Administering Oral, Topical, and Inhalant Medications
Upon completing this chapter, you should be able to:
1 Describe the legal and professional responsibilities of the LPN/LVN related to medication administration.
2 List the different classifications of drugs based on their specific actions.
3 Identify the parts of a valid medication order.
4 Compare and contrast various medication record systems such as the medication administration record (MAR), medication cards, and computerized systems.
5 Discuss medication dispensing and delivery systems.
6 Discuss the advantages and disadvantages of the unit-dose system and the prescription system.
7 Consider special needs when administering oral and topical medications to an elderly patient.
8 Identify four principles to be followed when giving a medication through a feeding tube.
9 Discuss your responsibilities in the event of a medication error.
1 Demonstrate the accounting of doses of controlled drugs that must be withdrawn from the locked narcotics cabinet or dispensed from an automatic dispensing unit.
2 Give oral and topical medications using the Five Rights and five rules.
3 Prepare and apply topical medications such as eye ointments, eardrops, nasal medications, transdermal patches, and topical ointments.
4 Teach a patient to use a metered-dose inhaler.
5 Instill a vaginal and a rectal suppository safely and effectively.
6 Write a care plan for a patient who is receiving medication to include patient specific data, an identified nursing diagnosis, and interventions that you used.
7 Document medication administration and your patient’s response to the therapy.
 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  ,
, NURSING RESPONSIBILITIES IN MEDICATION ADMINISTRATION
Accuracy during all steps of medication administration is extremely important. Medications are chemicals that alter actions performed by cells of the body. If the wrong medication is given to a patient, it could have serious consequences. All procedures related to medication administration should be followed exactly to promote safety and avoid making a medication error. However, should an error be made, report it promptly in accordance with agency policy and take appropriate action to promote patient safety and well-being.
To administer medications, you must be able to interpret the medication order correctly and then give the correct medication to the patient. The procedures for administering medications accurately using the various routes can be mastered with practice. Attentiveness to each step of the task is essential when administering medications. Nurses are legally responsible for being knowledgeable about each medication they administer to patients: the correct dose, the route by which it should be given, desired effects, side effects, interactions with other medications, and any contraindications. Medication orders that are unclear, incomplete, or ambiguous should be questioned to avoid errors. Assessment of the patient after medication has been administered provides data for evaluating the effectiveness of the drug and guiding health teaching. On discharge from the health care facility, patients need to know how often to take each drug, if the medication should be taken before or after meals, if certain foods or fluids should be avoided, the expected effect, what to do about side effects if they occur, and what to do if they forget to take a dose at the prescribed time. In accordance with 2009 National Patient Safety Goals, involving and educating patients and families in care and treatment is a safety measure.
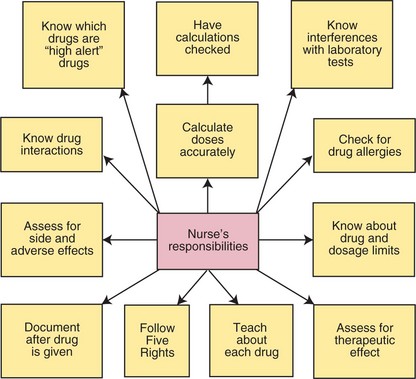
The Five Rights of medication administration provide a framework for safe delivery of drugs to patients (see Chapter 33). Box 34-1 presents pertinent National Patient Safety Goals of The Joint Commission as they relate to medication administration. Practice in the clinical setting helps establish a consistent, efficient routine for giving drugs. Concept Map 34-1 depicts the nurse’s responsibilities when administering medications.
CLASSIFICATION OF DRUGS
As mentioned in Chapter 33, drugs are classified in various ways. It is an advantage to learn drugs by the class to which they belong. To learn the possible side effects of each medication, begin by learning drugs by classification and then learn the most common side effects of the classification to which the drug belongs. Drugs are classified in various ways; one of the most useful is based on the effect of the drug on the body (Table 34-1). In this system, drugs that reduce pain and discomfort are classified as analgesics; those that control severe pain are potent analgesics or opioid narcotics, which may produce a stuporous state as a result of their effect on the central nervous system. For a complete list of drug classifications, consult a drug handbook or pharmacology textbook. The classification index in the Physicians’ Desk Reference also serves as a convenient reference.
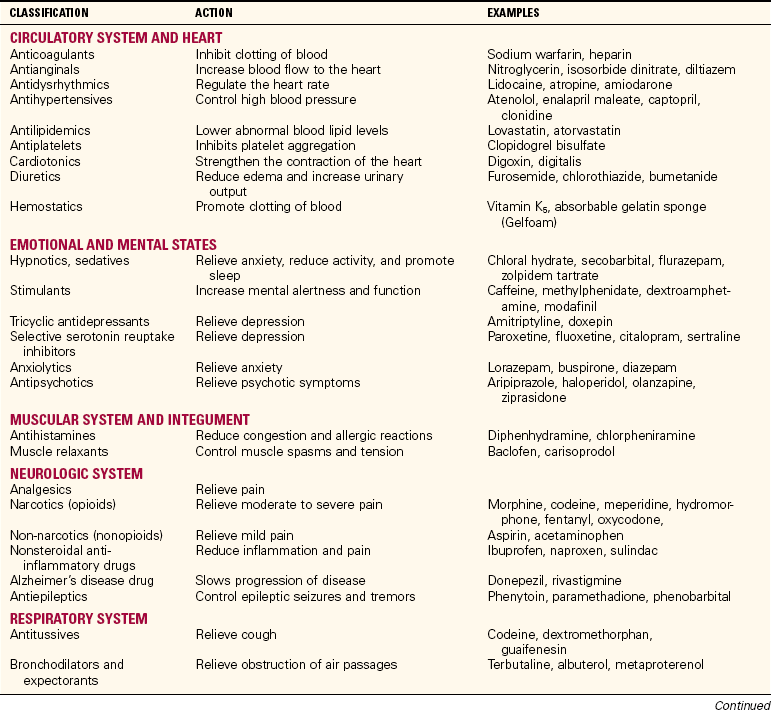
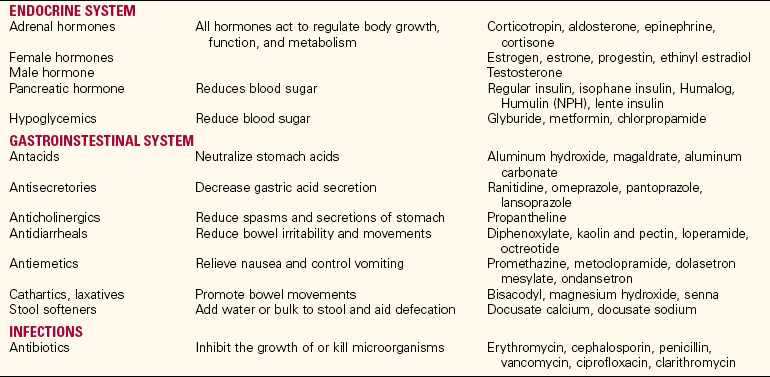
Although there may be subdivisions within a class of drugs, the major side effects within that class will be the same. By learning the side effects of one major drug in the class, you will know what the major side effects of other similarly acting drugs in the class will be. This prevents the necessity of memorizing a multitude of separate facts about drug side effects. Different classifications and some examples of medications within each group are shown in Table 34-1.
MEDICATION ORDERS
The physician prescribes the type of treatment in a series of instructions written on the physician’s order sheet of the hospital chart. The written prescription for a drug is called the medication order or the drug order. Physicians’ orders are part of the patient record.
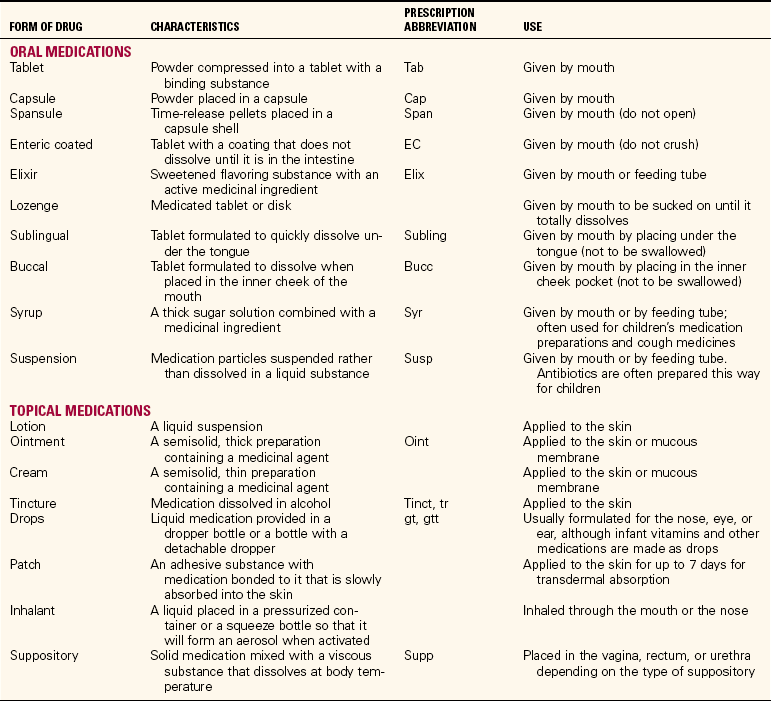
Medication orders must meet certain standards specified by state law and by regulations established by inspecting agencies. A complete drug order must include the full name of the patient, the name of the drug, the dosage to be given, the route of administration, how often it is to be given, the date and time written, and the signature of the prescriber. Some orders also specify the total number of doses that are to be given. Examples of medication orders are given in Table 34-2. Oral and topical medications come in many different forms (Table 34-3).
