DIAGNOSIS.
Physical examination should be directed at determining the presence of and distribution of body fat by measuring height, weight, body circumference (extremity and waist), and nutritional status. In addition, the presence of associated causes of obesity should be investigated.
Abdominal (visceral) fat is metabolically active. Measurement of circumference is needed to identify the distribution of body fat and to determine the risks associated with increased waist circumference. Waist circumferences that are above 40 inches for men and above 35 inches for women increase the risk for premature death and disability as a consequence of overweight or obesity. Waist circumference is the best predictor of visceral (intraabdominal) fat and total fat. The most clinically telling physical sign of serious underlying disease is increased waist circumference, which is linked to insulin resistance, hypertension, dyslipidemia, type 2 diabetes, coronary heart disease, sleep apnea, and gallbladder disease.108
Waist circumference measurements have a high correlation with BMI.129 Measurement of extremity circumference may also be useful in the adult population for the physician to rule out lipedema, a symmetrical “swelling” of both legs, extending from the hips to the ankles, caused by deposits of subcutaneous adipose tissue.
Although BMI and waist circumference measurements are the most clinically feasible methods to identify clients who are overweight or obese, additional methods may be used to measure subcutaneous fat or body composition.70 Methods that are known for accuracy but often only used in research settings include hydrostatic weighing and dual-energy x-ray absorptiometry (DEXA).37,144
Additional methods that require less expensive equipment include the use of skinfold measurement calipers and the measurement of bioelectrical impedance. Skinfold measurements using calipers (the pinch test) are performed in several locations on the body (e.g., midbiceps, midtriceps, and subscapular areas). Measurements greater than 1 inch are thought to indicate excessive body fat. Skinfold measurement has been questioned in relationship to accuracy because interobserver variability may be high.159 Skinfold measurement should be taken into consideration along with body type and height.
Bioelectrical impedance analysis (BIA) measures the impedance or resistance to an electrical signal that is circulated through the body. A person who has more fat mass will have larger impedance because there will be more resistance to the electrical signal traveling through the body since fat mass contains less water. BIA measures have been shown to be reliable and valid; however, variability among individuals can be high, and inaccuracy can occur in situations of altered hydration status and extreme obesity in those being measured.24,122 Additionally, BIA has not been shown superior to BMI as a predictor of overall adiposity in a general population.263
All of these examples of measures can provide a baseline measurement for relative fat mass and can be used to monitor progress of body composition as people advance through a weight loss program.
TREATMENT.
Both physical activity and nutrition are important in addressing obesity. Physical activity and nutrition are modifiable factors that respond similarly to the same interventions. To maintain a healthy weight, it is important to keep energy expenditure at or above energy intake. This can be accomplished by decreasing caloric intake, increasing exercise energy expenditure, or both.
Weight loss is regarded as a major aspect of treatment for the person who is obese. Although the amount of weight loss necessary is arguable, 10% loss in body weight is regarded as a standard that improves health.
The National Weight Control Registry (www.nwcr.ws/) reports that weight loss and maintenance of the weight loss are best accomplished if individuals participate in regular intensive exercise, attend support groups, restrict the amount and kinds of food eaten, and weigh themselves often.
A multidisciplinary approach with emphasis on weight loss maintenance should be directed toward anyone with a BMI of 30 and above and for those people with a BMI in the 25 to 29 range who have associated health problems. Such a treatment program includes moderate calorie intake, behavior modification, exercise, and social support.
Medications for obesity are widely available over the counter and by prescription. The use of pharmacologic agents to inhibit appetite, reduce fat absorption, and increase metabolic rate is highly controversial and provides at best only a short-term benefit. Drug therapy is thought to work best when it is part of an overall program aimed at lifestyle change involving dietary changes, exercise, and behavior modification.255,260 To be effective, drug treatment for obesity should be continued indefinitely much like treatment for any chronic condition.5,74,260 Researchers continue to look for drugs that can prevent or alter the physiology of obesity.
