26 RESIN-BONDED FIXED DENTAL PROSTHESES
Resin-bonded fixed dental prostheses (FDPs) have had variable popularity since the technique for splinting mandibular anterior teeth with a perforated metal casting was described by Rochette in 1973.1 His work suggested an alternative to conventional metal-ceramic fixed FDPs and its substantial removal of tooth structure needed to create strong, anatomically contoured, and esthetic restorations (see Chapter 7). A prosthesis that requires minimal removal of tooth structure is appealing, particularly for abutment teeth that are intact and caries free. The primary goal of the resin-bonded partial FDP is the replacement of missing teeth and maximum conservation of tooth structure.
The advent of electrolytic etching of the metal surface to provide micromechanical retention for metal adhesion to enamel led to the technique’s broad application.2 The restoration is simple in concept and consists of one or more pontics supported by thin metal retainers bonded lingually and proximally to the enamel of the abutment teeth (Fig. 26-1). These conservative prostheses depend on bonding between etched enamel and the metal casting and require precise and defined metal engagement of the abutment. The early use of these bonded retainers tested the limits of its application. There was a limited understanding of the treatment planning required and of the degree of resistance and retention form necessary. In general use, poor design of the early retainers (with some bonded only to lingual enamel) was compounded by the difficulty of properly etching the metal. As a result, several failures occurred, and the technique was used more conservatively from 1986 to 1996. During and since that period, design parameters have been enumerated and tested clinically.3-5 Such designs, combined with new technologies for adhesive bonding of resin to most alloys, have led to a simpler, more reliable prosthetic procedure that complements the dentist’s prosthodontic armamentarium.

Fig. 26-1 A, Facial view of resin-bonded retainer replacing the right central incisor, which was lost as a result of trauma. B, Lingual view of the retainer. Note the extension of the retainer over the marginal ridges of both abutment teeth, which is an aspect of all designs for anterior retainers.
DEVELOPMENT OF RESIN-BONDED FIXED DENTAL PROSTHESES
Bonded Pontics
The earliest resin-bonded prostheses were extracted natural teeth or acrylic teeth used as pontics bonded to the proximal and lingual surfaces of abutment teeth with composite resin.6,7 The composite resin connectors were brittle and required supporting wire or a stainless steel mesh framework. These bonded pontics were limited to short anterior spans and had a limited lifetime, with degradation of the composite resin bond to the wire or mesh and subsequent fracture. Such restorations should be presented to patients only as short-term replacements.8-10
Cast Perforated Resin-Bonded Fixed Dental Prostheses (Mechanical Retention)
In 1973, Rochette1 introduced the concept of bonding metal to teeth by using flared perforations of the metal casting to provide mechanical retention. He used the technique principally for periodontal splinting but also included pontics in his design. Howe and Denehy11 recognized the metal framework’s improved retention (over bonded pontics) and began using FDPs with cast-perforated metal retainers bonded to abutment teeth and metal-ceramic pontics to replace missing anterior teeth. Their design recommendation, extending the framework to cover a maximum area of the lingual surface, suggested little or no tooth preparation. Patient selection limited these FDPs to mandibular teeth or situations with minimal occlusal contact. The restorations were bonded with a heavily filled composite resin as a luting medium.
This concept was expanded to replacement of posterior teeth by Livaditis.12 Perforated retainers were used to increase resistance and retention. Cast retainers were extended interproximally into the edentulous areas and onto occlusal surfaces. The design included a defined occlusogingival path of placement by tooth modification, which involved lowering the proximal and lingual height of contour of the enamel on the abutment teeth. These restorations were placed in normal occlusion; many have survived and have been seen on recall for up to 13 years (Fig. 26-2). Despite this success, the perforation technique presents the following limitations:

Fig. 26-2 Lingual view of an early perforated resin-bonded fixed dental prosthesis replacing a premolar at the 13-year recall. Note the loss of resin from the perforations, the poor gingival embrasures, and the generalized wear of the occlusal composite resin restoration on the molar abutment.
Clinical results with the perforated technique were monitored for 15 years in a study at the University of Iowa.14 The results from this well-controlled study suggest that for anterior FDPs, the perforated retainers have a 50% failure at 110 months and 63% at about 130 months (Table 26-1).
Table 26-1 ESTIMATE TIME TO 50% FAILURE (DEBONDINGS) IN STUDIES WITH AT LEAST 10-YEAR MEAN
| Study | Months to 50% failure |
|---|---|
| UNIVERSITY OF IOWA | |
| Perforated design | 110 |
| Etched metal* | 250 |
| UNIVERSITY OF MARYLAND | |
| Etched metal† | 190 |
* Boyer et al, 1993: 143 anterior and 30 posterior fixed dental prostheses (FDPs).14
† de Rijk et al, 1996: 61 anterior and 84 posterior FDPs.72
Etched Cast Resin-Bonded Fixed Dental Prostheses (Micromechanical Retention—“Maryland Bridge”)
A technique for the electrolytic etching of cast base metal retainers was developed at the University of Maryland by Thompson and Livaditis.2,15 Etched cast retainers have definite advantages over the cast-perforated restorations:
During the course of this work, the need for a composite resin with a low film thickness for luting the casting became apparent. This led to the first generation of resin cements, which allowed micromechanical bonding into the undercuts in the metal casting created by etching and simultaneously provided adequate strength and allowed complete seating of the cast retainers. Comspan,* the first of these cements, was moderately filled (60% by weight) with a film thickness of approximately 20 μm.16 Such cements are not chemically adhesive to the metal.
Electrolytic etching of base metal alloys proved to be critically dependent on the base metal alloy and attention to detail in the laboratory. Initial etching methods were developed for a nickel-chromium (Ni-Cr) alloy† and a nickel-chromium-molybdenum-aluminum-beryllium (Ni-Cr-Mo-Al-Be) alloy.17‡ These methods were followed by simplified techniques,18 chemical etching,19 or gel etching.20 They all yield similar results, provided that the technique is optimized for a specific alloy.21 Proper etching requires evaluation of the alloy surface with a scanning electron microscope. The degree of undercut created by this etching process can be seen in Figure 26-3. Lack of attention to detail can result in electropolishing or surface contamination.22 With time, both severely degrade bond strengths in a moist environment.
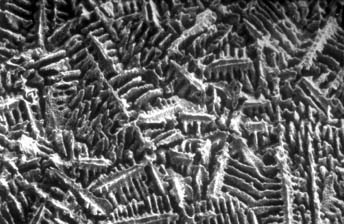
Fig. 26-3 Scanning electron micrograph (SEM) at 1000× magnification of a nickel-chromium-molybdenum-aluminum-beryllium (Ni-Cr-Mo-Al-Be) alloy electrolytically etched. The microstructure is selectively removed to create a highly undercut surface that can be wet by hydrophobic composite resins.
Highly variable results were reported for dental laboratories in etching the same alloy.23 Etching and bonding techniques were adopted on the basis of bond strength testing of specimens subjected to only 24 hours or 7 days of water exposure. When resin-to-metal test specimens were aged for 6 months in water and then thermally stressed by 10,000 or more thermal cycles, large reductions in bond strengths were recorded.24,25 Therefore, data from specimens that have not been aged and thermally stressed should be viewed skeptically. Even particle abrasion provides initially high resin-to-metal bonds, which can degrade to almost zero with time.26
Well-researched and tested resin systems for direct adhesion to metal surfaces have now completely supplanted metal etching as retention mechanisms.27 This is discussed subsequently.
Macroscopic Mechanical Retention Resin-Bonded Fixed Dental Prostheses (“Virginia Bridge”)
As a result of concerns about etching base metal and the desire to use alternative alloys, several methods have been developed to provide visible macroscopic mechanical undercuts on the inner surface of FDP retainers. The first was developed at the Virginia Commonwealth University School of Dentistry and is known as the Virginia Bridge.28 It involves a “lost salt crystal” technique. On the definitive cast, the abutments are coated with a model spray, and a lubricant is then applied. Within the outlines of the retainers, specially sized salt crystals* (150 to 250 μm) are sprinkled over the surface in a uniform monolayer, leaving a 0.5-mm border without crystals at the periphery of the pattern. This is followed by application of a resin pattern. After pattern investment, the salt crystals are dissolved from the surface of the pattern. Adequate bond strengths are possible with this method,29 but casting thickness must be increased to allow for the retention layer. Although no long-term results have been reported with this technique, it does allow the use of almost any metal-ceramic alloy. In general, however, macroscopic mechanical retention methods have been supplanted by direct adhesion with resin, which is possible for most casting alloys if the correct surface treatment is provided.
Chemical Bonding Resin-Bonded Fixed Dental Prostheses (Adhesion Bridges)
During the 1980s and early 1990s, when etched castings were the method of choice for retention of resin-bonded FDPs, extensive research was under way in Japan to develop adhesive systems for direct bonding of metal for this application. The first of these resin systems† is based on a formulation of a methyl methacrylate polymer powder and methyl methacrylate liquid modified with the adhesion promoter 4-methacryloxyethyl-trimellitic anhydride (4-META).30 It was developed with a unique tri-n-butylborane catalyst system that is added to the liquid before combining with the powder. On base metal alloys, Super-Bond has the highest initial bond strengths of any adhesive resin system. Unfortunately, the hydrolytic stability of these bonds over time depended on the alloy’s Cr-Ni ratio.31,32 Its advantages include its lower elastic modulus and higher fracture toughness in comparison with bisphenol-A-glycidyl dimethacrylate (bisGMA)–based resin cements,33,34 yielding better clinical results with less well-adapted castings.35 This system had shown poor clinical results with bonding high–gold content alloy retainers to abutment teeth.36 However, alloy primers have been developed that provide a more stable bond to noble alloy surfaces,37,38 which has been confirmed in a clinical study.39
Super-Bond’s introduction was followed by a bisGMA-based composite resin luting cement* that is modified with the adhesion promoter 10-methacryloxydecyl dihydrogen phosphate (MDP). MDP’s chemical structure and use are described in the literature.40
Panavia resin luting agent has shown excellent bonds to particle-abraded Ni-Cr and chromium-cobalt (Cr-Co) alloys41,42 as well as tin-plated gold and gold palladium-based alloys.21,43
Panavia has a tensile bond to etched enamel (10 to 15 MPa) comparable with that of the traditional bisGMA low-film thickness composites (e.g., Comspan and Conclude). The combination of metal electrolytic etching, followed by application of an adhesive such as Panavia, does not improve the tensile bond to the alloy, and its strength is actually slightly lower than that of the bond of Panavia to airborne particle abraded (sandblasted) base metal alloys.44 The most recent versions are Panavia 21 and Panavia F 2.0, the latter being a dual cure system (chemical and visible light) that releases fluoride. Both incorporate a self-etching primer system (ED Primer) for bonding to enamel and dentin.
Tin plating of noble alloys allows resin-to-metal bond tensile bond strengths only slightly lower than those for either the electrolytically etched or particle abraded Ni-Cr-Be alloys (18 to 30 MPa). However, tensile bond strengths are certainly greater than the bond to etched enamel.45,46 Tin plating of the metal surface also requires particle abrasion of the alloy surface just before bonding for adequate tin nucleation sites (Fig. 26-4).47,48 Tin plating can be completed in the dental laboratory, chairside, or intraorally to achieve metal bonding. One popular tin-plating system† (Fig. 26-5A) involves the use of a tin amide solution, which is applied to the metal surface with a saturated cotton pledget held on the end of a battery-powered probe (4 V). The probe is grounded elsewhere on the metal (Fig. 26-5B). Tin-plating times are usually 5 to 10 seconds, and a light gray surface is produced. Plating is followed by copious rinsing with water and drying; the adhesive resin is then applied.
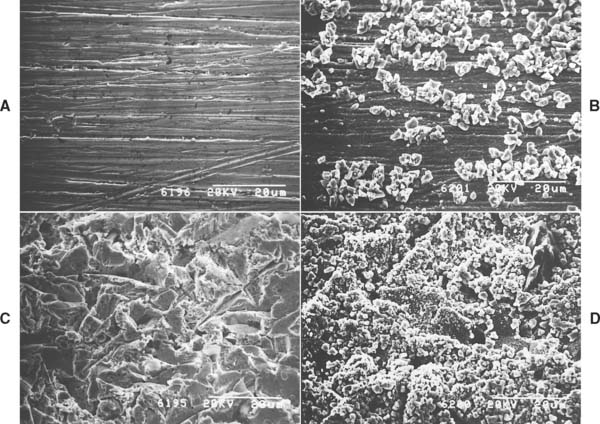
Fig. 26-4 Variations in tin-plating patterns with two surface treatments. A, Sandpaper (600 grit) prepared gold alloy (Firmilay, Jelenko, Armonk, New York) surface. B, Tin plating exhibiting local clumping and random distribution of tin particles. C, Gold alloy surface after 50 μm alumina particle abrasion. D, Particle-abraded gold alloy surface after tin plating with an even distribution of fine tin particles.

