Nursing Care of Women with Complications During Labor and Birth
1 Define each key term listed.
2 Discuss each obstetric procedure discussed in this chapter.
3 Illustrate the nurse’s role in each obstetric procedure.
4 Analyze the nurse’s role in a cesarean birth.
5 Describe factors that contribute to an abnormal labor.
6 Explain each intrapartum complication discussed in this chapter.
7 Discuss the nurse’s role in caring for women with each intrapartum complication.
 , p. 181)
, p. 181) , p. 180)
, p. 180) , p. 192)
, p. 192) , p. 183)
, p. 183) , p. 193)
, p. 193) , p. 184)
, p. 184) , p. 176)
, p. 176) , p. 186)
, p. 186) , p. 174)
, p. 174) , p. 186)
, p. 186) , p. 176)
, p. 176) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
Childbirth is a normal, natural event in the life of most women and their families. When the many factors that affect the birth process function in harmony, complications are unlikely. However, some women experience complications during childbirth that threaten their well-being or that of the infant.
Obstetric Procedures
Nurses assist with several obstetric procedures during birth; they also care for women after the procedures. Some procedures, such as amniotomy or amnioinfusion, are performed to prevent complications during birth. Other procedures are needed when the woman has a complication that necessitates an intervention to promote a positive outcome for the mother and fetus.
Amnioinfusion
An amnioinfusion is the injection of warmed sterile saline or lactated Ringer’s solution into the uterus via an intrauterine pressure catheter during labor after the membranes have ruptured. Indications for this procedure include the following:
• Oligohydramnios (lower-than-normal amount of amniotic fluid)
• Umbilical cord compression resulting from lack of amniotic fluid
• Goal of reducing recurrent variable decelerations in the fetal heart rate
Amnioinfusion replaces the “cushion” for the umbilical cord and relieves the variable decelerations of the fetal heart rate that may occur during contractions when decreased amniotic fluid is present. It can be administered as a one-time bolus for 1 hour or as a continuous infusion. Continuous monitoring of uterine activity and fetal heart rate is essential. The nurse should change the underpads on the bed as needed to maintain patient comfort and should document the color, amount, and any odor of the fluid expelled from the vagina.
Amniotomy
Amniotomy is the artificial rupture of membranes (amniotic sac) (AROM) by using a sterile sharp instrument. It is performed by a physician or nurse-midwife. The nurse assists the health care provider with the procedure and cares for the woman and fetus afterward.
Amniotomy is done to stimulate contractions. It may provide enough stimulation to start labor before it begins naturally, but more often it is done to enhance contractions that have already begun. It may be done to permit internal fetal monitoring (see Chapter 6). The amniotomy stimulates prostaglandin secretion, which stimulates labor, but the loss of amniotic fluid may result in umbilical cord compression.
Technique
To determine if amniotomy is safe and indicated, the health care provider does a vaginal examination to assess the cervical effacement and dilation and the station of the fetus. A disposable plastic hook (Amnihook) is passed through the cervix, and the amniotic sac is snagged to create a hole and release the amniotic fluid.
Complications
Three complications associated with amniotomy may also occur if a woman’s membranes rupture spontaneously (spontaneous rupture of membranes [SROM]). These complications are prolapse of the umbilical cord, infection, and abruptio placentae.
Prolapse of the Umbilical Cord: Prolapse may occur if the cord slips downward with the gush of amniotic fluid (pp. 194-195).
Infection: Infection may occur because the membranes no longer block vaginal organisms from entering the uterus. Once performed, an amniotomy commits the woman to delivery within a certain time frame; the physician or nurse-midwife delays amniotomy until he or she is reasonably sure that birth will occur before the risk of infection markedly increases.
Abruptio Placentae: Abruptio placentae (separation of the placenta before birth) is more likely to occur if the uterus is overdistended with amniotic fluid (hydramnios) when the membranes rupture. The uterus becomes smaller with the discharge of amniotic fluid, but the placenta stays the same size and no longer fits its implantation site (see Chapter 5 for more information about abruptio placentae).
Nursing Care
The nursing care after amniotomy is the same as that after spontaneous membrane rupture: observing for complications and promoting the woman’s comfort.
 Nursing Tip
Nursing Tip
Observe for wet underpads and linens after the membranes rupture. Change them as often as needed to keep the woman relatively dry and to reduce the risk for infection or skin breakdown.
Observing for Complications: The fetal heart rate is recorded for at least 1 minute after amniotomy. Rates outside the normal range of 110 to 160 beats/min for a term fetus suggest a prolapsed umbilical cord. A large quantity of fluid increases the risk for prolapsed cord, especially if the fetus is high in the pelvis.
The color, odor, amount, and character of amniotic fluid are recorded. The fluid should be clear, possibly with flecks of vernix (newborn skin coating), and should not have a bad odor. Cloudy, yellow, or malodorous fluid suggests infection. Green fluid means that the fetus passed the first stool (meconium) into the fluid before birth. Meconium-stained amniotic fluid is associated with fetal compromise during labor and infant respiratory distress after birth.
The woman’s temperature is taken every 2 to 4 hours after her membranes rupture according to facility policy. A maternal temperature of 38° C (100.4° F) or higher suggests infection. An increase in the fetal heart rate, especially if above 160 beats/min, may precede the woman’s temperature increase.
Promoting Comfort: When amniotomy is anticipated, several disposable underpads are placed under the woman’s hips to absorb the fluid that continues to leak from the woman’s vagina during labor. Disposable underpads are changed often enough to keep her reasonably dry and to reduce the moist, warm environment that favors the growth of microorganisms.
Induction or Augmentation of Labor
Induction is the intentional initiation of labor before it begins naturally. Augmentation is the stimulation of contractions after they have begun naturally.
Labor involves the complex interaction between fetus and mother. Before labor is induced, it is important that fetal maturity be confirmed by ultrasound or amniotic fluid analysis (lecithin/sphingomyelin [L/S] ratio) (see Chapter 5), and the status of the cervix is determined. The Bishop score is used to assess the status of the cervix in determining its response to induction (Table 8-1). A score of 6 or more indicates a favorable prognosis for induction. Continuous uterine activity and fetal heart rate monitoring during labor induction is essential.
Table 8-1
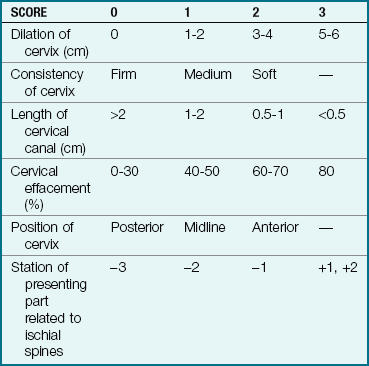
A high score is predictive of a successful labor induction because the cervix has ripened, or softened, in preparation for labor. The American College of Obstetricians and Gynecologists (ACOG) recommends a score of 6 or above before induction of labor. Modified from Stables, D., & Rankin, J. (2005). Physiology in childbearing: With anatomy and related biosciences (2nd ed.). Edinburgh: Elsevier; Gabbe, S., Niebyl, J., Simpson, J., et al (Eds.), (2009). Obstetrics: Normal and problem pregnancies (5th ed.). New York: Churchill-Livingstone.
Indications
Labor is induced if continuing the pregnancy is hazardous for the woman or the fetus. The following are some of the indications for labor induction:
• Gestational hypertension (see Chapter 5)
• Ruptured membranes without spontaneous onset of labor
• Medical problems in the woman that worsen during pregnancy, such as diabetes, kidney disease, or pulmonary disease
• Fetal problems, such as slowed growth, prolonged pregnancy, or incompatibility between fetal and maternal blood types (see Chapter 5)
Convenience for the health care provider or the family is not an indication for inducing labor. However, the woman who has a history of rapid labors and lives a long distance from the birth facility may have her labor induced because she has a higher risk of giving birth en route if she awaits spontaneous labor.
Contraindications
Labor is not induced in the following conditions:
• Placenta previa (see Chapter 5)
• Umbilical cord prolapse (see pp. 194-195)
• High station of the fetus, which suggests a preterm fetus or a small maternal pelvis
• Active herpes infection in the birth canal, which the infant can acquire during birth
• Abnormal size or structure of the mother’s pelvis
• Previous classic (vertical) cesarean incision (see Figure 8-4, p. 182)
The physician may attempt to induce labor in a preterm pregnancy if continuing the pregnancy is more harmful to the woman or the fetus than the hazards of prematurity would be to the infant.
Technique
Amniotomy may be the only method used to initiate labor, but it is more likely to be used in combination with oxytocin (Pitocin) administration to stimulate contractions. Induction and augmentation of labor may rely on both pharmacological and nonpharmacological methods.
Pharmacological Methods to Stimulate Contractions
Cervical Ripening: Induction of labor is easier if the woman’s cervix is soft, partially effaced, and beginning to dilate. These prelabor cervical changes occur naturally in most women. Methods to hasten the changes, or “ripen” the cervix, ease labor induction because oxytocic drugs have no effect on the cervix.
Prostaglandin in the form of a gel or commercially prepared vaginal insert softens the cervix when applied before labor induction. The procedure should be explained to the woman and her family. A fetal heart rate baseline is recorded. An intravenous (IV) line with saline or heparin sodium (Hep-Lock) may be placed in case uterine hyperstimulation occurs and IV tocolytics (drugs that reduce uterine contractions) are needed. After insertion of the prostaglandin gel, the woman remains on bed rest for 1 to 2 hours and is monitored for uterine contractions. Vital signs and fetal heart rate are also recorded. Oxytocin induction can be started when the insert is removed—usually after 6 to 12 hours. Signs of uterine hyperstimulation include uterine contractions that last longer than 90 seconds and/or more than five contractions in 10 minutes.
The vaginal insert can be removed by pulling on the netted string that protrudes from the vaginal orifice. The contractions and fetal heart rate are monitored, and oxytocin may be started as needed. Some women who receive cervical ripening products begin labor without additional oxytocin stimulation. Misoprostol (Cytotec) is frequently used during labor.
