Chapter 13 The history of respiratory physiology
 That breathing was essential for life was clear to the ancient Egyptian civilisations 5000 years ago, but the reasons for this were unknown. Early explanations for the function of breathing involved the air drawn into the lungs fuelling combustion in the heart, and removing ‘sooty and fuliginous spirits’ from the body. In the Renaissance, advances in knowledge of anatomy led to the discovery of the pulmonary circulation and the observation that blood changed colour on passing through the lungs.
That breathing was essential for life was clear to the ancient Egyptian civilisations 5000 years ago, but the reasons for this were unknown. Early explanations for the function of breathing involved the air drawn into the lungs fuelling combustion in the heart, and removing ‘sooty and fuliginous spirits’ from the body. In the Renaissance, advances in knowledge of anatomy led to the discovery of the pulmonary circulation and the observation that blood changed colour on passing through the lungs.The historical path along which we have gained our current knowledge of respiratory physiology is long and varied. There are periods when our understanding leapt forward in just a few years, interspersed by prolonged periods when progress was negligible, and even some periods when progress was reversed. That breathing is essential for life was clear from the beginnings of history, but the mechanism of breathing and the reasons for it remained elusive for many centuries. Progress usually occurred in parallel with understanding in other scientific disciplines, particularly chemistry, physics and anatomy. Innovative ideas on the physiology of breathing led, in more than one instance, to the premature death of the physiologist, and the history of respiratory physiology includes some of the most famous controversies seen in medical science.
This chapter is of necessity only a brief overview of the subject, and ends around 100 years ago, when the explosion of scientific progress makes the subject too large for such a short account. Significant advances in respiratory physiology in the last 100 years are reported in the other chapters of this book, and the reader interested in the history of this period is referred to more authoritative accounts.1,2,3 For more general information on the history of respiratory physiology numerous recent sources (by historical standards) are available.4,5,6
Ancient Civilisations
Egyptian Physiology7
Ancient Egyptian civilisations existed from around 3100BC to 332BC when the Graeco-Roman period began. The most remarkable contribution made to history by ancient Egyptians is their writings, though knowledge of their language was mostly lost after 500AD. Approximately 1300 years later, 19th century scholars were able to use the Coptic language to assist in translating the ancient Egyptian writings. This has allowed an insight into medical knowledge from as early as 1820BC, the date of the earliest known medical writings in the Kahun papyrus.
Medical papyri. Many Egyptian papyri are concerned with medical topics, mostly descriptions of pragmatic ‘recipes’ for the treatment of a multitude of specific conditions.7
The longest and best known of the medical papyri is the Ebers Papyrus,8,9 which dates from about 1534bc, and is accepted as being a compilation of various earlier works. The Ebers Papyrus is unique in containing a section on physiology, including comments on respiration. The overall purpose of respiration is described thus:
As to the air that penetrates into the nose. It enters into the heart and the lung. They are those which give air to the entire body.9
Further sections include detailed descriptions of specific numbers of metu conducting ‘moisture and air’ to many parts of the body. These metu seem to mostly relate to blood vessels but also probably included such structures as tendons, muscles and the ureters. At first, this primitive view of anatomy is surprising considering the embalming abilities of ancient Egyptians, though in practice, embalming was carried out using very small inconspicuous incisions that would have revealed very little internal anatomy. Two metu are described to each ear, through which ‘the breath of life enters into the right ear and the breath of death enters into the left’,9 illustrating the ‘magical’ aspect of medicine at the time.
Ancient Greece
Greek writers were primarily philosophers, but they were also outstanding physicians, with one of their number, Hippocrates, forming a school that is now widely attributed with the foundation of modern medical conduct. Early Greek philosophers such as Anaximenes (570bc–?) clearly stated that ‘pneuma’ or air was essential to life,6 but in contrast to this correct observation, Alcmaeon reportedly claimed that goats breathed through their ears and that some air passed from the nose directly to the brain.4 Empedocles (495–435bc) disputed many of Alcmaeon’s writings, suggesting instead that breathing occurred through the skin, and that blood flow from the heart was tidal in nature, ebbing and flowing to and from the heart. Empedocles successfully combined physiology and philosophy in his description of the ‘innate heat’ in the heart, which was closely related to the soul, and which was distributed throughout the body by the heart. This concept of heat generation within the heart gained acceptance throughout the ancient Greek period, and was to remain at the centre of respiratory physiological ideas for about 1000 years.
The writings of Plato, Aristotle and the Hippocratic school only rarely directed their attention to respiration, but their contribution to scientific method and thinking was enormous. Subsequent philosopher-physicians adopted a more scientific approach to investigating physiology. At this time, dissection became widely practised, sometimes in public, and on both animals and humans. Animal vivisection also undoubtedly took place, and there are even disputed reports of human vivisection of criminals.4 Herophilus (circa 325bc) distinguished between arteries and veins, and, along with Aristotle, asserted that they contained air. Erasistratus (304–250bc), more widely renowned as the father of philosophy, was the first to apply scientific principles to explain breathing. His view was that air was taken into the lungs and passed to the heart along the pulmonary artery. In the heart, air was converted into a ‘vital spirit’ that was distributed to all parts of the body by the arteries, whilst the brain further converted the vital spirit into ‘animal spirit’ which travelled down the hollow nerves to activate muscles. Erasistratus seemed to understand that heart valves only allowed flow to occur in one direction, but failed to apply this knowledge to elucidate the transport of vital spirit or blood around the body. After Erasistratus, Greek interest moved away from medicine to philosophy and the physical sciences, and the progression of physiological knowledge halted for about 400 years.
Roman Medicine and Galen (129–199AD)
By the age of 28 years Claudius Galen was physician to the gladiators of Pergamun, and 12 years later became physician to the Roman emperor Marcus Aurelius. He wrote many works on anatomy and physiology, many of which still exist in modern form including two with much material on respiration On the usefulness of the parts of the body and On the use of breathing.10,11 Galen’s work provides the first direct evidence of experimentation and the application of clinical observations to explain physiology.
Galen’s system of physiology and anatomy. In Galen’s descriptions, food was processed in the gut before being used by the liver to produce blood, which passed to the right heart. Much of this blood flowed into the pulmonary artery to nourish the lung, whilst the remainder passed across invisible pores in the inter-ventricular septum, to be combined with ‘pneuma’ brought from the lung via the pulmonary vein (Figure 13.1). In the left heart, the pneuma instilled the blood with vital spirit that was circulated to the body and brain as described by Erasistratus.
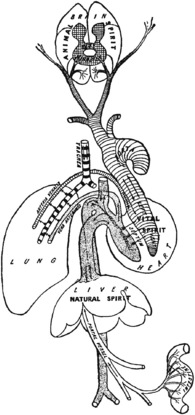
Fig. 13.1 Illustration reconstructing Galen’s scheme of cardiovascular and respiratory physiology as described in the text.
Galen did not use illustrations in his writings; this diagram is taken from reference 12.
Anatomically Galen regarded the lungs as having three types of intertwining vessels, the pulmonary artery, pulmonary vein and the ‘rough artery’ (trachea). On respiratory mechanics, Galen regards the ribs as primarily providing protection for the intra-thoracic organs, particularly the heart, but he also clearly describes the role of the intercostal muscles and diaphragm in effecting both inspiratory and expiratory movements. He understood the potential problems of diaphragmatic splinting, describing respiration as ‘little and fast’ in such conditions as pregnancy and ‘water or phlegm in the liver’.