Fig. 26-5 Intraoral tin plating. A, Tin-plating system in which direct current is used to deposit tin from an amide solution (Tin Plater, Danville Engineerng, San Ramon, California). B, Tin plater in use intraorally. Note the gray color change. The tin is being deposited from the solution and carried to the metal in the cotton pledget affixed to one electrode of the plater; the circuit is completed with the alligator clip, which is in electrical contact with the prosthesis.
Particle abrasion of the alloy surface with 50 μm alumina before bonding or tin plating not only creates a roughened, higher surface area substrate for bonding but also creates a molecular coating of alumina.49 The alumina on the surface aids in oxide bonding of the phosphate-based adhesive systems (e.g., Panavia to alloy surfaces). Studies of this bonding mechanism are also reinforced by laboratory data on bonding to alumina and zirconia surfaces.50-52
These adhesive systems have now shown nearly the same degree of long-term clinical bonding (since 1983 in Japan) as the conventional composites on etched base metal (since 1981 in the United States).15 Laboratory data support their efficacy. The favorable findings for direct adhesion to base metal have rendered alloy etching and macroscopic retention mechanisms obsolete.53 This simplifies the laboratory and clinical procedures for placement of resin-bonded FDPs.
A laboratory method for resin bonding to both base and noble metal is the Rocatec System.* In this method, the metal surface is initially particle abraded with 120-μm alumina. This is followed by abrasion with a special silicate particle–containing alumina (Fig. 26-6). This second particle abrasion step deposits a molecular coating of silica and alumina on the alloy surface. Silane is then applied to the surface, making it adhesive to composite resin. Various silane application techniques have been compared by Norling and colleagues.54 The Rocatec system has been compared with Panavia for bonding to a range of surfaces and is adequate in this regard.25,27,49 However, it requires careful laboratory technique and is generally confined to bonding composite resin veneers to alloy castings because of the concern that the silane-treated surface may become contaminated before or during the clinical bonding procedures.
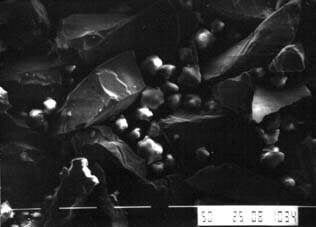
Fig. 26-6 Scanning electron micrograph of air abrasion particles (Rocatec Special, 3M ESPE, Norristown, Pennsylvania) composed of a mixture of 50-μm alumina (dark irregular particles) and smaller silicate particles (light color) used for final abrasion of metals, during which a molecular coating of silicate is tribochemically deposited on the metal. This silicate layer on the metal allows reaction with a silane-priming solution for subsequent bonding of resin to the metal.
Since the mid-1990s, several competing primer and cement systems for direct adhesive bonding to noble alloys have evolved (Table 26-2). All entail particle abrasion of the alloy surface, followed by application of a primer and then the resin cement. These primers have been studied in the laboratory55-59 and evaluated clinically.39,60 Their usage is justified and simplifies bonding to both gold- and palladium-based alloys.
Table 26-2 Adhesive Resin Cements and Primers for Noble Alloys
| Cement | Primer | Manufacturer |
|---|---|---|
| Bistite II DC | Metaltite | Tokyuyama Dental |
| CBMetabond | MTL-V Primer | Parkell Inc. |
| Linkmax | Metal Primer II | GC America |
| Multilink | Multilink Primer | Ivoclar Vivadent |
| Panavia 21 | Alloy Primer | Kuraray America |
| Self Adhesive Systems | ||
| Maxcem | Kerr Dental | |
| Rely X Unicem | 3M-ESPE | |
Changing the method of attachment of the resin to the metal framework does not change the design of the framework itself, because the limiting factor in the system is still the bond of resin to enamel. The evolution of Japanese designs for resin-bonded FDPs61 has paralleled that in North America and Europe. There is an almost universal agreement concerning the need for mechanical retention of the framework to limit the stress on the bond interfaces (resin-to-metal and resin-to-enamel) and in the composite resin, which can become fatigued with time.62-64
DESIGN CONCEPTS
The guidelines for optimum design of resin-retained FDPs have been empirically derived. The principle underlying these restorations has always been that it is necessary to cover as much enamel surface as possible, as long as occlusion, esthetics, or periodontal health is not compromised. To emphasize the significance of maximum enamel coverage, Crispin and associates65 reported 3-year failure rates of up to 50% when using small bonded areas and minimal retention designs.
The initial designs of etched cast retainers included an “interproximal wraparound” concept developed to resist occlusal forces and provide a broader area for bonding. Enamel preparations consisted of creating occlusal clearance, placement of occlusal/cingulum rests, and lowering the lingual and proximal height of contour, thus creating proximal extensions.
Frameworks should seat in an occlusogingival direction and should have no facial-lingual displacement (Fig. 26-7A). The contemporary design has improved retention with well-placed and precise grooves on abutment teeth (Fig. 26-7B). It is detailed in the following sections. Contemporary mouth preparations, in an effort to minimize failures, do not preserve as much tooth structure as did their predecessors; nevertheless, they are still limited to enamel and conform to conservative design principles. The new designs have been tested in laboratory studies.66,67
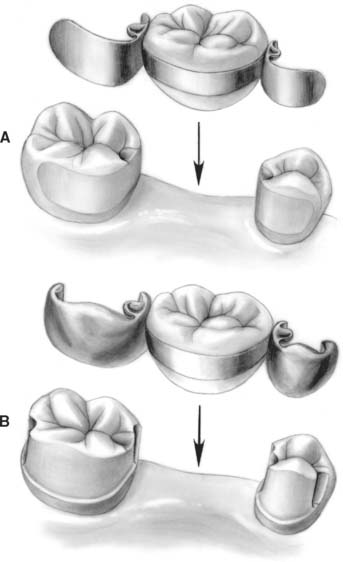
Fig. 26-7 Comparison of initial and contemporary posterior resin-bonded fixed dental prosthesis designs. A, Original design. Minimal modification of lingual and proximal enamel allowed sufficient buccal extension of the metal. Once seated, the retainer could not be displaced from buccal to lingual aspects. B, More extensive enamel preparation is now used with proximal grooves at the buccal-proximal line angles of the edentulous space. Note that with this design, the abutment teeth cannot be displaced from the retainer.
Three principles are fundamental to achieve predictable results with resin-bonded FDPs: proper patient selection, correct enamel modification, and framework design. The treatment is not a panacea, and if any of the contraindications are present, the patient should be treated with a conventional FDP or an implant-supported prosthesis.
ADVANTAGES
When used appropriately, resin-bonded FDPs offer several advantages over conventional fixed prosthodontics (Box 26-1). Because of the unique preparation design, minimal tooth structure needs to be removed. In general, the preparation is confined to enamel only. Because of the conservative nature of the preparation, the potential for pulpal trauma is minimized. Anesthesia is not routinely used during tooth preparation (without anesthesia, it is possible to monitor the proximity of the preparation to the dentoenamel junction by the patient’s comfort level). The prosthesis can often be kept entirely supragingival; as a result, periodontal irritation is kept to a minimum. In a periodontal evaluation of restorations that averaged 10 years in service, the periodontal response was not significantly different from that for unrestored contralateral teeth.68 Only when the retainer gingival margins were less than 0.5 mm from the gingival crest was there a correlation with a detrimental gingival response. Concurrently, impression making is simplified because of the supragingival margins. Because the abutment teeth are, in addition to being nonsensitive, maintained with normal proximal contacts, fabrication of traditional interim restorations (see Chapter 15) is usually not required other than in selected patients. However, judicious placement of composite resin is important for maintaining occlusal clearances after the final impression and until the final restoration is bonded.69 (see Fig. 26-14.) Chair time is significantly reduced in comparison with that for conventional fixed prosthodontics, and the cost incurred by the patient is lower. Both may be reduced by as much as 50%.70
Box 26-1 Advantages and Disadvantages of Resin-Bonded Fixed Dental Prostheses
ADVANTAGES
Minimal removal of tooth structure
Minimal potential for pulpal trauma
Anesthesia not usually required