Surgical treatment, referred to as bariatric surgery, may be considered for some obese people if serious attempts to lose weight have failed, if BMI is greater than 40 kg/m2 with or without comorbidities, or if there is a BMI of 35 kg/m2 with significant health-related comorbidities5,74,194,239,260 and complications of obesity that are life-threatening. Surgical approaches rely on reconfiguring or redirecting the gastrointestinal system through gastric restriction called vertical gastric banding (VGB) or gastric bypass procedures (e.g., Roux-En-Y gastric bypass [RYGB]). Bariatric surgery has been shown to provide the greatest degree of sustained weight loss in people with morbid obesity.157 Other benefits and complications of bariatric surgery are listed in Table 2-4.
Table 2-4
Potential Benefits and Complications of Bariatric Surgery
| Potential Benefits | Potential Complications |
| Weight loss | Nephrolithiasis |
| Improved serum lipids | Hepatic failure |
| Decreased blood pressure | Cholelithiasis |
| Improved or resolved diabetes mellitus | Malnutrition |
| Reflux | |
| Improved or resolved sleep apnea | Small bowel obstruction (SBO) |
| Hemorrhage | |
| Reduced venous stasis | Iron deficiency anemia |
| Decreased joint pain | Vitamin B12 malabsorption |
| Improved quality of life | Gastric prolapse |
| Overall improved function |
Courtesy Tamara L. Burlis, PT, DPT, CCS, Washington University Program in Physical Therapy, St Louis, MO. Used with permission, 2006. Data compiled from a variety of published studies.
Laparoscopic RYGB has been referred to as the “gold standard” operation for surgical control of obesity. It is effective in achieving weight loss, improving comorbidities and quality of life, and reducing recovery time and perioperative complications.224 This procedure is safe, effective, and decreases overall costs.194
Evidence supports this shift in surgical approach for individuals having laparoscopic surgery based on studies demonstrating improved SF-36 scores,93,193,194,239 decreased recovery times,193,224 earlier return to work,193 less postoperative pain,193,224 and comparable amounts of weight loss.61,193
The relationship(s) between biologic and behavioral factors influencing obesity is not yet completely understood. However, regardless of the medical and surgical treatments available to treat obesity, behavioral change in the frequency and type of eating and exercise habits remains the foundation of both prevention and intervention.256
Behavior in both prevention and treatment is influenced by what options are available (e.g., vending machines, safe parks in which to walk), how and to whom health information is portrayed (e.g., media versus health practitioner), and what type of support is given to individuals who seek and/or need to make a change.135
Practitioners require knowledge of what motivates change, how behavioral change occurs, what resources are needed to make change, and strategies useful for promoting change. Across the theoretic foundations guiding this knowledge, the combined merits of providing accurate information, understanding barriers preventing change, anticipating personal readiness for change, and providing structure and support over extended periods to enable sustained new behaviors have been recognized as helpful.20
Although lifestyle programs have been shown to be the most successful in creating durable change, regulation of body weight (to either prevent gain or maintain loss) is still affected by a myriad of intrapersonal and environmental factors that interact to make obesity control difficult. Tailoring all interventions to the “personal environment” of each individual is critical in overcoming the intrinsic and extrinsic pressures in the American culture that affect the current epidemic of obesity.161
PROGNOSIS.
The management of obesity continues to be challenging, particularly because its effect on the whole person is so broad and the causes/influences are so numerous that prognosis relies on significant and sustained lifestyle changes that must last a lifetime. When therapy is confined to dietary measures alone, treatment of obesity is less likely to be successful. Because the risk of mortality and morbidity from obesity rises in proportion to the degree of obesity and the presence of complications, treatment is essential. For example, among the cardiovascular problems associated with obesity, hypertension in combination with obesity increases the risk for development of cerebrovascular disease, specifically cerebral thrombosis.
Weight loss alters conditions associated with obesity and even moderate weight loss in an obese person (i.e., 10 to 20 lbs) provides substantial changes in risk factors. Following weight loss in the obese, a decrease in blood pressure usually occurs with a regression of left ventricular hypertrophy, total and HDL cholesterol are favorably changed, and glucose tolerance improves in those people with type 2 diabetes mellitus.
The addition of exercise to a comprehensive program of caloric reduction and behavior modification can improve results. Regular exercise can maximize body composition change and increase the probability of maintaining weight loss.
Patterns of fat distribution are important in determining the risks associated with obesity. Visceral fat within the abdominal cavity is more hazardous to health than subcutaneous fat around the abdomen. Upper body obesity around the waist and flank is a greater health hazard than lower body obesity marked by fat in the thighs and buttocks.
People who are obese with high waist-to-hip ratios (greater than 1.0 in men and 0.8 in women) have a significantly greater risk of diabetes mellitus, stroke, coronary heart disease, and early death than equally obese people with lower ratios. Waist circumference alone has also been designated as an independent predictor of health risks and may replace the waist-to-hip measurement as a predictor of increased risk. For women, weight-related health risks increase when the waist measurement is 35 inches or more; for men, this figure is 40 inches or more.
Although the connection between obesity (BMI greater than 30) and coronary heart disease is well established, it remains unknown whether a similar link exists for those who are mildly overweight. Research has shown that people whose BMI at midlife (30 to 55 years of age) was between 23 and 24.9 had a 50% higher risk of heart attack compared with those whose BMI was under 20. Women whose BMI was greater than 29 had a 3.6 times greater risk of heart attack compared with the leanest group.264 Moderately higher adiposity at younger ages (18 years) is associated with increased premature death in younger and middle-aged women.252
Smoking and Tobacco Use
Smoking and the use of tobacco products are associated with a number of chronic diseases, including chronic pulmonary diseases and cardiovascular conditions, as well as many types of cancers. Smoking also decreases the health of individuals who smoke. Some of the significant links between smoking and disease are reported in the Surgeon General’s report.220
Beside the obvious health risks associated with tobacco use as a lifestyle choice, it can become a psychologic problem because of the addictive qualities of this substance. For this reason, we have chosen to include tobacco use as part of a discussion of Substance Abuse in Chapter 3.
Alcohol and Other Drugs
Whether to consider substance use/abuse a behavioral condition or a psychologic problem remains uncertain. Many psychologists and addiction counselors say it is a condition, illness, or problem with multiple factors, including physical, psychologic, social, economic, and spiritual. Others place it on a continuum from behavior to disorder, depending on the individual’s relationship to the substance(s) and how that individual’s friends, family, colleagues, or coworkers are affected. Substance use is considered by some a “choice,” whereas addictions may be diagnosed as a disorder and then categorized as a pathologic psychologic disorder.
Addiction specialists and drug educators want to make it clear that alcohol is a drug. The commonly used phrase today when discussing substance use and abuse is “alcohol and other drugs.”
Culturally and socially, we live in a world that advertises and encourages the use of alcohol and other drugs as part of the American lifestyle. Addictions may be considered unique disorders that have their start in personal or lifestyle behaviors and choices but later become addictions with diagnosable pathology. Someone who drinks or uses drugs recreationally may not be an alcoholic or addicted, but when the use of substances has consequences in other areas of their life, then a problem is identified. There can be a fine line between lifestyle choices and behaviors and addictions and psychologic disorders. For now, we have chosen to place alcohol and other drug use in Chapter 3 but mention it here as a possible lifestyle, behavior, or choice that can impact the health of the individual and/or family members.
Domestic Violence
Domestic violence (DV) can be classified under categories of child abuse, intimate partner violence (IPV), and elder abuse. Because of the wide variety of practice settings in which they work, physical therapists are likely to encounter individuals of all ages who have been victims or survivors of DV.
DV is the physical, emotional/psychological, or sexual abuse; financial exploitation; neglect; or stalking of an individual by a person with whom they have a marital, familial, social, or dependency relationship. DV occurs in all socioeconomic and racial/ethnic groups. In all forms of DV, the incidence of abuse of individuals with disabilities is greater than in the nondisabled population.211,240,251,279
Physical abuse involves nonaccidental physical injury, which can range from superficial bruises and welts to broken bones, burns, serious internal injuries, and death. Emotional and psychologic abuse can result from acts or omissions that cause or could cause serious behavioral, cognitive, emotional, or mental disorders as a result of actions such as confinement or the constant use of verbally abusive language and criticism.