An alternative to prostaglandin for cervical ripening is insertion of one or more laminaria into the cervix (Hacker et al., 2009). A laminaria is a narrow cone of a substance that absorbs water and is known as an “osmotic dilator.” The laminaria swells inside the cervix, thus beginning cervical dilation. Oxytocin induction follows, usually on the next day.
Oxytocin Administration: Initiation or stimulation of contractions with oxytocin (Pitocin) is the most common method of labor induction and augmentation. Oxytocin is administered by registered nurses with additional training in the induction of labor and electronic fetal monitoring. Augmentation of labor with oxytocin follows a similar procedure.
Oxytocin for induction or augmentation of labor is diluted in an IV solution. The oxytocin solution is a secondary (piggyback) infusion that is inserted into the primary (nonmedicated) IV solution line so it can be stopped quickly while an open IV line is maintained. The infusion of oxytocin solution is regulated with an infusion pump. Administration begins at a very low rate and is adjusted upward or downward according to how the fetus responds to labor and to the woman’s contractions. The dose is individualized for every woman. When contractions are well-established, it is often possible to reduce the rate of oxytocin. Augmentation of labor usually requires less total oxytocin than induction of labor because the uterus is more sensitive to the drug when labor has already begun.
Continuous electronic monitoring is the usual method to assess and record fetal and maternal responses to oxytocin. Many health care providers prefer internal methods of monitoring when oxytocin is used because these techniques are more accurate, especially for contraction intensity.
Nonpharmacological Methods to Stimulate Contractions
Walking: Many women benefit from a change in activity if their labor slows. Walking stimulates contractions, eases the pressure of the fetus on the mother’s back, and adds gravity to the downward force of contractions. If she does not feel like walking, other upright positions often improve the effectiveness of each contraction. She can sit (in a chair, on the side of the bed, or in the bed), squat, kneel while facing the raised head of the bed for support, or maintain other upright positions.
Nipple Stimulation of Labor: Stimulating the nipples causes the woman’s posterior pituitary gland to naturally secrete oxytocin. This improves the quality of contractions that have slowed or weakened, just as IV administration of synthetic oxytocin does. The woman can stimulate her nipples by doing the following:
• Pulling or rolling them, one at a time
• Gently brushing them with a dry washcloth
If contractions become too strong with these techniques, the woman simply stops stimulation.
Complications of Augmentation of Labor
The most common complications related to overstimulation of contractions are fetal compromise and uterine rupture (see pp. 195-196). Fetal compromise can occur because blood flow to the placenta is reduced if contractions are excessive. Most placental exchange of oxygen, nutrients, and waste products occurs between contractions. This exchange is likely to be impaired if the contractions are too long, too frequent, or too intense.
Water intoxication sometimes occurs because oxytocin inhibits the excretion of urine and promotes fluid retention. Water intoxication is not likely with the small amounts of oxytocin and fluids given intravenously during labor, but it is more likely to occur if large doses of oxytocin and fluids are given intravenously after birth.
Oxytocin is discontinued, or its rate reduced, if signs of fetal compromise or excessive uterine contractions occur. Fetal heart rates outside the normal range of 110 to 160 beats/min, late decelerations, and loss of variability (see Chapter 6) are the most common signs of fetal compromise. Excessive uterine contractions are most often evidenced by contraction frequency greater than every 2 minutes, durations longer than 90 seconds, or resting intervals shorter than 60 seconds. The resting tone of the uterus (muscle tension when it is not contracting) is often higher than normal. Internal uterine activity monitoring allows determination of peak uterine pressures and uterine resting tone.
In addition to stopping the oxytocin infusion, the registered nurse chooses one or more of the following measures to correct adverse maternal or fetal reactions:
• Increasing the nonmedicated intravenous solution
• Changing the woman’s position, avoiding the supine position
The health care provider is notified after corrective measures are taken. A tocolytic (drug that reduces uterine contractions) may be ordered if contractions do not quickly decrease after oxytocin is stopped.
 Safety Alert!
Safety Alert!
In 2007, intravenous oxytocin was added to a list of high-alert medications by the Institute of Safe Medical Practices. High-alert medications have a higher risk of causing significant adverse reaction when used incorrectly. The nurse must be aware of signs and symptoms of increased uterine activity and monitor fetal heart rate every 15 minutes during active labor and every 5 minutes during the transitional phase. Safety interventions for oxytocin-induced uterine contractions or fetal heart rate abnormalities include the following:
• Notifying the health care provider and the registered nurse
• Repositioning the woman to left or right lateral position
• Decreasing the dose of oxytocin to half of the current rate or discontinuing oxytocin
• Preparing an intravenous (IV) bolus of lactated Ringer’s
• Administering oxygen at 10 L/min via a nonrebreather facial mask
• Preparing IV terbutaline for administration
• Assessing uterine contractions and fetal heart rate every 5 minutes
Nursing Care
In 2007, the American Academy of Pediatrics (AAP) and the College of Obstetricians and Gynecologists (ACOG) recommended all patients undergoing oxytocin-induced labor be cared for by an RN with 1 : 1 or 1 : 2 ratio. Fetal heart rate must be assessed and recorded every 15 minutes during active labor and every 5 minutes during transition. Baseline maternal vital signs are assessed, and a fetal monitor tracing is performed to identify contraindications to induction or augmentation before the procedure begins.
If abnormalities are noted in either, the nurse stops the oxytocin and begins measures to reduce contractions and increase placental blood flow. The woman’s blood pressure, pulse rate, and respirations are measured every 30 to 60 minutes. Her temperature is taken every 2 to 4 hours. Recording her intake and output helps identify potential water intoxication.
Version
Version is a method of changing the fetal presentation, usually from breech to cephalic. There are two methods: external and internal. External version is the more common one. A successful version reduces the likelihood that the woman will need cesarean delivery.
Risks and Contraindications
Few maternal and fetal risks are associated with version, especially external version. Version is not indicated if there is any maternal or fetal reason why vaginal birth should not occur, because that is its goal. The following are examples of maternal or fetal conditions that are contraindications for version:
• Disproportion between the mother’s pelvis and fetal size
• Abnormal uterine or pelvic size or shape
• Abnormal placental placement
• Previous cesarean birth with a vertical uterine incision
Version may not be attempted in a woman who has a higher risk for uterine rupture, such as several prior cesarean births or high parity. It is not usually attempted if the fetal presenting part is engaged in the pelvis. The main risk to the fetus is that it will become entangled in the umbilical cord, thus compressing the cord. This is more likely to happen if there is not adequate room to turn the fetus, such as in multifetal gestation (e.g., twins) or when the amount of amniotic fluid is minimal.
Technique
External version is done after 37 weeks of gestation but before the onset of labor. The procedure begins with a non–stress test (NST) or biophysical profile (BPP, see Table 5-1) to determine if the fetus is in good condition and if there is adequate amniotic fluid to perform the version. The woman receives a tocolytic drug to relax her uterus during the version.
Using ultrasound to guide the procedure, the physician pushes the fetal buttocks upward out of the pelvis while pushing the fetal head downward toward the pelvis in either a clockwise or a counterclockwise turn. The fetus is monitored frequently during the procedure. The tocolytic drug is discontinued after the external version is completed (or the effort abandoned). Rh-negative women receive a dose of Rh0(D) immune globulin (RhoGAM).
Internal version is an emergency procedure. The physician usually performs internal version during a vaginal birth of twins to change the fetal presentation of the second twin.
Nursing Care
Nursing care of the woman having external version includes assisting with the procedure and observing the mother and fetus afterward for 1 to 2 hours. Baseline maternal vital signs and a fetal monitor strip (part of the NST or BPP) are taken before the version. The mother’s vital signs and the fetal heart rate are observed to ensure return to normal levels after the version is complete.
Vaginal leaking of amniotic fluid suggests that manipulating the fetus caused a tear in the membranes, and this is reported. Uterine contractions usually decrease or stop shortly after the version. The physician is notified if they do not. The nurse reviews signs of labor with the woman because version is performed near term, when spontaneous labor is expected.
Episiotomy and Lacerations
Episiotomy is the surgical enlargement of the vagina during birth. Either the physician or a nurse-midwife performs and repairs an episiotomy. A laceration is an uncontrolled tear of the tissues that results in a jagged wound. Lacerations of the perineum and episiotomy incisions are treated similarly.
Perineal lacerations and often episiotomies are described by the amount of tissue involved:
• First degree: Involves the superficial vaginal mucosa or perineal skin
• Second degree: Involves the vaginal mucosa, perineal skin, and deeper tissues of the perineum
• Third degree: Same as second degree, plus involves the anal sphincter
• Fourth degree: Extends through the anal sphincter into the rectal mucosa
Women with third- and fourth-degree lacerations may have more discomfort postpartum if they are constipated after birth.
 Nutrition Considerations
Nutrition Considerations
Third- or Fourth-Degree Laceration
Pay special attention to a woman’s diet and fluids if she had a third- or fourth-degree laceration. A high-fiber diet and adequate fluids help to prevent constipation that might result in a breakdown of the perineal area where the laceration was sutured.
Indications
Fetal indications for an episiotomy are similar to those for forceps or vacuum extraction (see p. 180). Additional maternal indications include the following:
• Better control over where and how much the vaginal opening is enlarged
• An opening with a clean edge rather than the ragged opening of a tear
Routine episiotomy has been challenged by several recent studies that do not support many of its supposed benefits. Nevertheless, it is so common that the nurse can expect to give postpartum care to many women with episiotomies. Perineal massage and stretching exercises before labor are becoming popular techniques to decrease the need for episiotomy during birth.
Risks
As in other incisions, infection is the primary risk in an episiotomy or laceration. An additional risk is extension of the episiotomy with a laceration into or through the rectal sphincter (third or fourth degree), which can cause prolonged perineal discomfort and stress incontinence.