Table 34-2
| ORDER | MEANING |
| Digoxin 0.25 mg PO daily | Digoxin (a drug that strengthens the heart) in a dose of 0.25 mg to be given orally every day |
| Methylprednisolone 4 mg PO qid | Methylprednisolone (a type of cortisone) in a dose of 4 mg to be given orally four times a day |
| Maalox 30 mL PO q2h when awake | Maalox (an antacid) in a dose of 30 mL to be given orally every 2 hours during waking hours |
DOSAGE OF MEDICATIONS
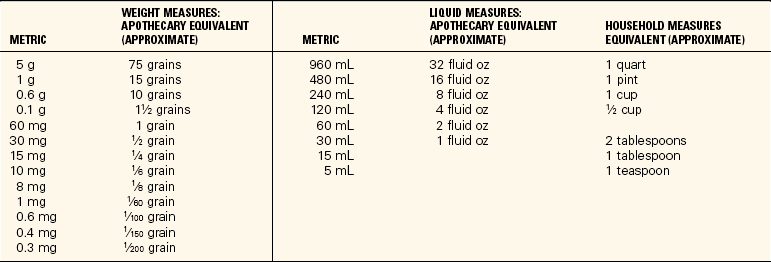
In Canada, the metric system is the only system of weight and measurement; although it is the primary system of measuring medication dosage in the United States, the apothecary system is still occasionally used. The apothecary system was brought to America from England during colonial times. You must be familiar with this system because it has not been fully phased out as yet. Although use of the metric system is the standard, you still need to be able to convert values from one system to the other. It is helpful to keep a table of conversion values in the area where medications are prepared to ensure accurate calculations (Table 34-4).
Each dose of medication should be taken from a labeled package or container clearly stating the name and dosage of the drug. There is widespread use of medications supplied as unit doses, with each dose packaged separately with its own label.
Checking any conversions and calculations for a divided dose with another colleague is recommended at all times as a medication safety measure. Consult pediatric textbooks for additional information about how to confirm dosages and to prepare divided doses of medications for infants and children.
ROUTES OF MEDICATION ADMINISTRATION
The selected route of administration depends on several factors: the condition of the patient, the nature of the drug (taste, stability, and so on), and the rate of absorption via one route versus another. The oral route (PO, or per os, which means “by mouth”) is used for many solid and liquid medications because it is the simplest, most convenient, and least expensive (see Table 34-3). Those patients who have difficulty swallowing pills must have them crushed and given mixed in some food or juice. Some pills cannot be crushed because this changes their effect on the body. In this case, ask the physician to order the medication in liquid form.
Topical medications are instilled in the form of eyedrops or eardrops, or applied as ointments, pastes, or lotions to the skin or mucous membrane. The rectal route is often used to give medications to children or for patients who are vomiting. (Skills detailing the procedures for giving solutions as enemas can be reviewed in Chapter 30.) A number of medications affecting the respiratory system are given as inhalants. Parenteral routes are used for injecting medications into the body tissues, commonly via subcutaneous, intramuscular, intravenous, percutaneous, and intradermal routes. These are described in detail in Chapters 35 and 36.
REGULARLY SCHEDULED MEDICATION ORDERS
To maintain the desired level of medication in the bloodstream, the drug may be given several times a day. The physician’s order will specify how often the medication is to be given, such as three times a day (tid), every 4 hours (q4h), and so forth.
Each health care agency has policies that designate the time of day corresponding to the frequency ordered by the physician. It is imperative that the agency policy be followed. For example, on some nursing units the schedule of times might be as follows:
| Order | Schedule |
| daily | 0900 |
| bid | 0900 and 1700 |
| tid | 0900, 1300, and 1700 |
| qid | 0900, 1300, 1700, and 2100 |
| q4h | 0100, 0500, 0900, 1300 (and so on) |
PRN MEDICATION ORDERS
Medications taken “as needed” (PRN or prn) are given in response to a patient’s request or when the need is indicated. Examples of these medications usually include analgesics (to control pain), tranquilizers or sedatives (for restlessness), and laxatives (for constipation). Some PRN medication orders specify when or how often the medication can be given (e.g., at bedtime PRN, meaning “at bedtime as needed” and q 4 hr PRN, meaning “as often as every 4 hours as needed”). Table 34-5 shows two examples of PRN orders.
STAT AND SINGLE-DOSE MEDICATION ORDERS
Numerous occasions arise when a stat medication or a single dose of a drug must be given. The stat (give immediately) or single-time order may consist of more than one drug, or it may involve spacing the drops or tablets over a short period of time, such as when giving radiopaque tablets in preparation for a gallbladder series or eyedrops to dilate the pupils for refraction. Preoperative medications are prime examples of drugs given one time. Stat orders indicate that the order has top priority and the medication must be administered without delay. In emergencies, many orders are on a stat basis. The following are examples of stat and single-dose orders:
RENEWAL ORDERS
Drugs are potent and are capable of causing adverse reactions as well as the desired effects. Many drugs can result in drug addiction or drug dependency. Therefore, many hospitals have medication policies limiting the time for which certain types of medication orders are valid. Opiate analgesics generally have a 48- or 72-hour limit, sedatives and antibiotics may have a 5- or 7-day limit, and a 30-day limit may be imposed by some agencies on all medications. At the end of the specified period, the order is no longer considered valid, and no additional doses of the drug may be given. If you think the medication will need to be continued, phone the physician and obtain a new order rather than just holding the drug. The physician must give or write a renewal order to continue the medication.
STOP OR DISCONTINUE ORDERS
Medications are given to the patient until the specified number of doses has been administered or until the order has expired or has been canceled. Usually a change in medication is ordered by the physician, who writes a stop or discontinue order for one drug and then prescribes a new one. Examples of stop orders are “stop gentamicin” or “discontinue probenecid.” All medication orders are automatically canceled whenever a patient undergoes surgery or general anesthesia. New orders must be rewritten after surgery, even for routine medications.
MEDICATION RECORDS
After the physician writes a medication order on the patient’s chart, it is transcribed onto the medication administration record (MAR). Medication orders are usually transcribed onto the patient’s MAR, on the computer-generated care plan, and/or on medication cards (Figure 34-1). Sometimes medications are listed on the patient’s Kardex card also.
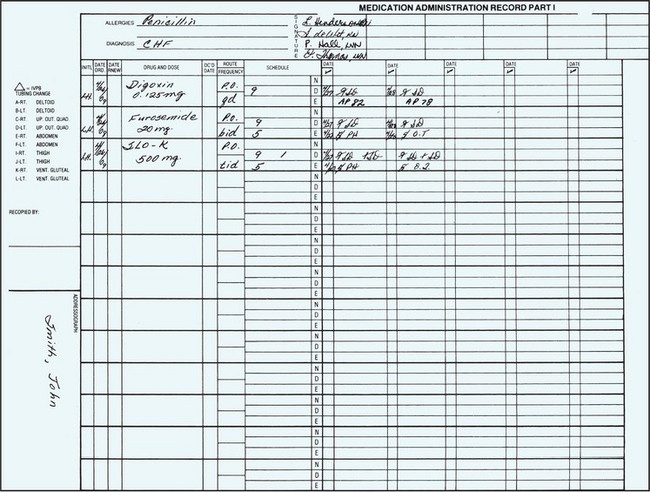
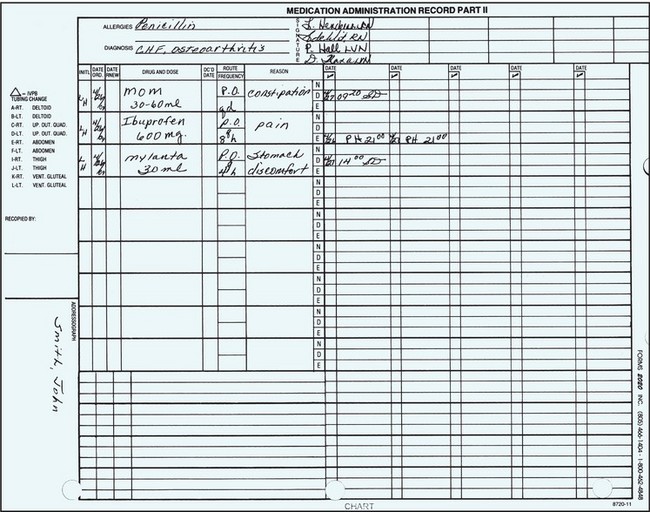
MEDICATION ADMINISTRATION RECORD (MAR)
One of the forms commonly used to record a patient’s medications is the MAR, on which nurses record the doses of drugs administered each day. A copy of the MAR is placed on the patient’s chart. For added convenience, the forms may be in binders or in a special Kardex kept in the medication area and referred to when giving regularly scheduled and PRN medications.
