Muscles That Influence the Spine
Second only to the vertebral column and spinal cord, the muscles of the spine are the most important structures of the back. A thorough understanding of the back muscles is fundamental to a comprehensive understanding of the spine and its function. The purpose of this chapter is to discuss the muscles of the back and other muscles that have an indirect influence on the spine. The intercostal muscles provide an example of the latter category. These muscles do not actually attach to the spine, but their action can influence the spine by virtue of their attachment to the ribs. The abdominal wall muscles, diaphragm, hamstrings, and others can be placed into this same category. These muscles have a less direct yet important influence on the spine. Chapter 5 discusses the sternocleidomastoid, scalene, suprahyoid, and infrahyoid muscles.
The musculature of the spine and trunk plays an important role in the normal functioning of the vertebral column. Beside their obvious ability to create the variety of spinal movements, many of these muscles also help to maintain posture. In addition, the back and trunk muscles function as shock absorbers, acting to disperse loads applied to the spine. The shear bulk of these muscles also protects the spine and viscera from outside forces.
Although it is beyond the scope of this text to detail the kinesiology of the muscles influencing the spine, a few generalities are in order. Most muscles have two attachment sites. One is usually more proximal and stable. This has been classically called the origin. The other is usually more distal and mobile, and this has usually been called the insertion. For some muscles, this designation is pretty straightforward, but for others (e.g., the rectus abdominis muscle) it is less easy to identify the more mobile attachment. Therefore, it does not make good biomechanical sense to try to define an “origin” and “insertion” for every muscle.
There is a complicated interplay of many muscles when a motion of the body, especially of the spine, is produced. Sometimes this is termed muscle coordination. Some of the specifics of this complex interplay are only beginning to be understood, especially in asymmetric motions of the trunk (van Dieen, 1996; Danneels et al., 2001; Andersson et al., 2002; Masani et al., 2009; Shin & D’Souza, 2010; Comfort, Pearson, & Mather, 2011). Muscles known as prime movers are the most important. Other muscles, known as synergists, assist the prime movers. For example, the psoas major and rectus abdominis muscles are prime movers of the spine during flexion of the lumbar spine from a supine position, as in the performance of a sit-up. However, the erector spinae muscles also undergo an eccentric contraction toward the end of the sit-up. This contraction of the erector spinae group helps to control the motion of the trunk and allows a graceful, safe accomplishment of the movement. The erector spinae muscles are acting as synergists in this instance.
Besides producing motion, muscle contraction also stabilizes the spine by making it stiffer. This is important not only for maintaining posture (Cholewicki et al., 1997; Quint et al., 1998) but also for providing a stable base for other motions of the body, such as appendicular motions (Lorimer Moseley et al., 2002; Akuthota et al., 2008; Borghuis et al., 2008; Zazulak et al., 2008).
Muscle coordination seems to be under the control of the central nervous system. The central nervous system is constantly receiving afferent information from the muscles and other surrounding tissues, such as ligaments and tendons. On the basis of this information, the central nervous system appears to use reflex pathways to finely control muscle activity. Some of the details of this process are beginning to be understood (Kang et al., 2002; Hultborn, 2006). Interestingly, the specifics of the interplay of the muscles in producing a motion of the body are not always constant. In other words, the same motion may not always be produced by the same muscles working together in the same way. The central nervous system can alter muscle activity depending on the circumstances, such as muscle fatigue, to accomplish the same goal (Clark et al., 2003). This appears to be especially true when there is an abnormality in the system, such as pain or abnormal joint function (McPartland et al., 1997; Hirayama et al., 2001; Lehman et al., 2001; van Dieen et al., 2003; Tsao, Galea, & Hodges, 2008).
The muscles of the spine and other muscles associated with the back can, and frequently do, sustain injury. Other painful conditions of muscles (or fascia) are commonly seen by clinicians besides frank injury or pathology of muscles. For example, fatigue of the back muscles can be a source of pain (e.g., motion-induced intermittent low back pain) (Takahashi et al., 2007). In addition, myofascial trigger points can be a source of pain and are sometimes associated with a condition known as myofascial pain syndrome (Travell & Simons, 1983, 1992; Wheeler, 2004). Another condition is fibromyalgia or fibromyalgia syndrome (Krsnich-Shriwise, 1997; Arnold, 2010). Both of these conditions are not well understood but are being increasingly accepted as true syndromes. They are similar in presentation but are distinct entities (Schneider, 1995). A complete understanding of the anatomy of the muscles associated with the spine aids in the differential diagnosis of pain arising from muscles versus pain arising from neighboring ligaments or other structures.
The back muscles are discussed from superficial to deep. This is accomplished by dividing the muscles into six layers, with layer one the most superficial and layer six the deepest. Other important muscles of the spine are described after a discussion of the six layers of back muscles. These include the suboccipital muscles, small muscles of the spine, anterior and lateral muscles of the cervical spine, and iliac muscles. The muscles that have an indirect yet important influence on the spine are discussed last. The muscles that influence the spine are summarized in Tables 4-1 and 4-2 and Box 4-1 (Table 4-2 and Box 4-1 are found at the end of the chapter).
BOX 4-1 Summary of Actions of Spinal Muscles
Muscles Acting on the Head at the Atlanto-Axial and Atlanto-Occipital Joints
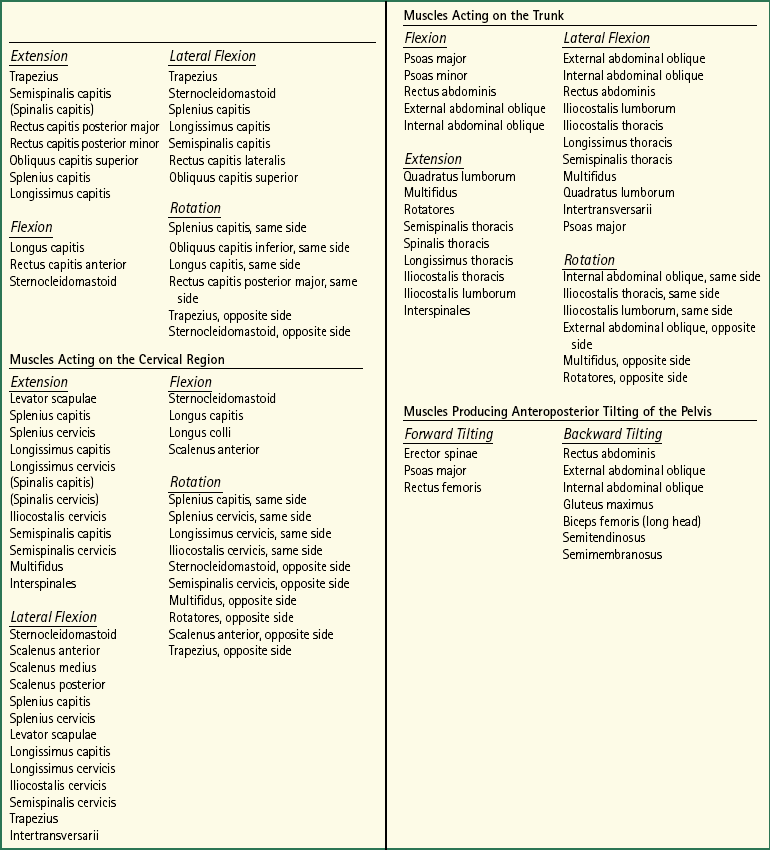
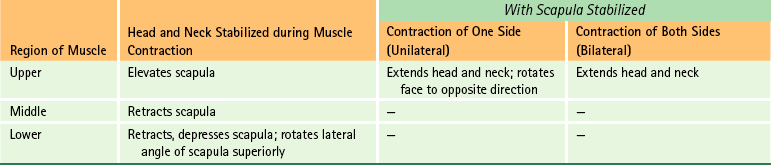
Table 4-2
Summary of Muscles Affecting the Spine1
1See Tables 5-10 through 5-12 for information on the scalene, sternocleidomastoid, and suprahyoid and infrahyoid muscles.
2See text for further details.
Six Layers of Back Muscles
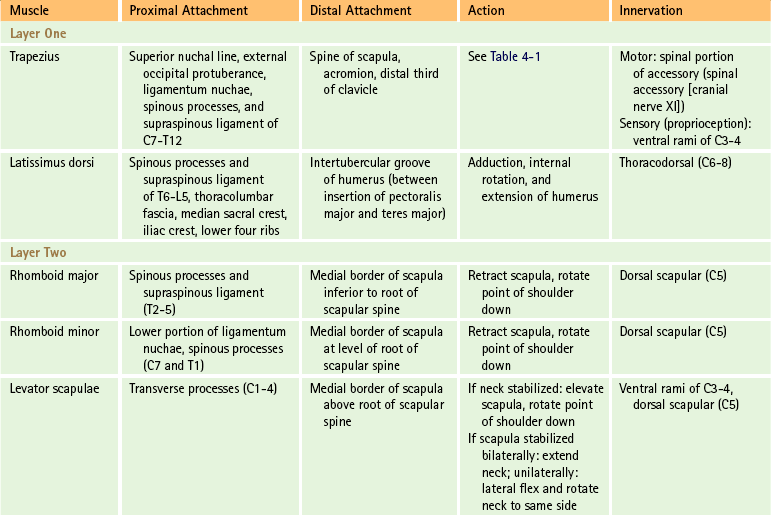
The first layer of back muscles consists of the trapezius and latissimus dorsi muscles (Fig. 4-1). These two muscles course from the spine (and occiput) to either the shoulder girdle (scapula and clavicle) or the humerus, respectively.
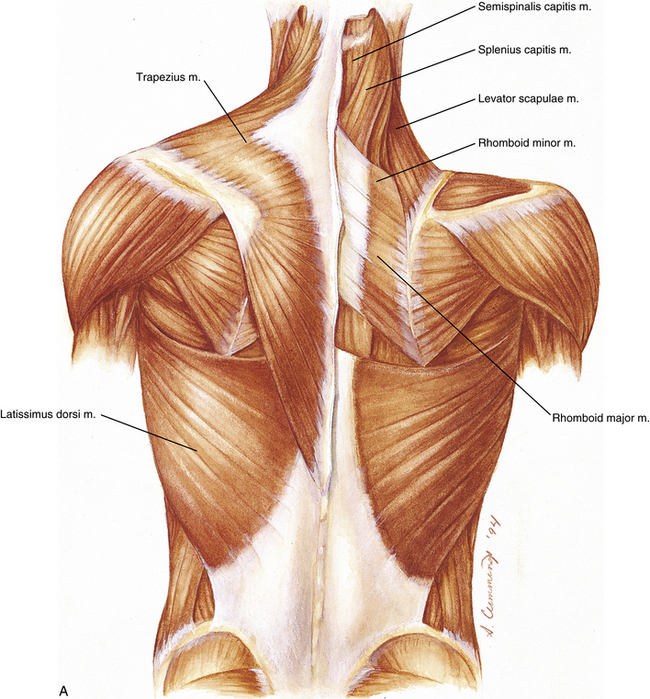

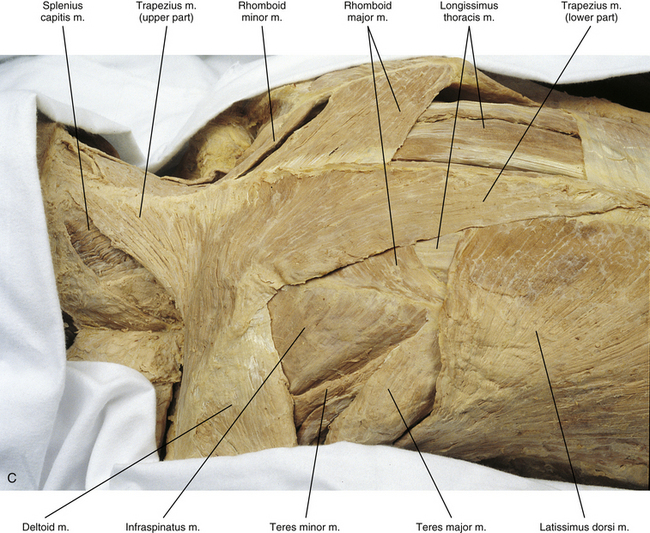
FIG. 4-1 A, First (left) and second (right) layers of back muscles. B, Dissection of these same two layers. C, Close-up, taken from a left posterior oblique perspective. The serratus posterior inferior muscle of the third layer can also be seen in panel B and in Figure 4-2, A and B.
Trapezius Muscle
The trapezius muscle is the most superficial and superior back muscle (see Fig. 4-1). It is a large, strong muscle that is innervated by the accessory nerve (cranial nerve XI). In addition to its innervation from the accessory nerve, the trapezius muscle receives some proprioceptive fibers from the third and fourth cervical ventral rami. Because the trapezius muscle is so large, it has many attachment sites. This muscle arises in the midline from the superior nuchal line, external occipital protuberance, ligamentum nuchae of the posterior neck, spinous processes of C7 to T12, and supraspinous ligament between C7 and T12. It attaches distally onto the spine of the scapula, acromion, and distal third of the clavicle. Detailed morphometric measurements have been performed on this muscle (Kamibayashi & Richmond, 1998).
Because of its size and the many locations of its attachments, the trapezius muscle also has many actions. Most of these actions result in movement of the neck and scapula (i.e., the “shoulder girdle” as a whole). The function of the trapezius muscle depends on which region of the muscle is contracting (upper, middle, or lower). The middle portion retracts the scapula, whereas the lower portion depresses the scapula and at the same time rotates the scapula so that its lateral angle moves superiorly (i.e., rotates the point of the shoulder up). The actions of the upper part of the trapezius muscle also depend on whether the head or neck or the scapula is stabilized. When moving the head and neck, the actions of the upper fibers of the trapezius muscle are also determined by whether the muscle is contracting unilaterally or bilaterally. When the head and neck are stabilized by other muscles, then there is some conflicting evidence as to whether the upper fibers of the trapezius muscle help in elevation of the scapula. Based upon information gathered from cadaveric dissections of the attachment points and directions of the upper fibers of the trapezius muscle, Johnson and colleagues (1994) concluded that these fibers do not aid in elevation of the scapula. On the other hand, there is good electromyographic evidence that the upper fibers of the trapezius muscle are active during elevation of the shoulder (Campos et al., 1994; Guazzelli et al., 1994). Table 4-1 summarizes the actions of the trapezius muscle and Table 4-2 summarizes all of the muscles that are discussed in this chapter.
Latissimus Dorsi Muscle
The latissimus dorsi muscle is the more inferior and lateral of the two muscles that constitute the first layer of back muscles (see Fig. 4-1). This large muscle has an extensive region for its proximal attachment, which includes the following:
• Spinous processes and supraspinous ligament of T6-L5 (although the supraspinous ligament ends between L2 and L4)
• Posterior sacrum (median sacral crest) (see Chapter 8)
The latissimus dorsi muscle derives much of its origin from the thoracolumbar fascia. This is a tough and extensive aponeurosis (see the following discussion). The latissimus dorsi muscle passes superiorly and laterally to attach into the floor of the intertubercular groove of the humerus, between the laterally located attachment of the pectoralis major muscle and the medially located attachment of the teres major muscle. Contraction of the latissimus dorsi muscle results in adduction, medial rotation, and extension of the humerus.
