Chapter 6 Patient education and self management
KEY POINTS
 Patient education should be planned and have a sound theoretical base, applying health psychology and educational theory to practice.
Patient education should be planned and have a sound theoretical base, applying health psychology and educational theory to practice.INTRODUCTION
Patient education is an essential additive intervention in the care of people with rheumatic diseases. Therapists’ professional codes of conduct emphasise the importance of ensuring patients are provided with adequate information to gain informed consent and enable informed choices about treatment. However, patient education goes beyond just providing information: targeting behaviour, beliefs and attitudes. It may be provided both formally and informally. In either case it should be planned and goal oriented, based on an assessment. Interventions should adopt theoretical models and not only apply educational and counselling methods but a psycho-educational approach. The goal of patient education is self-management, i.e. the patient is empowered and able to take responsibility for the day-to-day management of the illness. Patients are considered as partners in the whole education process.
DEFINING PATIENT EDUCATION
Patient education is any combination of planned and organized learning experiences designed to facilitate voluntary adoption of behaviour and/or beliefs conducive to health (Burckhardt et al 1994).
This definition points out the main issues of patient education: interventions ought to be planned just as in any other therapeutic intervention. This requires assessment of patients’ educational needs, definition of educational goals, clear plans and procedures for achieving these and (re)evaluation. Targets may be attitudes, beliefs, motivation and behaviour. A basic knowledge and understanding of the disease and possible interventions is helpful, but knowledge does not necessarily lead to changes in attitudes and behaviour. A systematic approach should be used as knowledge, attitudes, values, emotions and behaviours influence each other. The patient’s decision for behavioural change is always voluntary – the health professionals’ task is to provide effective interventions and optimal learning situations. A summary of patient education approaches is provided in Table 6.1.
Table 6.1 Summary of patient education approaches
| APPROACH | EDUCATIONAL METHODS | EXAMPLE |
|---|---|---|
| Educational | Information | Using a teaching approach, e.g. short lectures, explanations, written information. |
| Counselling | Counselling | Communication approach, specifically adapted to and reinforcing individual’s motivation |
| Psycho-educational | Cognitive behavioral interventions Motivational interviewing |
Assessing and enabling changes in beliefs and attitudes; problem solving; skills training; goal-setting and contracting; home programmes. |
SELF-MANAGEMENT
Self-management is the ‘individual’s ability to manage the symptoms, treatment, physical and psychosocial consequences and life style changes inherent in living with a chronic condition’ (Barlow et al 2002, Newman et al 2004). This implies several important points:
EMPOWERMENT
Empowerment is a relatively new term in the context of care but is an important aim in relation to self-management. It’s the precondition for and consequence of self-management ability. Empowered patients are able to develop and strengthen their own (health) competencies, such as the appropriate knowledge, attitudes and skills needed to cope with the disease in their own life context (Virtanen et al 2007).
DEVELOPING PATIENT EDUCATION INTERVENTIONS: A 7-STEP APPROACH
Taal et al (1996) suggested a 7-step approach for the development, conduct and evaluation of patient education (Box 6.1). This structure is applied in this chapter.
BOX 6.1 7-step approach to development of patient education
(after Taal et al 1997)
STEP 1: ANALYSE THE PROBLEMS
It has consistently been demonstrated that effective interventions ought to be tailored to the needs of the individual patient. Before developing a patient education intervention, a careful and thorough analysis of the patient’s health behaviour in relation to his/ her health problem is needed. This analysis aims to understand possible determinants for the patient’s coping and self-management abilities.
Coping with a chronic disease is a lifelong and daily challenge. Disease acceptance and coping with a chronic disease is an interaction between person and disease. It matters which life aspects are important to an individual and how the disease interferes in the patient’s life. Limitations in physical ability might be a huge problem for one individual, whereas another person perceives the impact on social networks, e.g. loss of friends, as much more important.
Important factors influencing health behaviour and coping are:
There is evidence that individual beliefs and attitudes are better predictors of patients’ abilities to cope with the illness than disease severity, age or gender (Buchi et al 1998) (Fig. 6.1).
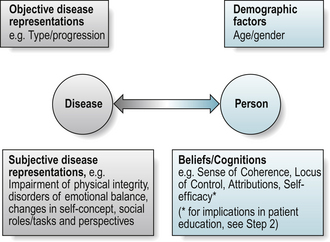
Beliefs or cognitions: sense of coherence, health locus of control, self-efficacy
Sense of coherence (SOC) is considered as an adaptive dispositional orientation (i.e. within the personality) that enables coping with adverse experience (Antonovsky 1979, 1990, Eriksson & Lindstrom 2006). SOC integrates the meaningfulness, comprehensibility and manageability of a situation or disease. The more a person is able to understand and integrate (comprehensibility), to handle (manageability) and to make sense (meaningfulness) of an experience or disease, the greater the individual’s potential to successfully cope with the situation or the disease. As it is a personality trait it is more likely to be a predictor of behaviour than a factor to influence in interventions. High SOC is associated with perceived good health and predictive of positive health outcomes (Eriksson & Lindstrom 2005).
Health locus of control (HLC)(Rotter 1954) differentiates between whether people attribute an outcome to their own abilities or actions and, as such, is under their personal (internal) control (e.g. I did not exercise enough today because I was not in the mood, or did not put in enough effort) or whether an outcome is independent of one’s actions (external control), attributing it to fate or chance (e.g. bad weather, no time, no social support). Findings related to HLC predicting health behaviour are weak and inconsistent (Wallston 1992) (see Ch. 5, Section 4).
Self-efficacy theory is considered as one of the most powerful determinants of behaviour (Bandura 1977). The confidence a person has to successfully execute a specific behaviour or task in the future, i.e. (self)-efficacy expectation, and the person’s belief that the desired behaviour has a positive effect, i.e. outcome expectation, determine the initiation of the process to perform a behaviour, to expend effort and to continue to do so when difficulties are arising (Bandura 1990). (See Ch. 5, Section 4).
Self-efficacy refers to perceived ability in specific domains of activities. It is a specific state, although a variety and range of positive mastery experiences may lead to a general sense of self-efficacy (Bandura 1977). A patient with rheumatoid arthritis (RA) might very well have high self-efficacy to follow a drug prescription correctly but low self-efficacy for using joint protection methods correctly.
Patients with chronic diseases who demonstrate high self-efficacy have a better prediction for rehabilitation outcome (Hammond et al 1999). In people with RA, higher self-efficacy has been shown to be associated with better ability to cope with their disease, as well as with better current (Taal et al 1996) and future (2 and 5 year) health status (Brekke et al 2001, 2003).
Motivation and goal setting
Adopting health behaviours is ‘unfortunately’ not just a logical, rational decision-making process solely dependent on information. Rather it depends on complex interactions, including attitudes to illness, expectations of health, previous experiences of the illness and social pressure (Price 2008).
