Manual Therapy in the Management of Upper Extremity Musculoskeletal Disorders

▪ There has been tremendous growth and maturation in manual therapy practice over the past two decades.
▪ Efficacy has been demonstrated for the use of manual therapy in the management of upper extremity. musculoskeletal disorders, but the current best evidence is of moderate methodologic quality.
▪ Despite this growth, there is still much that is unknown, particularly related to the selection of manual therapy techniques.
▪ No formal evidence-based guidelines are available to aid in selection.
▪ Strong clinical reasoning skills are required to make the best evidence-informed selection. Consider the “wise action” approach.
▪ Maitland’s description of technique as the brainchild of ingenuity remains clinically relevant.
In 1992, in describing the growth and maturation of manual therapy since his introduction to this area of practice, Rothstein1 commented, “Much time has passed, and although a lot has changed, little has changed.” He noted that although this approach to the management of musculoskeletal disorders had become mainstream and a part of every physical therapy curriculum, there had been little maturation and scientific development in this area. He pointed to the lack of research published in credible, peer-reviewed journals, with the foundation of this practice based primarily on anecdotal observations and the opinions of experts of varying credentials. In some respects, a similar statement could be made regarding the current state of manual therapy practice. Much has changed and inarguably for the better. Our knowledge base has expanded considerably. An overwhelming amount of primary research has been published pertaining to areas such as the mechanical effects, efficacy, and mechanisms of manual therapy. This is evident in the number of recently published systematic and critical reviews.2-6 However, despite this growth, gaps in knowledge still exist with regard to the practical application of manual therapy techniques. The available evidence offers limited guidance in the selection of technique, direction of movement, vigor, dosage, and progression for any particular upper extremity musculoskeletal disorder. Consistent with Rothstein’s earlier observations, techniques are often selected based on anatomic and biomechanical assumptions and on the presumed benefit of the technique.
The intent of this chapter is to provide a brief review of the proposed mechanisms of manual therapy, review the currently available evidence as it relates to the efficacy of manual therapy in the management of upper extremity musculoskeletal disorders, and discuss the principles and reasoning processes relevant to the selection of a technique. Although it is recognized that manual therapy encompasses a disciplined clinical reasoning approach to the examination and management of musculoskeletal disorders, for the purpose of this chapter, the term is used in reference to joint-based passive movement techniques that are commonly used for the purposes of decreasing pain and improving joint range of motion. Neurodynamic and soft tissue–based techniques are not discussed because they are covered elsewhere in this volume.
It has been reported that manual therapy likely works through both biomechanical and neurophysiologic mechanisms and that the potential interaction of the two has been often overlooked. A model has been proposed suggesting that a mechanical stimulus initiates a number of potential neurophysiologic responses that produce the clinical outcomes associated with manual therapy. The parameters of the mechanical stimulus may produce unique neurophysiologic responses at the peripheral, spinal, and supraspinal levels, resulting in decreased pain, improvement in motion, and functional outcomes (Fig. 120-1). As stated by the authors, this comprehensive model accounts for the complex interactions of the peripheral and central nervous systems, which compose the pain experience, and is intended to help guide future research in this area as well as allow clinicians to visualize the potential mechanisms involved in the clinical effects of manual therapy.2
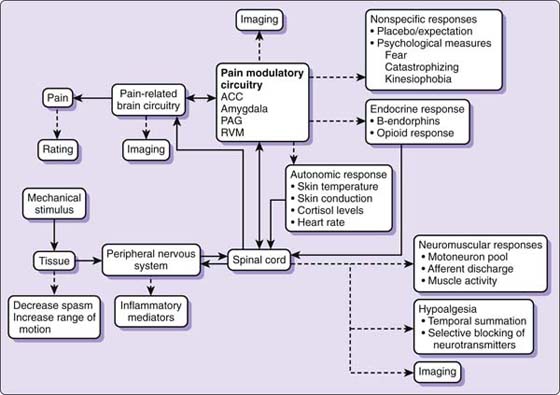
Figure 120-1 Mechanisms of manual therapy comprehensive model. ACC, anterior cingular cortex; PAG, periaqueductal gray; RVM, rostral ventromedial medulla. (From Bialosky JE, Bishop MD, Price DD, et al. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14:531–538.)
The clinical relevance of this model is highlighted when considering the proposed mechanical effects of manual therapy on the joint and periarticular connective tissues. Often purported to exert an effect by means of joint repositioning,7 the evidence suggests that any change in joint position is most likely transient and therefore unlikely to result in a lasting therapeutic outcome. With respect to the ability of manual therapy to affect connective tissue, or more specifically to elongate shortened tissue, one has to consider the nature of this type of problem and the effects of tensile stress on connective tissue. This is described in detail in other chapters and is not reviewed here (see Chapters 122, 124 and 125). As with joint repositioning, any effects are most likely to be transient with increases in motion or tissue length related to the viscoelastic properties of the connective tissue.8 It has been recommended that when true joint stiffness secondary to shortening of periarticular joint structures is the limiting factor in loss of motion, other treatment methods such as orthotic intervention may be more beneficial than passive joint mobilization. However, manual therapy may be of value in preconditioning the tissues before active exercise or orthotic intervention and allow for a greater therapeutic benefit than either alone.