Technique
The episiotomy is performed with blunt-tipped scissors just before birth. One of the following two directions is chosen (Figure 8-1):
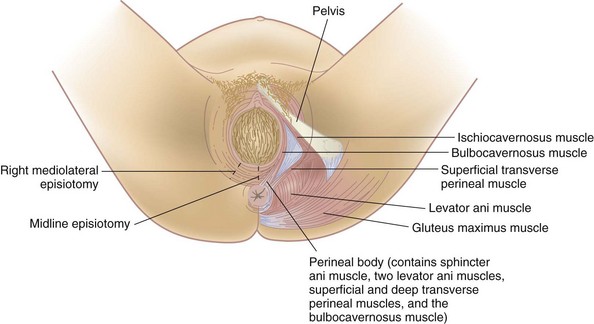
• Midline (median), extending directly from the lower vaginal border toward the anus
• Mediolateral, extending from the lower vaginal border toward the mother’s right or left
A median episiotomy is easier to repair and heals neatly. The mediolateral incision provides more room, but greater scarring during healing may cause painful sexual intercourse. A laceration that extends a median episiotomy is more likely to involve the rectal sphincter than one that extends the mediolateral episiotomy.
Nursing Care
Nursing care for an episiotomy or laceration begins during the fourth stage of labor. Cold packs should be applied to the perineum for at least the first 12 hours to reduce pain, bruising, and edema. After 12 to 24 hours of cold applications, warmth in the form of heat packs or sitz baths increases blood circulation, enhancing comfort and healing. Mild oral analgesics are usually sufficient for pain management. See Chapter 9 for postpartum nursing care of the woman with an episiotomy or laceration.
Forceps and Vacuum Extraction Births
Obstetric forceps and vacuum extractors are used by an obstetrician to provide traction and rotation to the fetal head when the mother’s pushing efforts are insufficient to accomplish a safe delivery. Forceps are instruments with curved blades that fit around the fetal head without unduly compressing it (Figure 8-2). Several different styles are available to assist the birth of the fetal head in a cephalic presentation or the after-coming head in a breech delivery. Forceps may also help the physician extract the fetal head through the incision during cesarean birth.
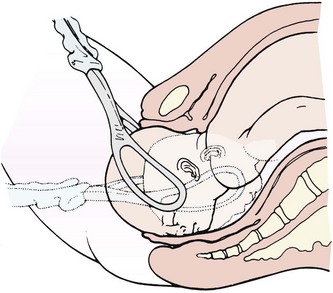
FIGURE 8-2 Use of forceps to assist the birth of the fetal head. After applying the forceps to each side of the fetal head and locking the two blades, the physician pulls, following the pelvic curve.
A vacuum extractor uses suction applied to the fetal head so the physician can assist the mother’s expulsive efforts (Figure 8-3). The vacuum extractor is used only with an occiput presentation. One advantage of the vacuum extractor is that it does not take up room in the mother’s pelvis, as forceps do.
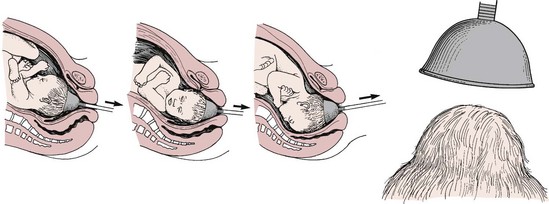
FIGURE 8-3 Use of the vacuum extractor to rotate the fetal head and assist with delivery. The arrows indicate the direction of traction on the vacuum cup. The vacuum cup is positioned on the midline, near the posterior fontanelle.
Indications
Forceps or vacuum extraction may be used to end the second stage of labor if it is in the best interest of the mother or fetus. The mother may be exhausted, or she may be unable to push effectively. Women with cardiac or pulmonary disorders often have forceps or vacuum extraction births because prolonged pushing can worsen these conditions. Fetal indications include conditions in which there is evidence of an increased risk to the fetus near the end of labor. The cervix must be fully dilated, the membranes ruptured, the bladder empty, and the fetal head engaged and at +2 station for optimal outcome.
Contraindications
Forceps or vacuum extraction cannot substitute for cesarean birth if the maternal or fetal condition requires a quicker delivery. Delivery by these techniques is not done if they would be more traumatic than cesarean birth, such as when the fetus is high in the pelvis or too large for a vaginal delivery.
Risks
Trauma to maternal or fetal tissues is the main risk when forceps or vacuum extraction is used. The mother may have a laceration or hematoma (collection of blood in the tissues) in her vagina. The infant may have bruising, facial or scalp lacerations or abrasions, cephalhematoma (see Chapter 12), or intracranial hemorrhage. The vacuum extractor causes a harmless area of circular edema on the infant’s scalp (chignon) where it was applied.
Technique
The health care provider catheterizes the woman to prevent trauma to her bladder and to make more room in her pelvis. After the forceps are applied, the physician pulls in line with the pelvic curve. An episiotomy is usually done. After the fetal head is brought under the mother’s symphysis, the rest of the birth occurs in the usual way.
Birth assisted with the vacuum extractor follows a similar sequence. The health care provider applies the cup over the posterior fontanelle of the fetal occiput, and suction is created with a machine to hold it there. Traction is applied by pulling on the handle of the extractor cup.
Nursing Care
If the use of forceps or vacuum extraction is anticipated, the nurse places the sterile equipment on the delivery instrument table. After birth, care is similar to that for episiotomy and perineal lacerations. Ice is applied to the perineum to reduce bruising and edema. The physician is notified if the woman has signs of vaginal hematoma, which include severe and poorly relieved pelvic or rectal pain.
The infant’s head is examined for lacerations, abrasions, or bruising. Mild facial reddening and molding (alteration in shape) of the head are common and do not necessitate treatment. Cold treatments are not used on neonates because they would cause hypothermia.
Pressure from forceps may injure the infant’s facial nerve. This is evidenced by facial asymmetry (different appearance of right and left sides), which is most obvious when the infant cries. Facial nerve injury usually resolves without treatment. The scalp chignon from the vacuum extractor does not necessitate intervention and resolves quickly.
Cesarean Birth
Cesarean birth is the surgical delivery of the fetus through incisions in the mother’s abdomen and uterus. Cesarean birth rates in the United States are 27.6% (National Center for Health Statistics [NCHS], 2008), and the goal of Healthy People 2020 (U.S. Department of Health and Human Services, 2010) is to reduce cesarean sections to 15%. This is the basis for some of the changes in the management of the second stage of labor, such as the following:
• Position variation (upright or horizontal)
• Epidural analgesia and subarachnoid analgesia that allows ambulation and delivery in squatting position
• Oxytocin (Pitocin) augmentation of labor
• Spontaneous open glottis pushing when fetus is at +1 station
• Use of vacuum-assisted delivery rapidly replacing forceps delivery
• Trial of labor before repeat cesarean (vaginal birth after cesarean [VBAC])
In 1997 the World Health Organization (WHO) recommended minimal intervention with maximum patience, support, and tender loving care (TLC). Although the total percentage of cesarean births has increased from 2002, the rate of VBAC has decreased in the United States (NCHS, 2008).
Indications
Several conditions may necessitate cesarean delivery:
• Inability of the fetus to pass through the mother’s pelvis (cephalopelvic disproportion)
• Maternal conditions such as gestational hypertension or diabetes mellitus
• Active maternal herpes virus, which may cause serious or fatal infant infection
• Previous surgery on the uterus, including the classic type of cesarean incision
• Fetal compromise, including prolapsed umbilical cord and abnormal presentations
Contraindications
There are few contraindications to cesarean birth, but it is not usually done if the fetus is dead or too premature to survive or if the mother has abnormal blood clotting.
Risks
Cesarean birth carries risks to both mother and fetus. Maternal risks are similar to those of other types of surgery and include the following:
• Risks related to anesthesia (see Chapter 7)
Risks to the newborn may include the following:
To help prevent the unintentional birth of a preterm fetus, the physician often performs amniocentesis before a planned cesarean birth to determine if the fetal lungs are mature (see Chapter 5).
Technique
Cesarean birth may occur under planned, unplanned, or emergency conditions. The preparation is similar for each and includes routine preoperative care such as obtaining informed consent. If the woman wears eyeglasses, they should accompany her to the operating room because she is usually awake to bond with the infant after birth.
Preparations for Cesarean Birth: As with other surgery, several laboratory studies are done to identify anemia or blood-clotting abnormalities. Complete blood count, coagulation studies, and blood typing and screening are common. One or more units of blood may be typed and cross-matched if the woman is likely to need a transfusion. The baseline vital signs of the mother and the fetal heart rate are recorded.
The woman receives an IV drug to reduce gastric acidity and speed stomach emptying. Antibiotics may be ordered for the woman who has an increased risk for infection (such as prolonged ruptured membranes), displays signs of infection, or is positive for group B streptococcus (GBS).
If a vertical skin incision is expected, the woman’s abdomen may be shaved from just above her umbilicus to her mons pubis, where her thighs come together. If a Pfannenstiel (transverse, or “bikini”) skin incision is planned, the upper border of the shave is about 3 inches above her pubic hairline.
An indwelling Foley catheter is inserted to keep the bladder empty and prevent trauma to it. The catheter bag is placed near the head of the operating table so the anesthesiologist can monitor urine output, an important indicator of the woman’s circulating blood volume. The circulating nurse scrubs the abdomen by using a circular motion that goes outward from the incisional area. The father or woman’s partner may don a hat, mask, and gown and provide support to the mother at the head of the table (see Figure 8-5, D).
Types of Incisions: There are two incisions in cesarean birth: a skin incision and a uterine incision. The directions of these incisions are not always the same.
Skin incisions: The skin incision is done in either a vertical or a transverse direction. A vertical incision allows more room if a large fetus is being delivered, and it is usually needed for an obese woman. In an emergency, the vertical incision can be done more quickly. The transverse, or Pfannenstiel, incision is nearly invisible when healed but cannot always be used in obese women or in women with a large fetus.
