The Family After Birth
1 Define each key term listed.
2 Describe how to individualize postpartum and newborn nursing care for different patients.
3 Describe specific cultural beliefs that the nurse may encounter when providing postpartum and newborn care.
4 Describe postpartum changes in maternal systems and the nursing care associated with those changes.
5 Modify nursing assessments and interventions for the woman who has a cesarean birth.
6 Explain the emotional needs of postpartum women and their families.
7 Recognize the needs of a grieving parent.
8 Identify signs and symptoms that may indicate a complication in the postpartum mother or newborn.
9 Describe the nursing care of the normal newborn.
10 Describe nursing interventions to promote optimal infant nutrition.
11 Discuss the influences related to the choice of breastfeeding or bottle feeding the newborn.
12 Explain the physiological characteristics of lactation.
13 Compare various maternal and newborn positions used during breastfeeding.
14 Identify principles of breast pumping and milk storage.
15 Illustrate techniques of formula feeding.
16 Compare the nutrients of human milk with those of infant formulas.
17 Discuss the dietary needs of the lactating mother.
18 Discuss the principles of weaning the infant from the breast.
19 Plan appropriate discharge teaching for the postpartum woman and her newborn.
 , p. 223)
, p. 223) , p. 208)
, p. 208) , p. 223)
, p. 223) , p. 200)
, p. 200) , p. 201)
, p. 201) , p. 199)
, p. 199) http://evolve.elsevier.com/Leifer
http://evolve.elsevier.com/Leifer
The postpartum period, or puerperium, is the 6 weeks following childbirth. This period is often referred to as the fourth trimester of pregnancy. This chapter addresses the physiological and psychological changes in the mother and her family and the initial care of the newborn.
Adapting Nursing Care for Specific Groups and Cultures
The nurse must adapt care to a person’s circumstances, such as those of the single or adolescent parent, the poor, families who have a multiple birth, and families from other cultures.
Adolescents, particularly younger ones, need help to learn parenting skills. Their peer group is very important to them, so the nurse must make every effort during both pregnancy and the postpartum period to help them to fit in with their peers. They are often passive in caring for themselves and their infants. They may also be single and poor. Poor, young adolescent mothers often have several children in a short time, which compounds their social problems.
A single woman may have problems making postpartum adaptations if she does not have a strong support system. Often she must return to work very soon because she is the sole provider for her family.
Poor families may have difficulty meeting their basic needs before a new infant arrives, and a new family member adds to their strain. Women may have inadequate or sporadic prenatal care, which increases their risk for complications that extend into the puerperium and to their child. They may need social service referrals to direct them to public assistance programs or other resources.
Families who add twins (or more) face different challenges. The infants are more likely to need intensive care because of preterm birth, which delays the parents’ attachment and assumption of newborn care. It is also difficult for the parents to see the individuality of each infant, and they may be more likely to attach to them as a set. The infants may require care at a distant hospital if their problems are severe. Financial strains mount with each added problem.
Cultural Influences on Postpartum Care
The United States has a diverse population. Special cultural practices are often most evident at significant life events such as birth and death. The nurse must adapt care to fit the health beliefs, values, and practices of that specific culture to make the birth a meaningful emotional and social event as well as a physically safe event. See Chapter 6 for specific cultural practices during labor, delivery, and postpartum.
Using Translators
The nurse may need an interpreter to understand and provide optimal care to the woman and her family. If possible, when discussing sensitive information the interpreter should not be a family member, who might interpret selectively. The interpreter should not be of a group that is in social or religious conflict with the patient and her family, an issue that might arise in many Middle Eastern cultures. It is also important to remember that an affirmative nod from the woman may be a sign of courtesy to the nurse rather than a sign of understanding or agreement. Cultural preferences influence the presence of partners, parents, siblings, and children in the labor and delivery room (Figure 9-1).

Dietary Practices
Some cultures adhere to the “hot” and “cold” theory of diet after childbirth. Temperature has nothing to do with which foods are hot and which are cold; it is the intrinsic property of the food itself that classifies it. For example, “hot” foods include eggs, chicken, and rice. Women may also prefer their drinking water hot rather than cool or cold. Other hot-cold dietary practices include a balance between yin foods (e.g., bean sprouts, broccoli, and carrots) and yang foods (e.g., broiled meat, chicken, soup, and eggs).
Postpartum Changes in the Mother
Table 9-1 summarizes nursing assessments for the postpartum woman. See Chapter 10 for additional information about postpartum complications.
Table 9-1
Summary of Nursing Assessment Postpartum*
| ASSESSMENT | INTERVENTIONS |
| Vital signs | Report temperature above 38° C (100.4° F) or abnormal heart or respiratory rates |
| Fundus | Evaluate firmness, height, and location. |
| Lochia | Observe for character, color, amount, odor, and presence of clots. |
| Perineum | Observe for hematoma, edema, and episiotomy using REEDA scale; note hemorrhoids and degree of discomfort, if any. |
| Bladder | Observe for fullness, output, burning, and pain. |
| Breasts | Check for engorgement, nipple tenderness, and breastfeeding. |
| Bowels | Determine passage of flatus, bowel sounds, and defecation. |
| Pain | Determine location, character, severity, use of relief measures, and need for analgesics. |
| Extremities | Observe for signs of thrombophlebitis, ability to ambulate, and Homans sign. |
| Emotional | Evaluate family interaction, support, and any signs of depression. |
| Attachment | Observe for interest in newborn, eye contact, touch contact, and ability to respond to infant cries. |
| Cultural variations | Observe for cultural practices that the staff can incorporate into a plan of care. |
REEDA, Redness, edema, ecchymosis, drainage, approximation.
*Routine assessments are usually done every 4-6 hours unless risk factors exist. An acronym that helps remember and organize the postpartum assessment is BUBBLE-HE Breast; Uterus; Bladder; Bowels; Lochia; Episiotomy (perineum); Homans sign; Emotions or bonding.
Reproductive System
Following the third stage of labor, there is a fall in the blood levels of placental hormones, human placental lactogen, human chorionic gonadotropin, estrogen, and progesterone that help return the body to the prepregnant state. The most dramatic changes after birth occur in the woman’s reproductive system. These changes are discussed in the following sections, and the nursing care is discussed for each area as applicable.
Uterus
Involution refers to changes that the reproductive organs, particularly the uterus, undergo after birth to return them to their prepregnancy size and condition. The uterus undergoes a rapid reduction in size and weight after birth. The uterus should return to the prepregnant size by 5 to 6 weeks after delivery. The failure of the uterus to return to the prepregnant state after 6 weeks is called subinvolution (see Chapter 10).
Uterine Lining: The uterine lining (called the endometrium when not pregnant and the decidua during pregnancy) is shed when the placenta detaches. A basal layer of the lining remains to generate new endometrium to prepare for future pregnancies. The placental site is fully healed in 6 to 7 weeks.
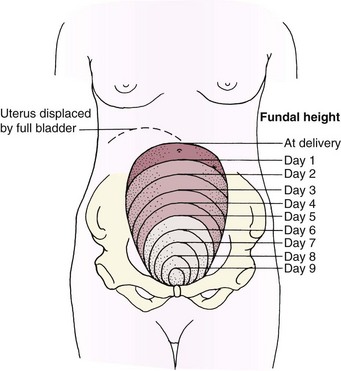
Descent of the Uterine Fundus: The uterine fundus (the upper portion of the body of the uterus) descends at a predictable rate as the muscle cells contract to control bleeding at the placental insertion site and as the size of each muscle cell decreases. Immediately after the placenta is expelled, the uterine fundus can be felt midline, at or below the level of the umbilicus, as a firm mass (about the size of a grapefruit). After 24 hours the fundus begins to descend about 1 cm (one finger’s width) each day. By 10 days postpartum, it should no longer be palpable (see Skill 9-2). A full bladder interferes with uterine contraction because it pushes the fundus up and causes it to deviate to one side, usually the right side (Figure 9-2).
 Nursing Tip
Nursing Tip
If the mother’s uterus is soft, massage it (supporting the lower segment), then expel clots so it will remain contracted. If her bladder is also full, massage the uterus until firm, and then address emptying the bladder. Control bleeding first, and then keep it controlled by emptying the bladder.
Afterpains: Intermittent uterine contractions may cause afterpains similar to menstrual cramps. The discomfort is self-limiting and decreases rapidly within 48 hours postpartum. Afterpains occur more often in multiparas or in women whose uterus was overly distended. Breastfeeding mothers may have more afterpains because infant suckling causes their posterior pituitary to release oxytocin, a hormone that contracts the uterus. Mild analgesics may be prescribed. Aspirin is not used postpartum because it interferes with blood clotting.
Lochia: Vaginal discharge after delivery, called lochia, is composed of endometrial tissue, blood, and lymph. Lochia gradually changes characteristics during the early postpartum period:
• Lochia rubra is red because it is composed mostly of blood; it lasts for about 3 days after birth.
• Lochia serosa is pinkish because of its blood and mucus content. It lasts from about the third through the tenth day after birth.
• Lochia alba is mostly mucus and is clear and colorless or white. It lasts from the tenth through the twenty-first day after birth.
Lochia has a characteristic fleshy or menstrual odor; it should not have a foul odor. The woman’s fundus should be checked for firmness, because an uncontracted uterus allows blood to flow freely from vessels at the placenta insertion site.
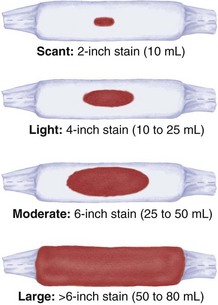
Many facilities use perineal pads that contain cold or warm packs. These pads absorb less lochia, and that fact must be considered when estimating the amount (Skill 9-1). If a mother has excessive discharge of lochia, a clean pad should be applied and checked within 15 minutes. The peripads applied during a given time period are counted or weighed to help determine the amount of vaginal discharge. One gram of weight equals about a 1-mL volume of blood. The nurse should assess the underpads on the bed to determine if bleeding has overflowed onto the bed linen.
Skill 9-1 Estimating the Volume of Lochia








The flow of lochia is briefly heavier when the mother ambulates, because lochia pooled in the vagina is discharged when she assumes an upright position. A few small clots may be seen at this time, but large clots should not be present. The quantity of lochia may briefly increase when the mother breastfeeds, because suckling causes uterine contraction. The rate of discharge increases with exercise. Women who had a cesarean birth have less discharge of lochia during the first 24 hours because the uterine cavity was sponged at delivery. The absence of lochia is not normal and may be associated with blood clots retained within the uterus or with infection.
Nursing Care: The fundus is assessed at routine intervals for firmness, location, and position (Skill 9-2) in relation to the midline. Women who have a higher risk for postpartum hemorrhage (see Chapter 10) should be assessed more often. While doing early assessments, the nurse explains the reason they are done and teaches the woman how to assess her fundus. If her uterus stops descending, she should report that to her birth attendant.
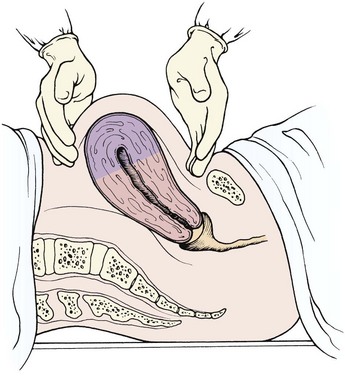
Skill 9-2 Observing and Massaging the Uterine Fundus
1. Identify the need for fundal massage. The uterus will be soft and usually higher than the umbilicus. A firm fundus does not need massage.
2. Place the woman in a supine position with the knees slightly flexed. Lower the perineal pad to observe lochia as the fundus is palpated.
3. Place the outer edge of nondominant hand just above the symphysis pubis, and press downward slightly to anchor the lower uterus.
4. Locate and massage the uterine fundus with the flat portion of the fingers of the dominant hand in a firm, circular motion.
5. When the uterus is firm, gently push downward on the fundus, toward the vaginal outlet, to expel blood and clots that have accumulated inside the uterus. Keep the other hand on the lower uterus to avoid inverting it.
6. If a full bladder contributes to uterine relaxation, have the mother void. Catheterize her (with a health care provider’s order) if she cannot void.
7. Document the consistency and location of the fundus before and after massage.
8. Give any prescribed medications, such as oxytocin, to maintain uterine contraction. Have the mother nurse her infant if she is breastfeeding to stimulate the secretion of natural oxytocin.
A poorly contracted (soft or boggy) uterus should be massaged until firm to prevent hemorrhage. Lochia flow may increase briefly as the uterus contracts and expels it. It is essential not to push down on an uncontracted uterus to prevent inverting it. If a full bladder contributes to poor uterine contraction, the mother should be assisted to void in the bathroom or on a bedpan if she cannot ambulate. Catheterization may be necessary if she cannot void.
The woman should be taught the expected sequence for lochia changes and the amount she should expect. The woman should report any of the following abnormal characteristics:
• Foul-smelling lochia, with or without fever
• Lochia rubra that persists beyond the third day
• Unusually heavy flow of lochia
• Lochia that returns to a bright red color after it has progressed to serosa or alba
Medications that may be given to stimulate uterine contraction include the following:
• Oxytocin (Pitocin), often routinely given in an intravenous infusion after birth
• Methylergonovine (Methergine), given intramuscularly or orally
An infant suckling at the breast has a similar effect because natural oxytocin release stimulates contractions.
Mild analgesics relieve afterpains adequately for most women. The breastfeeding mother should take an analgesic immediately after breastfeeding to minimize sedation and side effects passing to the newborn. Afterpains persisting longer than the expected time should be reported.
Cervix
The cervix regains its muscle tone but never closes as tightly as during the prepregnant state. Some edema persists for a few weeks after delivery. A constant trickle of brighter red lochia is associated with bleeding from lacerations of the cervix or vagina, particularly if the fundus remains firm.
Vagina
The vagina undergoes a great deal of stretching during childbirth. The rugae, or vaginal folds, disappear, and the walls of the vagina become smooth and spacious. The rugae reappear 3 weeks postpartum. Within 6 weeks the vagina has regained most of its prepregnancy form, but it never returns to the size it was before pregnancy.
