CHAPTER 15 Periodontal Response to External Forces
Adaptive Capacity of the Periodontium to Occlusal Forces
The periodontium attempts to accommodate to the forces exerted on the crown. This adaptive capacity varies in different persons and in the same person at different times. The effect of occlusal forces on the periodontium is influenced by the magnitude, direction, duration, and frequency of the forces.
When the magnitude of occlusal forces is increased, the periodontium responds with a widening of the periodontal ligament space, an increase in the number and width of periodontal ligament fibers, and an increase in the density of alveolar bone.
Changing the direction of occlusal forces causes a reorientation of the stresses and strains within the periodontium (Figure 15-1).24 The principal fibers of the periodontal ligament are arranged so that they best accommodate occlusal forces along the long axis of the tooth. Lateral (horizontal) and torque (rotational) forces are more likely to injure the periodontium.
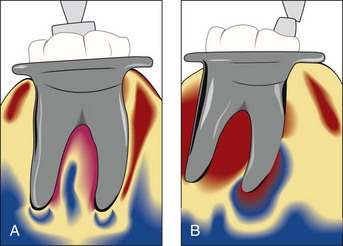
Figure 15-1 Stress patterns around the roots changed by shifting the direction of occlusal forces (experimental model using photoelastic analysis). A, Buccal view of an ivorine molar subjected to an axial force. The shaded fringes indicate that the internal stresses are at the root apices. B, Buccal view of ivorine molar subjected to a mesial tilting force. The shaded fringes indicate that the internal stresses are along the mesial surface and at the apex of the mesial root.
The response of alveolar bone is also affected by the duration and frequency of occlusal forces. Constant pressure on the bone is more injurious than intermittent forces. The more frequent the application of an intermittent force, the more injurious is the force to the periodontium.
Trauma from Occlusion
An inherent “margin of safety” common to all tissues permits some variation in occlusion without adversely affecting the periodontium. However, when occlusal forces exceed the adaptive capacity of the tissues, tissue injury results.44,45 The resultant injury is termed trauma from occlusion, also known as traumatism or occlusal trauma.
Thus trauma from occlusion refers to the tissue injury not the occlusal force. An occlusion that produces such an injury is called a traumatic occlusion.2 Excessive occlusal forces may also disrupt the function of the masticatory musculature and cause painful spasms, injure the temporomandibular joints, or produce excessive tooth wear. However, the term trauma from occlusion is generally used in connection with injury in the periodontium.
Acute and Chronic Trauma
Trauma from occlusion may be acute or chronic. Acute trauma from occlusion results from an abrupt occlusal impact such as that produced by biting on a hard object (e.g., olive pit). Restorations or prosthetic appliances that interfere with or alter the direction of occlusal forces on the teeth may also induce acute trauma.
Acute trauma results in tooth pain, sensitivity to percussion, and increased tooth mobility. If the force is dissipated by a shift in the position of the tooth or by wearing away or correction of the restoration, the injury heals and the symptoms subside. Otherwise, periodontal injury may worsen and develop into necrosis, accompanied by periodontal abscess formation, or may persist as a symptom-free, chronic condition. Acute trauma can also produce cementum tears (Figure 15-2) (see Chapter 2).
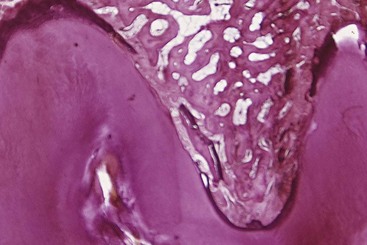
Figure 15-2 Cemental tear presumably caused by acute trauma from occlusion in human autopsy specimen. Note the repair process depositing bone on the displaced, torn cementum and recreating a periodontal ligament.
Chronic trauma from occlusion is more common than the acute form and is of greater clinical significance. It most often develops from gradual changes in occlusion produced by tooth wear, drifting movement, and extrusion of teeth, combined with parafunctional habits, such as bruxism and clenching, rather than as a sequela of acute periodontal trauma (see Chapter 20). The features of chronic trauma from occlusion and their significance are discussed next.
The criterion that determines if an occlusion is traumatic is whether it produces periodontal injury, not how the teeth occlude. Any occlusion that produces periodontal injury is traumatic. Malocclusion is not necessary to produce trauma; periodontal injury may occur when the occlusion appears normal. The dentition may be anatomically and aesthetically acceptable but functionally injurious. Similarly, not all malocclusions are necessarily injurious to the periodontium. Traumatic occlusal relationships are referred to by such terms as occlusal disharmony, functional imbalance, and occlusal dystrophy. These terms refer to the effect of the occlusion on the periodontium, not to the position of the teeth. Because trauma from occlusion refers to the tissue injury rather than the occlusion, an increased occlusal force is not traumatic if the periodontium can accommodate it.
Primary and Secondary Trauma from Occlusion
Trauma from occlusion may be caused by alterations in occlusal forces, reduced capacity of the periodontium to withstand occlusal forces, or both. When trauma from occlusion is the result of alterations in occlusal forces, it is called primary trauma from occlusion. When it results from reduced ability of the tissues to resist the occlusal forces, it is known as secondary trauma from occlusion.