Uterine incisions: The more important of the two incisions is the one that cuts into the uterus. There are three types of uterine incisions (Figure 8-4): low transverse, low vertical, and classic.
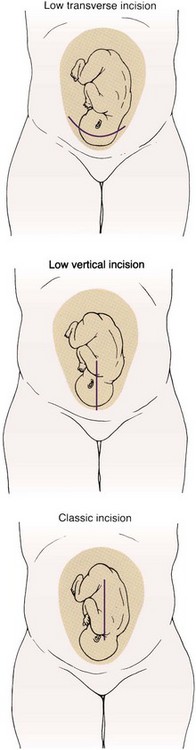
FIGURE 8-4 Three types of uterine incisions for cesarean birth. The low transverse uterine incision is preferred because it is not likely to rupture during a subsequent birth, allowing vaginal birth after a cesarean birth. The low vertical and classic incisions may occasionally be used. The skin incision and uterine incision do not always match.
Low transverse incision: A low transverse incision is preferred because it is not likely to rupture during another birth, causes less blood loss, and is easier to repair. It may not be an option if the fetus is large or if there is a placenta previa in the area where the incision would be made. This type of incision makes VBAC possible for subsequent births.
Low vertical incision: A low vertical incision produces minimal blood loss and allows delivery of a larger fetus. However, it is more likely to rupture during another birth, although less so than the classic incision.
Classic incision: The classic incision is rarely used because it involves more blood loss and is the most likely of the three types to rupture during another pregnancy. However, it may be the only choice if the fetus is in a transverse lie or if there is scarring or a placenta previa in the lower anterior uterus.
Sequence of Events
After the woman has been given a spinal anesthetic, scrubbed, and draped, the physician makes the skin incision. After making the uterine incision, the physician ruptures the membranes (unless they are already ruptured) with a sharp instrument. The amniotic fluid is suctioned from the operative area, and its amount, color, and odor are noted.
The physician reaches into the uterus to lift out the fetal head or buttocks. Forceps or vacuum extraction may be used to assist birth of the head. The infant’s mouth and nose are quickly suctioned to remove secretions, and the cord is clamped. The physician hands the infant to the nurse, who receives the infant into sterile blankets and places the infant into a radiant warmer. A pediatrician is usually available for resuscitation.
After the birth of the infant, the physician scoops out the placenta and examines it for intactness. The uterine cavity is sponged to remove blood clots and other debris. The uterine and skin incisions are then sutured in layers (Figure 8-5).
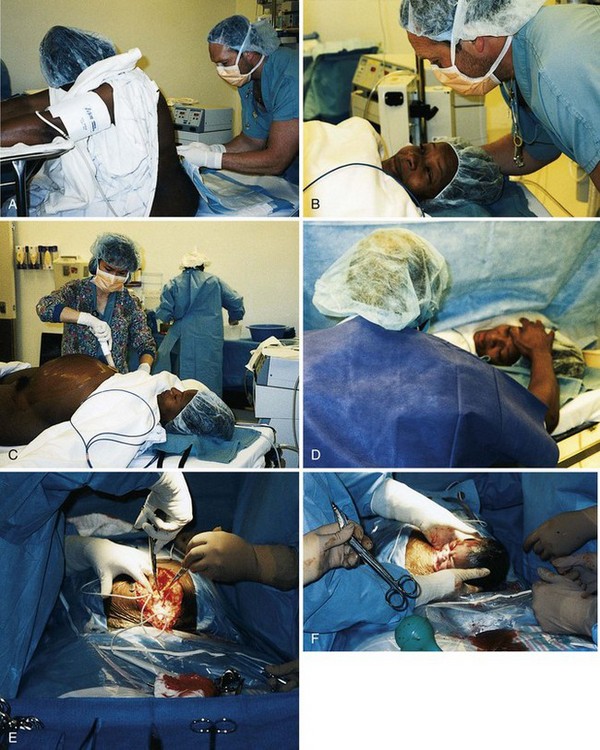

FIGURE 8-5 Cesarean section birth. A, Spinal anesthetic is given. B, The anesthesiologist reassures the woman. C, The nurse preps the abdomen. D, The partner encourages the woman. E, A vertical incision is made. F, The head of the infant is lifted out of the uterus. G, The body of the infant is lifted out of the uterus. H, The infant is placed on the mother’s abdomen and the infant’s secretions are suctioned with a bulb syringe. Note the active muscle tone of the newborn. I, The placenta is delivered from the uterus. J, The parents and the newborn bond. (Courtesy Pat Spier, RN-C.)
Nursing Care
The registered nurse assumes most of the preoperative and postoperative care of the woman. This includes obtaining the required laboratory studies, administering medications, performing preoperative teaching, and preparing for surgery. Women who have cesarean births usually need greater emotional support than those having vaginal births. They are usually happy and excited about the newborn but may also feel grief, guilt, or anger because the expected course of birth did not occur. These feelings may linger and resurface during another pregnancy. Emotional care of the partner and family is essential; they are included in explanations of the surgery as much as the woman wishes. The partner may be frightened when an emergency cesarean is needed but may not express these feelings because the woman needs so much support. The nurse informs the partner of when he or she may enter the operating room because 30 minutes or more may be needed to administer a regional anesthetic and for surgical preparations if there is no emergency. The partner dons surgical attire during this time.
The partner may be almost as exhausted as the woman if a cesarean birth is performed after hours of labor. The thoughtful nurse includes the partner and promotes his or her emotional and physical well-being. The mother, neonate, and partner are kept together as much as possible after birth, just as in a vaginal birth. The woman and her partner are encouraged to talk about the cesarean birth so they can integrate the experience. The nurse answers questions about events surrounding the birth. The focus is on the birth rather than on the surgical aspects of cesarean delivery.
Nursing assessments after cesarean birth are similar to those after vaginal birth, including assessment of the uterine fundus. Assessments are done every 15 minutes for the first 1 or 2 hours according to hospital policy. Recovery room assessments after cesarean birth include the following:
• Vital signs to identify hemorrhage or shock; a pulse oximeter is used to better identify depressed respiratory function
• IV site and rate of solution flow
• Fundus for firmness, height, and midline position
The fundus is checked as gently as possible. The woman flexes her knees slightly and takes slow, deep breaths to minimize the discomfort of fundal assessments. While supporting the lower uterus with one hand, the fingers of the other hand are gently “walked” from the side of the uterus toward the midline. Massage is not needed if the fundus is already firm.
Safety Alert!
Although assessing the uterus after cesarean birth causes discomfort, it is important to do so regularly because the woman may have a relaxed uterus that causes excessive blood loss.
The woman is told to take deep breaths at each assessment and to cough to move secretions from her airways. A small pillow or folded blanket supports her incision when she coughs or moves, which reduces pain. Changing her position every 1 or 2 hours helps expand her lungs and also makes her more comfortable.
Pain relief after cesarean birth may be accomplished by a patient-controlled analgesia (PCA) pump or by intermittent injections of narcotic analgesics. Epidural narcotics provide long-lasting pain relief but are associated with delayed respiratory depression and itching (see Chapter 7), which vary with the drug injected. The woman is changed to oral analgesics after about the first 24 hours. Nursing Care Plan 8-1 on p. 187 details interventions for selected nursing diagnoses that pertain to the woman with an unplanned cesarean birth.
8-1  Nursing Care Plan
Nursing Care Plan
The Woman with an Unplanned Cesarean Birth
A woman, para 0, gravida 1, has been using breathing, relaxation, and imagery techniques during the first stage of labor, and her husband has been helpful and supportive. However, the labor is not progressing, and there are signs of fetal distress. The physician orders that the patient be prepared for an emergency cesarean section.
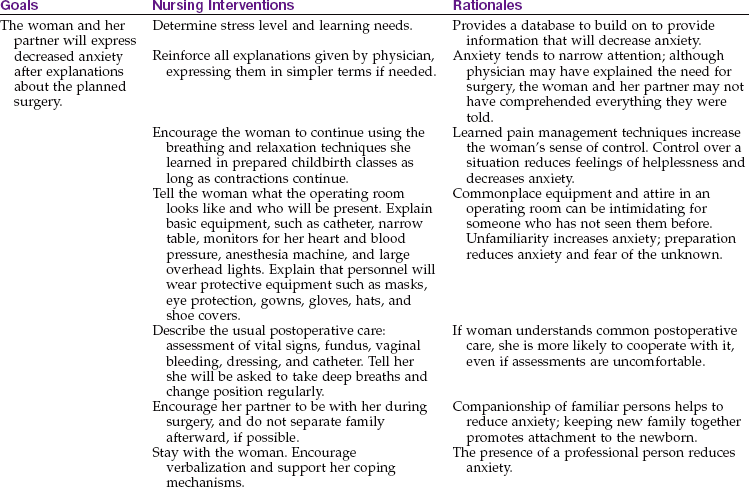
Impaired comfort related to decreased coping ability
| Goals | Nursing Interventions | Rationales |
| The woman will verbalize reduced discomfort or will be able to use effective techniques to decrease perception of pain. | Determine the nature, duration, and location of pain. | Never assume that the pain is related to a contraction. Locating the site of pain helps identify complications that may be occurring (e.g., embolism). Assessing pain and contractions can help identify a prolonged contraction that can cause fetal hypoxia. |
| Encourage the woman to continue using coping mechanisms learned during prenatal classes. Use therapeutic touch to increase comfort. | A feeling of loss of control can increase the perception of pain. Reduction of tension can promote comfort. | |
| Maintain a calm manner and environment. | A calm manner calms the parents and reduces anxieties and tensions that elevate pain perception. |
Abnormal Labor
A normal labor is labor that evidences a regular progression in cervical effacement, dilation, and descent of the fetus. Abnormal labor, called dysfunctional labor, does not progress. Dystocia is a term used to describe a difficult labor.
