Oral Manifestations of Systemic Diseases
After studying this chapter, the student will be able to:
1 Define each of the words in the vocabulary list for this chapter.
2 Describe the difference between gigantism and acromegaly and list the physical characteristics of each.
3 State the oral manifestations of hyperthyroidism.
4 Describe the difference between primary and secondary hyperparathyroidism.
5 List the oral and systemic manifestations that occur in the uncontrolled diabetic state.
6 List the major clinical characteristics of type 1 and type 2 diabetes.
7 Define Addison disease and describe the changes that occur on the skin and oral mucosa in a patient with Addison disease.
8 Compare and contrast the cause, laboratory findings, and oral manifestations of each of the following: iron deficiency anemia, pernicious anemia, folic acid deficiency, and vitamin B deficiency.
9 Compare and contrast the definitions and oral manifestations of thalassemia major and sickle cell anemia.
11 Describe the difference between primary and secondary aplastic anemia.
12 Describe the oral manifestations of polycythemia.
13 Explain why platelets may be deficient in polycythemia vera.
14 Describe the most characteristic oral manifestations of agranulocytosis.
15 Describe and contrast acute and chronic leukemia.
16 State the purpose of each of the following laboratory tests: platelet count, bleeding time, prothrombin time, partial thromboplastin time, and international normalized ratio.
17 List two causes of thrombocytopenic purpura.
18 Describe the oral manifestations of thrombocytopenia and nonthrombocytopenic purpura.
19 Define hemophilia and describe its oral manifestations and treatment.
20 Describe the difference between primary and secondary immunodeficiency.
21 Describe the oral problems that would be expected to occur in a patient with radiation-induced xerostomia.
22 List two drugs that are associated with gingival enlargement.
(ah-gran′u-lo-si-to′sis) Marked decrease in the number of granulocytes, particularly neutrophils.
(ah-ne′me-ah) Reduction of the number of red blood cells, quantity of hemoglobin, or volume of packed red blood cells to less than normal.
( -pla′zhe-ah) (adjective, aplastic) Lack of development.
-pla′zhe-ah) (adjective, aplastic) Lack of development.
(ar-thral′-jĭ-ah) Severe pain in a joint.
The process by which lipid accumulates within the walls of large and medium-sized arteries. It leads to reduced blood flow to and death of vital organs.
(aw′′to-ĭ-mu′nĭ-te) Immune-mediated destruction of the body′s own cells and tissues; immunity against self.
(kah-tab′ah-lizm) Component of metabolism that involves the breakdown of tissues.
(ko-ag′′u-la′shun) Formation of a clot.
(ek′′ĭ-mo′sis) Small, flat, hemorrhagic patch larger than a petechia on the skin or mucous membrane.
(fi′brin) Insoluble protein that is essential to the clotting of blood.
(he-mat′ah-krit) Volume percentage of red blood cells in whole blood.
(he-mol′ĭ-sis) Release of hemoglobin from red blood cells by destruction of the cells.
(he′′mo-sta′sis) Stoppage or cessation of bleeding.
(hep′′ah-to-meg′ah-le) Enlargement of the liver.
(hor′mōn) Secreted molecules produced in the body that have a specific regulatory action on target cells that are distant from their sites of synthesis; an endocrine hormone is frequently carried by the blood from its site of release to its target.
(hi′′per-kal-se′me-ah) Excess calcium in the blood.
(hi′′per-gli-se′me-ah) Excess glucose in the blood.
(hi′′po-kro′mik) Stained less intensely than normal.
(hi′′po-fos′′fah-te′me-ah) Deficiency of phosphates in the blood.
(in′sū-lin) Hormone produced in the pancreas by the beta cells in the islets of Langerhans; insulin regulates glucose metabolism and is the major fuel-regulating hormone.
shock Profound hypoglycemia, or low blood sugar, that necessitates emergency intervention.
(ke′′to-ah′′sĭ-do′sis) Accumulation of acid in the body resulting from the accumulation of ketone bodies.
(mi′kro-sĭt) Red blood cell that is smaller than normal.
(mi-al′-jĕ-ah) Muscle pain.
(nu′′tro-pe′ne-ah) Decreased number of neutrophils in the blood.
(os′′te-o-po-ro′sis) Abnormal rarefaction of bone.
(par′′ah-thor′mōn) Parathyroid hormone.
(pe-te′ke-ah) Minute red spot on the skin or mucous membrane caused by escape of a small amount of blood.
(plt′let) Disc-shaped structure, also called a thrombocyte, found in the blood; it plays an important role in blood coagulation.
(pol′′e-si-the′me-ah) Increase in the total red blood cell mass in the blood.
(pol′′i-dip′se-a) Chronic excessive thirst and intake of fluid.
(pur′pu-rah) Blood disorders characterized by purplish or brownish-red discolorations caused by bleeding into the skin or tissues.
(re-sep′ter) Cell surface protein to which a specific hormone can bind; such binding leads to biochemical events.
(sple′′no-meg′ah-le) Enlargement of the spleen.
(throm′bo-sīt) Platelet.
(throm′′bo-si′′to-pe′ne-ah) Decrease in the number of platelets in circulating blood.
Many diseases that affect the body as a whole are associated with alterations of the oral mucosa, maxilla, and mandible. Systemic diseases can cause mucosal changes such as ulceration or mucosal bleeding. Generalized immunodeficiency can lead to the development of opportunistic diseases such as infection and neoplasia. Bone disease can affect the maxilla and mandible, and systemic disease can cause dental and periodontal changes. Drugs prescribed for a systemic disease can affect the oral tissues.
Local factors are frequently involved in manifestations of systemic disease in the oral mucosa. In some systemic diseases the mucosa is more easily injured; therefore mild irritation and chronic inflammation can cause lesions that would not occur without the presence of the systemic disease.
This chapter includes systemic diseases that have oral manifestations. Some overlapping occurs among the diseases included in this chapter and those included in other chapters. Some of the diseases discussed in this chapter could have been included appropriately in other chapters. Included here are endocrine disorders, disorders of red and white blood cells, disorders of platelets and other bleeding and clotting disorders, and immunodeficiency disorders. Oral changes can be similar for several different systemic diseases, and similar oral lesions can occur without the presence of systemic disease. Because of this, many oral lesions described in this chapter are also described elsewhere in this text.
ENDOCRINE DISORDERS
The endocrine system consists of a group of integrated glands and cells that secrete hormones. The secretion of hormones by these glands is controlled by feedback mechanisms in which the amount of hormone circulating in blood triggers factors that control production. Diseases of this system can result from (1) conditions in which too much or too little hormone is produced, and (2) from either dysfunction of the glands themselves or a problem in the mechanism that controls hormone production. Some of the endocrine gland diseases in which oral changes occur are included here.
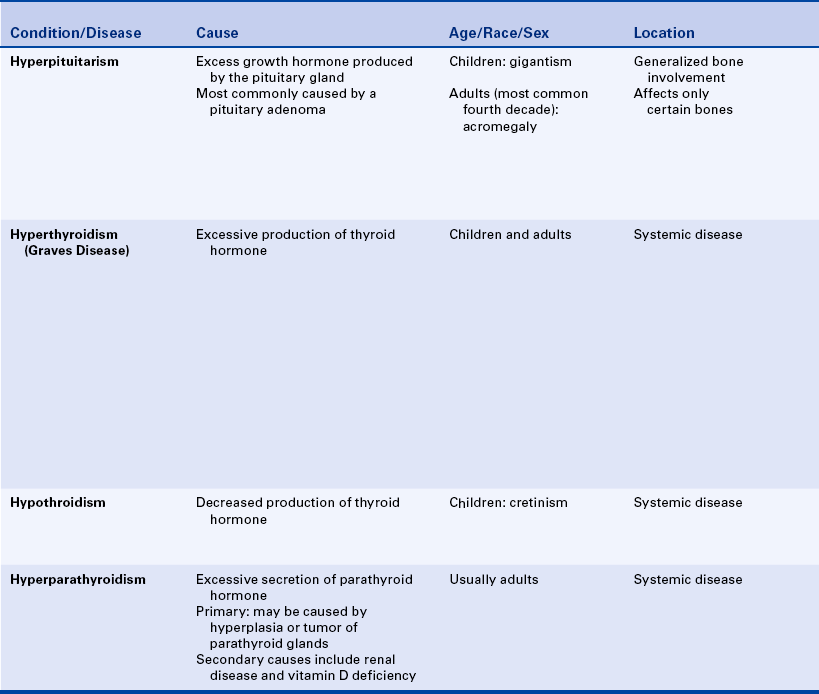
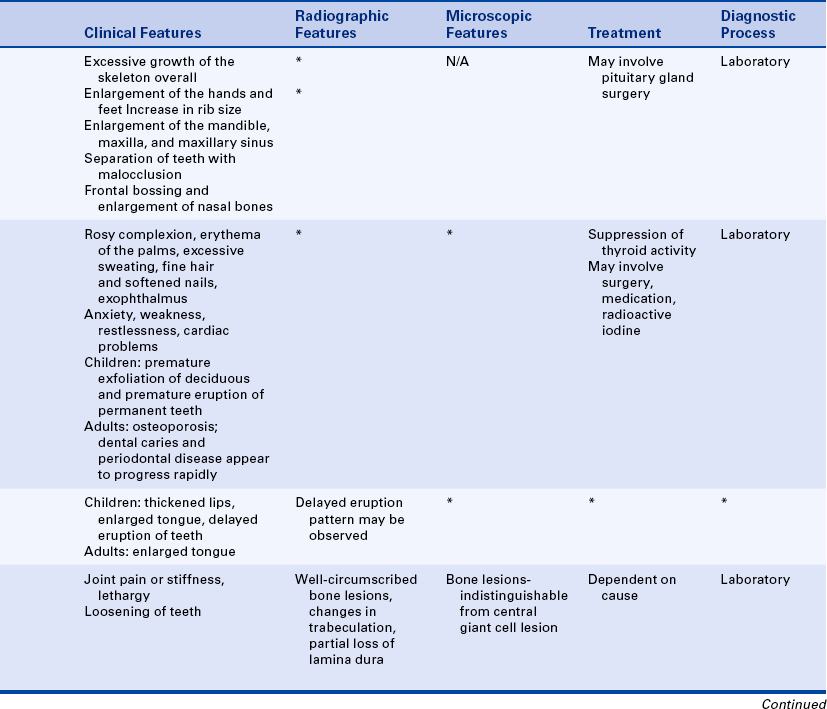
HYPERPITUITARISM
Hyperpituitarism is excess hormone production by the anterior pituitary gland. It is caused most often by a benign tumor (pituitary adenoma) that produces growth hormone. If the increase in growth hormone production occurs during development before the closure of the long bones, gigantism results. Acromegaly results when the hypersecretion occurs in adult life.
Clinical Features and Oral Manifestations
Gigantism includes excessive growth of the overall skeleton. Affected individuals can be more than 8 feet tall and weigh several hundred pounds; and as adults they experience headaches, chronic fatigue, and muscle and joint pain.
Acromegaly affects both men and women and most commonly occurs in the fourth decade of life. The onset is slow and insidious. Patients experience poor vision, sensitivity to light, enlargement of the hands and feet, and an increase in rib size. The facial changes include enlargement of the maxilla and mandible, frontal bossing (an enlargement of the bones of the forehead), and enlargement of the nasal bones. An enlargement of the maxillary sinus also occurs, which causes a characteristically deep voice. The enlargement of the maxilla and mandible results in separation of teeth and malocclusion. Mucosal changes such as thickened lips and macroglossia (enlarged tongue) have also been described in patients with acromegaly (Figure 9-1).