Reporting on the efficacy of manual therapy, DiFabio9 stated that there was a paucity of valid research in all areas and a particular absence of controlled trials involving manual therapy applied to the peripheral joints. Recently, numerous studies of variable quality and design have been published related to the use and effect of manual therapy techniques in the management of select upper extremity musculoskeletal disorders. The majority of the published work has been related to the management of specific shoulder and elbow disorders with several systematic and critical reviews now available.3-5 In a recent search, no systematic reviews could be found pertaining to the use of joint-based manual therapy specifically at the wrist or hand. However, one systematic review of therapy interventions for improving joint motion included two case series involving the use of manual therapy in the management of distal radius fractures and one prospective cohort study investigating its use for stiffness and pain after immobilization for metacarpal fracture.10 The authors concluded that there was evidence to support the use of mobilization to increase range of motion after metacarpal fracture, but the results were inconclusive with respect to management of the distal radius fractures. A limited number of studies have been published that have investigated the use of joint mobilization in the management of carpal tunnel syndrome and mobilization with movement for de Quervain’s tenosynovitis. No definitive conclusions can be drawn in terms of efficacy because these studies are of low to moderate quality.11-13
A review of physiotherapy interventions for shoulder pain found that combining mobilization with exercise resulted in additional benefit compared with exercise alone for rotator cuff disease, but not for adhesive capsulitis.14 The authors concluded that the overall results of their review provided little evidence to guide treatment parameters.
Another systematic review found inconsistent evidence of the effectiveness of manual therapy for various shoulder disorders compared with control interventions and no treatment.4 Fourteen randomized, controlled trials (RCTs) meeting the inclusion criteria of the review were analyzed within subgroups of adhesive capsulitis, shoulder impingement syndrome, and nonspecific shoulder pain. The authors concluded that there was no clear evidence to suggest additional benefits of manual therapy over other interventions in the management of shoulder impingement syndrome and that manual therapy was not shown to be more effective than other conservative interventions for adhesive capsulitis. They noted that the lack of clear description of techniques and treatment parameters as well as the wide range of manual therapy made it difficult to provide clear guidelines for the clinician, but acknowledged that high-grade mobilizations may be more effective in improving range of motion compared with low-grade mobilizations. They also acknowledged the contrasting view of an earlier published review regarding treatment efficacy for impingement syndrome that concluded the evidence of the addition of joint mobilization is moderately strong.15,16
Camarinos and Marinko3 concluded in their review that the evidence suggests that the patients receiving manual therapy interventions for painful shoulder conditions, particularly high-grade/end-range mobilization, demonstrated improvements in both active and passive range of motion. No definitive conclusions could be made with regard to the efficacy of treating pain. Common to the previous reviews, it was stated that the optimal form of manual therapy technique could not be identified.
Similarly, the consensus regarding the effectiveness of manual therapy in the management of tennis elbow appears to be that there is limited high-quality evidence available to guide the clinician in the selection of a particular method.17,18 Herd and Meserve5 reported that in terms of specific techniques, Mulligan’s mobilization with movement (MWM) was the most frequently studied and was shown to provide benefits such as decreased pain immediately and during short-term and long-term follow-up. They cautioned that the generalizability of the studies was limited due to the design and outcome measures used. Consistent with this view are the findings of a systematic review of MWM for all peripheral joints.19 The authors’ stated purpose was to undertake a systematic review to critically evaluate the literature regarding the overall efficacy of MWM prescription and use at peripheral joints in an attempt to formulate guidelines for clinical practice. They identified 25 studies that met their inclusion criteria with 4 being true RCTs, 6 RCTs with participants as their own control, and the remainder divided among non-experimental designs, case studies, and case reports. Each article was assessed for methodological quality using a valid and reliable critical appraisal tool with the RCTs deemed to be of moderate methodological quality. Three of the 4 true RCTs were related to tennis elbow and 1 to the shoulder. In the 6 RCTs in which the participants were their own control, 3 were related to tennis elbow, 2 to the ankle, and 1 to the shoulder. It was concluded that, in general, the efficacy of MWM was well established with common effects including increases in strength, reduction in pain, increases in pain pressure thresholds, and improved function. However, due to the methodological quality of the studies the authors were unable to provide any specific guidelines for clinical practice.
Several randomized clinical trials of higher quality have been published demonstrating the efficacy of manual therapy in the management of painful shoulder and elbow conditions. Review of the techniques used in these trials may provide some guidance in the selection of technique process.
Yang and colleagues20 compared the use of three mobilization techniques in the management of subjects with frozen shoulder syndrome. Inclusion criteria were having a painful stiff shoulder for at least 3 months, having limited range of motion of 25% or greater compared with the noninvolved shoulder in at least two shoulder motions, and having physician consent. The techniques that were compared were described as midrange mobilization, end-range mobilization, and MWM. A multiple treatment trial design was used over a 12-week period. Improvement in mobility and functional ability was reported in all subjects. Comparing the effectiveness of the three techniques, end-range mobilization and MWM were found to be more effective than midrange mobilization. MWM was also found to improve movement strategies in terms of scapulohumeral rhythm.