Fig. 26-14 Temporary replacement of occlusal stops is crucial whenever they have been removed as a result of enamel recontouring. The composite resin stops shown here will be removed when this posterior inlay/onlay resin-bonded fixed dental prosthesis is bonded.
The restoration can be rebonded, in which particle abrasion and adhesive resin systems are used (as long as the debonding occurred with no sequelae involving the abutment teeth). If one retainer remains bonded, it can be gently loosened with a monobevel, single-ended instrument and a soft mallet. Any deformation of the metal framework in relation to the tooth structure can cause a crack to propagate through the luting composite resin. The monobevel chisel is positioned at an incisal or occlusal edge at an oblique angle to the long axis of the tooth along a mesial or distal line angle. The mallet should be used lightly (limited by patient response); repeated tapping causes debonding. However, with mechanically retentive designs, which include grooves and slots, the framework may require sectioning and removal of the sections (Fig. 26-8). As an alternative, ultrasonic scalers have been proposed to help remove partially debonded prostheses.69 Ultrasonic scalers with special tips are available for this specific purpose. They are applied at the incisal and gingival margins, but the procedure requires a high-power setting and can take considerable time. The debonding rate with rebonded restorations is high,71 and design modifications and a new or alternative restoration should be considered.

Fig. 26-8 Removal of a retainer with a contemporary design. A, The retainer has been sectioned with a carbide bur to allow separation of the mesial and distal retentive features. The monobevel chisel is oriented to provide a wedging action between the metal and the enamel, which allows a crack to propagate through the brittle resin. B, The cracking of the resin has propagated debonding between the metal and the resin. The mesial retainer half can now be removed in a similar manner. This retainer was removed because of fatigue fracture of the metal at the junction of the pontic metal with the premolar retainer arm (not shown), where the retainer was thinner than 1 mm. The poor periodontal support of the molar abutment allowed large lateral movements of the pontic and molar during function.
DISADVANTAGES
The primary disadvantage associated with resin-bonded FDPs relates to the fact that their longevity is less than that of conventional prostheses. This has been the subject of considerable investigation. Studies of first-generation etched metal FDPs at the University of Iowa (more anterior prostheses than posterior) and the University of Maryland (more posterior prostheses than anterior), with an average service time of more than 10 years, have revealed relative success. According to the results, an estimated 50% will fail after 250 months and 190 months, respectively (see Table 26-1).14,72,73 These studies also indicate that the rate of debondings does not increase with time.
In a study conducted in a private practice setting, contemporary designs with a mean service time of 6 years achieved a 93% success rate.3 This differs with the findings in a multicenter study in Europe, in which debonding rates increased with the time after placement (almost 50% at 5 years) and were related to preparation design, luting agent selection, and the area of placement within the dental arch.74 Another European study revealed retention rates of 60% at 10 years for early designs. In one study, posterior and mandibular resin-bonded FDPs demonstrated higher dislodgment rates,75 which may have resulted from occlusal forces (see Chapter 4) and increased isolation difficulty during the bonding procedure.71,76 In light of these studies, the likelihood of eventual debonding should be discussed with the patient before treatment. In comparison, a meta-analysis of clinical studies of conventional FDPs indicated a doubling of the failure rate for every 5 years of service from 0 to 15 years.77 When these results are projected from 15 years to 20 years, a 50% failure rate for conventional FDPs would take about 20 years.73
Extensive enamel modifications are required with retentive design to the proximal and lingual surfaces of the abutment teeth (see Fig. 26-7B). If the restoration is removed, composite resin bonding could restore the enamel contours, but transition to a more traditional prosthesis is likely. Enamel is limited in thickness, which requires precision in design and preparation with attention to detail.78 Enamel lingual surfaces of anterior teeth are almost always thinner than 0.9 mm.79
Space correction is difficult with resin-bonded FDPs. When the pontic space is greater or less than the dimensions of a normal tooth, achieving an esthetic result with this restoration is difficult. As with conventional fixed prostheses, treatment of diastemata is demanding, although a cantilever option may be appropriate.
Good alignment of abutment teeth is required because the prosthesis’s path of placement is limited by potential penetration of the enamel thickness. However, some posterior teeth, which are mesially or mesiolingually tilted, can be onlayed with a bonded retainer (see Figs. 26-18 and 26-20).
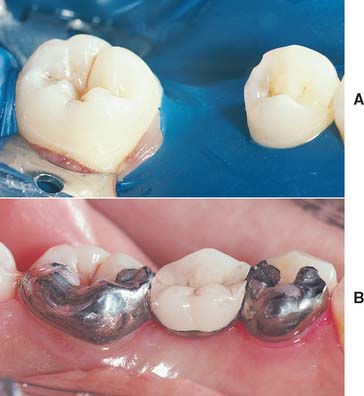
Fig. 26-18 A, Preparation for large premolar pontic. The first premolar has been prepared with mesial and distal rests and a distobuccal groove. B, The final restoration, which displays extensive metal on the occlusal surface of the premolar. This may be esthetically unacceptable for some patients.
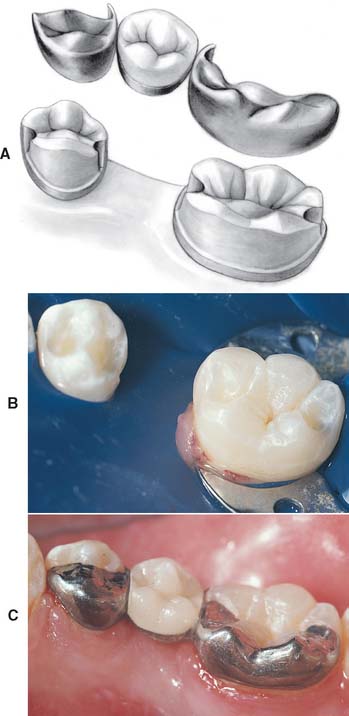
Fig. 26-20 A, Schematic of a resin-bonded fixed dental prosthesis onlay design. A thin veneer of metal is extended onto the occlusal surface of the teeth with approximately 0.5 mm reduction of the enamel where necessary. B, Preparation of molar and premolar. The lingual cusp of the premolar is covered to add additional mechanical retention on this short clinical crown. C, Completed restoration. The lingual cusps of the molar could also have been onlayed. However, the mesial and distal rests were deemed sufficient in this situation.
Esthetics is compromised on posterior teeth. Posterior resin-bonded FDP design requires the extension of the metal framework onto the occlusal surface of posterior teeth. These occlusal rests and occasional onlaying of cusps are visible, which might be objectionable to some patients (see Fig. 26-18).
Clinical indications and contraindications are quite specific. In the presence of any contraindications, a conventional FDP or an implant-supported crown should be considered.
INDICATIONS
In the treatment plan for any fixed prosthesis, the patient’s individual needs must be properly identified. The presence of any existing disease, its causes, and how it relates to the treatment prognosis must be assessed. Periodontal and general dental health must be reestablished, and the proposed abutment teeth should not exhibit mobility; however, periodontal splinting of teeth with a resin-retained FDP has been successful with strict provision of mechanical retention of each tooth within the alloy framework.
Resin-bonded restorations have been used for many years to replace missing anterior teeth in children (Fig. 26-9).11 Conventional fixed prosthodontic techniques are generally contraindicated in young patients because of management problems, inadequate plaque control, the large size of the pulps, and the fact that children routinely participate in sports. One or two anterior teeth with mesial and distal abutments can generally be replaced with a resin- bonded FDP. Depending on circumstances, a greater number of teeth can be involved.

