Promoting Bowel Elimination
Upon completing this chapter, you should be able to:
1 Describe the process of normal bowel elimination.
2 Identify abnormal characteristics of stool.
3 Discuss the physiologic effects of hypoactive bowel and nursing interventions to assist patients with constipation.
4 List safety considerations related to giving a patient an enema.
5 Describe three types of intestinal diversions.
6 Discuss the stoma and peristomal assessment and skin care.
7 Discuss the psychosocial implications for a patient who has an ostomy.
1 Use nursing measures to promote regular bowel elimination in patients.
3 Perform a focused assessment of the bowel.
4 Assist RN in identifying appropriate nursing diagnoses for a patient with bowel problems.
5 Prepare to administer an enema.
6 Assist and teach the patient who is incontinent with a bowel retraining program.
7 Provide ostomy care, including irrigation and changing the ostomy appliance.
anus ( , p. 577)
, p. 577)
appliances (p. 590)
atrophy ( , p. 577)
, p. 577)
bile (p. 578)
bowel training program (p. 588)
chyme ( , p. 577)
, p. 577)
colostomy ( , p. 590)
, p. 590)
constipation (p. 578)
defecate ( , p. 577)
, p. 577)
diarrhea ( , p. 580)
, p. 580)
effluent ( , p. 590)
, p. 590)
excoriation ( , p. 584)
, p. 584)
fecal impaction ( , p. 579)
, p. 579)
fecal incontinence ( , p. 580)
, p. 580)
feces ( , p. 577)
, p. 577)
flatus ( , p. 579)
, p. 579)
gastrocolic reflex ( , p. 577)
, p. 577)
hemorrhoid ( , p. 578)
, p. 578)
ileostomy ( , p. 590)
, p. 590)
melena ( , p. 578)
, p. 578)
occult ( , p. 578)
, p. 578)
 ,
, periostomal ( , p. 592)
, p. 592)
peristalsis ( , p. 577)
, p. 577)
rectum ( , p. 577)
, p. 577)
sphincter ( , p. 577)
, p. 577)
steatorrhea ( , p. 578)
, p. 578)
stoma ( , p. 590)
, p. 590)
stool (p. 576)
vagal response ( , p. 588)
, p. 588)
Valsalva maneuver ( , p. 577)
, p. 577)
The term bowel refers to the intestine. Bowel elimination, the excretion of solid waste, is the final step in the process of digestion. The processing of nutrients through digestion was discussed in Chapter 26. In this chapter, normal functions of the intestinal tract are reviewed and conditions that affect the composition and appearance of stool (waste eliminated from the colon) are discussed. Ways to assist the patient in achieving and maintaining regular elimination of waste matter from the bowel and procedures to alleviate problems related to alterations in elimination are presented. When an alternative for waste elimination is needed due to disease of the intestine, an ostomy (opening into the intestine) may be performed. The basic nursing care for such a procedure completes this chapter.
OVERVIEW OF STRUCTURE AND FUNCTION OF THE INTESTINAL SYSTEM
Which structures of the intestinal system are involved in waste elimination?
 The small intestine—consisting of the duodenum, the jejunum, and the ileum—carries chyme (liquefied food and digestive juices) from the stomach to the large intestine.
The small intestine—consisting of the duodenum, the jejunum, and the ileum—carries chyme (liquefied food and digestive juices) from the stomach to the large intestine.
The small intestine attaches to the large intestine at the cecum. The ileocecal valve controls the progress of substances into the large intestine.
The large intestine has four main portions: the ascending colon, transverse colon, descending colon, and sigmoid colon. It is larger in diameter than the small intestine but only about 1.5 m (59.5 inches) long (Figure 30-1).
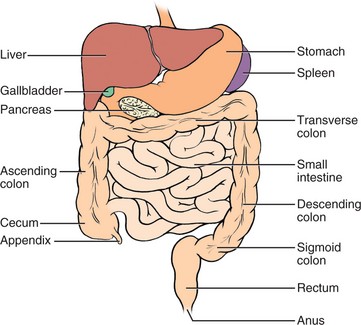
The rectum (distal portion of the large intestine where feces are stored) connects to the anus (opening of the rectum at the skin).
The walls of the intestines have four layers: mucosa, submucosa, muscular layer, and a serous layer called serosa.
What are the functions of the intestines?
The small intestine further processes chyme into a more liquid state. Food substances are absorbed into the bloodstream from the villi on the walls of the small intestine.
In the large intestine, water, sodium, and chlorides are reabsorbed and waste material is propelled to the anus.
The large intestine contains bacteria that break down waste products. Water is extracted from the waste during transit.
Peristalsis (wavelike movement through the intestines) moves chyme and gas formed by bacterial action through the intestines. The circular, longitudinal, and oblique muscle layers of the intestine expand and contract to accommodate and move the chyme.
The movement of liquid and gas causes the rumbling noise of bowel sounds. It takes about 18 to 72 hours for food to move from the mouth to the anus.
Feces (intestinal waste material) is stored in the sigmoid until it moves into the rectum for expulsion through the anus.
As the rectum fills, the pressure on the sphincter (circular muscle that closes an orifice) of the anus increases until the urge to defecate (expel feces) occurs.
The abdominal muscles contract to help force the evacuation of the rectum.
The internal anal sphincter, located at the top of the anal canal, is under involuntary control; the external sphincter at the end of the anal canal is controlled voluntarily.
The gastrocolic (stomach to colon) reflex initiates peristalsis, which in turn initiates the urge to defecate; it is stimulated by eating. Reflex emptying of the rectum can be stopped by tightening the voluntary anal sphincter.
Intra-abdominal pressure increases when a person holds the breath, closes the glottis, and tightens the abdominal muscles. This initiates voluntary defecation and is called the Valsalva maneuver.
The vermiform appendix attaches to the cecum of the ascending colon and has no known digestive function.
What effect does aging have on the intestinal tract?
Atrophy (decrease in size) of the villi in the small intestine may decrease the total absorptive surface. It has not been proven that decreased absorption of nutrients, other than fats and vitamin B12, actually occurs.
Sometimes twisting of blood vessels supplying the large intestine compromises the blood flow to the large intestine. Motility in the large intestine may decrease in some individuals, but bowel habits do not change with aging in the healthy individual.
CHARACTERISTICS OF STOOL
Stool is another term for feces. Normal feces are one quarter solid material and three quarters water. The solid material consists of about 30% dead bacteria and 70% undigested roughage from carbohydrate, fat, protein, and inorganic matter. The appearance of stool is influenced by diet and metabolism.
NORMAL CHARACTERISTICS OF STOOL
Normal stool is light to dark brown, soft, and formed in children and adults. Infant stool may be a dark yellow depending on the type of feedings. The light to dark brown color is caused by bile (orange or yellow digestive fluid produced by the liver). The color of feces may be changed by certain vitamins, drugs, or diet. Stool is usually tubular in shape and has a diameter of about 2.5 cm (1 inch).
ABNORMAL CHARACTERISTICS OF STOOL
The most serious abnormality is blood in the stool. Fresh blood in the stool is easily visible as bright red on the surface of the stool. Occult (hidden) or old blood is suspected when the stool changes from a normal brown appearance to a dark black color with a sticky appearance. The observance of blood in the stool should be reported promptly and recorded on the patient’s chart.
Serious causes of blood in the stool include hemorrhage from ulcers in the stomach or duodenum; severe inflammation or irritation, as in ulcerative colitis or diverticulitis; cancer; and other diseases that cause hemorrhage. Collection of a stool specimen and testing for occult blood are presented in Chapter 24.
Bright red blood in the stool is a sign of a recent gastrointestinal (GI) hemorrhage or bleeding that occurred in the large intestine. The color indicates that the blood has not undergone digestion in the upper part of the bowel, nor has it been in the intestinal tract for hours. As blood moves through the stomach or small intestine, it undergoes partial digestion, which changes it to a dark, tarry substance (melena). Eating beets may make the stool appear red, but this should not be confused with blood.
Pale white or light gray stool indicates an absence of bile in the intestine. This is usually due to an obstruction in the bile or common duct leading to the intestine from the liver and gallbladder. This finding should be reported to the physician.
Other abnormal characteristics of feces are the presence of large amounts of mucus, fat, pus, or parasites, such as worms. Unusual amounts of mucus in the stool indicate an irritation or inflammation of the inner surface of the intestines. The mucus coats the stool and gives it a slimy appearance. The presence of pus indicates drainage of an ulcer that is inflamed or infected. The most common parasitic worms found in the intestines are the tapeworm, pinworm, and roundworm. Stools with an abnormally high fat content (steatorrhea) are usually foul smelling and float on water.
The first signs of colorectal cancer are changes in bowel patterns and stool characteristics; in accordance with the Healthy People 2010 goal (3.5) to reduce colorectal cancers, patients should be encouraged to report these changes and to participate in colon cancer screening programs.
HYPOACTIVE BOWEL AND CONSTIPATION
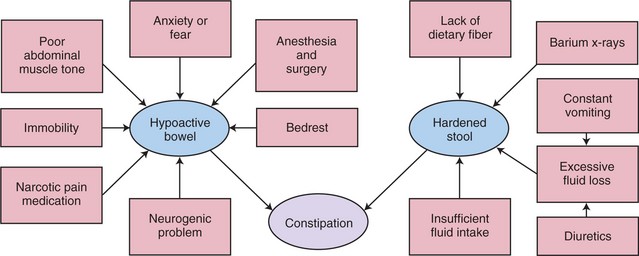
An absence or reduction of peristaltic movement of the bowel results in a hypoactive bowel. Some injuries and diseases cause a hypoactive bowel, but often this condition is a complication of immobility. In the normal person, lack of sufficient fiber in the diet and decreased exercise may produce a sluggish or hypoactive bowel (Health Promotion Points 30-1). Sometimes irritable bowel syndrome (IBS) causes hypoactivity of the bowel, although hyperactivity is more common.
Constipation (decreased frequency of bowel movement or passage of hard, dry feces) is the most common problem of a hypoactive bowel. With constipation, feces become more compacted and hardened, making them more difficult to expel. Feces tend to back up into the colon. Constipation may occur when muscle tone is lacking, when there is irregularity of bowel movements, or when excessive worry, anxiety, and fear are present.
Nurses must be aware of the potential of illnessinduced constipation. Any patient restricted to bed rest is at risk for constipation. Patients who are receiving medications that can cause constipation, undergoing barium x-ray studies, or recovering from surgery are at risk for bowel evacuation problems. Many medications can contribute to constipation (Box 30-1). It is extremely important that every nurse be alert to patients at risk for constipation in order to prevent its occurrence (Concept Map 30-1).
Abdominal distention is caused by flatus (gas) accumulation in the intestinal tract when peristalsis is reduced or absent. Just as fecal matter will collect in the hypoactive bowel, so will flatus. Distention and gas pains occur frequently after abdominal surgery. The discomfort and pain are caused by the stretching of the intestinal wall and spasm of the muscle layers.
HYPERACTIVE BOWEL AND DIARRHEA
An increase in motility of the gastrointestinal tract or increased peristalsis results in a hyperactive bowel. Causes of a hyperactive bowel include inflammation in the gastrointestinal tract, certain drugs, infectious agents, and diseases such as diverticulitis, ulcerative colitis, Crohn’s disease, and irritable bowel syndrome. Patients who have gastric bypass surgery may also experience diarrhea (frequent loose stool).
Diarrhea occurs when increased peristalsis pushes food through the intestinal tract too fast. The increased speed does not allow enough time for the absorption of nutrients, electrolytes, and water, and the feces are liquid or semi-formed. Evacuations are more frequent, with an increased number of stools per day. Often, diarrhea is simply the body trying to rid itself of pathogens (Cultural Cues 30-1). Moderate diarrhea lasting a couple of days usually clears up by itself. At times, diarrhea can lead to temporary fecal incontinence (the lack of voluntary control over the anal sphincter) and inability to retain feces. See Box 30-2 for a list of common antidiarrheal medications.
FECAL INCONTINENCE
Persons of all ages may become incontinent of feces because of illness such as cerebrovascular accident, traumatic injury, or neurogenic dysfunction. Incontinence is a distressing condition that causes a loss of dignity. Incontinent patients often feel embarrassed or anxious. They can also experience loss of self-respect or fear of loss of control over what is happening to them. It is important to reassure them that there are programs available to assist them with the problem.
APPLICATION of the NURSING PROCESS
Every patient is assessed regarding bowel status every day in an inpatient facility. Home care nurses assess bowel status at each visit. The patient is questioned about the regularity of bowel evacuation, problems, and any abnormal characteristics in the appearance of the stool. If possible, the stool is visually examined. Focused Assessment 30-1 provides guidelines for bowel assessment. Many people think that it is abnormal not to have a bowel movement every day, but it is normal for many people to have a bowel movement only every 2 to 3 days. Look at all the factors that affect bowel function and the patient’s normal pattern before determining whether there is a problem (Cultural Cues 30-2).
Distention is revealed by an abdomen that is rounder and tighter in appearance than normal. The patient’s abdomen is assessed for distention by percussion, and the nurse gently palpates the four quadrants of the abdomen to check for tenderness and masses. The patient may complain of abdominal discomfort and often describes it as gas pain. Percussion is used to detect abnormal amounts of gas. Areas of gas produce a drum-like, hollow tone. Review assessment of the abdomen in Chapter 22.
Nursing Diagnosis
When assessment data indicate an intestinal problem, the correct nursing diagnosis is chosen from the NANDA-I list. Possible choices are as follows:
• Constipation related to hypoactive bowel
• Diarrhea related to food intolerance
• Bowel incontinence related to loss of anal sphincter control
• Pain related to abdominal distention
• Self-care deficit, toileting related to traction
• Disturbed body image related to bowel incontinence
• Deficient knowledge related to factors that contribute to constipation
The full diagnosis is written using the related cause particular to each patient.
Planning
A plan is developed for the patient’s care by writing expected outcomes for each nursing diagnosis chosen. Outcomes must be realistic and can be both short and long term. Sample expected outcomes for the previous nursing diagnoses are as follows:
• Constipation will be relieved by walking a mile a day.
• Episodes of diarrhea will decrease within 3 days.
• Patient will improve bowel control within 2 months of starting a retraining program.
• Pain from distention will be decreased within 24 hours.
• Patient will maintain as much independence as possible in toileting by using an over-the-bed trapeze and a urinal during this shift.
• Body image will improve as incontinence lessens.
• Patient will identify foods to add to diet to increase fiber during this shift.
See Nursing Care Plan 30-1 for further examples of expected outcomes.
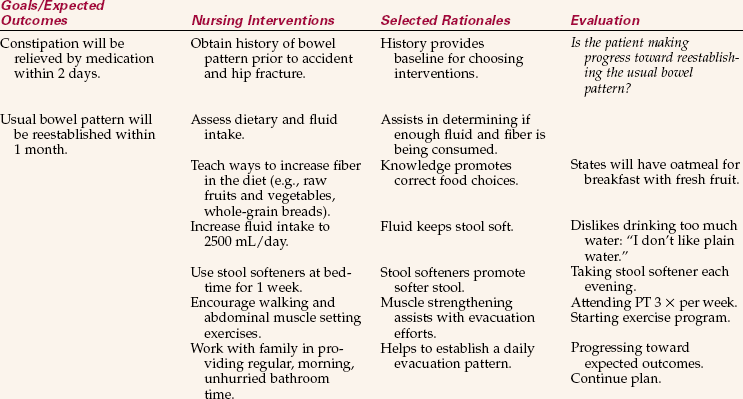
NURSING CARE PLAN 30-1
Care of the Patient with Constipation
Martina Svoboda, age 64, fractured her left hip in a fall a month ago. Her hip is healing, but she still has difficulty walking. While in the hospital, her usual bowel pattern became disrupted. She has had difficulty with constipation ever since (“having difficulty with bowels.”). She is presently staying at her daughter’s home. The stool is hard and dry; she has a BM every third day.
Another aspect of planning is to provide time in the shift work schedule for the administration of ordered treatments such as enemas. Time must be planned to carry out a bowel retraining program if that is part of the care plan for the incontinent patient. When an incontinent patient is assigned, more time must be allotted for attempts at toileting and for cleaning the patient (Assignment Considerations 30-1).
Implementation
You must assist the bed rest patient with use of the bedpan or bedside commode. Privacy is of great importance in making the patient comfortable enough to defecate. Patients are often embarrassed by thesounds and smells accompanying defecation of feces. Patients should be assisted to as much of a sitting position as their condition allows (Cultural Cues 30-3). The abdominal muscles and gravity can then assist with defecation. Gloves are always worn when helping the patient off the bedpan. Check to see that the patient is thoroughly cleaned, especially if the patient cannot lift up off of the pan in order to clean the anus and surrounding area. The bedpan should be thoroughly cleansed and dried and put away. The bedside commode should be emptied and cleaned promptly after use (Safety Alert 30-1).
When the average patient has not experienced bowel evacuation within 3 days, measures should be taken to assist elimination. Assessment data guide the measures to be implemented. The least invasive measures are used first. Encouraging and monitoring activity, adequate fluid intake, and a diet with sufficient fiber may lead to regular bowel elimination. Noninvasive measures that can be used to promote bowel elimination include the consumption of 1 to 3 tablespoons of bran mixed with applesauce, small amounts of prune juice, warmed prune juice and cola, hot water with lemon juice, or stewed or dried prunes. Be careful because some people are particularly sensitive to the effects of prunes, and diarrhea may develop.
If these actions are not successful, more invasive measures to promote bowel elimination should be implemented. These measures include the administration of medications to soften the stool, suppositories to stimulate the urge to defecate, laxatives to stimulate bowel activity, and enemas to empty the rectum. All of these measures require a physician’s order for inpatients. Measures to rid the bowel of barium are essential after a patient has had barium x-rays. Encourage an increase in fluid intake of 3500 mL/day for the next 24 hours unless contraindicated. A laxative is often recommended.
Home care patients are encouraged to phone the nurse if they have not had a bowel movement in 3 days. Impaction may be prevented if constipation is treated early. The caregiver for the patient is given instruction on how to insert a suppository or how to give a small-volume enema so that these measures might be carried out if less invasive measures do not work.
When the patient experiences incontinence, cleansing should occur as soon as possible (Assignment Considerations 30-2). Skin care must be thorough and gentle because feces are irritating to the skin and can cause excoriation (abrasion of the skin). The patient who is having diarrhea stools may need a skin protectant around the anus to prevent skin breakdown and considerable discomfort. Products such as petroleum jelly, A & D ointment, cod liver oil ointments with zinc oxide, and commercial skin barrier products are helpful to protect the skin. Gentle washing with soap and water, rinsing, and patting dry are essential to protect the skin. Baby wipes are useful during diarrhea episodes.
When diarrhea is thought to be caused by bacteria or a virus, the physician may want to let it run its course for at least 24 hours so that the body has a chance to rid itself of the offending organism. Diarrhea from other causes simply leads to fluid and electrolyte loss and should not be allowed to continue for long periods of time. Treatment involves placing the patient on a clear liquid diet to rest the bowel, replacing fluids and electrolytes, and seeking medication to stop the loose stools. Observe for signs of dehydration when the patient has severe diarrhea: decreased skin turgor, dry mucous membranes with thick saliva, and increased thirst. Self-medication for diarrhea should not continue for more than 48 hours without consulting a physician (Nutritional Therapies 30-1).
Evaluation
Evaluation for patients with problems of bowel function is based on whether expected outcomes and goals have been met. If outcomes and goals are not being met, the plan needs to be reconsidered and revised. Examples of evaluation statements might be as follows:
• Patient is walking 1 mile a day.
• Patient has increased fluid intake to 3500 mL, is eating bran at breakfast, and is producing stool every other day.
• Bowel movement occurs every morning despite continued use of pain medication.
• Patient has been continent of stool for 6 days.
• Patient is feeling better about self since bowel regimen has produced continent stool for 3 days in a row.
• Patient identified foods high in fat and milk products as causing diarrhea.
Nursing Care Plan 30-1 provides other examples of evaluation.
Documentation: Any changes in bowel habits should be documented: stool characteristics, episodes of constipation or diarrhea, and measures taken to remedy the problem. The teaching plan is documented along with times ofeach teaching session and material covered. Evaluation of teaching is also noted. All measures to promote bowel elimination must be documented. The number and approximate amount of diarrhea stools are charted on the appropriate flow sheets (intake and output and daily activity sheets).
RECTAL SUPPOSITORIES
Rectal suppositories used to promote bowel movements are glycerin and bisacodyl suppositories. Suppositories that promote bowel evacuation do so by (1) stimulating the inner surface of the rectum and increasing the urge to defecate, (2) forming gas that expands the rectum, or (3) melting into a lubricating material to coat the stool for easier passage through the anal sphincter. See Chapter 34 for the procedure to insert a rectal suppository.
ENEMAS
An enema is the introduction of fluid into the rectum and colon by means of a tube. Enemas are given to stimulate peristalsis and the urge to defecate or to wash out the waste products or feces. Cleansing enemas are given when the bowel is to be examined by x-ray, colonoscopy, or sigmoidoscopy or when the bowel is distended by flatus. The volume of a cleansing enema depends on the age of the patient: infant or toddler, 50 to 150 mL (normal saline only); ages 3 to 5, 200 to 300 mL; school age, 300 to 500 mL; adult, 500 to 1000 mL. Figure 30-2 shows the equipment used for a cleansing enema. An enema kit will contain either a bag or a bucket for the solution. The commercially disposable enema, such as the Fleet enema, is convenient and easy to use when only a small amount of fluid is needed to stimulate a bowel movement. Enemas can be given at any time, but it is best to try to give them before the morning bath and bed linen change.

TYPES OF ENEMAS
The type of enema to be given is prescribed by the physician and will vary depending on the patient’s age and condition, the purpose of the enema, and the preference of the physician (Table 30-1). The type of solution is specified, and you are expected to know how to prepare it unless a commercial enema has been ordered. The commercially packaged enema may require more lubricant on the nozzle; other supplies needed are the same as for any type of enema. When other types of enemas are ordered, consult the hospital’s procedure manual for the ingredients and the proportions to use.