Johnson and colleagues21 compared the effectiveness of anterior and posterior glide mobilization techniques for improving shoulder external rotation range of motion in patients with adhesive capsulitis. Inclusion criteria included a diagnosis of primary or idiopathic adhesive capsulitis, unilateral condition, age between 25 and 80 years, normal findings on radiographs within the previous 12 months, no previous shoulder surgery, no previous manipulation under anesthesia, and external rotation range of motion that worsened with shoulder abduction. All subjects received six therapy sessions consisting of ultrasound, joint mobilization, and upper body ergometer exercise. Treatment differed between groups in the direction of the mobilization technique performed. No significant difference in shoulder external rotation range of motion between groups was noted at baseline. By the third treatment, individuals in the anterior mobilization group had a mean improvement in external rotation of 3 degrees. The individuals in the posterior mobilization group had a mean improvement of 31.3 degrees. Both groups were reported to have a significant decrease in pain.
Also investigating the effects of joint mobilization on range of motion and disability in patients with stiff and painful shoulders, Vermeulen and colleagues22 compared the use of high-grade and low-grade mobilization techniques in the management of phase II (freezing) adhesive capsulitis. The mobilization techniques included inferior glide of the head of the humerus, inferior glide in abduction/external rotation, posterior glide, anterior glide, and lateral distraction of the humerus. The high-grade group received grade III or IV mobilization, whereas the low-grade group received the same techniques as grade I or II. (See discussion of grades of movement.) Improvement was demonstrated in joint mobility and reduction of disability in both groups. Statistically significant improvement in passive abduction and active and passive external rotation was reported in the high-grade group. The authors concluded that high-grade mobilization techniques appear to be more effective in improving glenohumeral joint mobility and reducing disability than low-grade mobilization, with the overall difference between the two interventions being small. Because there was no control group not receiving mobilization, the natural history of the disorder must be considered when interpreting these results (see Chapter 89 and 90).
Teys and colleagues23 investigated the effects of a MWM technique on range of motion and pressure pain threshold in individuals with limited and painful shoulder motion. Twenty-four participants meeting the inclusion criteria of inability to elevate the arm more than 100 degrees in the plane of the scapula because of the presence of anterior shoulder pain and duration of pain longer than 1 month and for less than 1 year received treatment consisting of either a MWM technique or a sham technique. A control condition was also included in which the participant was seated, but without any manual contact between the therapist and participant. The MWM technique consisted of the application of a posterolateral glide to the affected shoulder. The authors reported significant and clinically meaningful improvements in both range of motion and pressure pain threshold immediately after treatment in the MWM group. No follow-up was reported.
Last, Bisset and colleagues24 investigated the efficacy of MWM and exercise compared with corticosteroid injection or a wait-and-see approach over 1 year in patients diagnosed with tennis elbow. Physical therapy consisting of MWM and exercise was demonstrated to have a superior benefit over the wait-and-see approach in the first 6 weeks and over corticosteroid injection after 6 weeks with outcome measures of global rating of change, pain-free grip, and assessor’s rating of severity. The MWM techniques included sustained lateral glide with pain-free grip and sustained lateral glide of the elbow with movement.25
Again, although the preceding may provide some guidance in the selection of a manual therapy technique, the generalizability is limited to the diagnoses and conditions studied. When presented with a patient not fitting these criteria, sound clinical reasoning is paramount in the decision-making process and is highlighted in the following discussion.
The selection of a manual therapy technique for any particular peripheral joint disorder is often based on the therapist’s personal preferences, biases, and previous experiences with that technique along with a consideration of the problem being addressed. Pathoanatomic, biomechanical, and neurophysiologic principles are also influencing factors. As evident, despite the growth and maturation of manual therapy practice, standardized, evidenced-based guidelines remain unavailable to assist in this decision-making process. Limited evidence is available of specific joints and diagnoses that may aid in technique selection; however, whether this can be applied to other joints and conditions is unknown. Principles that have long guided clinicians and remain popular have been questioned in terms of their validity and efficacy, with the findings often contradictory to the stated principle.8,26 A classic example is that the concave–convex rule, which describes a method to determine the direction of a glide, is not always correct. To increase glenohumeral external rotation, the concave–convex rule says to apply an anterior glide; however, a recent study demonstrated that greater improvement in external rotation was achieved with a posterior glide.21
The difficulty in developing standardized guidelines is multifactorial, but at least in part is due to the variability often seen in the clinical presentation of individuals referred with the same diagnosis. It is not uncommon for one person to respond favorably to a particular technique while another does not. Exploring the reasons for this is beyond the scope of this chapter, but this clinical dilemma highlights the value of a patient-centered, disciplined clinical reasoning approach when deciding which technique(s) to choose. This approach or treatment paradigm has been described in great detail elsewhere with the essence best captured by the term wise action approach.27,28 When using the approach, a wise action is chosen with consideration to the best of science, the best of current therapies, and the best of the patient/therapist relationship. As evident, this is consistent with the description of evidence-based/informed practice. The following reviews the principles and processes involved in the selection of a technique that are thought to be important in allowing the clinician to arrive at this wise action. These principles have been described thoroughly by Hengeveld and Banks29,30 and are components of what has been referred to as the Maitland/Australian approach.
After a thorough examination in which an assessment is made of the nature of the patient’s movement-related disorder, the therapist will then decide whether treatment by passive movement is indicated and appropriate. Conditions that may preclude this type of treatment include those with an active underlying disease process, unstable fractures, severe osteoporosis, long-term steroid or anticoagulant use, surgical procedures in which the tissue must be protected, or a condition in which a strong psychosocial component is suspected. Although this list can go on, the decision is ultimately made by applying the wise action principle.
