5 Diagnostic methods
In previous chapters we have dipped into the vast amount of information that exists in relation to the neuromuscular component of the human body.
A great many diagnostic aids exist for discovering just what is happening when aspects of this network of tissues malfunction. The great beauty of neuromuscular technique, as devised by Lief, is the way in which diagnostic and therapeutic processes are combined. The thumb, as it glides close to the spinal attachments of the paraspinal musculature, is assessing the tissue tone, density, temperature, etc., and at the same moment is capable of treating any tissues that display evidence of dysfunction (see discussion of STAR characteristics – sensitivity, tissue texture alteration, asymmetry, reduced range of motion – in Ch. 3). The response of the searching thumb or finger to whatever information the tissues impart can be immediate. The use of greater or lesser degrees of pressure, varying in direction and duration, allows the practitioner to judge and treat at the same time, and with great accuracy (Figs 5.1 & 5.2).
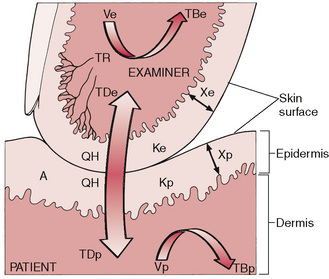
Figure 5.1 This diagram depicts some of the physical and physiological factors that affect the thermoreceptor (TR) discharge rate and consequently the temperature sensed in an examiner’s skin in contact with a patient’s skin. The temperature and rate of change of the examiner’s thermoreceptors are functions of the net effects of the time that the tissues are in contact, their contact area (A), the temperatures (TBe and TBp) and volume flow rates (Ve and Vp) of blood perfusing the examiner’s and patient’s skin, epidermal thickness (Xe and Xp) and thermal conductivity (Ke and Kp) of both, dermal temperature (TDe and TDp) of both, as well as of the net heat exchange rate (QH) between the two tissues. QH is strongly affected by the heat transfer properties of material trapped between the two skin surfaces, for example air, water, oil, grease, hand lotion, dirt, tissue debris and fabric (Adams, Steinmetz, Heisey, Holmes & Greenman 1982).

Figure 5.2 Light ‘skin on skin’ palpation can give indications of deeper dysfunction due to modification of sympathetic and circulatory activity.
If treatment of musculoskeletal dysfunction is to be focused and meaningful, a diagnostic or assessment plan is required. Whilst local muscular changes will become more apparent as treatment progresses, an overall diagnostic picture is required to enable a coherent plan to emerge and for prognosis and progress to be judged.
Neuromuscular technique – assessment and diagnosis
If therapeutic intervention is to be structured and organized – and something other than hit and miss – there is a basic need for evaluation and assessment of the way in which the mechanical component of the body is adapting to its current situation, of the extent of changes from the norm, and of the ways in which patterns of pain, malcoordination and restriction are interacting. These changes might involve reflexively active structures such as myofascial trigger points, locally traumatized areas, fibrotic alterations, shortened and/or weakened muscles, joint restrictions and/or general or systemic factors (such as exist in arthritic conditions).
NMT provides a diagnostic/assessment tool and also offers, when it switches from assessment to actively therapeutic mode, a means whereby precisely focused and modulated degrees of force can be directed towards influencing restricted tissues. Myofascial release techniques, as well as ischaemic compression (osteopathic inhibitory technique), can be applied to precise targets via the contacting thumb or finger in NMT. Perhaps NMT’s greatest usefulness in assessment relates to the opportunity it offers for the identification of local soft tissue dysfunction in a gentle non-invasive manner. In the USA, as well as in the UK, the focus of many therapists utilizing NMT in recent years has been towards the identification and treatment of myofascial trigger points (and the often widespread musculoskeletal dysfunction that produces or is associated with them).
Palpation
There is no valid substitute for skilful palpatory diagnosis in ascertaining the relatively minute structural changes – primary or reflex – that often have far-reaching effects on the body’s economy.
It is generally agreed that the pads of the fingers are the most sensitive portion of the hand available for use in diagnosis. Indeed, the combination of the thumb and first two fingers is the finest mechanism, and can be adapted to conform with the variable areas under palpatory consideration.
Palpatory diagnosis
Skin assessment before adding lubricant
One of the most successful methods of palpatory diagnosis is to run the pads of a finger or several fingers extremely lightly over the (unlubricated) area being assessed, feeling for changes in the skin texture that may indicate alterations in the tissues below. After localizing any changes in this way, deeper periaxial structures can be evaluated by means of the application of greater pressure. There are a number of specific changes to be sought in light palpatory examination in both acute and chronic dysfunction.
Skin changes (Lewit 1992)
Over an area of acute or chronic dysfunction, skin will feel tense, and will be relatively difficult to move or glide over the underlying structures. The skin above reflexively active structures will therefore be more adherent to the underlying fascia, something that will be evident in any attempt to glide or roll it, compared with skin covering normal areas. By applying a series of bilateral ‘pushes’ of skin on fascia, assessment is possible for asymmetry of movement.
 The skin overlying reflexively active areas such as trigger points (or active acupuncture points) tends to produce a sensation of ‘drag’ as it is lightly stroked, because of increased hydrosis. There is also an apparent – very slight – sensation of undulation, a rising and falling, palpable on a light stroke, described illustratively as ‘hills and valleys’.
The skin overlying reflexively active areas such as trigger points (or active acupuncture points) tends to produce a sensation of ‘drag’ as it is lightly stroked, because of increased hydrosis. There is also an apparent – very slight – sensation of undulation, a rising and falling, palpable on a light stroke, described illustratively as ‘hills and valleys’.
Over areas of reflexogenically induced dysfunction, the skin will also lose its fully elastic quality, so that on light stretching (taking an area of skin to its easy resistance barrier on stretching) it will test as less elastic than neighbouring skin.
Methods for assessing these skin changes are described in more detail later in this chapter.
Assessment after adding lubricant
Dysfunctional patterns revealed by means of assessment of skin changes should become apparent in the application of neuromuscular palpation/assessment strokes, as described in detail in Chapters 6 & 7.
Induration
A slight increase in diagnostic pressure will show whether or not the superficial musculature has an increased indurated feeling (‘dense’, ‘firm’, less elastic). When chronic dysfunction exists, the superficial musculature will demonstrate a tension and immobility, indicating fibrotic changes within and below these structures. These changes are discussed further in the text dealing with the application of basic spinal and abdominal NMT (Chapters 6 & 7).
Temperature changes
In acute dysfunction, a localized increase in temperature may be evident. In chronic lesion conditions there may, because of relative ischaemia, be a reduced temperature of the tissues. This usually indicates that fibrotic changes have occurred.
Tenderness
Tenderness requires investigation. Is the tissue inflamed? Is the local area reflexively active? What is the nature and cause of the tenderness?
Key questions
The questions that need to be asked when palpation elicits the sort of changes briefly outlined above, include:
Deeper palpation: Peter Lief’s perspective
In deeper NMT palpation, the pressure of the palpating fingers or thumb needs to increase sufficiently to make contact with structures such as the periaxial (paravertebral) musculature, without provoking a defensive response. The changes that might be noted could include immobility/rigidity, tenderness, oedema, deep muscle tension, fibrotic and interosseous changes. Apart from the fibrotic changes, that are characteristic of chronic dysfunction, all these changes can be found in either acute or chronic problems.
As Peter Lief (1963), son of the innovator of NMT, explains:
Palpation is the main method of detection. Gross lesions are easily palpable, but sometimes they are so minute that their detection presents considerable difficulty, especially to the beginner. It sometimes takes many months of practice to develop the necessary sense of touch, which must be firm, yet at the same time sufficiently light, in order to discern the minute tissue changes that constitute the palpable neuromuscular lesion.
