Chapter Seven The health history
The purpose of the health history is to collect subjective data—what the person says about themself. The history is combined with the objective data from the physical examination and laboratory studies to form the database. The database is used to make a judgment or a diagnosis about the health status of the individual.
The following health history provides a complete picture of the person’s past and present health. It describes the individual as a whole and how the person interacts with the environment. It records health strengths and coping skills. The history should recognise and affirm what the person is doing right: what they are doing to help stay well. For the well person, the history is used to assess their lifestyle, including such factors as exercise, diet, risk reduction and health promotion behaviours.
For the ill person, the health history includes a detailed and chronological record of the health problem. For all, the health history is a screening tool for abnormal symptoms, health problems and concerns, and it records ways of responding to the health problems.
In many settings the patient fills out a printed history form or checklist. This allows the person ample time to recall and consider such items as key health events and relevant family history. The interview is then used to validate the written data and to collect more data on lifestyle management and current health problems. In a hospital setting this is most often completed as part of the admission process. In some situations the nurse completes the health history at the time the person is admitted to the ward or unit. However, the health history may also be completed prior to the person arriving at the hospital at a formal pre-admission interview, or by the person completing the printed history form themselves prior to admission. At the time of admission the nurse should always check through the information with the patient and clarify the details to ensure the information is accurate and complete.
Although history forms vary, most contain information in this sequence of categories:
The health history discussed in the following section follows this format and presents a generic database for all clinicians. Those in primary care settings may use all of it, whereas those in a hospital may focus primarily on the history of present illness and the functional, or patterns of living data. Each chapter in this textbook details specific areas for subjective data collection relevant to the particular area being assessed. The following information provides an overview of the health history including biographical data, the reasons for seeking care, past history and history of present illness (including analysis of symptoms) and review of symptoms, function and risk.
THE HEALTH HISTORY—THE ADULT
Biographical data
The biographical data set includes the person’s name, address and phone number, age and birth date, gender, marital status, religion, first language spoken (and other languages), occupation, usual and present (an illness or disability may have prompted change in occupation), and next of kin name and contact details. In some circumstances the person’s nominated medical power of attorney (if any) is also recorded. The name and address of the person’s usual general practitioner is recorded. Often this information is collected and prepared on an admission form by an administrator prior to the person arriving at the ward or unit. The nurse should recheck the validity of the recorded information.
Source of history
1. Record who furnishes the information—usually the person themself, although the source may be a relative or friend.
2. Judge how reliable the informant seems and how willing they are to communicate. What is reliable? A reliable person always gives the same answers, even when questions are rephrased or are repeated later in the interview.
3. Note any special circumstances, such as the need for an interpreter. Sample statements include:
Reason for seeking care
This is a brief spontaneous statement in the person’s own words that describes the reason for the visit. Think of it as the ‘title’ for the story to follow. It states one (possibly two) symptoms or signs and their duration. A symptom is a subjective sensation that the person feels from the disorder. A sign is an objective abnormality that you as the examiner could detect on physical examination or in laboratory reports. Whatever the person says is the reason for seeking care is recorded, enclosed in quotation marks to indicate the person’s exact words.
The reason for seeking care is not a diagnostic statement. Avoid translating it into the terms of a medical diagnosis. For example, Mr J Schmidt enters with shortness of breath, and you ponder writing ‘emphysema’. Even if he is known to have emphysema from previous visits, it is not the chronic emphysema that prompted this visit, but rather the ‘increasing shortness of breath’ for 4 hours.
Some people try to self-diagnose based on similar signs and symptoms in their relatives or friends, or based on conditions they know they have. Rather than record a woman’s statement that she has ‘strep throat’, ask her what symptoms she has that make her think this is present and record those symptoms.
Occasionally a person may list many reasons for seeking care. The most important reason to the person may not necessarily be the one stated first. Try to focus on which is the most pressing concern by asking the person which one prompted them to seek help now.
PRESENT HEALTH OR HISTORY OF PRESENT ILLNESS
In this section you are trying to ascertain how the person perceives or describes their usual level of health. For people seeking healthcare for illness, this section is a chronological record of the reason for seeking care, from the time the symptom first started until now. Isolate each reason for care identified by the person and say, for example, ‘Please tell me all about your headache, from the time it started until the time you came to the hospital’. If the concern started months or years ago, record what occurred during that time and find out why the person is seeking care now.
As the person talks, do not jump to conclusions and bias the story by adding your opinion. Collect all the data first. Although you want the person to respond in a narrative format without interruption from you, your final summary of any symptom the person has should include these eight critical characteristics:
1. Location. Be specific; ask the person to point to the location. If the problem is pain, note the precise site. ‘Head pain’ is vague, whereas descriptions such as ‘pain behind the eyes’, ‘jaw pain’ and ‘occipital pain’ are more precise and are diagnostically significant. Is the pain localised to this site or radiating? Is the pain superficial or deep?
2. Character or quality. This calls for specific descriptive terms such as burning, sharp, dull, aching, gnawing, throbbing, shooting, vice-like. Use similes—does blood in the stool look like sticky tar? Does blood in vomitus look like coffee grounds?
3. Quantity or severity. Attempt to quantify the sign or symptom such as ‘profuse menstrual flow soaking five pads per hour’. The symptom of pain is difficult to quantify because of individual interpretation. What one person may identify as ‘terrible pain’, another may describe as ‘not too bad’. With pain, avoid adjectives and ask how it affects daily activities. Then the person might say, ‘I was so sick I was doubled up and couldn’t move’, or ‘I was able to go to work, but then I came home and went to bed’.
