JF, Waldron KR. Is dentition an accurate indication of age in the horse? Vet Record. 1994;135(2):31–34.
28 Richardson JD, Cripps PJ, Lane JG. An evaluation of the accuracy of ageing horses by their dentition. Vet Record. 1995;137(5):117–121.
29 Muylle S, Simoens P, Lauwers H. Aging horses by an examination of their incisor teeth: an (im)possible task. Vet Record. 1996;138(13):295.
30 Allen T. Examination. In: Allen T, ed. Manual of equine dentistry. St Louis: Mosby; 2003:49–53.
31 Carmalt JL, Townsend HGG, Allen AL. Effect of dental floating on the rostrocaudal mobility of the mandibles of horses. J Am Vet Med Assoc. 2003;223:666–669.
32 Rucker BA. Equine cheek teeth angle of occlusion: how to calculate and clinical use for incisor shortening. Equine Vet Edu. 2004:176–182.
33 Rucker BA, Excursion to molar contact. Am Assoc Eq Pract Dental Wet Lab Notes, Lexington, KY, 2008, pp 31–37
34 Rucker BA. Incisor procedures for field use. Am Assoc Eq Pract Proceedings. 1996;41:22.
35 Rucker BA. Utilizing cheek teeth angle of occlusion to determine length of incisor shortening. Am Assoc Eq Pract Proceedings. 2002;48:448–452.
36 Rucker BA, Incisor and molar occlusion: how to determine the cheek teeth angle of occlusion in clinical cases. Am Assoc Eq Pract Dental Wet Lab Notes, 2005, pp 1–10
37 Collinson M. Food processing and digestibility in horses. Victoria: BSc dissertation. Monash University; 1994. pp 36–42
38 Miles AEW, Grigeon C. Colyer’s variations and diseases of the teeth of animal (revised). Cambridge: Cambridge University Press; 1990. p. 121
39 Johnson TJ. Surgical removal of mandibular periostitis (bone spurs) caused by bit damage. Am Assoc Eq Pract Proceedings. 2002;48:458–462.
40 Stock S, Periodontal parameters in the normal and pathological equine tooth. World Equine Dental Congress Proceedings, 1997, pp 92–95
41 Dixon PM, Tremaine WH, Pickles K, et al. Equine dental disease part 2: a long term study of 400 cases: disorders of development and eruption and variations in position of cheek teeth. Equine Vet J. 1999;31:519–528.
42 van den Enden MSD, Dixon PM. Prevalence of small occlusal pulpar exposure in 110 equine cheek teeth with apical infections and idiopathic fractures. Vet J. 2008;178:364–371.
43 duToit N, Burden FA, Kempson SA, et al. Pathological investigation of caries and occlusal pulp exposure in donkey cheek teeth using computerized axial tomography with histology and ultrastructural examinations. Vet J. 2008;178:387–395.
44 Tremaine H. Equine endoscopy in the horse. Cl Tech in Eq Pract. 2005;4:181–187.
45 Goff C. A study to determine the advantages of oral endoscopy for the detection of dental pathology in the standing horse. Am Assoc Eq Pract Proceedings. 2006;52:266–268.
46 Easley J. How to perform and interpret an endoscopic examination of the equine oral cavity. Am Assoc Eq Pract Proceedings. 2008;54:383–385.
47 Simhofer H, Griss R, Zenter K. The use of oral endoscopy for detection of cheek teeth abnormalities in 300 horses. Vet J. 2008;178:396–404.
48 Barakzai SZ, Dixon PM. A study of open-mouthed oblique radiographic projections for evaluating lesions of the erupted (clinical) crown. Equine Vet Edu. 2003;5(3):183–188.
49 Freeman DE. Sinus disease. Vet Clinics N Am Eq Practice. 2003;19:209–243.
50 Ruggles AJ, Ross MW, Freeman DE. Endoscopic examination of normal paranasal sinuses in horses. Vet Surg. 1991;20:418–423.
51 Ruggles AJ, Ross MW, Freeman DE. Endoscopic examination and treatment of paranasal sinuses in 16 horses. Vet Surg. 1993;22:508–514.
52 Galloway S, Equine oral photography. Notes from Am Assoc Eq Pract Dental Wet Lab, 2008, Lexington, KY
53 Wiggs RB, Lobprise HB. Veterinary dentistry principles and practice. Philadelphia, New York: Lippincott-Raven; 1997. p. 96
54 Pence P. The dental examination. In: Pence P, ed. Equine dentistry: a practical guide. Lippincott. Philadelphia: Williams and Wilkins; 2002:53–78.
55 Floyd MR. The modified Triadan system: nomenclature for veterinary dentistry. J Vet Dent. 1991;4:18.
56 Foster DL, Nomenclature for equine dental anatomy based on the modified Triadan system. Proceedings, Annual Meeting of the International Association of Equine Dental Technicians, Detroit, 1993, p. 35
57 Klugh DO. Periodontal disease. In: Robinson EN, ed. Current Therapy in Equine Medicine 6. St Louis: Sprayberry KA. Saunders; 2009:328–334.