Experiments on respiration. Galen’s experiments provided mixed results:
‘Covering the mouth and nostrils of a boy with a large ox-bladder, or any such vessel, so that he was unable to draw breath at all outside it, we saw him breathing unhindered through a whole day’.
Galen’s conclusion from this study is contradictory: ‘Hence it is clear that the arteries all through the animal draw in the outer air very little or not at all’. Modern views of this experiment are that the ox-bladder was unlikely to be air tight, or that Galen’s assistants must have removed the bladder to allow the boy to breathe easily when their master was not directly supervising the experiment.11
The functions of breathing. Apart from providing pneuma to the heart, Galen described other functions for breathing:
Galen’s legacy. Galen was the first physician to apply the Hippocratic method of scientific thinking to physiology, and he ingeniously combined the knowledge of his predecessors with his own thinking to produce an impressive treatise on the workings of the human body. Also, it is from the writings of Galen that we have obtained our knowledge of many of his predecessors: most of what is known of Erasistratus’s views on physiology is derived from Galens’ comments on it. Galen’s work also deserves a place in history as the longest unchallenged scientific work. The physiology described in this section was taught in medical schools throughout the world, and scientifically mostly unchallenged, for around 1400 years.
There was also a darker and more controversial side to Galen. He is widely believed to have been conceited, dogmatic and abusive of those criticising him.6 On the usefulness of the parts of the body contains several prolonged and personal refutations of the ideas of his predecessors, for example, accusing ‘Asclepiades, wisest of men’ of making errors ‘no child would fail to recognise, not to mention a man so full of his own importance’.
After Galen
When Galen died, the study of physiology and anatomy effectively ceased. The Roman Empire was in decline, and in 389AD Christian fanatics burned down the library in Alexandria, which contained many writings by the Greek philosopher-physicians.
Preservation of knowledge now fell to scholars of the Byzantine and Arabic empires. The latter embraced Galen’s ideas with enthusiasm and translated many Greek works into Arabic, almost certainly adding their own refinements as they did so. The greatest of these Arabic scholars was Avicenna (circa 980–1037) whose canon was an impressive document pulling together and classifying all the available medical knowledge of the time, creating what has been described as a popular medical encyclopaedia of the medieval period. Some years later, Ibn Al Nafis13 (1210–1288), a prolific Arabic writer on many subjects, studied Avicenna’s writings and wrote his own treatise Sharh Tashirh Al-Qanun (Commentary on the Anatomy of the Canon of Avicenna). In this he challenged Galen’s scheme of pores in the inter-ventricular septum through which blood passed, and instead suggested that blood passed through the lung substance where it permeated with the air.5,13 This was an early breakthrough in explaining the true nature of the pulmonary circulation, but Ibn Al Nafis’ work did not become well known for many more centuries.
The Renaissance
In the 12th and 13th centuries, scholastic pursuits began again with the foundation of many European universities, firstly Oxford, Cambridge and Bologna closely followed by Paris, Naples and Padua. Soon, many of the ancient documents were translated from Greek or Arabic into Latin, and human dissection began to be performed after many centuries of interdiction by the Pope. Knowledge of anatomy again began to advance, though interest in the function of the body only began again with Leonardo da Vinci in the 15th century.
Leonardo Da Vinci (1452–1519)4
Leonardo exemplified the Renaissance trend for combining art with science. His anatomical drawings are both extensive and ingenious, being mostly surrounded by extensive explanatory notes.14,15 These notes are written in Latin and in mirror writing, possibly simply because Leonardo was left-handed and received no formal schooling to correct this, or possibly to make his notes harder to read by uneducated persons described by him as ‘bad company’.4
Although Leonardo is known to have dissected over 30 human cadavers, most of his drawings of the respiratory system are based on dissections of animals, including Figure 13.2 showing in beautiful detail the structure of the pig lung. In the commentary on this drawing, Leonardo considers the use of the ‘substance’ of the lung and extends Galen’s protective function of the lung parenchyma when he states that ‘the substance is interposed between these ramifications [of the trachea] and the ribs of the chest to act as a soft covering’. Structures entering the chest cavity are labelled a–e and their functions described:
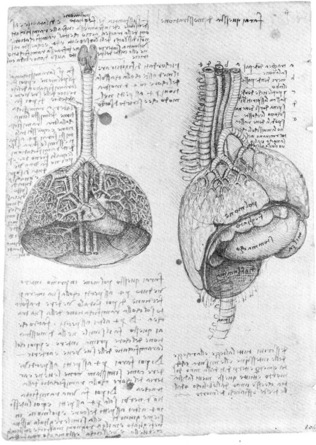
Fig. 13.2 Leonardo’s drawing of the thoracic organs of a pig (c. 1508). The organs are labelled in mirror writing in Latin: polmone, lung; feghato, liver; milza, spleen; stommacco, stomach; djaflamma, diaphragm; spina, spine. See text for an explanation of labels a–e above the drawing on the right.
(The Royal Collection © 2010, Her Majesty Queen Elizabeth II.)
Leonardo adhered to other Galenic ideas such as the presence of air in the pleural space, but was unsure how the air entered or left this space, and in his later drawings he was clearly beginning to doubt that air was always present. Leonardo’s adherence to Galen’s ideas was in some areas unshakable, in particular his depiction of the inter-ventricular pores in several drawings of the cardiovascular system.
He did however challenge some Galenic ideas by application of his engineering expertise. For example, he did not accept that the heart generated innate heat, instead writing that heat generation in the heart resulted from mechanical friction between the blood and the walls of the heart.4 Similarly, his engineering knowledge made him intrigued by the actions of the chest wall and respiratory muscles, including the complexities of defining the different function of internal and external intercostal muscles. For the diaphragm, Leonardo described four functions – dilating the lung for inspiration; pressing the stomach to drive food into the intestine; contracting with the abdominal muscles to drive out abdominal superfluities; and to separate the spiritual (thoracic) organs from the natural (abdominal) ones. Finally, he considered in detail the movements of the trachea and bronchi on breathing, showing them to dilate and open wider at branches on inspiration as shown to the right of Figure 13.3.

Fig. 13.3 Leonardo’s drawing of the pulmonary circulation in relation to the bronchi (c. 1513). Pulmonary vessels arise from several parts of the heart, leading Leonardo to propose a dual blood supply to the lung. Coronary arteries and veins can be clearly seen on the heart. At the lower end of the main drawing, Leonardo has drawn a small circle containing the letter N. The notes describe the structure as having ‘a crust, like a nutshell’ containing a ‘dust and watery humour’ possibly representing his discovery of a lung cyst16 or a tuberculous cavity.14
(The Royal Collection © 2010, Her Majesty Queen Elizabeth II.)
Leonardo and the bronchial circulation. In Figure 13.3, Leonardo depicts in detail the relationship of the pulmonary circulation to a bronchus. Much of the commentary in the drawing is concerned with the superiority of drawings rather than words to describe such anatomical configurations. The figure clearly shows a dual blood supply to the lung, and suggests that the smaller of these two supplies is to ‘nourish and vivify the trachea’. From this drawing, many writers have credited Leonardo with discovering the bronchial circulation, though this claim is disputed.16,17 The drawing is believed to be based on an ox, a species recently shown to have distinct small pulmonary veins draining directly into the left atrium, which may be those found by Leonardo.
The possibility of artistic license in his drawings has caused disputes that will never be resolved, such as that of the bronchial circulation. For example, in Figure 13.2 the perfectly branching pattern of the bronchi on the lung surface is clearly not based on true observation of pig lungs. In Figure 13.3 of ox lungs, the right upper lobe bronchus that arises directly from the trachea in this species is absent. However, in spite of these misgivings regarding his drawings, Leonardo’s genius in combining art, science and engineering in the study of physiology is undisputed.