The “four Ps” of labor (see Chapter 6) interact constantly throughout the birth. Abnormalities in the powers, passengers, passage, or psyche may result in a dysfunctional labor. In addition, the length of labor may be unusually short or long. Labor abnormalities may necessitate use of forceps or cesarean delivery, and they are more likely to result in injury to the mother or fetus.
It is essential for nurses to understand the normal birth process so that deviations from normal can be recognized and prompt interventions implemented. Effective support for the woman and her family is part of competent and compassionate care. Risk factors for dysfunctional labor include the following:
• Overdistention of uterus (hydramnios or multifetal pregnancy)
• Cephalopelvic disproportion (CPD)
• Overstimulation of the uterus
Problems with the Powers of Labor
Increased uterine muscle tone usually occurs during the latent phase of labor (before 4 cm of cervical dilation) and is characterized by contractions that are frequent, cramplike, and poorly coordinated. These contractions are painful but nonproductive. The uterus is tense, even between contractions, which reduces blood flow to the placenta. Hypertonic labor dysfunction is less common than hypotonic dysfunction. Box 8-1 summarizes the differences between hypertonic and hypotonic labor dysfunction.
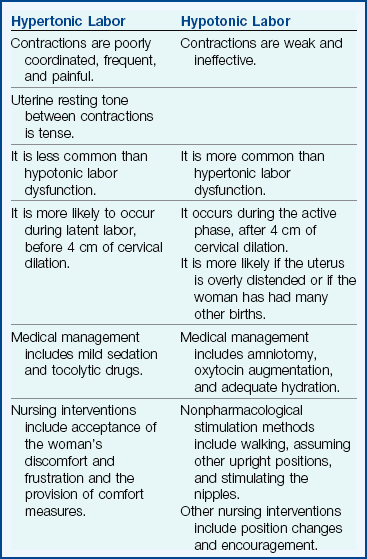
Medical Treatment: Medical treatment may include mild sedation to allow the woman to rest. Tocolytic drugs (see p. 193) such as terbutaline (Brethine) may be ordered.
Nursing Care: Women with increased uterine muscle tone are uncomfortable and frustrated. Anxiety about the lack of progress and fatigue impair their ability to tolerate pain. They may lose confidence in their ability to give birth. The nurse should accept the woman’s frustration and that of her partner. Both may be exhausted from the near-constant discomfort. It is important not to equate the amount of pain a woman reports with how much she “should” feel at that point in labor. The nurse provides general comfort measures that promote rest and relaxation.
Decreased Uterine Muscle Tone
A woman who has decreased uterine muscle tone has contractions that are too weak to be effective during active labor. The woman begins labor normally, but contractions diminish (hypotonic labor dysfunction) during the active phase (after 4 cm of cervical dilation), when the pace of labor is expected to accelerate. This is more likely to occur if the uterus is overdistended, such as with twins, a large fetus, or excess amniotic fluid (hydramnios). Uterine overdistention stretches the muscle fibers and thus reduces their ability to contract effectively.
Medical Treatment: The physician usually performs an amniotomy if the membranes are intact. Augmentation of labor with oxytocin or by nipple stimulation increases the strength of contractions. IV or oral fluids may improve the quality of contractions if the woman is dehydrated.
Nursing Care: The woman is reasonably comfortable but frustrated because her labor is not progressing. In addition to providing care related to amniotomy and labor augmentation, the nurse gives emotional support to the woman and her partner. She is allowed to express her frustrations. The nurse tells the woman when she makes progress to encourage continuation of her efforts.
Position changes may help to relieve discomfort and enhance progress. Contractions are usually stronger and more effective when the woman assumes an upright position or lies on her side, although they may be less frequent. Walking or nipple stimulation may intensify contractions. Nursing Care Plan 8-2 details interventions for selected nursing diagnoses that pertain to the woman with labor dysfunction.
8-2 Nursing Care Plan
The Woman with Hypotonic Labor Dysfunction
A woman, para 0, gravida 1, is admitted at 7 pm because of premature rupture of the membranes. Contractions remain irregular at 7 am the next morning. The woman appears anxious and fearful concerning her lack of progress.
Ineffective coping related to frustration with slow labor and delayed birth
1. A woman, para 0, gravida 1, has been admitted with ruptured membranes. Contractions are irregular and ineffective, and progress in dilation and effacement of the cervix is very slow. An oxytocin IV infusion is started after 15 hours. What could happen if the health care provider decided not to augment labor?
Ineffective Maternal Pushing
The woman may not push effectively during the second stage of labor because she does not understand which techniques to use or fears tearing her perineal tissues. Epidural or subarachnoid blocks (see Chapter 7) may depress or eliminate the natural urge to push. An exhausted woman may be unable to gather her resources to push appropriately.
Nursing Care: Nursing care focuses on coaching the woman about the most effective techniques for pushing. If she cannot feel her contractions because of a regional block, the nurse tells her when to push as each contraction reaches its peak.
The exhausted woman may benefit from pushing only when she feels a strong urge. The fearful woman may benefit from explanations that sensations of tearing or splitting often accompany fetal descent but that her body is designed to accommodate the fetus. Promoting relaxation, relieving fatigue, changing position, and increasing hydration can help the woman sustain the energy level needed for effective pushing.
Problems with the Fetus
A large fetus (macrosomia) is generally considered to be one that weighs more than 4000 g (8.8 lb) at birth. The large fetus may not fit through the woman’s pelvis. A very large fetus also distends the uterus and can contribute to hypotonic labor dysfunction.
Sometimes a single part of the fetus is too large. For example, the fetus may have hydrocephalus (an abnormal amount of fluid in the brain) (see Chapter 14). In that case the fetal body size and weight may be normal, but the head is too large to fit through the pelvis. These infants are often in an abnormal presentation as well.
Shoulder dystocia may occur, usually when the fetus is large. The fetal head is born, but the shoulders become impacted above the mother’s symphysis pubis. A shoulder dystocia is an emergency because the fetus needs to breathe. The head is out, but the chest cannot expand. The cord is compressed between the fetus and the mother’s pelvis. The health care provider may request that the nurse apply firm downward pressure just above the symphysis (suprapubic pressure) to push the shoulders toward the pelvic canal. Squatting or sharp flexion of the thighs against the abdomen may also loosen the shoulders.
Nursing Care: If the woman successfully delivers a large infant, both mother and child should be observed for injuries after birth. The woman may have a large episiotomy or laceration. The large infant is more likely to have a fracture of one or both clavicles (collarbones). The infant’s clavicles are felt for crepitus (crackling sensation) or deformity of the bones, and the arms are observed for equal movement (unilateral Moro reflex). The woman is more at risk for uterine atony and postpartum hemorrhage because her uterus does not contract well after birth to control bleeding at the placental site.
Abnormal Fetal Presentation or Position
Labor is most efficient if the fetus is in a flexed, cephalic presentation and in one of the occiput anterior positions (see Chapter 6). Abnormalities of fetal presentation and position prevent the smallest diameter of the fetal head from passing through the smallest diameter of the pelvis for the effective progress of labor.
Abnormal Presentations: The fetus in an abnormal presentation, such as the breech or face presentation, does not pass easily through the woman’s pelvis and interferes with the most efficient mechanisms of labor (see Chapter 6).
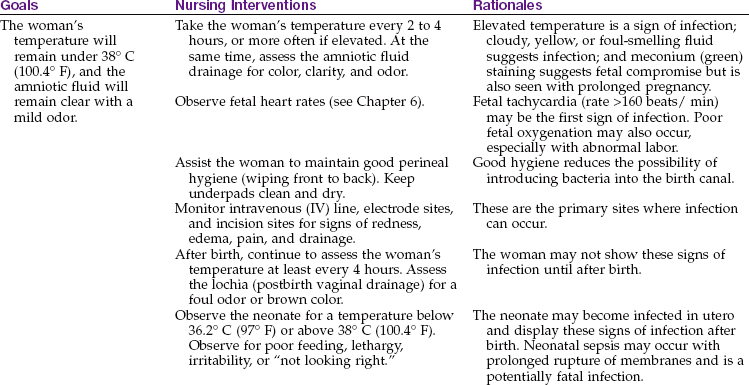
In the United States, most fetuses in the breech presentation are born by cesarean delivery. During vaginal birth in this presentation, the trunk and extremities are born before the head. After the fetal body delivers, the umbilical cord can be compressed between the fetal head and the mother’s pelvis. The head, which is the single largest part of the fetus, must be quickly delivered so the infant can breathe. Figure 8-6 illustrates the sequence of delivery for a vaginal breech birth.
FIGURE 8-6 The mechanism of labor in a breech birth. A, Breech before onset of labor. B, Engagement and internal rotation of buttocks. C, Lateral flexion. D, External rotation and restitution of buttocks. E, Internal rotation of shoulders and head. F, Face rotates to sacrum. Note that there is no flexion of the head so that the smallest diameter of the fetal head is not passing through the pelvis. The umbilical cord is compressed between the fetal head and the bony pelvis. G, The head is born as the fetal body is elevated.
Intrapartum nurses must be prepared to assist with a breech birth, because a woman sometimes arrives at the birth facility in advanced labor with her fetus in a breech presentation. External version is sometimes used to avoid the need for cesarean delivery in the case of a breech presentation; however, external version is not always successful, and the fetus sometimes returns to the abnormal presentation.
Abnormal Positions: A common cause of abnormal labor is a fetus that remains in a persistent occiput posterior position (left [LOP] or right [ROP]). The fetal occiput occupies either the left or the right posterior quadrant of the mother’s pelvis. In most women the fetal head rotates in a clockwise or counterclockwise direction until the occiput is in one of the anterior quadrants of the pelvis (left [LOA] or right [ROA]).
Labor is likely to be longer when rotation does not occur. Intense and poorly relieved back and leg pain characterizes labor when the fetus is in the occiput posterior position. Women with a small or average-size pelvis may have difficulty delivering infants who remain in an occiput posterior position. The physician may use forceps to rotate the fetal head into an occiput anterior position.
