Chapter Three Developmental tasks and health promotion across the life cycle
Much of this book details the method of collecting subjective and objective data about a person to construct a database. The database is used to assess the health state; to applaud health strengths and assets; and to uncover, diagnose and treat health problems. To fit this database into a meaningful frame, we must consider the developmental stage of that individual at that particular time. Appraising the life tasks that currently absorb the individual lets us appreciate the holistic frame of reference.
Consider Sally, a 14-year-old adolescent girl, with chronic asthma. In the initial interview with Sally and her parents concerns were raised that Sally had recently become withdrawn, moody and her asthma symptoms had intensified; Sally’s parents reveal that she has recently been diagnosed with mild depression by her general practitioner. The management and nursing care of Sally’s asthma management is affected by the knowledge that adolescents who have depression are less concordant and engaged with their asthma management; therefore, working collaboratively with the adolescent can become more problematic than usual (Galil, 2000). Complicating Sally’s care are the developmental tasks she is working towards as an adolescent. She may be experiencing frustration at the continual dependence on her parents, have an inability to form close relationships with her peers due to her chronic asthma and time off school and may have a perceived barrier in her own search for identity; all of which can increase her risk of morbidity and mortality (Galil, 2000). Early intervention to address comorbid depressive disorders increases compliance, improves outcomes and enables the adolescent to continue to appropriately meet developmental expectations (Galil, 2000). Ask yourself—what interventions would you use which would enable Sally to meet the developmental tasks at this stage of her life span? Had these same symptoms been presented by a 38-year-old woman who is considering whether or not to start a family, would your interventions have been the same?
Growth is continuous and change is perpetual throughout the life cycle. Development is lifelong, not only in biological growth but also in maturation of the physiological systems, in cognitive development and in personality development. Developmental stages are ‘qualitative changes in thinking, feeling and behaving that characterise particular time periods of development’ (Berk, 2010). During each of the stages, certain issues are dominant and consume more of the individual’s attention and energy. The stages are not precisely distinct; transitions occur and overlap exists between stages.
The following sections combine data to give a general portrayal of the individual in each age period of the life cycle. Each portrayal considers the physical, psychosocial, cognitive and behavioural development of the person. The stages are:
2. Early childhood: Toddler (1 to 3 years)
3. Early childhood: Preschooler (3 to 5 or 6 years)
4. School child (6 to 10 or 12 years)
5. Preadolescent (10 to 12 or 13 years)
6. Adolescent (12 or 13 to 19 years)
7. Early adult (20 to 40 years)
Infancy (birth to 1 year)
The first year is the most dramatic and rapid period of growth and development. The infant changes from a totally dependent being into a person who interacts with the environment and forms close relationships with other people (Fig 3.1).

Physical development
Weight, height and head circumference reflect physical growth and are sensitive indicators of the infant’s general health. The average healthy term infant weighs 3.4 kg, with 95% of full-term infants ranging from 2.5 to 4.6 kg. During the first few days, the infant loses a little weight but regains the birth weight by 10 days. Growth spurts double the birth weight by 4 to 6 months and triple the birth weight by 1 year. Length increases 50% by 1 year.
Head circumference reflects brain size; head growth shows brain growth. At birth, the average head circumference is 35 cm, with about 95% of infants within the range of 32.6 to 37.2 cm. Brain growth occurs rapidly during the first 2 years. Nutrition is essential, with the proper type and amount of fat calories and essential fatty acids required for brain development (Ch 16).
The central nervous system is the organ system that makes the most dramatic gains. Tremendous brain growth occurs during infancy. Also, the infant has numerous primitive reflexes that are present at birth or soon after and persist for specific time periods. These are under subcortical control; as the cerebral cortex grows and matures, it inhibits their expression. In a healthy infant, these reflexes should disappear at specific times during the first year (Ch 22). Certain protective reflexes (cough, gag, sneeze, eye-blink) are always present. Visual acuity is very poor at birth (about 20/800) and for the first few months because of immature and widely spaced foveas (i.e. the area on the retina of keenest vision). But acuity develops rapidly and is close to adult levels by the end of the first year.
Psychosocial development
Erik Erikson (1902–1994) focused on cultural and societal influences as determinants of behaviour. Erikson was concerned with the growth of the ego, the conscious, organised, rational part of the personality. He described eight stages of ego development that encompass the life span (Erikson, 1963).
Each stage is characterised by a distinct conflict relating to the person’s physiological maturation and to what society expects of a person at that age. Each conflict is a bipolar issue, a point at which personality development may go one way or another through the choices made by the infant’s caregivers or, later, by the individual. The bipolar aspect means that the conflict can be resolved along a continuum, and have a more positive or a more negative outcome.
Erikson’s first stage, trust versus mistrust, has a broad psychosocial dimension. The crucial element in this stage is the quality of the parent–child relationship. The infant is completely helpless and depends on the parent for food, warmth, comfort and companionship. When the parent is responsive and consistent in nurturing, the psychological conflict is resolved on the positive side and the infant learns trust. The security from this trust extends to trust in others and in the self. The infant learns that the world is a safe and reliable place and that they are welcome in it. If the parent is unresponsive, haphazard or abusing, the infant learns mistrust. Since the infant never feels secure, they experience anxiety and alienation and may protect themself by withdrawing. Without a trusting foundation, this individual will flounder in attempts to resolve future crises.
Absolute trust actually is not the healthy goal of this conflict. When resolution of this crisis is successful, the infant holds relatively more trust than mistrust. Total trust would impede survival in later years because not everyone or everything in the world should be trusted.
Cognitive development
Jean Piaget (1896–1980) described stages of cognitive development in the growing child. Cognition is defined as how the individual perceives and processes information about the world; it is the ability to know. Piaget believed that a child’s thinking develops progressively from simple reflex behaviour into complex logical and abstract thought. This development is biologically inherent in each maturing child and occurs independently of any special training.
The child’s cognitive development proceeds through four definite and sequential stages. Each stage demonstrates a qualitative change, representing a new way of thinking and behaving. Although the ages of reaching the stages are approximate, the sequence of stages never varies. All children move through the same stages in the same order; no stage is skipped. Each stage is the foundation for the next, and the next stage builds on the stage before it. At each stage, the child’s scheme (how the child views the world) becomes more intricate and complex.
According to Piaget, the first stage of sensorimotor skills (birth to 2 years) is a time of intelligent activity, although full language skill has not yet developed. Infants perceive information through the five senses and learn to modify their behaviour in response to these environmental stimuli. At birth, the only response is an array of reflexes (crying, rooting, sucking, grasping) that occur automatically. Gradually, the infant learns the important concept of object permanence—that objects and people continue to exist even when they are no longer in sight.
Piaget believed that object permanence begins around 7 months, when the infant searches for an object that is partly hidden but does not search for one completely out of sight. By 9 to 10 months, the infant looks behind a screen for an object, but only if it was seen to be hidden there. By 18 to 24 months, the concept is fully developed and the child conducts a true search in many places for objects hidden from sight. As this concept develops, the child also learns that they are separate from objects in the environment. Last, by age 2 the child has acquired mental representation (or thought) and can think of an external event without actually experiencing it.
Piaget’s work stimulated tremendous research and formed the base of our practice of providing developmentally stimulating environments for children. However, recent research indicates Piaget underestimated the cognitive capacity of infants and toddlers, perhaps because he lacked today’s sophisticated experimental techniques (Berk, 2010). Infants as young as 3 months old appear to have an abstract understanding of the world as a real and predictable place. Spelke and colleagues (1992) showed that infants acted surprised and looked longer at ‘magical’ events, such as an object disappearing through a hidden trapdoor, or an object stopping in midair without support. Spelke concluded that infants know that objects continue to exist even when they do not look at them, and they know that objects cannot pass through barriers. Infants have an awareness of real physical events even though they lack the motor coordination to demonstrate this.
Behavioural development
Gross motor skills.
These skills include posture, head balance, sitting, crawling and walking. Their development is predictable because it follows the direction of myelinisation (laying down of myelin) in the nervous system; cephalo-caudal (head-to-foot direction) and proximodistal (central-to-peripheral direction, or midline before extremities).*
Some head balance already is present at birth for protection; when prone, the infant can turn the head to the side to avoid suffocation. Otherwise there is marked head lag, as when pulled to a sitting position from a lying position. By 3 months of age, the infant can raise the head and chest from a prone position with the arms extended for support. By 4 months of age, the head and chest are raised 90 degrees with only slight head lag when pulled to a sitting position. Sitting alone without support occurs at 6 to 7 months of age.
After 7 months, the infant ventures from the sitting position to explore the environment, and crawling begins. At 8 months, the infant pulls to a stand and stands while holding onto an object for support. Between 9 and 11 months, the infant starts to ‘cruise’ the room, walking upright while holding onto the furniture. Usually, the infant can stand independently around 11 months, and by 12 months the infant walks alone.
Fine motor skills.
The development of fine motor skills involves using the hands and fingers for prehension, or the act of grasping. The infant is born with a grasp reflex; it fades at 2 months of age and is absent at 3 months of age. At 3 months the infant expresses interest in an object more with the eyes than with the hands. At 4 months, the infant inspects their hands, looks from object to hands and back, and may try to grasp an object with the hands but overshoots the mark. The voluntary two-handed grasp is present at 4 to 5 months.
Further distal refinement follows at 8 to 10 months with a crude pincer grasp using the index, fourth and fifth fingers. By 10 months, the index finger is an apposition with the thumb for a neat pincer grasp, and the infant is absorbed in picking up raisins, finger foods and toys (Fig 3.2). By 11 months the infant puts objects into a container and removes them. And at 13 months the child builds a tower of two blocks.

Language skills.
Crying is the infant’s first means of communication. Cries are undifferentiated at first, but by 1 month of age the infant alters the pitch and intensity of the cry to communicate different needs, such as hunger, discomfort or loneliness. Vocal sounds build rapidly; the infant laughs out loud at 3 months, coos when they awaken or when someone talks to them at 2 to 4 months, and babbles at 6 months. At 9 to 10 months, the infant can imitate the sounds of others, although they may not necessarily understand them. At 12 months, an infant usually can say the first recognisable word with meaning.
Personal−social skills.
Throughout the first year, the infant learns more and more social ties that bind them to other people. Early on, the infant shows a visual preference for the human face, and even in the first 30 to 60 minutes following birth watches the mother intently (look back at Fig 3.1). The social smile erupts at 6 to 8 weeks, to the family’s delight and continual reinforcement. At 4 months, the infant laughs and enjoys other people, and at 6 months extends arms to the parent to be picked up.
Imitation, or the copying of another person’s behaviour, is present in a limited way in newborns. Even the young infant will copy adult facial expressions such as opening the mouth, protruding the tongue and pursing the lips. As the neurological system develops, at 7 months, the infant imitates others’ actions, at 9 months their sounds and at 10 months waves bye-bye and enjoys interactive games such as pat-a-cake and peek-a-boo. At 11 months, the infant can help with feeding and dressing and follows simple directions. Emotions develop during the first year, and by 12 months the infant can give a hug or kiss and show jealousy, fear or anger.