Anatomy in the Renaissance
After Leonardo, the pursuit of medical knowledge in the universities continued, with anatomy in particular aided by the continuing resurgence of dissection and vivisection. Andreas Vesalius (1514–1564) is primarily remembered as the founder of modern anatomy, his dissections culminating in the publication in 1543 of De Humanis Corporis Fabrica, a book of seven volumes including over 250 anatomical illustrations (Figure 13.4).18 His ideas met with resistance from his contemporaries whenever his views were at odds with those of Galen, and this eventually forced Vesalius to cease his study of anatomy and to return to work as a physician. Nevertheless, the Fabrica continued to gain acceptance and became the foundation for future anatomy texts. Vesalius was also a skilled physiologist. He was the first to describe an experiment reproduced much later, in which a section of the chest wall of an animal was carefully removed without breaching the pleura beneath, so enabling direct observation of lung movements through the transparent pleura.6
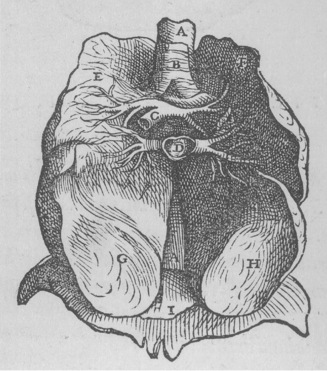
Fig. 13.4 Figure from Book VI of Vesalius’s Fabrica,18 showing an anterior view of the lungs after removal of the heart. A, oesophagus; B, trachea; C, pulmonary artery; D, pulmonary vein; I, diaphragm. E–H refer to the lobes of the lung – Vesalius’s illustrations always showed each lung to have four lobes.
(Reproduced by permission of the Special Collections, Leeds University Library.)
The pulmonary circulation.19 Unaware of the earlier writings of Ibn Al Nafis, Servetus (1509–1553), in his religious treatise Christianismi restitutio,20 again challenged the existence of Galen’s interventricular pores. He wrote that rather than passing through the middle wall of the heart, ‘blood is urged forward by a long course through the lung … and is poured from the pulmonary artery to the pulmonary vein’.21 He also commented that on passing through the lung the blood changed colour, becoming ‘reddish-yellow’, though an explanation for this observation was still two centuries away. Tragically, Christianismi restitutio was deemed to be heretical by the Christian church, and the book, along with its author, was burned at the stake in 1553. Only three copies of Christianismi restitutio are believed to exist today,21 though more recent reprints are available.22
Just a few years later, Realdus Colombo (1516–1559) became the third physiologist to apparently independently describe the pulmonary circulation. Colombo, a pupil of Vesalius, posthumously published his account of anatomy, De Re Anatomicae, in which he clearly describes blood flowing through the lung whilst mixing with air.23 There is a suspicion that Colombo had previously had access to Servetus’s Christianismi restitutio, or that he knew of the writings of Ibn Al Nafis from 300 years earlier, causing confusion as to which of these eminent physiologists should be credited with the discovery of pulmonary blood flow.5,19
Experimental Physiology in the 17th Century
At the start of the 17th century the dominance of Italian universities with respect to medicine and anatomy subsided, and progress in the understanding of respiration moved to England, where a new approach of experimental philosophy was developing.4
Discoveries to Assist the Respiratory Physiologists
Circulation. William Harvey (1578–1657) studied at Cambridge and Padua Universities, so was well placed to combine the Italian methods and knowledge of anatomy with the English approach of physiological experimentation engendered by Francis Bacon. The most notable of Harvey’s teachers in Padua was Hieronymus Fabricius, who is credited with the discovery of the venous valves, including the simple demonstration in arm veins that valves prevent blood from flowing distally. In 1616 Harvey first presented his ideas of the blood circulating continuously in a lecture to the College of Physicians in London. After a further 12 years of experimentation, Harvey published De Motu Cordis, in which he describes the circular motion of the blood in both the lesser (pulmonary) and greater (systemic) circulation.24,25 Harvey’s comments on respiration in De Motu Cordis are sparse, and though he refers in several places to a future separate treatise on respiration, it seems this was never written.
Atmospheric pressure.4 The Italian physicists Berti and Torricelli, both of whom were acquainted with Galileo, accidentally discovered air pressure in their search to create a vacuum. First Berti, with a water barometer built of lead pipe attached to his house in Rome, measured the height of the water column at 27 feet. Torricelli and a mathematician colleague Vivianni then made the first mercury barometer using mercury in a glass tube inverted over a bowl of mercury, and so allowed the height of the column to be visualised.
The microscope. Harvey and his numerous pre-decessors who described blood flowing through the lung tissue were not able to determine by what route this occurred or how the blood and air were mixed. Harvey thought it most likely that the blood and air came into contact through pores in the lung structures. Marcelus Malpighi (1628–1694) used a primitive microscope to observe lung tissue. His original communication in 1661, De Pulmonibus,26,27 consisted of two letters to his friend Borrelli who was a professor of science in Pisa.5 Malpighi used frogs for his studies, and describes in detail the lung preparations used, remarking that he had ‘destroyed almost the whole race of frogs’ in the course of his work.27 He described lung tissue to be ‘an aggregate of very light and very thin membranes, which, tense and sinuous, form an almost infinite number of orbicular vesicles and cavities, such as we see in the honeycomb of bees’. This first description of the alveoli was accompanied by a drawing of his preparation (Figure 13.5), and he went on to describe how the vesicles were all terminations of branches of the bronchi, and that under normal circumstances the blood and air were separated by them.
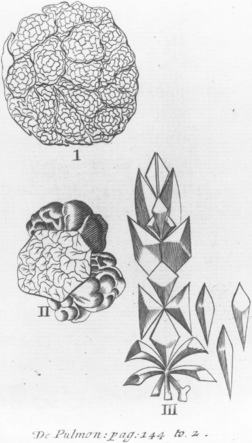
Fig. 13.5 Drawing of Malpighi’s preparation of frog lungs.26 I, Seen from the surface of the lungs; II, showing the cut surface of the lung (including blood vessels on the surface of the vesicles [alveoli]); III, a schematic representation of the branching of the bronchi into vesicles.
(Reproduced by permission of the Special Collections, Leeds University Library.)
The mystery of the structure of lung tissue was now solved. Blood flowed from the right heart to the lung, through Malpighi’s ‘smallest of vessels’ past the air containing vesicles, and returned to the left heart. However, scientists were still no closer to discovering the purpose of this elaborate arrangement.
The Oxford Physiologists and the ‘Use of Breathing’1,5,6
In the mid-17th century a remarkable group of scientists happened upon each other in London, where the group held meetings to exchange ideas and discuss scientific topics, often holding the meetings in their lodgings. The group was initially referred to by its members in London as the ‘Invisible College’ but later, in Oxford, became the ‘Experimental Philosophy Club’. After around 15 years in existence the club was granted a royal charter by the King and formed the Royal Society of London. Of the numerous notable club members, four are worthy of particular note here in view of their contribution to knowledge of respiration.