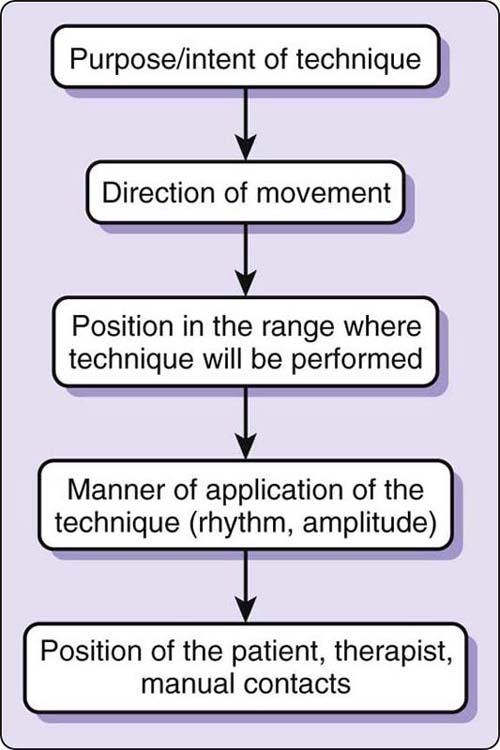
Once it is determined that the patient and his or her condition are appropriate for treatment by passive movement, one must then consider the purpose or intent of the technique. The answer to this question is fairly generic at this point and may include stretching a tight or shortened tissue to relieve pain or to impart a controlled degree of stress on the tissue or joint. Next, the direction of movement should be determined, with the intent of the technique, anatomic and biomechanical considerations, and previous experience being some of the factors influencing this decision. With the intent of the technique and direction of movement selected, consideration is then given to where in the joint available range of motion the technique will be applied and the manner of application. Possibilities include the beginning of range, midrange, end range, or through range, with the manner of application referring to the amplitude and rhythm of the movement.
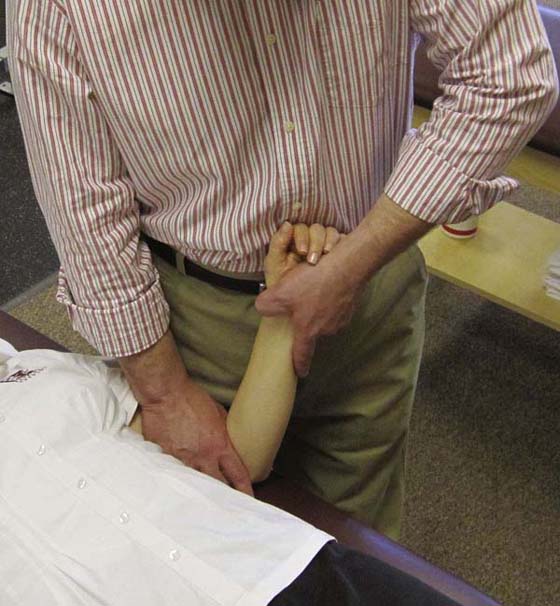
These decisions are also influenced largely by the intent of the technique, pathoanatomic and pathobiologic considerations, and the type of disorder. The type of disorder is a phrase that is used to refer to the reason the patient is seeking treatment. This could be pain, stiffness, weakness, “giving way,” etc. Once these determinations are made, the position of the patient, the position of the therapist, and the manual contacts that will best allow the technique to be performed are considered. The patient’s position should be one in which he or she is comfortable and relaxed and that allows easy access to the joint being treated. The therapist’s starting position should be one that allows complete control of the movement and allows forces to be applied in the direction intended and is comfortable and easy to maintain. In general, manual contacts should be as broad as possible for the technique in use to distribute the force over a larger contact area. This should allow better patient comfort as well as therapist control of the movement. When possible, the passive movement should be accomplished by movement of the body or arms of the therapist and not by pushing with the fingertips or hands (Fig. 120-2).
Grades of movement are used to denote the position in the available range where the technique is performed and the amplitude of the movement. They are best thought of as a guide to facilitate communication between the therapist and the exact points in the range.31 They also may allow the therapist to think in finer detail about the technique and enhance acquisition of the skill. Grades I through V have been described and are often depicted on a movement diagram (Box 120-1). Grade I is a small-amplitude movement performed at the beginning of the available range. Grade II is a large-amplitude movement performed in the resistance-free part of the range. Grade III is a large-amplitude movement performed into resistance or up to the limit of the available range. Grade IV is a small-amplitude movement performed into resistance or up to the limit of the available range. Grade V is small amplitude, high-velocity thrust performed usually, but not always, at the end of the available range. Pluses and minuses are often used, particularly with grades III and IV, to give further detail related to the vigor of the technique. For example, grade V would be performed at that part in the range where resistance to movement is first perceived, whereas grade V+ would be a more vigorous technique taken further into the resistance portion of the range. The concept of grades of movement can be applied to both passive accessory motion (glide) and passive physiologic motion. Again, it is important to emphasize that the clinical utility of grades of movement is that they provide a simple means of communicating aspects of the technique (where in the range the technique is performed, the amplitude of the movement, and the vigor or strength used) that would otherwise require lengthy descriptions.
Box 120-1 Grades of Movement
Small-amplitude movement performed at the beginning of the available range |
|
Grade II |
Large-amplitude movement performed in the resistance-free part of the range |
Grade III* |
Large-amplitude movement performed into resistance or up to the limit of the available range |
Grade IV* |
Small-amplitude movement performed into resistance or up to the limit of the available range |
Grade V |
Small-amplitude, high-velocity thrust performed usually, but not always, at the end of the available range |
* Pluses and minuses may be used with grades III and IV to give further detail related to the vigor of the technique.