The presence of a lesion is always revealed by an area of hypersensitivity to pressure, an area which may be better described as being ‘a painful spot’. After these have been detected and noted, specific attention is given to them in the subsequent treatments.
Note: the word ‘lesion’ as used by Lief and Youngs (see below) refers to what is now described as ‘somatic dysfunction’.
Youngs’ NMT description: tissue changes and objectives
Youngs (1964) has described what it is that the palpating fingers are seeking and finding and, as in NMT diagnosis and treatment often take place together, what they are achieving:
The changes which are palpable in muscles and soft tissues associated with reflex effects have been listed by Stanley Lief. They are essentially ‘congestion’. This ambiguous word can be interpreted as a past hypertrophic fibrosis. Reflex cordant contraction of the muscle reduces the blood flow through the muscular tissue and in such relatively anoxic regions of low pH and low hormonal concentration, fibroblasts proliferate and increased fibrous tissue is formed. This results in an increase in the thickness of the existing connective tissue partitions – the epimysia and perimysia, and also this condition probably infiltrates deeper between the muscle fibres to affect the normal endomysia. Thickening of the fascia and subdermal connective tissue will also occur if these structures are similarly affected by a reduced blood flow. Fat may be deposited, particularly in endomorphic types, but fibrosis is most pronounced in those with a strong mesomorphic component – a useful pointer for both prognosis and prophylaxis.
Fibrosis seems to occur automatically in areas of reduced blood flow, e.g., in a sprained ankle – where swelling is marked and prolonged, in the lower extremities where oedema of any origin has been constant over a period, in the gluteals where prolonged sitting is a postural factor, and in the neck and upper dorsal region where psychosomatic tension is frequent to a marked degree – depending upon the constitutional background. Where tension is the aetiological factor, fibrosis seems teleological.
Many devices have been developed to ease the strain on muscles which tend to be permanently contracted, e.g., locking of the knee joint, or the exact balance of the head on the shoulders, where only gentle contraction is needed to maintain postural integrity. If postural integrity is lost through some cause or another, then the strain on the muscle may be eased by structural alteration and the increase of fibrous tissue in the muscles acts to maintain normal position of the head. Fibrous tissue can then take the strain instead of the muscle fibres. It is this long-term homeostatic reflex which apparently operates in all cases of undue muscle contraction, whether due to strain or tension.
From this one can amplify Stanley Lief’s beneficial effects of neuromuscular treatment as follows:
1. To restore muscular balance and tone.
2. To restore normal trophicity in muscular and connective tissues by altering the histological picture from a patho-histological to a physiologic–histological pattern with normal vascular and hormonal response.
3. To affect reflexively the related organs and viscera and to tonify them naturally.
4. To improve drainage of blood and lymph through the areas subject to gravitational or postural stasis, e.g., abdominal vessels not necessarily connected with viscera.
Thus the hyperaemia, resulting from [NMT] treatment automatically operates to reverse the original patho-histological picture and consequently normality will be approached.
Trigger points
In clinical terms it is safe to say that a chronic state of dysfunction exists if soft tissues have been consistently stressed for more than a few weeks, for after such a short period fibrotic adaptations begin to be palpable.
There is clinical evidence that trigger points have a consistent distribution, and their localization can be predicted by studying the patterns of referred dysfunction and pain to which they give rise. Similarly patterns of referred pain are predictable if the trigger point can be located (Travell 1957, Travell & Simons 1992).
A patient with unexplained pain, the examination of which reveals no local cause, may well have trigger points feeding pain messages into the target area. Thus the point at which the patient feels pain, and the point at which the pain originates, are often not the same, and knowledge of the reference patterns as illustrated in Chapter 3 (see Fig. 3.6) is therefore important.
Whether treatment of trigger points consists of anaesthetic injections, acupuncture, cryotherapy, or pressure and stretch techniques (NMT), or combinations such as INIT (see Ch. 9), the diagnostic aspect remains the same. Deep palpation and pressure on the located point must reproduce the symptoms in the target area in order to ‘prove’ the connection.
Zones of dysfunction: connective tissue changes
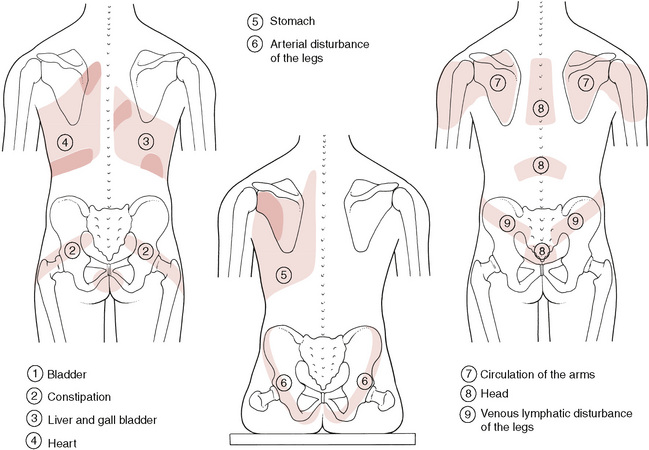
As well as trigger points there exist a number of palpable and often visible (Box 5.1) zones of soft tissue alteration, possibly involving viscerosomatic activity, in which diseased or stressed organs negatively influence soft tissues paraspinally and elsewhere (Bischof & Elmiger 1960). Viscerosomatic reflexes and the processes of facilitation (sensitization) were discussed in Chapter 3. Some of these zones overlap and incorporate ‘trigger’ points, so a general awareness and knowledge of their existence is useful if an understanding of what can be achieved in NMT is to be more complete (Fig. 5.3).
Box 5.1 Assessing the dominant eye
In making a visual diagnosis it is important for the practitioner/therapist to be sure of the information he or she is acquiring. American osteopathic physician Edward Stiles (1984) made a valuable contribution to this area by pointing out that it is often for reasons of position, in observing structure, that a student or practitioner fails to see what is obvious:
By being so positioned as to bring into play the non-dominant eye this becomes far more likely. The orientation of the subject in the field of view is determined by the position of the dominant eye, and thus it is essential to initially ascertain which eye this is.
Hold your hands straight in front of you with the palms facing each other. Bring them together to make an aperture (gap) of about 1–2 inches across. Looking through this aperture, focus on an object across the room from you. Close first one eye and then the other. When the non-dominant eye is closed the image you see through the aperture will not change. When you close the dominant eye the image shifts out of the field of vision.
The dominant eye is not always on the same side as the dominant hand. If dominant hands and eyes are on different sides, this can lead to problems of accurately assessing palpatory findings, and the advice given is to palpate with eyes closed, where possible, in such cases.
When assessing visually, make sure that the dominant eye is lined up with the area or object being viewed. In an example where assessment of the chest is being made, Stiles suggested that, because most accurate visual information would be gained when the dominant eye was over the midline, the observation of the supine patient should be from the head of the table, and that this should be approached from the side that brings the dominant eye closest to the patient.
As organs mainly receive their autonomic supply homolaterally, changes of a reflex nature will normally be found on the same side of the body surface:
• On the right side will be found the connective tissue reflex zones from the liver, gall bladder, duodenum, appendix, ascending colon, ilium, etc.
• On the left side will be found the reflex zones from the heart, stomach, pancreas, spleen, jejunum, transverse colon, descending colon, rectum, etc.
• Central zones occur as a result of dysfunction in the bladder, uterus and head.
• Changes on the homolateral side of the body occur due to dysfunction of the lungs, suprarenal glands, ovaries, kidneys, blood vessels and nerves on that side.
According to Teiriche-Leube & Ebner (quoted in Teiriche-Laube 1960), these changes in the connective tissue and muscles can take the following forms:
For Teiriche-Leube & Ebner’s description of some of these zones, see Box 5.2.
Box 5.2 Altered connective tissue zones resulting from disturbed organs and functions
1 Bladder
Small ‘drawn in’ area above anal cleft. Iliotibial tract may be drawn in. Swelling lateral aspect of ankles.
Symptoms – Bladder dysfunction. Cold feet and legs (below the knee). Rheumatic diagnosis.
2 Constipation
‘Drawn in’ band 2–3 inches (5–8cm) wide, running from middle third of the sacrum downwards and laterally.
3 Liver and gall bladder
Large ‘drawn in’ zone over right thoracic region and a band along lateral costal border on the right side. Small ‘drawn in’ area between lower vertebral border of scapula to spine at the 5th and 6th dorsal level. 7th cervical area appears swollen or congested.
Symptoms – Liver and gall bladder dysfunction and anyone who has suffered from hepatitis.
4 Heart
Tension over left thoracic region including lower costal margin. If hepatic circulation is involved, right costal margin will also be affected. The area between the left scapula and 2nd and 3rd dorsal vertebrae will be indurated. Posterior aspect of axilla appears thickened.
6 Arterial disease of legs
A V-shaped configuration of the buttocks is noticed when sitting, rather than the normal rounded shape.
Symptoms – Circulatory disturbance accompanied by angiospasm.
7 Arms
‘Drawn in’ areas over scapula extending over posterior deltoid.
Symptoms – Circulatory arm and hand problems. Neuritis paraesthesia.
Using NMT in its assessment mode, as described in Chapters 6 & 7, or in specialized skin diagnosis (see below), these and other areas of soft tissue dysfunction can be readily located, identified and treated, even if no obvious symptoms of the associated conditions or diseases are present. It is clear that soft tissue changes often precede the appearance of symptoms of underlying pathology, and in this alone the diagnostic value of these zones is evident.
Practitioners using German connective tissue massage/manipulation (CTM) claim that it is often possible to beneficially influence symptoms of organ dysfunction, and to improve the function of these organs (liver, stomach, etc.), by treatment of the congested fibrotic reflex zone. This is not, however, to be considered an end in itself because it is clear that underlying causative factors and pathology (nutrition, infection, etc.) should also be dealt with. However, the value of this neuromuscular modality should not be underestimated.
Mackenzie’s abdominal reflex areas
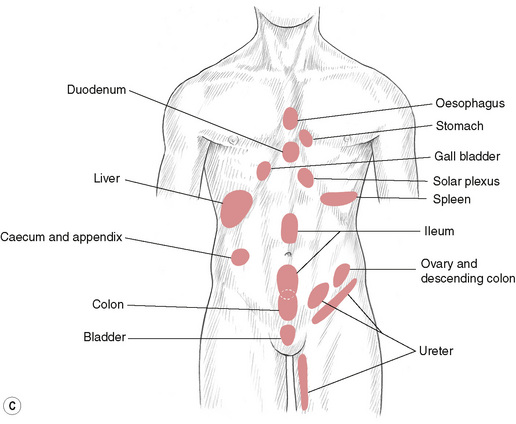
Youngs (1964) points out that Sir James Mackenzie established a clear relationship between the abdominal wall and the internal abdominal organs (Mackenzie 1909). Mackenzie showed that organs that cannot react directly to painful stimuli (i.e. the majority) react by producing spasm and paraesthesia in the reflexively related muscle wall (the myotome), often augmented by hyperaesthesia of the overlying skin (dermatome) (see Figures 5.4A, B, C).
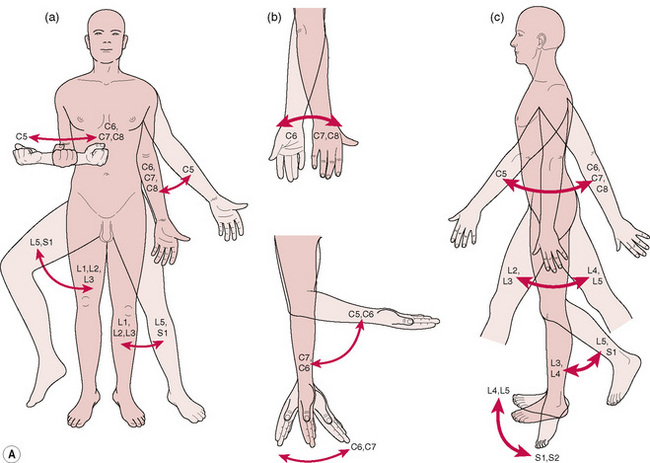
Figure 5.4A Reflex myotomes: These examples show which spinal nerves innervate the skeletal muscles that produce the movements indicated by the arrows. A, Rotation and abduction/adduction of the arm and hip. B, Flexion/extension of the hand and wrist; pronation/supination of the hand. C, Flexion/extension/hyperextension of the arm, hip, and knee; dorsiflexion and plantar flexion of the foot. C, Cervical spinal nerves; L, lumbar spinal nerves; S, sacral spinal nerves; T, thoracic spinal nerves.
(From Thibodeau GA, Patton KT: Anatomy and Physiology, ed 5, St Louis, 2003, Mosby.)
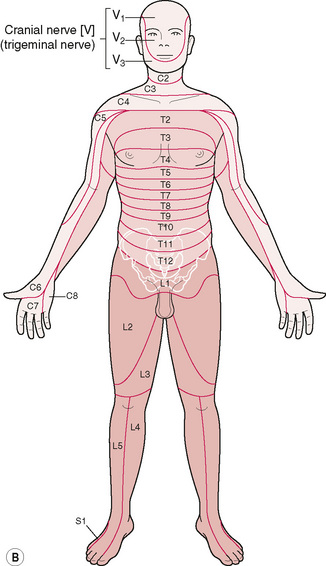
Figure 5.4B Anterior view of Dermatomes. Relating to the relationship between the spinal nerve & skin.
The reflexes involved occur via the autonomic nervous system and may be viscerosomatic or – as has been shown by many researchers, including Lief – the origin may be somatic and the reflex, therefore, somaticovisceral.
Mackenzie’s abdominal reflex areas are as illustrated in Fig. 5.4C and, although there is sometimes a degree of individualization, it is reasonable to state that the presence in abdominal muscles and connective tissues of contracted or sensitive areas indicates (in the absence of recent trauma or strain) some underlying dysfunction that is causing or resulting from the soft tissue lesion. (See also discussion in Chapter 7 of Pain variables in somatic abdominal tissues.)
Skin: reflex effects and hyperalgesic skin zones
The work of Mackenzie early in the 20th century, as well as research into connective tissue zones evolving out of Bindegewebsmassage in Germany, demonstrates that the surface of the body offers evidence of internal dysfunction (see Fig. 5.4C), and that it is possible to influence the interior by application of reflexively powerful stimuli from the surface.
Koizumi (1978) found that stimulation of the skin of the abdomen produced profound inhibition of intestinal movement. Stimulation of the skin produces an increase in sympathetic activity associated with the intestine, thereby inhibiting peristalsis. Koizumi noted that this was a strong effect, and that the intestine often became completely quiescent.
Stimulation of other skin areas, notably the neck, chest, forelimbs and hindlimbs, inhibited sympathetic activity, and therefore actually augmented intestinal motility. Vagal involvement in these changes was thought to be minimal, for when the vagi were sectioned the same responses were still noted. Reflexes disappeared, however, when the sympathetic nerve supply to the intestine (the splanchnic nerves) was sectioned. If we consider the involvement of these mechanisms in affecting internal function, via stimulus applied to the skin, we may better appreciate the findings of Chapman (Owen 1980), Bennett (Arbuckle 1977) and others, in their work on the multitude of reflex areas, that they have so painstakingly charted, and which are discussed later in this chapter.
The sometimes dramatic effects obtained by the use of CTM (see previous chapter) can also be seen to relate to the patterns of therapeutic and diagnostic opportunities that this knowledge offers. For example, various techniques are available to us in diagnosing from, and treating, the cutaneous structures for reflex effect. These include skin rolling, as well as the delicate ‘skin distraction’ or stretching method, advocated by Lewit (1992, 1999). Lewit discusses hyperalgesic skin zones that are likely to be present in the skin overlying most areas of reflex activity. He points out a major advantage afforded by an awareness of hyperalgesic skin zones (HSZs): unlike the eliciting and mapping of areas, points or zones, which rely upon the subjective reporting of the patient, these areas are palpable to the operator.
A popular method of identifying relative tension in skin is to ‘roll’ it.
A fold of skin is formed, and this is rolled between the fingers (see Fig. 8.17). This method may produce some discomfort, or even transient pain (a sharp ‘cutting’ sensation is often reported), but is useful in that the increased tension, and visibly thicker skin fold thus produced (compared with surrounding tissues) can then be diagnostic of a HSZ.
Lifting skin folds (assessment)
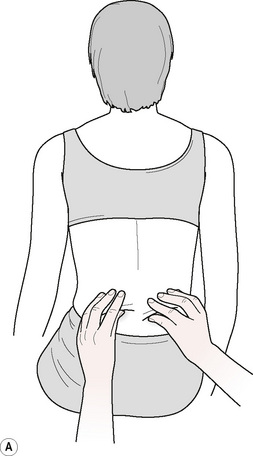
The assessment methods used in CTM are designed to obtain a picture of the mobility of the various layers of the connective tissue, as well as an idea of their consistency. One such method involves the lifting of skin folds, with the patient sitting. The skin is gripped between thumb and fingers, with care being taken not to pinch the fold (Fig. 5.5). The fold comprises sufficient tissue to allow it to be lifted away from the fascial layer. This is usually performed by starting at the lower costal margin and going up as far as the region of the shoulders. In some areas, especially overlying the mid-dorsal region, if there is any dysfunction involving the liver, gall bladder, stomach or heart, restriction of tissue elasticity will be noted. By lifting two folds simultaneously, right and left, it is possible to compare the relative freedom of these tissues.

Stretching superficial tissue (assessment)
A second method may be used, in which relatively smaller areas are assessed, with the patient prone or seated.
• With fingers lightly flexed, and using only enough pressure to produce adherence between the fingertips and the skin, a series of short pushing motions are made simultaneously with both hands, which stretches the tissues to their elastic barrier (Fig. 5.6).
• Usually the pattern of testing goes from inferior to superior, sometimes in an obliquely diagonal direction towards the spine.
• If the patient is seated and the operator works from behind, tissues from the buttocks to the shoulders may be tested, always comparing the sides for symmetry of range of movement to the elastic barrier.
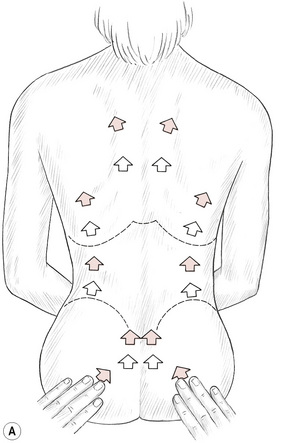
Figure 5.6A Testing and comparing skin and fascial mobility as bilateral areas are ‘pushed’ to their elastic barriers.
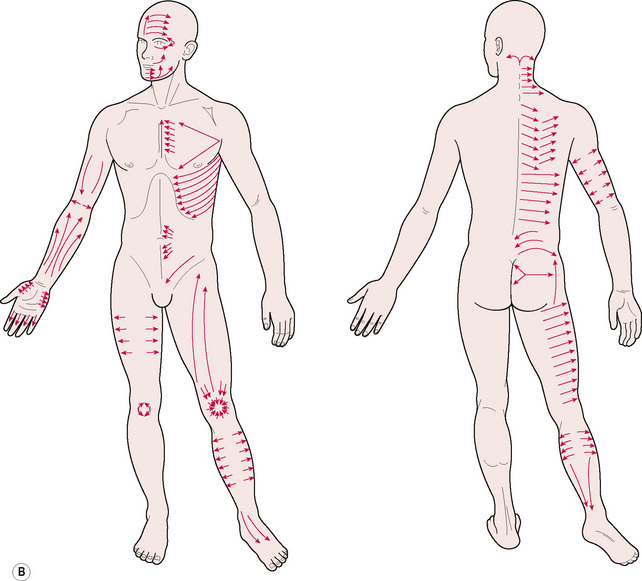
Figure 5.6B These lines indicate directions of application of CTM using tension, shear, bending and torsion forces, in assessment and treatment. Restricted mobility of superficial tissue-on-fascia will be evident when dysfunction exists, giving similar feedback to that noted in use of the ‘pushing’ methods illustrated in Figure 5.6A, and skin rolling approaches described above and illustrated in Figure 8.17.
Two quite different evaluations can be performed simultaneously:
1. Becoming aware of asymmetry and noting areas of interest for more refined assessment, wherever skin does not slide as easily on the underlying tissue on one side, compared with the other
2. Additionally and alternatively, the possible organ or system reflexes may be noted, if that is of interest to the therapist (see Box 5.1).
Areas investigated, direction of stretch of tissues, and possible implications of reduced elasticity include:
1. The buttocks – stretching tissue from the ischial region towards the lateral borders of the sacrum (arterial and constipation zone).
2. From the posterior aspect of the trochanters, towards the iliac crests (venous lymphatic and arterial disturbances of legs).
3. From the trochanters, towards sacroiliac joints (venous lymphatic zone).
4. Over the sacrum, working from the apex towards the upper sacral segments (bladder and headache zones).
5. Over the lumbar region, on either side of the spine, working upwards (kidney zone).
6. Bilaterally up the spine, from lower costal region to the mid-thoracic level (liver and gall bladder zone (right side), and heart, stomach (left) and pulmonary (bilateral)).
7. Between the scapulae (headache zone).
8. Over the scapulae, from inferior angle, towards spine of scapula (arm zone).
Normal variations will exist independent of reflex activity, and in individuals carrying increased adipose tissue a generally greater degree of tension or adherence will be noted, compared with a thinner individual.
An older person’s skin will feel looser, in comparison with that of a younger individual. The skin over the lumbar region is naturally less mobile than that in other regions.
Note that it is adherence (‘tightness of tissues to each other’) that is being assessed, and this may or may not be accompanied by sensitivity. In connective tissue massage assessment of this sort is made regularly, as it is seen to be both diagnostic and prognostic, showing the rate of progress or lack of it, and providing a possible insight into visceral and functional status.
Skin distraction (diagnostic and therapeutic)
Lewit (1992) describes a method that he finds reliable, painless and therapeutically very useful. Any area of skin may be assessed in this way, large or small, with fingertip or hand contact.
In a small area, the fingertips (both index fingers) or index and middle fingertips of both hands, are placed close together, resting on the tissues to be tested. By separating the fingers, the skin is pulled apart and stretched to its easy elastic barrier (Fig. 5.7).
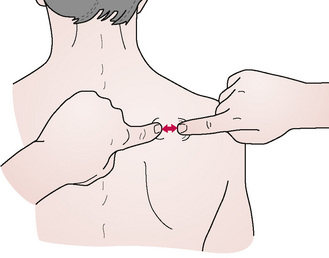
Figure 5.7 Hyperalgesic skin zones that lie above reflexive dysfunction (e.g. trigger points) are identified by means of the sequential stretching to their elastic barrier of local areas of skin. A series of such stretches indicates precisely those areas where elasticity is reduced in comparison to surrounding tissues. These are then tested for sensitivity and potential to cause referred pain by the application of ischaemic compression (inhibition).
A minimum of force is used, in order simply to take out the slack in the skin. The ‘easy’ end-position is noted, as is the degree of ‘springing’ available in the tissues. This is compared in several directions, over the area being assessed, and comparison is also made with the presumably healthy tissue on the contralateral side.
If a hyperalgesic skin zone (HSZ) is present, then a greater degree of resistance will be noted after the slack has been taken up. Where there is such resistance, if the end-position of stretch is held for between 10 and 20 seconds, the resistance will be felt to ease, and the normal physiological degree of springing will then be noted. This is a measurable phenomenon and, by marking the first stretch position with a skin pencil and marking the stretch position available after ‘release of the tissue’, a significant increase is usually noted.
The techniques may be used for even small areas (e.g. between the toes). These may be stretched by fingertip (light) pressure and separation. Larger areas, such as regions of the back, may be contacted by the ulnar border of the hands in order to introduce separation stretch. The hands are crossed and placed on the tissue to be tested or treated. Separation of the hands introduces stretch to take up the slack. (See Figs 8.20A and 8.20B.)
Having introduced this initial degree of stretch, resistance (end-feel) is then noted. If the tissues are resistant to stretch, and springiness is absent, the maintenance of the stretch (painless) achieves a release of the tissues over a period of less than half a minute as a rule.
All trigger points, tender points, connective tissue zones, Mackenzie’s abdominal areas, etc. are characterized by the presence of such a HSZ in the overlying tissues. This very useful tool allows easy identification of reflex activity and is itself an ideal form of treatment of these reflexes in sensitive individuals, and further provides accurate evidence of the subsequent situation. Techniques for treating skin and superficial tissue are further discussed in Chapter 8.
Scar tissue often leads to the presence of HSZs around the scar, and these frequently become focal points of reflex activity. Specific release methods, as described in Chapter 8, may be used to alter the status of tissues affected by scar tissue (Lewit & Olšanská 2004). Acupuncture can also be a useful method of treating very sensitive aspects of the scars themselves (Baldrey 1993).
Chapman’s reflexes in diagnosis and treatment
The reflexes described by Chapman are now commonly termed ‘neurolymphatic’ reflexes. These can be used in diagnosis and treatment, and as a guide to the effectiveness of treatment. See additional discussion of these reflexes in Chapter 4.
In 1965 I described the technique for using these as follows (Chaitow 1965):
Treatment applied through these reflexes, as advocated by Chapman and Owens, consists of a firm but gentle rotary pressure imparted by the index or middle finger. The finger should not be allowed to slip. As these areas are acutely sensitive great care should be taken not to overtreat as the reflex will become fatigued and no benefit will be derived.
My current view coincides with the above method except that I now use a variable thumb pressure that fits in with the general neuromuscular technique. Knowledge of the exact location of the reflexes is of primary importance.
Methodology
• By gentle palpation, the practitioner/therapist should first ascertain the presence of involved reflexes. (See Table 5.1 and Figs 5.8A-F.)
• The anterior reflexes should be tested first.
• If found to be present, the anterior reflex should be treated first, then the posterior counterpart of the involved anterior reflexes should be treated.
• The anterior reflex has, therefore, a dual role: namely, for assessment, and then to initiate the reflex treatment.
• The anterior reflex is later of value to ascertain the effectiveness of treatment (after both anterior and posterior reflexes have been treated).
• If, on re-palpating the reflexes, there is no change in the feel or tenderness, the treatment should be repeated.
• If there is again no change, this indicates either that the pathology is too great for rapid change, or that pathology is irreversible.
• It may also indicate that some musculoskeletal factor is maintaining the reflex.
• Primary treatment should then be directed at this factor rather than the reflex.
• The degree of treatment should be ascertained by palpation.
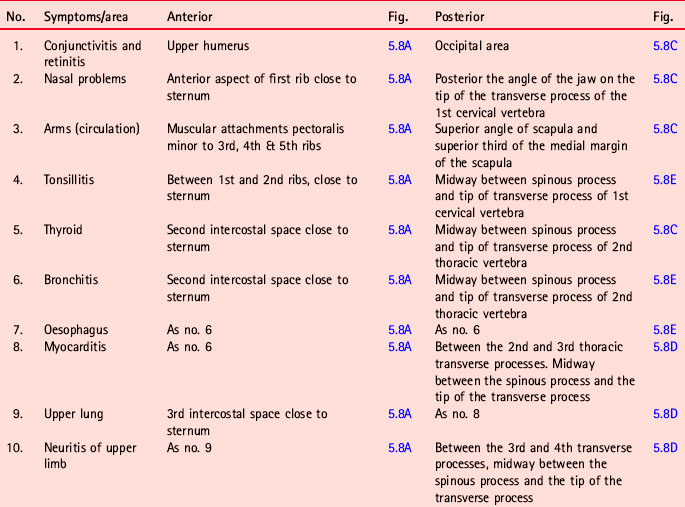
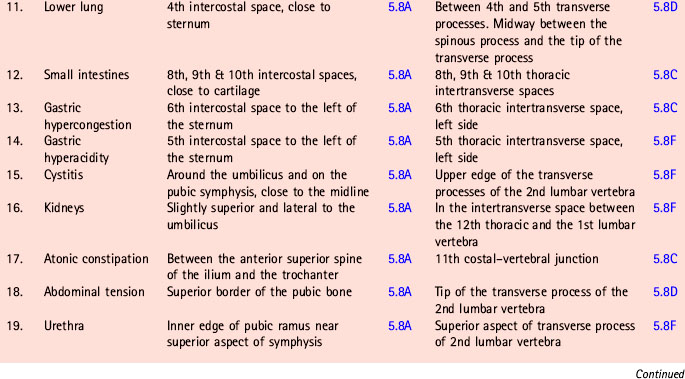
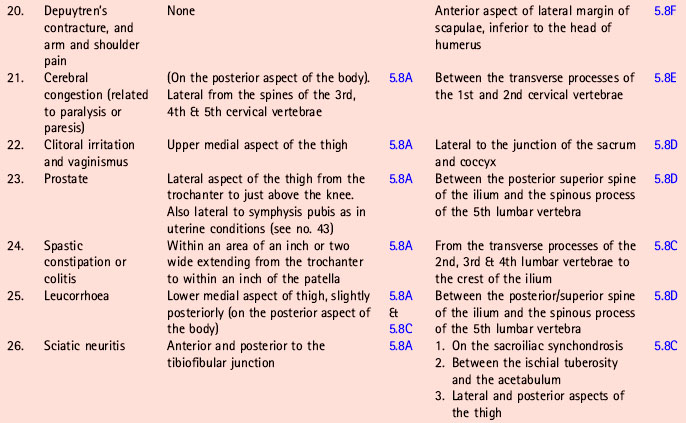
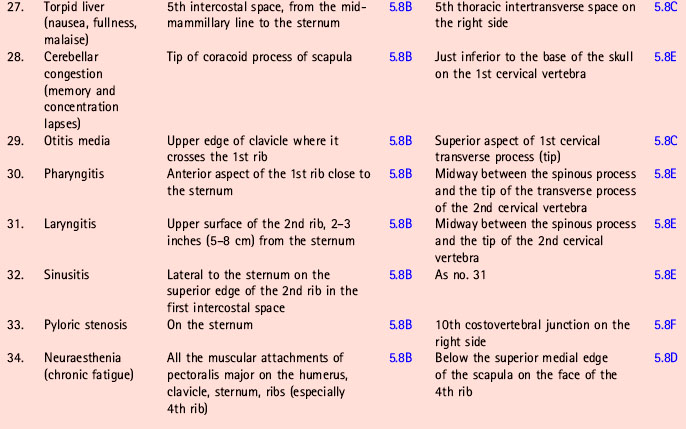
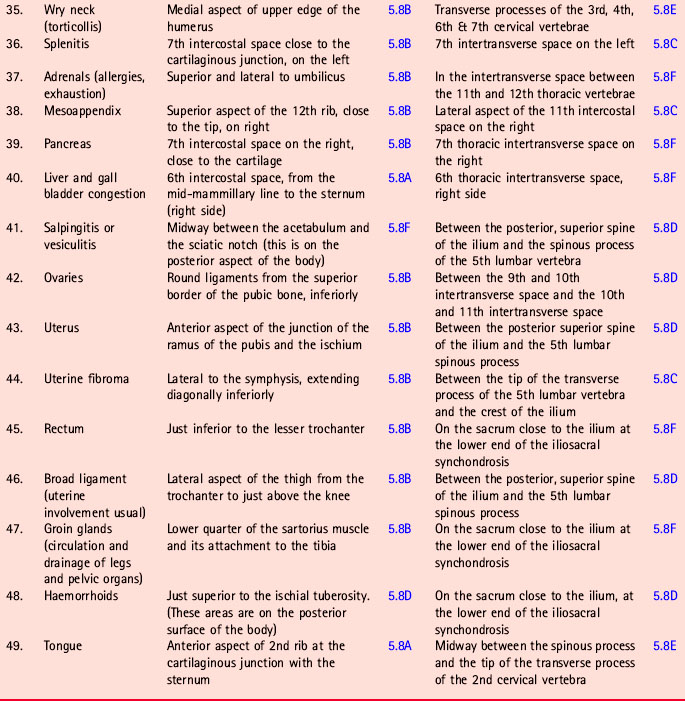
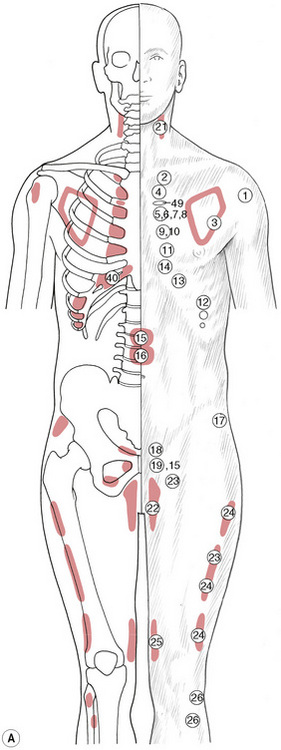
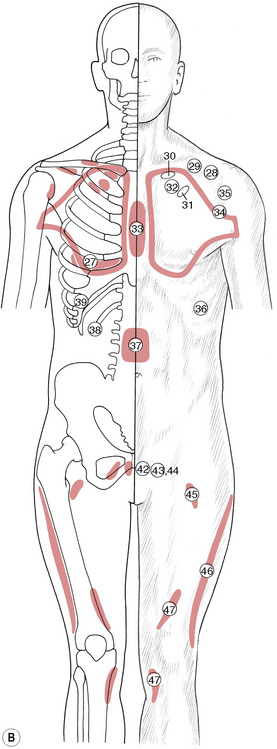
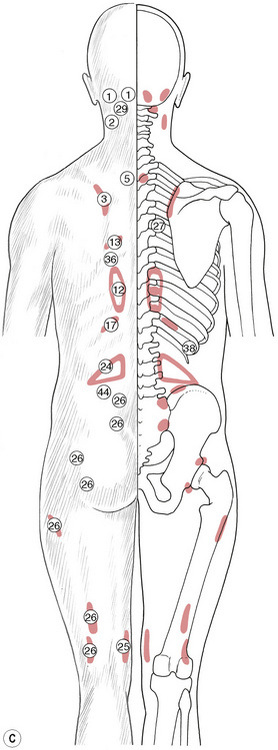
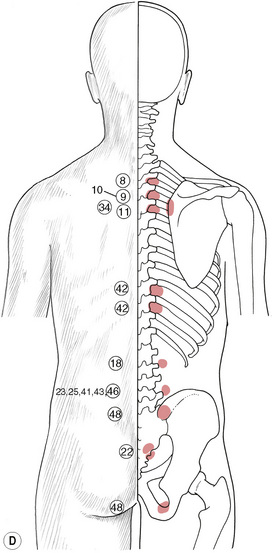
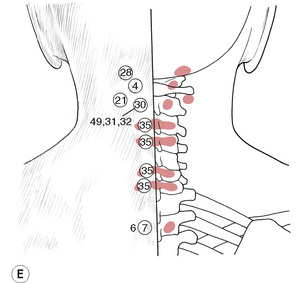
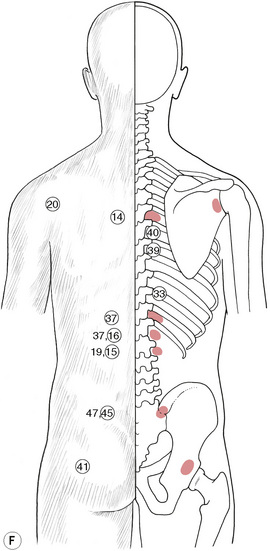
Figure 5.8C, D, E Chapman’s neurolymphatic reflexes. Symptom/area numbers are described in Table 5.1.
Chapman and Owens described dosage of treatment in terms of seconds, but in practice I feel that anyone experienced in neuromuscular treatment would have the degree of sensory awareness required to ‘feel’ when sufficient treatment had been given.
I would stress that I have found the reflexes of Chapman useful in differential diagnosis, and in the treatment of various conditions from spastic constipation to migraine – but always as a part of a broader approach to the patient as a whole. That they can influence lymphatic drainage dramatically, I have no doubt. I am less sure of the effect on visceral conditions, but have found that the reflexes themselves provide an excellent guide to progress. If they are no longer present, then invariably the condition is progressing well. These personal observations are confirmed by Patriquin (1997).
Chapman’s neurolymphatic reflexes (Fig. 5.8A-F)
The research evidence for, and the possible mechanisms relating to, Chapman’s neurolymphatic reflexes, were presented in Chapter 4.
In this chapter the method used in their application, as well as their positions, are discussed.
Chapman (Owen 1980) suggested a vibratory treatment in stimulating the neurolymphatic reflexes, lasting 10–15 seconds. He used fingertip pressure to impart the required energy, although thumb pressure of varying intensity is just as effective. This can be applied as a gradually intensifying pressure building up over 5–8 seconds, easing for 2 or 3 seconds and then repeated. Altogether this should not take more than half a minute.
These points can be overtreated and the optimum time would seem to be from 15 to 30 seconds with the pressure (or squeeze) of a variable nature. If the patient is able to report a referred pain resulting from the pressure, then pressure/treatment can be continued for up to 1 minute, with fluctuations in the degree of pressure, until the patient indicates a diminution in the referred pain or until the time has elapsed.
It is important to realize that the objective ‘feel’ of these contractions is unlikely to change during such treatment. Any changes resulting from the treatment will occur later, when homeostatic forces have come into operation. The variation in pressure during the treatment is more desirable than a constantly held degree of pressure, which may irritate and exacerbate the condition. In the foreword to Owen’s book An Endocrine Interpretation of Chapman’s Reflexes (1980), in which Owen describes his and Chapman’s research, noted osteopathic researcher Fred Mitchell recommends that pressure should be applied by the pad of the middle finger. This should be maintained as a light direct pressure, in an effort to decongest the fluid content of the palpable reflex point. Mitchell believed that the determining factor for the amount of treatment is whether a decrease in oedema takes place, or whether a dissolution of the gangliform contraction occurs, together with reduction in the sensitivity of the point over a period of between 20 and 120 seconds.
The stimulation threshold is being raised in these points, by such stimulation, and inhibition of noxious impulses is being achieved. There is nothing to be gained from achieving local pressure anaesthesia (numbing) by exaggerated effort. Reflexes that are not painful should not be treated: only an active (and therefore sensitive) reflex point requires attention.
The reflexes may be treated as part of a general neuromuscular treatment, or on their own in accordance with the recommendations of Chapman, Owen and Mitchell, which suggest the treating of the reflexes by light digital pressure of the anterior reflex followed by the corresponding posterior reflex.
• The anterior point should then be re-examined and, if there has been a palpable change, or sensitivity has diminished, then no more action is required.
• If no such change is found, the treatment to the anterior and then the posterior points is again carried out and, if still no change is noted, it is assumed that pathology is too great for a rapid change or is irreversible, or that there is a musculoskeletal factor maintaining the dysfunction.
If this approach is adopted, the grouping of reflexes into systems, is a useful method. If one of a group is found to be active then all others in the group should be examined and, if active, treated; for example:
• The endocrine group comprises: prostate, gonads, broad ligaments, uterus, thyroid and adrenals.
• The gastrointestinal group comprises the colon, thyroid, pancreas, duodenum, small intestine and liver.
• The infections group comprises liver, spleen and the adrenals.
The advice, therefore, is to use reflexes intelligently, treating only what is palpable and sensitive. Some of the anterior reflexes (the ones that should, in theory, be treated first) lie on the posterior aspect of the body.
It is suggested that reference be made to Owen (1980) for more detailed study. Table 5.1 gives the reflex by name, number and description of location, together with an indication of the figure on which it is indicated (it was not possible to incorporate all the drawings on to one picture without creating a confusing series of overlaps). It is also suggested that practitioners learn to search appropriate areas for the type of sensitive tissue changes that represent the superficial manifestation of these reflexes, and to use Fig. 5.8A-F and Table 5.1 to become familiar with the patterns and groups of these important aids to healing.
The illustrations will aid in locating these useful diagnostic and therapeutic areas.
Bennett’s neurovascular reflexes
(Note these will be sensitive to light pressure if active.) (See Figs 5.9A–C & Box 5.3.)
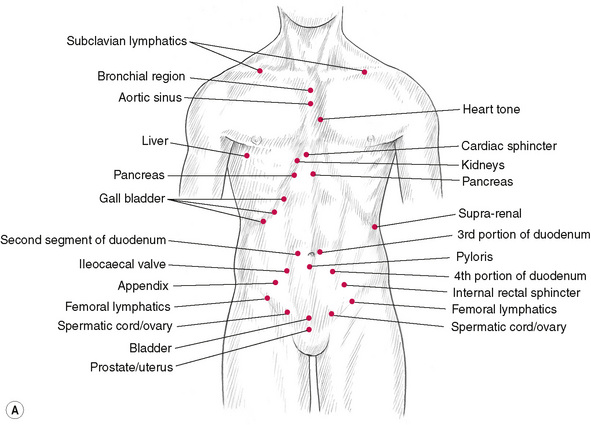

Box 5.3 Bennett’s neurovascular reflexes
| Reflex name | Site |
|---|---|
| 1. Parotid gland | Raised area on masseter when jaw clenched Diagnostic and treatment point. Associated conditions: prostate problems, mumps, premenstrual problem, mastitis, lymphatic stasis. |
| 2. Cardiac sphincter | Tip of xyphoid process Diagnostic and treatment point. If sensitive may relate to incompetent sphincter, heartburn. |
| 3. Liver | Midclavicular line; right 5th intercostal Diagnostic and treatment point. |
| 4. Gall bladder | Below costal cartilages right 9th, 10th, 11th ribs Diagnostic and treatment point. All points mentioned are treatment points; only 11th rib point is diagnostic. Pain may be noted as far lateral as mid-axillary line. |
| 5. Pancreas | Medial to 6th and 7th rib heads. 1 inch below xyphoid process Diagnostic point. 5th and 6th costal cartilages right and left. |
| 6. Pyloris | Lower border of umbilicus Diagnostic and treatment point. |
| 7. 2nd segment of duodenum | 1 inch and 45° above umbilicus on right Diagnostic and treatment point. Note: Order of treatment in this region should follow sequence of pyloris–duodenum–pancreas–liver–gall bladder. |
| 8. 3rd portion of duodenum | 1 inch and 45° above umbilicus on left Diagnostic and treatment point. |
| 9. 4th portion of duodenum | 1 inch and 45° lateral and below umbilicus (left) Diagnostic and treatment point. |
| 10. Kidneys | Tip of 8th rib. Bilateral Diagnostic and treatment point. |
| 11. Ileocaecal valve | On right side midway between anterior–superior iliac spine and umbilicus Diagnostic and treatment point. |
| 12. Internal rectal sphincter | On left midway between anterior/superior iliac spine and umbilicus Diagnostic and treatment point. |
| 13. Appendix | Directly over the organ Diagnostic and treatment point. |
| 14. Bladder | Just above pubic arch on midline Diagnostic and treatment point. |
| 15. Prostate/uterus | Symphysis pubis Diagnostic and treatment point. |
| 16. Spermatic cord/ovary | Approx. 1–1½ inches either side of bladder reflex (Note: thyroid to be treated when ovaries receiving attention) Diagnostic and treatment point. |
| 17. Supra-renal | One finger-width below tip 12th rib. Diagnostic point is tip of 12th rib. Diagnostic and treatment point. |
| 18. Anterior pituitary | Right, lateral aspect of eyebrow Diagnostic and treatment point. |
| 19. Posterior pituitary | Left, lateral aspect of eyebrow Diagnostic and treatment point. |
| 20. Thyroid | Over the organ Diagnostic and treatment point. |
| 21. Carotid sinus | On carotid artery, below angle of jaw Diagnostic and treatment point. |
| 22. Aortic sinus | Manubriosternal junction on ridge, or just inferior Diagnostic and treatment point. |
| 23. Heart tone | Sternal end of 3rd rib. Contact on cartilage (left) Diagnostic and treatment point. |
| 24. Subclavian lymphatics | Just inferior to and slightly medial to midpoint of clavicle Diagnostic and treatment point. |
| 25. Femoral lymphatics | On Poupart’s ligament. Midway between symphysis pubis and anterior superior iliac spine Diagnostic and treatment point. |
| 26. Maxillary sinus | Lateral to nares; bilaterally Diagnostic and treatment point. |
| 27. Bronchial region | Midway between manubrium sternum and episternal notch Diagnostic and treatment point. |
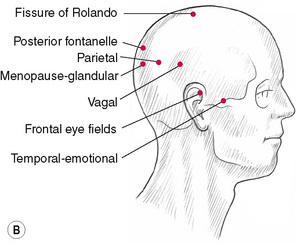
| 28. Frontal-emotional | Frontal eminences of forehead Diagnostic and treatment point. |
| 29. Vagal | 2 inches superior and 2 inches posterior to external auditory meatus Diagnostic and treatment point. |
| 30. Parietal | 2 inches superior and 3 inches posterior to external auditory meatus Diagnostic and treatment point. |
| 31. Temporal-emotional | Midway between outer aspect of eye and external auditory meatus. Just superior to zygomatic bone Diagnostic and treatment point. |
| 32. Anterior fontanelle | Over anatomical area Diagnostic and treatment point. |
| 33. Mid-sylvian | 1 inch superior to anterior aspect of external auditory meatus Diagnostic and treatment point. |
| 34. Fissure of Rolando | Approx. 1½ inches posterior to anterior fontanelle Diagnostic and treatment point. |
| 35. Frontal eye fields | 1½ inches superior to frontal eminences Diagnostic and treatment point. |
| 36. Extrinsic eye muscles | Superior to eyelids with closed eyes Diagnostic and treatment point. |
| 37. Posterior fontanelle | Over anatomical area Diagnostic and treatment point. |
| 38. Menopause-glandular | ½ inch inferior and lateral to posterior fontanelle Diagnostic and treatment point. |
All the points on the cranium are useful for treating emotional and stress conditions. Those marked ‘emotional’ are the strongest. Light pressure only is suggested. Reference to these reflexes will be found in the chapter on treatment techniques (Ch. 6).
The way in which Bennett’s neurovascular (NV) reflex points are used depends largely on the therapeutic objective: as diagnostic indicators; to influence specific muscle function; or to ease symptoms, particularly those deriving from emotional causes.
As with Chapman’s neurolymphatic points, neurovascular points might be seen as useful additional sources of information regarding the organ, structure or function to which they appear to be linked. If the region of the point palpates as sensitive, further confirmation should be sought of the dysfunction indicated by the reflex.
Applied kinesiology methodology tends to use these neurovascular points as a means of modifying specific muscles with which they are purported to be reflexly linked.
Walther (1988) explains:
A specific muscle responds to only one [neurovascular] reflex, but most reflexes influence more than one muscle. Bennett’s reflexes are primarily on the anterior surface of the trunk and on the head. The reflexes on the head are those used in applied kinesiology, with few exceptions.
The way in which these reflexes are treated is as follows:
1. The point is located and a contact is made with the pad or tip of one finger.
2. The skin overlying the point is ‘tugged’ lightly and the finger contact is maintained until a pulsation is noted.
3. If the pulsation does not appear, the direction in which the skin ‘tug’ is made is varied until a pulsation is noted.
4. After the pulsation is noted, the finger contact is maintained for a further 15–20 seconds.
Walther (1988) describes how neurovascular points can be used to treat symptoms related to emotional causes:
Many of the emotional problems dealt with by this technique are those found in general examination to determine the reason for a recurring [problem]. It is not necessary … to know the precise emotional factor … Ask the person to think about the problem with the eyes closed, and watch for rapid eye movement (REM) which [may be] associated with the emotional experience … The NV reflex is located bilaterally on the frontal bone eminence [see point 28 (frontal-emotional) on Fig. 5.9C and description in Box 5.3] and is treated with a light tugging contact [see above] … until a maximum pulsation is felt. It may be necessary to hold the contact points for several minutes.
Conclusions
Speransky (1943) stated that ‘the nervous system contains a record of the past history of the organism’. For the practitioner, the signs present in the musculoskeletal system constitute a map of past and present dysfunctions. It presents him or her with the opportunity to treat, alleviate and prevent further dysfunction.
Apart from palpation for tissue changes and reflex trigger areas, diagnosis should involve an evaluation of the gross stress patterns and postural factors. Each patient is an individual challenge, and indeed this challenge is renewed at each visit. Thus, whilst the mechanics of treatment are similar, the emphasis will probably be different at each visit. It is important that the patient understands this, and the nature of the problem as well as the goals being aimed for. A cooperative patient will accept the time and effort required to achieve that goal.
• Observation of the dynamic posture, or body in motion, gives an idea of balance, posture, gravitational stress, gross structural anomalies, etc.
• Observation of certain body areas in individual movement will then help the understanding of their stress patterns, restrictions, and so on.
We need to learn to appreciate the arrangement of the various body structures and their interrelationships so that myofascial tensions can then be visualized. When these gross and local postural patterns, in active and passive modes, have been observed, an overall impression can be added to the palpatory impressions, both superficial and deep, which the hands evaluate with the patient standing, supine or prone.
• By lightly passing the hands over the various structures, alterations in tissue density and configuration can be felt.
• The deeper palpation to localize the dysfunction can then be performed or left to the neuromuscular treatment, where diagnosis coincides with treatment.
A history will have been taken before observation, palpation and mobility tests, and such history should be comprehensive, taking note of traumatic incidents, habits, occupational positions and postures, emotional state and history, congenital deformity and surgery, as well as general medical history and specific details of the presenting problems.
Mobility tests form part of the diagnostic procedures in soft tissue assessment and, because all manual therapists are concerned with joint mobility, these tests will also be part of any overall assessment. Active motion, movement of one part of the body in relation to another, powered by conscious muscular effort as well as passive motion in which an outside force acts on the body to induce movement, are both of diagnostic importance. Eventually it is possible to distinguish between healthy tissue, and tissue in which there is dysfunction. This can be learned only by experience.
Observation, static and active; palpation, superficial and deep; a comprehensive and detailed history; mobility tests as required; localization of trigger areas; re-evaluation during the course of treatment; and an intelligent cooperative understanding of the patient’s problems, are the diagnostic tools with which to undertake the task in hand.
Finding ‘points’ using NMT
Knowledge of Chapman’s neurolymphatic areas, Bennett’s reflexes, Mackenzie’s reflex areas, connective tissue zones, and trigger points, might appear a massive task for the memory – and so it is.
However, the application of the general knowledge of their existence enables treatment to be effective even without precise knowledge of all the individual reflexes involved. The aim of this chapter has been to try to classify some of the more obvious diagnostic indicators, so that the practitioner’s awareness of the range of diagnostic and therapeutic possibilities can be broadened.
Arbuckle B. Selected writings. National Osteopathic Institute, 1977.
Baldry P. Acupuncture, trigger points and musculoskeletal pain. London: Churchill Livingstone, 1993.
Beal M. Palpatory testing for somatic dysfunction in patients with cardiovascular disease. J Am Osteopath Assoc. 1983;82:822-831.
Bischof I., Elmiger G. Connective tissue massage. In: Licht E., editor. Massage, manipulation and traction. New Haven, 1960. Connecticut
Chaitow L. An introduction to Chapman’s reflexes. British Naturopathic Journal. 1965;6(4):111-113.
DiGiovanna E., editor. An osteopathic approach to diagnosis and treatment. Philadelphia: Lippincott, 1991.
Koizumi K. Autonomic system reactions, caused by excitation of somatic afferents: study of cutaneo-intestinal reflex. In: Korr I., editor. The neurobiological mechanisms in manipulative therapy. New York: Plenum Press, 1978.
Lewit K. Manipulative therapy in rehabilitation of the locomotor system, ed 2. London: Butterworths, 1992.
Lewit K. Manipulative therapy in rehabilitation of the locomotor system, ed 3. London: Butterworths, 1999.
Lewit K., Olšanská S. Clinical importance of active scars: abnormal scars as a result of myofascial pain. J Manipulative Physiol Ther. 2004;27:399-402.
Lief P. British Naturopathic Journal. 1963;5(10):304-324.
Mackenzie J. Symptoms and their interpretations. 1909. London
Owen C. An endocrine interpretation of Chapman’s reflexes. Newark, Ohio: American Academy of Osteopathy, 1980.
Patriquin D. Chapman’s reflexes. In: Ward R., editor. Foundations for osteopathic medicine. Baltimore: Williams & Wilkins, 1997.
Speransky A. A basis for the theory of medicine. New York: International Publishers, 1943.
Stiles E. Patient Care. 1984:117-164. 15 May:16–87; 15 August
Teiriche-Leube H. Grundriss der Bindesgewebsmassage. Stuttgart: Fisher, 1960.
Travell J. Symposium on mechanisms and management of pain syndromes. Proceedings of the Rudolph Virchow Medical Society. 1957.
Travell J., Simons D. Myofascial pain and dysfunction. vol 1. Baltimore: Williams & Wilkins; 1983.
Travell J., Simons D. Myofascial pain and dysfunction. vol 2. Baltimore: Williams & Wilkins; 1992.
Walther D. Applied kinesiology. Pueblo, Colorado: SDC Systems, 1988.
Youngs B. NMT of lower thorax and low back. British Naturopathic Journal. 1964;5(11):176-190. 340–358