Primary trauma from occlusion occurs if trauma from occlusion is considered the primary etiologic factor in periodontal destruction and if the only local alteration to which a tooth is subjected is from occlusion. Examples include periodontal injury produced around teeth with a previously healthy periodontium after the (1) insertion of a “high filling,” (2) insertion of a prosthetic replacement that creates excessive forces on abutment and antagonistic teeth, (3) drifting movement or extrusion of teeth into spaces created by unreplaced missing teeth, or (4) orthodontic movement of teeth into functionally unacceptable positions. Most studies on experimental animals of the effect of trauma from occlusion have examined the primary type of trauma. Changes produced by primary trauma do not alter the level of connective tissue attachment and do not initiate pocket formation. This is probably because the supracrestal gingival fibers are not affected and therefore prevent apical migration of the junctional epithelium.49
Secondary trauma from occlusion occurs when the adaptive capacity of the tissues to withstand occlusal forces is impaired by bone loss resulting from marginal inflammation. This reduces the periodontal attachment area and alters the leverage on the remaining tissues. The periodontium becomes more vulnerable to injury, and previously well tolerated occlusal forces become traumatic.
Figure 15-3 depicts three different situations on which excessive occlusal forces can be superimposed, as follows:
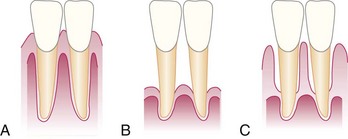
Figure 15-3 Traumatic forces can occur on A, normal periodontium with normal height of bone; B, normal periodontium with reduced height of bone; or C, marginal periodontitis with reduced height of bone.
The first case is an example of primary trauma from occlusion, whereas the last two represent secondary trauma from occlusion. The effects of trauma from occlusion in these different situations are analyzed in the following discussion.
It has been found in experimental animals that systemic disorders can reduce tissue resistance and that previously tolerable forces may become excessive.22,52,62 This could theoretically represent another mechanism by which tissue resistance to increased forces is lowered, resulting in secondary trauma from occlusion.
Stages of Tissue Response to Increased Occlusal Forces
Tissue response occurs in three stages4,8: injury, repair, and adaptive remodeling of the periodontium.
Stage I: Injury
Tissue injury is produced by excessive occlusal forces. The body then attempts to repair the injury and restore the periodontium. This can occur if the forces are diminished or if the tooth drifts away from them. If the offending force is chronic, however, the periodontium is remodeled to cushion its impact. The ligament is widened at the expense of the bone, resulting in angular bone defects without periodontal pockets, and the tooth becomes loose.
Under the forces of occlusion, a tooth rotates around a fulcrum or axis of rotation, which in single-rooted teeth is located in the junction between the middle third and the apical third of the clinical root and in multirooted teeth in the middle of the interradicular bone (Figure 15-4). This creates areas of pressure and tension on opposite sides of the fulcrum. Different lesions are produced by different degrees of pressure and tension. If jiggling forces are exerted, these different lesions may coexist in the same area.
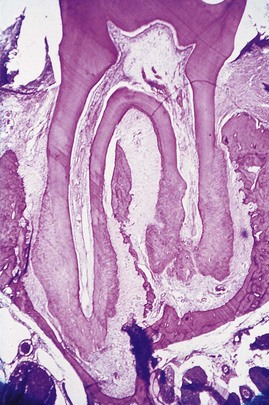
Figure 15-4 Areas of tension and pressure in opposite sites of the periodontal ligament caused by experimentally induced orthodontic movement in a rat molar.
 Science Transfer
Science Transfer
Periodontal tissues within the bony housing of the socket transmit forces to the surrounding bone and cause osseous changes such as resorption in regions of compression and bone apposition in regions of tension. The periodontal ligament provides a viscoelastic gel–like milieu that protects the dentition from excessive forces by its cushioning or dampening effect.
Occlusal trauma first results in vasodilation with associated extrusion and pain on biting. This will resolve quickly if the occlusal trauma in eliminated by therapy such as occlusal adjustment. These changes can also be associated with increased pulpal sensitivity and pain with hot and cold from vascular events in the periodontium causing vasodilation of the pulp, and these patients can get almost immediate relief of pain by occlusal adjustment.
Trauma from occlusion is not the initial cause of plaque-induced periodontal pockets and bone loss, but patients with occlusal trauma and periodontitis may have accentuation of bone loss. Many patients will benefit when occlusal therapy is part of the overall periodontal treatment protocol.