The latissimus dorsi muscle is innervated by the thoracodorsal nerve, which is a branch of the posterior cord of the brachial plexus. The thoracodorsal nerve is derived from the anterior primary divisions of the sixth through eighth cervical nerves.
Thoracolumbar (or Lumbodorsal) Fascia
Because of its clinical significance, the anatomy of the thoracolumbar fascia deserves further discussion. This fascia extends from the thoracic region to the sacrum. It forms a thin covering over the erector spinae muscles in the thoracic region, whereas in the lumbar region the thoracolumbar fascia is strong and is composed of three layers. The posterior layer attaches to the lumbar spinous processes, interspinous ligaments between these processes, and median sacral crest. This layer has its own superficial and deep laminae (Macintosh & Bogduk, 1987a). This posterior layer is a strong sheet of dense connective tissue that links two of the largest muscles of the body—latissimus dorsi and gluteus maximus. It is, therefore, important in transferring forces between the spine, pelvis, and lower limbs (Vleeming & Stoeckart, 2007). The middle layer attaches to the tips of the lumbar transverse processes and intertransverse ligaments and extends superiorly from the iliac crest to the twelfth rib. The anterior layer covers the anterior aspect of the quadratus lumborum muscle and attaches to the anterior surfaces of the lumbar transverse processes. Superiorly the anterior layer forms the lateral arcuate ligament (see Diaphragm). The anterior layer continues inferiorly to the ilium and iliolumbar ligament. The posterior and middle layers surround the erector spinae muscles posteriorly and anteriorly, respectively (see Fifth Layer), and meet at the lateral edge of the erector spinae, where these two layers are joined by the anterior layer (Standring et al., 2008). Barker and Briggs (1999) have demonstrated in a cadaveric study that the thoracolumbar fascia may continue more superiorly than classically described. They found that the superficial lamina of the posterior layer ran superiorly to be continuous with the rhomboid muscles, whereas the deep lamina of the posterior layer was continuous superiorly with the splenius muscles. These superior extensions of the fascia were of variable thickness, but seemed thick enough to transmit tension. This means that the thoracolumbar fascia may have a more global influence on biomechanics than thought previously.
The lateral union of the three principal layers of the thoracolumbar fascia serves as a posterior aponeurosis for origin of the transversus abdominis muscle. More recent evidence has shown that because of its indirect attachment to the lumbar transverse processes via the thoracolumbar fascia, the transversus abdominis muscle may play a greater role in lumbar segmental control than previously believed (Barker et al., 2007). The direction of the fibers within each lamina of the posterior layer makes the thoracolumbar fascia stronger along its lines of greatest stress. When the thoracolumbar fascia is tractioned laterally by the action of the abdominal muscles, the distinct direction of fibers of the posterior layer’s two laminae helps aid in extension of the spine and the maintenance of an erect posture.
Some investigators believe that because the posterior and middle layers surround the erector spinae muscles, injury to these muscles at times may lead to a “compartment” type of syndrome within these two layers of the thoracolumbar fascia (Peck et al., 1986). This syndrome results from edema within the erector spinae muscles. The edema stems from injury and increases the pressure in the relatively closed compartment composed of the erector spinae muscles wrapped within the posterior and middle layers of the thoracolumbar fascia. This may result in increased pain and straightening of the lumbar lordosis (Peck et al., 1986). However, further research is necessary to determine the best approach available to diagnose this condition and the frequency with which it occurs.
Second Layer
The second layer of back muscles includes three muscles that, along with the first layer, connect the upper limb to the vertebral column. All three muscles lie deep to the trapezius muscle and attach distally onto the scapula’s medial border. They include the rhomboid major, rhomboid minor, and levator scapulae muscles (see Fig. 4-1). Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
Rhomboid Major and Minor Muscles
The rhomboid major muscle arises by tendinous fibers from the spinous processes of T2 through T5 and the supraspinous ligament at those levels. The muscle fibers run in an inferolateral direction and attach via a tendinous band on the medial border of the scapula between the root of the scapular spine and the inferior angle.
The rhomboid minor muscle is located immediately superior to the rhomboid major; its fibers also course in an inferolateral direction. Beginning from the lower portion of the ligamentum nuchae and the spinous processes of C7 and T1, the rhomboid minor muscle ends on the scapula’s medial border at the level of the scapular spine’s root.
Both rhomboid muscles are innervated by the dorsal scapular nerve, which arises from the anterior primary division of the C5 spinal nerve.
Because the fibers of these two muscles are parallel, their actions are similar. In addition to the other muscles that insert on the scapula, they help stabilize its position and movement during active use of the upper extremity. Specifically, the rhomboid muscles retract and rotate the scapula such that the lateral angle moves inferiorly (i.e., rotates the point of the shoulder down).
Levator Scapulae Muscle
The levator scapulae muscle arises by tendinous slips from the transverse processes of the atlas and axis (see Chapter 5) and the posterior tubercles of the transverse processes of C3 and C4. Its fibers descend and attach onto the scapula’s medial border between the root of the scapular spine and the superior angle. It is innervated by branches from the ventral rami of the C3 and C4 spinal nerves and the dorsal scapular nerve (C5). If the cervical spine is fixed, the levator scapulae muscle helps in elevating and rotating the scapula such that the lateral angle moves inferiorly (i.e., rotates the point of the shoulder down). When the scapula is stabilized, contraction of this muscle laterally flexes and rotates the neck to the same side. Bilateral contraction helps in extension of the cervical spine.
Third Layer
The third layer of back muscles is sometimes called the intermediate layer of back muscles. This is because the two small muscles of this group lie between layers one and two (the superficial back muscles) and layers four through six (the deep back muscles).
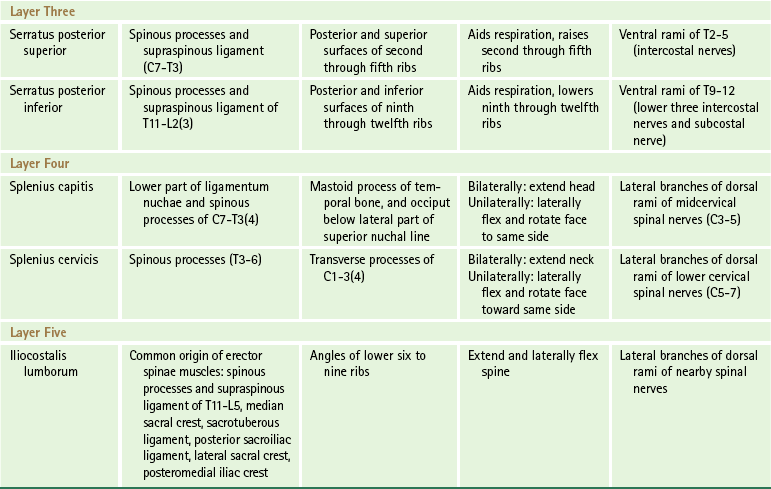
The third layer of back muscles consists of two thin, almost quadrangular muscles: the serratus posterior superior and serratus posterior inferior (Fig. 4-2, A and B).
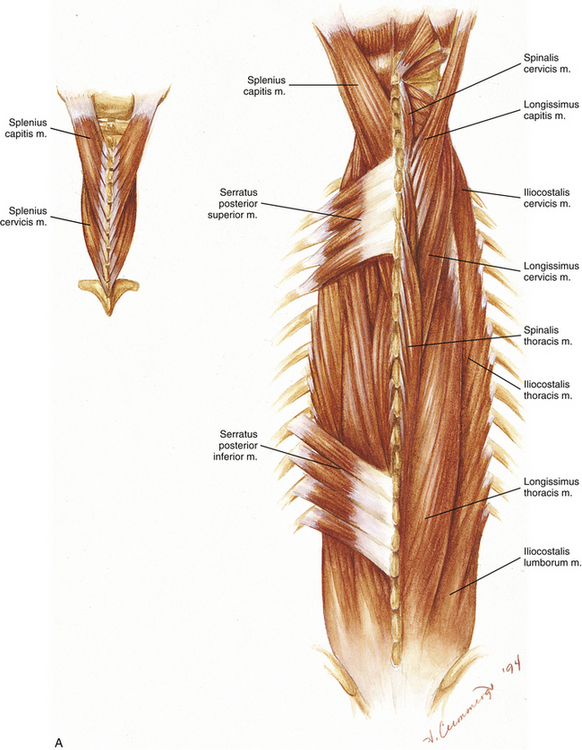
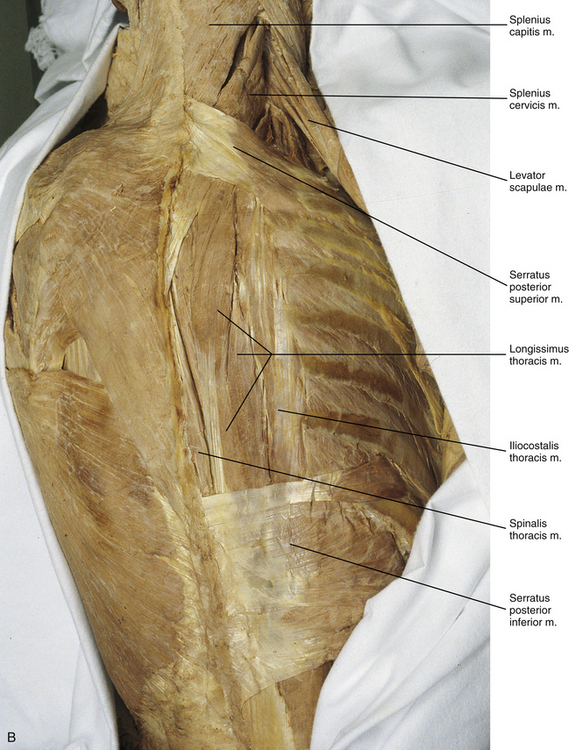
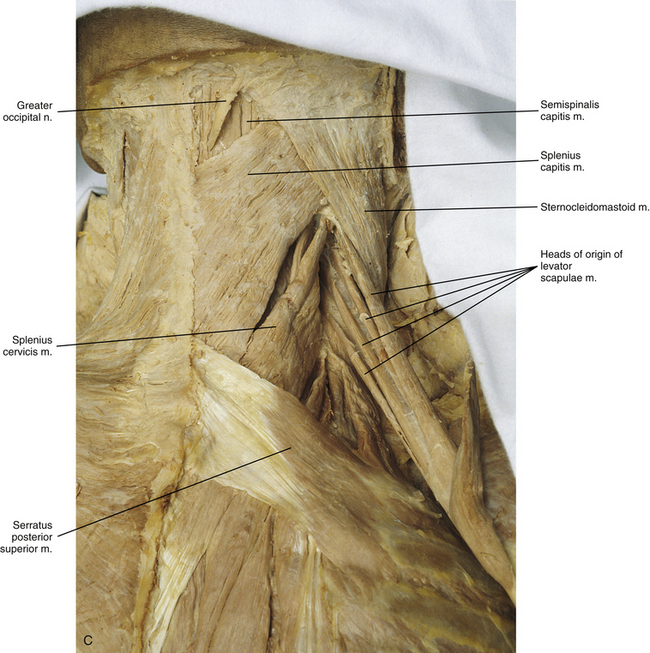
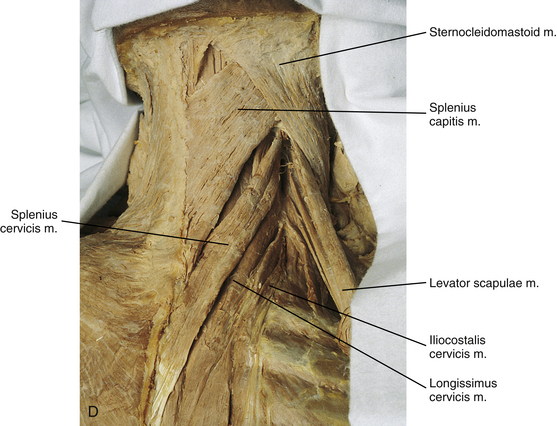
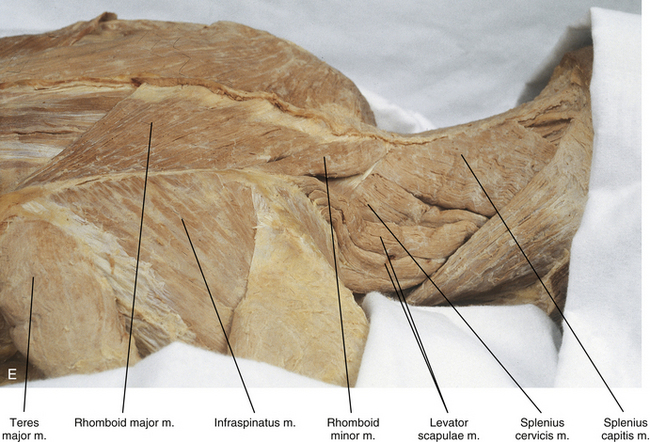
FIG. 4-2 A, Third, fourth (also see inset), and fifth layers of back muscles. B, Serratus posterior superior and inferior muscles that compose layer three. C-E, Splenius capitis and cervicis muscles of layer four and levator scapulae muscle of layer three. C, Right posterior view. D, Right posterior view with the serratus posterior superior muscle removed. E, Right lateral view.
Serratus Posterior Superior and Serratus Posterior Inferior Muscles
The serratus posterior superior muscle arises from the spinous processes of C7 through T3 and the supraspinous ligament that runs between them. Its fibers course inferolaterally to attach onto the posterior and superior aspect of the second through fifth ribs. This muscle is innervated by the anterior primary divisions (ventral rami) of the second through fifth thoracic nerves (intercostal nerves).
The serratus posterior inferior muscle arises from the spinous processes and intervening supraspinous ligament of T11 to L2. Its fibers run superolaterally to attach onto the posterior and inferior surfaces of the lower four ribs, and this muscle is innervated by the lower three intercostal nerves (T9 to T11) and the subcostal nerve. These nerves are all anterior primary divisions of their respective spinal nerves. The serratus posterior superior and inferior muscles may help with respiration. More specifically, the serratus posterior superior muscle elevates the second through fourth ribs, which may aid inspiration. The serratus posterior inferior muscle lowers the ninth through twelfth ribs, which may help with forced expiration. However, electromyographic evidence refutes a respiratory function for these muscles (Vilensky et al., 2001); they may function primarily in proprioception.
Fourth Layer
The most superficial layer of deep back muscles is the fourth layer, which consists of two muscles whose fibers ascend in a superolateral direction. This layer is composed of the splenius capitis and splenius cervicis muscles (Fig. 4-2, C to E). Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
Splenius Capitis and Splenius Cervicis Muscles
The splenius capitis muscle begins from the lower half of the ligamentum nuchae and the spinous processes of C7 through T3 or T4. Its fibers run superolaterally to attach to the mastoid process of the temporal bone and to the occiput just inferior to the lateral third of the superior nuchal line.
