ALTERATIONS OF THE REPRODUCTIVE SYSTEMS



Alterations of the reproductive system span a wide range of concerns, from delayed sexual development and suboptimal sexual performance to structural and functional abnormalities. Many common reproductive disorders carry potentially serious physiologic or psychologic consequences. Sexual or reproductive dysfunction, such as impotence or infertility, can dramatically affect self-concept, relationships, and overall quality of life. Conversely, organic and psychosocial problems, such as alcoholism, depression, situational stressors, chronic illness, and medications, can affect ovulation and menstruation, sexual performance, and fertility and may be risk factors for the development of some types of reproductive tract cancers.1 Prostate cancer is the second leading cause of cancer death in men, breast cancer is the second leading cause of cancer death in women. Diagnosis and treatment of reproductive system disorders are complicated because of the stigma and symbolism associated with the reproductive organs and the emotion-laden beliefs and behaviors related to reproductive health. Treatment and diagnosis for related problems may be delayed because of embarrassment, guilt, fear, or denial.
ALTERATIONS OF SEXUAL MATURATION
The process of sexual maturation, or puberty, is marked by the development of secondary sexual characteristics, rapid growth, and, ultimately, the ability to reproduce. A variety of congenital and endocrine disorders can disrupt the timing of puberty, or sexual maturation. These disorders may cause puberty to occur too late (delayed puberty) or too early (precocious puberty). Both types involve a disrupted onset of sex hormone production by the gonads.
Although there are conflicting and inconsistent reports, the age of pubertal onset appears to be decreasing for girls.2 This earlier onset appears primarily in breast development not age of menarche. There is little change in the age of puberty for boys. On average breast development begins at age 10.4 for white girls and 9.5 years for black girls. The average age for menarche is 12.6 years for white girls and 12.2 black girls.3–5
Delayed Puberty
About 3% of children in North America experience delayed development of secondary sex characteristics.6 The first sign of puberty in girls is usually thelarche, or breast development. Thelarche should begin by the time a girl is 13 years old. Normally boys tend to mature later than girls, around 14 to 14.5 years of age. In boys the first sign is enlargement of the testes and thinning of the scrotal skin. Puberty is considered delayed if there are no clinical signs of puberty by age 13 in girls or age 14 in boys (2 standard deviation [SD] above the mean age of pubertal onset). Clinical diagnosis also can be made in the absence of menarche by age 15 or 16. Boys especially tend to be embarrassed by sexual immaturity7; therefore, early diagnosis and treatment are recommended, as well as reassurance for boys as well as girls.
In 95% of cases, delayed puberty is a physiologic delay, that is, hormonal levels are normal and the hypothalamic-pituitary-gonadal (HPG) axis is intact, but maturation is happening slowly.8 This constitutional delay tends to be familial and is much more common in boys than in girls. Physiologic delay is difficult to distinguish from isolated gonadotropin deficiency and is usually diagnosed retrospectively once pubertal progression is complete.
Delayed puberty also may be related to consequences of any chronic condition that delays bone aging (i.e., lung disease, renal failure, cystic fibrosis) (Box 23-1).6 Many clinicians recommend intervention (i.e., exogenous sex steroid administration) in physiologic cases of delayed puberty to reduce the psychologic effects (e.g., self-esteem issues, embarrassment) often associated with delayed puberty.8,9
The other 5% of cases are caused by a disruption of the hypothalamic-pituitary-gonadal axis of various etiologies (see Box 23-1).10 Human gonadal function is partially controlled by luteinizing hormone (LH) and follicle-stimulating hormone (FSH), the release of which is regulated by the pulsatile secretion of hypothalamic gonadotropin-releasing hormone (GnRH).8,10 Most recently, the G-protein–coupled receptor 54 (GPR54) has been identified as the gatekeeper gene for activation of the GnRH axis based on loss of function studies in mice and humans. GPR54 is required for the normal function of this axis, and data suggest that the ligand kisspeptin-1 may act as a neurohormonal regulator of the GnRH axis.11 The mechanisms of childhood inhibition of GnRH release and activation are poorly understood but appear to involve feedback inhibition by sex steroids and presumably other central nervous system (CNS) pathways.12 Given the myriad etiologies contributing to the occurrence of delayed puberty, a thorough evaluation should be conducted that includes physical examination and medical and family history. Such evaluation should specifically target known contributors to delayed puberty.6,8 Laboratory workup generally consists of x-ray studies for bone age, measurement of thyroid function, serum levels of prolactin and adrenal and gonadal steroids, radioimmunoassay of plasma gonadotropins, and screening for systemic disorders. Adolescents with high gonadotropin levels require a karyotype, to rule out genetic causes, and those with low levels need skull imaging (lateral skull film, computed tomography [CT], or magnetic resonance imaging [MRI]) to rule out pituitary or other CNS infiltrate or tumor.6 Treatment of delayed puberty depends on the cause; the goal of treatment is the development of secondary sex characteristics and fertility, when possible. Insufficient sex hormone secretion can be corrected by hormone replacement therapy, such as estrogen for girls and testosterone for boys.13 Idiopathic hypogonadotropic hypogonadism is treated with synthetic GnRH or sex hormone administration, or both, and may be lifelong.6,8,13
Precocious Puberty
Precocious puberty is a rare event, affecting about 1 in 10,000 girls and less than 1 in 50,000 boys. Recently, precocious puberty has been redefined as sexual maturation before age 6 in black girls or age 7 in white girls, and before age 9 in boys.3 This reflects a trend toward earlier puberty, primarily for breast development in girls (see What’s New? Precocious Puberty). All cases of precocious puberty require thorough evaluation.
Precocious puberty may be partial, complete, or mixed (heterosexual) types (Box 23-2) and can be further categorized into central (GnRH-dependent) and peripheral (GnRH-independent) (Box 23-3). Central precocious puberty is GnRH-dependent and occurs when the hypothalamic-pituitary-gonadal axis is working normally but prematurely. Besides the premature development of secondary sex characteristics, precocity causes premature closure of the epiphysis of long bones, which results in shorter stature. Central precocious puberty results from failure of central inhibition of the GnRH pulse generator (the gonadostat). The diagnosis of central precocious puberty is one of exclusion. Because a CNS lesion may be missed, children with presumed central precocious puberty require long-term surveillance. Peripheral puberty is GnRH-independent and develops when sex hormones are produced by some mechanism other than stimulation by the gonadotropins. Sex steroid–producing tumors (i.e., gonadal tumors), testotoxicosis, and exposure to exogenous sex steroids (i.e., hormonal contraceptives and environmental endocrine disruptors) are some of the causes (see Box 23-3).
Complete precocious puberty refers to the onset and progression of all pubertal features (i.e., thelarche, pubarche, and menarche).
Partial precocious puberty is the partial development of appropriate secondary sex characteristics alone or in combination. A girl with incomplete precocious puberty might undergo thelarche or pubarche and, rarely, premature menarche. Premature thelarche is seen in girls between 6 months and 2 years of age. Premature pubarche tends to occur
between ages 5 and 8 years. Premature pubarche is usually the consequence of an early increase in the adrenal androgens that leads to early growth of pubic hair and possibly a transient acceleration in growth and bone maturation that has no significant effect on timing of puberty or final height. Sparse hair growth on the genitalia, in the absence of thelarche or menarche, does not represent precocious puberty.
The diagnosis and cause of premature development are often obvious. A thorough history and physical examination are done to determine the velocity of the process and to rule out life-threatening CNS, ovarian, or adrenal neoplasms. Family occurrence helps exclude tumors. Children with precocious puberty also have a tendency toward obesity.14–16
Treatment for all forms of precocious puberty includes identifying and removing the underlying cause or administering appropriate hormones (see Boxes 23-2 and 23-3). In many cases, precocious puberty can be reversed. Management goals include diagnosing and treating intracranial disease; arresting maturation until early teen years; maximizing eventual adult height; reducing emotional problems; and providing contraception, if necessary. The most common form, central precocious puberty, is usually treated with potent GnRH agonist analogs, which induce reversible, selective suppression of the hypothalamic-pituitary-gonadal axis. Treatment does not seem to affect body composition or increase obesity in children with central precocious puberty. Because many of these children are obese and childhood obesity is predictive of morbidity in adolescence and adulthood, it is important for clinicians to include assessment and management of obesity as part of the treatment for central precocious puberty.
Mixed precocious puberty (virilization of a girl or feminization of a boy) causes the child to develop some secondary sex characteristics of the opposite sex. This condition is usually evident at birth and is rare in older children (Box 23-4).
DISORDERS OF THE FEMALE REPRODUCTIVE SYSTEM
Hormonal and Menstrual Alterations
Primary Dysmenorrhea
Primary dysmenorrhea is painful menstruation associated with the release of prostaglandins in ovulatory cycles, but not with pelvic disease. The severity of dysmenorrhea is directly related to the duration and amount of menstrual flow. Between 50% and 90% of women ages 15 to 25 years are affected, some (10% to 15%) severely enough to miss work or school. Primary dysmenorrhea usually begins with the onset of ovulatory cycles, around age 15 or 16 years. The incidence peaks in women during the late teens and early 20s, and decreases slowly thereafter.17 Secondary dysmenorrhea is related to pelvic pathology, manifests in later reproductive years, and may occur any time in the menstrual cycle.18
PATHOPHYSIOLOGY Dysmenorrhea is primarily the result of the effects of excessive endometrial prostaglandin production, enhanced by progesterone. Women with painful periods produce 10 times as much prostaglandin F (PGF2α), a potent myometrial stimulant and vasoconstrictor, as asymptomatic women. Elevated levels of prostaglandins (especially PGF2α and PGE2α) are found in endometrial fluid of dysmenorrheic women and correlate positively with pain. Compared with proliferative endometrium, secretory endometrium produces three times the amount of prostaglandins, and the discharged endometrium produces even more.19 In addition, leukotrienes heighten sensitivity of pain fibers in the uterus and vasopressin contributes to myometrial hypersensitivity, constriction of endometrial blood vessels, and resultant ischemia, endometrial bleeding, and pain caused by prostaglandins. Prostaglandins are primarily released during the first 48 hours of menstruation, when symptoms are the most intense. Women who are anovulatory because they use oral contraceptives do not have primary dysmenorrhea. Secondary dysmenorrhea results from disorders such as endometriosis, pelvic adhesions, inflammation, cervical stenosis, uterine fibroids, polyps, tumors, cysts, intrauterine devices (IUDs), or imperforate hymen. Dysmenorrhea may be more severe in women who are obese, who smoke, are nulliparous, have delayed childbearing, and are sexually inactive.20
CLINICAL MANIFESTATIONS The chief symptom of dysmenorrhea is pelvic pain associated with the onset of menses. The pain often radiates into the groin and may be accompanied by backache, anorexia, vomiting, diarrhea, syncope, and headache. The latter symptoms are caused by entry of prostaglandins and prostaglandin metabolites into the systemic circulation. Usually, the discomfort associated with primary dysmenorrhea begins shortly before the onset of menstruation and rarely persists beyond the second day.
EVALUATION AND TREATMENT Primary dysmenorrhea can be differentiated from secondary dysmenorrhea by a thorough history and pelvic examination. In women who desire contraception, dysmenorrhea may be relieved with hormonal contraceptives. Hormonal contraception stops ovulation and creates an atrophic endometrium, thereby decreasing prostaglandin synthesis and myometrial contractility. Nonsteroidal anti-inflammatory medication (e.g., ibuprofen) is the treatment of choice. Prostaglandin inhibitors work in the majority of women with primary dysmenorrhea and are most effective if started at the first sign of bleeding or cramping.21 Regular exercise and stress reduction are thought to prevent or reduce symptoms.22 Other comfort measures include local application of heat, massage, relaxation techniques, vitamin B, and magnesium supplementation, and high-frequency transcutaneous electrical nerve stimulation (TENS).23,24 Orgasm may relieve or worsen symptoms.
Amenorrhea
Amenorrhea means lack of menstruation, the most common cause of which is pregnancy. Primary amenorrhea is the failure of menarche and the absence of menstruation by age 14 years without the development of secondary sex characteristics or by age 16 years regardless of the presence of secondary sex characteristics (see p. 817 for discussion of delayed puberty). Primary amenorrhea differs from delayed puberty in that most cases of delayed puberty require only reassurance, but when the diagnosis of primary amenorrhea is reached, a thorough evaluation must be undertaken. Secondary amenorrhea is the absence of menstruation for a time equivalent to three or more cycles or 6 months in women who have previously menstruated.
PATHOPHYSIOLOGY There are numerous classifications of the etiologies of primary amenorrhea. One approach to understanding the pathophysiology is through compartmentalization. Compartment IV disorders include CNS disorders, in particular hypothalamic disorders. In some of the congenital syndromes that cause primary amenorrhea, the hypothalamic-pituitary-ovarian (HPO) axis is dysfunctional. The hypothalamus is unable to synthesize GnRH, so the pituitary fails to secrete LH and FSH. Therefore, the ovary does not receive the hormonal signals that normally initiate the ovarian and endometrial changes of the menstrual cycle, and ovulation and menstruation do not occur. Because the ovarian hormones are absent, estrogen-dependent sex characteristics do not develop.
Compartment III disorders are disorders of the anterior pituitary, including tumors. Some anatomic defects of the CNS, whether congenital or acquired, impinge on the hypothalamic-pituitary unit so as to interfere with or interrupt the secretion of GnRH or FSH and LH. Examples of such defects include hydrocephalus, craniopharyngiomas, and other space-occupying lesions of the CNS (see Box 23-1). Again the target organ, the ovary, does not receive the necessary signals, and ovulation and menstruation do not occur. In some cases these lesions develop between the onset and conclusion of puberty. Therefore, skeletal growth may occur and secondary sex characteristics may develop, but sexual maturation is interrupted before menarche, which normally concludes puberty.
Compartment II disorders involve the ovary. Several genetic disorders are associated with primary amenorrhea. These include gonadal dysgenesis (Turner syndrome), androgen insensitivity syndrome (AIS), formerly known as testicular feminizing syndrome or male pseudohermaphroditism. Among all the chromosomal abnormalities of Turner syndrome (45,X/46,XX; structural X or Y abnormalities; mosaicism),25 the ovaries lack gametes and ovarian failure is complete. Without primitive gametes and follicles, follicular development and estrogen secretion cannot occur. Lack of estrogen accounts for failure of secondary sex characteristic development and amenorrhea, although there are high levels of circulating FSH and LH. In AIS, the individual is male genetically but female morphologically. The individual does not develop male genitalia because androgen receptors are absent in undifferentiated target organs. The gonads are found either in the abdomen or in the inguinal canal, and they produce both androgens and estrogens. Because target tissues lack androgen receptors but have estrogen receptors, most individuals with AIS have female external genitalia and female secondary sex characteristics. With the exception of a small vagina, internal female genitalia are absent, accounting for amenorrhea and infertility.
Compartment I disorders are anatomic defects of the outflow tract associated with primary amenorrhea. They include congenital absence of the vagina and uterus and congenital uterine hypoplasia (infantile uterus). Females without a uterus or vagina usually have normal ovarian function. Therefore, skeletal growth occurs and secondary sex characteristics develop in the proper sequence, but menstruation does not occur. In cases of uterine hypoplasia the uterus does not respond to hormonal stimulation during puberty.
CLINICAL MANIFESTATIONS The major clinical manifestation of primary amenorrhea is the absence of the menses. The cause of the amenorrhea determines whether secondary sex characteristics and height are affected.
EVALUATION AND TREATMENT Diagnosis of primary amenorrhea is based on history and physical examination. If ovarian steroid hormone levels are low, the individual has the appearance of an immature female. Physical examination may show structural or physiologic alterations. Laboratory studies may be required to document karyotype, abnormal levels of gonadotropins, and ovarian hormones. Diagnostic imaging is used to document structural abnormalities (Figure 23-1).