Fig. 26-9 Resin-bonded fixed dental prostheses are particularly useful in the treatment of young patients with congenitally missing teeth. Note the unusual tooth pattern with the first premolar in the canine space and the missing lateral incisors.
Sound teeth or those with minimal restorations are suitable as an abutment with a resin-bonded retainer. For bonding to anterior teeth, the presence of Class III restorations is not a contraindication to a bonded retainer. However, large multiple restorations or a Class IV restoration would limit the resulting bond and the abutment’s mechanical integrity. In the posterior region, existing Class II lesions proximal to the edentulous space can be incorporated into the retainer design. Minimal or moderate alloy restorations in the abutment teeth should be replaced with dentin bonding and composite resin, or they can sometimes be incorporated into the preparation design. The incorporation of a mesio-occlusal amalgam into the retainer design, shown in Figure 26-10, was placed before the advent of high-strength dentin bonding systems. The appearance of the restoration at the 9-year recall appointment is also presented.

Fig. 26-10 A, Preparation for resin-bonded fixed dental prosthesis incorporating an existing amalgam restoration by use of a shallow inlay preparation, in which the amalgam reduction is short of the depth of the dentoenamel junction (with current dentin bonding technology, a composite resin base would be substituted for the amalgam). Note the shallow distal rest on the premolar and the lack of mesiolingual slot/groove preparation on the premolar abutment. B, Appearance of the restoration at 9-year recall appointment, in which luting resin is still present as a sealant in the molar lingual groove.
As demonstrated in clinical studies, single posterior teeth can be replaced with resin-bonded FDPs.3,72
Significant clinical crown length should be present to maximize retention and resistance form. In addition to replacing missing teeth, the resin-bonded prosthesis can be used for periodontal splinting and postorthodontic fixation.
The restorations may be used both anteriorly and posteriorly. However, excellent moisture control must be practiced during cementation.
Proper patient selection also requires an aggressive and ongoing follow-up program to detect debonding and the presence of caries resulting from debonding. However, caries rates on bonded retainers are low.80,81
CONTRAINDICATIONS
Because of the apparent advantages of resin-retained restorations, they have often been used in inappropriate circumstances, which led to failures that reduced patients’ (and dentists’) confidence in the technique. Fortunately, these failures were usually correctable by more conventional methods. If any of the following contraindications exist in a particular clinical situation, an alternative approach to treatment should be selected.
In patients with parafunctional habits, the use of resin-bonded FDPs should be considered cautiously, because the resistance to displacement of these retainers is lower than in conventional FDPs. They should be used judiciously when above-average lateral forces are likely to be applied (e.g., in a patient with parafunctional habits or in a patient who requires an anterior tooth replacement in the presence of an unstable or nonexistent posterior occlusion). In these instances, all means of mechanical retention of the framework (grooves, occlusal rests, interproximal extension of metal) (see Fig. 26-7B) should be used. The patient should be informed about the possibility of debonding. Periodontal splints can also be fabricated, but they require strict attention to mechanical retention.82,83
Long edentulous spans should be avoided because they place excessive force on the metal retention mechanism; with repeated loading, fatigue of the bonding interfaces or even the metal is possible.
Retention is dependent on an adequate surface area of enamel and sufficient clinical crown for proximal contouring and placement of grooves. This can be difficult if the abutment teeth have short clinical crowns (Fig. 26-11). Surgical crown lengthening may therefore be necessary as a way to increase the bondable surface area and because subgingival margins must be avoided.

Fig. 26-11 Minimal clinical crown length is available for adequate retention as a result of hyperplastic gingival tissue on the maxillary canines. Surgical crown lengthening is indicated.
Extensively restored or damaged teeth are unsuitable as abutments. One sound abutment and one extensively restored abutment can be incorporated into a combination FDP. In one retrospective clinical study with restorations in function for an average of more than 10 years, combination FDPs with one conventional retainer and one bonded retainer were very successful.84
Compromised enamel on abutment teeth as a result of hypoplasias, demineralizations, or congenital problems (e.g., amelogenesis imperfecta or dentinogenesis imperfecta) adversely affects resin bond strength.
As previously mentioned, edentulous spaces that are larger or smaller than normal tooth size or diastemas are not easily accommodated. The labiolingual thickness of anterior abutment teeth and translucency of the enamel should be assessed to determine whether the shade of the abutment teeth will be changed (a consequence of reduction of tooth translucency by the metal retainer85,86). Graying of the abutments can be eliminated with opaque resins and by limiting the incisal extent of the metal on the lingual surface. Translucent resins cause optical coupling of the metal to the tooth; appreciable graying of the enamel results. A trial insertion of the metal with water between the metal and the tooth provides a preview of the possible graying. Similarly, when the pontic of a resin-bonded FDP is custom stained, a trial resin that does not polymerize should be used to visualize the final shade of the abutment teeth with the metal backing (Fig. 26-12).

Fig. 26-12 A, Evaluation of resin-bonded fixed dental prosthesis for characterization of the pontic showing extensive graying of the central incisor abutment when translucent resin optically couples the dark metal to the tooth. B, Use of opaque resin prevents the darkening of the abutment and raises the value slightly. Opaque and translucent resins can be combined to provide the correct shade for the abutment; the pontic can then be characterized accordingly.
The presence of a deep vertical overlap prevents adequate enamel reduction and can place excessive forces on resin-bonded FDPs; this situation should be approached cautiously.
Nickel-based alloys have been the primary metal for resin-bonded FDPs. Patients who are allergic to nickel should be identified and offered an alternative.87 Tin plating and laboratory-applied bonding systems allow the use of noble alloys. However, with the lower elastic modulus of most noble alloys, the metal thickness should be increased approximately 30% to 50% to make the stiffness of the noble metal framework equal to that of base metal.88 This is an important factor in treatment planning and can influence the amount of occlusal clearance required for the metal (which is critical in patients with an increased vertical overlap).
FABRICATION
In the fabrication of resin-bonded FDPs, attention to detail in the following three phases is necessary for predictable success:
Preparation of the Abutment Teeth
Whether anterior or posterior teeth are prepared, common principles dictate tooth preparation design. A distinct path of placement must exist, proximal undercuts must be removed to provide “planes of metal” on the lingual and proximal surfaces, occlusal rest seats and proximal groove/slots must provide resistance form, and a definite and distinct gingival margin should be established wherever possible (Fig. 26-13).

Fig. 26-13 Preparation design for anterior resin retainer fixed dental prosthesis. Note the lowering of the height of contour in the interproximal, the slight extension of the metal toward the facial aspect (but not so much that it compromises esthetics), and the use of small but distinct proximal grooves.
On anterior teeth, the procedure is similar in many ways to the lingual reduction needed for a pinledge preparation (see Chapter 10), but the amount of reduction is less because the enamel must not be penetrated. If necessary, the opposing teeth can be recontoured to increase interocclusal clearance. There must be sufficient enamel area for successful bonding, and the metal retainers must encompass enough tooth structure and have sufficient resistance form to prevent the individual abutment tooth from being displaced in any direction out of the framework.
Rotary instrument selection depends on the operator’s preference. Gingival margins and circumferential preparation are easily accomplished with a chamfer or round-tipped diamond. Occlusal rest seats and cingulum notches can be prepared with a diamond or carbide inverted cone bur. The other crucial retentive features (e.g., slots, grooves) can be made with a tapered fissure bur.
The dentist should determine the restoration design before beginning tooth preparation. This may include surveying the abutment teeth and making diagnostic preparations on a cast.
Step-by-step procedure
Anterior Tooth Preparation and Framework Design
When designing the anterior prosthesis, use the largest possible surface area of enamel that will not compromise the esthetics of the abutment teeth. The retentive retainers (wings) should extend one tooth mesial and distal if a single tooth is replaced (Fig. 26-15). If two teeth are replaced, double abutments on either side can be considered, but only if the periodontal support of the abutments is compromised. With proper mechanically retentive designs, two maxillary incisor pontics can be retained by two lateral incisors, unless the latter have short clinical crowns or a deep vertical overlap is present. If a combination of tooth replacement and splinting is used, the framework may cover more teeth.