The splenius cervicis muscle arises from the spinous processes of T3 through T6, and its fibers run parallel to the fibers of the splenius capitis muscle to attach superiorly onto the transverse processes of the atlas and axis and the posterior tubercles of the transverse processes of C3 and sometimes C4. These attachment sites are deep to the origins of the levator scapulae. The splenius capitis and cervicis muscles are innervated by lateral branches of the posterior primary divisions (dorsal rami) of the midcervical and lower cervical spinal nerves, respectively. When the splenius muscles of both sides act together, they extend the head and neck. When the muscles of one side contract, they laterally flex the head and neck and slightly rotate the face toward the side of contraction.
Fifth Layer
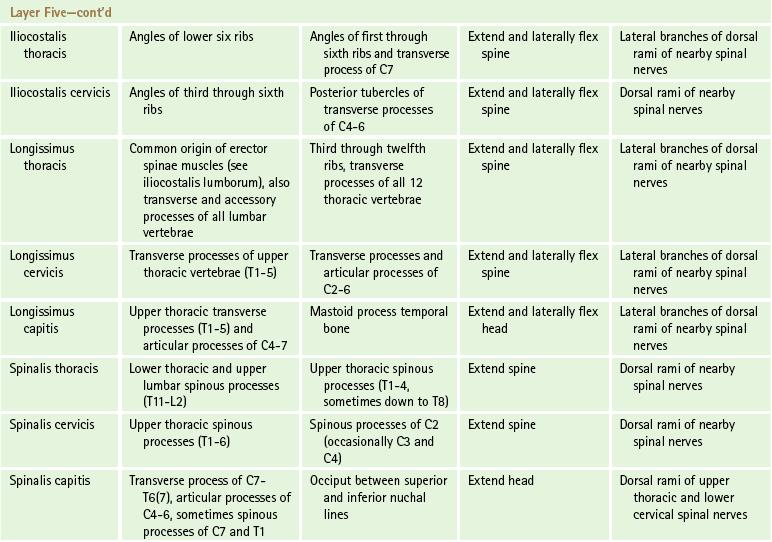
The largest group of back muscles is the fifth layer. This layer is composed of the erector spinae group of muscles (Fig. 4-3, A; see also Fig. 4-2, A and B). This erector spinae group is also collectively known as the sacrospinalis muscle. The muscles that comprise this group are a series of longitudinal muscles that course the length of the spine, filling a groove lateral to the spinous processes. Because of this location, these muscles generally have a similar function, which is to extend and laterally flex the spine. The erector spinae muscles are all segmentally innervated by lateral branches of the posterior primary divisions (dorsal rami) of the nearby spinal nerves and are covered posteriorly in the thoracic and lumbar regions by the thoracolumbar fascia. These longitudinal muscles can be divided into three groups. These three groups are, from lateral to medial, the iliocostalis, the longissimus, and the spinalis groups of muscles. Each of these groups, in turn, consists of three subdivisions. The subdivisions are named according to the general area of the spine to which they insert (e.g., lumborum, thoracis, cervicis, capitis). The descriptions that follow attempt to simplify the arrangement of the erector spinae group as much as possible. In reality, there is much individual variation in the actual arrangements of these muscles with many long sequentially overlapping multisegmental bundles and diverse multilayered insertions (Nomizo & Sakai, 2009). This complex arrangement also leads to apparent discrepancies in the segmental innervation pattern of this group of muscles. The erector spinae muscles are discussed from the most lateral group to the most medial, and each group is discussed from inferior to superior.
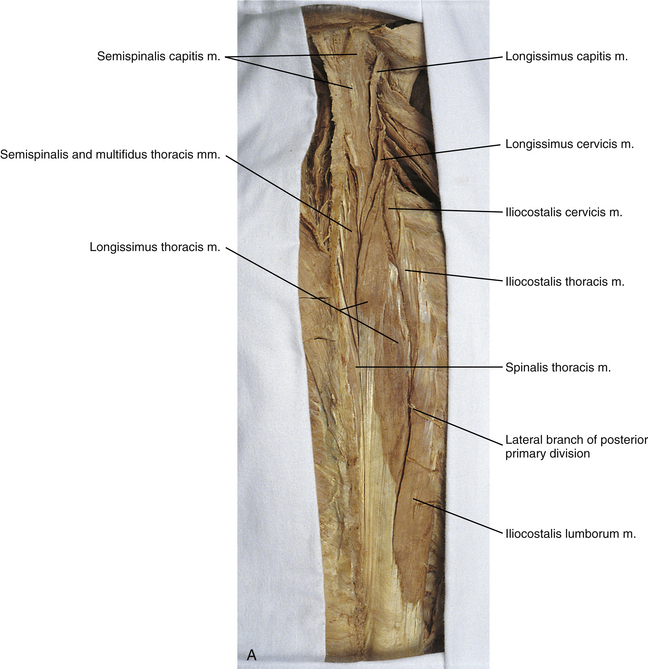
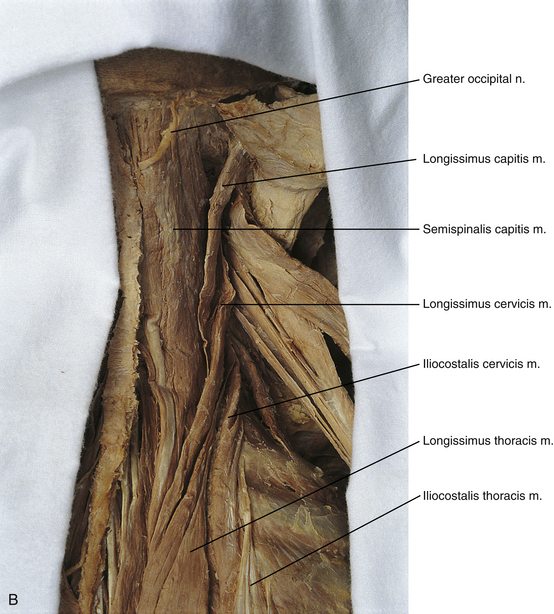
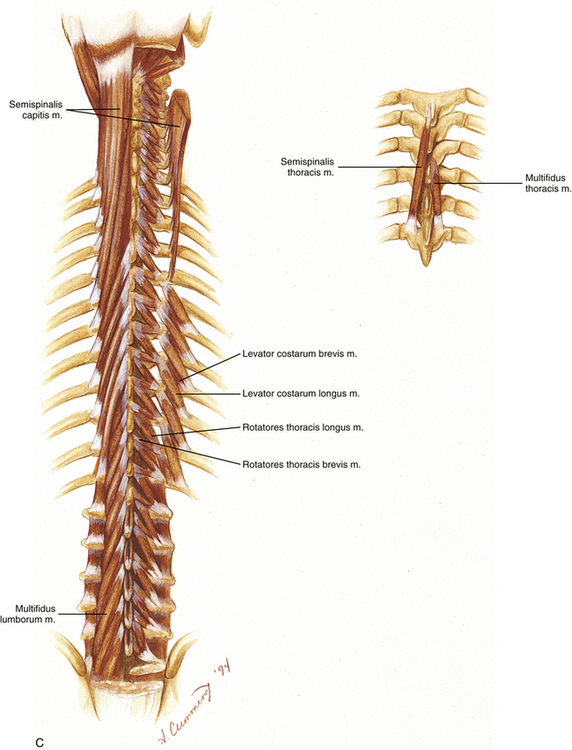
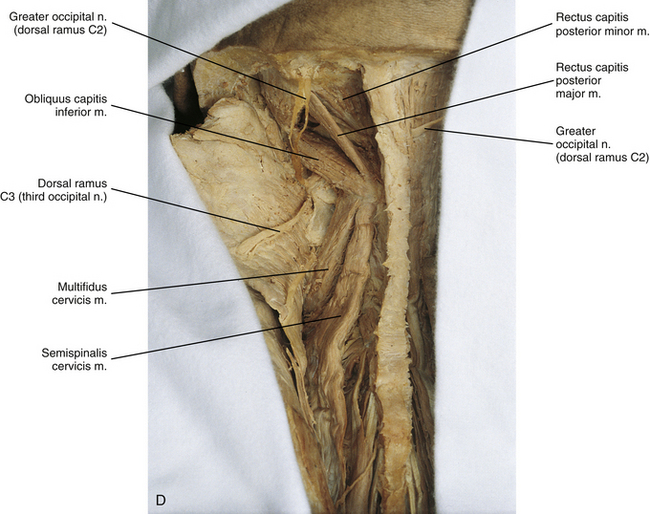
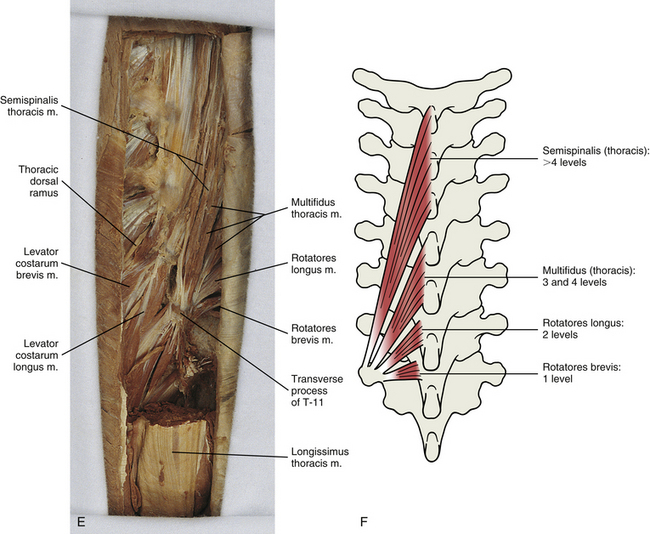
FIG. 4-3 A, Fifth layer of back muscles of the right side. B, Right semispinalis capitis muscle of the sixth layer from a cadaveric dissection. C, Sixth layer of back muscles. (Left) Semispinalis capitis and thoracis and multifidus lumborum muscles. (Right) Semispinalis capitis has been cut from its superior attachment and folded laterally to display rotatores, intertransversarii, and interspinales muscles. The levator costarum longus and brevis muscles are visible in the thoracic region. (Inset) Semispinalis and multifidus muscles. D, Semispinalis cervicis and multifidus cervicis muscles in a left posterior view of the upper cervical region. E, Semispinalis, multifidus, and rotatores longus and brevis muscles as they arise from a single left lower thoracic transverse process (transverse process of T11). F, Illustration demonstrating semispinalis, multifidus, and rotatores longus and brevis muscles arising from a single transverse process. The number of vertebral segments ascended before terminating is listed for each muscle.
Iliocostalis Muscles
The iliocostalis (iliocostocervicalis) group of muscles is subdivided into lumborum, thoracis, and cervicis muscles (see Fig. 4-3, A and B). Inferiorly the iliocostalis muscles derive from the common origin of the erector spinae muscles.
Iliocostalis lumborum: The iliocostalis lumborum muscle is the most inferior and lateral of the erector spinae muscles. It originates from the common origin of the erector spinae muscles, which includes the following:
• Spinous processes and supraspinous ligament of T11 through L5 (supraspinous ligament ends between L2 and L4)
The iliocostalis lumborum muscle runs superiorly to attach onto the posterior and inferior surfaces of the angles of the lower six to nine ribs. This muscle extends and laterally flexes the thoracolumbar spine and is innervated by lateral branches of the posterior primary divisions of lumbar and lower thoracic spinal nerves.
Macintosh and Bogduk (1987b) further described the anatomy of the iliocostalis lumborum muscle based on a series of elegant dissections. They found that part of this muscle arises from the posterior superior iliac spine and the posterior aspect of the iliac crest and ascends to attach onto the lower eight or nine ribs. They called this part the iliocostalis lumborum pars thoracis. Another part of the classically described iliocostalis lumborum muscle begins from the tips of the lumbar spinous processes and associated middle layer of the thoracolumbar fascia of L1 to L4 (see Thoracolumbar [or Lumbodorsal] Fascia) and attaches onto the anterior edge of the iliac crest. They called this part the iliocostalis lumborum pars lumborum and found that it formed a considerable mass of muscle. More recent evidence from the Visible Human Project corroborates this classification (Daggfeldt et al., 2000).
Iliocostalis thoracis: The iliocostalis thoracis muscle starts from the superior aspect of the angles of the lower six ribs and ascends to end on the angles of approximately the upper six ribs and transverse process of the C7 vertebra. This muscle extends and laterally flexes the thoracic spine and is innervated by the lateral branches of the posterior primary divisions (dorsal rami) of the thoracic spinal nerves.
Iliocostalis cervicis: The iliocostalis cervicis muscle arises from the superior aspect of the angle of the third through sixth ribs and attaches superiorly onto the posterior tubercles of the transverse processes of the C4 to C6 vertebrae. It laterally flexes and extends the lower cervical region and is innervated by the dorsal rami of the upper thoracic and lower cervical spinal nerves.
Longissimus Muscles
The longissimus muscles are located medial to the iliocostalis group. The longissimus group consists of thoracis, cervicis, and capitis divisions. The lateral branches of the posterior primary divisions (dorsal rami) of the spinal nerves exit the thorax and then course laterally and posteriorly between the iliocostalis muscles and longissimus thoracis muscle (see Fig. 4-3, A). This fact is used in the gross anatomy laboratory not only to quickly find the lateral branches of the posterior primary divisions, but also to demonstrate the separation between these two large muscle masses. After providing motor and sensory innervation to the sacrospinalis muscle, the lateral branches continue to the skin of the back, providing cutaneous sensory innervation.
Longissimus thoracis: The longissimus thoracis muscle is the largest of the erector spinae muscles. It arises from the common origin of the erector spinae muscles (see Iliocostalis Lumborum). In addition, many fibers begin from the transverse and accessory processes of the lumbar vertebrae (see Chapter 7). This muscle is the longest muscle of the back, thus the name longissimus. It ends superiorly on the third through twelfth ribs, between their angles and tubercles (see Chapter 6). The longissimus thoracis muscle also attaches onto the transverse processes of all 12 thoracic vertebrae. This muscle functions to hold the thoracic and lumbar regions erect, and laterally flexes the spine when it acts unilaterally. It is innervated by lateral branches of the thoracic and lumbar posterior primary divisions.
Macintosh and Bogduk (1987b) found fibers of the longissimus thoracis muscle that are confined to the lumbar and sacral regions. These fibers began from lumbar accessory and transverse processes and ended on the medial surface of the posterior superior iliac spine. The authors called these fibers the longissimus thoracis pars lumborum.
Longissimus cervicis: The longissimus cervicis muscle arises from the transverse processes of the upper thoracic vertebrae (T1 to T5) and ascends to end on the posterior tubercle of the transverse processes and the articular processes of C3 through C6 and onto the posterior aspect of the transverse process and the articular process of C2. Bilateral contraction of these muscles extends the neck. Unilateral contraction produces a combination of extension and lateral flexion of the neck to the same side. The longissimus cervicis muscle is innervated by lateral branches of the upper thoracic and lower cervical posterior primary divisions.
Longissimus capitis: The longissimus capitis muscle derives from upper thoracic transverse processes (T1 to T5) and articular processes of C4 through C7. It terminates on the mastoid process of the temporal bone, and its action is to extend the head. If it acts unilaterally, the longissimus capitis muscle can laterally flex the head and rotate it to the same side. It is innervated by the posterior primary divisions of upper thoracic and cervical spinal nerves.
Spinalis Muscles
The spinalis muscle group begins from spinous processes and ends on spinous processes, except for the spinalis capitis muscle. This muscle group consists of thoracis, cervicis, and capitis divisions.
Spinalis thoracis: The spinalis thoracis muscle fibers are the most highly developed of this muscle group. It arises from the lower thoracic and upper lumbar spinous processes (T11 to L2) and ascends to attach onto the upper thoracic spinous processes (T1 to T4 and perhaps down to T8). Laterally the fibers of this muscle blend with the fibers of the longissimus thoracis muscle. The spinalis thoracis muscle functions to extend the thoracic spine. It is innervated by posterior primary divisions of thoracic nerves.
Spinalis cervicis: The spinalis cervicis muscle begins from upper thoracic spinous processes (T1 to T6) and ends on the spinous processes of C2 and occasionally C3 and C4. Maintaining the tradition of the erector spinae muscles, the spinalis cervicis extends the cervical region. This muscle is usually quite small and frequently absent.
Spinalis capitis: The spinalis capitis muscle differs from the other spinalis muscles in that it does not typically start from or end on spinous processes. This muscle is difficult to differentiate from the more lateral semispinalis capitis muscle (see the following discussion). Its inferior attachment is blended with that of the semispinalis capitis muscle from the transverse processes of the C7 to the T6 or T7 vertebrae, the articular processes of C4 to C6, and sometimes from the spinous processes of C7 and T1. The fibers of this muscle blend with those of the semispinalis capitis muscle and attach with the latter muscle onto the occiput between the superior and inferior nuchal lines. The spinalis capitis muscle is sometimes called the biventer cervicis muscle because an incomplete tendinous intersection passes across it. When the left and right spinalis capitis muscles contract simultaneously, the result is extension of the head. Unilateral contraction results in lateral flexion of the head and neck and also rotation of the head away from the side of contraction. This muscle is innervated by upper thoracic and lower cervical posterior primary divisions.
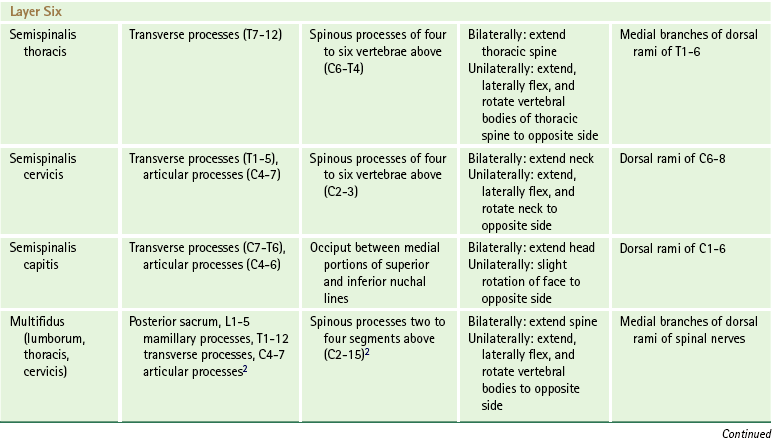
Sixth Layer
The sixth layer of back muscles includes the deep back muscles with fibers that course superiorly and medially. They are sometimes called the transversospinalis group because they generally attach inferiorly from transverse processes and end superiorly onto spinous processes (see Fig. 4-3, B to F). Some even suggest that this group be called the spinotransverse group, since this may be more consistent with the pattern of development of this muscle mass (Cornwall, Stringer, & Duxson, 2011). The muscles in this layer are arranged such that the length of the muscles becomes progressively shorter from superficial to deep. Although the actions of these muscles are described separately, remember that these muscles (especially the shorter ones) function primarily in a postural role as stabilizers rather than as prime movers. However, their fibers are organized in parallel, which indicates these muscles are also involved with “fine-tuning” spinal motions (Cornwall, Stringer, & Duxson, 2011). This group is classically described as being composed of the semispinalis, multifidus, and rotatores muscles, but recent evidence suggests that this may be an oversimplification and that there appears to be some “blending” (i.e., interconnections) between muscles of different lengths, especially the shorter ones (Cornwall, Stringer, & Duxson, 2011).
Semispinalis Muscles
The semispinalis muscles are located only in the thoracic and cervical regions and are divided into three parts: semispinalis thoracis, semispinalis cervicis, and semispinalis capitis muscles (see Fig. 4-3, B to F), although fascicles of similar length and arrangement have newly been described throughout the lumbar spine (Cornwall, Stringer, & Duxson, 2011).
Semispinalis thoracis: The semispinalis thoracis muscle consists of thin muscular fasciculi located between long tendons that attach inferiorly to the transverse processes of the lower six thoracic vertebrae and superiorly to the spinous processes of C6 to T4 (see Fig. 4-3, C). The semispinalis thoracis muscle is innervated by the medial branches of the posterior primary divisions of the upper six thoracic spinal nerves.
Semispinalis cervicis: The semispinalis cervicis muscle is a thicker mass of muscle that begins from the transverse processes of the upper five or six thoracic vertebrae (see Fig. 4-3, D). It may arise from the articular processes of the lower four cervical vertebrae also. This muscle mainly terminates on the spinous process of the axis, but also attaches to the spinous processes of C3 to C5. It derives its innervation from the posterior primary divisions (dorsal rami) of the C6 to C8 spinal nerves.
Semispinalis capitis: The semispinalis capitis muscle is thick and powerful and represents the best-developed portion of the semispinalis muscle group (see Fig. 4-3, B to D). Detailed morphometric measurements have been performed on this muscle (Kamibayashi & Richmond, 1998). It arises from the transverse processes of C7 to T6 and the articular processes of C4 to C6. The semispinalis capitis muscle attaches superiorly onto the medial part of the area between the occiput’s superior and inferior nuchal lines. Usually it is blended with the spinalis capitis muscle, and is likewise supplied by the dorsal rami of the first through sixth cervical spinal nerves.
When the muscles of both sides act jointly, the semispinalis thoracis and cervicis muscles function to extend the thoracic and cervical portions of the spine, respectively, whereas unilateral contraction of these muscles not only slightly extends the spine but also rotates the vertebral bodies to the opposite side. The semispinalis capitis muscles together function to extend the head and, working separately, slightly rotate the head to the opposite side.
Multifidus Lumborum, Thoracis, and Cervicis Muscles
The multifidus muscles lie deep to the semispinalis muscles, where they fill the groove between the transverse and spinous processes of the vertebrae. This group consists of multiple muscular and tendinous fasciculi that arise from the dorsal aspect of the sacrum and posterior superior iliac spine, mamillary processes of the lumbar vertebrae, transverse processes of the thoracic vertebrae, and articular processes of the lower four cervical vertebrae. These fasciculi ascend two to four (or sometimes five) vertebral segments before ending on a spinous process. Multifidi muscles insert onto all the vertebrae except the atlas. The multifidus muscles produce extension of the vertebral column. They also generate some rotation of the vertebral bodies away from the side of contraction, and they are also active in lateral flexion of the spine.
This muscle group has been found to contract during axial rotation of the trunk in either direction (Oliver & Middleditch, 1991). When the oblique abdominal muscles contract to produce trunk rotation, some flexion of the trunk is produced as well (see Anterolateral Abdominal Muscles). The multifidus muscles oppose this flexion component and maintain a pure axial rotation, thereby acting as stabilizers during trunk rotation. The multifidus muscles are innervated segmentally by the medial branches of the posterior primary divisions of the spinal nerves.
In the lumbar spine, where the multifidus group is best developed, this muscle mass is arranged into five bands, each attaching superiorly to one lumbar spinous process (Macintosh et al., 1986). In each band the deepest fascicles actually run from the mamillary process below to the lamina of the vertebra two segments above. The more superficial fascicles are longer and run from mamillary processes to spinous processes three to five segments above. In the lower lumbar spine the inferior attachments of the fascicles include the posterior aspect of the sacrum lying adjacent to the spinous tubercles, posterior sacroiliac ligaments, posterosuperior iliac spine, and deep surface of the erector spinae aponeurosis.
Each band of the multifidus lumborum muscle mass is actually a myotome arranged such that the fibers that move a particular lumbar vertebra (e.g., those that attach superiorly to a single spinous process) are innervated by the medial branch of the dorsal ramus of that segment’s spinal nerve. For example, the multifidus band inserting onto the spinous process of L2 is innervated by the medial branch of the dorsal ramus (posterior primary division) of L2. Specifically in the lumbar region, the multifidus muscle mass produces primarily extension (Macintosh & Bogduk, 1986). Rotation of the lumbar spine is seen only secondarily, in conjunction with extension.
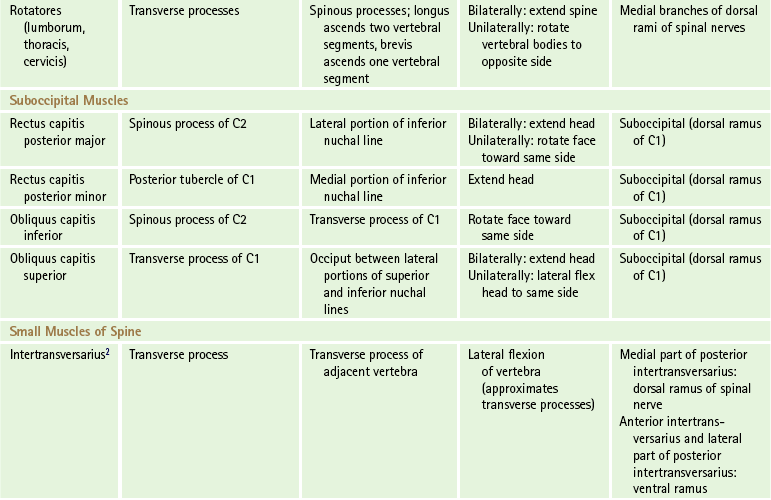
Rotatores Lumborum, Thoracis, and Cervicis Muscles
The rotatores muscles are located deep to the multifidus group. They constitute the deepest muscle fasciculi located in the groove between the spinous and transverse processes. This groove runs the entire length of the vertebral column from sacrum to axis. The two groups of rotatores muscles are determined by their length. The fascicles of the rotatores brevis begin on transverse processes and attach to the root of the vertebral spinous process immediately superior. The fascicles of the rotatores longus have similar origins but end on the root of the spinous process of the second vertebra above. The rotatores longus muscles are located immediately superficial to the rotatores brevis muscles. The rotatores muscles are best developed in the thoracic region and are only poorly developed in the cervical and lumbar regions, where they are difficult to distinguish from multifidus muscles. Acting bilaterally, these muscles help in extension of the spine, although unilateral contraction helps produce rotation of the spine such that the vertebral bodies move away from the side contracted. The rotatores muscles’ main function probably is to stabilize the vertebral column. These muscles are segmentally innervated by the medial branches of the posterior primary divisions of the spinal nerves.
The muscles of the fifth and sixth layers may be torn (strained) during hyperflexion of the spine or while lifting heavy loads. The muscles of these layers are composed of many individual strands that may tear near their musculotendinous junction. This tearing results in pain and tenderness, which may refer to neighboring regions (see Chapter 11). Localizing the torn muscle during physical examination may be difficult because many attachment sites of these muscles are deep. However, the costal attachments of the iliocostalis lumborum muscle and the iliac attachment of the longissimus thoracis muscle are close to the surface, and pain from these muscles may be localized to these attachment sites during examination (Bogduk, 2005).
Other Muscles Directly Associated with The Spine
The suboccipital muscles are a group of four small muscles located inferior to the occiput in the most superior portion of the posterior neck. They are the deepest muscles in this region, located under the trapezius, splenius capitis, and semispinalis capitis muscles. The suboccipital muscles consist of two rectus muscles (major and minor) and two obliquus muscles (superior and inferior). These muscles are concerned with extension of the head at the atlanto-occipital joint and rotation of the head at the atlanto-axial articulations. All are innervated by the posterior primary division of the C1 spinal nerve, which is also called the suboccipital nerve. The small number of muscle fibers per neuron for this group of muscles ranges from three to five (Oliver & Middleditch, 1991). This high degree of innervation allows these muscles to rapidly change tension, thus fine tuning the movements of the head and controlling head posture with a considerable degree of precision. Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
Rectus Capitis Posterior Major Muscle
The rectus capitis posterior major muscle (Fig. 4-4) begins at the spinous process of C2, widens as it ascends, and attaches superiorly to the lateral portion of the occiput’s inferior nuchal line. When acting bilaterally, the rectus capitis posterior muscles (both major and minor) produce extension of the head. Unilateral contraction turns the head so that the face rotates toward the side of the shortening muscle.
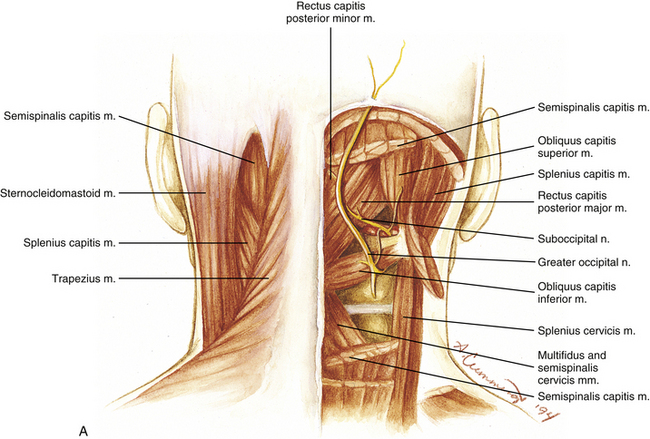
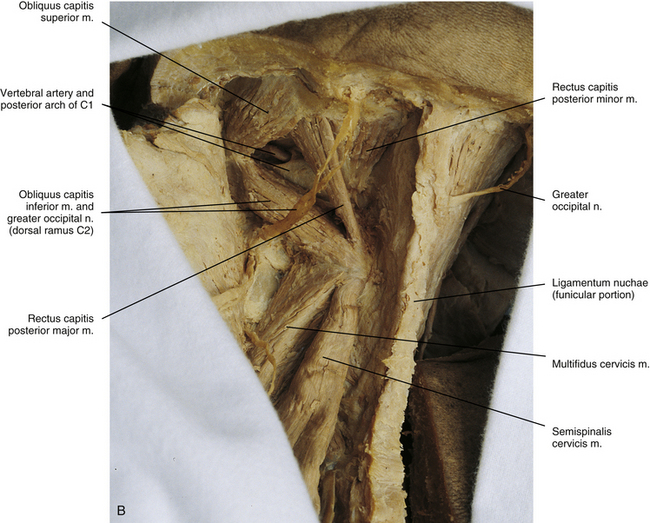
FIG. 4-4 (A) Illustration and (B) photograph of the suboccipital region. Three of the suboccipital muscles—the rectus capitis posterior major, obliquus capitis inferior, and obliquus capitis superior—form the suboccipital triangle. The remaining suboccipital muscle, the rectus capitis posterior minor, lies medial to the triangle. Notice the vertebral artery and the posterior arch of the atlas deep within the suboccipital triangle. A and B, Suboccipital muscles of the right and left sides, respectively.Suboccipital region.
Rectus Capitis Posterior Minor Muscle
The rectus capitis posterior minor muscle is located just medial to and partly deep to the rectus capitis posterior major muscle (see Fig. 4-4). It attaches inferiorly to the posterior tubercle of the atlas and becomes broader as it ascends. It ends on the medial portion of the occiput’s inferior nuchal line and the area between that line and the foramen magnum.
A connective tissue bridge between the rectus capitis posterior minor muscle and dorsal spinal dura mater at the atlanto-occipital junction has been consistently observed in cadavers (Hack et al., 1995). These bridges are also observable on magnetic resonance imaging (MRI) (Humphreys et al., 2003). They may serve to anchor the dura mater posteriorly. Also, there is usually a soft tissue connection between the rectus capitis posterior minor muscle and the posterior atlanto-occipital membrane (Zumpano, Hartwell, & Jagos, 2006). Contraction of the rectus capitis posterior minor muscle produces extension of the head.
Obliquus Capitis Inferior Muscle
The obliquus capitis inferior muscle is the larger of the two obliquus muscles (see Fig. 4-4). It arises on the spinous process of the axis and passes laterally and slightly superiorly to attach onto the transverse process of C1. This muscle rotates the atlas such that the face is turned to the same side of contraction. The length of the transverse processes of the atlas gives this muscle a considerable mechanical advantage (Standring et al., 2008).
Obliquus Capitis Superior Muscle
The obliquus capitis superior muscle arises from the transverse process of the atlas (see Fig. 4-4). It becomes wider as it runs superiorly and posteriorly. This muscle ends on the occiput between the superior and inferior nuchal lines, lateral to the attachment of the semispinalis capitis muscle, overlapping the insertion of the rectus capitis posterior major muscle. Head extension and lateral flexion to the same side are produced by contraction of this muscle. The left and right obliquus capitis superior muscles, in conjunction with the two rectus muscles of each side, probably act more frequently as postural muscles than as prime movers (Standring et al., 2008).
Three of the four suboccipital muscles on each side of the upper cervical region form the sides of a suboccipital triangle. The boundaries of each suboccipital triangle are (a) the obliquus capitis inferior muscle, below and laterally; (b) the obliquus capitis superior muscle, above and laterally; and (c) the rectus capitis posterior major muscle, medially and somewhat above. The roof of this triangle is composed of the splenius capitis muscle laterally and the semispinalis capitis muscle medially. Deep to these muscles is a layer of dense fibrofatty tissue that also helps to form the roof. The floor of the triangle is composed of the posterior arch of the atlas and the posterior atlanto-occipital membrane. The suboccipital triangle contains the horizontal portion (third part) of the vertebral artery, dorsal ramus of the C1 spinal nerve (suboccipital nerve), and suboccipital plexus of veins.
Intertransversarii Muscles
The intertransversarii muscles (Fig. 4-5) extend between adjacent transverse processes. These muscles are most highly developed in the cervical region. The cervical intertransversarii muscles usually begin at C1 (although the muscle between C1 and C2 often is absent) and continue to T1. They consist of anterior and posterior subdivisions that run between adjacent anterior and posterior tubercles, respectively. The ventral ramus of the spinal nerve exits between each pair of anterior and posterior intertransversarii muscles and innervates each anterior intertransversarius muscle. Each posterior intertransversarius muscle in the cervical region is further subdivided into a medial and a lateral part. The posterior primary division (dorsal ramus) of the spinal nerve frequently pierces the medial part of a posterior intertransversarius muscle and innervates that part of the muscle. The anterior primary division (ventral ramus) innervates the lateral part of the posterior intertransversarius muscle along with the anterior intertransversarius muscle, as mentioned. The intertransversarii muscles function to flex the spine laterally by approximating adjacent transverse processes. They also help to stabilize adjacent vertebrae during large spinal movements.
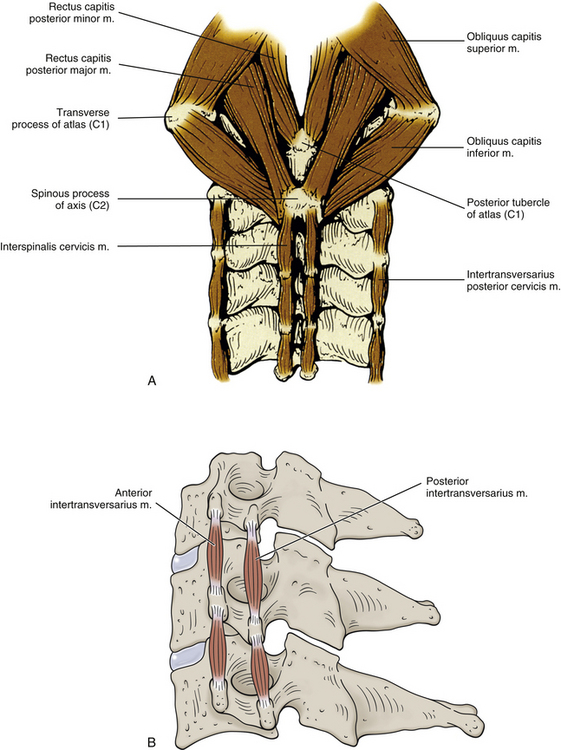
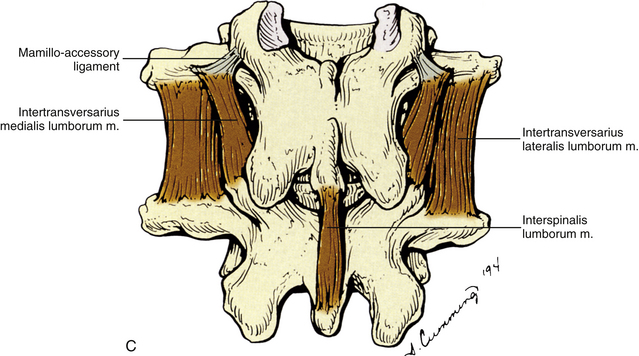
FIG. 4-5 A, Suboccipital, cervical interspinales, and cervical intertransversarii muscles. B, Lateral view showing the anterior and posterior cervical intertransversarii muscles (intertransversarius, singular),C, Lumbar interspinalis, and left and right lumbar intertransversarii muscles. Also illustrated is the mamillo-accessory ligament. Notice the intertransversarii medialis lumborum muscles on each side, taking part of their origin from the left and right mamillo-accessory ligaments.
The thoracic intertransversarii muscles are small and are usually only present in the lower thoracic region. They are not divided into subdivisions and are innervated by the dorsal rami (posterior primary divisions). There have been transversocostal muscles identified that attach to the medial aspects of the first three ribs and pass superiorly to attach to the adjacent transverse process (Darwish & Ibrahim, 2009). These may be embryologically related to the upper thoracic intertransversarii muscles.
The lumbar intertransversarii muscles are found between all lumbar vertebrae. As with the posterior portion of the cervical intertransversarii muscles, the lumbar group of muscles divides into medial and lateral divisions. Each medial division passes from the accessory process, mamillo-accessory ligament, and mamillary process of the vertebra above to the mamillary process of the vertebra below (see Fig. 4-5, C). Each lateral intertransversarius muscle in the lumbar region can be further subdivided into an anterior and posterior division. The anterior division runs between adjacent transverse processes, and the posterior division courses from the accessory process of the vertebra above to the transverse process of the vertebra below. Both the anterior and posterior divisions of the lateral intertransversarii muscles are innervated by lumbar anterior primary divisions (ventral rami). The medial intertransversarii muscles are innervated by lumbar posterior primary divisions.
The lumbar intertransversarii muscles generally are thought to laterally flex the lumbar region and stabilize adjacent vertebrae during spinal movement. However, the intertransversarii muscles are short and lie close to the axes of motion for lateral flexion and rotation of the spine, which places them at a considerable biomechanical disadvantage. Thus their usefulness as lateral flexors or stabilizers has been questioned (Bogduk, 2005). In addition, the intertransversarii and interspinales muscles have been found to possess up to six times more muscle spindles than the other deep back muscles. The large number of muscle spindles in these muscles has led Bogduk (2005) to speculate that the intertransversarii muscles function as proprioceptive transducers, providing afferent information for spinal and supraspinal circuits. These circuits help to maintain posture and produce smooth and accurate movements of the spine by adjusting and regulating neural activity to the back muscles.
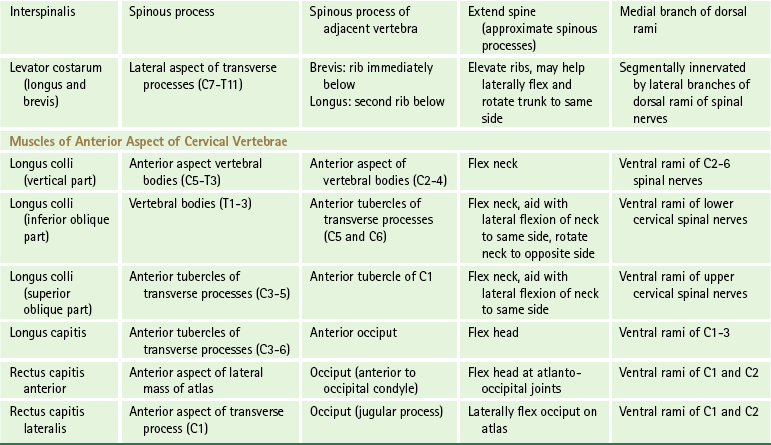
Interspinales Muscles
The interspinales muscles (see Fig. 4-5, A and C) are small muscles that extend between adjacent spinous processes. They are located on each side of the interspinous ligament. Interspinales muscles are present as small, distinct bundles of fibers throughout the cervical region, beginning at the spinous processes of C2 and continuing to the spinous process of T1. The thoracic interspinales muscles are variable and are located only in the upper and lower few segments. The lumbar region, as with the cervical region, has interspinales muscles running between all the spinous processes. The interspinales muscles are innervated by the medial branches of the posterior primary divisions of spinal nerves. The interspinales muscles function to extend the spine and may act as proprioceptive organs (Bogduk, 2005).
Levator Costarum Muscles
The levator costarum muscles (see Fig. 4-3, C) are muscular fasciculi that arise from the tips of the transverse processes of C7 to T11 and run inferiorly and laterally, parallel with the posterior borders of the external intercostal muscles. Each of the levator costarum brevis muscles attaches to the superior surface, between the tubercle and angle, of the rib immediately inferior to its level of origin. Sometimes, especially in the lower thoracic levels, fasciculi attach to the second rib below. These fasciculi are known as levator costarum longus muscles and are located medial to the brevis muscle originating from the same transverse process. The levator costarum muscles elevate the ribs and may help laterally flex and rotate the trunk to the same side. They are segmentally innervated by lateral branches of the posterior primary divisions (dorsal rami) of the spinal nerves.
Muscles Associated with the Anterior Aspect of the Cervical Vertebrae
The muscles associated with the anterior aspect of the cervical vertebrae include the longus colli, longus capitis, rectus capitis anterior, and rectus capitis lateralis muscles (Fig. 4-6). These muscles are responsible for flexing the neck and occiput and may be injured during extension injuries of the cervical region. Detailed morphometric measurements have been performed on these muscles (Kamibayashi & Richmond, 1998).
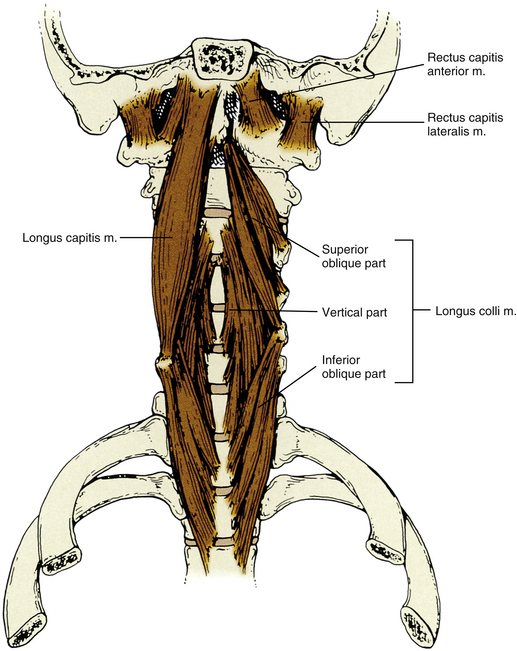
FIG. 4-6 Muscles associated with the anterior aspect of the cervical vertebrae and the occiput. (Right) Three parts of the longus colli muscle (vertical, inferior oblique, superior oblique). (Left) Longus capitis muscle. The rectus capitis anterior and lateralis muscles also can be seen as they pass from the atlas to the occiput.
Longus Colli Muscle
The left and right longus colli muscles (see Fig. 4-6) are located along the anterior aspect of the cervical vertebral bodies. Each of these muscles consists of three parts: vertical, inferior oblique, and superior oblique. Together the three parts of this muscle flex the neck (Cagnie et al., 2010). The superior and inferior oblique parts also may aid with lateral flexion. The inferior oblique part also rotates the neck to the opposite side. The longus colli muscle is innervated by branches of the anterior primary divisions of C2 to C6. This muscle is probably one of the muscles responsible for reversal of the cervical lordosis after extension injuries of the neck. The longus colli muscle has been found to contain a high density of muscle spindles. This implies an important proprioceptive function for this muscle (Boyd-Clark et al., 2002). The origins, insertions, and unique characteristics of the three parts of the longus colli muscle are listed next.
Vertical portion: The vertical portion of the longus colli muscle both begins and ends on vertebral bodies. More specifically, this muscle attaches inferiorly to the anterior aspect of the vertebral bodies of C5 to T3 and ascends to end superiorly on the vertebral bodies of C2 to C4.
Inferior oblique portion: The inferior oblique portion of the longus colli muscle arises from the vertebral bodies of T1 to T3 and passes superiorly and laterally to attach onto the anterior tubercles of the transverse processes of C5 and C6.
Superior oblique portion: The superior oblique portion of the longus colli muscle begins from the anterior tubercles of the transverse processes of C3 to C5. Its fibers course superiorly and medially and converge to terminate on the anterior tubercle of the atlas by means of a narrow tendon. This tendinous insertion can be torn during an extension injury of the neck. Such an injury can be followed by the deposition of calcium in the region, a condition known as retropharyngeal calcific tendonitis. The calcium may be seen on plain film x-ray approximately 3 weeks after injury and usually appears as an irregular and sometimes subtle region of increased radiopacity located just anterior to the atlas. Typically the calcium is resorbed as the injury heals and then is no longer visible on an x-ray film.