Sexual abuse ranges from nontouching offenses, such as exhibitionism, to fondling, rape, molestation, or the forced use of a child or an adult in the production of pornographic materials.
Neglect can involve the withholding of or failure to provide adequate food, shelter, clothing, hygiene, medical care, and/or supervision needed for optimal health and well-being. Neglect also includes refusal or delay in seeking health care, abandonment, inadequate supervision, and expulsion from home. Emotional neglect in children includes allowing a child to witness chronic or extreme spousal abuse or permitting truancy or drug/alcohol use. Stalking, another form of DV, is defined by the National Criminal Justice Association as “a course of conduct directed at a specific person that involves repeated visual or physical proximity, nonconsensual communication, or verbal, written or implied threats, or a combination thereof, that would cause a reasonable person fear.”189
Child Abuse
Child abuse involves the physical or emotional abuse or neglect or sexual abuse of a child under the age of 18 years, unless a state’s protection law specifies a different age limit. It is estimated that 12 out of every 1000 children in the United States are victims of physical or sexual abuse or neglect and that many more cases are never reported.251 Almost 1500 children die each year as the result of abuse; the majority of these children are less than 3 years of age.251
Because children are prone to accidents, it is important for clinicians to distinguish between the signs of accidental versus inflicted injuries and to determine if there is a reasonable suspicion of child abuse or neglect. The clinical manifestations often associated with child abuse are listed in Table 2-5.
Table 2-5
Clinical Manifestations of Domestic Violence
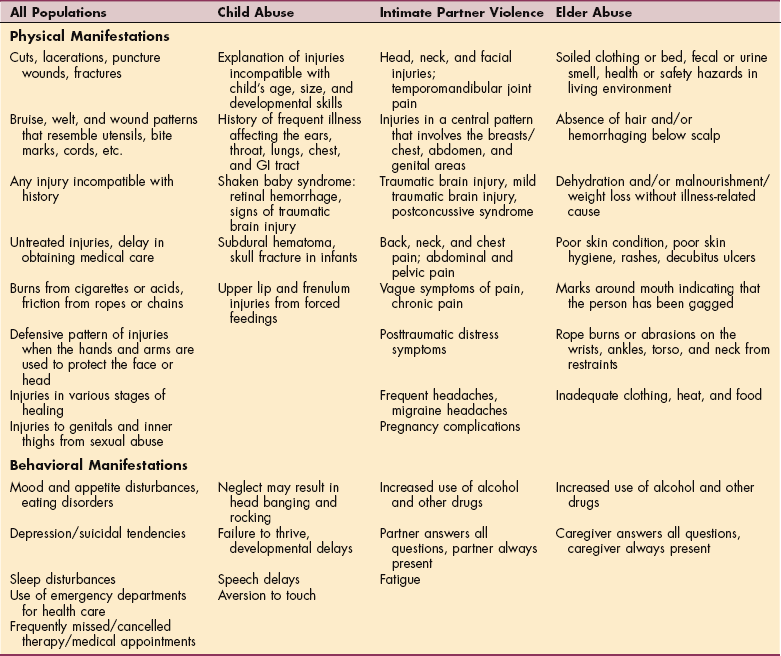
Courtesy Claudia B. Fenderson, PT, EdD, PCS, Mercy College, Dobbs Ferry, New York, 2007.
Generally, accidental bruising, fractures, and burns are rarely found in infants who are not yet crawling or walking. In older children, accidental injuries, such as those occurring from falls, usually result in contusions over bony prominences. Bruises on the buttocks or other areas of the body are suspicious for abuse.
Sexual abuse should be suspected if bruising is found on the inner thighs. Contusions around the mouth of infants and young children often are the result of force-feeding. Other indicators of abuse include marks resembling finger imprints, which may occur when a child is forcibly held, shaken, or slapped. Injuries that resemble straps, cords, bites, or utensils should be reported to appropriate child abuse agencies.
Many types of burns are associated with child abuse, and these injuries account for 10% of child abuse cases.206 Most occur in children under 10 years of age, with the majority of inflicted burns occurring in children less than 2 years old.206
Immersion burns can be identified by sharply delineated water lines. These are often seen as glove or stocking distribution patterns that result from holding the hands or feet in very hot water. A doughnut pattern may result if a child is held in a tub of scalding water. This pattern occurs when the buttocks are spared from burns because they make contact with the bottom of the tub instead of the hot water that burns the legs and lower trunk. “Sparing” may also occur in the creases of the body and palms of the hands when, as a defensive mechanism, a child will flex the body or hands when held in very hot water.
Contact burns resulting from having hot liquid thrown at a child differ from those resulting when young children pull pots of hot liquid off a stove. In the latter case, the first point of contact occurs on the face, chin, neck, and axilla (because they look up as they reach for the handle) and the flow pattern lessens along the torso. When hot liquids are thrown at a child, the burns are usually not present on the neck and axillary area.
Contact burns that are accidental burns often can be distinguished from intentional burns. Accidental burns tend to be superficial because of the tendency to pull away when something hot is encountered. Brushing against a hot object, such as a cigarette, causes a burn pattern that is shallow and irregular, not the symmetric and deep pattern that occurs when a cigarette is used to intentionally burn a child. These burns are often found inside the palm of the hand or on the back or buttocks. Irons and curling irons may be used to intentionally inflict injury; the therapist must judge whether the explanation of the injury is reasonable and accounts for the child’s age, height, and motor abilities.
Shaken baby syndrome (SBS) generally occurs when a frustrated caregiver shakes an infant vigorously, usually in an attempt to stop crying or other unwanted behaviors. In most cases, there is an unawareness of the dangers of shaking. Shaken baby syndrome usually occurs in infants under 3 years of age and can result in serious, sometimes fatal, injury and disability.
Because of the weakness of an infant’s neck muscles and the size of the head, shaking results in multiple forces of the fragile brain against the skull. This impact can result in direct trauma to the brain, swelling, subdural hematoma, and subarachnoid hemorrhaging. This in turn can lead to traumatic brain injury, seizures, cerebral palsy, brain damage, and death. SBS is the most common cause of mortality in infants,213 and one of four infants dies as the result of being shaken.209
Other sequelae of SBS include retinal hemorrhage, blindness, spinal paralysis, mental retardation, and learning disabilities. Symptoms of SBS include irritability, seizures, vomiting, diminished eating, decreased responsiveness, and changes in breathing. Fractures of the ribs and long bones often accompany SBS. These symptoms of SBS warrant emergency attention. The injuries associated with SBS are not attributable to accidental falls.
The medical history of children should be carefully reviewed since many medical disorders can mimic signs of child abuse. Osteogenesis imperfecta is a collagen defect in which fractures can occur with minimal or even no apparent force. Hemophilia, a clotting factor disorder, often causes persistent bleeding with little or no injury. Illness and medical treatment involving platelet irregularities can also result in excessive bleeding/bruising. Allergies can result in “allergic shiners” that resemble the contusions associated with a “black eye.”
Mongolian spots are darkly pigmented areas caused by entrapment of melanocytes; they are often found on the sacrum or lower back of many African-American and Hispanic infants (Fig. 2-2). Although these spots resem- ble bruises, they do not change in size and fade over a period of years. Another cultural consideration is that contusions may be difficult to perceive in darkly pigmented children. On autopsy, significant bleeding may be found when external injury was not detected.

Figure 2-2 Mongolian spots (congenital dermal melanocytosis). The therapist must be aware of Mongolian spots, which can be mistaken for bruising from child abuse in certain population groups (e.g., Asian, East Indian, Native American, Inuit, African, and Latino or Hispanic heritage). They are also present in about 1 in 10 fair-skinned infants. Mongolian spots are bluish gray to deep brown to black skin markings that often appear on the base of the spine, on the buttocks and back, and even sometimes on the shoulders, ankles, or wrists. Mongolian spots may cover a large area of the back. When the melanocytes are close to the surface, they look deep brown. The deeper they are in the skin, the more bluish they look, often mistaken for signs of child abuse. These spots “fade” with age as the child grows and usually disappear by age 5. (From Goodman CC, Snyder TE: Differential diagnosis for the physical therapist: screening for referral, ed 4, Philadelphia, 2007, WB Saunders. Courtesy Dr. Dubin Pavel.)
Intimate Partner Violence
Although often used synonymously with DV, IPV occurs between current or former partners in both heterosexual and homosexual relationships. Individuals involved may, or may not be, cohabiting or involved in sexual activity. IPV is usually considered to be a recurrent pattern of abuse that often worsens with time. It is responsible for a wide range of injuries and accounts for approximately 33% of homicides of women in the United States.214 Although approximately 92% to 95% of IPV victims are women, men are also victims of abuse.49
Two of the most vulnerable groups at risk for IPV include individuals with disabilities and pregnant women. Women with disabilities have indicated that their primary health concern is abuse,109 which is not surprising when considering that they are twice as likely to be abused as nondisabled women.211
Pregnancy and the postpartum period represent a time of significantly higher risk for IPV. The reported incidence of abuse of pregnant women varies from 0.9% to 24%.94,96,133 These rates indicate that violence during pregnancy is more common than placenta previa, preeclampsia, or gestational diabetes.94 Ferris79 reported that previous abuse is the strongest indicator that abuse will occur during pregnancy. Additionally, if abuse occurs during the first trimester, it will most likely continue in the postpartum period. Often the abuse and injuries worsen throughout the course of the pregnancy.
Physical injury may occur to any area of the body, although there are three frequently occurring patterns associated with IPV. Head, neck, and facial injuries are commonly seen, and this pattern is suggestive of battering. Perciaccante208 found that women involved in IPV were 7.5 times more likely to have sustained head, neck, and facial injuries than women with other forms of trauma. Second, injuries resulting from IPV occur in a central pattern, involving the breasts/chest, abdomen, and genital areas. A third common pattern of injury is suggestive of a defensive posture in which there are bruises, cuts, and/or fractures to the hands or arms, consistent with raising them to protect the head and face. The pattern of injuries resulting from IPV differs from those associated with household and sports-related accidents.
Medical problems frequently encountered as the result of IPV include chronic neck, back, and pelvic pain; headaches; temporomandibular joint dysfunction; and a history of bone fractures and musculoskeletal pain. IPV survivors also have a higher rate of central nervous system symptoms; individuals with traumatic brain injury, mild traumatic brain injury, and postconcussive syndrome should be screened for IPV.
Elder Abuse
Elder abuse is any intentional or negligent act by a caregiver or other person that causes harm, or a serious risk of harm, to an older person. Legislation regarding elder abuse varies widely from state to state and in some states only involves elderly individuals living in their own residence; other states also include those living in long-term care facilities. Generally, elder abuse is defined as occurring in anyone over 60 or 65 years of age.
It is estimated that more than 1.8 million seniors in the United States are victims of abuse.205 The true incidence is difficult to ascertain because many cases of abuse are never reported. The definitions of types of abuse of older adults are similar to those of IPV, although there are some indicators of abuse that are specific to the older adult population.
Physical abuse is more likely to involve the use of physical restraints and over-medication. Emotional/psychologic abuse can involve isolating the elderly from acquaintances and threatening abandonment and placement in a long-term care facility. Financial exploitation, the illegal or improper use of funds or assets, is more common in this age group. Self-neglect occurs when an older person fails to provide for his or her own welfare and medical care. Passive neglect is the nonwillful failure to provide care and often occurs when an elderly person is unable to take care of his or her spouse.
Indicators of elder abuse include being fearful, withdrawn, or hesitant to talk and/or demonstrating signs of depression and extreme changes in mood. Issues in detecting abuse are hampered by the victim’s shame, reluctance to report abuse because of reliance on the perpetrator for financial support, fear that the abuse will worsen, and concern about victimization of other family members or pets. Detection of abuse of older adults is also difficult because so many live in isolation and see few outsiders. Perpetrators of elder abuse may attribute an older person’s complaints of abuse to dementia.
Whenever possible, therapists should attempt to interview seniors in private. Therapists should be alert for explanations that are not compatible with the nature of the injury and delays in seeking prompt medical attention. In the aging adult, additional signs of abuse may include dehydration or malnourishment in the absence of illness, poor skin condition and hygiene, and the presence of sores and pressure ulcers.