Infant’s periodic health examination
Table 3.1 lists the services that you as healthcare provider should address during the infant’s well-baby checkups. Note the aspects of screening at birth, the immunisation schedule and the parent counselling items regarding diet and injury prevention. Screening measures include those for high-risk groups, such as hearing impairment and screening for lead poisoning. Note also that these tables are not intended to be a complete list of all the steps that should be included in the examination checkup. Instead, the table lists preventive services that were studied and shown to be clinically effective (The Royal Australian College of General Practitioners ‘Red Book’ Task force, 2009).
TABLE 3.1 Periodic health examination: birth to 10 years
| Interventions considered and recommended for the periodic health examination | Leading causes of death |
|---|---|
| Interventions for the general population | |
| Interventions for high-risk populations | |
| Population | Potential interventions |
| Preterm or low birth weight | Haemoglobin/haematocrit |
| Infants of mothers at risk for HIV | HIV testing |
| Low income; immigrants | Haemoglobin/haematocrit; PPD |
| TB contacts | PPD |
| Aboriginal and Torres Strait Islanders | Haemoglobin/haematocrit; PPD; hepatitis A vaccine16; pneumococcal vaccine17 |
| Travellers to developing countries | Hepatitis A vaccine |
| Residents of long-term care facilities | Hepatitis A vaccine; influenza vaccine |
| Certain chronic medical conditions | PPD; pneumococcal vaccine; influenza vaccine |
| Increased individual or community lead exposure | Blood lead level |
| Family h/o skin cancer; naevi; fair skin, eyes, hair | Avoid excess/midday sun, use protective clothing and sunscreen |
CPR, Cardiopulmonary resuscitation; HIV, human immunodeficiency virus; PPD, purified protein derivative; TB, tuberculosis; TSH, thyroid-stimulating hormone
1 Whether screening should be universal or targeted to high-risk groups will depend on the proportion of high-risk individuals in the screening area, and other considerations.
2 If done during first 24 hr of life, repeat at age 2 wk.
3 Optimally between day 2 and 6, but in all cases before newborn nursery discharge.
4 2, 4, 6 and 12 mth, once at age 4 yr.
5 2, 4, 6 mth, once at age 4 yr.
8 Birth; total of 3 doses required following the birth dose, at either 2, 4 and 6 mth or at 2, 4 and 12 mth.
9 18 mth; or older child without hx of chickenpox or previous immunisation. Include information on risk in adulthood, duration of immunity and potential need for booster doses.
10 2, 4 and 6 mth. Third dose of vaccine is dependent on vaccine brand used.
11 One injection at 6 wk, 3 and 5 mths.
12 One injection at 6 wk, 3 mth, 5 mth.
16 Two doses of hepatitis A vaccine are required for Aboriginal and Torres Strait Islander children living in areas of higher risk (Queensland, Northern Territory, Western Australia and South Australia).
17 Medical-at-risk children require a fourth dose of 7vPCV at 12 months of age and a booster dose of 23vPPV at 4 years of age.
Adapted from The Guidelines for Preventive Activities in General Practice, 7th edn, 2009, www.racgp.org.au/redbook/iv and US Preventive Services Task Force: Guide to clinical preventive services, 2006, http://www.ahrq.gov/clinic/uspstfix.htm.
Early childhood, toddler (1 to 3 years)
With successful completion of first-year tasks, the child enters the second year secure in a basic sense of trust. That security plus maturing muscles and developing language enable the child to launch into the process of exploring the environment (Fig 3.3). The toddler explores everything, inhaling the world with the zeal of all first-time adventurers. Developmental tasks of this next stage include:
1. Differentiating self from others, particularly the mother
2. Tolerating separation from mother or parent
3. Withstanding delayed gratification
4. Controlling bodily functions
5. Acquiring socially acceptable behaviour
6. Acquiring verbal communication
7. Interacting with others in a more empathic way (i.e. understanding another person’s emotional state).
Physical development
The rate of growth decelerates during the second year, with the child gaining an average of 2.5 kg in body weight and 12 cm in length.
Toddler lordosis describes the normal upright posture of the toddler, with the potbelly; sway back and short, slightly bowed legs. The increase in head circumference slows, and the head circumference equals the chest circumference between 1 and 2 years. After the second year, the chest circumference exceeds individual head and abdominal measurements, and the extremities grow faster than the trunk.
Maturation of the physiological systems is detailed in the corresponding physical examination chapters in this text. Neurological advances are cited now because they permit developmental changes during the toddler years. For example, most brain growth occurs during the first 2 years, and changes in certain cortical areas permit language and motor development. In the spinal cord, myelination is almost complete by age 2, matching the gross motor achievements in locomotion. Visual acuity is close to 20/40 at 2 years and close to 20/30 by age 3 (Barnard and Edgar, 1996). The maturing convergence–accommodation mechanism matches the toddler’s fascination with minute objects.
Psychosocial development
Autonomy is the goal of all daily activities. The pursuit of independence occupies the toddler. For example, muscle maturation allows walking, exploring and some self-care in feeding and dressing; refined visual acuity enhances close scrutiny and attention span; and language advances so the toddler can make known independent demands, such as ‘me do’, ‘mummy way’ or ‘me out’. Between 12 and 18 months, the toddler ventures away from the parent to explore the immediate environment, still using them as a home base to come back to for support. Practice builds confidence, which encourages more exploration. Between 18 months and 3 years, it occurs to the toddler that they really have become quite separate from the parent. This creates some anxiety, which is manifested in the negativism, or the ‘terrible twos’ behaviour, normally seen at this age.
Autonomy versus shame and doubt (1 to 3 years).
The quest for autonomy characterises the psychological conflict of Erikson’s second stage. The toddler wants to be autonomous and to govern their own body and experiences. The toddler wants to apply newly attained skills to explore the world. However, the toddler has not yet attained any sense of discrimination or judgment. The parent lives in the balance of letting the toddler explore but also firmly protecting the child from experiences that are dangerous or frustrating for the child’s current ability level. This conflict is resolved favourably when the parent uses patience and appropriate guidance and has reasonable expectations of the toddler’s capabilities and attention span. A parent who is overcontrolling or undercontrolling may foster a negative outcome. Then the child may feel shame and experience doubts about their own ability.
Erikson believed that toilet training symbolises this stage. The toddler’s muscle maturation has progressed to the ‘holding on’ and ‘letting go’ of things; this naturally extends to the sphincter muscles.
Cognitive development
During the second year, the toddler is still considered to be in Piaget’s sensorimotor period. The readiness for independence is demonstrated between 12 and 18 months as the child now tries out new activities and new experiments to reach a goal. To reach a desired toy in her toybox, a girl at this age may try the various routes of taking out each object one by one, overturning the box and dumping the contents out or climbing into the box herself. Learning comes by trial and error.
Between 18 and 24 months, the child develops mental representation for external events. This is a major achievement because the toddler can think through plans to reach a goal rather than merely perform them and observe the results by trial and error.
The concept of object permanence is now fully developed. The toddler comprehends both visible and invisible displacements. That means the child can search for an object in several places, even though it was not seen as it was hidden.
Around age 2, Piaget’s preoperational stage begins. This use of symbols to represent objects and experiences is discussed in the next section on preschoolers.
Behavioural development
Motor skills.
Locomotion advances as the toddler usually walks alone at 12 months, runs stiffly at 18 months and runs well without falling at 2 years. At 2 years, the child can also walk up and down stairs. The child jumps with both feet by 2 years.
Fine motor development shows increasing manual dexterity. At 15 months, the child can drop a pellet into a narrow-neck container and can hurl and retrieve objects. Fourteen-month-old hands can hold a pencil and make scribbles, whereas by 2 years the toddler can reproduce a vertical line from a demonstration.
Language skills.
Language progresses from a vocabulary of about two words at 1 year to a spurt of about 200 words by 2 years. Then the 2-year-old combines words into simple two-word phrases—‘all gone’, ‘me up’, ‘baby crying’. This is called telegraphic speech, which is usually a combination of a noun and a verb and includes only words that have concrete meaning. Interest in language is high during the second year, and a 2-year-old seems to understand all that is said to them. A 3-year-old uses more complex sentences with more parts of speech.
Personal–social skills.
Toddlers are usually compliant and cooperative with parents who are warm and sensitive and have reasonable expectations (Berk, 2010). However, parents are often surprised at the swift transformation of their loving affectionate child into a determined toddler who resists requests. Toddlers want their parents’ approval but also want to assert themselves and do as many things for themselves as they can. As they test their powers, they sometimes clash with parents’ restrictions and a battle of wills results. ‘No’ seems to be a favourite word.
This negativism is a normal part of the quest for autonomy. Although they protest vigorously, toddlers seem to fare better with firm, consistent limits. The thought of a limitless world and of personal untested powers is disabling to the child. Knowing where they stand, even if they disagree, is reassuring to toddlers.
Ritualism emerges along with the negativity. A 2-year-old wants things done in the same way; any change in schedule or habit is upsetting. A consistent routine assures the child that the world is predictable and orderly. Ritualism is heightened at age 2½, especially at bedtime, when the child insists on the same order of nighttime tasks or the same order of coloured blankets on the bed.
Although attachment to the parent is still strong, the toddler begins to play alone. Children 1 and 2 years of age venture away to explore but still need the reassurance of the parents being there. Play with peers can be comical to the observer. Toddlers engage in parallel play—that is, playing the same thing side by side without interaction and without trying to influence each other’s behaviour. The two children seemingly ignore each other yet unobtrusively check the other out to note what is happening. Imitation in play is apparent, both of peer activities and especially of parent activities such as sweeping, lawn mowing or cooking. As the toddler is increasingly able to form mental images, play reveals increased imagination.
Toddler periodic health examination
Study Table 3.1 for the immunisation schedule, examination, screening measures and parent counselling measures to address with parents of young children. Note the screening measures for high-risk categories of lead poisoning, tuberculosis exposure and anaemia.
Early childhood, preschool (3 to 5 or 6 years)
Successful mastery of the toddler tasks, plus a highly energised state, make the preschooler ready for this time of developing initiative and purpose. Although parental relationships are still the most important, the preschooler begins to turn to other children and adults to broaden learning and play. Tasks during this period include:
1. Realising separateness as an individual
2. Identifying gender role and its functions
4. Developing a sense of initiative
5. Interacting with others in socially acceptable ways
Physical development
Most physiological systems are now mature, but the musculoskeletal system is still developing. The preschooler needs interrupted time and space through play to practise their newly developed gross motor skills and develop their fine motor skills. They develop gross motor skills through running, jumping, hopping, climbing and catching. Fine motor activities using the muscles in the hand will develop the skills needed for handwriting. The rate of growth continues at a slower pace and the average child gains about 2 kg in weight and 7 cm in height per year. The appearance changes as the ‘baby face’ matures, the potbelly slims and the legs elongate more than the trunk does. Muscles are growing, and cartilage is changing to bone at a faster rate than before. Nutrition is crucial for bone growth. A serious nutrient loss at this age alters the shape, thickness and growth of bones.