Motivation for behavioural change is determined by cognitions, emotions and intentions and is central for applying what has been learned. The distinction between approach (success-related) and avoidance (failure-related) motivation is fundamental in explaining human behaviour (Elliot et al 2001). Important factors for effective goals are that they should be:
Compliance, adherence and concordance
In the past, there was much focus on patient’s compliance with treatment. The term compliance denotes following a prescribed regimen, indicating a more passive patient role. This is an inappropriate term in therapy as we work collaboratively with clients. Adherence suggests a more equitable role in which the patient participates in goal-setting and treatment with shared responsibility for outcome (Agras 1989) and probably reflects well the tenacity patients with chronic disease need to maintain behavioral adjustments over their life (-time) (Haynes et al 2002, Price 2008). In relation to medication-taking the term concordance is now commonplace. It refers to the interactional decision-making process in agreeing a management plan between patient and health professional. Partnership may optimise therapy and health gains and discordance is resolved through compromise or agreeing to disagree (Treharne et al 2006). “Concordance” is likely to become a more common term in therapy practice in future.
Adherence to treatment
Non-adherence is considered as one of the main barriers to the effectiveness of treatment interventions (Carr 2001). The following factors are important determinants of adherence:
Social support
Family and friends form a social network that may be a source for social support. However, this may be perceived as positive or problematic, contributing to decreased or increased depression respectively in people with RA. Size and perceived availability of social network contribute to reducing negative affective reactions of patients with RA (Fitzpatrick et al 1988). Support is problematic when it is not needed or desired or when it does not meet the recipient’s needs. Both, positive and problematic support were demonstrated to be associated with coping and depression with arthritis (Revenson et al 1991) and lack of sympathy and understanding from the social network contributes to fatigue (Riemsma et al 1998). Positive and negative social support has the same effects on men and women, but effective social support strategies differ between men and women (Kraaimaat et al 1995). For women, it is their perceived degree of emotional support, whilst for men it is the number of friends that significantly contributes to support.
There are inconsistent findings as to whether family members should participate in self-management education programmes. There are studies reporting no effects (van Lankveld et al 2004) or even negative effects on self-efficacy and fatigue (Riemsma et al 2003a,b). Positive effects have also been identified, such as high levels of satisfaction with social support and positive quality of life outcomes (Minnock et al 2003), quality of marital status and pain severity (Waltz et al 1998).
STEP 2: MAKE USE OF A THEORETICAL MODEL
As with other therapeutic interventions, patient education must be planned and goal oriented, thus including assessment, intervention and evaluation. What are the aims of the new patient education programme you want to develop and thus what elements should be included? Which components have been demonstrated to work successfully in changing patients’ attitudes, beliefs and behaviour? There is a wide range of theories and models to guide practitioners in designing effective and efficient patient education interventions.
Several models and theories are commonly used in patient education.
The Health Belief Model
The Health Belief Model (HBM) (Becker et al 1977) (see Ch. 5) is one of the oldest models but still provides an important framework for designing theory-based interventions, though newer models and their components seem to better explain the complexity of behaviour (and behaviour changes) (Fig. 6.2).
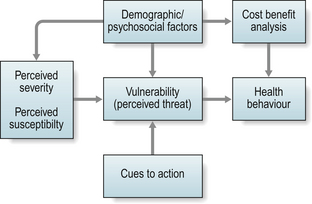
The implications for patient education are:
Low perceived susceptibility may reduce motivation. There is some evidence that increasing worries created by information (e.g. mass media campaigns, information booklets) can help to change (self-reported) health behaviour (Sogaard & Fonnebo 1992).
The Theory of Reasoned Action and Theory of Planned Behaviour
The Theory of Reasoned Action (Fishbein & Ajzen 1975) and the Theory of Planned Behaviour (Ajzen 1985) (see Ch. 5) also consider intention and perceived control as other important determinants for health behaviour. Intention towards a behaviour is shaped by the person’s attitudes and subjective norm (expectancies of social environment) which act as pros and cons towards a behaviour. Perceived control emerged from work on locus of control and perceived self-efficacy and it was assumed that intention and perceived control interact.
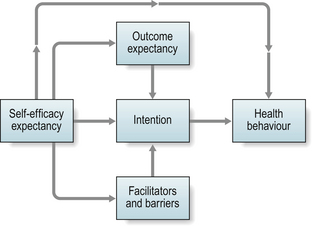
Social Cognitive Theory
Self-efficacy (Bandura 1977, 1990) is a central concept in social cognitive theory and is acquired by direct experience, vicarious experience (role modelling), verbal persuasion and reinterpretation of physiological signals. Action-oriented interventions in occupational and physiotherapy provide unique possibilities to acquire self-efficacy. Direct experience is the most powerful strategy. Success leads to success (see Chs. 5 & 6, Steps 1 & 5) (Fig. 6.3).
The Transtheoretical Model
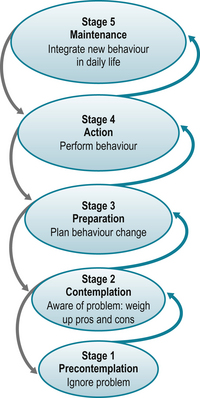
The development of the Transtheoretical Model (TTM) (Prochaska et al 1992) was an important step to better understand behavioural change, demonstrating that individuals cycle through a series of five stages of readiness to change when modifying health behaviours.
In the pre-contemplation and contemplation stages there is no or little problem awareness and thus no intention to change in the future (i.e. the next 3–6 months). In the preparation stage taking action is planned for the near future (i.e. within a month). In the action stage activities are performed to modify behaviour, experiences or the environment and in the maintenance stage the new behaviour is consolidated and integrated into daily life (i.e. it is performed regularly over at least 6 months). Behaviour change takes time and regression, i.e. relapse into previous behaviours, is the rule rather than the exception, visualised by the spiral pattern of the TTM (Fig. 6.4).
The second key construct relates to the processes of change, i.e. the strategies that are important when moving from one stage to the next. In the lower stages (1–3) cognitive and affective strategies are important, whereas in the upper stages (4 and 5) behavioural processes are most important. The TTM states that lower stages of change are associated with lower levels of self-efficacy, in which the cons are more important than the pros. In contrast, in the upper stages behaviour performance is associated with higher levels of self-efficacy and pros outweigh cons.
The implications for patient education are:
Adult Learning-the learning process
Health professionals have the responsibility to fully explore the patient’s situation and tailor interventions based on personal needs, anticipate patients’ difficulties in following recommendations and communicate in a way that is effective (Stone 1979). Learning, i.e. gathering knowledge and skills, is not automatic and has to be enhanced by teaching and methodological choices. Favourable learning situations involve several learning processes. Learning processes do not occur in isolation but in combination (Berlinger et al 2006).
Learning as a self-directed process
Self-directedness (Fig. 6.5) is:
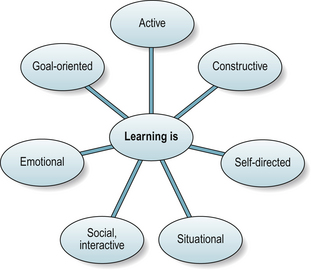
Figure 6.5 Adult learning processes.
After Berlinger et al 2006, with permission of H.E.P Verlag AG.
Learning as a constructive process
Implications for patient education from a learning point of view
People may have one or more learning styles: activists prefer learning through doing; theorists prefer reading and discussion; pragmatists prefer to act and see what they learn from it; reflectors prefer to consider before acting (Honey & Mumford 1992). Adapt teaching to best suit the person’s preferred learning style. In group education, a mix of approaches, particularly a practical, task-focussed approach, is more likely to be effective than solely talks and discussion.
STEP 3: INFLUENCE KNOWLEDGE, BEHAVIOUR AND HEALTH STATUS
Effective patient education enables understanding about the condition and health care, coping, changing health behaviours to self-manage effectively, improving or maintaining health status and reducing health costs. It requires effective teaching and learning strategies. Information giving is an important part, but not all of patient education. Solely providing information does not necessarily mean a person learns or changes. Patient education tailored to the person’s needs is more effective (Lorish et al 1985).
Identifying needs
First, assess and prioritise aspect/s of education to focus on:
Patient education needs are not just informational needs. For example, five people with RA attended occupational therapy and physiotherapy and were given information about joint protection and home exercises. At follow-up, they are honest and tell you they have either not tried or are doing little. Are they all “unmotivated, uncompliant” patients? Asking them why, can identify that their reasons may differ (Table 6.2). In practice, different approaches may then be relevant to enable change.
Table 6.2 Examples of educational needs and patient education actions
| EDUCATIONAL NEED | ACTION |
|---|---|
| Not understanding need to use, e.g. exercise/ joint protection (cognitive need). | Assess readiness to learn. Improve quality of information giving; recheck understanding and recall. |
| Knowing why and how but not wanting to (attitudinal need). | Assess importance of and readiness to change. Explore illness, health and exercise beliefs – any attitudinal barriers? E.g. exercise is ineffective; joint protection irrelevant at this disease stage; other strategies (e.g. diet, herbal remedies) are more effective. Consider psychological strategies (e.g. active listening, counselling, motivational interviewing) to discuss barriers and beliefs. |
| Knowing why, how and want to but lacks confidence (attitudinal need). | Explore self-efficacy for behaviour; assess confidence in and readiness to change. Start at simple, achievable levels building gradually. Goal-setting, collaborative action plans and regular review improve confidence step-by-step. Group programmes provide opportunity to see others succeed (modelling). |
| Wants to but experiencing pain when trying. Observation/ discussion identify performing incorrectly (psychomotor need). | Teach correct techniques step-by-step again, allow adequate practice, with feedback, to improve skill. Check over several sessions. |
| Knowing why, how and want to but not making time (behaviour need). | Habit change helped by discussing: daily and weekly routines; identify possible barriers, collaborative problem solving, discuss times and practice routines. Goal-setting, action plans and review. |
What do people want to learn?
Patient education interventions should be based on identifying target group’s needs (Lorig & Visser 1994). Priorities must be set about what to teach in the time available. Better to teach fewer things well than many badly. Written information can supplement lower priority topics. Determine:
Information needs of an individual can be assessed formally using the Educational Needs Assessment Tool, which identifies the importance of 39 items in seven domains (managing pain, movement, managing feelings, arthritis process, treatment, self-help and support) and is available for rheumatoid arthritis, osteoarthritis, systemic lupus erythematosis, ankylosing spondylitis and connective tissue disease (Hardware et al 2004, Hill et al 2004).
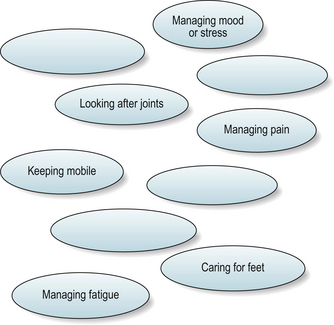
Informally, negotiating multiple behavioural changes may be helped by agenda setting. After gaining rapport, initial data, and open-endedly asking about the person’s information needs, an agenda-setting chart may help identify options. This visually displays their topics of interest or concern and you can then add what you commonly offer (Fig. 6.6). If concerns or topics outside your practice are raised, actively listen and acknowledge these. Concerns may prevent the person gaining education benefits. Explain if you cannot personally address some issue/s and ask if there is action they need to take, referral elsewhere is needed or if airing the concern was sufficient today. Continue identifying topics of interest, allowing time to reflect and discuss options. (“What do you think? How do you feel about any of these?”). Adopt a ‘curious state of mind’ to identify their priorities: “Which of these do you feel most ready to think about changing?” (Rollnick et al 1999).
To plan group programmes, topics can be identified by: surveys with larger numbers of people (items should be generated initially with patients to ensure it is not health professional driven); matrix assessments (e.g. 15–20 people, a variation of the Delphi process), in which the group write individual needs first, then the number interested in each topic is identified and a consensus gained of higher and lower priorities; focus groups (6–12 people) led by a person unfamiliar to the group, to identify concepts; or individual un- or semi-structured interviews (Lorig et al 2001). If the programme will be used widely, the opinions of many people are needed to ensure representativeness.
A survey of people with rheumatoid, inflammatory and psoriatic arthritis (n = 365, disease duration 10.5 (SD 8.5) years; 36% < 5 years) identified: most (70–75%) were ‘very interested’ in learning more about joint protection, keeping mobile, maintaining independence and managing the disease themselves; two thirds (60–69%) about arthritis, its potential future effects and treatment, managing pain, fatigue and mood, and communicating with health professionals; and half (50–55%) about diet, complementary therapies and claiming benefits. There were no significant differences between people with more or less than 5 years disease duration or diagnostic groups (Hammond & Badcock 2002). This helped structure content and priorities within a health-professional-led modular education programme (Hammond et al 2008). The lay-led Arthritis Self-Management Programme is also based on detailed needs assessment (Lorig et al 1985).
Information giving – cognitive change
As well as what to teach we need to consider how to teach it. The majority of people (70%) prefer a patient-centred approach respecting their views, but 30% prefer a biomedical approach demonstrating authority (Swenson et al 2006). Patients’ preferred approach should be determined. Better outcomes are associated with a patient-centred approach. Patients want: clear explanations (oral and written); to lead discussions and ask questions; be listened to and understood; and to remain in control of their condition, which paradoxically can include refusing interventions even when recognising their importance (Ward et al 2007).
Some information giving is factual, e.g. what is arthritis, how does exercise affect joints. But much focuses on helping people change, e.g. why, what, when and how to….for example, exercise. Giving information, talking about action and telling people what to do, rather than asking what they want first and identifying if they are ready to learn, may undermine autonomy (personal freedom) and lead to resistance. This may be apparent though for example, reluctance, arguing, defensiveness, objecting, denial or not following advice. Good consulting enables the person to express their fears about change, without feeling judged or pressurised into action (Rollnick et al 1999).
Information giving is best as information exchange. Useful questions in a patient-centred approach are:
These help elicit readiness to learn. Use open-ended questions to probe for responses, as almost half of people are reluctant to ask questions even if wanting more information (Ley 1988). If they do not want information (pre-contemplation) and are resistive, explore why. Confirm you appreciate change is difficult, they have other demands in life and there are barriers to change. Identify barriers to readiness (see Table 6.2 for examples) and address these. People also have a choice not to learn or to change.
If they are ready, practical considerations are:
Recall of verbal information can be improved by many strategies. (For examples see Box 6.2). Written information should be provided to reinforce verbal information (Box 6.3).
BOX 6.2 Strategies to enhance recall
Simplification-use non-technical words (e.g. bend not flex). Explain technical terms when necessary (e.g. inflammation). Keep explanations short. Use short sentences. Keep to a few key messages each session. Explicit categorisation – structure information to “tell them what you are going to tell them, tell them, and tell them what you told them.” Summarise pre- and post- each topic, and at the beginning and end of the session overall. This helps people encode information more readily. Repetition – ensure key facts are repeated by paraphrasing, and asking the person to repeat back or paraphrase what learnt. Use specific rather than general statements, e.g. rather than “you need to regularly exercise to keep fit,” state “you are aiming to exercise or be physically active five times a week for 30 minutes in total a day getting yourself a little out of breath. We can discuss what you believe is achievable to get started”. Then mutually determine this (e.g. walking 5 minutes a day for 3 days this week).In one-to-one education, adapt teaching to best suit the person’s preferred learning style(s). In group education, a mix of approaches, particularly a practical, task-focused approach, is more effective than talks and discussion. Much of our therapy includes teaching skills (e.g. exercise, joint protection). The more the practical component, with feedback on performance, the better.
Enabling attitudinal changes
Readiness to change (see the Transtheoretical model) and self-efficacy (see Social Cognition theory) influence willingness to make behavioural changes. Such changes require perceiving importance of change, confidence to do so and these influence readiness to make specific behaviour changes (Rollnick et al 1999). Discussion should promote behaviour change-talk to help identify the pros and cons of change and work through any ambivalence towards changing (Table 6.3).
Table 6.3 Three topics to encourage behaviour change talk (after Rollnick et al 1999)
| IMPORTANCE: WHY? | CONFIDENCE: HOW? | READINESS: WHEN? |
|---|---|---|
| Is it worthwhile? | Can I do it? | Shall I do it now? |
| How will it benefit me? | How will I do it? | What about other priorities? |
| Why should I? | How will I cope with doing it? | |
| What will change as a result? | ||
| At what costs? | ||
| Will it make a difference? | ||
| What could happen if I don’t do it? |
Motivational interviewing is a technique for helping people explore their motivations for making changes, based on a collaborative process of listening, exploring values and concerns and guiding to make decisions, respecting autonomy to choose whether to change or not (Rollnick et al 2008). There is a growing body of evidence that it promotes self-management in chronic diseases but has been little evaluated in rheumatic diseases as yet (Shannon & Hillsden 2007). Short training courses are available and texts by Rollnick et al (1999 & 2008) provide practical examples of applying techniques in practice.
STEP 4: TEACH EFFECTIVE SELF-MANAGEMENT SKILLS
Effective skills include exercise, relaxation, joint protection, strategies for coping with pain and stress, communicating effectively with health professionals, problem-solving, and goal-setting. Learning these new skills demands a lot of effort and takes much training time (Taal et al 1996). The content of programmes should be evidence-based using effective evidence-based teaching techniques. People should not just be provided with information (verbally and in written form) but the skills themselves need adequate practice with feedback during education sessions. There should be a structured approach to encouraging people to practice skills sufficiently (Taal et al 1996). Materials and equipment to enable this should be supplied as far as possible to reduce barriers to home practice, and feedback and review provided. The person also needs to know when to apply the skill appropriately. Some techniques are recommended for use permanently (e.g. joint protection) but others vary with health status (e.g. relaxation). The person also needs to know how to modify self-management methods to suit changing needs. This decision-making process also needs discussion.
STEP 5: STRENGTHEN SELF-EFFICACY APPRAISALS AND USE EFFECTIVE METHODS OF TEACHING SELF-MANAGEMENT SKILLS
As the person shifts from precontemplation to contemplation and preparation, a structured approach to strengthening self-efficacy, teaching self-management skills and changing habits and routines is needed.
Strengthening self-efficacy
Social cognitive theory highlights self-efficacy (confidence) is key to enabling behavioural change (Bandura 1977). It can be improved through:
Applying these approaches within education programmes increases use of exercise, relaxation, cognitive symptom and fatigue management, and joint protection (Barlow et al 1998, Hammond et al 2008, Lorig et al 1985, Taal et al 1996).
Effective teaching
Effective teaching requires forward planning to enable effective information and skills learning. The environment should be comfortable, with appropriate temperature and lighting, free of distracting noise, and comfortable seating. Careful consideration should be given to audio-visual aids. For group programmes, whilst powerpoint is ‘professional’ it may take time to set up correctly. Many patients are not familiar with teaching and training environments. It can convey a more ‘formal’ atmosphere, promoting people watching the screen rather than the therapist and each other. A pre-prepared flip-chart is cheaper and less formal. Group comments can be added to spare sheets and it is easily updated as teaching topics change. Careful attention is needed to vary tone of voice. Particularly if a standard programme is being followed, key points and concepts must be taught as stated but not simply ‘read out’ A personalised approach should be taken.
Developing psychomotor skills requires people to form schemas or movement patterns in their minds (Schmidt & Lee 2005). Mackway-Jones and Walker (1999) recommend six stages for teaching:
This means the person will have seen three demonstrations and heard two descriptions before doing it themselves. In a group situation, the last two stages can be shared amongst the group members (working in pairs or threes) with each person trying the skill in turn (see Fig. 6.8). This is much less ‘threatening’ than talking through the skill in front of the whole group and provides further opportunity for modelling. Watching less skilled “demonstrators” allows opportunities to problem-solve when others make mistakes.

Behavioural approaches and goal-setting
Change is the person’s responsibility. But there can be barriers to changing behaviour, including not having (making) the time, and forgetting. Once the person knows how to perform a specific skill, regular practice is needed to consolidate skill and develop new habits and routines. Teaching people how to set long and short-term goals and action plans helps promote this. Long term goals are what they wish to achieve from the education. Short-term are the steps to achieve this. Short-term goals should state: what, how much, when, how often and the time frame. Getting people to write goals down, and/or say aloud in a group what they intend to do, increases the likelihood they will fulfill them. Goals should be what the person wants to do, not what the therapist expects them to do. An example of applying behavioural approaches in education can be found in Chapter 10.