Fig. 26-15 Clinical view of an anterior prosthesis demonstrating the extent of coverage of the metal retainer, which forms planes on the mesial and distal lingual surfaces.
Cantilevering pontics with resin-bonded FDPs is also possible. This has been successful in selected situations in the anterior region89 and is particularly useful for replacement of lateral incisors for which cantilevers from either the central incisor or canine are possible. The retainer design is critical and requires adequate mechanical engagement of the abutment tooth.
The gingival margin should be designed so that there exists a slight supragingival chamfer that delineates the gingival extension of the preparation. Any undercut enamel is removed at this time. The chamfer finish line should extend incisally through the distal marginal ridge area so that mesial, lingual, and distal “planes” are created (see Fig. 26-15). Abutments should have parallel proximal surfaces whenever possible.
The finish line on the proximal surface, adjacent to the edentulous space, should be placed as far facially as practical. A 0.5-mm-deep slot, prepared with a tapered carbide bur, should be placed slightly lingual to the labial termination of the proximal reduction (Fig. 26-16). Great care in paralleling the proximal grooves is required. A paralleling instrument is very helpful during this procedure, and its importance has been demonstrated in highly successful clinical studies.4,5 This device is also helpful when many teeth are to be incorporated in the framework (e.g., an extensive periodontal splint).
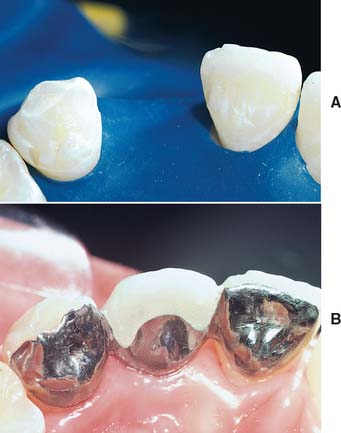
Fig. 26-16 A, Preparation design for an anterior prosthesis. Proximal grooves have been prepared on the mesial and distal surfaces of the abutment teeth. This mechanical retention is particularly important on the canine, where a distinct wear facet is seen. B, The gold alloy retainer is thicker than if a base metal alloy had been used. Note the extent of the metal into the canine distal proximal embrasure, whereas the central mesial extension has been limited because of the incisor diastema.
The occlusion is assessed to ensure at least 0.5 mm of interocclusal clearance for the metal retainers in maximum intercuspation and throughout the lateral and protrusive excursive pathways. If inadequate clearance exists, selective enameloplasty is performed. On occasion, additional clearance can be obtained by reducing the opposing teeth. However, this is contraindicated if there is wear or attrition on the incisal edges.
The restoration must extend labially past the proximal contact point. To optimize esthetics, the proximal wrap in the anterior region may be achieved in part with the porcelain pontic78,90 (see Fig. 26-15).
Preparation of mandibular anterior teeth is similar to that for the maxillary incisors. Lingual enamel thickness is 11% to 50% less than for maxillary teeth, and tooth preparation must therefore be more conservative.78,80 Periodontal splinting and combinations of splinting and tooth replacement are commonly used in the mandibular anterior region (Fig. 26-17). These present a challenge: providing mechanical retention can prove difficult.

Fig. 26-17 Mandibular anterior resin-bonded fixed dental prostheses. A, Note the inadequate abutment tooth lingual metal coverage and lack of extension into the proximal embrasures. A debonding is present on the right lateral incisor. B, A 10-year recall view, in which a more appropriate design has been employed.
Posterior Tooth Preparation and Framework Design
The basic framework for the posterior resin-bonded FDP consists of three major components: the occlusal rest (for resistance to gingival displacement), the retentive surface (for resistance to occlusal displacement), and the proximal wrap and proximal slots (for resistance to torquing forces) (see Fig. 26-7B).
A spoon-shaped occlusal rest seat, similar to that described for a partial removable dental prosthesis (see Chapter 21), is placed in the proximal marginal ridge area of the abutments adjacent to the edentulous space. An additional rest seat may be placed on the opposite side of the tooth (Fig. 26-18). The rest is an important retention feature and simultaneously provides resistance to both occlusal and lateral forces. It should be designed to function as a shallow “pin.”
To resist occlusal displacement, the restoration is designed to maximize the bonding area without unnecessarily compromising periodontal health or esthetics. Proximal and lingual axial surfaces are reduced to lower their height of contour to approximately 1 mm from the crest of the free gingiva. The proximal surfaces are prepared so that parallelism results without undercuts. In the interproximal area, a gingival chamfer is not desirable to avoid enamel penetration. The result is a knife-edge margin. Occlusally, the framework should be extended high on the cuspal slope, well beyond the actual area of enamel recontouring (provided that it does not interfere with the occlusion) (Fig. 26-19).
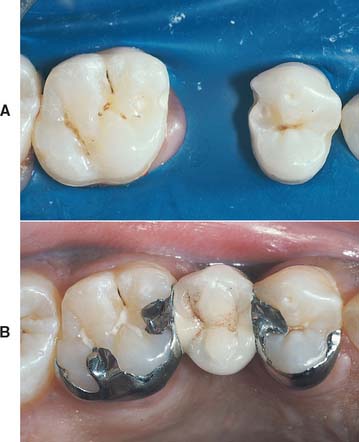
Fig. 26-19 A, Preparation for a maxillary premolar prosthesis. A groove has been placed at the mesial extension of the premolar retainer arm to eliminate the use of a mesial occlusal rest. This could compromise esthetics. Note that the lingual groove preparation on the molar extends gingivally as the preparation is carried down the buccal slope of the groove, which adds mechanical retention. B, The completed prosthesis.
Resistance to lingual displacement is more easily managed in the posterior region of the mouth. A single path of placement should exist. The alloy framework should be designed to engage at least 180 degrees of tooth structure when viewed from the occlusal aspect. This proximal wrap enables the restoration to resist lateral loading by engaging the underlying tooth structure and is assisted in this regard by grooves in the proximal aspect just lingual to the buccal line angle. Distal to the edentulous space, the retainer resistance is augmented by a groove at the lingual proximal line angle. Moving a properly designed resin-bonded FDP in any direction except parallel to its path of placement should not be possible, nor should it be possible to displace any tooth to the buccal aspect from the framework (see Figs. 26-7B, 26-18, and 26-19).
In general, preparation differs between maxillary and mandibular molar teeth only on the lingual surfaces. The lingual wall of the mandibular tooth may be prepared in a single plane. The lingual surface of the maxillary molars requires a two-plane reduction because of occlusal function and the taper of these functional cusps in the occlusal two thirds. However, the mandibular lingual retainer may be carried over the lingual cusps to augment resistance and retention form on short clinical crowns of mesially and lingually inclined molars (this may require a two-plane modification78,91) (Fig. 26-20).
A wide range of extensions of the casting onto the occlusal surfaces of posterior teeth is possible. They include shoeing of cusps, encircling of cusps, and extensions of metal through the central fossa from a mesial to distal direction with the lingual cusps exposed. The clinician is limited only by imagination, available enamel, occlusion, and the display of metal tolerated by the patient. Several examples of preparations and restorations are presented in Figures 26-21 and 26-22.
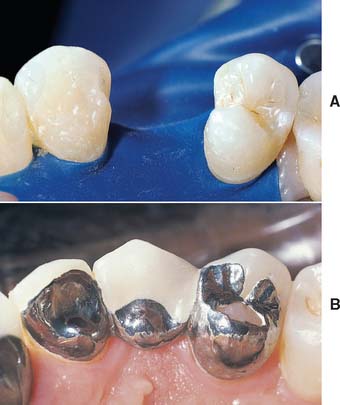
Fig. 26-21 A, Preparations for a premolar resin-bonded fixed dental prosthesis. The distal aspect of the canine had a small Class III composite resin restoration. This has been replaced and modified to create a distal slot for the retainer. The premolar has both mesial and distal occlusal rest preparations. B, Bonded prosthesis. The gingival margin of the restoration is very close to the free gingival crest (the ideal is 1 mm above the gingival crest). Meticulous plaque control is essential.

Fig. 26-22 A, Incorporation of an amalgam restoration into a resin-bonded fixed dental prosthesis (FDP). Note the margin placement at the gingival level, the use of two distal grooves, and a distinct gingival finish line on the canine abutment. B, Another completed resin-bonded FDP with an inlay component.
On occasion, a combination restoration can be used. This type of FDP includes a resin-bonded retainer on one of the abutment teeth and a conventional cast restoration on the other. As previously noted, this type of FDP has been very successful in clinical studies.84 Periodontal splinting is the most demanding of the restoration designs; splints and splint-FDP combinations require care in designing adequate mechanical retention. An example of multiple rest design with interproximal extension of the metal is shown in Figure 26-23. The posterior splint-FDP entails the use of multiple rests and distinct mechanical retention of the abutment in the retainer, which can be important when the abutment is the most distal tooth in the arch (Fig. 26-24). The anterior splint must engage as much enamel as possible to aid in retention (Fig. 26-25) and is more demanding in tooth alignment and preparation design.
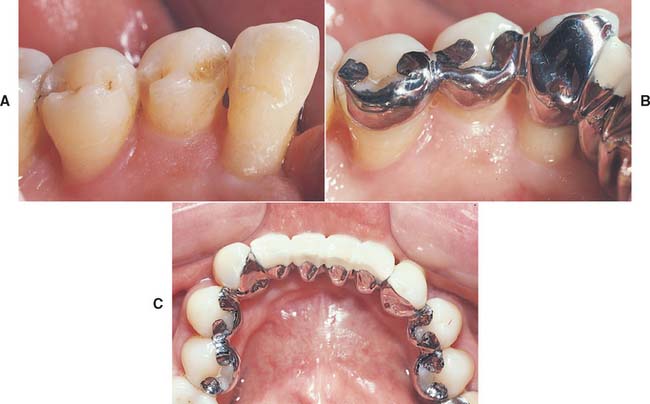
Fig. 26-23 A, One portion of the mandibular arch with teeth prepared as abutments for a resin-bonded splint replacing the mandibular incisors. Here both mesial and distal rests are used, in addition to extending the preparation into the proximal contact area. B, A bonded restoration. The extension to the second premolar was intended to help stabilize these mobile teeth, on the basis of a consultation with the periodontist. C, The completed restoration. The use of multiple rests on each posterior abutment is evident.