Psychosocial development
Although still primarily egocentric, the preschooler now broadens the scope to include some awareness of other people’s interests, needs and values. As this happens, the conscience or superego develops. The child learns right from wrong and their corresponding rewards and punishments.
Identifying the gender role.
As children become aware of their separateness, they also learn that they belong to a further differentiated category—male or female. They are learning gender, or how males and females do differ. As early as age 2, children label themselves as ‘girl’ or ‘boy’ and assign their family members and pets to these basic gender categories. Then children begin to develop gender roles by a process called gender typing, or how society says males and females should differ. Children learn the behaviours and attitudes that their culture says are right for a man or a woman. The parents have a strong influence in gender typing, as is seen, for example, as a preschool girl imitates words and actions she has observed in her mother. But her social circle is enlarging, and the girl also picks up important messages from peers, teachers, books and television about how girls and boys should differ. These messages can forge strong gender stereotyping, and the preschooler often develops rigid rules about what boys and girls should wear and about what roles they can ‘be’ when they play make-believe (Berk, 2010).
Learning at this stage has a broader scope, though, than just learning the appropriate gender role. As the girl mentioned earlier identifies with her mother, she assimilates and internalises the mother’s ideals and values. She learns the standards of society presented to her by the words and deeds of the mother. This is the development of the conscience, which now will direct the girl’s behaviour. Interaction with peers helps to develop the conscience too, as in play; children construct notions of justice and fair play.
Initiative versus guilt (4 to 5 years).
For this stage of ego development, Erikson believed that the child’s chief task is to develop a sense of initiative. With increasing locomotor and mental power, the child now has an energy surplus, resulting in determination and enterprise. The child plans and attacks a new task with gusto and wants to stay with it. Any failures are easily forgotten in the quest to test the world. When the parent encourages, reassures and cheers the child on (while protecting them from harm), the child learns self-assertion, spontaneity, self-sufficiency, direction and purpose. But if the parent ridicules, punishes or prevents the child from following through on tasks that could be done, the child feels guilty. The guilt exists not only when the child acts inappropriately but also when they are thinking of goals they would like to accomplish.
By nurturing successes and promoting a healthy self-image, the parents help the preschooler develop self-esteem. Self-esteem is the judgment the child makes about their own worth as well as any feelings about the judgment (Berk, 2010). Self-esteem is most important because it becomes the way we value our own competence. Our self-esteem affects our emotional experiences, future behaviour and long-term psychological adjustment (Berk, 2010).
Cognitive development
Piaget’s preoperational stage covers age 2 to 7 years, a longer span than the preschool years. It is characterised by symbolic function, because the child now uses symbols to represent people, objects and events. This process is liberating. Now the child can conjure up thoughts of the father, for example, without actually seeing him or hearing his voice. The symbolic function is revealed in child’s play, as in delayed imitation. That means a child can witness an event, form a mental representation of it and imitate it later in the absence of the model. For example, a little boy watches his father dress and leave for work, then later in the day the boy wraps a tie around his neck, packs his ‘briefcase’ and heads for the door.
Although representational thought is a great milestone, the preschooler’s thinking continues to be limited. Thinking is concrete and literal. The preschooler focuses on only one aspect of a situation at a time and ignores others, a characteristic known as centration. For example, given a pile of blocks, a preschooler will sort by colour (red, blue, yellow), or by shape (square, triangle, circle), but not by both. According to Piaget, a child in the preoperational stage is egocentric. This child cannot see another’s point of view and feels no need to elaborate their own point of view, because the child assumes everyone else sees things as they do (Piaget, 1968). However, recent research suggests that 4-year-olds can have an awareness of another’s view (Berk, 2010).
Behavioural development
Motor skills.
The physical bumbling of the toddler fades, and the preschool child demonstrates admirable gross motor and fine motor control (Fig 3.4). A 4-year-old child can hop on one foot. A 5-year-old child can skip on alternate feet and jump rope and may begin to swim and skate. Girls often achieve fine motor milestones ahead of boys of the same age. A 3-year-old child can draw a circle; a 4-year-old child can cut on a line with scissors, draw a person and make crude letters. A 5-year-old can string beads, control a crayon well and copy a square and letters and numbers, and has demonstrated preference for the right or left hand.

Language skills.
Between 3 and 4 years of age, the child uses three- to four-word telegraphic sentences containing only essential words. By 5 to 6 years, the sentences are six to eight words long, and grammar is well developed.
Piaget labelled the earlier speech pattern as egocentric (Piaget, 1975). Children at this age talk incessantly. They are wrapped up in their own thoughts and talk to themselves merely for the pleasure of hearing their own voices say the words. Piaget believed speech here is in the form of a monologue to the self, or a collective monologue between two children, in which they talk at each other but are still absorbed in themselves, and no communication has occurred.
However, more recent research challenges Piaget’s views and demonstrates that this private speech is a problem-solving tool that is beneficial to all children as they try new tasks or work through unfamiliar situations (Berk, 2010). Children chatter to themselves between the ages of 4 and 6; this chatter becomes inaudible muttering during early elementary school, and then it mostly drops away. Researchers noted that when a child undertakes a new task, an adult usually explains the steps needed to perform the task, often in detail, as directions or strategies. When the child next works through the task alone, they use private speech as a way of repeating the adult’s expert advice as their own independent guidelines. This evolves into muttering because one often uses verbal shorthand with one’s own self; that is, the child omits saying the words that refer to familiar steps and verbalises only the words that refer to the still-confusing steps. Finally, as the child has mastered the skill, the air is silent because the mind has internalised the private speech into thinking inner speech. Private speech reemerges throughout life as we confront new tasks or unfamiliar or stressful situations (Berk, 2010).
Personal–social skills.
The preschooler is self-assertive, but the negativism of the toddler years has diminished. This child wants to please others. By taking on the values of the family and developing a conscience, the child monitors their own behaviour to maximise acceptance. The preschooler is proud of their self-sufficiency and accomplishes everyday self-care (dressing, feeding and toileting) almost completely. The world enlarges because the child’s anxiety towards strangers and fear of separation decreases; the at-home preschooler is able to tolerate brief separations from the parents to enjoy visiting peers or preschool. Some preschoolers have already been in day care from an early age, and parental separations are less of an issue.
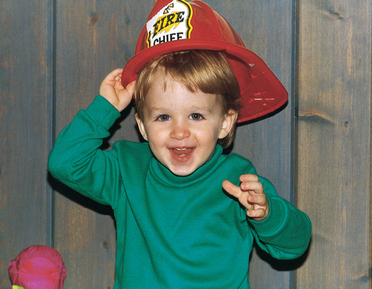
With their growing social regard, preschoolers enjoy cooperative play with each other. This means that they play the same game and interact while doing it. The child’s imagination runs rampant, and this factor shows in the play. Preschoolers love to dress up and imitate the sex role behaviours of their parents as well as admired adult models, such as nurses, doctors, media heroes, firefighters or police officers. Often this make-believe or fantasy play is a coping strategy: a sheltered workshop in which the preschooler can work out conflicts and fears or master life experiences.
It is easy for fantasy and reality to blur. Children experience the greatest number of new fears between 2 and 6 years of age. Visions of ghosts and monsters, fear of the dark, fear of being lost—all arise from the child’s increased imagination as well as from some frightening experiences that the child really has had. Also, beginning around age 2½ or 3 years, children often invent imaginary playmates. The imaginary friend often serves as an alter ego and tries out behaviours that the child yearns to try or takes the blame when the child misbehaves. Although it is important for a time, the imaginary friend is easily given up when the child enters school.
Middle childhood, school-age child (6 to 10 or 12 years)
The best preparation for this age is a firm foundation in trust, autonomy and initiative. Secure in these attributes, the child is able to move into a larger world and tackle these tasks:
1. Mastering skills that will be needed later as an adult
2. Winning approval from other adults and peers
3. Building self-esteem and a positive self-concept
Physical development
Physical growth is slow but steady during the school years. The average child gains about 3 kg and grows about 5.5 cm per year. The growth rates in boys and girls are basically the same, with boys only slightly heavier and taller than girls. Asian children and Indigenous Australian children tend to be slightly smaller than Caucasian or African children of the same age. The preadolescent growth spurt occurs earlier in girls, at about age 10, as compared with age 12 for boys.
The physical appearance of the school-age child is relatively slimmer than that of the younger child because of the older child’s proportionately longer legs, diminishing body fat and a lower centre of gravity. Although the cranium achieved most of its growth in the early years, now the bones of the face and jaw grow faster. During these years, primary teeth are lost, which the school child hails as a big event and developmental milestone. The eruption of large permanent teeth into a mouth and face that looks too small for them gives this child the ungainly, so-called ugly duckling appearance.
Body carriage is more agile and graceful. Bones continue to ossify during these years, and bone replaces cartilage. Muscles are stronger and more developed, though not yet fully mature. Neuromuscular control is more coordinated. All these refinements ready the school child for repetitive pursuit of activities requiring fine motor skills, such as writing, drawing, needlework, small model building and playing instruments, and large muscle activities, such as running, throwing, jumping, biking and swimming.
Psychosocial development
Erikson highlighted the directing of energy into learning skills when he characterised middle childhood as a period focused on industry versus inferiority. In this stage, age 6 to 11 years, the child focuses much of the time at school. Now, the approval and esteem of people outside the immediate family become important. The child wins this recognition by working and producing. Play and fantasy give way to mastering the skills that the child will need later to compete in the adult world. This child values independence in tackling a new task and takes pleasure in carrying it through to completion. The young worker is eager, diligent and absorbed. Also, the value of social relationships emerges as the child sees the benefits of working in an organised group. Children learn to divide labour and to cooperate to achieve a common goal.
Real achievement at this stage builds a feeling of confidence, competence and industry. The child is rewarded by their own inner sense of satisfaction in achieving a skill and, more importantly at this age, by external rewards such as approval from teachers, parents and peers in the form of marks, allowance or special gifts. Problems arise when the child feels inferior. If the child believes that they cannot measure up to society’s expectations, the child loses confidence and does not take pleasure in the work. A gnawing feeling of inferiority and incompetence grows and may continue to haunt this child.
The reality is that no one can master everything. There is bound to be something at which each child will feel inferior. Caring parents and teachers will try to balance these weaker skills with areas in which the child can excel. The problem is that, in some cultures, success in certain areas has a higher social value, particularly among peers. For example, in some western cultures, team sports are admired more than playing chess, or success in reading may be rewarded more than success in drawing. The challenge to adults is to provide the successful experiences and positive reinforcement so that each child can achieve.
At this age, peer approval is beginning to be significant. During middle childhood, it is important to belong to a peer group. The peer group is a key socialising agent. Group solidarity is enhanced by secret codes or strict rules. The child conforms to group rules because acceptance is paramount. The child begins to prefer peer group activities to activities with the parents.
Cognitive development
Piaget labels the stage of middle childhood, age 7 to 11 years, as the period in which the child focuses on concrete operations. At this age, the child can use symbols (mental representations) of objects and events in more logical ways. This means a child can experience mentally what they would have had to do physically before. For example, to describe the classic hopscotch manoeuvres to you, a girl now can articulate them (‘first you hop on one foot …’) rather than merely performing them.
