14 Dento-osseous Structures, Blood Vessels, and Nerves
The development of the dentitions has been discussed and a brief review of the development of the neurocranium and splanchnocranium has been presented in Chapter 2. Therefore, in this chapter the focus is on the dentoalveolar and dento-osseous structures of the permanent dentition. The forms of the roots of the teeth and their sizes and angulations govern the shape of the alveoli in the jawbones, and this in turn shapes the contour of the dento-osseous portions facially.
The osseous structures that support the teeth are the maxilla and the mandible. The maxilla, or upper jaw, consists of two bones: a right maxilla and a left maxilla sutured together at the median line. Both maxillae in turn are joined to other bones of the head (Figure 14-1). The mandible, or lower jaw, has no osseous union with the skull and is a movable (ginglymoarthrodial) joint.
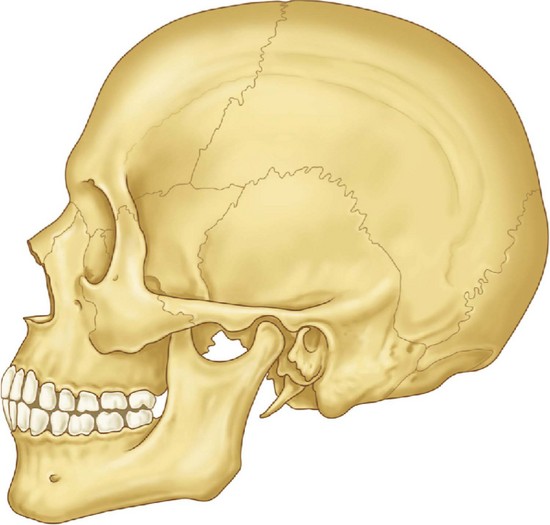
Figure 14-1 Representation of an adult skull with permanent dentition. The maxilla consists of a body and four processes (malar, nasal, alveolar, and palatine) that articulate by synarthrosis with cranial and other facial bones, (e.g., frontal, nasal, ethmoid, malar bones). The mandible articulates with the temporal bone by the temporomandibular joint (see Figure 15-6).
The Maxillae
The maxillae make up a large part of the bony framework of the facial portion of the skull. They form the major portion of the roof of the mouth, or hard palate, and assist in the formation of the floor of the orbit and the sides and base of the nasal cavity. They support the 16 permanent maxillary teeth.
Each maxilla is an irregular bone, somewhat cuboidal in shape, which consists of a body and four processes: the zygomatic, frontal, palatine, and alveolar processes. The maxilla is hollow and contains the maxillary sinus air space, also called the antrum of Highmore. From the dental viewpoint, in addition to its general shape and the processes mentioned, several landmarks on this bone are among the most important, including the incisive fossa, canine fossa, canine eminence, infraorbital foramen, posterior alveolar foramina, maxillary tuberosity, pterygopalatine fossa, and incisive canal.
The body of the maxilla has the following four surfaces: anterior or facial, infratemporal, orbital, and nasal.
ANTERIOR SURFACE
The anterior or facial surface (Figures 14-2 and 14-3) is separated above from the orbital aspect by the infraorbital ridge. Medially it is limited by the margin of the nasal notch, and posteriorly, it is separated from the posterior surface by the anterior border of the zygomatic process, which has a confluent ridge directly over the roots of the first molar. The ridge corresponding to the root of the canine tooth is usually the most pronounced and is called the canine eminence.
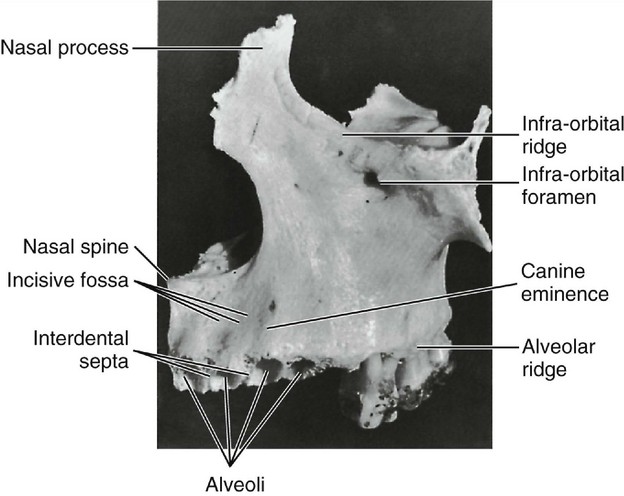
Anterior to the canine eminence, overlying the roots of the incisor teeth, is a shallow concavity known as the incisive fossa. Posterior to the canine eminence on a higher level is a deeper concavity called the canine fossa. The floor of this canine fossa is formed in part by the projecting zygomatic process. Above this fossa and below the infraorbital ridge is the infraorbital foramen, the external opening of the infraorbital canal. The major portion of the canine fossa is directly above the roots of the premolars.
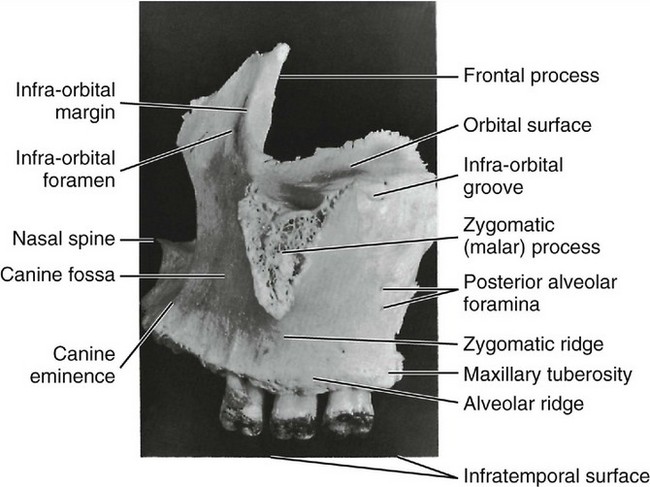
POSTERIOR SURFACE
The posterior or infratemporal surface (Figures 14-3 and 14-4) is bounded above by the posterior edge of the orbital surface. Inferiorly and anteriorly, it is separated from the anterior surface by the zygomatic process and the zygomatic ridge, which runs from the inferior border of the zygomatic process to the alveolus of the maxillary first molar. This surface is more or less convex and is pierced in a downward direction by two or more posterior alveolar foramina. These two canals are on a level with the lower border of the zygomatic process and are somewhat distal to the roots of the third molar.
The inferior portion of this surface is more prominent where it overhangs the root of the third molar and is called the maxillary tuberosity. Medially, this tuberosity is limited by a sharp, irregular margin that articulates with the pyramidal process of the palatine bone and, in some cases, the lateral pterygoid plate of the sphenoid bone. The maxillary tuberosity is the origin for some fibers of the medial pterygoid muscle.
A portion of the infratemporal surface superior to the maxillary tuberosity is the anterior boundary to the pterygomaxillary fissure.
ORBITAL SURFACE
The orbital surface is smooth and together with the orbital surface of the zygomatic bone forms the floor of the orbit. The junction of this surface and the anterior surface forms the infraorbital margin or ridge, which runs superiorly to form part of the nasal process. Its posterior border or edge coincides with the inferior boundary of the inferior orbital fissure.
The thin medial edge of the orbital surface is notched anteriorly, forming the lacrimal groove. Behind this groove, it articulates for a short distance with the lacrimal bone, then for a greater length with a thin portion of the ethmoid bone, and terminates posteriorly in a surface that articulates with the orbital process of the palatal bone. Its lateral area is continuous with the base of the zygomatic process (see Figure 14-3).
Traversing the posterior portion of the orbital surface is the infraorbital groove. This groove begins at the center of the posterior surface and runs anteriorly. The anterior portion of this groove is covered, becoming the infraorbital canal, the anterior opening of which is located directly below the infraorbital ridge on the anterior surface.