Nursing Care: During labor the nurse should encourage the woman to assume positions that favor fetal rotation and descent. These positions also reduce some of the back pain. Good positions for back labor include the following:
• Sitting, kneeling, or standing while leaning forward
• Rocking the pelvis back and forth while on hands and knees (Figure 8-7) to encourage rotation

FIGURE 8-7 The hands-and-knees position can help the fetus rotate from an occiput posterior to an occiput anterior position. Gravity causes the fetus to float downward toward the pool of amniotic fluid. This position can be practiced before labor.
• Side-lying (on the left side for an ROP position, on the right side for an LOP position)
• Squatting (for second-stage labor)
• Lunging by placing one foot in a chair with the foot and knee pointed to that side; lunging sideways repeatedly during a contraction for 5 seconds at a time
After birth, the mother and infant are observed for signs of birth trauma. The mother is more likely to have a hematoma of her vaginal wall if the fetus remained in the occiput posterior position for a long time. The infant may have excessive molding (alteration in shape) of the head, caput succedaneum (scalp edema, see Chapter 12), and possibly injury from forceps or the vacuum extractor.
Multifetal Pregnancy
If the woman has more than one fetus, several factors can make dysfunctional labor likely:
• Uterine overdistention contributes to poor contraction quality.
• Abnormal presentation or position of one or more fetuses interferes with labor mechanisms.
• Often one fetus is delivered as cephalic and the second as breech unless a version is done.
Because of the difficulties inherent in multifetal deliveries, cesarean birth is common. Birth is almost always cesarean if three or more fetuses are involved.
Nursing Care: When the woman has a multifetal pregnancy, each fetus is monitored separately during labor. An upright or side-lying position with the head slightly elevated aids breathing and is usually most comfortable. Labor care is similar to that for single pregnancies, with observations for hypotonic labor.
The nursery and intrapartum staffs prepare equipment and medications for every infant expected. An anesthesiologist and a pediatrician are often present at birth because of the potential for maternal or neonatal problems. One nurse is available for each infant. Another nurse focuses on the mother’s needs.
Problems with the Pelvis and Soft Tissues
Some women have a small or abnormally shaped pelvis that impedes the normal mechanisms of labor. The gynecoid pelvis is the most favorable for vaginal birth. Absolute pelvic measurements are rarely helpful to determine whether a woman’s pelvis is adequate for birth. A woman with a “small” pelvis may still deliver vaginally if other factors are favorable. She often delivers vaginally if her fetus is not too large, the head is well flexed, contractions are good, and her soft tissues yield easily to the forces of labor.
In contrast, some women have vaginally delivered several infants much larger than 9 lb (4082 g), yet others cannot deliver one weighing 10 lb (4536 g). Obviously, the pelvis of each was “adequate,” or even “large,” according to standard measurements. However, the pelvis was not large enough for her largest infant. The ultimate test of a woman’s pelvic size is whether her child fits through it at birth. A trial of labor may be indicated, and a cesarean delivery is done if necessary.
Soft Tissue Obstructions
The most common soft tissue obstruction during labor is a full bladder. The woman is encouraged to urinate every 1 or 2 hours. Catheterization may be needed if she cannot urinate, especially if a regional anesthetic or large quantities of IV fluids were given, which fill her bladder quickly yet reduce her sensation to void.
Less common soft tissue obstructions include pelvic tumors, such as benign (noncancerous) fibroids. Some women have a cervix that is scarred from previous infections or surgery. The scar tissue may not readily yield to labor’s forces to efface and dilate.
Problems with the Psyche
Labor is stressful, but women who have had prenatal care and have adequate social and professional support usually adapt to this stress and can labor and deliver normally. The most common factors that can increase stress and cause dystocia include lack of analgesic control of excessive pain, absence of a support person or coach to assist with nonpharmacological pain relief measures, immobility and restriction to bed, and a lack of ability to carry out cultural traditions.
Increased anxiety releases hormones such as epinephrine, cortisol, and adrenocorticotropic hormone that reduce contractility of the smooth muscle of the uterus. The body responds to stress with a “fight-or-flight” reaction that impedes normal labor by the following mechanisms:
• Using glucose the uterus needs for energy
• Diverting blood from the uterus
• Increasing tension of the pelvic muscles, which impedes fetal descent
• Increasing perception of pain, creating greater anxiety and stress and thus worsening the cycle
Nursing Care
Promoting relaxation and helping the woman conserve her resources for the work of childbirth are the principal nursing goals. The nurse uses every opportunity to spare her energy and promote her comfort (see Chapter 7).
Abnormal Duration of Labor
Any of the previously discussed factors may be associated with a long or difficult labor (dystocia). The average rate of cervical dilation during the active phase of labor is about 1.2 cm/hr for the woman having her first child and about 1.5 cm/hr if she has had a child before. Descent is expected to occur at a rate of at least 1.0 cm/hr in a first-time mother and 2.0 cm/hr in a woman who has had a child before.
A Friedman curve is often used to graph the progress of cervical dilation and fetal descent. The Friedman curve is used as a guide to assess and manage the normal progress of labor rather than using a rigid determination of “normal length of labor.” Nursing interventions such as encouraging pushing in the second stage of labor to be delayed until after full cervical dilation has occurred, alternative positioning of the patient during the first and second stages of labor, and electronic fetal monitoring along with the popular use of epidural anesthesia have had an impact on the length of the first and second stages of labor and the positive outcome for mother and newborn. Therefore the Friedman curve remains a management guide in assessing cervical dilation in relation to the descent of the fetal head. It may be referred to when determining the need for a cesarean section.
Prolonged labor can result in several problems, including the following:
• Maternal or newborn infection, especially if the membranes have been ruptured for a long time (usually about 24 hours)
• Postpartum hemorrhage (see Chapter 10)
In addition, mothers who have difficult and long labors are more likely to be anxious and fearful about their next labor.
Nursing Care: Nursing care focuses on helping the woman conserve her strength and encouraging her as she copes with the long labor. The nurse should observe for signs of infection during and after birth in both the mother (see Chapter 10) and the newborn (see Chapter 12).
Precipitate Birth
A precipitate birth is completed in less than 3 hours, and there may be no health care provider present. Labor often begins abruptly and intensifies quickly, rather than having a more subtle onset and gradual progression. Contractions may be frequent and intense, often from the onset. If the woman’s tissues do not yield easily to the powerful contractions, she may have uterine rupture, cervical lacerations, or hematoma.
Fetal oxygenation can be compromised by intense contractions because normally the placenta is resupplied with oxygenated blood between contractions. In precipitate labor, this interval may be very short. Birth injury from rapid passage through the birth canal may become evident in the infant after birth. These injuries can include intracranial hemorrhage or nerve damage.
Nursing Care: Women who experience precipitate birth may have panic responses about the possibility of not getting to the hospital in time or having their health care provider present. Although they are relieved after birth, they require continued support and reassurance concerning the deviation from their expected experience. After birth the nurse observes the mother and the infant for signs of injury. Excessive pain or bruising of the woman’s vulva is reported. Cold applications limit pain, bruising, and edema. Abnormal findings on the newborn’s assessment (see Chapter 12) are reported to the physician.
Premature Rupture of Membranes
Premature rupture of membranes (PROM) is spontaneous rupture of the membranes at term (38 or more weeks of gestation) more than 1 hour before labor contractions begin. A related term, preterm premature rupture of membranes (PPROM), is rupture of the membranes before term (before 37 weeks of gestation) with or without uterine contractions. Vaginal or cervical infection may cause prematurely ruptured membranes; it has been associated with nutritional deficiency involving copper and ascorbic acid (Hacker et al., 2009).
Diagnosis is confirmed by testing the fluid with nitrazine paper, which turns blue in the presence of amniotic fluid. A sample of vaginal fluid placed on a slide and sent to the laboratory will show a ferning pattern under the microscope, confirming that it is amniotic fluid (see Chapter 6). Treatment is based on weighing the risks of early delivery of the fetus against the risks of infection in the mother (chorioamnionitis, or inflammation of the fetal membranes) and sepsis in the newborn. An ultrasound determines gestational age, and oligohydramnios is confirmed if the amniotic fluid index (AFI) is less than 5 cm. Oligohydramnios in a gestation less than 24 weeks can lead to fetal pulmonary and skeletal defects. If PROM occurs at 36 weeks of gestation or later, labor is induced within 24 hours. Because the cushion of amniotic fluid is lost, the risk for umbilical cord compression is great.
Nursing Care: The nurse should observe, document, and report maternal temperature above 38° C (100.4° F), fetal tachycardia, and tenderness over the uterine area. Antibiotic and steroid therapy may be anticipated, cultures may be ordered, and labor may be induced or a cesarean section may be indicated. Nursing care for the woman who is not having labor induced immediately primarily involves monitoring and teaching the woman. Teaching combines information about infection and preterm labor and includes the following:
• Report a temperature that is above 38° C (100.4° F).
• Avoid sexual intercourse or insertion of anything in the vagina, which can increase the risk for infection.
• Avoid orgasm, which can stimulate contractions.
• Avoid breast stimulation, which can stimulate contractions because of natural oxytocin release.
• Maintain any activity restrictions prescribed.
• Note any uterine contractions, reduced fetal activity, or other signs of infection (see the section on amniotomy).
• Record fetal kick counts daily, and report fewer than 10 kicks in a 12-hour period.
Preterm Labor
Preterm labor occurs after 20 and before 37 weeks of gestation. The main risks are the problems of immaturity in the newborn. One goal of Healthy People 2020 is that 90% of all women will receive prenatal care starting in the first trimester. Preterm delivery is a major cause of perinatal morbidity and mortality and has a major medical and economic impact and is a factor, for example, in the rising costs of health care. Early prenatal care can prevent premature labor or identify women at risk (Box 8-2).
Early prenatal care allows women to be educated concerning signs of preterm labor so that interventions can occur early. Home uterine activity monitoring can be initiated for women at risk for preterm labor.
Signs of Impending Preterm Labor
A transvaginal ultrasound showing a shortened cervix at 20 weeks of gestation may be predictive of impending preterm labor. The ultrasound may be advised for high-risk women. A cervical or vaginal fetal fibronectin test has been approved by the Food and Drug Administration (FDA) (Hacker et al., 2009) for clinical use in the United States. Fibronectin is a protein produced by the fetal membranes that can leak into vaginal secretions if uterine activity, infection, or cervical effacement occurs. The presence of fibronectin in vaginal secretions between 22 and 24 weeks of gestation is predictive of preterm labor.
Levels of maternal corticotropin-releasing hormone (CRH) increase significantly in the weeks before preterm labor. Stress reduction and improved nutrition are indicated if CRH levels are high. Diagnosis of preterm labor is based on cervical effacement and dilation of more than 2 cm.
Maternal symptoms of preterm labor include the following:
• Contractions that may be either uncomfortable or painless
• Feeling that the fetus is “balling up” frequently
• Pelvic pressure or a feeling that the fetus is pushing down
• A change in the vaginal discharge
• Abdominal cramps with or without diarrhea
Laboratory tests include glucose level, electrolyte level, urinalysis and culture, and an ultrasound of the fetus to determine maturity, position, and other problems that may exist. Treatment of preterm labor is more aggressive at 28 weeks of gestation than at 34 weeks of gestation.
Tocolytic Therapy
The goal of tocolytic therapy is to stop uterine contractions and keep the fetus in utero until the lungs are mature enough to adapt to extrauterine life. Magnesium sulfate is the drug of choice for initiating therapy to stop labor. A continuous IV infusion is given, and therapeutic levels are monitored. Oral magnesium therapy may continue after contractions stop. The woman should be informed that a warm flush may be perceived during the initiation of therapy. Overdose can affect the cardiorespiratory system, and vital signs are recorded every hour. If the fetus is born during magnesium therapy, drowsiness may be present and resuscitation may be required. The nursery staff should be notified if magnesium sulfate therapy was used within 2 hours before delivery, because neonatal toxicity can result in serious complications in the newborn (Gibbs et al., 2008).
β-Adrenergic drugs such as terbutaline (Brethine) are given subcutaneously to stop uterine contractions. Cardiac side effects such as increased pulse rate and blood pressure can occur. Propranolol should be available to counter the effects of the drug. Ritodrine (Yutopar) may be given intravenously to stop preterm labor. Hypotension, cardiac dysrhythmia, and pulmonary edema may occur. Women with diabetes who are receiving these drugs must be closely monitored.
Prostaglandin synthesis inhibitors such as indomethacin are another type of drug used to stop labor contractions and can be given orally or rectally. This type of drug causes a reduction in amniotic fluid, which is helpful when polyhydramnios is a problem. However, this drug can stimulate the ductus arteriosus to close prematurely, causing fetal death. Close fetal monitoring is essential.
Calcium channel blockers such as nifedipine (Procardia) can be given orally to stop labor contractions. Because the drug causes vasodilation, maternal flushing and hypotension could be a side effect.
Antimicrobial therapy is often initiated in women with preterm labor because studies have shown that subclinical chorioamnionitis is often present (Hacker et al., 2009). Preventing this from spreading to the fetus improves the outcome of therapy.
Contraindications
Tocolytics should not be used in women with preeclampsia, placenta previa, abruptio placentae, chorioamnionitis, or fetal demise. In these cases it would not improve the obstetric outcome to delay birth of the fetus.
Stopping Preterm Labor
The initial measures to stop preterm labor include identifying and treating infection, activity restriction, and hydration.
Speeding Fetal Lung Maturation: If it appears that preterm birth is inevitable, the physician may give the woman steroid drugs (glucocorticoids) to increase fetal lung maturity if the gestation is between 24 and 34 weeks. Betamethasone may be given for this purpose in two intramuscular injections 24 hours apart. Thyroid hormones in the form of thyroid-releasing hormone (tRH) have been found to enhance pulmonary maturation in fetuses younger than 28 weeks (Hacker et al., 2009).
Activity Restrictions: Bed rest was often prescribed for women at risk for preterm birth. However, the benefits of bed rest are not clear, and many adverse maternal effects can occur. Therefore total bed rest is prescribed less frequently than in the past. Activity restrictions are often more moderate, such as resting in a semi-Fowler’s position or partial bed rest.
Nursing Care: Nurses should be aware of the symptoms of preterm labor because they may occur in any pregnant woman, with or without risk factors. Symptoms are taught and regularly reinforced for women who have increased risk factors. Nursing care includes positioning the woman on her side for better placental blood flow, assessing vital signs frequently, and notifying the health care provider if tachycardia occurs. Signs of pulmonary edema (chest pains, cough, crackles, or rhonchi) and intake and output should be closely monitored. If the woman is monitored at home, appropriate activities and restrictions are identified, and arrangements for household responsibilities such as child care should be made with family or with the help of social services. If delivery occurs, monitoring the fetal heart rate is essential, and preparation for admission to the neonatal intensive care unit is initiated. Full emotional support of the parents is offered because they may be grieving the loss of the normal birth process.
Prolonged Pregnancy
Prolonged pregnancy lasts longer than 42 weeks. Other terms that are often used interchangeably for prolonged pregnancy include postmature, postdate, or postterm. The term postmature most accurately describes the infant whose characteristics are consistent with a prolonged gestation (see Chapter 13).
Risks
The greatest risks of prolonged pregnancy are to the fetus. As the placenta ages, it delivers oxygen and nutrients to the fetus less efficiently. The fetus may lose weight, and the skin may begin to peel; these are the typical characteristics of postmaturity. Meconium may be expelled into the amniotic fluid, which can cause severe respiratory problems at birth. Low blood glucose levels are a likely complication after birth.
The fetus with placental insufficiency does not tolerate labor well. Because the fetus has less reserve than needed, the normal interruption in blood flow during contractions may cause excessive stress on the infant. If the placenta continues functioning well, the fetus continues growing. This can lead to a large fetus and the problems accompanying macrosomia.
There is little physical risk to the mother other than laboring with a large fetus if placental function remains normal. Psychologically, however, she often feels that pregnancy will never end. She becomes more anxious about when labor will begin and when her health care provider will “do something.”
Medical Treatment
The physician or nurse-midwife will evaluate whether the pregnancy is truly prolonged or if the gestation has been miscalculated. If the woman had early and regular prenatal care, ultrasound examinations have usually clarified her true gestation. Any pregnancy that lasts longer than 40 weeks must be monitored closely with twice weekly non–stress tests (NSTs), amniotic fluid indexes (AFIs), biophysical profiles (BPPs), and daily kick counts (see Chapter 5). Oligohydramnios (decreased amniotic fluid) in a postterm pregnancy is an indication for labor induction (Briscoe et al., 2005). If the woman’s pregnancy has definitely reached 42 weeks, labor is usually induced by oxytocin. Prostaglandin application to ripen the cervix before oxytocin administration increases the probability of successful induction.
Nursing Care
Nursing care involves careful observation of the fetus during labor to identify signs associated with poor placental blood flow, such as late decelerations (see Chapter 6). After birth, the newborn is observed for respiratory difficulties and hypoglycemia.
Emergencies during Childbirth
Several intrapartum conditions can endanger the life or well-being of the woman or her fetus. They necessitate prompt nursing and medical action to reduce the likelihood of damage. Nursing and medical management often overlap in emergencies.
Prolapsed Umbilical Cord
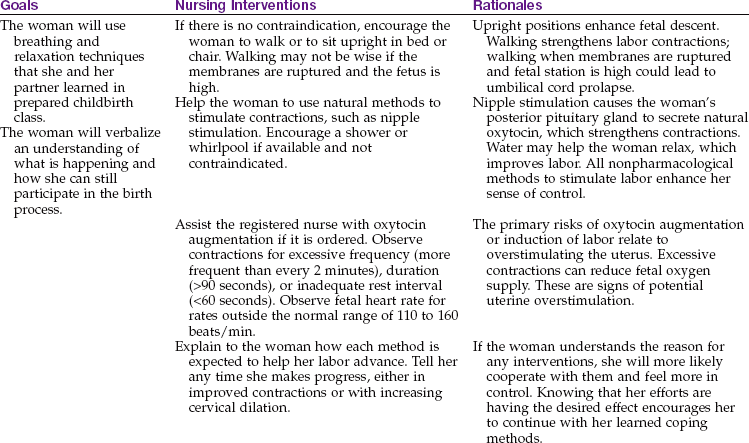
The umbilical cord prolapses if it slips downward in the pelvis after the membranes rupture. In this position, it can be compressed between the fetal head and the woman’s pelvis, interrupting blood supply to and from the placenta. It may slip down immediately after the membranes rupture, or the prolapse may occur later. A prolapsed cord (Figure 8-8) can be classified in the following ways:
FIGURE 8-8 Prolapsed umbilical cord. Note the pressure of the presenting part on the umbilical cord, which will interfere with oxygenation of the fetus. A, Occult (hidden) prolapse of cord. The cord will be compressed between the fetal head and the mother’s bony pelvis. B, Complete prolapsed cord. Note that the membranes are intact. C, Cord is presenting in front of the fetal head and may be seen in the vagina. D, Frank breech presentation with prolapsed cord.
• Complete: The cord is visible at the vaginal opening.
• Palpated: The cord cannot be seen but can be felt as a pulsating structure when a vaginal examination is done.
• Occult: The prolapse is hidden and cannot be seen or felt; it is suspected on the basis of abnormal fetal heart rates.
Risk Factors
Prolapse of the umbilical cord is more likely if the fetus does not completely fill the space in the pelvis or if fluid pressure is great when the membranes rupture. These conditions are more likely to occur in the following situations:
• The fetus is high in the pelvis when the membranes rupture (presenting part is not engaged).