Nursing Care: Couples often are hesitant to ask questions concerning resumption of sexual activity after childbirth, and many resume activity before the 6-week checkup. It is important for the nurse to teach the woman that it is considered safe to resume sexual intercourse when bleeding has stopped and the perineum (episiotomy) has healed. However, the vagina does not lubricate well in the first 6 weeks after childbirth (or longer in the breastfeeding mother). A water-soluble gel such as K-Y or a contraceptive gel can be used for lubrication to make intercourse more comfortable. Instructing the woman to correctly perform the Kegel exercise helps her strengthen muscles involved in urination, bowel function, and vaginal sensations during intercourse.
Perineum
The perineum is often edematous, tender, and bruised. An episiotomy (incision to enlarge the vaginal opening) may have been done, or a perineal laceration may have occurred. Women with hemorrhoids often find that these temporarily worsen during the pressure of birth.
Nursing Care: The perineum should be assessed for normal healing and signs of complications (Skill 9-3). The REEDA acronym helps the nurse remember the five signs to assess.
Skill 9-3 Assessing the Perineum
1. Provide privacy; explain purpose of procedure.
2. Put on gloves (provide protection from contact of bodily fluids).
3. Ask woman to turn on side and flex upper leg, lower perineal pad, and lift up upper buttock; if necessary, use flashlight to inspect perineum.
4. Observe for edema, bruising, and hematoma.
5. Examine episiotomy or laceration for REEDA (redness, edema, ecchymosis, discharge, and approximation).
6. Observe hemorrhoids for extent of edema (can interfere with bowel elimination).
7. Apply clean peripads, taking care to only touch edges.
8. Reposition woman into position of comfort.
9. Dispose of soiled contents in appropriate waste container, and wash hands.
 Memory Jogger
Memory Jogger
Redness. Redness without excessive tenderness is probably the normal inflammation associated with healing, but pain with the redness is more likely to be infection.
Edema. Mild edema is common, but severe edema interferes with healing.
Ecchymosis (bruising). A few small superficial bruises are common. Larger bruises interfere with normal healing.
Discharge. No discharge from the perineal suture line should be present.
Approximation (intactness of the suture line). The suture line should not be separated. If intact, it is almost impossible to distinguish the laceration or episiotomy from surrounding skin folds.
Note: The REEDA acronym is also useful when assessing a cesarean incision for healing.
Comfort and hygienic measures are the focus of nursing care and patient teaching. An ice pack or chemical cold pack is applied for the first 12 to 24 hours to reduce edema and bruising and numb the perineal area. A disposable rubber glove filled with ice chips and taped shut at the wrist can also be used. The cold pack should be covered with a paper cover or a washcloth. When the ice melts, the cold pack is left off for 10 minutes before applying another for maximum effect. In some cultures, women believe that heat has healing properties and may resist the use of an ice pack.
After 24 hours, heat in the form of a chemical warm pack, a bidet, or a sitz bath increases circulation and promotes healing. The sitz bath may circulate either cool or warm water over the perineum to cleanse the area and increase comfort. Sitting in 4 to 5 inches of water in a bathtub has a similar effect (Skill 9-4).
Skill 9-4 Assisting with a Sitz Bath
1. Wash hands, explain procedure, and provide privacy.
2. Assess woman’s condition; analyze appropriateness of procedure.
3. Place sitz bath on toilet seat; turn flow of water on.
4. Help woman remove pad and sit in flow of water for 20 minutes.
5. When completed, assist woman to pat perineum dry (front to back); apply clean perineal pad.
6. Assist woman in returning to room (then to chair or bed).
8. Record in medical record that sitz bath was taken, condition of woman, and condition of perineum.

The woman is taught to do perineal care after each voiding or bowel movement to cleanse the area without trauma. A plastic bottle (peribottle) is filled with warm water, and the water is squirted over the perineum in a front-to-back direction. The perineum is blotted dry. Perineal pads should be applied and removed in the same front-to-back direction to prevent fecal contamination of the perineum and vagina (Skill 9-5).
Skill 9-5 Performing Perineal Care
2. Explain procedure to woman.
3. Assist the woman to the bathroom.
4. Instruct woman to wash her hands before and after each perineal care.
5. Remove soiled pad from front to back; discard in appropriate waste container.
6. Squeeze peribottle or pour warm water or cleansing solution over perineum without opening labia.
7. Pat dry with clean tissue. Use each tissue one time. Pat from front to back, then discard tissue.
8. Apply medicated ointments or sprays as directed. Do not apply perineal pad for 1 to 2 minutes (otherwise the medication will be absorbed in the pad).
9. Apply clean perineal pad from front to back, touching only side and outside of pad to lessen risk of infection.
10. Do not flush toilet until woman is standing upright; otherwise, the flushing water can spray the perineum.
11. Always perform perineal care after each voiding, stool, or at least every 4 hours during puerperium.
12. Report clots, increase in lochia flow, or excessive abdominal cramping.
Topical and systemic medications may be used to relieve perineal pain. Topical perineal medications reduce inflammation or numb the perineum. Commonly prescribed medications include the following:
In addition to these topical medications, witch hazel pads (Tucks) and sitz baths reduce the discomfort of hemorrhoids.
To reduce pain when sitting, the mother can be taught to squeeze her buttocks together as she lowers herself to a sitting position and then to relax her buttocks. An air ring, or “donut,” takes pressure off the perineal area when sitting. The mother should inflate the ring about halfway. (If it is inflated fully, she tends to topple off when she sits on it.) A small eggcrate pad is an alternative to the air ring.
Return of Ovulation and Menstruation
The production of placental estrogen and progesterone stops when the placenta is delivered, causing a rise in the production of follicle-stimulating hormone and the return of ovulation and menstruation. Menstrual cycles resume in about 6 to 8 weeks if the woman is not breastfeeding. The early menstrual periods may or may not be preceded by ovulation. Return of ovulation is more delayed in the breastfeeding mother. However, ovulation may occur at any time after birth, with or without menstrual bleeding, and pregnancy is possible. Therefore pregnancy can occur unless birth control is practiced. Regular oral contraceptives are not used during early breastfeeding, but a minipill can be used effectively.
Breasts
Both nursing and nonnursing mothers experience breast changes after birth. Assessments for both types of mothers are similar, but nursing care differs.
Changes in the Breasts: For the first 2 or 3 days the breasts are full but soft. By the third day the breasts become firm and lumpy as blood flow increases and milk production begins. Breast engorgement may occur in both nursing and nonnursing mothers. The engorged breast is hard, erect, and very uncomfortable. The nipple may be so hard that the infant cannot easily grasp it. The breasts of the nonnursing mother return to their normal size in 1 to 2 weeks.
Nursing Care: At each assessment the nurse checks the woman’s breasts for consistency, size, shape, and symmetry. The nipples are inspected for redness and cracking, which makes breastfeeding more painful and offers a port of entry for microorganisms. Flat or inverted nipples make it more difficult for the infant to grasp the nipple and suckle.
Both nursing and nonnursing mothers should wear a bra to support the heavier breasts. The bra should firmly support the nursing mother’s breasts but not be so tight that it impedes circulation. Some nonnursing mothers may prefer to wear an elastic binder to suppress lactation.
The nonnursing mother should avoid stimulating her nipples, which stimulates lactation. She should wear a bra at all times to avoid having her clothing brush back and forth over her breasts and should stand facing away from the water spray in the shower.
The nipples should be washed with plain water to avoid the drying effects of soap, which can lead to cracking. The nonnursing woman should minimize stimulation when washing her breasts. Breastfeeding is discussed on pp. 221-229.
Cardiovascular System
Cardiac Output and Blood Volume
Because of a 50% increase in blood volume during pregnancy, the woman tolerates the following normal blood loss at delivery:
Despite the blood loss there is a temporary increase in blood volume and cardiac output because blood that was directed to the uterus and the placenta returns to the main circulation. Added fluid also moves from the tissues into the circulation, further increasing her blood volume. The heart pumps more blood with each contraction (increased stroke volume), leading to bradycardia. After the initial postbirth excitement wanes, the pulse rate may be as low as 50 to 60 beats/min for about 48 hours after birth. To reestablish normal fluid balance, the body rids itself of excess fluid in the following two ways:
Coagulation
Blood clotting factors are higher during pregnancy and the puerperium, yet the woman’s ability to lyse (break down and eliminate) clots is not increased. Therefore she is prone to blood clot formation, especially if there is stasis of blood in the venous system. This situation is more likely to occur if the woman has varicose veins, has had a cesarean birth, or must delay ambulation. Dyspnea (difficult breathing) and tachypnea (rapid breathing) are hallmark signs of a pulmonary embolus and necessitates immediate medical intervention.
Blood Values
The massive fluid shifts just described affect blood values such as hemoglobin and hematocrit, making them difficult to interpret during the early puerperium. Fluid that shifts into the bloodstream dilutes the blood cells, which lowers the hematocrit. As the fluid balance returns to normal, the values are more accurately interpreted, usually by 8 weeks postpartum.
The white blood cell (leukocytes) count may rise as high as 12,000 to 20,000/mm3, a level that would ordinarily suggest infection. The increase is in response to inflammation, pain, and stress, and it protects the mother from infection as her tissues heal. The white blood cell count returns to normal by 12 days postpartum.
Chills
Many mothers experience tremors that resemble shivering or “chills” immediately after birth. This tremor is thought to be related to a sudden release of pressure on the pelvic nerves and a vasomotor response involving epinephrine (adrenaline) during the birth process. Most women will deny feeling cold. These tremors or “chills” stop spontaneously within 20 minutes. The nurse should reassure the woman and cover her with a warm blanket to provide comfort. Chills accompanied by fever after the first 24 hours suggest infection and should be reported.
Orthostatic Hypotension
Resistance to blood flow in the vessels of the pelvis drops after childbirth. As a result, the woman’s blood pressure falls when she sits or stands, and she may feel dizzy or lightheaded or may even faint. Guidance and assistance are needed during early ambulation to prevent injury.
Nursing Care: After the fourth stage, vital signs are taken every 4 hours for the first 24 hours. The temperature may rise to 38° C (100.4° F) in the first 24 hours. A higher temperature or the persistence of a temperature elevation for more than 24 hours suggests infection. The pulse rate helps to interpret temperature and blood pressure values. Because of the normal postpartum bradycardia, a high pulse rate often indicates infection or hypovolemia.
If diaphoresis bothers the woman, she should be reminded that it is temporary. The nurse should help her shower or take a sponge bath and provide dry clothes and bedding.
The nurse checks for the presence of edema in the lower extremities, hands, and face. Edema in the lower extremities is common, as it is during pregnancy. Edema above the waist is more likely to be associated with pregnancy-induced hypertension, which can continue during the early postpartum period.
The woman’s legs should be checked for evidence of thrombosis at each assessment, looking for a reddened, tender area (superficial vein) or edema, pain and, sometimes, pallor (deep vein). Homans sign (calf pain when the foot is passively dorsiflexed) is of limited value in identifying thrombosis in the postpartum phase (see Chapter 10). Early and regular ambulation reduces the venous stasis that promotes blood clots.
Urinary System
Kidney function returns to normal within a month after birth. A decrease in the tone of the bladder and ureters as a result of pregnancy combined with intravenous fluids administered during labor may cause the woman’s bladder to fill quickly but empty incompletely during the postpartum period. This can lead to postpartum hemorrhage when the full bladder displaces the uterus, or a possible urinary tract infection because of stasis of the urine in the bladder.
Nursing Tip
The woman who voids frequent, small amounts of urine may have increased residual urine because her bladder does not fully empty. Residual urine in the bladder may promote the growth of microorganisms.
Nursing Care: The nurse should regularly assess the woman’s bladder for distention. The bladder may not feel full to her, yet the uterus is high and deviated to one side. If she can ambulate, the mother should go to the bathroom and urinate. The first two to three voidings after birth or after catheter removal are measured. Women who receive intravenous infusions or have an indwelling catheter continue to have their urine output measured until the infusion and/or catheter are discontinued. The following measures may help a woman to urinate:
• Provide as much privacy as possible.
• Remain near the woman, but do not rush her by constantly asking her if she has urinated.
• Have the woman place her hands in warm water.
• Have the woman use the peribottle to squirt warm water over her perineal area to relax the urethral sphincter. Be sure to measure the amount of water in the peribottle when it is filled so the amount used can be deducted from the amount of urine voided.
Some discomfort with early urination is expected because of the edema and trauma in the area. However, continued burning or urgency of urination suggests bladder infection. High fever and chills may occur with kidney infection.
Gastrointestinal System
The gastrointestinal system resumes normal activity shortly after birth when progesterone decreases. The mother is usually hungry after the hard work and food deprivation of labor. The nurse should expect to provide food and water to a new mother often!
Constipation may occur during the postpartum period owing to several factors:
• Medications may slow peristalsis.
• Abdominal muscles are stretched, making it more difficult for the woman to bear down to expel stool. A cesarean incision adds to this difficulty.
• Soreness and swelling of the perineum or hemorrhoids may make the woman fear her first bowel movement.
• Slight dehydration and little food intake during labor make the feces harder.
Nursing Care: The mother is encouraged to drink lots of fluids, add fiber to her diet, and ambulate. A stool softener such as docusate calcium (Surfak) or docusate sodium (Colace) is usually ordered. These measures are generally sufficient to correct the problem. Because constipation is a common problem during pregnancy, measures she has used to relieve it are discussed at that time and efforts are made to build on her knowledge. A common laxative is bisacodyl (Dulcolax), given orally or as a suppository when a laxative is indicated.
Integumentary System
Hyperpigmentation of the skin (“mask of pregnancy,” or chloasma, and the linea nigra) disappears as hormone levels decrease. Striae (“stretch marks”) do not disappear but fade from reddish purple to silver.
Musculoskeletal System
The abdominal wall has been greatly stretched during pregnancy and may now have a “doughy” appearance. Many women are dismayed to discover that they still look pregnant after they give birth. They should be reassured that time and exercise can tighten their lax muscles. Also, some women have diastasis recti, in which the longitudinal abdominal muscles that extend from the chest to the symphysis pubis are separated. Abdominal wall weakness may remain for 6 to 8 weeks and contribute to constipation. Hypermobility of the joints usually stabilizes within 6 weeks, but the joints of the feet may remain separated and the new mother may notice an increase in shoe size. The center of gravity of the body returns to normal when the enlarged uterus returns to its prepregnant size.
A woman can usually begin light exercises as soon as the first day after vaginal birth. Women who have undergone a cesarean birth may wait longer. The woman should consult her health care provider for specific instructions about exercise. Common postpartum exercises include the following:
• Abdominal tightening. In the supine or erect position, the woman inhales slowly and then exhales slowly while contracting her abdominal muscles. After a count of 10, she relaxes the muscles. She should begin with 3 repetitions and increase the number to 5, then 10. This may be done 3 times and then 5 times daily, up to 10 times each day.
• Head lift. The woman lies flat on her bed with her knees bent and inhales. While exhaling, she lifts her head, chin to chest, and looks at her thighs. She holds this position to a count of three, and then relaxes. This is repeated several times. After the third week (or when the health care provider permits), the head lift may progress to include the head and shoulders. This may be done 5 to 10 times daily.
• Pelvic tilt. While lying supine with her knees bent and feet flat, the woman inhales and exhales, flattening her lower back to the bed or exercise surface and contracting her abdominal muscles. She holds the position to a count of three. She begins with 5 repetitions and works up to 10 repetitions daily.
• Kegel exercises. Perineal exercises may be resumed immediately after birth to promote circulation and healing. The mother tightens the muscles of the perineal area, as if to stop the flow of urine, and then relaxes them. She should inhale, tighten for a count of 10, exhale, and relax. She may do the exercise five times each hour for the first few days. Then she may increase the number of repetitions. She should not actually stop her urine flow when urinating, however, because this could lead to urine stasis and urinary tract infection.
Immune System
Prevention of blood incompatibility and infection are addressed in the postpartum period according to each woman’s specific needs.
Rho(D) Immune Globulin
The woman’s blood type and Rh factor and antibody status are determined on an early prenatal visit or on admission if she did not have prenatal care. The Rh-negative mother should receive a dose of Rho(D) immune globulin (RhoGAM) within 72 hours after giving birth to an Rh-positive infant. This prevents sensitization to Rh-positive erythrocytes that may have entered her bloodstream when the infant was born. RhoGAM is given to the mother, not the infant, by intramuscular injection into the deltoid muscle. The woman receives an identification card stating that she is Rh negative and has received RhoGAM on that date.
Rubella (German Measles) Immunization
Rubella titers are done early in pregnancy to determine if a woman is immune to rubella. A titer of 1:8 or greater indicates immunity to the rubella virus. The mother who is not immune is given the vaccine in the immediate postpartum period. The vaccine prevents infection with the rubella virus during subsequent pregnancies, which could cause birth defects. A signed informed consent is usually required to administer the rubella vaccine.
The rubella vaccine is given subcutaneously in the upper arm. The woman should not get pregnant for the next 1 month. The vaccine should not be administered if she is sensitive to neomycin. Women vaccinated during the postpartum period may breastfeed without adverse affects on the newborn (CDC, 2009).
Adaptation of Nursing Care following Cesarean Birth
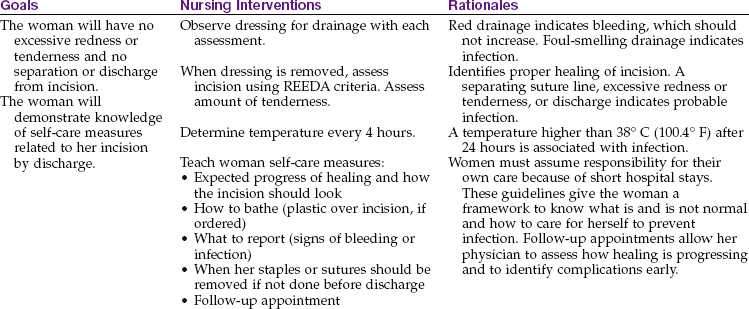
The woman who has a cesarean birth has had surgery as well as given birth. Many of her reactions to the surgical birth depend on whether she expected it. The woman who had an unexpected, emergency cesarean often has many questions about what happened to her and why, because there was no time to answer these questions at the time of birth. In addition, her anxiety may have limited her ability to comprehend any explanations given. Occasionally a woman may feel that she failed if she was unable to give birth after laboring. Terms such as failed induction and failure to progress imply that the woman herself was not competent in some way. Some variations of normal postpartum care are needed for the woman who has a cesarean birth (Nursing Care Plan 9-1).
9-1  Nursing Care Plan
Nursing Care Plan
The Woman Having a Cesarean Birth
Uterus
The nurse should check the fundus as on any new mother; it descends at a similar rate. Checking her fundus when a woman has a transverse skin incision is not much different from checking the woman who had vaginal birth. If she has a vertical skin incision, the nurse should gently “walk” the fingers toward the fundus from the side to her abdominal midline. If the fundus is firm and at its expected level, no massage is necessary.
Lochia
Lochia is checked at routine assessment intervals, which vary with the time since birth. The quantity of lochia is generally less immediately after cesarean birth because surgical sponges have removed the contents of the uterus.
Dressing
The dressing should be checked for drainage as with any surgical patient. When the dressing is removed, the incision is assessed for signs of infection. The wound should be clean and dry, and the staples should be intact. The REEDA acronym previously described is a good way to remember key items to check on an incision: redness, edema, ecchymosis, drainage, and approximation. Staples may be removed and Steri-Strips applied shortly before hospital discharge on the third day. If a woman leaves earlier, the staples may be removed in her health care provider’s office.
The woman can shower as soon as she can ambulate reliably. A shower chair reduces the risk for fainting. The dressing or incision can be covered with a plastic wrap, and the edges secured with tape. The woman should be told to position herself with her back to the water stream. The dressing is changed after the woman finishes her shower. A similar technique can be used to cover an intravenous infusion site. If the infusion site is in her hand, a glove can cover it.
Urinary Catheter
An indwelling urinary catheter is generally removed within 24 hours of delivery. Urine is observed for blood, which may indicate trauma to the bladder during labor or surgery. The blood should quickly clear from the urine as diuresis occurs. Intake and output are measured until both the intravenous infusion and the catheter are discontinued. The first two to three voidings are measured, or until the woman urinates at least 150 mL. The nurse should observe and teach the woman to observe for the following signs of urinary tract infection because use of a catheter increases this risk:
Frequency of urination is hard to assess in any postpartum woman because of normal postpartum diuresis. However, frequent voidings of small quantities of urine, especially if associated with the described signs and symptoms, suggest a urinary tract infection.
Respiratory Care
Lung sounds should be auscultated each shift for clarity. Diminished breath sounds, crackles, or wheezes indicate that lung secretions are being retained. When she is confined to bed, the woman should take deep breaths and turn from side to side every 2 hours. She should be encouraged to cough to move secretions out of her lungs. To reduce incisional pain from coughing or other movement, the nurse can have the woman hold a small pillow or folded blanket firmly against her incision. An incentive spirometer may be used to give the woman a “target” for deep breaths. The woman should begin ambulating as early as possible to mobilize lung secretions.
Preventing Thrombophlebitis
The woman who has undergone a cesarean birth has a greater risk for thrombophlebitis. She should do simple leg exercises, such as alternately flexing and extending her feet or moving her legs from a flexed to an extended position when turning. The nurse should assess for signs of thrombosis as previously described. Early and frequent ambulation also reduces the risk for thrombophlebitis.
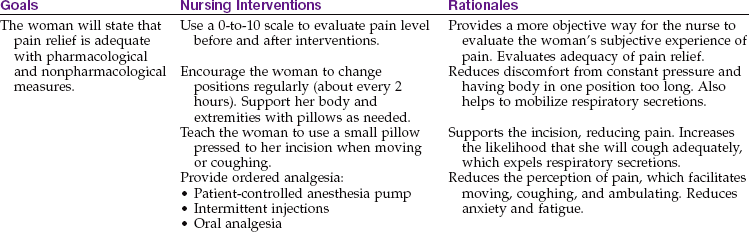
Pain Management
Pain control is essential to reduce the woman’s distress and facilitate movement that can prevent several complications. The severity, frequency, character, and location of discomfort are assessed. Using a 0-to-10 scale helps to quantify the subjective experience of pain better. Zero would be no pain at all, and 10 would be the worst pain ever. The scale helps the nurse to choose the most appropriate relief methods and provides a method to evaluate the amount of relief the woman receives from the pain interventions.
Some women receive epidural narcotics for long-lasting pain relief. These drugs can cause respiratory depression many hours after they are given, sometimes up to 24 hours. Therefore hourly respiratory monitoring and a pulse oximeter are usual until the drug’s effects have worn off. Naloxone (Narcan) should be readily available to reverse the respiratory depression. If the woman has pain not controlled by the epidural narcotic, the health care provider must be consulted for specific orders.
Many women have a patient-controlled analgesia (PCA) pump to provide them with analgesia. The pump has a syringe of a narcotic analgesic inside. It is programmed to deliver a specific dose of the drug when the woman pushes a button. To prevent overdose, there is a lockout interval during which pushing the button has no effect. As with any narcotic, the drug inside the PCA pump is counted at shift change, and the facility’s protocol for record keeping is followed to account for all drug doses received, remaining, or wasted when the PCA drug is discontinued.
Most women change to an oral analgesic on the day after surgery. The woman should be instructed to call for pain medication when she first becomes uncomfortable. Pain is much harder to relieve if it becomes severe.
The breastfeeding mother should be reassured that timing the administration of analgesia immediately after breastfeeding minimizes passage via breast milk to the infant. It can be explained that adequate pain control helps her to relax so she can breastfeed better and have the energy to become acquainted with her infant.
Emotional Care
The birth of an infant brings about physical changes in the mother but also causes many emotional and relationship changes in all family members.
Mothers
The transition to motherhood brings many hormonal changes, changes in body image, and psychological acceptance of the self as a mother figure. Fluctuating hormones in pregnancy and the puerperium have an effect on mood, causing early elation at delivery that can be followed by mild depression with tearfulness, irritability, and fatigue peaking on the fifth day postpartum. Most women recover in a few days. However, the physiological factors that affect mood can interact with minor anxieties and stresses to result in a clinical depression. Rubin (1967) has described three phases of postpartum change that have been a framework for nursing care for 35 years (Box 9-1). More recent studies have found that women progress through the same three phases, although at a more rapid pace than originally described. The nurse can refer to the three phases when providing postpartum care.
Postpartum Blues
New mothers often experience conflicting feelings of joy and emotional letdown during the first few weeks after birth, often called the postpartum blues, or the baby blues. She may feel let down, but overall she finds pleasure in life. The symptoms are self-limiting. When providing discharge teaching, the nurse should prepare the woman for these feelings and reassure her that they are normal and temporary.
Postpartum Depression
Postpartum depression is a persistent mood of unhappiness discussed in Chapter 10. When teaching about the postpartum blues as described above, the nurse should explain that persistent depression is not expected and should be reported to her health care provider.
Fatigue
Postpartum assessment typically includes physical assessment and psychological bonding and must also include evaluation for fatigue (Benson-Soros & Glazer, 2005). Today’s modern lifestyle often has the woman working through most of her pregnancy, rooming-in after delivery with responsibility for newborn care, and then returning home after delivery in 48 hours or less to accept full home responsibilities. Therefore, many women do not have the opportunity to rest and adapt in the postpartum phase. The nurse should assess the level of maternal fatigue and initiate appropriate relief measures such as taking on the care of the newborn for a few hours, or scheduling care that allows for periods of rest. Discussion of the home environment and available support persons should be reviewed before discharge.
Fathers
New fathers typically display intense interest in their new child (engrossment) (Figure 9-3). Their behaviors with their infant parallel those of the new mother. A man’s relationship with his own parents, previous experiences with children, and relationship to the mother are important influences on how he will relate to his infant. According to Goodman (2005), new fathers often experience four phases of adjustment to fatherhood characterized by the following:
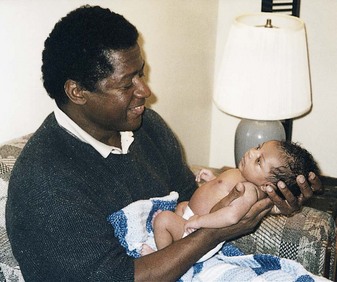
FIGURE 9-3 This father shows intense interest in his new infant (engrossment). The father’s reaction to the newborn parallels the mother’s. Eye-to-eye contact (en face position) helps the bonding process. (Courtesy Pat Spier, RN-C.)
• Having expectations and personal intentions
• Confronting reality and overcoming frustrations
Adjustment to fatherhood is facilitated by involvement in the infant’s care. Fathers should be included when the nurse is giving instructions about infant care and handling. The nurse must be tactful and supportive of a new father who is trying to assume his new role.
Siblings
The influence of a new child’s birth on siblings depends on their age and developmental level. Toddlers may respond with regression and anger when the mother’s attention turns to the infant. Preschool children typically look at and discuss the newborn but may hesitate to actively touch or hold the infant. Older children often enjoy helping with care of the infant and are very curious about the newcomer.
Grandparents
The grandparents’ involvement with a new child is often dictated by how near they live to the younger family. Grandparents who live a long distance from them cannot have the close, regular contact that they may desire. Grandparents also differ in what they expect their role to be, and culture sometimes determines their expected role. Some feel that their child-rearing days are over and want minimal day-to-day involvement in raising the children. Others expect regular involvement in the grandchild’s life, second only to the parents (Figure 9-4). If parents and grandparents agree on the grandparents’ role, little conflict is likely.

Grieving Parents
The postpartum period is usually a joyful time, but nurses occasionally care for grieving parents. With most of these parents, the nurse should simply listen to them and support them. Therapeutic communication techniques such as open-ended questions or reflection of feelings help the parents express their grief—an early step in resolving it.
It seems strange to talk of grief when a healthy infant is born, but even a healthy child may be much different in size, sex, or appearance from what parents expected. Most parents eventually come to accept their unique infant and his or her characteristics. Their feelings about their child are not right or wrong—feelings simply exist. The nurse should accept and encourage their expressions of grief to allow them to move forward and accept the infant they have.
A woman who has experienced the loss of a newborn may experience regret, remorse, and sorrow. This can be one of the most difficult kinds of grief. The woman may question what she could have done differently to prevent the loss. Anniversaries of these events are painful and feelings often last for many years, if not forever. The birth of a new child may awaken grief that parents thought they had resolved (“We have one child, but we almost had two”).
If the condition of a newborn is poor, the parents may wish to have a baptism performed. The minister or priest is notified. In an emergency, the nurse may perform the baptism by pouring water on the infant’s forehead while saying, “I baptize you in the name of the Father, and of the Son, and of the Holy Spirit.” If there is any doubt as to whether the infant is alive, the baptism is given conditionally: “If you are capable of receiving baptism, I baptize you in the name of the Father, and of the Son, and of the Holy Spirit.”
If the infant dies, is stillborn, or has a birth defect, the parents’ reactions depend on whether the event was expected. If they have known for some time that the fetus is not living, they may have already begun the grief process and will not display all the typical behaviors. If the death was not expected, the nurse is likely to encounter the following reactions typical of any grieving:
• Anger (often directed at the physician or staff; rarely, at the infant)
The nurse may encounter grieving families at any point in their grieving process and in many settings. Grieving is often chronic if the infant has a birth defect because of constant reminders of what might have been.
If a newborn dies or is stillborn, nursing units have a protocol to help parents to accept and resolve the event. The parents should be allowed to progress at their individual pace regarding when or if they want to see and hold the infant. The parents should be prepared for the infant’s appearance. For instance, a stillborn infant may have blue skin, which often is peeling. The nurse should try to keep the infant warm so he or she feels more natural to the parents. If this is not possible, they should be prepared for the coolness of the infant’s skin and the limp body. The infant should be wrapped in a blanket and the parents allowed to unwrap the infant when and if they want to do so. If an anomaly is present, the infant should be wrapped so the most normal part is showing.
The nurse should listen to the parent’s responses to determine the level of support needed; answer questions; and understand the grief behaviors individual to the family or culture. Providing privacy and planning for an interdisciplinary grief conference before discharge is important in the overall plan of care. Parents should be provided with private time with the infant if possible and given mementos to take home. The support system of the parents (and grandparents) should be examined, and some information concerning the expected grief process, its influence on behavior and the ability to perform activities of daily living, coping mechanisms, and resources for follow-up care should be discussed.
Most nursing units make a memory packet containing items such as a lock of hair, footprints on a hospital birth certificate, the identification band, a photograph, and clothing or blankets. Some type of code, such as a flower or ribbon on the mother’s door, alerts personnel from other departments that a grieving family is inside. This reduces the chance of well-intentioned but painful remarks or questions being made such as, “What did you have, a boy or girl?”
Parenthood
Whether the parents have one or several children, becoming a parent requires learning new roles and making adjustments. Parents having their first child find themselves in a triangular relationship. Many parents say that parenthood, not marriage, made the greatest change in their lives. Adjustments are even greater for women who have professions or who are in the work force because the changes are more extensive.
The demands of parenthood affect communication between the partners, and there is little doubt that children detract from the relationship at times. It is not unusual for one member to feel left out. The division of responsibility can be a source of conflict, particularly when both parents work. Parents often feel inept, which may cause lower self-esteem, depression, and anger. These feelings can be overwhelming.
Fatigue triggers irritability. Even in the ideal situation, waking up two or three times every night is wearing on anyone. For the new mother, physiological changes continue to play a part in her emotional lability (instability). Both parents are concerned with increased economic responsibilities. Loss of freedom and a decrease in socialization may give the couple a sense of loneliness.
Ideally, preparing parents for the lifestyle changes that occur with a new child begins before conception. Parenting courses, group discussions, and support from relatives or friends can be explored. Social service agencies, public health nurses, and other professional resources should be suggested as appropriate. Encouraging parents to share their concerns and worries with one another and to keep communication lines open is foremost. Reestablishing a relationship into which the newborn fits with a minimum of disruption can be accomplished when the parents identify their own needs, set priorities, maintain their sense of humor, and relax their standards.
These tools can make the transition to parenthood a rewarding yet sometimes difficult experience—one in which the stable family can grow and become stronger. Parents who find themselves at an impasse should seek early intervention with a professional counselor.
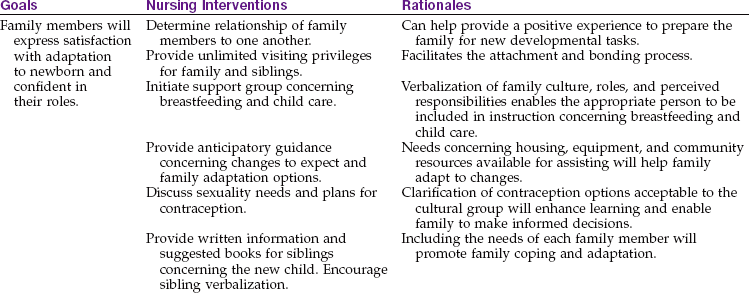
The Family Care Plan
The family care plan is similar to the traditional nursing care plan except that the “patient” is the entire family rather than the woman in the hospital. It is most appropriate to use a family care plan in obstetrics when dealing with the birth of a child, who will have a profound impact on the family processes. Studying the family as the patient can offer insight to community-based care and help the nurse integrate knowledge of family structure, culture, and composition into a plan of care that will meet some of the goals of Healthy People 2020, (U.S. Department of Health and Human Services, 2010). The data required in a family care plan are listed in Nursing Care Plan 9-2. The nurse should use information concerning cultural practices (see Chapter 6) and family processes presented in general psychology to recognize the implications of specific nursing diagnoses to the delivery of nursing care to families. Data collection includes the following:
9-2 Nursing Care Plan
The Family Care Plan
A woman is admitted to the postpartum unit after delivering a healthy baby girl. The husband, two sons (ages 14 and 10), and the woman’s mother are present in the room. The woman tells the nurse she would like to stay in the hospital as long as she can because she has forgotten everything about baby care.
Phase 2: Care of the Newborn
This section presents the Phase 2 care of the newborn after transport to the postpartum unit. Care immediately after birth (Phase 1) was discussed in Chapter 6. Newborn assessments and ongoing care (Phase 3) are presented in Chapter 12. Care of the preterm and the postterm infant is presented in Chapter 13.
Admission to the Postpartum or Nursery Unit
If the infant has adequate cardiorespiratory and heat-regulating functions, he or she usually remains undisturbed while the parents and infant become acquainted. The nurse can usually assess temperature, heart rate, and respirations while the parents continue to hold their infant. Within an hour, the admitting nurse does a complete physical and gestational age assessment of the infant and gives prophylactic medications. Chapter 12 offers the expected characteristics, deviations, and related nursing care of the normal newborn.
The “intensive care concept” has been introduced to the care of all newborns for the immediate neonatal period until they have evidenced a normal transition to extrauterine life (Thureen et al., 2005). The three phases of this transition are as follows:
• Phase 1: 0 to 30 minutes (period of reactivity; see Chapter 6)
• Tachycardia, gradually lowering to normal rate
• Rales present on auscultation
• Infant is alert; frequent Moro (startle reaction) reflex, tremors, crying, increased motor activity (because of sudden release from confines of uterus, response to light)
• Phase 2: 30 minutes to 2 hours (decreased responsiveness)
• Phase 3: 2 to 8 hours (second period of reactivity; see Chapter 12)
Supporting Thermoregulation
The temperature of the term newborn is 36° to 36.5° C (96.8° to 97.7° F; skin) or 36.5° to 37° C (97.7° to 98.6° F; axillary). Maintenance of body temperature is very important to the newborn infant, who has less efficient means of generating heat than an older infant. Hypothermia (low body temperature) can cause other problems, such as the following:
• Hypoglycemia (low blood sugar) since the infant uses glucose to generate heat
• Respiratory distress, because the higher metabolic rate consumes more oxygen, sometimes beyond the infant’s ability to supply it
Hypoglycemia can be both the cause and the result of hypothermia; therefore the nurse must evaluate both factors. Respiratory distress can also require more glucose for the increased work of breathing, causing hypoglycemia.
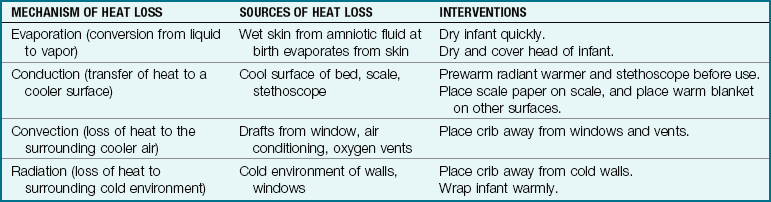
Heat is lost by any of the following four means:
• Evaporation of liquids from the skin
• Conduction caused by direct skin contact with a cold surface
• Convection of heat away from the body by drafts
• Radiation caused by being near a cold surface, although not in direct contact with it
Conduction, convection, and radiation can also be used to add heat to the body. Newborns lose heat quickly after birth because amniotic fluid evaporates from their body, drafts move heat away, and they may contact cold surfaces (Table 9-2).
The infant remains in a radiant warmer and is monitored until the temperature is stabilized and he or she can be cared for in an open crib, clothed, and wrapped in a blanket. The first bath is delayed until the body temperature is stabilized at 36.5° to 37° C (97.7° to 98.6° F). The temperature should be recorded 30 minutes after the bath and 1 hour after transfer to an open crib. Sponge baths are given to newborns in most hospitals, although research has shown that tub baths can safely be given (Association of Women’s Health, Obstetric, and Neonatal Nurses [AWHONN], 2007).
Observing Bowel and Urinary Function
Newborns may not urinate for as long as 24 hours, and occasionally an infant may not void for 48 hours. If an infant urinates in the birthing or operating room, the staff nurse should be informed and the voiding documented on the delivery record. If a long period elapses before the second voiding, it will have been established that the urinary tract is open. Seventy percent of term newborns pass meconium in the first 12 hours. Meconium should be passed before discharge for assurance of a patent gastrointestinal tract.
Providing for Security
The possibility of abduction must be addressed in any facility that cares for infants and children. In the maternal-newborn setting, security begins with identification bands that the nurse matches every time the infant is reunited with the parent (see Figure 9-5).
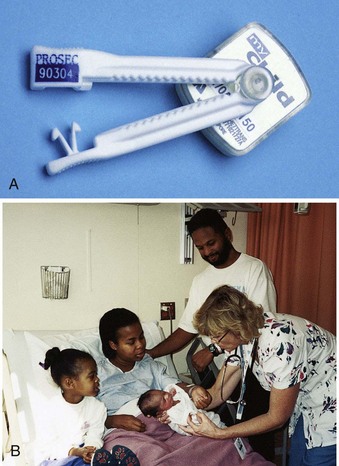
FIGURE 9-5 Identification. A, This umbilical clamp can be used as identification (with an identical numbered wristband for the mother) and also as protection from abduction, because it has a lightweight transponder attached to the clamp. When the transponder passes out of the unit, an alarm sounds unless neutralized by a coded signal inputted by the hospital staff. The umbilical clamp is removed before discharge. B, The nurse compares the identification bracelet of the newborn with the bracelet on the mother’s wrist as the father and sibling look on. (B courtesy Pat Spier, RN-C.)
Identifying the Infant: Wristbands with preprinted numbers are placed on the mother, the infant, and often the father or another support person in the birthing room as the primary means of identifying the infant. The nurse should check to be sure that all numbers in the set are identical (Figure 9-5). Other identifying information such as mother’s name, birth attendant’s name, date and time of birth, sex of the infant, and usually the mother’s hospital identification number should be completed. The bands are applied relatively snugly on the infant and have only a finger’s width of slack because infants lose weight after birth.
Each time the infant returns to the mother after a separation, the nurse must check the preprinted band numbers to see that they match. The nurse should either look at the numbers to see that they are identical or have the mother read her own band number while the nurse reads the infant’s band. Some identification bands or umbilical clamps have an alarm that alerts the staff if the infant is removed from the hospital unit. These alarm chips are removed at the time of discharge to the home.
Recognition of Employees: Parents should be able to recognize employees who are authorized to take the infant from the mother’s room. Employees wear photo identification badges, and maternal-newborn nurses may have an additional badge. They may wear distinctive uniforms. Some units use a code word that changes on a regular basis. The family is taught very early how to recognize an employee who is allowed to take the infant and to refuse to release their infant to any other person. Security measures should be reinforced when providing later care.
Other Security Measures: The mother is taught to keep the infant away from the door to the room. In a semiprivate room the two bassinets are often placed between the mothers. The mother should not leave her infant alone in the room for any reason. If she is alone in her room, she should leave the bathroom door ajar while she toilets or return the infant to the nursery if she showers or naps. These measures also reduce the risk that the infant would aspirate mucus because no one was present for suctioning.
Evaluating Gestational Age
A thorough gestational age assessment is done using a scale such as the new Ballard form (see Chapter 13). However, the birthing room nurse does a quick assessment to evaluate whether the infant seems to be of the appropriate gestational age. The infant who seems to be preterm may be admitted to the nursery more rapidly than one who is of the expected term gestation. Characteristics to assess include the following:
• Skin. Is the skin thin and somewhat transparent (preterm) or peeling (postterm, or possible intrauterine growth restriction [IUGR]).
• Vernix. Is this cheesy substance covering most of the skin surface (preterm), is it present only in creases (term), or is it absent (postterm)? Greenish vernix indicates that meconium was passed before birth, which may indicate that the infant is postterm or had poor placental support.
• Hair. Is the skin heavily covered with fine lanugo hair (preterm), or is hair only in a few places (term)? Dark-skinned infants often have more lanugo than light-skinned ones.
• Ears. When folded toward the lobe, do the ears spring back slowly (preterm) or quickly (term or postterm)? Abundant vernix can stick the ear in place, so that possibility should be considered if the ear does not quickly return to its erect position.
• Breast tissue. Is there no or minimal breast tissue under the nipple (preterm), or is there a palpable mass of tissue 5 mm or more (term)? (A millimeter is about the thickness of a dime.)