Longus Capitis Muscle
The longus capitis muscle is located anteriorly and slightly laterally to the longus colli muscle (see Fig. 4-6). It arises as a series of thin tendons from the anterior tubercles of the transverse processes of C3 to C6. The tendinous origins unite to form a distinct muscular band that courses superiorly toward the occiput. This muscular band attaches onto the region of the occiput anterior to the foramen magnum and posterior to the pharyngeal tubercle. The longus capitis muscle functions to flex the head (Cagnie et al., 2010) and is innervated by branches of the anterior primary divisions of C1 to C3.
Rectus Capitis Anterior Muscle
The rectus capitis anterior muscle is small and located deep to the inserting fibers of the longus capitis muscle (see Fig. 4-6). It attaches inferiorly to the anterior aspect of the lateral mass and the most medial part of the transverse process of the atlas. The rectus capitis anterior muscle attaches superiorly to the occiput just in front of the occipital condyle. This muscle functions to flex the head at the atlanto-occipital joints and is innervated by the anterior primary divisions of the first and second cervical nerves. It appears that the hypoglossal nerve also may help supply this muscle in some people (Shimokawa et al., 2004).
Rectus Capitis Lateralis Muscle
The rectus capitis lateralis muscle is another small muscle. It arises from the anterior aspect of the transverse process of the atlas and courses superiorly to end on the jugular process of the occiput (see Fig. 4-6). It laterally flexes the occiput on the atlas and is innervated by the anterior primary division of the first and second cervical nerves. It appears that the hypoglossal nerve also may help supply this muscle in some people (Shimokawa et al., 2004).
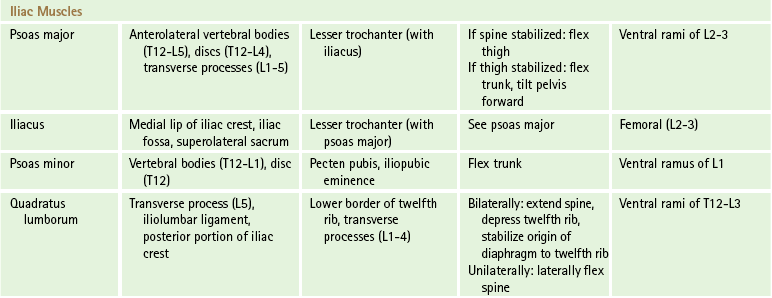
Iliac Muscles
The muscles of the iliac region—the psoas major, psoas minor, and quadratus lumborum (Fig. 4-7)—sometimes are called the posterior abdominal wall muscles. However, they may be classified properly as spinal muscles because they all have direct action on the vertebral column and are attached to the lumbar region. All three of these muscles attach inferiorly onto either the pelvis or the femur; therefore they also help connect the lower limbs to the spine.
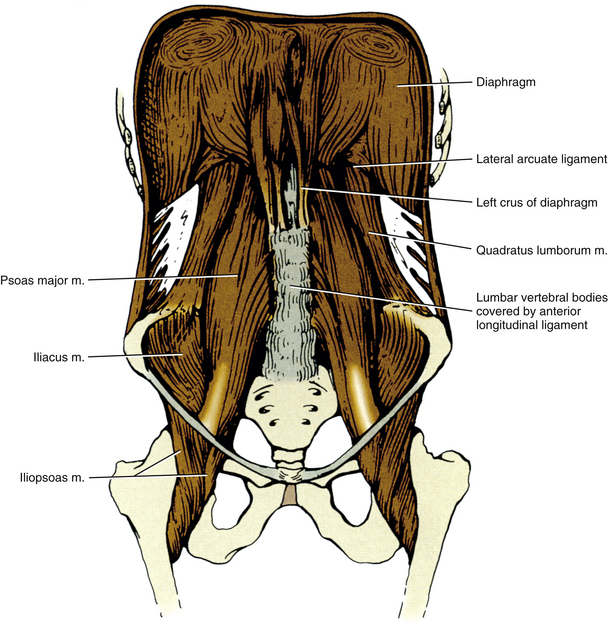
FIG. 4-7 Iliac muscles and the diaphragm. The left and right crura of the diaphragm are prominently displayed. Also notice the left and right quadratus lumborum, psoas major, and iliacus muscles.
Psoas Major and Iliacus Muscles
The psoas major muscle (see Fig. 4-7) arises from the anterolateral portion of the bodies of T12 to L5, the intervertebral discs between these bones, and the transverse processes of all the lumbar vertebrae. It descends along the pelvic brim, passes deep to the inguinal ligament and in front of the hip capsule, and terminates via a tendon onto the femur’s lesser trochanter. The lateral side of this tendon of the psoas major muscle receives the bulk of the fibers of the iliacus muscle. Together they form what is sometimes loosely called the iliopsoas muscle. The iliacus muscle begins from the inner lip of the iliac crest, upper two thirds of the iliac fossa, and superolateral portion of the sacrum. It ends via the psoas major tendon on the femur’s lesser trochanter.
The psoas major muscle, along with the iliacus muscle, functions primarily to flex the thigh at the hip. If the lower limb is stabilized, these muscles are concerned primarily with flexing the trunk and pelvis. They are important in raising the body from the supine to the sitting position. Electromyographic evidence further suggests that the psoas major muscle is involved in balancing the trunk when in the sitting position (Standring et al., 2008). When the neck of the femur is fractured, this muscle acts as a lateral rotator of the thigh, which results in the characteristic laterally rotated position of the lower limb after such a fracture. Both the psoas major and the iliacus muscles usually are innervated by fibers arising from the L2 and L3 spinal cord levels. The iliacus muscle receives branches of the femoral nerve, and the psoas major muscle is supplied by direct fibers from the ventral rami of the L2-3 spinal nerves. Sometimes the L1 and L4 spinal nerves also send branches into the psoas major muscle.
Psoas Minor Muscle
The psoas minor muscle is a variable muscle, absent in approximately 40% of the population (Standring et al., 2008). When present, it is located on the anterior surface of the psoas major muscle. The psoas minor muscle attaches superiorly to the lateral aspect of the bodies of T12 and L1 and the interposing intervertebral disc. It descends to attach inferiorly by a long tendon to the pecten pubis and iliopubic eminence. The psoas minor muscle acts as a weak trunk flexor and is innervated by fibers arising from the anterior primary division of the L1 spinal nerve.
Quadratus Lumborum Muscle
The quadratus lumborum muscle (see Fig. 4-7) lies along the tips of the transverse processes of the lumbar vertebrae and is irregularly quadrangular in shape. It attaches inferiorly to the transverse process of L5, iliolumbar ligament, and posterior aspect of the iliac crest adjacent to that ligament. Superiorly the quadratus lumborum muscle is attached to the lower border of the twelfth rib and the tips of the transverse processes of L1 to L4. If the pelvis is fixed, this muscle laterally flexes the lumbar spine. When both muscles contract, they help with extension of the spine. Each quadratus lumborum muscle also depresses the twelfth rib and aids in inspiration by stabilizing the origin of the diaphragm to the twelfth rib. It is innervated by fibers from the ventral rami of the T12 to L3 (sometimes L4) spinal nerves.
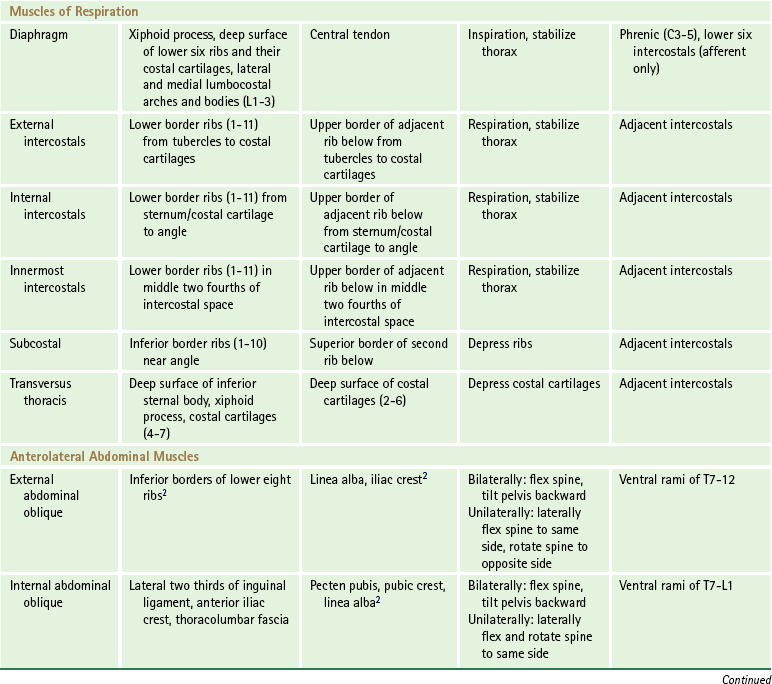
Muscles That Indirectly Influence the Spine
All the muscles of respiration have attachments to ribs. In addition to aiding respiration, all these muscles are involved to some extent with stabilizing the thoracic cage during trunk movements. The muscles of respiration are composed of the following: those that connect adjacent ribs (intercostals), those that span across more than one rib (subcostals), those that attach ribs to the sternum (transverse thoracis), those connecting ribs to vertebrae (levator costarum and serratus posterior superior and posterior inferior), and the diaphragm. Because the levator costarum and posterior serratus muscles have vertebral attachments, they are considered true back muscles and were discussed in previous sections.
Diaphragm
The diaphragm is the principal muscle of respiration (see Fig. 4-7). It is a domelike musculotendinous sheet that is convex superiorly. It completely separates the thoracic and abdominal cavities, except where it has apertures that allow for the passage of the esophagus, aorta, inferior vena cava, sympathetic trunks, and splanchnic nerves. This sheet consists of muscle fibers that attach to the entire border of the thoracic outlet. These fibers converge superiorly and medially and end as a central tendon. From anterior to posterior, muscle fibers arise from the posterior surface of the xiphoid process, the deep surface of the lower six ribs and their costal cartilages, interdigitations with the origin of the transversus abdominis muscle, lateral and medial lumbocostal arches, and first three lumbar vertebrae. The portions of this muscle that arise from the lumbar vertebrae form the left and right crura.
The lateral lumbocostal arch, also known as the lateral arcuate ligament, is a thickening of the fascia of the quadratus lumborum muscle. It attaches medially to the transverse process of L1, arches over the upper portion of the quadratus lumborum, and ends laterally on the lower border of the twelfth rib.
The medial lumbocostal arch, or medial arcuate ligament, is a similar structure, except that it is associated with the psoas major muscle. This arch also is attached to the transverse process of L1, but arches medially over the psoas major muscle and is connected to the lateral aspect of the body of L1 or L2.
The crura of the diaphragm arise from the anterolateral surfaces of the upper two (on the left) or three (on the right) lumbar vertebrae, their discs, and the anterior longitudinal ligament. The two crura meet in the midline and arch over the aorta’s anterior aspect to form what is sometimes called the median arcuate ligament.
The lower ribs are fixed when the diaphragm first contracts; then the central tendon is drawn inferiorly and anteriorly. The abdominal contents provide resistance to further descent of the diaphragm, which leads to protrusion of the anterior abdominal wall (“abdominal” breathing) and elevation of the rib cage (“thoracic” breathing). The diaphragm is innervated by the left and right phrenic nerves, which arise from the ventral rami of C3 to C5. Also, some afferent fibers from the peripheral aspect of this muscle are carried in the lower six or seven intercostal nerves. These nerves, and the sensory fibers of the phrenic nerves, are responsible for the referred pain patterns seen with some diaphragmatic pathology.
External, Internal, and Innermost Intercostal Muscles
The intercostal muscles (Fig. 4-8, A) comprise three sets of superimposed muscles located between adjacent ribs. These sets of muscles consist of the external intercostal, internal intercostal, and innermost intercostal muscles.
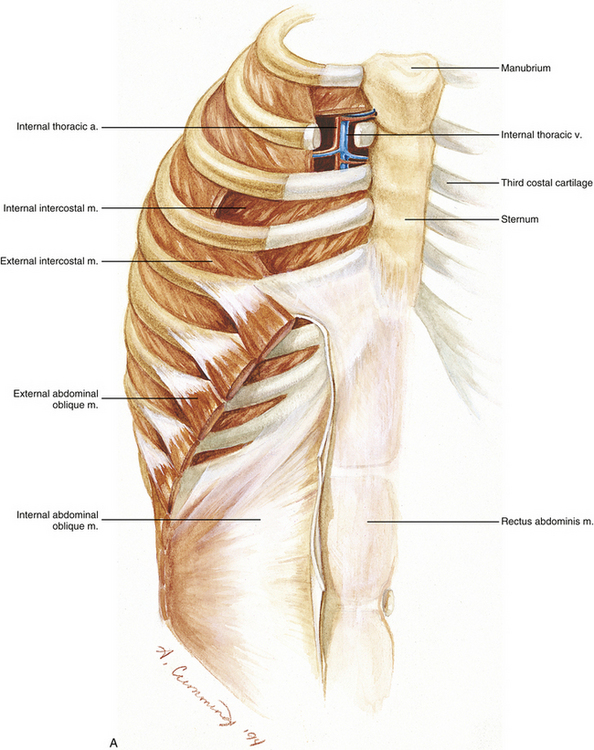
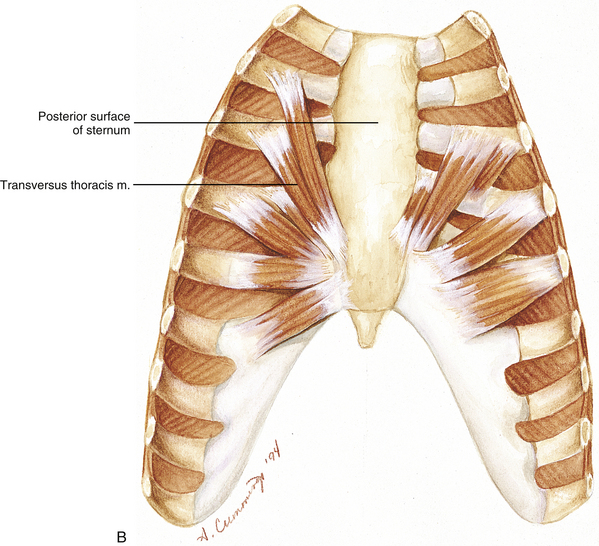
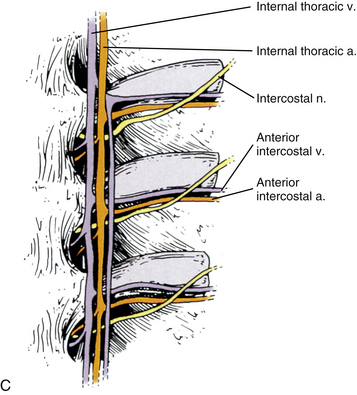
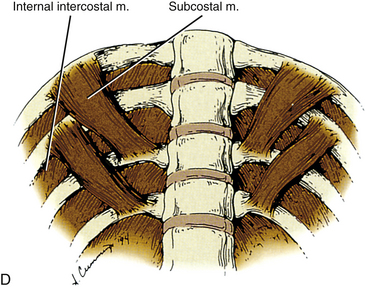
FIG. 4-8 A, Anterolateral view of the thoracic and abdominal walls. Upper aspect, Cutaway view of the medial intercostal spaces demonstrating the internal thoracic artery and vein. The external intercostal muscle has been reflected between the third and fourth ribs to show the internal intercostal muscle to best advantage. The external abdominal oblique muscle also has been reflected and cut away to reveal the internal abdominal oblique muscle. B, Internal view of the anterior thoracic wall showing the transversus thoracis muscle. C, Detail of B showing several intercostal spaces just lateral to the sternum. D, Internal view of the posterior thoracic wall showing several subcostal muscles.