Armed with the ability to use thinking to experience things or events, the school child can:
• Use numbers. While counting with numbers begins in preschool years, the school-age child has the combinational skill to add and subtract, multiply and divide.
• Read. By using printed symbols (words) for objects and events, the child can process a significant amount of information. Also, reading fosters independence in learning.
• Serialise. While this begins in preschool years, the school-age child can order objects by an increasing or decreasing scale, such as according to number size (smallest to largest) or weight (lightest to heaviest).
• Classify. This is the ability to sort objects by something they have in common. While young children can do this, the school-age child is able to organise a hierarchy of classes and subclasses. It shows in the school-age child’s penchant for collections: rocks, shells, novelty cards, cars and dolls. A child spends many hours sorting the collections, and the logic of the classification system gets more complex as the child grows.
• Understand conservation principles. Understanding conservation of matter is the ability to tell the difference between how things seem and how they really are. It is the ability to see that mass or quantity stays constant even though shape or position is transformed. For example, the child who can conserve sees that two equal amounts of water remain the same even if one is poured into a beaker with a different shape.
At this age, thinking is more stable and logical. The school-age child can decentre and consider all sides of a situation to form a conclusion. The school-age child is able to reason, but this reasoning capacity is still limited because they cannot yet deal with abstract ideas.
Preadolescence (10 to 12 or 13 years)
This period covers grades four/five to years seven/eight, ending with puberty (Fig 3.5). Although this stage is still part of childhood, children in this group have common skills and interests that set them apart. It becomes more difficult now to typify characteristics of a single year. Because of rapid growth, the age levels start to blend and overlap. A child may be at one level physically and intellectually but at another level socially. Children of the same age show diverse development levels.

Physical development
Physical growth is markedly different at this stage; boys show slow and steady growth, whereas girls have rapid growth. On average, the growth spurt begins in girls at age 10 years and reaches its greatest velocity at 12, whereas in boys the growth spurt begins at 12 and attains its maximum velocity at 14 years.
Even among girls, growth is varied. In a group of 11-year-old girls, each girl looks different from the others. Some look like children, and some are starting to look like adolescents. At 10 years, some girls have begun their growth spurt and have begun to grow pubic hair and to have breast development. At 12 years, girls demonstrate the most rapid growth in height and weight. The breasts enlarge, the areolae darken, growth of axillary hair begins and menarche occurs.
Physical size among 11-year-old boys is fairly uniform. At 12 years, boys show a wider range of growth. Most demonstrate the onset of secondary sex characteristics with initial genital growth, appearance of pubic hair and the occurrence of erections and nocturnal emissions.
Boys and girls both exhibit a great amount of physical restlessness. Their activity is well directed into individual and team sports. Their percolating energy makes it hard for them to sit still, and it shows by tapping the foot or drumming the fingers.
Psychosocial development
Parent–child ties exhibit some strain as the child gradually starts to drift away from the family. The parents continue to set standards and values, but the child begins to challenge authority and to reject their standards. Parents decrease in stature in the child’s eyes as the child learns that parents are not perfect and do not know everything. Yet the child loves the parents. They need and want some restrictions. Making up one’s own rules is too frightening.
At 9 to 10 years, the child demonstrates a new ability to love by establishing a relationship with a best friend. This is important because the best friend is the first one outside the family that the child loves as being as important as themself. By sharing interests, goals and secret ideas with the best friend, the child learns a lot about themself. This is comforting because the child realises that they are not so different from other children after all. This yields a valuable lesson in self-acceptance.
Preadolescents demonstrate social interest outside the family. There is strong identity with the peer group by a small clique or a larger, more loosely organised crowd formation. Girls and boys stay within their own gender group. The clique has an exclusive membership, and one is privileged to belong. The code of the clique is important, with rules for dressing, speaking and behaving in common. The child merges their own identity with that of the peer group. The child is substituting conformity with the family to that with the peers because they need the security of a temporary identity before formulating a clear sense of self (Berk, 2010).
Despite the fact that peer groupings are composed of the same gender, some preadolescents show an emerging interest in mixed groups, an interest that will flourish in adolescence.
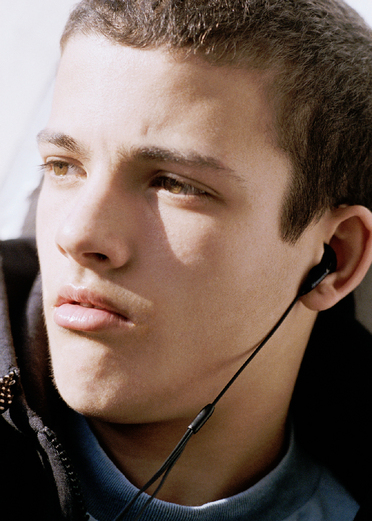
Adolescence (12 or 13 to 19 years)
This is a transition stage between childhood and adulthood (Fig 3.6). Beginning at puberty and extending through the teenage years, the most important task of adolescence is the search for identity—‘who I really am’. With successful mastery of skills from the previous stage, childhood ends. Now the adolescent must process the information from earlier stages and assume a personal identity that is more than just the sum of childhood experiences. The search for identity is the motive behind all the other tasks of the period:
1. Searching for one’s identity
2. Appreciating one’s achievements
3. Growing independent from parents
4. Forming close relationships with peers
5. Developing analytical thinking
6. Evolving one’s own value system

Physical development
Adolescence begins with puberty. Puberty is a time of dramatic physiological change. It includes the growth spurt—rapid growth in height, weight and muscular development; development of primary and secondary sex characteristics; and maturation of the reproductive organs.
A changing body affects a person’s self-concept. With bodies that are changing so rapidly, it is difficult for boys and girls to adjust. Their self-awareness peaks; they continually compare how their body looks with that of their peers and to some ideal standard of attractiveness. They are keenly attuned to the appearance of secondary sex characteristics but are embarrassed if these appear too early or too late. It is best when their own development parallels that of close friends and peers. Being an early maturer or, especially, a late maturer adds to normal self-doubts that they experience.
Physical health is generally good. Childhood illnesses are behind them, and the risks of adult illnesses are not yet present. What does place their health at risk are episodes of poor or immature judgment resulting in accidents, drug or alcohol abuse, driving a car while impaired with drugs or alcohol, sexually transmitted infections (STIs) and unwanted pregnancy. Psychological dysfunction may occur, such as anorexia nervosa or depression. Suicide acts and attempts affect an increasing number of adolescents. Suicide is a leading cause of death in this age group. Its incidence would probably be higher if more accidental deaths were investigated.
Adolescent’s periodic health examination
Study Table 3.2 for screening procedures and counselling measures. The physical examination should now include self-care on skin self-examination, breast self-examination or testicular self-examination, and frequency of pelvic examinations (see Chs 17, 25, 26, 27 and 28 for details). It is particularly important to include counselling on substance use, unwanted pregnancy prevention and STI risk reduction.
TABLE 3.2 Periodic health examination: ages 11–24 years
| Interventions considered and recommended for the periodic health examination | Leading causes of death |
|---|---|
| Interventions for the general population | |
| Interventions for high-risk populations | |
| Population | Potential interventions |
| High-risk sexual behaviour | RPR/VDRL; screen for gonorrhoea (female), HIV, chlamydia (female); hepatitis A vaccine, hepatitis B vaccine |
| Injection or street drug use | RPR/VDRL; HIV screen; hepatitis A vaccine; advice to reduce infection risk, hepatitis B vaccine |
| TB contacts | PPD |
| Aboriginal and Torres Strait Islanders | Influenza vaccine; pneumococcal polysaccharide (23vPPV) vaccine |
| Travellers to developing countries | Hepatitis A vaccine |
| Certain chronic medical conditions | Pneumococcal vaccine; influenza vaccine |
| Susceptible to varicella, measles, mumps | Varicella vaccine; MMR |
| Blood transfusion between 1978–1985 | HIV screen |
| Institutionalised persons; healthcare/lab workers | Hepatitis A vaccine; PPD; influenza vaccine |
| Family h/o skin cancer; naevi; fair skin, eyes, hair | Avoid excess/midday sun, use protective clothing, sunscreen |
| Prior pregnancy with neural tube defect | Folic acid 4.0 mg |
ATV, all-terrain vehicle; HIV, human immunodeficiency virus; HPV, human papillomavirus; MMR, measles-mumps-rubella; PPD, purified protein derivative; RPR, rapid plasma reagin; STI, sexually transmitted infection; TB, tuberculosis; VDRL, Venereal Disease Research Laboratories
1 Periodic blood pressure for persons aged ≥ 21 yr.
2 If sexually active at present or in the past ≤ 3 yr. If sexual history is unreliable, begin Pap tests at age 18 yr.
4 These vaccines are for one cohort only and within this age range and should only be given if there is no prior history of disease or vaccination. Dose schedules may vary between jurisdictions.
5 This vaccine is for one cohort only within this age range.
6 3 doses given over 6 months.
Adapted from The Guidelines for Preventive Activities in General Practice, 7th edn, 2009, www.racgp.org.au/redbook/iv and US Preventive Services Task Force: Guide to clinical preventive services, 2006, http://www.ahrq.gov/clinic/uspstfix.htm.
Psychosocial development
Erikson believed the main psychological conflict of adolescence (the fifth stage in his theory) to be ego identity versus identity confusion. The adolescent is preoccupied with how they look to others, and how that image fits with their own view of the self. If this process is successful, a sense of ego identity emerges, culminating in what Erikson terms a career choice. If unsuccessful, the teen is unsure of their skills, self-worth or sexual identity, then identity confusion results. The adolescent feels cut adrift and experiences anxiety about being a social outcast (Fig 3.7).
Finding one’s own identity is stressful. In the search for identity, teens often form cliques; wear fad clothing; and follow singers, movie stars or charismatic heroes in an attempt to siphon identity from them. Falling in love also feeds the quest for personal identity; the teen projects their own ego qualities onto another person and tries to understand them as they are reflected by the loved one.
Cognitive development
Adolescence corresponds to Piaget’s fourth stage, in which the person focuses on formal operations and the ability to develop abstract thinking, deal with hypothetical situations and make logical conclusions from reviewing evidence. Now, thinking is no longer confined to the concrete or the real but encompasses all that is possible. Abstract thinking is liberating. The adolescent is no longer limited to the present but can ponder the lessons of the past and the possibilities of the future. The adolescent can now analyse and use scientific reasoning. They can imagine hypotheses then set up experiments to test them. They learn to use logic and solve problems by methodically eliminating each possibility, one by one. This opens the doors to new academic achievements such as mastering advanced mathematical concepts, chemistry, physics or logic.
This analytic thinking extends to values. Developing personal values is a part of the search for identity. The adolescent does not accept packaged values of parents or institutions but can reason through their inconsistencies and recognise injustices. The adolescent is sensitive to hypocrisy and notes when an adult professes a value (such as honesty) and then acts counter to it (such as cheating on tax returns).