Slightly excessive pressure stimulates resorption of the alveolar bone, with a resultant widening of the periodontal ligament space. Slightly excessive tension causes elongation of the periodontal ligament fibers and apposition of alveolar bone. In areas of increased pressure, the blood vessels are numerous and reduced in size; in areas of increased tension, they are enlarged.68
Greater pressure produces a gradation of changes in the periodontal ligament, starting with compression of the fibers, which produces areas of hyalinization.55-57 Subsequent injury to the fibroblasts and other connective tissue cells leads to necrosis of areas of the ligament.53,57 Vascular changes are also produced: within 30 minutes, impairment and stasis of blood flow occur; at 2 to 3 hours, blood vessels appear to be packed with erythrocytes, which start to fragment; and between 1 and 7 days, disintegration of the blood vessel walls and release of the contents into the surrounding tissue occur.54,64 In addition, increased resorption of alveolar bone and resorption of the tooth surface occur.30,35
Severe tension causes widening of the periodontal ligament, thrombosis, hemorrhage, tearing of the periodontal ligament, and resorption of alveolar bone.
Pressure severe enough to force the root against bone causes necrosis of the periodontal ligament and bone. The bone is resorbed from viable periodontal ligament adjacent to necrotic areas and from marrow spaces, a process called undermining resorption.26,44
The areas of the periodontium most susceptible to injury from excessive occlusal forces are the furcations.23
Injury to the periodontium produces a temporary depression in mitotic activity and the rate of proliferation and differentiation of fibroblasts,63 in collagen formation, and in bone formation.30,59,61,63 These return to normal levels after dissipation of the forces.
Stage II: Repair
Repair is constantly occurring in the normal periodontium, and trauma from occlusion stimulates increased reparative activity.
The damaged tissues are removed, and new connective tissue cells and fibers, bone, and cementum are formed in an attempt to restore the injured periodontium (Figure 15-5). Forces remain traumatic only as long as the damage produced exceeds the reparative capacity of the tissues.
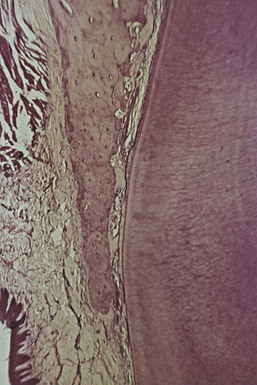
Figure 15-5 Experimental occlusal trauma in rats. Area of necrosis of the marginal periodontal ligament and resorption and remodeling in more apical periodontal sites.
When bone is resorbed by excessive occlusal forces, the body attempts to reinforce the thinned bony trabeculae with new bone (Figure 15-6). This attempt to compensate for lost bone is called buttressing bone formation and is an important feature of the reparative process associated with trauma from occlusion.17 It also occurs when bone is destroyed by inflammation or osteolytic tumors.
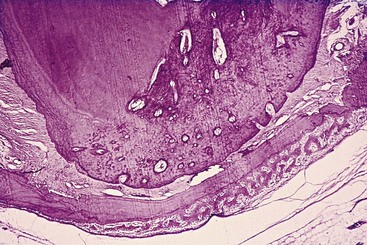
Figure 15-6 Apical area of a premolar subjected to experimental occlusal trauma in a dog, causing intrusion of the tooth and areas of necrosis in the periodontal ligament. Note the active bone formation on the outer aspect of the bone and the resorptive activity in the periphery of the necrotic site.
Buttressing bone formation occurs within the jaw (central buttressing) and on the bone surface (peripheral buttressing). In central buttressing the endosteal cells deposit new bone, which restores the bony trabeculae and reduces the size of the marrow spaces. Peripheral buttressing occurs on the facial and lingual surfaces of the alveolar plate. Depending on its severity, peripheral buttressing may produce a shelflike thickening of the alveolar margin, referred to as lipping (Figure 15-7), or a pronounced bulge in the contour of the facial and lingual bone8,17 (see Chapter 14).

Figure 15-7 A, Widening of the periodontal ligament space in cervical area and a change in the shape of marginal alveolar bone as a result of chronic prolonged trauma from occlusion in rats. B, Comparable change in shape of marginal bone found in a human autopsy case.
Cartilage-like material sometimes develops in the periodontal ligament space as an aftermath of the trauma.14 Formation of crystals from erythrocytes has also been shown.58
Stage III: Adaptive Remodeling of the Periodontium
If the repair process cannot keep pace with the destruction caused by the occlusion, the periodontium is remodeled in an effort to create a structural relationship in which the forces are no longer injurious to the tissues.19 This results in a widened periodontal ligament, which is funnel shaped at the crest, and angular defects in the bone, with no pocket formation. The involved teeth become loose.68 Increased vascularization has also been reported.9
The three stages in the evolution of traumatic lesions have been differentiated histometrically by the relative amounts of periodontal bone surface undergoing resorption or formation5,8 (Figure 15-8). The injury phase shows an increase in areas of resorption and a decrease in bone formation, whereas the repair phase demonstrates decreased resorption and increased bone formation. After adaptive remodeling of the periodontium, resorption and formation return to normal.