HYPERTHYROIDISM
Hyperthyroidism, also called thyrotoxicosis, is characterized by excessive production of thyroid hormone. It is much more common in women than in men. Hyperthyroidism has several different causes. The most common cause is a condition called Graves disease. The exact cause of Graves disease is not clear, but it appears to result from an autoimmune disorder in which a substance that abnormally stimulates the thyroid gland is produced. Other causes of hyperthyroidism include hyperplasia of the gland, benign and malignant tumors of the thyroid, pituitary gland disease, and metastatic tumors.
Clinical Features
The clinical features of hyperthyroidism include goiter, rosy complexion, erythema of the palms, excessive sweating, fine hair, and softened nails. Exophthalmos (protrusion of the eyeballs) may be seen. Anxiety, weakness, restlessness, and cardiac problems may be associated with the disorder.
Oral Manifestations
Hyperthyroidism in children may lead to premature exfoliation of deciduous teeth and premature eruption of permanent teeth. In adults osteoporosis may occur, which may affect alveolar bone. Dental caries and periodontal disease appear to develop and progress more rapidly in these patients than in other patients. Burning discomfort of the tongue has also been reported.
Treatment
Treatment of hyperthyroidism may include surgery, medications to suppress thyroid activity, or the administration of radioactive iodine. The treatment of hyperthyroidism is the most common cause of hypothyroidism. Clinical mismanagement of hyperthyroidism may lead to hypothyroidism and is thus described as iatrogenic or clinician-caused disease.
HYPOTHYROIDISM
Hypothyroidism is characterized by decreased output of thyroid hormone. When hypothyroidism is present during infancy and childhood, it is known as cretinism. In older children and adults the condition is known as myxedema. Causes include developmental disturbances, autoimmune disease, iodine deficiency, drugs, and pituitary disease. In infants facial and oral changes include thickened lips, enlarged tongue, and delayed eruption of teeth. Adults with hypothyroidism may have an enlarged tongue.
HYPERPARATHYROIDISM
Hyperparathyroidism results from excessive secretion of parathyroid hormone (parathormone) (PTH), which is secreted by the parathyroid glands. The four parathyroid glands are located near the thyroid gland. PTH plays an important role in calcium and phosphorus metabolism. Elevated blood levels of calcium (hypercalcemia), low levels of blood phosphorus (hypophosphatemia), and abnormal bone metabolism characterize hyperparathyroidism.
Hyperparathyroidism may be the result of hyperplasia of the parathyroid glands, a benign tumor of one or more of the parathyroid glands (parathyroid adenoma), or (less commonly) a malignant parathyroid tumor. The disease is found in middle-age adults and is far more common in women than in men.
Calcium is obtained mainly from dairy products and plays an important role in the contraction of all types of muscle. PTH maintains normal blood levels of calcium through its effects on the kidney, gastrointestinal tract, and bone. It increases the uptake of dietary calcium from the gastrointestinal tract and is able to move calcium from bone to circulating blood when necessary. The hormone appears to be able to remove calcium from bone through the action of osteoclasts.
Hyperparathyroidism that results from an abnormality of the parathyroid glands is called primary hyperparathyroidism. Secondary hyperparathyroidism occurs when calcium is abnormally excreted by the kidneys and the parathyroid glands increase their production of PTH to maintain adequate blood levels of calcium. The most common cause of secondary hyperparathyroidism is kidney failure. Problems with absorption of nutrients and fat-soluble vitamins such as vitamin D through the gut or small intestine are also an important cause of hyperparathyroidism.
Clinical Features
The clinical manifestations of hyperparathyroidism are varied. Patients with mild cases can be asymptomatic. Joint pain or stiffness may be present. The disease can affect the kidneys, skeletal system, and gastrointestinal system. In severe disease lethargy and coma can occur.
Oral Manifestations
The oral manifestations of hyperparathyroidism include changes in the bone of the mandible and maxilla. The chief oral manifestation is the appearance of well-defined unilocular or multilocular radiolucencies (Figure 9-2, A). Microscopically these lesions appear indistinguishable from central giant cell granulomas (described in Chapter 2) (Figure 9-2, B). There have also been reports of a few cases of peripheral giant cell granulomas associated with hyperparathyroidism. Other radiographic changes that occur in hyperparathyroidism include a generalized mottled appearance of the bone and partial loss of the lamina dura. Loosening of teeth can also occur.
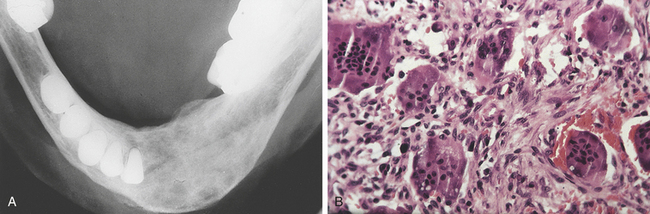
FIGURE 9-2 A, Radiograph of a mandibular lesion in a patient with hyperparathyroidism. B, Microscopic appearance of a jaw lesion occurring in a patient with hyperparathyroidism. The histologic appearance is identical to that of a central giant cell granuloma. (A courtesy Drs. Paul Freedman and Stanley Kerpel.)
Diagnosis and Treatment
The diagnosis of hyperparathyroidism involves the measurement of PTH blood levels and can also include serum calcium and phosphorus measurements. Treatment is directed at correcting the cause of the increased production of the hormone. Causes of increased production of hormone can include tumors, renal disease, and vitamin D deficiency. Bone lesions resolve when the hyperparathyroidism is treated successfully.
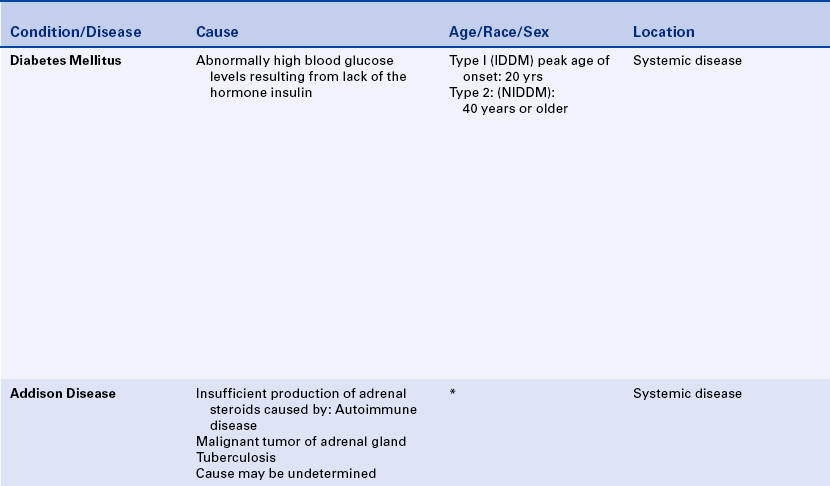
DIABETES MELLITUS
Diabetes mellitus is a chronic disorder of carbohydrate (glucose) metabolism and is characterized by abnormally high blood glucose levels (hyperglycemia), which result from a lack of the hormone insulin, defective insulin that does not work effectively to lower blood glucose levels, or increased insulin resistance because of obesity. Diabetes is appropriately considered a syndrome because it has several components, including both acute and chronic complications. This disorder of carbohydrate metabolism also leads to disorders of protein and fat metabolism. Normally glucose signals the beta cells of the pancreas to make insulin. This hormone is then secreted directly into the bloodstream to facilitate the uptake of glucose into fat and skeletal muscle cells. In the presence of insulin, fat and skeletal muscle cells can use glucose as an energy source. When insulin is lacking, these cells are starved of energy. Without insulin to meet the body’s demand for carbohydrate, tissues are broken down (catabolism), and weight loss occurs, as well as severe hyperglycemia that can lead to diabetic coma. Furthermore, the production of ketone acid from the breakdown of fatty tissue is a life-threatening condition and is a common metabolic disturbance in type 1 (insulin-dependent) diabetes. These ketone acids (acetone) can lower the pH of the blood (ketoacidosis), an acute condition that can lead to coma and death. White blood cell function is affected in patients with diabetes mellitus. Phagocytic activity of macrophages is reduced; chemotaxis of neutrophils is delayed; and lymphocyte function (T lymphocytes) is also adversely affected. These changes increase a patient’s susceptibility to infection. In addition, collagen production is abnormal, thus affecting the healing process. With chronic hyperglycemia, collagen and other proteins become tagged with carbohydrate. These resulting advanced glycation end products (AGEs) impair healing and may also play a contributory role in the progression of atherosclerosis. Atherosclerosis leads to death of heart muscle (myocardial infarction or heart attack), stroke, and kidney failure.
The precise cause of diabetes mellitus is unknown. Genetic and environmental factors have been implicated in its onset. Sixteen million Americans have been diagnosed with diabetes mellitus. It is estimated that an additional seven million Americans have undiagnosed diabetes and therefore are at risk for life-threatening complications of untreated diabetes.
Types of Diabetes
Insulin-Dependent Diabetes Mellitus
Two major types of diabetes have been recognized and classified. The first type (type 1 diabetes) is called insulin-dependent diabetes mellitus (IDDM). Autoimmunity appears to play a key role in the development of type 1 diabetes, leading to the destruction of the insulin-producing beta cells of the pancreas and ultimately profound insulin deficiency. Only 3% of all diabetic patients have this type of diabetes. Type 1 diabetes can occur at any age, but its time of onset is usually at a peak age of 20 years. The onset is abrupt and can have the three Ps (or the complications of these signs): (1) polydipsia (excessive thirst and intake of fluid), (2) polyuria (excessive urination), and (3) polyphagia (excessive appetite). Patients usually have a thin body build.
Complications can occur in 90% of individuals with type 1 diabetes within 20 years of diagnosis. Difficulty in controlling blood glucose levels is a major problem for patients with IDDM. In recent years it has become increasingly evident that long-term rigorous control of blood glucose levels is important in minimizing the extent of chronic complications in patients with IDDM. Damage to the small blood vessels (microvascular disease) in diabetes leads to complications with organ systems; these include particularly the eye, kidney, and nerves. Atherosclerosis of medium-size blood vessels (macrovascular disease) in diabetes affects, for example, the coronary and cerebral arteries. The former supply blood to the heart, whereas the latter bring blood to the brain. Macrovascular disease is best minimized, however, with good control of serum cholesterol and blood pressure. Thus, a diabetic must control not only blood sugar but also serum cholesterol and blood pressure to reduce the likelihood of vascular complications. Rigorous control of glucose is more likely achieved with multiple subcutaneous injections of insulin throughout the day to simulate physiologic conditions rather than with a single daily injection. Multiple insulin injections, proper diet, exercise, and frequent determinations of blood glucose levels at home constitute the current approach to the management of the patient with type 1 diabetes. In some cases oral hypoglycemic medications (typically used in type 2 diabetes) are added as part of the medical management of patients with type 1 diabetes. These drugs may enhance the action of injected insulin. However, multiple insulin injections can more readily lead to low blood sugar (hypoglycemia); severe hypoglycemia (insulin shock) constitutes a medical emergency. The disease is controlled by replacement of the hormone insulin; however, insulin injections are not a cure for diabetes. All patients with IDDM remain dependent on insulin for their entire lives. Studies are now in progress to assess the efficacy of nasal preparations of insulin; to monitor the transplantation of insulin-producing beta cells to control blood glucose in humans; and to determine if stem cell infusions into animals will reverse diabetes. If these approaches are successful, some patients may be spared from life-time injections.
An increasing number of patients with type 1 diabetes are now entering insulin pump therapy. The patient must still monitor blood sugar levels by testing several times a day. The insulin pump is external and approximately the size of a pager; it delivers insulin through plastic tubing placed under the skin. The patient programs the pump to deliver small amounts of rapid-acting insulin on the hour over a 24-hour period according to the patient’s metabolic needs. Thus the pump can maintain even more rigorous, predictable control of blood sugar levels than multiple insulin injections. Insulin dosage with the pump is also lower than with multiple insulin injections, making life-threatening hypoglycemia less frequent. Very recent advances in technology now include replaceable blood glucose sensors in the pump. These sensors monitor blood glucose levels and have an alarm to tell the patient when glucose levels are too low or too high. However, the blood glucose sensors do not tell the pump how much insulin to automatically deliver to the patient. The patient must still deliver the insulin from the pump because the pump still lacks “a brain.” Frequent blood sugar testing is still necessary. With further advances in pump technology, the sensor may tell the pump if the blood sugar is too high and then the pump might automatically deliver the right amount of insulin to match the blood sugar for that patient. Such improvements in pump design would then “close the loop,” and possibly represent the technological equivalent of a cure for diabetes. The patient with diabetes who uses insulin pump therapy should carry a backup supply of syringes in case the pump fails to deliver insulin; such failure can lead to the rapid development of ketoacidosis, resulting in signs and symptoms of nausea, abdominal cramps, disorientation, and fatigue.
Noninsulin-Dependent Diabetes Mellitus
The second type (type 2 diabetes) is noninsulin-dependent diabetes mellitus (NIDDM). Increased insulin resistance, rather than profound insulin deficiency, is characteristic of type 2 diabetes. Approximately 95% of all diabetic patients have type 2 diabetes. The onset of this type of diabetes is gradual and usually occurs in patients who are 35 to 40 years of age or older. When the metabolic rate starts to slow down with age, on comes the contributing factor of weight gain. However, there is now an epidemic of type 2 diabetes among children in major U.S. cities, particularly in minority neighborhoods; this epidemic has significant social, cultural, and ethical dimensions. Poor, high-crime neighborhoods in the inner cities restrict control of free space; people are less likely to get out and exercise; this may contribute to obesity. Hence, where you live may be an even more important determinant in developing type 2 diabetes than a person’s genetic make-up. Fast-food companies also target their advertisements to the minority neighborhoods where less expensive but high-caloric food is a strong inducement—this is an ethically objectionable practice because it causes harm. Children are thus likely to succumb to pressures from other children and eat high caloric foods. Studies have shown that second- and third-generation individuals whose parents were born in countries with a low diabetes rate ultimately approximate the diabetes rate in the United States. The Western diet is “obesogenic.” The urban minority populations tragically bear the brunt of diabetes in the United States and suffer from its myriad life-threatening complications. Dentists and dental hygienists can play a major role in educating their patients about diabetes and oral health and, in doing so, advance public health.
Obesity is a common finding in many people with type 2 diabetes, and therefore, this form of diabetes may be preventable. Obesity probably decreases the number of receptors for insulin binding in sensitive tissues such as fat and muscle, thereby leading to the development of the diabetic state. Hormones from fatty tissue (adipokines) may also contribute to insulin resistance. Complications are less common in this type of diabetes than in type 1 diabetes. However, the onset of type 2 diabetes among children is of extreme concern because life-threatening and debilitating complications may occur in young adulthood at the active peak of life. Some patients achieve control of blood glucose levels with diet and weight reduction alone, whereas others require oral hypoglycemic agents. These medications also lower blood glucose levels but, unlike insulin, are not given by injection. However, some patients with type 2 diabetes require insulin injections to obtain control of blood glucose levels. In April 2005 the Food and Drug Administration approved Byetta, an injectable product for the treatment of type 2 diabetes; it was made available to pharmacies in June 2005. Byetta is not insulin. It is delivered subcutaneously (like insulin) at a fixed dose before the morning and evening meals. Byetta lowers blood sugar and has the potential to help restore the response of the body’s insulin-producing cells. Hypoglycemia is also less frequent than with insulin administration and occurs when patients are taking only a specific type of oral medication. This relatively new drug represents a significant advance in the management of type 2 diabetes for patients who cannot control their blood sugar by past conventional therapy.
Clinical Features
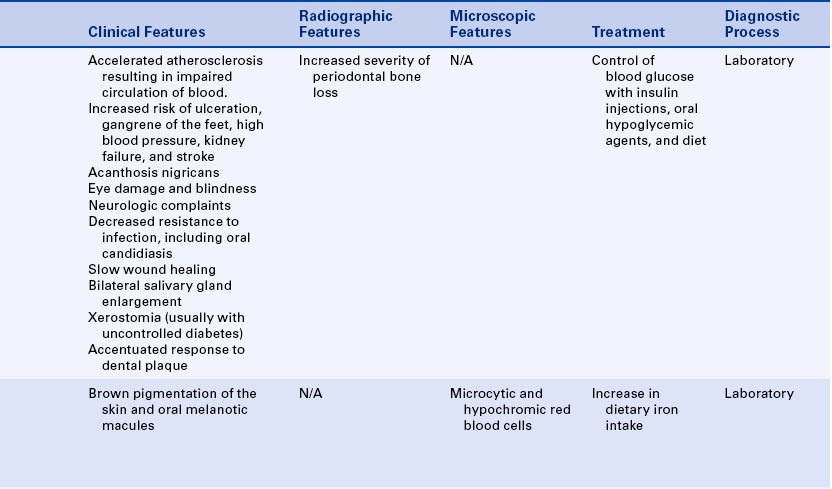
The vascular system is the most severely affected system in diabetes, leading to a myriad number of devastating systemic complications. Accelerated atherosclerosis (thickening of the blood vessel wall from fibrofatty plaques), is a common complication of diabetes leading to impaired circulation of blood and impaired transport of oxygen and nutrients to tissues. Heart attack caused by atherosclerosis of the coronary arteries is the most common cause of death among patients with diabetes. This blood vessel disease also increases the risk of ulceration and gangrene of the feet, high blood pressure, kidney failure, and stroke. Gangrene of the lower extremities is about 100 times more common in patients with diabetes than in the general population. Blood vessel changes in the eye (diabetic retinopathy, microvascular, or small artery disease) can lead to hemorrhage, which can result in blindness. The nervous system can also be affected in diabetes. This is partly the result of vascular damage and results in a variety of neurological complaints such as numbness or tingling in the fingers and toes. A patient with frost-bite, for example, may have little or no feeling in the fingers or toes. In such instances, the frost-bite may lead to death of tissue, necessitating amputation of fingers or toes. Decreased resistance to infection is seen, particularly in uncontrolled diabetes. Skin infections, especially furuncles (boils), urinary tract infections, and tuberculosis are common.
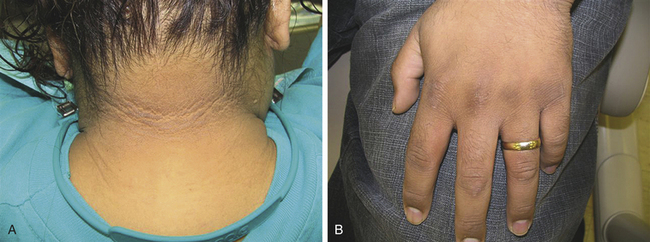
A skin disorder called acanthosis nigrans has been reported to be associated with type 2 diabetes mellitus and has been suggested to be a useful clinical indicator in screening for type 2 diabetes. Obesity in children and adults appears to increase the risk of development of this skin condition. Acanthosis nigricans is characterized by hyperpigmented, velvety-textured plaques that appear symmetrically distributed in folds and creases of the body. Acanthosis nigricans affecting the neck (Figure 9-3, A) and hands (Figure 9-3, B) may be identified by the dental hygienist during physical/clinical evaluation of a patient.
Oral Complications
The oral complications of diabetes are most severe when blood glucose levels are not controlled. In some patients control is difficult, even with careful monitoring of these levels and insulin injections. These patients are said to have brittle diabetes and may benefit from recent advances with insulin pump therapy.
Increased colonization of the oral mucosa by Candida albicans and an increased prevalence of oral candidiasis have been reported in patients with diabetes mellitus, as has mucormycosis, a rare fungal infection that affects the palate and maxillary sinuses. These infections generally are seen in poorly controlled or uncontrolled diabetes mellitus. (Both oral candidiasis and mucormycosis are described in Chapter 4.) The presence of such fungal infections is indicative of compromised innate and acquired immune responses that occur in diabetes mellitus.
Bilateral, asymptomatic parotid gland enlargement occurs in some patients; this results from either a deposition of fat or hypertrophy of the salivary gland tissue.
Xerostomia (dry mouth) is usually associated with uncontrolled diabetes mellitus. Dehydration of the oral tissues can result, increasing the risk of the development of oral candidiasis and dental caries, and may diminish taste sensation. Altered subgingival flora has been described in diabetes and may be the result of immunologic or salivary changes. Other significant oral findings include burning mouth syndrome, which may or may not be related to xerostomia. Burning mouth or tongue has been reported to occur in undiagnosed cases of type 2 diabetes. These may mostly resolve after medical diagnosis of the diabetes and subsequent treatment toward improving blood sugar control. Xerostomia can be a physically and psychologically debilitating condition.
Patients with diabetes mellitus have an accentuated response to plaque. The gingiva can be hyperplastic and erythematous, and acute and fulminating gingival abscesses can occur. Excessive periodontal bone loss, tooth mobility, and early tooth loss can also be associated with diabetes mellitus (Figure 9-4). Periodontal disease is considered to be a significant complication of diabetes. Slow wound healing and increased susceptibility to infection occur as a result of the immunologic changes and defective collagen production.

FIGURE 9-4 Periapical radiograph of a patient with diabetes mellitus shows severe alveolar bone loss.
The patient with diabetes who is receiving good medical management and whose glucose levels are controlled can receive any indicated dental treatment. Early identification of oral infections is important. Infection aggravates diabetes because it often results in the loss of blood glucose control, thus creating a vicious cycle because susceptibility to infection is increased. Therefore elimination of infection is extremely important in patients with diabetes. Antibiotic medication, calculus and plaque removal, effective oral hygiene care, and adequate nutrition are especially important in the management of the patient with diabetes. One final point deserves mention here. People with well-controlled diabetes of either type can lead long, productive lives. However, diabetes control is not an “in-between.” A patient either controls his or her diabetes, or does not—there is also no such thing as “mild” diabetes. Good control of diabetes represents a synthesis of effort between the physician, nurse, nutritionist, dentist, and dental hygienist. It is truly a team effort.
ADDISON DISEASE
Addison disease, also known as primary adrenal cortical insufficiency, is characterized by an insufficient production of adrenal steroids. A malignant tumor or tuberculosis may be responsible for destruction of the adrenal gland. However, in most cases the cause of the destruction of the adrenal cortex is unknown. In these patients the condition may be an autoimmune disease. Another known common cause is the spread of tuberculosis infection to the adrenal gland.
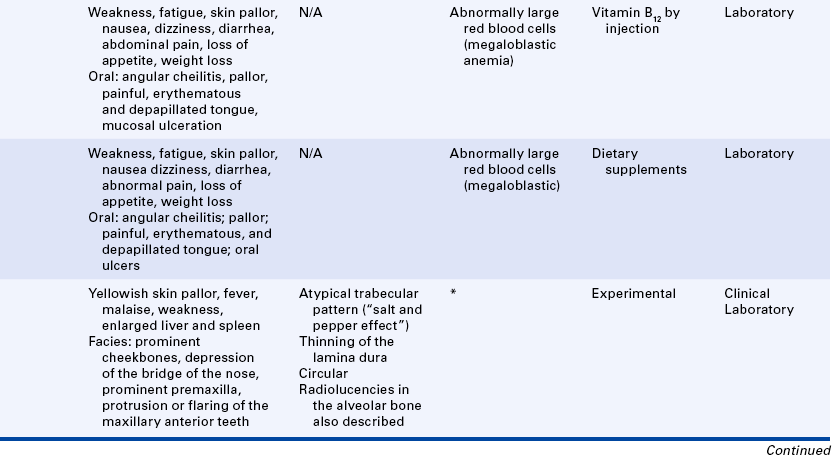
As a result of the decreased production of adrenal steroids, the pituitary gland increases its production of adrenocorticotropic hormone, which would normally increase the production of adrenal steroids. This hormone is similar to melanin-stimulating hormone and causes stimulation of melanocytes. Brown pigmentation (bronzing) of the skin occurs, and melanotic macules can develop on the oral mucosa. Treatment of Addison disease involves steroid replacement therapy.
BLOOD DISORDERS
The complete blood count (CBC) is important in the diagnosis of blood disorders. The CBC is a series of tests that examines the red blood cells, white blood cells, and platelets. It provides information about the number of each type of cell, the ratio of types of cells, and the appearance of the cells. The information included in a CBC and normal values are included in Box 9-1.
DISORDERS OF RED BLOOD CELLS AND HEMOGLOBIN
Anemia is defined as a reduction in the oxygen-carrying capacity of the blood that in most cases is related to a decrease in the number of circulating red blood cells. There are many different types and causes of anemia.
Nutritional anemias occur when a substance necessary for the normal development of red blood cells is in scant supply in the bone marrow. The most common deficiencies are of iron, folic acid, or vitamin B12. These deficiencies can occur when the intake of the nutrient is insufficient or when disorders of absorption prevent its uptake. Anemia can also occur when suppression of the bone marrow stem cells takes place, resulting in an inability of the bone marrow to produce red blood cells.
Oral manifestations are similar for all types of anemia and include skin and mucosal pallor, angular cheilitis, erythema and atrophy of the oral mucosa, and loss of filiform and fungiform papillae on the dorsum of the tongue. Circumvallate papillae and foliate papillae are not affected.
Iron Deficiency Anemia
Iron deficiency anemia occurs when an insufficient amount of iron is supplied to the bone marrow for red blood cell development. This type of anemia can occur as a result of a deficiency of iron intake, blood loss from heavy menstrual bleeding or chronic gastrointestinal bleeding, poor iron absorption, or an increased requirement for iron as in pregnancy or infancy.
The Plummer-Vinson syndrome can develop as a result of long-standing iron deficiency anemia. This syndrome includes dysphagia (difficulty swallowing), atrophy of the upper alimentary tract, and a predisposition to the development of oral cancer.
Clinical Features and Oral Manifestations
Iron deficiency anemia is most often asymptomatic. Nonspecific symptoms such as weakness and fatigue can occur. Oral mucosal signs in severe cases include angular cheilitis; pallor of the oral tissues; and an erythematous, smooth, painful tongue (Figure 9-5). The changes in the oral mucosa occur as a result of a lack of nutrients to the epithelium. The filiform papillae on the dorsum of the tongue disappear first because they have the highest metabolic requirements. Disappearance of the fungiform papillae can also occur in chronic and severe cases.

Diagnosis and Treatment
The diagnosis of iron deficiency anemia is made by laboratory tests, which show a low hemoglobin content of red blood cells and a reduced hematocrit value. Iron is needed for hemoglobin synthesis; therefore in iron deficiency anemia the red blood cells appear smaller than normal (microcytic) and lighter in color than normal (hypochromic). Increasing the intake of iron is the treatment for iron deficiency anemia; dietary supplements are usually used. The oral lesions resolve when the deficiency is corrected.
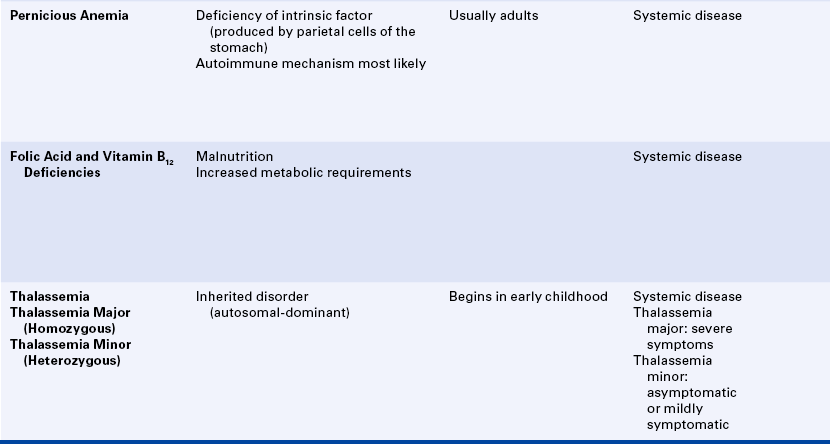
Pernicious Anemia
Pernicious anemia is a vitamin B12 deficiency that is caused by a deficiency of intrinsic factor, a substance secreted by the parietal cells of the stomach. Intrinsic factor is necessary for the absorption of vitamin B12. Normally vitamin B12 is transported across the intestinal mucosa by intrinsic factor. An autoimmune mechanism is the most likely cause of pernicious anemia. Antibodies to components of gastric mucosa have been identified in patients with pernicious anemia. Other causes include surgical removal of the stomach (gastrectomy), gastric cancer, or gastritis. Vitamin B12 is needed for deoxyribonucleic acid (DNA) synthesis; when it is lacking, the development of rapidly dividing cells such as bone marrow cells and epithelial cells is affected.
Clinical Features and Oral Manifestations
The clinical signs of pernicious anemia are weakness, pallor, and fatigue on exertion. Other constitutional signs can include nausea, dizziness, diarrhea, abdominal pain, loss of appetite, and weight loss. Neurologic changes such as severe paresthesia may also occur in patients with pernicious anemia.
Oral manifestations of pernicious anemia include angular cheilitis; mucosal pallor; painful, atrophic and erythematous mucosa; mucosal ulceration; loss of papillae on the dorsum of the tongue; and burning and painful tongue (Figure 9-6).

Diagnosis and Treatment
The diagnosis of pernicious anemia is made by laboratory testing. The diagnostic features include low serum vitamin B12 levels and gastric achlorhydria (lack of hydrochloric acid). Pernicious anemia is a megaloblastic anemia. Megaloblastic anemia is characterized by red blood cells that are immature, abnormally large, and have nuclei (megaloblasts). Immature neutrophils and platelets are also seen in both the bone marrow and the circulating blood. The Schilling test, which detects an inability to absorb an oral dose of vitamin B12 (cyanocobalamin), is another method used to diagnose pernicious anemia. Treatment consists of injections of vitamin B12. The oral mucosa improves in time, but the papillae on the dorsum of the tongue may not regenerate completely.
Folic Acid and Vitamin B12 Deficiency Anemia
Dietary deficiencies of folic acid and vitamin B12 can result in anemia and can occur in association with malnutrition and increased metabolic requirements. Malnutrition can occur in association with alcoholism, and pregnant women can experience a deficiency because of increased metabolic demands. Folic acid and vitamin B12 are essential for DNA synthesis.
Diagnosis and Treatment
The diagnosis of these anemias is based on laboratory test results that include serum assays of folic acid and vitamin B12. These are also megaloblastic anemias. Thus, as in pernicious anemia, the red blood cells are immature, abnormally large, and nucleated (megaloblasts). Treatment involves dietary supplements.
Thalassemia
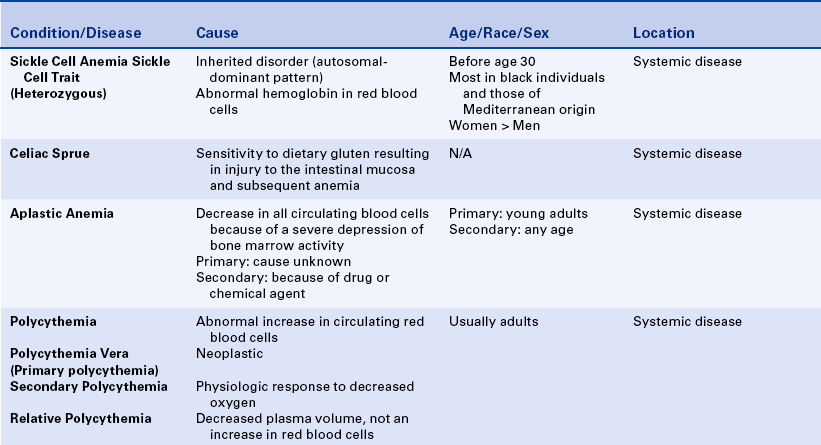
Thalassemia, also called Mediterranean or Cooley anemia, is the name of a group of inherited disorders of hemoglobin synthesis. It has an autosomal inheritance pattern; no predilection for either sex is seen. The heterozygous form (see Chapter 6), in which only one gene at a locus is involved, is called thalassemia minor and can be asymptomatic or only mildly symptomatic. The homozygous form, in which the genes on both chromosomes are involved, is called thalassemia major and is associated with severe hemolytic anemia, which results from damage to the red blood cell membranes and destruction of the red blood cells.
Clinical Features and Oral Manifestations
The severe form of the disease begins early in life. The child has a yellowish skin pallor, fever, malaise, and weakness. An enlarged liver and spleen are common. The characteristic facies includes prominent cheekbones, depression of the bridge of the nose, an unusual prominence of the premaxilla, and protrusion or flaring of the maxillary anterior teeth. Intraoral radiographs show a peculiar trabecular pattern of the maxilla and mandible. There is a prominence of some trabeculae and a blurring and disappearance of others, resulting in a “salt and pepper” effect. Thinning of the lamina dura and circular radiolucencies in the alveolar bone have also been described.
Sickle Cell Anemia
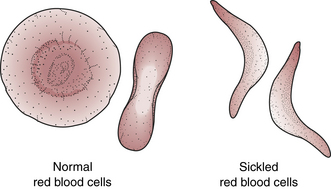
Sickle cell anemia is an inherited disorder of the blood that is found predominantly in black individuals and those of Mediterranean origin. Persons who are heterozygous for the disease are generally asymptomatic. This is called sickle cell trait. Those who are homozygous are much more severely affected. The disease presents before age 30 years. Sickle cell anemia occurs as a result of an abnormal type of hemoglobin in red blood cells. Because of this abnormal hemoglobin, the cells develop a sickle shape in the presence of decreased oxygen; hence the name sickle cell anemia. Exercise, exertion, administration of a general anesthetic, pregnancy, or even sleep can trigger a sickling of the red blood cells. Because of the change in their shape, the red blood cells are no longer able to pass through small blood vessels and are destroyed more rapidly than normal.
Clinical Features and Oral Manifestations
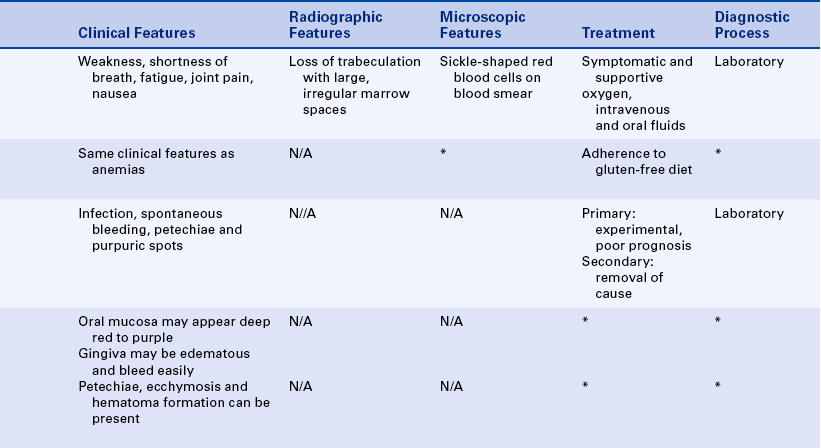
The patient with sickle cell anemia experiences weakness, shortness of breath, fatigue, joint pain, and nausea. Oral manifestations are seen on dental radiographs (Figure 9-7). A loss of trabeculation takes place, with the appearance of large, irregular marrow spaces. This change is most prominent in the alveolar bone. Changes in the skull have been described as a hair-on-end pattern because the trabeculae radiate outward.

Diagnosis and Treatment
The sickle-shaped cells are seen on a blood smear (Figure 9-8). The number of red blood cells is usually low, as is the hemoglobin content. Management of sickle cell anemia is largely symptomatic and supportive and involves the administration of oxygen and intravenous and oral fluids. Sickle cell anemia can result in profound changes of the heart such as enlargement and lead to cardiac failure.
Celiac Sprue
Celiac sprue is a chronic disorder associated with sensitivity to dietary gluten, a protein found in wheat and wheat products. When gluten is ingested, there is injury to the intestinal mucosa. Malabsorption of other nutrients such as vitamin B12 and folic acid occurs because of mucosal injury. As a result, anemia and the oral and clinical signs associated with it develop.
Aplastic Anemia
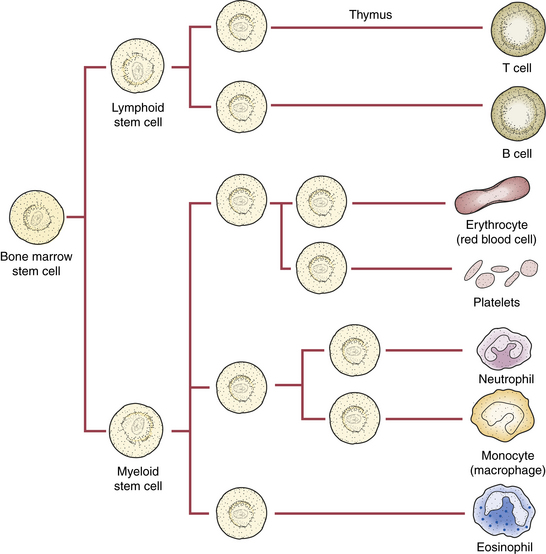
In aplastic anemia patients experience a dramatic decrease in all the circulating blood cells (pancytopenia) because of a severe depression of bone marrow activity. All the blood cells are produced in the marrow (Figure 9-9). The cause of primary aplastic anemia is unknown. In secondary aplastic anemia the bone marrow failure is a result of a drug or chemical agent. Chemotherapy, radioactive isotopes, radium, and radiant energy have been associated with the development of aplastic anemia. Primary aplastic anemia occurs most frequently in young adults.
Oral Manifestations
These are related to the generalized decrease in white blood cells and platelets and include infection, spontaneous bleeding, petechiae, and purpuric spots (Figure 9-10).

Diagnosis and Treatment
In both forms of aplastic anemia a generalized decrease of circulating blood cells occurs. In addition to anemia, leukopenia (a decrease in white blood cells) and thrombocytopenia (a decrease in platelets) occur. White blood cells are essential in the defense against infection (see Chapters 3 and 4), and platelets are essential in the clotting of blood. Primary aplastic anemia is usually progressive and fatal. Treatment of secondary aplastic anemia involves removing the cause.
Polycythemia
Polycythemia is characterized by an increase in the number of circulating red blood cells. This increase can be either absolute or relative. Normal red blood cell production is carefully regulated and involves both the precursor cells in the bone marrow and the hormone erythropoietin, which is produced by the kidney.
Types of Polycythemia
The three forms of polycythemia are (1) polycythemia vera (primary polycythemia), (2) secondary polycythemia, and (3) relative polycythemia.
Polycythemia Vera (Primary Polycythemia): In polycythemia vera a neoplastic proliferation of bone marrow stem cells results in an abnormally high number of circulating red blood cells. The production of red blood cells is uncontrolled. The cause of this disorder is unknown. It is somewhat more common in men than in women, and the age of onset is usually between 40 and 60 years. It is generally seen in white individuals and is extremely rare in black individuals. The symptoms of polycythemia vera include headache, dizziness, and itching of the skin (pruritus). The increase in red blood cells leads to impaired blood flow, vascular stasis, and poor circulation. The formation of thrombi can cause a disruption of the blood supply to the brain, heart, or peripheral vessels. A decrease in platelets (thrombocytopenia) can occur because of the disruption of the marrow from which they are derived.
Secondary Polycythemia: In secondary polycythemia the increase in red blood cells is caused by a physiologic response to decreased oxygen. A decrease in oxygen in the blood triggers an increase in erythropoietin by the kidneys, which results in increased production of red blood cells. A number of factors can cause a decrease in oxygen, including pulmonary disease, heart disease, living at high altitudes, and an elevation in carbon monoxide. The increase in carbon monoxide has been associated with tobacco smoking.
Relative Polycythemia: This is caused by a decreased plasma volume and not an increase in red blood cells. In acute forms the cause is usually easily recognized. Causes of acute relative polycythemia include diuretic use, vomiting, diarrhea, or excessive sweating. A chronic form of relative polycythemia has been called stress polycythemia. Most patients with this type of polycythemia are middle-age white men who are under physiologic stress, mildly overweight, hypertensive, and heavy smokers. The risk of cerebrovascular accidents (stroke) and myocardial infarction (heart attack) is increased in these patients.
Oral Manifestations
The oral mucosa in patients with polycythemia may appear deep red to purple, and the gingiva may be edematous. The gingiva may bleed easily, and submucosal petechiae, ecchymosis, and hematoma formation can be present. There can be excessive bleeding after oral surgical procedures. Abnormalities of the oral mucosa result from an increase in circulating red blood cells, the impaired blood flow, and thrombocytopenia.
Diagnosis and Treatment
Diagnosis of the different forms of polycythemia involves laboratory testing and measurement of the hemoglobin content and the hematocrit. Treatment is related to the type of polycythemia and may include removal of causative factors, chemotherapy, and phlebotomy (bloodletting). Oral lesions generally do not require local treatment; however, patients tend to have increased bleeding after oral surgery.
DISORDERS OF WHITE BLOOD CELLS
Three groups of white blood cells are found in the circulation: granulocytes, lymphocytes, and monocytes. The three types of granulocytes are polymorphonuclear leukocytes (neutrophils), eosinophils, and basophils. The primary function of the neutrophils is to defend the body against foreign invaders such as bacteria, viruses, and fungi (described in Chapter 4). These cells are produced primarily in the bone marrow and are released into the circulating blood (see Figure 9-9). Their response to infection is known as the inflammatory response (see Chapter 2).
Agranulocytosis
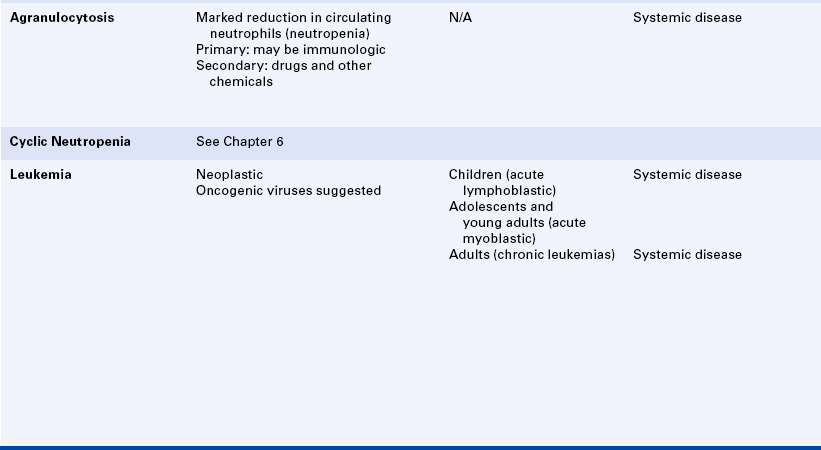
In agranulocytosis a significant reduction in circulating neutrophils occurs (leukopenia), which has serious consequences. Any of the white blood cells can be involved, but leukopenia most commonly involves the neutrophils. A reduction in the number of circulating neutrophils is called neutropenia.
Agranulocytosis can result from either a problem in the development of neutrophils or a problem in accelerated destruction of neutrophils. Primary and secondary forms of agranulocytosis have been described. The cause of the primary form is unknown and may be an immunologic disorder. The secondary form of agranulocytosis is most commonly produced by drugs and other chemicals. Secondary agranulocytosis is most commonly seen in women.
Clinical Features and Oral Manifestations
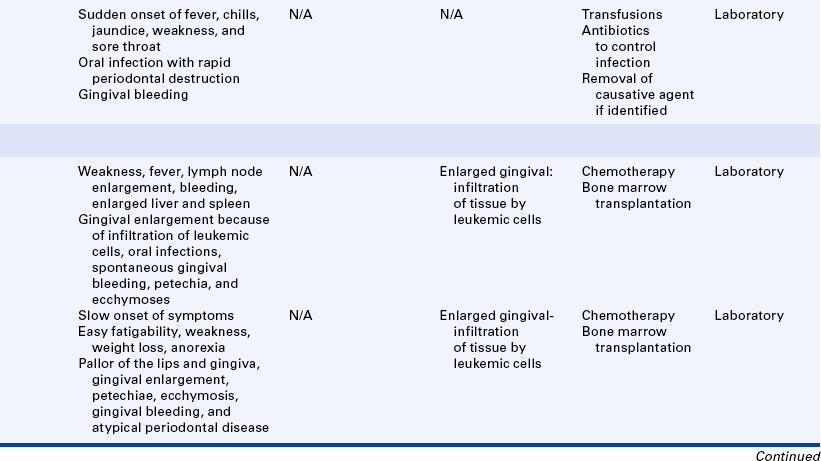
Clinically patients experience a sudden onset of high fever, chills, jaundice (icterus), weakness, and sore throat. Orally the most characteristic feature is the presence of infection. Necrotizing ulcerations, excessive bleeding from the gingiva, and rapid destruction of the supporting tissue of the teeth have been described. Regional lymphadenopathy can accompany the oral problems.
Diagnosis and Treatment
The diagnosis is made by laboratory testing. The white blood cell count, which is normally 5000 to 10,000 cells/mm3, is dramatically reduced to less than 1000 cells/mm3. Treatment includes transfusions; antibiotics to control infection; and, in the secondary form, removal of the causative agent. Infections can become overwhelming and cause death. All surgical procedures, including dental hygiene procedures, are contraindicated.