MEDICATION CARDS
Medication cards are rarely used now, but may be encountered in small long-term care facilities or rehabilitation centers. For each patient, one card is made for each medication ordered. The card is used when the dose is prepared, at the bedside to help identify what is being given, and to chart after the medication is given. Information on the card includes patient’s name; room number; physician’s name; name of drug; dose, route, and time of administration; the date the order was written; and the initials of the person making the card.
MEDICATION ADMINISTRATION AND TECHNOLOGY
There is a rapid increase in the use of technology, such as computerized physician order entry (CPOE) systems, bar code scanners, and personal digital assistants (PDAs), to improve medication administration safety. In the CPOE system, the prescriber directly enters the medication order in the computer; this decreases potential for transcription errors. Other features of the CPOE system include alerts about drug interactions, nursing implications for administration, and updates on new drug information. CPOE also has the potential to incorporate patient-specific information such as allergies, laboratory results, or vital signs. Bar code scanners are used to scan the medication package and the patient ID bands. When scanning is combined with a patient-specific profile, an electronic cross-check of the five rights is ensured. PDAs are not currently widely used; however, in the future there is a potential for each nurse to download and upload specific patient information to a PDA that is connected to the larger hospital information system.
MEDICATION ADMINISTRATION SYSTEMS
There are three types of medication administration systems: the stock supply of medicines, the individual prescription system, and the unit-dose method. The unit-dose system is the most commonly used medication administration system in health care agencies. The advantages of the unit-dose system and the individual prescription system have made the stock supply system less popular. The unit-dose system can be modified in various ways and can be operated from a stationary (fixed) or a mobile center where the medications are prepared.
The fixed site is generally a small medication room, a medication drawer in the patient’s room, or a station set aside for this purpose. MARs or medication cards and trays are commonly used as part of the medication procedure. The mobile method requires a cart that can be pushed from room to room as the medications are prepared and administered.
UNIT-DOSE SYSTEM
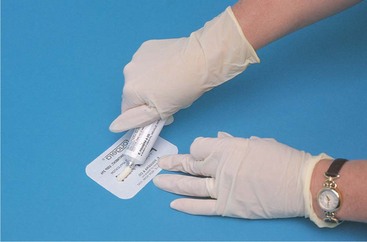
The unit-dose system provides a premeasured, prepackaged, and prelabeled dose of a medication for the patient (Figure 34-2). Almost all oral medications, liquids, suppositories, and lotions are now available in unit doses and in prefilled cartridges or syringes for injection. This system is considered safest because the dose prescribed is the dose dispensed. Medications dispensed using the unit-dose system may be administered from a mobile cart or from the fixed medication preparation center. The medication is opened at the bedside. It is customary to keep medication records in a binder or Kardex file on top of the cart from which medications are administered.

The unit-dose system provides a number of benefits. The pharmacy supplies the exact dose of medication ordered, and each dose is administered at the bedside, enhancing patient safety and reducing medication errors. The system also saves time for the nurse. Another benefit is that the patient is charged only for medications that are used. Finally, this system allows keeping a minimum amount of drugs on the nursing units.
PRESCRIPTION SYSTEM
The prescription system is similar to the unit-dose system except that a sufficient number of doses for several days are supplied. This system is used in pharmacies in the community and in outpatient clinics. As the name implies, a prescription is written for each drug ordered and is filled by the pharmacist, who then provides individual containers holding doses for several days.
The prescription system can be used in connection with a fixed or a mobile preparation site. Its advantages include the fact that only a limited amount of drugs needs to be kept on the nursing units. In the long-term care facility, a week’s or month’s supply of each medication is often provided in a bubble pack. Each day’s dose is pushed out of a bubble on the pack as needed. Home care patients use prescription system–prepared drugs from the local pharmacy or by-mail pharmacies.
PREPARATION OF ORAL CONTROLLED SUBSTANCES FROM A DISPENSER
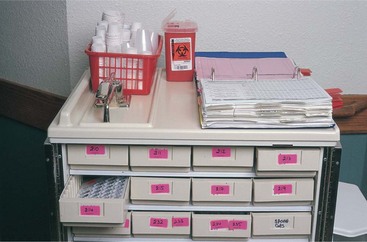
A controlled dispensing system is used for distributing opiate analgesics and hypnotics (Figure 34-3). Legally controlled substances must be under lock and key at all times. Automated controlled-substance dispensing machines are often used in the clinical setting to monitor and control narcotic use (Figure 34-4). A significant advantage of this type of system is that a code number is used to enter the system. This eliminates the problem of having to find the nurse who has the keys to the locked cabinet and increases efficiency. Each nurse has a password by which to gain entry to the system.

When not in a dispensing machine, the drugs are supplied in a controlled dispenser or a commercially prepared package. Most medications are supplied in small pull-strip boxes with a roll of numbered doses of a particular medication. These often have 25 tablets or capsules per box. The first pill to be dispensed is numbered “25,” so that there is an accurate count of the remaining pills in the box. Tablets or capsules may be prepared in plastic sectioned containers, usually with 25 compartments clearly marked on top of the container as number 25, 24, 23, and so forth. The top surface of the container is movable, so that when the small opening in the cover is centered over one of the compartments, the container can be inverted over the medicine cup and the tablet or capsule falls into the cup without being handled. Each dose given must be accounted for and the number remaining verified at the time each shift counts the controlled substances before handing over the keys to the compartment to the next shift. One nurse from the oncoming shift and one nurse from the shift going off duty do the count together. Any discrepancy must be resolved before the nurses on the ending shift leave the unit.
As soon as the medicine has been dispensed, verify the label on the dispenser with the patient’s medication record. Replace the dispenser. Record the medication on the proof-of-use form and administer the drug to the patient. At the end of the shift, the remaining controlled drugs are counted, or a computerized count is obtained from the dispensing machine.
TOPICAL DRUGS
Topical drugs are applied externally to the skin and the mucous membranes; they may also have a systemic effect. Drug solutions instilled in the eye, ear, and nose are topical and act locally on these tissues. Other common forms of topical drugs include ointments, creams, pastes, liniments, and lotions that are used to treat local conditions. Drops and ointments for the eye must be sterile and nonirritating to the tissues. Solutions to be instilled in the eye, ear, or nose are generally prepared in dropper bottles.
Ointments are medicines manufactured in an oily base, such as petrolatum or lanolin, which keeps the drug in prolonged contact with the skin surface to obtain a soothing and anti-inflammatory effect. To protect against local infections, many contain antibiotics. Pastes are stiffer in consistency than ointments and do not melt at body temperature. Aluminum paste and zinc oxide are examples of pastes that are used to absorb secretions and protect the skin. Lotions and liniments are topical drugs in liquid form, such as calamine lotion, which are used to cool, soothe, and reduce inflammation or itching of the skin. Lotions are patted on gently, whereas liniments are rubbed into the skin. Liniments provide temporary relief of pain or soothing warmth by their action, which dilates the superficial blood vessels.
Suppositories are small cylinder-shaped, semisolid substances that are inserted into body orifices, such as the rectum, vagina, urethra, or ostomy stoma. Suppositories contain medication that is absorbed through mucous membranes.
Medications can also be dissolved in solutions and applied topically in the form of irrigations. Vaginal irrigations are the most common type of medicinal irrigation. Irrigations are presented in Chapter 38.
APPLICATION of the NURSING PROCESS
First check the order for each medication, noting the patient’s name, drug name, dosage, route, time, and the date the order was written to be certain it is still valid. Check the patient record for allergies. Determine why the patient is receiving the drug. If previous doses have been given, assess for therapeutic effect (the drug is working as intended). Assess for interactions among the drugs the patient is receiving. Check lab values and determine if there is any contraindication to taking the drug.
Assess what the patient knows about each medication and define learning needs. Assess for side effects to the drug if previous doses have been given. Decide whether the route in which the drug is ordered will be effective for the patient. For example, if the patient is nauseated, an oral dose may not be retained. Assess for drugs that must be given with food or on an empty stomach so that timing of the dose will be appropriate. When topical medications are to be applied, assess for adverse effects such as inflammation, swelling, redness, or discharge.