Robert Boyle (1627–1691).28 Assisted by Hooke, Boyle constructed a ‘new pneumatical engine’ that was capable of pumping air out of closed containers to produce a vacuum. He soon demonstrated that flames were extinguished and animals died in the vacuum, and so began to believe there was some vital component present in air that was necessary for both combustion and animal life. Other experiments led Boyle away from the truth about the purpose of respiration. Enclosing a candle and a chick together, he observed that the chick survived much longer than the flame, indicating that combustion and respiration were different. Similarly, using a mercury gauge, observations that the pressure within closed vessels did not change when animals expired led Boyle to believe that the vital component was present in only tiny amounts. For a scientist so dedicated to experimentation, Boyle was often considered to be poor at interpreting their results,4 often leaving this important task to his close friend Robert Hooke.
Robert Hooke (1635–1702).29 A crucial partnership between Hooke and Boyle brought about the studies described in the previous paragraph. However, Hooke is best known in the area of respiration for a dramatic demonstration to the Royal Society in 1667.30 Keeping animals alive by artificial ventilation with bellows had been demonstrated many times before by both Leonardo da Vinci and Vesalius. However in Hooke’s demonstration, he used two pairs of bellows to provide a constant stream of air and ventilated a dog with part of the chest wall removed, and with ‘numerous small holes pricked in the outer coat of the lungs’ (pleura). With this experiment he achieved successful apnoeic ventilation for well over an hour, and so conclusively demonstrated that ‘bare motion of the lungs without fresh air contributes nothing to the life of the animal’.
Richard Lower (1631–1691). Lower performed many animal experiments to investigate the known colour change of blood on exposure to air. Firstly he proved that the colour change occurred within the lungs, rather than in the heart, demonstrating the colour difference between blood from the pulmonary artery and vein. He then proceeded to show that the colour change occurred only when air was present within the lung, by, for example, ceasing artificial respiration of an animal and observing that blood in the pulmonary vein quickly turned blue.
John Mayow (1641–1679).4 Mayow was the youngest of the Oxford physiologists, having studied with Lower and worked as Boyle’s laboratory assistant. His major work on respiration, Tractatus Quinque Medico-Physici,31 was published in 1674, a few years after Boyle, Lower and Hooke had moved on from their studies of respiration. Tractatus Quinque was an impressive treatise, bringing together in a single book the ideas of Mayow’s eminent colleagues, supplemented with his own experimental work and ideas on chemistry and the physiology of respiration. His many experiments were illustrated with a single page drawing containing six figures (Figure 13.6). Mayow again showed that animal respiration and combustion had similar effects on the volume of air within the enclosed glasses. By good fortune, Mayow found a much greater change in volume than Boyles pressure changes. Mayow’s use of water, and observations over a longer time period, allowed the carbon dioxide to be absorbed into the water and the temperature within the vessel to return to ambient. This led him to extend Boyle’s ideas that air contained a vital component, which he named nitro-aerial spirit. When breathed in by animals nitro-aerial spirit combined with salino-sulphureous particles in the blood to produce a ‘fermentation’, which ultimately gave rise to muscular contraction. This last observation occurred from Mayow’s appreciation of increased breathing during exercise.
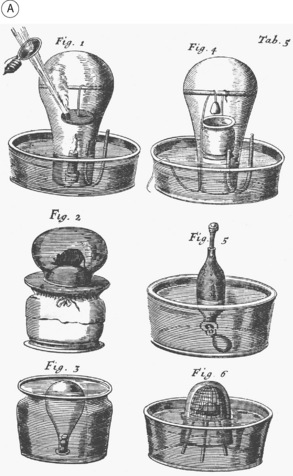
Fig. 13.6 Illustration of Mayow’s experiments on respiration.31 A, Combustible materials, ignited by a magnifying glass and the sun’s heat (Fig. 1) or animal respiration (Fig. 6) cause the water to rise within the enclosed glass, or a moistened bladder to be drawn into the glass (Fig. 2). Chemical reactions were instituted within the closed glasses by for example adding iron to spirit of nitre (Fig. 4) directly or leaving globules of iron in the base of a glass in contact with diluted spirit of nitre. Fig. 5 shows Mayow’s system for transferring air from one glass to another. B, drawing of the bladder in the bellows to demonstrate the passive expansion and contraction of the lungs by the chest wall.
Tractatus Quinque also contains excellent sections on respiratory mechanics. Mayow clearly understood that lung movement was brought about only by expansion and contraction of the chest wall. He demonstrated this by placing a bladder within a pair of bellows fitted with a glass window to allow observation of the bladder inflating and deflating as the bellows were worked (Figure 13.6B). Mayow then applied his knowledge of physiology to pathology, by explaining that difficulty in breathing occurs if the abdominal contents resist the descent of the diaphragm, a situation seen with over-eating, enlarged abdominal viscera, orthopnoea and even in the ‘hysteric passion’. He fully understood the problems of pneumothorax, giving advice to his surgical colleagues:
Here, by the way, surgeons should be warned not to close the wound if the chest has been perforated except when the thorax is contracted to the utmost; for, otherwise, if the opening made by the wound is closed when the chest cavity is expanded it will be impossible for the chest to contract on account of the resistance of the air inside, or for the lungs to expand, except partially, and, in consequence, suffocation will occur.
Tractatus Quinque was controversial soon after it was written, with Mayow being accused of failing to acknowledge his use of other people’s ideas, and ‘clogging the work with absurd additions of his own’. The work was rarely referred to by his peers, and remained obscure for over a century. In particular, it is likely that the chemists of the following century (see below) who discovered oxygen were completely unaware of Mayow’s work.
Physiology Hibernates
After the death of Mayow, the study of respiratory physiology again halted, this time for about 100 years. The other Oxford scientists had already moved on to different pursuits such as physical chemistry (Boyle), architecture (Hooke) and lucrative private medicine (Lower). The other great centres of learning in Europe did not take up the mantle of respiratory research. The cause of this stagnancy is uncertain:4 this was another politically turbulent period of history in Europe, and conditions may not have been conducive to academic study. There may even have been a sense that respiration was now effectively explained, considering that knowledge of other closely related scientific disciplines, particularly chemistry, was still at a very primitive stage.
Chemistry and Respiration
Different Types of Air
Phlogiston.6 George Ernst Stahl (1660–1734) had begun to investigate the chemistry of combustion in the early 18th century and provided the scientific community with a completely erroneous explanation, which was nevertheless widely accepted. Stahl proposed that all combustible substances were made up of two components: calx, combined with a fiery principle named phlogiston. On burning, the phlogiston was driven off from the substance leaving just the calx, or ash. Substances such as charcoal, which left very little ash, must have contained a greater proportion of phlogiston. Combustion in an enclosed space was extinguished when the air contained within became saturated with phlogiston. Calcination of metals (intense heating in air until oxidation occurs) was explained as driving off the phlogiston contained in the metal, whilst conversion of the metal oxide back to metal by heating with charcoal was achieved by the charcoal donating its phlogiston to recreate the metal. A powerful piece of evidence contradicted the phlogiston theory for metal calcination. Boyle, Mayow and others had all demonstrated that when metals were calcined, they gained weight, so could not have lost phlogiston. Stahl provided a very dubious explanation of this by explaining that on calcination the metal also lost some of its ‘negative weight’.
Although the phlogiston theory was a complete inversion of what we now know to be true, it fitted with almost all known observations of combustion in the 18th century, with only the single exception already described. Stahl’s views therefore became very enduring, and are believed to have impeded progress in understanding the chemistry of gases for many decades.