Retention Enema
Often an oil-retention enema is ordered for a patient who is constipated. The oil must be retained in the rectum to soften and coat the hardened feces. Between 120 and 180 mL of warm oil is instilled rectally in the same manner as the cleansing enema, except that the oil should be retained at least 20 minutes. Prepackaged enemas are usually used for this purpose, but mineral oil or olive oil can be used.
AMOUNT AND TEMPERATURE OF SOLUTION
Disposable enema units contain about 240 mL of solution (Figure 30-3). They may be given at room temperature, but work best when slightly warmed (Safety Alert 30-2). No special preparation is needed; they are ready for use when taken from the package. With the patient in the left Sims’ position, the prelubricated nozzle is inserted into the rectum, and the solution is instilled by squeezing the flexible plastic bottle. Rolling the bottle up from the bottom aids in instilling the entire contents.
The amount of solution used for a cleansing enema for adults is between 500 and 1000 mL; smaller amounts are used for children (Safety Alert 30-3). Hold the container approximately 12 to 18 inches above the patient’s anus and allow the warm solution to run inslowly; a greater height creates too much pressure because the fluid runs in too rapidly and causes painful distention of the rectum and colon. This stimulates the urge to defecate immediately, so that the patient cannot retain the fluid.
RECOMMENDED POSITION
The position of choice when giving an enema is the left Sims’ position with the hips slightly elevated (Figure 30-4). This allows the fluid, aided by the force of gravity, to flow downward along the natural curve of the rectum and descending colon. If the patient is unable to turn to the side, the supine position can be used (Skill 30-1).
Skill 30-1 Administrating an Enema
An enema is given to evacuate the bowel. Tap water, soapsuds, or saline solution of 500 to 1000 mL is given to the adult with an enema bucket or bag. A disposable enema, consisting of 120 mL of hypertonic solution, may be ordered. An oil-retention enema may be required to soften stool so that evacuation can occur more easily.
Review and carry out the Standard Steps in Appendix 3.
3. ACTION If possible, place the patient in the left Sims’ position and drape with the bath blanket. Place the underpad under the buttocks.
RATIONALE Solution travels up the colon more easily when the patient is lying on the left side. Underpad will protect the linens from moisture or soiling.

4. ACTION Put on gloves. Fill the enema bag with the correct solution; temperature of the water should be between 100° and 105° F (37.8° and 40.5° C). Expel air from the tubing by opening the clamp and allowing the solution to run through. Use the bedpan or sink to collect the solution; reclamp the tube.

RATIONALE Gloves prevent transfer of microorganisms. The physician orders the type of solution. Water that is too hot may burn the patient; water too cool may cause cramping. Expelling air from tube prevents air from being introduced into the colon, which could cause the patient discomfort.
5. ACTION Position the bedside commode or put the bedpan close at hand. Generously lubricate the end of the enema tube and, while the patient takes a deep breath, gently insert it about 4 inches in the adult anus. Direct the tube toward the umbilicus. Ask the patient to take a deep breath through the mouth to relax the anal sphincter. Twisting the tube gently helps it pass through the sphincter.
RATIONALE Bedpan or bedside commode will be needed as soon as all the fluid has been instilled. Generous lubricant is needed if the patient has hemorrhoids. It is possible to perforate the wall of the rectum with the tube if force is used; gentle pressure and slow advancement are best.
6. ACTION With the container about 12 to 18 inches above the anus, open the clamp on the tube, steady the tube in place, and allow the solution to flow slowly into the bowel over 5 to 10 minutes. Lowering slightly and again raising the container to this height will regulate the speed of the flow. Slight pressure on the tubing with the clamp can also slow the flow. When the patient expresses discomfort, stop the flow by kinking the tubing or clamping it, and instruct the patient to take deep breaths by mouth until the cramping and urge to expel the fluid pass. Continue until the patient can retain no more or the container is empty. Clamp the tubing and withdraw it, asking the patient to squeeze the sphincter shut; place the soiled tube on a paper towel.
RATIONALE Too forceful a flow may damage the bowel. Instilling the fluid slowly prevents cramping and usually obtains the best result with the least discomfort. Some patients can hold only a few hundred milliliters of solution at a time; others can tolerate the entire volume.
For Disposable or Oil-Retention Enema
7. ACTION Add extra lubricant to the tip if the amount of prelubrication seems insufficient. Insert the tip into the anal opening as directed previously. Gently squeeze the bottle, and roll it up from the bottom as the contents enter the bowel. Squeeze as much of the fluid into the patient as possible. Remove the tip slowly and hold the buttocks together.
RATIONALE The lubricant on the tip sometimes dries out. Disposable enemas contain approximately 120 to 240 mL of solution. Slow instillation achieves the best result. An oil-retention enema is given in the same manner, but the patient should retain it for 20 minutes to 2 hours so that it will soften the stool.
8. ACTION Assist the patient onto the bedpan or bedside commode. If the patient uses the toilet, request to see the result before flushing. If a bedpan is used, raise the head of the bed to a sitting position. Place call bell and toilet paper within reach.
RATIONALE This provides a container for collection of enema return and the opportunity to observe characteristics of stool expelled.
9. ACTION When the bowel contents have been expelled, assist the patient in cleaning the anal area; observe the results of the enema, noting the color, amount, and consistency of the stool. Remove and clean the bedpan or bedside commode.
RATIONALE Results of the enema are judged by the stool expelled.
10. ACTION Restore the patient unit, lower the bed, and place the call bell within reach.
RATIONALE Shows consideration for the patient and provides safety.

RECTAL TUBE
When a patient is uncomfortable because of flatus in the lower bowel, a rectal tube can be inserted in the anus. The tube is similar to the enema tubing. This allows the gas to be expelled without the patient’s straining to open the anal sphincter. Oral medications to reduce gas have mostly eliminated the use of this tube.
FECAL IMPACTION
Fecal impaction means that the rectum and sigmoid colon become filled with hardened fecal material. The most obvious sign of fecal impaction is the absence of (or only a small amount of) bowel movement for more than 3 days in a patient who usually has a bowel movement more frequently. Impaction occurs in patients who are very ill, are on bed rest, or are not fully aware of their surroundings due to a state of confusion. The very young and very old are more prone to fecal impaction.
Nursing care focuses on prevention of fecal impaction by daily assessment of bowel patterns of all patients. Fecal impaction is easier to remove when an oil-retention enema is ordered and given, and then a cleansing enema is given 2 to 3 hours later. Sometimes the physician will order the impaction to be digitally broken up after the oil has had time to soften the stool (Steps 30-1).
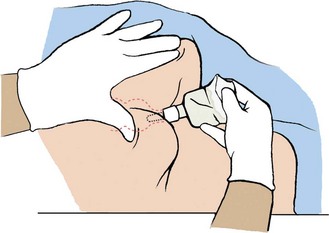
Removal of a fecal impaction digitally must be done gently and the patient watched for signs of vagal response (activation of the vagal nerve) from stimulation of the sphincter and rectal wall (Figure 30-5). The vagal response may cause a slow pulse and cardiac dysrhythmia, and an alteration in blood pressure may develop. Should this occur, immediately stop the procedure, place the patient in a supine position, monitor vital signs, and notify the physician. A dose of atropine may be ordered to counteract the vagal response.
BOWEL TRAINING FOR INCONTINENCE
The treatment for incontinence is training for bowel control. This is a long process, but it helps the patient regain self-esteem. A special effort should be made to help the very elderly patient overcome incontinence.
A bowel training program is based on the principles for establishing regular bowel elimination: adequate diet, sufficient fluids, adequate exercise, and sufficient rest (Box 30-3). A regular time for evacuation should be established. A reasonable goal is to achieve defecation within 1 hour of the established time. Factors that will help establish the time include prior bowel habits of the patient or the nurse’s observation of when incontinent movements tend to occur. Many bowel retraining programs are timed around a triggering meal when gastrocolic reflexes are the strongest.
After a regular time for evacuation has been established, all efforts must be made to provide the patient with an environment that is conducive to evacuation. Privacy and adequate time are only two parts of the environment that are considered. The patient must also feel safe in the environment and know that if a problem occurs, the nurse is available to provide assistance. In anticipation of a successful evacuation, provide the patient with toilet tissue and remember to plan for hand hygiene after the evacuation (Safety Alert 30-4; see also Safety Alert 17-1).
Some patients with a neurogenic dysfunction may require digital stimulation to relax the anal sphincter. Using a gloved and lubricated finger, insert the finger 1 to 2 cm into the rectum and gently rotate the finger for 30 to 60 seconds.
Suppositories, stool softeners, and bulk laxatives may be used to assist in establishing a normal, regular bowel pattern. The type of suppository used will depend on the physician’s order. As a rule, suppositories are inserted about 1 hour before the triggering meal or the established evacuation time. In some bowel retraining programs, a suppository is used every day for the first week, then every other day for the second and third weeks, and thereafter only as needed to maintain a regular movement every 2 to 3 days.
When stool softeners and bulk laxatives are used as part of a bowel training program, remember that a fluid intake of at least 2500 mL per day is required. In most cases, stronger types of laxatives and enemas are not considered part of a bowel training program.
BOWEL OSTOMY
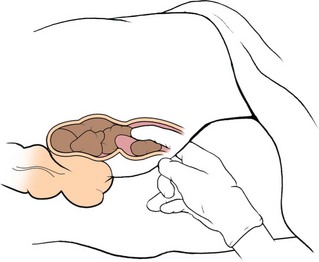
Disease or trauma can damage the intestinal system and require surgical intervention, which alters the process of elimination. A diversion of intestinal contents from the normal path is called an ostomy. An ostomy results in the formation of an external stoma (opening into the intestine), or an internal tissue pouch with a valve nipple opening. The internal pouch forming the continent ostomy is usually constructed from a segment of bowel (Figure 30-6). This type of ostomy is emptied with a catheter (Steps 30-2). Patients with stoma ostomies use various appliances (devices to gather and contain output) and special procedures to aid in effective, controlled elimination through the stoma.
Human elimination is a subject that many adults view with embarrassment or distaste. Physical conditions that create the need for an ostomy carry a heavy psychosocial burden for the patient as well as many new demands in handling elimination. Soiling, wetness, and the presence of odor from feces are all socially unacceptable in adult society, and the possibility of such things is often of grave concern to the new ostomy patient. There is also concern about ability to care for oneself and to return to work and recreation activities performed before surgery. You must keep your body language neutral and not display any sign of distaste when caring for the ostomy patient. An attitude of acceptance is very important.
Conditions that can require ostomy include cancer, abdominal trauma, congenital malformation of the bowel, and severe chronic Crohn’s disease or ulcerative colitis. Patients facing an ostomy frequently experience fear, concern, and denial followed by information seeking. Fear may focus on the loss of a normal body function and change in body image, the possibility of rejection by others, the loss of physical or sexual attractiveness, or the prospect of death from the underlying disease.
The patient may be helped by a visit from a member of the United Ostomy Association, which is a support network of persons with ostomies. The patient needs a support system in place before discharge from the hospital. The local office of the American Cancer Society is a good source of information about ostomy support groups or visitors in the area, as is the United Ostomy Association, which can be reached at (800) 826-0826 or on the Internet at www.uoaa.org.
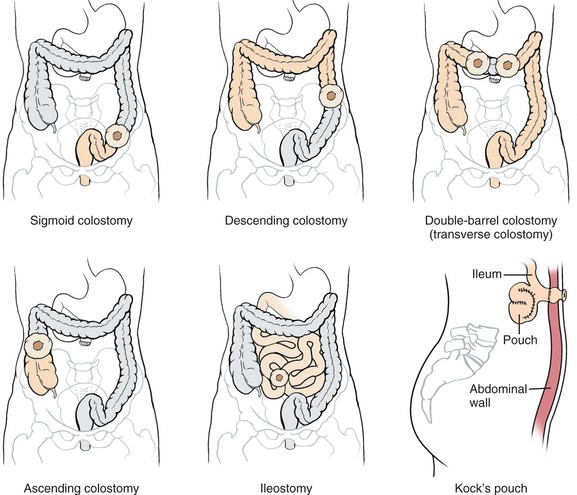
OSTOMY CARE
An ileostomy is an opening surgically created at the ileum to divert intestinal contents. This is done because lower portions of the bowel have been surgically removed. Effluent (fecal matter) from an ileostomy is liquid. A colostomy is an opening into the colon. The stoma is the entrance to the opening. An appliance is the apparatus that attaches to the skin plus a pouch (bag) worn over the stoma to collect effluent (Figure 30-7). Colostomy effluent is more formed. Patient care involves providing skin care around the stoma, applying the appliance, or if there is a continent ileostomy, draining it with a catheter. Diet can adversely affect the ostomy patient and is an important part of teaching (Patient Teaching 30-1). Evaluation of care for the ostomy patient hinges on whether the patient is experiencing problems with the ostomy, the skin around the stoma, or the appliance. Care of the ostomy patient is complex and is covered more thoroughly in a medical-surgical nursing text.

Skin Care
Periostomal (around the stoma) care includes assessment of the health of the stoma and skin surrounding it. The stoma should appear pink or red, which indicates adequate blood supply. It should look like healthy mucous membrane, such as the membrane inside the mouth.
Assess the skin around the stoma for signs of irritation or breakdown. With an ileostomy, enzymes in the effluent can quickly cause excoriation. When changing the faceplate (every 3 to 5 days), the stoma and skin are washed with mild soap and water and patted dry. A skin barrier paste is applied, with care to prevent any of it from getting on the stoma. Skin barriers are commercially available along with other ostomy supplies (Figure 30-8). A karaya ring may be attached to the skin to hold the faceplate in place; it is often part of the faceplate. Karaya is a plant material that becomes gelatinous (soft and sticky) when wet; it helps prevent excoriation.

Applying an Ostomy Appliance
There are many different sizes and types of ostomy appliances. All appliances have a faceplate, or disk, that attaches to the abdomen, and a pouch for collecting effluent. The appliance is positioned with the stoma protruding through the opening in the center of the faceplate. It is essential that the appliance be the correct size for the patient’s stoma. The stoma must be measured so that the right-size appliance can be chosen. The pouch attaches over the stoma and is fastened onto the faceplate. Some patients wear a belt that also supports the pouch so that it is not pulled loose from the faceplate as effluent fills the pouch. A clamp at the bottom of the pouch allows effluent to be drained. Pouches are simply emptied and rinsed as needed and are detached and replaced only every few days. It is best to empty stool from the pouch when it becomes one third to one half full so that the weight of the effluent does not pull the appliance loose (Skill 30-2).
Skill 30-2 Changing an Ostomy Appliance
You will initially change the ostomy appliance, but should take each opportunity to teach the patient this skill. An ostomy pouch is changed when adherence to the skin is no longer adequate or every 2 days if the skin condition is compromised. The type of pouch applied depends on the type of ostomy.
Review and carry out Standard Steps in Appendix 3.
1. ACTION Assess for type of ostomy and location. Assess stoma for color and appearance. Assess size of stoma using stoma measuring device. Assess skin condition around stoma.
RATIONALE Stoma measuring device provides data regarding stoma size for choice of correct appliance. If the stoma is more than 6 months old, a precut appliance of the correct size may be used. Red or dark pink color indicates adequate blood supply. Stoma should not be receding or protruding. Skin breakdown may be caused by stool action on skin, improperly fitting pouch, perspiration, irritation to skin from appliance, allergic reaction, or bacterial or fungal infection.
3. ACTION Measure the stoma with the stoma measuring device. Prepare the skin barrier or pouch with faceplate by cutting an opening in the center approximately  inch (for urostomy) to ¼ inch (for colostomy) larger than the stoma. Smoothing the cut edges with your finger will help prevent irritation or leakage around the stoma.
inch (for urostomy) to ¼ inch (for colostomy) larger than the stoma. Smoothing the cut edges with your finger will help prevent irritation or leakage around the stoma.
RATIONALE Drawing the pattern on the paper side of the plate and cutting out on top of the line will ensure more accurate sizing. The edges of the pouch can injure or irritate the stoma if the opening is too small. Too small an opening may restrict blood flow or prevent correct adherence of the appliance to the skin.
4. ACTION Put on gloves. Empty old pouch.
RATIONALE Prevents transfer of microorganisms. Prevents the weight of the pouch contents from loosening the pouch and spilling.
5. ACTION Remove old pouch by stabilizing the skin with one hand and pulling the backing from the skin with the other hand; discard the old pouch in the plastic bag. Save the tail closure clip.
RATIONALE Readies the area for new pouch application.
6. ACTION Clean the stoma and skin gently with warm water and soft cloth. Dry the skin well by patting. Place tissue or piece of tampon at stoma opening to prevent leakage.
RATIONALE Cleaning and drying prepares skin for attachment of new appliance. Tissue or tampon will absorb any leakage.
7. ACTION Change gloves. Remove paper from skin barrier on back of appliance. Apply skin barrier paste to periostomal area. Wet fingers, and spread paste around the stoma, but not on it.
RATIONALE Reduces transfer of microorganisms. Prepares an adhesive surface on the skin for attachment of pouch appliance.
8. ACTION Center and carefully apply the pouch appliance while having patient push out the abdomen.
RATIONALE This prevents skin wrinkles from occurring while pouch is pressed into place.
9. ACTION Gently press down the skin barrier ring around the stoma while abdomen is pushed out by patient. Check that seal is wrinkle free.

RATIONALE Adheres appliance to skin without causing wrinkles. Good adherence prevents leakage.
10. ACTION Reinforce ring with tape as needed.
RATIONALE Balances weight of pouch and prevents edges from loosening during showering.
11. ACTION Instruct patient to lie quietly or sit still for 5 minutes to allow body heat to seal pouch well.
RATIONALE Body heat activates the skin barrier and causes it to adhere to the skin.
12. ACTION Place deodorant inside pouch if patient desires.
RATIONALE Various types of ostomy deodorants are available commercially.
13. ACTION Attach and secure pouch tail closure so that bow of clip fits curve of abdomen. Allow a 1-inch fold-over of pouch before closing the clip.
RATIONALE Closes pouch; when bow fits curve of abdomen, clip is less noticeable through clothing.
14. ACTION Attach belt to faceplate of pouch if belt is to be worn.
RATIONALE If stoma is flush to the skin, a belt may be needed to prevent leakage from the pouch.
15. ACTION Remove gloves and perform hand hygiene.
RATIONALE Reduces transfer of microorganisms.
16. ACTION Assist patient to replace gown or clothing and position for comfort. Restore the area.
 Patient is draped during procedure to prevent chilling.
Patient is draped during procedure to prevent chilling.
Old pouch must be disposed of as hazardous waste. Plastic discard bag should be closed securely before discarding.
Some pouches can be washed and reused. Rinse with tepid water, wash with warm soap and water, rinse with vinegar solution (1 part water, 7 parts vinegar), and allow to dry.
Irrigating a Colostomy
To irrigate a colostomy, a solution is instilled into the colon via the stoma; it is similar to giving an enema (Steps 30-3).
NCLEX-PN® EXAMINATION–STYLE REVIEW QUESTIONS
Choose the best answer(s) for each question.
1. Based on an understanding of normal physiology, the nurse knows that functions of the large intestine are to: (Select all that apply.)
2. The nurse is doing preprocedural teaching with a patient who is scheduled to have a barium enema. Which of the following statements by the patient indicates a need for additional teaching?
1. “I will have to increase my fluid intake after the procedure.”
2. “The barium increases my risk for diarrhea.”
3. A nurse is preparing to give a patient an enema. The patient should be placed in the left Sims’ position because:
1. it is the most comfortable position.
2. bringing the knee to the abdomen straightens the colon.
4. If the solution for an enema is too cool,
1. the solution runs in too slowly.
2. cramping and discomfort may occur.
5. Which abnormal stool characteristics is the cause for the greatest immediate concern?
6. Which statement by the patient indicates an understanding of the information that was taught for self-care related to diarrhea?
1. “I should consume clear liquids for 2 days and then try applesauce.”
2. “I should increase my consumption of fruits and vegetables.”
3. “I should eat small, frequent meals that include high-quality proteins.”
4. “I should try over-the-counter antidiarrheals for at least 3 days.”
7. The nurse is attempting to manually remove a fecal impaction. What is the most serious complication that can occur during the procedure?
1. Vagal response causes severe pain in the rectal area.
2. Vagal response causes semiliquid stool and cramping.
3. Vagal response predisposes to future episodes of reimpaction.
4. Vagal response causes slow pulse and cardiac dysrhythmias.
8. The nursing student is reviewing the procedure for how to administer a cleansing enema solution. Which statement by the student indicates a correct understanding of the procedure?
1. “The amount of solution for an adult, is between 1000 and 1500 mL.”
2. “The enema tube should be inserted about 6 to 10 inches into the anus.”
3. “The temperature of the solution should be between 110° and 120° F.”
4. “If the physician orders enemas until clear,’ three is the maximum.”
9. The nurse is changing the stoma appliance for a patient who has an existing colostomy. Below are the steps for the procedure. Place these steps (1 though 7) in the correct order.
_______1. Center and carefully apply the pouch appliance.
_______2. Remove old pouch by stabilizing the skin with one hand.
_______3. Instruct patient to lie quietly or sit still for 5 minutes.
_______4. Apply skin barrier paste to periostomal area.
_______5. Clean the stoma and skin gently with warm water and soft cloth.
_______6. Gently press down the skin barrier ring around the stoma.
10. An elderly patient living in an extended care facility has a nursing diagnosis of Bowel incontinence related to confusion. Which intervention would be the best for this patient?
CRITICAL THINKING ACTIVITIES ? Read each clinical scenario and discuss the questions with your classmates.
Lana Jakubowsky had a stroke and has been incontinent of feces. Her condition is improving and she is regaining muscle tone in her left arm and leg.
Scenario B
Von Troung, age 78, has had the flu and diarrhea for 3 days. He is confused, and the skin around his anus is very inflamed.