STEP 6: THE INVOLVEMENT OF PEOPLE FROM THE PERSON’S SOCIAL ENVIRONMENT
Using self-management effectively will be helped by support from significant others. As discussed above, there is conflicting evidence for the effectiveness of including significant others in education programmes. Keefe et al (1996) identified people attending a group OA programme with their spouse did better than those attending without a spouse in terms of improved pain and disability. However, Riemsma et al (2003a) in a trial with people with RA found that those in a spouse-attended group fared worse than those attending non-spouse attended groups. Post-education interviews identified those attending groups without spouses felt more able to discuss their problems openly without fear of upsetting those close to them. Having significant others attend is thus not always helpful. But encouraging their involvement through asking patients to share information materials with relatives and getting them to assist in practice is important. This allows the person to decide on the degree of involving relatives, as not all are supportive. Providing a carers-only education meeting is also beneficial.
STEP 7: PROPER EVALUATION OF INTERVENTION EFFECTIVENESS
Outcomes most relevant to the aims of the intervention provided should be selected.
Further generic and disease specific arthritis measures are described and reviewed in Katz (2003), Lorig et al (1996) and in Chapter 4.
EVIDENCE FOR PATIENT EDUCATION INTERVENTIONS
Effectiveness depends on the quality and type of education provided.
ONE-TO-ONE WRITTEN AND VERBAL INFORMATION GIVING
Individual education is the commonest provided in practice. Surprisingly, there is relatively little evidence for effectiveness in arthritis. Written information has been evaluated in several studies. Barlow et al (1997b, Barlow & Wright 1998) conducted a randomised controlled trial (n = 108) evaluating the arc (Arthritis Research Campaign) RA booklet with people with established RA (15 years duration). Knowledge about arthritis and treatment, mood, reassurance and coping significantly improved. Walker et al (2007) tested the additional effect of a mind map in people with RA alongside the arc RA booklet (n = 363; 13 years duration). Knowledge significantly improved but those with low literacy (15% of participants) did not. Good quality written information is important but those functionally illiterate need good quality, structured verbal information giving.
The evidence for effectiveness of individual verbal education is less clear. A trial (n = 150) comparing receiving a booklet on RA, treatment, and self-management methods with 1 hour of individualised instruction from a therapist plus the booklet found both groups significantly improved knowledge in comparison to usual care only, suggesting additional individual education was redundant (Maggs et al 1996). However, attitudinal (eg self-efficacy) and behavioural changes were not evaluated.
There are few studies of education provided during routine appointments. Riemsma et al (1997) randomised people with established RA (n = 216; average 13 years duration) to three groups: (1) usual care (i.e. information giving during routine appointments as necessary from a rheumatology nurse); (2) usual care plus an arthritis self-help book; and (3) structured one-to-one education based on the provided self-help book during routine appointments. Nurses in the latter group received training in education, goal-setting and progress review. All groups improved similarly, suggesting structured behavioural education was no more effective than “ad hoc” information giving. However, nurses providing structured education reported difficulty applying it in routine practice due to time constraints. Hill et al (2001) compared structured 1:1 education (7 × 30 minute sessions), provided by a rheumatology nurse using a self-efficacy approach, about RA, drug treatment and self-management, with routine out-patient care (i.e. ad hoc information giving) (n = 100; disease duration 12 years). Significant improvements occurred in knowledge and drug therapy concordance in the education group but not health status. Attitudinal and health behaviour change were not evaluated. Sufficient time for education is needed to be effective. Further studies of individualised education are needed to identify the most effective and cost-effective methods, particularly to enable health behaviour changes.
GROUP EDUCATION
Riemsma et al (2003b) reviewed group patient education trials from 1966–1998 for people with RA specifically. Education had small but significant effects on disability, joint counts, patients’ global assessment and psychological status (anxiety and depression) at 3 months, but not 12 months. Few studies conducted longer-term follow-ups. They further compared:
Only behavioural interventions showed significant effects. Other reviews have identified longer-term benefits result from behavioural patient education in RA, improving pain, functional ability and tender joint counts (Hirano et al 1994, Superio-Cabuslay et al 1996).
HEALTH PROFESSIONAL LED GROUP PROGRAMMES
Recently, trials of health-professional led cognitive-behavioural therapy (CBT) approach group education have shown mixed results. For example, a five session programme (12.5 hours) of relaxation, psychological coping, managing pain and mood using CBT approaches, with didactic teaching about RA, medication, joint protection and thermotherapy was compared to usual care (n = 79; RA duration 13 years; 7 facilitators) (Kirwan et al 2005). Patient knowledge improved, but at 8 months no significant differences in pain, self-efficacy, mood or health status occurred.
An eight session programme (52 hours) teaching active coping strategies, diet, relaxation and exercise using CBT approaches with didactic teaching about RA and medication was compared to usual care (n = 208; RA duration 13 years; 10 facilitators) (Giraudet-le Quintrec et al 2007). At 1 year, knowledge and helplessness improved but not health behaviours or health status.
A nine session modular programme (22.5 hours) using CBT approaches including joint protection, exercise, managing fatigue, mood and pain with information about RA and medication was compared to a five session (10 hour) programme teaching similar content but not using CBT approaches (n = 167; disease duration 7 years) (Hammond et al 2008). At one year, the modular programme led to significant improvements in pain, self efficacy, use of health behaviours and health status. As well as applying CBT approaches, reflection about the personal need for change was encouraged. Modules were led by one facilitator to promote continuity discussing about the personal impact of arthritis and change. Small group practice actively promoted modelling (Hammond 2003). How programmes are taught matters.
LAY-LED GROUP ARTHRITIS EDUCATION PROGRAMMES
Substantial research has been undertaken evaluating the Arthritis Self-Management Programme (ASMP). This 15 hour programme uses CBT approaches and is equally effective delivered by trained lay leaders as health professionals (Lorig et al 1986), improves self-efficacy, health behaviours and health status for at least 4 years and reduces health care costs (Lorig et al 1993) and is effective in the UK (Barlow et al 1998). The full 15 hour programme is significantly more effective than shortened versions (Lorig et al 1998) and than a generic chronic disease self-management programme (Lorig et al 2005). A mail delivered and an internet delivered version of the ASMP have been tested, with similar results to the small group programme (Lorig et al 2004, 2008).