Numerous options are available when considering the type of movement to be used and the method of application. Treatment by passive movement can include the use of physiologic motions, accessory motions, or any combination of the two (Fig. 120-3). For example, if the purpose/intent of a technique is to improve external rotation at the shoulder, the choices could include external rotation, anterior or posterior glide, a combined motion of anterior glide and external rotation, or even the combined physiologic motions of external rotation and abduction. Further decisions to be made would include where in the range to perform the technique, i.e., the grade of movement, the strength of the technique, and the rhythm in which the technique is performed (Fig. 120-4).
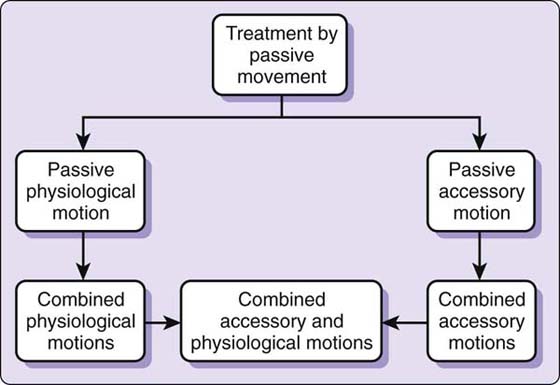
Figure 120-3 Passive movement options for manual joint-based techniques. (Modified from Hengeveld E, Banks K. Principles of selection and progression of mobilization/manipulation techniques. In: Hengeveld E, Banks K, eds. Maitland’s Peripheral Manipulation, 4th ed. Edinburgh: Elsevier Butterworth Heinemann, 2005, p. 187.)
Figure 120-4 Rhythm of movement options for manual joint-based techniques. (Modified from Hengeveld E, Banks K. Principles of selection and progression of mobilization/manipulation techniques. In: Hengeveld E, Banks K, eds. Maitland’s Peripheral Manipulation, 4th ed. Edinburgh: Elsevier Butterworth Heinemann, 2005, p. 185.)
This decision-making process is aided by the use of the wise action approach. When considering the best of science, questions to ask could be the following. (1) Is there any evidence available to support one particular technique or movement over the other? (2) Based on anatomy, what tissues could be limiting motion and what is the best position to stretch them? (3) Considering the pain sciences and proposed mechanisms of manual therapy, what is the dominant pain mechanism and would one type of movement be more appropriate than another? Reflection on the best of current therapies may lead you to question whether one particular approach, such as Mulligan’s MWM, would be more appropriate and whether there is evidence to support this.
Last, when considering the best of the patient/client interaction, attention is focused on the clinical presentation and the assessments made after the patient interview and physical examination. These assessments, which have been referred to as hypothesis categories, can include the patient’s perspective on his or her experience, activity capabilities and restrictions, the pathobiological mechanisms of the disorder, contributing factors to the development and maintenance of the problem, contraindications to and precautions of treatment, and prognosis. Taken collectively, this allows an assessment of what Maitland referred to as the SINS of the problem.
SINS is an acronym for the severity, irritability, nature, and stage of the disorder. Severity encompasses not only the amount or intensity of a symptom, often assessed by means of a numerical pain rating, but also the degree to which the problem is restricting participation in activities relevant to the individual. Irritability is a construct that is used to describe the amount of activity required to bring the symptoms on, the amount of the symptom brought on, and how long it takes to settle. Nature refers to many aspects of the disorder, including the pathobiological mechanisms, psychosocial factors, and the medical diagnosis. Stage can refer to how acute or chronic the problem is, but perhaps more important, the stability of the disorder.
Thinking about the clinical presentation in such great detail can enhance the development of clinical reasoning strategies and promote pattern recognition skills. Thinking in a global sense, four distinct clinical patterns have been described along with empirically based guidelines for the selection and progression of passive movement techniques for each. The four patterns include a pain-dominant group, a stiffness-dominant group, a group with components of both pain and stiffness, and a group in which momentary pain is the dominant feature (Fig. 120-5).
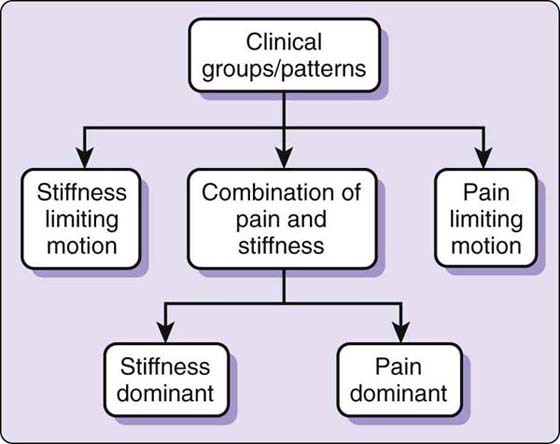
Figure 120-5 Clinical presentation groups. (Modified from Hengeveld E, Banks K. Principles of selection and progression of mobilization/manipulation techniques. In: Hengeveld E, Banks K, eds. Maitland’s Peripheral Manipulation, 4th ed. Edinburgh: Elsevier Butterworth Heinemann, 2005.)