Nursing Diagnosis
Look at the classification of each medication and determine how nursing diagnoses are related to each prescribed medication. A hospitalized patient has acute problems, but other chronic problems may also be present for which the patient is receiving medication. These chronic problems need to be addressed with nursing diagnoses on the care plan. For example, a patient who had a colon resection may also be diabetic and hypertensive. Patient care is often very complex. By looking at the medications patients are receiving that are unrelated to the primary condition for which they are hospitalized, chronic conditions can be uncovered and addressed. For example, if the patient is in the hospital for a hip replacement and the major nursing diagnosis on the care plan is Impaired physical mobility related to hip replacement, but the medication administration record includes digoxin (Lanoxin) as a scheduled medication, then the patient may also have the nursing diagnosis of Decreased cardiac output. Digoxin is given to increase contractility of the heart. A few examples of nursing diagnoses for which medications are part of the treatment plan include the following:
• Ineffective tissue perfusion related to increased blood pressure (antihypertensives)
• Ineffective tissue perfusion related to cardiac arrhythmia (antiarrhythmics)
• Impaired tissue integrity related to wound infection (antibiotics)
• Imbalanced nutrition: less than body requirements related to nausea (antiemetics)
• Deficient knowledge related to action or side effects of prescribed medications
Planning
Plan and incorporate times for medication administration into the daily shift work schedule. A grid on the daily worksheet for assigned patients and the times of their medications is very useful. Plan to take juice or crackers to the room when a patient’s medication is scheduled between meals and needs to be taken with food. If a patient has difficulty swallowing, plan time to sit the patient upright and coach in the swallowing process. Plan to assess for side effects of the medication before giving the next scheduled dose. The overall goals of medication administration are as follows:
• All medications ordered will be safely administered to each patient on time.
• Serious side effects of medication will be identified quickly.
• The medication will be effective.
• No allergic reaction to the medication will occur.
• The patient will understand why the drug is prescribed, adhere to the medication schedule, and report serious side effects.
Expected outcomes for the previous nursing diagnoses might be:
• Pain will be relieved for 3 hours after administration of analgesic.
• Blood pressure is controlled within normal limits by antihypertensive medication within 1 week.
• Heart rate is regular and without signs of atrial fibrillation while taking antiarrhythmic medication.
• Wound culture will be negative at the end of antibiotic therapy.
• Patient will eat a meal without nausea with antiemetic 30 minutes prior to the meal.
• Patient will verbalize the reason for the medication and the side effects that might occur before discharge.
Implementation
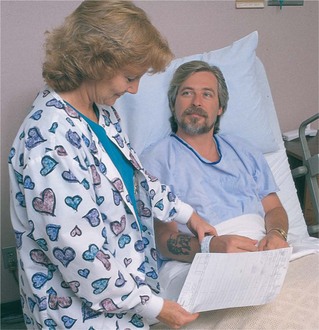
When preparing any medication, remember to check the label three times and to follow the five rights of medication administration. Always check for patient allergy to the medication before giving it, and document after administering the drug. Patient teaching is an integral part of medication administration (Communication Cues 34-1 and Nursing Care Plan 34-1).
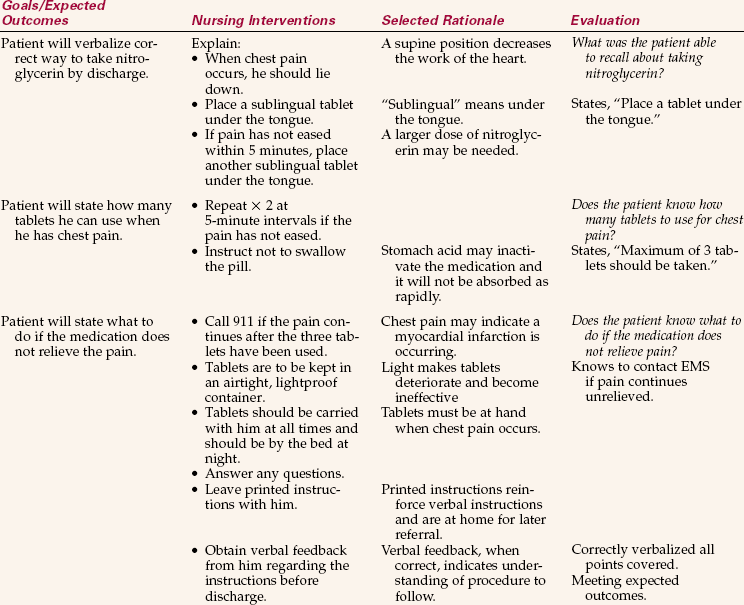
NURSING CARE PLAN 34-1
Care of the Patient Discharged with a New Medication
Phillip Hertog suffered a myocardial infarction and is being discharged home tomorrow. He has nitroglycerin ordered and has never used this medication and doesn’t “understand the directions.”
Never used medication, doesn’t understand/Deficient knowledge related to prescription for nitroglycerin sublingual tablets.
Supporting Assessment Data: Subjective: States has never used nitroglycerin and does not “understand the directions.” Objective: Has an anxious expression and is picking at the bedcovers.
Oral Medication
Oral drugs may be supplied as a tablet, capsule, spansule (time-released pellets put into a capsule), lozenge, or as a liquid in the form of a syrup, elixir, or suspension (Cultural Cues 34-1). When giving a drug in tablet or capsule form, be sure to offer sufficient water with which to swallow the medication. Some people want to take all their pills at once; others will want to take them one at a time. Remember: Any water that is used must be entered on the intake sheet if the patient is on intake and output recording (Skill 34-1). It is important to assess for side effects of the drug before giving another dose of the medication.
Skills 34-1 Administering Oral Medications
The unit-dose system of medication administration is the most commonly used system in health care facilities today. Each medication is usually packaged in a single-dose package. These packages are either commercially prepared or prepared in the facility pharmacy. Most nursing units have at least one unit-dose cart containing drawers in which each patient’s medications are stored. However, some hospitals have started installing an individual patient medication drawer in the patient’s room. Ideally, the cart is taken to each room and the medications are distributed to the patients. Medications may also be in a central location, such as the medication room. In this situation, the nurse must carry the MAR to the bedside to properly identify the patient when giving medications. Patients are identified by at least two identifiers. The keys to successful implementation of any system are following the principles of medication administration and the consistent use of the MAR when checking and giving medications.

1. ACTION Verify that the medication record has been compared with the physician’s orders within the past 24 hours. Check each patient’s allergies.
RATIONALE Mistakes are sometimes made when transcribing orders onto the MAR. Checking on allergies ensures that no patient is given a medication containing an ingredient to which the patient is allergic.
2. ACTION Determine that MARs are present at the cart for all patients to receive medications.
RATIONALE Sometimes the unit secretary has a MAR for order changes.
3. ACTION Assess for side effects of previously given doses of the drug(s). Question the patient or assess the area where a topical medication was applied and is to be given.
4. ACTION Assess supplies on cart and restock as necessary.
RATIONALE Drinking cups, disposable gloves, and medication cups for liquid medication are needed.
5. ACTION Determine which patients are NPO (including those who are scheduled to have dialysis) and which are off the floor for procedures or surgery.
RATIONALE Patients who are NPO must not receive oral medications, although sometimes a medication will be ordered preoperatively to be taken with one sip of water. (Some medications, such as antihypertensives, are held before dialysis.) Knowing which patients are off the unit helps plan medication administration time.
6. ACTION Calculate any doses that are not individual unit doses.
RATIONALE Ensures that the correct amount of drug will be administered as ordered.
7. ACTION Perform hand hygiene.
RATIONALE Medications must be administered using aseptic technique.
8. ACTION Take the medication cart to the patient’s room.
RATIONALE Unit-dose medications are administered to one patient at a time, with the cart at the door of the room.
9. ACTION Verify that the patient is present to receive medications.
RATIONALE The patient may be in the shower, undergoing a respiratory treatment, or severely nauseated, which could prevent or delay the taking of oral medications.
10. ACTION Remove the patient drawer containing the medications, and place it on the work space on top of the cart. Position the MAR sheet beside the drawer. Perform the first check of each medication due at this hour by removing the medication from the drawer and checking the package label with the MAR order. Note the following:
Place the package beside the information on the MAR and proceed to the next medication ordered for this time. Review signs and symptoms of adverse effects for which you must assess; look up any medication with which you are unfamiliar.

RATIONALE This completes the first check in following four of the Five Rights of medication administration. Legally you must know the action, normal dosage, adverse effects, interactions, and nursing implications for every drug you give.
11. ACTION Return the drawer to its place in the cart, and then carefully check each medication a second time with the MAR, checking the following:
Place each package into the medicine cup, unopened, as the second check is finished.
RATIONALE This completes the second check of medication using the Five Rights. Counting the number of medications on the MAR to be given at the designated time (e.g., 0900) and then counting the medications you have out can prevent overlooking a dose. All MAR sheets must be checked; some patients have orders continued on a second and even a third sheet. Unit-dose packages are not to be opened until after the third medicine check, when you are with the patient.
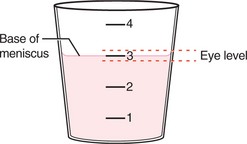
12. ACTION Pour the liquid medication dose into a medication cup unless it is in a dose-measured cup already; carefully check the dosage amount. Do not pour over the MAR sheet because a spill may occur. To pour a liquid medication from a multidose bottle, read the dosage from the bottom of the meniscus, the lowest point. When liquid medications are supplied in a premeasured cup, remove the lid carefully at the bedside so as not to spill the contents. If a multidose bottle is supplied, measure the dose accurately.

RATIONALE A spill on the MAR sheet will require that the sheet be recopied.
13. ACTION Take the medications and the MAR sheet in to the patient. Identify the patient by comparing the information on the armband with the information imprinted on the MAR, and by asking the patient to state his or her name; explain the procedure, thereby completing the Five Rights check.
RATIONALE Comparison of the patient’s full name and hospital number is the most fail-safe method of identification. Asking the patient to state her name provides the second required identification check. The patient should be told why you need to check the identification band.
14. ACTION Check each medication for the third time as you prepare to open it to give to the patient. Tell the patient what the medication is (i.e., “your heart medication”). Check the following:
If the patient does not recognize the medication or indicates that no “heart medication” has ever been taken, stop and recheck the original order. If there is no question, open the medication and place it in the medicine cup.
RATIONALE When the drug is kept in its wrapper until it has been checked the third time and verified with the patient, it can be returned to the drawer if the patient refuses it or if it is not the correct medication. The third check of the medicine provides an added safety check for following the five rights of medication administration. Many medication errors are made because the date and time were not also checked along with the drug name and dosage. Even though drugs are dispensed in unit-dose packages, more than one package or part of a tablet may be required for the ordered dose.
15. ACTION Pour water for the patient to use to take the pills; perform any assessment necessary before the patient takes the medication (e.g., take an apical pulse rate before administering digitalis preparations, assess the blood pressure before giving an antihypertensive medication; record the data). Assess for adverse effects from previous doses of the medications you are about to give. Assess to see if any PRN medications are needed at this time.
RATIONALE Liquid is necessary for the swallowing of pills. The heart rate and rhythm must be known before digitalis is administered; certain antihypertensive medications are withheld if the blood pressure is below a specified level. You must assess for adverse effects of a drug before giving another dose. Giving PRN medications while in the room saves time.
16. ACTION Give the medications to the patient with water or other acceptable liquid. Adhere to fluid-restriction requirements for patients whose intake of fluid is restricted.
RATIONALE Some medications cannot be taken with particular foods. Patients whose intake of fluid is restricted must space their fluid intake over 24 hours and are not allowed unlimited fluid for taking medications.
17. ACTION Observe the patient take the medications, and for those patients who have difficulty swallowing, put on a glove and check the inside of the mouth to see that the pills were actually swallowed. For patients who have difficulty in swallowing, placing the pill as far back on the tongue as possible before taking a sip of water helps.
RATIONALE Sometimes pills fall onto the bed or floor when the patient places the medicine cup or hand to the mouth with the pills. A pill may remain in the mouth for the patient who has difficulty swallowing. Medication may not work correctly unless it reaches the stomach.
18. ACTION Initial the doses given and sign your name on the MAR according to agency policy. If the medicine is not given, circle the time of the dose and follow agency policy regarding further charting.
RATIONALE Documentation of an administered dose is done after the patient has taken the medication. The MAR may need to be flagged so that a dose not given may be given at a later time when the patient returns to the floor or is no longer restricted to taking nothing by mouth.
19. ACTION Proceed to prepare and administer medications to the next patient.
RATIONALE Each patient should receive medications within 30 minutes of the time scheduled.
20. ACTION Return the unit-dose cart and supplies to the central area.
RATIONALE Returning the cart makes it available for the delivery of medications by the pharmacy or for use by another nurse.
21. ACTION For each medication given, ask yourself whether the patient had any signs or symptoms of adverse effects. Evaluate whether the medication appears to be effective in treating the condition for which it is prescribed. Recheck each MAR for the time you are giving medications to ensure that every medication scheduled for that time has been signed off.
RATIONALE Ensures that further doses of a medication are not given without consulting the physician if the patient is experiencing adverse effects. If a medication is not effective, its use needs to be questioned. Rechecking ensures that no dose has been overlooked.
 If medications are prepared for administration in the medication room, complete the two checks for each drug ordered before going to the patient’s room; perform the third check at the bedside.
If medications are prepared for administration in the medication room, complete the two checks for each drug ordered before going to the patient’s room; perform the third check at the bedside.
Patients should be sitting up as high as possible to swallow medications. Instruct not to hyperextend the neck when swallowing, but to slightly tuck in the chin instead. Offer a straw if the patient has difficulty drinking from a cup.
When a patient is on intake and output (I & O) recording, the amount of water used to take medications must be noted on the I & O sheet.
Consider each MAR and think about possible drug interactions among the drugs ordered for the patient.
If a patient is quite weak, check the swallowing reflex by offering a sip of water first, before giving medications to swallow.
Tell the patient not to swallow a sublingual or buccal medication and explain why it must be left under the tongue or in the cheek pocket.
If the patient is weak or has poor hand-eye coordination, place a large clean towel or sheet across the patient’s chest to catch “dropped” pills.
When preparing liquid medications, pour the dose into a graduated medicine cup. The exact level of the dose is read at the lowest point of the meniscus (curved upper surface) of the liquid in the cup when held at eye level (Figure 34-5). Always pour the liquid out the side of the bottle away from the label so that any residual liquid will not run down the label and distort the words on it.
Sublingual medications are placed under the tongue. They should never be swallowed. The drug dissolves in the sublingual pocket and is quickly absorbed by the vessels in the oral mucosa. Buccal medications are placed in the pocket between the teeth and the cheek. Swallowing these medications alters their absorption and may make them totally ineffective.
Eye and Ear Medications
Ophthalmic (eye) medications may be in the form of drops, ointment, or an eye disk. An error with an eye medication can cause significant damage, and it is imperative to check each medication very carefully before instilling it. The word ophthalmic must be clearly visible on the medication container and the medication must be in date. Skill 34-2 shows the steps for instilling eyedrops and eye ointment. Eye medications must be kept sterile. Careful hand hygiene is necessary before beginning the procedure.
Skills 34-2 Instilling Eye Medication
Eye medications are used to control glaucoma, treat eye infections, decrease inflammation, provide moisture to the eye, and cleanse the eye. Each medication is ordered for an individual patient and should never be used for more than one patient. Cotton balls or tissues may be used to catch the excess solution. Hand hygiene must be performed before instilling eyedrops, and disposable gloves are worn.
Review and carry out the Standard Steps in Appendix 3.
1. ACTION Determine that the ordered eye medications are on hand and that the patient is ready for them to be instilled.
RATIONALE Assists in smooth procedure performance.
2. ACTION Check the eye medication with the MAR, following the principles in the five rights of medication administration, twice before performing hand hygiene and once after identifying the patient. Double check if the instillation is for the right eye, left eye, or both eyes.
RATIONALE Prevents medication errors.
3. ACTION Assess the eye(s) for inflammation, swelling, discharge, and change in vision.
4. ACTION Consider the order in which the eye medications are to be instilled if there is more than one.
RATIONALE Some types of medications must be instilled before other types.
5. ACTION Plan sufficient time to instill the medications as ordered. You may need to remove a dressing, clean the eye, and instill drops over a set time period.
RATIONALE Instilling eye medication often takes longer than giving an oral medication.
6. ACTION Check the patient’s ID band, comparing it with the MAR. Ask the patient to state her name. Perform hand hygiene and don gloves.
RATIONALE Ensures that the medication is given to the right patient. Prevents transfer of microorganisms.
7. ACTION Remove the cap from the bottle of medication; place it upside down on the table.
RATIONALE Prepares the dropper bottle for use and protects sterility of the cap.
8. ACTION Place the patient in a sitting or reclining position. Ask the patient to look at the ceiling and tilt the head slightly to the side of the affected eye. With a tissue beneath the fingers, retract the lower lid over the bony orbit by pulling it downward to expose the conjunctival sac. If the patient is sitting in a chair, stand beside the chair.
RATIONALE Allows easier visualization of the eye and easy retraction of the eyelid. Looking upward inhibits the desire to blink.
9. ACTION Stabilize the container above the eye over the conjunctival sac and drop the designated number of drops directly into the conjunctival sac without touching the surface of the eye. Do not place drops on the cornea. Block the entrance to the lacrimal gland by placing a finger over it.