• The fetus is very small, as in prematurity.
• There are abnormal presentations, such as footling breech or transverse lie.
Medical Treatment: The experienced physician may push the fetus upward from the vagina. Oxygen and a tocolytic drug such as terbutaline may be given. The primary focus is to deliver the fetus by the quickest means possible, usually cesarean delivery.
Nursing Care: The main risk of a prolapsed cord is to the fetus. When a prolapsed cord occurs, the first action is to displace the fetus upward to stop compression against the pelvis. Maternal positions such as the knee-chest or Trendelenburg (head down) can accomplish this displacement (Figure 8-9). Placing the mother in a side-lying position with her hips elevated on pillows also reduces cord pressure.
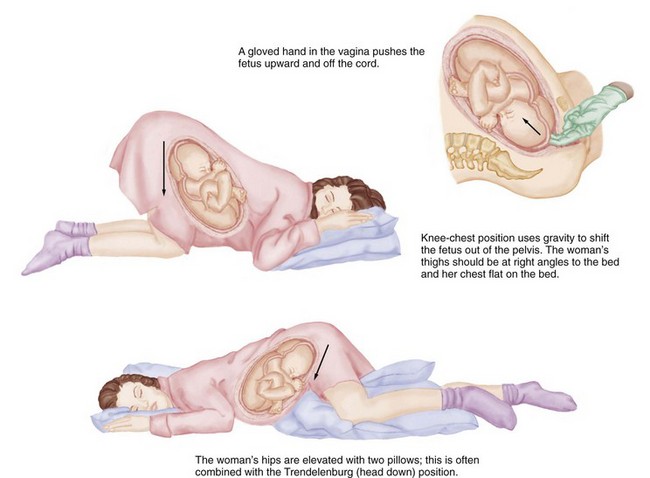
FIGURE 8-9 Positioning of the mother when the umbilical cord prolapses. These positions can be used to relieve pressure on the prolapsed umbilical cord until delivery can take place.
In addition to prompt corrective actions and assisting with emergency procedures, the nurse should remain calm to avoid increasing the woman’s anxiety. Prolapsed cord is a sudden development; anxiety and fear are inevitable reactions in the woman and her partner. Calm, quick actions on the part of nurses help the woman and her family to feel that she is in competent hands. After birth the nurse helps the woman to understand the experience. She may need several explanations of what happened and why.
Uterine Rupture
A tear in the uterine wall occurs if the muscle cannot withstand the pressure inside the organ. There are three variations of uterine rupture:
1. Complete rupture: There is a hole through the uterine wall, from the uterine cavity to the abdominal cavity.
2. Incomplete rupture: The uterus tears into a nearby structure, such as a ligament, but not all the way into the abdominal cavity.
3. Dehiscence: An old uterine scar, usually from a previous cesarean birth, separates.
Risk Factors
Uterine rupture is more likely to occur if the woman has had previous surgery on her uterus, such as a previous cesarean delivery. The low transverse uterine incision (see Figure 8-4) is least likely to rupture. Because the classic uterine incision is prone to rupture, a vaginal birth after this type of incision is not recommended. Uterine rupture may occur in the unscarred uterus if the woman:
Characteristics
The woman may have no symptoms, or she may have sudden onset of severe signs and symptoms, such as the following:
Medical Treatment
If the fetus is living when the rupture is detected and/or if blood loss is excessive, the physician performs surgery to deliver the fetus and to stop the bleeding. Hysterectomy (removal of the uterus) is likely for an extensive tear. Smaller tears may be surgically repaired.
Nursing Care
The nurse should be aware of women who are at high risk for uterine rupture. Women who are having a trial of labor after a previous cesarean section (VBAC) and women who are receiving oxytocin are at highest risk for uterine rupture and must be monitored closely during labor. When uterine rupture occurs, the woman is prepared for immediate cesarean section. Measures to alleviate anxiety in the woman and her partner are necessary as emergency measures are being initiated.
Uterine rupture is sometimes not discovered until after birth. In these cases the woman does not have dramatic symptoms of blood loss. However, she may have continuous bleeding that is brighter red than the normal postbirth bleeding. A rising pulse rate and falling blood pressure reading are signs of hypovolemic shock, which may occur if blood loss is excessive.
Uterine Inversion
Uterine inversion occurs if the uterus turns inside out after the infant is born. Inversion may be partial or complete. The physician may note a small depression in the top of the uterus or may discover that the uterus is not in the abdomen and protrudes from the vagina with its inner surface showing. Rapid onset of shock is common. Uterine inversion is more likely to occur if the uterus is not firmly contracted, especially if the health care provider pulls on the umbilical cord to deliver the placenta. Inversion can also occur during vigorous fundal massage when the uterus is not firm and is pushed downward toward the pelvis.
Medical Treatment
The physician will try to replace the inverted uterus while the woman is under general anesthesia. The anesthetic agent is chosen to cause uterine relaxation; tocolytic drugs also may be used. After the uterus is replaced, oxytocin is given to contract the uterus and control bleeding. If replacement of the uterus is not successful, the woman may require a hysterectomy.
Nursing Care
Nursing care during the emergency supplements medical management. Two IV lines are usually established to administer fluids and medications and to combat shock. During the recovery period the woman’s uterus is assessed at least every 15 minutes for firmness, height, and deviation from the midline; the lower uterus is supported at each assessment (see Chapter 9, Figure 9-2 and Skill 9-2). The woman’s vital signs and the amount of vaginal bleeding are assessed. An indwelling catheter may be used to keep her bladder empty so that the uterus can contract well. The catheter is assessed for patency and the output recorded; output may fall below 25 or 30 mL/hr with shock. The patient should take nothing orally until her condition is stable and the health care provider orders oral intake. After birth the nurse provides explanations and emotional support to the woman and her partner.
Amniotic Fluid Embolism
Amniotic fluid embolism occurs when amniotic fluid, with its particles such as vernix, fetal hair, and sometimes meconium, enters the woman’s circulation and obstructs small blood vessels in her lungs. It is more likely to occur during a very strong labor because the fluid is “pushed” into small blood vessels that rupture as the cervix dilates. Amniotic fluid embolism is characterized by abrupt onset of hypotension, respiratory distress, and coagulation abnormalities triggered by the thromboplastin contained in the amniotic fluid.
Treatment includes providing respiratory support with intubation and mechanical ventilation as necessary, treating shock with electrolytes and volume expanders, and replacing the coagulation factors such as platelets and fibrinogen. Packed red blood cells are sometimes given intravenously.
The woman’s intake and output are monitored closely. A pulse oximeter monitors oxygen saturation. The woman may be transferred to the intensive care unit for closer monitoring and nursing care.
Get Ready for the NCLEX® Examination!
Key Points
• The nurse observes the character of the amniotic fluid and fetal heart rate when the membranes are ruptured. Fluid should be clear and have a mild odor; the fetal heart rate should remain near its baseline level and between 110 and 160 beats/min at term.
• The nurse observes the fetal condition and character of contractions if any methods to stimulate labor are used. These methods may include walking, nipple stimulation, amniotomy, or oxytocin infusion.
• After version, the nurse observes for leaking amniotic fluid and for a pattern of contractions that may indicate labor has begun. Before discharge, signs of labor are reviewed with the woman so she will know when to return to the birth center.
• Nursing care after episiotomy or perineal lacerations includes comfort measures such as cold applications and analgesics.
• Nursing care after cesarean birth is similar to that after vaginal birth with the addition of assessing the wound, indwelling catheter patency, and intravenous flow. The woman and her partner may need extra emotional support after cesarean birth.
• Nursing measures such as encouraging position changes, aiding relaxation, and reminding the woman to empty her bladder can promote a more normal labor.
• Nursing care after births involving instruments (forceps or vacuum extraction) and after abnormal labor and birth includes observations for maternal and newborn injuries or infections. Infection is the most common hazard after membranes rupture prematurely, especially if there is a long interval before delivery.
• When oxytocin is given to the woman in labor, the nurse must be aware of signs and symptoms of increased uterine activity and monitor the fetal heart rate every 15 minutes during active labor and every 5 minutes during the transition phase.
• Nurses should be aware of the subtle symptoms a woman may have at the beginning of preterm labor and encourage her to seek care at the hospital promptly.
• After any type of emergency, the woman and her family need emotional support, explanations of what happened, and patience with their repeated questions.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Healthy People 2020: www.health.gov/healthypeople/document/tableofcontents.htm
• National Center for Health Statistics: www.cdc.gov/nchs/fastats
• Preterm labor: www.merck.com/mmpe/sec18/ch264/ch264k.html
Review Questions for the NCLEX® Examination
1. The nurse notes that a woman’s contractions during oxytocin induction of labor are every 2 minutes; the contractions last 95 seconds, and the uterus remains tense between contractions. What action is expected on the basis of these assessments?
1. No action is expected; the contractions are normal.
2. The rate of oxytocin administration will be increased slightly.
2. Select the appropriate nursing intervention during the early recovery period to increase the woman’s comfort if she had a forceps-assisted birth and a median episiotomy.
1. Application of a cold pack to her perineal area
2. Encouragement of perineal stretching exercises
3. A woman has an emergency cesarean delivery after the umbilical cord was found to be prolapsed. She repeatedly asks similar questions about what happened at birth. The nurse’s interpretation of the woman’s behavior is that she:
1. cannot accept that she did not have the type of delivery she planned.
2. is trying to understand her experience and move on with postpartum adaptation.
3. thinks the staff is not telling her the truth about what happened at birth.
4. is confused about events because the effects of the general anesthetic are persisting.
4. What nursing intervention during labor can increase space in the woman’s pelvis?
5. A woman is being observed in the hospital because her membranes ruptured at 30 weeks of gestation. While giving morning care, the nursing student notices that the draining fluid has a strong odor. The priority nursing action is to: