CHAPTER 24 Dermatomes
What is a dermatome?
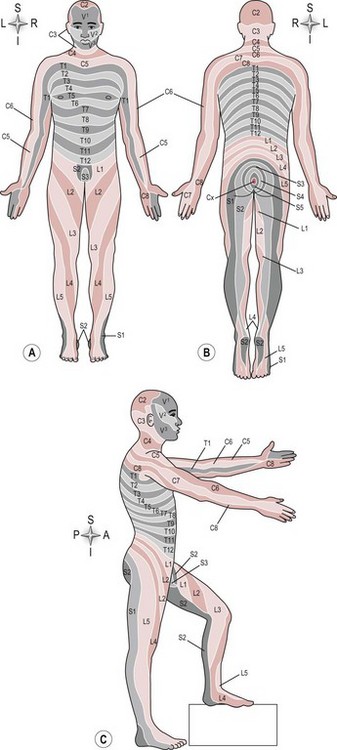
A dermatome is defined as the area of skin supplied by one spinal nerve root level. There are 31 pairs of spinal nerves leaving the spinal cord (S2.13) and each one supplies a different area of skin. Therefore the skin supplied by all the individual spinal nerve roots ultimately produces a dermatome map that represents the entire body (Fig. 24.1).
Why do I need to assess dermatomes?
Assessing a dermatome gives information related to nerve integrity, in other words whether the nerve pathway from the skin to the spinal cord is intact. Knowledge of the cutaneous supply of both the spinal nerve root (dermatome) and the peripheral nerve allows the therapist to differentiate between lesions of each (Petty 2006). For example, a sensory loss of the area over the deltoid muscle at the shoulder is identified as dermatome C5. The same area of skin is also part of the sensory distribution of the radial nerve (posterior cutaneous nerve of the arm C5/6/7/8 T1). It is therefore likely, but not certain that the lesion is at the level of the spinal nerve root because a lesion of the peripheral nerve is likely to be more extensive. Accurate diagnosis is only possible with knowledge of anatomy and accurate assessment.
 Caution
Caution
A sensory loss related to a single dermatome may be indicative of a lesion at the spinal nerve root but must be confirmed by a similar finding for that particular root level for myotomes (S3.31) and reflexes (S3.22).
In terms of neurologically impaired patients, the clinical presentation of any sensory loss only requires assessment using a dermatome distribution when there is involvement of either the spinal cord specifically or the peripheral nervous system, e.g. in spinal cord injury (SCI) and Guillain–Barré syndrome (GBS). As neither of these pathologies affects the spinal nerve root in isolation, dermatome testing is less clinically useful as a diagnostic tool, however it is a very useful way of mapping the sensory loss. The map produced gives the therapist a highly relevant outcome measure by which the extent and level of sensory loss can first be estimated and then re-evaluated. This is especially important in recovering conditions such as GBS and in SCI, where a rising level of sensory loss may reflect a serious deterioration of the injury.
How do I assess a dermatome?
Patient
To complete a dermatome assessment, the therapist needs to access the patient’s skin over the trunk, upper and lower limbs, both anteriorly and posteriorly. This will require a change of position. For the patient’s comfort the therapist could start the assessment in supine and move to prone.
Therapist

 Clinical hints and tips
Clinical hints and tipsRecording
Record any loss of sensation or abnormal sensation for each dermatome. Traditionally, the findings are recorded on a body chart with shaded areas used to represent areas of skin with abnormal sensation. Different sensations will require different shading design and hence a key to ensure the findings are clear to another clinician. This mapping should be completed accurately so that any increase in the area (condition worsening) or decrease in the area (condition improving) can be identified.
Analysis
If the tests indicate a specific area of loss, a spinal nerve root deficit may be suspected and may be confirmed by comparing any abnormal findings for the same root level for myotome testing and reflexes. If the loss is widespread the lesion is likely to be more generalized to the peripheral nervous system and can be used to identify the extent and level of a lesion.