Laboratory Procedures
Bonding the Restoration
Cements (bonding agents)
Composite resins play an important role in bonding the metal framework to etched enamel. A variety of resin adhesives have been introduced specifically for this purpose. Conventional bisGMA-type resins (e.g., Comspan*) originally used for luting resin-bonded FDPs have been replaced by these more recently developed resin-metal adhesives, which continue to improve.
As mentioned earlier in this chapter, Panavia 21† is an adhesive monomer (MDP), a glass-filled bisGMA composite with a long history of successful application (Fig. 26-26B). Panavia 21 exhibits excellent bond strengths with base metal alloys and tin-plated noble metals. It has an anaerobic setting reaction and does not set in the presence of oxygen. To ensure a complete cure, the manufacturer provides a polyethylene glycol ge‡ that can be placed over the restoration margins. The gel creates an oxygen barrier and can be washed away after the material has completely set. The latest version of this luting agent§ is both chemically and light cured; as an alternative to the gel, a curing light can be used to polymerize the margins. Panavia 21 is supplied in opaque and tooth-colored (TC) forms. Because of the anaerobic setting reaction, both types can be mixed and do not set until air is excluded (as in seating of the restoration). This allows the application of opaque to the lingual aspect of an anterior retainer and the translucent tooth color to the interproximal aspect so that an opaque line is not visible from the facial aspect. Both types can be mixed ahead of time and applied to the bonding surfaces of the retainer at a convenient time (Fig. 26-26C). This method makes it possible to mask the unesthetic metallic gray retainer, thus preventing it from showing through translucent enamel.92

Fig. 26-26 Bonding procedures using an adhesive resin. A, Anterior resin-bonded fixed dental prosthesis preparation with mesial and distal groove retention based on the presence of incisal wear facets. Note the use of rubber dam for moisture control. B, Anaerobic-setting adhesive composite resin paste-dispensing system. C, Use of both opaque and translucent composite resin with the opaque on the lingual aspect and the translucent in the interproximal aspect for esthetics. D, The restoration has been seated, and the excess resin has been removed while the resin between the retainers and the enamel sets anaerobically. The margin resin and excess remain nonsetting. E, Oxygen-barrier gel is applied for margin resin setting. F, The final restoration, which was cast from a high–gold content alloy and tin plated. To provide good mechanical retention, the casting is increased in thickness by 50%, in comparison with a higher stiffness (elastic modulus) base metal alloy.
Step-by-Step Bonding Procedures
Step-by-step procedure with Panavia 21 resin adhesive cement
As for any adhesive luting system, the manufacturer’s instructions must be closely followed to maximize the cemented restoration’s physical properties (see Fig. 26-26).
POSTOPERATIVE CARE
All resin-bonded restorations should be scrutinized at the regular recall examinations (see Chapter 32). Because debonding or partial debonding can occur without complete loss of the prosthesis, visual examination and gentle pressure with an explorer should be performed to confirm such a complication. Because debonding is most commonly associated with biting or chewing hard food,94 patients should be warned about this danger. If the patient perceives any changes in the restoration, he or she should seek early attention. Early diagnosis and treatment of a partially debonded prosthesis can prevent significant caries (Fig. 26-27).94

Fig. 26-27 Maxillary three-unit, resin-bonded fixed dental prosthesis. The distal retainer became debonded, but this was not detected promptly, which resulted in a carious lesion.
The restoration can usually be rebonded successfully. The bonding surface should be cleaned with airborne particle abrasion and the enamel surface refreshed by careful removal of the remaining resin with rotary instruments, followed by etching. If a prosthesis debonds more than twice, reevaluating the preparation and remaking the prosthesis is probably necessary.
Attention to periodontal health is crucial, because this retainer design has the potential to accumulate excess plaque as a result of lingual overcontouring and the gingival extent of the margins.68 The patient should be taught appropriate plaque-control measures (see Chapter 32). Calculus removal is recommended with hand instruments over ultrasonic scalers to reduce the risk of debonding.
REVIEW OF TECHNIQUE
The following list summarizes the steps involved in preparation and placement of a resin-bonded FDP:
SUMMARY
One of the basic principles of tooth preparation for fixed prosthodontics is conservation of tooth structure. This is the primary advantage of resin-bonded FDPs. Precision and attention to detail are just as important in resin-bonded FDPs as they are in conventional prostheses. To provide a long-lasting prosthesis, the practitioner must plan and fabricate a resin-bonded restoration with the same diligence used for conventional restorations. The techniques can be very rewarding but must be approached carefully. Careful patient selection is an important factor in predetermining clinical success.
 GLOSSARY*
GLOSSARY*
ad·he·sion \ăd-hē′zhun\ n (1624) 1: the property of remaining in close proximity, as that resulting from the physical attraction of molecules to a substance or molecular attraction existing between the surfaces of bodies in contact 2: the stable joining of parts to each other, which may occur abnormally 3: a fibrous band or structure by which parts abnormally adhere—comp CAPSULAR FIBROSIS, FIBROUS A., INTRACAPSULAR A., MYOFIBROTIC CAPSULAR CONTRACTURE
airborne-particle abrasion \âr′bôrn′ pär′t -kal a-brā′zhun\: the process of altering the surface of a material through the use of abrasive particles propelled by compressed air or other gases
-kal a-brā′zhun\: the process of altering the surface of a material through the use of abrasive particles propelled by compressed air or other gases
antiflux \ăn′tē-flŭks′\ n: materials that prevent or confines solder attachment or flow
autopolymerizing resin \ô′tō-p l-a-m
l-a-m r-ī′zing rz′n\: a resin whose polymerization is initiated by a chemical activator
r-ī′zing rz′n\: a resin whose polymerization is initiated by a chemical activator
base metal \bās mt′l\: any metallic element that does not resist tarnish and corrosion—see NOBLE METAL
bond strength \bnd strngkth, strngth\: the force required to break a bonded assembly with failure occurring in or near the adhesive/adherens interface
bond·ing \bn′dng\ n (1976) 1: joining together securely with an adhesive substance such as cement or glue 2: the procedure of using an adhesive, cementing material or fusible ingredient to combine, unite, or strengthen 3: adhesive technique in dentistry involving conditioning of enamel and/or dentin so as to create tags in the tooth structure for mechanical retention of restorative material.
bonding agent \bn′dng ā′jent\: a material used to promote adhesion or cohesion between two different substances, or between a material and natural tooth structures
can·ti·lever \kăn′tl-ē′ver\ n (1667): a projecting beam or member supported on one end
cantilever fixed dental prosthesis \kăn′tl-ē′ver fkst dn′tl prs thē′sis\: a fixed dental prosthesis in which the pontic is cantilevered, i.e., is retained and supported only on one end by one or more abutments
cat·a·lyst \kăt′l-st\ n (1902): a substance that accelerates a chemical reaction without affecting the properties of the materials involved
1ce·ment \s-mnt\ n (14c) 1: a binding element or agent used as a substance to make objects adhere to each other, or something serving to firmly unite 2: a material that, on hardening, will fill a space or bind adjacent objects—syn luting agent
2ce·ment \s-mnt\ vt (15c): to unite or make firm by or as if by cement; to lute
ce·men·ta·tion \s′mn-tā′shun\: 1: the process of attaching parts by means of a cement 2: attaching a restoration to natural teeth by means of a cement (GPT-4)
1etch \ch\ vb, vt (1634) la: to produce a retentive surface, especially on glass or metal, by the corrosive action of an acid lb: to subject to such etching 2: to delineate or impress clearly
2etch \ch\ n (1896) 1: the effect or action of an etching acid on a surface 2: a chemical agent used in etching
etch·ant \ch′ănt\ n: an agent that is capable of etching a surface
etch·ing \ch′ing\ vt (1632) 1: the act or process of selective dissolution 2: in dentistry, the selective dissolution of the surface of tooth enamel, metal, or porcelain through the use of acids or other agents (etchants) to create a retentive surface
groove \grōōv\ n: a long narrow channel or depression, such as the indentation between tooth cusps or the retentive features placed on tooth surfaces to augment the retentive characteristics of crown preparations
guiding planes\ gī′dng plānz\: vertically parallel surfaces on abutment teeth or/and dental implant abutments oriented so as to contribute to the direction of the path of placement and removal of a removable partial denture
1lute \lōōt\ n (15c): a substance, such as cement or clay, used for placing a joint or coating a porous surface to make it impervious to liquid or gas—see CEMENT
2lute \lōōt\ vt; lut·ed \lōō′td\; lut·ing \lōō′tng\: to fasten, attach, or seal—see CEMENT
noble metal \nō′bal mt′l\: those metal elements that resist oxidation, tarnish, and corrosion during heating, casting, or soldering and when used intraorally; examples include gold and platinum—comp BASE METAL
nonprecious metal: see BASE METAL
par·al·lel·o·me·ter \păr′a-l-lm′-tar\ n 1: an instrument used for determining the exact parallel relationships of lines, structures, and surfaces in dental casts and prostheses 2: an apparatus used for making one object parallel with another object, as in paralleling attachments and abutments for fixed dental prostheses or precision attachments for removable partial dentures
precious metal alloy \prsh′as mt′l ăl′oi′, a-loi′\: an alloy predominantly composed of elements considered precious, i.e., gold, the six metals of the platinum group (platinum, osmium, iridium, palladium, ruthenium, and rhodium), and silver
res·in \rz′n\ n (14c) 1: any of various solid or semisolid amorphous natural organic substances that usually are transparent or translucent and brown to yellow; usually formed in plant secretions; are soluble in organic solvents but not water; are used chiefly in varnishes, inks, plastics, and medicine; and are found in many dental impression materials 2: a broad term used to describe natural or synthetic substances that form plastic materials after polymerization. They are named according to their chemical composition, physical structure, and means for activation of polymerization—see AUTOPOLYMERIZING R, COPOLYMER R.
resin-bonded prosthesis \rz′n-bn′dd prs-thē′ss\: a fixed dental prosthesis that is luted to tooth structures, primarily enamel, which has been etched to provide mechanical retention for the resin cement. Early design incorporated perforations on the lingual plate (Rochette Bridge) through which the resin bonded material passed to achieve a mechanical lock; subsequently, use of acid etching of the metal plate (Maryland Bridge) eliminated the need for perforations.
Rochette, Alain L. Attachment of a splint to enamel of lower anterior teeth J Pros Dent 1973; 30: 418–423.
Livaditis, GJ, Thompson, VP.: Etched castings: an improved retentive mechanism for resin-bonded retainers J Pros Dent 1982; 47–52
resin-bonded splint \rz′n bn′dd splnt\: a fixed splint made of heavy wire, fibrous resin materials or/and cast metal that is bonded to the labial or lingual surface of natural teeth with an acid etch technique. It is used to stabilize traumatically displaced or periodontally compromised teeth
resistance form \r-zs′tans form\: the features of a tooth preparation that enhance the stability of a restoration and resist dislodgment along an axis other than the path of placement
re·tain·er \r-tā′nar\ n (1540): any type of device used for the stabilization or retention of a prosthesis—see DIRECT R., FIXED PARTIAL DENTURE R., INDIRECT R.
re·ten·tion \r-tn′shun\ n (15c): that quality inherent in the dental prosthesis acting to resist the forces of dislodgment along the path of placement—see DIRECT R, INDIRECT R.
retention form \r-tn′shun form\: the feature of a tooth preparation that resists dislodgment of a crown in a vertical direction or along the path of placement
Rochette Bridge [Alain L. Rochette, French physician and dentist]: a resin-bonded fixed dental prosthesis incorporating holes within the metal framework and lutes to the lingual aspect of teeth adjacent to an edentulous space that replaces one or more teeth—see RESIN-BONDED PROSTHESIS
Rochette, Alain L. Attachment of a splint to enamel of lower anterior teeth JPD 1973; 30:418–23
semiprecious metal alloy \sm′ē-prsh′as mt′l ăl′oi′, a-loi′\: an alloy composed of precious and base metals. There is no distinct ratio of components separating semiprecious alloys from another group
span length \spăn lngkth\: the length of a beam between two supports
1un·der·cut \ŭn′dur-kŭt\ n (1859) 1: the portion of the surface of an object that is below the height of contour in relationship to the path of placement 2: the contour of a cross-sectional portion of a residual ridge or dental arch that prevents the insertion of a prosthesis 3: any irregularity in the wall of a prepared tooth that prevents the withdrawal or seating of a wax pattern or casting
2un·der·cut \ŭn′dur-kŭt\ v (ca. 1598): to create areas that provide mechanical retention for materials placement
STUDY QUESTIONS
1 Rochette A. Attachment of a splint to enamel of lower anterior teeth. J Prosthet Dent. 1973;30:418.
2 Livaditis G, Thompson VP. Etched castings: an improved retentive mechanism for resin-bonded retainers. J Prosthet Dent. 1982;47:52.
3 Barrack G, et al. A long-term prospective study of the etched-cast restoration. Int J Prosthodont. 1993;6:428-434.
4 Brabant A. Indication and design: the key to successful resin-bonded fixed partial dentures. In: Degrange M, Roulet J-F, editors. Minimally Invasive Restorations with Bonding. Chicago: Quintessence Publishing; 1997:201-210.
5 Marinello CP, et al. Resin-bonded fixed partial dentures and extracoronal attachments for removable partial dentures. In: Degrange M, Roulet J-F, editors. Mininally Invasive Restorations with Bonding. Chicago: Quintessence Publishing; 1997:221-240.
6 Ibsen R. Fixed prosthetics with a natural crown pontic using an adhesive composite. J South Calif Dent Assoc. 1973;41:100.
7 Portnoy J. Constructing a composite pontic in a single visit. Dent Surv. 1973;39:30.
8 Heymann H. Resin-retained bridges: The natural-tooth pontic. Gen Dent. 1983;31:479.
9 Heymann H. Resin-retained bridges: The acrylic denture-tooth pontic. Gen Dent. 1984;32:113.