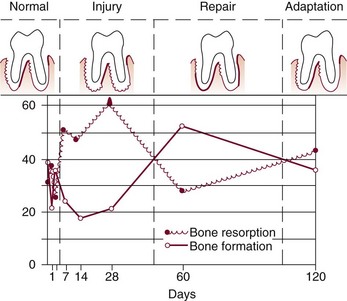
Figure 15-8 Evolution of traumatic lesions as depicted experimentally in rats by variations in relative amounts of areas of bone formation and bone resorption in periodontal bone surfaces. Horizontal axis, days after initiation of traumatic interference. Vertical axis, percentage of bone surface undergoing resorption or formation. The stages in the evolution of the lesions are represented in the top drawings, which show the average amount of bone activity for each group.4
Effects of Insufficient Occlusal Force
Insufficient occlusal force may also be injurious to the supporting periodontal tissues.6,37 Insufficient stimulation causes thinning of the periodontal ligament, atrophy of the fibers, osteoporosis of the alveolar bone, and reduction in bone height. Hypofunction can result from an open-bite relationship, an absence of functional antagonists, or unilateral chewing habits that neglect one side of the mouth.
Reversibility of Traumatic Lesions
Trauma from occlusion is reversible. When trauma is artificially induced in experimental animals, the teeth move away or intrude into the jaw. When the impact of the artificially created force is relieved, the tissues undergo repair. Although trauma from occlusion is reversible under such conditions, it does not always correct itself, and therefore it is not always temporary or of limited clinical significance. The injurious force must be relieved for repair to occur.23,50 If conditions in humans do not permit the teeth to escape from or adapt to excessive occlusal force, periodontal damage persists and worsens.
The presence of inflammation in the periodontium as a result of plaque accumulation may impair the reversibility of traumatic lesions.31,50
Effects of Excessive Occlusal Forces on Dental Pulp
The effects of excessive occlusal forces on the dental pulp have not been established. Some clinicians report the disappearance of pulpal symptoms after correction of excessive occlusal forces. Pulpal reactions have been noted in animals subjected to increased occlusal forces7,36 but did not occur when the forces were minimal and occurred over short periods.36
Influence of Trauma from Occlusion on Progression of Marginal Periodontitis
The clinical impressions of early investigators and clinicians assigned an important role to trauma from occlusion in the etiology of periodontal lesions. Since then, numerous studies have been performed attempting to determine the mechanisms by which trauma from occlusion may affect periodontal disease.
Initial studies involved the placement of high crowns or restorations on the teeth of dogs or monkeys, resulting in a continuous or intermittent force in one direction.2,21 These investigations provided an orthodontic type of force and gave clear descriptions of changes occurring in pressure zones and tension zones. These procedures usually resulted in tooth displacement and consolidation in a new, nontraumatized position.
Trauma from occlusion in humans, however, is the result of forces that act alternatively in opposing directions. These were analyzed in experimental animals with “jiggling forces,” usually produced by a high crown combined with an orthodontic appliance that would bring the traumatized tooth back to its original position when the force was dissipated by separating the teeth. In another method, the teeth were separated by wooden or elastic material wedged interproximally to displace a tooth toward the opposite proximal side. After 48 hours, the wedge was removed and the procedure was repeated on the opposite side.
These studies resulted in a combination of changes produced by pressure and tension on both sides of the tooth, with an increase in the width of the ligament and increased tooth mobility. None of these methods caused gingival inflammation or pocket formation, and the results essentially represented different degrees of functional adaptation to increased forces.49,68
To mimic the problem in humans more closely, studies were then conducted on the effect produced by jiggling trauma and simultaneous plaque-induced gingival inflammation.
The accumulation of bacterial plaque that initiates gingivitis and results in periodontal pocket formation affects the marginal gingiva, but trauma from occlusion occurs in the supporting tissues and does not affect the gingiva (Figure 15-9). The marginal gingiva is unaffected by trauma from occlusion because its blood supply is not affected, even when the vessels of the periodontal ligament are obliterated by excessive occlusal forces.25 It has been repeatedly proved that trauma from occlusion does not cause pockets or gingivitis* nor does it increase gingival fluid flow.† Furthermore, experimental trauma in dogs does not influence bacterial repopulation of pockets after scaling and root planing.32 However, mobile teeth in humans harbor significantly higher proportions of Campylobacter rectus and Peptostreptococcus micros than nonmobile teeth.27
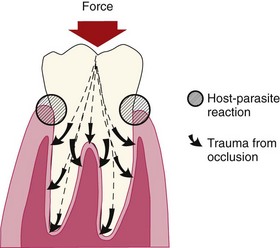
Figure 15-9 The reaction between dental plaque and the host takes place in the gingival sulcus region. Trauma from occlusion appears in the tissues supporting the tooth.
†References 28, 34, 37, 42, 43, 51.