• Genitalia. For males, is the scrotum smooth and small (preterm) or pendulous and covered with rugae or ridges (term)? For females, are the labia majora and labia minora of nearly equal size (preterm) or do the labia majora cover the labia minora (term)?
• Sole creases. Are the sole creases on the anterior third of the foot only (preterm), over the anterior two thirds (term), or over the full foot (term or postterm)? Peeling skin may be obvious on the feet in postterm or IUGR infants.
Observing for Injuries or Anomalies
The nurse notes signs of injury or anomalies while performing other assessments and care. The infant’s movements and facial expression during crying are observed for symmetry and equality of movement. The head and face should be assessed for trauma, especially if forceps were used. A small puncture wound is usually apparent on the scalp if an internal spiral electrode was used for fetal monitoring (see Chapter 6). If the infant was born vaginally in a breech presentation, the buttocks may be bruised.
Many anomalies, such as spina bifida (open spine) or a cleft lip, are immediately obvious (see Chapter 14). The fingers and toes should be counted to identify abnormal numbers or webbing. The feet should be observed for straightness or to determine if deviated feet can be returned to the straight position. The length of arms and legs should also be checked for equality. Urination or meconium passage, which confirms patency, must also be noted.
Obtaining Vital Signs
Vital signs observation begins while parents and infant are bonding. They are measured at 15- to 30-minute intervals at first, then hourly, and every 4 to 8 hours after the infant is stable.
Respiratory Rate: For best accuracy, the respiratory and heart rates are assessed before disturbing the infant. The respirations are counted for 1 full minute. Newborn respirations are difficult to count because they are shallow and irregular. The rate can be auscultated by listening with a stethoscope. Placing a hand lightly over the abdomen or watching the abdomen rise and fall also helps to identify each breath. If the infant is crying, a pacifier or gloved finger to suck may quiet him or her so the respiratory rate can be counted.
Heart Rate: The newborn’s heart rate is assessed apically. A small pediatric head is used on the stethoscope if possible to limit extraneous noise. The nurse should count for 1 minute. The normal rate is 110 to 160 beats/min. A consistently low or high heart rate can indicate a pathological condition.
Nursing Tip
In the past, newborns were placed in a prone position to facilitate the drainage of mucus. Because the prone position has been associated with sudden infant death syndrome (SIDS), it is now recommended that newborns be placed on their side or on their back to sleep. Teach all parents this newer information because they may have been taught to keep a previous infant in a prone position.
Temperature: Some facilities require an initial rectal temperature for newborns, but many have discontinued this practice. To avoid perforating the rectum, the nurse should insert a lubricated thermometer no more than 0.5 inch into the rectum. The thermometer is held securely near the buttocks while it is in place. The nurse must not force the thermometer into the rectum because the infant could have an imperforate anus.
An axillary temperature is most commonly used. The thermometer is placed in the axilla, keeping it parallel to the chest wall. The infant’s arm is folded down firmly against the thermometer for the required time. Tympanic temperatures are less accurate in newborns and are not generally used during the neonatal period.
Blood Pressure: A newborn’s blood pressure is measured with an electronic instrument. When blood pressure is assessed on a newborn, all four extremities or one arm and one leg are assessed to identify substantial pressure differences between the upper and lower extremities, which can be a sign of coarctation of the aorta. The normal range of blood pressure is between 65 and 95 mm Hg systolic over 30 to 60 mm Hg diastolic in term infants.
Obtaining Weight and Other Measurements
Weight: The infant is weighed in the birthing room or when admitted to the nursery. Disposable paper is put on the scale, and the scale is balanced to zero according to its model. The unclothed infant is then placed on the scale. The nurse’s hand should not touch the infant but should be kept just above him or her to prevent falls (see Chapter 12, Figure 12-11). The weight must be converted to grams for gestational age assessment.
Measurements: Three typical measurements are length, head circumference, and chest circumference. A disposable tape measure is used. The tape should not be pulled out from under the infant to avoid giving a paper cut. Measurements must also be noted in centimeters for gestational age assessment.
Length: There are several ways to measure length. Some facilities have a tape measure applied to the clear wall of a bassinet. The nurse places the infant’s head at one end, extends the leg, and notes where the heel ends. Another method is to bring the infant to the bassinet or warmer with the scale paper. The paper is marked at the top of the head, the body and leg are extended, and the paper is marked where the foot is located. Length is measured between the marks. Still another method involves placing the zero end of the tape at the infant’s head, extending the body and leg, and stretching the tape to the heel (see Chapter 15, Skill 15-1).
Head circumference: The fullest part of the infant’s head is measured just above the eyebrows. Molding of the head may affect the accuracy of the initial measurement (see Chapter 12, Figure 12-5, A).
Providing Umbilical Cord Care
The health care provider may leave a long segment of umbilical cord. If so, the nurse applies a plastic clamp near the skin and cuts the cord just above the clamp. The cord is assessed for the number and type of blood vessels soon after it is cut. The normal umbilical cord has three vessels: two arteries and one vein. The woman’s name “AVA,” for “artery-vein-artery,” helps the nurse remember the normal number of vessels. A two-vessel cord is associated with other internal anomalies, often of the genitourinary tract. To distinguish the arteries from the vein, the nurse should look at the freshly cut end of the cord. The arteries project slightly from the surface, and the vein looks like a flattened cylinder that does not project from the cut surface.
Umbilical cord care is aimed at preventing infection. It usually includes an initial application of triple-dye solution or antibiotic ointment. Some facilities apply alcohol applications at each diaper change to promote drying of the cord. However, the value of this practice is controversial. The diaper should be fastened low to allow air circulation to the cord. The cord should become dry and brownish black as it dries. The clamp is removed when the end of the cord is dry and crisp, usually in about 24 hours. The parents are taught to report redness of the area or a moist, foul-smelling umbilical cord. Tub baths are usually delayed until the cord falls off—about 10 to 14 days after birth (Skill 9-6).
Skill 9-6 Providing Umbilical Cord Care
1. Identify infant (see Figure 9-5, B).
2. Check umbilical clamp placement for tight closure. There should be no bleeding from the cord.
3. Keep cord dry and exposed to the air.
4. Assess the cord for presence of vessels.
5. Using an alcohol wipe, start from the base of the cord and gently wipe upward and outward.*
6. Lift the cord away from the infant’s abdomen to facilitate cleansing of all areas.
7. Observe cord and abdominal area for redness, discharge, or foul odor.
8. Diaper infant, and be sure the upper end of diaper is folded down below the cord so it does not rub against the cord.
9. Document cord care and observations, solutions used to cleanse the area, condition of the cord, teaching of the parents, and their response.

*Note: Some hospitals use triple dye, alcohol, or other solutions per facility policy. Cord care is completed with every diaper change per facility protocol.
Bleeding from the cord during the first few hours usually indicates that the cord clamp has become loose. Because of the newborn’s small blood volume, even a small amount of bleeding can be a significant percentage of the blood volume. The clamp should be checked for closure and another applied if needed.
Hypoglycemia
The brain is totally dependent on a steady supply of glucose for its metabolism. Until infants begin regular feedings, they must use the glucose stored in their bodies. A blood glucose level below 40 mg/dL in the term infant indicates hypoglycemia. If the screening test indicates hypoglycemia, a venous blood sample is drawn for a more accurate evaluation. The infant is fed formula or is breastfed as soon as the sample is obtained to prevent a further drop in blood glucose.
Some infants have an increased risk for low blood glucose after birth. Infants at higher risk include the following:
• Preterm and postterm infants
• Infants of diabetic mothers, if maternal glucose is poorly controlled
• Large-for-gestational-age (LGA) infants
• Small-for-gestational-age (SGA) infants
• Infants who are cold-stressed
• Infants whose mothers took ritodrine or terbutaline to stop preterm labor
These infants undergo a blood glucose evaluation within 1 hour after birth and at intervals until their glucose level is stable. They are usually nursed or given formula soon after birth to prevent a fall in their blood glucose level.
Although some infants have a higher risk to develop hypoglycemia, any infant can have a fall in blood glucose levels. Signs of hypoglycemia in the newborn include the following:
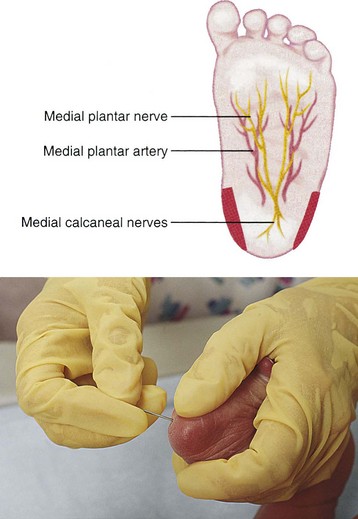
A heel stick is performed when obtaining capillary blood for the glucose screening test. The heel stick should avoid the center of the heel where bone, nerves, and blood vessels are near the surface (Figure 9-6).
Screening Tests
Several tests are done to screen for abnormalities that are known to cause physical or mental disability. The mandatory tests vary according to the state. Most of the disorders are associated with therapy that can prevent many, if not all, of the disabilities that would result if the disorder was left untreated. A test for phenylketonuria (PKU) is mandatory in all states. If the infant has this disorder, a special formula begun in the first 2 months of life can reduce disability and prevent severe mental retardation in most cases. The PKU test is done on the day of discharge for better accuracy and is repeated during early clinic visits. Other tests may include those for hypothyroidism, galactosemia, sickle cell disease, thalassemia, maple syrup urine disease, and homocystinuria. The Centers for Disease Control and Prevention (CDC) highly recommends routine screening for all newborns for cystic fibrosis (CF) by measuring immunoreactive trypsinogen levels, which are elevated in infants with CF.
Skin Care
Initial skin care after the infant’s condition is stable involves washing off the blood and amniotic fluid that may be present on the infant’s skin. Vigorous removal of all remnants of vernix is not advised, because vernix has a protective function on the skin. There should be little vernix present on the skin of the term infant. Until the infant’s first sponge bath and shampoo, the nurse must wear gloves while handling the infant. Care of the skin of the newborn is discussed in Chapter 12.
Promoting Bonding and Attachment
Bonding and attachment are terms often used interchangeably, although they differ slightly. Bonding refers to a strong emotional tie that forms soon after birth between parents and the newborn. Attachment is an affectionate tie that occurs over time as infant and caregivers interact. It is important for nurses to promote these processes to help parents claim the infant as their own. Bonding actually begins during pregnancy as the fetus moves and shows individual characteristics on sonogram.
Both partners should view, hold, and—most important—touch the infant as soon as possible after birth. They must do this to reconcile the fantasy child of pregnancy with the real child they now have. Many parents are not surprised to know the sex of their infant at birth if the sonogram revealed it earlier. However, some do not want to know the infant’s sex before birth, and some are surprised when the predicted sex differs from the actual one. Most parents count all fingers and toes.
To prevent infant hypothermia, the unclothed infant is kept near the parent’s skin. Parents soon identify individual characteristics, such as a nose that looks like Grandpa’s, long fingers like the father’s, or a cry just like an older sibling. All of these parental behaviors help to identify the infant as a separate individual.
For some, parental feelings do not come naturally. Difficulty in bonding or rejection or indifference in one or both parents should be recorded, and a referral to social services should be considered. Mothers who have little social support may have difficulty forming attachments with their newborns.
Nursing Care to Promote Bonding and Attachment: The nurse observes parenting behaviors, such as amount of affection and interest shown to the infant. The amount of physical contact, stimulation, eye-to-eye contact (en face position; see Figure 9-3), and time spent interacting with the infant are significant. Adults tend to talk with infants in high-pitched voices. The extent to which the parents encourage involvement of siblings and grandparents with the newborn should be noted. This information provides a basis for nursing interventions that may encourage bonding and foster positive family relationships (Figure 9-7).
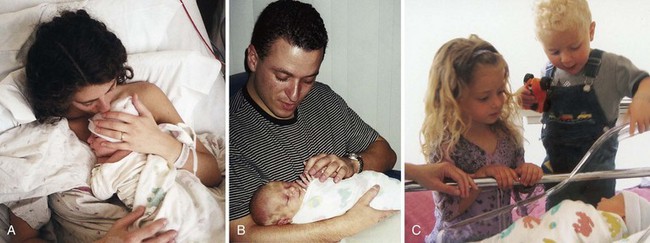
FIGURE 9-7 A, Mother-infant bonding is obvious in this picture of a mother and her newborn infant. B, An uncle bonds with the newborn as he examines features and fingers. C, Siblings get their first introduction to their newborn brother.
Parents must learn what their infant’s communication cues mean. Soon after birth, most parents begin to recognize when an infant is signaling discomfort from hunger as opposed to discomfort from other causes, such as a wet diaper or boredom. In addition, the parents should quickly be able to distinguish their infant’s cry from the cries of other infants. Although this process is just beginning when the mother and infant leave the birth facility, the nurse should note its early signs.
The nurse should observe for parent-infant interactions that dictate a need for additional interventions. Some of these include indifference to the infant’s signals of hunger or discomfort, failure to identify their infant’s communication, avoidance of eye contact with the infant, or discussing the infant in negative terms. However, the family’s culture should also be considered.
Nursing interventions to facilitate parent-infant attachment vary. Calling the infant by name, holding the infant en face, and talking in gentle, high-pitched tones help the nurse to model appropriate behavior for the parent. Role modeling is especially important to adolescent mothers who may feel self-conscious when interacting with their child. Expected infant behaviors should be discussed and unique characteristics pointed out to enhance the bonding process. This is especially important if the parents’ “fantasy” child differs from the “real” child in sex, physical attributes, or health.
Providing and Teaching Routine Care
A newborn infant stays in the mother’s room most of the time unless either mother or infant has a problem that necessitates separation. Routine assessments and care provide an opportunity for the nurse to teach the parents normal newborn characteristics, signs of problems that should be reported, and how to provide care for the infant. Involving the parents in care of their infant helps them to learn most successfully. First-time parents may be sensitive to critical remarks, and therefore the nurse should praise their efforts while tactfully giving suggestions for needed improvement.