10 Jordan R, et al. Temporary fixed partial dentures fabricated by means of the acid-etch resin technique: a report of 86 cases followed for up to three years. J Am Dent Assoc. 1978;96:994.
11 Howe D, Denehy GE. Anterior fixed partial dentures utilizing the acid-etch technique and a cast metal framework. J Prosthet Dent. 1977;37:28.
12 Livaditis G. Cast metal resin-bonded retainers for posterior teeth. J Am Dent Assoc. 1980;101:926.
13 Williams VD, et al. The effect of retainer design on the retention of filled resin in acid-etched fixed partial dentures. J Prothet Dent. 1982;48:417.
14 Boyer DB, et al. Analysis of debond rates of resin-bonded prostheses. J Dent Res. 1993;72:1244.
15 Thompson VP, et al. Resin bond to electrolytically etched non-precious alloys for resin bonded prostheses. J Dent Res. 1981;60:377.
16 Levine W. An evaluation of the film thickness of resin luting agents. J Prosthet Dent. 1989;62:175.
17 Livaditis GJ, et al. Etched casting resin bonded retainers, Part 1: Resin bond to electrolytically etched non-precious alloys. J Prosthet Dent. 1983;50:771.
18 McLaughlin G, et al. Comparison of bond strengths using one-step and two-step alloy etching techniques. J Prosthet Dent. 1985;53:516.
19 Livaditis G. A chemical etching system for creating micromechanical retention in resin-bonded retainers. J Prosthet Dent. 1986;56:181.
20 Doukoudakis A, et al. A new chemical method for etching metal frameworks of the acid-etched prosthesis. J Prosthet Dent. 1987;58:421.
21 Re G, et al. Shear bond strengths and scanning electron microscope evaluation of three different retentive methods for resin-bonded retainers. J Prosthet Dent. 1988;59:568.
22 Wiltshire WA. Tensile bond strengths of various alloy surface treatments for resin bonded bridges. Quintessence Dent Technol. 1986;10:227.
23 Sloan KM, et al. Evaluation of laboratory etching of cast metal resin-bonded retainers [Abstract no. 1220]. J Dent Res. 1983;63:305.
24 Kern M, et al. Influence of prolonged thermal cycling and water storage on the tensile bond strength of composite to NiCr alloy. Dent Mater. 1994;10:19.
25 Kern M, et al. Durability of resin bonds to a cobalt-chromium alloy. J Dent. 1995;23:47.
26 Thompson VP, et al. [Bonded bridge technics: electrolytic etching of NiCr alloy]. Dtsch Zahnarztl Z. 1986;41:829.
27 Ozcan M, et al. A brief history and current status of metal-and ceramic surface-conditioning concepts for resin bonding in dentistry. Quintessence Int. 1998;29:713.
28 Moon P. Resin bonded bridge tensile bond strength utilizing porous patterns. J Dent Res. 1984;63:320.
29 Moon P. Bond strengths of the lost salt procedure: a new retention method for resin-bonded fixed prostheses. J Prosthet Dent. 1987;57:435.
30 Masuhara E. A Dental Adhesive and Its Clinical Application. Tokyo: Quintessence, 1982.
31 Ohno H, et al. The adhesion mechanism of dental adhesive resin to alloy—relationship between Co-Cr alloy surface structure analyzed by ESCA and bonding strength of adhesive resin. Dent Mater. 1986;5:46.
32 Salonga JP, et al. Bond strength of adhesive resin to three nickel-chromium alloys with varying chromium content. J Prosthet Dent. 1994;72:582.
33 Asmussen E, et al. Adherence of resin-based luting agents assessed by the energy of fracture. Acta Odontol Scand. 1993;51:235.
34 Northeast SE, et al. Tensile peel failure of resin-bonded Ni/Cr beams: an experimental and finite element study [see comments]. J Dent. 1994;22:252.
35 Degrange M, et al. Bonding of luting materials for resin-bonded bridges: clinical relevance of in vitro tests. J Dent. 1994;22:S28.
36 Hannsson O. Clinical results with resin-bonded prostheses and an adhesive cement. Quintessence Int. 1994;25:125.
37 Matsumura H, et al. Adhesive bonding of noble metal alloys with a triazine dithiol derivative primer and an adhesive resin. J Oral Rehabil. 1999;26:877.
38 Matsumura H, et al. Bonding of silver-palladium-copper-gold alloy with thiol derivative primers and tri-n-butylborane initiated luting agents. J Oral Rehabil. 1997;24:291.
39 Hikage S, et al. Clinical longevity of resin-bonded bridges bonded using a vinyl-thiol primer. J Oral Rehabil. 2003;30:1022.
40 Yamashita A. A Dental Adhesive and Its Clinical Application. Tokyo: Quintessence, 1983.
41 Omura I, et al. Adhesive and mechanical properties of a new dental adhesive. J Dent Res. 1984;63:233.
42 Tjan A, et al. Bond strength of composite to metal mediated by metal adhesive promoters. J Prosthet Dent. 1987;57:550.
43 Imbery TA, et al. Tensile strength of three resin cements following two alloy surface treatments. Int J Prosthodont. 1992;5:59.
44 Thompson V. Cast-bonded retainers. In: Wei SHY, editor. Textbook of Pediatric Dentistry: Total Patient Care. Philadelphia: Lea & Febiger; 1988:233-245.
45 Breeding LC, et al. The effect of metal surface treatment on the shear bond strengths of base and noble metals bonded to enamel. J Prosthet Dent. 1996;76:390.
46 Dixon DL, et al. Shear bond strengths of a two-paste system resin luting agent used to bond alloys to enamel. J Prosthet Dent. 1997;78:132.
47 Bertolotti RL, et al. Intraoral metal adhesion utilized for occlusal rehabilitation. Quintessence Int. 1994;25:525.
48 Wood M, et al. Repair of porcelain/metal restoration with resin bonded overcasting. J Esthet Dent. 1992;4:110.
49 Kern M, et al. Effects of sandblasting and silica-coating procedures on pure titanium. J Dent. 1994;22:300.
50 Kern M, et al. Bonding to alumina ceramic in restorative dentistry: clinical results over up to 5 years. J Dent. 1998;26:245.
51 Kern M, et al. Sandblasting and silica-coating of dental alloys: volume loss, morphology and changes in the surface composition. Dent Mater. 1993;9:151.
52 Kern M, et al. Bonding to zirconia ceramic: adhesion methods and their durability. Dent Mater. 1998;14:64.
53 Barrack G. A look back at the adhesive resin-bonded cast restoration. J Esthet Dent. 1995;7:263.
54 Norling B, et al. Resin-metal bonding via three silica deposition processes [Abstract no. 993]. J Dent Res. 1991;70:390.
55 Yoshida K, et al. Effects of adhesive primers on bond strength of self-curing resin to cobalt-chromium alloy. J Prosthet Dent. 1997;77:617.
56 Aguilar LT, et al. Tensile bond strength of adhesive systems—effects of primer and thermocycling. Pesqui Odontol Bras. 2002;16:37.
57 Matsumura H, et al. Evaluation of two thione primers and composite luting agents used for bonding a silver-palladium-copper-gold alloy. J Oral Rehabil. 2002;29:842.
58 Shimizu H, et al. Use of metal conditioners to improve bond strengths of autopolymerizing denture base resin to cast Ti-6Al-7Nb and Co-Cr. J Dent June. 30, 2005. (Epub)
59 Watanabe I, et al. Shear bond strengths of laboratory-cured prosthetic composite to primed metal surfaces. Am J Dent. 2003;16:401.
60 Chadwick RG, et al. A retrospective observational study of the effect of surface treatments and cementing media on the durability of gold palatal veneers. Oper Dent. 2004;29:608.
61 Yamashita A, et al. Adhesion bridge background and clinical procedure. In: Gettleman L, et al, editors. Adhesive Prosthodontics: Adhesive Cements and Techniques. Nijmegen, The Netherlands: Eurosound; 1988:61-76.
62 Aquilino S, et al. Tensile fatigue limits of prosthodontic adhesives. J Dent Res. 1991;70:208.
63 Saunders W. The effect of fatigue impact forces upon the retention of various designs of resin-retained bridgework. Dent Mater. 1987;3:85.
64 Zardiakas L, et al. Tensile fatigue of resin cements to etched metal and enamel. Dent Mater. 1988;4:163.
65 Crispin B, et al. Etched metal bonded restoration: three years of clinical follow-up. J Dent Res. 1986;65:311.
66 el Salam Shakal MA, et al. Effect of tooth preparation design on bond strengths of resin-bonded prostheses: a pilot study. J Prosthet Dent. 1997;77:243.
67 Pegoraro LF, et al. A comparison of bond strengths of adhesive cast restorations using different designs, bonding agents, and luting resins. J Prosthet Dent. 1987;57:133.
68 Romberg E, et al. 10-Year periodontal response to resin bonded bridges. J Periodontol. 1995;66:973.
69 Krell KV, et al. Ultrasonic debonding of anterior etched-metal resin bonded retainers. Gen Dent. 1986;34:378.
70 Creugers NH, et al. A method to compare cost-effectiveness of dental treatments: adhesive bridges compared to conventional bridges. Community Dent Oral Epidemiol. 1992;20:280.
71 Creugers NH, et al. Risk factors and multiple failures in posterior resin-bonded bridges in a 5-year multi-practice clinical trial. J Dent. 1998;26:397.
72 de Rijk WG, et al. Maximum likelihood estimates for the lifetime of bonded dental prostheses. J Dent Res. 1996;75:1700.
73 Thompson VP, et al. Longevity of resin-bonded fixed partial dentures: better than conventional fixed restorations? In: Degrange M, Roulet J-F, editors. Minimally Invasive Restorations with Bonding. Chicago: Quintessence Publishing; 1997:185-200.
74 Creugers NH, et al. Long-term survival data from a clinical trial on resin-bonded bridges. J Dent. 1997;25:239.
75 De Kanter RJ, et al. A five-year multi-practice clinical study on posterior resin-bonded bridges. J Dent Res. 1998;77:609.
76 Olin PS, et al. Clinical evaluation of resin-bonded bridges: a retrospective study. Quintessence Int. 1991;22:873.
77 Creugers NHJ, et al. A meta-analysis of durability on conventional fixed bridges. Community Dent Oral Epidemiol. 1994;22:448.
78 Eshleman J, et al. Tooth preparation designs for resin-bonded fixed partial dentures related to enamel thickness. J Prosthet Dent. 1988;60:18.
79 Shillingburg HT, et al. Thickness of enamel and dentin. J South Calif Dental Assoc. 1973;41:33.
80 Djemal S, et al. Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil. 1999;26:302.
81 Wood M, et al. Resin-bonded fixed partial dentures. II. Clinical findings related to prosthodontic characteristics after approximately 10 years. J Prosthet Dent. 1996;76:368.
82 Marinello CP, et al. Experiences with resin-bonded bridges and splints—a retrospective study. J Oral Rehabil. 1987;14:251.
83 Marinello CP, et al. First experiences with resin-bonded bridges and splints—a cross-sectional retrospective study, Part II. J Oral Rehabil. 1988;15:223.
84 Wood M, et al. Ten-year clinical and microscopic evaluation of resin-bonded restorations. Quintessence Int. 1996;27:803.
85 Simonsen R, et al. Etched Cast Restorations: Clinical and Laboratory Techniques. Chicago: Quintessence Publishing, 1983.
86 Wood M, et al. Adhesive resin bonded cast restorations. In: Dale BG, Aschheim KW, editors. Esthetic Dentistry: A Clinical Approach to Techniques and Materials. Philadelphia: Lea & Febiger; 1992:151-162.
87 Blanco-Dalmau L. The nickel problem. J Prosthet Dent. 1982;48:99.
88 Nakabayashi N, et al. Relationship between the shape of adherend and the bond strength. Jpn J Dent Mater. 1987;6:422.
89 Briggs P, et al. The single unit, single retainer, cantilever resin-bonded bridge. Br Dent J. 1996;181:373.
90 Simonsen R, et al. General considerations in the framework design and tooth modification. Quintessence Dent Technol. 1983;7:21.
91 Simonsen R, et al. Posterior design principles in etched cast restorations. Quintessence Int. 1983;3:311.
92 Caughman WF, et al. A double-mix cementation for improved esthetics of resin-bonded prostheses. J Prosthet Dent. 1987;58:48.
93 Caughman W, et al. The effect of finishing resin-bonded fixed partial dentures on postcementation tensile strength. J Prosthet Dent. 1988;59:149.
94 Gilmour ASM. Resin bonded bridges: a note of caution. Br Dent J. 1988;167:140.