RATIONALE Only the amount of drops ordered is to be instilled. Drops on the cornea cause discomfort and/or damage. Some medications have adverse effects if they enter the systemic circulation through the lacrimal gland.
10. ACTION Replace the cap on the bottle without contaminating the dropper tip or the rim of the top. If the dropper tip becomes contaminated, replace the medication with a new bottle.
RATIONALE If the dropper tip becomes contaminated, the medication will be contaminated.
11. ACTION For eye ointment, remove the cap from the tube and set it down on a table upside down. Expose the conjunctival sac, and apply a thin ribbon of ointment along the entire length of the visible conjunctival sac. To end the ribbon, simply twist the tube with a lateral movement of the wrist without touching the eye or the lid. Recap the tube and return it to storage.

RATIONALE The ointment tube tip will be contaminated if it touches the eye. Drops and ointment placed in the conjunctival sac will spread over the entire eye.
12. ACTION Ask the patient to close the eyelid gently and to move the eyes side to side and up and down with the eyelids closed to distribute the medication.
RATIONALE Closing the eyelid tightly causes the medication to be pushed out. Rolling the eyeball around distributes the ointment over the entire eyeball.
13. ACTION With a tissue or a cotton ball, gently remove the excess medication from the outside of the lid and discard it into a designated container.
15. ACTION Assess for desired effect of the eye medication and for adverse effects.
RATIONALE The signs to assess will depend on the type of medication. If adverse effects occur, the medication may need to be changed.
16. ACTION Evaluate own technique and consider any changes to be made for next instillation.
If a dressing was removed, reapply a dressing using aseptic technique.
If the eye has crusting or debris is present, clean the lids and lashes with sterile normal saline and sterile cotton balls before instilling the medication. Wipe from the inner canthus at the nose to the outer canthus near the temple. Use a clean cotton ball for each wiping stroke.
Eye medications should be at room temperature for administration; eye ointment will flow more easily at room temperature.
If eyedrops are to be sent home with the patient for continued instillation, be certain that the patient can identify the different bottles correctly, if there is more than one medication.
Assess the area for inflammation, swelling, pain, and discharge; determine if a change in vision has occurred.
Otic (ear) medication is mostly used in children to decrease the pain of otitis media, but may also be used to treat external otitis and to soften cerumen (earwax) so that it can be removed more easily. Otic medication administration is presented in Steps 34-1, p. 670. For the child younger than 3 years, pull the ear lobe downward to straighten the canal; in the adult, pull the top of the pinna out and upward (Figure 34-6).

Nasal Medications
Nasal medications come in soft plastic atomizer or dropper bottles. An atomizer bottle contains decongestant, antihistamine, antibiotic, or steroid, depending on the patient’s need. To use an atomizer bottle, have the patient clear the nose as much as possible. While holding one nostril shut, insert the top of the atomizer into the other nostril. The patient squeezes the bottle while breathing in. The process is repeated on the other side (Safety Alert 34-2). One or two squirts per nostril is the usual dosage. The top of the bottle should be wiped clean before the cap is replaced.
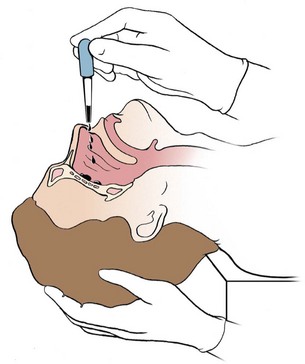
When nose drops are prescribed, the patient should lie down face up, with the head off the bed and the neck hyperextended. The drops are pulled into the dropper by depressing the rubber top of the dropper while the stem is in the liquid and letting go. The tip of the dropper is held just above the nostril and the correct number of drops is gently expelled into the nostril by lightly squeezing the rubber top (Figure 34-7).The patient should remain in the head-back position for a few minutes.
Inhalation Medications
Inhalation therapy is used for patients with respiratory conditions, which can originate in any area from the nasal passageways to the deep lung tissues. Drugs used for inhalation therapy are always water soluble to ensure quick absorption into the respiratory system without creating tissue inflammation. Various mechanical devices are designed for aerosol treatment, such as atomizers, sprays, and hand-held metered-dose inhalers (Figure 34-8).

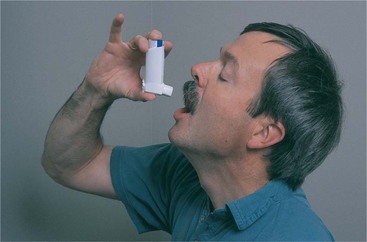
Metered-dose inhalers (MDIs) and nasal sprays come in containers labeled with directions for use. The MDI is held in front of the mouth, the cylinder for theinhalant is depressed, and a spray of medication is released. A variety of drugs are available in MDI form: antispasmodics, bronchodilators, mucolytic agents, proteolytic enzymes, and anti-inflammatories. Using a spacer with the device enhances delivery of the medication deeper into the bronchioles. Patients must be taught how to properly use an MDI (Figure 34-9 and Patient Teaching 34-1).
Short-acting insulin (Exubera) is now available in a new inhaled form. For type 2 diabetes, it may be used alone or in conjunction with dietary modifications, oral antidiabetic drugs, or injected insulin. For type 1 diabetes, this inhaled form maybe used along with injected intermediate or long-acting insulin. Exubera is contraindicated for patients with pulmonary disease or those who smoke. The medication is administered 10 minutes before a meal. Teach your patient that the medication is available in 1-mg and 3-mg blister packages; however, she should not substitute three 1-mg blisters for one 3-mg blister. This will result in an overdose. For additional information, consult www.exubera.com.
Five groups of drugs are commonly dispensed in inhalers for treatment of the lungs (Table 34-6). The patient should not take more than one drug from any one of the groups.
Table 34-6
Inhalant Drugs for Respiratory Problems
| DRUG | EXAMPLE |
| Beta-agonist drugs (stimulants) that open the small airways | Metaproterenol (Alupent), albuterol (Proventil, Ventolin), and terbutaline (Brethaire) |
| Anticholinergics used to decrease bronchospasm and open the large airways | Atropine, ipratropium (Atrovent) |
| Corticosteroids used to decrease inflammation | Beclomethasone (Beclovent, Vanceril), triamcinolone (Azmacort), and flunisolide (AeroBid) |
| Leukotriene modifiers for maintenance therapy of chronic asthma | Montelukast (Singulair) |
| Antiallergics used to decrease mucosal response to allergens | Cromolyn sodium (Intal) |
Vaginal Medications
A vaginal irrigation is also called a douche. Topical solution is introduced into the vaginal cavity for the following purposes:
• To cleanse the vagina in preparation for surgery
• To supply antiseptics to reduce bacterial growth
• To remove odors or foul discharge
• To apply heat or cold to soothe inflamed tissues or reduce oozing of blood
The normal secretions of the vaginal tissues are naturally acidic, which helps protect against vaginal infection. Vaginal irrigations are considered a clean procedure, except when given postoperatively or after childbirth, then principles of surgical asepsis are followed. Medicated solutions used for vaginal irrigations are 2% sodium bicarbonate solution, diluted hydrogen peroxide, povidone-iodine solution, a weak solution of acetic acid (1 tablespoon vinegar to 1000 mL of fluid), or a medication that is diluted in water. The amount of solution ranges from 1500 to 2000 mL, given slowly over a period of 10 to 15 minutes at a temperature of 100° to 105° F (37.7° to 40.5° C) unless the purpose is to apply heat; then it should be 110° F (43° C). The patient should receive instruction in the correct way to perform the irrigation (Patient Teaching 34-2).
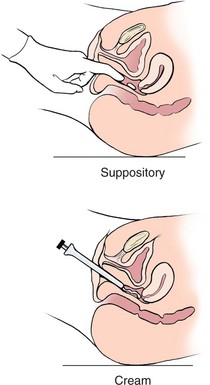
Other topical medications applied to the vagina are suppositories, ointments, and creams prescribed to treat infections and inflammation (Cultural Cues 34-2). Applicators are used for inserting the smaller vaginal suppositories at the distal end of the vagina. An applicator is also required for vaginal ointments. The applicator fits the top of the tube and enough medication is squeezed into the barrel to fill it, after which the applicator is inserted into the vagina, where the plunger deposits the ointment (Figure 34-10). After use, the applicator is washed with soap and water and stored for the patient’s futureuse, or it is discarded. The patient may be instructed on how to insert the medication herself. After medication has been inserted, a small pad or panty shield may be worn to keep from soiling clothing or bedding.