The external intercostal muscles, 11 on each side, have attachments that extend along the shafts of the ribs from the tubercles to just lateral to the costal cartilages. More anteriorly, each is replaced by an aponeurosis, called the external intercostal membrane, which continues to the sternum. Each external intercostal muscle attaches superiorly to the lower border of one rib and attaches inferiorly on the upper border of the adjacent rib below. The fibers of each are directed obliquely; in the posterior chest, they run inferolaterally, although at the front, they course inferomedially and somewhat anteriorly.
The 11 pairs of internal intercostal muscles are located immediately deep to the external intercostals. Their attachments begin anteriorly at the sternum, or at the costal cartilages for ribs 8 through 10, and continue posteriorly to the costal angles. At that point, they are replaced by an aponeurotic layer, termed the internal intercostal membrane, which continues posteriorly to the anterior fibers of the superior costotransverse ligament. Each internal intercostal muscle attaches superiorly to the floor of the costal groove and corresponding portion of the costal cartilage and runs obliquely inferior to its attachment on the superior surface of the adjacent rib below. The fibers of the internal intercostal muscles are arranged orthogonally to those of the external intercostals.
The fibers of the innermost intercostal muscles lie just deep to and run parallel with those of the internal intercostals. They are poorly developed in the upper thoracic levels but become progressively more pronounced in the lower levels. They are attached to the deep surfaces of adjacent ribs and are best developed in the middle two fourths of the intercostal space. The intercostal veins, arteries, and nerves (from superior to inferior) can be found in the superior aspect of the intercostal space, passing between the fibers of the internal and innermost intercostal muscles.
Although the intercostal muscles play a role in respiration, their exact function is still controversial (Standring et al., 2008). Conflicting evidence exists regarding the actions of the various layers of the intercostals during inspiration and expiration. Results from studies using electromyography show differences in the activity of upper versus lower intercostal muscles during the different phases of respiration. In addition, activity has been recorded in the intercostal muscles during many trunk movements, and they appear to act as stabilizers of the thoracic cage (Oliver & Middleditch, 1991). The intercostal muscles are innervated by branches of the adjacent intercostal nerves.
Subcostal Muscles
The subcostal muscles (Fig. 4-8, D) are musculotendinous fasciculi that usually are best developed only in the lower thorax. Each arises from the inferior border of one rib, near the angle, and runs obliquely medial and inferior to the second or third rib below. The fibers of the subcostal muscles are parallel to those of the internal intercostals. They probably help depress the ribs and are innervated by branches from adjacent intercostal nerves.
Transversus Thoracis Muscle
The transversus thoracis, or sternocostalis, muscle is located on the deep surface of the anterior thoracic wall (Fig. 4-8, B). It arises from the posterior surface of the inferior one third of the sternal body, the posterior surface of the xiphoid process, and the posterior surfaces of the costal cartilages of the lower three or four true ribs. It terminates on the inferior and deep surfaces of the costal cartilages of the second through sixth ribs. The fibers of the muscle form a fanlike arrangement, with the upper fibers being almost vertically oriented and the intermediate fibers more obliquely oriented. The lowermost fibers not only are horizontal but also are continuous with the most superior fibers of the transversus abdominis muscle. The transversus thoracis muscle pulls the costal cartilages, to which it inserts in an inferior direction, and is innervated by the adjacent intercostal nerves.
Anterolateral Abdominal Muscles
Although the four muscles composing the anterolateral abdominal wall do not have direct attachments to the spine, they are involved in producing several movements of the trunk, including flexion, lateral flexion, and rotation. They are also important as postural muscles and in increasing intraabdominal pressure. These muscles include the external abdominal oblique, internal abdominal oblique, transversus abdominis, and rectus abdominis muscles.
External Abdominal Oblique Muscle
The external abdominal oblique (obliquus externus abdominis) muscle (see Fig. 4-8, A) is the largest and most superficial of these muscles. It arises as eight muscular slips from the inferior borders of the lower eight ribs. The upper slips attach near the cartilages of the ribs, whereas the lower ones attach at a progressively greater distance from the costal cartilages. The serratus anterior, latissimus dorsi, and sometimes pectoralis major muscles interdigitate with these slips. The lower fibers descend almost vertically, attaching to approximately the anterior half of the outer lip of the iliac crest. The upper and middle fibers pass inferomedially and become aponeurotic by the time they pass a line connecting the umbilicus and anterior superior iliac spine. The external oblique aponeurosis is a strong sheet of dense connective tissue whose fibers continue inferomedially to the midline, where they blend with the linea alba. The linea alba is a tendinous raphe running in the midline from the xiphoid process to the pubic symphysis. The inferior portion of the aponeurosis of the external abdominal oblique muscle forms the inguinal ligament, the reflected portion of that ligament, and the lacunar ligament. It also has an opening, the superficial inguinal ring, which allows passage of the spermatic cord in the male and the round ligament of the uterus in the female. The external abdominal oblique muscle is innervated by the ventral rami of the T7 to T12 spinal nerves.
Internal Abdominal Oblique Muscle
The internal abdominal oblique (obliquus internus abdominis) muscle (see Fig. 4-8, A), located immediately deep to the external abdominal oblique muscle, begins from the lateral two thirds of the inguinal ligament, the anterior two thirds of the iliac crest, and the thoracolumbar fascia. The uppermost fibers end on the lower borders of the lower three or four ribs and are continuous with the internal intercostal muscles. The lowest fibers become tendinous and attach to the pubic crest and the medial portion of the pecten pubis. Here they are joined by the transversus abdominis aponeurosis, and together their united attachment forms the conjoint tendon, or inguinal falx. The intermediate fibers diverge from their lateral attachment and become aponeurotic. The internal oblique aponeurosis continues toward the midline, where it blends with the linea alba. In the upper two thirds of the abdomen, this aponeurosis splits into two laminae at the lateral border of the rectus abdominis muscle. These laminae pass on either side of that muscle before reuniting at the linea alba. In the lower one third of the abdomen, the entire aponeurosis, along with the aponeurosis of the transversus abdominis muscle, passes anteriorly to the rectus abdominis muscle. The internal abdominal oblique muscle is innervated by branches of the ventral rami of the T7 to L1 spinal nerves.
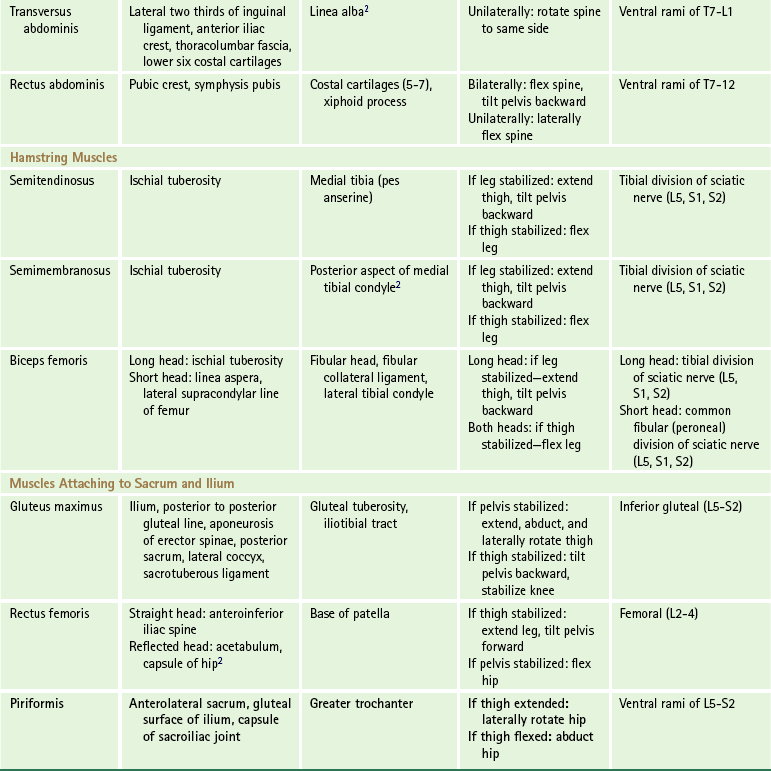
Transversus Abdominis Muscle
The transversus abdominis muscle is located deep to the internal abdominal oblique muscle. It arises from the lateral one third of the inguinal ligament or adjacent iliac fascia, the anterior two thirds of the outer lip of the iliac crest, the thoracolumbar fascia between the iliac crest and twelfth rib, and the internal aspects of the lower six costal cartilages, where it blends with the diaphragm. The fibers of the transversus abdominis muscle course basically in a horizontal direction and become aponeurotic. The lowest fibers of the transversus abdominis aponeurosis curve inferomedially and, along with the fibers from the internal oblique aponeurosis, form the conjoint tendon (see the preceding discussion). The rest of the fibers of this aponeurosis pass horizontally to the midline, where they blend with the linea alba. The upper three fourths of the fibers run posteriorly to the rectus abdominis muscle, whereas the lower one fourth course anteriorly to this muscle. The transversus abdominis muscle is innervated by the anterior primary divisions of the T7 to L1 spinal nerves.
Rectus Abdominis Muscle
The rectus abdominis muscle (see Fig. 4-8, A) is a long, straplike muscle extending the entire length of the anterior abdominal wall. The linea alba forms the medial border of this muscle and separates the two (right and left). The lateral border of the rectus abdominis muscle usually can be seen on the surface of the anterior abdominal wall and is termed the linea semilunaris. This muscle attaches inferiorly to the pubic crest (sometimes as far laterally as the pecten pubis) and also to ligamentous fibers anterior to the symphysis pubis. The left and right rectus abdominis muscles may interlace in this region. Superiorly this muscle attaches to the fifth through seventh costal cartilages and the xiphoid process. Sometimes the most lateral fibers may reach the fourth or even third costal cartilages. The rectus abdominis muscle is crossed by three horizontal fibrous bands called the tendinous intersections. Typically they are found at the level of the umbilicus, the inferior tip of the xiphoid process, and halfway between these two points.
The rectus abdominis muscle is enclosed by the aponeurosis of the abdominal obliques and transversus abdominis muscles. Sometimes this aponeurosis is called the rectus sheath. In the upper portion of the anterior abdominal wall, the external oblique and anterior lamina of the internal oblique aponeuroses pass anteriorly to the rectus abdominis muscle, whereas the posterior lamina of the internal oblique and transverse aponeuroses lie posterior to the rectus abdominis muscle. This arrangement changes about halfway between the umbilicus and pubic symphysis, forming a curved line known as the arcuate line. Inferior to this line, all three aponeurotic layers are found anterior to the rectus abdominis muscle, and only the transversalis fascia (the layer of fascia deep to the anterolateral abdominal muscles) separates this muscle from the parietal peritoneum, although this traditional description of the rectus sheath may be too simplistic (Standring et al., 2008). The rectus abdominis muscle is supplied by the anterior primary divisions of the lower six or seven thoracic spinal nerves.
The abdominal muscles act to retain the abdominal viscera in place and oppose the effects of gravity on them in the erect and sitting positions. When the thorax and pelvis are fixed, these muscles, especially the obliques, increase the intraabdominal pressure. This is important for childbirth, forced expiration, emptying the bladder and rectum, and vomiting. It is also the basis of the Valsalva maneuver (i.e., increasing abdominal pressure for diagnostic purposes). The external abdominal oblique muscle can further aid expiration by depressing the lower ribs. If the pelvis is fixed, these muscles, primarily the recti, bend the trunk forward and flex the lumbar spine (Brown et al., 2011). If the thorax is fixed, the lumbar spine still flexes, but the pelvis is moved upward. With unilateral contraction the trunk is laterally flexed to that side. In addition, the external abdominal oblique muscle can help produce rotation of the trunk away from the side of contraction, whereas the internal oblique muscle turns it to the same side. The transversus abdominis muscle probably has an effect only on the abdominal viscera and does not produce any appreciable movement of the vertebral column, although rotational movements are a distinct possibility (Standring et al., 2008). Contraction of the transversus abdominis muscle has been shown to significantly decrease laxity (or, rather, increase stiffness) of the sacroiliac joint, implying a stabilizing role of the transversus abdominis muscle for the sacroiliac joints (Richardson et al., 2002). Because of its indirect attachment to the lumbar transverse processes via the thoracolumbar fascia, it is possible that this muscle also plays a role in lumbar segmental control (Barker et al., 2007).
Other Muscles That Have Clinical Relevance to the Back
The tilting of the pelvis on the heads of the femurs in an anteroposterior direction is an important component of posture and locomotion. Movement of the anterior portion of the pelvis in a proximal direction (e.g., bringing the pubic symphysis toward the umbilicus) is termed backward tilting and involves flexion of the lumbar spine. Tilting of the pelvis in the opposite direction tends to extend the lumbar spine. This forward tilting of the pelvis is accomplished by contraction of the erector spinae and psoas major muscles. Backward tilting of the pelvis is accomplished not only by the rectus abdominis and the two oblique abdominal muscles but also by the hamstring and gluteus maximus muscles (Fig. 4-9). The imbalance of the muscles, responsible for pelvic tilt, is often evident in people with low back pain. These individuals may have shortened and tight psoas major and erector spinae muscles combined with weakened gluteal and abdominal muscles (Oliver & Middleditch, 1991).
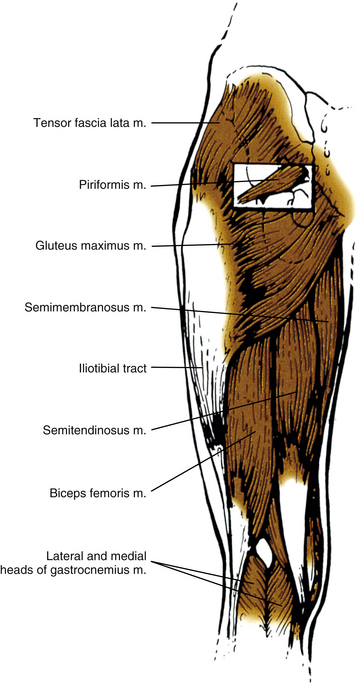
Hamstring Muscles
The posterior group of thigh muscles, commonly known as the hamstrings, acts to extend the hip and flex the knee joints. This group consists of the semitendinosus, semimembranosus, and biceps femoris muscles. The latter muscle has two heads superiorly, long and short (see Fig. 4-9).