As long as inflammation is confined to the gingiva, the inflammatory process is not affected by occlusal forces.33 When inflammation extends from the gingiva into the supporting periodontal tissues (i.e., when gingivitis becomes periodontitis), plaque-induced inflammation enters the zone influenced by occlusion, which Glickman has called the zone of co-destruction.15,16,18
Two groups have studied this topic experimentally with conflicting results, probably because of the different methods used. The Eastman Dental Center group in Rochester, NY, used squirrel monkeys, produced trauma by repetitive interdental wedging, and added mild-to-moderate gingival inflammation; experimental times were up to 10 weeks. They reported that the presence of trauma did not increase the loss of attachment induced by periodontitis.43,46-48 The University of Gothenburg group in Sweden used beagle dogs, produced trauma by placing cap splints and orthodontic appliances, and induced severe gingival inflammation; experimental times were up to 1 year. This group found that occlusal stresses increase the periodontal destruction induced by periodontitis.11,12,40
When trauma from occlusion is eliminated, a substantial reversal of bone loss occurs, except in the presence of periodontitis. This indicates that inflammation inhibits the potential for bone regeneration.31,39,49,50 Thus it is important to eliminate the marginal inflammatory component in cases of trauma from occlusion because the presence of inflammation affects bone regeneration after the removal of the traumatizing contacts.31 It also has been shown in experimental animals that trauma from occlusion does not induce progressive destruction of the periodontal tissues in regions kept healthy after the elimination of preexisting periodontitis.11
Trauma from occlusion also tends to change the shape of the alveolar crest. The change in shape consists of a widening of the marginal periodontal ligament space, a narrowing of the interproximal alveolar bone, and a shelflike thickening of the alveolar margin.9,40,43 Therefore, although trauma from occlusion does not alter the inflammatory process, it changes the architecture of the area around the inflamed site.18,40 Thus, in the absence of inflammation, the response to trauma from occlusion is limited to adaptation to the increased forces. In the presence of inflammation, however, the changes in the shape of the alveolar crest may be conducive to angular bone loss, and existing pockets may become intrabony.
Other theories that have been proposed to explain the interaction of trauma and inflammation include the following:
Clinical and Radiographic Signs of Trauma from Occlusion Alone
The most common clinical sign of trauma to the periodontium is increased tooth mobility. In the injury stage of trauma from occlusion, destruction of periodontal fibers occurs, which increases tooth mobility. In the final stage the accommodation of the periodontium to increased forces entails a widening of the periodontal ligament, which also leads to increased tooth mobility. Although this tooth mobility is greater than the so-called normal mobility, it cannot be considered pathologic because it is an adaptation and not a disease process. If it does become progressively worse, then it can be considered pathologic.
Other causes of increased tooth mobility include advanced bone loss, inflammation of the periodontal ligament of periodontal or periapical origin, and some systemic causes (e.g., pregnancy). The destruction of surrounding alveolar bone, such as occurs in osteomyelitis or jaw tumors, may also increase tooth mobility (see Chapter 30).
Radiographic signs of trauma from occlusion may include the following:
In summary, trauma from occlusion does not initiate gingivitis or periodontal pockets, but it may constitute an additional risk factor for the progression and severity of the disease. An understanding of the effect of trauma from occlusion on the periodontium is useful in the clinical management of periodontal problems.
Pathologic Tooth Migration
Pathologic migration refers to tooth displacement that results when the balance among the factors that maintain physiologic tooth position is disturbed by periodontal disease. Pathologic migration is relatively common and may be an early sign of disease, or it may occur in association with gingival inflammation and pocket formation as the disease progresses.
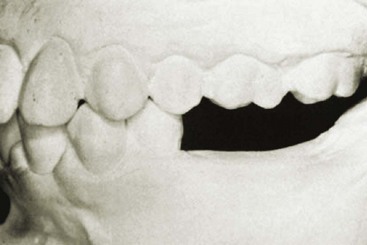
Pathologic migration occurs most frequently in the anterior region, but posterior teeth may also be affected. The teeth may move in any direction, and the migration is usually accompanied by mobility and rotation. Pathologic migration in the occlusal or incisal direction is termed extrusion. All degrees of pathologic migration are encountered, and one or more teeth may be affected (Figure 15-10). It is important to detect migration in its early stages and prevent more serious involvement by eliminating the causative factors. Even in the early stage, some degree of bone loss occurs.

Figure 15-10 Labial migration of maxillary central incisors, especially the right incisor. A, Frontal view. B, Lateral view.
Pathogenesis
Two major factors play a role in maintaining the normal position of the teeth: the health and normal height of the periodontal attachment apparatus and the forces exerted on the teeth. The latter includes the forces of occlusion and pressure from the lips, cheeks, and tongue. Factors that are important in relation to the forces of occlusion include (1) tooth morphologic features and cuspal inclination; (2) the presence of a full complement of teeth; (3) a physiologic tendency toward mesial migration; (4) the nature and location of contact point relationships; (5) proximal, incisal, and occlusal attrition; and (6) the axial inclination of the teeth. Alterations in any of these factors start an interrelated sequence of changes in the environment of a single tooth or group of teeth that may result in pathologic migration. Thus pathologic migration occurs under conditions that weaken the periodontal support, increase or modify the forces exerted on the teeth, or both.
Weakened Periodontal Support
The inflammatory destruction of the periodontium in periodontitis creates an imbalance between the forces maintaining the tooth in position and the occlusal and muscular forces the tooth ordinarily needs to bear. The tooth with weakened support is unable to maintain its normal position in the arch and moves away from the opposing force unless it is restrained by proximal contact. The force that moves the weakly supported tooth may be created by factors such as occlusal contacts or pressure from the tongue.