Cyclic Neutropenia
Cyclic neutropenia is a form of agranulocytosis. A severe depression of granulocytes (neutrophils) occurs at periodic intervals. Cyclic neutropenia is described in detail in Chapter 6.
Leukemia
Leukemias are malignant neoplasms of the hematopoietic (blood-forming) stem cells. They are disorders that primarily originate in the bone marrow. The most dramatic feature of leukemias is the excessive number of abnormal white blood cells in the circulating blood. The pathogenesis is unknown. However, current investigations are focusing on oncogenic viruses (see Chapter 7). Many different types of leukemias exist. They are classified by the cell type involved and the maturity of the neoplastic cells (Box 9-2). Leukemias are described in this chapter with other abnormalities of blood. They also have been included in Chapter 7, together with other white blood cell neoplasms. Many different types of leukemias are known; this text gives only an overview of the two general categories, acute and chronic, with focus on the oral manifestations. The student is encouraged to use other texts for a more complete description of leukemias. Oral lesions are most common in acute leukemias but may also occur in chronic forms.
Acute leukemias
Acute leukemias are characterized by the presence of very immature cells (blast cells) and by a rapidly fatal course if not treated. They can involve immature lymphocytes (acute lymphoblastic leukemia) or immature granulocytes (acute myeloblastic leukemia). Acute lymphoblastic leukemia primarily affects children and young adults and has a good prognosis. Acute myeloblastic leukemia involves adolescents and young adults (age range 15 to 39 years), and the prognosis is not as good. The onset of acute leukemia is sudden and dramatic.
Clinical Features: Clinically patients experience weakness, fever, enlargement of lymph nodes, and bleeding. The lymph node enlargement can include cervical lymphadenopathy (enlargement of the lymph nodes in the neck) and is typically seen earlier in the course of disease, with the leukemias involving immature lymphocytes. A general loss of cells produced by the bone marrow occurs. The fatigue mainly results from anemia, the fever from infection, and the bleeding from a decrease in platelets (thrombocytopenia). In advanced disease enlargement of the spleen (splenomegaly) and liver (hepatomegaly) occurs when these organs are infiltrated by the leukemic cells.
Oral Manifestations: Oral manifestations can include gingival enlargement (which can be severe) caused by infiltration of leukemic cells (Figure 9-11) and oral infections (including acute necrotizing ulcerative gingivitis because white blood cells are not functioning). In addition, if a decrease in platelets occurs, bleeding gums, petechiae, and ecchymoses may be present. Toothache as the result of invasion of the pulp by leukemic cells has been reported.

Diagnosis And Treatment: In acute leukemia laboratory findings include an elevated white blood cell count with the presence of many immature cells, anemia, and a low platelet count. In young children with acute lymphocytic leukemia, the prognosis with treatment is very good. In adolescents and adults with acute myelocytic leukemia the prognosis is poor. Remissions occur with chemotherapy, and then relapses occur. Bone marrow transplantation is a treatment for this form of leukemia.
Chronic Leukemias
In addition, several different types of chronic leukemias exist. They are all characterized by a slow onset, and they all primarily affect adults. The disease can be present for months before a diagnosis is made, and occasionally the diagnosis is made during a routine physical examination based on laboratory testing. One of the forms of chronic leukemia, chronic myeloid leukemia, is associated with a distinctive chromosomal abnormality, the Philadelphia chromosome. Another form of chronic leukemia, chronic lymphocytic leukemia, is the most common form and accounts for about one quarter of the total cases of leukemia. It may be asymptomatic for a long time. About half the patients with this type of leukemia have abnormal karyotypes; however, the abnormality is different from the Philadelphia chromosome.
Clinical Features and Oral Manifestations: The clinical onset is slow. The symptoms are nonspecific and include easy fatigability, weakness, weight loss, and anorexia. Oral manifestations include pallor of the lips and gingiva, gingival enlargement, petechiae and ecchymosis, gingival bleeding, and atypical periodontal disease. Cervical lymphadenopathy may be an early manifestation of chronic leukemia.
Diagnosis and Treatment: The white blood cell count can increase to 500,000/mm3, and most of the total cells can be leukemia cells. Remissions occur with chemotherapy; however, they are of short duration, and the long-term prognosis is poor. Bone marrow transplantation is used to treat both chronic and acute leukemia.
BLEEDING DISORDERS
Patients with bleeding disorders can have one of a number of different defects.
Hemostasis (the cessation of bleeding) is a complex process that involves a number of events (Figure 9-12). When a blood vessel is damaged, marked constriction of the vessel (vasoconstriction) occurs in an attempt to stop the flow of blood. Platelets (thrombocytes) that are produced by the bone marrow and circulating in blood adhere to the damaged surface and aggregate to form a temporary clot. To stop the bleeding permanently, it is necessary for fibrin to be produced. Fibrin tightly binds the aggregating platelets to form a clot. A cascade of circulating plasma proteins that are made almost exclusively in the liver and called clotting factors or coagulation factors is necessary to convert the precursor fibrinogen to fibrin (Table 9-1; Figure 9-13).
Table 9-1
Factors Involved in Coagulation∗
| Factor Name | Name |
| I | Fibrinogen |
| II | Prothrombin |
| III | Tissue factor |
| IV | Calcium ions |
| V | Proaccelerin |
| VII | Proconvertin |
| VIII | Antihemophilic factor |
| IX | Plasma thromboplastin |
| X | Stuart factor |
| XI | Plasma thromboplastin antecedent |
| XII | Hageman factor |
| XIII | Fibrin-stabilizing factor |
∗Factors are numbered in the order in which they were discovered and not in the order in which they function. (No factor VI is included.)
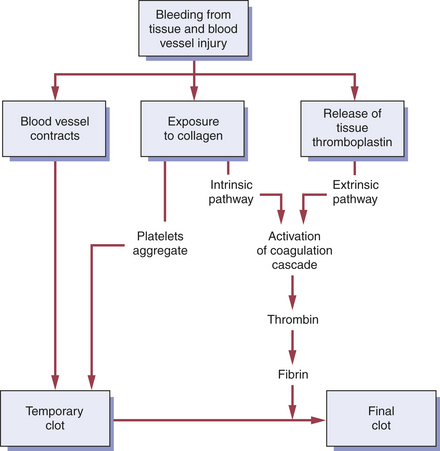
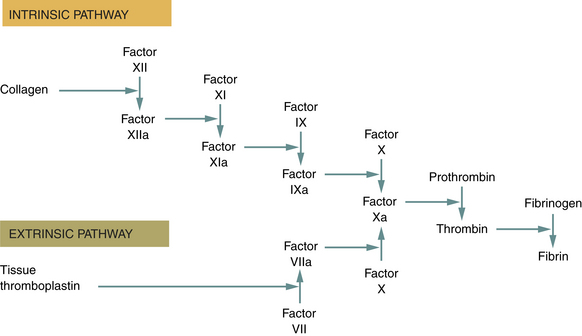
FIGURE 9-13 Coagulation cascade. Coagulation factors remain inactive until needed. As each coagulation factor becomes activated (a), it is responsible for the activation of another factor until all have been activated and the final clot is formed. The two pathways by which this cascade is activated are the intrinsic and extrinsic pathways.
Finally, anti-clotting mechanisms are activated to prevent the spread of more clots and to allow the clot to dissolve so that the damaged vessel can be repaired. This complexity is necessary to prevent inappropriate clotting. Successful hemostasis depends on the walls of the blood vessels, adequate numbers of functioning platelets, and adequate levels of properly functioning clotting factors.
Defects in hemostasis are caused by abnormalities of either platelets or coagulation factors. These defects can be diagnosed with a few laboratory tests (Table 9-2). Normal values may differ according to the specific test used and the individual laboratory.
Table 9-2
Laboratory Tests for Hemostasis
| Test | Normal Values |
| Platelet count (number of platelets) | 150,000-400,000/mm3 |
| Bleeding time (platelet function) | 1-6 minutes∗ |
| Prothrombin time (fibrin clot formation—extrinsic pathway) | 11-16 seconds∗ |
| Partial thromboplastin time (fibrin clot formation—intrinsic pathway) | 25-40 seconds∗ |
∗Normal values may differ according to the specific test used and the individual laboratory.
Platelet Count
The platelet count, which is usually requested with a CBC, provides a quantitative or numeric evaluation of platelets. A normal platelet count should be 150,000 to 400,000/mm3. A platelet count less than 100,000/mm3 is considered thrombocytopenia. Spontaneous gingival bleeding can occur when a patient’s platelet count is less than 20,000/mm3. In addition, a physician can request specific clotting factor assays, which can also be performed in patients with suspected or known clotting factor deficiencies. Nearly all bleeding disorders are caused by abnormalities of either platelets or clotting factors. Rarely bleeding disorders result from capillary fragility or weakness of the blood vessel walls.
Bleeding Time
The bleeding time provides an assessment of the adequacy of platelet function, not platelet number. The test measures how long it takes a standardized skin incision to stop bleeding by the formation of a temporary hemostatic plug or clot. The normal range of bleeding time depends on the way the test is performed but is usually between 1 and 6 minutes. The bleeding time is prolonged, or greater than 5 to 10 minutes, in patients with platelet abnormalities. Aspirin can also prolong the bleeding time but has no effect on the platelet count.
Prothrombin Time
The prothrombin time (PT) measures the patient’s ability to form a clot. It is performed by measuring the time it takes for a clot to form when calcium and a tissue factor are added to the patient’s plasma. A normal PT is usually between 11 and 16 seconds. The value is usually compared with a normal control, which is generated daily by the laboratory using standardized plasma. A prolonged or greater than normal PT can be associated with postoperative bleeding because of abnormal clot formation. A prolonged PT is usually not associated with bleeding unless it is longer than 1.5 times the control. Most often physicians use PT to monitor anticoagulant therapy (as in coumarin or warfarin sodium) for preventing myocardial infarction. A more accurate determination of PT is the international normalized ratio (INR), an expression of the ratio of PT to thromboplastin activity. The INR is more accurate because it is standardized from laboratory to laboratory. Values less than 3.0 are considered within normal range. Patients on anticoagulants such as warfarin may have INR values of 4 to 5.
Partial thromboplastin time
The partial thromboplastin time (PTT) also measures the effectiveness of clot formation. Two different pathways exist by which clot formation occurs. PT measures one of these, and PTT measures the other. The test is performed by measuring the time it takes for a clot to form after the addition of kaolin, a surface-activating factor, and cephalin, a substitute platelet factor, to the patient’s plasma. A normal PTT is usually 25 to 40 seconds. Prolongation of the PTT to 45 to 50 seconds can be associated with mild bleeding problems. With further prolongation (more than 50 seconds) severe bleeding can occur. PTT is also used by physicians to monitor heparin therapy, which is commonly used for kidney hemodialysis in patients with renal failure.
Purpura
Purpura is a reddish-blue or purplish discoloration of the skin or mucosa that results from spontaneous extravasation of blood. It can be caused by a defect or deficiency in blood platelets or an increase in capillary fragility. A significant oral clinical finding is the oozing of blood at the gingival margins in several sites without the presence of gingivitis or inflammation. Petechiae, ecchymoses, and hemorrhagic blisters can also be present.