Behavioural development
Socially, the adolescent is in limbo, because they reject identity with the parents but are not yet sure of their own individual identity. The perfect solution to this dilemma is immersion in a peer group. Pressure to belong to a peer group intensifies at this age. The adolescent is influenced strongly by the group’s norms for dress and behaviour. By identifying with peers, the adolescent joins a sheltered workshop in which they feel safe and can experiment with various roles. Group members are allies in the universal goal of seeking freedom from parental domination.
Group identity means the adolescent spends more time away from home and the parents. Adolescents often feel ambivalent towards the parents. They desperately want to be independent from the parents but realise that economically, and even emotionally, this is impossible. Their stated desire to escape from parental dominance conceals their anxiety about leaving the safety of the family. The conflict is exacerbated when the parents try to maintain rigid control and use the protective stance that worked during earlier childhood. Often, things go more smoothly when the parents are not as strict; allow privacy; respect the adolescent’s budding identity; and, above all, take the adolescent seriously.
Developing close friendships is important to personal identity. In preadolescence the experience of the relationship with the best friend is valuable in teaching intimacy, trust and regard for another person. These lessons become a link in the new quest of developing close relationships with the opposite sex. Finding a girlfriend or boyfriend enables the adolescent to learn their own sex role identity. In many settings, group dating (youth groups, school dances) is the norm at first. This decreases stress from paired dating. When adolescents do pair off, the healthy goal is a monogamous relationship involving affection and fidelity.
Most adolescents worry that an occasional homosexual thought or act means that they are homosexual. These adolescent experiences are common and do not turn a person into a gay or a lesbian. Of course, some teenagers do discover that they have a homosexual orientation and that this lifestyle feels natural for them.
The end of adolescence is more difficult to define. Some societies have recognised rites of passage, usually at puberty, when the young person earns a place in the adult world with its attendant responsibilities. But in complex Western societies, the adolescent remains dependent on their parents through the teen years and into their twenties for economic and educational reasons. This extends the period of adolescence. Consequently, the role is not well defined in our society, and this is a source of conflict.
Early adulthood (20 to 40 years)
The young adult is concerned with emancipation from their parents and building an independent lifestyle. The young adult has finished most formal schooling and is ready to embark on a chosen path (Fig 3.8). The tasks of this era include:
1. Growing independent from the parents’ home and care
2. Establishing a career or vocation
3. Forming an intimate bond with another and choosing a mate
4. Learning to cooperate in a marriage relationship
5. Setting up and managing one’s own household
6. Making friends and establishing a social group
7. Assuming civic responsibility and becoming a citizen in the community

Physical and cognitive developments are now steady and do not affect the young adult as much as they have before. Rather, sociocultural factors and values buffet the novice adult.
Physical development
By early adulthood, the body reaches its maximum potential for growth and development. All body systems now operate at peak efficiency. The young adult enjoys maximum muscle tone and coordination, a high energy level and optimum mental power. This person exudes freshness and vitality.
Since growth has finished, nutritional needs depend on maintenance and repair requirements and on activity levels. If activity decreases from its level during adolescence, calories must be reduced. Sensible nutrition is a major problem for many adults; overweight and obesity are at epidemic levels in Australia. The diet should be high in fruits, vegetables and grains but all too often it is high in sugar, salt and fat. A sedentary lifestyle adds further problems. However, more adults are learning that frequent steady exercise maintains weight, muscle strength and joint flexibility; builds heart and lung capacity; and reduces stress. Table 3.2 lists these and other preventive counselling measures to address during healthcare visits.
Cognitive development
During adolescence, cognitive functioning reached the new level of formal operations, or the capacity for abstract thinking. This level continues, but the young adult’s thinking is different from the adolescent’s. The young adult is less egocentric and operates in a more realistic and objective manner. Now the young adult is close to maximum ability to acquire and use knowledge. The potential for sophisticated problem solving and creative thinking is at a new height.
Education continues for many young adults, from formal courses in a University/TAFE/Polytechnic environment to on-the-job training and continuing education classes. Usually, this education prepares the young adult to do some type of work. Work is an important factor in the young adult’s life because it is tied closely with ego identity. A person with job satisfaction feels challenged, rewarded and fulfilled, whereas when a person is frustrated with work, they can feel bored and apathetic.
However, some young adults cannot find work. Those from dysfunctional families, those from low-income households, refugees and those who have recently migrated to Australia may lack the resources to obtain the education they need. Because Australia has become an increasingly technological society, fewer jobs are available for people with little schooling. Unemployment has profound social implications which may include a lack of money for housing, proper nutrition and transport.
Psychosocial development
Erikson’s sixth stage covers the first years of early adulthood, from 20 to 24 years. He believed the major psychological conflict to be resolved is that of intimacy versus isolation. Once self-identity is established after adolescence, it can be merged with another’s in an intimate relationship. During the early 20s, the adult seeks the love, commitment and intimacy of an intense lasting relationship. This mature relationship includes mutual trust, cooperation, sharing of feelings and goals, and complete acceptance of the other person. Although Erikson had a heterosexual union in mind, this intimacy could be satisfied through a homosexual relationship or through a bond with a cause or an institution.
Erikson believed that without a secure personal identity, a person cannot form a love relationship. The result is the negative outcome of a person who is isolated, withdrawn and lonely. This person may fill the void with numerous transient liaisons or promiscuity, but Erikson believed that these experiences will be found to be shallow and the person will feel remote and alone.
Daniel Levinson’s (1986, 1996) time frame of early adulthood is much broader than Erikson’s. It encompasses 22 to 40 years. Levinson believes that an adult’s life alternates between periods of structure building, in which a lifestyle is fashioned, and periods of transition, in which this lifestyle is evaluated, appraised and modified.
The era of Early Adulthood has two structure-building periods. In the twenties (about 22 to 28 years), the novice adult establishes the ‘entry structure’, a first provisional lifestyle linking them to adult society. They are building a home base. During this time, the first set of important choices is made concerning a mate, friends, an occupation, values and lifestyle. In making these choices, the person must juggle the conflicting drives of (1) exploring many possibilities and keeping options open on the one hand, and (2) securing some stability on the other hand (Levinson, Darrow and Klein, 1986).
The Age Thirty Transition, age 28 to 33 years, is a time of self-reflection. Questions asked include ‘Where am I going?’ and ‘Why am I doing these things?’ This is the first major reassessment in life. A person ponders aspects that they want to add, exclude or modify in life. The person feels, ‘If there is anything I want to change I had better start now, or it will be too late’ (Levinson et al, 1986).
According to Levinson, the rest of the thirties (33 to 40 years) is characterised by settling down. A person takes the reforms or the reaffirmations established during the transitional period of the thirties and fashions a culminating life structure, one that realises their youthful aspirations. During these years, the adult strives to establish a niche in society and to build a better life in all the choice points. This person is building a nest, using deliberation and seeking order and stability.
Sometimes, the reforms include having children. The addition of children brings a major readjustment to the couple’s relationship. Roles are reshaped in the new family unit. For some couples, the father is more involved in child care than most fathers were in past generations. The mother’s role may include a choice between full-time parenting or a return to employment outside the home. Women are fully in the work force now. Although the opportunities are wider, the risk for stress exists because choices must often be made. The tension shifts from having no choice in a former traditional role to whether or not the right decision is being made now.
However, for many women, the luxury of having options does not exist. Single parents struggle to support themselves and their children. Often they have neither the time nor the financial resources to provide the basic needs for their children or for themselves.
Middle adulthood (40 to 64 years)
At some point in the forties, the realisation dawns and grows that life is half over. No longer does the dream of young adulthood seem fully attainable. To some, it seems that there is more time to look back on than to see ahead. How the person deals with these feelings and builds a meaningful life structure is the task of middle adulthood. Its composite tasks include:
1. Accepting and adjusting to the physical changes of middle age
2. Reviewing and redirecting career goals
3. Achieving desired performance in career
4. Developing hobby and leisure activities
5. Adjusting to ageing parents
6. Helping adolescent children in their search for identity
Physical development
A look in the mirror brings rueful recognition of the beginning of ageing effects on the body. The skin loses its taut surface and forms wrinkles around the eyes, mouth and forehead. Some notice pouches under the eyes and sagging jowls. The hair thins a little, starts to lose pigment and turns grey, and in men the hairline often recedes. An abdominal paunch grows from increased fat deposits and decreased physical activity. Internally, most organ systems hold constant, with some small decrease in respiratory capacity and cardiac function. Sensory function remains intact except for some visual changes (e.g. decreased accommodation for near vision, or presbyopia).
In the late forties and early fifties, females experience menopause, the decreasing frequency and finally the cessation of menstruation. This involves a decrease in the female hormones oestrogen and progesterone, which brings attendant symptoms such as atrophy of reproductive organs, vasomotor disturbances and mood swings (Ch 25). Although men do not have such an abrupt halt to reproductive ability, they experience a decrease in the production of testosterone, which causes decreased sperm and semen production and less intense orgasms.
Middle-aged adults are suddenly aware of the occasional death of their peers. This is a rude reminder of their own mortality. The Australian Institute of Health and Welfare estimates that 94% of males and 89% of females in the 45–54 age range have at least one risk factor for cardiovascular disease. Almost one in four Australians 25 years and over has either diabetes or impaired glucose metabolism, which increases the risk of heart disease and diabetes later in life (O’Brien, 2005). The leading causes of death during middle adulthood are cancer, cardiovascular diseases and injuries (Table 3.3). Morbidity is also increased, probably caused most often by obesity. Obesity is associated primarily with hypertension and also with cardiovascular disease, diabetes and mobility dysfunction such as arthritis. Chronic smoking leads to health problems in middle adulthood. Health statistics for the New Zealand population are just as concerning (New Zealand Government, 2008). The findings of the 2006–07 New Zealand health survey revealed 65.7% of people surveyed had a chronic health condition; the most common conditions were high blood pressure (13.6%), and asthma (11.2%). Other common health conditions were ischaemic heart disease, arthritis, neck or back disorders, migraine and eczema.
TABLE 3.3 Periodic health examination: ages 25–64 years
| Interventions considered and recommended for the periodic health examination | Leading causes of death |
|---|---|
| Interventions for the general population | |
| Interventions for high-risk populations | |
| Population | Potential interventions |
| High-risk sexual behaviour | RPR/VDRL; screen for gonorrhoea (female), HIV, chlamydia (female); hepatitis B vaccine; hepatitis A vaccine |
| Injection or street drug use | RPR/VDRL; HIV screen; hepatitis B vaccine; hepatitis A vaccine; advice to reduce infection risk |
| TB contacts | PPD |
| Aboriginal and Torres Strait Islanders | Pneumococcal vaccine; influenza vaccine |
| Travellers to developing countries | Hepatitis B vaccine; hepatitis A vaccine |
| Certain chronic medical conditions | Pneumococcal vaccine; influenza vaccine |
| Susceptible to measles, mumps or varicella | MMR; varicella vaccine |
| Institutionalised persons | Hepatitis A vaccine; pneumococcal vaccine; influenza vaccine |
| Healthcare/lab workers | Hepatitis B vaccine; hepatitis A vaccine; PPD; influenza vaccine |
| Family h/o skin cancer; fair skin, eyes, hair | Avoid excess/midday sun, use protective clothing, sunscreen |
| Previous pregnancy with neural tube defect | Folic acid 4.0 mg |
ATV, all-terrain vehicle; HIV, human immunodeficiency virus; MMR, measles-mumps-rubella; PPD, purified protein derivative; RPR, rapid plasma reagin; STI, sexually transmitted infection; TB, tuberculosis; VDRL, Venereal Disease Research Laboratories
1 Women who are or have been sexually active and who have a cervix: ≤3 yr.
3 Mammogram 1–2 yr, or mammogram 1–2 yr with annual clinical breast examination.
4 Serological testing, documented vaccination history and routine vaccination (preferably with MMR) are equally acceptable alternatives.