It is important to understand that the abnormality in pathologic migration rests with the weakened periodontium; the force itself is not necessarily abnormal. Forces that are acceptable to an intact periodontium become injurious when periodontal support is reduced, as in the tooth with abnormal proximal contacts. Abnormally located proximal contacts convert the normal anterior component of force to a wedging force that moves the tooth occlusally or incisally. The wedging force, which can be withstood by the intact periodontium, causes the tooth to extrude when the periodontal support is weakened by disease. As its position changes, the tooth is subjected to abnormal occlusal forces, which aggravate the periodontal destruction and the tooth migration.
Pathologic migration may continue after a tooth no longer contacts its antagonist. Pressures from the tongue, the food bolus during mastication, and proliferating granulation tissue provide the force.
Pathologic migration is also an early sign of localized aggressive periodontitis. Weakened by loss of periodontal support, the maxillary and mandibular anterior incisors drift labially and extrude, creating diastemata between the teeth (see Chapter 18).
Changes in the Forces Exerted on the Teeth
Changes in the magnitude, direction, or frequency of the forces exerted on the teeth can induce pathologic migration of a tooth or group of teeth. These forces do not have to be abnormal to cause migration if the periodontium is sufficiently weakened. Changes in the forces may result from unreplaced missing teeth, or other causes.
Unreplaced Missing Teeth
Drifting of teeth into the spaces created by unreplaced missing teeth often occurs. Drifting differs from pathologic migration in that it does not result from destruction of the periodontal tissues. However, it usually creates conditions that lead to periodontal disease, and thus the initial tooth movement is aggravated by loss of periodontal support (Figure 15-11).

Drifting generally occurs in a mesial direction, combined with tilting or extrusion beyond the occlusal plane. The premolars frequently drift distally (Figure 15-12). Although drifting is a common sequela when missing teeth are not replaced, it does not always occur (Figure 15-13).

Failure to Replace First Molars
The pattern of changes that may follow failure to replace missing first molars is characteristic. In extreme cases it consists of the following:
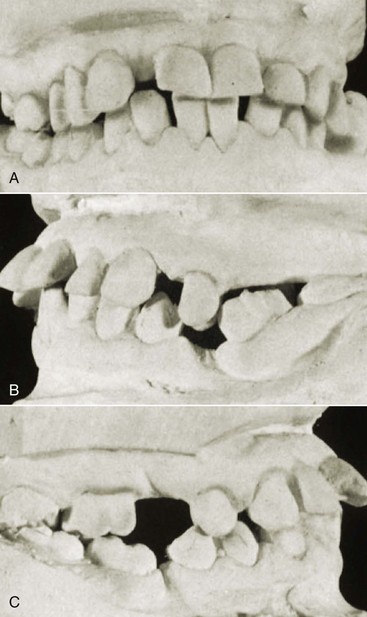
Figure 15-14 Examples of mutilation of occlusion associated with unreplaced missing teeth. Note pronounced pathologic migration, disturbed proximal contacts, and functional relationships with closing of the bite.

Figure 15-15 Maxillary incisors pushed labially in patient with bilateral unreplaced mandibular molars. Note extrusion of the maxillary molars.
The disturbed proximal contact relationships lead to food impaction, plaque accumulation resulting in gingival inflammation, and pocket formation, followed by bone loss and tooth mobility. Occlusal disharmonies created by the altered tooth positions traumatize the supporting tissues of the periodontium and aggravate the destruction caused by the inflammation. Reduction in periodontal support leads to further migration of the teeth and mutilation of the occlusion.
Other Causes
Trauma from occlusion may cause a shift in tooth position either by itself or in combination with inflammatory periodontal disease. The direction of movement depends on the occlusal force.
Pressure from the tongue may cause drifting of the teeth in the absence of periodontal disease or may contribute to pathologic migration of teeth with reduced periodontal support (Figure 15-16).
In tooth support weakened by periodontal destruction, pressure from the granulation tissue of periodontal pockets has been mentioned as contributing to pathologic migration.29,38 The teeth may return to their original positions after the pockets are eliminated, but if more destruction has occurred on one side of a tooth than on the other, the healing tissues tend to pull in the direction of the lesser destruction.
1 Ballbe R, Carranza FA, Erausquin R. Los paradencios del caso ocho. Rev Odont (Buenos Aires). 1938;26:606.
2 Bhaskar SN, Orban B. Experimental occlusal trauma. J Periodontol. 1955;26:270.
3 Biancu S, Ericsson I, Lindhe J. Periodontal ligament tissue reactions to trauma and gingival inflammation: an experimental study in the beagle dog. J Clin Periodontol. 1995;22:772.
4 Carranza FAJr. Histometric evaluation of periodontal pathology. J Periodontol. 1967;38:741.
5 Carranza FAJr, Cabrini RL. Histometric studies of periodontal tissues. Periodontics. 1967;5:308.
6 Cohn SA. Disuse atrophy of the periodontium in molar teeth of mice. J Dent Res. 1961;40:707.
7 Cooper MB, Landay MA, Seltzer S. The effects of excessive occlusal forces on the pulp. II. Heavier and longer term forces. J Periodontol. 1971;42:353.