In the pain group, as implied, the limitation of movement is due to pain. Stiffness cannot be assessed because pain is provoked easily and often early in the range. Pain at rest is common. If it were not for the pain, the joint may well have full range of motion. These are typically highly irritable disorders, with little activity provoking much pain that takes a long time to settle. Pathobiological mechanisms may include inflammation, peripheral sensitization with primary hyperalgesia, and centrally induced secondary hyperalgesia. The pain experience may be heightened by fear and anxiety associated with movement. Careful positioning is required with attention to finding a pain-easing position in which to perform the technique. It is also important that the joint is well supported and the manual contacts are comfortable. The patient should feel confident that the therapist will not move the joint into the painful part of the range. This can be accomplished by using the body to block motion, especially when performing passive physiologic techniques.
Often, the first choice of movement is an accessory motion performed early in the range, of small amplitude, and in a smooth, slow rhythm (Fig. 120-6). As the pain eases, the amplitude of the movement can be increased with the goal being to move through as large a range as possible with the least amount of pain. Treatment can be progressed to include passive physiologic motions following the same principles. As pain eases and stiffness is encountered, small-amplitude movements just to the point of resistance can be used to provoke a controlled degree of pain. Assessment is made while performing the technique, after the technique is applied, and on follow-up at the next treatment session. If no exacerbation is experienced, the vigor and duration of the technique can be progressed.
In the stiffness group, pain is minimal and often reported only when the stiff joint is stretched vigorously. The pain eases quickly when the stretch is released and no latent pain is experienced. Patients commonly seek treatment due to difficulty performing normal daily activities because of the loss of motion, but not pain. For example, a person with a stiff elbow lacking flexion may report difficulty fastening the top button of a shirt or bringing a glass to his or her mouth. Initial treatment can include the physiologic motion that is stiff (in this case, flexion) performed in the resistance portion of the range as a small-amplitude movement or an accessory motion performed at the limit of the stiff physiologic movement (Fig. 120-7).
As best stated by McClure and Flowers,8 when limited range of motion is thought to be due to a structural change in the periarticular tissues, the therapist should consider which structures could potentially limit that range of motion. Selection of a stretching technique should then be based on what type of maneuver will best put tension on the restricting tissue. The vigor of the technique can gradually be increased with each bout of mobilization typically lasting 1 to 2 minutes. A typical routine would include using the passive physiologic motion first, followed by the accessory motion at the limit of the physiologic range, and repeating this sequence three to four times. This can provoke a degree of treatment soreness that is often eased by performing the passive physiologic motion as a large-amplitude, through-range movement but not to the same degree of stretching.
Treatment can be progressed by performing combined physiologic and accessory motions synchronously or combining two physiologic motions performed in a synchronous manner. An example would be performing external rotation with forward elevation of the shoulder (Fig. 120-8). This could also be combined with an inferior glide of the head of the humerus so that two physiologic motions and one accessory motion are performed together. The patient could be supine or side-lying. When treating the stiff joint, other options such as orthotic intervention should be kept in mind with manual therapy as an adjunctive or complementary treatment for preconditioning and pain modulation.

Figure 120-8 Grade III or IV combined physiologic external rotation and flexion into resistance of available motion of the shoulder.
Most patients seeking treatment for musculoskeletal disorders of the upper extremity present with both pain and stiffness components to their problem. Determining which component is dominant can be quite a challenge, requiring greater attention to detail in the patient interview and physical examination. When pain is the greater component, guidelines similar to those for the pain group should be followed until the response to treatment, as related to the behavior of the pain, is known. Then treatment can be directed toward the stiffness component with greater confidence and less risk of exacerbation. When stiffness is the dominant component, treatment is similar to that for the stiffness group but with greater respect to the pain. Passive accessory motion can be performed in the position of the limited physiologic motion, but not quite as far into the range.
A challenging, but often rewarding, group to treat consists of those who present with momentary pain. Frequently described as catches, twinges, or jabs of pain, the individual will state that the pain only comes on with certain movements, but has difficulty identifying the painful movements. A movement may provoke the pain in an inconsistent manner. The challenge of the physical examination is to identify the offending movement, which is then often the direction first used as the treatment. A controlled degree of the familiar pain is then provoked by use of small-amplitude, end-range movements, usually an accessory motion or combined physiologic movement such as the shoulder quadrant position (Fig. 120-9). The rhythm of the movement can be a bit quicker or even staccato like. Any treatment soreness is usually eased by larger-amplitude, through-range maneuvers. Disorders of this type can be handled quite firmly, particularly when pathology such as instability or an intra-articular lesion has already been ruled out. They tend to be nonsevere, nonirritable, and very stable with minimal activity/participation restriction, involving pain that comes on quickly but can ease just as fast, and with the history revealing little to no change noted over time. The response to treatment can be fairly quick, with improvement in four to six sessions. Problems of this nature can often be underexamined and undertreated, with the value of treatment by passive movement not realized.
There are many other considerations that are relevant to the selection of the technique decision-making process that include the particular joint being treated, the medical diagnosis, the source of the symptoms, and the history and onset of the disorder, to name a few. It is beyond the scope of this chapter to review all these factors, and the reader is referred elsewhere for a detailed discussion.29,30 The intent of the preceding was to provide an introduction to this process, review general guidelines from one particular approach, and provoke thought, not only about the selection of a technique but also the detail required of the reasoning behind the selection.
Before concluding, a brief discussion of Mulligan’s MWM treatment approach is warranted because these techniques have gained popularity in both the clinical realm and research agenda. Introduced by Brian R. Mulligan, a physiotherapist from New Zealand, this approach has been summarized as follows:
MWM is a manual therapy treatment technique in which a manual force, usually in the form of a joint glide, is applied to a motion segment and sustained while a previously impaired action is performed. The technique is indicated if, during its application, the technique enables the impaired joint to move freely without pain or impediment. The direction of the applied force (translation or rotation) is typically perpendicular to the plane of movement or impaired action and in some instances it is parallel to the treatment plane.6
The proposed mechanism for the clinical efficacy of MWM is based on a mechanical model that proposes that minor positional faults occur after injury or strain, resulting in movement restrictions and/or pain. The MWM technique, or correctional mobilization, is thought to restore pain-free function by means of repositioning.7 The positional fault theory was challenged in a critical review of the literature published up until 2003 in which the authors concluded that there was no substantive evidence that supported or refuted the hypothesis that a reversal of a positional fault was the predominant mechanism of action for MWM.6 Although there has been some evidence of positional change after application of the technique, this was transient and could not account for any lasting benefit attributed to the technique. An alternative hypothesis was considered based on the hypoalgesic effect noted when an MWM technique was applied for tennis elbow. It was proposed that the combination of sympathoexcitation nonopioid hypoalgesia and improvement in motor function (pain-free grip strength) was an indirect sign of a possible involvement of endogenous pain-inhibition systems.6 This mirrors the model discussed earlier, proposing that the outcomes associated with manual therapy most likely result from the interaction of complex inhibitory mechanisms at the peripheral, spinal cord, and supraspinal levels.2 The clinical efficacy of the MWM has been demonstrated for a few select musculoskeletal disorders, as previously noted. Although there have been several RCTs investigating the effects, the level of evidence has been assessed to be of low to moderate quality. Like other manual therapy techniques and approaches, further research has been recommended to validate the proposed mechanisms and effectiveness of MWM. Continued use of MWM in clinical practice is advocated when used in the context of sound clinical reasoning strategies and can be thought of as another option falling under the category of a combined accessory glide with active or resisted physiologic motion technique.
Over the past two decades, manual therapy has grown, not only in popular acceptance, but also, through critical appraisal, it has been endorsed as a valuable component in the conservative management of musculoskeletal disorders. Curriculum development for manual therapy education is now guided by a set of standards developed through the collaborative effort of academic educators, researchers, and clinicians with expertise in this area.32 The growth of residency and fellowship training has been tremendous, with 28 orthopedic physical therapy residency programs and 20 orthopedic manual and manipulative therapy fellowship programs now credentialed by the American Physical Therapy Association.33 The credentialing process is stringent, requiring the submission of a valid practice analysis and a standardized curriculum consistent with evidence-based principles. A national organization now exists to promote research in orthopedic manual therapy and foster the principles of evidence-based practice within its membership.34 This organization is credited with the development of the Manual Therapy Description of Advanced Specialist Practice, which serves as criteria for residency and fellowship credentialing.35 Within the past 10 years, clinical prediction rules have been developed and validated related to the use of manipulative techniques in the treatment of spinal disorders.
Although we know more than ever, there is still much that is unknown related to this practice area. The degree of uncertainty that exists surrounding the selection of the best technique or set of techniques for a particular disorder remains best managed by adopting sound clinical reasoning strategies and applying the wise action principles. On a final note regarding the selection of a technique, it is advantageous to keep in mind the wisdom and insight provided by Geoffrey Maitland. Recognizing that no single technique can be ideal and appropriate for all patients and therapists alike, he described technique as the brainchild of ingenuity.29 Although a standardized description of a base set of techniques is required and necessary for teaching purposes and the acquisition of skill, adaptation is encouraged to deal with the variability encountered with respect to patient size, therapist size, and the clinical presentation at hand. This also allows the development of new techniques as new evidence and knowledge emerge.
1. Rothstein JM. Manual therapy: a special issue and a special topic. Phys Ther. 1992;72:839–841.
2. Bialosky JE, Bishop MD, Price DD, et al. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Man Ther. 2009;14:531–538.
3. Camarinos J, Marinko L. Effectiveness of manual physical therapy for painful shoulder conditions: a systematic review. J Man Manip Ther. 2009;17:206–215.
4. Ho CY, Sole G, Munn J. The effectiveness of manual therapy in the management of musculoskeletal disorders of the shoulder: a systematic review. Man Ther. 2009;14:463–474.
5. Herd CR, Meserve BB. A systematic review of the effectiveness of manipulative therapy in treating lateral epicondylalgia. J Manip Ther. 2008;16:225–237.
6. Vicenzino B, Paungmali A, Teys P. Mulligan’s mobilization-with-movement, positional faults and pain relief: current concepts from a critical review of literature. Man Ther. 2007;12:98–108.
7. Mulligan BR. Manual Therapy: “NAGS, “SNAGS,” MWMS” etc. 5th ed Wellington: Plane View Services Ltd; 2004.
8. McClure PW, Flowers KR. Treatment of limited shoulder motion: a case study based on biomechanical considerations. Phys Ther. 1992;72:929–936.
9. DiFabio RP. Efficacy of manual therapy. Phys Ther. 1992;72:853–864.
10. Michlovitz SL, Harris BA, Watkins MP. Therapy interventions for improving joint range of motion: a systematic review. J Hand Ther. 2004;17:118–131.
11. Coyle JA, Robertson VJ. Comparison of two passive mobilizing techniques following Colles’ fracture: a multi-element design. Man Ther. 1998;3:34–41.
12. Tal-Akabi A, Rushton A. An investigation to compare the effectiveness of carpal bone mobilisation and neurodynamic mobilisation as methods of treatment for carpal tunnel syndrome. Man Ther. 2000;5:214–222.
13. Handoll HH, Madhok R, Howe TE. Rehabilitation for distal radial fractures in adults. Cochrane Database Syst Rev. 2002;(2):D003324. Review. Update in: Cochrane Database Syst Rev. 2006;3:CD003324.
14. Green S, Buchbinder R, Hetrick S. Physiotherapy interventions for shoulder pain. Cochrane Database Syst Rev. 2003;(2):D004258.
15. Michener LA, Walsworth MK, Burnet EN. Effectiveness of rehabilitation for patients with subacromial impingement syndrome: a systematic review. J Hand Ther. 2004;17:152–164.
16. Desmeules F, Côté CH, Frémont P. Therapeutic exercise and orthopedic manual therapy for impingement syndrome: a systematic review. Clin J Sport Med. 2003;13:176–182.
17. Bisset L, Paungmali A, Vicenzino B, Beller E. A systematic review and meta-analysis of clinical trials on physical interventions for lateral epicondylalgia. Br J Sports Med. 2005;39:411–422.
18. Vicenzino B, Cleland JA, Bisset L. Joint manipulation in the management of lateral epicondylalgia: a clinical commentary. J Man Manip Ther. 2007;15:50–56.
19. Hing W, Bigelow R, Bremner T. Mulligan’s mobilization with movement: a systematic review. J Man Manip Ther. 2009;17:E39–E66.
20. Yang JL, Chang CW, Chen SY, et al. Mobilization techniques in subjects with frozen shoulder syndrome: randomized multiple-treatment trial. Phys Ther. 2007;87:1307–1315.
21. Johnson AJ, Godges JJ, Zimmerman GJ, et al. The effect of anterior versus posterior glide joint mobilization on external rotation range of motion in patients with shoulder adhesive capsulitis. J Orthop Sports Phys Ther. 2007;37:88–99.
22. Vermeulen HM, Rozing PM, Obermann WR, et al. Comparison of high-grade and low-grade mobilization techniques in the management of adhesive capsulitis of the shoulder: randomized controlled trial. Phys Ther. 2006;86:355–368.
23. Teys P, Bisset L, Vicenzino B. The initial effects of a Mulligan’s mobilization with movement technique on range of movement and pressure pain threshold in pain-limited shoulders. Man Ther. 2008;13:37–42.
24. Bisset L, Beller E, Jull G, et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. Br Med J. 2006;333(7575):939.
25. Vicenzino B. Lateral epicondylalgia: a musculoskeletal physiotherapy perspective. Man Ther. 2003;8:66–79.
26. Brandt C, Sole G, Krause MW, Nel M. An evidence-based review on the validity of the Kaltenborn rule as applied to the glenohumeral joint. Man Ther. 2007;12:3–11.
27. Jones MA, Rivett DA. Introduction to clinical reasoning. In: Jones MA, Rivett DA, eds. Clinical Reasoning for Manual Therapists. Edinburgh: Elsevier Butterworth Heinemann; 2004:3–24.
28. Butler DS. Clinicians and their decisions. In: Butler DS, ed. The Sensitive Nervous System. Adelaide: Noigroup Publications; 2000:128–151.
29. Hengeveld E, Banks K. Principles of selection and progression of mobilization/manipulation techniques. In: Hengeveld E, Banks K, eds. Maitland’s Peripheral Manipulation. 4th ed Edinburgh: Elsevier Butterworth Heinemann; 2005:179–236.
30. Hengeveld E, Banks K. Principles and method of mobilization/manipulation techniques. In: Hengeveld E, Banks K, eds. Maitland’s Peripheral Manipulation. 4th ed Edinburgh: Elsevier Butterworth Heinemann; 2005:165–178.
31. Jones MA, Magarey ME. Clinical reasoning in the use of manual therapy techniques for the shoulder girdle. In: Tovin BJ, Greenfield BH, eds. Evaluation and Treatment of the Shoulder: An Integration of the Guide to Physical Therapist Practice. Philadelphia: F.A. Davis; 2001:317–346.
32. Manipulation Education Manual for Physical Therapist Professional Degree Programs 2004. Available at http://www.apta.org/AM/Template.cfm?Section=Top_Issues2&TEMPLATE=/CM/ContentDisplay.cfm&CONTENTID=54914. Accessed December 5, 2009
33. APTA Credentialed Clinical Residency and Fellowship Programs. Available at http://www.apta.org/AM/Template.cfm?Section=Residency&CONTENTID=70296&TEMPLATE=/CM/ContentDisplay.cfm. Accessed December 5, 2009
34. AAOMPT History. Available at http://aaompt.org/about/index.cfm. Accessed December 5, 2009
35. A Description of Advanced Clinical Practice in Orthopaedic Manual Physical Therapy Practice. Available at http://aaompt.org/publications/dasp.cfm. Accessed December 5, 2009