Feeding and elimination patterns are assessed by discussing them with the mother as well as observing at diaper changes. The mother should be asked how many wet and soiled diapers the infant has had since the last assessment. Voidings are usually totaled for the shift. Stools are also tallied and are described. Meconium stools are expected during the birth facility stay, although they may change to transitional stools before discharge.
If the infant is breastfed, the nurse should discuss with the mother how well the infant is nursing, the frequency and duration of nursing sessions, and any difficulty she is having. Her breasts are checked for engorgement, and her nipples are checked for flatness, inversion, trauma, or tenderness; these problems can impede successful breastfeeding. If the infant is fed formula, the mother should be asked how many ounces the infant has taken since the previous assessment. This is also a good time to remind the mother that bacteria multiply rapidly in formula, so she should discard any leftovers.
The infant’s skin should be observed for jaundice at each assessment. Infants have a large number of erythrocytes because they live in a low-oxygen environment in utero. Excess erythrocytes are broken down after birth, which releases bilirubin into the bloodstream. High levels of bilirubin cause yellow skin color, starting at the head and progressing downward on the body. Extremely high levels of bilirubin can cause kernicterus (see Chapter 14).
The infant needs only a shirt and diaper for clothing. A light receiving blanket is used to swaddle the infant and another receiving blanket is placed over the child. A cap is used because the infant’s head is the largest body surface area and can be a source of significant heat loss.
Teaching is an important part of mother-infant care. Parent teaching of infant care includes the following:
• Maintenance of an open airway by positioning and use of the bulb syringe
• Temperature maintenance and assessment after discharge
The first feeding should be observed carefully since anomalies that cause choking could be present.
Breastfeeding
Nutrition is especially important in the first few months of life because the brain grows rapidly. Energy use is high because of the newborn’s rapid growth. More in-depth discussions of the nutritional needs of the infant are found in Chapters 15 and 16. The mother may choose to nurse her infant or bottle feed. The nurse should support the mother in either decision.
Advantages and Disadvantages
Breastfeeding has many advantages for the newborn:
• Breast milk contains the full range of nutrients that the infant needs and in the right proportions. No commercial formula has the exact nutritional composition of breast milk.
• Breast milk is easily digested by the infant’s maturing digestive system.
• Breast milk does not cause infant allergies.
• Breastfeeding provides natural immunity because the mother transfers antibodies through the milk. Colostrum is particularly high in antibodies.
• Breast milk promotes elimination of meconium. Breastfed infants are rarely constipated.
• Suckling at the breast promotes mouth development.
• Breastfeeding is convenient and economical.
• Breastfeeding eliminates the risks of a contaminated water supply or improper dilution.
• Infant suckling promotes a return of the uterus to its prepregnant state.
• Breastfeeding may play a significant role in improving brain development of the infant.
• Breast milk production uses maternal fat stores, which facilitates maternal weight loss.
• Breastfeeding enhances a close mother-child relationship.
• Breastfeeding may decrease the occurrence of childhood respiratory disorders.
There are also some contraindications to breastfeeding (American Academy of Pediatrics, 2005):
• There is a potential for most maternal medications to enter breast milk. Use of antimetabolites, antineoplastic drugs, or chloramphenicol is an absolute contraindication to breastfeeding.
• True galactosemia is a contraindication to breastfeeding.
• Women who have untreated active tuberculosis, infection with human immunodeficiency virus (HIV), or active herpes zoster infection of the breast should not breastfeed. Cancer may become worse with the hormonal changes of lactation.
Physiology of Lactation
Infectious Diseases and Breastfeeding
The only infections that are absolute contraindications to breastfeeding are HIV and the human T cell lymphotrophic viruses (HTLV 1 and 2), all of which can be transmitted to the infant via breast milk. Maternal hepatitis A infection is not a contraindication to breastfeeding because the infant can receive immunoglobulin and hepatitis A vaccine therapy. Infants of hepatitis B virus–positive (HBV) mothers should receive HBV vaccine therapy before discharge and can breastfeed. In mothers who are infected with the hepatitis C virus, breastfeeding is contraindicated in the presence of liver failure. In mothers infected with the herpes simplex virus or the varicella zoster virus, breastfeeding is contraindicated when lesions on the breast are present.
Mothers who have active pulmonary tuberculosis (TB) must be isolated from their newborn infants, but infants can be fed breast milk that is pumped because the breast milk does not contain the tubercle bacilli. Certain drugs decrease the breast milk volume, such as levodopa, barbiturates, antihistamines, pyridoxine, estrogens, androgens, and bromocriptine.
Hormonal Stimulation
To better support the nursing mother, the nurse must understand how breast milk production occurs and how the milk changes over time. The following two hormones have a major role in the production and expulsion of breast milk:
• Prolactin from the anterior pituitary gland causes the production of breast milk.
• Oxytocin from the posterior pituitary gland causes the milk to be delivered from the alveoli (milk-producing sacs) through the duct system to the nipple (milk ejection, or let-down reflex). The mother usually feels a tingling in her breasts and sometimes abdominal cramping as her uterus contracts (Figure 9-8).
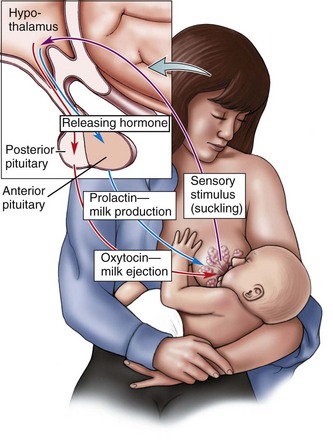
FIGURE 9-8 Lactation reflex arc. The infant suckling on the breast stimulates nerve fibers in the areola of the nipple that travel to the hypothalamus. The hypothalamus stimulates the anterior pituitary to secrete prolactin; this stimulates milk production and stimulates the posterior pituitary to release oxytocin, which causes a “let-down” reflex, contracting the lobules in the breast and squeezing milk out into the nipple and to the infant.
During pregnancy the glandular tissue of the breasts grows under the influence of several hormones. The woman also secretes high levels of prolactin, the hormone that causes milk production. However, other hormones from the placenta inhibit the breasts’ response to prolactin. The influence of prolactin is unopposed after birth and the expulsion of the placenta, and milk production begins. If milk is not removed from the breast, prolactin secretion abates and the breasts return to their prepregnant state.
Infant suckling at the breast stimulates the release of oxytocin so that milk is delivered to the nipple, where it is ingested by the newborn. Prolactin secretion increases as milk is removed from the breasts, thus stimulating further milk production. Therefore feedings that are infrequent or too short can reduce the amount of milk produced. The opposite is also true, which explains why a mother can produce enough milk for twins.
Very little milk is stored between feedings. Most is manufactured as the infant nurses. The composition of milk changes slightly from the beginning of a feeding until the end of that feeding, as follows:
Phases of Milk Production
Milk production changes after birth in the following three phases:
Late in pregnancy and for the first few days after birth, colostrum is secreted by the breasts. This yellowish fluid is rich in protective antibodies. It provides protein, vitamins A and E, and essential minerals, but it is lower in calories than milk. It has a laxative effect, which aids in eliminating meconium.
Approximately 7 to 10 days after birth, the transitional milk emerges as the breasts gradually shift from production of colostrum to production of mature milk. Transitional milk has fewer immunoglobulins and proteins but has increased lactose (milk sugar), fat, and calorie content.
Mature milk is secreted by 14 days after birth. Mature human breast milk has a bluish color, which leads women to think that it is not “rich” enough to nourish the infant. The nurse should explain that the apparent “thinness” of the milk is normal and that the milk has 20 kcal/oz and all the nutrients the infant needs.
Assisting the Mother to Breastfeed
Ideally the infant is nursed soon after birth. Although the infant may obtain little colostrum, this first nursing session has the following other advantages:
• Promotes mother-infant bonding
• Maintains infant temperature
• Infant suckling stimulates oxytocin release to contract the mother’s uterus and control bleeding
The newborn should be put to breast within the first hours when the alert state allows for suckling and bonding. Breastfeeding should not be delayed beyond 6 hours after delivery. If the mother is too tired or uncomfortable to nurse at this time, or if the infant seems disinterested, she should be reassured that she can still breastfeed successfully. Table 9-3 reviews techniques the nurse can teach a new mother who wants to breastfeed.
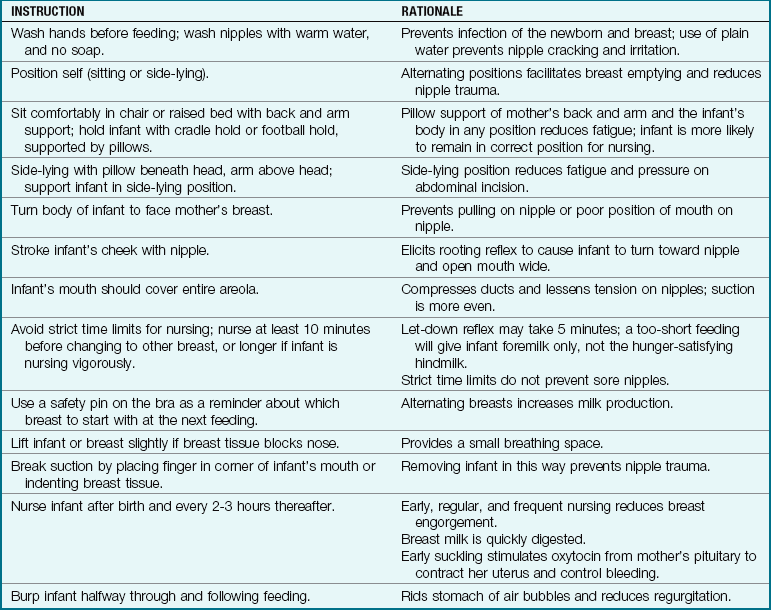
The focus of the nurse in the early hours of breastfeeding should be to help the mother position the infant correctly and help the infant have an open, gaping mouth in preparation for suckling. Frequent reassurance and praise of the mother’s efforts are essential.
 Communication
Communication
Cross-Cultural Communication
To verify that a woman (or family) understands what the nurse has told her, have the woman repeat the teaching in her own words. An affirmative nod may indicate courtesy, not understanding, when the primary languages and the cultures of the nurse and family are different.
 Cultural Considerations
Cultural Considerations
Galactagogues
Mothers from many cultures use galactagogues (breast-milk stimulators), and nurses should be aware of these practices. Beer, brewer’s yeast, rice, gruel, fenugreek tea, and sesame tea are commonly used postpartum. Garlic eaten by the mother to prevent newborn illness will flavor her breast milk but will not harm the newborn. Cultural practices should be respected.
Positions for Breastfeeding
Any of several positions may be used for breastfeeding. The mother may sit in bed or in a chair and hold the infant in a cradle hold, with the head in her antecubital area (Figure 9-9, A). To prevent arm fatigue, the infant’s body should be supported with pillows or folded blankets. She may prefer the football hold (see Figure 9-9, B), supporting the infant’s head with her hand while the infant’s body rests on pillows alongside her hip. The football hold is good for mothers who have a cesarean incision. The mother may prefer to lie on her side with the infant’s body parallel to hers (see Figure 9-9, C). Pillows or folded blankets can be used to support the infant in the proper position. Mothers often use the side-lying position when feeding the infant during the night. It is also good for mothers who have had a cesarean birth.
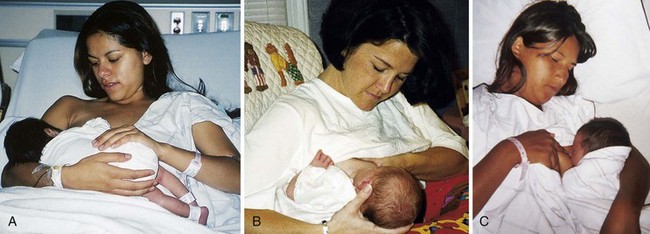
FIGURE 9-9 Positions for nursing. A, Cradle hold. B, Football hold. The mother supports the infant’s head with her hand while the infant’s body rests on pillows alongside her hip. The mother has control of the infant’s head and can see the position of the infant’s mouth on the breast. The football hold avoids pressure on a cesarean incision and is comfortable for mothers with large breasts. C, Side-lying position. (Courtesy Pat Spier, RN-C.)
Regardless of the position selected for breastfeeding, the infant’s body should be in “chest-to-chest” position with the mother, with the head and neck in alignment. If the infant’s chest faces the ceiling of the room, then the infant will have to turn his or her head away from midline to grasp the breast nipple. This position makes swallowing difficult for the infant. The infant should be at the level of the breast nipple to allow easy flow of milk. Holding the infant above the level of the nipple works against gravity flow; holding the infant below the level of the nipple exerts a pressure on the nipple that can cause soreness and bruising. The nipple should be centered to the nose of the infant with the nipple aimed to the roof of the infant’s mouth so that the lower jaw latches on first. When the infant’s mouth is wide open before latch-on, a more effective latch-on will occur as the mother moves her arm to bring the infant closer to the breast (Box 9-2).
Breastfeeding Techniques
The mother is taught to wash her hands before each breastfeeding session. She should wash her breasts gently with plain water. Manually expressing a few drops of colostrum will make the nipple more erect in preparation for breastfeeding. Breastfeeding should begin with the opposite breast from the one that began the last feeding session.
Position of the Mother’s Hands: The mother should hold her breast in a C position, with the thumb above the nipple and the fingers below it. The thumb and fingers should be well back from the nipple, and the nipple should not tip upward. She can also use the scissors hold to grasp the breast between her index and middle fingers, but her fingers are more likely to slip downward over the nipple. Most infants do not need to have the breast indented for breathing room. The mother can lift the infant’s hips higher if her breasts are very large or if the infant buries the nose in her breast.
Latch-on: The mother is taught to allow the infant to become alert and hungry but not frantic. To elicit latch-on, the mother should hold her breast so the nipple brushes against the infant’s lower lip. A hungry infant usually opens the mouth wide with this stimulation. As soon as the infant’s mouth opens wide, the mother should bring the infant close to her breast so that her areola is well into the mouth. The infant’s lips should flare outward. The infant’s tongue position can be checked to be sure it is under the nipple by gently pulling down on the lower lip (Figure 9-10).