Adapted from The Guidelines for Preventive Activities in General Practice, 7th edn, 2009, www.racgp.org.au/redbook/iv and US Preventive Services Task Force: Guide to clinical preventive services, 2006, http://www.ahrq.gov/clinic/uspstfix.htm.
Cognitive development
Intelligence levels remain generally constant during middle adulthood. Intelligence is further enhanced by the knowledge that comes with life experience, self-confidence, a sense of humour and flexibility. The middle-aged adult is interested in how new knowledge is applied, not just in learning for learning’s sake. Continuing education courses meet the need to keep knowledge current in occupational and personal interest areas. Many middle-aged adults are seeking college degrees for the first time or are pursuing advanced degrees.
Psychosocial development
Physical, personal and social forces all interact during the era of middle adulthood. How a person reacts to the physical cues of ageing affects their personality and self-perception. A success or disappointment in the career affects a person’s self-image, stress level and interpersonal relationships.
Erikson believed that the most important task for personality development is resolution of the conflict of generativity versus stagnation. Erikson believed that during the middle years adults have an urge to contribute to the next generation. This need can be fulfilled either by producing the next generation or by producing something to pass on to the next generation. Thus, middle-aged adults want to rear their own children or to engage in other creative, socially useful work. The motivation is to create and/or nurture those who will follow.
The middle-aged adult needs to be needed, to leave something behind and to leave their mark on the world. Generativity is sharing, giving, contributing to the growth of others. If this need is not fulfilled, the negative outcome is stagnation. Stagnation means experiencing boredom and a sense of emptiness in life, which leads to being inactive, self-absorbed, self-indulgent and a chronic complainer.
Levinson (1986) describes the era of middle adulthood as beginning with a mid-life transition. Roughly between 40 and 45 years, the person starts a major reassessment: ‘What have I done with my life?’
The rest of the forties, according to Levinson, involves making choices and building a new life structure. The person confronts reality; some goals simply cannot be met. This must be accepted and goals adjusted. The person takes stock and emerges with a new perception of the self and the environment. For those who have come through the mid-life transition and have found inner meaning, life will be ‘less tyrannised by the ambitions, passions and illusions of youth’ (Levinson et al, 1986).
For women, the mid-life transition includes the issue that the biological boundary of childbearing is now in sight. Women feel a time pinch that forces a survey of their life. Ageing and biology force women to review options that were set aside and that will be closed off in the now-foreseeable future. Even those satisfied with the number of children that they have or those without children will face this review.
Whatever the central issue, all those in mid-life transition explore the meaning of their career, their family and their personal identity. In terms of career, a person who spent the thirties searching for power and responsibility may now crave inner meaning (Levinson, 1986). Also, the middle-aged adult is aware of the time left until retirement. This may result in a reordering of career goals or in a new career path.
Career reassessment is intertwined with personal and family reassessment. New roles emerge as the middle-aged adult deals with growing children and ageing parents. This is popularly termed the ‘sandwich generation’. The adult is often caught in a ‘squeeze’ between the simultaneously changing needs of adolescent children and ageing parents.
Role realignment occurs in the individual’s relationship with ageing parents. Even if the parents are healthy and active, a role reversal occurs. The middle-aged adult gradually starts to take the parent’s place as the one in charge. When one of the parents dies, the middle-aged adult is confronted with loss of the protective myth that ‘Death cannot happen to me or my loved ones’ (Caplan, 1990). The parent was a shield between the self and death. Once the parent dies, the middle-aged adult is more vulnerable and realises the limited quantity of time left.
Another family task facing the middle-aged adult is to help the adolescent child in their search for identity. The parent must adjust to the adolescent’s desire to be independent and less involved in the family activities and the need for increased responsibility. Some parents nurture the independence and delight in the budding individual. Others tend to be overprotective and controlling. They may feel that their adolescent is too immature, or they do not want the adolescent to make the same mistakes that they did. The adolescent resents this attempt to relive the parent’s life through their own. Also, some parents dread the empty nest.
Once the youngest child does leave home, the parent faces the empty nest. If the parent (often the mother) has focused only on the children, she may feel left with little to live for. Will she find something as important as the children to replace them? This dilemma is more poignant now than it was in the past when adult children stayed fairly close to home. With society’s current mobility, the grown child often starts a new nuclear family at a faraway location.
The empty nest leaves parents alone as a couple again. They may face a relationship that is devoid of meaning apart from their children. They may find themselves dissatisfied, that they do not know each other; that they have drifted apart. Divorce may result and loom as a major crisis. Other couples may find this a positive and liberating phase. Their marriage is happier, with shared activities, increased freedom and more time to travel. They look back on the shared memories of parenting with a satisfied smile.
Late adulthood (65+ years)
Although negative stereotypes exist for each age group, none is more prevalent than the one for ageing adults. Ageism means discrimination based on age. It is a derogatory attitude that characterises older adults as sick, senile and useless and as a burden on the economy. It reveals our society’s anxiety about ageing. The attitude stems in part from our cultural emphasis on youth, beauty and vigour. Other cultures respect and revere their ageing members.
This ageist attitude is changing, partly because late adulthood is now the fastest-growing segment of our population and its members command attention. People over 65 years should be seen not as a homogeneous group with predictable reactions but as individuals with specific needs and widely divergent responses (Fig 3.9). Developmental tasks of this group include:
1. Adjusting to changes in physical strength and health
2. Forming a new family role as an in-law and/or grandparent
3. Affiliating with one’s age group
4. Adjusting to retirement and reduced income
5. Developing postretirement activities that enhance self-worth and usefulness
6. Arranging satisfactory physical living quarters
7. Adjusting to the death of spouse, family members and friends

Physical development
Everyone does not age at the same rate. One person at 60 years can look older and feel weaker than another at 75 years. The widely divergent response depends on subjective attitude, physical activity, nutrition, personal habits and the occurrence of physical illness. Although ageing is known to be a lifelong process, its mechanism is not fully understood. An inevitable decline occurs in body functions that seem to be independent of stress, trauma and disease. Illness affects ageing people more than those in other age groups. Incidence of chronic disease increases, resistance to illness decreases and recuperative power decreases. That is, after an acute illness an older person does not recover as quickly or as completely as a younger person. Everyday body aches and pains increase. Some people over 65 become preoccupied with their physical discomfort, whereas others adjust to a few aches with equanimity. All these events mean that the older person is increasingly dependent on the health care system for advice, health teaching and physical care (Table 3.4).
TABLE 3.4 Periodic health examination: age 65 and older
| Interventions considered and recommended for the periodic health examination | Leading causes of death |
|---|---|
| Interventions for the general population | |
| Interventions for high-risk populations | |
| Population | Potential interventions |
| Institutionalised persons | PPD; hepatitis A vaccine; hepatitis B vaccine |
| Chronic medical conditions; TB contacts; low income; immigrants; alcoholics | PPD; pneumococcal vaccine; influenza vaccine |
| Persons ≥ 75 yr; or ≥ 70 yr with risk factors for falls | Fall prevention intervention |
| Cardiovascular disease risk factors | Consider cholesterol screening |
| Family h/o skin cancer; naevi; fair skin, eyes, hair | Avoid excess/midday sun, use protective clothing, sunscreen |
| Aboriginal and Torres Strait Islanders | Pneumococcal vaccine; influenza vaccine |
| Travellers to developing countries | Hepatitis A vaccine; hepatitis B vaccine |
| High-risk sexual behaviour/Injection or street drug use | Hepatitis A vaccine; HIV screen; hepatitis B vaccine; RPR/VDRL advice to reduce infection risk |
| Healthcare/lab workers | PPD; hepatitis A vaccine; hepatitis B vaccine |
| Persons susceptible to varicella | Varicella vaccine |
CPR, Cardiopulmonary resuscitation; HIV, human immunodeficiency virus; PPD, purified protein derivative; RPR, rapid plasma reagin; STI, sexually transmitted infection; TB, tuberculosis; VDRL, Venereal Disease Research Laboratories
2 Mammogram q 1–2 yr, or mammogram q 1–2 yr with annual clinical breast exam.
3 All women who are or have been sexually active and who have a cervix: q ≤ 3 yr. Consider discontinuation of testing after age 65 yr if previous regular screening with consistently normal results.
Adapted from The Guidelines for Preventive Activities in General Practice, 7th edn, 2009, www.racgp.org.au/redbook/iv and US Preventive Services Task Force: Guide to clinical preventive services, 2006, http://www.ahrq.gov/clinic/uspstfix.htm.
Cognitive development
Ageing does not have a predictable effect on intelligence. Intellectual function depends on various factors, such as motivation, interest, sensory impairment, educational level, general health, social concerns, involvement in community activities or stimulating leisure activities, as well as a compensatory tendency to conserve time and emotional energy. People over 65 years do have a slower reaction time. They often have decreased ability for complex decision making and decreased speed of performance, but no decrease in general knowledge occurs. These adults experience little or no loss in verbal comprehension or in the application of experience. Age-related memory declines are usually on tasks that need deliberate processing (i.e. problems remembering names, where they placed their keys or other objects, appointments or medication schedules) (Berk, 2010).
Psychosocial development
Levinson (1986) suggests a relationship between physical changes of the body and personality. By 60 years, most people are aware of some body decline. Although variations exist, most people over 65 have at least one serious illness or limiting condition and are aware of the increasing frequency of death in peers. These issues, coupled with society’s negative connotation of ageing, may lead to a fear that the person has lost all vestiges of youth, even those to which they had a tenuous hold during middle adulthood. The person fears that the youth within is dying. The task, then, is to look for a new form of youthfulness, a new force of inner growth to sustain the last era.
The era of late adulthood directs this inner youthfulness towards new creative endeavours. The adult over 65 has stepped off centre stage both in formal employment and in the family clan. This can be traumatic because it means a loss of recognition and authority. But now the person can direct energy inwards. When financially and socially secure, the older adult can pursue whatever activity is important. They have paid their dues to society and can now pursue whatever is pleasing. The person creates a new balance with society; they are less interested in society’s extrinsic rewards and more interested in using inner resources (Fig 3.10).

Confronting tasks.
How an older adult responds to retirement depends largely on job satisfaction. If the job was rote and meaningless, the person may welcome the release provided by retirement. But if the job signified power and status, or had high complexity, retirement may have a devastating effect. The retired person feels the loss of title and authority. A loss of professional associates who had common interests and were intellectually stimulating also occurs, and a social outlet is lost when co-workers constituted a friendship group.