Most ASMP studies have been with community recruited volunteers, who may be particularly motivated. Is it effective when delivered to people recruited from primary care? A UK study (n = 812) recruited people with hip or knee OA (average age 68 years) from 74 GP Practices. A third did not attend. At 1 year, the ASMP reduced anxiety and increased self-efficacy for symptom management but did not affect health status or health care use (Buszewicz et al 2006). A US study (n = 187) of people with either RA, OA or fibromyalgia recruited from primary care identified at 4 months there was no difference between ASMP and control groups for any health status or satisfaction measures (Solomon et al 2002). The authors suggest that primary care participants may be more representative of people with arthritis and thus evidence from studies with volunteers is not necessarily generalisable. Nevertheless, for volunteers it is effective.
On average, ASMP participants in community trials are 70 years old, with 15 years disease duration and 72% have OA (Bruce et al 2007). Is the ASMP equally effective in OA, RA and fibromyalgia? The recent internet-based ASMP trial identified it was significantly effective in OA in improving pain, fatigue, disability, self-efficacy, self-reported health and reducing distress. In RA it was significantly effective in improving pain and self-reported health. It was not effective in fibromyalgia (Lorig et al 2008).
Trials of patient education in other conditions have similarly shown marked differences in outcomes. Further research is needed to identify what are effective patient education processes, who benefits most from such group programmes and what strategies maintain changes longer-term.
CONCLUSION
Brady et al (2000) recommended all team members help people with arthritis in perceiving that self-management is valuable. Regular encouragement is needed to help people commence using a variety of self-management methods and ongoing support is needed to help maintain it. If group programmes are available, repeated offers to refer should be given. People may not initially wish to attend, but may want to do so in the future. People may be at different stages of change for different strategies and their use of methods will wax and wane as their arthritis and life events vary over time. Patient education is a long-term process not just a one-off event.
http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4070141 “Toolkit for Producing Patient Information.” – guidance on how to produce written information for patients. (accessed March 2009).
www.motivationalinterviewing.org Information on techniques and training resources. (accessed March 2009).
http://www.crd.unimelb.edu.au/heiq/ Information about the Health Education Impact Questionnaire. (accessed March 2009).
http://www.patienteducation.stanford.edu/programs/asmp.html Arthritis self-Management Programme website (includes access to relevant programme evaluation questionnaires). (accessed March 2009).
References and further reading
Agnew P.J., Maas F. Compliance in wearing wrist working splints. J. Occup. Ther. J. Res.. 1995;15(3):165-180.
Agras W.S. Understanding compliance with the medical regimen: the scope of the problem and a theoretical perspective. Arthritis Care Res.. 1989;2(3):S2-S7.
Ajzen I. From intentions to actions: A theory of planned behavior. In: Action Control: From Cognitions To Behaviour. Seattle WA: Hogrefe & Huber; 1985:11-39.
Antonovsky A. Health, Stress and Coping. San Francisco: Jossey-Bass; 1979.
Antonovsky A. Personality and health: testing the sense of coherence model. In: Friedman H.S., editor. Personality and Disease. New York: Wiley; 1990:155-177.
Bandura A. Self-efficacy: towards a unifying theory of behaviour change. Psychol. Rev.. 1977;84:191-215.
Bandura A. Self-regulation of motivation through anticipatory and self-reactive mechanisms. Nebr. Symp. Motiv.. 1990;38:69-164.
Barlow J.H., Williams B., Wright C.C. The reliability and validity of the arthritis self-efficacy scale in a UK context. Psychol. Health Med.. 1997;2:3-17.
Barlow J.H., Pennington J.C., Bishop P.E. Patient education leaflets for people with rheumatoid arthritis: a controlled study. Psychol. Health Med.. 1997;2(3):221-235.
Barlow J.H., Wright C.C. Knowledge in patients with rheumatoid arthritis: a longer-term follow-up of a randomized controlled trial of patient education leaflets. Br. J. Rheumatol.. 1998;37:373-376.
Barlow J.H., Turner A.P., Wright C.C. Long-term outcomes of an arthritis self-management programme. Br. J. Rheumatol.. 1998;37:1315-1319.
Barlow J., Wright C., Sheasby J., et al. Self-management approaches for people with chronic conditions: a review. Patient Educ. Couns.. 2002;48:177-187.
Becker M.H., Haefner D.P., Kasl S.V., et al. Selected psychosocial models and correlates of individual health-related behaviors. Med. Care. 1977;15(Suppl. 5):27-46.
Berlinger, D., Birri, T., Zumsteg, B., 2006. Didactic principles for effective practice. In: From Practice to Practice, From Learning to Teaching (in German). aeb series, Bern, Switzerland, pp. 96–100.
Brady T.J., Sniezek J.E., Conn D.L. Enhancing patient self-management in clinical practice. Bull. Rheum. Dis.. 2000;49(7):1-4.
Brekke M., Hjortdahl P., Kvien T.K. Self-efficacy and health status in rheumatoid arthritis: a two-year longitudinal observational study. Rheumatology. 2001;40(4):387-392.
Brekke M., Hjortdahl P., Kvien T.K. Changes in self-efficacy and health status over 5 years: a longitudinal observational study of 306 patients with rheumatoid arthritis. Arthritis Rheum.. 2003;49(3):342-348.
Bruce B., Lorig K., Laurent D. Participation in patient self-management programs. Arthritis Rheum.. 2007;57(5):851-854.
Brus H., van de Laar M., Taal E., et al. Determinants of compliance with medication in patients with rheumatoid arthritis: the importance of self-efficacy expectations. Patient Educ. Couns.. 1999;36(1):57-64.
Buchi S., Sensky T., Sharpe L., et al. Graphic representation of illness: a novel method of measuring patients’ perceptions of the impact of illness. Psychother. Psychosom.. 1998;67(4–5):222-225.
Burckhardt C.S., Lorig K., Moncur C., et al. Arthritis and musculoskeletal patient education standards. Arthritis Found. Arthritis Care Res.. 1994;7:1-4.
Buszewicz M., Rait G., Griffin M., et al. Self management of arthritis in primary care: a randomised controlled trial. Br. Med. J.. 2006;333(7574):879-883.
Callahan L.F., Brooks R.F., Pincus T. Further analysis of learned helplessness in arthritis using a “Rheumatology Attitudes Index.”. J. Rheumatol.. 1988;15:418-426.
Carr A. Barriers to the effectiveness of any intervention in OA. Best Pract. Res. Clin. Rheumatol.. 2001;15(4):645-656.
Department of Health, 2003. Toolkit for producing patient information, V2.0 http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_4070141 (accessed 27.11.08).
Elliot A.J., Chirkov V.I., Kim Y., et al. A cross-cultural analysis of avoidance (relative to approach) personal goals. Psychol. Sci.. 2001;12(6):505-510.
Emmons R.A. Abstract versus concrete goals: personal striving level, physical illness, and psychological well-being. J. Pers. Soc. Psychol.. 1992;62(2):292-300.
Eriksson M., Lindstrom B. Validity of Antonovsky’s sense of coherence scale: a systematic review. J. Epidemiol. Community Health. 2005;59(6):460-466.