Fixed air and vitiated air. Joseph Black (1728–1799) was a Scottish chemist whose work focussed on the chemistry of alkalis, a group of substances widely used at the time for the treatment of kidney complaints. He demonstrated that heating chalk (CaCO3) caused a gas to be liberated, and a reduction in weight to occur. To explain the large observed weight loss, Black believed the liberated gas to be air rather than phlogiston. After further experiments Black found that the same gas was produced by fermentation, by burning charcoal, and was present in expired air. From these observations he named it ‘fixed air’, believing that the gas made up all the non-respirable portion of air. Only a few years later in 1772, the discovery of ‘vitiated air’ (nitrogen) demonstrated that fixed air was present in only small quantities in air. Black’s explanation of the chemical reactions of carbon dioxide did not involve phlogiston at all, which must have been surprising considering the fundamental place phlogiston held in the chemistry of the time, but the phlogiston theory continued unchallenged.
Dephlogisticated air. Two chemists independently demonstrated the concept of oxygen and respiration. Joseph Priestley32 (1733–1804) in England carried out a range of experiments with respiratory gases. His work was published in Experiments and observations on different kinds of air,33 which included an illustration of the equipment used (Figure 13.7). Initially described by Priestley as ‘pure air’, the gas produced by heating mercuric oxide was found to cause a candle to burn with ‘a remarkably vigorous flame’ and allow a mouse to survive much longer than in ‘common air’. Priestley tried breathing the pure air himself with no apparent ill effects. His experiments on plants led to the major discovery that vegetation, in particular fast growing species such as spinach, reversed the gaseous changes caused by respiration, burning candles or putrefaction within his closed vessels. He fully appreciated the import of this discovery on a global scale by commenting that air in the common atmosphere that has been reduced to a noxious state by respiration or combustion ‘has never failed to be perfectly restored by vegetation, so that the growing vegetables with which the surface of the Earth is overspread, may be a cause of the purification of the atmosphere’. An advocate of phlogiston, Priestley soon renamed his ‘pure air’ as ‘dephlogisticated air’. He believed his experiments confirmed the phlogiston theory, i.e. the mercuric oxide removed phlogiston from the air so allowing candles to burn longer, or animals to respire longer, before the air became saturated with phlogiston.
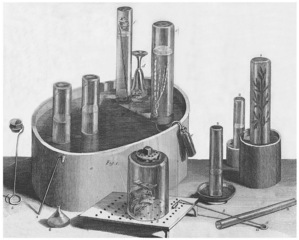
Fig. 13.7 Frontispiece from Priestley’s ‘Experiments and observations on different kinds of air’,33 showing the variety of apparatus used in his experiments. Mice can be seen contained within a beer glass (d) which allowed them to breathe for 20–30 minutes in ‘common air’, whilst others are held in receivers open at the top and bottom for use in later experiments (at the front of the illustration). Plants can be seen growing in the jar on the far right.
(Reproduced by permission of the Special Collections, Leeds University Library.)
Fire air. Carl Scheele32 (1742–1786) studied chemistry and pharmacy in Sweden. Unaware of Priestley’s work Scheele, using a variety of methods, also produced oxygen, which he named ‘fire air’. He too demonstrated its effect on burning candles and animal respiration, but he also failed to use his results to challenge the phlogiston theory.
Oxygen
Antoine-Laurent Lavoisier35 (1743–1794) was born in Paris and graduated in science before the age of 20, specialising in chemistry soon after. In a very productive few years commencing around 1772 Lavoisier studied combustion and respiration, during which time he was visited by Priestley who discussed his own experiments with ‘pure air’. Lavoisier approached chemistry differently, in effect introducing quantitative studies to the qualitative ones of his predecessors.6 He showed that when metals were calcined in a closed jar the combined weight of apparatus, air and jar remained unchanged, so proving that it was air combining with the metal that increased their weight. In experiments with animals breathing nearly pure oxygen, he observed that the animals expired before all the oxygen was used up, and this led him to investigate the harmful effects of carbon dioxide in the atmosphere.
Respiratory experiments over acidified water allowed the CO2 produced by respiration to be absorbed, and allowed quantification of oxygen consumption, which in a resting subject was measured by Lavoisier as 1200 cubic inches per hour (≈ 330 ml.min−1), a result very close to the modern value (page 203). However, it is Lavoisier’s discovery that ‘eminently respirable air’ was a chemical element, and his naming of the element as oxygen, for which he is most remembered. Once again, the contribution made by the scientists of the time to this seminal discovery is controversial, for example Priestley was later irritated at Lavoisier’s use of the ideas they discussed in 1774, and Mayow’s work is never referred to in Lavoisier’s writings in spite of him being aware of it at the time.4 Lavoisier’s interests were wider than his study of science, and he was closely involved in a French financial institution responsible for generating tax revenues, the Ferme Generale. Income from this clearly provided the resources for Lavoisier’s extensive experiments, but also resulted in accusations of financial impropriety which led to his untimely death at the guillotine in 1794.6 After Lavoisier’s death, his friend Lagrange commented that ‘It took but a second to cut off his head; a hundred years will not suffice to produce one like it’.34
Early Development of Current Ideas of Respiratory Physiology
Tissue Respiration
Ancient ideas of some type of combustion in the heart to generate heat gave way in the 16th century to the suggestion that heat was generated by friction within the ever-moving blood. As chemistry developed, the similarities between combustion and respiration became progressively more compelling, but where this oxidation reaction took place eluded even Lavoisier who believed it occurred in the bronchi. The impetus to look beyond the lungs and heart to find the site of combustion in the body came from the discovery of calorimetry by Adair Crawford (1748–1795).35 Measurements made by Crawford and Lavoisier of the heat generated by the body made it clear to Lavoisier’s mathematician friend Lagrange, and his colleague Hassenfratz, that if all the heat were produced in the lungs their temperature ‘would necessarily be raised so much that one would have reason to fear they would be destroyed’36
In Italy, further experiments into where in the body combustion took place were performed by Lazzaro Spallanzani (1729–1799), though his work was only published posthumously in 1803.37 He studied respiration in a huge variety of creatures including insects, reptiles, amphibians and mammals, and described how those creatures without lungs exchanged oxygen and carbon dioxide via their integument. That respiration still occurred in the absence of lungs led Spallanzani to his most important respiratory discovery when he showed that a variety of tissues from recently deceased creatures (including humans) continued to respire for some time, so showing that the tissues were the site of oxygen consumption.
In the 19th century, advances in science led to improved techniques for gas and temperature measurement. Heat production was measured in animals and humans and found to correlate with the specific heat capacity of the oxygen consumed and carbon dioxide produced. The respiratory quotient was measured at between 0.6 and 1.0, and found to depend on diet. Finally, with the birth of organic chemistry, and the foundation of the laws of conservation of energy, the modern account of energy metabolism was elucidated.6
Blood Gases
Once it was clear that oxygen metabolism occurred in the tissues, the search was on to find how the blood carried oxygen to, and returned carbon dioxide from, the tissues in sufficient quantities. However, other fundamental discoveries were needed before this question could be addressed in detail.
Partial pressure. John Dalton (1766–1844), whose law on partial pressures (page 516) is widely used today, first developed the concept that mixtures of gases could exist together irrespective of the pressure and temperature of the mixture. His description stated that the particles of each component gas had no interaction with those of the other gases and so ‘arranged themselves just the same as in a void space’ whilst paradoxically occupying the whole space allotted to the mixture of gases. He illustrated this as shown in Figure 13.8.38
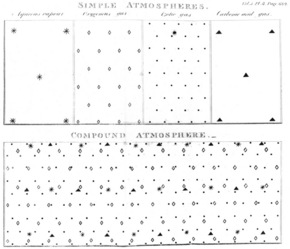
Fig. 13.8 Dalton’s drawing to illustrate a compound atmosphere, made up of a mixture of simple atmospheres.38 Two centuries after it was drawn, this diagram would be helpful to today’s physiology students when first learning of Dalton’s law of partial pressures. Aqueous vapour, water vapour; oxygenous gas, oxygen; azotic gas, nitrogen; carbonic acid gas, carbon dioxide.
(Reproduced by permission of the Wellcome Library of the History of Medicine.)
Paul Bert (1833–1886), most famous for his studies of altitude physiology and medicine, also made a significant contribution to fundamental respiratory physiology by discovering that it was the partial pressure, rather than concentration, of respiratory gases that affected biological systems.39,40 In an elegant series of experiments, he exposed animals to a variety of atmospheric pressures whilst maintaining the partial pressure of oxygen constant, with no ill effect on the animals. Whenever inspired Po2 was reduced below that of air at atmospheric pressure, irrespective of the total pressure, the animal suffered the consequences of hypoxia. He repeated the experiments on humans in a large specially constructed chamber (Figure 13.9) and showed that by breathing supplementary oxygen, the harmful effects of low ambient pressure could be entirely alleviated.

Fig. 13.9 Figure from La pression barométrique39 showing Paul Bert breathing oxygen whilst sitting in the chamber at progressively sub-atmospheric pressure. Note the sparrow in the cage above the subject – the bird falls in its cage when the pressure reaches 450 mmHg, but Bert persists with the experiment down to 410 mmHg, maintained conscious by intermittently breathing oxygen.
(Reproduced by permission of the Wellcome Library of the History of Medicine.)
Bert applied his knowledge to the recently discovered pastime of ballooning, and assisted his friend Gaston Tissandier to use oxygen to ascend to record new heights in his balloon. However, in his enthusiasm for altitude, M. Tissandier and two friends undertook a balloon flight with the specific aim of reaching 8000 m (26 200 feet) altitude, but in their enthusiasm they did not have time to consult Bert on the likely oxygen requirement. An unusually rapid ascent (Figure 13.10) resulted in confusion in all three balloonists, who were unable to breathe the oxygen and lost consciousness (page 280). Only Tissandier recovered sufficiently to record their altitude as 8600 m (28 200 feet), before battling with hypoxia to intermittently breathe oxygen and facilitate a controlled descent, during which the full tragedy of the flight unfolded, and he discovered that his two friends had died some time earlier in the flight.

Fig. 13.10 Diagram of the high altitude ascent of the balloon Zenith on April 15th 1875.39 The dashed line indicates estimated altitude, as the only survivor of the flight Gaston Tissandier, was too hypoxic to make recordings of the altitude.
(Reproduced by permission of the Wellcome Library of the History of Medicine.)
Haemoglobin and its dissociation curve. Boyle and Mayow had both used a vacuum to extract gases from blood and surmised that this may have been air or nitro-aerial spirit (oxygen). In the 19th century the excellence of German chemists led them to dominate this field of research. Gustav Magnus (1802–1870) extracted oxygen and carbon dioxide from blood, showing that the former was more abundant in arterial blood and vice versa.41 Lothar Meyer did similar experiments in 1857, but showed that the liberation of oxygen as pressure was reduced was not linear, so demonstrating that the oxygen was not simply dissolved in the blood.42 Meanwhile, the red compound in blood was identified and soon chemically found to be a combination of globulin proteins and an iron containing haematin. The affinity of this new ‘haemoglobin’ for oxygen was soon understood, and Hüfner quantified this binding by showing that 1.34 ml of oxygen combined with 1 g of crystallised haemoglobin, a remarkably accurate measurement (page 189).43 By 1888, Hüfner had used haemoglobin solutions to record the relationship between the partial pressure of oxygen and haemoglobin saturation, and obtained a rectangular hyperbola.5 Finally in 1904, Christian Bohr and colleagues showed that when fresh whole blood was used to measure the haemoglobin dissociation an S-shaped curve was found, and that the curve altered with varying partial pressures of carbon dioxide (Figure 13.11).44
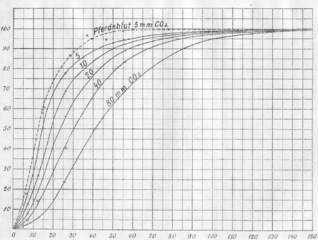
Fig. 13.11 The first publication (from 1904) showing the shape of the oxy-haemoglobin dissociation curve.44 Note the effect of blood Pco2 on the position and shape of the curve (page 192). Pferdeblut, horse blood.
(Reproduced by permission of the Special Collections, Leeds University Library.)
The oxygen secretion controversy.1,45 Measurement of the partial pressure of oxygen in arterial blood in the 19th century provoked a huge scientific controversy. In 1870, Bohr and colleagues developed a primitive aerotonometer and found arterial Po2 to be around 80 mmHg (10.7 kPa), though in some measurements the arterial Po2 was found to be slightly higher than the alveolar Po2. At around this time, physiologists studying other body systems were discovering numerous active membrane transport systems in such places as the kidney and bowel. This led Bohr to suggest that active transport of oxygen may occur in the lung and he soon had the support for this hypothesis from the eminent respiratory physiologist John Scott Haldane. In his laboratories in Oxford, Haldane devised a new technique for measuring arterial Po2. His technique involved the subject breathing small concentrations of carbon monoxide, and then using direct colour matching of the subject’s blood with standard samples to ascertain the carboxy-haemoglobin concentration from which the Po2 could be calculated.46 To standardise the light used for comparing colours, experiments had to be done during daylight, and by today’s standards several aspects of the technique seem remarkably subjective, but nevertheless Haldane was an excellent scientist who applied rigorous methodology. Using his technique Haldane found the average arterial Po2 to be 200 mmHg (26.7 kPa) so claiming to have proved that oxygen secretion was occurring in the lung.
A Danish husband and wife team, August and Marie Krogh,47 became Haldane’s adversaries over oxygen secretion. August Krogh, a former pupil of Bohr, continued to refine the technique of aerotonometry, using analysis of smaller volumes of gas from continuously flowing blood samples. His results always showed arterial Po2 to be slightly less than alveolar Po2 even when tested across a variety of inspired oxygen concentrations. Meanwhile his wife performed extensive investigations of the diffusing capacity of the lung for carbon monoxide to show that, in theory, the lung was easily able to passively absorb sufficient oxygen without the need for active secretion.
Following a bitter exchange of contradictory scientific papers over a period of 20 years, the Kroghs did begin to win the argument. By 1911, Haldane and his team seemed to accept that oxygen secretion may only be occurring when inspired oxygen levels were low. They demonstrated this, using their usual methodology, in an adventurous study of Po2 measurements on the summit of Pikes Peak at an altitude of 4300 m (14 100 feet) where they again found arterial Po2 to be higher than alveolar Po2.48
Haldane never abandoned his faith in oxygen secretion, in spite of subsequent investigations in his lifetime by Barcroft who also found the phenomenon did not exist. Why a physiologist as brilliant as Haldane had such an unshakeable believe in an erroneous hypothesis remains unexplained, and for this reason the controversy continues. When a review of these events was published in the Lancet in 198745 the dispute over Haldane’s contribution was reignited.49,50
Lung Mechanics51
Galen knew that inflation of the lungs was a passive phenomenon and occurred as a result of chest movement brought about by the respiratory muscles. However, the way in which this occurred was not understood for many centuries until the discovery of air pressure and therefore the existence of a vacuum, when it soon became clear that chest expansion would draw air into the lungs. Even then there were those who would not accept the scientific explanation; Rene Descartes proposed in 1662 that when the chest expanded, the air outside was pushed away from the chest, compressing adjacent air until the air near the mouth was forced into the lungs.6 Mayow’s elegant demonstration with the bladder within the bellows, described above, provided clear confirmation of the scientific theory.
Around 1500 years after Galen, Vesalius’ experiments demonstrated that on puncturing the pleura, the lung retracted into the chest cavity. Many of his successors repeated this observation, Mayow commenting that ‘the lungs, as if shrinking from observation, cease their movement and collapse at once on the first entrance of light and self-revelation’.31 It was another 160 years before further investigation of lung elasticity occurred. In 1820 Carson measured the pressure in the trachea (with a closed airway) when the chest was opened, and so made the first measurement of lung recoil pressure.52 A short time later, Ludwig recorded a sub-atmospheric pressure in the pleura, leading to the proposal by Donders in 1849 that in the intact subject the recoil outwards by the chest wall is equal to the lung recoil inwards4 (Chapter 3). Finally, John Hutchinson, whose work on lung volumes is described below, produced the first lung compliance curves in humans, obtained shortly after the subject’s death.
Elasticity and surfactant. For some time lung recoil seems to have been adequately explained as simply resulting from the inherent elasticity of lung tissue. At the start of the 20th century the geometry and size of the alveoli was well known, and around 100 years had elapsed since Laplace had described the relationship between pressure, surface tension and the radii of curved surfaces (page 28). Yet the inherent instability of lung tissue based on these laws was not recognised until 1929, when Kurt von Neergard first questioned whether tissue elasticity alone was sufficient explanation for the properties of lung tissue.53 von Neergard’s experiments demonstrated that surface tension in alveoli was indeed lower than expected by Laplace’s law, and just a few years later Richard Pattle demonstrated that lung tissue contained an insoluble protein layer that reduced the surface tension of alveoli to almost zero,54 and surfactant (page 29) was discovered.
Lung volumes. The first measurements of the volume of air contained in the lung were made in the 17th century by Borelli, who also raised the concept of a residual volume.6 Following this, numerous scientists measured a confusing variety of lung volumes by various methods, such as estimating total lung capacity from plaster casts made in the chest cavity of cadavers. Measurement of lung volumes similar to those in modern use was first made by John Hutchinson in 1846, alongside his description of the first pulmonary spirometer.55 Hutchinson’s spirometer (Figure 13.12) differs little from the water spirometers used until very recently, with a volume measuring chamber over water counterbalanced with weights to offer minimal resistance to the subject’s breathing. Hutchinson described the following divisions of the air in the chest, with the modern equivalents (page 36) in parentheses:
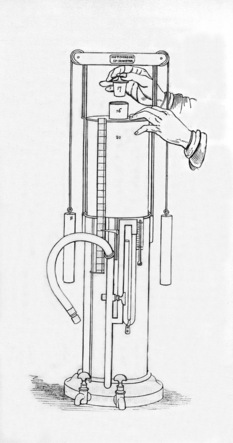
Fig. 13.12 The Hutchinson spirometer (1846).55 This figure shows the operator removing the bung to reset the level of the spirometer before making another measurement.
(Reproduced by permission of the Special Collections, Leeds University Library.)
In the same paper,55 Hutchinson reported his measurements of vital capacity in 1970 healthy subjects to establish normal values. He showed with great accuracy that vital capacity was directly related to subject height and age, and obtained measurements comparable with today, e.g. 188 in3 at 60°F for a 55-year-old male subject 5 feet 4 inches tall (188 in3 equals 3.31 L BTPS, compared with a modern predicted normal value of 3.64 L). He then measured vital capacity in 60 patients with phthisis (cough) from a variety of causes, and compared the results obtained with predicted normal values based on height and weight etc. and was able to use his results to demonstrate declining lung volumes as their respiratory disease progressed.
Control of Ventilation
Galen’s observations of gladiator injuries had shown that the brain was responsible for respiratory activity, and that the phrenic nerves were involved in bringing about this action.
More specific localisation of the respiratory centre did not begin until the 18th century, when the French physiologist Antoine Lorry (1725–1783) showed that in animals all parts of the brain above the brainstem could be removed before respiration ceased.4 In 1812, the French physiologist Antoine Legallois published reports of similar, but more precise, experiments showing that rhythmic inspiratory movements ceased only when the medulla was removed.56 During the next 150 years a long series of distinguished investigators carried out more detailed localisation of the neurones concerned in the control of respiration and studied their interaction.4 These experiments resulted in the description of anatomical regions which, when isolated in animals, caused a specific respiratory pattern, for example the apneustic and pneumotaxic centres. The complexity of respiratory control in the intact animal is such that this crude anatomical approach to unravelling the various interactions was limited, and human studies of function were mostly impossible until recent imaging techniques were developed (page 61).
The origin of rhythmicity in the respiratory centre received much attention from 19th century physiologists.57 The role of afferent neural inputs into the respiratory centre, particularly those from the vagus nerve, were clearly demonstrated. In particular, Hering and Breuer described how lung inflation led to inhibition of inspiratory activity, and a ‘deflation’ reflex was also described (page 67). These observations gave rise to the basis of the Selbsteuerung (self-steering) hypothesis where rhythm generation was simply two alternating inhibitory reflexes.
Chemical control of breathing.58 Rapid breathing followed by gasping and death had been observed by the Oxford physiologists in the 17th century in their experiments on animals in closed atmospheres. As the analysis of gases in blood improved, so the chemical control of breathing could be elucidated. In 1868, Pflüger performed a comprehensive study in dogs showing that both oxygen lack and carbon dioxide excess stimulated respiration, and that the former was the stronger stimulant.59 Soon after, a fellow German physiologist Miescher-Rusch investigated the carbon dioxide response in humans to show that the respiratory system exerted very tight control over carbon dioxide concentrations and concluded that this, rather than oxygen, was the predominant chemical stimulus to breathing.60 Leon Fredericq demonstrated in a series of very elegant experiments that the chemical control of breathing predominated over the vagal reflex control described in the previous paragraph.61 He managed to cross connect the blood supply to and from the heads of two animals and, for example, produce apnoea in one dog by hyperventilating the other, the apnoea occurring even though the dog’s lungs were not inflated to induce the Hering–Breuer reflex. Finally, at the start of the 20th century, further improvements in analytical chemistry led to the work of Haldane and Priestley, published in 1905, which involved meticulous quantitative analysis of the chemical control of breathing and the interactions between oxygen, carbon dioxide and exercise.62
References
*1. West JB. Respiratory physiology: People and ideas. Oxford: American Physiology Society & Oxford University Press; 1996.
2. West JB. A century of pulmonary gas exchange. Am J Respir Crit Care Med.. 2004;169:897-902.
3. Macklem PT. A century of the mechanics of breathing. Am J Respir Crit Care Med.. 2004;170:10-15.
4. Proctor DF. A history of breathing physiology. New York: Marcel Dekker; 1995.
5. Gottlieb LS. A history of respiration. Springfield, Illinois: Charles C Thomas; 1964.
6. Perkins JF. Historical development of respiratory physiology. In: Fenn WO, Rahn H, editors. Handbook of Physiology. Section 3: Respiration. Washington: American Physiological Society, 1964.
*7. Nunn JF. Ancient Egyptian Medicine. London: British Museum Press; 1996.
8. Bryan CP. Ancient Egyptian medicine: the papyrus Ebers. Chicago: Ares; 1974.
9. Ghalioungui P. The Ebers papyrus. A new English translation, commentaries and glossaries. Cairo: Academy of Scientific Research and Technology; 1987.
*10. May MT. Galen – On the usefulness of the parts of the body. New York: Cornell University Press; 1968.
11. Furley DJ, Wilkie JS. Galen on respiration and the arteries. Princeton NJ: Princeton University Press; 1984.
12. Singer C. A short history of anatomy & physiology from the Greeks to Harvey. New York: Dover Publications; 1957.
*13. West JB. Ibn al-Nafis, the pulmonary circulation, and the Islamic Golden Age. J Appl Physiol.. 2008;105:1877-1880.
14. Leonardo da Vinci. Anatomical drawings from the Royal Collection. London: Royal Academy of Arts; 1977.
15. Clark K. The drawings of Leonardo da Vinci in the collection of Her Majesty the Queen at Windsor Castle (Volume 3). London: Phaidon Press; 1969.
16. Mitzner W, Wagner E. On the purported discovery of the bronchial circulation by Leonardo da Vinci. J Appl Physiol.. 1992;73:1196-1201.
17. Charan NB, Carvalho P. On the purported discovery of the bronchial circulation by Leonardo da Vinci: A rebuttal. J Appl Physiol.. 1994;76:1836-1838.
18. Vesalius A. De Humani Corporis Fabrica Libri Septem. Venice: Basel; 1543.
19. Coppola ED. The discovery of the pulmonary circulation: A new approach. Bull Hist Med.. 1957;31:44-77.
20. Servetus M. Christianismi Restitutio. 1553
21. O’Malley CD. Michael Servetus: A translation of his geographical, medical and astrological writings with introductions and notes. Philadelphia: American Philosophical Society; 1953.
22. Servetus M. Christianismi Restitutio. Frankfurt: Minerva; 1966.
23. Colombo R. De Re Anatomica libri XV. Paris: Andreum Wechelum; 1572.
24. Harvey W. De Motu Cordis. Frankfurt: Wm Fitzeri; 1628.
25. Harvey W. Movement of the heart and blood in animals. Oxford: Blackwell Science; 1957.
26. Malpighi M. De Pulmonibus. Bologna, 1661.
27. Young J. Malpighi’s ‘De Pulmonibus’. Proc R Soc Med Lond.. 1929;23:1-11.
28. West JB. Robert Boyle’s landmark book of 1660 with the first experiments on rarified air. J Appl Physiol.. 2005;98:31-39.
29. Harsch V. Robert Hooke, inventor of the vacuum pump and the first altitude chamber (1671). Aviat Space Environ Med.. 2006;77:867-869.
30. Hooke R. An account of an experiment made by Mr Hook of preserving animals alive by blowing through their lungs with bellows. Phil Trans R Soc Lond.. 1667;2(28):539-540.
31. Mayow J. Medico-Physical works: Being a translation of Tractatus Quinque Medici-Physici. Edinburgh: The Alembic Club; 1907.
*32. Severinghaus JW. Priestley, the furious free thinker of the enlightenment, and Scheele, the taciturn apothecary of Uppsala. Acta Anesthesiol Scand.. 2002;46:2-9.
33. Priestley J. Experiments and observations on different kinds of air. London: J.Johnson; 1775.
34. Lusk G. Nutrition. Clio Medica: A series of primers on the history of medicin, Volume 10. New York: Hoeber Inc. 1933.
35. Crawford A. Experiments and observations on animal heat, and the inflammation of combustible bodies: being an attempt to resolve these phenomena into a general law of nature. London: J. Johnson; 1788.
36. Hassenfratz JH. Mémoire sur la combinaison de l’oxygèn dans le sang et sur la manière dont la calorique se degage. Ann Chim Paris. 1791;9:261-274.
37. Spallanzani L. Mémoire sur la respiration. Geneva: Paschoud; 1803.
38. Dalton J. Experimental essays on the constitution of mixed gases; on the force of steam or vapour from water and other liquids in different temperatures, both in a Torricellean vacuum and in air; on evaporation; and on the expansion of gases by heat. Mem Lit Phil Soc, Manchester. 1802;5:535-602.
39. Bert P. La pression barométrique. Paris: Masson; 1878.
40. Hitchcock MA, Hitchcock FA. Paul Bert. Barometric Pressure. Researches in experimental physiology. Columbus Ohio: College Book Company; 1943.
41. Magnus H. Ueber die im blute enthalten gase, sauerstoff stickstoff und kohlensäure. Ann Phys Chem.. 1837;40:583-606.
42. Meyer L. Die gase des blutes. Z Rat Med.. 1857;8:256.
43. Hüfner G. Ueber die quantität sauerstoff, welche 1 gramm hämoglobin zu binden vermag. Z Phys Chem.. 1877;1(5):317-329.
44. Bohr C, Hasselbalch K, Krogh A. Ueber einen in biologischer beziehung wichtigen einfluss, den die kohlensäurespannung des blutes auf dessen sauerstoffbindung übt. Skand Arch Physiol.. 1904;16:402-412.
*45. Milledge JS. The great oxygen secretion controversy. Lancet. 1985;2:1408-1411.
46. Haldane JS, Lorrain Smith J. The oxygen tension of arterial blood. J Physiol.. 1891;20:497-520.
47. Schmidt-Nielsen B. August and Marie Krogh and respiratory physiology. J Appl Physiol.. 1984;57:293-303.
48. Douglas CG, Haldane JS, Henderson Y, Schneider EC. Physiological observations made on Pike’s Peak, Colorado, with special reference to adaptation to low barometric pressures. Phil Trans R Soc Lond.. 1913;203:185-318.
49. Passmore R. Haldane and Barcroft. Lancet. 1986;1:443.
50. Cunningham DJC. The oxygen secretion controversy. Lancet. 1986;1:683.
51. Otis AB. History of respiratory mechanics. In: Fishman AP, Macklem PT, Mead JT, Geiger SR, editors. Handbook of Physiology. Section 3: The respiratory system. Bethesda: American Physiological Society, 1986.
52. Carson J. On the elasticity of the lungs. Phil Trans R Soc Lond.. 1820;110:29-44.
53. von Neergard K. Neue auffassungen über einen grundbegriff der atemmechanik. Die retraktionkraft der lunge, abhängig von der oberflächenspannung in den alveolen. Z Ges Exp Med.. 1929;66:1-22.
54. Pattle RE. Properties, function and origin of the alveolar lining layer. Nature. 1955;175:1125-1126.
55. Hutchinson J. On the capacity of the lungs, and on the respiratory functions, with a view of establishing a precise and easy method of detecting disease by the spirometer. Med Chir Trans (Series 2). 1846;29:137-252.
56. Legallois C. Experiences sur le principe de la vie. Paris: d’Hautel; 1812.
57. Widdicombe J. Reflexes from the lungs and airways: historical perspective. J Appl Physiol.. 2006;101:628-634.
58. Remmers JE. A century of control of breathing. Am J Respir Crit Care Med.. 2005;172:6-11.
59. Pflüger E. Ueber die ursache der athembewegungen, sowie der dyspnoë und apnoë. Arch Ges Physiol.. 1868;1:61-106.
60. Miescher-Rüsch F. Bemerkungen zur lehre von den atembewegungen. Arch Anat u Physiol Leipzig.. 1885;6:355-380.
61. Fredericq L. Sur la cause de l’apnée. Archiv Biol Liége. 1900;17:561-576.
62. Haldane JS, Priestley JG. The regulation of lung ventilation. J Physiol.. 1905;32:225-266.