8 Dotto CA, Carranza FAJr, Itoiz ME. Efectos mediatos del trauma experimental en ratas. Rev Asoc Odontol Argent. 1966;54:48.
9 Dotto CA, Carranza FAJr, Cabrini RL, et al. Vascular changes in experimental trauma from occlusion. J Periodontol. 1967;38:183.
10 Ericsson I. The combined effects of plaque and physical stress on periodontal tissues. J Clin Periodontol. 1986;13:918.
11 Ericsson I, Lindhe J. Lack of effect of trauma from occlusion on the recurrence of experimental periodontitis. J Clin Periodontol. 1977;4:115.
12 Ericsson I, Lindhe J. Effect of longstanding jiggling on experimental marginal periodontitis in the beagle dog. J Clin Periodontol. 1982;9:497.
13 Ericsson I, Thilander B, Lindhe J, et al. The effect of orthodontic tilting movements on the periodontal tissues of infected and noninfected dentitions in dogs. J Clin Periodontol. 1977;4:278.
14 Everett FG, Bruckner RJ. Cartilage in the periodontal ligament space. J Periodontol. 1970;41:165.
15 Glickman I. Occlusion and the periodontium. J Dent Res. 1967;46(suppl):53.
16 Glickman I, Smulow JB. Alterations in the pathway of gingival inflammation into the underlying tissues induced by excessive occlusal forces. J Periodontol. 1962;33:7.
17 Glickman I, Smulow JB. Buttressing bone formation in the periodontium. J Periodontol. 1965;36:365.
18 Glickman I, Smulow JB. Effect of excessive occlusal forces upon the pathway of gingival inflammation in humans. J Periodontol. 1965;36:141.
19 Glickman I, Smulow JB. Adaptive alterations in the periodontium of the rhesus monkey in chronic trauma from occlusion. J Periodontol. 1968;39:101. 28
20 Glickman I, Smulow JB. The combined effects of inflammation and trauma from occlusion to periodontitis. Int Dent J. 1969;19:393.
21 Glickman I, Weiss L. Role of trauma from occlusion in initiation of periodontal pocket formation in experimental animals. J Periodontol. 1955;26:14.
22 Glickman I, Smulow JB, Moreau J. Effect of alloxan diabetes upon the periodontal response to excessive occlusal forces. J Periodontol. 1966;37:146.
23 Glickman I, Stein RS, Smulow JB. The effects of increased functional forces upon the periodontium of splinted and nonsplinted teeth. J Periodontol. 1961;32:290.
24 Glickman I, Roeber F, Brion M, et al. Photoelastic analysis of internal stresses in the periodontium created by occlusal forces. J Periodontol. 1970;41:30.
25 Goldman H. Gingival vascular supply in induced occlusal traumatism. Oral Surg Oral Med Oral Pathol. 1956;9:939.
26 Gottlieb B, Orban B. Changes in the tissue due to excessive force upon the teeth. Leipzig: G Thieme; 1931.
27 Grant DA, Grant DA, Flynn MJ, et al. Periodontal microbiota of mobile and nonmobile teeth. J Periodontol. 1985;66:386.
28 Hakkarainen K. Relative influence of scaling and root influence and occlusal adjustment on sulcular fluid flow. J Periodontol. 1986;57:681.
29 Hirschfeld I. The dynamic relationship between pathologically migrating teeth and inflammatory tissue in periodontal pockets: a clinical study. J Periodontol. 1933;4:35.
30 Itoiz ME, Carranza FAJr, Cabrini RL. Histologic and histometric study of experimental occlusal trauma in rats. J Periodontol. 1963;34:305.
31 Kantor M, Polson AN, Zander HA. Alveolar bone regeneration after removal of inflammatory and traumatic factors. J Periodontol. 1976;46:687.
32 Kaufman H, Carranza FAJr, Enders B, et al. The influence of trauma from occlusion on the bacterial repopulation of periodontal pockets in dogs. J Periodontol. 1984;55:86.
33 Kenney EB. A histopathologic study of incisal dysfunction and gingival inflammation in the rhesus monkey. J Periodontol. 1971;42:3.
34 Kobayashi K, Kobayashi K, Soeda W, et al. Gingival crevicular pH in experimental gingivitis and occlusal trauma in man. J Periodontol. 1998;69:1036.
35 Kvam E. Scanning electron microscopy of tissue changes on the pressure surface of human premolars following tooth movement. Scand J Dent Res. 1972;80:357.
36 Landay MA, Nazimov H, Seltzer S. The effects of excessive occlusal forces on the pulp. J Periodontol. 1970;41:3.
37 Levy G, Mailland ML. Etude quantitative des effets de l’hypofonction occlusale sur la largeur desmodontale et la resorption osteoclastique alveolaire chez le rat. J Biol Buccale. 1980;8:17.
38 Lindhe J, Ericsson I. The influence of trauma from occlusion on reduced but healthy periodontal tissues in dogs. J Clin Periodontol. 1976;3:110.
39 Lindhe J, Ericsson I. The effect of elimination of jiggling forces on periodontally exposed teeth in the dog. J Periodontol. 1982;53:562.
40 Lindhe J, Svanberg G. Influence of trauma from occlusion on progression of experimental periodontitis in the beagle dog. J Clin Periodontol. 1974;1:3.
41 Macapanpan LC, Weinmann JP. The influence of injury to the periodontal membrane on the spread of gingival inflammation. J Dent Res. 1954;33:263.
42 Martin LP, Noble WH. Gingival fluid in relation to tooth mobility and occlusal interferences. J Periodontol. 1974;45:444.
43 Meitner S. Co-destructive factors of marginal periodontitis and repetitive mechanical injury. J Dent Res. 1975;54:C78.
44 Orban B. Tissue changes in traumatic occlusion. J Am Dent Assoc. 1928;15:2090.
45 Orban B, Weinmann JP. Signs of traumatic occlusion in average human jaws. J Dent Res. 1933;13:216.
46 Polson AM. Trauma and progression of marginal periodontitis in squirrel monkeys. II. Codestructive factors of periodontitis and mechanically produced injury. J Periodontal Res. 1974;9:108.
47 Polson AM. The relative importance of plaque and occlusion in periodontal disease. J Clin Periodontol. 1986;13:923.
48 Polson AM, Zander HA. Effect of periodontal trauma upon intrabony pockets. J Periodontol. 1983;54:586.
49 Polson AM, Meitner SW, Zander HA. Trauma and progression of marginal periodontitis in squirrel monkeys. III. Adaption of interproximal alveolar bone to repetitive injury. J Periodontal Res. 1976;11:279.
50 Polson AM, Meitner SW, Zander HA. Trauma and progression of marginal periodontitis in squirrel monkeys. IV. Reversibility of bone loss due to trauma alone and trauma superimposed upon periodontitis. J Periodontal Res. 1976;11:290.
51 Ramfjord SP, Kohler CA. Periodontal reaction to functional occlusal stress. J Periodontol. 1959;30:95.
52 Rothblatt JM, Waldo CM. Tissue response to tooth movement in normal and abnormal metabolic states. J Dent Res. 1953;32:678.
53 Rygh P. Ultrastructural cellular reactions in pressure zones of rat molar periodontium incident to orthodontic movement. Acta Odontol Scand. 1972;30:575.
54 Rygh P. Ultrastructural vascular changes in pressure zones of rat molar periodontium incident to orthodontic movement. Scand J Dent Res. 1972;80:307.
55 Rygh P. Ultrastructural changes in pressure zones of human periodontium incident to orthodontic tooth movement. Acta Odontol Scand. 1973;31:109.
56 Rygh P. Ultrastructural changes of the periodontal fibers and their attachment in rat molar periodontium incident to orthodontic tooth movement. Scand J Dent Res. 1973;81:467.
57 Rygh P. Elimination of hyalinized periodontal tissues associated with orthodontic tooth movement. Scand J Dent Res. 1974;82:57.
58 Rygh P, Selvig KA. Erythrocytic crystallization in rat molar periodontium incident to tooth movement. Scand J Dent Res. 1973;81:62.
59 Solt CW, Glickman I. A histologic and radioautographic study of healing following wedging interdental injury in mice. J Periodontol. 1968;39:249.
60 Sottosanti JS. A possible relationship between occlusion, root resorption and the progression of periodontal disease. J West Soc Periodontol. 1977;25:69.
61 Stahl SS. Accommodation of the periodontium to occlusal trauma and inflammatory periodontal disease. Dent Clin North Am. 1975;19:531.
62 Stahl SS, Miller SC, Goldsmith ED. The effects of vertical occlusal trauma on the periodontium of protein deprived young adult rats. J Periodontol. 1957;28:87.
63 Stallard RE. The effect of occlusal alterations on collagen formation within the periodontium. Periodontics. 1964;2:49.
64 Svanberg G, Lindhe J. Vascular reactions to the periodontal ligament incident to trauma from occlusion. J Clin Periodontol. 1974;1:58.
65 Vollmer WH, Rateitschak KH. Influence of occlusal adjustment by grinding on gingivitis and mobility of traumatized teeth. J Clin Periodontol. 1975;2:113.
66 Waerhaug J, Hansen ER. Periodontal changes incidental to prolonged occlusal overload in monkeys. Acta Odontol Scand. 1966;24:91.
67 Wentz FM, Jarabak J, Orban B. Experimental occlusal trauma imitating cuspal interferences. J Periodontol. 1958;29:117.
68 Zaki AE, Van Huysen G. Histology of the periodontium following tooth movement. J Dent Res. 1963;42:1373.
69 Zander HA, Muhlemann HR. The effect of stresses on the periodontal structures. Oral Surg Oral Med Oral Pathol. 1956;9:380.