4. Timing (onset, duration, frequency). When did the symptom first appear? Give the specific date and time, or state specifically how long ago the symptom started prior to arrival. ‘The pain started yesterday’ will not mean much when you return to read the record in the future. The report must include questions such as: How long did the symptom last (duration)? Was it steady (constant) or did it come and go during that time (intermittent)? Did it resolve completely and reappear days or weeks later (cycle of remission and exacerbation)?
5. Setting. Where was the person or what was the person doing when the symptom started? What brings it on? For example, ‘Did you notice the chest pain after mowing the lawn, or did the pain start by itself?’
6. Aggravating or relieving factors. What makes the pain worse? Is it aggravated by weather, activity, food, medication, standing bent over, fatigue, time of day, season and so on? What relieves it (e.g. rest, medication or ice pack)? What is the effect of any treatment? Ask, ‘What have you tried?’ or ‘What seems to help?’
7. Associated factors. Is this primary symptom associated with any others (e.g. urinary frequency and burning associated with fever and chills)? Review the body system related to this symptom now rather than wait for the physical assessment.
8. Patient’s perception. Find out the meaning of the symptom by asking how it affects daily activities and quality of life. Also ask directly, ‘What do you think it means?’ This is crucial because it alerts you to potential anxiety if the person thinks the symptom may be ominous.
You may find it helpful to organise this same question sequence into the mnemonic PQRSTU to help remember all the points. Note that you still need to address the patient’s perception of the problem.
P: Provocative or Palliative. What brings it on? What were you doing when you first noticed it? What makes it better? Worse?
Q: Quality or Quantity. How does it look, feel, sound? How intense/severe is it?
R: Region or Radiation. Where is it? Does it spread anywhere?
S: Severity scale. How bad is it (on a scale of 1 to 10)? Is it getting better, worse, staying the same?
T: Timing. Onset—Exactly when did it first occur? Duration—How long did it last? Frequency—How often does it occur?
U: Understand patient’s perception of the problem. What do you think it means?
Past health
Past health events may have residual effects on the current health state. Also, the previous experience with illness may give clues as to how the person responds to illness and to the significance of illness for themself.
Childhood illnesses.
Measles, mumps, rubella, chickenpox, pertussis and strep throat. Avoid recording ‘usual childhood illnesses’, because an illness common in the person’s childhood (e.g. measles) may be unusual today. Ask about serious illnesses that may have sequelae for the person in later years (e.g. rheumatic fever, scarlet fever and poliomyelitis).
Accidents or injuries.
Motor vehicle accidents, fractures, penetrating wounds, head injuries (especially if associated with unconsciousness) and burns.
Serious or chronic illnesses.
Diabetes, hypertension, heart disease, sickle-cell anaemia, cancer and seizure disorder.
Hospitalisations.
Cause, name of hospital, how the condition was treated, how long the person was hospitalised and name of the medical practitioner.
Operations.
Type of surgery, date, name of the surgeon, name of hospital and how the person recovered.
Obstetric history.
Number of pregnancies, number of deliveries in which the fetus reached full term, number of preterm pregnancies (preterm), number of incomplete pregnancies (abortions) and number of children living (living). For each complete pregnancy, note the course of pregnancy; labour and delivery; sex, weight and condition of each infant; and postpartum health.
Family history
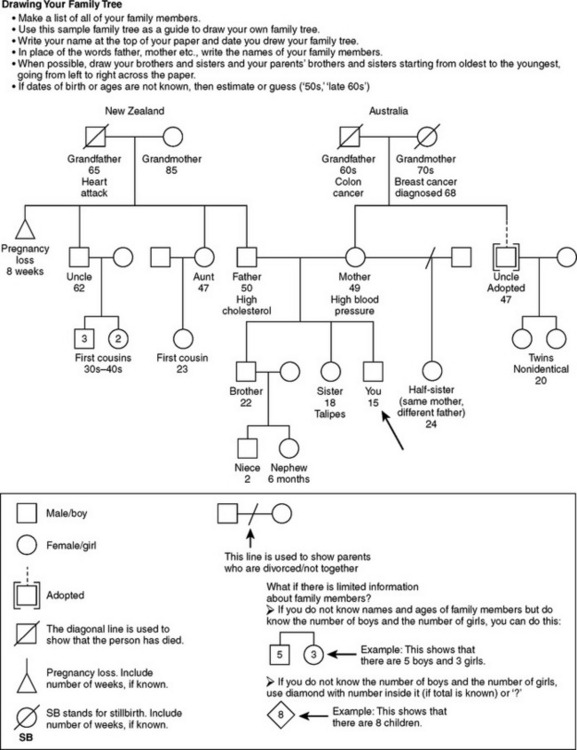
Ask about the age and health or the age and cause of death of blood relatives, such as parents, grandparents and siblings. These data may have genetic significance for the patient. Also ask about close family members, such as spouse and children. You need to know about the person’s prolonged contact with any communicable disease or the effect of a family member’s illness on this person.
Specifically ask for any family history of heart disease, high blood pressure, stroke, diabetes, blood disorders, cancer, sickle-cell anaemia, arthritis, allergies, obesity, alcoholism, mental illness, seizure disorder, kidney disease and tuberculosis. Construct an accurate family tree, or genogram, to show this information clearly and concisely (Fig 7.1).