Eriksson M., Lindstrom B. Antonovsky’s sense of coherence scale and the relation with health: a systematic review. J. Epidemiol. Community Health. 2006;60(5):376-381.
Fishbein M., Ajzen I. Belief, Attitude, Intention and Behaviour. An Introduction to Theory and Research. Reading, MA: Addison-Wesley; 1975.
Fitzpatrick R., Newman S., Lamb R., et al. Social relationships and psychological well-being in rheumatoid arthritis. Soc. Sci. Med.. 1988;27(4):399-403.
Garcia Popa-Lisseanu M.G., Greisinger A., Richardson M., et al. Determinants of treatment adherence in ethnically diverse, economically disadvantaged patients with rheumatic disease. J. Rheumatol.. 2005;32(5):913-919.
Giraudet-LeQuintrec J.-S., Mayoux-Benhamou A., Ravaud P., et al. Effect of a collective educational program for patients with rheumatoid arthritis: a prospective 12-month randomised controlled trial. J. Rheumatol.. 2007;34(8):1684-1691.
Hammond A., Lincoln N., Sutcliffe L. A crossover trial evaluating an educational-behavioural joint protection programme for people with rheumatoid arthritis. Patient Educ. Couns.. 1999;40:1044-1051.
Hammond A., Badcock L. Improving education about arthritis: identifying the educational needs of people with chronic inflammatory arthritis. Rheumatology. 2002;41(Suppl. 1):87(216).
Hammond A. Patient education: helping people change. Musculoskeletal Care. 2003;1(2):84-97.
Hammond A., Bryan J., Hardy A. Effects of a modular behavioural arthritis education programme: a pragmatic parallel-group randomised controlled trial. Rheumatology. 2008;47(11):1712-1718.
Hardware B., Lacey E.A., Shewan J. Towards the development of a tool to assess educational needs in patients with arthritis. Clin. Eff. Nurs.. 2004;8(2):111-117.
Haynes R.B., McDonald H.P., Garg A.X. Helping patients follow prescribed treatment: clinical applications. JAMA. 2002;288(22):2880-2883.
Hennell S.L., Brownsell C., Dawson J.K. Development, validation and use of a patient knowledge questionnaire (PKQ) for patients with early rheumatoid arthritis. Rheumatology. 2004;43:467-471.
Hewlett S., Cockshott Z., Kirwan J., et al. Development and validation of a self-efficacy scale for use with British patients with Rheumatoid Arthritis (RASE). Rheumatology. 2001;40:1221-1230.
Hill J., Bird H.A., Hopkins R. The development and use of a patient knowledge questionnaire. Br. J. Rheumatol.. 1991;30:45-49.
Hill J., Bird H., Johnson S. Effect of patient education on adherence to drug treatment for rheumatoid arthritis: a randomised controlled trial. Ann. Rheum. Dis.. 2001;60:869-875.
Hill J., Tennant A., Adebajo A. Further development of an educational needs tool (ENAT) for patients with rheumatoid arthritis. Arthritis Rheum.. 2004;50(Suppl. 9):616.
Hirano P.C., Laurent D.D., Lorig K. Arthritis patient education studies: 1987–1991: a review of the literature. Patient Educ. Couns.. 1994;24:9-54.
Honey P., Mumford A. The Manual of Learning Styles. Honey, Ardingly House: Berkshire; 1992.
Katz, P. (Ed.), 2003. Patient outcomes in rheumatology. Arthritis Care Res. 49 (S5) S1–S244.
Keefe F.J., Caldwell D.S., Baucom D., et al. Spouse-assisted coping skills training in the management of osteoarthritic knee pain. Arthritis Care Res.. 1996;9(4):279-291.
Keefe F.J., Lefebvre J.C., Kerns R.D., et al. Understanding the adoption of arthritis self-management: stages of change profiles among arthritis patients. Pain. 2000;87(3):303-313.
Kirwan J.R., Hewlett S., Cockshott Z., et al. Clinical and psychological outcomes of patient education in rheumatoid arthritis. Musculoskelet. Care. 2005;3(1):1-16.
Kraaimaat F.W., Van Dam-Baggen R.M., Bijlsma J.W. Association of social support and the spouse’s reaction with psychological distress in male and female patients with rheumatoid arthritis. J. Rheum.. 1995;22(4):644-648.
Lempp H., Scott D.L., Kingsley G.H. Patients’ views on the quality of health care for rheumatoid arthritis. Rheumatology. 2006;45(12):1522-1528.
Ley P. Communicating with Patients: improving communication, satisfaction and compliance. London: Chapman and Hall, 1988.
Lineker S.C., Badley E.M., Hughes E.A., et al. Development of an instrument to measure knowledge in individuals with rheumatoid arthritis: the ACREU rheumatoid arthritis knowledge questionnaire. J. Rheum.. 1997;24:647-653.
Lorig K., Chastain R., Ung E., et al. Development and evaluation of a scale to measure perceived self efficacy in people with arthritis. Arthritis Rheum.. 1985;23:37-44.
Lorig K., Feigenbaum P., Regan C., et al. A comparison of lay-taught and professional – led self-management courses. J. Rheum.. 1986;13:763-767.
Lorig K., Mazonson P.D., Holman H.R. Evidence suggesting that health education for self-management in patients with chronic arthritis has sustained health benefits while reducing health care costs. Arthritis Rheum.. 1993;36(4):439-446.
Lorig K., Visser A. Arthritis patient education standards: a model for the future. Patient Educ. Couns.. 1994;24:3-7.
Lorig K., Stewart A., Ritter P., et al. Outcome Measures for Health Education and other Health care Interventions. Thousand Oaks, CA, USA: Sage; 1996.
Lorig K., Gonzalez V.M., Laurent D., et al. Arthritis self-management variations : three studies. Arthritis Care Res.. 1998;11(6):448-455.
Lorig K., et al. Patient Education: A Practical Approach, third ed. London: Sage; 2001.
Lorig K., Ritter P.L., Laurent D., et al. Long-term randomized controlled trials of tailored-print and small-group arthritis self-management interventions. Med. Care. 2004;42(4):346-354.
Lorig K.R., Ritter P.L., Laurent D.D., et al. The internet-based arthritis self-management program: a one-year randomized trial for patients with arthritis or fibromyalgia. Arthritis Rheum.. 2008;59(7):1009-1017. 0004-3591
Lorig K., Ritter P.L., Plant K. A disease-specific self-help program compared with a generalized chronic disease self-help program for arthritis patients. Arthritis Care Res.. 2005;53(6):950-957.
Lorish C.D., Parker J., Brown S. Effective patient education: a quasi-experimental study comparing an individualised strategy with a routinised strategy. Arthritis Rheum.. 1985;28:1289-1297.
Lubrano E., Helliwell P., Parson W., et al. Patient education in psoriatic arthritis: a cross-sectional study on knowledge by a validated self-administered questionnaire. J. Rheum.. 1998;25(8):1560-1565.