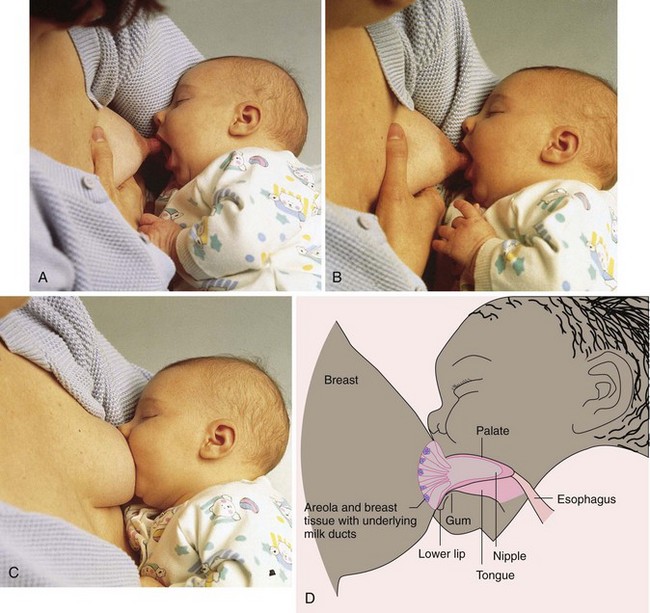
Suckling Patterns: Suckling is the term that specifically relates to giving or taking nourishment at the breast. Infants have different suckling patterns when they breastfeed. Some suck several times before swallowing, and others swallow with each suck. After 4 days the infant generally swallows with every suck at the beginning of breastfeeding, taking in approximately 0.14 mL, and has about two sucks per swallow near the end of the feeding, taking in 0.01 mL with each suck. A soft “ka” or “ah” sound indicates that the infant is swallowing colostrum or milk (nutritive sucking). Noisy sucking or smacking sounds or dimpling of the cheeks usually indicates improper mouth position. “Fluttering” sucking motions indicate nonnutritive suckling.
Removing the Infant from the Breast: When the infant must be repositioned or changed to the other breast, the mother should break the suction and remove the infant quickly. She can break the suction by inserting a finger in the corner of the infant’s mouth or indenting her breast near the mouth (Figure 9-11). Pulling the infant away from the breast can cause sore nipples.

Evaluating Intake of the Infant
Often the mother must be reassured that she is providing adequate milk for her infant because she cannot see the milk consumed as she can with bottle feeding. Signs that breastfeeding is successful include the following:
• Breast feels firm before feedings and softer after.
• “Let-down” reflex occurs—a tingling sensation with milk dripping from breasts when a feeding is due.
• Infant nurses at the breast for 10 to 15 minutes per breast 8 to 10 times a day.
• An audible swallow is heard as infant sucks.
• Infant demands feeding and appears relaxed after feeding.
Preventing Problems
Teaching can help new mothers prevent many problems with breastfeeding. If the mother can avoid problems, she is less likely to become discouraged and stop nursing early. Lactation consultants are available in many birth settings to help with breastfeeding problems. Local chapters of La Leche League may be available to the mother for ongoing support after discharge. Most birth centers have “warm lines” to help with breastfeeding or other problems that occur in mothers and infants after birth.
Frequency and Duration of Feedings: Breastfed infants usually nurse every 2 to 3 hours during the early weeks because their stomach capacity is small and because breast milk is easily digested. Some infants cluster several feedings at frequent intervals and then wait a longer time before nursing again. It is best to maintain flexibility during the early weeks. However, if the infant has not nursed for 3 hours, the mother should gently waken the infant and try to breastfeed.
If feedings are too short, the infant may get little milk or only the foremilk. It may take as long as 5 minutes for the woman’s let-down reflex to occur. The infant will soon be hungry again if he or she does not receive the richer hindmilk. This can frustrate the mother because her infant wants to “eat all the time.” Engorgement will occur if milk is not removed from the breasts, and milk production will decrease or stop. Mothers should be taught how to recognize signs of early hunger in their infants. Crying is usually a late sign of hunger (Box 9-3).
The infant should nurse at least 10 minutes on the first breast, or longer if still nursing vigorously. The mother should then remove the infant from the first breast and have the infant nurse at the second breast until he or she is satisfied. The total duration of early feedings should be at least 15 minutes per breast. The mother should not switch back and forth between breasts several times during a feeding session.
Infants who breastfeed usually do not swallow much air. To burp the infant, the mother can hold the infant in a sitting position in her lap and pat or rub the back to assist (Figure 9-12). Alternately, the infant can be placed against the mother’s shoulder for burping. A soft cloth protects the adult’s clothing from any “spit-ups.”

FIGURE 9-12 The mother can burp the infant by holding the infant in a sitting position on her lap, supporting the chin and chest, and gently patting or rubbing the back. In this position the mother can see the infant’s face in case of spit-ups.
The mother should begin the next nursing session using the breast that was not used first in the previous session. A safety pin attached to her bra helps her to remember which breast to use the next time.
The Sleepy Infant: Some newborns are sleepy and need to be awakened for feedings until a routine of feeding on demand is established. To bring the infant to an alert state in preparation for feeding, the infant should be unwrapped, the diaper can be changed, the mother should hold the infant upright and talk softly to him or her, or she may provide a gentle massage of the back, palms, or soles of the feet. When the infant is awake, feeding will be more successful.
The Fussy Infant: Some infants awaken from sleep crying lustily, eliminating the opportunity to observe for early cues of hunger (see Box 9-3). These infants must be calmed before successful feeding can be attempted. The infant is wrapped snugly (swaddled) and held close. The mother should talk calmly to the infant. When the infant calms, feeding can begin. Stiffening and crying after feeding starts can indicate a sore mouth from thrush, gas, cramps, or some illness that requires a health care provider’s intervention. Collaboration with a lactation consultant is advisable.
Flat or Inverted Nipples: To help the nipples become erect for feedings, the mother can gently roll them between her thumb and forefinger.
Supplemental Feedings and Nipple Confusion: Supplemental feedings of formula or water should not be offered to the healthy newborn who is breastfeeding. Successful breastfeeding is based on supply and demand. The hungry infant will nurse and stimulate maternal milk production to meet physiological needs. A form of “imprinting” may occur if a newborn is given a bottle of formula and finds it easy to obtain fluid from the nipple with minimal effort. When the infant is then placed at the breast, considerably more effort is needed to obtain the breast milk. As a result, the hungry infant may become fretful and irritable, which causes the mother to lose confidence and decide the infant prefers the formula and artificial nipple. This is often called “nipple confusion.” When lactation is firmly established, usually after the neonatal period, the use of a pacifier to meet nonnutritional sucking needs will not cause nipple confusion.
Breast Engorgement: Early, regular, and frequent nursing helps to prevent breast engorgement. If engorgement does occur and the breast and areola are very tense and distended, the mother can pump her breasts to get the milk flow started and soften the areola. She may use a breast pump or manual expression of milk. Cold applications between feedings and heat just before feedings may help to reduce discomfort and engorgement.
Manual massage of all segments of the breasts helps to soften them and express milk downward in the duct system. The mother cups her hands around the breast near the chest wall and firmly slides her fingers forward toward the nipple. She rotates her hands to massage all areas of the breast.
Nipple Trauma: Cracks, blisters, redness, and bleeding may occur. Correct positioning of the infant is the best preventive measure. Feeding formula at this time can worsen the trauma and pain because it is likely to cause engorgement since less milk is removed. Warm water compresses applied to the breasts offer some relief. Rubbing a small amount of breast milk into the nipples may aid healing. Ointments are not effective; if used, they should be removed before nursing.
Special Breastfeeding Situations
The mother’s body adjusts the milk supply to the greater demand of multiple infants. Twins can be fed one at a time or simultaneously. The mother may want to use the crisscross hold when nursing simultaneously. She will need help to position two infants at the breast in a cradle hold in each arm. She positions the first infant in a cradle hold, then her helper positions the second infant at the other breast in the crook of her arm. Their bodies cross over each other. The infants and the mother’s arm are supported with pillows.
Premature Birth
Breastfeeding is especially good for a preterm infant because of its immunological advantages (see Chapter 13 for more information on the preterm infant). If the infant cannot nurse, the mother can pump her breasts and freeze the milk for gavage (tube) feedings. When nursing the preterm or small infant, the mother may prefer the cross–cradle hold. She holds the infant’s head with the hand opposite the breast that she will use to nurse. She uses the same arm to support the infant’s body. The hand on the same side as the nursing breast is used to guide the breast toward the infant’s mouth.
Delayed Feedings
When breastfeeding must be temporarily delayed, the mother should be taught how to pump her milk in order to resume full breastfeeding (Figure 9-13).

FIGURE 9-13 Breast pumps. Breast pumps can be manual (A), electric (B), or battery-operated and pump directly into a bottle or freezer bag. One or both breasts can be pumped, and suction pressure is adjustable. Most hospitals and breastfeeding clinics help new mothers establish breastfeeding and breast pumping schedules to fit their individual needs.
Storing and Freezing Breast Milk
Milk stored at room temperature over 4 hours has an increased potential for bacterial contamination. Various commercial containers are available for the storage of breast milk, each with advantages and disadvantages. The container size should hold about as much milk as the infant will consume at one feeding.
Milk may be safely stored in glass or hard plastic. Leukocytes may stick to the glass but are not destroyed. Several types of plastic bottles are available in stores. Clear hard plastic bottles are made of polycarbonate and, although little research is available, they are considered safe for storing and freezing milk. Dull or cloudy hard plastic bottles are polystyrene or milky white polypropylene. Polystyrene bottles are not designed for frozen milk storage. Polymers become unstable when heating after freezing. When used for freezing, polypropylene bottles alter the lysozyme, lactoferrin, and vitamin C content of breast milk. Polyethylene containers are usually clear plastic bags that may be at risk for puncture and invasion by microorganisms; some brands contain a special nylon between the polyethylene layers to reduce the puncture risk. The loss of lysozyme and fat is significant, and some valuable antibodies that adhere to polyethylene are lost to the infant. Any plastic material used for infants should be labeled as bisphenol A (BPA)–free.
Milk can be thawed in the refrigerator for 24 hours (best to preserve immunoglobulins) or by holding the container under running lukewarm water or placing it in a container of lukewarm water, rotating (not shaking) the bottle often. Microwaving is not advised because it destroys some immune factors and lysozyme contained in the milk and can cause hot spots to develop because of uneven heating.
Milk can be stored in the refrigerator (4° C [39° F]) up to 24 hours without significant changes occurring or in the freezer (−4° C [−20° F]) for up to 3 months. Freezing can destroy some antimicrobial factors in the breast milk.
Maternal Nutrition
To maintain her own nutrient stores while providing for the infant, the mother needs 500 additional calories each day over her nonpregnant diet (see Table 4-4). She should choose foods from each of the following groups in the MyPyramid food guide:
She needs to drink fluids to satisfy her thirst (about 8 to 10 glasses per day), excluding those containing caffeine. Women with lactose intolerance may use substitutes such as tofu, soy milk, and canned salmon with bones as a substitute for milk products. A calcium supplement is probably needed to prevent maternal bone loss. The health care provider usually recommends that the nursing mother continue taking prenatal vitamins during lactation, although routine supplementation has been shown to be unnecessary for the well-nourished mother.
Some foods eaten by the mother may change the taste of the milk or cause the infant to have gas. Foods that often cause problems are chocolate, cabbage, beans, and broccoli. If the mother suspects that a particular food is causing fussiness or gas in the infant, she can eliminate it from her diet for a few days to determine if the infant has fewer problems. These problems do not indicate an allergy to breast milk, only irritation with some food by-product contained in the milk.
Many medications taken by the mother are secreted in breast milk but in varying concentrations depending on the drug. In general, timing the drug dose so that it passes its peak of action before the infant’s nursing sessions can reduce the amount delivered to the infant.
Weaning
Gradual weaning is preferred to abrupt weaning, which can cause engorgement, lead to mastitis, and be upsetting to the infant. There is no one best time to wean. Even a short period of breastfeeding provides the infant with many immunological and digestive advantages. As the infant matures, he or she will gradually become less interested in the breast, especially when solid foods are added to the diet around 6 months.
The nurse can teach mothers the following tips when she wants to wean her infant:
• Eliminate one feeding at a time. Wait several days and eliminate another one. The young infant will need formula from a bottle; the older infant may be weaned from the breast to a cup.
• Omit daytime feedings first, starting with the one in which the infant is least interested.
• Eliminate the infant’s favorite feeding last. This will often be the early morning or bedtime feeding.
• Expect the infant to need “comfort nursing” if he or she is tired, ill, or uncomfortable.
If the mother must wean abruptly for some reason, breast engorgement is likely to occur. A supportive bra, ice packs, analgesics, or cabbage leaves applied to the breasts may relieve discomfort. Breast pumping is not advised because the breast must remain full enough to decrease the milk supply cycle.
Formula Feeding
Women choose to formula feed for many reasons. Some are embarrassed by breastfeeding or may have little social support. Others are uncomfortable when they cannot see the amount of milk the infant takes at each feeding. Women who have many other commitments and cannot maintain the flexibility needed when lactation is established may find that formula feeding is the only realistic choice. A few women must take medications or have other illnesses that make breastfeeding unwise. Regardless of the reason for choosing to formula feed, the nurse should fully support the mother and reassure her that her infant can receive good nutrition and emotional closeness.
Types of Infant Formulas
Before the first formula feeding, most hospitals have the policy of offering water to the newborn to assure patency of the gastrointestinal tract. If the infant sucks, swallows, and retains the water, formula is then offered. If the infant has an anomaly such as esophageal atresia (tracheoesophageal fistula) (see Chapter 28), aspiration can occur. Aspiration of water involves less risk than aspiration of formula.
Most formulas are modifications of cow’s milk. Similac and Enfamil are examples of cow’s milk–based formulas. Infants who do not tolerate cow’s milk formulas or who come from a family with many allergies may be given soy or protein hydrolysate formulas, such as Nutramigen. Soy formulas include ProSobee and Isomil. Other formulas are available to meet special needs, such as those of the preterm infant or the infant with PKU. Common formulas are available in three forms:
Specific types of infant formulas are discussed in Chapter 16.