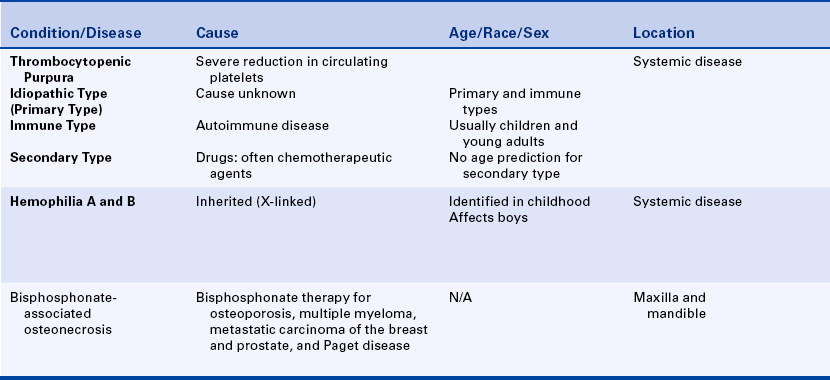
Thrombocytopenic Purpura
Thrombocytopenic purpura is a bleeding disorder that results from a severe reduction in circulating platelets. The normal platelet level is 150,000 to 400,000/mm3 of blood. Spontaneous bleeding occurs when platelet levels fall to less than 20,000/mm3. When the cause is unknown, the condition is called idiopathic thrombocytopenic purpura. An autoimmune type of process has been identified for thrombocytopenia; therefore it is sometimes called immune thrombocytopenia. The condition can also be secondary to an existing disease or condition. Secondary thrombocytopenic purpura is often associated with drugs, including those used for cancer chemotherapy. The idiopathic or primary form is usually seen in young patients, with the greatest incidence occurring before the age of 10 years. No age predilection for the secondary type and no sex predilection for either type are seen.
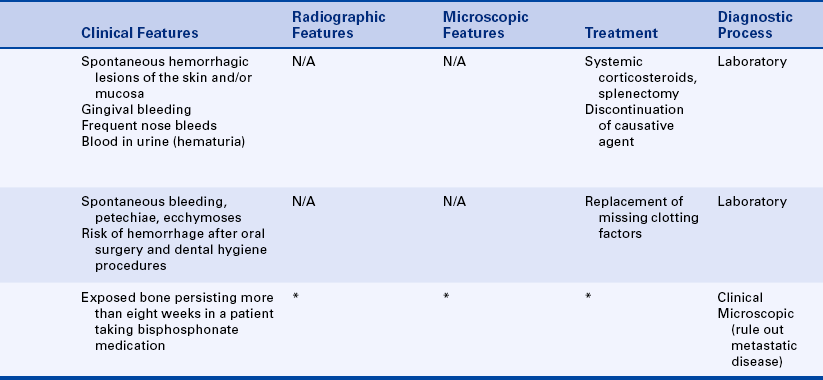
Clinical and Oral Manifestations: Clinically spontaneous purpuric or hemorrhagic lesions of the skin develop that can vary in size and severity. In addition, these patients bruise easily, can have blood in the urine (hematuria), and have frequent nosebleeds (epistaxis). Oral manifestations include spontaneous gingival bleeding and clusters of petechiae or purpuric spots.
Diagnosis and Treatment: Laboratory tests show a significant decrease in platelets. Bleeding time can be prolonged to an hour or more, and the capillary fragility test result is positive. Treatment depends on the cause and includes transfusions, corticosteroids, and splenectomy. Any dental surgical procedure, including scaling, is contraindicated until laboratory test results confirm sufficient improvement in the patient’s bleeding problem.
Nonthrombocytopenic Purpura
Nonthrombocytopenic purpuras are bleeding disorders that can result from either a defect in the capillary walls or disorders of platelet function. Vascular wall alterations occur in vitamin C deficiency and infections and can also result from chemicals and allergy. Many factors can cause disorders of platelet function, including drugs, allergy, and autoimmune disease. By far the most common reason for a prolonged bleeding time is the ingestion of drugs that affect platelet function. Ingestion of small doses of aspirin (0.3 to 1.5 g) produces an impairment of platelet function for 7 to 10 days. The nonsteroidal antiinflammatory drugs (e.g., ibuprofen, naproxen, indomethacin) can also adversely affect platelet function. Patients with kidney failure and those with leukemia can have impaired platelet function. von Willebrand disease is one of the most common inherited disorders of bleeding in humans. In most cases, it is transmitted as an autosomal-dominant disorder of platelet function. There are several autosomal-recessive variants that have been identified. Both men and women may be affected with this disorder.
Hemophilia
Hemophilia is a disorder of blood coagulation that results in severely prolonged clotting time. The problem results from a deficiency of one of the plasma proteins involved in the coagulation cascade that is necessary for the conversion of fibrinogen to fibrin (see Figure 9-12).
Types of Hemophilia
The two most common types of hemophilia are type A and type B. These types of hemophilia are inherited as X-linked recessive traits and therefore are transmitted through an unaffected carrier and occur in males and in homozygous females. The carrier mother may have a mildly prolonged coagulation time. (Inheritance patterns, including sex-linked inheritance, are described in Chapter 6.)
Type A hemophilia is the classic and most common type and is caused by a deficiency of the clotting factor called plasma thromboplastinogen or factor VIII. This deficiency is characterized by severe hemorrhage after even mild-to-moderate injury or surgery. Type B, or Christmas disease, is less common. The clotting defect is in plasma thromboplastin or factor IX.
IMMUNODEFICIENCY
Immunity is described in Chapter 3. Immunodeficiency can involve the different parts of the immune system either alone or together. It can involve the cell-mediated (T-cell) response or the humoral (B-cell or antibody) response. Deficiencies in phagocytosis can also be considered deficiencies in immunity. Immunodeficiency diseases are divided into primary and secondary immunodeficiencies. Primary immunodeficiencies are those of genetic origin; secondary immunodeficiencies result from some other underlying disorder. The signs and symptoms that occur in a person with immunodeficiency depend on the degree of the deficiency and the type of immune response involved. The most common complication arising in persons with either primary or secondary immunodeficiency is infection. The type of infection is related to the type of immunodeficiency. Individuals with deficiency in humoral immunity are more likely to develop bacterial infections; those with deficiency in cell-mediated immunity are more likely to develop viral infections, fungal infections, and infections by intracellular bacteria such as tuberculosis. Autoimmune diseases and neoplasm may also be associated with certain immune deficiencies.
PRIMARY IMMUNODEFICIENCIES
Primary immunodeficiencies are immunodeficiencies of genetic origin and can involve B cells, T cells, or both. These primary immunodeficiencies have provided much information about the functions of the different immunologic responses and are extremely rare.
Three examples are included here. The first is Bruton disease, also called X-linked congenital agammaglobulinemia (lack of immunoglobulins), which is a disorder in which B cells do not mature. Plasma cells are deficient throughout the body; T cells are normal. Autoimmune diseases are common in these patients.
The second example is DiGeorge syndrome, which is also called thymic hypoplasia. It is a disorder in which the thymus is deficient or lacking; therefore T lymphocytes do not mature. Infants and children with this syndrome are extremely susceptible to fungal and viral infections and bacterial infections that require T- and B-cell cooperation. B lymphocytes and immunoglobulins are not affected.
The third example is severe combined immunodeficiency. Most infants with this type of immunodeficiency die within the first year of life and are vulnerable to all forms of viral, fungal, and bacterial infections.
SECONDARY IMMUNODEFICIENCIES
Secondary immunodeficiencies are those that occur as a result of an underlying disorder. They are much more common than the primary immunodeficiency disorders. Disorders that can have accompanying immunodeficiency include malnutrition, which can lead to inadequate synthesis of antibodies; viral infection; cancer; renal diseases in which antibodies are excreted abnormally; and Hodgkin’s disease. They can also occur with the use of immunosuppressive drugs, including corticosteroids; drugs that are used, along with radiation, to suppress the immune system in organ and bone marrow transplantation and to treat autoimmune diseases; and drugs used for cancer chemotherapy. Table 9-3 lists some of the most common drugs that can cause immunodeficiency and the reasons they are generally used. Acquired immunodeficiency syndrome, which occurs as a result of infection with the human immunodeficiency virus (HIV), is an example of a secondary immunodeficiency. HIV infection is described in detail in Chapter 4. With the emergence of combination regimens of antiretroviral therapy, HIV infection is now a chronic illness amenable to treatment.
Table 9-3
Examples of Drugs That Can Cause Immunosuppression
| Name | Use |
| Azathioprine | Prevention of rejection of renal transplantsTreatment of rheumatoid arthritis |
| Cyclosporine | Prevention of rejection of renal transplants |
| Cyclophosphamide | Cancer chemotherapy |
| Methotrexate | Cancer chemotherapy |
| Prednisone | Treatment of autoimmune diseases (such as rheumatoid arthritis, pemphigus vulgaris, Behçet syndrome, lupus erythematosus) |
ORAL MANIFESTATIONS OF THERAPY FOR ORAL CANCER
Oral cancer can be treated by surgery, radiation therapy, chemotherapy, or any combination of the three. Radiation therapy and chemotherapy can result in the development of several different oral manifestations.
RADIATION THERAPY
During radiation therapy the patient often experiences mucositis (Figure 9-14), which begins about the second week of therapy and subsides a few weeks after its completion. The mucositis is painful and appears as erythematous and ulcerated mucosa. Difficulty in eating, pain on swallowing, and loss of taste can occur as a result of the mucositis. If the radiation affects the major salivary glands, irreversible salivary gland destruction can occur, resulting in severe xerostomia. As a result, the mucosal tissues are easily irritated, and the patient is prone to the development of rampant caries (Figure 9-15) and oral candidiasis. Pilocarpine hydrochloride taken during the course of radiation treatment decreases the severity of radiation-induced xerostomia. A patient who has received radiation therapy for oral cancer is also at risk for the development of osteoradionecrosis (necrosis of bone from radiation therapy) because of the decreased blood supply to the bone after radiation therapy. Osteoradionecrosis develops in the mandible more frequently than in the maxilla, and the risk for its development does not decrease with time.

Patients for whom head and neck radiation is planned should have an oral evaluation before the initiation of radiation therapy. Potential sources of oral infection should be eliminated, and teeth for which the prognosis is questionable should be removed. The role of the dental hygienist in the management of patients receiving head and neck radiation treatment expected to result in xerostomia involves fluoride application both by the dental hygienist and the patient, patient education in oral hygiene care, and frequent follow-up appointments to ensure patient compliance.
Saliva substitutes can be used by the patient for symptomatic relief of xerostomia.
CHEMOTHERAPY
The complications of cancer chemotherapy are predictable and differ for the various types of chemotherapy used. Mucositis and oral ulceration are frequent complications because drugs used for cancer chemotherapy affect rapidly dividing cells and therefore the basal cells of the epithelium. The epithelium becomes atrophic and ulcerated with minor irritation. Cells of the bone marrow are also affected; therefore a decrease in all blood cells (red blood cells, white blood cells, and platelets) can result. The patient can experience anemia because of a decrease in red blood cells, is at increased risk for opportunistic infections (e.g., candidiasis) because of a decrease in white blood cells, and is at increased risk for bleeding problems because of a decrease in the number of platelets.
Before the initiation of cancer chemotherapy, the patient should receive an oral evaluation to identify and eliminate any source of oral infection that may exacerbate during the course of chemotherapy.
EFFECTS OF DRUGS ON THE ORAL CAVITY
Many drugs can cause changes in the oral tissues. Xerostomia can be caused by drugs used to control blood pressure. Antianxiety medications, antipsychotic medications, and antihistamines can also cause xerostomia (Figure 9-16). Drugs such as prednisone that suppress the immune system can increase the risk of candidiasis and other oral infections (Figure 9-17). Antibiotics can also increase the risk of candidiasis. Tetracycline taken when teeth are forming can cause tooth discoloration (Figure 9-18). Phenytoin (Dilantin) and nifedipine (Procardia) can cause gingival enlargement (Figure 9-19). Cyclosporine, an immunosuppressant drug used to prevent rejection of transplanted organs, can also cause gingival enlargement.


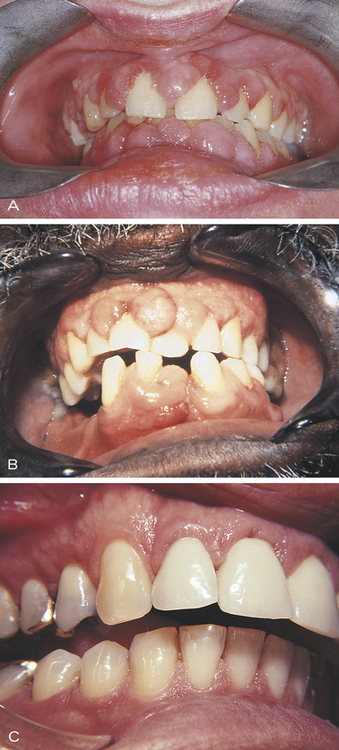
FIGURE 9-19 Drug-induced gingival hyperplasia. A, Gingival enlargement caused by phenytoin (Dilantin). B and C, Gingival hyperplasia caused by nifedipine (Procardia). (A courtesy Dr. Edward V. Zegarelli; B and C courtesy Dr. Victor M. Sternberg.)
The complete medical history should include a listing of the medications taken by a patient and is useful in establishing the diagnosis of drug-induced oral lesions.
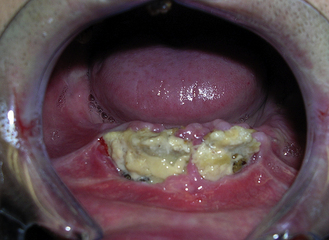
Recently, osteonecrosis of the maxilla and mandible associated with bisphosphonate therapy has been reported. (Figure 9-20). Intravenous bisphosphonate therapy has been used in patients with multiple myeloma and in patients with metastatic carcinoma of the breast and prostate to prevent tumor-associated bone destruction. The drug may also act against tumor cells. Bisphosphonate therapy is used experimentally in patients with Paget disease, and oral bisphosphonate therapy is used to treat osteoporosis. The American Academy of Oral and Maxillofacial Surgery has defined bisphosphonate-associated osteonecrosis (BON) as exposed, necrotic bone in the maxillofacial region that has persisted for more than 8 weeks in a patient with current or previous treatment with a bisphosphonate and no history of radiation therapy to the jaws. Intravenous bisphosphonate therapy is associated with a higher risk for the development of osteonecrosis of the jaws than oral bisphosphonate therapy. Local factors associated with this condition in patients on bisphosphonate medications include dentoalveolar surgery, history of inflammatory dental disease, and trauma to areas such as tori and exostoses where minimal soft tissue protects the bone. At present, there is no well-defined treatment for this condition. The medication remains in the bone for many years and therefore, discontinuation of the medication is not indicated to prevent or manage the condition.
Greenberg, M.S., Glick, M., Ship, J.A. Burket’s oral medicine, ed 11. Hamilton: BC Decker; 2008.
Little, J.W., et al. Dental management of the medically compromised patient, ed 7. St Louis: Mosby; 2008.
Neville, B.W., et al. Oral and maxillofacial pathology, ed 3. St Louis: Saunders; 2009.
Sciubba, J.J., Regezi, J.A., Jordan, R.C.K. Oral pathology: clinical-pathologic correlations, ed 5. Philadelphia: Saunders; 2007.
Vinay Kumar, V., Abbas, A.K., Nelson, F. Robbins and Cotran pathologic basis of disease, ed 7. Philadelphia: Saunders; 2005.
Wynn, R.L., Meiller, T.F., Crossley, H.L. Drug information handbook for dentistry, ed 14. Hudson, Ohio: Lexi-Comp; 2008.
Avcu, N., et al. The relationship between gastric-oral Helicobacter pylori and oral hygiene in patients with vitamin B12-deficiency anemia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:166.
Centers for Disease Control and Prevention. Iron deficiency—United States, 1999-2000. MMWR Morb Mortal Wkly Rep. 2002;51:89.
Chavez, E.M., et al. A longitudinal analysis of salivary flow in control subjects and older adults with type 2 diabetes. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:166.
Collin, H., et al. Oral symptoms and signs in elderly patients with type 2 diabetes mellitus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90:299.
Fletcher, P.D., Scopp, I.V., Hersh, R.A. Oral manifestations of secondary hyperparathyroidism related to long-term hemodialysis therapy. Oral Surg Oral Med Oral Pathol. 1977;43:218.
Garg, A.K., Malo, M. Manifestations and treatment of xerostomia and associated oral effects secondary to head and neck radiation therapy. J Am Dent Assoc. 1997;128:1128.
Guggenheimer, J., et al. Insulin-dependent diabetes mellitus and oral soft tissue pathologies. I. Prevalence and characteristics of non-candidal lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:564.
Guggenheimer, J., et al. Insulin-dependent diabetes mellitus and oral soft tissue pathologies. II. Prevalence and characteristics of Candida and candidal lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;89:570.
Hardin, D.S. Screening for type 2 diabetes in children with acanthosis nigricans. Diabetes Educ. 2006;32:547.
Hess, L.M., et al. Factors associated with osteonecrosis of the jaw among bisphosphonate users. Am J Med. 2008;121:475.
Inokuchi, T., Sano, K., Kamingo, M. Osteoradionecrosis of the sphenoid and temporal bones in a patient with maxillary sinus carcinoma: a case report. Oral Surg Oral Med Oral Pathol. 1990;70:278.
Khocht, A., Schneider, L.C. Periodontal management of gingival overgrowth in the heart transplant patient: a case report. J Periodontol. 1997;68:1140.
Kong, A.S., et al. Acanthosis nigricans and diabetes risk factors: prevalence in young persons seen in southwester US primary care practices. Ann Fam Med. 2007;5:202.
McDonough, R.J., Nelson, C.L. Clinical implications of factor XII deficiency. Oral Surg Oral Med Oral Pathol. 1989;68:264.
Miranda, J., et al. Prevalence and risk of gingival enlargement in patients treated with nifedipine. J Periodontol. 2001;72:605.
Moore, P.A., et al. Type 1 diabetes mellitus and oral health: assessment of periodontal disease. J Periodontol. 1999;70:409.
Moore, P.A., et al. Type 1 diabetes mellitus and oral health: assessment of coronal and root caries. Community Dent Oral Epidemiol. 2001;29:183.
Moore, P.A., et al. Type 1 diabetes mellitus, xerostomia and salivary flow rates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;92:281.
Ohishi, M., et al. Acute gingival necrosis caused by drug-induced agranulocytosis. Oral Surg Oral Med Oral Pathol. 1988;66:194.
Redding, S.W., Luce, E.B., Boren, M.W. Oral herpes simplex virus infection in patients receiving head and neck radiation. Oral Surg Oral Med Oral Pathol. 1990;69:578.
Ruggiero, S.L., et al. Osteonecrosis of the Jaws and Bisphosphonate Therapy. J Dent Res. 2007;86:1013.
Sreebny, L.M., Valdini, A., Yu, A. Xerostomia. II. Relationship to nonoral symptoms, drugs and diseases. Oral Surg Oral Med Oral Pathol. 1989;68:419.
Vernillo, A.T. Diabetes mellitus: relevance to dental treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:263.
Vernillo, A.T. Dental considerations for the treatment of patients with diabetes mellitus. J Am Dent Assoc. 2003;134:24S.
Wahlin, Y.B. Effects of chlorhexidine mouth rinse on oral health in patients with acute leukemia. Oral Surg Oral Med Oral Pathol. 1989;68:279.
Wu, J., Fantasia, J.E., Kaplan, R. Oral manifestations of acute myelomonocytic leukemia: a case report and review of the classification of leukemias. J Periodontol. 2002;73:664.
Kleinfield NR: Diabetes and its awful toll quietly emerge as a crisis, The New York Times, January 9, 2006, pp A1, A18-A19.
Kleinfield NR: Living at an epicenter of diabetes: defiance and despair, The New York Times, January 10, 2006, pp A1, A20-A21.
Urbina I: In the treatment of diabetes, success often does not pay, The New York Times, January 11, 2006, pp A1, A22-A23.
Santora M: East meets west, adding pounds and peril, The New York Times January 12, 2006, pp A1, A22-A23.
REVIEW QUESTIONS
1. Hyperpituitarism results from an excessive production of growth hormone. Which of the following most often causes it?
2. Hyperthyroidism in children can lead to:
3. Hypercalcemia, hypophosphatemia, and abnormal bone metabolism are characteristic of which of the following conditions?
4. All of the following are chronic complications of diabetes mellitus except:
5. Polydipsia, polyuria, and polyphagia are all characteristic of which of the following?
6. Which of the following is not a feature of type 2 diabetes mellitus?
A Those with it have increased insulin resistance.
B It occurs at 40 years of age or older.
C Autoimmunity is the key to its development.
D Glucose control can be achieved without daily insulin injections in many cases.
7. Which of the following oral complications is not associated with diabetes mellitus?
8. Which one of the following is false concerning Addison disease?
A It is also known as primary adrenal cortical insufficiency.
B It is characterized by an insufficient production of adrenal steroids.
C It may be caused by a malignant tumor that destroys the adrenal gland.
D It is a condition in which the pituitary adenoma destroys the adrenal gland.
9. Which of the following statements is false regarding diabetes mellitus?
A Candidiasis may be indicative of compromised immunity in a patient with diabetes.
B Insulin pump therapy may lead to more predictable control of blood sugar.
C Hypoglycemic agents are more commonly used in the treatment of type 2 diabetes than in type 1 diabetes.
D Diabetes mellitus is not appropriately considered a syndrome.
10. Which of the following statements is false?
A Primary immunodeficiencies are less common than secondary immunodeficiencies.
B Persons with T-lymphocyte deficiencies are susceptible to viral and fungal infections.
C All primary immunodeficiencies are combined B-lymphocyte and T-lymphocyte deficiencies.
D Secondary immunodeficiency can result from corticosteroid medication.
11. Iron deficiency anemia can be caused by:
13. Achlorhydria, failure to absorb vitamin B12, and megaloblastic anemia are characteristic features of which of the following?
14. Which one of the following is not a characteristic of sickle cell anemia?
A It is an inherited blood disorder found predominantly in blacks.
B It occurs as a result of an abnormal type of hemoglobin and decreased oxygen in the red blood cells.
C The individual with sickle cell anemia can experience weakness, fatigue, and joint pain.
15. Which of the following is characterized by a decrease in platelets?
16. Secondary aplastic anemia can be caused by:
17. Which of the following is characterized by an abnormal increase in circulating red blood cells?
18. Leukopenia most often involves which cell type?
19. If a patient’s white blood cell count is 1000/mm3, the patient has:
20. Excessive numbers of abnormal white blood cells are characteristic of:
21. Normal bleeding time is usually between:
22. The normal prothrombin time is:
23. The international normalized ratio is:
A An expression of the ratio of prothrombin time to thromboplastin activity.
B More accurate than the prothrombin time because it is standardized from laboratory to laboratory.
24. Symptoms of leukemia can be similar to those found in:
25. Which of the following is not characteristic of primary hyperparathyroidism?