It is important to develop postretirement activities that enhance self-worth and give a feeling of usefulness. These activities may include developing a new ‘semi-retired’ career, or a hobby, sport interest or community service activity. The transition to retirement is eased if these activities are well in place before the last formal day on the job.
Having the retired person spend more time at home may affect the marriage relationship. Traditionally, it was the husband who was suddenly at home and ‘under foot’. Now more employed women exist who face the same retirement adjustment. Some couples do find that having one or both at home more means an invasion of previously held ‘turf’, such as the kitchen, garden or workshop. Other couples develop a more egalitarian relationship. They are now free of earlier sex role definitions and are able to share household tasks and leisure activities equally.
Family roles are also adjusted with the marriage of grown-up children and the addition of in-laws. How the sons- or daughters-in-law are absorbed into the family affects the older adult. This often involves a new role as grandparent. Being able to indulge and provide moral support to a grandchild is usually positive for all, unless the caretaking becomes a burden to the grandparent.
Retirement often involves financial adjustment. This may involve a reduced income, perhaps only minimal superannuation benefits and a limited pension. This may be hard if the person is used to a higher standard of living. Even if the retired person owns their own home, the cost of maintaining it may exceed the income.
Establishing suitable living arrangements has both financial and family significance. In our culture, the extended family mostly has disappeared today. No longer do three generations live under one roof. In the past, the older adult contributed light household tasks that gave a sense of personal worth. Now, the contributions to the extended family that were made by the older family member have been replaced by advances in household mechanisation, food processing and day care centres.
Thus many adults over 65 choose to live independently, either as couples or alone. When it becomes difficult to manage self-care, they face the choice of moving in with grown children or moving into a retirement home or assisted living/nursing home. All of these choices involve some disbursement of personal belongings and the relinquishing of some privacy.
Through the late adult years, each person is reminded of their own limited time left by the increasing frequency of death and serious illness of friends, colleagues, siblings or of other family members, perhaps including the spouse.
The life review.
One important task of late adulthood is performing a life review. Older adults have finished all or most of their life’s work. Their contribution to society and to their own immortality is mostly completed (Levinson et al, 1986). The life review is a cataloguing of life events, a considering of one’s successes and failures with the perspective of age. The objective of the task is to gain a sense of integrity in reviewing one’s life as a whole (Fig 3.11).

This period relates to Erikson’s last ego stage, with its key psychological conflict of ego integrity versus despair. A successful resolution to this final conflict occurs when the adult accepts ‘one’s one and only life cycle as something that had to be and that, by necessity, permitted of no substitutions’ (Erikson, 1963). The older adult reviews events, experiences and relationships and realises that these have been mostly good. There are cherished memories. The person has had a meaningful part in human history and can meet death with equanimity.
Failure to resolve this last conflict leaves the person with a sense of despair, resentment, futility, hopelessness and a fear of death. However, a successful outcome completes a cycle. The contented older adult who does not fear death serves as a role model for younger adults that life can be trusted.
Levinson believes everyone has a sense of utter despair at some point during this time. To gain a sense of integrity, one has to confront the lack of integrity (Levinson et al, 1986). Some goals have not been achieved, and what is worse is that the damage is done and it is too late to set it right. The person realises that whatever values were held, they cannot fully live up to them. This must be reconciled; it is an imperfect world. The task is to make peace with the self.
This final sense of what life is about is a close parallel to Erikson’s last stage. Levinson likens the person’s perspective at this time as a ‘view from the bridge’ at the end of the life cycle (Levinson et al, 1986). One ‘must come finally to terms with the self—knowing it and loving it reasonably well, and being ready to give it up’.
DEVELOPMENTAL SCREENING TESTS
The Denver II—Revision and Restandardization of the Denver Developmental Screening Test (DDST)
Time required: 10 to 25 minutes
Authors: W Frankenburg, J Dodds, P Archer, B Bresnick, H Shapiro
This is a screening instrument designed to detect developmental delays in infants and preschoolers. It tests four functions: gross motor, language, fine motor-adaptive and personal–social skills.
The Denver II is not an intelligence test; it does not predict current or future intellectual ability. It is not diagnostic; it does not suggest treatment regimens. What the Denver II does do is screen; it helps identify children who may be slow in development. This is important because early detection increases the opportunities for effective treatment.
The Denver II was revised in 1989 and restandardised for a sample including three ethnic groups, three residence categories (rural, suburban and urban) and three levels of maternal education (less than high school, high school and more than high school). These norms should ameliorate the limitations of the earlier DDST concerning its relevance to various population groups (Frankenburg, Fandal and Sciarillo, 1981). The Denver II also appears to address the limitations experienced by Olade (1984) in using the earlier DDST in developing countries. Olade’s study of African children in Nigeria suggested that language differences (naming certain colours, limited use of plurals and parents’ last names) and unfamiliar interactive games (peek-a-boo) affected DDST results. These items are omitted or adjusted in the Denver II. However, the culture of developing countries must still be considered when using screening tests.
The Denver II is easily incorporated into the daily professional regimen of nurses, physicians and teachers. The 125 items are arranged in chronological order and are displayed in groupings corresponding to recommended ages for health maintenance visits. The clear pictorial charts aid in administering, scoring and interpreting the test. It is reliable and economical. The materials are few in number, attractive to children and easily maintained and replaced. The scoring avoids diagnostic labelling (such as mental retardation, language disorder and cerebral palsy). Instead, the child’s performance is scored as ‘normal’, ‘abnormal’ or ‘questionable’, and includes an adjustment in scoring for premature infants.
Uses of the Denver II include (Frankenburg et al, 1981):
• Screening of infants, whose rapid rate of development makes it difficult to rely on professional opinion or on parent history alone
• Longitudinal following of a single child in healthcare or educational setting
• Follow-up in clinics, where a child may be seen briefly, infrequently or by different examiners
Adult life stress measures
Some tools are available that attempt to quantify the impact of life change on a person’s health. They are based on the assumption that a relationship exists between daily life stress and a person’s susceptibility to physical and psychological problems. Many of the life change events are the developmental tasks discussed earlier in the chapter.
The Hassles and Uplifts Scale
This is a 53-item self-administered questionnaire whose purpose is to assess day-to-day stress (Table 3.5). Take this test yourself just before you go to bed one day. Consider each item on the list, and circle a number on the left-hand side regarding how much of a hassle the item was for you that day. On the right-hand side, circle a number regarding how much of an uplift the same item was for you that day. Total scores are obtained by summing across ratings given to all items.
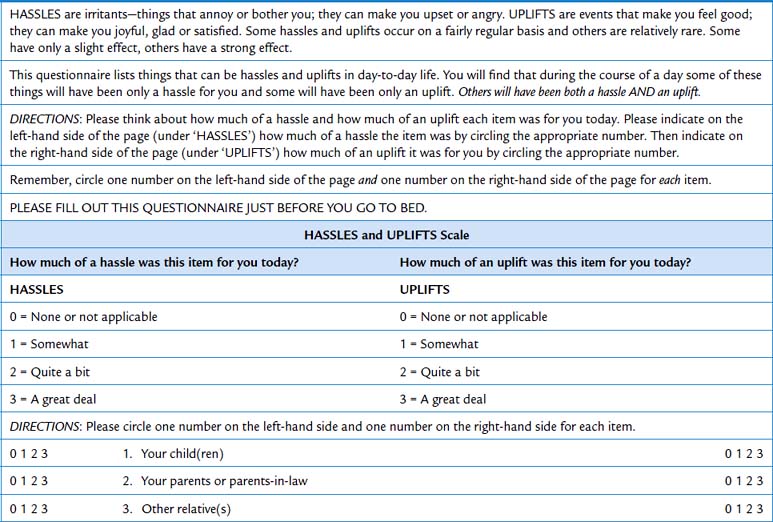
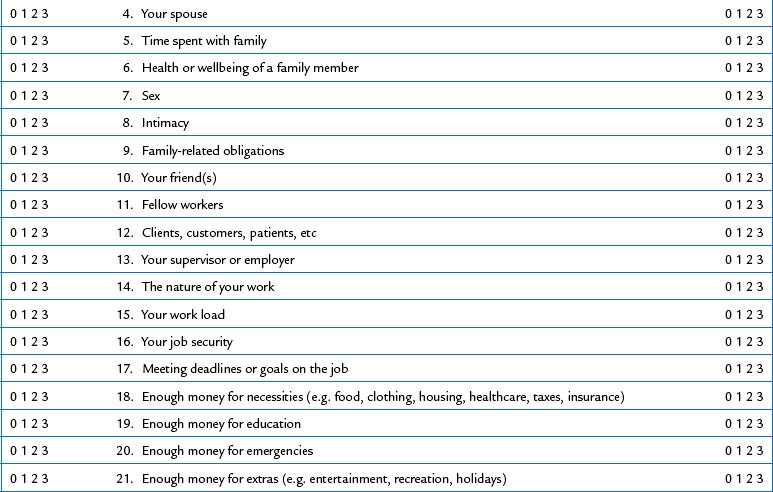
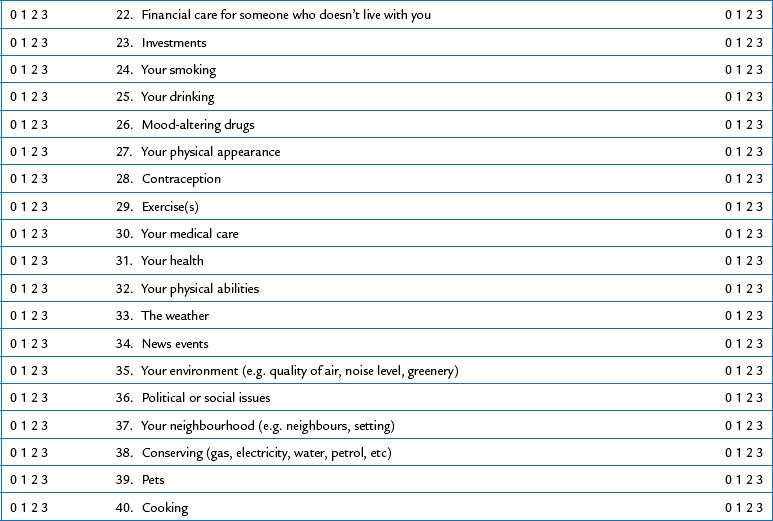
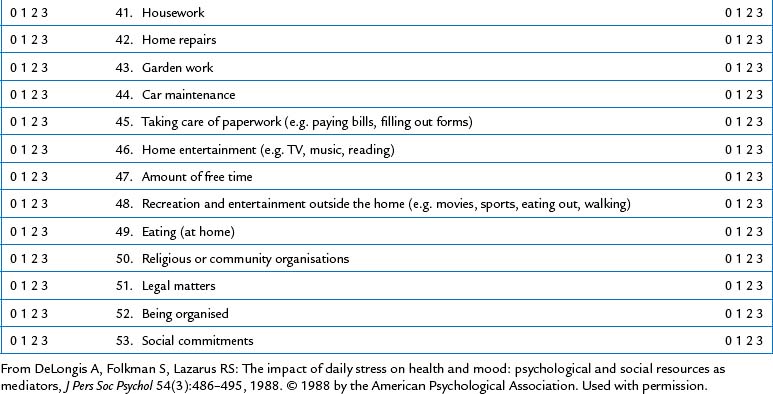
Relatively minor but frequently experienced stresses, termed Hassles in this tool, have been found to correlate strongly with negative health status (Weinberger, Hiner and Tierney, 1987). DeLongis, Folkman and Lazarus (1988) found a significant relationship between daily stress and concurrent or later occurrence of physical health problems, such as flu, sore throat, headaches and backaches. There was great individual variation, however, with one-third of the respondents reporting a somewhat improved health and mood with increased stress levels! Regarding daily stress and psychological disturbance, they found that individuals with unsupportive social relationships and low self-esteem had a greater risk of psychological and somatic health problems, both on their stressful days and following their stressful days, than did individuals with positive social networks and high self-esteem (DeLongis, Folkman and Lazarus, 1988).
CULTURAL AND SOCIAL CONSIDERATIONS
Much of the developmental content of this chapter has been normed to the findings of research and experience with people from the dominant, European heritage cultures. Given the rate of demographic change, it is imperative to consult with cultural brokers and/or patient advocates from the patient’s cultural heritage who have a deeper understanding of the expected norms of the various developmental tasks.
The immunisation protocols from other nations differ from those of Australia and careful examinations of health records must be undertaken. When assessments are conducted, competent interpreters must be used.
Abdullah ASM, Simon JL. Health promotion in older adults: Evidence-based smoking cessation programs for use in primary care settings. Geriatrics. 2006;61(3):30–34.
Arnett JJ. Emerging adulthood: a theory of development from the late teens through the twenties. Am Psychol. 2000;55(5):469–480.
Australian Bureau of Statistics. Causes of death Australia. Canberra: Australian Bureau of Statistics, 2008.
Australian Bureau of Statistics, Australian Institute of Health and Welfare. The health and welfare of Australian Aboriginal and Torres Strait Islander Peoples. Canberra: Australian Bureau of Statistics and Australian Institute of Health and Welfare, 2008.
Australian Government Department of Health and Ageing. National bowel cancer screening program. Available at www.cancer screening.gov.au/internet/screening/publishing.nsf/Content/bowel-1lp, 2007.
Australian Institute of Health and Welfare Dental Statistics and Research Unit. Research report No 9. Social determinants of oral health. Canberra: AIHW, 2003.
Barnard S, Edgar D. Pediatric eye care. Oxford, England: Blackwell Science, 1996.
Berk LE. Development through the lifespan, 5th edn. Boston: Allyn and Bacon, 2010.
Bos R. Health impact assessment and health promotion. Bull World Health Organ. 2006;84(11):914–915.
Bryant LL, Altpeter M, Whitelaw NA. Evaluation of health promotion programs for older adults: an introduction. J Appl Gerontol. 2006;25(3):197–213.
Budd GM, Hayman LL. Childhood obesity: determinants, prevention, and treatment. J Cardiovasc Nurs. 2006;21(6):437–441.
Caplan G. Loss, stress, and mental health. Community Mental Health Journal. 1990;26:27–48.
Christie D, Viner R. ABC of adolescence: adolescent development. Br Med J. 2005;330:301–304.
DeLongis A, Folkman S, Lazarus RS. The impact of daily stress on health and mood: psychological and social resources as mediators. J Pers Soc Psychol. 1988;54(3):486–495.
Durocher HJ. As they grow. 4–5 years: ‘I’ll get it right!’. Parents. 2006;81(8):123–124.
East L, Folkman, Jackson, O’Brien L. Father absence and adolescent development: a review of the literature. J Child Health Care. 2006;10(4):283–295.
Erikson EH. Childhood and society. New York: WW Norton, 1963.
Erikson EH. Identity: youth and crisis. New York: WW Norton, 1968.
Ertem IO, et al. Promoting child development at sick-child visits: a controlled trial. Pediatrics. 2006;118(1):e124–e131.
Fitzgerald B. An existential view of adolescent development. Adolescence. 2005;40(160):793–799.
Fonda AR, et al. Using child health checks to assess the prevalence of overweight and obesity among urban indigenous children. Medical Journal of Aust. 2010;192(10):596.
Frankenburg WK, Fandal AW, Sciarillo W. The newly abbreviated and revised Denver Developmental Screening Test. J Pediatr. 1981;99(6):995–999.
Fulkerson JA, et al. Family dinner meal frequency and adolescent development: a relationship with developmental assets and high-risk behavior. J Adolesc Health. 2006;39(3):337–345.
Galil N. Depression and asthma in children. Current Opinion in Pediatrics. 2000;12(4):331–335.
Gattellari M, Ward J. Does evidence-based information about screening for prostate cancer enhance consumer decision-making? A randomised controlled trial. J Med Screen. 2003;10:27–29.
Girolami G, et al. Parent’s knowledge and perception about child development: evidence from a practice-based survey. Pediatr Phys Ther. 2006;18(1):91–92.
Gregory AT, Lowy MP, Zwar NA. Men’s health and wellbeing: taking up the challenge in Australia—editorial. Med J Aust. 2006;Oct 16; 185(8):411.
Haines J, Neumark-Sztainer D. Prevention of obesity and eating disorders: a consideration of shared risk factors. Health Educ Res. 2006;21(6):770–782.
Klaff LG. As they grow. 1 year: walk on!. Parents. 2006;81(8):115–116.
Kosters JP, Gotzsche PC. Regular self-examination or clinical examination for early detection of breast cancer. Cochrane Database Syst Rev. 2008:1.
Levinson DJ. A conception of adult development. Am Psychol. 1986;41:3–13.
Levinson DJ. The seasons of a woman’s life. New York: AA Knopf, 1996.
Levinson DJ, Darrow CN, Klein EB. The seasons of a man’s life, ed 2. New York: Ballantine, 1986.
Moninger J. As they grow. 6–8 years: funny business. Parents. 2006;81(8):127–128.
Nakasato YR, Carnes BA. Health promotion in older adults: promoting successful aging in primary care settings. Geriatrics. 2006;61(4):27–31.
National Breast Cancer Centre. Advice about familial aspects of breast cancer and ovarian cancer: a guide for health professionals. Available at www.nbocc.org.au/bestpractice/resources/BOG182_adviceaboutfamiliala.pdf, 2006.
National Breast Cancer Centre. Position statement: Early detection of breast cancer. Available at www.nbocc.org.au/resources/documents/EDP_early detectionposition0804.pdf, 2004.
Neumark-Sztainer D, et al. Self-weighing in adolescents: helpful or harmful? Longitudinal associations with body weight changes and disordered eating. J Adolesc Health. 2006;39(6):811–818.
New Zealand Government. A portrait of health: Key results for the 2006/07 New Zealand health survey. Available at http://www.moh.govt.nz/moh.nsf/pagesmh/7601/$File/portrait-of-health-june08.pdf, 2008.
Niemeier HM, et al. Fast food consumption and breakfast skipping: predictors of weight gain from adolescence to adulthood in a nationally representative sample. J Adolesc Health. 2006;39(6):842–849.
Nilsson M, et al. It takes two: reducing adolescent smoking uptake through sustainable adolescent–adult partnership. J Adolesc Health. 2006;39(6):880–886.
O’Brien K: Living dangerously: Australians with multiple risk factors for cardiovascular disease, Bulletin No. 24. AIWH. Cat. no. AUS 57. Canberra: Australian Institute of Health and Welfare, 2005.
Olade RA. Evaluation of the Denver Developmental Screening Test as applied to African children. Nurs Res. 1984;33(4):204–207.
Olds DL. Effects of nurse home-visiting on maternal life course and child development: age 6 follow-up results of a randomized trial. Pediatrics. 2004;114(6):1550–1559.
Padula CA, Sullivan M. Long-term married couples’ health promotion behaviors: identifying factors that impact decision making. J Gerontol Nurs. 2006;32(10):37–47.
Penm E. Cardiovascular disease and its associated risk factors in Aboriginal and Torres Strait Islander Peoples 2004–2005. Canberra: Australian Institute of Health and Welfare, 2008.
Piaget J. Judgment and reasoning in the child. Totowa, NJ: Littlefield, Adams, 1968.
Piaget J. The construction of reality in the child. New York: Ballantine, 1975.
Rydz D, et al. Screening for developmental delay in the setting of a community pediatric clinic: a prospective assessment of parent-report questionnaires. Pediatrics. 2006;118(4):e1178–e1186.
Smith J, McSherry W. Spirituality and child development: a concept analysis. J Adv Nurs. 2004;45(3):307–315.
Smith LM, et al. The infant development, environment, and lifestyle study: effects of prenatal methamphetamine exposure, polydrug exposure, and poverty on intrauterine growth. Pediatrics. 2006;118(3):1149–1156.
Spelke ES, et al. Origins of knowledge. Psychol Rev. 1992;99:605–632.
Srof BJ, Velsor-Friedrich B. Health promotion in adolescents: a review of Pender’s health promotion model. Nurs Sci Q. 2006;19(4):366–373.
Stathakis V: Hospitalised injuries, Victoria, July 1992–June 1998, October 1999, Report No. 160, Monash University Accident Research Centre, 1999.
Struck BD, Ross KM. Health promotion in older adults: prescribing exercise for the frail and home bound. Geriatrics. 2006;61(5):22–27.
The Cancer Council Australia. National cancer prevention policy 2007–2009. NSW: The Cancer Council Australia, 2007.
The Royal Australian College of General Practitioners ‘Red Book’ Task force. Guidelines for preventive activities in general practice, 7th edn. South Melbourne: The Royal Australian College of General Practitioners, 2009.
Thomas H. Obesity prevention programs for children and youth: why are their results so modest? Health Educ Res. 2006;21(6):783–795.
Thomas S, Stewart J. Optimising health promotion activities. J Community Nurs. 2005;19(1):9–10. 12
van Beek Y, et al. Maternal expectations about infant development of preterm and full-term infants: a cross-nation comparison. Infant Child Dev. 2006;15(1):41–58.
Van Breeman C. Adolescent development amidst progressive illness: a support group model. J Palliat Care. 2006;22(3):240–241.
van Mechelen W, Verhagen E. Injury prevention in young people—time to accept responsibility. Lancet. 2005;366(Special Issue):S46.
Wagner J, Jenkins B, Smith JC. Nurses’ utilization of parent questionnaires for developmental screening. Pediatr Nurs. 2006;32(5):409–412. 452–454
Weinberger M, Hiner SL, Tierney WM. In support of Hassles as a measure of stress in predicting health outcomes. J Behav Med. 1987;10(1):19–31.
Woolf SH, Jonas S, Lawrence RS. Health promotion and disease prevention in clinical practice. Baltimore: Williams & Wilkins, 1996.
Worried parents can refer to child development factsheet. Infant. 2006;2(4):160.
Worsham NL, Crawford EK. Parental illness and adolescent development. Prev Res. 2005;12(4):3–6.
Zehle K, et al. ‘It’s not an issue at the moment’: a qualitative study of mothers about childhood obesity. Am J Matern Child Nurs. 2007;32(1):36–41.