Preparation
The parent should wash the hands before preparing formula and feeding the infant. Bottles and nipples can be washed in hot, soapy water, using a nipple brush, and rinsed well. Bottles can be washed in a dishwasher, but nipples should be washed by hand to slow their deterioration. Bottles of formula can be prepared one at a time, or a 24-hour supply can be prepared. Formula should be refrigerated promptly and kept refrigerated until ready to use.
Ready-to-feed formulas require no dilution. Diluting them with water reduces the amount of nutrients the infant receives and can be dangerous. Ready-to-feed formula for home use comes in bottles and cans. The mother should wash the can’s lid and open it with a freshly washed can opener. She then pours the approximate amount the infant will take at a feeding into a bottle and caps the bottle.
 Safety Alert!
Safety Alert!
Overdilution or underdilution of concentrated liquid or powdered formulas can result in serious illness.
Concentrated liquid formula also comes in a can. After washing the can and opening it, the mother pours recommended proportions of concentrated liquid formula and tap water into the bottles and caps them. The usual proportions are one part concentrated liquid formula plus one part tap water. Water for formula dilution does not need to be boiled unless its safety is questionable.
Powdered formula is a popular choice for nursing mothers who want to feed their infant an occasional bottle of formula. It is also less expensive than ready-to-feed liquid formulas. The parent measures the amount of tap water into the bottle and adds the number of scoops recommended for that quantity. Sterilization is not required unless the quality of the water is in doubt.
Bottled cow’s milk and evaporated milk are nutritionally inadequate for use as infant formula and stress the kidneys of the newborn and young infant.
Feeding the Infant
Formula is digested more slowly than breast milk, and most formula-fed infants initially feed about every 3 to 4 hours (Skill 9-7). Like the breastfeeding mother, the formula-feeding mother should be encouraged to avoid rigid scheduling.
Skill 9-7 Bottle Feeding the Infant
3. Verify formula prescribed and expiration date on the bottle.
4. Change diaper and provide cord care (see Skill 9-6).
6. Select an appropriate nipple. Cross-cut nipple offers rapid feedings; single-hole nipple offers regular milk flow; preemie nipple offers softer nipple that requires less sucking effort from the infant.
7. Open bottle (you should hear a “pop” to indicate bottle was previously unopened); place selected nipple on the bottle and tighten securely. Use room-temperature formula.
8. Hold infant in “cradle position” with infant’s head slightly elevated above the body (see figure).
9. Touch infant’s lips with nipple and gently insert nipple along infant’s tongue. Hold bottle so nipple is always full of formula.
10. Feed infant slowly. Stop to “burp or bubble” infant after feeding 1 to 1.5 oz (30 to 45 mL) and at end of feeding.
11. If formula runs out of the side of the mouth during infant feeding, the nipple holes may be too large. The nipple should be discarded and replaced with a different one.
12. To burp the infant, sit the infant on your lap with his or her body leaning slightly forward. Support the head and gently pat the middle or upper back (see Figure 9-12).
13. Place the infant in the crib on his or her side or back after feeding.
14. Leftover formula should be discarded because microorganisms from the infant’s mouth grow rapidly in warm formulas.
15. Document the amount taken; type of formula; any regurgitation; sucking strength; and parent teaching that was provided.

Many mothers prefer to warm the formula somewhat, but this is not necessary. Placing the bottle in a container of hot water takes the chill off the milk. Microwave heating of infant formula is not recommended, because heating is uneven and may result in hot spots that can cause mouth burns in the infant.
The nurse should caution parents not to prop the bottle, even when the infant is older. Propping the bottle may cause the infant to aspirate formula and is associated with dental caries (cavities) and ear infections.
Fathers or partners are encouraged to assist with feedings. When teaching new parents about infant care, the father or other support person should be involved to aid his or her involvement and attachment to the infant as well as enhance support for the mother. Tips concerning safe bottle feeding of the infant can be found in Chapter 16.
Discharge Planning
Discharge planning begins on admission or even earlier, when parents attend childbirth classes. Because mothers and infants are discharged quickly after birth, self-care and infant care teaching must often begin before the mother is psychologically ready to learn. Some birth facilities use clinical pathways (also called care maps, care paths, or multidisciplinary action plans [MAPs]) to ensure that important care and teaching are not overlooked (see Chapter 12). These plans guide the nurse to identify areas of special need that necessitate referral as well as a means to keep up with the many facets of routine care needed after birth. The nurse must take every opportunity to teach during the short birth facility stay. Ample written materials for both new mother and infant care should be provided to refresh the memory of parents who may be tired and uncomfortable when teaching occurs.
Postpartum Self-Care
The nurse teaches the new mother how to best care for herself to reduce her risk for complications. The health care provider may prescribe more specific instructions for some patients.
Follow-Up Appointments
Most health care providers want to see postpartum women 2 weeks and 6 weeks after birth. The nurse should emphasize the importance of these follow-up appointments that verify that involution is proceeding normally and identify any complications as soon as possible. Signs of problems the woman should report have been discussed in previous sections and danger signs are discussed later in the chapter.
At the 2-week appointment the healing of the mother’s perineum or cesarean incision is assessed. At the 6-week appointment the mother’s general health and recuperation from birth are assessed. The health care provider does a vaginal examination to check the uterus to ensure that involution is complete. Any incision is assessed for healing. The breasts are carefully examined for any signs of problems. Occasionally a complete blood count is done, and vitamins or iron supplements, or both, are ordered if anemia is present.
The woman has the opportunity to discuss any physical or psychological problems she may be having. The health care provider and the nurse usually inquire about how she is adapting to motherhood. Is she getting enough rest? How is breastfeeding coming along? Does she have help at home? How is the partner adapting to this new role?
Hygiene
A daily shower is refreshing and cleanses the skin of perspiration that may be more profuse in the first days after birth. Perineal care should be continued until the flow of lochia stops. Douches and tampons should not be used for sanitary protection until after the 6-week checkup.
Sexual Intercourse
Coitus should be avoided until the episiotomy is fully healed and the lochia flow has stopped. Having sexual relations earlier can lead to infection, trauma, and/or another pregnancy. A water-soluble lubricant can make intercourse more comfortable for the woman.
Ovulation, and therefore pregnancy, can occur before the 6-week checkup. The health care provider usually discusses contraception with the woman, but the nurse must often clarify or reinforce any explanations. It is important to emphasize that breastfeeding is not a reliable contraceptive.
Diet and Exercise
A well-balanced diet and moderate exercise promote healing and recovery from birth. Because constipation may be a problem, the mother is taught about high-fiber foods (e.g., whole-grain breads, and fruits and vegetables with the skins). Breastfeeding mothers should not try to lose weight while nursing. The formula-feeding mother should delay a strict reducing diet until released by her health care provider to do so. Moderate exercise can aid in the return of the uterus to its prepregnancy state and promote a feeling of well-being. Most health care providers recommend that new mothers continue any prescribed prenatal vitamins until after the 6-week checkup.
Danger Signs
By teaching the mother changes to expect as she returns to the prepregnant state, the nurse gives her a framework to recognize when something is not progressing normally. Hemorrhage, infection, and thrombosis are the most common complications. The mother should report the following:
• Fever higher than 38° C (100.4° F)
• Persistent lochia rubra or lochia that has a foul odor
• Bright red bleeding, particularly if the lochia has changed to serosa or alba
• Prolonged afterpains, pelvic or abdominal pain, or a constant backache
• Signs of a urinary tract infection
• Pain, redness, or tenderness of the calf
• Localized breast tenderness or redness
• Discharge, pain, redness, or separation of any suture line (cesarean, perineal laceration, or episiotomy)
• Prolonged and pervasive feelings of depression or being let down; generally not enjoying life
Newborn Discharge Care
Discharge planning for the infant begins at birth. Because of short stays after birth, the nurse must teach the parents how to care for their newborn at every opportunity. Discharge teaching will then be more of a summary than an attempt to crowd all teaching into a short time.
Most newborns are checked by a health care professional at birth and before discharge. The infant is assessed at this early check for jaundice, feeding adequacy, urine and stool output, and behavior. If the newborn is discharged before 72 hours of age, the American Academy of Pediatrics (AAP) recommends that a follow-up visit be scheduled within 2 days of discharge to assess the infant for jaundice, because the bilirubin level usually peaks between 3 to 5 days of age (Maisels, 2005).
Infants are usually seen again at 6 to 8 weeks after birth to begin well-baby care. When providing discharge teaching, the nurse should emphasize the value of these visits. It should be explained that immunizations can be given to prevent many illnesses. The health care provider assesses the infant for growth and development, nutrition, and any problems the parents or infant are having. Teaching parents about the infant’s upcoming needs (anticipatory guidance) helps them to plan ahead to prevent injuries and promote healthy growth and development.
The nurse should teach parents the importance of using infant car safety seats and their correct use (Figure 9-14). The newborn should be placed in semireclining position in the car seat in the car’s back seat (never in the front), facing the rear until 1 year of age and a weight of 22 lb (10 kg) are attained. The seat’s harness is snugly fastened, and the seat is secured to the automobile seat with the seat belt. Parents should consult their car’s instruction manual for specific instructions on securing safety seats. The U.S. Department of Transportation has a toll-free vehicle safety hotline to help parents solve problems when using car safety seats: 800-424-9393. The AAP guidelines for appropriate care safety seats can be found online at www.aap.org/family/Carseatguide.htm.

FIGURE 9-14 A new mother prepares to leave the birth facility. The infant is placed in a car seat that will be rear-facing and secured by the car’s seat belt for the ride home.
Nursing Tip
If siblings are waiting on return from the hospital, it is helpful if the father arrives carrying the infant. This leaves the mother’s arms free for hugs before turning attention to the new child.
The nurse must emphasize to the parent that even in a low-impact accident, their infant will probably be thrown from their arms—or even the car safety seat if the infant is improperly restrained—and become a “missile” within the car or even ejected from it. Death is a likely result. Air bags can prevent serious injuries to older children and adults in motor vehicle accidents. However, the air bag thrusts an infant toward the rear, causing a whiplike motion that can seriously injure the neck or head.
New parents are often overwhelmed at the volume of information given in such a short time. They should be reassured that the birth facility staff is available 24 hours a day to help them to care for their infant and to refresh their memory if they forget what they have been told (see Discharge Planning and Parent Teaching in Chapter 12).
Get Ready for the NCLEX® Examination!
Key Points
• It is essential to consider all patients individually to better incorporate their culture and special needs into the plan of care.
• From its level at the umbilicus, the uterus should descend about one finger’s width per day after birth. It should no longer be palpable at 10 days postpartum.
• A slow pulse is common in the early postpartum period. A maternal pulse rate that would be high normal at other times may indicate hemorrhage or infection in the postpartum patient.
• A full bladder interferes with uterine contraction, which can lead to hemorrhage.
• Measures to prevent constipation should be emphasized at each assessment: fluid intake, a high-fiber diet, and activity.
• RhoGAM is given within 72 hours to the Rh-negative mother who delivers an Rh-positive infant.
• The postpartum check should include the status of fundus, lochia, breasts, perineum, bowel and bladder elimination, vital signs, Homans sign, pain, and evidence of parent-infant attachment.
• Neonatal screening tests such as the phenylketonuria (PKU) test identify disorders that can be treated to reduce or prevent disability.
• The nurse must always keep the possibility of infant abductions in mind when providing care.
• The facility’s specific protocol for security should be maintained during care. Most persons will not be offended by precautions but will be grateful for the protection.
• Bonding and attachment require contact between parents and infant. The nurse should promote this contact whenever possible.
• More breast milk removed means more milk produced. Early, regular, and frequent nursing promotes milk production and lessens engorgement.
• Duration of nursing on the first breast should be at least 10 minutes to stimulate milk production.
• The nursing mother needs 500 extra calories each day plus enough fluid to relieve thirst (about 8 to 10 glasses).
• Weaning from the breast should be gradual, starting with the feeding the infant is least interested in and ending with the one in which he or she has the most interest.
• Commercially prepared formulas are available in ready-to-feed, concentrated liquid or in powdered form. Dilution, if required, must be followed exactly according to instructions.
• Discharge planning should take place with every instance of mother or newborn nursing care as the nurse teaches the mother normal findings, significance, and what to report. Written materials should be provided to augment all teaching.
Additional Learning Resources
 Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Study Guide for additional learning activities to help you master this chapter content.
Go to your Evolve website (http://evolve.elsevier.com/Leifer) for the following FREE learning resources:
• Answer Guidelines for Critical Thinking Questions
• Answers and Rationales for Review Questions for the NCLEX® Examination
• Glossary with English and Spanish pronunciations
• Interactive Review Questions for the NCLEX® Examination
• Patient Teaching Plans in English and Spanish
 Online Resources
Online Resources• Breastfeeding Support Consultants Center for Lactation Education: www.bsccenter.org
• Car Safety Seats: Information for Families: www.aap.org/family/Carseatguide.htm
• International Lactation Consultant Association: www.ilca.org
• La Leche League International: www.lalecheleague.org
Review Questions for the NCLEX® Examination
1. Which assessment is an expected finding 24 hours after birth?
1. Scant amount of lochia alba on the perineal pad
2. Fundus firm and in the midline of the abdomen
2. Nursing the infant promotes uterine involution because it:
1. uses maternal fat stores accumulated during pregnancy.
2. stimulates additional secretion of colostrum.
3. causes the pituitary to secrete oxytocin to contract the uterus.
3. The best way to maintain the newborn’s temperature immediately after birth is to:
1. dry the infant thoroughly, including the hair.
2. give the infant a bath using warm water.
4. Eight hours postpartum the woman states she prefers the nurse to take care of the infant. The woman talks in detail about her birthing experience on the phone and to anyone who enters her room. She complains of being hungry, thirsty, and sleepy and is unable to focus on the infant care teaching offered to her. The nurse would interpret this behavior as:
1. inability to bond with the infant.
2. development of postpartum psychosis.
5. A new mother asks how often she should nurse her infant. The nurse should tell her to feed the infant: