6 Basic spinal NMT
Defining NMT
NMT, as the term is used in this book, is summarized in Box 6.1.
Box 6.1 Aims of NMT and allied approaches
• Neuromuscular technique, as the term is used in this book, refers to the manual application of specialized pressure and strokes, usually delivered by a finger or thumb contact, which have a diagnostic (assessment mode) or therapeutic (treatment mode) objective.
• Therapeutically, NMT aims to produce modifications in dysfunctional tissue, encouraging a restoration of normality, with a primary focus of deactivating focal points of reflexogenic activity such as myofascial trigger points.
• An alternative focus of NMT application is towards normalizing imbalances in hypertonic and/or fibrotic tissues, either as an end in itself or as a precursor to joint mobilization/rehabilitation.
• NMT utilizes physiological responses involving neurological mechanoreceptors, Golgi tendon organs, muscle spindles and other proprioceptors, in order to achieve the desired responses.
• Insofar as they integrate with NMT, other means of influencing such neural reporting stations, including positional release (strain/counterstrain) and muscle energy methods (such as reciprocal inhibition and post-isometric relaxation induction) are seen to form a natural set of allied approaches.
• Traditional massage methods that encourage a reduction in retention of metabolic wastes and enhanced circulation to dysfunctional tissues are included in this category of allied approaches.
In this text the ‘European’ version of NMT, as developed by Stanley Lief, based partly on traditional Ayurvedic massage, is one of two areas of NMT focus.
The other NMT version described is the American NMT model, that resulted from the original work of Nimmo, Simons and Travell – with further development by St John and Walker, among others (see Chapters 10 and 13).
A confusing element relating to the term NMT emerges, because of its use by Dvorak et al (1988), when they describe what are, in effect, variations on the theme of the use of isometric contractions in order to encourage a reduction in hypertonicity. These methods, all of which form part of what is known as muscle energy technique (MET) in osteopathic medicine and proprioceptive neuromuscular facilitation (PNF) in physiotherapy, are described briefly in Chapter 8, and form the focus of a further title in the series of which this book is part (Chaitow 2001, 2006).
Dvorak et al (1988) have listed various MET methods (as NMT) as follows:
1. Methods that involve self-mobilization by patient action, to encourage movement past a resistance barrier, are described as ‘NMT 1’.
2. Isometric contraction and subsequent passive stretching of agonist muscles, involving postisometric relaxation, are called ‘NMT 2’.
3. Isometric contraction of antagonists, followed by stretching, involving reciprocal inhibition, are described as ‘NMT 3’.
Use of the terms NMT 1, 2 and 3 in these ways, by Dvorak et al (1988), in order to describe these methods, succeeds in adding to, rather than reducing, semantic confusion, and it is hoped that this aberrant set of descriptors will not persist.
Unique aspects of NMT
What is unique to NMT, as discussed in this book, is its concentration on the soft tissues, not just to give reflex benefit to the body, not just to prepare for other therapeutic methods such as exercise or manipulation, not just to relax and normalize tense fibrotic muscular tissue, and not just to enhance lymphatic and general circulation and drainage, but to do all these things and, at the same time, to be able to offer the practitioner diagnostic information via the palpating and treating instrument, which is usually the thumb.
NMT can usefully be integrated in treatment that is aimed at postural reintegration, tension release, pain relief, improvement of joint mobility, reflex stimulation/modulation or sedation. There are many variations of the basic technique, as developed by Stanley Lief, the choice of which will depend upon particular presenting factors, or personal preference. Similarities between some aspects of NMT and other manual systems (see Ch. 8) should be anticipated, as techniques have been borrowed and adapted from other systems where appropriate. For example, in Chapter 11 Dennis Dowling demonstrates the clinical value of using progressive inhibition of neuromuscular structures (PINS), a unique way of utilizing NMT effects, in pain control. Use of PINS in pain control offers an example of the evolution of new applications of the basics, which NMT provides (Dowling 2000).
And just as there are current evolutionary paths involving NMT principles, so there have been parallel evolutions of methods that derive from similar backgrounds. In Chapter 12 Howard Evans describes Thai yoga massage methods that are truly a blend of the model of manual care that evolved in Thailand, based on the same root approaches deriving from Ayurvedic massage which let to Lief’s NMT. Evans’ approach is further influenced by having studied Lief’s methods giving him a useful Western and Eastern set of approaches which he has fused and described (Evans 2009).
NMT can be applied generally, or locally, and in a variety of positions (with the patient seated, supine, prone, side-lying, etc.). The order in which body areas are dealt with is not regarded as critical in general treatment, but seems to be of some consequence in postural reintegration (Rolf 1977).
In Chapter 13, Cohen describes both the historical work of Raymond Nimmo, and the continuing evolution of his methods, which form a major part of American Version NMT, as described by DeLany in Chapter 10.
Most used NMT approaches – and ‘variable pressure’
The basic spinal NMT treatment and the basic abdominal (and related areas) NMT treatment (see Ch. 7) are the most commonly used, and will be described in detail in this and the next chapter. The methods described are in essence those of Stanley Lief ND DC and Boris Chaitow ND DC, both of whom achieved a degree of skill in the application of NMT that is unsurpassed. The inclusion of data on reflex areas and effects, together with basic NMT methods, provides the practitioner with a useful therapeutic tool, the limitations of which will be determined largely by the degree of intelligence and understanding with which it is employed.
As Boris Chaitow has written (personal communication, 1983):
The important thing to remember is that this unique manipulative formula is applicable to any part of the body for any physical and physiological dysfunction and for both articular and soft tissue lesions.
To apply NMT successfully it is necessary to develop the art of palpation and sensitivity of fingers by constantly feeling the appropriate areas and assessing any abnormality in tissue structure for tensions, contractions, adhesions, spasms.
It is important to acquire with practice an appreciation of the ‘feel’ of normal tissue so that one is better able to recognise abnormal tissue. Once some level of diagnostic sensitivity with fingers has been achieved, subsequent application of the technique will be much easier to develop. The whole secret is to be able to recognise the ‘abnormalities’ in the feel of tissue structures. Having become accustomed to understanding the texture and character of ‘normal’ tissue, the pressure applied by the thumb (in general), especially in the spinal structures, should always be firm, but never hurtful or bruising. To this end the pressure should be applied with a ‘variable’ pressure, i.e. with an appreciation of the texture and character of the tissue structures and according to the feel that sensitive fingers should have developed. The level of the pressure applied should not be consistent because the character and texture of tissue is always variable. These variations can be detected by one’s educated ‘feel’. The pressure should, therefore, be so applied that the thumb is moved along its path of direction in a way which corresponds to the feel of the tissues.
This variable factor in finger pressure constitutes probably the most important quality any practitioner of NMT can learn, enabling him to maintain more effective control of pressure, develop a greater sense of diagnostic feel, and be far less likely to bruise the tissue.
Variation of applied digital pressure during the application of NMT is probably the most important single feature that deserves emphasis and re-emphasis to anyone learning or using these methods. This feature of NMT is discussed again later in this chapter.
Thumb considerations
 NMT thumb technique (Fig. 6.1)
NMT thumb technique (Fig. 6.1)
Thumb technique as employed in NMT, in either assessment or treatment modes, enables a wide variety of therapeutic effects to be produced.
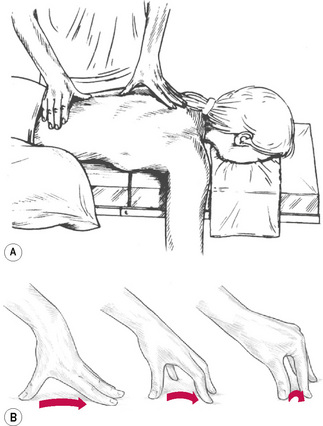
The tip of the thumb can deliver varying degrees of pressure, via any of four facets; the very tip may be employed or the medial or lateral aspect of the tip can be used to make contact with angled surfaces.
For more general (less localized and less specific) contact, of a diagnostic or therapeutic nature, the broad surface of the distal phalange of the thumb is often used. It is usual for a light non-oily lubricant to be used to facilitate easy, non-dragging, passage of the palpating digit.
• For balance and control, the hand should be spread, the tips of fingers providing a fulcrum or ‘bridge’ in which the palm is arched in order to allow free passage of the thumb towards one of the fingertips as the thumb moves in a direction that takes it away from the practitioner’s body.
• During a single stroke, which covers between 2 and 3 inches (5–8 cm), the fingertips act as a point of balance, while the chief force is imparted to the thumb tip via controlled application through the long axis of the extended arm of body weight.
• The thumb, therefore, never leads the hand but always trails behind the stable fingers, the tips of which rest just beyond the end of the stroke.
• Unlike many bodywork/massage strokes, the hand and arm remain still as the thumb, applying variable pressure (see below), moves through its pathway of tissue.
• The extreme versatility of the thumb enables it to modify the direction of imparted force in accordance with the indications of the tissue being tested or treated.
• As the thumb glides across and through those tissues it becomes an extension of the practitioner’s brain. In fact, for the clearest assessment of what is being palpated, the practitioner should have the eyes closed, in order that every minute change in the tissue can be felt and reacted to.
• The thumb and hand seldom impart their own muscular force, except in dealing with small localized contractures or fibrotic ‘nodules’.
• In order that pressure/force be transmitted directly to its target, the weight being imparted should travel in as straight a line as possible, which is why the arm should not be flexed at the elbow or the wrist by more than a few degrees. The positioning of the practitioner’s body in relation to the area being treated is also of the utmost importance in order to facilitate economy of effort and comfort.
• The optimal height vis-à-vis the couch, and the most effective angle of approach to the body areas being addressed, must be considered and the descriptions and illustrations will help to make this clearer.
• The degree of pressure imparted will depend on the nature of the tissue being treated, with a great variety of changes in pressure being possible during strokes across and through the tissues. When being treated, the patient should not feel strong pain, but a general degree of discomfort is usually acceptable as the seldom stationary thumb varies its penetration of dysfunctional tissues.
• A stroke or glide of 2–3 inches (5–8 cm) will usually take 4–5 seconds – seldom more unless a particularly obstructive indurated area is being dealt with. If reflex pressure techniques are being employed, a much longer stay on a point will be needed, but in normal diagnostic and therapeutic use the thumb continues to move as it probes, decongests and generally treats the tissues.
• It is not possible to state the exact pressures necessary in NMT application because of the very nature of the objective, which in assessment mode attempts to meet and match the tissue resistance precisely, to vary the pressure constantly in response to what is being felt.
• In subsequent or synchronous (with assessment) treatment of whatever is uncovered during evaluation, a greater degree of pressure is used and this too will vary, depending upon the objective – whether this is to inhibit, to produce localized stretching, to decongest and so on. Obviously, on areas with relatively thin muscular covering, the applied pressure would be lighter than in tense or thick, well covered areas such as the buttocks.
• Attention should also be paid to the relative sensitivity of different areas and different patients. The thumb should not just mechanically stroke across or through tissue but should become an intelligent extension of the practitioner’s diagnostic sensitivities so that the contact feels to the patient as though it is sequentially assessing every important nook and cranny of the soft tissues. Pain should be transient and no bruising should result if the above advice is followed.
• The treating arm and thumb should be relatively straight because a ‘hooked’ thumb, in which all the work is done by the distal phalange, will become extremely tired and will not achieve the degree of penetration possible via a fairly rigid thumb.
Hypermobile thumbs
Some practitioners have hypermobile joints and it is difficult for them to maintain sustained pressure without the thumb giving way and bending back on itself. This is a problem that can be overcome only by attempting to build up the muscular strength of the hand or by using a variation of the above technique; for example, a knuckle or even the elbow may be used to achieve deep pressure in very tense musculature. Alternatively, the finger stroke as described below can take over from a hypermobile thumb.
Alternatively an instrument such as the ‘T’-bar (see Ch. 10, Fig. 10.1B,C) may be used to ease mechanical stress on the thumb joints.
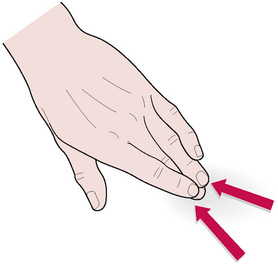
NMT finger technique (Fig. 6.2)
In certain localities, the width of the thumb prevents the degree of tissue penetration needed for successful assessment and/or treatment. In such regions the middle or index finger can usually be suitably employed. The most usual area for use of finger, rather than thumb, contact is in the intercostal musculature, and in attempting to penetrate beneath the scapula borders in tense fibrotic conditions.
• The middle or index finger should be slightly flexed and, depending on the direction of the stroke (most usually toward the practitioner) and density of the tissues, supported by one of its adjacent members.
• As the treating finger strokes with a firm contact, and usually a minimum of lubricant, a tensile strain is created between its tip and the tissue underlying it.
• This is stretched and lifted by the passage of the finger which, like the thumb, should continue moving unless or until dense, indurated tissue prevents its easy passage. When treating, these strokes can be repeated once or twice, as tissue changes dictate.
• The angle of pressure to the skin surface is between 40° and 50°.
• The fingertip should never lead the stroke but should always follow the wrist, the palmar surface of which should lead, as the hand is drawn towards the practitioner. It is possible to impart a great degree of ‘pull’ on underlying tissues, and the patient’s reactions must be taken into account in deciding on the degree of force to be used. Transient pain, or mild discomfort, is to be expected, but no more than that. All sensitive areas are indicative of some degree of dysfunction, local or reflex, and are thus important, and their presence should be recorded. The patient should be told what to expect, so that a cooperative, unworried attitude evolves.
• As mentioned above, unlike the thumb technique, in which force is largely directed away from the practitioner’s body, in finger treatment the motive force is usually towards the practitioner.
• The arm position therefore alters, and a degree of flexion is necessary to ensure that the pull, or drag, of the finger across the lightly lubricated tissues is smooth.
• Unlike the thumb, which makes a sweep across the palm towards the fingertips, whilst the rest of the hand remains relatively stationary, the whole hand will move when finger technique is applied.
• Certainly some variation in the degree of angle between fingertip and skin is allowable during a stroke, and some slight variation in the degree of ‘hooking’ of the finger is sometimes also necessary.
• However, the main motive force is applied by pulling the slightly flexed, middle or index, finger towards the practitioner, with the possibility of some lateral emphasis if needed. The treating finger should always be supported by one of its neighbours.
Use of lubricant
The use of a lubricant to facilitate the smooth passage of, for example, the thumb over the surface is an essential aspect of NMT. The lubricant used should not allow too slippery a passage of the thumb or finger, and a suitable balance between lubrication and adherence is found by mixing 2 parts of rapeseed (or almond) oil to 1 part of lime or rose water. At times, the degree of stimulus imparted via this contact can be enhanced by increasing the tensile strain between the thumb or finger and the skin. If a cream is used, standard aqueous ointment, inexpensively available from any pharmacy, is hypoallergenic and offers an appropriate, non-greasy, medium.
If a stimulant effect is required (see notes on Connective tissue massage in Chapters 4 and 5), possibly in order to achieve a rapid vascular response, then no lubricant should be used.
Clinical experience shows that similar reactions will be achieved (with lubricant) where NMT is applied along the intermuscular septa, or at the origins and insertions of muscles.
It should be clear that whatever underlying tissues are being treated should be visualized. Depending upon the presenting symptoms, and the area involved, any of a number of procedures may be undertaken as the hand moves from one site to another:
• Superficial stroking in the direction of lymphatic flow
• Direct pressure along the line of axis of stress fibres
• Deeper alternating ‘make and break’ stretching and pressure efforts
• Subtle weaving, insinuating, movements that attempt to melt into the tissues to obtain information or greater access
• Crowding of bunched tissues toward the direction in which they are shortening.
As variable pressure is being applied, the practitioner needs to be constantly aware of diagnostic information that is being received via the contact hands, as this is what should determine the variations in pressure and the direction of force being applied.
Any changes in direction, or degree, of applied pressure should ideally take place without any sudden release, or application, of force, which might irritate the tissues and produce pain or a defensive contraction.
Lief’s basic spinal treatment followed the pattern as set out below. The fact that the same pattern is followed at each treatment does not mean that the treatment is necessarily the same each time. The pattern gives a frame-work and a useful starting and ending point, but the degree of emphasis applied to the various areas of dysfunction that manifest themselves is a variable factor based always on what information the palpating hands are picking up: this is what makes each treatment different.
The areas of dysfunction noted during NMT application should be recorded on a case card, together with all relevant material and assessment and diagnostic findings relating to myofascial tissue changes, trigger points and reference zones, areas of sensitivity, restricted motion, fibrotic changes, asymmetrical features, and so on.
Lief’s basic spinal treatment
Lief’s basic spinal NMT treatment follows a pattern in which the patient is prone, with a pillow of medium thickness under the chest, forehead supported by the patient’s hands or, ideally, resting in a split head-piece or face-hole. Alternatively – and more appropriately – a contoured cushion, which supports the entire body, should be used.
1. The whole spine from occiput to sacrum, including the gluteal area, should be lightly oiled or creamed.
2. The practitioner should begin by standing half-facing the head of the couch on the left of the patient, with the hips level with the mid-thoracic area.
3. To facilitate the intermittent application of pressure and the transfer of weight via the arm to the exploring and treating thumb, the practitioner should stand with the left foot forward of the right by 12–18 inches (30–45 cm), weight evenly distributed between them, knees slightly flexed.
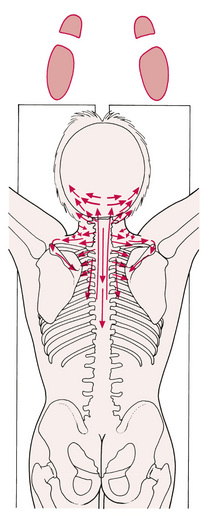
4.The first contact, to the left side of the patient’s head, is a gliding, light-pressured movement of the medial tip of the right thumb, from the mastoid process along the nuchal line to the external occipital protuberance. This same stroke, or glide, is then repeated with deeper pressure (see Fig. 6.4A,B).
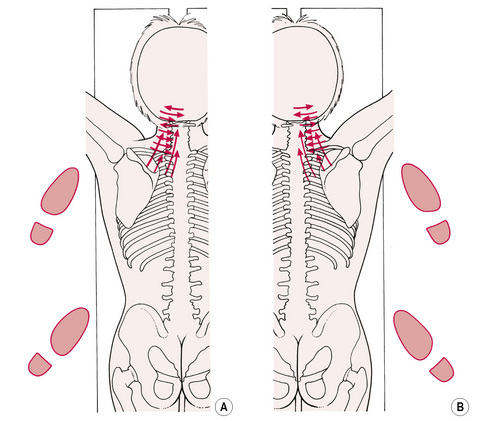
Figure 6.4A, B First positions of suggested sequence of applications of NMT, to ensure optimal thumb and/or finger contact with primary trigger point sites and with the origins and insertions of most muscles. Note foot positions.
The non-treating hand’s role
• The practitioner’s left hand should at this time rest on the upper thoracic or shoulder area to act as a stabilizing contact.
• Whichever hand is operating at any given time, the other hand can give assistance by means of gently rocking or stretching tissues to complement the efforts of the treating hand, or it can be useful in distracting tissues that are ‘mounding’ as the treating hand works on them.
• Whenever the practitioner changes to the other side of the table, it is suggested that one hand always maintains light contact with the patient. Indeed, it is suggested that, once treatment has commenced, no breaks in contact be allowed.
• There is often a noticeable increase in tension in the tissues if the series of strokes, stretching movements and pressure techniques that make up NMT are interrupted by even a few seconds because of a break in contact. Continuity would seem, in itself, to be of therapeutic value, simply as a reassuring and calming feature.
What the treating thumb feels
The movement of the right thumb through the tissue is slow – not uniformly slow, but deliberately seeking and feeling for ‘contractions’ and ‘congestions’ (to use two words that will be meaningful to any manual therapist). If and when such localized areas are felt, the degree of pressure can be increased and, in a variably applied manner, this pressure carries the thumb tip across, or through, the restricting tissues, decongesting, stretching and easing them.
The patient will often report a degree of pain but may say that it ‘feels good’. This is a contradiction in terms, but constructive pain is usually felt as a ‘nice hurt’.
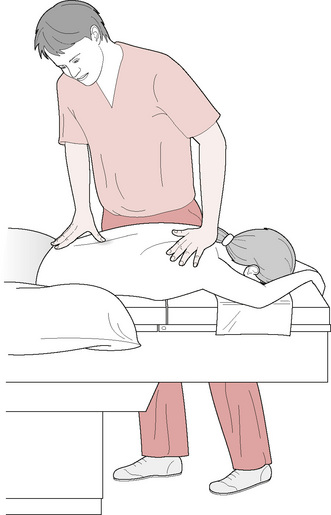
Practitioner’s posture (Fig. 6.3)
• When applying thumb strokes, whether facing the head or the foot of the table, the treating arm should not be flexed, because the optimum transmission of weight from the practitioner’s shoulder, through the arm to the thumb tip, is best achieved with a relatively straight arm.
• This demands that the practitioner ensures the table height is suitable for his or her own height. The practitioner should not be forced to stand on tiptoe to treat the patient, nor should an unhealthy bent posture have to be adopted.
• The practitioner’s weight should be evenly spread between the separated feet, both of which are forward facing at this stage.
• In this way, by slightly altering the weight distribution from the front to the back foot, and vice versa, an accurate, controlled degree of pressure can be exerted with minimal arm or hand effort.
The mechanics of NMT – achieving economy of effort
• The hand itself should not be rigid but in a relaxed state, moulding itself to the contours of the neck or back tissues.
• To some extent the fingertips stabilize the hand.
• The thumb’s glide is controlled by this support, so that the actual stroke is achieved by the tip of the extended thumb being brought slowly across the palm towards the fingertips.
• The fingers, during this phase of cervical treatment, would be placed on the opposite side of the neck to that being treated.
• The fingers maintain their position as the thumb performs its diagnostic/therapeutic glide. Figure 6.4A,B will aid the reader to a better understanding of this description.
However, were all the effort to be on the part of the thumb, it would soon tire. Consider which parts of the practitioner’s arm/hand are involved with the various aspects of the glide/stroke as delivered by the thumb (finger strokes involve completely different mechanics):
1. The transverse movement of the thumb is a hand or forearm effort.
2. The relative straightness, or rigidity, of the last two thumb segments is also a local muscular responsibility.
3. The vast majority of the energy imparted via the thumb results from transmission of body weight, through the straight arm and into the thumb.
4. Any increase in pressure can be speedily achieved by simple weight transfer from back towards front foot, and a slight ‘lean’ on to the thumb from the shoulders.
5. A lessening of imparted pressure is achieved by reversing this body movement.
Treatment continues
• The first two strokes of the right thumb having been completed – one shallow and almost totally diagnostic, and the second, deeper, imparting therapeutic effort – the next stroke is half a thumb-width caudal to the first.
• Thus a degree of overlap occurs as these strokes, starting on the belly of the sternocleidomastoid, glide across and through the trapezius, splenius capitus and posterior cervical muscles.
• A progressive series of strokes is applied in this way until the level of the cervicothoracic junction is reached.
• Unless serious underlying dysfunction is found, it is seldom necessary to repeat the two superimposed strokes at each level of the cervical region.
Variable pressure – the key to painless pressure
• If underlying fibrotic tissue appears unyielding, a third, or fourth, slow deep glide may be necessary.
• The degree of discomfort felt by the patient is of some importance. The sensitivity of this region is well known and if pressure is too deep, or sustained for too long, the defensive resistance that may be created can make the treatment counterproductive.
• It is possible to achieve deep, penetrating pressure if it is variable in nature and not held for long, without undue pain or discomfort.
• Thus a thinking, intuitive feel for the work is a prerequisite of successful application.
Deactivating trigger points
Should trigger points be located during the NMT assessment/treatment strokes – as indicated by the reproduction, in a target area, of an existing, familiar, pain pattern – then a number of choices are open:
1. The point can be marked and noted (on a chart and if necessary on the body with a skin pencil) for later attention, or treatment can be offered immediately.
2. Sustained pressure, or ‘make and break’ pressure, can be used (see Chapters 8 & 9 for details and choices).
3. Application of a positional release approach (strain/counterstain) will reduce activity in the hyperreactive tissue, as outlined in Chapter 8 (Simons 2002).