Rectal Medications
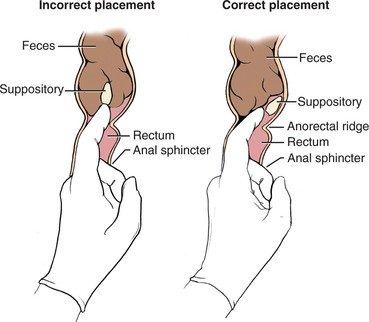
Rectal medications are dispensed in the form of suppositories (Figure 34-11). There are suppositories to prevent vomiting, soothe hemorrhoids, prevent bladder spasms, promote bowel evacuation, and reduce fever. See Steps 34-2 for the procedure to insert a rectal suppository.
Topical Skin Medications
Many types of topical medications can be applied to the skin. These types include lotions, ointments, creams, and patches. The steps for medication administration must be followed when applying any topical medication. Ointments, oils, lotions, and creams are combinations of skin emollients and a medication and are applied by rubbing into the skin. Skill 34-3 provides the steps for applying a topical skin preparation.
Skills 34-3 Administering Topical Skin Medications
Many types of topical medications can be applied to the skin. Lotions, ointments, creams, and patches are all used on the skin. The steps for medication administration must be followed when applying any topical medication.
Review and carry out the Standard Steps in Appendix 3.
1. ACTION Determine that ordered medication is on hand and that patient is available for the application and has already bathed.
RATIONALESaves time; prevents medication from being washed off.
2. ACTION Assess for any side or adverse effects of the medication.
RATIONALEFurther doses should not be applied if there is an adverse reaction.
3. ACTION Gather any dressing materials that may be needed.
RATIONALEGather any dressing materials that may be needed.
4. ACTION Plan sufficient time to perform the application without interruption.
RATIONALETime required for application depends on whether dressings are involved and the area to be treated.
5. ACTION Check the medication against the MAR twice following the five rights of medication administration.
RATIONALEEnsures giving the right drug in the right dose and applying it on the right location.
6. ACTION Identify the patient by checking the identification band with the MAR. Ask the patient to state her name.
RATIONALE Ensures that the right patient receives the medication.
7. ACTION Perform hand hygiene and don gloves.
RATIONALE Reduces transfer of microorganisms. Gloves also protect the nurse from absorbing medication through the hands.
8. ACTION Place the medication bottle and supply of gauze dressings or cotton balls on a convenient working surface. Shake the bottle well; perform the third drug check with the MAR; remove the cap and place it upside down on the working surface.
RATIONALE Prepares supplies for application. Third check of the drug helps prevent medication error.
9. ACTION Pick up a gauze dressing or cotton ball. With the bottle in your nondominant hand with the label facing upward, carefully pour the lotion onto the applicator. Catch excess solution in a basin, paper wrapper, or waste container.
RATIONALE Keeping the label facing upward prevents soiling if some of the medicine drips down the side of the bottle while pouring. Applying the lotion to the gauze or cotton ball prevents spills.
10. ACTION Apply the lotion to the affected area by patting it on lightly. Do not rub. Repeat steps 9 and 10 until the area is covered, using a new applicator each time. Observe the skin for change in color, swelling, rash, and so on.
RATIONALE Rubbing makes pruritus (itching) worse. Friction irritates lesions. Skin assessment must be documented.
11. ACTION Discard the gauze or cotton balls in the designated container; remove gloves and replace the cap on the lotion.
RATIONALE Disposes of potentially infectious waste; preserves the medication.
For Application of Cream or Ointment
12. ACTION Apply the medication with a gloved finger or tongue blade to dry skin. Apply thin film in the direction of hair growth.
RATIONALE A glove protects the nurse from absorbing the medication. A tongue blade will spread an even layer of ointment.
13. ACTION Apply a dressing if ordered.
RATIONALE A dressing helps keep the cream or ointment on the skin.
14. ACTION Measure out the correct amount of ointment on a paper measuring guide.
RATIONALE The measurement must be exactly what is ordered.
15. ACTION Wash off any remaining ointment from a previous application.
RATIONALE Remaining ointment would increase the dosage the patient is receiving.
16. ACTION Gently apply the paper to the patient’s skin, distributing the ointment over about a 2-inch area, but not rubbing it into the skin. Rotate the site with each application; use the chest and upper arms so as to apply over as hairless an area as possible. Tape the paper in place around the edges, or place a piece of plastic wrap over the paper and tape it into place.
RATIONALE Medication will slowly disperse into the skin and bloodstream. Hair may prevent contact of the ointment with the skin, decreasing absorption. Taping and/or covering the paper with plastic wrap protects the patient’s clothing.
17. ACTION Remove gloves and perform hand hygiene; return medication to storage area.
RATIONALE Reduces transfer of microorganisms; prepares medication for next use.
Transdermal (through the skin) medications are supplied in a sustained-release patch that is applied to clean, dry, hairless skin and left in place, or as a paste that is spread on a small area of skin. The drug is slowly absorbed through the skin and is absorbed into the bloodstream. Several types of drugs are now available in skin patch form: nitroglycerin to dilate coronary arteries, scopolamine to relieve motion sickness, estrogen to combat symptoms of menopause, nicotine to assist smoking cessation, and fentanyl, an opioid analgesic, for severe chronic pain. Skin patches should be applied to areas where there is adequate circulation, such as the chest, shoulders, or upper arm. Scopolamine patches are placed behind the ear. Each new patch should be applied to a different area so as not to irritate the skin. Hair should be removedbefore applying a patch. The effect of the medication from a skin patch will begin in about 30 minutes and may remain in the system for 30 minutes after the patch is removed. The patch should be dated and initialed so it is evident when it was applied (Assignment Considerations 34-1).
Nitroglycerin also is dispensed as a paste. It is applied to the skin, but not rubbed in. A ribbon of the ointment in the amount prescribed is applied to the measuring applicator, and the paper is folded to distribute the paste or a wooden applicator is used to spread the paste over a 2¼ × 3½-inch (5.6 × 8.8-cm) area of the paper. The paper is placed paste side down on a clean, nonhairy area of skin and taped into place. When one applicator is removed, the skin is cleansed and the next applicator is applied in a different, clean area.
Administering Medications via Feeding Tube
Many oral medications can be given through a feeding tube. Liquid medications are best, but if a tablet is crushable or a capsule can be opened and the contents mixed with liquid, or the liquid within the capsule can be aspirated with a needle and syringe, then the medication can be administered through the feeding tube. Medications that should not be crushed and administered through the tube are sublingual or buccal, enteric-coated, or sustained-release preparations or products with a carcinogenic potential (e.g., antineoplastics). For a small-bore tube, medications must be well dissolved in the liquid before administration. Do not mix the medication with a tube feeding because many things can interrupt or prevent delivery of the entire dose of medication. Skill 34-4 provides the steps for administering medications through a feeding tube.
Skills 34-4 Administering Medications Through a Feeding Tube
When the patient cannot take anything by mouth, but has a feeding tube in place, oral medications can be administered through the tube. Liquid medications are best, but many medications may be crushed and mixed with water for administration. The medication dose must be followed by more water to irrigate the tube so that clogging does not occur. Each medication is mixed with water individually; medications are not combined so as to prevent clumping.
1. ACTION Follow beginning procedures for the administration of oral medications by checking the order and assessing for allergies and adverse effects. Check the medications with the MAR, performing two checks before preparing each medication and one check after preparing each one.
RATIONALE Follows the principles of the Five Rights of medication administration.
2. ACTION Assess for patency and position of the feeding tube.
RATIONALE Follow correct procedure for verifying placement and patency of the feeding tube (see Chapter 27).
3. ACTION Verify that needed supplies are on hand. Fill a container with warm water.
RATIONALE Procedure will not have to be stopped to gather supplies. Water is used to dissolve the medications.
4. ACTION Perform hand hygiene
RATIONALE Medicines are prepared with aseptic technique.
5. ACTION Crush each medication to be given that comes in a tablet, if it can safely be crushed and administered. If medication is a liquid in a gel capsule, the liquid may be aspirated with a syringe and needle. For capsules containing powder, open the capsule and pour the powder into a medicine cup.
6. ACTION Mix each medication with 30 mL of warm water. Gelatin capsules may be dissolved by dropping the capsule into warm water and allowing to sit for 15 minutes.
RATIONALE Prepares medications for administration because they must be liquid to traverse the tube.
7. ACTION Correctly identify the patient by checking the identification band with the name and hospital number on the MAR. Ask the patient to state his or her name if conscious and able.
RATIONALE Prevents giving a medication to the wrong patient.
8. ACTION Place the patient in a high Fowler’s position, unless contraindicated.
RATIONALE Gravity helps medication progress down the tube into the stomach or small intestine. At least a 30-degree elevation of the head is essential.
9. ACTION Put on gloves and attach the irrigation syringe to the tube while keeping the tube pinched off.
RATIONALE Readies the syringe to receive the water and medication. Prevents air from entering the tube.
10. ACTION Add 15 to 30 mL of water to the syringe and add the dissolved medication just as the water is about to finish entering the tube. If necessary, apply gentle pressure with the syringe plunger or bulb to instill the liquid.