Review of symptoms, function and risks
The purposes of this section are (1) to evaluate the past and present health state of the person, (2) to double check in case any significant data were omitted in the present illness section, (3) to evaluate health promotion practices and (4) to identify potential health risks. The items within each section are not inclusive, and only the most common symptoms are listed. If the present illness section covered one body system, you do not need to repeat all the data here. For example, if the reason for seeking care is earache, the present illness section describes most of the symptoms listed for the auditory system. Just ask now what was not asked in the ‘present illness’ section.
Another area of review is to determine the effect of illness and symptoms on the person’s function. Functional assessment measures a person’s self-care ability in the areas of general health; activities of daily living, such as bathing, dressing, toileting, eating, walking; or those needed for independent living, such as housekeeping, shopping, cooking, doing laundry, using the telephone, managing finances; nutrition; social relationships and resources; self-concept and coping; and home environment. Functional assessment may also mean that the health history may be supplemented by a standardised instrument on functional assessment. These instruments objectively measure a person’s present functional status and monitor any changes over time (Granger et al, 1995; Katz et al, 1963; Mahoney and Barthel, 1965; Pearlman, 1987). Whether or not you use any of these formalised instruments, functional assessment questions such as those listed in the following sections should be included in the standard health history. These questions provide data on the lifestyle and type of living environment to which the person is accustomed.
As you progress through each section you will also be prompted to ask questions related to the person’s usual health maintenance and health promotion strategies. This may be an opportunity for beginning health teaching. You will also identify factors that could put the person at risk during their hospitalisation or admission to the health service. For example, known areas of potential risk include; skin breakdown, unrelieved pain, falls, confusion, medication errors.
Medical terms are used below, but they need to be translated for the patient. (Note that symptoms and health promotion activities are merely listed here. These terms are repeated and expanded in each related chapter with suggested ways to pose questions and a rationale for each question.)
When recording information, avoid writing ‘NAD (no abnormalities detected)’. You need to record the presence or absence of all symptoms, otherwise the reader does not know about which factors you asked.
A common mistake made by beginning clinicians is to record some physical finding or objective data here, such as ‘skin warm and dry’. Remember that the history should be limited to patient statements or subjective data—factors that the person says were or were not present.
General overall health and wellbeing
Perception of health.
Ask the person questions such as: ‘How do you define health?’ ‘How do you view your situation now?’ ‘What are your concerns?’ ‘What do you think will happen in the future?’ ‘What are your health goals?’ ‘What do you expect from us as nurses, medical practitioners, (or other healthcare professionals)?’
Interpersonal relationships/resources.
Educational level achieved and current employment. For example: ‘How would you describe your role in the family?’ ‘How would you say you get along with family, friends and co-workers?’ Ask about support systems composed of family and significant others: ‘To whom could you go for support with a problem at work, with your health or a personal problem?’ Include contact with spouse, siblings, parents, children, friends, organisations, workplace: ‘Is time spent alone pleasurable and relaxing, or isolating?’
Values and beliefs/spiritual resources.
Cultural and ethnic background and practices as well as religious/spiritual beliefs, values and practices. For example: ‘Do you identify with any specific cultural group?’ ‘In your culture are there some health practices that are important to you?’ ‘Does religious faith or spirituality play an important part in your life? Do you consider yourself to be a religious or spiritual person?’ ‘How does your religious faith or spirituality influence the way you think about your health or the way you care for yourself?’ ‘Are you a part of any religious or spiritual community or congregation?’ ‘Would you like me to address any religious or spiritual issues or concerns with you?’
Coping and stress management.
Kinds of stresses in life, especially in the last year, any change in lifestyle or any current stress, methods tried to relieve stress and if these have been helpful. For example: ‘Have there been any significant changes in your life in the past year?’ ‘How do you think this has affected your health?’ ‘How do you relieve tension or stress?’
Health and lifestyle management
Current medications.
Note all prescription and over-the-counter medications. Ask specifically about vitamins, oral contraceptives, aspirin, sedatives and antacids, because many people do not consider these to be medications. For each medication, note the name, dose and schedule, and ask ‘How often do you take it each day?’ ‘What is it for?’ and ‘How long have you been taking it?’ If possible ask the person to bring all of their current medications in with them so that you can carefully record all of the details in the person’s history. Finally, note any complementary therapies used.
For each medication, record the name, purpose and daily schedule. Does the person have a system to remember to take the medicine? Does medicine seem to work? Are there any side effects? If so, does the person feel like skipping medicine because of them? Also consider the following issues:
• Some people take a large number of drugs, prescribed by different medical practitioners.
• Is cost a problem? When the person is unable to afford a drug, they may decrease the dosage, take one pill instead of two or not refill the empty bottle immediately.
• Is travelling to the pharmacy to refill a prescription a problem?
• Has the person ever shared medications with neighbours or friends? Some establish ‘lay referral’ networks by comparing symptoms and thus medications.
Tobacco, alcohol, street drugs.
‘Do you smoke cigarettes (pipe)?’ ‘At what age did you start?’ ‘How many packs do you smoke per day?’ ‘How many years have you smoked?’ Record the number of packs smoked per day (PPD) and duration, e.g. 1 PPD × 5 years. Then ask, ‘Have you ever tried to quit?’ and ‘How did it go?’ to introduce plans about smoking cessation.
Healthcare professionals often fail to question about alcohol unless problems are obvious. Be alert, then, to early signs of hazardous alcohol use. Ask whether the person drinks alcohol. If yes, ask specific questions about the amount and frequency of alcohol use: ‘When was your last drink of alcohol?’ ‘How much did you drink that time?’ ‘What do you drink?’ ‘Out of the last 30 days, about how many days would you say that you drank alcohol?’ ‘Have you ever had a drinking problem?’ Any history of alcohol treatment? Involvement in recovery activities? History of family member with problem drinking?
Ask specifically about marijuana, cocaine, crack cocaine, amphetamines and barbiturates. Indicate frequency of use and how usage has affected work or family.
Environment/hazards.
Housing and neighbourhood (living alone, knowledge of neighbours), safety of area, adequate heat and utilities, access to transportation and involvement in community services. Note environmental health, including hazards in workplace, hazards at home, use of seat belts, geographical or occupational exposures and travel or residence in other countries, including time spent overseas.
Occupational health.
Ask the person to describe their job. Ever worked with any health hazard, such as asbestos, inhalants, chemicals, repetitive motion? Wear any protective equipment? Any work programs in place that monitor exposure? Aware of any health problems now that may be related to work exposure? Note the timing of the reason for seeking care and whether it may be related to work or home activities, job titles or exposure history. Finally, ask the person what they like or dislike about the job.
Assessing activity and exercise
Focus your questions on the person’s usual daily activities and the effect of symptoms on their ability to be active and independent: ask ‘Tell me how you spend a typical day’. Note ability to perform ADLs: independent or needs assistance with feeding, bathing, hygiene, dressing, toileting, bed to chair transfer, walking, standing or climbing stairs. Any use of wheelchair, prostheses or mobility aids? Record leisure activities enjoyed and the exercise pattern (type, amount per day or week, method of warm-up session, method of monitoring the body’s response to exercise).
Cardiovascular function.
Precordial or retrosternal pain, palpitation, cyanosis, dyspnoea on exertion (specify amount of exertion, e.g. walking one flight of stairs, walking from chair to bath or just talking), orthopnoea, paroxysmal nocturnal dyspnoea, nocturia, oedema, history of heart murmur, hypertension, coronary artery disease, anaemia.
Bleeding tendency of skin or mucous membranes, excessive bruising, lymph node swelling, exposure to toxic agents or radiation, blood transfusion and reactions.
Coldness, numbness and tingling, swelling of legs (time of day, activity), discolouration in hands or feet (bluish red, pallor, mottling, associated with position, especially around feet and ankles), varicose veins or complications, intermittent claudication, thrombophlebitis, ulcers.
Respiratory function.
Nasal discharge and its characteristics, any unusually frequent or severe colds, sinus pain, nasal obstruction, nosebleeds, allergies or hay fever or change in sense of smell.
History of lung diseases (asthma, emphysema, bronchitis, pneumonia, tuberculosis), chest pain with breathing, wheezing or noisy breathing, shortness of breath, how much activity produces shortness of breath, cough, sputum (colour, amount), haemoptysis, toxin or pollution exposure.
Musculoskeletal function.
History of arthritis or gout. In the joints: pain, stiffness, swelling (location, migratory nature), deformity, limitation of motion, noise with joint motion? In the muscles: any pain, cramps, weakness, gait problems or problems with coordinated activities? In the back: any pain (location and radiation to extremities), stiffness, limitation of motion or history of back pain or disc disease? How much walking per day? What is the effect of limited range of motion on daily activities, such as on grooming, feeding, toileting, dressing? Are any mobility aids used?
Assessing nutrition and metabolism (including skin, hair and nails)
Mouth pain, frequent sore throat, bleeding gums, toothache, lesion in mouth or tongue, dysphagia, hoarseness or voice change, tonsillectomy, altered taste. Pattern of daily dental care, use of prostheses (dentures, bridge) and last dental checkup.
Current weight, history of sudden weight increase or loss, appetite, food intolerance, heartburn, indigestion, pain (associated with eating), other abdominal pain, pyrosis (oesophageal and stomach burning sensation with sour eructation), nausea and vomiting (character), vomiting blood, history of abdominal disease (ulcer, liver or gallbladder, jaundice, appendicitis, colitis), flatulence, use of antacids. (Alternatively, diet history and substance habits can be placed here.)
History of diabetes or diabetic symptoms (polyuria, polydipsia, polyphagia), history of thyroid disease, intolerance to heat and cold, change in skin pigmentation or texture, excessive sweating, relationship between appetite and weight, abnormal hair distribution, nervousness, tremors and need for hormone therapy.
Recall of all food and fluids taken over the last 24 hours (see Ch 16 for suggested method of inquiry). ‘Is that menu typical of most days?’ Describe eating habits and current appetite. Ask ‘Who buys food and prepares food?’ ‘Are your finances adequate for food?’ ‘Who is present at mealtimes?’ Indicate any food allergy or intolerance. Daily intake of caffeine (coffee, tea, cola drinks).
History of skin disease (eczema, psoriasis, hives), pigment or colour change, change in mole, excessive dryness or moisture, pruritus, excessive bruising, rash or lesion. Recent loss of hair, change in texture. Nails: change in shape, colour or brittleness. Amount of sun exposure; method of self-care for skin and hair.
Assessing kidney, bladder and bowel function
Kidney and bladder function.
Usual pattern of voiding, frequency, urgency, nocturia (the number of times the person awakens at night to urinate, recent change), dysuria, polyuria or oliguria, hesitancy or straining, narrowed stream, urine colour (cloudy or presence of haematuria), incontinence, history of urinary disease (kidney disease, kidney stones, urinary tract infections, prostate), pain in flank, groin, suprapubic region or low back. Measures to avoid or treat urinary tract infections, pelvic floor exercises, screening for prostate cancer. Review fluid intake—types and amount over a 24-hour period and compare to output. Review any difficulties with getting to the toilet and toileting.
Bowel function.
Usual pattern of elimination, frequency of bowel movement, any recent change, stool characteristics, constipation or diarrhoea, black stools, rectal bleeding, rectal conditions (haemorrhoids, fistula). Review any difficulties with getting to the toilet and toileting. Measures to treat bowel problems, screening for bowel cancer.
Assessing mental status, neurological and sensory function
Mental status.
Any nervousness, mood change, depression or any history of mental health dysfunction or hallucinations. Find out about interpersonal relationships, coping patterns.
Neurological.
History of seizure disorder, stroke, fainting, blackouts. In motor function: weakness, tic or tremor, paralysis or coordination problems. In sensory function: numbness and tingling (paraesthesia). In cognitive function: memory disorder (recent or distant, disorientation). Any unusually frequent or severe headache, any head injury, dizziness (syncope) or vertigo.
Assessing sexuality and reproductive function
Breast and regional lymphatics.
Breast pain, lump, nipple discharge, rash, history of breast disease, any surgery on the breasts. Axillary tenderness, lump or swelling, rash. Discuss breast awareness practices, date of last mammogram.
Male reproductive system.
Penis or testicular pain, sores or lesions, penile discharge, lumps, hernia. Presently in a relationship involving intercourse? Are the aspects of sex satisfactory to the patient and partner? Any changes in erection or ejaculation, use of contraceptive? Is the contraceptive method satisfactory? Aware of contact with a partner who has any sexually transmitted infection (gonorrhoea, herpes, chlamydia, venereal warts, HIV/AIDS or syphilis)?
Perform testicular self-examination/testicular awareness? How frequently?
Female reproductive system.
Menstrual history (age at menarche, last menstrual period, cycle and duration, any amenorrhoea or menorrhagia, premenstrual pain or dysmenorrhoea, intermenstrual spotting), vaginal itching, discharge and its characteristics, age at menopause, menopausal signs or symptoms, postmenopausal bleeding. Presently in a relationship involving intercourse? Are the aspects of sex satisfactory to the patient and partner? Any dyspareunia, use of contraceptive? Is the contraceptive method satisfactory? Aware of contact with a partner who has any sexually transmitted infection (gonorrhoea, herpes, chlamydia, venereal warts, HIV/AIDS or syphilis)?
DEVELOPMENTAL CONSIDERATIONS
Children
The health history is adapted to include information specific for the age and developmental stage of the child (e.g. the mother’s health during pregnancy, labour and delivery and the perinatal period). Note that the developmental history and nutritional data are listed as separate sections because of their importance for current health.
Biographical data
Include the child’s name, nickname, address and phone number, parents’ names and work numbers, child’s age and birth date, birthplace, gender and information on other children and family members at home.
Reason for seeking care
Record the parent’s spontaneous statement. Because of the frequency of well-child visits for routine healthcare, there will be more reasons such as ‘time for the child’s checkup’ or ‘she needs the next baby shot’. Reasons for health problems may be initiated by the child, parent or by a third party such as the classroom teacher.
Sometimes the reason stated may not be the real reason for the visit. A parent may have a ‘hidden agenda’, such as the mother who brought her 4-year-old child in because ‘she looked pale’. Further questioning revealed that the mother had heard recently from a former university friend whose own 4-year-old child had just been diagnosed with leukaemia.
Present health or history of present illness
If the parent or child seeks routine healthcare, include a statement about the usual health of the child and any common health problems or major health concerns.
Describe any presenting symptom or sign, using the same format as for the adult. Some additional considerations include:
• Severity of pain: ‘How do you know the child is in pain (e.g. pulling at ears alerts parent to ear pain)?’ Note effect of pain on usual behaviour (e.g. does it stop child from playing?).
• Associated factors, such as relation to activity, eating and body position.
• The parent’s intuitive sense of a problem. As the constant caregiver, this intuitive sense is often very accurate. Even if proved otherwise, this factor gives you an idea of parent’s area of concern.
• Parent’s coping ability and reaction of other family members to child’s symptoms or illness.
Past health
Prenatal status.
How was this pregnancy spaced? Was it planned? What was the mother’s attitude towards the pregnancy? What was the father’s attitude? Was there medical supervision for the mother? At what month was the supervision started? What was the mother’s health during pregnancy? Were there any complications (bleeding, excessive nausea and vomiting, unusual weight gain, high blood pressure, swelling of hands and feet, infections—rubella or sexually transmitted diseases, falls)? During what month were diet and medications prescribed and/or taken during pregnancy (dose and duration)? Record the mother’s use of alcohol, street drugs or cigarettes and any x-ray studies taken during pregnancy.
Start with an open-ended question: ‘Tell me about your pregnancy’. If she questions the relevancy of the statement, mention that these questions are important to gain a complete picture of the child’s health.
Labour and delivery.
Parity of the mother, duration of the pregnancy, name of the hospital, course and duration of labour, use of anaesthesia, type of delivery (vertex, breech, caesarean section), birth weight, Apgar scores, onset of breathing, any cyanosis, need for resuscitation and use of special equipment or procedures.
Postnatal status.
Any problems in the nursery, length of hospital stay, neonatal jaundice, whether the baby was discharged with the mother, whether the baby was breast or bottle fed, weight gain, any feeding problems, ‘blue spells’, colic, diarrhoea, patterns of crying and sleeping, the mother’s health postpartum and the mother’s reaction to the baby.
Childhood illnesses.
Age and any complications of measles, mumps, rubella, chickenpox, whooping cough, strep throat and frequent ear infections. Also, any recent exposure to illness.
Serious accidents or injuries.
Age of occurrence, extent of injury, how the child was treated and complications of auto accidents, falls, head injuries, fractures, burns and poisonings.
Serious or chronic illnesses.
Age of onset, how the child was treated, and complications of meningitis or encephalitis; seizure disorders; asthma, pneumonia and other chronic lung conditions; rheumatic fever; scarlet fever; diabetes; kidney problems; sickle-cell anaemia; high blood pressure and allergies.
Operations or hospitalisations.
Reason for care, age at admission, name of surgeon or primary care providers, name of hospital, duration of stay, how child reacted to hospitalisation and any complications. (If child reacted poorly, they may be afraid now and will need special preparation for the examination that is to follow.)
Immunisations.
Age when administered, date administered and any reactions following immunisations. See Chapter 3 for immunisation schedules.
Developmental history
Growth.
Height and weight at birth and at 1, 2, 5 and 10 years, any periods of rapid gain or loss, and process of dentition (age of tooth eruption and pattern of loss).
Milestones.
Age when child first held head erect, rolled over, sat alone, walked alone, cut their first tooth, said their first words with meaning, spoke in sentences, was toilet trained, tied shoes, dressed without help. Does the parent believe this development has been normal? How does this child’s development compare with siblings or peers?
Current development (children 1 month to preschool).
Gross motor skills (rolls over, sits alone, walks alone, skips, climbs), fine motor skills (inspects hands, brings hands to mouth, pincer grasp, stacks blocks, feeds self, uses crayon to draw, uses scissors), language skills (vocalises, first words with meaning, sentences, persistence of baby talk, speech problems), and personal–social skills (smiles, tracks movement with eyes to midline, past midline, attends to sound by turning head, recognises own name). If the child is undergoing toilet training, indicate the method used, age of bladder/bowel control, parents’ attitude towards toilet training and terms used for toileting.
Family history
As with the adult, draw a family tree for the child, including siblings, parents and grandparents. Give the age, health or age and cause of death of each. Ask specifically for the family history of heart disease, high blood pressure, diabetes, blood disorders, cancer, sickle-cell anaemia, arthritis, allergies, obesity, cystic fibrosis, alcoholism, mental illness, seizure disorder, kidney disease, mental retardation, learning disabilities, birth defects and sudden infant death. (When interviewing the mother, ask about the ‘child’s father’, not ‘your husband’, in case of the separation of the child’s biological parents.)
General overall health and wellbeing
Perception of health.
Ask the parent or guardian questions such as: ‘How do you define health?’ ‘How do you view your child’s situation now?’ ‘What are your concerns?’ ‘What do you think will happen in the future?’ ‘What do you expect from us as nurses, medical practitioners (or other healthcare professionals)?’
Interpersonal relationships/resources.
Within the family constellation, record the child’s position in family; whether the child is adopted; who lives with the child; who is the primary caretaker; who is the caretaker if both parents work outside of the home; any support from relatives, neighbours or friends; and the ethnic or cultural milieu.
Indicate family cohesion. Does the family enjoy activities as a unit? Has there been a recent family change or crisis (death, divorce, move)? Record information on child’s self-image and level of independence. Does the child use a security blanket or toy? Is there any repetitive behaviour (bed-rocking, head-banging), pica, thumb-sucking or nail-biting? Note method of discipline used. Indicate type used at home. How effective is it? Who disciplines the child? Is there any occurrence of negativism, temper tantrums, withdrawal or aggressive behaviour?
Provide information on the child’s friends: whether the child makes friends easily. How does the child get along with friends? Do they play with same-age or older or younger children?
Ask about the mother’s occupation and father’s occupation. Indicate the number of hours each parent is away from home. Do parents perceive their income as adequate? What is the effect of illness on financial status?
Values and beliefs/spiritual resources.
Cultural and ethnic background and practices as well as religious/spiritual beliefs, values and practices. For example: ‘Do you/your family identify with any specific cultural group?’ ‘In your culture are there some health practices that are important to you?’ ‘Does religious faith or spirituality play an important part in your family life? ‘How does your religious faith or spirituality influence the way you think about your health of your family members?’ ‘Are you a part of any religious or spiritual community or congregation?’ ‘Would you like me to address any religious or spiritual issues or concerns with you?’
Coping and stress management.
Does the child have the ability to adapt to new situations? Record recent stressful experiences (death, divorce, move, loss of special friend). How does the child cope with stress? Has there been any recent change in behaviour or mood? Has counselling ever been sought? ‘What is it about your child’s present situation that is most worrying for you?’
Activity/sleep/rest.
Record the child’s play activities. Indicate amount of active and quiet play, outdoor play, time watching television and special hobbies or activities. Indicate pattern and number of hours at night and during the day and the child’s routine at bedtime. Is the child a sound sleeper or are they wakeful? Does the child have nightmares, night terrors or somnambulation? How does the parent respond? Does the child have naps during the day?
Record school attendance. Has the child had any experience with day care or nursery school? In what grade is the child in school? Has the child ever skipped a grade or been held back? Does the child seem to like school? What is their school performance? Are the parent and child satisfied with the performance? Were days missed in school? Provide a reason for the absence. (These questions give an important index to child’s functioning outside the home.)
Health and lifestyle management
• Current medications. Any prescription and over-the-counter medications (or vitamins) the child takes, including the dose, daily schedule, why the medication is given and any problems. For each medication, note the name, dose and schedule, Finally, note any complementary therapies used.
• Tobacco, alcohol, non-prescription drugs. Has the child ever tried cigarette smoking? How much did they smoke? Has the child ever tried alcohol? How much alcohol did they drink weekly or daily? Has the child ever tried other drugs (marijuana, cocaine, amphetamines, barbiturates)?
• Environment/hazards. Where does the family live (house, apartment)? Is the size of the home adequate? Is there access to an outdoor play area? Does the child share a room, have their own bed and have toys appropriate for their age?
Inquire about home safety (precautions for poisons, medications, household products, presence of gates for stairways and safe yard equipment). Provide information on the child’s residence (adequate heating, ventilation, bathroom facilities), neighbourhood (residential or industrial, age of neighbours, safe play areas, playmates available, distance to school, amount of traffic, is area remote or congested and overcrowded, is crime a problem, presence of air or water pollution), and car (child safety seat, seat belts).
• Health maintenance. Who is the primary healthcare provider? When was the child’s last checkup? Who is the dental care provider, and when was the last dental checkup? Provide date and result of screening for vision, hearing etc.
Assessing activity and exercise
Focus your questioning on the child’s level of independence with usual daily activities and the effect of symptoms on their ability to be active.
Cardiovascular function.
Excessive bruising, lymph node swelling and exposure to toxic agents or radiation. Congenital heart problems, history of murmur and cyanosis (what prompts this condition?). Is there any limitation of activity, or can the child keep up with peers? Is there any dyspnoea on exertion, palpitations, high blood pressure or coldness in the extremities?
Respiratory function.
Nasal discharge and its characteristics, frequency of colds, nasal stuffiness, nosebleeds and allergies. Croup or asthma, wheezing or noisy breathing, shortness of breath, chronic cough.
History of cleft lip or palate, frequency of sore throats, toothache, caries, sores in mouth or tongue, tonsils present, mouth breathing, difficulty chewing, difficulty swallowing and hoarseness or voice change.
Assessing nutrition and metabolism (including skin, hair and nails)
The amount of nutritional information needed depends on the child’s age; the younger the child, the more detailed and specific the data should be. For the infant, record whether breastfeeding or bottle-feeding is used. If the child is breastfed, record nursing frequency and duration, any supplements (vitamin, iron, fluoride, bottles), family support for breast feeding and age and method of weaning. If the child is bottle fed, record type of formula used, frequency and amount, any problems with feeding (positing, colic, diarrhoea), supplements used and any bottle propping. Record introduction of solid foods (age when the child began eating solids, which foods, whether foods are home or commercially made, amount given, child’s reaction to new food, parent’s reaction to feeding).
For preschool and school-age children and adolescents, record the child’s appetite, 24-hour diet recall (meals, snacks, amounts), vitamins taken, how much junk food is eaten, who eats with the child, food likes and dislikes and parent’s perception of child’s nutrition. A week-long diary of food intake may be more accurate than a spot 24-hour recall. Also, consider cultural practices in assessing child’s diet.
Significant gain or loss of weight, failure to gain weight appropriate for age. Child’s pattern of brushing teeth and last dental checkup.
History of diabetes or thyroid disease; excessive hunger, thirst or urinating; abnormal hair distribution; and precocious or delayed puberty.
Birthmarks, skin disease (eczema, psoriasis, hives), pigment or colour change, mottling, change in mole, pruritus, rash, lesion, acne, easy bruising or petechiae, easy bleeding and changes in hair or nails. Amount of sun exposure; method of self-care for skin and hair.
Assessing kidney, bladder and bowel function
Kidney and bladder function.
Painful urination, polyuria/oliguria, narrowed stream, urine colour (cloudy, dark), history of urinary tract infection, whether toilet trained, when toilet training was planned, any problems, bedwetting (when the child started, frequency, associated with stress, how child feels about it).
Review fluid intake—types and amount over a 24-hour period and compare to output. Review any difficulties with getting to the toilet and toileting.
Assessing mental status, neurological and sensory function
Mental status: any nervousness, mood change, depression or any history of mental health dysfunction or hallucinations. Find out about interpersonal relationships, coping patterns.
Neurological system.
(Behaviour and cognitive issues are covered in the sections on development and interpersonal relationships.) Headache, head injury, dizziness. History of seizure disorder, fainting. In motor function: weakness, tic or tremor, paralysis or coordination problems. In sensory function: numbness and tingling (paraesthesia).
Assessing sexuality and reproductive function
Breast and regional lymphatics.
For preadolescent and adolescent girls, when did they notice that their breasts were changing? What is the girl’s self-perception of development? For older adolescents, does the girl perform breast self-examination? (See Ch 27 for suggested phrasing of questions.)
Male reproductive system.
Penis or testicular pain, whether told if testes are descended, any sores or lesions, discharge, hernia or hydrocele or swelling in scrotum during crying. For the preadolescent and adolescent boy, has he noticed any change in the penis and scrotum? Is the boy familiar with normal growth patterns, nocturnal emissions and sex education? Screen for sexual abuse. What is the child’s attitude towards the opposite sex? Who provides sex education? How does the family deal with sex education, masturbation, dating patterns? Is the adolescent in a relationship involving intercourse? Does he have information on birth control and sexually transmitted infections? (See Chs 25 and 26 for suggested phrasing of questions.)
Female reproductive system.
Has the girl noted any genital itching, rash, vaginal discharge? For the preadolescent and adolescent girl, when did menstruation start? Was she prepared? Screen for sexual abuse. (See Ch 25 for suggested phrasing of questions.)
What is the girl’s attitude towards the opposite sex? Who provides sex education? How does the family deal with sex education, masturbation, dating patterns? Is the adolescent in a relationship involving intercourse? Does she have information on birth control and sexually transmitted infections? (See Chs 25 and 26 for suggested phrasing of questions.)
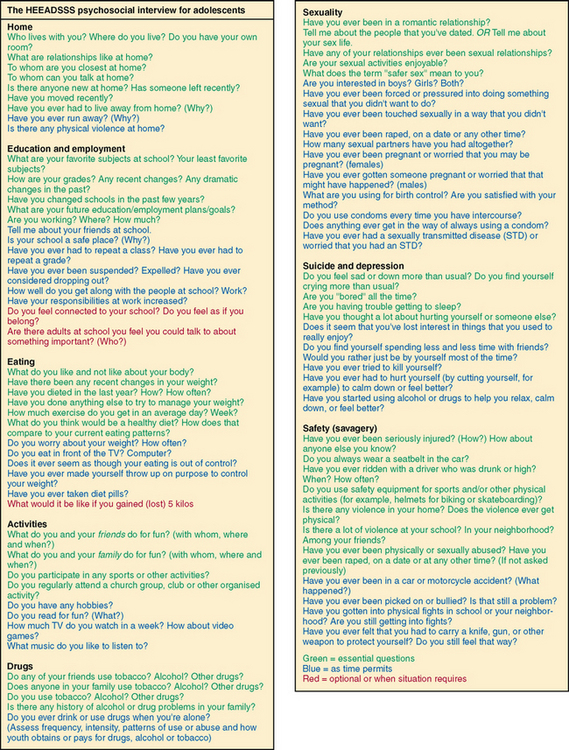
The adolescent
This section presents a psychosocial review of symptoms intended to maximise communication with young people. The HEEADSSS method of interviewing focuses on assessment of the Home environment, Education and employment, Eating, peer-related Activities, Drugs, Sexuality, Suicide/depression and Safety from injury and violence (Fig 7.2). The tool minimises adolescent stress because it moves from expected and less threatening questions to those that are more personal. The tool presents the questions in three colours: green are considered essential to explore with every adolescent; blue are important for you to ask if time permits; red questions delve in more deeply if the situation demands it (Goldenring and Rosen, 2004). Interview the young person alone; the parent can wait outside and fill out past health questionnaires. The other areas for health history can be adapted from the adult section described above.
Australian Commission on Safety and Quality in Health Care, 2010a. Clinical handover. Available at http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/content/PriorityProgram-05#Tools.
Australian Commission on Safety and Quality in Health Care. Falls prevention guidelines. Available at http://www.safetyandquality.gov.au/internet/safety/publishing.nsf/Content/FallsGuidelines, 2010.
Australian Government Department of Health and Ageing. The Australian immunisation handbook, 9th edn. Available at http://www.health.gov.au/internet/immunise/publishing.nsf/Content/Handbook-home.
Bennett RL, et al. Recommendations for standardized human pedigree nomenclature. Pedigree Standardization Task Force of the National Society of Genetic Counselors. Am J Hum Genet. 1995;56(3):745–752.
Goldenring JM, Rosen DS. Getting into adolescent heads: an essential update. Contemp Pediatr. 2004;21(1):64–75.
Granger CV, et al. Reliability of a brief outpatient functional outcome assessment measure. Am J Phys Med. 1995;74(6):469–475.
Katz S, et al. Studies of illness in the aged. The Index of ADL: a standardized measure of biological and psychosocial function. JAMA. 1963;185:94–98.
Lesser JM, et al. Challenges and strategies for taking a comprehensive history in the elderly. Geriatrics. 2005;60(11):22–25.
Mahoney FI, Barthel DW. Functional evaluation: the Barthel Index. Md State Med J. 1965;14:61–65.
New Zealand Ministry of Health, Immunisation handbook. Ministry of Health, Wellington, 2006. Available at http://www.moh.govt.nz/moh.nsf/indexmh/immunisation-handbook-2006.
Pearlman R. Development of a functional assessment questionnaire for geriatric patients: the comprehensive older person’s evaluation (COPE). J Chronic Dis. 1987;40:85S–94S.
Post SG, et al. Physician and patient spirituality: professional boundaries, competency, and ethics. Ann Intern Med. 2000;132:578–583.
Volk RJ, et al. The Alcohol Use Disorders Identification Test (AUDIT) as a screen for at-risk drinking in primary care patients of different racial/ethnic backgrounds. Addiction. 1997;92(2):197–206.