4. Initiation of an isometric contraction followed by local and whole muscle stretching should be used (Lewit 1999).
5. A combination of pressure, positional release and muscle energy technique (MET) (integrated neuromuscular inhibition technique (INIT), as described in Ch. 9) can be introduced (Chaitow 1994).
6. Alternatively, spray and stretch methods can be used (vapocoolant technique, as discussed in Chapter 8) (Kostopoulos D, Rizopoulos K 2008, Sola & Bonica 1990, Travell & Simons 1992).
7. An acupuncture needle or procaine injection can be used (as, it is suggested, can laser or microcurrent application) (Baldry 2001, McMakin 1998).
8. Sustained pressure, if applied, should be variable: deep pressure for 5–7 seconds, followed by a slight easing for a further few seconds, and so on, repeated until the local or reference pain changes (usually diminishing, but sometimes increasing), or until 2 minutes have elapsed. It is suggested that no more than this amount of manual pressure should be applied to a trigger point at any one session.
9. Further ease of the hyper-reactive patterns in a trigger point can be achieved by the application of a hot towel to the area, followed by effleurage (Lowe & Honeyman-Lowe 1999).
10. Whichever approach is used, a trigger point will only be permanently deactivated if the muscle in which it lies is restored to its normal resting length, and MET can assist in achieving this (Travell & Simons 1992).
The neck treatment continues
• Once the right thumb has completed its series of transverse strokes across the long axis of the cervical musculature, the left hand, which has been resting on the patient’s left shoulder, now comes into play.
• A series of strokes is applied by the left thumb, upward from the left of the upper thoracic area towards the base of the skull.
• The fingers of the left hand rest (and act as a fulcrum) on the front of the shoulder area at the level of the medial aspect of the clavicle.
• The thumb tip should be angled to allow direct pressure to be exerted against the left lateral aspects of the upper thoracic and the lower cervical spinous processes as the thumb glides cephalad.
• The subsequent strokes of the thumb should be in the same direction, but placed slightly more laterally.
• The fingers should then be placed on the patient’s head at about the temporo-occipital articulation. The left thumb then deals in the same way with the mid and upper cervical soft tissues, finishing with a lateral stroke or two across the insertions on the occiput itself.
In travelling from the nuchal line to the level of the cervicothoracic junction, and back again, in a series of overlapping searching/gliding movements, common sites of a number of possible trigger points will have been evaluated.
• The midpoint of the sternomastoid, at the level of the posterior angle of the jaw, can be the source of an intensely painful trigger point, which refers to an area from above the temple in the ear region, to below the angle of the jaw.
• Similar triggers exist in the splenius capitis, upper trapezius, posterior cervical and other muscles of the region, all with different target areas. (See Fig. 3.6 for these and other examples of trigger point distribution patterns.)
Posterior reflex centres
Also in the cervical area are to be found the posterior neurolymphatic reflex centres (Chapman’s reflexes), notably those connected with conjunctivitis, cerebellar congestion, and ear, nose and throat problems of an inflammatory or congested type, from sinusitis to tonsillitis.
It is suggested that a study is made of the illustrations of neurolymphatic reflex positions (see Ch. 5). Treatment of these points is via lightly sustained pressure, as described in Chapter 4.
Among the more important tsubo or acupressure points in the upper cervical area are:
• Gall bladder 20, which lies bilaterally in a depression midway between the occipital protuberance and the mastoid at the base of the skull.
• Bladder 10, which lies bilaterally just lateral to the large bundle of muscular insertions at the occiput.
• Triple heater 17, which lies bilaterally in the depression between the lobe of ear and the mastoid process.
These points, if sensitive, should receive a sustained or variable pressure, as for the other trigger points. Their influence is felt in a variety of conditions relating to the head, such as migraine, neuralgia, cold symptoms, hypertension and hypotension, and liver dysfunction.
Goodheart (1987) mentions levator scapulae ‘weakness’ as indicating digestive problems and recommends pressure techniques in the cervicothoracic area and on the medial border of the scapula to help normalize this.
Following NMT treatment of the left side of the cervical area, the same procedures are repeated on the right.
A tall practitioner can probably adapt to treat both sides from one standing position; however, a move to the opposite side makes for a more controlled delivery of the appropriate strokes.
Origins and insertions
During NMT assessment and treatment, special notice should be given to the origins and insertions of the muscles that are being accessed. Where bony landmarks are palpable by the thumb tip, they should be treated by slow, variably applied, pressure.
All bony surfaces within reach of the probing finger or thumb should be searched for undue sensitivity and dysfunction of their attachments – described by Lewit (1999) as ‘periosteal pain points’ (PPP) – which are amongst the commonest sites of trigger points, according to Travell & Simons (1992). See Table 4.4 in Chapter 4 for a list of the major PPP.
Duration of treatment
Treatment of the left cervical area should take no more than 2–3 minutes and, in the absence of dysfunction, can be comfortably and successfully dealt with in 90 seconds. Indeed, in its assessment mode, the entire basic spinal NMT treatment can usually be completed in 15 minutes.
Adopting a new position
Once both left and right cervical areas have been treated, the practitioner moves to the head of the table (Fig. 6.5).
• Resting the tips of the fingers on the lower, lateral aspect of the patient’s neck, the thumb tips are placed just lateral to the first thoracic–spinal process.
• A degree of downward (toward the floor) pressure is applied via the thumbs, which are then drawn cephalad, alongside the lateral margins of the cervical spinous processes, searching for irregularities, asymmetries (see TART notes in Chapter 3).
• This bilateral stroke culminates at the occiput, where a lateral stretch, or pull, is introduced across the bunched fibres of the muscles inserting into the base of the skull.
• The upward stroke should contain an element of pressure medially, towards the spinous process, so that the pad of the thumb is pressing downward (towards the floor), whilst the lateral thumb tip is directed towards the centre, attempting to contact the bony contours of the spine, all the time being drawn slowly cephalad to end at the occiput.
• This combination stroke is repeated two or three times.
• The fingertips, which have been resting on the sternomastoid, may also be employed at this stage, to lift and stretch the muscle posteriorly and laterally.
• The lateral stretch, via the thumbs, across the occipital protuberance may be likened to ‘trying to break open a melon’.
• The thumb tips insinuate themselves deep into the medial fibres of the paraoccipital bundle, and an outward stretch is initiated, using the leverage of the arms, as though attempting to ‘open out’ the occiput.
• The thumbs are then drawn laterally across the fibres of muscular insertion into the skull, in a series of strokes culminating at the occipito-parietal junction.
• The fingertips, which act as a fulcrum to these movements, rest on the mastoid area of the temporal bone.
• Several strokes are then performed, by one thumb, or the other, running caudally, directly over the spinous processes, from the base of the skull to the upper thoracic area. Pressure should be moderate and slow.
• Standing in the same position, the left thumb should then be placed on the right lateral aspect of the first thoracic vertebra, and a series of strokes performed caudally, and laterally, as well as diagonally towards the scapula.
• The fingers should be splayed out ahead of the thumb in whichever direction it is travelling, so that the force transmitted via the extended arm can be controlled.
• The fingers act as a fulcrum, with the thumb tip being drawn across the palm, towards the the tip of the middle or little finger.
• The thumb should never lead the hand, nor be solely ‘digging’ or pressing, without the stabilizing and controlling action of the hand, or fingertips, also being in operation.
• A series of strokes, shallow and then deep, is therefore applied from T1 to about T4 or T5, and outwards towards the scapula, and along and across the upper trapezius fibres and the rhomboids.
• The left hand treats the right side, and vice versa, with the non-operative hand resting on the neck or head, stabilizing it.
• Weight transfer to the thumb is achieved, as described previously, by leaning forward.
Trapezius and sternomastoid muscles
Standing at the head of the table, facing caudally, allows the practitioner to access the region of the upper trapezius from above, so to speak. By lowering the angle at which the hand contacts the muscle, perhaps by kneeling or at least by lowering the centre of gravity significantly, and by standing a little to one side of the centre, it is possible to apply a series of sensitively searching contacts into the area of the thoracic outlet (see Fig. 6.5).
• Strokes that start in this triangular depression would move towards the trapezius fibres and through them towards the upper margins of the scapula. A treasure-house of trigger points awaits this searching digit.
• As it is often difficult to apply pressure to the trapezius or sternocleidomastoid muscles in such a way as to involve underlying bony structures, it may be necessary lightly to pinch (flat pincer grip), or squeeze, the more sensitive areas of dysfunction to assess trigger points and their related target areas of pain.
• Several strokes should also be applied directly over the spinous processes, caudally as far down as the mid-thoracic area. Trigger points sometimes lie on the attachments to the spinous processes, or between them.
By referring to the illustrations of trigger points (see Ch. 3, Fig. 3.6), the location of some of the commonest trigger points in this area can be predicted, and their presence rapidly established.
When it is not possible to apply thumb pressure onto such a point, a flat pincer compression (using pads of fingers) of the involved muscle area, instead of direct pressure, using varying pressure as described earlier in this chapter, will usually induce a reduction of the referred pain. Once pain reduces, the pressure should be released. If no success is achieved by these means, one of the other trigger point treatment approaches, as previously outlined in Chapter 3 (see Box 3.5), should be used.
Left-side trunk treatment
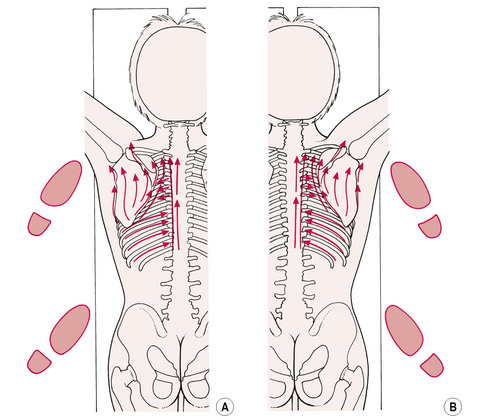
• The practitioner then moves to the patient’s left side and stands in the same manner as at the commencement of the treatment, but at the level of the patient’s waist (see Fig. 6.6A).
• With the right hand now resting at the level of the lower thoracic spine, the left thumb commences a series of strokes in a cephalad direction, from the mid-thoracic area.
• Each stroke covers two or three spinal segments, and runs immediately lateral to the spinous processes, so that the angle of pressure imparted via the medial tip of the thumb is roughly towards the contralateral nipple.
• Again, light assessment and deep therapeutic strokes are employed, and a degree of overlap occurs on successive strokes.
• In this way the first two strokes might run from T8 to T5, followed by two strokes (one light, one deeper) from T6 to T3, and finally two strokes from T4 to T1.
• Deeper and more sustained pressure can be exerted if marked congestion, or resistance to the gliding, probing thumb, is noted.
• In the thoracic area a second line of cephalad strokes may be employed, to include the spinal border of the scapula, as well as one or two searching lateral probes along the inferior spine of the scapula, and across the musculature inferior to, and inserting into, the scapula.
Right-side treatment
Treatment of the right side of the mid and upper thoracic region may be carried out without necessarily changing position, other than to lean across the patient. However, the shorter practitioner should change sides so that, standing half-facing the head of the patient, the right thumb can perform the strokes discussed above.
• Apart from trigger points in the lower trapezius fibres, others may be sought in levator scapulae, supraspinatus and infraspinatus, and subscapularis (by accessing via the axilla).
• The connective tissue zones affecting the arm, stomach, heart, liver and gall bladder are apparent in this region, and neurolymphatic reflexes relating to the arm, thyroid, lungs, throat and heart occur in the upper thoracic spine, including the scapular area (see Chapter 5).
• The intercostal spaces are rich sites of soft tissue dysfunction. The thumb tip, or a fingertip, should be run along both surfaces of the rib margin, as well as in the intercostal space itself.
• In this way the fibres of the small muscles involved will be treated adequately.
• If there is over-approximation of the ribs, a simple stroke along the space may be all that is possible until a degree of normalization has taken place.
• These intercostal areas are extremely sensitive, and care should be taken not to distress the patient.
• In most instances the intercostal spaces on the side opposite that on which the practitioner is standing will be treated using the finger stroke, as illustrated (see Figs 6.2 & 6.6A, B).
• The tip of a finger should be placed in the intercostal space, and gently but firmly brought upwards and around the curve of the trunk towards the spine, feeling for contracted or congested tissues in which trigger points might be located.
Change of position
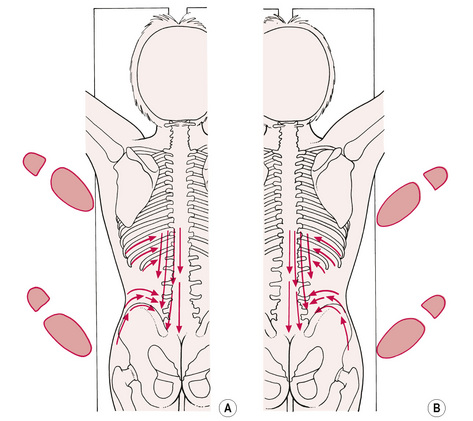
• The practitioner now half turns so that, instead of facing the patient’s head, he or she faces the patient’s feet. The pattern of strokes is now carried out on the patient’s left side by the practitioner’s right hand (see Fig. 6.7A & B).
• A series of strokes, starting from T8 to T11, followed by T11 to L1 and then L1 to L4, is carried out, as previously described.
• Two or more gliding strokes, with the pressure downwards but angled so that the medial aspect of the thumb is in contact with the lateral margin of the spinous processes, are performed at each level.
• The lower intercostal areas are treated in much the same way as described above.
• The practitioner then steps back from the table and glides the thumb, to allow access to a stroke that runs along the superior iliac crest, from just above the hip to the sacroiliac joint.
• Several such strokes may be applied into the heavy musculature above the crest of ilium.
• To treat the opposite side, the practitioner changes sides, so that he or she is facing the patient’s waist and half-turned towards the feet; the left hand can deal with the lower thoracic and upper lumbar area, and the iliac crest, in the manner described above.
• One or two strokes should then be applied, running caudad over the tips of the spinous processes from the mid-thoracic area to the sacrum, searching for attachment trigger points.
The area we have been describing contains a network of reflex areas and points:
1. The tsubo or acupressure points lying symmetrically on either side of the spine and along the midline have great reflex importance. Associated points (see Fig. 4.3) are located alongside the spine.
2. These points are virtually identical to those described in Thai Yoga Massage as Sen back points (or lines). Evans (2009, p58) describes accessing them as follows: ‘To locate these lines we allow the thumbs to feel for the spinous processes of the vertebrae and then let them fall into the two channels either side of the spine. We can follow these channels with our thumbs from the pelvis to the seventh cervical vertebrae, although in practice we usually stop at the lower edge of the scapulae. In general we are following the medial borders of the erector spinae muscles.’
3. The so-called ‘Bladder meridian’ acupuncture points lie in two lines running parallel with the spine, one level with the medial border of the scapula, and the other midway between it and the lateral border of the spinous processes.
4. Goodheart’s work (1987) suggests that rhomboid weakness indicates liver problems and that pressure on C7 spinous process, and a point on the right of the interspace between the 5th and 6th thoracic spinous process, assists its normalization. Latissimus dorsi weakness apparently indicates pancreatic dysfunction. Lateral to 7th and 8th thoracic interspace is the posterior pressure reflex to normalize this. These and other reflexes would appear to derive from Chapman’s reflex theories, and may deserve further study.
5. In general terms, dysfunction of the erector spinae group of muscles, between 6th and 12th thoracic, suggests liver involvement. Similarly 4th, 5th and 6th thoracic area congestion or sensitivity usually involves stomach reflexes and gastric disturbance, whereas T12 and L2 indicate possible kidney dysfunction.
6. Connective tissue zones (see Ch. 5) relating to the stomach, head and lower limb circulation, are located in this region.
7. Jones’ tender points (see Ch. 4, Fig. 4.5B in particular) in this region may relate to extension strains.
Left hip position
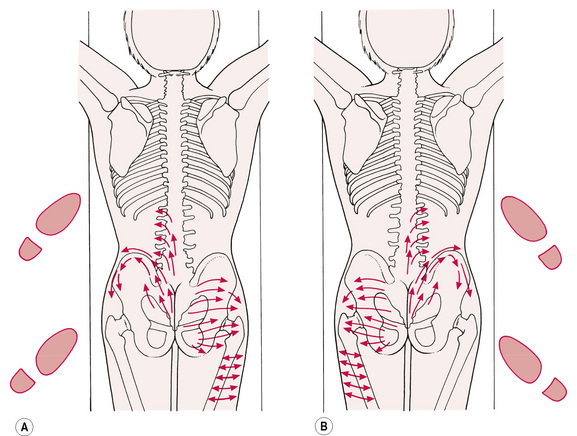
The next treatment position requires the practitioner to stand at the level of the patient’s left hip, half-facing the head of the couch:
• The left hand and thumb describe a series of cephalad strokes from the sacral apex towards the sacroiliac area, and then laterally along the superior and inferior margins of the iliac crest to the insertion of the tensor fascia lata at the anterior, superior iliac spine (see Fig. 6.8A,B).
• A further series of short strokes of the thumb upwards and laterally in the lumbar area may be described as attempting to stretch the paraspinal muscles away from the spine, notably the sacrospinal group.
• Having treated both left and right sides of the lumbar spine, as above, the practitioner uses a series of two-handed gliding manoeuvres, in which the hands are spread over the upper gluteal area laterally, the thumb tips are placed at the level of the second sacral foramen with a downward (towards the floor) pressure; they glide in a cephalad direction, and slowly laterally, to pass over and through the fibres over the sacroiliac joint. This gliding stroke is repeated several times. (Note: the arrow directions on the figures are not meant to be definitive; for example, these strokes could be performed with the thumbs moving caudad, rather than cephalad, as illustrated).
• Still standing on the left, the practitioner leans across the patient’s upper thigh and engages the right thumb on to the ischial tuberosity.
• A series of gliding movements is carried out from that point, laterally to the hip and caudally, towards the gluteal fold.
• A further series of strokes, always applying deep, probing but variable pressure, is then carried out from the sacral border, across the gluteal area, to the hip margins. The fingertips during these strokes are splayed out so that they can guide and balance the hand and thumb movement.
• In these deep muscles the line of the thumb’s direction is more towards the tip of the index finger, or middle finger, rather than to the little fingertip, as it was in the cervical area.
• In deep, tense gluteal muscle, the thumb may be inadequate to the task of prolonged pressure application, and the elbow may be used to sustain deep pressure, for minutes at a time if necessary (see notes on the use of elbow in Ch. 8). Care should be taken, however, as the degree of pressure possible via the elbow is very great, and tissue damage and bruising can result from its careless use.
The practitioner then moves to the right side, repeating the strokes as described. Alternatively, rather than changing sides, the practitioner may lean across the patient, using hooked finger strokes to access the tissues above the hip, and around the curve of the iliac crest effectively.
Trigger points, connective tissue zones and neurolymphatic reflexes that may be involved in the lower lumbar and gluteal areas are shown in Box 6.2.
Box 6.2 Trigger points, connective tissue zones and neurolymphatic reflexes of the lower lumbar, gluteal and lateral thigh areas
• The trigger points that are found in the lower lumbar and gluteal areas include those in the following muscle groups: iliocostal, multifidus, longissimus, gluteus medius and gluteus minimus (see Fig. 3.6 for illustrations of many of these).
• The connective tissue zones that may be involved include those that involve arterial and venous disturbance to the legs, constipation, liver, gall bladder, heart and bladder (see Fig. 5.3).
• The neurolymphatic reflexes, located in this area, include those involving the following areas and conditions: the appendix, haemorrhoids, female generative organs, vasculitis, sciatic nerve, abdominal tension and constipation, prostate, colitis, kidneys, adrenal glands, digestive system, pancreas, liver, spleen and gall bladder. The TFL contains neurolymphatic reflexes to the groin glands, the broad ligaments, spastic constipation and colitis, and the prostate (see Ch. 5).
Lateral thigh and gluteal structures
Having treated the low lumbar area and the gluteals, the practitioner might usefully include a series of strokes across the fibres of the tensor fascia lata (TFL), from the hip area to the lateral knee area.
The tensor fascia lata contains neurolymphatic reflexes to the groin glands, the broad ligaments, spastic constipation and colitis, prostate, etc., and is itself a major contributor to knee, pelvic and low back problems via its influence on the mechanics of the region. It is commonly extremely sensitive to pressure, and care is needed to prevent patient distress in treating it. (See also Alternative methods for treating TFL in Chapter 8.)
Completion of treatment
This completes the basic spinal NMT treatment, apart from any manipulative, mobilization or additional soft tissue procedures that might be indicated or thought desirable.
• Boris Chaitow completed the spinal treatment by standing at the head of the table, leaning over the patient’s upper thoracic area, with the palms of both hands totally in contact with the upper lumbar region so that the thenar eminences were resting on the paraspinal musculature, and the fingers pointing laterally.
• The heel of the hand imparted the main contact, laterally.
• A series of gliding strokes was performed, with the hands rhythmically alternating with each other, so that, as the right hand stroked downwards towards the end of its movement on the gluteals, the left was being brought back to the lower thoracic area.
• After the right hand reached the gluteal region, it was brought back to the start.
• In this way a series of 10 to 20 deep, rhythmic, strokes was carried out, in order to stimulate local circulation and drainage, as well as to help relax the patient, who may well have tensed during the NMT treatment of the lumbar and gluteal areas.
• As stated previously, the basic ‘assessment’ treatment should take no more than 15–20 minutes; however, far longer may be needed if whatever is found, of a dysfunctional nature, were to be treated.
The patient should have a sense of release from tension, and a sense of well-being lasting for some days. Many feel a sense of tiredness, and a great desire to sleep; this should be encouraged. Pain may result in those areas that have borne the brunt of the deeper pressure application, and this should be explained to the patient, who should be encouraged to note any changes in his or her condition, and to report these at the subsequent visit, or by phone/email.
The frequency of application of NMT will vary with the condition. In chronic conditions, one or two treatments weekly are all that is required, for several weeks, or until progress dictates that the interval be lengthened. In acute conditions, treatment may be much more frequent (but almost always less invasive): daily if possible until ease is achieved. Of necessity, this must depend upon what other modalities are employed.
Baldry P. Myofascial pain and fibromyalgia syndromes. Edinburgh: Churchill Livingstone, 2001.
Chaitow L. Integrated neuromuscular inhibition technique. British Journal of Osteopathy. 1994;13:17-20.
Chaitow L. Muscle energy techniques, ed 2. Edinburgh: Churchill Livingstone, 2001.
Chaitow L. Muscle energy techniques, ed 3. Edinburgh: Churchill Livingstone, 2006.
Dowling D. Progressive neuromuscular inhibition technique (PINS). J Am Osteopath Assoc. 2000;100(5):285-298.
Dvorak J., Dvorak V., Schneider W. Manual medicine therapy. Stuttgart: Georg Thieme, 1988.
Evans H. A Myofascial Approach to Thai Massage. Edinburgh: Churchill Livingstone, 2009.
Goodheart G. Applied kinesiology workshop procedure manuals 1976–1987. Detroit: Published privately, 1987.
Kostopoulos D., Rizopoulos K. Effect of topical aerosol skin refrigerant (Spray and Stretch technique) on passive and active stretching. Journal of Bodywork and Movement Therapies. 2008;12(2):96-104.
Lewit K. Manipulation in rehabilitation of the motor system, ed 3. London: Butterworths, 1999.
Lowe J-C., Honeyman-Lowe G. Ultrasound treatment of trigger points: differences in technique for myofascial pain syndrome and fibromyalgia patients. Medecine du Sud-est. 1999:12-15. April–May–June, no. 2
McMakin C. Microcurrent treatment of myofascial pain in head, neck and face. Topics in Clinical Chiropractic. 1998;5(1):29-35.
Rolf I. Rolfing – integration of human structures. New York: Harper & Row, 1977.
Simons D. Understanding effective treatments of myofascial trigger points. Journal of Bodywork and Movement Therapies. 2002;6(2):81-88.
Sola A., Bonica J. Myofascial pain syndromes. In: Bonica J.J., editor. The Management of Pain 1. ed 2. Philadelphia: Lea and Febiger; 1990:354.
Travell J., Simons D. Myofascial pain and dysfunction: the trigger point manual. vol 2. Baltimore: Williams & Wilkins; 1992. the lower extremities