Lubrano E., Helliwell P., Moreno P., et al. The assessment of knowledge in ankylosing spondylitis patients by a self-administered questionnaire. Br. J. Rheumatol.. 1998;37:437-441.
Mackway-Jones K., Walker M. Pocket guide to Teaching for Medical Instructors. London: BMJ Books, 1999.
Maggs F.M., Jubb R.W., Kemm J.R. Single blind randomized controlled trial of an educational booklet for patients with chronic arthritis. Br. J. Rheumatol.. 1996;35:775-777.
Meenan R.F., Mason J.H., Anderson J.J., et al. AIMS2: the content and properties of a revised and expanded Arthritis Impact Measurement Scales health status questionnaire. Arthritis Rheum.. 1992;35:1-10.
Minnock P., Fitzgerald O., Bresnihan B. Quality of life, social support, and knowledge of disease in women with rheumatoid arthritis. Arthritis Rheum.. 2003;49(2):221-227.
Neame R., Hammond A. Beliefs about medications: a questionnaire survey of people with rheumatoid arthritis. Rheumatology. 2005;44(6):762-767.
Newman S., Steed L., Mulligan K. Self-management interventions for chronic illness. Lancet. 2004;364(9444):1523-1537.
Osborne R.H., Elsworth G.R., Whitfield K. The Health Education Impact Questionnaire (heiQ): An outcomes and evaluation measure for patient education and self-management interventions for people with chronic conditions. Patient Educ. Couns.. 2007;66(2):192-201.
Pincus T., Yazici Y., Bergman M. Development of a multidimensional health assessment questionnaire (MDHAQ) for the infrastructure of standard clinical care. Clin. Exp. Rheum.. 2005;23(5, Suppl. 39):S19-S28.
Price P. Education, psychology and ‘compliance’. Diabetes Metab. Res. Rev.. 2008;24(Suppl.1):S101-S105.
Prochaska J.O., DiClemente C.C., Norcross J.C. In search of how people change. Applications to addictive behaviors. Am. Psychol.. 1992;47(9):1102-1114.
Revenson T.A., Schiaffino K.M., Majerovitz S.D., et al. Social support as a double-edged sword: the relation of positive and problematic support to depression among rheumatoid arthritis patients. Soc. Sci. Med.. 1991;33(7):807-813.
Riemsma R.P., Tall E., Brus H.L., et al. Coordinated individual education with an arthritis passport for patients with rheumatoid arthritis. Arthritis Care Res.. 1997;10(4):238-249.
Riemsma R., Rasker J., Taal E., et al. Fatigue in rheumatoid arthritis: the role of self-efficacy and problematic social support. Br. J. Rheumatol.. 1998;37(10):1042-1046.
Riemsma R., Taal E., Rasker J. Group education for patients with rheumatoid arthritis and their partners. Arthritis Rheum.. 2003;49(4):556-566.
Riemsma, R.P., Kirwan, J., Rasker, J., et al., 2003b. Patient education for adults with rheumatoid arthritis. Cochrane Database of Syst. Rev. (2) CD003688.
Rollnick S., Mason P., Butler C. Health Behaviour Change: A Guide for Practitioners. Edinburgh: Churchill Livingstone, 1999.
Rollnick S., Miller W.R., Butler C.C. Motivational Interviewing in Health Care: Helping Patients Change Behaviour. New York: Guilford Press, 2008.
Rotter, J.B., 1954. Social Learning and Clinical Psychology. Englewood Cliffs, NJ.
Schmidt R.A., Lee T. Motor Control and Learning: A Behavioural Emphasis, fourth ed. Human Kinetics Europe Ltd; 2005.
Shannon R., Hillsden M. Motivational interviewing in musculoskeletal care. Musculoskelet. Care. 2007;5(4):206-215.
Siegert R.J., Taylor W.J. Theoretical aspects of goal-setting and motivation in rehabilitation. Disability Rehabil.. 2004;26(1):1-8.
Sogaard A.J., Fonnebo V. Self-reported change in health behaviour after a mass media-based health education campaign. Scand. J. Psychol.. 1992;33(2):125-134.
Solomon D., Warsi A., Brown-Stevenson T., et al. Does self-management education benefit all populations with arthritis? A randomised controlled trial in a primary care physician network. J. Rheum.. 2002;29(2):362-368.
Stone G.C. Patient compliance and the role of the expert. J. Soc. Issues. 1979;5:34-59.
Superio-Cabuslay E., Ward M.M., Lorig K. Patient education interventions in osteoarthritis and rheumatoid arthritis. A meta-analysis comparison with non-steroidal anti-inflammatory drug treatment. Arthritis Care and Res.. 1996;9:292-301.
Swenson S.L., Zettler P., Lo B. ‘She gave it her best shot right away’: patient experiences of biomedical and patient-centered communication. Patient Educ. Couns.. 2006;61(2):200-211.
Taal E., Rasker J.J., Wiegman O. Patient Education and self-Management in the Rheumatic Diseases: a self-efficacy approach. Arthritis Care Res.. 1996;9(3):229-238.
Teutsch C. Patient-doctor communication. Med. Clin. North Am.. 2003;87(5):1115-1145.
Treharne G.J., Lyons A.C., Hale E.D., et al. ‘Compliance’ is futile but is ‘concordance’ between rheumatology patients and health professionals attainable? Rheumatology. 2006;45(1):1-5.
van Lankveld W., van Helmond T., Naring G., et al. Partner participation in cognitive-behavioral self-management group treatment for patients with rheumatoid arthritis. J. Rheum.. 2004;31(9):1738-1745.
Veehof M.M., Taal E., Willems M.J. Determinants of the use of wrist working splints in rheumatoid arthritis. Arthritis Rheum.. 2008;59(4):531-536.
Virtanen H., Leino-Kilpi H., Salantera S. Empowering discourse in patient education. Patient Educ. Couns.. 2007;66(2):140-146.
Walker D., Adebajo A., Heslop P., et al. Patient education in rheumatoid arthritis: the effectiveness of the ARC booklet and the mind map. Rheumatology. 2007;46:1593-1596.
Wallston K. Hocus-pocus, the focus isn’t strictly on locus: Rotter’s social learning theory modified for health. Cognit. Ther. Res.. 1992;16:183-199.
Waltz M., Kriegel W., van’t Pad Bosch P. The social environment and health in rheumatoid arthritis: marital quality predicts individual variability in pain severity. Arthritis Care Res.. 1998;11(5):356-374.
Ward V., Hill J., Hale C., et al. Patient priorities of care in rheumatology out-patient clinics: a qualitative study. Musculoskelet. Care. 2007;5(4):216-228.
Watson D., Clark L.A., Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J. Pers. Soc. Psychol.. 1988;54(6):1063-1070.