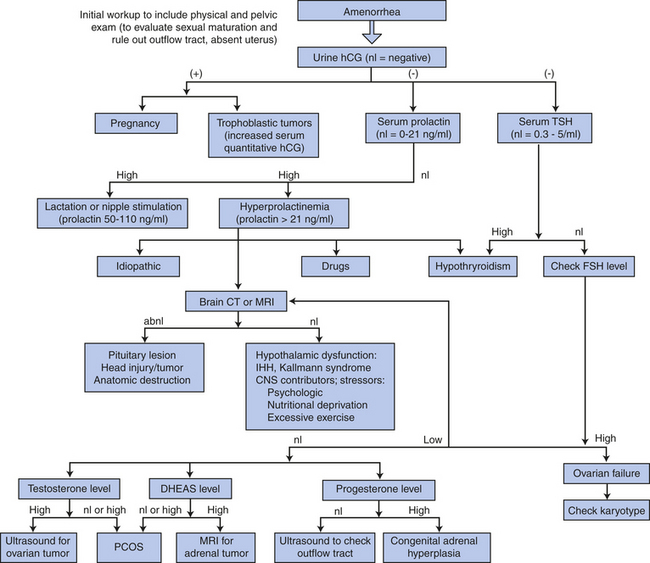
Figure 23-1 Diagnosis of amenorrhea. Pregnancy is the most common cause of amenorrhea. abnl, Abnormal; CNS, central nervous system; CT, computed tomography; DHEAS, dehydroepiandrosterone sulfate; FSH, follicle-stimulating hormone; hCG, human chorionic gonadotropin; IHH, idiopathic hypogonadotropic hypogonadism; MRI, magnetic resonance imaging; nl, normal; PCOS, polycystic ovary syndrome; TSH, thyroid stimulating hormone. (Adapted from Schorge JO et al, editors: Williams gynecology, New York, 2008, McGraw-Hill.)
Treatment involves correction of any underlying disorders and hormone replacement therapy to induce the development of secondary sex characteristics as necessary (see p. 817 for a discussion of delayed puberty). Although surgical alteration of the genitalia may be undertaken to correct structural abnormalities, surgery should be delayed until the affected individual can make a truly informed decision. Hormonal manipulation or embryo transplantation may make pregnancy possible for women with primary amenorrhea who have a uterus.
Secondary Amenorrhea
A wide variety of disorders and physiologic conditions are associated with secondary amenorrhea. Besides disease, secondary amenorrhea can be triggered by dramatic weight loss, whether the loss results from malnutrition or excessive exercise. Secondary amenorrhea is common during early adolescence and the perimenopausal period, pregnancy, and lactation. The most common causes (after pregnancy) are thyroid disorders (e.g., hypothyroidism), hyperprolactinemia, HPO interruption secondary to excessive exercise, stress, weight loss, and polycystic ovary syndrome (PCOS).
PATHOPHYSIOLOGY The causes of secondary amenorrhea are summarized in Figure 23-2. In women with normal ovarian steroid hormone levels, secondary amenorrhea may be caused by structural abnormalities (müllerian anomalies), Asherman syndrome (removal of the endometrial decidua basalis), or removal of the uterus. In women with elevated ovarian steroid hormone levels, inhibited ovulation leads to amenorrhea. An excess of ovarian hormones disrupts feedback relationships within the HPO axis, preventing ovulation. Depressed ovarian hormone levels, which are associated with a variety of clinical disorders, also cause amenorrhea by preventing ovulation. Lack of ovulation, termed anovulation, may result from increased levels of prolactin, decreased levels of gonadotropins, irregular secretion of gonadotropins, or abnormally low levels of CNS neurotransmitters (i.e., dopamine and GnRH). Any of these variables alters the feedback effects that the ovarian hormones have on the hypothalamus and pituitary.
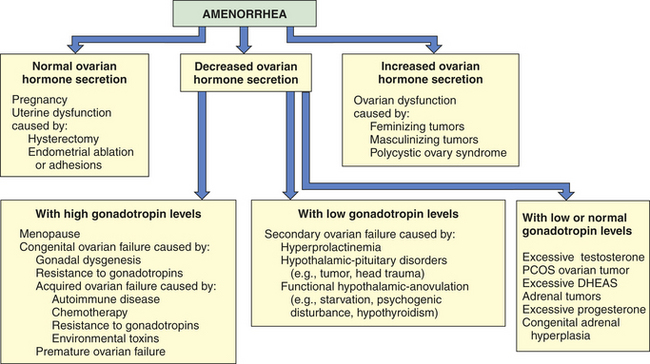
Figure 23-2 Causes of secondary amenorrhea. Of note, hypothyroidism is a relatively common condition and should be ruled out as the cause of hyperprolactinemia before more extensive evaluation (i.e., computed tomography or magnetic resonance imaging) occurs.
Hyperprolactinemia (overproduction of prolactin by the pituitary) may have indirect effects that lead to decreased secretion of GnRH by the hypothalamus. The result is a reduction in FSH and LH secretion followed by anovulation and secondary amenorrhea. It appears that elevated prolactin levels cause a compensatory increase in the secretion of dopamine, which in turn alters GnRH secretion. Anovulation thus occurs as a result of disruption in gonadotropin secretion. Feedback mechanisms in hypothyroidism cause an increased secretion of thyrotropin-releasing hormone (TRH), which binds to not only pituitary thyrotopes but also lactotropes. The subsequent increase in prolactin secretion initiates the dopamine-GnRH-gonadotropin disruption that leads to anovulation and amenorrhea.26
CLINICAL MANIFESTATIONS The major manifestation of secondary amenorrhea is the absence of menses. Infertility, vasomotor flushes, vaginal atrophy, acne, osteopenia, and hirsutism (abnormal hairiness) also may be present, depending on the underlying cause of the amenorrhea.
EVALUATION AND TREATMENT Pregnancy is the most common cause of amenorrhea and must be ruled out prior to other evaluations. Diagnosis of secondary amenorrhea involves the identification of underlying hormonal or anatomic alterations. A woman with secondary amenorrhea and normal secondary sex characteristics should have a complete history and physical examination. After ruling out pregnancy, initial evaluation includes measurement of thyroid-stimulating hormone (TSH) and prolactin levels (see Figure 23-1). Elevated prolactin levels warrant brain CT or MRI if TSH levels are normal. Hypothyroidism is treated with thyroid replacement. If the initial tests are normal, further testing would include measurement of gonadotropins (FSH), estrogen and testosterone, ultrasonography of the outflow tract and ovaries or adrenal MRI, or both. Depending on the cause of the amenorrhea, treatment may involve oral, vaginal, or injectable hormone replacement therapy19,27–29 (e.g., estrogens, thyroid hormone, glucocorticoids, gonadotropins, bromocriptine) or a corrective procedure, such as surgical removal of pituitary tumors. The American Society of Reproductive Medicine30 advises forgoing the common approach of “progesterone challenge” whereby withdrawal bleeding after administration of exogenous progestins or estrogen/progestins was thought to indicate an intact HPO axis, intact endometrium, and patent outflow tract. A diagnosis of PCOS might be treated with an insulin-sensitizing agent, such as metformin, as well as ovulation-inducing drugs if fertility is desired (a discussion of PCOS is contained on p. 824).
Abnormal Uterine Bleeding
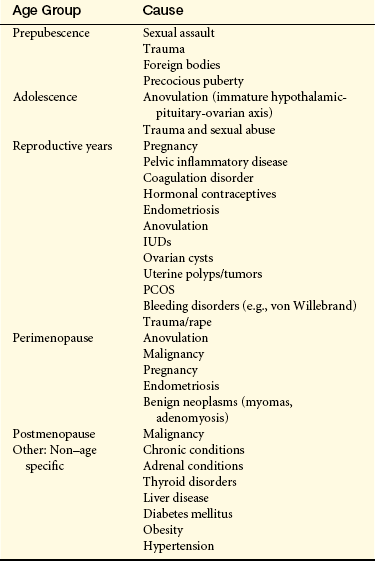
Menstrual irregularity or abnormal bleeding patterns (Table 23-1) account for approximately 33% of all gynecologic visits. Anovulatory cycles (failure to ovulate) because of various etiologies (age, stress, endocrinopathy) are the most common cause of cycle irregularity. Other causes include uterine tumors, polyps, ovarian cysts, pregnancy and its complications, and bleeding disorders (e.g., von Willebrand disease). Common causes of abnormal uterine bleeding based on age group and frequency are listed in Table 23-2. Pathophysiology and treatment options vary and are based on etiology.31
Table 23-1
| Term | Definition |
| Polymenorrhea | Cycles shorter than 3 wk; may indicate disturbance in endocrine control of ovulation |
| Oligomenorrhea | Cycles longer than 6-7 wk; may indicate disturbance in endocrine control of ovulation |
| Metrorrhagia | Intermenstrual bleeding or bleeding of light character occurring irregularly between cycles; may be a sign of organic disease |
| Hypermenorrhea | Excessive flow; may be a sign of organic disease |
| Menorrhea | Prolonged duration of flow |
| Menorrhagia | Increased amount and duration of flow |
| Menometrorrhagia | Prolonged flow associated with irregular and intermittent spotting between bleeding episodes |
Dysfunctional uterine bleeding (DUB) is heavy or irregular bleeding in the absence of organic disease, such as submucous fibroids, endometrial polyps, blood dyscrasias, pregnancy, infection, or systemic disease. The diagnosis of DUB is made once these other causes have been excluded. DUB affects 15% to 20% of all women at some time during their menstrual life and accounts for 70% of all hysterectomies and almost all endometrial ablation procedures.32 Perimenopausal women are by far the most affected by DUB.
PATHOPHYSIOLOGY More than 80% of DUB is associated with anovulatory cycles, and the remaining 20% is due to corpus luteum defects or atrophic endometrium.33 Although DUB may occur at any time during the reproductive years, 20% of cases occur in adolescents, and more than 50% of cases occur in perimenopausal women ages 40 to 50 years. Symptoms of hypomenorrhea, followed by missed periods or prolonged intervals between menses, could mark the onset of physiologic perimenopause or may be an early sign of pathologically premature ovulatory failure and secondary amenorrhea. Other conditions associated with chronic anovulation include PCOS, immaturity of the HPO axis, obesity, hyperthyroidism and hypothyroidism, and estrogen-secreting ovarian neoplasms.
DUB secondary to ovarian dysfunction is a result of either progesterone deficiency or relative estrogen excess. In perimenopausal women in their 40s and 50s, inhibin B and progesterone secretion is absent or low, yet estrogen (estradiol [E2]) continues to be secreted by the granulosa–theca cell complex, and levels are often erratic and high.34–36 (See Chapter 22 for a description of the many hormonal changes associated with the time before and just after menopause.) In the absence of growth-limiting progesterone and periodic desquamation, the endometrium attains an abnormal height with increasing hypervascularity and back-to-back glandularity, but without an intervening stromal support matrix. Menstrual flow may become irregular (metrorrhagia) and excessive (menorrhagia) or both (menometrorrhagia), resulting from the large quantity of tissue available for bleeding and the random breakdown of tissue that results in exposure of vascular channels. In the absence of adequate progesterone levels, usual endometrial control mechanisms are missing, such as vasoconstrictive rhythmicity, tight coiling of spiral vessels, and orderly collapse, and stasis does not occur. Unopposed estrogen induces a progression of endometrial responses beginning with proliferation, hyperplasia, and adenomatous hyperplasia; over a course of many years, unopposed estrogen may end with atypia and carcinoma.
DUB in ovulatory cycles is not common, and mechanisms underlying the bleeding are associated with organic lesions or corpus luteum defects.33 Excessive fibrinolytic activity and changes in prostaglandin production may be implicated.
CLINICAL MANIFESTATIONS Anovulatory DUB is characterized by unpredictable and variable bleeding in terms of amount and duration. Especially during perimenopause, dysfunctional bleeding also may involve flooding and the passage of large clots, which often indicate excessive blood loss. Excessive bleeding can lead to iron deficiency anemia and associated symptoms (fatigue, shortness of breath). Iron supplementation may be required.
EVALUATION AND TREATMENT Treatment goals include preventing or controlling abnormal bleeding, identifying underlying disease, and inducing regular menstrual cycles. Although no gold standard approach has been identified, usual therapy is hormonal and may consist of progestin-estrogen combination therapy (i.e., low-dose oral contraceptives), estrogen-only therapy (for acute episodes only), or progesterone-only therapy.31,37 For the woman with idiopathic menorrhagia not associated with anovulatory cycles, prostaglandin synthetase inhibitors may be effective in decreasing blood loss. Desmopressin, a synthetic analog of arginine vasopressin, is used to treat abnormal uterine bleeding in women with coagulation disorders (von Willebrand disease, which affects about 1% of the population).33 Recalcitrant bleeding may be controlled by suppression of the endometrium followed by surgical ablation. Total or partial ablation of the endometrium has replaced dilation and curettage (D&C) or hysterectomy as the surgical technique of choice for treatment of menorrhagia. Various techniques have been developed, including cryoablation, thermal balloon, circulated hot fluid, and electro- or microwave energy ablation.38 The best results are obtained if the endometrium is suppressed for 4 to 6 weeks with either high-dose progestin, GnRH agonist, or danazol. Endometrial ablation is successful in approximately 90% of women; only 50% become amenorrheic. The major indication for a D&C is diagnostic or as a curative procedure in the removal of products of conception, polyps, or focal endometrial hyperplasia.
More recently, the levonorgestrel-intrauterine system (LNG-IUS), a contraceptive hormonal IUD, is being used with success as effective as hysterectomy or ablation, or both, and is much less expensive. The LNG-IUS decreases blood loss by 86% to 97% by decreasing endometrial proliferation.
Polycystic Ovary Syndrome
Polycystic ovary syndrome (PCOS) has at least two of the following conditions: oligo-ovulation or anovulation, elevated levels of androgens, or clinical signs of hyperandrogenism and polycystic ovaries. Polycystic ovaries do not have to be present to diagnose PCOS, and conversely their presence alone does not establish the diagnosis. PCOS remains one of the most common endocrine disturbances affecting women, especially young women, and is a leading cause of infertility in the United States, where prevalence rates are estimated at between 4% and 12%, afflicting between 3.2 and 5.4 million young women.39 PCOS appears to be familial, and various features of the syndrome may be differentially inherited.40,41 Confusing the issue is the frequency, expression, and timing of PCOS (polycystic ovaries can be detected in prepubescent children). From 22% to 30% of women have polycystic ovaries on ultrasound, with 80% having one or more symptoms of the syndrome; 80% of women with normal ovaries also experience one or more PCOS symptoms. Signs and symptoms of women with PCOS may change over time, with metabolic syndrome becoming more prominent with age. In addition, polycystic ovaries may be associated with Cushing syndrome, acromegaly, premature ovarian failure, simple obesity, congenital adrenal hyperplasia, thyroid disease, androgen-producing adrenal tumors or ovarian tumors (Figure 23-3), and syndromes with hyperprolactinemia. Thus several factors contribute to difficulties in the diagnosis.
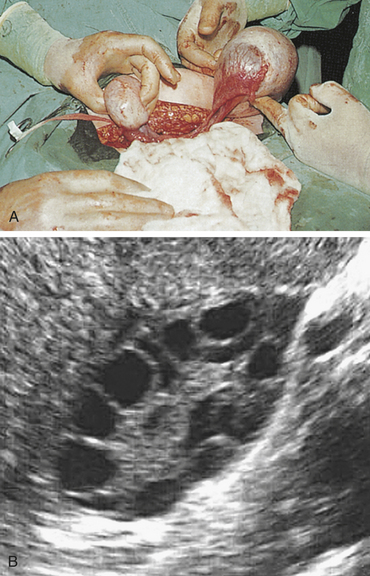
Figure 23-3 Polycystic ovary. A, Surgical view of polycystic ovaries. B, Ultrasound of polycystic ovary. (A from Symonds EM, Macpherson MBA: Diagnosis in color: obstetrics and gynecology, London, 1997, Mosby-Wolfe; B from King J: Polycystic ovary syndrome: J Midwifery Womens Health 51[6]:415-422, 2006. Reprinted with permission.)
PATHOPHYSIOLOGY Although the underlying cause of PCOS is unknown, a genetic basis is suspected. Initial identification of genes involved in steroid biosynthesis, androgen biosynthesis, and insulin receptors within the ovary indicate genetic involvement. No single factor fully accounts for the abnormalities of PCOS.41–44 A hyperandrogenic state is a cardinal feature in the pathogenesis of PCOS. However, glucose intolerance/insulin resistance (IR) and hyperinsulinemia often run parallel and markedly aggravate the hyperandrogenic state, thus contributing to the severity of signs and symptoms of PCOS.41,45 Obesity adds to and worsens IR. Although 50% of normal weight women with PCOS have IR, all obese women with PCOS do. Insulin stimulates androgen secretion by the ovarian stroma and reduces serum sex hormone–binding globulin (SHBG) directly and independently. The net effect is an increase in free testosterone levels. Excessive androgens affect follicular growth, and insulin affects follicular decline by suppressing apoptosis and enabling follicles, which would normally disintegrate, to survive46 (Figure 23-4). Further, there appears to be a genetic ovarian defect in PCOS, which makes the ovary either more susceptible to or sensitive to insulin’s stimulation of androgen production. Recent research suggests that decreased intraovarian receptors for estrogen receptor-α or insulin-like growth factor 1 (IGF-1), increased leptin levels, or direct insulin resistance within selective ovarian cells (fibroblasts) may contribute to this phenomenon.46 Intrauterine and early childhood environments may also contribute to the development of PCOS (see What’s New? Early Programming for PCOS?).
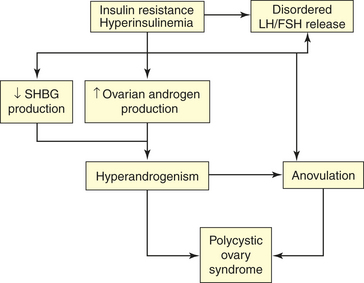
Figure 23-4 Insulin resistance and hyperinsulinemia in polycystic ovary syndrome (PCOS). See text. FSH, Follicle-stimulating hormone; LH, luteinizing hormone; SHBG, sex hormone–binding globulin.
Weight gain tends to aggravate symptoms, whereas weight loss may ameliorate some of the endocrine and metabolic events and thus decrease symptoms. Women with PCOS tend to have increased leptin levels (leptin levels are increased in thin as well as overweight women with PCOS).47 Leptin influences the hypothalamic pulsatility of GnRH and consequent interaction along the entire HPO axis. Feedback from the polycystic ovary is disturbed because of changes in ovarian steroid and nonsteroidal (inhibins and related proteins) hormones.
In PCOS there is dysfunction in follicle development.46 Inappropriate gonadotropin secretion triggers the beginning of a vicious cycle that perpetuates anovulation. Typically, levels of FSH are low or below normal and LH levels and LH bioactivity are elevated. An increased frequency of GnRH pulses appears to cause increased frequency of LH pulses.33,48 Persistent LH elevation causes an increase in androgens (dehydroepiandrosterone sulfate [DHEAS] from the adrenal glands and testosterone, androstenedione, and DHEA from the ovary). Androgens are converted to estrogen in peripheral tissues,
and increased testosterone levels cause a significant reduction (approximately 50%) in SHBG, which in turn causes increased levels of free estradiol. Elevated estrogen levels trigger a positive-feedback response in LH and a negative-feedback response in FSH. Because FSH levels are not totally depressed, new follicular growth is continuously stimulated, but not to full maturation and ovulation. The accumulation of follicular tissue in various stages of development allows an increased and relatively constant production of steroids in response to gonadotropin stimulation. Thus PCOS is characterized by excessive production of both androgen and estrogen.
Increased androgen secretion by the ovaries contributes to premature follicular failure (atresia) and persistent anovulation. In turn, persistent anovulation causes enlarged polycystic ovaries characterized by a smooth, pearly white capsule. This characteristic appearance is caused by an increase of surface area and increased volume of up to 2.8 times, doubling of growing and atretic follicles, thickening of the tunica (outermost area) by 50%, increasing cortical stromal thickening by one third and a fivefold increase in subcortical stroma, and escalating hyperplasia. With advancing age, menstrual irregularities may improve while metabolic syndrome and type 2 diabetes mellitus increases.
CLINICAL MANIFESTATIONS Clinical manifestations of PCOS usually appear within 2 years of puberty but may appear after a variable period of normal menstrual function and, possibly, pregnancy. The symptoms are related to anovulation and hyperandrogenism and include dysfunctional bleeding or amenorrhea, hirsutism, acne, and infertility. Approximately 41% of women with PCOS are obese.42 Box 23-5 contains a list of signs and symptoms, summary of hormonal disturbances, and complications of PCOS.
EVALUATION AND TREATMENT Diagnosis of PCOS is based on evidence of androgen excess, chronic anovulation, and inappropriate gonadotropin secretion. Tests for impaired glucose tolerance are recommended. As stated, polycystic ovaries do not have to be present and, conversely, their presence alone does not establish the diagnosis. Goals of treatment include reversing signs and symptoms of androgen excess, instituting cyclic menstruation, restoring fertility, and ameliorating any associated metabolic or endocrine, or both, disturbances.49,50 Traditionally, treatment of PCOS focused on correcting anovulation and the effects of hyperandrogenism with combined oral contraceptives (COCs), antiandrogens, and fertility agents. With a greater understanding of the role that insulin resistance and hyperinsulinemia play in this disease, insulin sensitizers, such as metformin,50,51 may be used to decrease insulin, prevent diabetes and heart disease (by reducing microvascular events), and restore fertility. Progesterone therapy is recommended to oppose estrogen’s effects on the endometrium and as a means to initiate monthly withdrawal bleeding (at the expense of continued hirsutism). For infertile women, clomiphene citrate, an antiestrogen, can be used to facilitate ovulation, although better effects are achieved (75% ovulation rates and 30% to 40% pregnancy rates) if therapy is combined with an insulin sensitizer.52–54 Women who are primed with human chorionic gonadotropin (hCG) before in vitro fertilization have greater success in achieving and maintaining pregnancy (58% to 82%).51 Only a small reduction of weight has shown a restoration of ovulation and increased insulin sensitivity by 71% in obese women with PCOS. Lifestyle changes are therefore encouraged, particularly weight loss and exercise. Reduction of insulin resistance by loss of abdominal fat appears crucial in restoring ovulation.49,55 For women who do not desire pregnancy, low-dose oral contraceptives may be used to suppress androgen production and hirsutism.
Premenstrual Disorders
Premenstrual syndrome (PMS) and premenstrual dysphoric disorder (PMDD) are the cyclic recurrence (in the luteal phase of the menstrual cycle) of distressing physical, psychologic, or behavioral changes that impair interpersonal relationships or interfere with usual activities.33 PMDD is listed as a mood disorder in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) (Box 23-6). The prevalence of PMS and PMDD is difficult to determine. It has been estimated that 5% to 10% of menstruating women have severe to disabling premenstrual symptoms, 3% to 8% have cyclic dysphoria warranting treatment, and 20% or more have mild to moderately distressing symptoms.56 To confuse matters, it seems that (1) symptoms are experienced to some degree by most adolescent and adult women and can occur throughout all menstrual phases, (2) the presence and severity of symptoms in any one woman may be inconsistent from month to month, (3) menstrual phase for peak symptom severity may differ depending on the population studied, and (4) inconsistent and overlapping use of terminology and criteria are used to describe these syndromes. PMDD is the term often used to refer to the premenstrual disorder with a predominant psychosocial or functional impairment similar to dysthymia and minor depression.33,57
It is thought that PMS/PMDD is the result of abnormal tissue response to the normal changes of the menstrual cycle. This biologic response may be triggered by fluctuating estrogen and progesterone levels. Given that premenstrual disorders occur almost exclusively in ovulatory cycles, it has been theorized that symptoms are triggered by the preovulatory estrogen peak or postovulatory increase in progesterone, or both.58 However, the mechanisms involved are not known. Furthermore, the neurotransmitters serotonin, gamma-aminobutyric acid (GABA), and noradrenaline may have mediating or moderating roles on symptom manifestation. These neurotransmitters have demonstrated interactions with estrogen and progesterone and all of these are neuroactive with known mood and behavior effects, including negative mood, irritability, aggression, and impulse control.33 Sex steroids also interact with the renin-angiotensin-aldosterone system (RAAS), which could explain some PMS/PMDD signs and symptoms (e.g., water retention, bloating, weight gain). A predisposition to PMS runs in families, perhaps because of genetics or shared environment. A woman’s menstrual experience tends to be similar to her mother’s or her sister’s experience. Although research is limited, further evidence supports a relationship between the severity and frequency of premenstrual symptoms and reports of low general well-being, history of major affective disorder, and personality characteristics, such as perfectionism, increased stress, poor nutrition, lack of exercise, low self-esteem, history of sexual abuse, and family conflict. In turn, when premenstrual symptoms are perceived as distressing, the quality of interpersonal relationships and self-image are negatively affected.
CLINICAL MANIFESTATIONS The pattern of symptom frequency and severity is more important than specific complaints. Nearly 300 physical, emotional, and behavioral symptoms have been attributed to PMS/PMDD. Emotional symptoms, particularly depression, anger, irritability, and fatigue, have been reported as the most prominent and the most distressing, whereas physical symptoms seem to be the least prevalent and problematic. Approximately 6% of women have classic PMS, as defined earlier, and 7% report premenstrual magnification of symptoms that occur during the entire cycle. Underlying physical or psychologic disease may be aggravated premenstrually and must be diagnosed and treated independently from PMS/PMDD.
EVALUATION AND TREATMENT Diagnosis of PMS/PMDD is based on prospective health history and symptoms. Diagnostic criteria for PMDD are presented in Box 23-7. Because the cause of PMS is not known and cannot be reduced to a single biologic explanation, and because the occurrence and severity of PMS are mediated by lifestyle and social and psychologic factors, treatment for PMS is symptomatic. Nonpharmacologic therapies, with or without medication, tend to be more effective in controlling symptoms than medication alone.
Initial treatment focuses on validation of the premenstrual experience, education on PMS and self-help techniques, and elimination of contributing factors or treatment of coexisting or underlying disorders. Individual, marriage, or family counseling; anger management and conflict resolution; and stress-reduction techniques, including biofeedback, relaxation and imagery, regular exercise, adequate rest, and time management, are recommended. Dietary changes, such as eating six small meals each day; increasing intake of complex carbohydrates, fiber, and water; and decreasing caffeine, alcohol, sugar, and animal fat can be beneficial (see Nutrition & Disease: Premenstrual Syndrome).
After a trial of nonpharmacologic therapies or if criteria for PMDD are met, medications may be added to the treatment regimen. Drugs often prescribed include vitamin and mineral supplements, selective serotonin reuptake inhibitors (SSRIs; some have been U.S. Food and Drug Administration (FDA) approved for use in PMDD), antiprostaglandins, and alprazolam. SSRIs relieve symptoms in about 60% to 90% of women and may be given continually or only during the
premenstrual period. Long-acting SSRIs, such as fluoxetine, should be tapered to prevent withdrawal symptoms. The rapid action of SSRIs suggests that it is indeed the serotonin effects as opposed to the antidepressant effects of these drugs that obtain the positive results observed with their use in PMS/PMDD treatment.56 Progesterone is often used, but has failed to show efficacy for severe PMS/PMDD in large randomized placebo controlled trials.59 However, progesterone’s muscle relaxant and sedative properties may be beneficial. Because the edema associated with PMS is a result of local fluid shifts rather than fluid retention, diuretics are not recommended.
In severe cases, menses can be abolished, which eliminates cyclic ovarian hormones and thus the biologic trigger for PMS. Elimination of menses can be accomplished with the use of oral contraceptives, medroxyprogesterone acetate, or GnRH agonists; emotional symptoms may not be relieved with the latter. In addition, if GnRH analogs are used, then continuous estrogen replacement therapy is needed because of the “medical menopause” that results.60 Of interest is that women with PMS may experience similar symptoms with synthetic hormones.61 Continuous administration of low-dose oral contraceptives for extended periods with fewer hormone-free days (3 to 4 days every 3 months) may reduce the frequency and severity of PMS/PMDD symptoms.62
Infection and Inflammation
Infections of the genital tract may result from exogenous or endogenous microorganisms. Exogenous pathogens are most often sexually transmitted (see Chapter 24). Endogenous causes of infection include microorganisms that are normally present in the vagina, bowel, or vulva. Infection occurs if these microorganisms migrate to a new location or overproliferate or if the immune system and other defense mechanisms are impaired.
A number of skin disorders can affect the vulva. They include reactive dermatitis, contact dermatitis, psoriasis, and impetigo. (For a discussion of skin disorders, see Chapter 44.) Most infectious disorders that affect the vulva and vagina are sexually transmitted, however. These disorders are described in Chapter 24.
Pelvic Inflammatory Disease
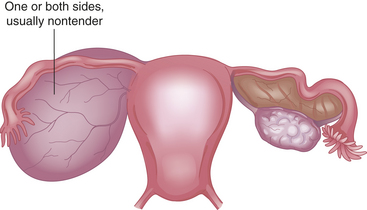
Pelvic inflammatory disease (PID) is an acute inflammatory process caused by infection (Figure 23-5). PID may involve any organ, or combination of organs, of the upper genital tract—the uterus, fallopian tubes, or ovaries—and, in its most severe form, the entire peritoneal cavity. (Inflammation of the fallopian tubes is termed salpingitis [Figure 23-6]; inflammation of the ovaries is called oophoritis.) Sexually transmitted microorganisms, such as chlamydia and gonorrhea, that migrate from the vagina to the uterus, fallopian tubes, and ovaries cause most cases of PID.
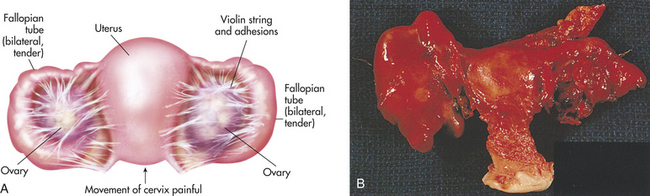
Figure 23-5 Pelvic inflammatory disease. A, Involvement of both ovaries and fallopian tubes. B, Total abdominal hysterectomy and bilateral salpingo-oophorectomy specimen showing unilateral pyosalpinx. (A from Seidel H et al: Mosby’s guide to physical examination, ed 4, St Louis, 1999, Mosby. B from Morse SA, et al: Atlas of sexually transmitted diseases and AIDS, ed 3, London, 2003, Mosby.)
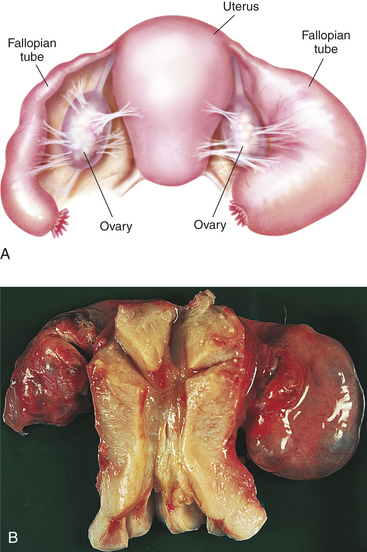
Figure 23-6 Salpingitis. A, Advanced pyosalpinx. Note the swollen fallopian tubes. B, Bilateral, retort-shaped, swollen, sealed tubes and adhesions of ovaries are typical of salpingitis. (A from Seidel H et al: Mosby’s guide to physical examination, ed 4, St Louis, 1999, Mosby. B from Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 1996, Mosby.)
PATHOPHYSIOLOGY The development of upper genital tract infections is mediated by the failure of a number of defense mechanisms that usually are effective in preventing PID. Virulence of the organism, size of the inoculum, and defense status of the individual determine whether an infectious process results.
PID usually is considered a polymicrobial infection.63,64 Although initiated by gonorrhea or chlamydia, the majority of cases (up to 84%) are caused by mixed nongonococcal/nonchlamydial bacteria, including anaerobes (Bacteroides species and peptostreptococci), facultative organisms (Gardnerella vaginalis, Haemophilus influenzae, and streptococci), and genital tract mycoplasmas (Mycoplasma hominis, Mycoplasma genitalis and Ureaplasma urealyticum). M. hominis and U. urealyticum have been isolated from the endocervix but not the fallopian tubes. Escherichia coli has been overemphasized as a causal agent but may contribute to pelvic infections in older women. Recovery of Neisseria gonorrhoeae (37% to 44%), Chlamydia trachomatis (10% to 45%), or both (9% to 12%) is variable; however, facultative or anaerobic bacteria have been isolated in about 50% of women with acute PID. About 25% to 50% of the time, only facultative or anaerobic microorganisms are recovered.65
PID develops when pathogenic microbes ascend from an infected cervix along the endometrial tissue to infect the uterus and adnexae. Gonorrhea or chlamydia may induce changes in the columnar epithelium that lines the upper reproductive tract, causing damage and facilitating invasion by other microorganisms. This observation is supported from the recovery of cytokines, such as interleukin 6 (IL-6), from the cervix and endometrium of women with acute PID,66 and the presence of antibodies to a chlamydial protein (CHSP60) in animal studies of chronic PID.67 The resultant inflammatory response leads to tubonecrosis with repeated infections and may predispose a woman to PID.63 Other mechanisms that may contribute to PID include lymphatic drainage with parametrial spread of the infection or the adherence of sexually transmitted bacteria to sperm that travel through the genital tract. Several investigators report that bacterial vaginosis (BV), a bacterial overgrowth of the vagina, and mycoplasma genitalis has been linked to clinical findings of PID and histologic endometritis. Women with BV are nine times more likely to develop PID63,68 and M. genitalis is found in 14% of nongonococcal and non-chlamydial PID.69 (See Chapter 24 for further discussion of BV.) After one episode of pelvic infection, 15% to 25% of women develop long-term sequelae, such as infertility, ectopic pregnancy, chronic pelvic pain, dyspareunia, pelvic adhesions, perihepatitis, and tubo-ovarian abscess. The incidence of complications increases markedly with repeated infections. Tubal infertility occurs in 8% to 11% of women after one episode, 20% to 30% after two episodes, and 40% to 50% after three episodes.70,71 The mortality rate associated with PID is 0.29 deaths per 100,000 women ages 14 to 44.33 Most deaths resulting from PID are caused by septic shock (see Chapter 46).
CLINICAL MANIFESTATIONS The clinical manifestations of PID vary from sudden, severe abdominal pain with fever to no symptoms at all. An asymptomatic cervicitis may be present for some time before PID develops. Of women with salpingitis, 67% to 75% may have a subclinical infection. The first sign of the ascending infection may be the onset of low bilateral abdominal pain, most often characterized as dull and steady with a gradual onset. Symptoms are more likely to develop during or immediately after menstruation. The pain of PID may worsen with walking, jumping, or intercourse. Other manifestations of PID include dysuria (difficult or painful urination) and irregular bleeding.
EVALUATION AND TREATMENT The diagnosis of PID is based on history, abdominal tenderness with or without rebound, presence of uterine and cervical movement tenderness on bimanual pelvic examination, mucopurulent discharge at the cervical os, white blood cells on Gram stain or wet mount of cervical discharge, leukocytosis, and increased erythrocyte sedimentation rate. To support the diagnosis, chlamydia and gonorrhea testing is done; sonography, laparoscopy, and culdocentesis are indicated when a woman has recurrent symptoms or symptoms unresponsive to outpatient treatment regimen, fever greater than 38.3° C (100.9 ° F), or an adnexal mass. Other conditions that cause pelvic pain must be excluded, including ectopic pregnancy, threatened abortion, ovarian torsion, or appendicitis (Figure 23-7).
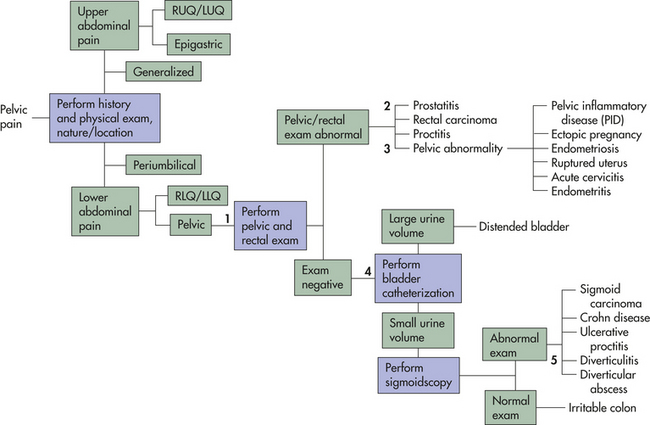
Figure 23-7 Diagnostic algorithm for pelvic pain. LLQ, Left lower quadrant; LUQ, left upper quadrant; RLQ, right lower quadrant; RUQ, right upper quadrant.
Because of the significance of the complications of PID, aggressive treatment is recommended. Treatment involves bed rest, avoidance of intercourse, and combined antibiotic therapy (Box 23-8). From 25% to 40% of women require hospitalization for intravenous administration of antibiotics and treatment of peritonitis or a tubo-ovarian abscess. To prevent recurrence, sexual partners also are treated with antibiotic combinations.72 Fluoroquinolone-resistant gonorrhea has become widespread in the United States, prompting changes in Centers for Disease Control and Prevention (CDC) recommendations for antibiotic regimens in PID treatment.73
Vaginitis
Vaginitis is infection of the vagina. The major causes of vaginitis are sexually transmitted pathogens (see Chapter 24) and Candida albicans. The incidence of sexually transmitted vaginitis remains highest in young women 15 to 24 years of age.72
The development of vaginitis is related to loss of local defense mechanisms, such as skin integrity, immune reaction, and particularly vaginal pH. The pH of the vagina depends on cervical secretions and the presence of normal flora that help maintain an acidic environment. A neutral or alkaline pH normally occurs before puberty, after menopause, and during pregnancy. The acidic nature of vaginal secretions during the reproductive years provides protection against a variety of sexually transmitted pathogens. Therefore, variables that alter the vaginal pH or the bactericidal nature of secretions (see Chapter 22) may predispose a woman to infection. These variables include douching; use of soaps, spermicides, feminine hygiene sprays, or deodorant menstrual pads or tampons; and conditions associated with increased glycogen content of vaginal secretions, such as pregnancy or diabetes. Antibiotics often destroy normal vaginal flora, facilitating overgrowth of C. albicans, causing a yeast vaginitis.
Normally, vaginal discharge is a clear, milky, or cloudy secretion with a slippery or clumpy texture. It is nonirritating, has a mild inoffensive odor, and turns yellow after drying. Throughout the menstrual cycle, the amount and texture of a woman’s discharge will change in response to hormonal fluctuation. Vaginal secretions increase at the time of ovulation, during pregnancy, and with sexual arousal; just before menstruation, vaginal discharge becomes thick and sticky. Although the amount of vaginal discharge alone is not an indication of infection, any other change in discharge may indicate a problem. Infection is suggested with a marked change in color or if the discharge becomes copious, malodorous, or irritating.
Diagnosis is based on history, physical examination, and examination of the discharge by wet mount. Treatment involves developing and maintaining an acidic environment, relieving symptoms (usually pruritus), and administering antimicrobial or antifungal medications to eradicate the infectious organism. If the infection can be sexually transmitted, a woman’s partner also will be treated.
Cervicitis
Cervicitis is a nonspecific term used to describe inflammation of the cervix prior to the identification of pathogens. Mucopurulent cervicitis (MPC) usually is caused by one or more sexually transmitted pathogens, such as Trichomonas, gonorrhea, Chlamydia, Mycoplasma, or Ureaplasma. Infection causes the cervix to become red and edematous. A mucopurulent (mucus- and pus-containing) exudate drains from the external cervical os, and the individual may report vague pelvic pain, bleeding, or dysuria. The cervix often becomes friable, bleeding easily during sexual intercourse or with pelvic examinations and Papanicolaou (Pap) smears. The infectious microorganisms are cultured or identified by immunoassay. Definitive diagnosis is followed by oral antibiotic therapy to prevent reinfection; sexual partners are treated as well.72
Vulvovestibulitis
Vulvovestibulitis (VV) (also referred to as vulvitis, vestibulitis, or vulvodynia) is inflammation of the vulva or vestibule of the genitalia, or both. In many cases, it may represent several disorders without an identifiable cause.74 VV is fairly common, affecting approximately 10% of women at some point in life. While the inflammation of VV may be caused by contact dermatitis (i.e., exposure to soaps, detergents, lotions, sprays, shaving, menstrual pads/tampons, perfumed toilet paper, tight-fitting clothes), the condition may be more complex and represent abnormalities in three interdependent systems: vestibular mucosa, pelvic floor musculature, and central nervous system pain regulatory pathways.75,76 The condition may also represent an autoimmune reaction, similar to fibromyalgia. The mechanisms are poorly understood, thus VV is often a difficult condition to evaluate and treat and many women suffer through years of misdiagnosis as a result.77 After ruling out and treating conditions that may contribute to or cause vulvar inflammation (e.g., Candida, sexually transmitted infection, seborrhea, psoriasis, lichen sclerosus, and contact dermatitis) there are few treatment options. Studies are limited but suggest that women may benefit from behavioral treatment (35% to 83% of women benefit) or vestibulectomy (61% to 94% success rate), a procedure that is understandably unacceptable to many women because of the invasiveness of the procedure.78 Other approaches with little or no research to support them include use of hydrocortisone cream, applying a water barrier (such as thick skin cream or solid vegetable shortening) during a period of healing, and overnight lidocaine applications.79 Women are advised to avoid potential irritants and to wear loose, cotton clothing. VV may increase susceptibility to vaginal infection; likewise, VV may be caused by vaginal infections (e.g., candidiasis, trichomoniasis) that spread to the labia, where they cause inflammation and edema. Other skin diseases, such as tinea cruris, psoriasis, lichen sclerosus, and inflammation of the apocrine (sweat) glands, can involve the vulva (see Chapter 44).
Bartholinitis
Bartholinitis, or Bartholin cyst, is an inflammation of one or both of the ducts that lead from the introitus (vaginal opening) to the Bartholin glands (Figure 23-8). The usual causes of bartholinitis are microorganisms that infect the lower female reproductive tract, such as streptococci, staphylococci, and sexually transmitted pathogens. Acute bartholinitis may be preceded by an infection, such as cervicitis, vaginitis, or urethritis.

Figure 23-8 Inflammation of Bartholin gland. (From Gardner HL, Kaufman RH: Benign diseases of the vulva and vagina, St Louis, 1969, Mosby.)
Infection or trauma causes inflammatory changes that narrow the distal portion of the duct, leading to obstruction and stasis of glandular secretions. The obstruction, or cyst, varies from 1 to 8 cm in diameter and is located in the posterolateral portion of the vulva. The cyst is usually reddened and painful, and pus may be visible at the opening of the duct; this exudate should be cultured. The individual may have symptoms of the initiating infection, fever, and malaise.
Most Bartholin cysts are asymptomatic and require no treatment. Chronic bartholinitis is characterized by the presence of a small cyst that is slightly tender but otherwise is asymptomatic. Symptoms occur if an exacerbation of infection causes an abscess to form in the gland itself.
Diagnosis of bartholinitis is based on the clinical manifestations and the identification of infectious microorganisms. Antibiotics are given to treat infection, and pain is relieved with analgesics and warm sitz baths. If an abscess forms, it is surgically drained.
Pelvic Organ Prolapse (POP)
The bladder, urethra, and rectum are supported by the endopelvic fascia and the perineal muscles, particularly the levator ani group. This muscular and fascial tissue loses tone and strength with aging and may fail to maintain the pelvic organs in the proper position. Progressive descent of the pelvic support structures may cause pelvic floor disorders, such as urinary and fecal incontinence and pelvic organ prolapse. Nearly 24% of women experience at least one pelvic floor disorder.80 Pelvic organ prolapse is thought to be caused by direct trauma, such as childbirth or pelvic surgery or damage to pelvic innervation, particularly the pudendal nerve. Pelvic organ descent is progressive and is related to the inherent strength or weakness of the woman’s musculofascial tissue. Prolapse of the bladder, urethra, rectum, or uterus may occur many years after an initial injury to the supporting structure. A strong familial tendency and possibly a multifactorial genetic component place some women at risk for the development of prolapse. Black and Asian women have the lowest risk of POP, and Hispanic women appear to have the highest risk.81 Risk factors in nulliparous women, which mimic the effects of childbirth, tend to be occupational activities that require heavy lifting or chronic medical conditions, such as chronic lung disease or refractory constipation. Some women at risk for pelvic organ prolapse have neural abnormalities that interfere with the innervation of the levator ani. A list of risk factors is contained in Box 23-9. (Chapter 22 contains a discussion of pelvic support structures.) Pelvic organ prolapse is the third most common indicator for hysterectomy in the United States. At least 30% of women will have repeat surgical procedures.82
The trend is to use terminology that describes physical examination findings, thus avoiding assumptions about structural involvement (Box 23-10). The terms cystocele and rectocele may be used when the structures involved (bladder, rectum) have been definitively identified (i.e., an anterior vaginal wall prolapse may or may not be a cystocele involving the urinary bladder) (see Figure 23-10, p. 835). Having a woman stand and strain maximally provides the best information about the degree of pelvic organ relaxation. Physical examination may be augmented with imaging by ultrasound, fluoroscope, or magnetic resonance. There are several systems used to describe prolapse. One in widespread clinical use is based on physical examination findings (see Box 23-10) and uses a grading system to describe the extent of the prolapse observed (Box 23-11). Subjective reports regarding the symptoms and effects of POP can be assessed through direct questioning or commonly used questionnaires, such as the Pelvic Floor Impact Questionnaire or the Pelvic Floor Distress Inventory.
Uterine prolapse is decent of the cervix or entire uterus into the vaginal canal (Figure 23-9). In severe cases the uterus falls completely through the vagina and protrudes from the introitus. Grade 1 uterine prolapse is not treated unless it causes discomfort. Grades 2 through 4 prolapse cause feelings of fullness, heaviness, and collapse through the vagina. Symptoms of other pelvic floor disorders also may be present. Treatment in these cases is the insertion of a pessary, which is a removable mechanical device that holds the uterus in position. The pelvic fascia may be strengthened through Kegel exercises (repetitive isometric tightening and relaxing of the pubococcygeal muscles) or by a course of estrogen therapy in menopausal women. Maintaining a healthy body mass index, preventing constipation, and treating chronic cough may help prevent prolapse. Surgical repair with or without hysterectomy is the treatment of last resort.
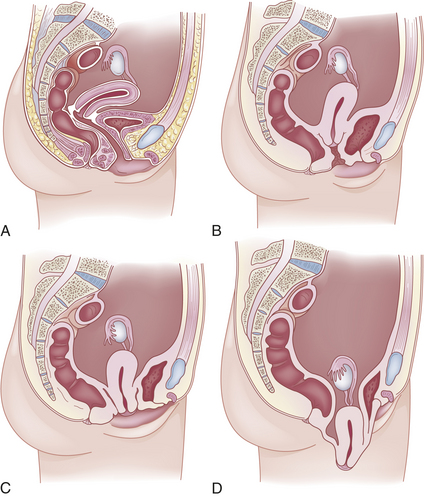
Figure 23-9 Degrees of uterine prolapse. A, Normal uterus (grade 0). B, Grade 1 prolapse: descent within the vagina. C, Grade 2 prolapse: descent to the hymen. D, Grade 4 prolapse: maximal possible descent of the uterus. Grade 3 prolapse not shown.
Figure 23-10 shows vaginal prolapse caused by cystocele and rectocele. Cystocele is descent of a portion of the posterior bladder wall and trigone into the vaginal canal and usually is caused by the trauma of childbirth. In severe cases the bladder and anterior vaginal wall bulge outside the introitus. Usually symptoms are insignificant in mild to moderate cases. Increased bulging and descent of the anterior vaginal wall and urethra can be aggravated by vigorous activity, prolonged standing, sneezing, coughing, or straining and can be relieved by rest or assumption of a recumbent or prone position. If the prolapse is large, women may complain of vaginal pressure or the feeling of “sitting on a ball.” A prolapse caused by a cystocele may be interpreted as incomplete bladder emptying, which can be controlled by a second voiding a few minutes after the first void or by manually reducing the anterior vaginal wall prolapse during voiding. Occasionally a cystocele causes significant residual urine and bladder infection.
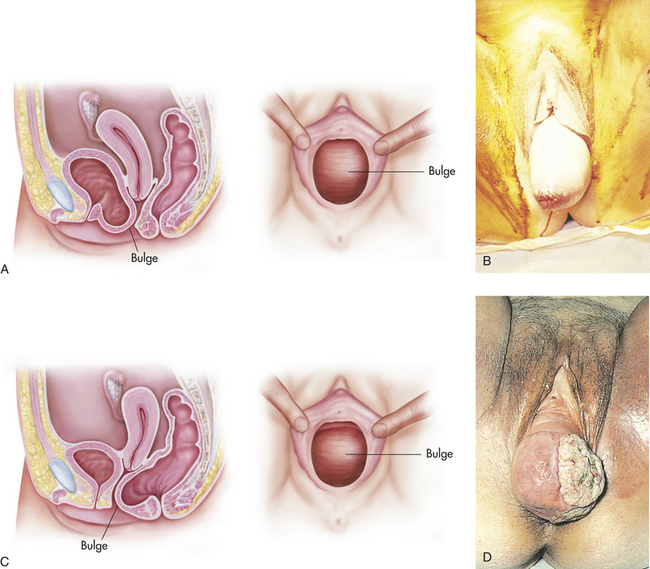
Figure 23-10 Cystocele and rectocele. A, Grade 2: anterior vaginal wall prolapse. B, Grade 4: prolapse. C, Grade 2: posterior wall prolapse. D, Grade 4: associated with ulceration of vaginal wall. Grades 1 and 3 not shown. (A and C from Seidel H et al: Mosby’s guide to physical examination, ed 4, St Louis, 1999, Mosby. B and D from Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Although commonly associated with urinary stress incontinence, cystocele does not cause it. Stress incontinence is likely the result of relaxation of the musculofascial supporting tissues of the urethra that also contribute to the cystocele. Operative correction of a large cystocele may actually cause rather than correct stress incontinence.83
Medical management includes vaginal pessary; Kegel exercises (prophylactic use produces best outcome); estrogen therapy for postmenopausal women; and, most important, reassurance that pressure symptoms are not the result of a serious condition. Surgical correction is used for severe anatomic injury unresponsive to medical treatment, and its success depends on treatment of generalized urogenital musculofascial supporting tissue relaxation, correction of underlying paravaginal defects, and elimination or prevention of contributing factors that increase intra-abdominal pressure, such as pregnancy, constipation, obesity, large pelvic tumors, bronchitis, and heavy manual labor.84
Urethrocele, or sagging of the urethra, is commonly associated with cystocele, especially in women with urinary stress incontinence. Like cystocele, urethrocele does not cause urinary incontinence. Urethrocele may be caused by the shearing effect of the fetal head on the urethra during childbirth. However, cystourethrocele may occur in nulliparous women and is most likely caused by congenital weakness and relaxation of the musculature of the pelvic floor or the endopelvic connective tissues or fascia. Treatment may be necessary after menopause.
A rectocele is the bulging of the rectum and posterior vaginal wall into the vaginal canal. During childbirth, women may sustain damage that can lead to a rectocele, but symptoms usually do not occur until several years after menopause.84 Familial and genetic predisposition and bowel habits contribute to rectocele development. Lifelong chronic constipation and straining may produce or aggravate a rectocele. Although most rectoceles are asymptomatic, larger ones with extensive relaxation cause vaginal pressure, rectal fullness, and incomplete bowel evacuation. If rectoceles are severe, defecation is difficult and can be facilitated by applying manual pressure to the posterior vaginal wall. Medical treatment focuses on the management and prevention of constipation and, if needed, the use of a pessary. Rectocele alone (without associated enterocele, uterine prolapse, and cystocele) seldom requires surgery.
An enterocele is herniation of the rectouterine pouch into the rectovaginal septum (between the rectum and posterior vaginal wall). It can be congenital or acquired. Congenital enterocele rarely causes symptoms or progresses in size; the acquired form usually is associated with other pelvic relaxation disorders such as uterine prolapse, cystocele, and rectocele. Most large enteroceles are found in grossly obese and older adults and can be complicated by rupture or complete eversion of the vagina with trophic ulceration, edema, and fibrosis. Treatment is surgical. Table 23-3 summarizes the symptoms and treatments of pelvic organ prolapse.

Benign Growths and Proliferative Conditions
Benign cysts of the ovary may occur at any time during the life span, but are most common during the reproductive years and, in particular, at the extremes of those years (Figure 23-11). An increase in benign ovarian cysts occurs when hormonal imbalances are more common, around puberty and menopause.85 Benign ovarian cysts are quite common, comprising a third of gynecologic hospital admissions. Two common causes of benign ovarian enlargement in ovulating women are follicular cysts and corpus luteum cysts. These cysts are called functional cysts because they are caused by variations of normal physiologic events. Follicular and corpus luteum cysts are unilateral. They are typically 5 to 6 cm in diameter but can grow as large as 8 to 10 cm. Most women are asymptomatic.
Benign cysts of the ovary are produced when a follicle or a number of follicles are stimulated but no dominant follicle develops and completes the maturity process. Every month about 120 follicles are stimulated, but normally only one succeeds in ovulating a mature ova.
Normally, during the early follicular phase of the menstrual cycle, follicles of the ovary respond to hormonal signals from the brain. The pituitary produces FSH to mature follicles in the ovary. As the follicles enlarge, granulosa cells in the follicle multiply and secrete estradiol. As a dominant follicle develops, it secretes higher levels of estradiol, which stimulates the LH surge that comes from the pituitary. The LH surge stimulates the follicle to rupture, releasing the ova and transforming the granulosa cells of the dominant follicle into the corpus luteum. If the dominant follicle develops properly before ovulation, the corpus luteum becomes vascularized and secretes progesterone. Progesterone arrests development of other follicles in both ovaries in that cycle. Progesterone, proteolytic enzymes, and prostaglandins trigger follicular rupture and release of the ovum.
Follicular cysts can be caused by a transient condition in which the dominant follicle fails to rupture or one or more of the nondominant follicles fail to regress. This disturbance is not well understood. It may be that the hypothalamus does not receive or send a message strong enough to increase FSH levels needed to develop or mature a dominant follicle. The hypothalamus monitors blood levels of estradiol and progesterone; when FSH is low, estradiol does not increase enough to stimulate LH. Recent evidence indicates that when progesterone is not being produced, the hypothalamus releases GnRH to increase the FSH level.86 FSH continues to stimulate follicles to mature, and the granulosa cells grow and, presumably, estradiol increases. This abnormal cycle continues to stimulate follicular size and causes follicular cysts to develop. Clinical symptoms of follicular cysts or even a single cyst is bloating, swollen and tender breasts, and heavy or irregular menses. After several subsequent cycles in which hormone levels once again follow a regular cycle and progesterone levels are restored, cysts usually are absorbed or regress.
Follicular cysts can vary in size and symptoms from one episode to the next and often can recur. Most are fluid filled; the more solid an ovarian cyst, the greater the chance of malignancy.
A corpus luteum cyst may develop because of a hormonal imbalance in low LH and progesterone levels causing an inadequate development of the corpus luteum. There is an intracystic hemorrhage that occurs in the vascularization stage, and the affected cyst then consists of blood. In normal cysts the blood is replaced by a clear fluid that accumulates in the cavity of the corpus luteum.
Corpus luteum cysts are less common than follicular cysts, but luteal cysts typically cause more symptoms, particularly if they rupture. Manifestations include dull pelvic pain and amenorrhea or delayed menstruation, followed by irregular or heavier than usual bleeding. Rupture occasionally occurs and can cause massive bleeding with excruciating pain; immediate surgery may be required. Corpus luteum cysts usually regress spontaneously in nonpregnant women. Oral contraceptives may be used to prevent future cysts from forming.
Dermoid cysts are ovarian teratomas that contain elements of all three germ layers; they are common ovarian neoplasms. These growths may contain mature tissue including skin, hair, sebaceous and sweat glands, muscle fibers, cartilage, and bone. Dermoid cysts are usually asymptomatic and are found incidentally on pelvic examination. Dermoid cysts have malignant potential and should be removed.
Torsion of the ovary may occur as a complication of ovarian cysts or tumors or enlargement of the ovary associated with infertility treatments. Ovarian torsion is rare but is a gynecologic emergency when present. Individuals present with acute, severe unilateral abdominal or pelvic pain related to a change of position.
Endometrial Polyps
An endometrial polyp is a benign mass of endometrial tissue, covered by a surface epithelium, and contains a variable amount of glands, stoma, and blood vessels. Endometrial polyps are usually solitary and originate at the fundus but also may be multiple (20% of the cases) or originate from the lower uterine segment or upper endocervix and contain mixed epithelium. Polyps are morphologically diverse and usually classified as hyperplastic, atrophic (or inactive), or functional. In the last case, the surface epithelium may be “out of phase” with other endometrial tissue. Hyperplastic polyps are often pedunculated and may be mistaken for endometrial hyperplasia or, if large, adenosarcoma (Figure 23-12). Although polyps most often develop in women between ages 40 and 50, they can occur at all ages. These are often related to estrogen stimulation. As many as 35% of women with abnormal uterine bleeding are found to have polyps.87

Figure 23-12 Endometrial polyp. It is protruding through the cervical os. (From Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Endometrial polyps are a common cause of intermenstrual or excessive menstrual bleeding. Diagnosis is made by transvaginal sonography or hysteroscopy. Risk factors include obesity, tamoxifen use, hypertension, and estrogenic states (i.e., anovulatory cycles and unopposed estrogen). Malignancy is extremely rare (1% to 2%), and coexistence of a separate endometrial atypical hyperplasia or adenocarcinoma is common. Women with polyps less than 1.5 cm can be observed. Uterine polyps have a high rate of spontaneous resolution. Polypectomy can be performed through hysteroscopy for symptomatic women or those with risk factors for malignancy.88
Leiomyomas
Leiomyomas, commonly called myomas or uterine fibroids, are benign smooth muscle tumors in the myometrium (Figure 23-13). Leiomyomas are the most common benign tumors of the uterus, affecting as many as 70% to 80% of all women, and most remain small, asymptomatic, and clinically insignificant.89 Prevalence increases in women ages 30 to 50 but decreases with menopause. The incidence of leiomyomas in black and Asian women is two to five times higher than that in white women.90
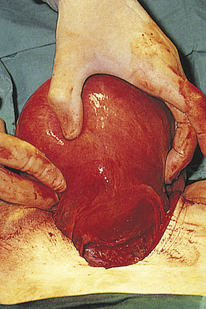
Figure 23-13 Uterine fibroid. The uterus is irregular because it contains multiple fibroids. (From Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
The cause of uterine leiomyomas is unknown, although their size appears to be related to estrogen, progesterone, growth factors, angiogenesis, and apoptosis. Leiomyomas are estrogen-and progesterone-sensitive and are found to have increased numbers of estrogen receptors.89 Uterine leiomyomas are not seen before menarche, and those that develop during the reproductive years generally decrease in size after menopause. Occurrence is thought to be related to increased estrogen exposure. Tumors in pregnant women enlarge rapidly but often decrease in size after termination of the pregnancy. Risk factors include heredity, nulliparity, obesity, PCOS, diabetes mellitus, and hypertension.
PATHOPHYSIOLOGY Most leiomyomas occur in multiples in the fundus of the uterus, although they may occur singly and throughout the uterus. Leiomyomas are classified as subserous, submucous, or intramural according to their location within the various layers of the uterine wall (Figure 23-14). Uterine leiomyomas are usually firm and surrounded by a connective tissue layer. Degeneration and necrosis may occur when the leiomyoma outgrows its blood supply and therefore are more common in larger tumors and may be accompanied by pain.
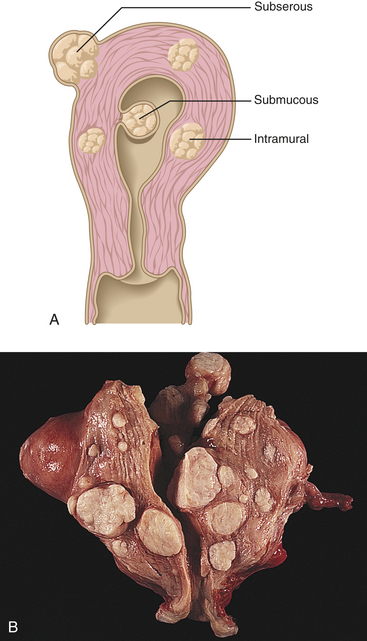
Figure 23-14 Leiomyomas. A, Uterine section showing whorl-like appearance and locations of leiomyomas, which are also called uterine fibroids. B, Multiple leiomyomas in sagittal section. Typical, well-circumscribed, solid, light gray nodules distort uterus. (B from Damjanov I, Linder J: Pathology: a color atlas, St Louis, 2000, Mosby.)
CLINICAL MANIFESTATIONS The major clinical manifestations of leiomyomas are abnormal uterine bleeding, pain, and symptoms related to pressure on nearby structures. They also may contribute to infertility and subfertility. The leiomyoma tends to make the uterine cavity larger, thereby increasing the endometrial surface area. This increase may account for the increased menstrual bleeding that is associated with leiomyomas. Pain is not an early symptom but tends to occur with the devascularization of larger leiomyomas. It is also associated with blood vessel compression that limits blood supply to adjacent structures. Symptoms of abdominal pressure are slow to develop, apparently because the tumor is relatively slow growing, enabling adjacent structures to adapt to pressure. Pressure on the bladder may contribute to urinary frequency, urgency, and dysuria. Pressure on the ureter may cause it to become distended “upstream” from the pressure point; rectosigmoid pressure may lead to constipation. A sensation of abdominal or genital heaviness may be felt with larger tumors.
EVALUATION AND TREATMENT Uterine leiomyomas are suspected when the bimanual examination discloses uterine enlargement and irregular, nontender nodularity of the uterus. Pelvic sonography confirms diagnosis.90 Treatment depends on the symptoms, tumor size, age, reproductive status, and overall health of the individual. Most myomas are asymptomatic and can be managed by observation only. Medical treatment for symptomatic or subfertile women is aimed at shrinking the myoma. Some leiomyomas shrink in response to oral contraceptives, however, oral contraceptive pills (OCPs) may enhance growth so should be monitored carefully. GnRH agonists are usually a temporary management for those close to menopause or as a presurgical treatment. GnRH side effects related to decreased estrogen, including hot flashes and osteoporosis, limit its usefulness. Various selective estrogen receptor modulators have been studied in conjunction with GnRH agonists and appear safe and effective.91 Antidepressants, such as mifepristone (RU486) have also shown some effectiveness in shrinking leiomyomas. Myomectomy may be undertaken and remains the standard of cure for women wishing to preserve their fertility. Hysterectomy is also an option. Newer experimental treatments that show promise include uterine artery embolization, laser ablation treatment with mifepristone, and the levonorgestrel intrauterine system. With each of these new therapies, benefits and risks should be carefully explored.92
Adenomyosis
Adenomyosis is the presence of islands of endometrial glands surrounded by benign endometrial stroma within the uterine myometrium. Endometrial cells migrate into the myometrial layer because of an unknown mechanism. Estrogen and progesterone likely play a role and, perhaps, metaplasia of müllerian tissue. Unlike endometriosis, this tissue does not respond to cyclic hormone changes. It commonly develops during the late reproductive years, with the highest incidence among women in their 40s and women on tamoxifen. Adenomyosis has been found in 18% of hysterectomy specimens and 53% of specimens from women taking tamoxifen. Ninety percent of all adenomyosis is found in parous women. Adenomyosis may be asymptomatic or may be associated with abnormal menstrual bleeding, dysmenorrhea, uterine enlargement, and uterine tenderness during menstruation. Secondary dysmenorrhea becomes increasingly severe as disease progresses. On bimanual examination the uterus is diffusely enlarged, globular, and most tender just before or after menstruation. Diagnosis is confirmed with ultrasonography or MRI. Treatment is symptomatic, similar to dysmenorrhea (i.e., nonsteroidal anti-inflammatory drugs [NSAIDs], COCs, and perhaps levonorgestrel-containing IUDs). Surgical treatment includes resection of localized areas of adenomyosis or, if severe, hysterectomy. GnRH and danazol are experimental.90
Endometriosis
Endometriosis is the presence of functioning endometrial tissue or implants outside the uterus. Like normal endometrial tissue, the ectopic (out of place) endometrium responds to the hormonal fluctuations of the menstrual cycle.
The incidence of endometriosis is difficult to determine, particularly in asymptomatic adolescent and fertile women. It is estimated that 2% to 22% of reproductive-age women and 2% to 4% of menopausal women have endometriosis. In addition, as many as 50% of women evaluated for pelvic pain, infertility, or a pelvic mass are diagnosed as having endometriosis, and 4% to 8% of fertile women have endometriosis. Moreover, the frequency and severity of symptoms do not correlate well with the extent or site of lesions.93 A large study has found that women with endometriosis are at greater risk for cancers (ovarian and non-Hodgkin lymphoma, endocrine, and brain), in particular for those with long-standing disease or early diagnosis, or both.94
The cause of endometriosis is not known, but several theories have been proposed. In 1927 Sampson95 proposed that endometriosis is caused by the implantation of endometrial cells during retrograde menstruation, in which menstrual fluids move through the fallopian tubes and empty into the pelvic cavity (Figure 23-15). It is now known that retrograde menstruation occurs in almost all women; however, not all women develop endometriosis.
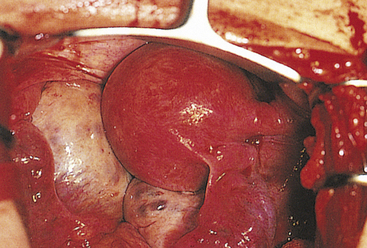
Figure 23-15 Endometriosis. The uterus is distended, and retrograde spill of menstrual loss has led to the development of endometriosis (dark purple patches). (From Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Another theory is that women with endometriosis have impaired cellular and humoral immunity. Alterations in cytokine and growth factor signaling have been identified. Cytotoxic T cell and natural killer (NK) cell activity has been found to be depressed. At the same time, increased numbers of macrophages appear to be stimulating endometrial cell proliferation outside the uterus. An autoimmune response is also suspected.93 Such alterations may cause the body to tolerate ectopic implantation of endometrial cells. Researchers also have proposed that endometrial cells spread through the lymphatic or vascular systems or that multipotential cells in the epithelial coverings of reproductive organs are somehow stimulated to develop into endometrial and metaplastic cells. A genetic predisposition to endometriosis has been documented. Studies show that incidence and severity of disease are greatest among women with female relatives who also have endometriosis.93 Some genetic polymorphisms have been identified. Environmental toxins have also been implicated (see What’s New? Do Environmental Toxins Contribute to Endometriosis?).
PATHOPHYSIOLOGY Endometrial implants can occur throughout the body but generally occur in the pelvic and abdominal cavities. The most common sites of implantation are the ovaries, uterine ligaments, rectovaginal septum, and pelvic peritoneum (Figure 23-16). Other sites of implantation are the sigmoid colon, small intestine, rectum, appendix,
WHAT’S NEW?
Do Environmental Toxins Contribute to Endometriosis
Dioxin and dioxin-like compounds—byproducts of industrial processing—are associated with an increased prevalence of endometriosis and with infertility in women with endometriosis. These compounds may increase interleukin levels, activate cytochrome P-450 enzymes, and create tissue remodeling. Together with estrogen, they stimulate endometriosis formation and blocking of normal progesterone-induced regression of endometrial tissue.
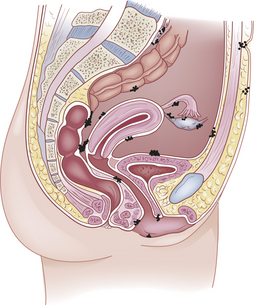
Figure 23-16 Pelvic sites of endometrial implantation. Endometrial cells may enter the pelvic cavity during retrograde menstruation.
Data from Caserta D et al: Hum Reprod Update 14(1):59-72, 2008.
bladder, uterus, vulva, vagina, cervix, lymph nodes, extremities, pleural cavity, lungs, laparotomy scars, and hernial sacs.
Cyclic changes depend on the blood supply of the implants and the presence of glandular and stromal cells. Given that blood supply is sufficient, the ectopic endometrium proliferates, breaks down, and bleeds in conjunction with the normal menstrual cycle. The bleeding causes inflammation, triggering a cascade of cellular inflammatory mediators, including cytokines, chemokines, growth factors, and protective factors such as secretory leukocyte protease inhibitor and superoxide dismutase.93 Pain occurs in surrounding tissues. The inflammation may lead to fibrosis, scarring, and adhesions.
CLINICAL MANIFESTATIONS The clinical manifestations of endometriosis can mimic other disease processes (i.e., pelvic inflammatory disease, irritable bowel syndrome, ovarian cysts, dysmenorrhea) and are variable in frequency and severity. These include primarily infertility and pain,93 dysmenorrhea, dyschezia (pain on defecation), dyspareunia (pain on intercourse), and less commonly, constipation, abnormal vaginal bleeding, and if implants are located within the pelvis, an asymptomatic pelvic mass having irregular, movable nodules and a fixed, retroverted uterus. Most symptoms of endometriosis can be explained by the proliferation, breakdown, and bleeding of the ectopic endometrial tissue with subsequent formation of adhesions. In most instances, however, the degree of endometriosis is not related to the frequency or severity of symptoms. Dysmenorrhea, for example, does not appear to be related to the degree of endometriosis. With involvement of the rectovaginal septum or the uterosacral ligaments, dyspareunia develops. Dyschezia, a hallmark symptom of endometriosis, occurs with bleeding of ectopic endometrium in the rectosigmoid musculature and subsequent fibrosis.
Twenty-five percent to 40% of women with infertility have endometriosis. The link between endometriosis and infertility is strong, yet the degree of disease and infertility is not as closely associated. That is, women with untreated minimal to mild disease may have high pregnancy rates or may experience infertility. The exact mechanism for infertility in women with endometriosis is unknown. Infertility may result from mechanical interference with ovulation or ovum transport through the fallopian tube because of adhesions and the effects of inflammation and cytokine activity. There are conflicting reports regarding the effect of endometriosis on sperm activity. An increased phagocytosis of spermatozoa by macrophages has been observed. Some researchers suggest impairment in follicle development as well as embryo development.96 Implantation defects also are postulated to be present (e.g., decreased uterine receptivity).93 Oxidative stress is thought to contribute to decreased ovarian and tubal function and further decreases uterine receptivity.97
EVALUATION AND TREATMENT A presumptive diagnosis can be made based on clinical manifestations but laparoscopy is required for definitive diagnosis of endometriosis. A uniform classification system that includes both extent and severity has been developed (Table 23-4) but still does not correlate well with a woman’s symptoms. Treatment is aimed at preventing or decreasing progression and spread, alleviating pain, and restoring fertility. Current therapies include suppression of ovulation with noncyclic estrogen-progestin COCs, depot medroxyprogesterone acetate (DMPA), danazol (which diminishes midcycle LH surge), GnRH agonists/analogs (to create a medical oophorectomy), gestrinone (a 19-nortestosterone derivative and antiprogestational steroid), mifepristone (RU486) (an antiprogestational and antiglucocorticoid agent that can inhibit ovulation and disrupt endometrial integrity), and atrophy of endometrium with progestins, including DMPA, oral progestins, or a levonorgestrel-containing IUD.98,99 A newer therapy is an injectable GnRH antagonist, which produces immediate inhibition of gonadotropin release. GnRH antagonists are shorter acting than GnRH but release histamine at the site of injection. Conservative surgical treatment includes laparoscopic removal of endometrial implants with conventional or laser techniques and presacral neurectomy for severe dysmenorrhea. Effectiveness may be increased when medical regimens are combined with surgical techniques. All treatments have risks or side effects, and recurrent symptoms develop in as many as 74% of women within a few years.99
Table 23-4
Classification System for Endometriosis (Requires Laparoscopic Visualization)
| Stage | Degree of Invasiveness |
| I | Minimal |
| II | Mild |
| III | Moderate |
Classification system also documents the location of lesions and presence of adhesions.
Data from: Practice Committee of the American Society for Reproductive Medicine: Fertil Steril 67(5):817-821, 1997.
Cancer
Malignant tumors of the female reproductive system are common. Endometrial carcinoma accounts for approximately 5.8% of all cancers in women, ovarian tumors account for 3.1% of all cancers, and cervical cancers account for 1.6%.1 Malignant neoplasms of the female reproductive tract account for about 1 in 8 (13.3%) diagnosed cancers and 1 in 9 (11.3%) cancer deaths in women in the United States.1
Cervical Cancer
Cancer of the cervix is the most common cancer in women worldwide; however, in the United States, it is the 14th most common type of cancer in women.1 In the United States, the rates of invasive cancer have steadily decreased (a 75% reduction since the 1960s) and mortality rates caused by cervical cancer have declined (more than 45% since the early 1970s) largely because of the increased prevalence and frequency of cervical cancer screening with the Pap smear. The incidence rate in black women (11.4 per 100,000) exceeds the rate in white women (8.5 per 100,000); the mortality rate is more than double (4.9 per 100,000) for black women compared to the mortality rate for white women (2.3 per 100,000). In 2009, the American Cancer Society estimated 11,270 new cases of cervical invasive cancer and 4070 cervical cancer deaths.1
It is now widely know that cervical cancer is almost exclusively caused by cervical human papillomavirus (HPV) infection. Infection with “high-risk” (oncogenic) types of HPV (predominantly 16 and 18) is a necessary precursor to development of the precancerous dysplasia of the cervix that leads to invasive cancer (also see Chapter 11). Precancerous dysplasia, also called cervical intraepithelial carcinoma (CIN) or cervical carcinoma in situ (CIS), occurs more often in younger women. Fifty percent of adolescents and young women acquire HPV (predominantly high-risk types) within 3 years of initiation of sexual intercourse; half of these are within 3 months (also see Chapter 24).100 However, most of these infections are spontaneously cleared by the immune system; the vast majority of these cases do not go on to develop into CIS or invasive cervical cancer.101 Smoking, immunosuppression, and poor nutrition are considered cofactors, perhaps explaining why some HPV infections do progress to cervical cancer. Infection with C. trachomatis also may be a cofactor in the development of one type of cervical cancer; squamous cell invasive cervical cancer.102 Human immunodeficiency virus (HIV)–positive women also are at greater risk for developing cervical cancer.101,103 Specific guidelines for screening and follow-up of abnormal cytology or positive HPV testing for HIV-positive women are available.103
PATHOGENESIS Cervical cancer is a slowly progressive disease that is staged according to histology (Tables 23-5 and 23-6). Testing for high-risk HPV is often positive for many years (10 or more) before dysplasia progresses to a high-grade squamous intraepithelial lesion (HSIL) prior to invasive cervical cancer. Other than HPV infection, the genetics of cervical cancer remains poorly understood. Several chromosome regions with recurrent loss of heterozygosity (LOH) have been identified (also see Chapter 11). However, the problematic tumor suppressor genes located on these chromosomal locations are yet to be identified. Recurrent amplifications have been mapped to the short arm of chromosome 3 in invasive cancer. Like other cancers, cervical cancer requires the accumulation of genetic alterations for carcinogenesis to occur.
Table 23-5
Cervical Epithelial Cell Abnormalities (Precancerous Cervical Neoplasias)
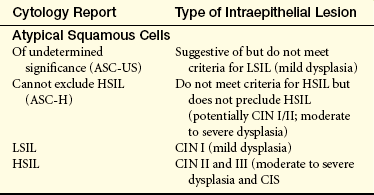
ASC-H, Atypical squamous cells, cannot exclude high-grade squamous intraepithelial lesion; ASC-US, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; CIS, carcinoma in situ; HSIL, high-grade squamous intraepithelial lesion; LSIL, low-grade squamous intraepithelial lesion.
Table 23-6
Clinical Staging for Cancer of the Cervix
| Stage | Characteristics |
| 0 | Cancer in situ, intraepithelial carcinoma; earliest stage of cancer; cancer confined to its original site |
| I | Carcinoma confined to cervix (extension to corpus disregarded) |
| IA | Earliest form of stage I; there is very small amount of cancer, which is visible only under a microscope |
| IA1 | Area of invasion is <3 mm (about 1/8 inch) deep and <7 mm (about 1/3 inch) wide |
| IA2 | Area of invasion is between 3 mm and 5 mm (about 1/5 inch) deep, and <7 mm (about 1/3 inch) wide |
| IB | Includes cancers that can be seen without a microscope; also includes cancers seen only with a microscope that have spread deeper than 5 mm (about 1/5 inch) into connective tissue of the cervix or are wider than 7 mm |
| IB1 | A IB cancer that is no larger than 4 cm (about 1 3/5 inches) |
| IB2 | A IB cancer that is >4 cm |
| II | Cancer has spread beyond the cervix to the upper part of the vagina; cancer does not involve the lower third of the vagina |
| IIA | Cancer has spread beyond the cervix to the upper part of the vagina; cancer does not involve the lower third of the vagina |
| IIB | Cancer has spread to the tissue next to the cervix, called the parametrial tissue |
| III | Cancer has spread to the lower part of the vagina or the pelvic wall; cancer may be blocking the ureters (tubes that carry urine from the kidneys to the bladder) |
| IIIA | Cancer has spread to the lower third of the vagina but not to the pelvic wall |
| IIIB | Cancer extends to the pelvic wall, blocks urine flow to the bladder, or both |
| IV | Most advanced stage of cervical cancer; cancer has spread to other parts of the body |
| IVA | Cancer has spread to the bladder or rectum, which are organs close to the cervix |
| IVB | Cancer has spread to distant organs beyond the pelvic area, such as the lungs |
Reprinted from the American Cancer Society’s Cancer Information Database with permission.
The progressive changes of cervical cells are classified on a continuum from cervical intraepithelial neoplasia (dysplasia), to cervical carcinoma in situ (full epithelial thickness of the cervix is involved), to invasive carcinoma (see Tables 23-5 and 23-6). Cervical dysplasia is replacement of some epithelial cells by atypical, neoplastic cells, and is “staged” depending on the depth of epithelial involvement (Figure 23-17). In cervical CIN III or HSIL, all or most of the cervical epithelium shows cellular features of carcinoma, but underlying tissue is not affected. Risk of progression to invasive carcinoma rises steadily with the severity of dysplasia. Women with CIN I (low grade intraepithelial lesion [LSIL] or mild dysplasia) have an 11% chance of progression to CIS and a 1% chance of progression to cervical invasion. Women with CIN II have a 22% chance of progression to CIS and a 5% chance of invasive lesions. At least 12% of women with CIN III (CIS) progress to cervical invasion. More than half (57%) of women with CIN I, 43% of women with CIN II, and 32% of women with CIN III will have a natural “regression” of lesions. At least a third or more of all cervical intraepithelial lesions will simply persist without progression or regression.
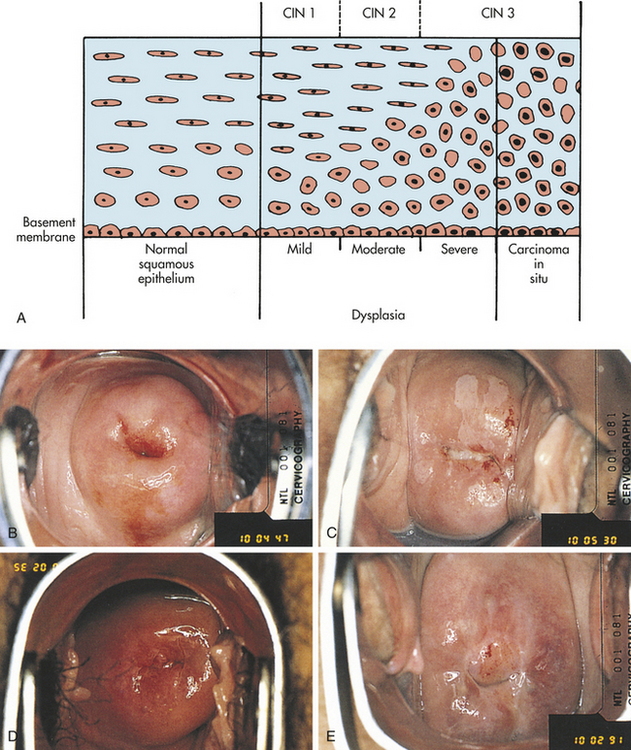
Figure 23-17 Cervical intraepithelial neoplasia (CIN). A, Diagram of cervical endothelium showing progressive degrees of CIN. B, Normal multiparous cervix. C, CIN stage 1. Note the white appearance of part of the anterior lip of the cervix associated with neoplastic changes. D, CIN stage 2. Lesions reflected in distant capillaries. E, CIN stage 3. Lesion predominantly around the external os. (A from Herbst AL et al: Comprehensive gynecology, ed 2, St Louis, 1992, Mosby. B-E, from Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Carcinoma in situ is most likely to develop in the squamous-columnar junction—the so-called transformation zone—where the columnar epithelium of the cervical lining meets the squamous epithelium of the outer cervix and vagina (Figure 23-18). In this zone, columnar epithelium is constantly being replaced by squamous epithelium in a process known as metaplasia. Metaplasia is thought to be affected by hormonal levels; change in cervical epithelium is not understood as well as endometrial tissue change in response to fluctuating hormones. Because metaplastic cells are at increased risk of incorporating foreign or abnormal genetic material, neoplastic changes are most common in the transformation zone.

Figure 23-18 Cervical carcinoma in situ. Typical transformation zone, where the columnar (grapelike) epithelium is replaced by metaplastic epithelium. At its outer edge, the metaplastic epithelium adjoins the squamous epithelium, which extends into the vagina. (From Coppleson M, Pixley E, Reid B: Colposcopy: a scientific approach to the cervix in health and disease, Springfield, IL, 1971, Charles C Thomas.)
Carcinoma in situ is generally a precursor of invasive carcinoma of the cervix. A number of factors, including tumor type, contribute to the rate at which carcinoma in situ becomes invasive. Invasive carcinoma of the cervix consists of direct invasion into adjacent tissues and metastasis through the lymphatics. Adjacent tissues most often involved are the ureters and structures of the lateral pelvic wall, the vaginal stroma and epithelium, and the lower uterine segment and myometrium. The internal, external, and common iliac lymph nodes and the obturator nodes are common sites of lymphatic involvement. A staging system for carcinoma of the cervix is shown in Table 23-6.
CLINICAL MANIFESTATIONS Because cervical neoplasms are asymptomatic, regular Pap test or HPV screening is necessary. About 90% of cervical cancer cases can be detected early through the use of regular screening tests (see What’s New? Is the Pap Smear for Cervical Cancer Screening Obsolete?). If symptoms exist, they may include vaginal bleeding or abnormal discharge. Bleeding is variable
and may occur after intercourse or between menstrual periods. At times, women will complain of abnormal menses or postmenopausal bleeding. Vaginal discharge is a less common presenting symptom and may be serosanguineous or yellowish. A new or foul odor also may be present. Bleeding and discharge are subtle and are likely to be disregarded by premenopausal women, who mistake these signs for variations of normal processes. Postmenopausal women are more likely to seek medical attention if these signs appear. With severe bleeding, symptoms of anemia may occur. Pelvic or epigastric pain is experienced only with large lesions. Advanced disease may cause urinary or rectal symptoms and pelvic or back pain.
EVALUATION AND TREATMENT Cervical cytology is most accurate if cells are obtained from both the endo- and ectocervix. When dysplasia is detected, colposcopy is usually indicated to identify lesions and for obtaining biopsies of the ectocervix and curettage biopsy of the endocervix. The transformation zone moves higher into the cervix as age increases, making biopsy more difficult. If invasive carcinoma is found, lymphangiography, CT scan, ultrasonography, or radioimmunodetection methods are used to assess lymphatic involvement. Cystoscopy and proctoscopy also may be performed.
The treatment depends on the degree of neoplastic change, the size and location of the lesion, and the extent of metastatic spread. For premalignant change or CIS (stage 0), cryosurgery or carbon dioxide laser therapy is commonly used; laser treatment may produce better results in the multiparous cervix. Loop diathermy conization and the loop electrosurgical excision procedure (LEEP) are alternative treatments. In LEEP, a small, looped wire with electric current generates heat and burns off cancer cells. Conization is removal of a cone-shaped section of tissue that includes the cancer; high-frequency current is used with cold-knife conization. The amount of tissue removed depends on the location of the lesion. None of these measures affects fertility or childbearing.
For invasive cervical carcinoma, treatment depends on the stage of the tumor (Table 23-7). Surgical intervention may include a hysterectomy, pelvic lymphadenectomy, and pelvic exenteration (radical removal of contents of body cavity). Radiation therapy is used most often in cases of small cell cancer with lymphatic involvement. External radiation usually is combined with one or two intracavitary implants. Multidrug chemotherapy regimens also have been used. Recent phase 3 trials suggest significant improvement in survival with combined chemotherapy and radiation therapy.104 Smokers tend to have a higher stage of disease at diagnosis, and their cancer is more resistant to radiation treatment.
Table 23-7
Cervical Cancer Treatment Options
| Stage | Treatment |
| 0 | Cryosurgery, laser surgery, loop diathermy conization, or loop electrosurgical excision procedure (LEEP) |
| IA | Surgery (total abdominal hysterectomy, may include oophorectomy), radiation therapy |
| IB | Surgery (radical hysterectomy with lymph node dissection), internal and external radiation therapy combined |
| IIA | Surgery (radical hysterectomy with lymph node dissection), internal and external radiation therapy combined |
| IIB | Internal and external radiation therapy combined |
| III | Internal and external radiation therapy combined |
| IVA | Internal and external radiation therapy combined; surgery (exenteration) for removal of uterus, vagina, cervix; could include bladder, colon, or rectum depending on the area of malignant spread |
| IVB | Radiation therapy for pain symptoms |
With early detection and treatment, prognosis is excellent. Overall, the 5-year survival rate is 95% for stage IA or lower (e.g., early detection). A cure rate of 100% is possible for women with dysplasia or carcinoma in situ.1 The prevention of HPV infection may be the key to substantially reducing the risk of cervical cancer. FDA-approved vaccines for two of the high-risk types of HPV show excellent promise.105,106
Vaginal Cancer
Cancer of the vagina is the rarest of the female genital cancers and accounts for less than 2% of gynecologic cancers.107 About 90% are squamous cell-type cancers; the remaining 10% of tumors are adenocarcinomas, sarcomas (rare), and melanomas (rare). Women with either an in situ or an invasive cervical or vulvar squamous cell cancer are at increased risk for squamous cell abnormality of the vagina, and may have a similar etiology.108 The mean age of women with invasive cancer of the vagina is 55 years; carcinoma in situ occurs about 10 years earlier. However, vaginal neoplasia is increasingly seen in younger women, likely because of an increase in HPV infection at younger ages. Vaginal sarcomas develop in children younger than 5 years and in women in the fifth to sixth decades. Clear-cell carcinomas, the most common form of adenocarcinomas, occur in conjunction with vaginal adenosis in young women with a history of in utero diethylstilbestrol (DES) exposure. Metastatic adenocarcinomas arise from the urethra, Bartholin gland, rectum, bladder, endometrium, endocervix, ovary, or a distant organ.108
Vaginal and cervical cancers are thought to have similar epidemiology. Both start as intraepithelial lesions, occur in sexually active women, and are associated with HPV infection.108,109 As mentioned, prior carcinoma of the cervix places a woman at higher risk for developing vaginal cancer. In utero exposure to nonsteroidal estrogens also has been considered a risk factor. It has been estimated that 100,000 to 160,000 women were exposed in utero to such nonsteroidal estrogens as DES, dienestrol, or hexestrol from 1960 to 1970. Apparently, exposure to such hormones during the first 3 months of gestation inhibits the normal replacement of columnar epithelium by squamous epithelium in the vagina of the fetus. The columnar epithelium, which is not normally found in the vagina, then may undergo malignant transformation. Not all women exposed to DES in utero develop neoplastic changes in the vagina, however. Between 0.14 and 1.4 cases of vaginal cancer develop per 1000 women at risk. Nineteen years is the average age at which clear-cell carcinoma develops as a result of DES exposure.
Like cervical neoplasms, vaginal cancers are classified as intraepithelial neoplasia (dysplasia), carcinoma in situ, or invasive carcinoma and are staged based on extension into local tissues and metastasis to distant organs. Vaginal cancer is generally asymptomatic, discovered by vaginal cytologic examination, and confirmed by colposcopy and biopsy. The major symptom of invasive cancer, independent of type, is vaginal bleeding (bloody discharge). Advanced disease causes vaginal discharge, vulvar pruritus, rectal or bladder symptoms, and pain or leg edema.
Biopsy techniques confirm the tumor type and determine its size, location, and extent. Treatment depends on these findings and the age of the individual. Vaginal dysplasia or carcinoma in situ is excised with upper vaginectomy, laser ablation or loop electrosurgical excision, cryotherapy, or laser surgery.108 Topical 5-fluorouracil (5-FU) also may be used. If the lesion is invasive, surgery may include hysterectomy and pelvic bilateral inguinal lymphadenectomy. Radiation and chemotherapy may follow surgery. Approximately 40% of individuals with invasive vaginal cancer develop recurrent cancer, which usually is confined to the pelvic area. The 5-year survival rate is 70% to 75% for early disease, 30% to 40% for stage III, and rare for stage IV.
Vulvar Cancer
Cancer of the vulva is responsible for about 3% to 5% of all gynecologic cancers107; an incidence of 3580 new cases was estimated for 2009.1 The majority (90%) are squamous cell carcinomas, although melanoma (5%), Bartholin gland carcinoma (2%), sarcoma (2%), and adenosquamous carcinoma (1%) may occur.110 A history of HPV infection is a risk factor but less so than with cervical or vaginal lesions. Squamous dysplasia of the vagina or cervix is a major risk factor,109 as are smoking and coffee use.110 Although it usually affects postmenopausal women (median age of presentation is women in their 60s), vulvar cancer has been diagnosed in women between ages 30 and 90. Although leukoplakia and lichen sclerosus were believed to be precursors, no prospective studies have been able to confirm such a relationship. Usually, women have a long history of vulvar irritation and pruritus (70%); urinary symptoms and discharge are less common. In addition, women may have a hard ulcerated area of the vulva, large cauliflower lesions, or lesions similar to those of chronic dermatitis. Biopsy confirms the diagnosis. Treatment options include primarily ablative or excisional surgery, and sometimes radiation with or without chemotherapy.110 Topical treatments under investigation include imiquimod cream, cidofovir emulsion, and 5-FU cream. Prognosis depends on lesion size and location, histology, and lymph involvement; risk of metastasis increases with tumor size. The 5-year survival rate is 85% to 90% for stage I and decreases to 20% for stage IV cancer.110
Endometrial Cancer and Uterine Sarcoma
Endometrial carcinomas arise within the glandular epithelium of the uterine lining. Cancer of the endometrium is the most common cancer of the pelvic region in women and accounts for 5.8% of all cancers in women. Estimates include 40,100 new cases in 2008, with approximately 3470 deaths.1,107 Although incidence rates are higher in white than in black women, mortality rates in black women are nearly twice as high. Most cases occur in postmenopausal women (Figure 23-19), with peak incidence occurring in the late 50s to early 60s.111 One in 30 American women will develop endometrial cancer. The primary risk factor is unopposed estrogen exposure with resultant hyperplasia.111 The World Health Organization has divided endometrial hyperplasia into two major categories according to whether cytologic atypia is present; only atypical hyperplasia has a significant risk of progressing to well-differentiated endometrial carcinoma. Estrogen-related exposures include unopposed (without an accompanying progestin) estrogen replacement therapy, tamoxifen, early menarche, late menopause, never having children, and a failure to ovulate (i.e., PCOS and anovulatory cycles typical of the late reproductive years). Obesity also is a known source of endogenous estrogen and is a risk factor for endometrial cancer. Other coexisting factors include diabetes, gallbladder disease, and hypertension likely related to obesity effects. A family history of colon, endometrial, or ovarian cancer could signal hereditary nonpolyposis colorectal cancer (HNPCC) and indicates further genetic testing.112

Figure 23-19 Endometrial cancer. Tumor fills the endometrial cavity. Obvious myometrial invasion is seen. (From Damjanov I, Linder J, editors: Anderson’s pathology, ed 10, St Louis, 2000, Mosby.)
Pregnancy and the use of combined hormonal contraceptives (i.e., COCs) containing synthetic estrogen and progestin have a protective effect as do progestin-containing IUDs.113 After 12 months of COC use, the risk of endometrial cancer is half that among women who have never used COCs; this effect seems to persist for at least 10 to 20 years after birth control pills are discontinued.111 Controlling obesity, hypertension, and diabetes may reduce an individual’s risk of endometrial cancer. A review of modifiable risk factors and prevention for endometrial hyperplasia and cancer indicates that obesity, inactivity, and dietary habits are considerable risk factors.114 The review authors advise that endometrial cancer prevention should also target these modifiable risk factors to include exercise, weight reduction, and increased fiber.115
About 75% of endometrial cancers are adenocarcinomas. Abnormal vaginal bleeding is the most common clinical manifestation of endometrial cancer. The bleeding is caused by disruption of the endometrial surface by neoplastic processes. Pain and weight loss are symptoms of late disease.
Screening methods for early detection of endometrial cancer are as effective as those for cervical cancer. Pap tests, which are highly effective in detecting cervical dysplasia, are ineffective in detecting early endometrial cancer.111 Endometrial biopsies, which allow for direct cytologic sampling of the endometrium, are required for diagnosis and are recommended to screen high-risk women at menopause and periodically. Transvaginal ultrasound (TVUS) may be used to measure endometrial thickness and screen postmenopausal and high-risk premenopausal women. An endometrial depth of less than 5 mm is suggestive of atrophic endometrium.111 Although cancer antigen (CA-125) is not a useful screen for endometrial cancer, it may predict the presence of extrauterine diseases that contribute to an undesired estrogenic environment (i.e., ovarian granulosa cell tumors increase estrogen levels and have an associated 30% risk of endometrial cancer).111 Once cancer is confirmed by biopsy, a laparoscopy may be performed to determine stage of disease. Evaluation for metastasis includes routine blood work, metabolic studies, chest x-rays, intravenous pyelography (IVP), barium enema, ultrasonography, lymphangiography, CT, MRI, and bone scans.
Treatment is based on the extent of the disease. For women with nonatypical hyperplasia, progestin therapy (orally or through levonorgestrel-containing IUD) may often suffice. However, treatment for atypical hyperplasia usually includes surgical intervention, such as curettage for carcinoma in situ, total abdominal hysterectomy with bilateral salpingo-oophorectomy, and lymphadenectomy. Chemotherapy, radiation, or hormone therapy with progestins also may be used in combination. The 1-year relative survival rate for endometrial cancer is 93%; the 5-year relative survival rate is 95% with early diagnosis and 64% if diagnosis occurred in the late stage. Relative survival rates for white women exceed those for black women by at least 18% at every stage.
Uterine sarcomas are rare neoplasms that arise from myometrial smooth muscle, endometrial stroma, or more rarely ubiquitous connective tissue elements. Uterine sarcomas constitute 2% to 8% of all uterine malignancies. The average age at diagnosis is the early 50s. The very low occurrence of these tumors explains the lack of epidemiologic data. Thus relatively few risk factors have been identified. However, chronic excess estrogen exposure, tamoxifen, and black race have been cited as risks. Symptoms include abnormal uterine bleeding, awareness of a mass, and pelvic pressure or pain. Vaginal discharge may be profuse and foul. Gastrointestinal and genitourinary complaints are common. The uterus often enlarges rapidly. Most commonly, serendipitous diagnosis occurs at the time of surgery for leiomyomas. Treatment consists of total hysterectomy with bilateral salpingo-oophorectomy and selective lymphadenectomy followed by radiation therapy. Five-year survival rates range from 50% in early disease to 5% in advanced disease. Like most cancers, stage is the most important determinant of prognosis. The survival rate at 5 years for stage I disease is 50%. Few women survive advanced-stage disease.116
Ovarian Cancer
The incidence of ovarian cancer is estimated as 21,550 women in the United States in 2009.1 In 2009 ovarian cancer accounted for 3% of all cancers among women and caused more deaths (14,600) than any other female reproductive cancer.1 From 2001 to 2005, the incidence declined at a rate of 3% per year. Ovarian cancer in women older than 40 years is associated with early menarche, late menopause, nulliparity, and the use of fertility drugs. Race and prior pelvic radiation also appear to increase risk. Factors that suppress ovulation decrease the risk of ovarian cancer and include multiple pregnancies, prolonged lactation, and the use of oral contraceptives. Oral contraceptives inhibit ovulation, and progestins likely have a direct biologic effect on ovarian tissue.117
PATHOGENESIS The cause of ovarian cancer is unknown at present. The great majority (approximately 90%) of ovarian cancers are sporadic and not associated with a known pattern of inheritance.118 Of the 5% to 10% that are familial, the majority are associated with the breast cancer susceptibility gene 1 (BRCA1) and a smaller number with mutations of BRCA2 or mismatched repair genes (HNPCC syndrome). Various pathways have been proposed, including the aberrant cellular proliferation that occurs with repetitive ovulatory tissue repair in the ovary. Spontaneous TP53 (a tumor-suppressor gene) mutations accompany this proliferation and likely play a major role in carcinogenesis activity.119 In sporadic ovarian cancer, BRCA1 and BRCA2 are rarely mutated.
The two major types of ovarian cancer are epithelial ovarian neoplasms and germ-cell neoplasms. Most ovarian malignancies are epithelial ovarian neoplasms that usually develop from the surface epithelium of the ovary or that which line cysts immediately beneath the ovarian surface. Most epithelial cancers arise from a single cell (i.e., clonal), involve loss of tumor suppressor genes, and activate oncogenes (see Chapter 11). Therefore, a number of abnormalities, including LOH, and amplification of several chromosomes are observed. Epithelial ovarian tumors may be serous, mucinous, endometrioid, or undifferentiated. These tumors are classified as (1) benign, (2) borderline malignant, or (3) frankly malignant (Figure 23-20). The malignant forms are collectively classed as ovarian adenocarcinomas and account for 90% of all ovarian malignancies. Of the ovarian adenocarcinomas, 40% to 50% are serous epithelial malignancies, which usually involve both ovaries and tend to be bulky. Serous tumors generally affect women from 50 to 55 years of age and are extremely rare in prepubertal girls. The 5-year survival rate is 90% if treated in stage I; however, only 25% of ovarian cancers are diagnosed this early. Five-year survival rates decline with stage of disease: 40% to 60% of women with stage II disease survive 5 years, 15% to 20% with stage III disease survive 5 years, and less than 5% with stage IV disease survive 5 years.120
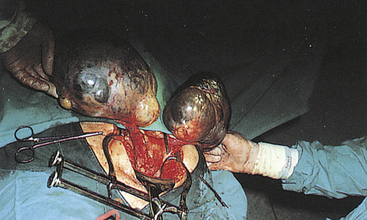
Figure 23-20 Ovarian tumors. Bilateral multicystic ovarian tumors. (From Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Germ-cell tumors are derived from the primitive germ cells (gametes) of the embryonic gonad and may be malignant or benign. The benign cystic teratoma accounts for approximately 10% of all ovarian tumors. If the germ-cell tumor is malignant, it tends to be a highly aggressive and rapidly growing tumor with a poor prognosis. Germ-cell tumors almost always occur in children or adolescents.
CLINICAL MANIFESTATIONS Given the location of the ovaries, assessing abnormalities on routine gynecologic examination poses difficulty. Furthermore, early disease is commonly asymptomatic. Thus the disease is frequently diagnosed after metastasis has occurred. Consequently, ovarian cancer is often termed the silent killer. The intrapelvic location of the ovaries and the range of tumor activity (from slow to rapid and relentless growth) cause diverse signs and symptoms. The most obvious symptoms are pain and abdominal swelling that arise from the primary ovarian mass or ascites and abdominal distention (Figure 23-21). Gastrointestinal manifestations may include dyspepsia, vomiting, and alterations in bowel habits caused by mechanical obstruction. Abnormal vaginal bleeding may occur if the postmenopausal endometrium is stimulated by a hormone-secreting tumor. The tumor also may cause ulcerations through the vaginal wall that result in bleeding. There also can be a feeling of pressure in the pelvis and leg pain.
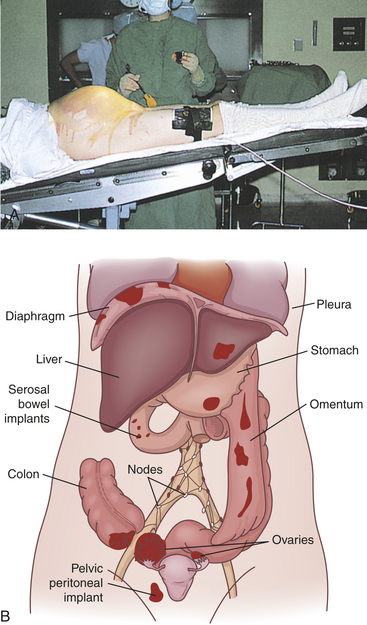
Figure 23-21 Large malignant ovarian tumor and metastasis of ovarian cancer. A, Tumor has caused massive abdominal distention. B, Pattern of spread for epithelial cancer of the ovary. (A from Symonds EM, Macpherson MBA: Color atlas of obstetrics and gynecology, London, 1994, Mosby-Wolfe.)
Systemic manifestations of nonmetastatic malignant disease include connective tissue inflammation (dermatomyositis), abnormal pigmentation (acanthosis nigricans), and subacute cerebellar degeneration. Tumor obstruction of vascular channels can cause venous and, occasionally, arterial thrombosis. Alterations in coagulability also occur, contributing to clot formation. Metastasis often causes pleural effusion.
EVALUATION AND TREATMENT Because ovarian cancer has no early symptoms and no effective screening techniques can detect it, disease usually is advanced by the time treatment is sought. Diagnosis is confirmed by biopsy, and extent of the disease is determined by ultrasound, CT, MRI, or other imaging techniques. Women undergoing surgery for early-stage ovarian cancer need thorough checking for spread to the abdomen and lymph nodes. Staging of disease requires exploratory surgery. The International Federation of Gynecologists and Obstetricians (FIGO) staging system is described in Table 23-8. Other preoperative studies may be used to determine the extent of metastasis. These include an upper gastrointestinal series, barium enema, IVP, mammography, and lymphography.
Table 23-8
FIGO Staging of Carcinoma of the Ovary
| Stage | Characteristics |
| I | Growth limited to the ovaries |
| IA | Growth limited to one ovary; no ascites |
| IA1 | No tumor on the external surface; capsule intact (90% 5-year survival with treatment) |
| IA2 | Tumor present on the external surface, or capsule(s) ruptured, or both |
| IB | Growth limited to both ovaries; no ascites |
| IB1 | No tumor on the external surface; capsule intact |
| IB2 | Tumor present on the external surface, or capsule(s) ruptured, or both |
| IC | Tumor either stage IA or stage IB, with ascites present or with positive peritoneal washings |
| II | Growth involving one or both ovaries with pelvic extension |
| IIA | Extension and/or metastases to the uterus and/or tubes |
| IIB | Extension to other pelvic tissues |
| IIC | Tumor either stage IIA or stage IIB but with ascites present or with positive peritoneal washings |
| III | Growth involving one or both ovaries with intraperitoneal metastases outside the pelvis, or positive retroperitoneal nodes, or both; tumor limited to the true pelvis with histologically proven malignant extension to small bowel or omentum |
| IV | Growth involving one or both ovaries with distant metastases; if pleural effusion is present, there must be positive cytology to allot a case to stage IV; parenchymal liver metastases indicate stage IV |
| Special category | Unexplored cases that are thought to be ovarian carcinoma |
FIGO, International Federation of Gynecologists and Obstetricians.
The search for a tumor marker that could be used as a screening tool for ovarian cancer is ongoing. Some types of germ cells and, rarely, adenocarcinoma may be associated with increased levels of alpha fetoprotein (AFP), hCG, or CA-125. Increased CA-125 levels are found in about 78% to 80% of nonmucinous ovarian cancers; however, elevated levels are produced in 29% of nongynecologic tumors and in a variety of noncancerous conditions, for example, endometriosis, PID, benign ovarian cysts, myomas, and pregnancy. Carcinoembryonic antigen is a nonspecific, nonsensitive test for ovarian cancer; when combined with transvaginal ultrasound, it is more sensitive and accurate than pelvic examination alone. Using a panel of markers may be more sensitive and specific. Further research is needed.121
The initial approach to treatment is surgery, which is performed to determine the stage of disease and to remove as much of the tumor as possible. Radiation therapy may follow if the tumor is smaller than 2 cm and is confined to the abdominopelvic area without involvement of the kidneys or liver. Radiation therapy may be administered externally, intraperitoneally, or both. The success of chemotherapy depends on whether the tumor is a discrete mass, the extent of disease, and whether there has been exposure to chemotherapeutic agents. The gold standard for previously untreated individuals is taxane and platinum.122 Most people, however, suffer relapses and less than 20% survive long term with stage III or IV disease. New therapies have extended clinical trials, including small-molecular-weight inhibitors, monoclonal antibodies, antisense therapy, and gene therapy.122
Sexual Dysfunction
Increased awareness of female sexual dysfunction is relatively new, and most of what is known comes from clinical observations and anecdotal reports from women. Adequate research is still needed. Both organic and psychosocial disorders can be implicated in sexual dysfunction. Organic problems may be the underlying cause in 10% to 20% of cases and can contribute to another 15%. The exact cause may not always be identified.
As in men, chronic illness can affect sexual functioning and response in women. For example, neuropathy in the pelvic region may increase the threshold for orgasm in diabetic women. Diminished intensity and gradual decline in orgasm may be analogous to the development of impotence in diabetic men. For women with heart disease, problems in sexual functioning more often are related to drug therapy than the disease itself. Table 23-9 outlines possible effects of specified chronic diseases on female sexual functioning.
Table 23-9
Possible Effects of Chronic Disease on Sexual Functioning in Women
| Disease | Sexual Function |
| Cerebral palsy | Intact genital sensations, decreased lubrication; difficulty with sexual activity/positioning because of muscle spasticity, rigidity, and/or weakness; pain with positioning caused by contracture of knees and hips or because of increased spasms with arousal |
| Cerebrovascular accident (CVA) | Difficulties in sexual positioning and sensitivity because of impaired motor strength, coordination or paralysis; decreased sex drive with stroke on the dominant side of the brain |
| Diabetes | Diminished intensity of orgasm and gradual decline in ability to achieve orgasm; decreased lubrication and/or recurrent vaginal infections with resultant dyspareunia |
| Chronic renal failure | Decreased arousal; increasingly rare and less intense orgasms; decreased lubrication |
| Rheumatoid arthritis (RA) | Painful sexual activity/positions because of swollen, painful joints, muscular atrophy and joint contracture; decreased sex drive because of pain, fatigue, and/or medication; genital sensations remain intact |
| Systemic lupus erythematosus (SLE) | Similar to RA; decreased lubrication and vaginal lesions result in painful penetration |
| Myocardial infarction (MI) | Most literature male oriented; problems related to medications |
| Multiple sclerosis (MS) | Diminished genital sensitivity; decreased lubrication; declining orgasmic ability; difficulty with sexual activity because of muscle weakness, pain, or incontinence |
| Spinal cord injury | Reflex sexual response with injury above sacral area; disrupted response with lesion at or below sacrum; loss of sensation, decreased lubrication; spasticity, incontinence, or pain with arousal; continued orgasmic sensations or sensations diffused in general or to specific body parts, such as breast or lips |
Disorders of desire (inhibited sexual desire, decreased libido) may be a biologic manifestation of depression, alcohol or other substance abuse, prolactin-secreting pituitary tumors, or testosterone deficiency. β-Adrenergic blockers used for heart disease also may inhibit sexual desire.
Vaginismus is an involuntary muscle spasm in response to attempted penetration. Common causes include prior sexual trauma or fear of sex; organic causes are less common and are similar to those that cause dyspareunia, including vulvovestibulitis. Even after the underlying organic problem is detected and successfully treated, vaginismus may persist.
Anorgasmia or orgasmic dysfunction is the inability of the woman to reach or achieve orgasm. Dysfunction follows a continuum from difficulty in arousal to lack of orgasm. Any chronic illness may affect arousal. Orgasmic dysfunction is linked to organic causes in less than 5% of cases. Diabetes, alcoholism, neurologic disturbances, hormonal deficiencies, and pelvic disorders, such as infections, trauma, and surgical scarring, are specific disorders that may block orgasm. Narcotics, tranquilizers, antidepressants, and antihypertensive medications also can inhibit orgasm.
Rapid orgasm is a relatively new diagnosis and seems to be rare. In this instance, once orgasm occurs there is little interest in further sexual activity. Rapid orgasm has no known organic cause.
Dyspareunia (painful intercourse) is common. Women may experience pain during arousal, at the time of orgasm, at the initiation of intercourse, midway during intercourse, or after intercourse. The pain may have a burning, sharp, searing, or cramping quality and may be described as external, vaginal, deep abdominal, or pelvic. A variety of psychosocial and organic causes have been identified. Inadequate lubrication may make penetration or intercourse difficult or painful. Drugs with a drying effect, such as antihistamines, certain tranquilizers, and marijuana, and disorders such as diabetes, vaginal infections, and estrogen deficiency can decrease lubrication. Other causes of dyspareunia include skin problems around the introitus or affecting the vulva; irritation or infection of the clitoris; disorders of the vaginal opening, such as scarring from episiotomy, intact hymen, or chronically infected hymenal remnants; bartholinitis; disorders of the urethra or anus; disorders of the vagina, such as infections, thinning of the walls caused by aging or decreased estrogen, or irritation caused by spermicides or douches; and pelvic disorders, such as infection, tumors, cervical or uterine abnormalities, and torn uterine ligaments.
Sexual dysfunction may develop as a coping mechanism. Women with a history of sexual trauma—rape, incest, or molestation—often have problems of desire, arousal, or orgasm or experience pain with sexual activity. In extreme cases total sexual aversion may develop. At other times, sexual dysfunction may be a symptom of marital or relationship problems. Unresolved anger may manifest as inhibited desire or diminished arousal. A population study indicated that relationship factors are more important in decreasing libido than age or menopause, whereas physiologic and psychologic factors are more prominent in genital arousal with decreased organic functioning.123
Impaired Fertility
Infertility affects approximately 15% of all couples and is defined as the inability to conceive after 1 year of unprotected intercourse with the same partner. Fertility can be impaired by factors in the man or the woman or both partners. Male factors include diminished quality and production of sperm and female factors are associated with malfunctions of the fallopian tubes, ovaries, or reproductive hormones. Adhesions from pelvic infection may cause blockage of one or both fallopian tubes, preventing access of the sperm to the ovum. Hormonal or local factors may disrupt ovulation or prevent a fertilized egg from implantation. Hyperthyroidism in males may affect production of sperm and motility.124 Hypothyroidism in females is also related to infertility as previously discussed. A number of diagnostic procedures are required in the routine investigation of the infertile couple (see Table 22-3). In many instances no cause may be identified.
Treatment of infertility is aimed toward correcting problems identified during the diagnostic workup. The best treatment for infertility is prevention, specifically of sexually transmitted infection that can result in scarring and adhesion formation in the reproductive tract of a man or woman.
Fertility Tests
Tests of reproductive function are performed most commonly when infertility exists. Both partners are examined, and several diagnostic evaluations may be completed. The types of tests and their normal values are summarized in Table 21-4. The man is evaluated for number, amount, structure, and motility of sperm and obstruction along the reproductive tract. Tests for women determine whether (1) the reproductive tract (cervix, uterus, fallopian tubes) is adequately patent to allow for passage of ovum and sperm, (2) ovulation occurs normally, (3) the endometrium is responding normally to hormones, and (4) reproductive tissues are free of tumors or infections. Hormonal assays evaluate the adequacy of pituitary function and target organ response. The position and size of organs or the presence of tumors can be detected by direct observation procedures using a laparoscope or by radiographic studies, such as plain films, or CT. Before testing and treatment, assessing knowledge of fertility with timing of sexual intercourse is essential. A mature ovum remains viable for 12 to 24 hours, and sperm retain their fertility for up to 5 days. A prospective study showed that almost all pregnancies resulted from sexual intercourse during a 6-day period ending on the day of ovulation.125