RATIONALE Water flushes tube feeding from the tube and decreases viscosity of fluid within the tube. Adding the medication before the syringe is empty prevents air from entering the tube. Pressure may be needed to initiate the flow.
11. ACTION Follow the first medication with at least 5 mL of water before administering the next one. Add next medication each time before the syringe is empty.
RATIONALE Ensures that the various medications don’t interact in the tube and clog it. Prevents air from entering the tube.
12. ACTION Follow the last medication with 30 to 60 mL of water. Pinch off the tube as the syringe empties.

RATIONALE Water flushes the tube of all medication and ensures patency of tube. Pinching off the tube prevents air from entering tube.
13. ACTION Clamp or plug the tube for 30 minutes before reconnecting a decompression tube to suction. For a feeding tube, clamp it only if the medications cannot be mixed with food. Otherwise the tube may be reconnected to the tube feeding. If tube feedings are intermittent, the tube is simply left clamped.

RATIONALE Prevents suctioning out the medication before it is absorbed. Prevents drug and food interactions. Reinitiates the tube feeding.
14. ACTION Leave the head of the bed elevated for at least 30 minutes, preferably for 60 minutes.
RATIONALE Prevents reflux of the medications back up the tube.
15. ACTION Clean up equipment, remove gloves, and perform hand hygiene.
RATIONALE Restores the unit. Reduces transfer of microorganisms.
16. ACTION Evaluate patency of the tube by visualizing free flow of liquid into it.
RATIONALE If liquid does not flow smoothly, tube may be becoming clogged and further irrigation may be needed.
17. ACTION Assess for adverse effects of the medication(s).
RATIONALE Assessment is performed before administering the next dose.
18. ACTION Evaluate for abdominal distention or nausea.
RATIONALE Medications may be irritating the stomach; if so, consult the physician.
Evaluation
Only by gathering evaluation data can it be determined whether the medication is effective. Evaluation for signs of adverse effects is essential before administration of the next dose. Sometimes signs and symptoms will not appear until after the prescription has been finished. Evaluation statements might be as follows:
• Experienced nausea within 30 minutes of taking antibiotic.
• Refused antihistamine; itching has subsided.
• White blood cell count is 7000/mm3, temperature 99° F (37.2° C); antibiotic effective.
• Red rash on chest possibly from antibiotic; physician notified.
• Verbalizes that she will take antihypertensive even if she feels well.
Evaluation statements indicating that the expected outcomes stated earlier in the chapter have been met include:
• Pain is relieved for 3½ hours by analgesic.
• Blood pressure is within normal range (e.g., 130/74) while the patient is taking antihypertensive medication.
• Heart rate is regular and within normal limits (e.g., 70 to 85/min) while patient is taking antiarrhythmic medication.
• Wound culture is negative after 5 days of antibiotic therapy.
• No nausea when antiemetic is taken 30 minutes before eating a meal.
• Patient verbalizes that medication “controls my blood pressure.”
Documentation
Documentation of medication administration is largely done on the MAR. PRN medications, one-time doses, and preoperative medications may also be charted in the nurse’s notes (follow agency policy). Data to be documented include the following:
• Medication name, dosage, route, and time administered
• Blood pressure and pulse before administration of antihypertensives and beta-blocker drugs
• Reason for a PRN medication’s administration
• Assessment data regarding side effects of the medication
• Patient teaching regarding the medication (Home Care Considerations 34-1)
Home Care Considerations 34-1
Medication Administration for the Home Care Patient
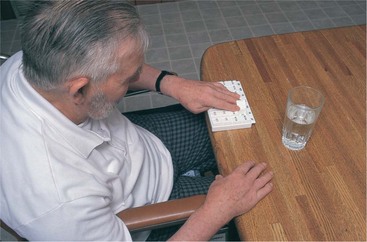
• A 7-day medication planner container is helpful for the patient who is unreliable in taking medications or for one who has difficulty managing to remove the tops from medication vials (Figure 34-12). The patient can easily see if a medication has been taken. A friend or neighbor can be enlisted to help set up the medications once a week if the patient lives alone.
• All medication must be kept out of the reach of children. Even if children are not living in the home, this is a concern if any children visit.
• Expiration dates should be checked for all prescription and nonprescription medications in the home. Discard outdated medications.
• Assess use of over-the-counter medications when performing a medication history.
• Advise patients that if they are ordering prescriptions by mail, they need to inform the local pharmacist where they sometimes have prescriptions filled. The local pharmacy should have a complete list of everything the patient is taking so that drug interactions or overdosage can be prevented.
• If possible assess the patient’s (or caregiver’s) preparation of the medication to observe the methods and techniques being used.
• Evaluation data indicative of the effectiveness of medication
MEDICATION ERRORS
In the United States, an estimated 1.5 million patients are harmed each year by medication errors (Metules & Bauer, 2007) in spite of all the safeguards. When a medication error is discovered, it is reported immediately. An incident or occurrence form is filled out for the medication error, and the agency policy for reporting drug errors is followed. After notifying the physician, orders are carried out to safeguard the patient. All medication errors must be reported.The goal is to prevent harm to the patient from the error and to prevent similar errors from happening again. The nurse who discovers the error is the one to report it and fill out the report. Therefore, the nurse who made the error may not be the same nurse who reports it and fills out the occurrence form. In accordance with National Patient Safety Goals, health facilities and all health care workers should be supporting efforts to track and monitor adverse events to improve health care delivery systems.
NCLEX-PN © EXAMINATION–STYLE REVIEW QUESTIONS
Choose the best answer(s) for each question.
1. The patient has returned from surgery several hours ago and is asking for pain medication. The nurse should give pain medication according to:
2. A nurse is caring for a patient who needs to have his morning dose of eyedrops to the right eye. Below are the steps for the procedure of instilling eyedrops. Place these steps (1 though 7) in the correct order.
______1. Document the doses given on the MAR.
______2. Stabilize the container above the eye over the conjunctival sac.
______3. Check the patient’s ID band, comparing it with the MAR.
______4. Block the entrance to the lacrimal gland by placing a finger over it.
______5. Drop the designated number of drops directly into the conjunctival sac without touching the surface of the eye.
______6. Ask the patient to look at the ceiling and tilt the head slightly to the side of the affected eye.
______7. Place the patient in a sitting or reclining position.
3. The final check of a medication dose should be done:
1. before leaving the medication cart or area.
2. before opening the dose at the patient’s bedside.
4. The nurse is performing the final check of the medication before administering it to the patient. Which information should be checked?
1. Patient’s name, birth date, room number, physician’s name, and drug dosage
2. Patient’s name, ID number, drug name, dosage, route, time, and drug allergies
3. Patient’s name, drug classification, dosage and date, and allergies
4. Patient’s name, birth date, ID number, and admitting diagnosis
5. A nursing student is preparing to give instructions to a patient on how to use a metered-dose inhaler. Which statement by the student nurse indicates that she knows what to tell the patient?
1. “I tell the patient to wait 10 minutes between puffs.”
2. “I teach him to close one nostril before depressing the canister.”
3. “I have him take in a deep breath and hold it before placing the mouthpiece.”
4. “I instruct him to inhale the medication and hold it for at least 10 seconds.”
6. When giving ear medication to a child younger than 3 years, the technique is to:
1. draw the earlobe slightly down and back.
2. pull the top of the pinna upward and back.
3. rotate the pinna until the eardrum is visualized.
4. apply gentle pressure to the face to ease the tissue forward.
7. After preparation of a liquid medication, the patient refuses it. What is the most appropriate nursing action?
1. Record the medication as “not taken” and discard it.
2. Record the dose as taken because it must be charged.
8. A nurse is preparing to give morning medication and he identifies a discrepancy between what the night shift nurse said in the shift report and what is written on the medication administration record (MAR). Which action would be the most appropriate?
1. Give the medication according to the MAR.
2. Call the night shift nurse at home.
9. An ambulatory surgery patient is to be discharged home and needs six doses of analgesic tablets for discomfort. What is the most appropriate nursing action?
1. Dispense six tablets from the controlled-substance dispenser.
2. Obtain a written prescription for the medication.
3. Call the hospital pharmacist to fill the order.
4. Ask the patient to call the physician’s office for the prescription.
10. A patient reports that he is taking an aspirin every day “to prevent heart attack” as well as Ecotrin (enteric-coated aspirin). Which nursing action is the priority?
CRITICAL THINKING ACTIVITIES ? Read each clinical scenario and discuss the questions with your classmates.
You are in the medication room preparing medications for your patients when a nurse who is standing next to you is called to take a patient to another nursing unit. She shows you the medications she has prepared for one of her patients and asks you to please administer them so they will not be given late.
Scenario B
Dan Hartford is receiving ampicillin for a respiratory infection. When you go in to give him the next dose, you notice that his face seems to have a red rash on it. When you question him, he states he has been itching a little across his chest and on his legs.