With the exception of the short head of the biceps femoris muscle, all three of these muscles attach proximally to the ischial tuberosity. The short head of the biceps femoris muscle arises from the lateral lip of the linea aspera and lateral supracondylar line of the femur. The semitendinosus and semimembranosus muscles are located posteromedially in the thigh, whereas the biceps femoris muscle is found posterolaterally.
Semitendinosus Muscle
The semitendinosus muscle, as its name implies, becomes tendinous approximately halfway along its course (see Fig. 4-9). This long tendon curves around the medial tibial condyle, passes superficial to the tibial collateral ligament, and ends by attaching to the superior portion of the medial surface of the tibia immediately below and posterior to the attachment sites of the sartorius and gracilis muscles. This grouping of muscular attachments sometimes is known as the pes anserine. The semitendinosus muscle is innervated by the tibial portion (L5, S1, and S2) of the sciatic nerve.
Semimembranosus Muscle
The semimembranosus muscle (see Fig. 4-9) arises as a tendon and expands into an aponeurosis that is deep to the semitendinosus muscle. The muscular fibers arise from this aponeurosis. The semimembranosus muscle ends primarily on the posterior aspect of the medial tibial condyle via a short tendon. It also sends slips laterally and superiorly, some of which help form the oblique popliteal ligament. The semimembranosus muscle is innervated by the tibial portion (L5, S1, and S2) of the sciatic nerve.
Biceps Femoris Muscle
The short head of the biceps femoris muscle joins the belly of the long head of the biceps femoris muscle on its deep surface as it descends in the thigh. After the two heads unite, the biceps femoris muscle gradually narrows to a tendon that attaches to the head of the fibula, the fibular collateral ligament, and the lateral tibial condyle (see Fig. 4-9). The long head of the biceps femoris muscle is innervated by the tibial portion (L5, S1, and S2) and the short head by the common fibular (peroneal) portion (L5, S1, S2) of the sciatic nerve.
These muscles produce flexion at the knee and extension at the hip when they contract. When the thigh is flexed, the hamstring muscles (especially the biceps femoris) help tilt the pelvis backward. Tight hamstrings sometimes are associated with low back pain.
Gluteus Maximus Muscle
The gluteus maximus muscle is the most superficial muscle in the gluteal region (see Fig. 4-9). It is considered the body’s largest muscle. Its large size is a characteristic feature of the human musculature and is thought to be a result of its role in attaining an upright posture (Standring et al., 2008). It arises from the area of the ilium posterior to the posterior gluteal line. It also begins from the erector spinae aponeurosis, posterior and inferior sacrum, lateral coccyx, sacrotuberous ligament, and the fascial covering of the gluteus medius. The fibers of the gluteus maximus muscle run inferolaterally and attach distally to the iliotibial tract and gluteal tuberosity of the femur between the attachment sites of the vastus lateralis and adductor magnus.
The gluteus maximus muscle can extend the thigh from a flexed position when the pelvis is fixed. It also helps in strong lateral rotation of the thigh. Its upper fibers are active in strong abduction at the hip. If the thigh is stabilized, this muscle, along with the hamstrings, helps rotate the pelvis posteriorly on the femur heads, as in rising from a stooped position. By virtue of its attachment to the iliotibial tract, the gluteus maximus muscle aids in stabilizing the femur on the tibia. It is also important for its intermittent action in various phases of normal gait. This muscle is innervated by the inferior gluteal nerve (L5 to S2).
Piriformis Muscle
The piriformis muscle is pear-shaped and lies deep to the gluteus medius muscle (see Fig. 4-9). It arises from the anterolateral sacrum by three musculotendinous slips. It also originates from the gluteal surface of the ilium (in proximity to the posterior inferior iliac spine), from the ventral sacroiliac ligament, and sometimes from the anterior surface of the sacrotuberous ligament. The piriformis muscle exits the pelvis via the greater sciatic foramen and is the largest structure within that foramen. It attaches distally by a tendon to the upper border of the femur’s greater trochanter. Normally this muscle lies immediately superior to the sciatic nerve as it exits the greater sciatic foramen, but sometimes (≈10%) the common fibular (peroneal) portion of the sciatic nerve pierces the piriformis and splits it (Moore & Dalley, 2006). Entrapment or irritation of the sciatic nerve (or a portion of it) in the region of the piriformis muscle often is termed piriformis syndrome (Rodrigue & Hardy, 2001; Halpin et al., 2009). With contraction, this muscle produces lateral rotation of the extended thigh. If the thigh is flexed, abduction at the hip occurs. It is innervated by branches from the ventral rami of the L5 to S2 spinal nerves.
Rectus Femoris Muscle
The quadriceps femoris muscle is the great extensor of the leg. This muscle consists of four parts (usually termed as individual muscles): vastus lateralis, vastus intermedius, vastus medialis, and rectus femoris muscles. The three vasti muscles originate on the femur, but the rectus femoris arises from the pelvis. The rectus femoris muscle begins as two (or three) heads. The straight head attaches to the anterior inferior iliac spine, and the reflected head attaches to the superior rim of the acetabulum and capsule of the hip. Sometimes a recurrent head that arises from the anterosuperior angle of the femur’s greater trochanter is described (Segal & Jacob, 1983). All the heads join, and the belly of the muscle then runs down the anterior thigh to attach by a broad aponeurosis to the base of the patella. By virtue of its proximal attachment sites, the rectus femoris muscle not only extends the knee but also flexes the hip. If the thigh is fixed, contraction of this muscle helps to tilt the pelvis forward. The rectus femoris muscle, along with the rest of the quadriceps femoris muscle, is innervated by the femoral nerve (L2 to L4).
Summary of Muscles Affecting the Spine
Table 4-2 provides a summary of the muscles that influence the spine. This table does not give a complete account of all the points of origin and insertion of some of the more complex muscles. A more detailed description of each muscle appears in the text of this chapter. Box 4-1 organizes the muscles that influence the spine according to the motion produced by their contraction.
References
Akuthota, V., et al. Core stability exercise principles. Curr Sports Med Rep. 2008;7(1):39–44.
Andersson, E.A., et al. Diverging intramuscular activity patterns in back and abdominal muscles during trunk rotation. Spine. 2002;27(6):E152–E160.
Arnold, L.M. The pathophysiology, diagnosis and treatment of fibromyalgia. Psychiatr Clin North Am. 2010;33(2):375–408.
Barker, P.J., Briggs, C.A. Attachments of the posterior layer of lumbar fascia. Spine. 1999;24:1757–1766.
Barker, P.J., et al. The middle layer of the lumbar fascia and attachments to lumbar transverse processes: implications for segmental control and fracture. Eur Spine J. 2007;16:2232–2237.
Bogduk, N. Clinical anatomy of the lumbar spine, 4th ed. London: Churchill Livingstone; 2005.
Borghuis, J., et al. The importance of sensory-motor control in providing core stability: implications for measurement and training. Sports Med. 2008;38(11):893–916.
Boyd-Clark, L.C., et al. Muscle spindle distribution, morphology, and density in longus colli and multifidus muscles of the cervical spine. Spine. 2002;27(7):694–701.
Brown, S.H., et al. Architectural analysis of human abdominal wall muscles. Spine. 2011;36(5):355–362.
Cagnie, B., et al. A magnetic resonance imaging investigation into the function of the deep cervical flexors during the performance of craniocervical flexion. J Manipulative Physiol Ther. 2010;33(4):286–291.
Campos, G.E., et al. Electromyographic study of the trapezius and deltoideus in elevation, lowering, retraction and protraction of the shoulders. Electromyogr Clin Neurophysiol. 1994;34(4):243–247.
Cholewicki, J., et al. Stabilizing function of trunk flexor-extensor muscles around a neutral spine posture. Spine. 1997;22(19):2207–2212.
Clark, B.C., et al. Derecruitment of the lumbar musculature with fatiguing trunk extension exercise. Spine. 2003;28(3):282–287.
Comfort, P., Pearson, S.J., Mather, D. An electromyographical comparison of trunk muscle activity during isometric trunk and dynamic strengthening exercises. J Strength Cond Res. 2011;25(1):149–154.
Cornwall, J., Stringer, M.D., Duxson, M. Functional morphology of the thoracolumbar transversospinal muscles. Spine. 2011;36(16):E1053–E1061.
Daggfeldt, K., et al. The visible human anatomy of the lumbar erector spinae. Spine. 2000;25(21):2719–2725.
Danneels, L.A., et al. A functional subdivision of hip, abdominal, and back muscles during asymmetric lifting. Spine. 2001;26(6):E114–E121.
Darwish, H.H., Ibrahim, A.F. Three muscles in the upper costovertebral region: description and clinical anatomy. Clin Anat. 2009;22:352–357.
Guazzelli, F.H., et al. Electromyographic study of the trapezius muscle in free movements of the shoulder. Electromyogr Clin Neurophysiol. 1994;45(5):279–283.
Hack, G.D., et al. Anatomic relation between the rectus capitis posterior minor muscle and the dura mater. Spine. 1995;20(23):2484–2486.
Halpin, R.J., et al. Piriformis syndrome: a real pain in the buttock? Neurosurgery. 2009;65(4):A197–A202.
Hirayama, J., et al. Effects of electrical stimulation of the sciatic nerve on background electromyography and static stretch reflex activity of the trunk muscles in rats. Spine. 2001;26(6):602–609.
Hultborn, H. Spinal reflexes, mechanisms and concepts: from Eccles to Lundberg and beyond. Prog Neurobiol. 2006;78(3-5):215–232.
Humphreys, B.K., et al. Investigation of connective tissue attachments to the cervical spinal dura mater. Clin Anat. 2003;16(2):152–159.
Johnson, G., et al. Anatomy and actions of the trapezius muscle. Clin Biomech. 2004;9(1):44–50.
Kamibayashi, L.K., Richmond, F.J.R. Morphometry of human neck muscles. Spine. 1998;23(12):1314–1323.
Kang, Y.-M., et al. Electrophysiologic evidence for an intersegmental reflex pathway between lumbar paraspinal tissues. Spine. 2002;27(3):E56–E63.
Krsnich-Shriwise, S. Fibromyalgia syndrome: an overview. Phys Ther. 1997;77:68–75.
Lehman, G.J., et al. Effects of a mechanical pain stimulus on erector spinae activity before and after a spinal manipulation in patients with back pain: a preliminary investigation. J Manipulative Physiol Ther. 2001;24(6):402–406.
Lorimer Moseley, G., et al. Deep and superficial fibers of the lumbar multifidus muscle are differentially active during voluntary arm movements. Spine. 2002;27(2):E29–E36.
Macintosh, J.E., Bogduk, N. The biomechanics of the lumbar multifidus. Clin Biomech. 1986;1:205–213.
Macintosh, J.E., Bogduk, N. The biomechanics of the thoracolumbar fascia. Clin Biomech. 1987;2:78–83.
Macintosh, J.E., Bogduk, N. The morphology of the lumbar erector spinae. Spine. 1987;12:658–668.
Macintosh, J.E., et al. The morphology of the human lumbar multifidus. Clin Biomech. 1986;1:196–204.
Masani, K., et al. Postural reactions of the trunk muscles to multi-directional perturbations in sitting. Clin Biomech (Bristol, Avon). 2009;24(2):176–182.
McPartland, J.M., et al. Chronic neck pain, standing balance, and suboccipital muscle atrophy: a pilot study. J Manipulative Physiol Ther. 1997;20(1):24–29.
Moore, K.L., Dalley, A.F. Clinically oriented anatomy, 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.
Nomizo, A., Sakai, T. Segmental level discrepancy of human iliocostalis muscles and their innervation. Anat Sci Int. 2009;84:161–169.
Oliver, J., Middleditch, A. Functional anatomy of the spine. Oxford, UK: Butterworth-Heinemann; 1991.
Peck, D., et al. Are there compartment syndromes in some patients with idiopathic back pain? Spine. 1986;11:468–475.
Quint, U., et al. Importance of the intersegmental trunk muscles for the stability of the lumbar spine. Spine. 1998;23(18):1937–1945.
Richardson, C.A., et al. The relation between the transverses abdominis muscles, sacroiliac joint mechanics, and low back pain. Spine. 2002;27(4):399–405.
Rodrigue, T., Hardy, R.W. Diagnosis and treatment of piriformis syndrome. Neurosurg Clin North Am. 2001;12(2):311–319.
Schneider, M.J. Tender points/fibromyalgia vs. trigger points/myofascial pain syndrome: a need for clarity in terminology and differential diagnosis. J Manipulative Physiol Ther. 1995;18(6):398–406.
Segal, P., Jacob, M. The knee. Chicago: Year Book; 1983.
Shimokawa, T., et al. Contributions of the hypoglossal nerve to the innervations of the recti capiti lateralis and anterior. Clin Anat. 2004;17:613–617.
Shin, G., D'Souza, C. EMG activity of low back extensor muscles during cyclic flexion/extension. J Electromyogr Kinesiol. 2010;20(4):742–759.
Standring S., et al, eds. Gray's anatomy: the anatomical basis of clinical practice, 40th ed, Edinburgh: Churchill Livingstone, 2008.
Takahashi, I., et al. Effects of the mechanical load on forward bending motion of the trunk: comparison between patients with motion-induced intermittent low back pain and healthy subjects. Spine (Phila Pa 1976). 2007;32:E73–E78.
Travell, J.G., Simons, D.G.. Myofascial pain and dysfunction: the trigger point manual. Baltimore: Williams & Wilkins; 1983;vol. 1.
Travell, J.G., Simons, D.G.. Myofascial pain and dysfunction: the trigger point manual. Baltimore: Williams & Wilkins; 1992;vol. 2.
Tsao, H., Galea, M.P., Hodges, P.W. Reorganization of the motor cortex is associated with postural control deficits in recurrent low back pain. Brain. 2008;131(Pt 8):2161–2171.
van Dieen, J.H. Asymmetry of erector spinae muscle activity in twisted postures and consistency of muscle activation patterns across subjects. Spine. 1996;21(22):2651–2661.
van Dieen, J.H., et al. Trunk muscle activation in low-back pain patients: an analysis of the literature. J Electromyogr Kinesiol. 2003;13(4):333–351.
Vilensky, J.A., et al. Serratus posterior muscles: anatomy, clinical relevance, and function. Clin Anat. 2001;14(4):237–241.
Vleeming, A., Stoeckart, R. The role of the pelvic girdle in coupling the spine and legs: a clinical-anatomical perspective on pelvic stability. In: Vleeming A., et al, eds. Movement, stability and lumbopelvic pain. Edinburgh: Churchill Livingstone; 2007:113–137.
Wheeler, A.H. Myofascial pain disorders: theory to therapy. Drugs. 2004;64(1):45–62.
Zazulak, B., et al. Neuromuscular control of trunk stability: clinical implications for sports injury prevention. J Am Acad Orthop Surg. 2008;16(9):497–505.
Zumpano, M.P., Hartwell, S., Jagos, C.S. Soft tissue connection between rectus capitis posterior minor and the posterior atlanto-occipital membrane. Clin Anat. 2006;19:522–527.