The rheumatological history
The rheumatism is a common name for many aches and pains which have yet got no peculiar appellation, though owing to very different causes.
Presenting symptoms
The major presenting symptoms of the rheumatological history are shown in List 23.1.
PERIPHERAL JOINTS
Pain and swelling
The underlying aetiology of joint pain can often be worked out by asking about the distribution, duration and characteristic of joint involvement: see Questions box 23.1.
Questions box 23.1
Questions to ask the patient with joint pain
 denotes symptoms for the possible diagnosis of an urgent or dangerous (alarm) problem.
denotes symptoms for the possible diagnosis of an urgent or dangerous (alarm) problem.
2. Is it only one joint (monoarthritis) or several joints (polyarthritis)? Show me where. (Lists 23.2, 23.3 and 23.4)
3. Are the joints swollen or red (arthritis), or not (arthralgia)?
4. Are they getting better or worse?
5. Is the pain worse in the morning (morning stiffness: rheumatoid arthritis) or after exercise (osteoarthritis)?
6. Have you injured the joint?
7. Is the pain worse at night? (Back pain especially—malignancy)
It is often useful to ask the patient to point to the painful place or area. For example, pain said to affect the knee may be in the popliteal fossa, the knee joint itself or the supra- or infra-patellar bursa. Remember also that pain in the knee or lower thigh may be referred from the hip (see Figure 23.1).
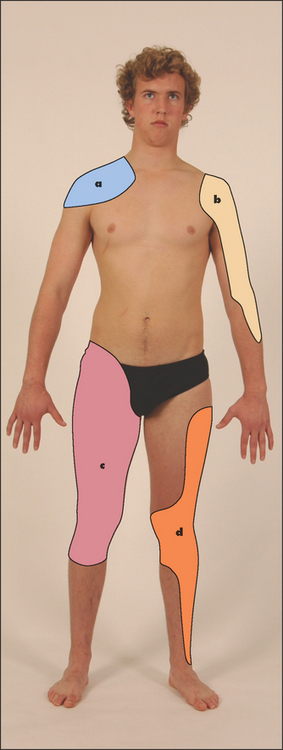
Figure 23.1 Map of referral patterns for different joints (a) Acromioclavicular and sternoclavicular joints; (b) scapulohumeral joint; (c) hip; (d) knee. (Adapted from Epstein O et al. Clinical examination, 4th edn. Edinburgh: Mosby, 2008.)
Patterns of presentation with rheumatological disease that can help establish the differential diagnosis include the following:
• Articular vs non-articular (joint itself or surrounding structures such as tendons)
• Inflammatory vs non-inflammatory (e.g. rheumatoid vs osteoarthritis)
• Peripheral vs axial (i.e. spinal or sacroiliac)
• Additive vs migratory (joints improve and new ones become involved) vs palindromic (recurrences and relapses)
• Inflammatory monoarthritis vs oligoarthritis (2–5 joints) vs polyarthritis (>5 joints)
The causes of monoarthritis (single joint) and polyarthritis (more than one joint) are outlined in Lists 23.2 and 23.3, and the patterns of polyarthritis in various diseases are outlined in List 23.4.
Morning stiffness
Ask about the presence of early-morning stiffness and the length of time that this stiffness lasts (typically it lasts for at least an hour). Morning stiffness classically occurs in rheumatoid arthritis and other inflammatory arthropathies, and the duration of stiffness is a guide to its severity. Stiffness after inactivity, such as sitting, is characteristic of osteoarthritis of the hip or knee.
Deformity
The patient may have noticed deformity of a joint or bone. If there has been progressive change in the shape of the area, this is more likely to be significant.
Instability
Joint instability may be described by the patient as a ‘giving way’, or occasionally ‘coming out’, of the joint in certain conditions. This may be due to true dislocation (e.g. with the shoulder or the patella) or alternatively to muscle weakness or ligamentous problems.
Change in sensation
This may occur as a result of nerve entrapment or injury, and sometimes as a result of ischaemia. Ask about numbness or paraesthesias (pins and needles). The distribution of the change of sensation should help distinguish nerve damage or entrapment (a specific distribution) from ischaemia.
Up to 50% of type 1 and some type 2 diabetics develop diabetic cheiroarthritisa The small and then larger joints of the hands are involved. There is pain and restriction of movement, especially extension of the fingers. The skin becomes thickened and tight. The cause is probably diabetic microangiopathy, which leads to damage to the skin and connective tissue.
BACK PAIN
This is a very common symptom. It is most often a consequence of local musculoskeletal disease.
Ask where the pain is situated, whether it began suddenly or gradually, whether it is localised or diffuse, whether it radiates to the limbs or elsewhere, and whether the pain is aggravated by movement, coughing or straining. Musculoskeletal pain is characteristically well localised and is aggravated by movement. If there is a spinal nerve root irritation there may be pain that occurs in a dermatomal distribution. This helps to localise the level of the lesion. Diseases such as osteoporosis (with crush fractures), infiltration of carcinoma, leukaemia or myeloma may cause progressive and unremitting back pain, which is often worse at night. The pain may be of sudden onset but is usually self-limiting if it results from the crush fracture of a vertebral body. In ankylosing spondylitis the pain is usually situated over the sacroiliac joints and lumbar spine; it is also worse at night and is associated with morning stiffness. The pain of ankylosing spondylitis is typically better with activity, which helps distinguish it from mechanical back pain.1,2 Pain from diseases of the abdomen and chest (e.g. dissecting abdominal or thoracic aortic aneurysm) can also be referred to the back.
LIMB PAIN
This can occur from disease of the musculoskeletal system, the skin, the vascular system or the nervous system.
Musculoskeletal pain may be due to trauma or inflammation. Muscle disease such as polymyositis can present with an aching pain in the proximal muscles around the shoulders and hips, associated with weakness. Pain and stiffness in the shoulders and hips in patients over the age of 50 years may be due to polymyalgia rheumatica. The acute or subacute onset of symptoms in multiple locations suggests an inflammatory process. Bone disease such as osteomyelitis, osteomalacia, osteoporosis or tumours can cause limb pain. Inflammation of tendons (tenosynovitis) can produce local pain over the affected area.
Vascular disease may also produce pain in the limbs. Acute arterial occlusion causes severe pain of sudden onset, often with coolness or pallor. Chronic peripheral vascular disease can cause intermittent claudication (page 87). Venous thrombosis can also cause diffuse aching pain in the legs associated with swelling.
Spinal stenosis can cause pseudo-claudication pain on walking but relieved by leaning forwards.
Nerve entrapment and neuropathy can both cause limb pain that is often associated with paraesthesias or weakness. The usual cause is synovial thickening or joint subluxation, especially for patients with rheumatoid arthritis. The vasculitis associated with the inflammatory arthropathies can also cause neuropathy leading to diffuse peripheral neuropathy or mononeuritis multiplex. Patients with chronic rheumatoid arthritis often develop subluxation of the cervical spine at the atlanto-axial joint. This is caused by erosion of the transverse ligament around the posterior aspect of the odontoid process (dens). The patient may describe shooting paraesthesias down the arms and an occipital headache. Neck flexion leads to indentation of the cord by the dens and can cause tetraplegia or sudden death. The abnormality may be obvious on lateral X-rays of the cervical spine (see Figure 26.3 on page 345). Injury to peripheral nerves can result in vasomotor changes and severe limb pain. This is called causalgia. Even following amputation of a limb, phantom limb pain may develop and persist as a chronic problem.
RAYNAUD’S PHENOMENON
Raynaud’sb phenomenon is an abnormal response of the fingers and toes to cold. Classically, the fingers first turn white, then blue and finally red after exposure to cold. It may be painful. Patients with Raynaud’s disease have Raynaud’s phenomenon without an obvious underlying cause. The disease tends to be familial and females are more likely to be affected. This is a benign condition. However, Raynaud’s phenomenon in patients with connective tissue diseases, especially systemic sclerosis, can lead to the formation of digital ulcers (see List 23.5). It may be the first sign of this condition (see Figure 21.1).
DRY EYES AND MOUTH
Dry eyes and dry mouth are characteristic of Sjögren’s syndrome (see List 23.6). This syndrome may occur in isolation (primary Sjögren’s) and is very common in association with rheumatoid arthritis and other connective tissue disease. Mucus-secreting glands become infiltrated with lymphocytes and plasma cells, which cause atrophy and fibrosis. The dry eyes can result in conjunctivitis, keratitis and corneal ulcers. Sjögren’s syndrome can also have an effect on other organs such as the lungs or kidneys.
RED EYES
The spondyloarthritides and Behçet’sc syndrome, but not rheumatoid arthritis, may be complicated by iritis (eye pain with central scleral injection—a ‘red eye’—radiating out from the pupil; see Figure 25.3 on page 329). In other diseases, such as Sjögren’s, red eyes may be due to dryness, episcleritis or scleritis.
SYSTEMIC SYMPTOMS
Fatigue is common with connective tissue disease. Weight loss and diarrhoea may occur with systemic sclerosis, because of small-bowel bacterial overgrowth. Mucosal ulcers and rashes are common in some connective tissue diseases such as systemic lupus erythematosus (SLE). Generalised stiffness can be due to rheumatoid arthritis or systemic sclerosis, but other causes include systemic infection (e.g. influenza), excessive exercise, polymyalgia rheumatica, neuromuscular disease (e.g. extrapyramidal disease, tetanus, myotonia, dermatomyositis) and hypothyroidism. Finally, on occasion fever may be associated with the connective tissue diseases, especially SLE, but infection should always be excluded.
Treatment history
Document current and previous anti-arthritic medications (e.g. non-steroidal anti-inflammatory drugs [NSAIDs], sulfasalazine, lefunomide, hydroxychloroquine, gold, methotrexate, steroids, tumour necrosis factor inhibitors and other biological agents). Any side effects of these drugs (e.g. gastric ulceration or haemorrhage—NSAIDs), steroid side effects or serious infections (biological agents) also need to be identified. Ask about physiotherapy and joint or tendon surgery in the past.
Past history
It is important to enquire about any history of trauma or joint surgery (perhaps just another type of trauma) in the past. Similarly, a history of recent infection—including hepatitis, streptococcal pharyngitis, rubella, dysentery, gonorrhoea or tuberculosis—may be relevant to the onset of arthralgia or arthritis. A history of tick bite may indicate that the patient has Lyme disease, but Ross river fever and parvovirus infection are more common associations with arthritis in Australia. Inflammatory bowel disease may be associated with arthritis, as described on page 224. A history of psoriasis may indicate that the arthritis is due to psoriatic arthritis. Joint disease may precede the rash in patients with psoriatic arthritis, so a family history of psoriasis (first-degree relative) may be a clue to this condition. It is also important to enquire about any history of arthritis in childhood. The smoking history is important: rheumatoid arthritis is more common in smokers, and smoking adds to their already increased risk of cardiovascular disease.
Social history
Determine the patient’s ability to function (see Table 23.1). Ask about the domestic set-up, occupation, hobbies and sporting interests. This is particularly relevant if a chronic disabling arthritis has developed. Any history of sexually transmitted infection in the past is important, but nonspecific urethritis and gonorrhoea are especially relevant.
TABLE 23.1
Functional assessment in rheumatoid arthritis
| Class | Assessment |
| Class 1 | Normal functional ability |
| Class 2 | Ability to carry out normal activities, despite discomfort or limited mobility of one or more joints |
| Class 3 | Ability to perform only a few of the tasks of the normal occupation or of self-care |
| Class 4 | Complete or almost complete incapacity, with the patient confined to a wheelchair or to bed |
Family history
Some diseases associated with chronic arthritis run in families. These include rheumatoid arthritis, gout and primary osteoarthritis, haemochromatosis, the spondyloarthritides and inflammatory bowel disease. A family history of bleeding disorder may explain an acutely swollen tender joint in a boy (haemophilia).
References
1. Van den Hoogen, HMM, Koes, BW, Van Eijk, JTM, Bouter, LM. On the accuracy of history, physical, and the erythrocyte sedimentation rate in diagnosing low back pain in general practice: a criteria based review of the literature. Spine. 1995; 20:318–327. [Unfortunately, distinguishing mechanical from non-mechanical causes of low back pain such as ankylosing spondylitis is clinically difficult. However, tenderness to pressure over the anterior superior iliac spines and over the lower sacrum may, based on other studies, be somewhat helpful for the positive diagnosis of ankylosing spondylitis.].
2. Deyo, RA, Rainville, J, Kent, DL. What can the history and physical examination tell us about low back pain. JAMA. 1992; 268:760–765.