If the covered portion of this canal were to be laid open, the orifices of the middle and anterior superior alveolar canal would be seen transmitting the corresponding vessels and nerves to the premolars, canines, and incisor teeth.
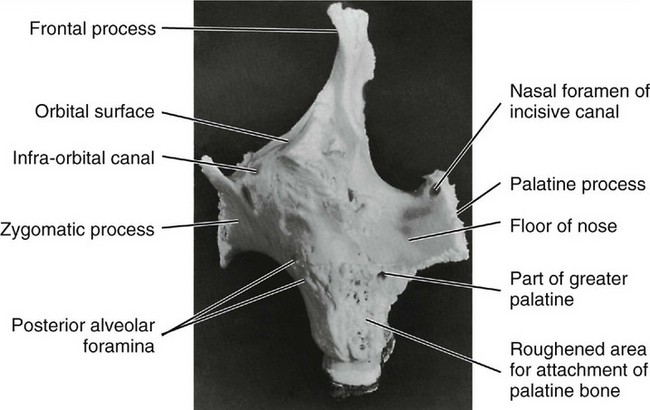
NASAL SURFACE
The nasal surface (Figures 14-5 and 14-6) is directed medially toward the nasal cavity. It is bordered below by the superior surface of the palatine process. Anteriorly, it is limited by the sharp edge of the nasal notch. Above and anteriorly, it is continuous with the medial surface of the frontal process. Behind this, it is deeply channeled by the lacrimal groove, which is converted into a canal by articulation with the lacrimal and inferior turbinate bones.
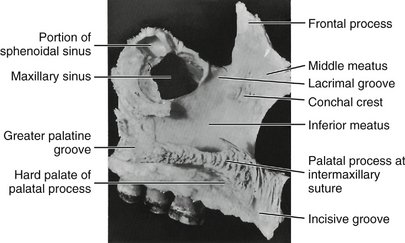
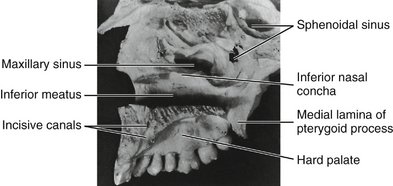
Figure 14-6 Medial view of right maxilla. This specimen has not been disarticulated completely and has the maxillary teeth in situ.
Behind this groove the upper edge of the nasal surface corresponds to the medial margin of the orbital surface, and the maxilla articulates in this region with the lacrimal bone, a thin portion of the ethmoid bone, and the orbital process of the palatine bone.
The posterior border of the maxilla, which articulates with the palatine bone, is traversed obliquely from above downward and slightly medially by a groove, which, by articulation with the palate bone, is converted into the greater palatine canal. Toward the posterior and upper part of this nasal surface, a large, irregular opening into the maxillary sinus (antrum of Highmore) may be seen. In an articulated skull, this opening is partially covered by the uncinate process of the ethmoid bone and the inferior nasal concha.
Anterior to the lacrimal groove, the nasal surface is ridged for the attachment of the inferior nasal concha. Below this the bone forms a lateral wall of the inferior nasal meatus. Above the ridge for a small distance on the medial side of the nasal process, the smooth lateral wall of the middle meatus appears.
ZYGOMATIC PROCESS
The zygomatic process may be seen in the lateral views of the maxillary bone as a roughly triangular eminence whose apex is placed inferiorly directly over the first molar roots. The lateral border is rough and spongelike in appearance, where it has been disarticulated from the zygomatic or cheek bone (see Figures 14-1 and 14-3).
FRONTAL PROCESS
The frontal process (see Figures 14-2 through 14-5) arises from the upper and anterior body of the maxilla.
Part of this process is formed by the upward continuation of the infraorbital margin medially. Its edge articulates with the nasal bone. Superiorly, the process articulates with the frontal bone. The medial surface of the frontal process forms part of the lateral wall of the nasal cavity. Anteriorly, the frontal process articulates with the nasal bone.
PALATINE PROCESS
The palatine process (Figures 14-2 through 14-8) is a horizontal ledge extending medially from the nasal surface of the maxilla. Its superior surface forms a major portion of the nasal floor. The inferior surfaces of the combined left and right palatine processes form the hard palate as far posteriorly as the second molar, where they articulate with the horizontal parts of the palatine bone (Figures 14-7 and 14-8) at the transverse palatine suture.
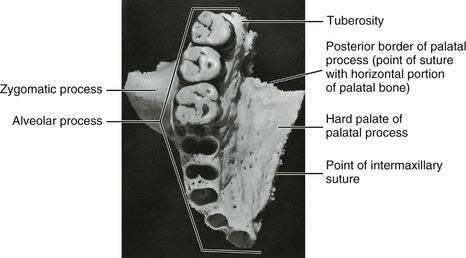
Figure 14-7 Palatine view of maxilla. Note the dental foramina in the deepest portion of the canine alveolus.
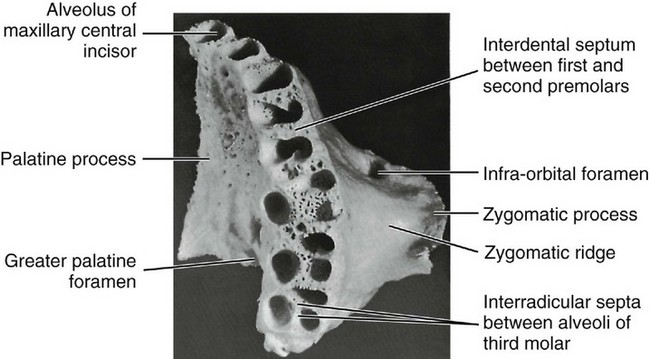
The inferior surface of the palatine process is rough and pitted for the palatine mucous glands in the roof of the mouth and is pierced by numerous small foramina for the passage of blood vessels and nerve fibers. At the posterior border of the process is a groove or canal that passes the greater palatine nerve and vessels to the palatal soft tissues. The posterior edge of the palatine process becomes relatively thin where it joins the palatine bone at the point of the greater palatine foramen. The palatine process becomes progressively thicker anteriorly from the posterior border. Anteriorly, the palatal process is confluent with the alveolar process surrounding the roots of the anterior teeth.
Immediately posterior to the central incisor alveolus, when looking at the medial aspect of the maxilla, one sees a smooth groove that is half of the incisive canal, when the two maxillae are joined together. The incisive fossa into which the canals open may be seen immediately lingual to the central incisors at the median line, or intermaxillary suture where the maxillae are joined. Two canals open laterally into the incisive foramen, the foramina of Stenson, carrying the nasopalatine nerves and vessels. Occasionally, two midline foramina are present, the foramina of Scarpi.
Extending laterally from the incisive foramen to the space between the lateral incisor and canine alveoli are the remnants of the suture between the maxilla and premaxilla. In most mammals the premaxilla remains an independent bone.
ALVEOLAR PROCESS
The alveolar process makes up the inferior portion of the maxilla; it is that portion of the bone which surrounds the roots of the maxillary teeth and which gives them their osseous support. The process extends from the base of the tuberosity posterior to the last molar to the median line anteriorly, where it articulates with the same process of the opposite maxilla (see Figures 14-7 and 14-8). It merges with the palatine process medially and with the zygomatic process laterally (see Figure 14-8).
When one looks directly at the inferior aspect of the maxilla toward the alveoli with the teeth removed, it is apparent that the alveolar process is curved to conform with the dental arch. It completes, with its fellow of the opposite side, the alveolar arch supporting the roots of the teeth of the maxilla.
The process has a facial (labial and buccal) surface and a lingual surface with ridges corresponding to the surfaces of the roots of the teeth supported by it. It is made up of labiobuccal and lingual plates of very dense but thin cortical bone separated by interdental septa of cancellous bone.
The facial plate is thin, and the positions of the alveoli are well marked on it by visible ridges as far posteriorly as the distobuccal root of the first molar (see Figure 14-2). The margins of these alveoli are frail, and their edges are sharp and thin. The buccal plate over the second and third molars, including the alveolar margins, is thicker. Generally, the lingual plate of the alveolar process is heavier than the facial plate. In addition, the alveolar process is longer where it surrounds the anterior teeth, sometimes extending posteriorly to include the premolars. In short, it extends farther down in covering the lingual portion of the roots.
The bone is very thick lingually over the deeper portions of the alveoli of the anterior teeth and premolars. The merging of the alveolar process with the palatal process brings about this formation. The lingual plate is paper thin over the lingual alveolus of the first molar, however, and rather thin over the lingual alveoli of the second and third molars. This thin lingual plate over the molar roots is part of the formation of the greater palatine canal (see Figure 14-8).
The alveolar process is maintained by the presence of the teeth. Should any tooth be lost, that portion of the alveolar process that supported the missing tooth will be subject to atrophic reduction. Should all of the teeth be lost, the alveolar process will eventually be virtually lost.
ALVEOLI (TOOTH SOCKETS)
The alveolar cavities are formed by the facial and lingual plates of the alveolar process and by connecting septa of bone placed between the two plates. The form and depth of each alveolus are determined by the form and length of the root it supports (see Table 1-1).
The alveolus nearest the median line is that of the central incisor (Figure 14-9; see also Figure 14-8). The periphery is regular and round, and the interior of the alveolus is evenly tapered and triangular in cross section, with the apex toward the lingual.

The second alveolus in line is that of the lateral incisor. It is generally conical and egg-shaped, or ovoid, with the widest portion to the labial. It is narrower mesiodistally than labiolingually and is smaller on cross section, although it is often deeper than the central alveolus. Sometimes, it is curved at the upper extremity (Figure 14-10; see also Figure 14-8).
The canine alveolus is the third from the median line. It is much larger and deeper than those just described. The periphery is oval and regular in outline, with the labial width greater than the lingual. The socket extends distally. It is flattened mesially and somewhat concave distally. The bone is so frail at the canine eminence on the facial surface of the alveolus that the root of the canine is often exposed on the labial surface near the middle third (see Figure 14-2).
The first premolar alveolus (see Figures 14-8 and 14-10) is kidney-shaped in cross section, with the cavity partially divided by a spine of bone that fits into the mesial developmental groove of the root of this tooth. This spine divides the cavity into a buccal and a lingual portion. If the tooth root is bifurcated for part of its length, as is often the case, the terminal portion of the cavity is separated into buccal and lingual alveoli. The socket is flattened distally and much wider buccolingually than mesiodistally (see Table 1-1).
The second premolar alveolus is also kidney-shaped, but the curvatures are in reverse to those of the first premolar alveolus. The proportions and depth are almost the same. The septal spine is located on the distal side instead of the medial side, because the second premolar root is inclined to have a well-defined developmental groove distally. This tooth usually has one broad root with a blunt end, but it is occasionally bifurcated at the apical third.
The first molar alveolus (Figures 14-8 and 14-11) is made up of three distinct alveoli widely separated. The lingual alveolus is the largest; it is round, regular, and deep. The cavity extends in the direction of the hard palate, having a lingual plate over it that is very thin. The lingual periphery of this alveolus is extremely sharp and frail. This condition may contribute to the tissue recession often seen at this site.

Figure 14-11 Alveoli of the molar area. Note the thinness of the buccal plates over the first molar roots compared with those of the second and third maxillary molars. The third molar alveoli are rarely separated as distinctly as in this specimen. Figures 14-9, 14-10, and 14-11 demonstrate a number of significant points concerning the maxillary alveoli. In Figure 14-9 the facial cortical plate of bone is thin over the anterior teeth and is considerably thicker over the posterior teeth, especially the molars. Cancellous bone seems to exist buccal to some of the posterior roots. In Figure 14-10 interradicular septa are thick but with numerous nutrient canals. In Figure 14-11 cancellous bone, furnishing numerous opportunities for blood supply, is evident in the apical portions of the alveoli. The anterior alveoli are lined laterally with a layer of smooth cortical bone. This lining is less prominent in the posterior alveoli.
The mesiobuccal and distobuccal alveoli of the first molar have no outstanding characteristics except that the buccal plates are thin. The bone is somewhat thicker at the peripheries than that found on the lingual alveolus. Nevertheless, it is thinner farther up on the buccal plate. It is not uncommon for one to find the roots uncovered by bone in spots when examining dry specimens.
The forms of the buccal alveoli resemble the forms of the roots they support. The mesiobuccal alveolus is broad buccolingually, with the mesial and distal walls flattened. The distobuccal alveolus is rounder and more conical.
The septa that separate the three alveoli (interradicular septa) are broad at the area that corresponds to the root bifurcation, and they become progressively thicker as the peripheries of the alveoli are approached. The bone septa are very cancellous, which denotes a rich blood supply, as is true of all the septa, including those separating the various teeth as well.
A general description of the alveoli of the second molar would coincide with that of the first molar; these alveoli are closer together, since the roots of this tooth do not spread as much. As a consequence, the septa separating the alveoli are not as heavy.
The third molar alveolus is similar to that of the second molar, except that it is somewhat smaller in all dimensions. Figure 14-11 shows a third molar socket to accommodate a tooth with three well-defined roots, a rare occurrence. Usually, the two buccal (and often all three) roots will be fused. The interradicular septum changes accordingly. If the roots of the tooth are fused, a septal spine will appear in the alveolus at the points of fusion on the roots marked by deep developmental grooves.
MAXILLARY SINUS
The maxillary sinus lies within the body of the bone and is of corresponding pyramidal form; the base is directed toward the nasal cavity. Its summit extends laterally into the root of the zygomatic process. It is closed in laterally and above by the thin walls that form the anterolateral, posterolateral, and orbital surfaces of the body. The sinus overlies the alveolar process in which the molar teeth are implanted, more particularly, the first and second molars, the alveoli of which are separated from the sinus by a thin layer of bone. Occasionally, the maxillary sinus will extend forward far enough to overlie the premolars also. It is not uncommon to find the bone covering the alveoli of some of the posterior teeth extending above the floor of the cavity of the maxillary sinus, forming small hillocks.
Regardless of the irregularity and the extension of the alveoli into the maxillary sinus, a layer of bone always separates the roots of the teeth and the floor of the sinus in the absence of pathological conditions. A layer of sinus mucosa is also always between the root tips and the sinus cavity.
MAXILLARY ARTICULATION
The maxilla articulates with the nasal, frontal, lacrimal, and ethmoid bones, above and laterally with the zygomatic bone, and occasionally with the sphenoid bone. Posteriorly and medially, it articulates with the palatal bone. Medially, it supports the inferior turbinate and the vomer and articulates with the opposite maxilla.
The Mandible
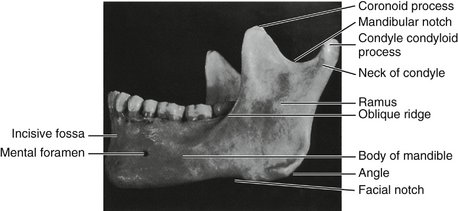
The mandible (Figures 14-12 through 14-23) is horseshoe-shaped and supports the teeth of the lower dental arch. This bone is movable and has no bony articulation with the skull. It is the heaviest and strongest bone of the head and serves as a framework for the floor of the mouth. It is situated immediately below the maxillary and zygomatic bone, and its condyles rest in the mandibular fossa of the temporal bone. This articulation is the temporomandibular joint.
The mandible has a horizontal portion, or body, and two vertical portions, or rami. The rami join the body at an obtuse angle.
The body consists of two lateral halves, which are joined at the median line shortly after birth. The line of fusion, usually marked by a slight ridge, is called the symphysis. The body of the mandible has two surfaces, one external and one internal, and two borders, one superior and one inferior.
To the right and left of the symphysis, near the lower border of the mandible, are two prominences called mental tubercles. A prominent triangular surface made by the symphysis and these two tubercles is called the mental protuberance (see Figure 14-16).
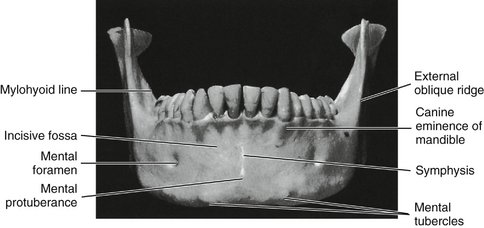
Immediately posterior to the symphysis and immediately above the mental protuberance is a shallow depression called the incisive fossa. The fossa is immediately below the alveolar border of the central and lateral incisors and anterior to the canines. The alveolar portion of the mandible overlying the root of the canine is prominent and is called the canine eminence of the mandible. However, this eminence does not extend down very far toward the lower border of the mandible before it is lost in the prominence of the mental protuberance and the lower border of the mandible.
The external surface of the mandible from a lateral viewpoint presents a number of important areas for examination.
The oblique ridge (oblique line, radiographically) extends obliquely across the external surface of the mandible from the mental tubercle to the anterior border of the ramus, with which it is continuous. It lies below the mental foramen. It is usually not prominent except in the molar area (see Figure 14-12).
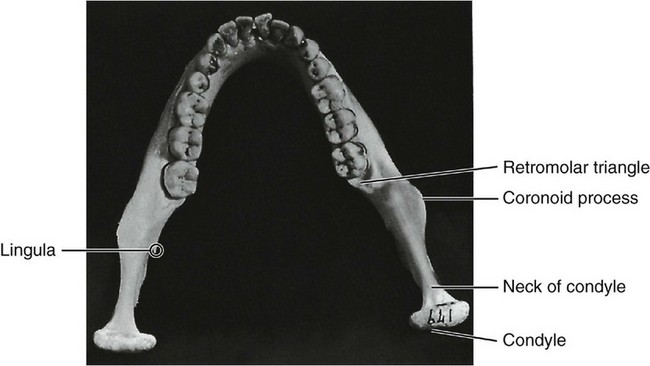
This ridge thins out as it progresses upward and becomes the anterior border of the ramus and ends at the tip of the coronoid process. The coronoid process is one of two processes making up the superior border of the ramus. It is a pointed, flattened, smooth projection and is roughened toward the tip to give attachment for a part of the temporal muscle.
The condyle, or condyloid process, on the posterior border of the ramus is variable in form. It is divided into a superior or articular portion and an inferior portion, or neck. Although the articular portion, the condyle, appears as a rounded knob when the mandible is viewed from a lateral aspect, from a posterior aspect, the condyle is much wider and oblong in outline (compare Figures 14-12 and 14-13).
The condyle is convex above, fitting into the mandibular fossa of the temporal bone when the mandible is articulated to the skull, and forms, with the interarticular cartilage that lies between the two surfaces and with the tissue attachment, the temporomandibular joint (see Figure 15-2).
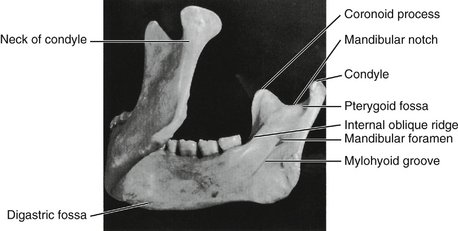
The neck of the condyle is a constricted portion immediately below the articular surface. It is flattened in front and presents a concave pit medially, the pterygoid fovea. A smooth, semicircular notch, the mandibular notch, forms the sharp upper border of the ramus between the condyle and coronoid process (see Figure 14-14).
The distal border of the ramus is smooth and rounded and presents a concave outline from the neck of the condyle to the angle of the jaw, where the posterior border of the ramus and the inferior border of the body of the mandible join. The border of this angle is rough, being the attachment of the masseter muscle (see Figure 15-18) and the stylomandibular ligament (see Figure 15-7).
An important landmark on the lateral aspect of the mandible is the mental foramen. It should be noted that this opening of the anterior end of the mandibular canal is directed upward, backward, and laterally. The foramen is usually located midway between the superior and inferior border of the body of the mandible when the teeth are in position, and most often, it is below the second premolar tooth, a little below the apex of the root. The position of this foramen is not constant, and it may be between the first premolar and the second premolar tooth. After the teeth are lost and resorption of alveolar bone has taken place, the mental foramen may appear near the crest of the alveolar border. In childhood, before the first permanent molar has come into position, this foramen is usually immediately below the first primary molar and nearer the lower border.
It is interesting to note that when the mandible is observed from a point directly opposite the first molar, most of the distal half of the third molar is hidden by the anterior border of the ramus. When the mandible is viewed from in front, directly opposite the median line, the second and third molars are located 5 to 7 mm lingually to the anterior border of the ramus (compare Figures 14-12 and 14-16).
INTERNAL SURFACE OF THE MANDIBLE
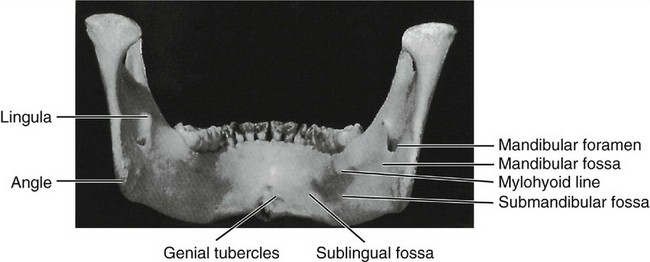
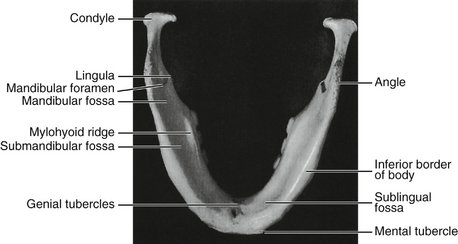
Observation of the mandible from the rear shows that the median line is marked by a slight vertical depression, representing the line of union of the right and left halves of the mandible, and that immediately below this, at the lower third, the bone is roughened by eminences called the superior and inferior mental spines, or genial tubercles (see Figures 14-15 and 14-34, C).
The internal surface of the body of the mandible is divided into two portions by a well-defined ridge, the mylohyoid line. It occupies a position closely corresponding to the lateral oblique ridge on the surface. It starts at or near the lowest part of the mental spines and passes backward and upward, increasing in prominence until the anterior portion of the ramus is reached; there, it smoothes out and gradually disappears (see Figures 14-14 and 14-34, C).
This ridge is the point of origin of the mylohyoid muscle, which forms the central portion of the floor of the mouth. Immediately posterior to the median line and above the anterior part of the mylohyoid ridge a smooth depression, the sublingual fossa, may be seen. The sublingual gland lies in this area.
A small, roughened oval depression, the digastric fossa, is found on each side of the symphysis immediately below the mylohyoid line and extending onto the lower border. Toward the center of the body of the mandible, between the mylohyoid line and the lower border of the bone, a smooth oblong depression is located, called the submandibular fossa. It continues back on the medial surface of the ramus to the attachment of the lateral pterygoid muscle. The submandibular gland lies within this fossa.
The mandibular foramen is located on the medial surface of the ramus midway between the mandibular notch and the angle of the jaw and also midway between the internal oblique line and the posterior border of the ramus. The mandibular canal begins at this point, passing downward and forward horizontally.
The anterior margin of the foramen is formed by the lingula, or mandibular spine, which gives attachment to the sphenomandibular ligament. Coming obliquely downward from the base of the foramen beneath the lingula is a decided groove, the mylohyoid groove. Behind this groove toward the angle of the mandible, a roughened surface for the attachment of the medial pterygoid muscle may be seen.
ALVEOLAR PROCESS
The border of the alveolar process outlines the alveoli of the teeth and is very thin at its anterior portion around the roots of the incisor teeth but thicker posteriorly where it encompasses the roots of the molars. The alveolar process, which comprises the superior border of the body of the mandible, differs from the same process in the maxillae in one very important particular: it is not as cancellous, and instead of the facial plate’s being relatively thin, it is equally as heavy as the lingual plate. Although the bone over the anterior teeth, including the canine, is very thin and may be entirely missing over the cervical portion of the root, the bone that does cover the root is the compact type.
The inferior border of the mandible is strong and rounded and gives to the bone the greatest portion of its strength (see Figure 14-15).
When one looks down on the mandible from a point above the alveoli of the first molars (see Figure 14-18), it can be noticed that although the alveolar border may be thinner anteriorly than posteriorly, the body of the bone is uniform throughout. The lines of direction of the posterior alveoli are inclined lingually to conform to the lingual inclination of the teeth when they are in position. The anterior teeth, of course, have their alveoli tipped labially; therefore when one looks down on the mandible from above the alveolar process, more of the bone may be seen lingual to the anterior teeth than lingual to the posterior teeth. In contrast, posteriorly, more of the bone may be seen buccal to the teeth than lingual. Therefore the outline of the arch of the teeth does not correspond to the outline of the arch of the bone. The dental arch is narrower posteriorly than the mandibular arch.
The lingual walls of the alveoli of the second and third molars are relatively thin near the bottoms of the sockets, although the bone near the periphery is somewhat thicker and very compact. If a specimen of the mandible from which the third molar has been removed is held up to the light, the bone at the bottom of the socket is so thin that light will penetrate it. This thinness of bone is consistent with the submandibular fossa below the mylohyoid ridge (see Figure 14-15; Figure 14-22, A and B; and Figure 14-24).
The bone buccal to the last two molars is very heavy and thick, being reinforced by the external oblique ridge. Posterior to the third molar a triangular shallow fossa is outlined; it is called the retromolar triangle (Figure 14-17). The cortical plate over this fossa is not as heavy as the bone surrounding it, and it is more cancellous under the thin cortical plate covering it.
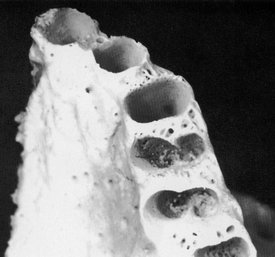
ALVEOLI
The first alveolus right or left of the median line is that of the first, or central, incisor. The periphery of the alveolus often dips down lingually and labially and exposes the root for part of its length. This arrangement makes an interdental spine out of the interdental septum separating the alveolus of the mandibular central incisors. The central incisor alveolus is flattened on its mesial surface and is usually somewhat concave distally to accommodate the developmental groove on the root (see Figures 14-18 and 14-19).
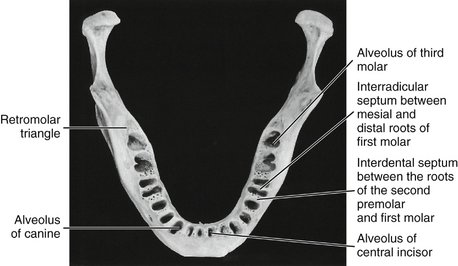

Figure 14-19 Closeup view of one of the three separate divisions of the mandibular alveoli (as shown in Figures 14-19, 14-20, and 14-21). This picture indicates the relative sizes and shapes of the incisors for comparison with other mandibular teeth.
The alveolus of the mandibular second, or lateral, incisor is similar to that of the central incisor. It usually has the following variations: the socket is larger and deeper to accommodate a larger and longer root; the periphery does not dip down as far on the lingual surface but may dip more on the labial aspect of the tooth, exposing more of the root of the lateral incisor. The interdental septum extends up just as high between the teeth as that between the central incisors.
The canine alveolus is quite large and oval and, of course, deep to accommodate the root of the mandibular canine. The lingual plate is stronger and much heavier than that over the alveoli just described, although the thin labial plate may thin out at its edges and expose just as much of the canine root on the labial side. The labial outline of the alveolus is wider than the lingual outline, and the mesial and distal walls of the sockets are irregular to accommodate developmental grooves, both mesially and distally, on the canine root (see Figures 14-18 and 14-20).

Figure 14-20 This view of the mandibular alveoli includes the canine, the first and second premolars, and a clear view of the mandibular first molar alveoli. Note the excellent design for the anchorage of first molar roots. Apparently, the blood supply for the interseptal bone lessens as anterior teeth are approached. The apical portion of the canine alveolus displays the single opening in the bone for the blood and nerve supply to the tooth pulp.
The alveoli of the first and second premolars are similar in outline. The outline is smooth and rounded, although the dimensions are greater buccolingually than mesiodistally. The alveolus of the second premolar is usually somewhat larger than that of the first premolar. The buccal plate of the alveoli is relatively thin, but the lingual plate is heavy; the interdental septum has become heavier at this point compared with the interdental septa found between the anterior teeth. The interdental septum between the canine and first premolar is relatively thin, although uniform in outline. The septum between the first premolar and second premolar is nearly twice as thick.
Progressing posteriorly (see Figures 14-18 and 14-20), the interdental septum between the second premolar socket and the alveolus of the mesial root of the first molar is twice as thick as that found between the first and second premolars. The socket of the first molar is divided by an interroot septum, which is strong and regular. The alveolus of the mesial root is kidney-shaped, much wider buccolingually than mesiodistally, and constricted in the center to accommodate developmental grooves found mesial and distal to the mesial root of the first molar. The alveolus of the distal root of the first molar is evenly oval with no constriction, conforming to the rounded shape of this root. The interdental septum between the alveoli of the mandibular first molar and the socket of the second molar is thick mesiodistally, although cancellous in character.
The mandibular second molar alveolus may be divided into two alveoli, as was the case in the first molar. However, often it is found to be one compartment near the periphery of the alveolus but divides into two compartments in the deeper portions. A septal spine occurs where the developmental grooves on the root are deep enough, or an interradicular septum will appear when the roots are entirely divided. The interdental septum between the second molar sockets and the third molar sockets is not as thick mesiodistally as the two interdental septa immediately anterior.
The mandibular third molar alveolus is usually irregular in outline (see Figure 14-21). Usually it is much narrower toward the distal than toward the mesial aspect of the alveolus. It may have interradicular septa or septal spines to accommodate itself to the irregularity of the root.

Figure 14-21 Alveoli of the first, second, and third molars. Features for special attention include the thin and perforated surface of the retromolar triangular space distal to the third molar alveolus and the cancellous formation in the alveoli proper and also in the interdental septa, which would allow a rich blood supply.
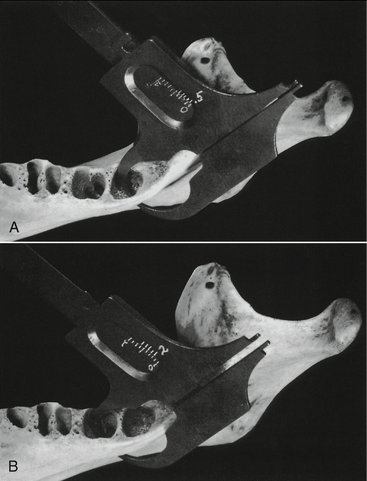
Figure 14-22 Illustration of the relative thickness of bone covering lingual mandibular second and third molar roots. A, Measurement of the thickness of bony cover lingual to the apex of the third mandibular molar immediately below the mylohyoid ridge. It measures only 0.5 mm. B, Repetition of measurement in the deepest portion lingually of the second molar alveolus. It measures fully 2 mm.

Figure 14-23 Comparison of the size and shape of mandibles at various ages. Top, Mandible of a 5-year-old. Notice the rounded bowlike form. Notice also the amount of space between the second deciduous molar and the ramus. Middle, Mandible of a 9-year-old. Notice the angular outline with constriction at the point of second permanent molar development. Bottom, Well-developed mandible of an individual approximately 50 years of age. The bone is regular in outline. The lingual constriction has lessened and has retreated to the third molar area.
Mesiodistal views of the teeth and their supporting structures can be made clinically using computed tomography to demonstrate the way that individual teeth relate to each other or to cortical and cancellous bone; however, vertical sections of a skull were made to illustrate these relationships1 shown in Figure 14-24. (See also Figure 13-29Figure 13-29.)
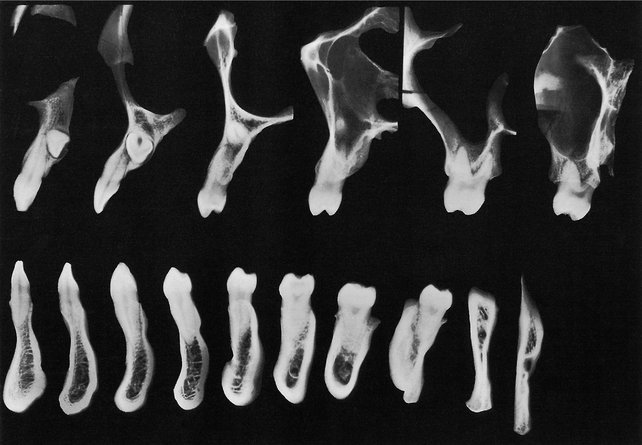
Figure 14-24 Some fine vertical sections of a skull made with radiographic problems in view. These radiographs of faciolingual sections show the extent of tooth attachment, the way in which individual teeth compare with each other, and the variances between cortical and cancellous bone in anchorage (see Figures 14-25 through 14-32). The maxillary canine was impacted in this specimen. Maxillary third molars were missing.
(From Updegrave WJ: Normal radiodontic anatomy, Dent Radiogr Photogr 31:57, 1958.)
Some classical illustrations of sections of the axial relations of the maxillary and mandibular teeth are shown in Figures 14-25 through 14-32. These figures demonstrate the directional lines of the axes of the teeth and their alveoli (see also Box 16-1 and Figure 16-20). In addition, the radiographs of the sections graphically illustrate the relative densities of the teeth and supporting structures and show the outline and relative thickness of the bone over the various teeth at the site of each section.2

Figure 14-25 Central incisor regions, showing relation of superior central incisor to inferior lateral incisor.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)

Figure 14-26 Lateral incisor regions. Note position of apex of superior lateral incisor.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)

Figure 14-27 Canine regions. Note anterior extremity of maxillary antrum.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)

Figure 14-28 First premolar regions.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)
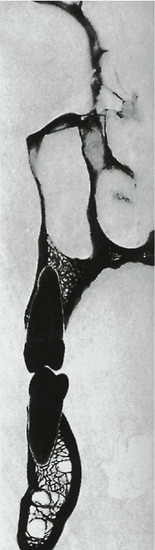
Figure 14-29 Second premolar regions.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)
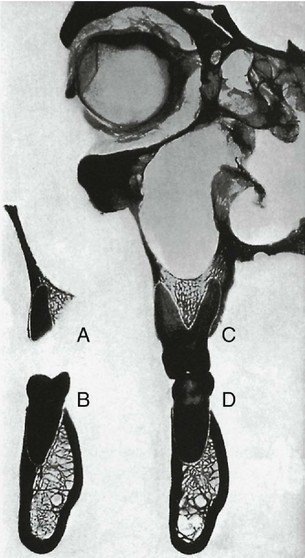
Figure 14-30 First molar regions, showing relations of distobuccal root (A), distal half (B), and mesiobuccal (C) and lingual roots with mesial half of lower molar (D).
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)
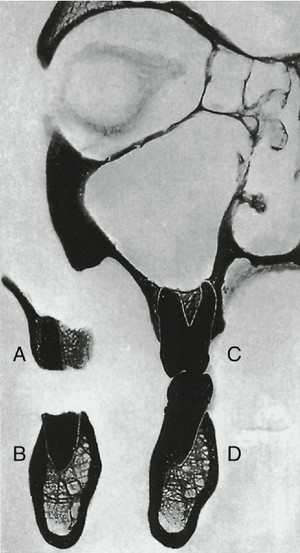
Figure 14-31 Second molar regions, showing relations of distobuccal root (A), distal root (B), and mesiobuccal (C) and lingual (D) roots with mesial half.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)
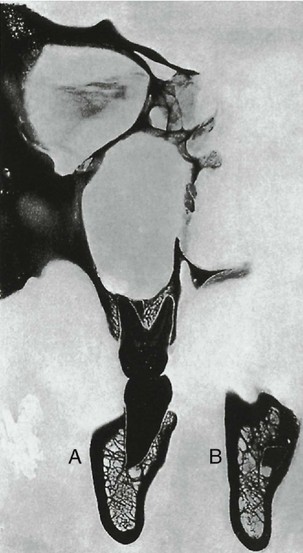
Figure 14-32 Third molar regions. A, Mesial root; B, apex of distal root; note deep groove for descending palatine artery.
(From MacMillan HW: The structure and function of the alveolar process, J Am Dent Assoc 11:1059, 1924.)
In Figures 14-25 through 14-32, note the axial relations of the superior and inferior teeth, the relative thickness of labial and lingual alveolar plates, the characteristics of the cancellous tissue, the relative densities, and the relation of the teeth to important structures. Compare the changes in the external contour and internal architecture of the adjacent sections. The sections in this series, with the exception of those in Figure 14-28, were taken from the same cadaver and are from the left side. A plaster cast was made before sectioning. The sections were reassembled in the cast and held in exact relation while being radiographed.
Figures 14-33, I and II illustrate the appearance of some of the bony landmarks of the maxilla and mandible as visualized in intraoral periapical radiography.3 Surfaces and dento-osseous structures are often important to recognize in relation to diagnostic and treatment aspects (Figure 14-34).
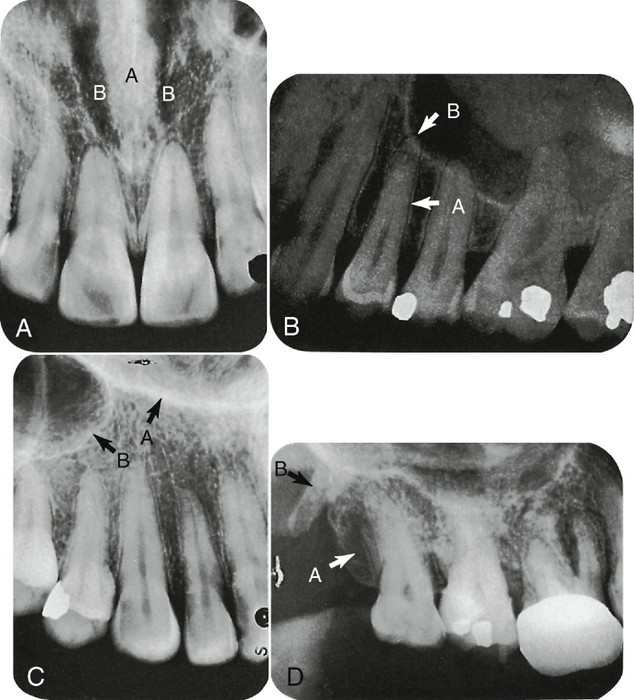
Figure 14-33 I A, Radiograph of central incisor region visualizing the nasal septum (A) and fossae (B). B, Radiograph demonstrating the normal appearance of the lamina dura (A) and the periodontal membrane (B). C, Radiograph depicting the Y (inverted) formed by the junction of the lateral wall (A) of the nasal fossa and the antemedial wall (B) of the maxillary sinus. D, Radiograph visualizing the tuberosity of the maxilla (A) and the hamular process of the sphenoid bone (B).
(From McCauley HB: Anatomic characteristics important in radiodontic interpretation, Dent Radiogr Photogr 18:1, 1945.)
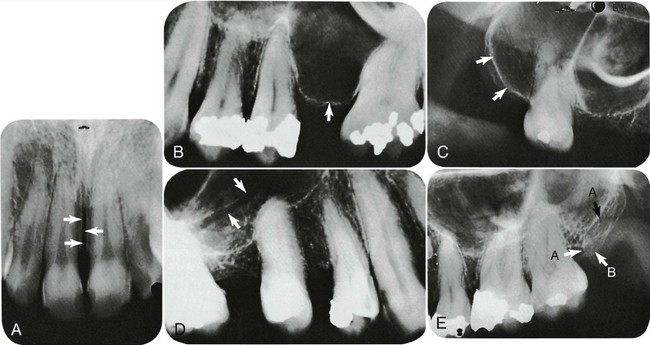
Figure 14-33 II A, Radiograph of the medial palatine suture, the appearance of which might be interpreted as a fracture. Radiographs visualize various extensions of the maxillary sinus. B, Alveolar extension. C, Tuberosity extension. D, Radiograph in which the canal for a superior alveolar artery is seen. E, Radiograph showing typical superimposition of the coronoid process: A, of the mandible on the tuberosity; B, of the maxilla.
(From McCauley HB: Anatomic characteristics important in radiodontic interpretation, Dent Radiogr Photogr 18:1, 1945.)
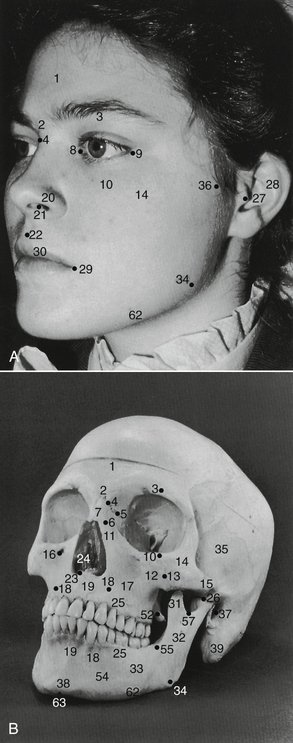
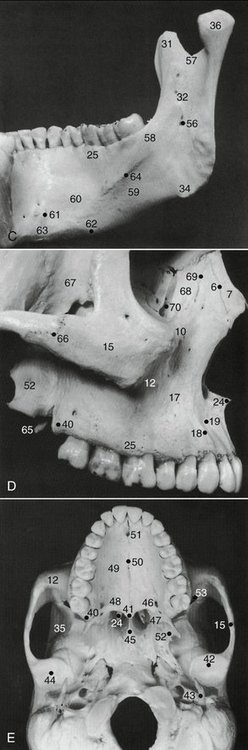
Figure 14-34 Surface landmarks. Various dental structures in the patient’s face can be quickly located by means of surface landmarks. Surface landmarks are identified in A. The photograph of the bony skull (B) was made from the same angle of view. Features of both are numbered and identified in the legend. The medial aspect of the mandible (C) shows anatomical details not clearly seen in the other illustrations. The maxilla and zygoma are shown in D. The bony anatomy of the hard palate and its adjoining structures is shown in E.
Arterial Supply to the Teeth
The arteries and nerve branches to the teeth are mere terminals of the central systems. This book must confine itself to dental anatomy and the parts immediately associated, and references will therefore be made only to those terminals that supply the teeth and the supporting structures.
INTERNAL MAXILLARY ARTERY
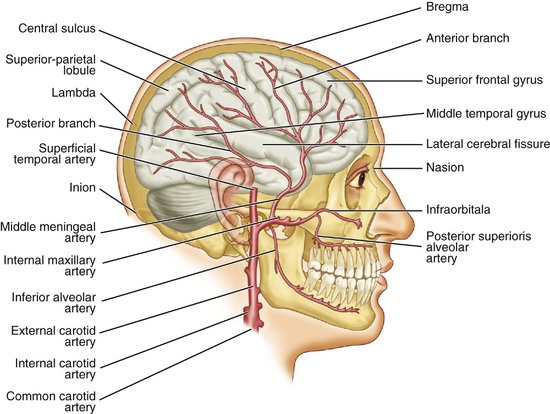
The arterial supply to the jaw bones and the teeth comes from the maxillary artery, which is a branch of the external carotid artery (see Figure 14-35). The branches of the maxillary artery that feed the teeth directly are the inferior alveolar artery and the superior alveolar arteries (Figure 14-35).
INFERIOR ALVEOLAR ARTERY
The inferior alveolar artery branches from the maxillary artery medial to the ramus of the mandible. Protected by the sphenomandibular ligament, it gives off the mylohyoid branch, which rests in the mylohyoid groove of the mandible and continues along on the medial side under the mylohyoid line. After giving off the mylohyoid branch, it immediately enters the mandibular foramen and continues downward and forward through the mandibular canal, giving off branches to the premolar and molar teeth. In the vicinity of the mental foramen, it divides into a mental and an incisive branch. The mental branch passes through the mental foramen to supply the tissues of the chin and to anastomose with the inferior labial and submental arteries. The incisive branch continues forward in the bone to supply the anterior teeth and bone and to anastomose with those of the opposite side.
The anastomosis of the mental and incisive branches furnishes a good collateral blood supply for the mandible and teeth.4
In their canals, the inferior alveolar and incisive arteries give off dental branches to the individual tooth roots for the supply of the pulp and periodontal membrane at the root apex (see Figure 5-12). Other branches enter the interdental septa, supply bone and adjacent periodontal membrane, and terminate in the gingiva. Numerous small anastomoses connect these vessels with those supplying the neighboring alveolar mucosa.
SUPERIOR ALVEOLAR ARTERIES
The posterior superior alveolar artery branches from the maxillary artery superior to the maxillary tuberosity to enter the alveolar canals along with the posterior superior alveolar nerves and supplies the maxillary teeth, alveolar bone, and membrane of the sinus. A branch of variable size runs forward on the periosteum at the junction of the alveolar process and maxillary body supplying the gingiva, alveolar mucosa, and cheek. When it is large, it may supplant in part the buccal artery.
A middle superior alveolar branch is usually given off by the infraorbital continuation of the maxillary artery somewhere along the infraorbital groove or canal. It runs downward between the sinus mucosa and bone or in canals in the bone and joins the posterior and anterior alveolar vessels. Its main distribution is to the maxillary premolar teeth.
Anterior superior alveolar branches arise from the infraorbital artery just before this vessel leaves its foramen. They course down the anterior aspect of the maxilla in bony canals to supply the maxillary anterior teeth and their supporting tissues and to join the middle and posterior superior alveolar branches in completing an anastomotic plexus.
Branches to the teeth, periodontal ligament, and bone are derived from the superior alveolar artery in the same manner as described for the inferior alveolar artery.
DESCENDING PALATINE AND SPHENOPALATINE ARTERIES
The palatal blood supply comes from two sources but chiefly from the descending palatine artery, which descends from its origin from the maxillary through the greater canal. Its greater palatine branch enters the palate through the greater palatine foramen and runs forward with its accompanying vein and nerve in a groove at the junction of the palatine and alveolar processes. It is distributed to the bone, glands, and mucosa of the hard palate and to the bone and mucosa of the alveolar process, in which it forms anastomoses with fine branches of the superior alveolaris. Minor branches of the descending palatine artery pass to the soft palate through lesser palatine foramina in the palatine bone.
The nasopalatine branch of the sphenopalatine artery courses obliquely forward and downward on the septum and enters the palate through the incisive canal. It has a limited distribution to the incisive papilla and adjacent palate and forms an anastomosis with the greater palatine.
Nerve Supply to the Jaws and Teeth
The sensory nerve supply to the jaws and teeth is derived from the maxillary and mandibular branches of the fifth cranial, or trigeminal nerve (Figure 14-36), whose ganglion, the trigeminal, is located at the apex of the petrous portion of the temporal bone. The innervation of the orofacial region includes, in addition to the trigeminal nerve (including V2 and V3), other cranial nerves, (e.g., VII, XI, XII) (Figure 14-37).
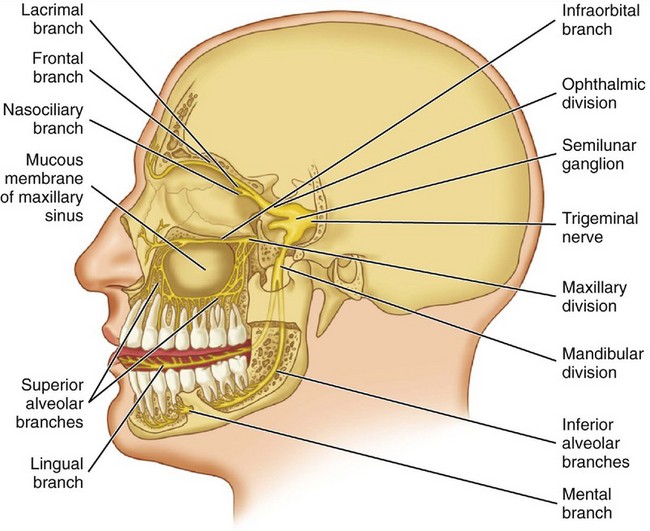
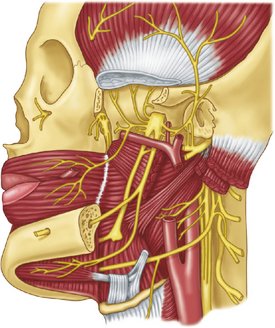
Figure 14-37 Mandibular nerve. The inferior alveolar nerve branch (in the cut section of the mandible and the mandibular canal) provides innervation for the mandibular teeth. The injection of a local anesthetic into the vicinity of the lingula (see Figure 14-17) blocks the sensory innervation of the inferior alveolar nerve and the lingual nerve (“mandibular block”), which results in a feeling of numbness of the mandibular teeth, lower lip, and side of the tongue on the side of the injection.
MAXILLARY NERVE
The maxillary nerve (see Figure 14-36) courses forward through the wall of the cavernous sinus and leaves the skull through the foramen rotundum.5 It crosses the pterygopalatine fossa, where it gives branches to the pterygopalatine ganglion, a parasympathetic ganglion. This ganglion gives off several branches, now containing visceral motor and sensory fibers, to the mucous membrane of the mouth, nose, and pharynx.
The branches of clinical significance include a greater palatine branch that enters the hard palate through the greater palatine foramen and is distributed to the hard palate and palatal gingiva as far forward as the canine tooth; a lesser palatine branch from the ganglion that enters the soft palate through the lesser palatine foramina; and a nasopalatine branch of the posterior or superior lateral nasal branch of the ganglion that runs downward and forward on the nasal septum. Entering the palate through the incisive canal, it is distributed to the incisive papilla and to the palate anterior to the anterior palatine nerve.
The maxillary nerve also has a posterior superior alveolar branch from its pterygopalatine portion. This nerve enters the alveolar canals on the infratemporal surface of the maxilla and, forming a plexus, is distributed to the molar teeth and the supporting tissues.
The maxillary nerve enters the orbit and, as the infraorbital nerve, runs forward in its floor, first in the infraorbital groove and then in the infraorbital canal. It terminates at the infraorbital foramen in branches distributed to the upper face. At a variable distance after it enters the orbit, a middle superior alveolar branch arises from the infraorbital nerve and runs through the lateral wall of the maxillary sinus. It is distributed to the premolar teeth and surrounding tissues and joins the alveolar plexus. The middle superior alveolar nerve may be associated closely with the posterior superior alveolar nerve as its origin but often branches near the infraorbital foramen.
An anterior superior alveolar branch leaves the infraorbital nerve just inside the infraorbital foramen and is distributed through bony canals to the incisor and canine teeth. All three superior alveolar nerves join in a plexus above the process. From the plexus, dental branches are given off to each tooth root and interdental branches to the bone, periodontal membrane, and gingiva, the distribution being similar to that described for the arteries.
MANDIBULAR NERVE
The mandibular nerve (see Figure 14-37) leaves the skull through the foramen ovale and almost immediately breaks up into its several branches. The chief branch to the lower jaw is the inferior alveolar nerve, which at first runs directly downward across the medial surface of the lateral pterygoid, at the lower border of which it is directed laterally and downward across the outer surface of the medial pterygoid muscle to reach the mandibular foramen. Just before entering the foramen, it releases the mylohyoid branch, which is a motor branch to the mylohyoid muscle and anterior belly of the digastric muscle.
The inferior alveolar nerve continues forward through the mandibular canal beneath the roots of the molar teeth to the level of the mental foramen. During this part of its course, it gives off branches to the molar and premolar teeth and their supporting bone and soft tissues. The nerves to the teeth do not arise as individual branches but as two or three larger branches that form a plexus from which inferior dental branches enter individual tooth roots and interdental branches supply alveolar bone, periodontal membrane, and gingiva.
At the mental foramen, the nerve divides and a smaller incisive branch continues forward to supply the anterior teeth and bone, and a larger mental branch emerges through the foramen to supply the skin of the lower lip and chin.
Other branches of the mandibular nerve contribute in some degree to the innervation of the mandible and its investing membranes. The buccal nerve, although chiefly distributed to the mucosa of the cheek, has a branch that is usually distributed to a small area of the buccal gingiva in the first molar area, but in some cases, its distribution may extend from the canine to the third molar. The lingual nerve, as it enters the floor of the mouth, lies against the body of the mandible and has mucosal branches to a variable area of lingual mucosa and gingiva. The mylohyoid nerve may sometimes continue its course forward on the lower surface of the mylohyoid muscle and enter the mandible through small foramina on either side of the midline. In some individuals, it is thought to contribute to the innervation of central incisors and periodontal ligament.
1. Updegrave WJ. Normal radiodontic anatomy. Dent Radiogr Photogr. 1958;31:57.
2. MacMillan HW. The structure and function of the alveolar process. J Am Dent Assoc. 1924;11:1059.
3. McCauley HB. Anatomic characteristics important in radiodontic interpretation. Dent Radiogr Photogr. 1945;18:1.
4. Jones TS, Shepard WC. A manual of surgical anatomy. Philadelphia: Saunders; 1945.
5. King BG, Showers MJ. Human anatomy and physiology, ed 6. Philadelphia: Saunders; 1969.
Callander CL. Surgical anatomy, ed 2. Philadelphia: Saunders; 1939.
Deaver JB. Surgical anatomy of the human body, ed 2. Philadelphia: Blakiston; 1926.
Head and neck: brain. In Brash JC, Jamieson EB, editors: Cunningham’s manual of practical anatomy, ed 10, New York: Oxford University Press, 1940.
Morris H. Human anatomy, ed 10. Philadelphia: Blakiston; 1942.
Pernkopf E. Vestibulum and cavum oris, pharynx, vol 1. 1963. Saunders, Philadelphia.
Rohen JW, Yokochi C. Color atlas of anatomy: a photographic study of the human body, ed 2. New York: Igaku-Shoin Medical; 1988.
 site for additional study resources.
site for additional study resources.