Assisted reproduction technology and traditional Chinese medicine
Infertility Patients and their Treatment Needs
Where does a couple looking for fertility treatment start?
Many patients will make their first appointment in the TCM (traditional Chinese medicine) clinic, based on their philosophical preferences and recommendations made by friends or the family doctor. Some patients will be wondering which is the correct approach for them. Is ART (assisted reproduction technology) or TCM better – For different types of patients? – For different types of infertility? – For different stages of infertility treatment? The answer is Yes on all counts and the advice given by the primary practitioner needs to be thoroughly informed (see Box 10.1).
The sort of treatments appropriate for patients who fall into the first four categories in Box 10.1 are those that we have discussed in the previous chapters. Patients who have had bad reactions to the drugs prescribed in ART clinics may need some rehabilitation, both physiologic in correcting the menstrual cycle, and emotional. Where there is Kidney weakness (which is the case for most functional infertility), Chong and Ren vessel function is vulnerable to disruption. What happens during an IVF cycle causes massive disruption to the natural function of the Chong and Ren vessels.
Where Kidney deficiency in the woman undergoing IVF is significant (this is the woman who is older, or who ovulates irregularly and poorly, who may have been trying to become pregnant for a long time), high doses of follicle stimulating drugs will be required to get a minimal response. Such high doses or repeated use can jeopardize what was already fragile ovary function, sometimes catastrophically. In the worst case scenario, menstrual cycles do not recover and a (peri)-menopausal pattern sets in.
For women in this category (men’s Kidney energy is not challenged directly by IVF), the aim of treatment is to restore Kidney Yin and Yang function in a regular cyclical fashion. Applying the principles outlined in Chapter 4 is the correct approach; however, be prepared for a longer than usual period of Kidney Yin reinforcement. In addition, Liver and Heart Qi stagnation will always need addressing after a failed IVF cycle – in some women more than others.
It is the last group mentioned in Box 10.1, those couples who wish to try everything, who present some unique challenges in the clinic. The combining of Chinese medical therapy with IVF requires careful thought – and like all the ART techniques of the last few decades, some experimentation. This is an area ripe for research – already underway in many countries (see below).
Such a combination throws TCM into a cutting-edge modern medical arena, but the beauty of this oldest of all existing medical systems is that it is universally applicable and unceasingly flexible. Even if the patient is taking drugs that stop the pituitary gland dead in its tracks; is having surgical procedures to remove artificially ripened gametes from their glandular homes; or is experiencing intense emotional stress, the doctor of Chinese medicine can still make a diagnosis incorporating all those factors and their effect on the body and mind, and can prescribe treatment which not only focuses on the particular imbalance but may also work with the medical interventions to make their results better and their side-effects less.
Referral to ART clinics is sometimes made too early and sometimes inappropriately. Some couples spend a lot of money and take unnecessary risks using drastic measures, when simple alternative methods could have been just as effective if they had been well enough informed to pursue them. Remember our patient in Chapter 1 with sharp corners? On the other hand, some patients pursue ‘natural’ therapies for too long, when their main or only chance of success is to use IVF.
We can put couples having difficulty falling pregnant into a number of different groups, according to their age and the cause of the infertility. Out of this, some generalizations and recommendations can be made (see Box 10.2).
A summary of these treatment options is given in Table 10.1. If at times there can be a serendipitous marriage between the two medical systems to achieve reasonably rapid and effective results, then we have found a happy solution. Infertility is an area where both Western and Chinese medical systems have strong, effective approaches and both have much to gain by listening to and using the strengths of the other.
Table 10.1
| Cause of infertility | Approach to treatment |
| Major impediment | ART |
| Minor impediment | |
| Young woman | TCM, nutritional or lifestyle program, drugs |
| Older woman | ART plus TCM |
| Combination of more than one minor factor | TCM or ART |
| No abnormality diagnosed | TCM, nutritional or lifestyle program |
Comparing Different Infertility Treatments
ART and TCM have such different approaches, philosophical underpinnings, and methods, that we might question whether they can in fact work together. But examining the context and comparing the approach, techniques and emphasis of these different types of treatment will afford us insights into ways they might best complement each other.
IVF and TCM – different approach
Traditional Chinese medicine is a medical therapeutic treatment and IVF is essentially a technologic strategy. IVF does involve drugs but they are not used in a therapeutic way, they are used to artificially stimulate many follicles to ripen – a process called controlled ovarian hyperstimulation. IVF does not look at the means to an end, it skips straight to the end. TCM can only work by improving or correcting the means (i.e., the Kidney deficiency, the Liver Qi stagnation, etc.), which hopefully leads to healthier gametes and healthier offspring. Table 10.2 outlines the different methodology and style inherent in these two approaches.
Table 10.2
IVF and TCM – different approach
| IVF | TCM |
| Technological regimen | Therapeutic treatment |
| Sophisticated and involved | Basic and minimally invasive |
| Clinical personnel | Clinical personnel |
| Infertility specialist – drugs and surgery, pathology tests | Infertility specialist |
| Anesthetists – local or general anesthetics | Herbs and acupuncture |
| Nurses – injections and blood samples | Diet and lifestyle |
| Radiologists – ultrasounds | Exercise, Qi Gong |
| Embryologists – monitor fertilization and embryo development | Some pathology tests |
The IVF clinic is sophisticated and uses advanced technology such as ultrasound equipment, blood testing labs, surgical tools, microscopes, and incubators. The Chinese medicine clinic is equipped with herbs and needles, and often only two bits of machinery – scales and a battery operated stimulator for electroacupuncture.
An IVF clinic is staffed with large numbers of people with different roles, reflecting the complexity of the technology.
The TCM clinic is often just one specialist who prescribes and administers different sorts of treatment and recommends relevant lifestyle changes. Sometimes pathology tests are ordered; these won’t necessarily change the treatment approach but they may indicate prognosis and progress.
IVF and TCM – different techniques
If we are to compare the philosophy behind the techniques used in these two medical models (see Table 10.3) the key feature is the holistic nature of TCM and the reductionist paradigm of modern medicine. In Western medicine, the mind and body are separated and the body is viewed, analyzed and treated as an entity which can be understood only by reducing it to its component parts. Such a Cartesian viewpoint, where we reduce the body to basic components separated from the whole, is nowhere so clearly shown as in IVF where the sperm and egg are put together outside the body in a dish in the laboratory.
Table 10.3
IVF and TCM – different techniques
| IVF | TCM |
| Reductionist | Holistic |
| New | Time tested |
| Possible side-effects | Few side-effects |
| Some risk to mother and baby | No risk to mother or baby demonstrated |
| Quick acting | Slow acting |
TCM looks at, and treats, the whole body and mind – the patient feels better, fertility is improved but in some cases the treatment process may be too slow to meet the specific needs of the patient.
The risks of IVF are yet to be fully elucidated. The procedure at a few decades old, is relatively new. From the TCM doctor’s point of view, it is the emphasis on quantity over quality that is the concern. The Kidney Jing, that hard-to-measure quality of inheritance, is ignored by IVF clinics. It may be some time before this risk, if it is real, can be fully assessed because large numbers of IVF babies have not yet tried to reproduce themselves.
Risks inherent in IVF to the mother include ovarian hyperstimulation syndrome and a higher frequency of pregnancy complications. An increased risk of developing non-invasive ovarian tumors has been shown in IVF patients.3 Other risks to the woman doing IVF include ovarian hyperstimulation syndrome, and side-effects of the drugs including abdominal discomfort, fatigue, and headaches. Chinese medicine treatment, because it has been tested and filtered through many hundreds of years of close observation has few side-effects or risks. Occasional digestive upset (from herbs) or bruising (from acupuncture) may occur.
Risks to the baby include higher rates of premature delivery, low birth weight, neonatal or later morbidity and birth defects. Such hazards are more pronounced in cases of multiple pregnancies but still apparent in singletons conceived with IVF.4–7
It is thought that some of these risks may be due to the infertility itself rather than the ART procedures. From our point of view, if the infertility was related to poor Kidney Jing in the first place, it is not surprising that this may be visited upon the offspring. TCM treatment of Kidney deficiency related infertility only succeeds if the Kidney is bolstered such that conception occurs and proceeds to a viable pregnancy and healthy offspring. Of course the sort of research done on IVF babies has not been done on babies conceived with the help of Chinese medicine, so it is impossible to assess the validity of this assumption.
However, the type of infertility appears not to influence adverse outcomes, i.e., women who were doing IVF because they had blocked tubes or because of male factor infertility showed no difference in adverse perinatal outcomes from other women. This indicates that the increase in adverse outcomes is more likely to be due to the procedures themselves than to the infertility which leads to their use.8
There is also evidence that defects in IVF babies are due to imprinting or epigenetic effects, i.e., the process (mediated by DNA methylation and stable chromatin modifications) by which certain genes are switched off or kept active. We know that in those first few days of life, chemical pollutants, dietary components, temperature changes and other external stresses can exert long-lasting effects on development, metabolism, and health, sometimes even persisting in subsequent generations.9–12 The impact of IVF culture medium and embryo manipulation is necessarily being closely examined in this context.
ART involves the manipulation of early embryos at a time when they may be particularly vulnerable to external disturbances. We know that environmental influences during embryonic and fetal development influence the individual’s susceptibility to cardiovascular disease13 and it appears that IVF children may indeed be at risk of vascular dysfunction similar in magnitude to that in children suffering from type 1 diabetes mellitus.14 Angiomas appear to be more prevalent among IVF children.15
Intracytoplasmic sperm injection (ICSI), in particular, has some biologists worried. If sperm are unable to make it as far as the fallopian tubes to fertilize an egg, presumably they are substandard and are rightly being discriminated against by the heartless but necessary process of natural selection. Further, if the sperm collected in an IVF procedure and placed in a Petri dish with some eggs are still unable to carry out fertilization, their biologic credentials are further in doubt. In Chinese medicine terms, we would describe sperm that lack the necessary to carry out penetration and fertilization of egg cells as reflecting quite serious Kidney Jing deficiency. This is not a good thing to be visited upon the putative new life. Of course, if the Jing is so deficient that it is incompatible with life, then the stages of cleavage and division that should happen after the sperm is injected into the egg will not proceed.
These concerns about lack of Kidney Jing do not apply to the sperm collected from men who have had a vasectomy or have some other mechanical blockage. In this case, there is no reason to think that their essential vitality (or Kidney Jing) is in any way defective, and relying on the methods of ART may be the only hope they have for becoming fathers (or becoming fathers again). Similarly, the effects of infections or exposure to radiation or chemicals that are short term should not have lasting effects on the Kidney Jing.
The artificial insertion of the sperm into the egg cytoplasm can change the way the sperm chromosomes line-up with the egg chromosomes (especially the X chromosome),16 and there is an increased risk of babies having a sex chromosome disorder if they are conceived after ICSI from a father with a very poor sperm count.17 There are higher than normal rates of embryopathy after ICSI.18 And a higher incidence of birth defects compared with IVF babies conceived without ICSI.19 Overall, absolute numbers of babies born with birth defects in babies conceived using ART are small; less than 10%. Many of the birth defects are minor and can be corrected.
Other risks associated with ART concern the pregnancy itself. A retrospective study found significant increases in odds ratio for gestational hypertension, placenta previa, need for cesarean section, and pre-term birth in IVF (singleton) pregnancies.20 ICSI appears to be related to a higher incidence of pre-term births and low birth weight babies.21
IVF is quick acting – a cycle is over in 4–6 weeks. However, not every IVF patient is pregnant in that time. Some IVF clinics have observed that if someone is going to get pregnant with IVF, they will most likely do so within 3 stimulated cycles.
On the other hand, improving the general health of the would-be parents and especially their gametes, can be quite a lengthy process, in particular the oocytes. It takes up to 9 months to nourish a follicle and its egg through all its stages of development from a nascent preantral stage. Sperm develop over a 3-month period and appear to respond quite rapidly to some treatment – some studies saw improvements after just 5 weeks of acupuncture treatment (see Ch. 7).
Typically, a treatment cycle with TCM that aims at improving the environment of the ovary and the eggs, might span 4–6 months or more, compared with the 4–6 weeks of a single IVF treatment cycle. TCM also aims to improve female fertility in other ways – specifically improving ovary function, regulating the menstrual cycle and balancing hormones. In this case, results can be seen more quickly, often around 3 months. In the case of relaxing the fine muscles of the fallopian tubes, the effect can be more immediate.
In summary, where TCM treatment of infertility is holistic, time tested and generally slow acting with few side-effects and little risk, IVF is specialized, relatively new and quick to get results but not without possible (though small) risk to mother and baby.
However, the results IVF achieves ensure that it is a technique which is here to stay. Most of the common criticisms made by patients about IVF (it is invasive, impersonal, experimental, and expensive) are compensated for by the fact that it provides results for a good number of the couples who use it. The price of any powerful and rapid medical protocol is the inherent risk involved (as we saw in Ch. 1).
IVF and TCM – different emphasis
The scope and emphasis of the two different sorts of treatments differ markedly. Table 10.4 summarizes this comparison.
Table 10.4
IVF and TCM – different emphasis
| IVF | TCM |
| Quantity of eggs | Quality of eggs |
| ICSI | Number, shape and vitality of sperm |
| Thickness of endometrium | Quality of endometrium |
| Few protocol variations | Endless treatment variations |
No matter how each patient presents, the IVF protocol is pretty much the same. There will be minor variations in doses of ovary-stimulating drugs, and there will occasionally be variations on timing of administration. But use of different drugs is often dictated by what is new or available, rather than the specific needs of an individual patient. The expertise of the fertility specialist comes therefore not so much in changing the prescription or timing for the dose of one of the drugs but from the technical surgical skill required when removing tiny egg cells from the ovary and transferring fragile embryos back to the uterus. And it is the expertise of scientists and embryologists who work in laboratories developing ways of managing eggs, sperm and embryos when they are outside of the body that has brought with it increased success rates and new techniques.
It is generally understood that IVF is essentially a numbers game – it increases the odds of success by increasing the numbers of eggs produced in a given month. This technique does not aim to affect the quality of the egg; rather it aims to increase the quantity of eggs, in the hope that in a large number, at least one will have what it takes.
The thickness of the lining of the uterus is the other factor measured by the radiographer. If it is inadequate, there is not much that the fertility specialist can do about it. If it is too thin (<6 mm), the transfer of any embryos may need to be postponed to a subsequent cycle in the hope that the endometrium might be adequate for a frozen embryo transfer.
The general health of the couple, in the absence of major pathology, is of minor concern. Whether the male partner has enough motile sperm is even becoming less important now in the days of ICSI. Sperm parameters will be measured but abnormalities are not treated (except for antioxidants in the case of DNA fragmentation) – they are circumnavigated with ICSI.
In contrast, Chinese medicine considers the overall health of the person (with special emphasis on Kidney Qi) who is making the gametes, based on the supposition that this will translate into healthier gametes. We know that the greatest determinant of a viable pregnancy is a viable embryo, which in turn depends largely on the fusion of healthy and compatible gametes. Unlike IVF, TCM treatment is not a numbers game. Treatment with Chinese medicine on its own does not usually increase the number of eggs ovulated. But it can influence some aspects of egg quality. This will be discussed below in detail when we look at TCM treatment for women preparing to do IVF.
In the clinic, we also use acupuncture to enhance release of the egg into and its journey down the fallopian tubes. In addition, TCM treatment aims to improve the fallopian tube environment and the endometrium thickness and quality. Chinese medicine can also influence the quality and vitality of the sperm.
The correct application of Chinese medicine in the treatment of infertility (as we saw in Ch. 4) is complex and demanding of its practitioners. Unlike the IVF treatment regimen, TCM has an endless number of variations – as numerous as the patients themselves. The skill of the TCM infertility specialist is in the correct diagnosis of subtle patterns of dysfunction, the correct prescription of herbs and their doses, the correct timing of the medicine, and the technical skill involved in applying acupuncture if that is part of the treatment program.
In the Clinic – Combining TCM and Art
Reputable texts of Chinese medicine can describe, with some authority, the presentation and treatment of different diseases and conditions based on some hundreds of years of observation and analysis by many generations of doctors working in clinics in China, refining and testing their protocols.
When it comes to treating patients using ART, none of us, here or in China, have more than a few years’ experience, and while what we have to offer the ART patient is no doubt valid and useful, we are not yet at the stage where textbooks stating ‘clinical truths’ can be published.
Hence, we will broach some ideas based on TCM principles but acted upon a new clinical (and pathologic, in the broad sense of the word) condition, namely, the patient with ‘controlled ovarian hyperstimulation’. However, we are not going to try and ‘cure’ this condition obviously, but we may try to enhance the ‘pathologic process’ and at the same time, contain it and protect the Zheng Qi of the patient. This is indeed new territory for a TCM doctor, and a different way of thinking.
Not only is this new treatment territory we find ourselves in, but also it may be a new clinical setting. Integrative medicine is one of the new frontiers many doctors are exploring and the combination of TCM and IVF is one of the stages it is being played out on increasingly. Driven by the demands of IVF patients, more IVF clinics are interested in working with acupuncturists and in some cases, are employing them.
The impetus for IVF patients to seek out acupuncture has its origins in some research published in 2002 that indicated that there was a small but significant increase in pregnancy rates if IVF patients had acupuncture on a certain day of their IVF treatment. The infertility chat rooms on the internet were soon full of this news. Since then, there has been more research, the results of which confirm this finding in some cases, or refute it in others. Hence, what claims can be made for acupuncture and TCM, what information is true and useful for IVF patients and indeed the place of acupuncture in the treatment of IVF patients in general, must be carefully assessed. It is contingent on all Chinese medicine practitioners to maintain vigilant and professional integrity in the face of demands from a particularly vulnerable and desperate section of the community.
TCM and IVF – points of influence
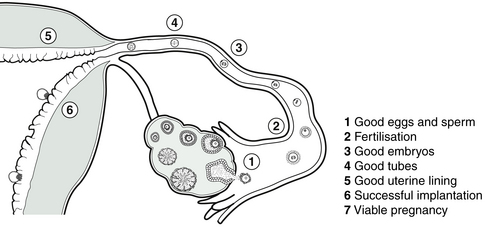
Before we talk in more detail about diagnosing and treating the IVF patient, let us recap the stages of an IVF treatment cycle and identify the points at which TCM may have a contribution to make. We have looked at the conceptual, philosophical, and practical differences between TCM and IVF. It is in fact these very differences that give the two methods the potential to skillfully complement or enhance each other’s strengths. The contributions of TCM and IVF influence fertility at different times at different levels and in different ways.
Figure 10.1 shows the points of influence of the two medical systems and Box 10.3 describes more fully the relative usefulness of the IVF and TCM at different stages of the path toward a viable pregnancy. Seen this way, it appears there may be a convenient dovetailing of the complementary contributions of TCM and IVF.
Diagnosis of the IVF patient
Diagnosis of the IVF patient begins and continues the way all our patients are diagnosed. That is with a collection of signs and symptoms much as we described in Chapter 4. If your patient has already undergone one or more IVF cycles, then information from this will add to your repertoire of diagnostic tools. It is not uncommon for patients coming to a TCM clinic requesting treatment for infertility to have a history of unsuccessful IVF cycles.
IVF history – a new diagnostic factor
Some of the pertinent questions you will ask the patient who has a history of IVF attempts are listed in Box 10.4.
How many stimulated IVF cycles?
The number of cycles already attempted not only gives you some idea of how fertile or not this couple is, but also allows an assessment of Kidney Jing stores. If a woman has completed a large number of cycles (≥5), especially if these have been over a short period of time, then it is likely her reserves will be depleted. Further evidence for this will be gleaned by the answers to the questions below.
How many mature eggs collected? (Dose of FSH required?)
A good response to the FSH drugs and plenty of ripe follicles with plenty of eggs collected indicates good Kidney Jing. Few eggs or high doses of FSH drugs imply depleted Kidney Jing (i.e., the pool of follicles available for recruitment is small). If a patient has done a number of IVF cycles it is useful to note how the response to the FSH drugs changes over time. If there is a trend to reduced numbers of eggs with repeated cycles, or a trend to higher FSH doses, then the depletion of Kidney Jing is being accelerated by the IVF process itself (or by aging). However, if egg numbers remain reasonably steady with repeated cycles and the dose of FSH administered does not rise, then ovarian reserve and resilience is good and the reason for the infertility is likely something other than poor egg quality or low Kidney Jing.
How many eggs fertilized? (with ICSI?)
This information gives us an indication of the maturity or quality of the eggs, as well as of the sperm function. If the eggs collected are immature, then some factor important to their development is lacking, likely the Kidney Yin or Jing.
If ICSI is required, then it usually indicates that sperm function is poor, although it should be noted that some clinics do ICSI routinely, whether there is a male factor or not.
How many embryos viable on Day 3 and on Day 5?
How the embryos develop tells us a lot about the energy of the eggs. As we discussed in Chapter 4, it is the egg cells that must provide the capacity to make the energy to drive the first few days of embryo cell division. If the egg is defective or has inadequate vitality, then the embryos will not develop past Day 3. This is an indication of low Kidney Jing or Yin or Yang. Or, since the genome of the embryo, made up of both mother’s and father’s chromosomes, must control growth after Day 3, sperm defects may also manifest at this stage.
How many transfers of embryos in total?
If a significant number of embryos (especially if they are blastocysts) has been transferred without a viable pregnancy eventuating, it is possible that there may be an issue with implantation. In this case, we turn our attention to the endometrium and look closely at any issues (such as immune factors) that might impact there – Blood or Yin deficiency, Blood stagnation or internal Heat can all contribute.
How many pregnancies (biochemical or viable) and miscarriages?
This information likewise tells about the success of implantation. Frequent early stage miscarriage indicates the possibility of immune factors rejecting the embryo, or some other failure of implantation or placentation. Once again, we need to look closely at Blood stasis or internal Heat, but also at Kidney Yang deficiency.
IVF history and TCM diagnosis
Let us now revisit our diagnostic categories relating to causes of infertility and include the information we get from the patient who has completed one or more IVF cycles.
Each of the diagnoses in Box 10.5 is characterized by symptoms and signs that we became familiar with in Chapter 4. For patients who have undergone IVF treatment, we can expand those characteristics. Women of different constitutions will react differently to different aspects of the IVF process. Symptoms or signs manifesting during, or related to the IVF cycle. As discussed in Chapter 4, it is important to realize that these categories are slightly contrived in the sense that they seldom occur in isolation. Real life means that they more often appear in crossover and mixed patterns. However, starting with discrete patterns like this, and describing some predictable responses to IVF treatments within the context of these patterns, gives us the manageable base from which we then create our diagnoses with the flexibility that clinical situations require.
Insufficient Kidney Jing
Women who are constitutionally Kidney Jing deficient tend to be frail and in more marked or obvious cases will have small hips and breasts and possibly small underactive ovaries. This woman likely started menstruating quite late and may have an irregular cycle. Her BBT charts may not show clear development of Kidney Yin to Kidney Yang in the luteal phase. Women in this category are born with low ovarian reserve. This may be related to genetic factors or factors operating during her mother’s pregnancy or in early infancy or childhood.
When such a woman is given FSH drugs, the blood tests will not show rapidly rising estrogen levels, indicating a poor response from the ovaries. In these cases, the FSH drugs may need to be continued longer than usual. If eggs are harvested, there are usually low numbers and egg quality is not optimal.
(Note Kidney Jing deficiency that is not constitutional but due to damage and depletion is also a common cause of infertility and poor response to IVF drugs, however the constitutional signs described above may not present in this case).
Insufficient Kidney Yin
This is the most common diagnosis seen in infertility clinics in the West. Women in their late 30s and early 40s who are peri-menopausal often fall into this category. Their menstrual cycles may have subtly shortened if the Yin deficiency has given rise to some internal Heat, and this may also be manifesting in nervous system symptoms, such as disturbed sleep and anxiety.
If the Yin deficiency is accompanied by, or has led to, Blood deficiency, the menstrual cycles may be longer than 28 days and the flow may become scanty. Scanty and dark flow can also be a result of internal Heat arising from Yin deficiency.
When Yin and Blood are lacking, the endometrium will not develop well and ultrasounds will show a thin lining (<10 mm at time of egg collection).
As in the previous category, the administration of FSH drugs may need to be extended and doses may need to be increased if the ovaries are not responding. These women do not produce large numbers of eggs and those they do produce are not always of good quality. Side-effects such as flushing or anxiety or irritability are possible. Hyperstimulation is unlikely in this category.
After an unsuccessful IVF cycle, the ovaries may take some time to recover as Yin and Blood stores are gradually replenished and the Chong vessel refills.
Some women with immune factors contributing to infertility may fall into this category.
Insufficient Kidney Yang
You may have diagnosed this patient with a Kidney Yang deficiency before she embarked on IVF, if her BBT charts had indicated a short luteal phase. Women with Yang deficiency tend to be lethargic, and this can be exacerbated markedly by drugs used during the IVF cycle. Depression or low mood may accompany the fatigue. While egg numbers may be adequate, often these do not make embryos that make it to blastocyst stage. Embryos may be transferred on Day 3 but implantation or sustained growth of the embryo may fail in these cases, resulting in a negative HCG test or a biochemical pregnancy (very low HCG). Women with untreated Kidney Yang deficiency who do conceive, are less able to support early stage pregnancy and may need more progesterone supplementation (or Kidney Yang herbs).
Heart Qi stagnation
Some forms of amenorrhea fall into this category (as seen in Ch. 5) but Heart Qi stagnation does not always disturb the menstrual cycle. The most common symptom confirming this diagnosis will be anxiety, insomnia, or palpitations. Women with instability of the Shen find doing IVF very emotionally taxing, and hence do not often cope with more than 1 or 2 cycles.
If there is no Kidney factor, then numbers of eggs and embryos are expected to be adequate. These women gain enormous benefit from acupuncture support during the IVF cycle, although there will still inevitably be some emotional cost. Where pregnancy does occur, this group of women will be strongly advised to continue acupuncture for the 1st trimester, to ensure the Shen is stable, the Bao and Luo mai are secured and the uterus stays closed.
Liver Qi stagnation
Liver Qi stagnation is not such a common cause of infertility on its own, and where it is, it is a pattern that is easily rectified with Chinese medicine. However, the impatient manner that women with Liver Qi stagnation exhibit often takes them to the IVF clinic prematurely. In the absence of any other pathology, egg and embryo quality is not of concern.
They tend to suffer side-effects such as headaches, abdomen discomfort and bloating, and irritability. There is a slightly increased risk of ovarian hyperstimulation syndrome with these patients, especially if they have been diagnosed with PCOS. Acupuncture during the IVF cycle is useful for these patients to reduce stress and ease side-effects.
Blood stagnation
Blood stagnation is a reasonably common pattern seen in the IVF clinics. In fact, IVF was initially designed for patients with blocked tubes (which is one form Blood stagnation can take). Most other forms of substantial Blood stagnation, such as endometriosis, polyps, cysts, and large fibroids will be dealt with surgically before IVF is attempted. More subtle Blood stagnation in the form of immune or clotting factors will be treated with blood thinning medications and Chinese herbs. Blood stagnation, as we saw in Chapter 5, and shall see below, appears to have deleterious effects on egg quality.
Phlegm-Damp
Women with Phlegm-Damp can have a difficult time with IVF, becoming lethargic and easily putting on weight, which is hard to move after the IVF cycle, whether they have conceived or not. These patients feel quite uncomfortable during IVF and acupuncture is useful for relief.
Patients diagnosed with PCOS often fall into this category and they are at increased risk of ovarian hyperstimulation syndrome. Large numbers of eggs may be retrieved but in these circumstances, they are not generally of good quality.
In summary, most of these categories of infertility benefit from TCM treatment prior to attending the IVF clinic, and some benefit greatly from treatment during the IVF cycle. Treatment of the IVF patient before and during the cycle is discussed in Chapter 11.
References
1. Jansen, R. Getting pregnant. Sydney: Allen and Unwin; 2003. [391].
2. Jansen, R. Getting pregnant. Sydney: Allen and Unwin; 2003. [389].
3. van Leeuwen, F.E., Klip, H., Mooij, T.M., et al. Risk of borderline and invasive ovarian tumors after ovarian stimulation for in vitro fertilization in a large Dutch cohort. Hum Reprod. 2011;26(12):3456–3465.
4. Finnström, O., Källén, B., Lindam, A., et al. Maternal and child outcome after in vitro fertilization – a review of 25 years of population-based data from Sweden. Acta Obstet Gynecol Scand. 2011;90:494–500.
5. Klemetti, R., Gissler, M., Sevón, T., et al. Children born after assisted fertilization have an increased rate of major congenital anomalies. Fertil Steril. 2005;84(5):1300–1307.
6. Olson, C.K., Keppler-Noreuil, K.M., Romitti, P.A., et al. In vitro fertilization is associated with an increase in major birth defects. Fertil Steril. 2005;84(5):1308–1315.
7. Reefhuis, J., Honein, M.A., Schieve, L.A., et aland the National Birth Defects Prevention Study. Assisted reproductive technology and major structural birth defects in the United States. Hum Reprod. 2009;24(2):360–366.
8. Chung, K., Coutifaris, C., Chalian, R., et al. Factors influencing adverse perinatal outcomes in pregnancies achieved through use of in vitro fertilization. Fertil Steril. 2006;86(6):1634–1641.
9. Feil, R., Fraga, M.F. Epigenetics and the environment: emerging patterns and implications. Nat Rev Genet. 2012;13:97–109.
10. Maher, E.R. Imprinting and assisted reproductive technology. Hum Mol Genet. 2005;14:133–138.
11. Maher, E.R., Brueton, L.A., Bowdin, S.C. Beckwith-Wiedemann syndrome and assisted reproduction technology (ART). J Med Genet. 2003;40:62–64.
12. Ludwig, M., Katalinic, A., Gross, S. Increased prevalence of imprinting defects in patients with Angelman syndrome born to subfertile couples. J Med Genet. 2005;42:289–291.
13. Barker, D.J. The origins of the developmental origins theory. J Intern Med. 2007;261:412–417.
14. Scherrer, U., Rimoldi, S.F., Rexhaj, E., et al. Systemic and pulmonary vascular dysfunction in children conceived by assisted reproductive technologies. Circulation. 2012;125:1890–1896.
15. Viot, G., Epelboin, S., Olivennes, F. Is there an increased risk of congenital malformations after ART? Results from a prospective French long-term survey of a cohort of 15162 children. Hum Reprod. 2010;25(Suppl 1):i53–i55.
16. Terada, Y., Luetjens, C.M., Sutovsky, P., et al. Atypical decondensation of the sperm nucleus, delayed replication of the male genome, and sex chromosome positioning following intracytoplasmic human sperm injection (ICSI) into golden hamster eggs: does ICSI itself introduce chromosomal anomalies? Fertil Steril. 2000;74(3):454–460.
17. Jansen, R. Getting pregnant. Sydney: Allen and Unwin; 2003. [149].
18. Lathi, R.B., Milki, A.A. Rate of aneuploidy in miscarriages following in vitro fertilization and intracytoplasmic sperm injection. Fertil Steril. 2004;81:1270–1272.
19. Davies, M.J., Moore, V.M., Willson, K.J., et al. Reproductive technologies and the risk of birth defects. N Engl J Med. 2012;366:1803–1813.
20. Poikkeus, P., Gissler, M., Unkila-Kallio, L., et al. Obstetric and neonatal outcome after single embryo transfer. Hum Reprod. 2007;22:1073–1079.
21. Aytoz, A., Camus, M., Tournaye, H., et al. Outcome of pregnancies after intracytoplasmic sperm injection and the effect of sperm origin and quality on this outcome. Fertil Steril. 1998;70:500–505.
22. Chung, K., Coutifaris, C., Chalian, R., et al. Factors influencing adverse perinatal outcomes in pregnancies achieved through use of in vitro fertilization. Fertil Steril. 2006;86(6):1634–1641.
23. Stener-Victorin, E., Waldenstrom, U., Andersson, S.A., et al. Reduction of blood flow impedance in the uterine arteries of infertile women with electro-acupuncture. Hum Reprod. 1996;11:1314–1317.